Investigation summary
What happened
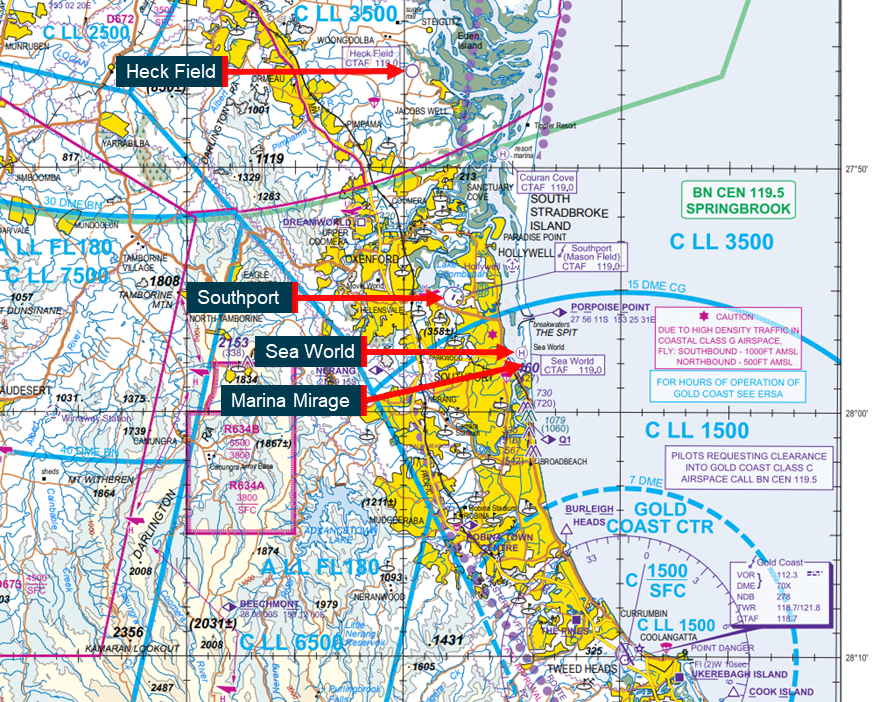
On 2 January 2023, 2 EC130 B4 helicopters registered VH‑XH9 and VH-XKQ were conducting scenic flights from the Sea World theme park on the Gold Coast, Queensland. A pilot and 5 passengers were on board VH‑XH9, and a pilot and 6 passengers were on board VH‑XKQ.
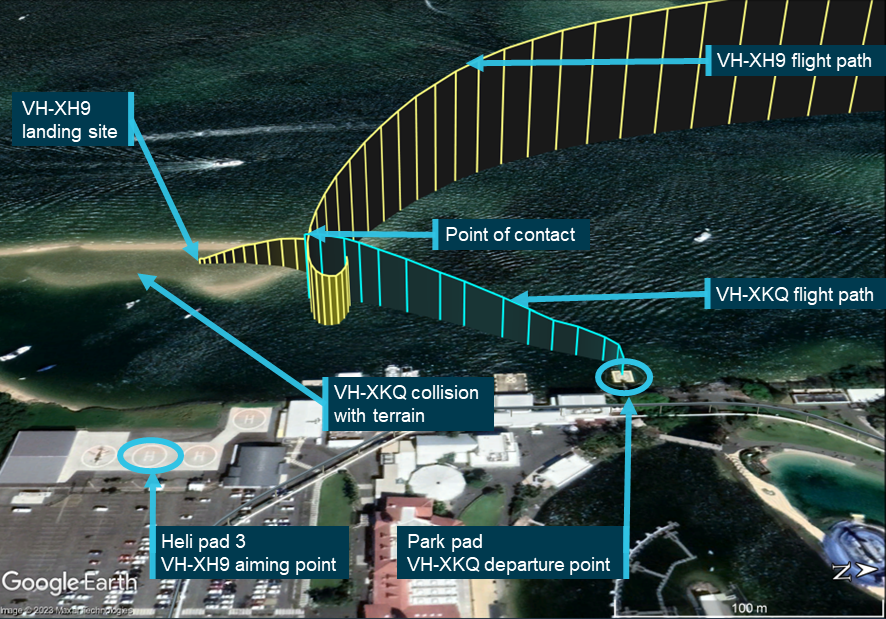
After conducting concurrent scenic flights throughout the day, at 1356:06 the helicopters collided at a height of 130 ft, around 155 m west-north‑west of the Sea World Helicopters heliport.
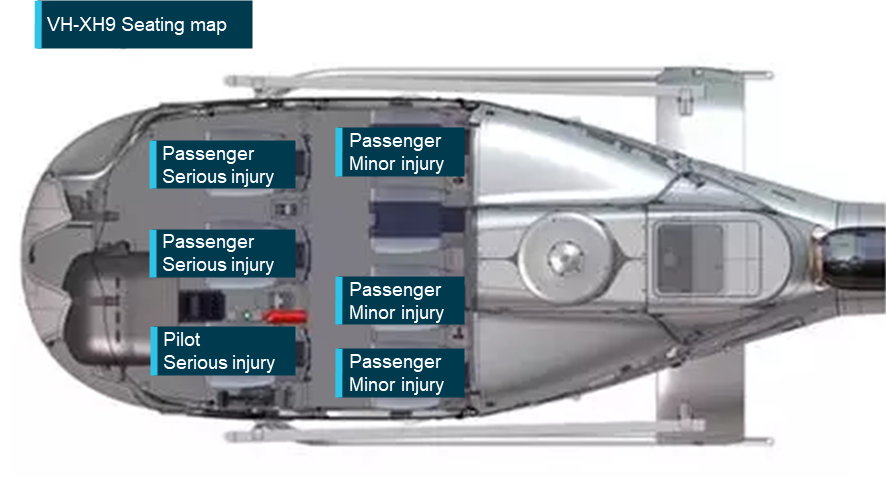
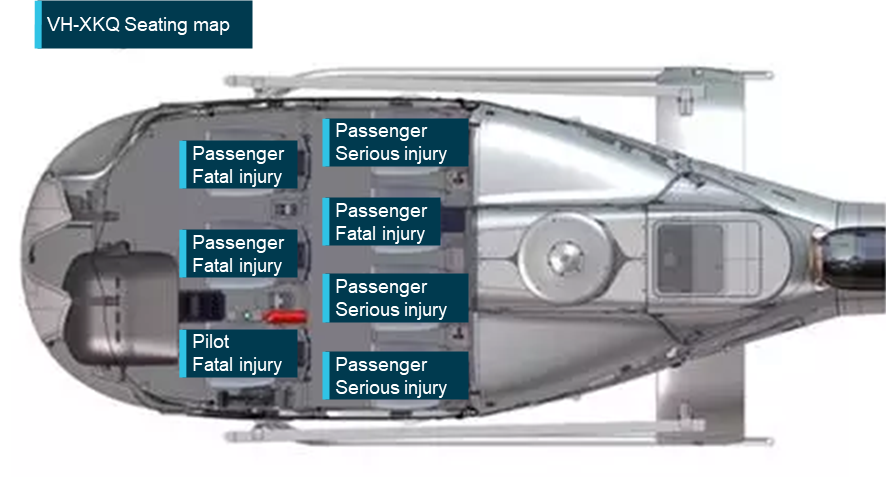
Following the collision, VH‑XKQ was uncontrollable and fell to the ground. The pilot and 3 passengers were fatally injured, 3 passengers were seriously injured, and the helicopter was destroyed. VH‑XH9 was substantially damaged from the collision, but the pilot made a controlled landing. The pilot and 2 passengers were seriously injured, and 3 passengers had minor injuries.
What the ATSB found
The accident occurred a week after the operator started using 2 EC130 B4 helicopters for its scenic flights. The pilots were conducting scenic flights in good weather, concurrently from 2 nearby helipads.
On the accident flight, an inbound call from VH‑XH9 failed to register with the pilot of VH‑XKQ, who was loading passengers at the time. Advice of clear airspace provided by the ground crew of VH‑XKQ was obsolete by the time of departure. The pilot of VH‑XH9, inbound, elected to wait for a taxi call from the pilot of VH‑XKQ as a cue to arrange separation. Neither pilot was aware of the existence of faults in the radio of VH‑XKQ that likely prevented broadcast of the taxi call.
Visibility was limited for the pilot of VH‑XKQ (departing helicopter) by restrictions on manoeuvring at the park pad and the angles of closure of the helicopters. The pilot of VH‑XH9 had sighted VH‑XKQ on the park pad and discarded that traffic as a threat, expecting to be alerted by the taxi call if that condition changed. Neither pilot had further information to target their search for the other helicopter.
The location required both pilots to manage separation from vessels on the water, with VH‑XKQ passing to the west and VH‑XH9 passing to the north of the same vessel. Additionally, VH‑XKQ had to check a second known conflict point, Sea World grass, for traffic, while VH‑XH9 had to manage their approach to the heliport.
Limitations in visibility from both helicopters and especially VH‑XKQ, combined with competing priorities and an understanding that the airspace was clear, led to a midair collision as both helicopters were passing through the conflict point created by the positioning of the helipads.
The operator had made changes to the location, facilities and helicopters to improve its product offering, and these changes brought unintended consequences. Over time these changes undermined risk controls used for management of separation and created the conflict point at which the helicopters collided. The unintended consequences were uncontrolled because the operator’s safety management system did not effectively manage aviation safety risk, and change management was incomplete or absent.
The operator’s procedures for scenic flights were not wholly specific to their operation and introduced variability in pilot decision‑making and conduct of the scenic flights. Additionally, the operator’s system of radio calls, hand signals and conspicuity devices, intended to warn pilots of the presence of another helicopter, was flawed. As a result, both pilots formed an incorrect understanding about the location of the other helicopter.
Passengers on board VH-XH9 and VH‑XKQ were incorrectly restrained. The ATSB was unable to determine the level of contribution of incorrect restraint to passengers’ injuries. However, sufficient research and knowledge of seatbelts exists to demonstrate that correct fitment improves outcomes for occupants of aircraft in the event of an accident.
The regulations required the passengers to be fitted with constant wear lifejackets in addition to the seatbelts in the helicopter. There has been no testing or verification of the ability of these 2 safety devices to be integrated while maintaining the integrity of each. As a result, helicopter tourism operations worldwide are fitting seatbelts incorrectly when combined with constant wear lifejackets.
What has been done as a result
Sea World Helicopters Pty Ltd
Sea World Helicopters (SWH) reviewed its processes and procedures with reference to other high intensity operations undertaken by the group (such as aerial firefighting and low-level power line operations). Following that review it implemented:
- updated job hazard analysis for scenic flight and operations from both helipads
- a new position of ‘Pad Boss’, trained ground staff acting in a traffic advisory role
- air traffic systems added as a supplement to each helicopter avionic system
- increased communication protocols for SWH pilots including amended operating procedures to mandate a second call on final approach and ensure pilots are not distracted by passengers during the approach phase
- increased aircraft visibility
- high intensity strobe lighting added to all SWH aircraft
- Airbus high‑visibility paint scheme added to main rotor blades
- mandatory human factors awareness training for all staff (previously delivered to pilots only).
- updated briefing videos and ground crew training on seatbelt fitment.
Civil Aviation Safety Authority
The Civil Aviation Safety Authority (CASA) initiated a review of airspace around Southport which received 87 submissions from airspace users. CASA published the results of that review in March 2025.
CASA has updated AC139.R-01 v3.0 Guidelines for heliports – design and operation to include guidance for operators to consider flight path interaction with nearby facilities, and state an expectation that operations from nearby helipads will not be simultaneous without determination of appropriate separation distances.
CASA has also updated multi-part advisory circular AC91-19, AC 121-04, AC 133-10, AC 135-12 and AC 138-10 v1.3 Passenger safety information to include information about fitment of multipoint restraints and the problems identified when fitting those restraints with constant wear lifejackets. The guidance did not contain information about the correct combined fitment and instead directed operators to consult lifejacket manufacturers.
Australian Transport Safety Bureau
The ATSB acknowledges the significant safety action that Sea World Helicopters has implemented since the accident to reduce the reliance on unalerted see-and-avoid through the addition of risk controls and improving the processes surrounding passenger restraint.
However, of the 11 safety issues identified by the ATSB in this investigation relating to Sea World Helicopters, 4 remained unaddressed by safety action already undertaken. The ATSB has therefore issued 4 safety recommendations to Sea World Helicopters to:
- formally consider the design of conflict points within its operation to identify opportunities for elimination or control
- develop objectives within its safety management system to focus on aviation safety risk
- improve change management processes by ensuring assessments are expanded beyond the area of change to the wider organisation, ensuring new opportunities to control risk are identified and existing risk controls are maintained
- clarify their change management procedure so that the introduction of additional helicopters is captured by change and risk management processes to ensure aviation safety is maintained or improved.
The ATSB has also issued 2 safety advisory notices to industry and more broadly concerning the correct use of passenger restraints, by themselves and with lifejackets.
The ATSB issued a safety advisory notice in September 2023 which highlighted the correct fitment of multipoint seatbelts and encouraged lifejacket manufacturers to produce guidance for use by aircraft operators on the combined use of constant wear lifejackets and multipoint seatbelts. The ATSB issued a further safety advisory notice with the Final report which calls for research organisations to determine a correct method of wearing a constant wear lifejacket with a multipoint seatbelt, while ensuring the correct function of each.
Safety message
The investigation report contains 28 safety factors that provide lessons to flight crews, operators, and other organisations. Overall, the most fundamental lesson is that changes that appear to improve safety can have unintended consequences. Without application of change management processes, it cannot be reasonably determined that a change will not undermine existing aviation safety. Consequently, there is a need for effective implementation of safety management systems with well-defined safety objectives and effective engagement with aviation safety risk.
While unalerted see-and-avoid is a vital last line of defence for pilots, multiple investigations have demonstrated that pilots' ability to visually identify and maintain awareness of one another is limited, and systems which rely on unalerted see-and-avoid commonly fail. Operators should seek mechanisms for supporting pilots in alerted-see-and-avoid. This should include consideration of how safe margins of separation will be maintained when risk controls fail.
As a result of limited available guidance to operators on how to fit constant wear lifejackets with seatbelts, multipoint seatbelts were being fitted incorrectly across the helicopter tourism sector. Seatbelts, when worn correctly, reduce movement, ensuring that other safety features such as energy absorbing seats work as designed. This reduces the risk of occupants contacting other objects or aircraft structures during an impact, thereby reducing the risk of injury or fatality.
Research and validation of the combined use of constant wear lifejackets and multipoint seatbelts is required so that operators can provide the correct fitment advice and ensure passengers are correctly restrained. Addressing this gap in research will have a positive impact on passenger safety worldwide.
The occurrence
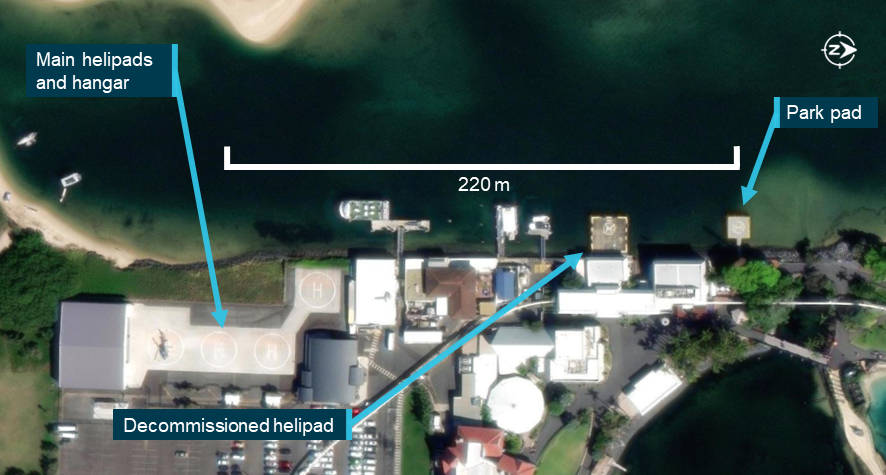
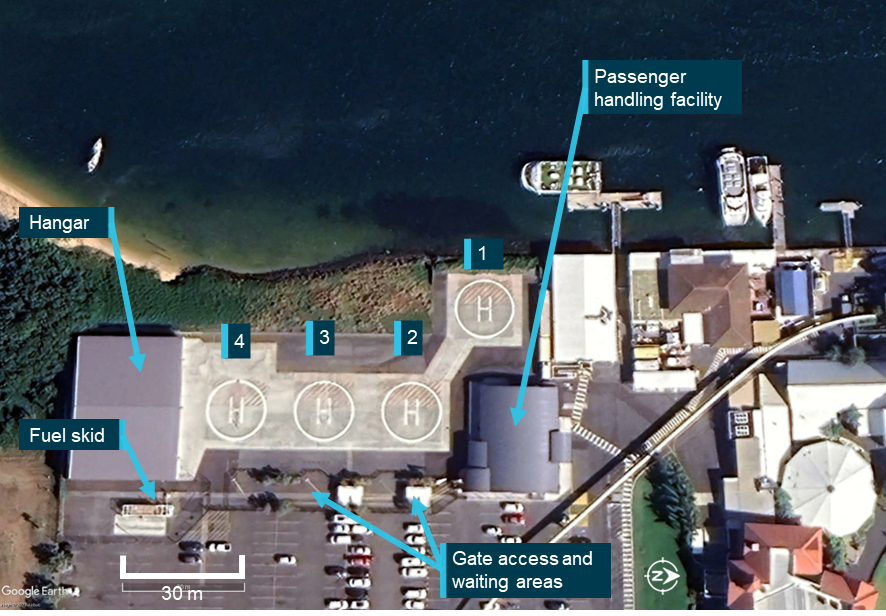
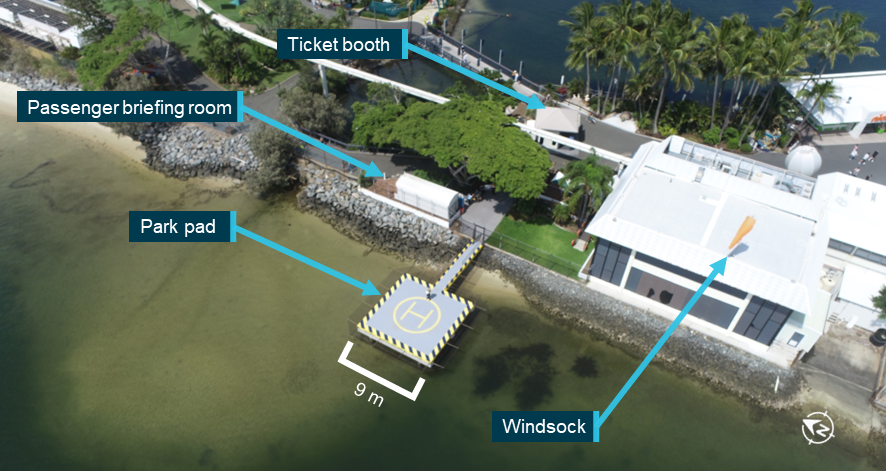
On 2 January 2023, Sea World Helicopters was conducting a series of scenic flights in 2 Eurocopter[1] EC130 B4 helicopters registered VH-XH9 (XH9) and VH‑XKQ (XKQ). The flights were performed under the visual flight rules (VFR)[2] from its base at Sea World on the Gold Coast, Queensland. The helicopters were operating from separate helipads about 220 m apart. XH9 was operating from helipad 3 at the operator’s heliport and XKQ from the park pad inside the theme park (Figure 1).
Figure 1: Helipad configuration at Sea World on 2 January 2023
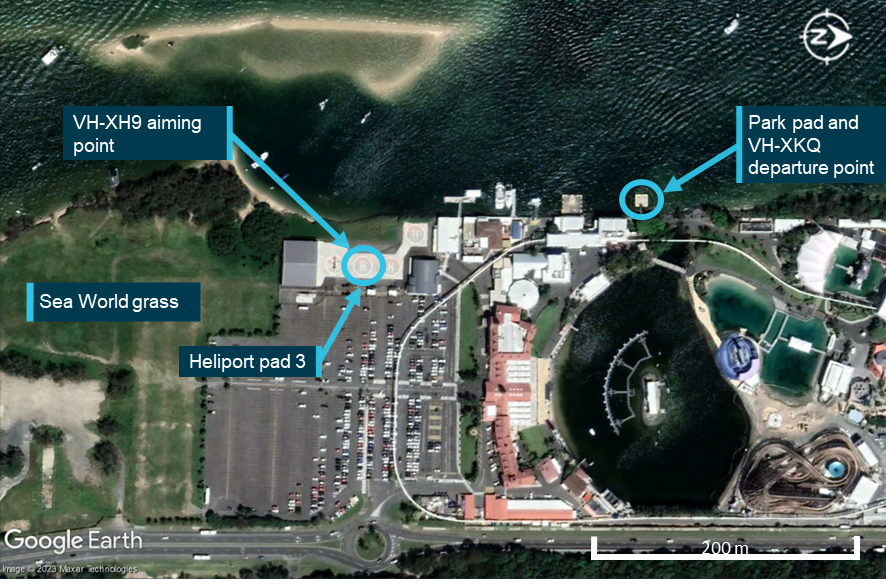
Source: Google Earth, annotated by the ATSB
The pilots of both helicopters flew in the morning, then after a lunch break commenced another series of flights. The first flight after lunch for the pilot of XH9 was a 10-minute scenic flight, which landed at about 1345 local time. Around the same time, the pilot of XKQ also conducted a 10-minute scenic flight, landing at about 1350.
The passengers boarding XH9 and XKQ had watched a safety briefing video, either at the operator’s heliport or in a briefing room near the park pad. The passengers were then fitted with a pouch‑style constant wear lifejacket[3] by ground crew and escorted to the helicopter.
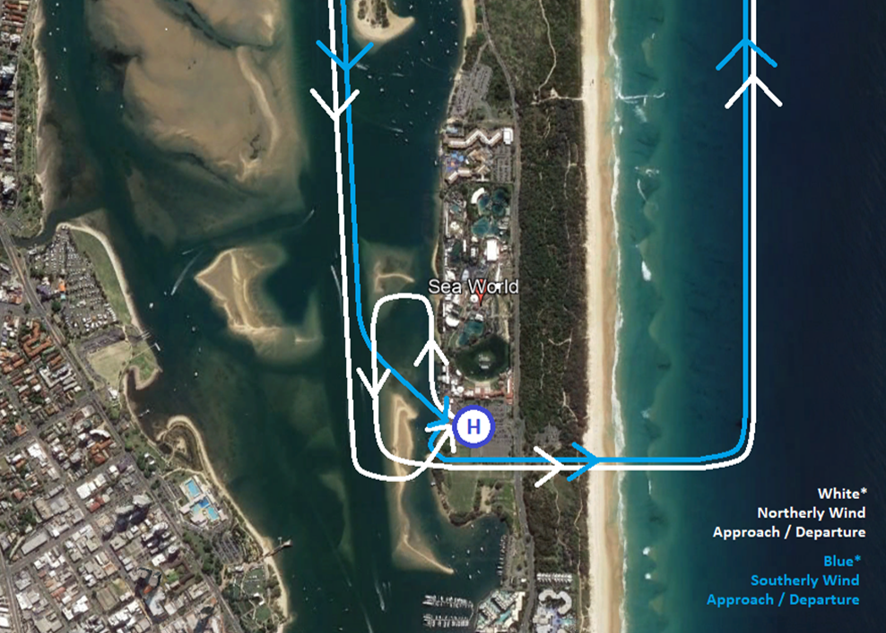
At 1351:40, XH9 departed helipad 3 at the operator’s heliport for a 5-minute scenic flight, with the pilot and 5 passengers on board. The pilot reported making a taxi call prior to lift-off before departing to the south-west, making an immediate left turn to the east over the Sea World grass,[4] and at 1352:05 the pilot made a departure call (Figure 2). They then entered the coastal lane at 90° for a clear view north and south, before turning left to track north at 500 ft over water following the guidance in En Route Supplement Australia[5] for that area.
Figure 2: Five-minute scenic flight route and standard radio calls

Source: Google Earth, annotated by the ATSB
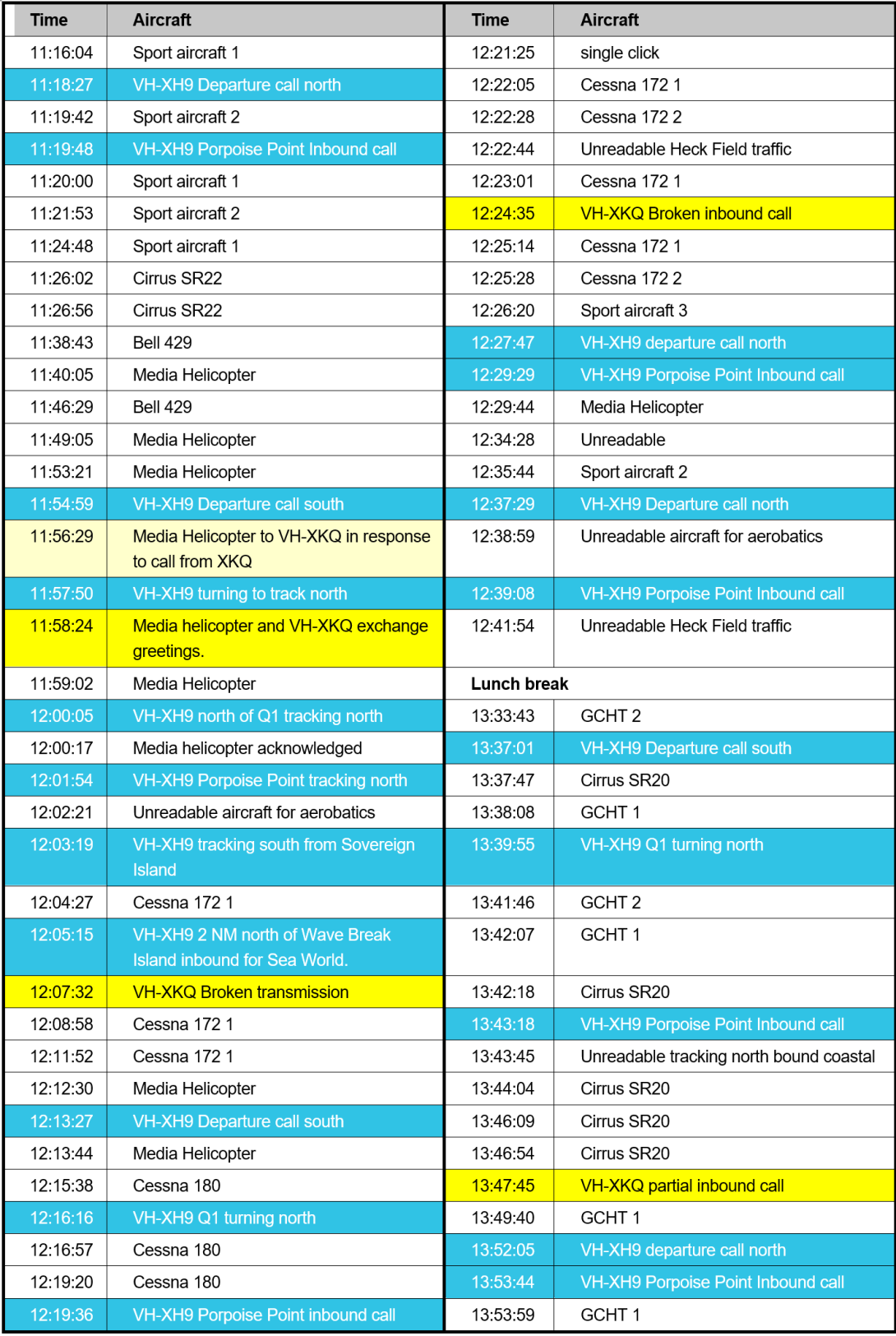
At 1353:20 ground crew began loading passengers into XKQ. At 1353:41, around the time the pilot of XKQ was accepting front seat passengers, the pilot of XH9 was recorded making an inbound radio call from Porpoise Point (Table 1).
Table 1: Recorded activities on board XH9 and XKQ
| Time | XH9 | XKQ |
| 1353:27 | Tracking north crossing southern breakwater of the Seaway near Porpoise Point | Loader 1 loading front seat passengers |
| 1353:31 | Tracking north crossing northern breakwater of Seaway | Loader 2 loading rear seat passengers |
| 1353:41 | Inbound call starts | |
| 1353:49 | Inbound call ends | |
| 1354:00 | Non-company AS350 VH-HTY calls tracking north at Broadbeach | |
| 1354:32 | Tracking south over Wave Break Island | Pilot interacting with passengers |
| 1355:06 | Loader completed pre-flight tasks | |
| 1355:11 | Around 1,600 m from park pad | Start of the ground crew clearing check window |
| 1355:20 | Around 1,220 m from park pad | Time of likely completion of the ground crew clearing check |
| 1355:28 | Around 900 m from park pad | Likely end of the ground crew clearing check window |
| 1355:43 | Around 425 m north-west of park pad | VH-XKQ takes off |
Source: operator data, passenger photos and videos, CTAF recording
Loading of passengers into XKQ was completed at 1355:06. The ground crew reported that they checked the doors of XKQ were closed and ensured the surrounding area was free from watercraft and aircraft. Video and photographs showed that that check would have likely happened at some point between 1355:11 and 1355:28. At that time, XH9 was around 1,220 m to the north of their location. The ground crew signalled that it was a ‘Tour 1’[6] and communicated to the pilot with a thumbs up that XKQ was ready for departure. The pilot acknowledged with a thumbs up. The ground crew member left the helipad and began readying the next flight. The helicopter remained on the pad for 23 seconds before departing.
In XH9, the track southbound along the section of waterway known as the Broadwater provided a clear view of the Sea World helipads. The pilot of XH9 stated that, while transiting the Broadwater, they saw passengers being loaded into XKQ and the doors of XKQ closing. The pilot of XH9 recalled that their assessment at the time was that they would be clear of XKQ and that it would pass behind them. Therefore, they were not required to make any further radio calls, and elected not to.
Prior to the departure of XKQ, a passenger recalled that the pilot advised the passengers to ‘talk amongst yourselves’, and the passenger did not recall hearing the pilot make any calls after that. Helicopter XKQ departed at 1355:42.
There were 2 vessels tracking south on the Broadwater between the park pad and the heliport which XKQ passed to the outside of while climbing towards the sandbar south-west of the helipad. Witnesses on board the southernmost vessel recalled seeing the pilot of XKQ looking at them as XKQ climbed from the park pad.
That vessel was also crossing XH9’s intended flight path. The pilot of XH9 reported adjusting their path to pass behind the vessel on their approach to the helipad (Figure 3). A passenger video from on board XH9 showed that during this period the pilot’s head was fixed straight ahead in the direction of the vessel and their aiming point.
Figure 3: Vessels on the Broadwater from XH9

Source: Witness videos, annotated by the ATSB
At 1355:59 a passenger on board XH9 saw that XKQ was approaching and attempted to verbally alert the pilot of XH9. At 1356:04 the passenger escalated contact by tapping the pilot on the shoulder.
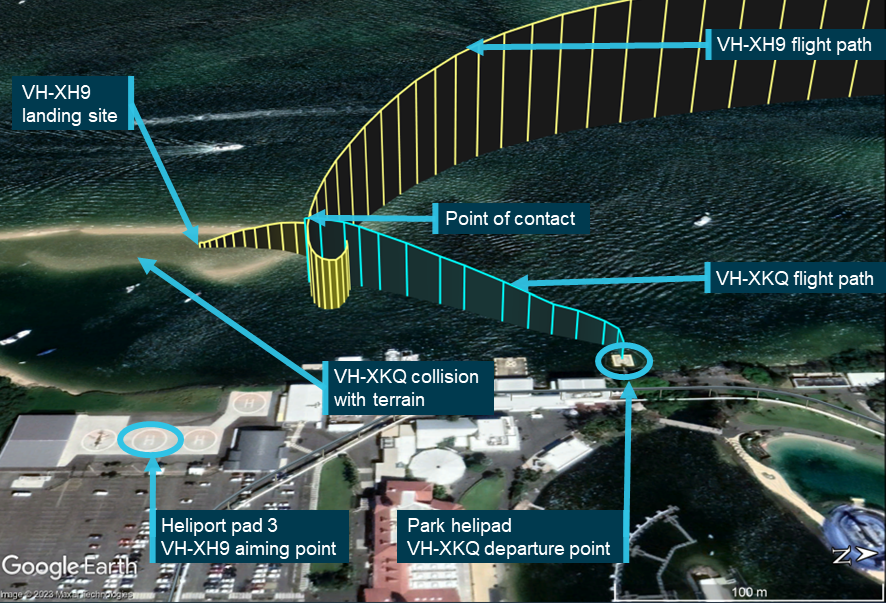
At 1356:06, as XKQ climbed while tracking approximately south, and XH9 descended while tracking approximately east-south-east, the helicopters collided. The height of the collision was estimated to be 39.6 m (130 ft) above ground level, and around 155 m west-north‑west of the heliport. The main rotor, engine, and tail separated from XKQ, leaving the pilot unable to control the helicopter, and it fell onto a sandbar.
XH9 was substantially damaged from the contact with XKQ. The acrylic windscreens and composite structure of the front of XH9 were shattered as the main rotor blades of XKQ passed through the cabin. The pilot and passengers in XH9 were immediately peppered with penetrating fragments. The pilot credited his sunglasses with saving his eyes from the shrapnel. The pilot reported that all flight instruments were missing or failed, the rotor system was damaged, and the engine rpm started to decay. Though injured during the collision, the pilot assessed controllability and found the flight controls remained intact. The pilot landed XH9 on the sandbar, a pre‑determined forced landing area, at 1356:35 (Figure 4).
The pilot and 3 passengers on board XKQ were fatally injured, and 3 passengers were seriously injured. The pilot and 2 passengers on board XH9 were seriously injured and 3 passengers had minor injuries. XKQ was destroyed and XH9 was substantially damaged.
Figure 4: The converging flight paths of XKQ and XH9 leading to the midair collision
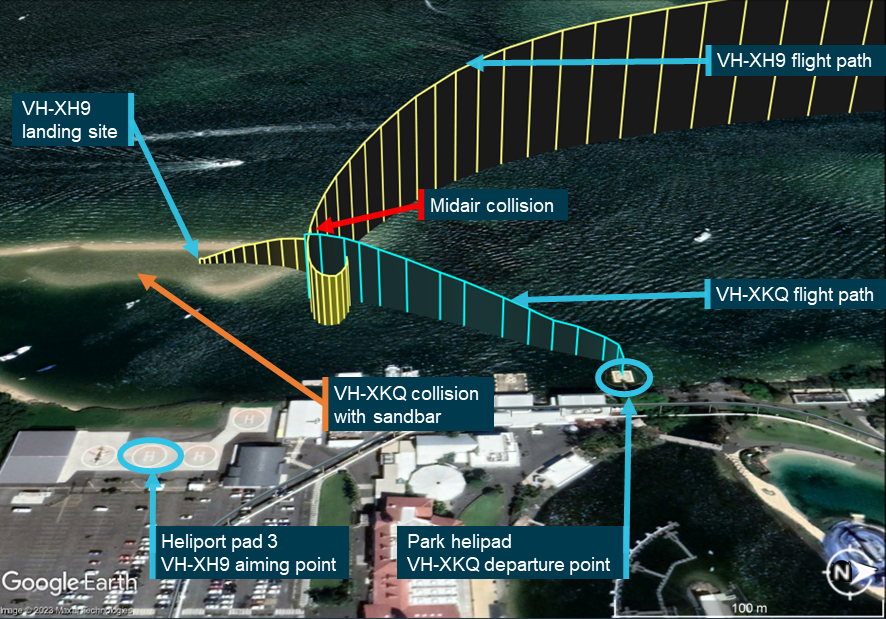
Note: Satellite image was taken near high tide. Sandbar was exposed at the time of the accident. Source: Google Earth, annotated by the ATSB
Context
Personnel information
Pilot of VH-XH9
The pilot obtained a Commercial Pilot Licence (Helicopter) in Australia in March 2012. They were inducted into helicopter operations at Sea World Helicopters on 18 May 2022 and held ratings and endorsements for:
- instrument flight
- night flight
- Grade 2 instruction
- low level
- formation flight.
The pilot’s logbook and operator’s records showed a total flying experience of about 3,150 hours. The pilot’s flying experience was gained entirely in helicopters. In the previous 30 days they had flown 78.0 hours.
The pilot had completed EC130 B4 flight training to learn the differences in systems, performance and operating characteristics of the new helicopter, and undertook a biennial flight review in an EC130. On 5 November 2022 they undertook a 1.8 hour flight in an EC130 B4 with the operator’s head of flight operations (HOFO). Since that time the pilot accrued 60.4 hours experience on the EC130 B4. The pilot completed training and checking for operations to and from the operator’s park pad facility with the HOFO in an EC130 B4 in a flight of 0.4 hours on 23 December 2022.
The pilot of XH9 held 3 roles with the operator:
- line pilot
- safety manager
- drug and alcohol management plan (DAMP) supervisor.
The pilot also had previous experience as an engineer and hazard and safety inspector from a different industry and became the safety manager after joining the company in May 2022. They were nominated to the Civil Aviation Safety Authority (CASA) as the operator’s safety manager on 27 November 2022.
The pilot completed DAMP awareness for Safety Sensitive Aviation Activity (SSAA) employees, and DAMP Supervisor training on 18 May 2022. While working for the operator the pilot completed the check and training activities listed below. Note that the table lists only activities related to operation of EC130 helicopters and DAMP. Additional flights in AS350 helicopters and additional ground based activities were conducted.
Table 2: Relevant training and checking activities for the pilot of XH9
| Date | Activity | Type | Examiner | Notes |
| 18 May 2022 | DAMP Supervisor |
- - | CASA | Ground based |
| 10 Oct 2022 |
EC130 proficiency exam | EC130 | Chief pilot | Ground based |
| 5 Nov 2022 | EC130 B4 flight training and helicopter flight review | EC130 | Chief pilot | No notes contained in the pilot’s file |
| 15 Nov 2022 | Pilot permitted maintenance | EC130 | Licenced engineer | Permitted to complete relevant airworthiness directives and inspections |
| 23 Dec 2022 |
Park pad familiarisation | EC130 | Chief pilot | No notes contained in the pilot’s file |
Pilot of VH-XH9 72-hour history
The pilot of XH9 had 2 days off on 28 and 29 December 2022 and was rostered to work for 4 days from 30 December 2022 until the day of the accident (2 January 2023). Sea World Helicopters records showed the pilot typically started work at about 0830 and finished at between 1730 and 1930, depending on the day. The pilot recalled a similar pattern, adding that work was busy due to the summer tourism period.
The pilot flew on each of the days prior to the accident, including flights in each of the EC130 B4 helicopters XKQ and XH9. The pilot also flew in the AS350 helicopter VH-SWL. The times flown in each helicopter on each day prior to the accident are shown in Table 3. In addition to flying helicopters, the pilot of XH9 spent time with new ground crew, training them in passenger handling.
Table 3: Hours flown by pilot of XH9, 30 December 2022 to 2 January 2023
| Date | Helicopter (hours flown) |
| 30 December 2022 | VH-XH9 (2.5 hours) |
| 31 December 2022 | VH-XKQ (1.2 hours) and VH-SWL (0.9 hours) |
| 1 January 2023 | VH-XKQ (5.0 hours) |
| 2 January 2023 | VH-XH9 (3.9 hours) |
Source: Operator
The pilot reported experience in flying busy summer tourism seasons and stated that their sleep over that period was consistent, retiring at 2130, rising at 0700 and starting work at 0830.
On the night before the accident the pilot of XH9 reported that they had one beer with a meal at a local tavern with their partner before sleeping from 2130. They recalled that they awoke at 0700 on the morning of the accident, and did not feel fatigued.
Evidence including mobile phone billing records showed the pilot likely had sleep opportunity of at least 8 hours each night.
Medical information
In May 2022 the pilot obtained a Class 1 medical certificate (that was valid until 3 May 2023). They were required to wear corrective lenses, which were worn on the day of the accident.
In mid-December 2022 the pilot underwent a diagnostic procedure to evaluate the risk of a disease. The pilot routinely used their designated medical examiner (DAME) as a general practitioner (GP). This arrangement meant that the pilot and their DAME were able to manage the diagnosis with an appropriate specialist to assess any significance with respect to safe conduct of flight. There was no evidence to suggest that this procedure had any bearing on the pilot’s ability to fly and their Class 1 medical certificate was valid on the day of the accident.
|
ATSB observation Many medical conditions do not result in the disqualification of a pilot’s licence and only require monitoring and management of potential risks. The risk to safe flight is not necessarily in the medical condition itself but in non-disclosure and mismanagement. In this case, the pilot’s use of their DAME as a GP and managing this process in consultation with their DAME represented best practice in managing fitness to fly. |
Toxicology
The Sea World Helicopters drug and alcohol management plan required the pilot of XH9 to be tested within 32 hours of an accident but was not carried out. The pilot of XH9 was admitted to hospital on 2 January 2023 and discharged on 4 January 2023. The pilot reported consenting to testing for alcohol and other drugs (AOD) and bloods were taken. Discussion with Pathology Queensland and the hospital showed that no AOD testing was conducted and would not be conducted unless it was considered necessary to inform treatment and improve outcomes for a patient.
The operator stated that they did not test the pilot of XH9 in line with their policies following the accident because they had been informed by the hospital that AOD testing had been conducted.
Pilot of VH-XKQ
The pilot obtained a Commercial Pilot Licence (Helicopter) in July 2007 and obtained an Air Transport Pilot Licence (Helicopter) in November 2013. The pilot was inducted into helicopter operations at Sea World Helicopters on 2 August 2019. They held ratings and endorsements for:
- float alighting gear
- Grade 1 instruction
- sling
- low level
- firefighting.
The pilot held a Class 1 medical certificate which was valid to 14 June 2023.
The pilot’s logbook and operator’s records showed a total flying experience of 6,208.5 hours in operation of single engine helicopters. They first flew the EC130 on 12 July 2016 and had accumulated 200.0 hours on the type. The pilot was qualified and authorised to check the competency of other pilots in the helicopter and had checked the pilot of XH9.
The pilot of XKQ held several roles with the operator. These roles comprised:
- head of flight operations
- head of operations (HOO) (Part 138)
- head of aircraft airworthiness and maintenance control (HAAMC)
- drug and alcohol management plan (DAMP) supervisor
- line pilot
- managerial responsibilities within the business.
The pilot of XKQ was acting in the capacity of a line pilot at the time of the accident. They had flown 448.2 hours over the previous year, 90.4 hours in the previous 90 days and 47.7 hours in the previous 30 days.
While working for the operator, the pilot of XKQ completed the training tasks detailed in Table 4 below.
Table 4: Relevant training and checking activities for the pilot of XKQ
| Date | Activity | Type | Examiner | Notes |
| 29 Aug 2020 | DAMP supervisor |
NA | CASA | Ground based |
| 1 May 2021 | Helicopter flight review Flight instructor proficiency check Low-level |
AS350 | CEO | No notes in file |
| 11 Mar 2022 | Base check with park pad procedures | AS350 | CEO | Conducted several landings onto new helipad. Confirmed procedure for approach departure. All flying to a very high standard. |
| 3 Sep 2022 | Base check | AS350 | CEO | All well flown with excellent judgement |
| 10 Nov 2022 | EC130 B4 proficiency exam |
EC130 | Self | Ground based |
| 30 Dec 2022 | Pilot permitted maintenance |
AS350 EC130 |
Licenced engineer |
Pilot of VH-XKQ 72‑hour history
The pilot’s roster and other information including records of communication and sign-in details were available to develop a timeline of the periods the pilot was likely working and to identify the pilot’s opportunity[7] to sleep in the days before the accident. Based on the available information, key points included:
- The pilot was rostered to work from 0900 to 1700 on 30 December 2022. Records show they signed in at 0832 and signed out at 2022. They conducted administrative tasks throughout that day. The pilot’s partner stated that the pilot's sleep that night was normal. Phone billing records did not indicate that the pilot was awake late in the evening.
- On the 2 days preceding the accident (31 December 2022 and 1 January 2023) the pilot was not rostered for duty.
- On 31 December 2022 telephone records show the pilot woke no later than about 0940. The pilot’s partner recalled that the pilot worked around their house and spent time with their family. That evening, the pilot had a family gathering at their house. Telephone records show the pilot had sleep opportunity between about 0300 to 1030 on 1 January 2023, achieving at most 7 hours 30 minutes sleep.
- 2 witnesses reported the pilot used cocaine on New Year's Eve. On 1 January the pilot was reported to have woken late and spent the day at home relaxing with their family.
- On 2 January, the day of the accident, the pilot departed their home at about 0830 and commenced work at about 0900. The pilot’s partner stated that the pilot had reported sleeping 10 hours the night before, and the recorded evidence showed a sleep opportunity of this duration was available to the pilot.
- All employees working at SWH on the day of the accident recalled that the pilot appeared happy on the day of the accident. One person said he seemed ‘a little distracted’. There were no reports of the pilot appearing tired, or evidence of the pilot showing signs of fatigue in video footage taken prior to the accident.
In combination, a witness statement and telephone records indicate the pilot slept about 10 hours in the 24 hours prior to the accident and had opportunity to sleep about 17.5 hours in the 48 hours prior to the accident. Another witness statement indicated the pilot had about 16 hours sleep opportunity in the 48 hours prior to the accident. Assuming the pilot woke about 0730 on the morning of the accident, the pilot had probably been awake for about 6.5 hours at the time of the accident. Therefore, it is unlikely the pilot of XKQ was experiencing a level of fatigue known to impair performance resulting from insufficient sleep in the prior 48 hours, or time awake prior to the accident.
Contextual information relevant to pilot workload and stress
Evidence existed that the pilot experienced stress a week before the accident. The pilot’s family members recalled the pilot worked long hours, had many work responsibilities, and had reported being under a lot of pressure at work, and provided verifiable examples of the demands the operator placed upon the pilot. Email, telephone billing records and other information showed the pilot often worked outside of their rostered hours.
Following review of the draft report, the operator provided 2 statements which claimed the pilot was experiencing personal stress at the time of the accident. The pilot’s partner disagreed with those claims.
Company pilots and other employees of Sea World Helicopters recalled the pilot appeared their normal self in the days and weeks before the accident, and there were no reports of concerns with the pilot’s performance either as a pilot or manager. The evidence available did not show that any stress experienced by the pilot affected aviation safety risk at the time of the accident.
Post-mortem toxicology and analysis
A post-mortem examination was conducted by a qualified pathologist on behalf of the Queensland Coroner. The toxicology analysis detected very low concentrations of the cocaine metabolites Benzoylecgonine (<0.1 mg/L) and Methylecgonine (<0.01 mg/L). The analysis also detected a common cutting agent for cocaine (Levamisole), with the levels of that substance unable to be quantified. The pathologist’s report indicated there was no evidence of significant natural disease, and no physical signs of chronic stimulant use.
The ATSB engaged a forensic pharmacologist to examine and interpret the results. They stated that it was not possible to indicate the time of use of cocaine based on the post‑mortem blood or urine samples. However, use on New Years Eve around 35 hours to 39 hours prior to the accident (as indicated by witnesses) would be consistent with the blood and urine detection of cocaine metabolites and levamisole. They added that the low concentrations detected suggest that the use was not likely to have been within 24 hours of the incident. The low concentrations also showed it was unlikely that the pilot’s psychomotor[8] skills were impaired during the accident flight.
The forensic pharmacologist also advised that cocaine consumption and subsequent withdrawal can cause fatigue, sleepiness and inattention. It was not possible to determine from blood and urine results alone whether the pilot of XKQ experienced cocaine withdrawal effects on the day of the accident. However, they stated that the evidence available, including the reported 10 hours’ sleep the pilot had the night prior to the accident, meant it was unlikely the pilot was experiencing these effects. The forensic pharmacologist stated:
This would suggest that whatever the dose of cocaine used by the pilot on New Years Eve or in the early hours of the morning of 1/1/2023, [they] had the opportunity to sleep and recover from any fatigue related effects which may have been present on 1/1/2023 and it would be unlikely that [they were] experiencing effects of cocaine induced fatigue/withdrawal. The unlikelihood of being appreciably affected by withdrawal effects of cocaine is further supported by the observations of several work colleagues on the day of the incident who reported the pilot had a normal, happy demeanour that morning and lunchtime.
They also warned that:
It is important to note that cocaine is an illicit drug and as with all illicit drugs, the end user is unlikely to have any knowledge of the actual amount of drug in the product being used. Cocaine like other drugs can be “cut” (diluted) with other substances. Some of the “cutting” agents found in cocaine in Australia includes levamisole (a toxic antiworming banned for human use) … These diluting agents may have toxic effects...
Ground crew information
There were 5 ground crew members working on the day of the accident. Two were assigned to the park pad and 3 were working from the main heliport. Their experience with the operator varied between 2 days to 9 months, and all but one had previous aviation experience, either as ground crew or as a pilot.
Ground crew members were responsible for all aspects of passenger management after check-in. This included pre-flight briefings, fitment of lifejackets and restraints, seating position of passengers in accordance with weight and balance requirements and providing the pilot confirmation that the helicopter was ready for departure.
Ground crew training for these tasks included a written assessment on the operator’s documented standard operating procedures and emergency procedures training. These covered the use of emergency equipment, and passenger briefing and management. Additionally, the training involved a practical component with familiarisation on the different helicopter types.
Some of the operator’s ground crew had also completed an additional internal assessment on hazards related to helipad operations and communication with pilots via hand signals and UHF radio. Of the 5 ground crew members working that day, one had completed this assessment. All 5 ground crew were recorded as having read and understood the operator’s documented procedures.
After completion of the required training, ground crew were buddied with a more experienced person until they were deemed competent to undertake their duties without direct supervision. One ground crew member working on the day of the accident was not yet approved to work independently, and they worked under the supervision of a trained team mate at the heliport.
Aircraft information
EC130 B4
The Eurocopter EC130 B4 is a French-manufactured light utility helicopter developed from the earlier Eurocopter AS350 Écureuil (Squirrel). It combined elements of the EC120 and the EC135 into the AS350 product line. The cabin was widened and lengthened, and an 11-blade shrouded Fenestron tail rotor replaced the conventional tail rotor of the AS350. The position of the pilot in command was moved from the front right in the AS350 (standard in most helicopters) to the front left in the EC130 B4.
The maximum all-up weight of the EC130 B4 was 2,427 kg. The single Safran (formerly Turbomeca) Arriel 2B1 turboshaft engine provided a take-off power output of 632 kW.
Both helicopters were operated in air transport[9] operations and visual flight rules (VFR) day meteorological conditions.
Airworthiness and maintenance
Both helicopters were to be maintained in accordance with the Airbus Helicopters EC130 master servicing manual and the Safran Arriel 2B1 maintenance manual, which required a periodic inspection every 150 hours or 12 months, whichever came first. The flight instruments, electrical and radio systems were to be maintained as per Schedule 5 as stipulated in Part 4A of the Civil Aviation Regulations 1988 (CASA Schedule 5).
Sea World Helicopters had an existing fleet of AS350 helicopters (see Sea World Helicopters fleet below) which had been maintained by Jetpoint Aviation (Jetpoint) since the change of ownership of the operator in November 2018 (see Organisational and management information below). Jetpoint was a CASA-authorised approved maintenance organisation (AMO) and could conduct maintenance at Southport Airfield or at the Sea World facilities, as required. Jetpoint was also engaged by Sea World Helicopters to conduct certification of airworthiness requirements, and other maintenance tasks.
In September 2021 Sea World Helicopters added one EC130 B4. When Sea World Helicopters registered 2 more EC130 B4 helicopters in November 2022 (XH9 and XKQ), Jetpoint was tasked with bringing them into service in Australia (see Implementation of aircraft), and reported resisting pressure from the operator to speed up the process following delays in delivery.
Inspection of the radio systems on board XH9 and XKQ was to be conducted as per CASA Schedule 5 and was predominantly a visual inspection. Any testing of the radio system ‘for correct performance by communication with ground stations or by other means’ was only required for aircraft equipped for instrument flight rules (IFR) flight which did not cover XH9 and XKQ. Instead, Jetpoint reported that the radios underwent basic functional tests on the apron at the aerodrome, however, this was not documented in the maintenance records.
Following these inspections and certification, a new maintenance release[10] was issued to each helicopter.
Sea World Helicopters fleet
Up until December 2022, the operator conducted most of its scenic flights in 2 AS350 SD2 (AS350) helicopters. Both AS350 helicopters were specifically configured to support the operator’s scenic flight business, being fitted with UHF radio for communication with other aircraft and ground crew, an airborne collision avoidance system (ACAS) with an audio alert and visual display, and an iPad for display of manifest information and electronic flight bag data. One helicopter was fitted with emergency floats which was a company requirement for departures over water from the park pad given there was no surrounding solid surface.
The operator had also temporarily introduced AS350 helicopters VH-BLA and VH-PHU from elsewhere in their group of companies to scenic flights at Sea World. The use of these helicopters was out of scope for this investigation.
The owner decided to replace the AS350 helicopters with EC130 helicopters and aimed to have 3 EC130 B4s and an AS350. They reported that the decision was driven by 2 factors:
- Firstly, because the company’s AS350 SD2 helicopters, which had been introduced to the scenic flight operation by the previous owner, were close to requiring rebuild or replacement of significant engine and airframe components.
- Secondly, the new owner sought to improve the product offering and use more modern looking helicopters. The EC130 B4, as a development of the AS350 airframe tailored for passenger transport and sightseeing (Airbus, 2024), was the preferred choice for the operator.
Implementation of EC130 helicopters
Three EC130 B4 helicopters were utilised by the operator at the time of the accident. These were:
- VH-XKK (XKK) – cross-hired from another company from 12 September 2021.
- VH-XKQ – purchased for Sea World Helicopters from Indonesia. Certificate of Airworthiness issued 2 December 2022.
- VH-XH9 – leased from New Zealand. Certificate of Airworthiness issued 9 December 2022.
The owner reported that the intent was that helicopter XKK was to be used exclusively for charter and personal use, though it was used as a substitute helicopter for scenic flights for a short period. The operator reported that acquisition of XKQ and XH9 was for the purpose of them becoming the primary scenic flight helicopters.
VH-XH9 overview
EC130 B4 serial number 3845 was manufactured in 2004 and operated in the United States between 2004 and 2012. The helicopter was then operated in Panama from 2012–2018 and New Zealand from 2018–2022. The helicopter was registered as VH‑XH9 on 2 November 2022, and following certification of airworthiness requirements, entered service in Australia on 2 December 2022.
Maintenance records showed no record of accidents or major repair prior to its entry into Australia. A periodic inspection was completed during the entry into Australia and the current maintenance release was issued 1 December 2022, at 6,750.0 hours total time in service (TTIS). Two throttle microswitches were replaced on 7 December 2022 and a 25/30 hour inspection was conducted on 30 December 2022. At the time of the accident, XH9 had accumulated 6,786.6 hours TTIS having been operated for 1.6 hours that day.
VH-XKQ overview
EC130 B4 serial number 4639 was manufactured in 2008 and operated in New Zealand from 2008–2019. The helicopter was then operated in Indonesia from 2019–2022. The helicopter was registered as VH‑XKQ on 2 November 2022, and following certification of airworthiness requirements, entered service in Australia on 9 December 2022.
Maintenance records showed no record of accident or major repair having been conducted prior to entry into Australia. A periodic inspection was completed during the entry to Australia and the current MR was issued 9 December 2022, at 2,258.3 hours TTIS. Endorsements on the MR indicated that a main rotor track and balance was conducted on 20 December 2022. At the time of the accident, XKQ had accumulated 2,268.5 hours TTIS, having been operated for 1 hour that day.
Emergency float system
XKQ was fitted with an emergency float system, consisting of 2 cylinders mounted in the aircraft belly, and 2 float bags mounted on the landing skids. The arming switch and pilot-activated firing push-button were located on the pilot’s collective.
Removable pilot controls on VH‑XKQ
In May 2009, during entry into New Zealand, XKQ was fitted with an optional modification for removable right pilot (dual) cyclic[11] and anti-torque pedals (this modification did not include the dual collective). The flight manual supplement provided pilots with instructions for fitment and removal of the pedals and cyclic without specialised tooling or technique. Regulations permit certain pilot maintenance activities, when the pilot has received specific training on that task. Fitment and removal of EC130 B4 dual controls was not recorded as part of the Sea World Helicopters pilot maintenance training curriculum. Installation or removal of the dual collective still required a licenced aircraft maintenance engineer (LAME) task.
The modification ‘instructions for continued airworthiness’ required the dual controls be inspected ‘at each scheduled inspection’. Maintenance records from New Zealand showed the dual controls were inspected every 100 hours/12 months. Indonesian maintenance documents recorded scheduled inspections, however, the content of these were not detailed.
The dual controls were not inspected during entry into Australia and were likely beyond inspection requirements. As such they were not recorded on the scheduled maintenance-due records thus providing no assurance they would meet the ongoing requirements of the instructions for continued airworthiness sheets. In addition, neither the modification nor the flight manual supplement were identified as being incorporated in the CASA certificate of airworthiness documentation.
An endorsement on Part 2 of the current MR showed the dual controls were fitted on 16 December 2022 by a LAME. The regulations permitted a passenger to be seated at a seat with dual controls installed. The operator’s procedures required that where it was not ‘possible or practical’ to remove the controls, the pilot was to provide the passenger with a ‘thorough briefing to ensure that the controls are not interfered with.’
Ground crew reported that the dual cyclic and pedals were removed on the morning of the accident. However, there was no endorsement in the MR detailing this action. Examination of XKQ following the accident identified the dual cyclic and pedals had been removed. In addition, the collective was still installed, consistent with someone other than a LAME removing the controls. Although a passenger was seated at that location on the accident flight there was no evidence the passenger interfered with or obstructed the collective control.
Onboard video camera systems
The AS350 helicopters in the operator’s fleet were fitted with Rugged Video camera systems. These systems comprised 4 cameras,[12] cabling, monitor, command module, switching, and recording devices. The cameras could be manually selected by the pilot, set to cycle through the cameras, or set to switch according to time and GPS location. Modification of the airframe to partially or fully install the equipment required certification through completion of an engineering order. The engineering order for the camera system installation required electro-magnetic interference/compatibility testing against instruments, radios and other avionics, prior to the helicopter being operated.
The EC130 B4 helicopters XH9 and XKQ were supplied without these systems. The operator purchased the camera systems, and they were installed by Jetpoint during certificate of airworthiness process. There was no certification for the installation in the maintenance records and the engineering order for the installation in the EC130 B4’s had not been amended. The absence of certification documentation for the EC130 B4’s meant the possibility of electro‑magnetic interference affecting any avionics systems could not be determined, nor if changes to the helicopter weight and balance had been considered.
The helicopters should not have been operated without that certification, and the operator used the camera systems onboard the helicopters without them being approved for use.
On the day of the accident, the camera systems were on but not recording, reportedly due to intermittent failure of footage on USBs supplied to passengers. Though the operator reported installation issues in interviews with the ATSB and had discussed overheating and failing monitors with a supplier, Jetpoint (the AMO) reported that they were not aware of any issues with either helicopter recording system.
Due to the large volume of data the systems produce and their primary aim of creating videos for sale to customers, the operator retained only around one week of video footage on a rolling basis. Videos of 21 prior flights in camera‑equipped helicopters were provided to the ATSB.
Electronic flight bags
Both of the operator’s AS350s and one of the EC130 helicopters (XKK) were fitted with iPads. The iPads were used to receive manifest information from the operator’s booking system and to run electronic flight bag (EFB) software. CASA described an EFB in AC 91-17v1.3 as:
An information system for flight crew members which allows storing, updating, delivering, displaying and/or computing digital data to support flight operations or duties.
The operator used OzRunways as a provider for their EFB software (Figure 5). OzRunways is an approved source of aeronautical information for flight planning, pilot briefing, and moving map data, though it must not be used as the primary tool for navigation as an iPad is not an approved navigation device.
OzRunways also provided a traffic service that tracked device location, and provided that information to other participating devices. This traffic feature could display the 18 closest aircraft transmitting their position as dots over a customisable base map.[13] The dots were labelled with position, call sign (as assigned in the application), relative GPS altitude, speed and direction of the traffic.
The system was designed to operate in real time and would update over the cellular network every 5 seconds. When the position information of an aircraft was older than 6 seconds, the dot displaying that aircraft would fade and be fully removed once the data was more than 20 seconds old.
Helicopters XKQ and XH9 did not come equipped with these iPad devices, though the operator had intended to fit them. In discussion of maintenance at a management meeting on 30 December 2022, the arrival of iPads was advised and the HOFO was tasked with sourcing suitable mounts for them. However, the meeting minutes did not record a requirement for alternative means of carriage, and they were not in place at the time of the accident.
Figure 5: iPad and OzRunways onboard company helicopters
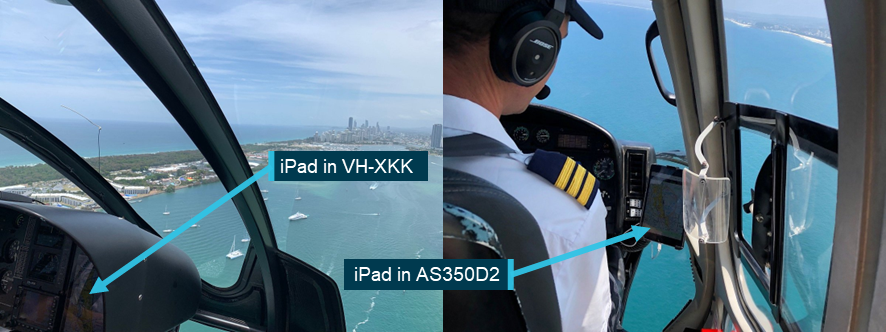
Source: TripAdvisor, annotated by the ATSB
Fire extinguishers
The maintenance records indicated that a fire extinguisher was installed in XH9. There was no part number or description to indicate what type of extinguisher it was, but it was due inspection on 1 June 2023 and no expiry date was noted. That did not match the data on the installed equipment. The labels on the extinguisher noted that a reweigh was due 2 May 2023, with the bottle expiring in December 2025. During examination post-accident, the ATSB identified that the fire extinguisher installed was a dry powder type. This was in contradiction to Airworthiness Bulletin[14] 26-002, Selection and Installation of Handheld Portable Fire Extinguishers which stated:
Dry chemical/powder extinguishing agents when discharged may cause serious impairment to visibility and should not be located or used in any enclosed compartment common to the flight crew of an aeroplane or helicopter.
Maintenance records indicated a halon-type fire extinguisher was fitted to XKQ on 9 December 2022. During examination of XKQ following the accident, neither a fire extinguisher nor a mount was located, though there was a placard pointing to the location where one would normally be. There was no endorsement on the MR to show that the fire extinguisher had been removed.
Part 133 (Australian Air Transport Operations—Rotorcraft) Manual of Standards paragraph 11.46(1)(a) required for this rotorcraft – ‘1 (hand-held fire extinguisher) to be installed in the flight crew compartment’. Further, Airworthiness Bulletin 26-002, Selection and Installation of Handheld Portable Fire Extinguishers stated:
Regardless of whether the regulations require a Fire Extinguisher or not, CASA recommends at least one Fire Extinguisher be fitted to an aircraft and that Fire Extinguisher be accessible to a pilot.
|
ATSB observation During examination of the helicopters and review of maintenance documentation, the ATSB identified multiple inconsistencies between aircraft records and components installed. This introduced vulnerabilities in assurance of airworthiness of these helicopters. The increased risk of uncertain airworthiness did not directly contribute to the accident. In this instance further examination by the ATSB was not likely to provide additional safety benefit to already established regulations and industry best practice. Regulations, technical documentation, guidance and safety studies have long established the importance of following procedures and accurate record keeping for effective maintenance of aircraft. |
Communication equipment
VH-XH9 communication equipment
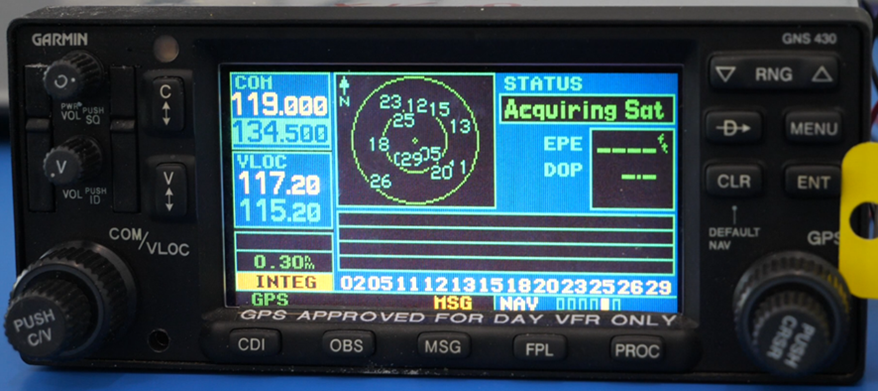
The avionics communications suite onboard XH9 consisted of 2 aviation band navigation and communication (Nav/Com) radios, and a commercial VHF/UHF radio. The radio designated Com 1 was a Garmin GNS430 with radio communication, radio navigation, and global navigation satellite system (GNSS) functions. The radio designated Com 2 was a Bendix King KX-165A with radio communication and radio navigation functions. The third (unused) radio was a Tait TM9300 commercial VHF/UHF digital/analogue mobile radio, however it was not configured for company communications. The pilot of XH9 reported in interview with the ATSB to using Com 2 as the primary radio on the day of the accident as the Com 1 switches were degraded and difficult to use.
A Precision Engineering 7000H audio switch panel permitted all helicopter occupants to communicate through aviation headsets. The audio panel included a 3-position switch for intercom modes:
- ISO (up): the pilot is isolated from the intercom and is connected only to the aircraft radio. The passengers could communicate amongst themselves, without interrupting the pilot.
- ALL (middle): all occupants will hear the aircraft radio and intercom.
- CREW (down): the pilot and copilot position are isolated from the intercom and connected only to the aircraft radio. The passengers can communicate amongst themselves, without interrupting the crew.
In addition, there was a remote isolate button on the cyclic. This allowed the pilot to select the ISO function momentarily,[15] while transmitting, without letting go of the cyclic.
VH-XKQ communication equipment
The avionics communications suite onboard XKQ consisted of 2 aviation band Nav/Com radios. The equipment setup was similar to XH9, with a GNS430 as Com 1, a KX165A as Com 2, and a Precision Engineering 7000H audio switch panel, with remote ISO switch on the cyclic. Unlike XH9, it did not have a third radio. The helicopter was also equipped with a mode C transponder and a CD player.
The VHF Com 1 antenna was a Chelton 21-4B whip antenna and was mounted on the forward right side of the cabin roof. Review of the maintenance records indicated the antenna was original from helicopter manufacture, with no documented unscheduled maintenance or replacement. In addition, the serial number, engraved on the antenna, enabled the antenna manufacturer to source its production and baseline testing records from 2008.
Conspicuity
Introduction
For a full discussion of factors related to visibility of the helicopters in this event, and results of analysis of all contextual factors associated with the limitations and opportunities the pilots of XH9 and XKQ had with respect to sighting the other’s helicopter, see the ATSB report Cockpit Visibility Study supporting AO-2023-001 – Midair collision involving Eurocopter EC130 B4, VH‑XH9, and Eurocopter EC130 B4, VH‑XKQ, Main Beach, Gold Coast, Queensland, on 2 January 2023 (AS‑2023-001) (Visibility study).
Aircraft are difficult to see from other aircraft. At the distances a pilot needs to detect them, they are often a small target against a background which may contain other objects on varied terrain. The likelihood of attention being turned to something is related to its salience,[16] the effort needed to detect it, the expectancy of it, and the value of detecting it (Wickens and McCarley 2007). Visual conspicuity devices increase salience and reduce effort of detection by making the target more obvious. Electronic conspicuity devices can also increase the expectancy and value of a target by telling the pilot where another aircraft is and how it is moving relative to them.
For an object to be detected visually it must be visible, of a detectable size, unshielded, and conspicuous. Conspicuity is dependent on the contrast between an object and the background. Increasing the contrast difference increases the likelihood of detection. The contrast between an aircraft and its background is affected by characteristics of the aircraft and environment. The following section contains basic information and relevant concepts. A detailed discussion relating to conspicuity and its impact on the detectability of XH9 and XKQ is contained in the Visibility Study.
Detectability of lights
The detectability of lights is dependent on 4 factors:
- brightness of the light
- background luminosity
- beam spread (both horizontal and vertical)
- distance between the light and the viewer.
Figure 6 reproduced in Hobbs (2004) shows the required intensity of lights to enable detection at 3 NM, in the foveal[17] eye region (looking straight at it) and at 10° into the periphery of forward sight. As light intensity at distance is determined by a square relationship, the required intensity at varying distances can be extrapolated from this chart. Against a background luminance of 3,000 candela (cd)[18] per square metre (a clear day), a light of 4,500 cd is required to be detected in the foveal region but 300,000 cd is required 10° into the periphery.
Figure 6: Required effective intensity of lights
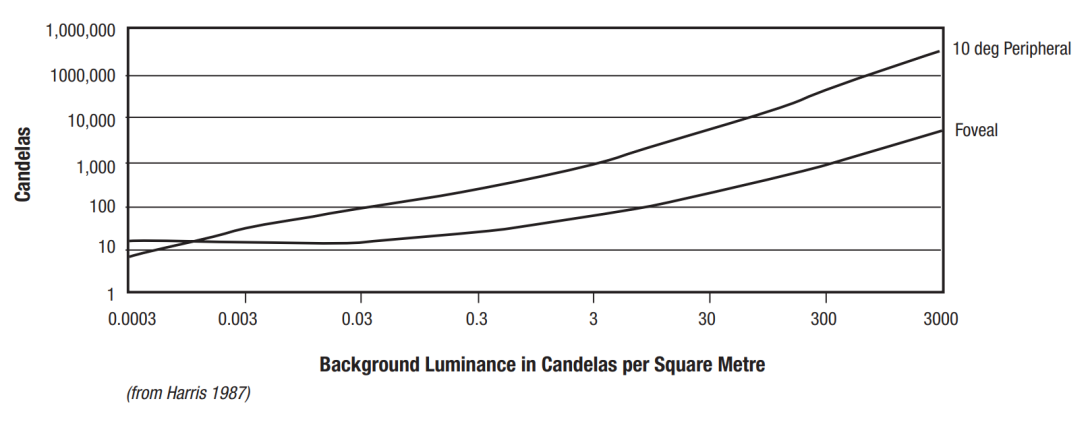
Source: Harris 1987 in ATSB – Hobbs 2004
Both XH9 and XKQ were differently equipped in visual and electronic conspicuity. The following sections will describe that equipment.
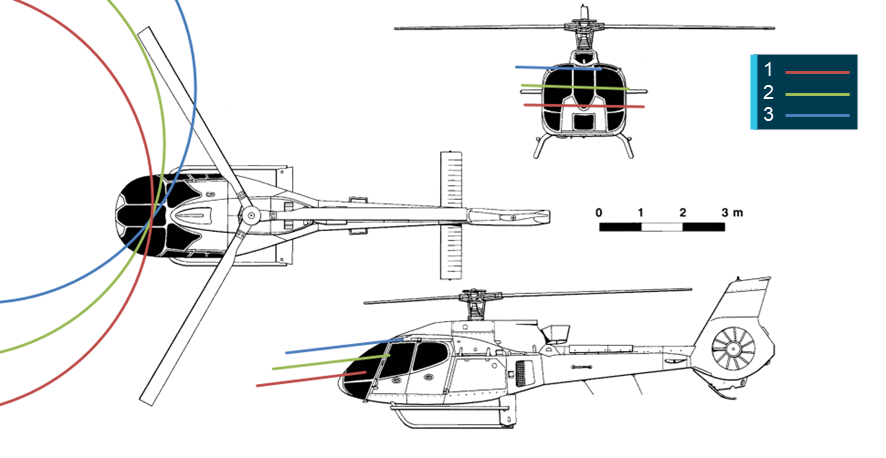
Lighting on VH-XKQ and VH-XH9
Position lights
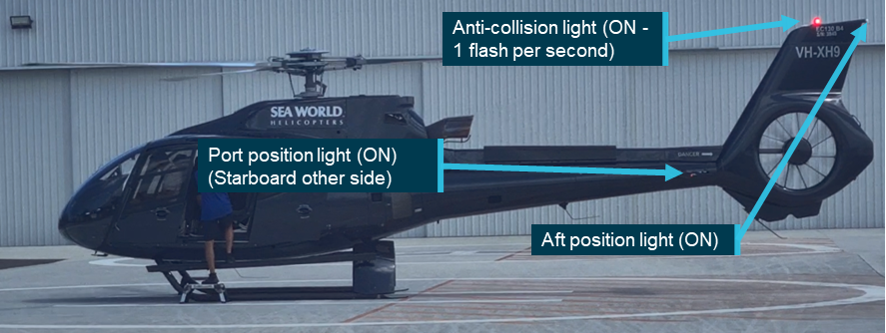
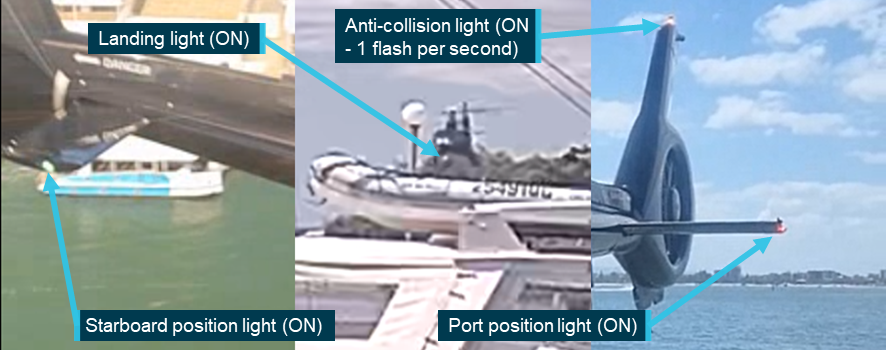
Both XKQ and XH9 were fitted with LED left (red), right (green) and rear (white) position lights. Video footage of both helicopters prior to, and during, the accident flight confirmed that the position lights on XH9 were switched on (Figure 7). The video footage also confirmed that the left and right position lights of XKQ were switched on (Figure 8). Video footage could not confirm that XKQ’s rear position light was active, likely due to the background luminosity and the distance of the camera from the light. However, all 3 lights were activated with one switch, so it was almost certainly on.
Figure 7: XH9 lighting configuration
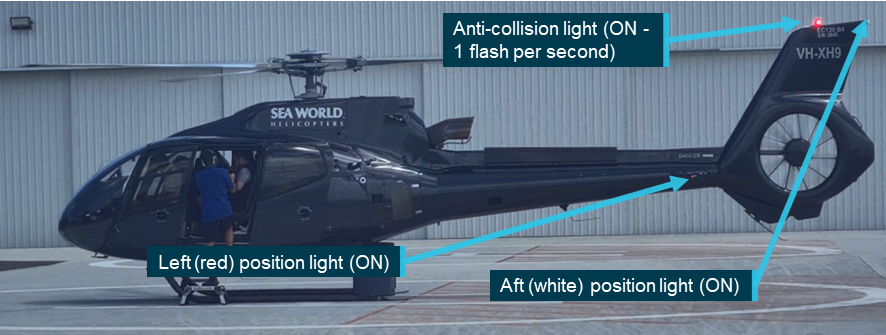
Source: Witness video, annotated by the ATSB
Figure 8: VH-XKQ lighting configuration
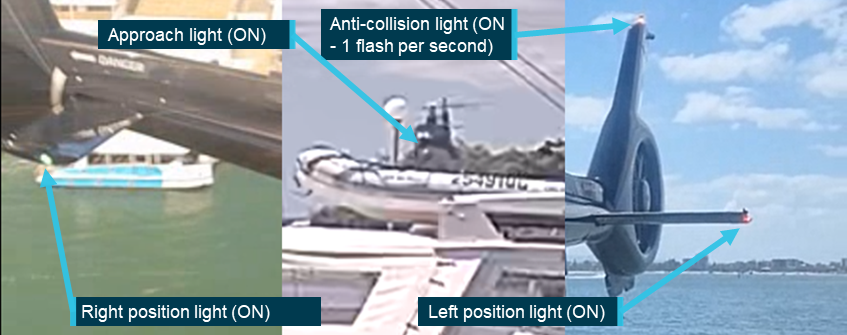
Source: Supplied, annotated by the ATSB
Anti-collision lights
Under Australian Civil Aviation regulations, aircraft operating by day VFR are required to be fitted with anti-collision lights. They must be either 1 red beacon or 2 white strobes or a combination of beacons and strobes. XH9 and XKQ had red flashing LED beacons on the top of the vertical fin (Figure 7 and Figure 8). Video footage of the helicopters prior to and during the accident flight indicated that these lights were active in the lead up to the collision.
Strobe lights
Neither XH9 nor XKQ were fitted with strobe lights, nor were they required to be.
Pulselite system
The Precise Flight Inc. Pulselite system, partially fitted to XH9 and fully installed in XKQ, was an approved solid-state electrical switching unit that pulsed existing external aircraft lights ‘to create an illusion of exaggerated motion’ intended to enhance conspicuity. The Pulselite system is typically connected to the approach and landing lights and other lights can be incorporated if desired.
A 3-position switch on the collective[19] allowed a pilot to select:
- pulse – steady pulsing of the lights
- off – allowed steady state use of lights
- traffic – pulse when traffic advisory is triggered by a linked system.
Selection of the approach/landing light to ON, would override the pulse system for normal steady illumination.
A flight manual supplement advised the pilot of normal operation and limitations of the system. The pilot of XH9 reported not being aware of the Pulselite system nor its operation. The flight manuals from each helicopter were not recovered and the ATSB could not ascertain if the supplement had been inserted into either manual.
Maintenance records showed Pulselite was fitted to XH9 in 2006, in the United States. Wreckage examination identified that the control unit was installed, but the collective switch was not present. XH9’s maintenance records did not record when, or why, the switch was removed.
Maintenance records showed Pulselite was installed on XKQ in 2009 during entry into New Zealand. XKQ was fitted with both the control unit and the appropriate collective switch for systems use. CCTV recording of XKQ departing the park pad (Figure 8 centre panel) showed the approach light steady on, consistent with the approach light being switched to ON.
Approach and landing lights
The EC130 B4 is fitted with a dual landing light system – landing light and approach light (Figure 9). The lights are operated independently. The landing light (right) had a narrower beam, a shallower angle and a higher power rating allowing it to illuminate more of the approach path. The approach light (left) was designed with a wider beam and steeper aim for illuminating the helicopter’s landing area. This light was also referred to as the ‘taxi’ light in the EC130 B4 flight manual. The lights were switched separately but activating either of them would illuminate the ‘LITE’ indication on the instrument panel. Table 5 describes the lighting fitted to XH9 and XKQ.
Figure 9: Exemplar EC130 B4 landing and taxi light configuration
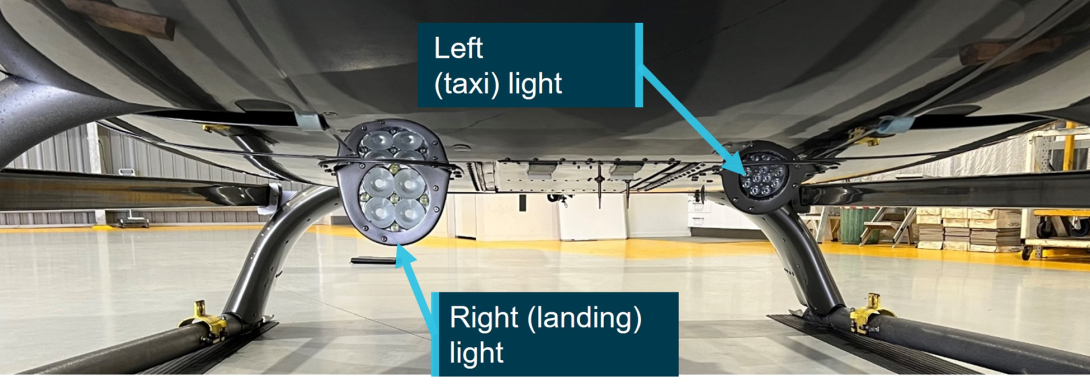
Source: ATSB
Table 5: Landing and taxi light configuration of VH‑XH9 and VH‑XKQ
| Helicopter | Light | Type | Brightness | Beam width | Beam height | Orientation |
| VH-XH9 | Taxi | LED | 15,000 cd |
40° |
unknown |
Down (30°) |
| VH-XH9 | Landing | Halogen | 310,000 cd |
15° |
9° |
Forward (15°) |
| VH-XKQ | Taxi | LED | unknown |
unknown |
unknown |
Down (30°) |
| VH-XKQ | Landing | Halogen | 400,000 cd |
13° |
14° |
Forward (15°) |
Source: ATSB
Video of XH9 from 1 January 2023 showed the lights were operational. Video of XH9 on the accident flight on 2 January 2023 showed the light switches were selected to off, and the lights were not lit throughout the accident flight.
Although CCTV recordings confirmed the landing light of XKQ was on and almost certainly remained on as the helicopter departed on the accident flight, the taxi light was not visible in the footage.
Aircraft fitment
High‑visibility rotor blades
To improve the conspicuity of a helicopter from above, the top of the main rotor blades can be painted in alternating sections of contrasting colours creating the appearance of concentric circles on the rotor disk when viewed from above. The undersides of main rotor blades are not painted, to reduce risk of flicker vertigo[20] for operating crew. Therefore, there is no increase in conspicuity when viewed from below. The conspicuity of low- and high-visibility paint schemes is displayed in Figure 10; the left and right images show blades coated with alternating colours while the centre image shows standard single colour blades.
Figure 10: Exemplar main rotor blade paint schemes

As the images shown are freezeframe, the impact of the high‑visibility paint scheme depicted is reduced. When the blades are rotating, a compete circular array is visible from above. Source: Airbus Helicopters
The top surface of the main rotor blades of XH9 were coated with a manufacturer‑designed high‑visibility paint scheme. A series of white sections overlaid the standard grey blade colour as shown in Figure 11.
Figure 11: XH9 showing high‑visibility main rotor blade colour scheme

Source: Operator, annotated by the ATSB
The top surface of the main rotor blades of XKQ, as shown in Figure 12, were not coated with a high‑visibility paint scheme nor were they required to be.
Figure 12: XKQ at the operator’s heliport showing standard visibility blades

Source: Operator, annotated by the ATSB
Airframe paint schemes
Paint schemes of the actual airframe can affect conspicuity of an aircraft by creating contrast on the target itself or against its background (White, 2016). Figure 13 presents 3 examples of the impact of aircraft paint scheme on conspicuity. The left image shows a grey/black paint scheme over a darker colour background, reducing the conspicuity of the helicopter fuselage. The centre panel shows a multi-coloured paint scheme with an external contrast between the red tail section and the cream-coloured ground. The right panel shows both internal and external contrast with the white and red contrasting with the green background and the black engine cover.
The fuselages of XH9 and XKQ were painted dark grey and black respectively, with lighter grey used for relevant markings and branding.
Figure 13: Examples of use of varying colour schemes

These images only represent a single snapshot in time from a particular angle; viewing the same helicopter from an alternate angle with a clear blue sky in the background may significantly alter the detectability of the paint schemes. Source: Airbus Helicopters, annotated by the ATSB
Background contrast
Video footage taken by passengers on board each helicopter captured the approach of the other helicopter (see Passenger cameras) and the background against which it would have been sighted. Footage from on board XKQ showed the dark grey body colour of XH9 contrasted against the blue sky and white clouds. Figure 14 shows XH9 against this background 7 seconds before the collision.
Figure 14: Footage from onboard XKQ showing the relative contrast between XH9 and its background
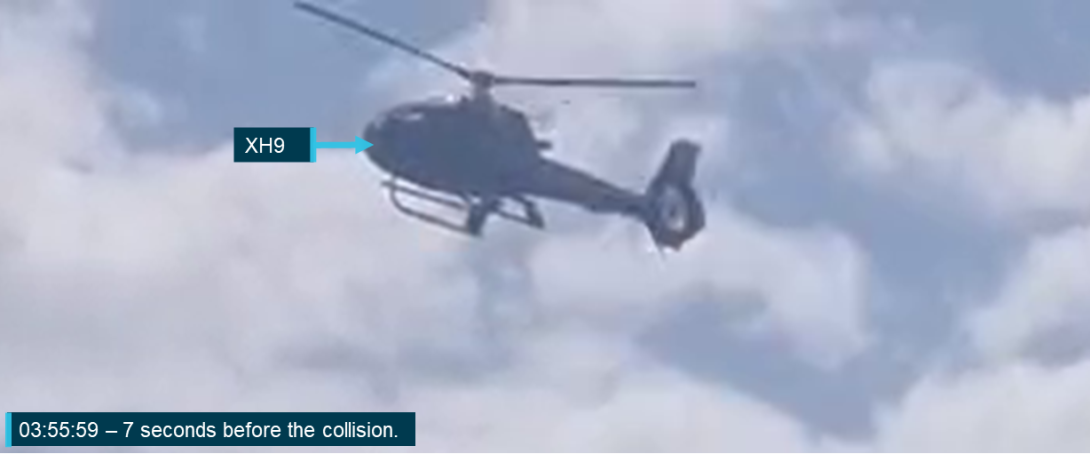
Source: Passenger video, annotated by the ATSB
Video from XH9 showed XKQ before take-off through to the collision. The footage showed the black body of XKQ contrasting with 3 distinct backgrounds.
- The helicopter was easily discernible against the light grey of the helipad.
- The helicopter was difficult to distinguish from dark green vegetation to the east of the pad.
- The helicopter was easily discernible against a white building between the park pad and the heliport.
Figure 15 shows XKQ contrasting with these 3 elements. Note that the upper surface of the plainly painted main rotor blades is not visible in any of the images.
Figure 15: VH-XKQ as captured from the rear seats of VH-XH9

Source: Passenger video, annotated by the ATSB
Electronic conspicuity and detection
Transponders
XH9 was fitted with an L3 Lynx NGT 9000D+ transponder (Lynx NGT) with Automatic Dependent Surveillance–Broadcast (ADS-B) ‘out’ capability. The ADS-B transponder was fitted to XH9 in New Zealand on 27 September 2022 and recorded data demonstrated functionality of the equipment up to 19 October 2022.
Following entry to Australia, the ADS-B registration details were to be updated. For flights from 2 December 2022 to 26 December 2022, externally recorded ADS-B data was either showing no data or the old New Zealand registration. From 27 December 2022 the new Australian registration was recorded but all tracking within Australia was intermittent.
On 20 December 2022, air traffic control at Gold Coast Airport could not identify XH9 on secondary surveillance radar. Following this, ATC advised XH9 would not be accepted into controlled airspace without a functioning transponder. A functional transponder was also a risk control for midair collision in cruise flight, being required for detection by ACAS.
It was reported that Jetpoint, the operator and its pilots were aware, and the helicopter continued operating tours outside of controlled airspace. In interview the CEO of Sea World Helicopters stated that they were aware of the issue and were not sure whether it was fixed stating ‘I was told that the transponder had been playing up on Niner [XH9] and they weren't taking it into controlled airspace. But we hardly were ever doing those flights anyway.’ They also noted that the owner was aware of the issue which was supported by an email chain where the ongoing transponder issue was discussed.
Despite this, there were no endorsements on the MR or in the helicopter’s logbook to indicate what, if any, troubleshooting had been conducted regarding this issue.
During the post-accident inspection of XH9, the ATSB lowered the airframe belly panel and found that the transponder antenna was disconnected. The belly panel had been lowered for maintenance on 7 December 2022. The intermittent transponder transmissions could indicate that the antenna cable was sitting on the antenna connection without being fully engaged, allowing the cable to disconnect at some point.
XKQ was equipped with a Garmin GTX327 transponder which was detectable by secondary surveillance radar and was detected on the day of the accident. The GTX327 does not provide ADS-B ‘out’ capability.
Airborne collision avoidance systems
A traffic alert and collision avoidance system (TCAS) fulfills the International Civil Aviation Organization (ICAO) airborne collision avoidance system (ACAS) standard, and the terms are often used interchangeably.
There are 2 types of ACAS: TCAS I and II, which differ by their alerting capability. Both XH9 and XKQ were fitted with TCAS I. TCAS I provides traffic advisories to assist the pilot in the visual acquisition of intruder aircraft. The level of protection provided by ACAS equipment depends on the type of transponder the intruder aircraft is carrying.
A limitation of ACAS systems, described by ICAO is that:
When a Mode C[21] interrogation is transmitted, all the Mode C transponders that detect it reply. Since the reply duration is 21 microseconds, aircraft whose ranges from ACAS are within about 3.2 km (1.7 NM) of each other generate replies that persistently and synchronously overlap each other when received at the interrogating aircraft.
To overcome that, ACAS systems use directional detection and interrogation at different intensities (whisper-shout).[22] Directional detection narrows interrogation to intruders ahead of the aircraft. However, helicopters may rotate through 180° during departure, and scenic flight routes spend more time turning than direct A-to-B flights.
Local pilots made general statements about TCAS system ‘pings’ on the ground and delayed announcements while airborne. They stated that for their operation, TCAS systems often produced inconsequential alerts and rarely provided actionable information about previously unknown aircraft, making ACAS only useful to them in cruise flight along coastal lanes.
The system as installed on XKQ was known to experience ‘pop ups’ and ‘drop offs’ when operating over water. It was also noted that a poor transponder receiver on the intruder aircraft, a geometry where the antennas are shadowed from each other and high traffic density limiting the detection range, normally resulted in traffic ‘pop ups’ at closer ranges.
The systems installed in the recently introduced XKQ and XH9 were new to the Sea World Helicopters pilots, and they stated that they had not yet learned the functionality of the systems. Company pilots who had flown both helicopters stated that the systems often presented nuisance traffic advisory alerts, or conversely did not provide timely information.
VH-XH9 traffic advisory system
The Lynx NGT transponder fitted to XH9 also provided traffic advisory alerts. The system could monitor the airspace around the aircraft using ADS-B ‘in’ (ATAS), and/or transponders. The ATAS system requires other aircraft to be enabled with ADS-B ‘out’ to provide traffic alerts, which not all VFR aircraft had.[23] XH9 would not detect transponder‑equipped aircraft unless that aircraft also had ADS-B ‘out’ capability, as transponder interrogation was disabled (Figure 16).
If XH9 was at or below 1,700 ft above ground level, the traffic advisory system (TAS) would not display or calculate alerts for aircraft below 380 ft which the system classified as being on the ground. A configuration option called ‘Ground Filtering Altitude’ could reduce that to 5 ft. However, this feature required an additional payment to the device manufacturer and configuration by an approved maintainer. This configuration was not installed in XH9 (Figure 16).
Figure 16: L3 Lynx NGT 9000D+ system configuration as fitted to VH-XH9
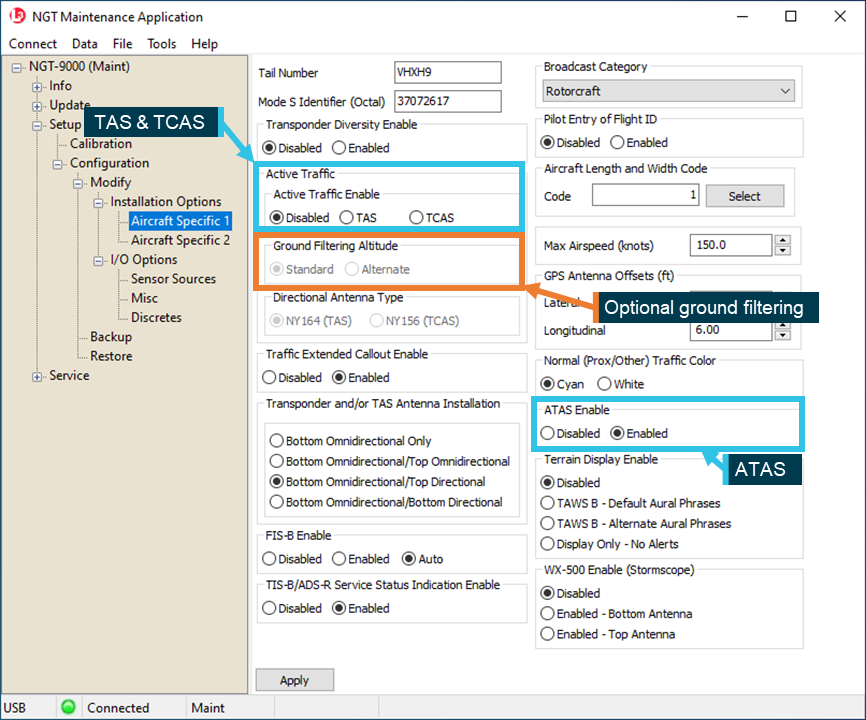
Note: FIS-B[24], TIS-B[25], and ADS-R[26] had been enabled in the system settings, however these systems are not available in Australia. Source: ATSB
When the system did provide traffic advisories it advised the pilot through their headset and displayed intruder aircraft on a small screen on the front of the unit. Aural alerts provided pilots with the relative bearing, altitude and range of intruder aircraft, with wording such as ‘traffic, traffic, 2 o’clock, high, 2 miles.’
The pilot of XH9 did not recall a visual display of traffic being available in XH9. Footage of previous flights in XH9 indicated the Lynx NGT displayed active traffic. However, the position of the transponder on the aircraft’s instrument console was consistent with the normal location of a transponder, which as a device pilots seldom refer to in flight, was not in a conspicuous position. In XH9 it was installed to the right of the pilot’s right knee (Figure 17). The screen was not well positioned for integration with an external scan, and it was not linked to any other cockpit displays.
Figure 17: Location of L3 Lynx NGT 9000D+ in VH-XH9

Source: Sea World Helicopters, annotated by the ATSB
VH-XKQ traffic advisory system
XKQ was equipped with an Avidyne TAS600 traffic advisory system (TAS). The TAS600 provided traffic advisories of range, altitude and bearing of nearby transponder-equipped aircraft. These advisories were announced via an aural signal through the pilot’s headset. The TAS600 would not detect aircraft without operating transponders.
The TAS600 had a flight mode and a ground mode. In flight mode above 400 ft, traffic advisories were announced, and in ground mode, below 400 ft they were muted. In both cases, receipt of a traffic advisory could display traffic and light a yellow ‘Traffic Alert’ flag on the Garmin GMX200 multifunction display fitted to XKQ. Additionally, Pulselite integration in XKQ would result in automatic activation of the Pulselite system, when traffic was detected and the Pulselite ‘traffic’ switch was selected.
The GMX200 was in a prominent position in the console suitable for reference while flying. Though the GMX200 was confirmed as functional during inspection for the helicopter’s export from Indonesia, it was not used on the accident flight. A company pilot reported to the ATSB at interview that operational difficulties with the GMX200 resulted in it not being used.
The midair collision took place below 400 ft where the TAS600 system was in ground mode. In ground mode there would have been no aural alert. With the GMX200 switched off there would be no display of traffic either. This was not pertinent for interactions with XH9 as that helicopter’s transponder was not transmitting and would not be detected.
The ACAS systems that XH9 and XKQ were fitted with did not announce traffic to the pilot below 380 ft (XH9) or 400 ft (XKQ). That meant any company traffic on approach or departure would not be provided to the pilot unless the pilot referred to a visual display.
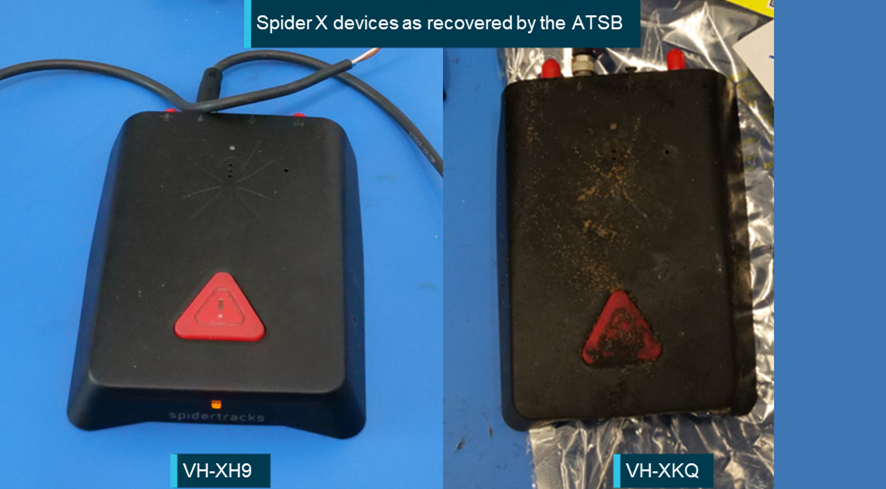
Wreckage recovery and examination
Overview
Investigators from the ATSB arrived onsite at about 1750 on 2 January 2023, about 4 hours after the accident. The sandbar where the helicopters were located had earlier been inundated by a 1.05 m high tide that peaked at 1706, partially submerging both helicopters in sea water. A higher tide of 1.49 m was due at 0605 on 3 January and further deterioration of evidence to the corrosive environment was a risk. This meant that the helicopters had to be recovered from site far more quickly than usual. In the time available at the accident site, the ATSB had uninhibited access to XH9 and took photographs and recovered evidence from that helicopter (Figure 18).
Figure 18: VH-XH9

XH9 landed near to the separated Fenestron from XKQ. The main rotor blades of XH9 display a high‑visibility paint scheme. Source: Queensland Police Service
XKQ came to rest inverted, with the engine, main gearbox, main rotor mast and main rotor system located approximately 15 m away from the fuselage. Access to XKQ in its position and location was limited, and controlled examination and recovery of components was not possible at that time.
Members of the Queensland Police Service (QPS) forensic crash unit had mapped and photographed the accident site, and provided that data to the ATSB. Additionally, QPS divers combed the area underneath the point of collision and around the sand bank for components.
The ATSB did not take immediate possession of the accident site and instead the Queensland Coroner, with the resource and support of the QPS, recovered the helicopters. On 2 January 2023 at 1640, a QPS barge had arrived onsite and secured the scene overnight before transporting the helicopters to the water police headquarters early the next day. The helicopters were loaded onto flatbed trucks and transported to a secure facility (Figure 19). They were securely stored for later examination by the ATSB.
Figure 19: QPS barge Stewart Kerlin II and transport of helicopters

Source: QPS and ATSB
Fuel testing
Aviation turbine fuel was stored at the Sea World Helicopters facility in a 30,000 L bulk container. The bulk fuel and daily fuel samples for both XH9 and XKQ were examined and found to be free of debris and contaminants. A fuel sample taken from the undamaged fuel tank in XH9 was also free of debris. In addition, testing detected nil water present in any of the fuel samples.
Aircraft wreckage
Examination of both helicopters identified no pre-existing defects that would affect normal operation of the:
- flight and engine controls
- engine, transmission and hydraulic systems (including chip detectors and filters)
- main rotor and tail rotor assemblies, including Starflex main rotor hub, blades and mounts
- drivetrain, between engine and main and tail rotor systems
- fuselage and landing gear.
VH-XH9 damage
Overview
The windscreen, forward cabin structure, and centre console of XH9 had sustained multiple main rotor blade strikes from XKQ. Debris and damage signatures along with injuries sustained by the occupants correlated to the right-to-left main rotor blade path of XKQ through the cabin of XH9. Each blade pass was successively higher, deeper and further to the right in the cabin, consistent with the relative movement of XKQ climbing left-to-right and XH9 descending.
A blade strike destroyed the flight instruments and severed the primary wiring loom in the centre console of XH9, thereby removing power from all remaining gauges and instrumentation. The analogue flight instruments, a digital ‘Vehicle and Engine Multifunction Display’ (VEMD), a video recording unit and its display were also destroyed, preventing further examination.
Based on physical evidence and flight path data, XKQ continued to climb relative to XH9 and both aircraft’s main rotor discs[27] passed through each other. A main rotor blade of XH9 had a scuff mark on the lower surface, about mid span. In addition, the skin delaminated on the upper and lower surfaces at the trailing edge, aft of the blade’s spar structure. Following consultation with Airbus Helicopters, it was concluded the scuff mark and delamination was consistent with contact from one of XKQ’s main rotor blades. XH9’s other blades were undamaged.
Apart from the front cabin structure, the airframe including the tail boom, fin, horizontal stabilisers, and skids were undamaged.
VH-XH9 avionics
Components retained from VH‑XH9 were examined at the ATSB’s technical facility in Canberra, Australian Capital Territory, except where noted otherwise. Visual inspection and application of power, where possible, noted the following radio system settings:
- Com 1 – Garmin 430: Damaged beyond repair due to main rotor blade strike. The ATSB could not determine the settings on this unit. The volume knob on the unit was found to be set at approximately 66% (2/3 rotation).
- Com 2 – Bendix King KX-165A: The selected frequency was 119.00 MHz (local CTAF), with a standby frequency 118.10 MHz (Archerfield Airport Tower). The volume knob on the unit was found to be set at approximately 50% (see Figure 20).
- Audio Panel: Both transmit and receive functions had only Com 2 selected. The audio panel volume control, for both the pilot and for the passengers, was positioned at approximately 40%. The intercom mode was set to ‘All’.
Figure 20: Bendix King KX-165A from VH-XH9 – indication on power up

Source: ATSB
When powered, the transponder code showed 1200, the standard transponder code used for VFR flights outside controlled airspace. Review of the fault and events log identified only one valid fault. The fault was indicative of the power being cut to the transponder. This likely occurred as the rotor blades of VH‑XKQ passed through the canopy and the back of the instrument panel of VH‑XH9, cutting the wiring.
The pilot’s headset was a Bose ANX ANR active noise reduction headset and was tested at a CASA-authorised avionics maintenance facility, observed by the ASTB. The headset displayed successful function of the microphone, both earpieces, and sidetone. Fresh batteries were installed, and the active noise reduction function was powered on and appeared functional.
VH-XKQ
Overview
XKQ was initially examined in the recovered inverted orientation, concentrating on flight controls, float system components and landing gear mounts. The airframe was then oriented upright for the remainder of the examination, providing access to the cabin and upper structure.
Flight control continuity was established, with nil pre-existing defects. Damage to the main rotor blades, drivetrain and engine was consistent with high power being delivered during the accident sequence. In summary, there was nil indication that the helicopter was not capable of operating normally.
Damage to the landing gear assembly was consistent with the right roll of approximately 80° on impact with terrain. Following the landing gear, the floor was the first section of the fuselage to strike terrain. The floor was fractured around the front right (passenger) seat but remained substantially attached with the floor bent upward 20° laterally and 7° fore/aft. Further aft, the floor remained structurally intact and remained attached to the rear fuselage.
All windscreens, windows, and window and door pillars were fractured. All doors had separated from the cabin. The rear cabin bulkhead buckled, allowing the roof to compress towards the floor, reducing the available space within the cabin, particularly for the front row occupants. Complete reduction in space was prevented by the seat backs.
All seats were substantially pushed diagonally to the right, in some cases bearing on adjacent seats. All seats remained attached to the seat tracks and the tracks remained attached to the floor. The seats’ passive energy absorbers minimally activated due to the high lateral deceleration and due to the cabin collapsing onto the seats. Some composite seat bases fractured due to impinging on other structures (See Appendix B – Survival analysis for more details).
All safety harnesses remained intact, with only one lap belt being partially cut due to pinching between adjacent structures. One safety harness rotating buckle, which should remain attached to a section of lap belt, was found loose in the wreckage.
Damage to both collective levers was consistent with the impact sequence. Some analogue flight instruments sustained impact‑related damage.
The polymer (caprolactone) fuel tank had shattered with only the forward, left and bottom of the tank remaining continuous. Footage of the impact showed fuel being forcibly ejected during the impact. All the remaining fuel drained from the tank.
The tail boom structure remained attached to the fuselage. However, the helicopter’s tail boom was severed, by its main rotor system. The Fenestron had separated from the helicopter at the tail boom junction plate. The rear driveshaft had sheared at the entrance to the Fenestron. The fan blades were undamaged but 3 static aerofoils (stators) showed impact damage.
VH-XKQ avionics
Components retained from VH‑XKQ were examined at the ATSB’s technical facility in Canberra, Australian Capital Territory, except where noted otherwise. When powered, the following radio system settings were noted:
- Com 1 – Garmin 430: The selected frequency was 119.00 MHz (local CTAF), with a standby frequency 134.50 MHz (Gold Coast Airport Automated terminal information service). The volume knob on the unit was found to be set at approximately 75% (The intercom switch was found in the CREW selection prior to being removed from the helicopter. The audio panel crew volume was positioned at approximately 25% and the passenger volume control was positioned at approximately 75%. (Figure 21).
- Com 2 – Bendix King KX-165A: The selected frequency was 118.70 MHz (Gold Coast Airport Tower), with a standby frequency 128.75 MHz (Gold Coast Airport Clearance delivery). The volume knob on the unit was found to be set at approximately 10%.
- Audio Panel: Both transmit and receive functions had only Com 1 selected. The intercom switch was found in the CREW selection prior to being removed from the helicopter. The audio panel crew volume was positioned at approximately 25% and the passenger volume control was positioned at approximately 75%.
Figure 21: Garmin GNS430 (Com 1) from VH‑XKQ – indication on power up after self‑test
Source: ATSB
As the Com 1 unit was being used for communications on the accident day it was tested at a CASA-authorised avionics maintenance facility, observed by the ATSB. The communication receiver and transmitter, along with the navigation and GPS, were functional. The transmission power at 9.5 W and modulation at 60% were found to be slightly low, however, the avionics technician advised it would not have affected normal operation. It was noted that various buttons required a ‘heavy push’ which can be encountered with older units.
As noted above, the audio panel intercom switch was in the CREW selection prior to being removed from the helicopter, the audio panel crew volume was positioned at approximately 25% and the passenger volume control was positioned at approximately 75%. However, the concentric volume knob had been dislodged from the volume control shaft. Damage and distortion to the audio panel prevented definitive identification of switch and volume selection prior to the accident sequence.
The transponder was in good condition. When powered, the unit displayed the last active transponder code as 1200. Mode selection[28] information was not retained at power down.
The pilot’s headset was a Bose A20 ANR active noise reduction headset and was tested at a CASA‑authorised avionics maintenance facility, observed by the ATSB. The headset displayed successful function of the microphone, both earpieces, and sidetone. The active noise reduction function was not tested due to the amount of corrosion in the control module.
The push-to-talk (PTT) switch on the pilot’s cyclic grip has 2 positions, halfway for intercom and full for radio transmit. Using the wiring diagram, the relevant wires to test the switch functionality were identified however, the trigger switch could not be depressed. This was likely due to saltwater ingress after the accident on the sandbar. The grip was then removed from the cyclic, with all wiring still connected and subject to X-ray examination at the Australian National University (ANU) CTLab.
The X-ray images showed all wiring securely attached, trigger switch springs in place and the 2 switches complete and undamaged. The switch assembly was then removed from the grip by the ATSB and the 2 side panels were removed from the switch to view the switch internals. The switch wiring was again confirmed secured. Some light surface corrosion was observed on the spring guide. The trigger could be depressed, albeit with some force required. Both switches were functionally tested with satisfactory results.
VHF Com 1 antenna
The VHF Com 1 antenna was not destroyed in the accident. The antenna and its mount, with the BNC connector[29] attached and a length of the coaxial cable, were removed from the airframe by the ATSB for examination and testing (see Examination of antenna components from VH‑XKQ).
Recorded information
Time reference
A number of electronic devices with differing clocks provided evidence that was used in the investigation. These were:
- tracking systems fitted to both XKQ and XH9
- iPhones and Android phones of passengers and witnesses
- action cameras
- Common traffic advisory frequency (CTAF) recording at Southport Airfield
- CCTV at various locations
- primary and secondary surveillance radar.
The onboard tracking systems were used to anchor the timeframe because:
- the same type of unit was installed on both helicopters
- the unit times concurred at the time of the midair collision
- the time signal comes from a high precision global navigation satellite system (GNSS)
- there is little opportunity for human intervention in system time setting.
All times stated in this report are with reference to the tracking systems. Other sources, if necessary, had adjustment applied to their time stamp for the purposes of analysis. Synchronisation between the tracking systems and CTAF recording has a margin of error of +/- 2 seconds.
Onboard recorders
Neither XH9 nor XKQ was fitted with a flight data recorder or cockpit voice recorder, nor were they required for the type of aircraft and operation.
Both helicopters were equipped with a tour camera system. On the day of the accident, the systems on each helicopter were not recording (see Onboard video camera systems).
Helicopter tracking devices
The operator’s AS350 and EC130 helicopters were fitted with SpiderTracks flight data monitoring and aircraft tracking units. These units showed the helicopter’s location to the operator and provided a ‘watch’ or ‘SOS’ capability to alert relevant personnel of the aircraft location in the event of an emergency. The system consisted of a head unit mounted on top of the instrument panel with an aircraft power source.
The operator’s AS350 helicopters and VH-XKK were fitted with legacy SpiderTracks units. These units recorded helicopter position information at 15 second intervals. If a pilot activated the emergency function, position tracking would increase to 5 second intervals. Data from the operator’s AS350s and VH-XKK for the 12 months and 90 days, respectively, leading up to the accident was collected by the ATSB and used to analyse the operator’s standard flight paths.
Both XKQ and XH9 were fitted with SpiderTracks ‘Spider X’ flight data monitoring and aircraft tracking units. Spider X included a standard reporting interval of 5 seconds, and an increased alert interval of 1 second if the emergency mode was activated. The Spider X units were also fitted with accelerometers, gyroscopes and a magnetometer to estimate, using a Kalman filter,[30] aircraft orientation (pitch, roll and heading) and vertical speed. This combined the helicopter’s position (latitude, longitude and GPS altitude) into a single attitude and heading reference system (AHRS) file. This data is downloaded to SpiderTracks once a helicopter lands and is available to the operator to review on an online portal.
Flight data from the AHRS units of XH9 and XKQ was used to create a timeline of all flights on the day of the accident to show the tempo of operations (Figure 22), align aircraft position with radio calls on the CTAF and in the development of accurate helicopter position and orientation in the lead‑up to the collision supporting the Visibility study report.
Figure 22: Timeline of scenic flights on 2 January for VH-XH9 and VH‑XKQ
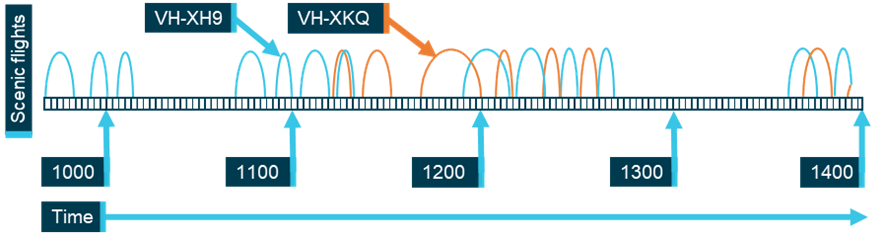
Hoops represent take-off and landing time for each scenic flight. Source: ATSB, Operator data
VH-XH9
The Spider X unit from XH9 was largely undamaged and was able to be powered on and the unit uploaded data to the SpiderTracks server from where it was recovered. The ATSB received all the data recorded by the unit, including AHRS data, from its arrival into Australia until the landing on the sandbar following the collision on the day of the accident.
As part of the data processing and verification undertaken as part of the visibility study supporting the investigation, the ATSB accessed the unfiltered sensor data from XH9’s Spider X unit. This data was used to assess and correct for the application of the Kalman filter. Further detail on this process is outlined in the Visibility study report.
VH-XKQ
Initially, the ATSB was only able to access flight data from XKQ that had already been uploaded to the SpiderTracks server. This included data up until the flight prior to the accident. Due to the sudden power removal associated with the accident, the data from the accident flight had not been uploaded. Because of subsequent saltwater immersion, the unit was unable to be powered up and data was not able to be recovered through its usual upload method. The ATSB examined the unit and removed the memory integrated circuit containing the relevant data. Data, including position and AHRS data, for the accident flight from the Spider X unit was recovered directly from the memory.
Common traffic advisory frequency (CTAF) recording
Common traffic advisory frequency (CTAF) calls are not required to be recorded, though it is normal for aerodromes to do so. The CTAF was recorded at Southport Airfield about 3.6 NM north-west of the Sea World Helicopters heliport (Figure 23). Southport Flying Club received CTAF radio calls through a regular vertical antenna. The estimated detection envelope for the antenna was 30 NM for aircraft above 500 ft. The system was equipped with an aerodrome frequency response unit (AFRU). If no-one had broadcast on the frequency within the last 5 minutes the AFRU would respond with the airfield name, otherwise it would respond with a short tone. CTAF recordings demonstrated that this system was functional.
The CTAF system at Southport Airfield clearly recorded sport aircraft equipped with 6‑watt radios in the circuit area at Heck Field, 9 NM away. Sea World Helicopters’ 5‑minute and 10‑minute flights were flown between 3 NM and 6 NM from Southport Airfield. Buildings along the foreshore of the Broadwater between Southport Airfield and Sea World Heliport were up to 250 ft tall. Therefore, at lower altitudes the built environment reduced the detection envelope, resulting in calls from aircraft around 200 ft and below near the Sea World Heliport not being detected at Southport Airfield.
Figure 23: Southport Airfield and building shielding to Sea World
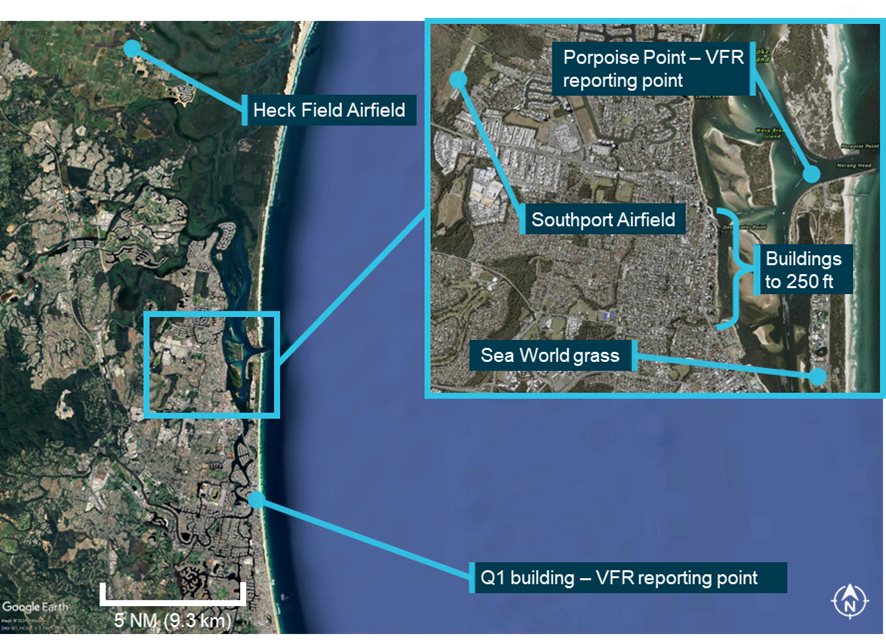
Source: Google Earth, inset Queensland Government Department of Resources, annotated by the ATSB
Both XKQ and XH9 had the same radio equipment, and the pilot who flew XKQ on 1 January 2023 flew XH9 on 2 January 2023, making the same standard radio calls in the same locations. Standard calls are listed in Table 6 below. On the day of the accident, while XKQ and XH9 were operating, around 16 other aircraft were recorded on the Southport Airfield CTAF frequency. The readability of recorded calls from XKQ and XH9 is shown in Figure 24 and Figure 25 below.
The ICAO Manual of Radiotelephony (2007) carried the following readability scale:
5. Perfectly readable
4. Readable
3. Readable but with difficulty
2. Readable now and then
1. Unreadable
The ATSB rated CTAF calls from XKQ and XH9 from 1 and 2 January 2023 against that scale. Calls expected to be detected as per the operator’s procedures (see Operational procedures and information) were identified from manifests and GPS tracks of the helicopters. Taxi calls were not expected to be detected and were excluded from the analysis. Absent calls were rated as 0. Half steps in the readability assessment exist due to inter-rater differences. Overall inter-rater agreement on readability was 87% with high concordance and no difference more than one step. Disagreement was mostly found between ratings of 4 and 5.
Table 6: Standard calls expected for scenic flights
| Tour time | Call 1 | Call 2 | Call 3 | Call 4 | Call 5 |
| 5 minute | Taxi | Departure | Inbound | ||
| 10 minute | Taxi | Departure | Turning | Inbound | |
| 15 and 20 minute | Taxi | Departure | Report prior to entering controlled airspace | Report after leaving controlled airspace | Inbound |
Source: Operator
Departure calls, position reports, and inbound calls from XH9 can be heard clearly over the 2 days of recordings. Of 96 total calls expected from XH9 (Figure 24), 87 were detected (90%). The 10% that were not detected all relate to the first 3 flights of 1 January 2023. The reason for those flights going undetected was not discerned. On 2 January the pilot of XH9 reported using Com 2, a Bendix KX165A, as they were dissatisfied with failing buttons on Com 1, a Garmin 430.
Figure 24: VH-XH9 transmission readability of scenic flight calls
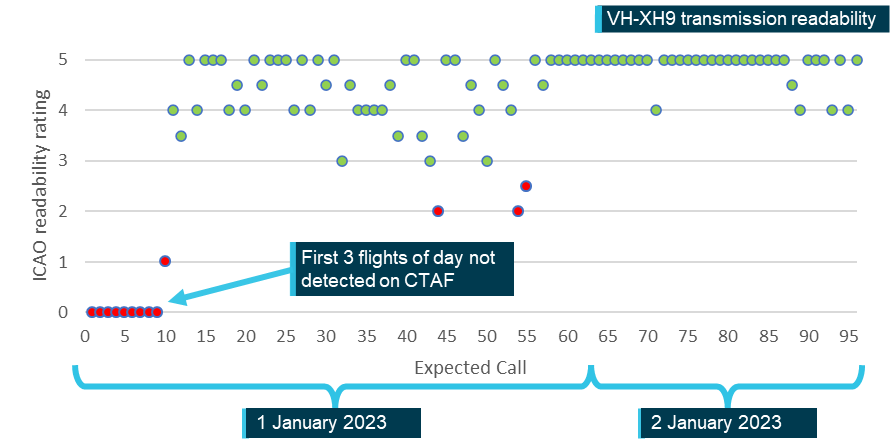
Source: ATSB
Transmissions from XKQ had a much lower rate of detection and most of the calls detected were unreadable (Figure 25). Of the 65 standard calls expected, 17 were detected (26%) most of which were unreadable. Most (94%) of the expected calls over the 2 days from XKQ were rated as absent or unreadable. The ATSB gathered evidence from pilots operating in the vicinity of Sea World when XKQ was operating on 2 January 2023 and none reported noticing issues with XKQ’s transmissions.
Figure 25: VH-XKQ transmission readability of scenic flight calls
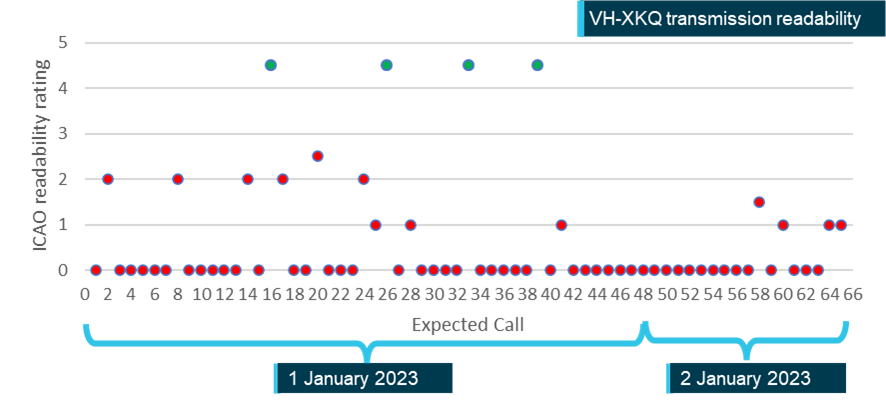
Source: ATSB
One ad-hoc exchange from XKQ was recorded on 2 January 2023. An exchange between the pilot of a media helicopter and the pilot of XKQ showed the pilot of XKQ received and transmitted a call at that time. That exchange was not included in the scenic flight radio analysis above. If included, it would improve the detection rate by 1.5%.
Additionally, at around 1145 on the day of the accident XKQ was flown into controlled airspace. These calls were not included in the analysis. The process would have required the pilot to switch frequencies to receive the automated terminal information service (ATIS) on Com 1 before transferring to Com 2 for controlled airspace communication. If the ATIS was not received on Com 1 the pilot would need to listen to it on Com 2.
Radar
Airservices Australia provided the ATSB with radar recordings of 2 January 2023. These recordings were used in conjunction with CTAF recordings to determine the locations of various aircraft in the area at the time of the accident.
Figure 26 shows an example of the output showing both helicopters on their penultimate flight. Other aircraft in the area were detected on primary radar, and XKQ was detected on secondary radar. The transponder code 1200 denotes an aircraft operating outside of controlled airspace. XH9 did not display a transponder code or height because its transponder was not working. As the helicopters were close to the ground when they collided, radar did not record the accident.
Figure 26: Radar screenshot from 1342:50 on 2 January 2023
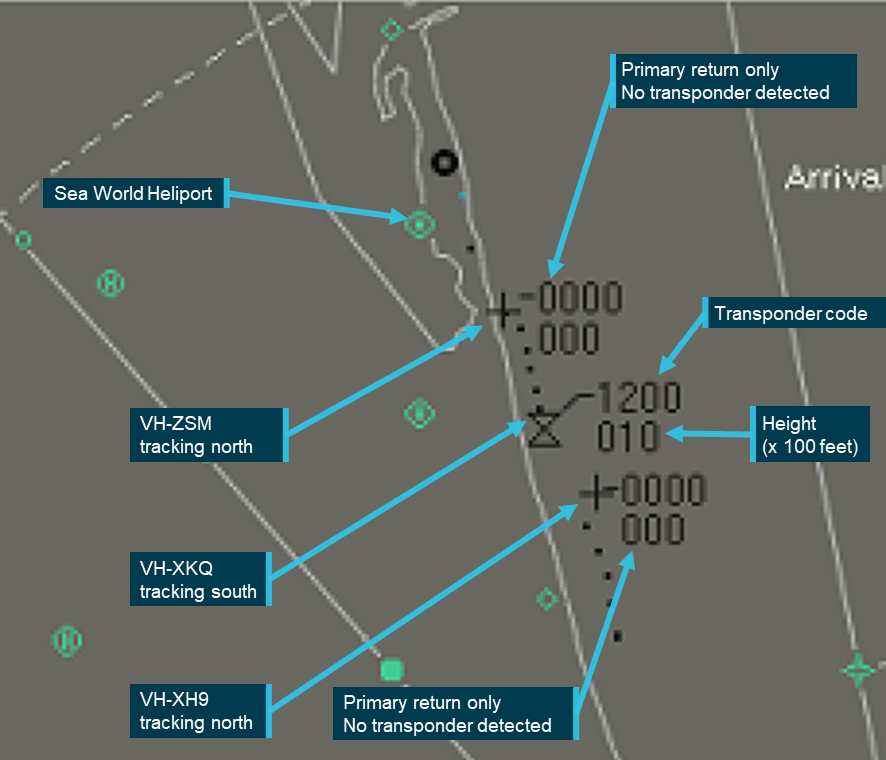
Source: Airservices Australia, annotated by the ATSB
Passenger cameras
Passengers of both helicopters captured photos and video of almost all elements of each flight. Four passengers’ phones were recovered from XKQ and were downloaded by Queensland Police Service. Photos and videos from 2 passengers on board XH9 were provided to the ATSB (3 passengers did not carry their devices on board the helicopter).
Witness cameras and closed-circuit television recordings
The ATSB appealed for witnesses to supply video or photographs showing the accident sequence or the aftermath, and 87 people contacted the ATSB. Witnesses provided additional videos and photographs, eyewitness accounts, information about previous flights with the operator, and local flying activities. This evidence contributed to the investigation and was used in simulation and analysis of the event to create a high level of understanding of the midair collision.
The accident, and rescue efforts by bystanders, was recorded in detail by numerous CCTV in addition to eyewitnesses with mobile phones. Most recordings started in response to the collision, and captured the landing of XH9, and the subsequent rescue efforts. Of those recordings made available to the ATSB, 7 recordings external to the helicopters were stable and detailed enough to be used for analysis purposes. Of these, 4 recordings captured the midair collision, 5 showed the XKQ impact with the ground, and 4 showed the landing of XH9 on the sandbar. Figure 27 shows the position and recording envelopes of CCTV and mobile phone recordings used in the investigation.
Figure 27: Video recordings capturing the accident
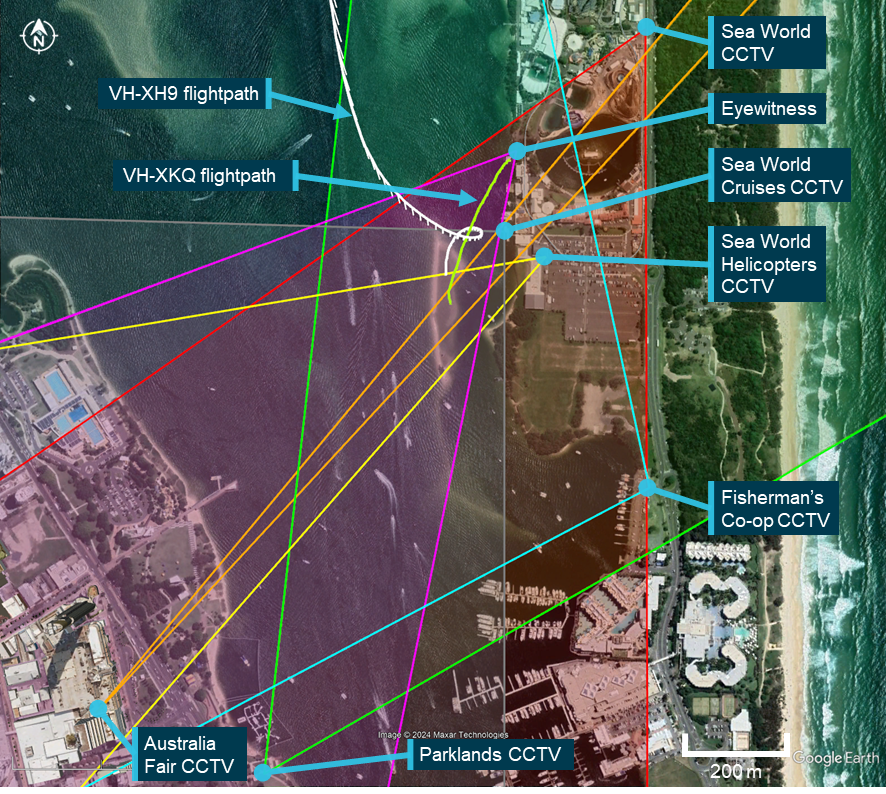
Source: Google Earth, annotated by the ATSB
Flight path and cockpit visibility reconstruction (Visibility study)
The ATSB Visibility study[31] used tracking device data and video recordings to determine the location of each helicopter, and their relative position to the other pilot during the 111 seconds leading up to the collision. The study also used laser scanning of an exemplar helicopter to create 3D models of the interior of the helicopter, and to assess the visibility available to the pilots during the accident flights. The pilot’s eye positions were calculated using manufacturer design data, pilot height, and video of the accident flights.
The study reconstructed the relative position of each helicopter from the calculated eye positions of the pilots at 1‑second intervals. Several iterations were made. Video evidence showed the head but not the eyes of the pilot of XH9 for the final moments of the approach. The pilot of XKQ however was not recorded for more than about a second during the departure, therefore their head and eye position is not known. Calculations were made for both pilots from the designed eye position of the helicopter, and a sensitivity analysis made calculations for head movements up to 500 mm from the pilot’s eye position.
Times in the Visibility study and simulation are reported in coordinated universal time (UTC) which is 10 hours behind (Australian) eastern standard time.
Simulation development
In parallel with this analysis and in accordance with ICAO Annex 13,[32] through an accredited representative from Bureau d'Enquêtes et d'Analyses pour la sécurité de l'aviation civile (BEA) (France), the ATSB collaborated with Airbus, and a simulation expert, iwiation GmbH, to develop a simulation showing a view from the pilot’s eye position of each helicopter. Airbus provided the aircraft design eye position for the EC130 B4. Based on this position 2 additional eye positions were defined representing tall and short pilot eye positions. The pilot’s height and onboard video were used to determine a representative location for each pilot eye position. The pilot eye position for XH9 was above and slightly behind the design eye position, while the pilot eye position for XKQ corresponded with the design eye position.
The reconstruction of cockpit visibility and the simulation were produced using separate tools and processing techniques. The differences between these approaches and the steps taken to verify and calibrate their output are described in the Visibility study.
Relevant contextual information related to visibility
Visual angle describes the apparent size of an object as it is perceived by a viewer. The visual angle spanned is the trigonometric product of the dimensions of the aircraft, distance from the viewer and its relative orientation. A helicopter has a much smaller profile from the front than the side.
It is not possible to state how large an object needs to be in a person’s field of view before they are able to distinguish it. This is due to a wide variety of factors including background contrast, where in the field of view it appears, relative motion, and physiological factors such as fatigue, age and variations in eyesight. Multiple studies and reports give a range of values as to the minimum perceptible size of an aircraft. A United States National Transportation Safety Board (NTSB) report from a midair collision in 1987 (NTSB, 1988) suggests 12 minutes of arc (0.2°). Other examples suggest between 24–36 minutes of arc (0.4–0.6°) is more realistic, especially if viewing conditions are sub‑optimal (Hobbs, 1991).
Photoreceptors (cones) in the middle of the retina allow accurate and detailed vision. They decrease towards the edges where different photoreceptors (rods) favouring detection of movement exist (Hadjikhani, 2000). Therefore, vision is more accurate and detailed in the centre of the visual field, and in the periphery, vision is less detailed but more sensitive to movement.
The detectability of an object is affected by its movement relative to the observer, such that objects which are moving or appear to be moving (through use of flashing lights for example) are easier to detect (Hobbs, 2004). This concept is discussed in greater detail in the Visibility study.
Visibility for ground crew at the park pad
When parked at the park pad while loading passengers, the pilot faced away from the airspace they would occupy after take‑off. As a result, the operator’s Base Operating Procedures required ground crew to look for hazards behind the helicopter and report them to the pilot.
Video analysis by the ATSB showed a window of opportunity for ground crew to perform a waterway and airspace check ran from 1355:11, shortly after crew completed loading, to 1355:28 when the gate was closed, and crew were off the pad. This was a 17 s window that ended 15 s prior to departure of XKQ. Additionally, during that window, the pilot was filmed looking towards the gangway on the helipad and looking away at 1355:20. This was probably at the time of the check. Tracking data was used to determine the position and heading of XH9 between these times.
The tracking data confirmed the approximate distance and elevation of XH9 from the ground crew. Dimensions of the helicopter supported the calculation of the profile XH9 would display and therefore how large it would appear (visual angle) to an observer on the park pad (Table 7).
Table 7: Visual angle spanned and distance of VH‑XH9 during loading events
| Time | Event | Approximate distance of XH9 to park pad (m) | Calculated visual angle spanned by XH9 (degrees) |
| 1355:06 | Loader completed pre-flight tasks on the pad | 1,824 | 0.088 |
| 1355:11 | Start of the clearing check window | 1,602 | 0.132 |
| 1355:20 | Time of likely completion of the check | 1,220 | 0.221 |
| 1355:28 | Likely end of the clearing check window | 901 | 0.364 |
| 1355:43 | VH-XKQ takes off | 425 | 1.233 |
Source: Produced by the ATSB from operator tracking data and passenger videos/photos
The data showed that during the 17 s opportunity to view it, the visual angle spanned by XH9 was below the reliably observable size of 0.4°, and for about the first half, below 0.2° (Table 7 and Figure 28). Further it had a low apparent movement from the point of view of an observer at the park pad, at around 0.4 deg/s (Figure 28).
At the time of the airspace check, XH9 was not displaying landing lights, and clouds created a mottled background in the sky to the north.
Figure 28 shows the change in visual angle XH9 spanned from the point of view of the ground crew on the park pad, as XH9 travelled south along the Broadwater. The dots on Figure 28 represent a timeline based on the location of XH9 while XKQ was preparing for departure. These charts are to be read together.
Figure 28: Visual angle VH-XH9 spanned from ground crew position
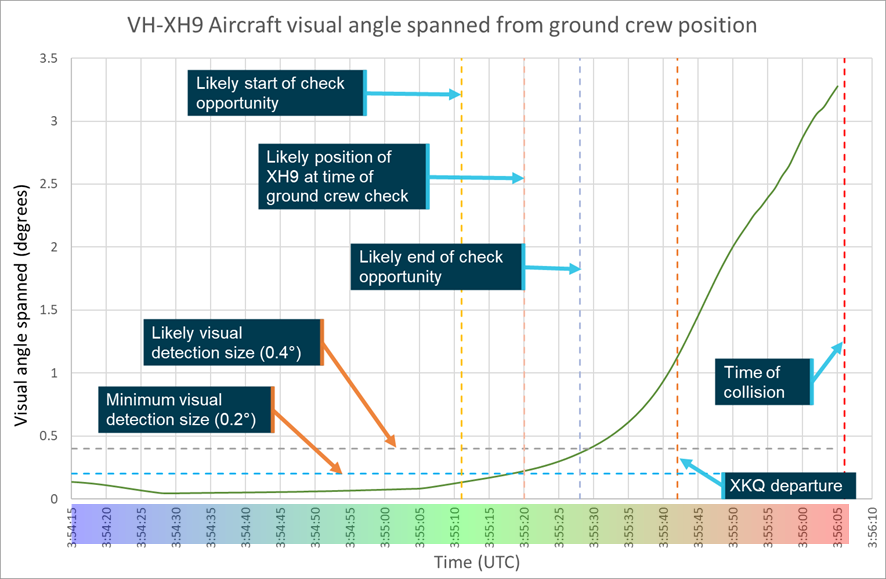
Source: ATSB
Figure 29: Passage of XH9 from the ground crew position
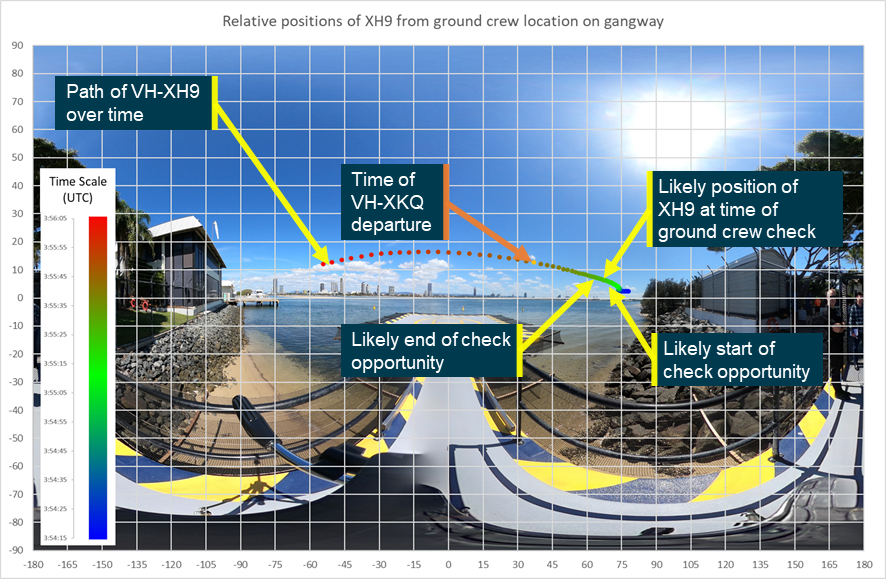
Note: The visual angle size of XH9 for the ground crew is depicted in Figure 28 and should be consulted to interpret this image. Source: ATSB
Though XH9 was not displaying landing or taxi lights, the operator’s procedures required helicopters to light their landing and taxi lights. While these lights may be useful for other aircraft, these lights would only aid ground crew detection in a narrow set of circumstances. The tight beams and orientation of the lights mean they would not often be pointing at the ground crew on the helipad (Figure 30). While angled away from the park pad the light would be less likely to be detected by an observer on the ground.
Figure 30: Orientation of EC130 showing when taxi lights (top image) and landing lights (bottom image) could be visible to ground crew on the park pad
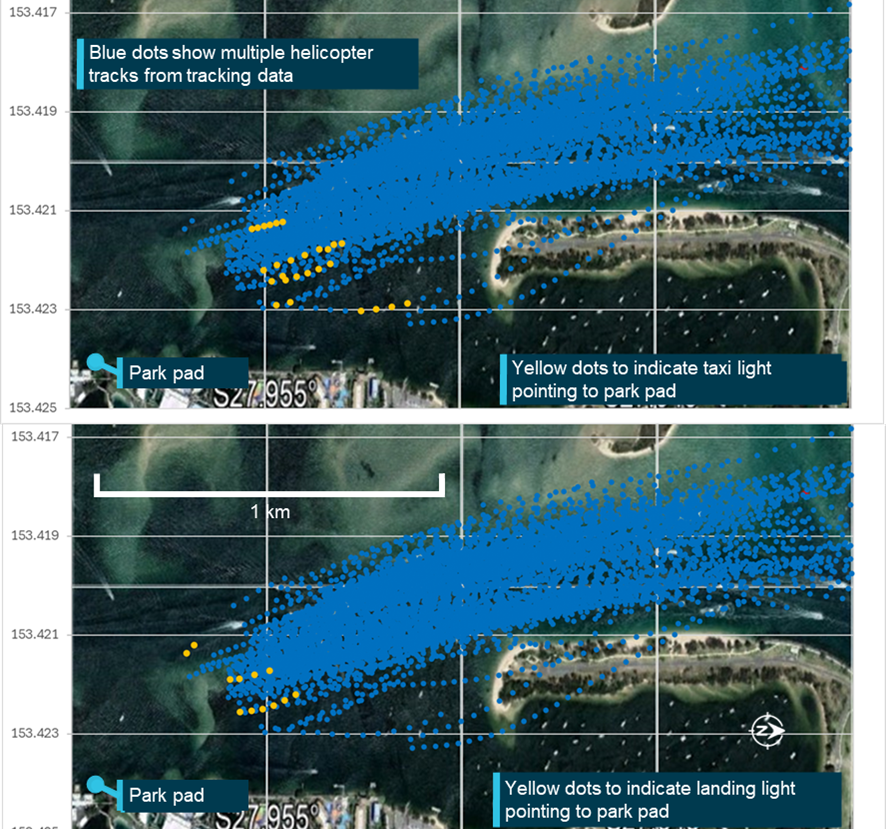
Note: Tracks are all available tracks from EC130 VH-XH9. Source: ATSB
Visibility for pilot of VH-XH9
The Visibility study also examined the position of XKQ from the pilot of XH9’s perspective. Figure 31 shows the visual angle XKQ spanned from the eye position of the pilot of XH9 as they progressed through their approach.
Figure 32 illustrates the position of XKQ and line of sight from the pilot’s eye position of XH9. Over the 111 second period captured in the analysis, from this position, their line of sight would be as depicted in the chart. Note that it is likely that the pilot’s head position and gaze changed during this period.
The grey shadow represents aircraft structure and is laid out on an equirectangular image.[33] The figure uses a colour gradient to illustrate the relative position of XKQ and the passage of time, with blue dots representing earlier events and red dots representing later events. Dots on the grey shadow indicate that XKQ was shielded at that time from that eye position.
The study determined that after XKQ lifted from the park pad it moved left relative to the orientation of the pilot of XH9, behind the cockpit pillar, and into the left window. The distance between the dots represents relative movement of XKQ from XH9. There is a significant gap at time of collision as relative movement is at its highest.
Visual angle spanned by XKQ is not depicted in Figure 32 and it must be read in conjunction with Figure 31, where the coloured dots are represented by a coloured bar on that chart.
Figure 31: Plot of visual angle spanned by XKQ from the pilot’s eye position of XH9
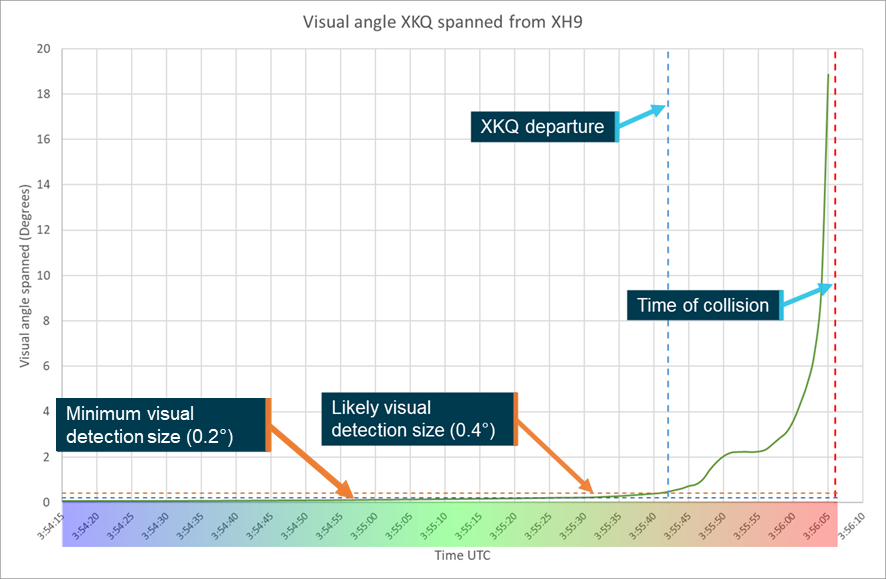
Source: ATSB
Figure 32: Relative position of XKQ overlaid on pilot of XH9’s eye position
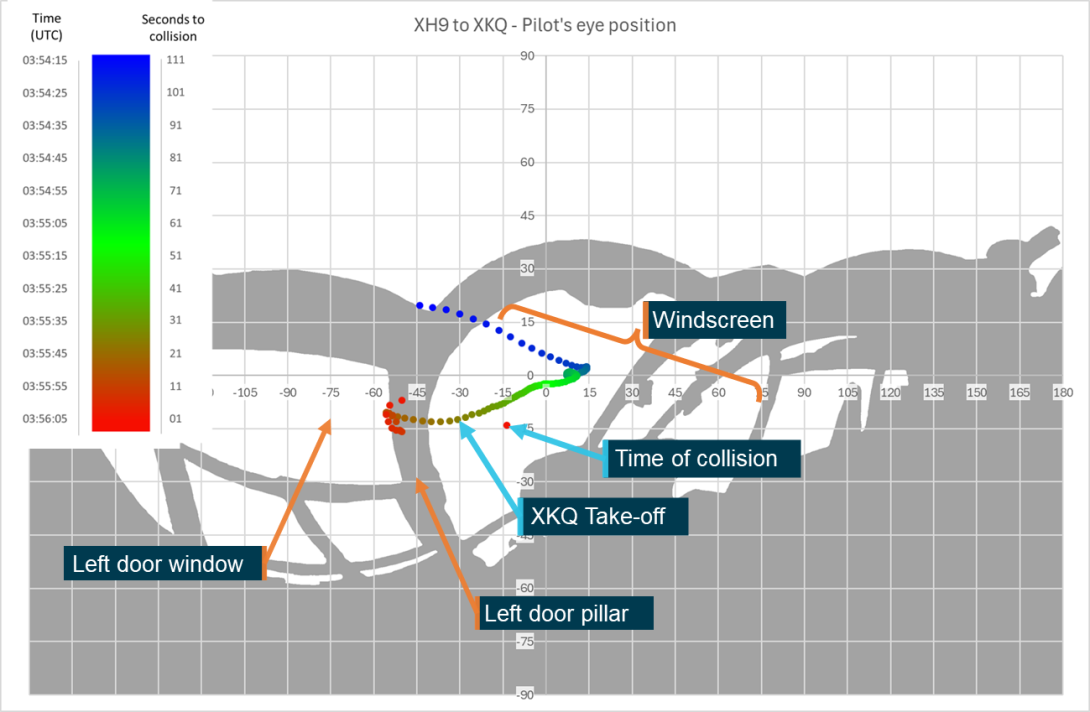
Note: Timescale reads from 111 seconds to collision (blue) while XKQ was still on the pad to time of collision (red). Source: ATSB
The Visibility study also reviewed the relative position of the vessel that the pilot of XH9 avoided while approaching to land. The vessel and helipad 3 at the heliport appeared centrally within the pilot’s windscreen, while XKQ was to the left, behind or outside of the cockpit pillar. Figure 33 shows the recreation of the pilot’s likely view of these elements 13 s prior to collision. Figure 34 shows the recreation 6 s before the collision when XKQ and the marine vessel were shielded by the cockpit structure. These times (13 and 6 seconds) encompass the estimated time required to detect an aircraft and manoeuvre to avoid collision from a distance and at close quarters. The FAA (2022) cited research that found identifying a collision risk, reacting and manoeuvring to avoid a midair collision takes on average 12.5 s. The ATSB (2002) cited research that found close proximity events can be resolved more quickly, stating it could take from around 3.9 s to 5.9 s to recognise the hazard (1.5–3.5 s), take avoiding action (0.4 s) and have the aircraft respond (2.0 s).
Figure 33: Relative positions of Heliport Pad 3, vessel and XKQ at 13 s prior to impact
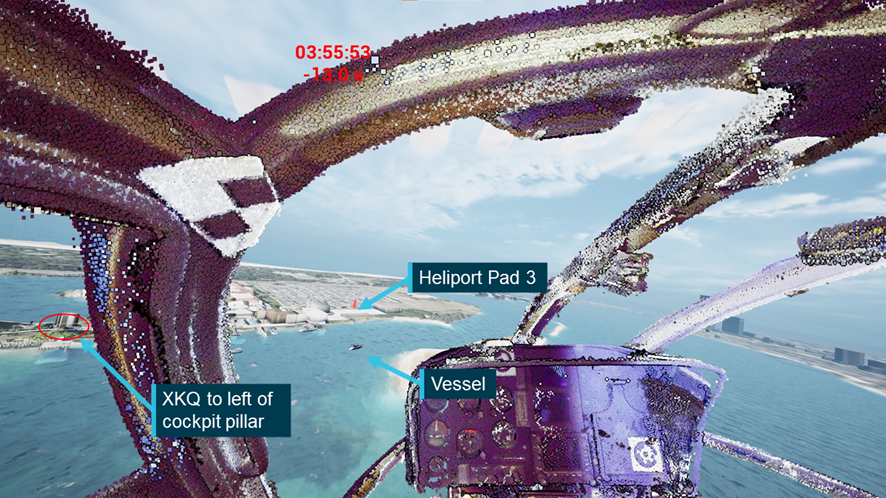
Source: iwiation GmbH, annotated by the ATSB
Figure 34: Relative positions of Heliport Pad 3, vessel and XKQ at 6 s prior to impact
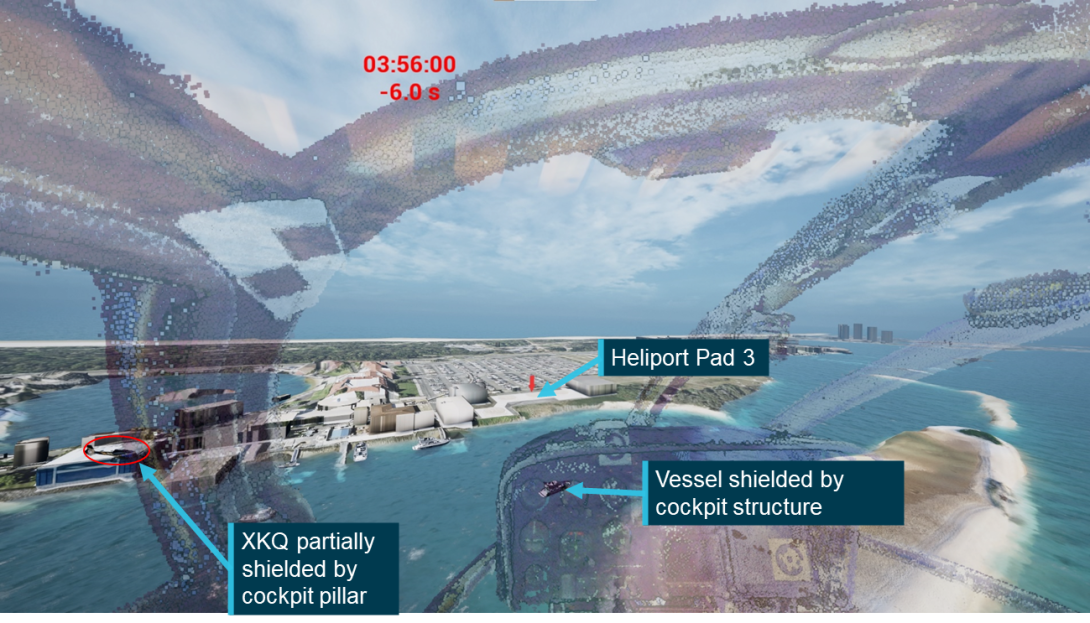
The opacity of the cockpit structure has been reduced to 60% to show the relative positions of both XKQ and the vessel which were likely partially or fully obstructed from pilot’s eye position. Source: iwiation GmbH, annotated by the ATSB
The simulation indicated that XKQ was partially or completely unshielded from the pilot of XH9 for around 5.5 seconds before the collision.
Visibility for pilot of VH-XKQ
In interview in the days following the accident, 2 company pilots stated that the visibility to the right was worse from the left seat of an EC130 versus the right seat of an AS350. Following review of the draft report Sea World Helicopters provided letters from 2 different pilots stating that visibility to the right was better in the left seat of an EC130 than from the right seat of an AS350.
Figure 36 illustrates the position of XH9 from the designed eye position of the pilot of XKQ. The Visibility study determined that from between 111 and 56 s before the collision, as the pilot of XKQ was preparing to depart, XH9 was visible through the pilot’s rear left window unshielded by cockpit structures. Looking in that direction would have required the pilot to rotate around 160° to look over their left shoulder, and due to the distance between the helicopters at that time, the visual angle that XH9 spanned was below the threshold of likely visual detection (Figure 35).
As XH9 approached the park pad, its apparent location from the designed eye position of the pilot of XKQ moved behind, then to the right. From 32 seconds prior to the collision, when XH9 was approximately 615 m from the park pad, it was obscured by cockpit structures. This is shown in the green dots in Figure 36. As XKQ picked up into the hover, the apparent location of XH9 moved upwards and from right to left, shielded by airframe structure. This is shown as the red dots in Figure 36. Figure 36 and Figure 37 should be read in conjunction with Figure 35.
Figure 35: Plot of visual angle spanned by XH9 from the pilot's eye position of XKQ
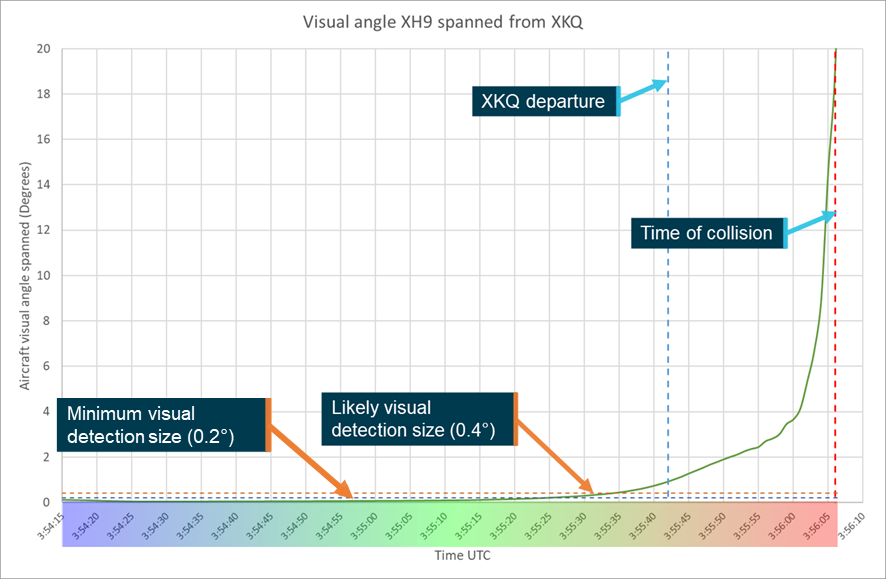
Source: ATSB
Figure 36: Relative position of XH9 overlaid on pilot of XKQ’s eye position
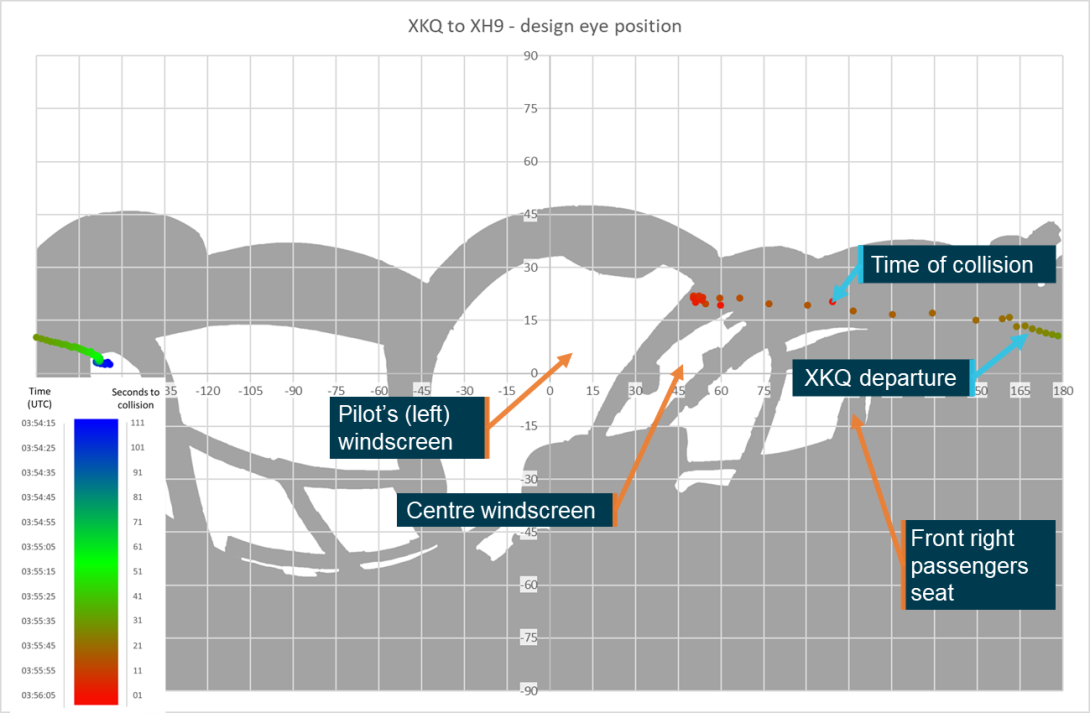
Note: Time scale reads from 111 seconds to collision (blue) to time of collision (red). Source: ATSB
The pilot of XKQ was wearing a peaked baseball cap and the Visibility study also reviewed the potential impact of the pilot’s cap. As XH9 was shielded from the pilot’s eye position before XKQ departed the park pad, the pilot’s cap would not have made sighting XH9 more difficult. Where the sun is visible, or close to the edge of the field of view, the sun’s glare can reduce a pilot’s ability to locate traffic. Given the location of the peak of the cap, as shown in Figure 37, and the relative position of the sun, the pilot’s cap likely reduced the direct and indirect impacts of the sun on the pilot’s vision.
Figure 37: Relative position of XH9 from XKQ overlaid with shielding of pilot’s cap
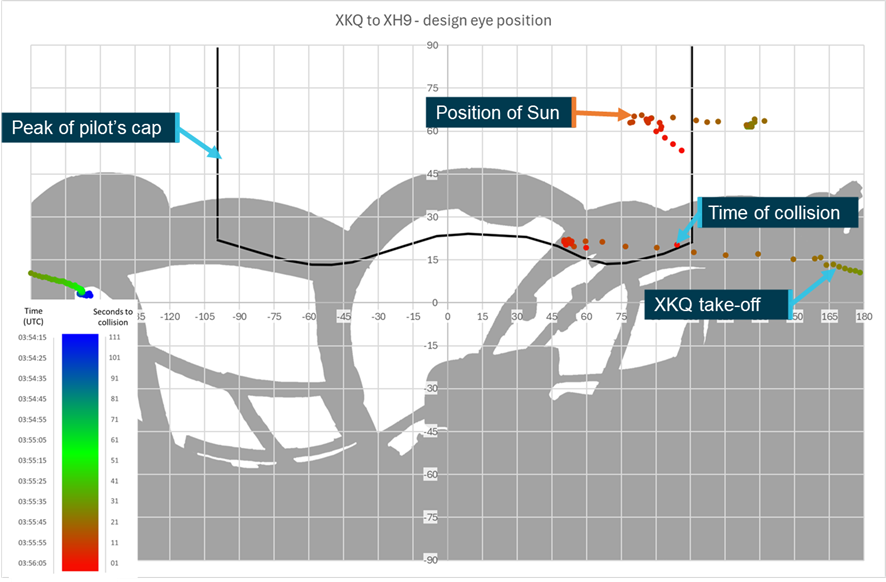
Note: Time scale reads from 111 seconds to collision (blue) to time of collision (red). Source: ATSB
Figure 38 and Figure 39 show simulated views from the pilot’s location in XKQ, 13 s and 6 s before the collision. In Figure 38 the view shows the relative location of XH9 behind the roof structure of XKQ.
Figure 38: Simulated view from XKQ, 13 s before collision (looking straight ahead)

Note: Pilot’s cap is represented by the transparent blue section at the top of the image. Source: iwiation GmbH, annotated by the ATSB
Figure 39: Simulated view from XKQ, 6 s before collision (looking straight ahead)
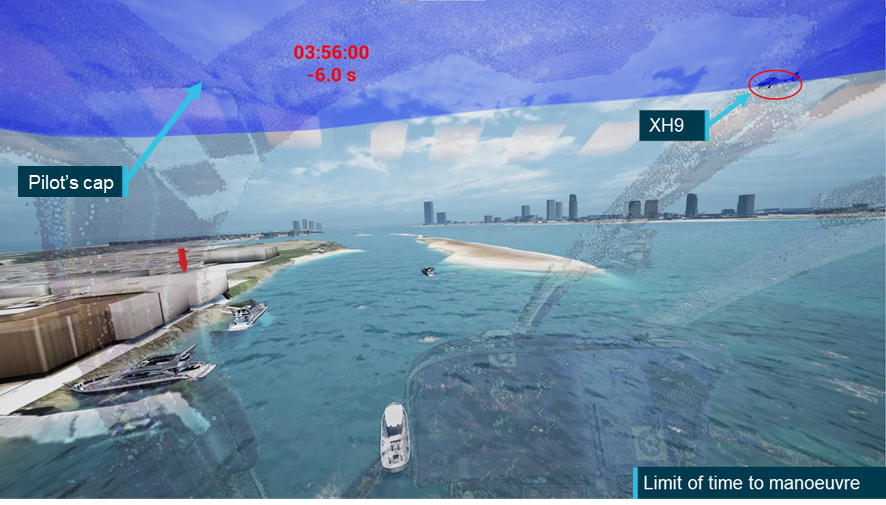
Note: Pilot’s cap is represented by the transparent blue section at the top of the image. Source: iwiation GmbH, annotated by the ATSB
Operator’s EC130 vision test
Following their review of the draft report, the operator provided a video titled ‘EC130 vision test’. The video was frame-in-frame footage of the new HOFO lifting an EC130 into a hover at the park pad. Action cameras were mounted to the pilot’s head and on the left of the cabin looking right (Figure 40). The recording showed a helicopter hovering at the park pad, the pilot coordinating with an inbound helicopter and using scanning techniques to demonstrate detection of an inbound helicopter.
The value of the operator’s ‘vision test’ as an investigative tool was limited. The limitations included:
- the pilots were aware of each other’s presence
- the fly past was coordinated
- the pilot at the park pad waited in the hover for the inbound helicopter
- the resulting relative bearing between the helicopters changed continuously (as opposed to staying the same in a collision scenario)
- the position, speed and profile of the inbound helicopter was not verified to be the same as XH9
- the position, attitude and orientation of the park pad helicopter was not verified to be the same as XKQ
- the position of the pilot and camera was not verified to be the same as the eye position of the pilot of XKQ.
The video demonstrated that if a pilot is aware of in inbound helicopter, coordinates with it and waits in a high hover over the helipad to establish visual contact, that they can see it and track its progress. The operator’s vision test’s value to the investigation lay solely in demonstrating the scanning techniques employed by the operator. The ATSB analysed the expected outcome of the scanning techniques demonstrated in the operator’s video via the results of the sensitivity analysis in the Visibility study.
Figure 40: Still images during EC130 visibility testing captured from the operator’s video

Source: Sea World Helicopters
Sensitivity analysis of opportunities to see the other helicopter
The ATSB’s Visibility study analysed the location of each helicopter relative to the eye position of each pilot and considered whether cockpit structures would shield the target helicopter. The study also conducted a sensitivity analysis consisting of 2 elements. The first assessed the effect of movement from the eye position (sideways, vertically and forwards) on airframe shielding of the other helicopter. The second considered the rotation of the pilot’s eyes assessing the impact of the change in field of view on the detectability of the approaching aircraft. Note that the sensitivity analysis is purely based on geometry, it does not consider environment or conspicuity of the target aircraft and does not represent natural pilot movement or consider the context of the mental models and goals of the pilots, or any risk controls associated with the activity.
In the operator’s EC130 vision test the pilot used 2 types of scanning movement. Measurements of the change in the pilot’s eye position and head inclination and rotation during these scanning movements were calculated by analysis of the operator’s video.
The first scanning movement was announced as a ‘normal scan’. It was conducted when the pilot knew the helicopter was there and the pilot rotated their head about 75 degrees to the right without their head moving from the nominal position before acquiring the inbound helicopter. This movement would not have revealed a conflict for the pilot of XKQ. From their eye position, XH9 was shielded the entire time of the flight (Figure 41).
Figure 41: Shielding chart of pilot of XKQ’s calculated eye position
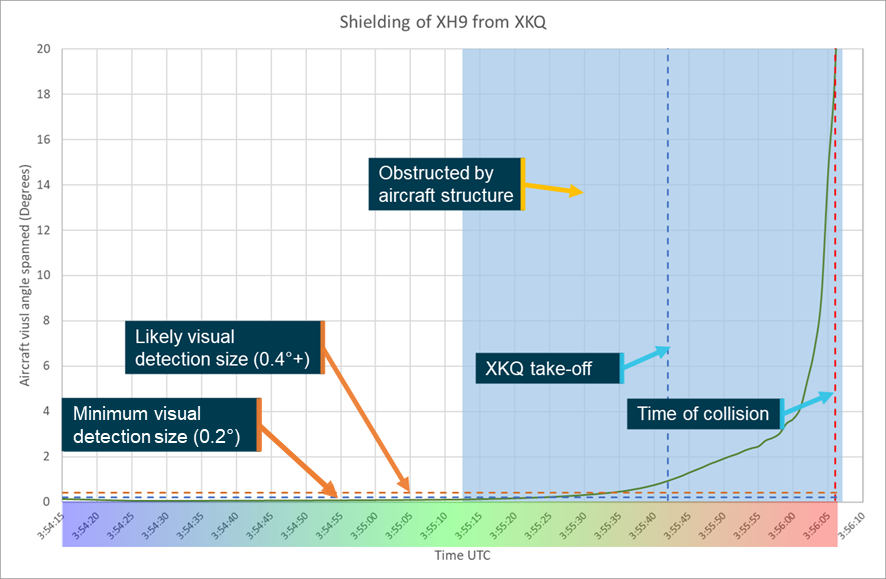
Source: ATSB
The second scan during the operator’s vision test was announced by the pilot as a ‘quick scan’ and conducted after the target helicopter had passed to search for additional unannounced targets. In addition to the rotation to the right, the pilot tilted their head about 30 degrees forward. That moved their eye position about 75 mm forward and 90 mm down for about 3 seconds. The closest sensitivity analysis measure to that scan was the ‘short pilot position’ (Figure 42). That moved the pilot’s eye position 80 mm forward and 110 mm down.
For the pilot of XKQ the operator stated that the check should be conducted before transitioning to forward flight. Figure 42 showed that during that time there was a 1‑second gap when at that position, XH9 traversed the upper right skylight. The 3‑second movement and the pilot’s gaze would have to coincide with that opportunity to detect a conflict.
For the final 13 seconds of the flight the same movement may have revealed XH9 if the pilot looked to the location of XH9 from the ‘short position’. However, it is possible that the pilot’s cap may have still prevented detection unless the pilot also tilted their head back as they were leaning forward.
The sensitivity analysis found the pilot of XKQ’s cap would provide protection for interference from the sun. However, the analysis showed that in scenarios where movement of the pilot eye position reduced shielding from cockpit structures (moving forwards, down or left), if the pilot continued looking straight ahead, the peak of the cap would shield the pilot’s view of XH9 in the times it was not shielded by helicopter structure. For a detailed description of the sensitivity analysis see the Visibility study.
Figure 42: Sensitivity chart for short position
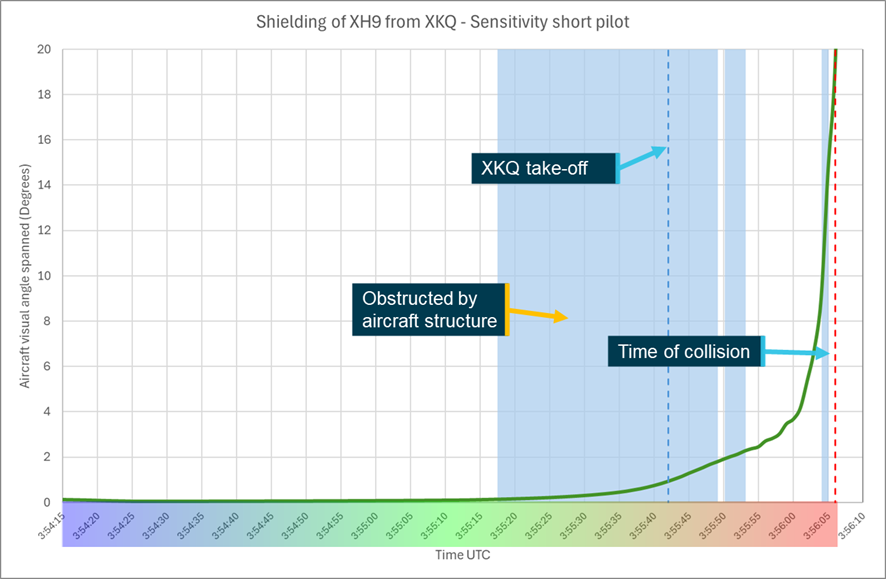
Source: ATSB
For the pilot of XH9, the sensitivity analysis found that movements of head position 50 mm to the left or 100 mm to 200 mm forward would reduce or remove the structural shielding from the pilot’s eye position, resulting in an increase in likelihood of detection. The analysis found that looking to the left (towards the target aircraft) would have also increased the likelihood of detection by placing the aircraft closer to the centre of the pilot’s vision where detection is more likely.
As previously stated, this analysis is based only on line of sight. It does not consider:
- awareness or expectation of conflicting traffic on the part of the pilots
- competing priorities for pilots
- assistance from risk controls not available to the pilot
- limitations of visibility and conspicuity.
Collision geometry
Tracking data showed that, at the time of the collision, the helicopters had a relative flight path angle of 73° (Figure 43). XH9 was approaching to land at 27 kt groundspeed, descending at 640 fpm[34] while XKQ was climbing at 42 kt and 590 fpm.
Figure 43: Flight paths at time of collision
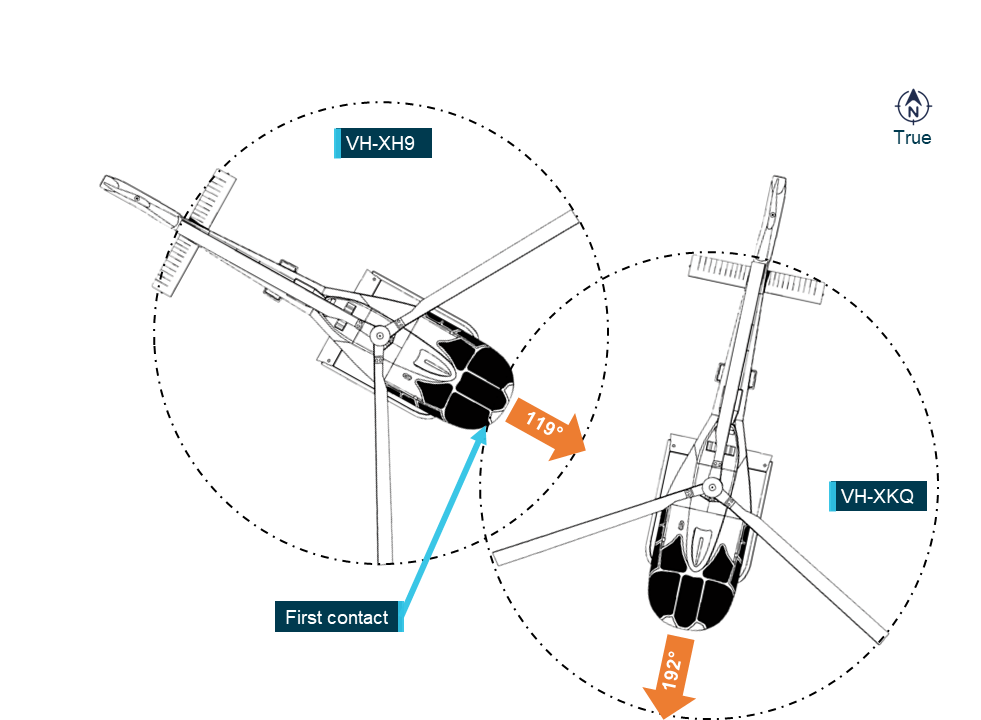
Note: EC130 main rotor blades rotate clockwise as viewed from above. Source: ATSB
The first contact was made with XKQ directly in front of XH9 when the main rotor blades of XKQ pierced the lower forward cabin windows and windscreen frame structures. Due to their relative flight paths, the main rotor blades of XKQ passed through XH9’s forward cabin multiple times. The nose of XH9 then collided with the Fenestron of XKQ.
XKQ continued straight ahead and broke up in‑flight approximately 2 seconds later with the fuselage, main rotor system, engine, and Fenestron falling separately onto the sandbar below.
CCTV recordings showed control of XH9 was momentarily lost. However, due to the flight controls being undamaged, the pilot quickly regained control. Approximately 1.5 seconds after the initial contact, XH9 was seen to make a sharp left descending turn through approximately 270° and then straighten to make a steep approach to the sandbar for a controlled landing.
Other testing
Examination of antenna components from VH‑XKQ
The Southport Airfield CTAF recordings demonstrated intermittent transmission from XKQ (see Common traffic advisory frequency (CTAF) recording). Examination of XKQ’s Com 1 radio revealed faults but no fault sufficient to cause transmission failure. Examination of the Com 1 antenna was conducted (see also Appendix A – Antenna examination).
The antenna components removed[35] from XKQ were:
- the VHF antenna (manufactured by Chelton, part number 21-4B, serial number 9906)
- the airframe mounting blister panel for the antenna (manufactured by Airbus, part number 350A 65 25 28.59)
- a short length of radio frequency (RF) coaxial cable (manufacturer unknown, part identifier 1RCA23E) and its BNC connector (manufacturer unknown) (Figure 45).
Testing was conducted in 5 stages:
- functional testing
- laboratory visual examination
- micro-computed tomography (CT) scanning
- manufacturer testing
- laboratory destructive testing.
Figure 44: The VHF Com 1 antenna (main) from XKQ at the accident site (inset)

Source: ATSB
Functional testing results
Connected to a handheld VHF radio, the antenna received broadcasts on 2 different frequencies without issue, but the transmission tests failed. A voltage standing wave ratio (VSWR)[36] test with the RF coaxial cable and antenna attached to a meter read 2.6. Application of fingertip pressure to the exterior of antenna coaxial connection caused the VSWR to vary between 2.6 and 1.8 and at one point showed 1.1. A value under 2 is considered acceptable (Bahl, 2009).
As the VSWR test showed improvement with slight pressure on the coaxial connection, transmission was tested with load from 4 different points. Looking forward as the antenna would be mounted, gentle pressure was applied via the coaxial cable connection in the fore, aft, up, and down directions. The test identified nil transmission when pressure was applied fore, aft and up, and a broken transmission with downward pressure.
Laboratory visual examination
The antenna and section of coaxial cable were visually examined at the ATSB’s technical facilities in Canberra (Figure 45). The antenna displayed evidence of physical damage where slight bending, scuffing and abrasion damage had occurred to the radiating element. There was no damage visually apparent to either the BNC[37] connector, or to the antenna base.
The bead of sealant[38] around the blister panel on the airframe had degraded and was absent at several locations around the bond line. Sealant between the blister mount and the antenna ground plate was complete yet had low adherence (very easy to remove), with some areas of nil adherence, likely due to deterioration over time and/or poor surface preparation. Further, the sealant between the antenna whip and coaxial body had gaps, exposing the join line in several locations.
The ground plate from the antenna, and the mounting blister had sustained extensive corrosion damage to the exposed aluminium surfaces at each fixing hole location. Surface corrosion on the antenna plate and mount surface had occurred.
Examination of site images captured the morning after the accident revealed the wreckage had shifted due to immersion of the sandbar with the early morning high tide that had swamped the site. While the antenna base and blister panel were determined to be clear of the waterline, it could not be ruled out that they were subject to immersion in salt water due to wave action.
Figure 45: The Com 1 antenna and BNC connector from XKQ
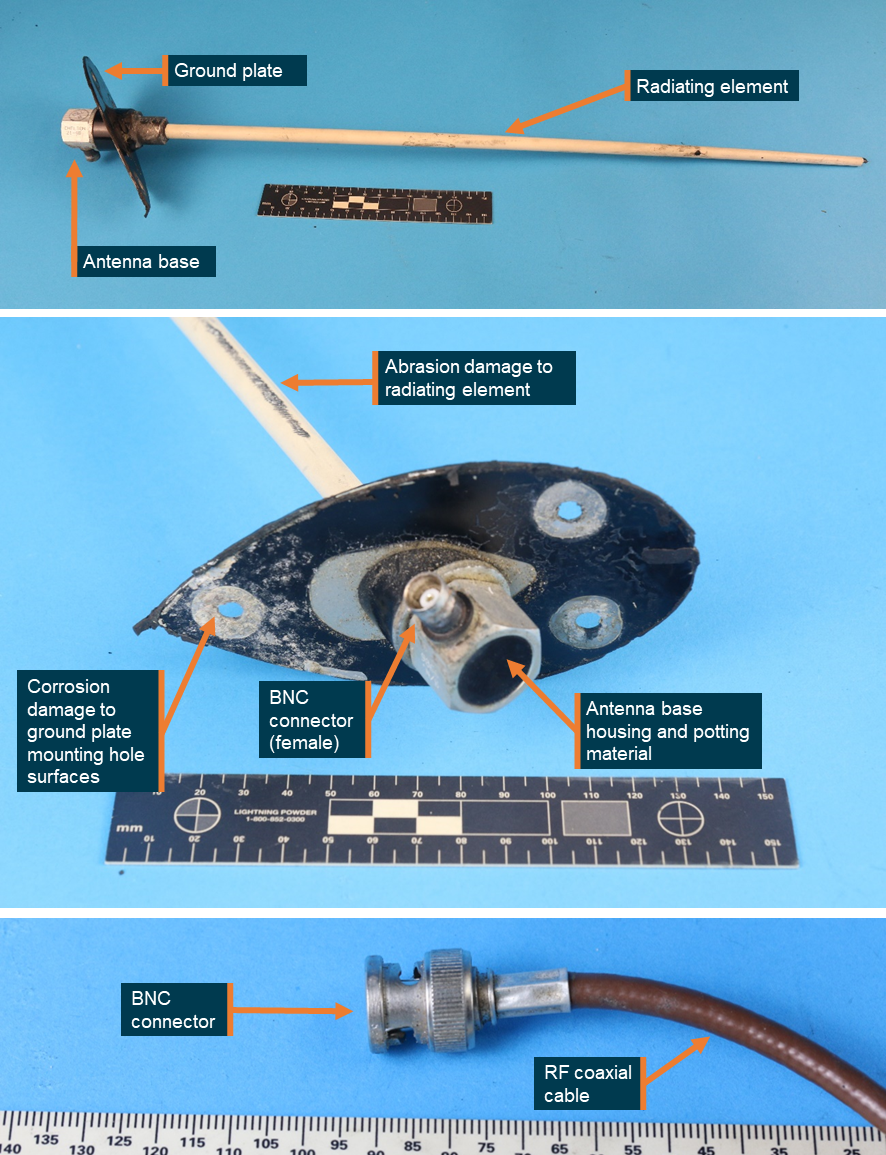
Surface corrosion was identified to each of the underside mounting holes of the ground plate. Source: ATSB
Micro-computed tomography
The antenna was submitted to the National Laboratory for X-ray Micro‑Computed Tomography (CTLab) at the Australian National University.[39], [40] Computed tomography (CT) scanning enabled high-resolution non-destructive evaluation of the internal condition of the antenna base and BNC connector prior to their disassembly.
The scans identified a crack indication within the soldered joint between the circuit board (Figure 46) and the link wire to the antenna base. Additionally, a potential defect was indicated where a single wire was identified to be protruding from the centre pin from within the BNC connector (Figure 47).
Figure 46: An X-ray of the antenna base identified a crack indication where the link wire was soldered to the circuit board (prior to destructive examination)
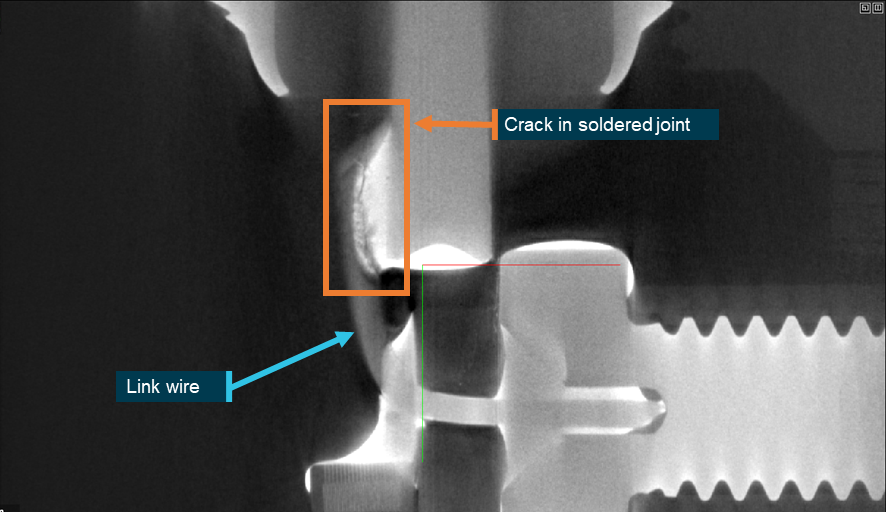
The X-ray image was captured when the antenna was intact. Source: Australian National University CTLab, annotated by the ATSB
Figure 47: An X-ray of the RF cable BNC connector identified a single RF cable wire protruding from the connector pin (prior to destructive examination)
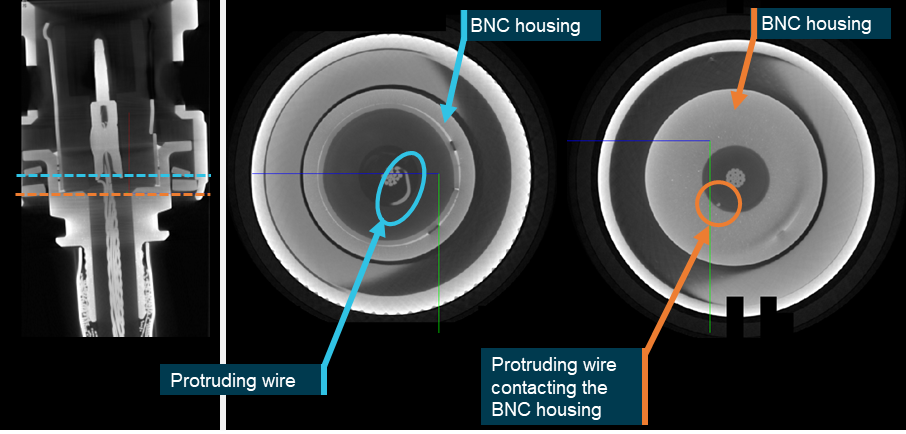
The X-ray image was captured when the BNC connector was intact prior to destructive sectioning. Source: Australian National University CTLab, annotated by the ATSB
Antenna manufacturer examination
Following the micro-CT examination, the antenna and the RF cable containing the BNC connector were submitted to Chelton (the antenna manufacturer) in the United Kingdom for electrical testing. An Accredited Representative to the investigation from the Air Accident Investigations Branch witnessed the testing on behalf of the ATSB.
Chelton confirmed that the part number 21-4B antenna from XKQ had been manufactured in 2008. They further advised that of the 2,166 21-4B antennas that had been produced in the last 10 years, 18 were returned, however no specific electrical faults were identified with those returned units.
Chelton’s report from the electrical testing noted:
- the antenna had sustained physical damage and demonstrated intermittent performance
- the RF cable containing the BNC connector displayed signs of corrosion damage and highly intermittent behaviour
- they were unable to determine if the physical damage was present pre-accident.
Destructive examination – antenna base
The antenna and coaxial cable were returned to the ATSB for destructive examination at the ATSB’s technical facilities in Canberra. Because irreversible changes were to be introduced during the examination, representatives of the directly involved parties to the investigation were invited to observe.[41]
The potting compound[42] from within the antenna base was dissected to expose the internal circuit board within the antenna base (Figure 48). High magnification optical examination confirmed that a through-crack (fracture) had developed where the link wire had been soldered to the circuit board, in the location previously identified from the micro-CT.
It was noted that the fracture surfaces of the soldered region for the link wire were discoloured from oxidation, which indicated that the cracking and fracture of the joint had not recently occurred and was unlikely to have been produced during the potting compound removal process. It was noted that the link wire that had fractured contained a portion that displayed an absence of remnant solder.
There was no evidence of degradation to the potting material as it remained firmly adhered in place to the circuit board within the antenna base. There was no evidence of corrosion to the internal surfaces of the antenna base or the circuit board. Because the antenna base remained sealed, the corrosion (oxidation) rate of the soldered link wire was therefore considered likely to be very low with restricted opportunity for external contaminants to migrate and oxidise the surfaces.
Figure 48: View from within the antenna base showing that the link wire at the soldered joint had cracked then fractured from the circuit board and then over time the surfaces had oxidised
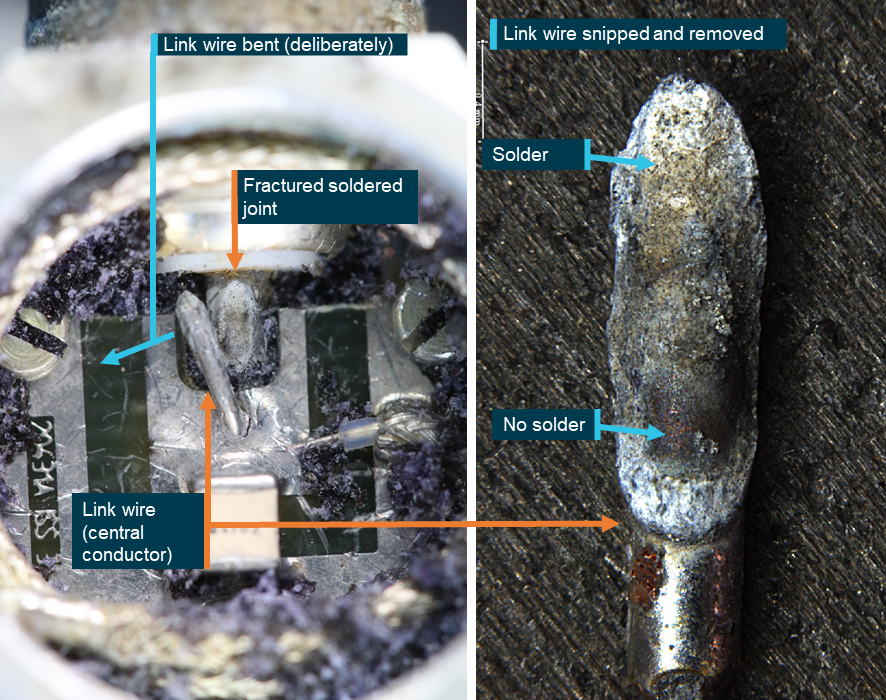
Upon removal of the potting compound, the link wire (central conductor) was able to be moved to the side, confirming that it had fractured from the circuit board. Source: ATSB
Destructive examination – BNC connector
The BNC connector was destructively cross‑sectioned to expose the constituent parts. A single wire from the core of the coaxial cable was found uncontained and outside of the contact pin (Figure 49), which was consistent with the defect identified during the micro-CT examination. Chelton indicated that an electrical fault could develop in the connector of the RF cable installed on the aircraft if that wire contacted the main body of the BNC connector.
Figure 49: Stray wire from the core of the coaxial cable within the BNC connector was found outside the centre pin
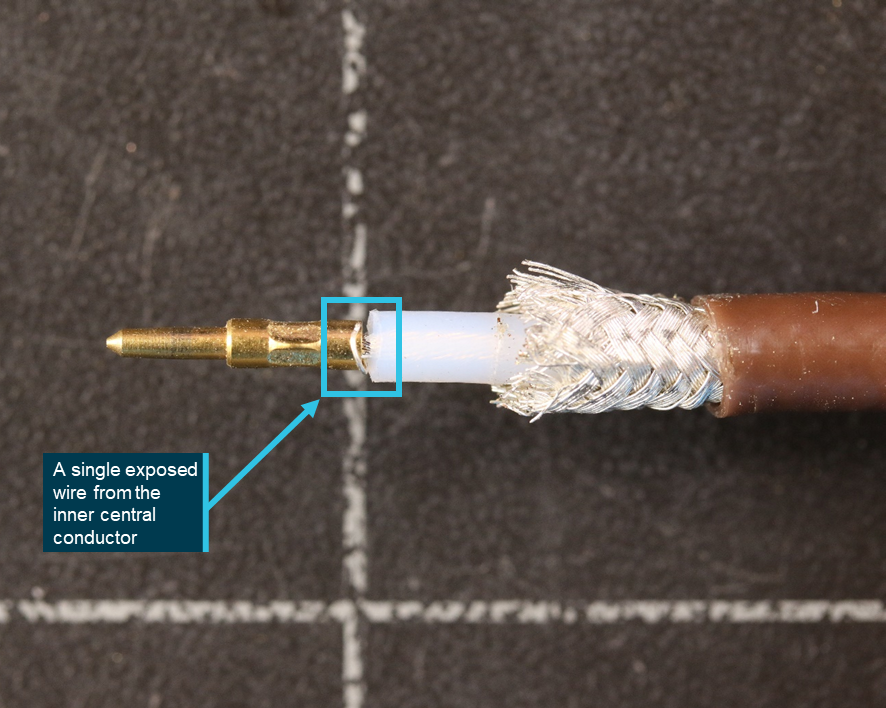
Source: ATSB
Summary of antenna damage and defects
During post-accident electrical testing, micro-CT scanning and the destructive examination, defects and intermittent performance were identified with the VHF Com 1 antenna, the blister panel, and the RF coaxial cable and its BNC connector.
Prior to recovery, the helicopter airframe had been partially immersed in salt water. As there was an 18‑month period between the date of the accident and the conduct of the examination, the corrosion that had developed on the alloy surfaces between the antenna mounting plate and blister panel may have developed after the accident. The level of corrosion prior to the accident, if any, could not be determined.
The Com 1 antenna exhibited relatively minor scuffing/abrasion to the white coated surface and a slight bend to the radiating element. The antenna damage was minimal compared to the destruction incurred by XKQ’s airframe. Additionally, there was no evidence of physical damage to the airframe mounting blister panel, the antenna base (containing the link wire and its circuit board), nor was there any external damage to the BNC connector and the attached RF coaxial cable. The overall presentation of the antenna damage was inconsistent with contact from a high energy object during the midair collision, or from terminal impact with the sand bar.
Cracking and fracture of the link wire from within the antenna base was examined to determine if it had occurred either prior to or at the time of the accident. Fracture surfaces that are newly created typically appear bright and shiny, which contrasts with the fracture surfaces from the soldered link wire that were dull and had oxidised. Because the internals of the antenna base had been sealed from the external environment by the potting compound, had the link wire fractured during the accident sequence, it is considered likely that the surfaces would have remained bright and shiny, rather than dull and oxidised. The aged appearance of the link wire fracture surfaces indicates that the defect had been present for a considerable period and that it was likely present prior to the accident.
Antenna mounting plate – corrosion effects
In antenna systems, especially those used for communication and navigation, the mounting plate acts as a ground plane, a critical component that reflects radio waves and ensures efficient signal transmission and reception. Corrosion affects the impedance matching[43] between the antenna and the mounting surface, causing signal reflection. This reflection lowers the antenna’s efficiency, limiting its range (Volakis, 2019).
Additionally, corrosion introduces parasitic resistance and capacitance on the mounting plate, increasing RF noise. This noise interferes with the antenna’s ability to cleanly transmit and receive signals, which can result in unclear communication or unreliable data reception (Shaffer, 1981).
Antenna base – soldered joint defect
A crack in a soldered joint within the circuit board of an antenna base can impact both the transmit and receive functions of the antenna. The crack creates an unstable connection that is vulnerable to vibration and temperature changes that are common in aviation environments. The instability can result in reduced efficiency and intermittent connectivity, disrupting both transmission and receipt of signals (Collin, 1992).
When transmitting, increased resistance due to the crack reduces the power output by dissipating energy as heat, limiting the range and clarity of outgoing signals. For reception, the crack’s resistance can lead to weaker signal capture, reducing sensitivity and potentially causing degraded signal quality. The cracked joint can also generate RF noise, which can interfere with the antenna’s ability to receive clear signals (Balanis, 2016).
BNC connector – stray wire effects
A stray wire protruding from a connector pin and contacting the BNC housing can have several effects. This unintended contact can result in a short circuit between the RF signal and ground, leading to a disruption of the signal path. As a result, the RF energy intended for transmission or reception may be diverted, causing significant signal loss or degradation (Pozar, 2017).
The interaction between the stray wire and the BNC housing can also introduce electromagnetic interference into the antenna system (Bilal and others, 2024). When the stray wire contacts the housing, it may cause unwanted coupling, which distorts the RF signal. This distortion can lead to issues such as reduced range, poor signal quality, or even total failure to transmit or receive. However, as transmission voltage is much higher than receive voltage, a stray wire could impact transmission to a greater extent than reception.
Survival information
When assessing whether an aircraft accident is survivable, several aspects need to be considered, including:
- acceleration and velocity changes imparted on the aircraft occupants
- occupant restraints
- liveable space inside the aircraft maintained
- post-crash factors.
The ATSB conducted an analysis of this accident using research and data from crashworthiness testing literature to assess the rated survivability of the accident. The results are discussed in detail in Appendix B – Survival analysis, and summarised here.
VH-XH9 passenger survival aspects
The forward cabin of XH9 was significantly compromised by contact with the main rotor blades and Fenestron from XKQ, resulting in the windscreen and forward cabin structure being destroyed, with acrylic window debris entering the cabin causing serious injury to the pilot and 2 front passengers, and minor injury to the 3 rear passengers (Figure 50). The flight controls remained intact and allowed the pilot to continue flying.
Following the contact with XKQ, and after momentary loss of control, the pilot landed on a nearby sandbar. While it was later identified that passengers were not correctly restrained (see Use and fitment of seatbelts below), this was of no consequence due to the controlled landing. All passengers were able to self-evacuate and were treated by first responders, with the pilot and 2 passengers being later transported to a local hospital.
Figure 50: VH-XH9 seating map and injuries
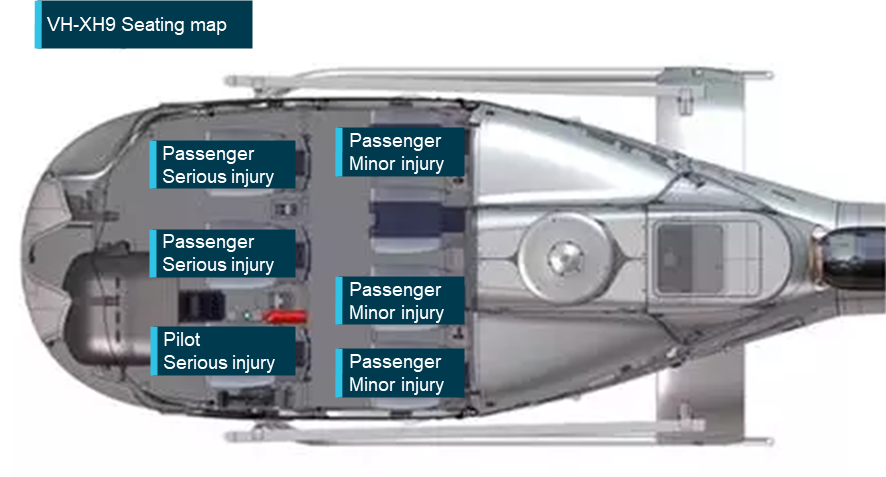
Source: Airbus Helicopters, annotated by the ATSB
VH-XKQ passenger survival aspects
Following the collision, XKQ fell to the sandbar. The fuselage struck the sand on its right side and compressed, resulting in fractured door frames, floor and undercarriage skids. The fuel tank also failed, fracturing into many pieces under the hydraulic loading with fuel being spilt in multiple directions. The fuselage then bounced approximately 0.5 m indicating the wet sand and fuselage absorbed considerable energy. Following the bounce XKQ rolled to the left, stopping upside down about 5 m away from the initial impact location.
Except for some damage to the composite seat buckets, the seats in XKQ withstood the loads applied without failure. The liveable space within the cabin was partially reduced (see Appendix B – Survival analysis), with the compression being stopped by the floor and roof bearing onto the seatbacks. Some occupant restraints did not perform optimally and others either completely or partially released. Some of this poor performance can be attributed to incorrect fitment and poor positioning of restraints, and at least 4 of the occupants were not correctly restrained.
Immediately after the impact, no occupants were capable of self-evacuating. All occupants were partially or fully unconscious, or fatally injured. Members of the public on the sandbar arrived at XKQ within 60 seconds. The first passenger was extracted within 40 seconds of their arrival, and 2 other occupants within 3 minutes.
It was reported by those first on the scene that within minutes the rear left outboard and rear right outboard passengers were conscious and responsive, however the rear left outboard passenger was trapped under the wreckage. Spilled fuel poured onto the trapped passenger. Members of the public found buckets and poured seawater over the trapped passenger to dilute the fuel and reduce the risk of chemical burns. Two survivors were airlifted, and one was transported by ground ambulance, to local hospitals.
As a result of the impact with terrain, the pilot and 3 passengers were fatally injured, and 3 passengers were seriously injured (Figure 51). It was determined that the impact experienced by the occupants of XKQ was at least 7 times more severe than that considered to be a 95th percentile survivable accident. Therefore, the ATSB considered this accident, based on existing survival data, to be normally not survivable, even though there were 3 survivors. This demonstrates the complexity of accident dynamics and the limitations of existing, outdated research and tools to support analysis of aircraft with composite airframes and multipoint safety harnesses.
For an accident to be survivable, the helicopter must provide a protective structure and ideally absorb energy from the impact forces, provide appropriate restraint to the occupants, and protect occupants from adverse environmental and post-crash factors. The magnitude of forces, location within the airframe, and intrinsic factors such as age, sex, health and physical conditioning can affect an occupant’s ability to tolerate impact forces.[44]
While the impact forces experienced in XKQ were assessed as not normally survivable, the variability between the occupants’ position in the helicopter and their individual characteristics, while not confirmed to be the reason, could potentially explain why some passengers were able to survive the impact.
Figure 51: XKQ seating map and injuries
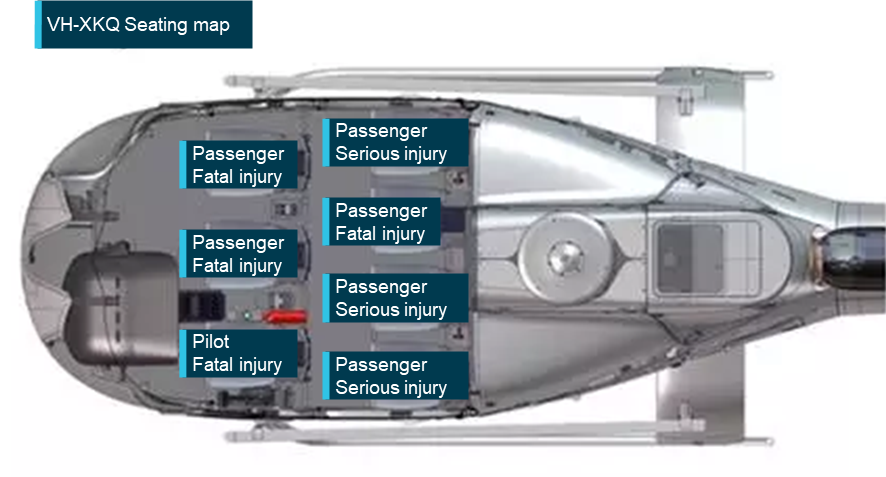
Source: Airbus Helicopters, annotated by the ATSB
VH-XKQ restraint performance
Three Airworthiness Directives assigned to Pacific Scientific buckle assemblies were reviewed and found not to be applicable to those fitted to XKQ. To rule out an unknown fault, the buckle assemblies from XKQ were recovered and initially submitted for X-ray examination at the ANU CTLab, then tested by the ATSB for serviceability. This included testing of the inertia reels and buckles for release and locking, with all found to be functioning correctly. The buckle assemblies were checked for retention of belts, release of belts, and correct action of the shoulder harness release plate and were all found to be working correctly. The only anomalies found were an additional dog spring located in the buckle of the pilot’s seatbelt and the separation of a normally fixed seatbelt tang[45] from the centre buckle of the rear left inboard passenger lap belt. While the additional dog spring was technically an incorrect installation, it did not appear to affect the buckle’s performance. The release of the seatbelt tang from the central buckle of the rear left inboard passenger lap belt could not be explained and remained latched appropriately in testing.
While the restraints on XKQ were all shown to be functional post-accident, video footage from passengers’ mobile phones and interviews with first responders showed that the restraints did not perform as expected during the accident sequence. The review identified:
- The front right passenger’s shoulder straps did not remain connected, and the passenger could be seen in video footage to flail significantly outside the cabin restrained only by the lap portion of the restraint system.
- The rear right outboard passenger could be seen in video footage to flail significantly outside the cabin restrained by their upper torso. First responders extracted the passenger from the helicopter without releasing the seatbelt.
- During recovery, the buckle of the rear left inboard seatbelt was found separated from all seatbelt tangs, when normally one side would be permanently connected.
- The rear left outboard passenger was found under the helicopter, well away from their original seated position.
Helicopter seating
The EC130 had 2 rows of seating. In the configuration used by the operator there were individual seats for the pilot and 6 passengers. Both XKQ and XH9 were fitted with 159 series Sicma Aero seats. The seats had met the dynamic testing requirements of TSO‑C127. That standard complied with the European Union Joint Aviation Requirements 27.562 emergency dynamic landing conditions requirements required for the EC130 certification basis.
Each seat consisted of a carbon composite bucket seat attached to a floor‑mounted aluminium frame featuring a passive energy absorption system designed to attenuate vertical impact loads. For the seats to work as designed the occupant must be restrained properly, sitting back into the seat with the lap portion of the seatbelt low and tight across the hips. The impact forces experienced by XKQ were highly lateral and therefore, while some seats had partially stroked[46] and distorted to some extent, the forces did not align with the principal design direction of the energy absorbing mechanism. In addition, not all occupants were properly restrained, see Appendix B – Survival analysis.
The seats were equipped with Pacific Scientific Co (Meggitt PLC)[47] 4-point (multipoint) restraints featuring manually adjusted lap belts, automatically adjusting inertia-reel shoulder harnesses and a central rotary buckle. The central rotary buckle is designed to release all straps except one (the right lap belt in these helicopters) when the buckle is rotated. Additionally, there is a lever above the centre rotary buckle that releases just the shoulder straps while retaining the lap belt connections. It was noted that the lap belts in each helicopter adjusted in opposite directions. That is, in XKQ the lap belts were tightened by pulling the adjuster strap towards the central buckle while in XH9 they tightened when pulled away from the central buckle.
Each seating position had an aviation headset connected to the helicopter’s avionics. This enabled everyone on board to communicate with each other and provided hearing protection.
Use and fitment of seatbelts
Regulatory requirements for the use and fitment of seatbelts
Regulation 91.570 of the Civil Aviation Safety Regulations 1998 (CASR), applicable to rotorcraft operations, required that the pilot in command direct passengers to fasten seatbelts during taxi, take-off and landing and whenever it is considered necessary for the safety of passengers. Section 9.02 of the Part 133 MOS further detailed when passengers must be restrained, and section 9.03 described what is meant by the fastening of a passenger’s seatbelt:
A passenger of a rotorcraft for a flight is taken to comply with section 9.02 if the passenger fastens the passenger’s seatbelt or shoulder harness, and keeps it fastened, during the period the passenger must be restrained under the section.
In addition, as outlined in regulations 133.235 and 133.240 of CASR and subsections 7.01(1) and 7.02(9) of the Part 133 MOS, passengers must be provided a safety briefing, instructions or demonstration advising when seatbelts must be worn and how to use the seatbelts (see Passenger safety briefing).
CASA advised that in addition to those requirements, an operator must have documented procedures that describe how those regulations have been met to have satisfied 119.205(1)(h) of the CASR which stated:
(h) details of each plan, process, procedure, program and system implemented by the operator to safely conduct and manage their Australian air transport operations in compliance with the civil aviation legislation;
Prior to the implementation of these regulations on 2 December 2021, regulation 251 of the Civil Aviation Regulations 1988 (CAR) similarly required that, for any operation type, passengers and crew wear a seatbelt at certain times. However, in the case of CAR 251, a crew member must be assigned to check that passengers’ seatbelts were fastened ‘without slack’ at the times required.
CASA advised that the requirement to check that seatbelts are fastened ‘without slack’ was covered by regulation 133.240 of the CASR which required passengers to be briefed on when seatbelts must be worn and how to use them (which, if detailing correct information would be without slack), and regulation 91.575 of the CASR which required passengers to follow directions given by the pilot in command.
The previous regulation CAR 251 placed a responsibility on an operator to ensure passengers' seatbelts were fastened 'without slack'. The current regulation no longer required that seatbelts are checked to ensure correct fitment (at any stage, which includes prior to take-off). The operator had met the previous requirement to have a crew member responsible by detailing the pilot in command to ensure passengers had their seatbelts correctly fastened for the duration of the flight. The ground crew would undertake the activity on behalf of the pilot in command (see Operator procedures for the fitment of seatbelts).
Research and guidance about the correct fitment of seatbelts
The seatbelts that were fitted to each helicopter met the requirements of United States Federal Aviation Administration (FAA) Technical Standards Order (TSO) c114.[48] As part of the standard (section d.), manufacturers were to provide instructions for use. However, the ATSB noted that, in general, these instructions were difficult to obtain and at the time of publishing this report, was unable to obtain the operating instructions for the Pacific Scientific seatbelts that were fitted to both helicopters. The ATSB referred to more generic guidance to establish the correct fitment.
Guidance to ensure that a seatbelt, and in this case a multipoint is fitted correctly and will be effective, as advised by various aviation regulators and Airbus Helicopters states:[49]
- For 4-point restraints, the lap belt portion of the restraint should be fitted and adjusted first before the shoulder harness.
- The lap portion of the seatbelt must be placed low and tight across the hips.
- Seatbelts must not be fitted across the abdomen as this can cause internal injuries or result in the person sliding out the bottom of the harness (submarining), nor should they be fitted across the thighs, or the seatbelt will not effectively prevent forward movement.
- Seatbelts must not be twisted, they must be fitted without slack, and adjusted to fit as tightly as comfort allows.
Correct fitment of seatbelts has been shown to reduce the likelihood of serious injury or fatality in an accident and has been highlighted in several previous accidents. For example, NTSB Aviation investigation final report WPR16FA055 (2020), found:
Onboard video imagery recorded during the accident flight confirmed that the pilot's harness lap belt was positioned properly, low and tight across his hips. Of the six passengers onboard, four passengers' lap belt positioning were visible in recorded cabin imagery and depicted that the lap belts were not tight across their hips and that the buckle was at or above their waists.
The loose and out-of-position seatbelts most likely allowed the passengers' bodies to shift out of position on the seat before and during the hard landing and did not restrain the occupants in the proper position for the seat to absorb the vertical landing loads for which it was designed.
Contributing to the severity of passenger injuries was the improper positioning of the passengers' seat belts.
See Related occurrences for a review of Australian and international investigations involving injury due to incorrect fitment or lack of restraint.
Operator procedures for the fitment of seatbelts
Sea World Helicopters’ procedures in the Aircraft Operations manual (SWH-ACO-MAN-15) required the following in relation to seatbelts:
7.1.1 Use of Seats and Seatbelts
a) The pilot in command [PIC] shall occupy a control seat and wear a seat belt properly fastened at all times.
b) The PIC shall ensure that all occupants have their seat belts / harnesses fitted and correctly adjusted during all stages of flight.
While the operation of the seatbelt was depicted on the passenger briefing card, there was no guidance about how to fasten seatbelts in the operator’s procedures.
Sea World Helicopters provided information to passengers about how to fit the different types of seatbelts on each of its helicopter types in its pre-flight safety briefing video, however aspects of existing guidance material were contradicted by examples shown in the video (Figure 52). This was due, in part, to the positioning of the constant wear lifejacket worn by passengers in the briefing video.
Figure 52: Still images from Sea World Helicopters passenger safety briefing video
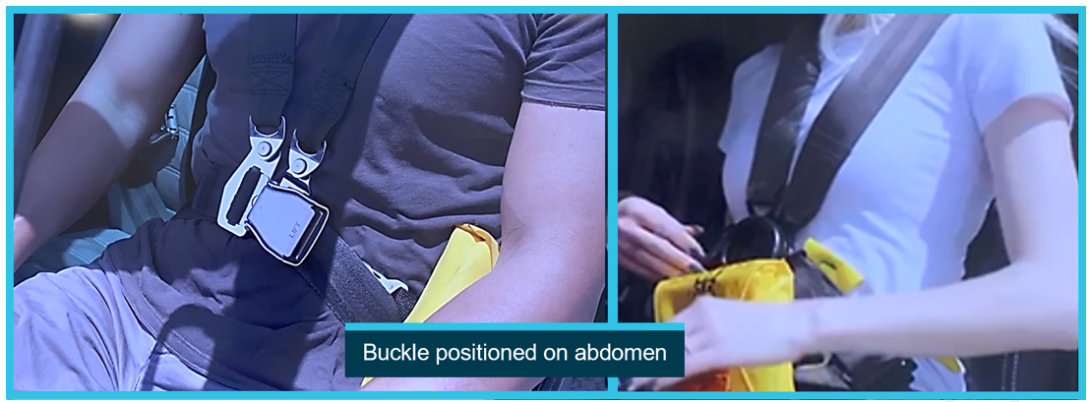
Image shows both Airbus AS350 (left) and EC130 (right) seatbelts. Source: Sea World Helicopters, annotated by the ATSB
Photographs, videos and interviews indicated that at least 4 passengers on the accident flights, and probably more, did not have their seatbelts fitted correctly (Figure 53). Incorrect fitment included:
- the buckle of the seatbelt positioned across the abdomen
- the belt passing above or over the lifejacket creating slack
- twisted seatbelt webbing.
Figure 53: Examples of passenger incorrect seatbelt fitment
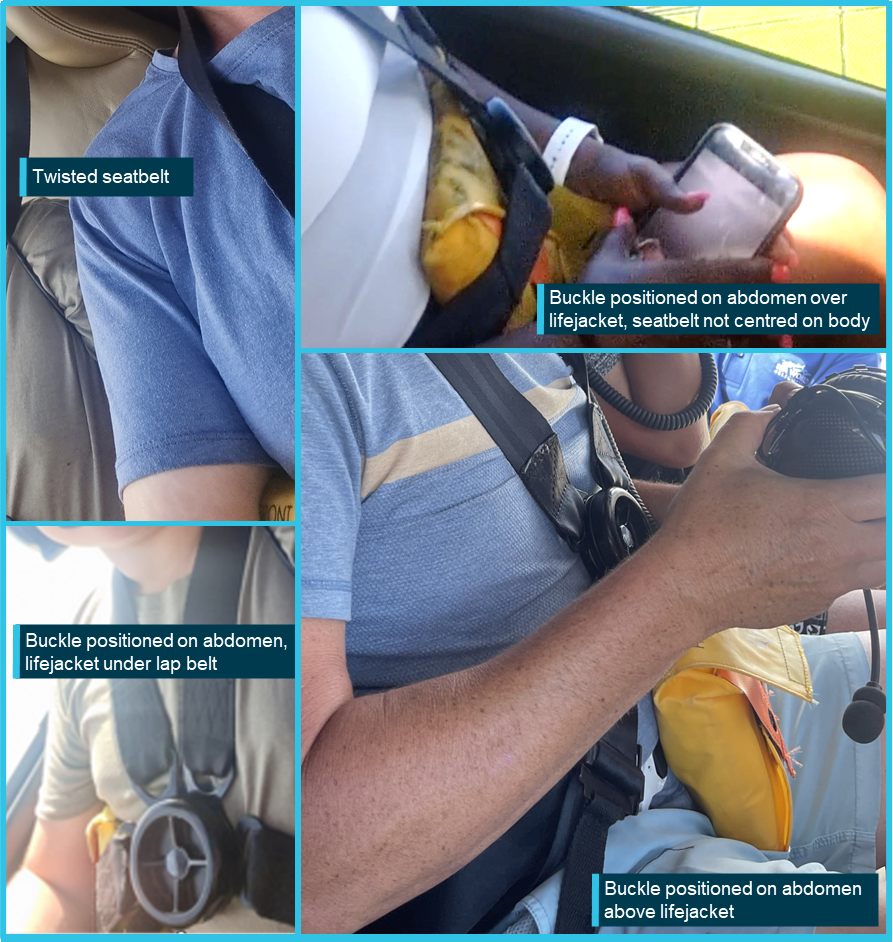
Source: Passenger photographs/video, annotated by the ATSB
Ground crew were tasked with fitting passengers’ seatbelts but were not trained in correct use. Consequently, seatbelts were not being fitted correctly by the operator on a regular basis. In interview, it was reported by one ground crew member that to streamline passenger loading, 2 portions of the 4‑point restraints would already be clipped together. When passengers boarded, there was then only 1 shoulder harness and 1 waist component that would require fastening. Unless the seatbelt was readjusted correctly with the lap belt of the harness fitted low and tight across the hips, this could lead to incorrect fitment of the seatbelt.
Fitment and use of lifejackets
Regulatory requirements for the fitment of lifejackets
Regulations that came into effect in December 2021 moved the requirements from Civil Aviation Order (CAO) 20.11 to Part 133 of the CASRs. The regulatory requirements for lifejackets were set out in section 11.49 of the Part 133 Manual of Standards (MOS) and the regulatory requirement for the fitment or wearing of a lifejacket was in subsection 11.49(3) of section 11.49 of the Part 133 MOS. There were no transitional provisions which still permitted compliance with previous regulation CAO 20.11. At the time of the accident the operator had not transitioned to the CASRs and instead observed CAO 20.11. That required that the lifejacket met the requirements of the TSO, and detailed when a lifejacket must be carried and the times it must be worn.
Subsection 11.49 (3) of the Part 133 MOS ‘Lifejackets and infant flotation cots’, was specific to rotorcraft and stated an occupant must wear the lifejacket for flights over water. Lifejackets were only required for flights where the helicopter cannot reach a suitable landing area in the event one engine becomes inoperative.
Operator procedures for the fitment of lifejackets
Sea World Helicopters’ procedures in the Aircraft Operations manual (SWH-ACO-MAN-15) required the following in relation to lifejackets:
4.10.2 For flights outside of auto-rotational distance from land, other than for the purposes of take‑off and landing, all occupants of the aircraft shall wear a life jacket.
and
7.1.2 Passenger Briefings and Demonstrations
c) Where life jackets are to be worn, the SWH staff members will give a practical demonstration on the ground before the passenger(s) board the aircraft including:
- Correct method of donning and securing the tapes with special instructions relating to any children aboard the aircraft;
- Method of actuating the compressed air cylinder; impress on passengers that life jackets are not to be inflated while the wearer is still inside the aircraft;
- Method of inflating by use of the mouthpiece should further inflation be required or the air cylinder fail to operate;
- Method of actuating the locater light; and
- Purpose and use of the whistle;
The operator used Eastern Aero Marine (EAM) Heli Vest adult lifejackets and EAM infant lifejackets. The Heli Vest is a pouch‑style lifejacket that is strapped around the wearer’s waist, often referred to as a constant wear lifejacket. As published publicly by EAM, its constant wear lifejackets were specifically designed for use in helicopter tour operations. If required, the lifejacket is donned by opening the pouch and pulling it over the head of the wearer. The lifejacket is then ready for use and is manually inflated as required. These lifejackets were used by the operator for passengers and were fitted by ground crew prior to boarding. From videos and photographs, all passengers were wearing a lifejacket on the day of the accident.
There were 2 Crewsaver constant wear yoke‑style lifejackets retrieved from the accident site. These lifejackets are ISO 12402-3 approved. They were not CASA‑approved or permitted by part 21 of the CASR. From passenger video evidence, neither pilot was wearing a lifejacket.
Lifejacket standards and guidance about use
EAM Heli Vest adult lifejackets are approved by the FAA to Technical Standard Order (TSO) C13e. This FAA approval is acceptable to CASA for use on Australian aircraft as detailed in regulation 21.502 of the CASR. To obtain an approval the equipment must meet the standard and undergo testing. One element of the testing ensured that the lifejacket could be donned from a seated position, while wearing a lap belt, within 25 seconds. The testing did not include donning with a multipoint seatbelt.
EAM provided guidance for the fitment of the Heli Vest adult lifejacket (Figure 54). The guidance covered the use of the lifejacket as an independent piece of equipment but did not provide any instruction on its use in the context of an aircraft. Figure 54 shows the operating instructions, available on the manufacturer’s website. These instructions are also printed on the lifejackets for reference by the wearer. In correspondence, EAM told the ATSB the instructions should be reinforced in operators’ safety briefings.
Figure 54: EAM Heli Vest operating instructions
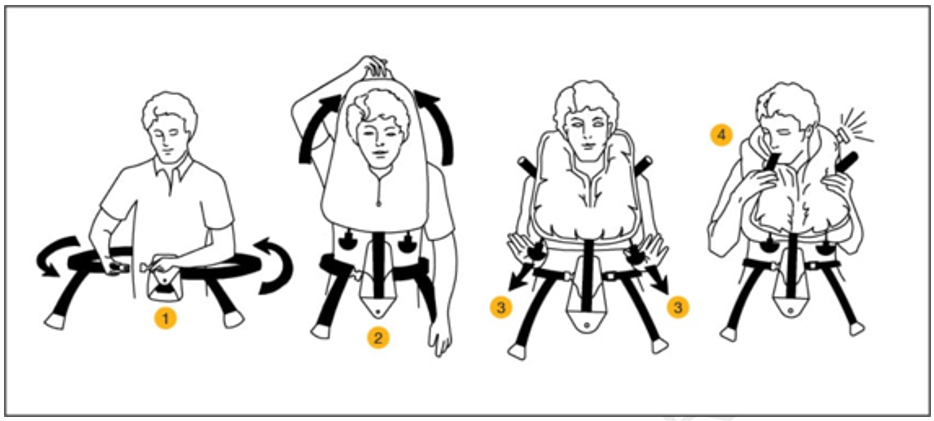
Source: Eastern Aero Marine
Fitment of lifejackets with multipoint restraints
Due to the identification of the incorrect fitment of passenger seatbelts, which was due in part to the presence of a constant wear lifejacket, the ATSB reviewed the prevalence of the incorrect fitment more broadly through a review of social media images. The review revealed numerous examples in the helicopter tourism industry, both in Australia and internationally, and incorrect fitment was not limited to Sea World Helicopters’ operation (Figure 55).
Figure 55: Examples of incorrect seatbelt fitment with constant wear lifejackets

Source: Safety briefing videos from YouTube and other social media
Guidance about the correct fitment of lifejackets with multipoint restraints
Guidance about the correct fitment of a multipoint restraint with a constant wear lifejacket in the context of helicopter tour operations was not readily available. The ATSB found one document that referred to the fitment of a conventional lifejacket and multipoint restraints together in a guidance document for small, fixed‑wing aircraft. The UK Civil Aviation Authority Safety Sense Leaflet 21 (2022) stated:
Wearing the life jacket in a single engine piston aircraft, all occupants should wear their lifejackets in flight. The lifejacket should normally be donned prior to entry into the aircraft and seatbelts should be fastened over the jacket.
CASA, the FAA and Transport Canada advised that they were not aware of guidance material in the context of lifejackets of any form with a multipoint restraint. In addition, information was requested from lifejacket manufacturers, and there was no formal guidance. Some informal advice was previously provided by EAM to the ATSB in 2018. That advice stated:
…recommend the harnesses to be fitted over the vests once they are secured around the occupant's waist, this way you will not compromise the release of the belt itself nor will it interfere with the vest
EAM advised that it would provide the same advice if an operator was to ask them directly. All other known manufacturers of constant wear lifejackets were contacted, and they did not provide and/or were not aware of advice explaining how to integrate their product with existing multipoint restraints onboard aircraft.
The ATSB also sought advice from the FAA Civil Aerospace Medical Institute, which undertakes research related to survivability. It was also not aware of specific guidance or peer reviewed research that addressed the use of constant wear lifejackets with multipoint restraints.
In September 2023 the ATSB released a Safety Advisory Notice (SAN) Fitment of constant wear lifejackets with seatbelts in aircraft (AO-2023-001-SAN-001), which highlighted the lack of guidance for operators about the correct fitment of constant wear lifejackets with seatbelts, and in particular multipoint restraints. The SAN also showed the prevalence of incorrect fitment of seatbelts due to interference from constant wear lifejackets. When released, the notice was sent directly to all known manufacturers of constant wear lifejackets and to regulatory authorities responsible for lifejacket certification, including CASA. The SAN advised:
The ATSB encourages manufacturers of constant wear lifejackets to provide operating instructions and/or guidance material to operators of aircraft on how to wear and use a constant wear lifejacket with a seatbelt (of any configuration) such that it does not interfere with the performance of the seatbelt during an accident.
Further, the ATSB encourages certification authorities to modify lifejacket standards to include the requirement for instructions on how to wear constant wear lifejackets while seated and wearing a seatbelt.
Passenger safety briefing
Regulatory requirements
The CASR Part 133 MOS was in force at the time of the accident and outlined the requirements for subregulation 133.240(1) of CASR in section 7.02 – Safety Briefings, instructions, or demonstrations, before take-off. Subsection 7.02(9) of section 7.02 required the safety briefing include (among other things):
(a) when seatbelts must be worn during the flight, and how to use them;
…..
(f) where the emergency exits are located;
……
(i) if life jackets are required to be carried, and worn, on the rotorcraft for the flight under section 11.49:
(i) where they are located and how to use them; and
((ii) the giving of a warning that life jackets must not be inflated inside the rotorcraft;
…..
(m) the requirement to comply with any safety directions and instructions given by a crew member;
(n) if a safety briefing card, for the rotorcraft, is required to be available to each passenger under subregulation 133.235(2) of CASR:
(i) where to find it; and
(ii) if it sets out different seating configurations for the rotorcraft — which configuration is in use for the flight;
(o) if special survival equipment relevant to a specific environment is intended to be used by a passenger — the location of the equipment and location of written instructions for its use;
(p) when, and how, to assume the brace position, including the position for passengers with infants.
As discussed above, Part 133 of the CASRs came into force in December 2021 and there were no transitional provisions which still permitted compliance with previous regulation CAO 20.11. The operator advised that, at the time of the accident, it was in the process of transitioning to operating under the new regulations and was therefore working with CAO Section 20.11. The briefing requirements as such did not include the location of the safety briefing card (if required), the brace position or that passengers are required to follow crew member instructions.
Research and guidance
CASA provided guidance about passenger safety briefings in a multi-part Advisory Circular (AC) AC 133-10 Passenger safety information. First released in August 2021, the key safety message stated:
Uninformed passengers can degrade the safety effects established by aircraft crashworthiness certification standards and cabin crew evacuation procedures. Conversely, well-informed and knowledgeable passengers contribute to survivability in an aircraft accident or incident.
The guidance explained that operators should be utilising a passenger briefing system that incorporates at a minimum an oral or audio-visual briefing and a passenger briefing card. It was noted that in relation to safety briefing cards, these did not provide an acceptable means of delivering safety information if used by themselves.
The AC also noted:
2.1.2 Accident investigations have shown that survival rates are improved when passengers are provided with accurate and effective information about the correct use of equipment such as seatbelts, and the actions they should take in a life-threatening situation such as how to adopt the brace position.
The AC also detailed suggested information for helicopter passenger safety briefings specifically, and included but was not limited to:
− seatbelts:
- importance of using a shoulder harness(es) where fitted
− flight safety and instructions:
- remain in the seat unless given permission to move, keep clear of the flight controls and any switches at all times, do not distract the pilot during take-off, manoeuvring or landing
− exit location and operation:
- familiarise themselves with the inside of the aircraft and exit locations
- locating the exit in relation to their left or right knee to assist with orientation if the aircraft lands or comes to rest in another position
- operation of all exits
For those operators conducting flights over water, briefing passengers about underwater egress was also encouraged.
In support of the requirement to brief passengers on the brace position, the AC included suggested brace positions for different aircraft configurations and included a position for use by occupants utilising a 4-point restraint in a helicopter. The AC was updated in February 2023 to include the use of 3-point restraints in helicopters.
Further guidance about CASR 133.240 specifically was contained in Acceptable Means of Compliance and Guidance Material Australian air transport operations – rotorcraft released in November 2023, which stated:
The intent of this regulation is for the operator and PIC to take responsibility for providing safety information to every passenger on board. This can be in the form of a briefing, instruction or demonstration. Passenger safety briefings must be given to each passenger who will be carried on the flight. A safety briefing, instruction or demonstration mentioned in this section must be given to a passenger before the rotorcraft’s engines are started for a flight, unless the briefing, instruction or demonstration has been given to the passenger before boarding the rotorcraft, following the operator’s pre-flight boarding procedures.
Airbus Helicopters (2019) had also produced Safety Information Notice 3444-S-25 Correct use of seats and restraint systems to minimize risk of injury, in response to an accident that occurred in Hawaii in 2016 (see Related occurrences). This notice stressed the importance of using the restraint system properly to reduce the risk of injury and provided detail of the emergency brace position.
Research has highlighted the importance of the use of a brace position in helicopters during an emergency to increase the chances of survival. For example, Brooks (1989) highlighted that the brace position increases survivability by reducing the strike envelope of the arms, legs and head on cabin contents and is therefore an important aspect of a pre-flight briefing for passengers.
Operator procedure for pre-flight safety briefings
Sea World Helicopters’ procedures in the Aircraft Operations manual (SWH-ACO-MAN-15) required that passengers be provided a briefing prior to departure which included but was not limited to the following:
7.1.2 Passenger Briefings and Demonstrations
- The use of seat belts and the appropriate method of fastening and adjustment; also recommend that passengers keep their seat belt fastened at all times in case of unexpected turbulence;
- Location and method of operation of emergency exits including doors and other openings which may be used for that purpose;
- Prior to embarkation, the SWH staff members shall ensure that all passengers are referred to the Helicopter Safety card and are familiar with it;
The operator would normally use a pre-recorded video to provide passengers with pre-flight safety information, but if time was restricted, the ground crew would verbally brief the passengers. The procedure in the Base Operating Procedures manual (SWH-BOP-SOP-75) required (amongst other things):
8.1.4 Load controller then
e) Load Controller/Loaders will observe the completion of the briefing video.
f) Load controller removes passengers from Briefing rooms ENSURE GUESTS UNDERSTOOD BRIEFING VIDEO
g) Escort the passengers to the locker area, this is where they are to place any bags, selfie sticks, loose items.
h) Fit life jackets to passengers
While Sea World Helicopters’ safety briefing video covered most of the required aspects (and was available in multiple languages), it did not contain information about the location and operation of the EC130 doors. It also did not contain information about a brace position or where passengers could find the safety briefing card on the helicopter, nor did regulations require it to at the time.
The operator had a safety briefing card specific to the EC130 (Figure 56) available for use. Among other things, the card depicted the location and operation of the EC130 doors and the brace position. The card also showed the fitment of 4-point restraints, however, the restraints were shown fitted to a seat and not a person, and the lap belt was not shown to be tightened before inserting the shoulder straps. While the card was available for use (although its exact location on the day of the accident could not be determined), the time available for passengers to review the card before take-off following boarding was limited.
Figure 56: Sea World Helicopters safety briefing card

Source: Sea World Helicopters
In addition to the pre-flight safety briefing, the operations manual contained procedures for in-flight emergencies, and some of these required the pilot to advise passengers to adopt a brace position. The operator did not provide guidance to pilots on passenger brace positions within the operations manual.
Interviews with surviving passengers confirmed that they had watched the pre-flight safety video. However, they were not provided with any additional safety information from the ground crew or pilot once they had boarded either helicopter, and they had not referred to or been advised of the presence of a safety briefing card.
Meteorological information
Overview
Bureau of Meteorology observations for 2 January 2023 showed that the weather was consistent with forecast conditions. There was a ridge of high pressure extending along the south‑east coast of Queensland, and scattered cloud over land at around 3,500 ft. Moderate south-easterly winds were forecast at around 15 kt with gusts up to 25 kt. While the forecast carried areas of reduced visibility due to showers and smoke, the area of operation was not affected.
The conditions from passenger photographs near Porpoise Point showed good visibility and small waves and a few whitecaps starting to form on the surface of the sea, suggesting wind speeds of 11 to 16 kt (Figure 57). The windsock at the park pad showed an approximate 12 kt easterly wind at the time of departure.
Figure 57: Passenger photographs showing in‑flight conditions
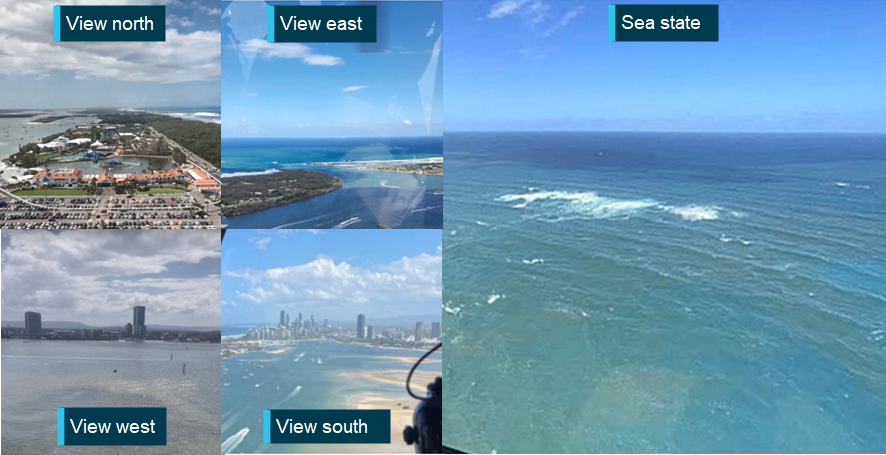
Source: Passengers on board XH9
Prevailing winds
Wind in the area was predominantly from the south‑east, and most approaches to the park pad and heliport were into the prevailing wind (Figure 58).
Figure 58: Wind rose showing prevailing winds
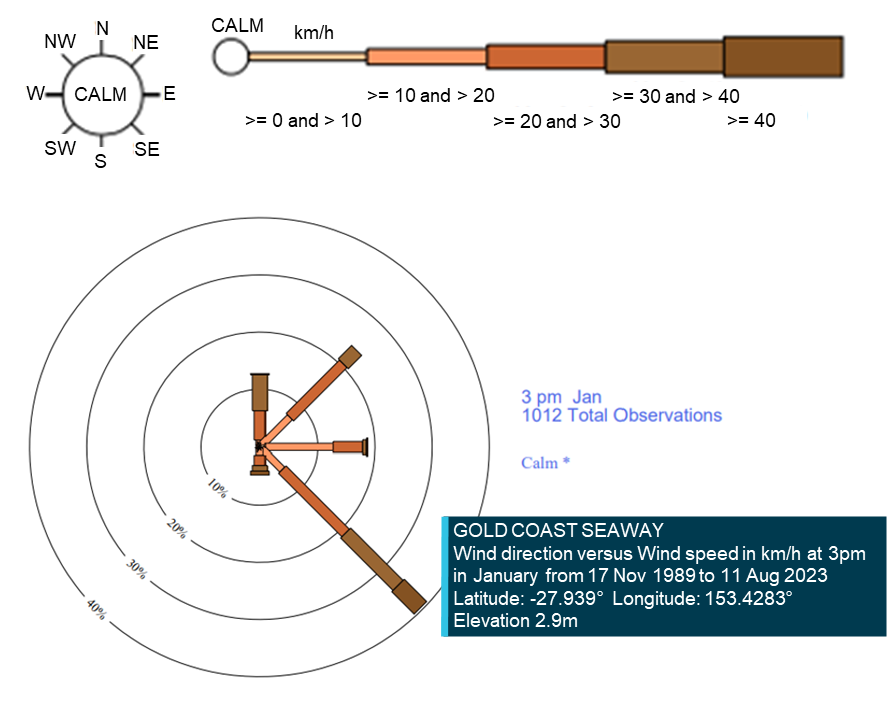
Source: Bureau of Meteorology, annotated by the ATSB
Sun position
The position of the sun relative to the helicopters and the collision location and altitude was obtained from the Geoscience Australia sun and moon position calculator.[50] The location of the sun relative to designed pilot eye position within both XH9 and XKQ for the final 111 seconds of flight prior to the midair collision is displayed at Figure 59 and Figure 60. The location data is presented over a 2-dimensional equirectangular developed from the Visibility study.
Figure 59: XH9 pilot – relative position of sun
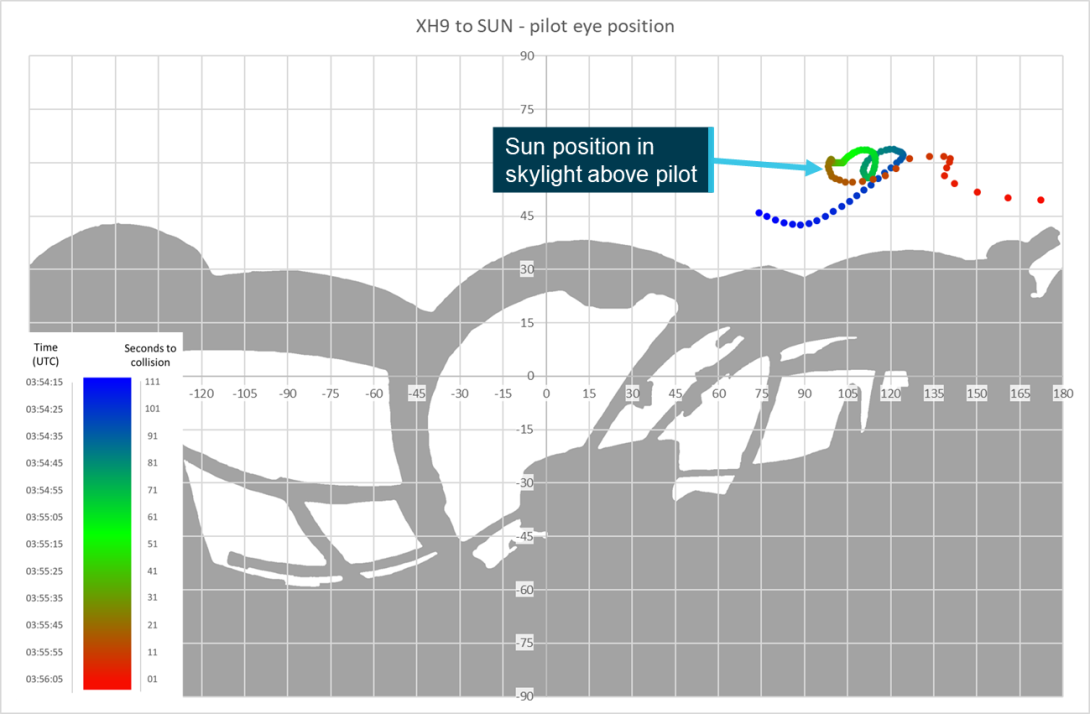
Source: ATSB
Figure 60: XKQ pilot – relative position of sun
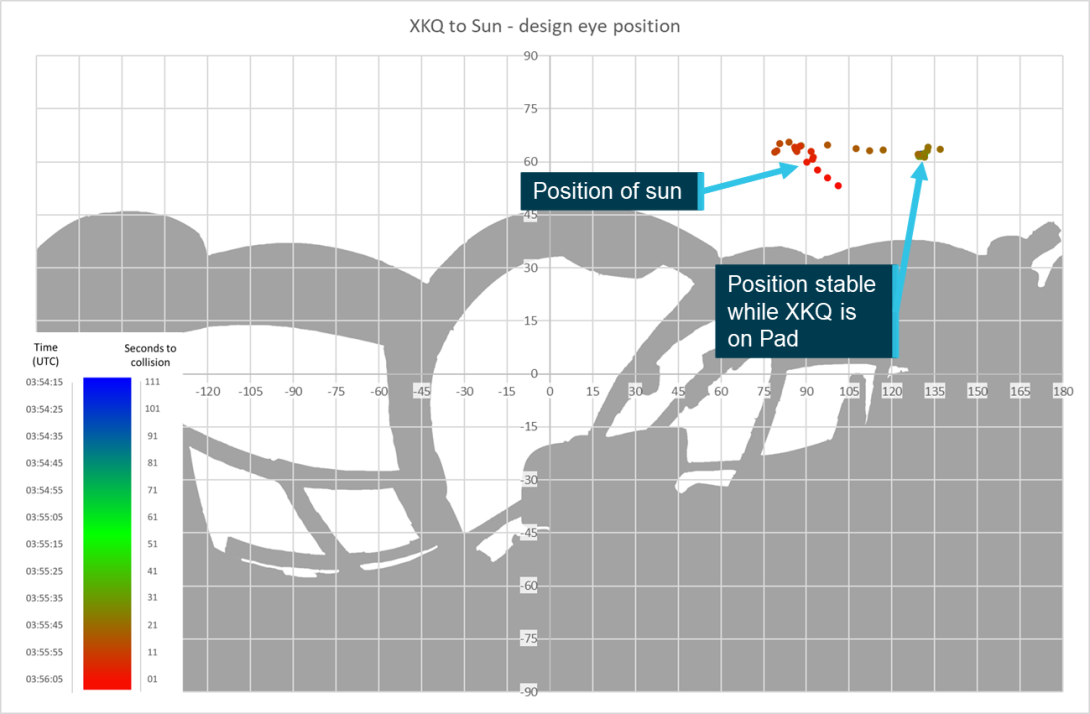
Source: ATSB
Aerodrome information
There were 2 helipad facilities with conflicting approach and departure paths in use at Sea World on the day of the accident. The heliport in the car park of the Sea World theme park, and the park pad, a helipad located within the Sea World theme park.
Both of the facilities were aerodromes and advisory circular AC139.R-01 (CASA, 2024) stated that:
2.1.1 While regulation 91.410 of CASR places the onus on the helicopter operator and pilot in command (PIC) to consider all circumstances associated with safely taking off or landing at a place prior to doing so, it also ensures via subregulation 91.410(3) of CASR that any place that can be safely used for such operations is considered an aerodrome for the purposes of the legislation.
Both facilities had been redeveloped by the operator over the course of 4 years. The park pad was 220 m north of the heliport. High density public spaces flanked each facility on the eastern side.
Ordinarily, aircraft make approaches and departures into wind. In this location the prevailing south-easterly winds (see Meteorological information) and open water allowed for into wind approaches, but public space to the east meant into wind departures were not always available. At Sea World, departures were commonly made with a downwind or crosswind component.
Between 1 December 2022 and 2 January 2023, 884 departures were made with a south-westerly component versus 5 to the north.
Main heliport
As part of the concession agreement with Village Roadshow Theme Parks (VRTP), Sea World Helicopters developed a heliport and dedicated passenger handling facility on the site of the old car park pad (see Organisational and management information). The facility, which covered around 6,000 m2 and provided for 4 independent helipads, opened on 15 August 2019 (Figure 61).
Figure 61: Sea World Heliport
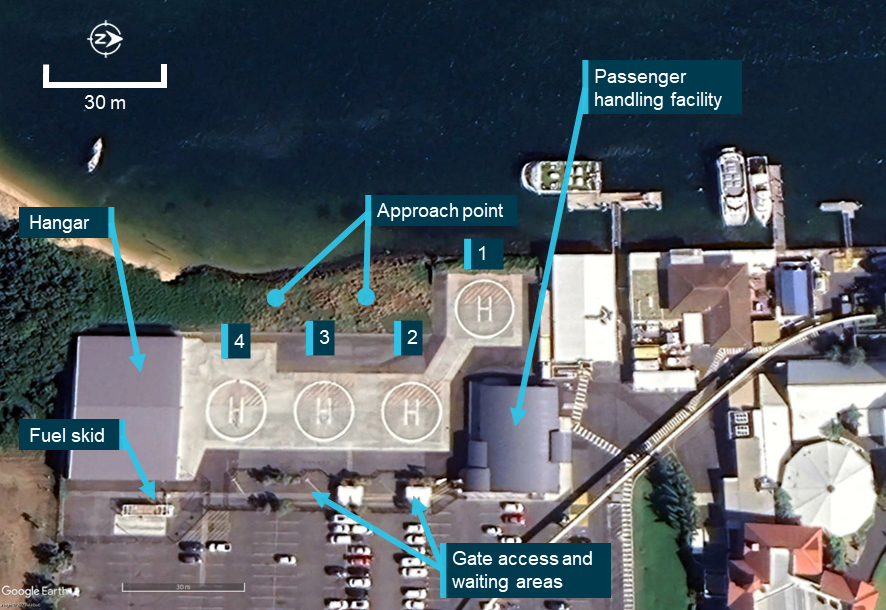
Source: Google Earth, annotated by the ATSB
The windsock was positioned at the north‑east end of the pad adjacent to pad 2. There was a fenced walkway on the east side of the pad to provide access to individual gates for each pad and to keep foreign objects from the car park blowing onto the helipads.
The final approach take-off area (FATO) was the area between the helipads and the water. Helicopters were to approach to a point in space 20 ft high on the western side of the fence and then transition to the helipad. Obstacles in that area included itinerant boats and the fence on the western edge of the helipad which created an edge exposure on approach and departure.
The touchdown and lift-off (TLOF) area at each pad was clearly marked in accordance with available guidance, and large enough to accommodate AS350s (D-12.94 m) and EC130s (D‑12.64 m) and allow them to turn without encroaching on neighbouring pads. Helicopters would always be parked facing east with the nose towards the gate and passenger waiting area which was provided for each pad.
Passenger handling facilities were designed around passenger handling flow. Calibrated scales were set into the floor at four counters where passengers were processed before being directed to a waiting area or briefing room. The briefing room had video briefing in several languages, and led directly to the walkway to the helipads, where passengers would be fitted with lifejackets and accompanied by ground crew for loading into the helicopters.
Approximately 72% of the operator’s traffic flew from the heliport facility in 2022.
The park pad (Figure 62) was owned by the theme park operator Village Road Show Theme Parks (VRTP). It was closed 12 November 2019 following the opening of the new heliport facility on the site of the old car park pad. The park pad was decommissioned as it required refurbishment prior to continued aviation use. It was always the intent of Sea World Helicopters and VRTP to continue operation of the park pad as part of the concession arrangement. However, shortly after the closure of the park pad, the COVID pandemic struck and refurbishment plans were put on hold. The park pad remained unused for over 2 years.
Figure 62: Park pad
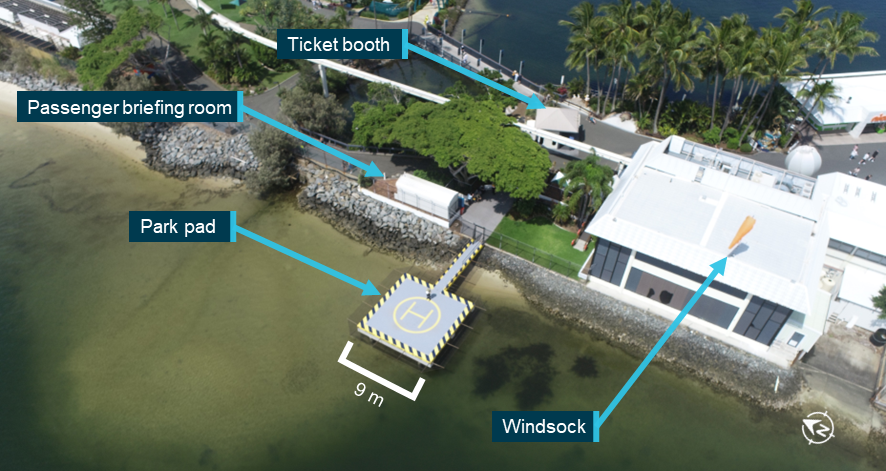
Source: ATSB
Improvements included a new briefing room and windsock, and it reopened on 12 March 2022. It was a 9 m square concrete helipad constructed over water and accessed by a footbridge. The footbridge was 8.7 m from the near edge of the pad to a lockable gate. A 1.2 m high handrail extended on both sides of the footbridge for 4.8 m from the gate. The distance from the end of the railing to the centre of the pad was 8.4 m. Smaller guide rails of approximately 15 cm high continued to the edge of the pad.
The windsock was fitted in an elevated position on the jellyfish house adjacent to the south of the pad. The jellyfish house itself was a bulky 2-storey building. The building was reported to generate mechanical turbulence for departures from the pad when the prevailing south easterly wind was blowing. As a guide on wake decay from bluff bodies, the ICAO Heliport Manual(2021) stated:
it should be assumed that the wake effects will not fully decay for a downwind distance of some ten to twenty structure widths.
The HLS had a touchdown/lift-off area (TLOF) suitable for an AS350 (D-12.94m) and an EC130 (D-12.64m). AS350s could park nose to the gate, and EC130s with a larger door, would park nose to the corner. The final approach take-off area (FATO) was over water and ostensibly clear of obstacles though transiting water vessels could (and would) infringe. Though the guidelines recommended an obstacle free area of 2 rotor diameters (D), the pad achieved an obstacle free area of 1.3 D for an AS350 with the railing in the gangway to the east being the closest hazard.
In interviews pilots stated that they would always land facing the gate of the park pad to ensure passengers remained in front of the helicopter and away from the tail, which is a customary practice in helicopter operations. Also, the operator found that the width of the EC130 meant that the helicopter had to face into a corner of the park pad to give passengers room on the helipad to walk around the open door.
The ticket booth had scales built into the floor weighing passengers and creating flight manifests at the time of booking. There was a briefing room between the ticket sales booth and the helipad where passengers viewed the operator’s safety briefing video. Following the video briefing passengers were fitted with lifejackets by ground crew and escorted by the operator’s ground crew through a gate to the helipad.
Traffic from this helipad represented approximately 28% of the operator's flights for 2022 for 8 months of operation.
Sea World grass
As well as Sea World Helicopters, there was another helicopter tour operator based around 990 m to the south in Marina Mirage. Traffic from both operators would cross the coast over the area called the Sea World grass (Figure 63). Pilots from both operators would listen out for each other’s taxi calls and scan for conflicting traffic on departure when approaching the Sea World grass location.
Figure 63: Sea World grass

Source: Google Earth, annotated by the ATSB
Airspace information
Southport CTAF area
The scenic flight operation was largely conducted in Class G airspace (Figure 64). Class G airspace is uncontrolled, meaning that both aircraft operating under instrument flight rules (IFR) or visual flight rules (VFR) are permitted and do not require clearance from air traffic control. Aircraft movements in Class G airspace are supported by communications on an area frequency or a CTAF appropriate to that area. Communication on that frequency was to be performed by appropriately licenced pilots to the standards set out in the Aeronautical Information Package[51] (AIP).
There was one mandatory requirement for broadcasts on a CTAF. Section 21.04 of the Part 91 MOS stated:
The pilot in command of an aircraft must ensure that broadcasts on the CTAF are made for a non-controlled aerodrome …. When the pilot in command considers it reasonably necessary to broadcast to avoid the risk of a collision with another aircraft.
Other recommended calls for the purpose of building traffic awareness among pilots using the airspace were detailed in AC 91-10 Operations in the vicinity of non-controlled aerodromes. These included the taxi, departure and inbound calls, which were required by procedures at Sea World Helicopters.
The Southport Airfield CTAF was 119.00 MHz. Southport was a private airfield around 3.6 NM north-west of the Sea World heliport. From 2 June 2011 the visual terminal chart listed the same frequency (ERSA listed from 15 November 2012) for operations at Heck Field, an aerodrome used for light aircraft and flight training around 12.5 NM north-north-west of the Sea World Heliport.
The area was not a mandatory broadcast area[52] and the CTAF did not have a defined boundary. The limits of the uncontrolled airspace were bounded by controlled airspace to the south, restricted areas to the west and the recommended positional broadcast at 10 NM from an aerodrome when conducting flight in that vicinity.
Rules of the air and operations at non-controlled aerodromes
The rules of the air govern right of way for aircraft. Regulation 91.325 of the CASR Basic Rule states:
A flight crew member must, during a flight, maintain vigilance, so far as weather conditions permit, to see and avoid other aircraft.
Once an aircraft has been detected, part 91.330 of the CASR Right of way Rules states amongst other things that if there is a risk of collision between 2 aircraft an aircraft must give way to another that is landing and give way to traffic on their right when converging at a similar altitude. These rules are clearly explained at the pilot safety hub on the CASA website.
Operations at uncontrolled aerodromes are described in CASA’s Visual flight rules guide (2024b) and in Airservices Australia’s Aeronautical Information Publication (AIP) En Route (ENR) 10.15 Helicopter operations - At aerodromes and helicopter access corridors and lanes. Helicopters do not have to conform with standard aeroplane circuit patterns, but only when landing outside of the runway in use and when the circuit flown does not cross the extended centre line of a runway in use.
CTAF congestion
The ATSB interviewed 7 helicopter pilots from Sea World Helicopters and another local helicopter operator who was current in operations in the local area, using the Southport CTAF. Each raised issues with congestion on the CTAF on account of it covering a large area of high-volume traffic. The CTAF covers the area shown in Figure 64. It includes Heck Field, the area below Southport Airfield to the controlled airspace boundary 2 NM north of Burleigh Heads.
The Southport Airfield CTAF was not congested at the time of the accident. Sport aviation activity at Heck Field had decreased around lunchtime, Southport Airfield was quiet, and 4 scenic flight helicopters (including XH9 and XKQ) were in the Southport airspace. Therefore, CTAF congestion was not relevant to this accident.
Figure 64: Local airspace
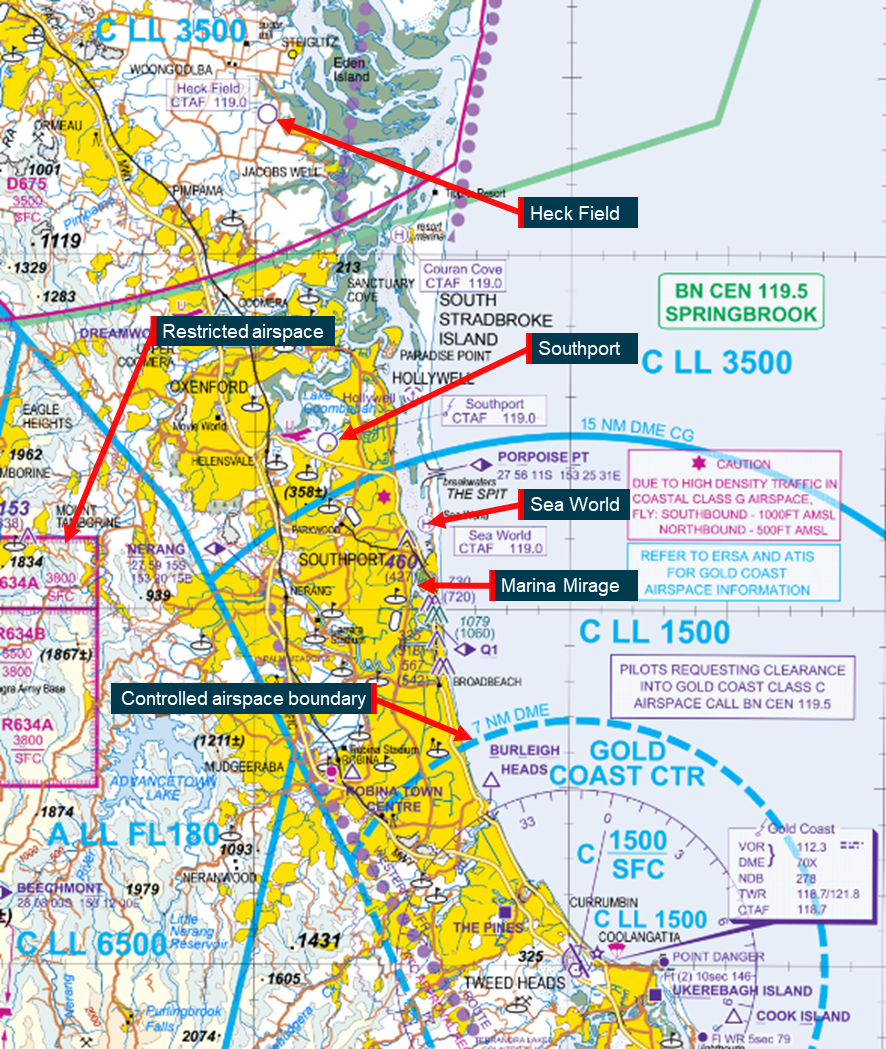
Source: © Airservices Australia 2024, annotated by the ATSB
Airservices Australia review
Airservices Australia (Airservices) analysed helicopter trajectory data from 2022. The report considered every occasion a pair of helicopters was airborne simultaneously and calculated how close they came together in 3-dimensional space using a MITRE score. A MITRE score considers the closest point of approach of a pair of aircraft using functions of time, and lateral and vertical separation. The score is used to assess risk of aircraft encounters in a volume of airspace (Kallinen et al., 2023). It was noted that the MITRE score is not a formal probability of collision but can be used to estimate a proxy risk metric.
Machine learning was used to detect patterns and create clusters. The clusters produced matched the scenic flight routes promoted by local helicopter tour operators. Combined with the MITRE scores of helicopter pairs, the clusters showed which routes had the greatest systemic risk of any pair of helicopters colliding.
The risk metric can be interpreted as the expected number of at-risk (of collision) events in 2022, and hence could be larger than one. Of 916 5-minute flights (tour 1 or tour 6)6 identified, 19 aircraft pairs were identified as being a potential conflict pair. The analysis found the highest risk cluster was associated with Sea World 5-minute flights arriving and departing from the helipads within 700 ft of each other. Across all clusters created by local helicopter tour operators, the highest risk collision pairs were detected at the Sea World helipads and over Sea World grass (Figure 65).
Figure 65: Airservices Australia results on 2022 flight data
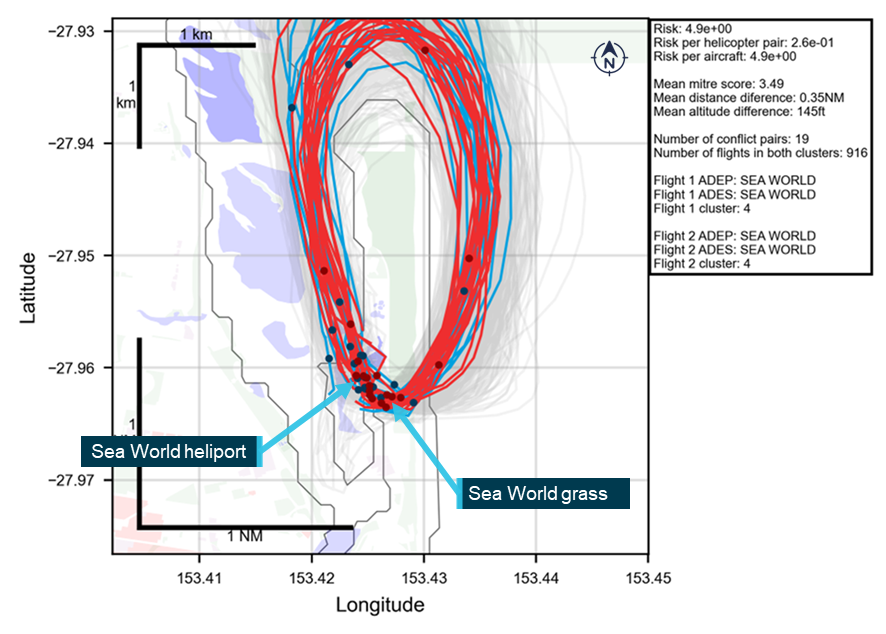
Each simultaneous pair has one red track and one blue track. The remainder of the tracks are grey. Blue dots on plot represent the location of blue trajectories at their closest point to a midair red trajectory; red dots on plot represent the location of red trajectories at their closest point to a midair blue trajectory. Source: Airservices Australia
For comparison, ratings of interactions with helicopter flights in and out of Sea World, and with another local tour operator, are tabled alongside local flights at Archerfield, Queensland in Table 8 below. Archerfield is included as an example of a controlled aerodrome with mixed use helicopter operations.
Table 8: Comparison of risk metric for Sea World and Archerfield
| Rank | Routes | Simultaneous pairs | Total flights | Risk metric | Risk per helicopter pair | Risk per aircraft |
| 1 | SWH Tour 1 flights | 19 | 916 | 4.90E+00 | 2.60E-01 | 5.40E-03 |
| 2 | SWH Tour 1 and Tour 2 flights | 19 | 1,294 | 3.00E+00 | 1.60E-01 | 2.30E-03 |
| 3 | SWH Tour 1 and other local operator Tour 2 | 43 | 1190 | 2.40E+00 | 5.60E-02 | 2.00E-03 |
| 25 | Archerfield local flights | 3 | 138 | 6.90E-04 | 2.30E-04 | 5.00E-06 |
Note: Routes are ranked from highest risk of an aircraft encounter (1) to lowest. Source: Airservices Australia data adapted for presentation by the ATSB
Airservices Australia repeated the analysis with flight data recovered from all Sea World Helicopters’ helicopters for the 90 days prior to and including the day of the accident (Figure 66). The analysis was broken down into 3 pair classifications:
- proximal: within 5 NM (30,380 ft) horizontal and 1,000 ft vertical
- close: within 1 NM (6,076 ft) horizontal and 1,000 ft vertical
- very close: within 200 ft horizontal and 200 ft vertical
Of interest, the very close pairs indicated aircraft separation which was within 61 m (200 ft) lateral and 200 ft (61 m) vertical.
Airservices noted limitations to the analysis including:
- The method to determine when one flight had ended, and another started. Noting if there was a 40 second time gap between trajectory data or if a helicopter remained in the same location for more than 5 seconds, it was assumed a flight had ended and another started.
- Flights with duration shorter than 3 minutes were not included.
- Flights in VH-XKK were excluded due to poor trajectory data.
- Altitude data was variable among helicopters with some arriving 150 ft above surface or at a negative altitude.
Despite the limitations, Airservices Australia stated that the close pairings were highly likely to be correct.
Airservices determined that there were 6 very close pairs, 1 being the accident flight. All 6 occurrences involved helicopters during the take-off and landing phases in close vicinity to the Sea World pads. Table 9 outlines each of the 6 very close pairs and the type of helicopters involved.
Table 9: Proximity events by helicopter pairing
| Pair helicopter type | Count of very close pairs |
| EC130 and EC130 | 3 |
| AS350 and EC130 | 2 |
| AS350 and AS350 | 1 |
The analysis noted that 5 of the 6 events had occurred after the introduction of the EC130 in the 2 weeks leading up to the accident. At the same time, flights conducted by Sea World Helicopters had increased 2-fold with the commencement of peak tourism season.
Figure 66: Flight proximity results of Sea World Helicopter aircraft for the 90 days prior to and including the day of the accident
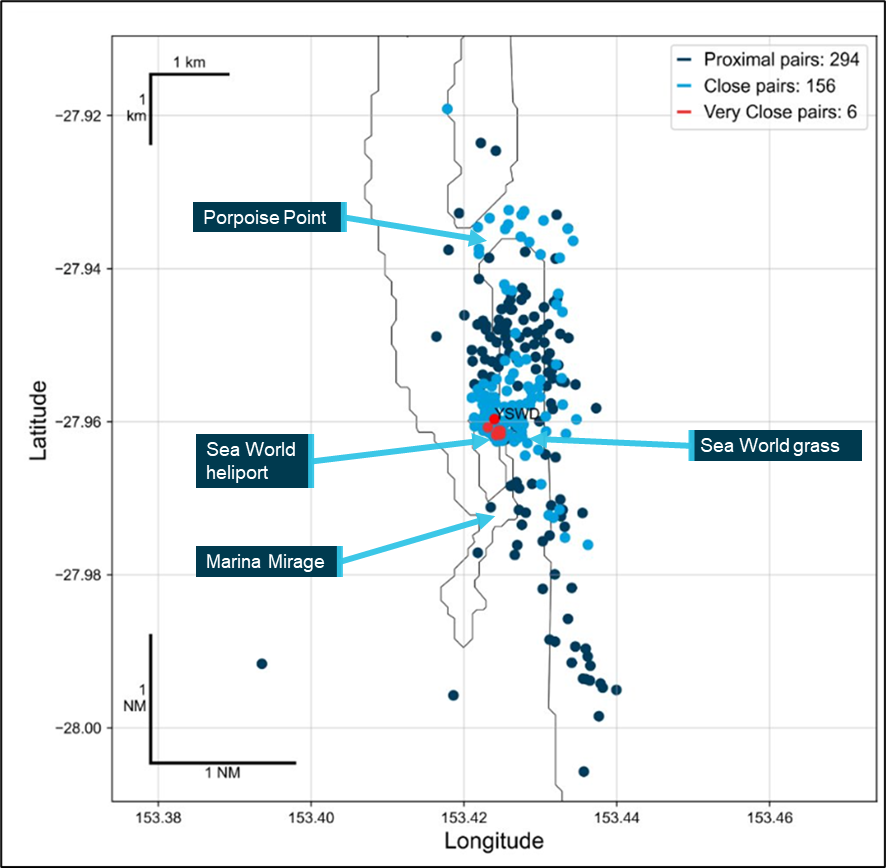
Note: Each dot represents the mid-point between the 2 helicopters at their closest point when they register as either proximal, close or very close in distance. Helicopters do not overfly the theme park. Source: Airservices Australia
Operational procedures and information
Training and checking
Sea World Helicopters’ manual SWH-TAC-MAN-23 Training and Checking described the operator’s training and checking system. Training and checking at Sea World Helicopters was conducted by the CEO and the HOFO (pilot of XKQ), and both were experienced instructors.
Pilots reported that the HOFO had a strong emphasis on communication and was insistent on correct radio procedure during training and checking activities. Additionally, the HOFO had a VHF radio in their office and would monitor the CTAF while they were at their desk. For outbound traffic, the calls were a taxi call prior to take-off and a departure call once airborne (see See-and-avoid below). All company pilots stated that a taxi call from an outbound helicopter was a signal to anyone inbound to arrange separation if required.
All pilots advised that the CTAF was very busy, stating that at times it was difficult to make radio calls at the required times due to congestion. One pilot stated that they were discouraged from engaging in ‘chatter’ on the CTAF to reduce the volume of calls on it. Training files and one pilot interview also stated that ground crew and pilots were also instructed to reduce chatter on UHF (if fitted to the helicopter) to reduce noise in the helicopters and avoid unnecessary communication where customers could hear it.
The CEO stated that pilots (on southerly departures) were taught to look and clear their airspace to the right on departure from the park pad. They were taught that due to the high frequency of short duration flights, that pilots should assume there would be conflicting helicopter traffic and always expect another helicopter to be there. Interviews with 4 current company pilots including the CEO showed that there was a general expectation that conflicting company traffic would be visible either ahead or to the right when departing the park pad. Additional requirements were stated to be avoid overflying boats, look out for yacht masts, birds and parasailers, and aim for the sandbar.
Following review of the draft report the CEO stated that they expected pilots to pause for 1 to 2 seconds at the top of the vertical climb from the helipad to conduct a scan before transitioning into forward flight. Review of the operator’s tour videos showed that it was normal for pilots, and specifically the pilot of XKQ, to transition to forward flight in one smooth motion without a pause.
Procedures for inbound pilots were to make an inbound call at Porpoise Point. The CEO stated that from that point no more calls would be made unless another helicopter was there. The documented procedures only required standard CTAF calls, and the pilots reported varied understanding of this rule (see Additional inbound calls below).
On the day of the accident, the pilot of XH9 did not make any additional calls as they expected any potential conflict would be signalled by a taxi call from the pilot of XKQ. Other company pilots including the CEO of the operator agreed that this was appropriate behaviour at this stage of flight. At that time, the CEO stated that at that late stage of the approach, the pilot of XH9 was not expected to make an additional call or direct attention to the park pad without a warning to do so.
Following review of the draft investigation report the CEO stated that they had changed their opinion after reading the police statement made by the pilot of XH9, within which the pilot stated they saw the doors of XKQ close. The CEO stated that the pilot should have kept their eyes on XKQ and made another radio call.
All pilots were instructed to avoid overflying vessels on the waterway and to keep within gliding distance of the sandbars in the Broadwater for use as predetermined forced landing areas,[53] especially on take-off and landing.
EC130 familiarisation
The HOFO trained 2 full time pilots in EC130 operations (Table 10). Practice flights started in XKK in November 2022. Both pilots received the same type of training which included approaches and departures to the heliport and park pad, following some of the common tour routes, and offsite training near the Pimpama River conservation area (Figure 67). The paths flown in training matched the paths flown in normal operations.
Table 10: EC130 training conducted by HOFO for line pilots
|
Helicopter |
Location |
Pilot 1 |
Pilot 2 |
||||
|
Take-off |
Landing |
Time (h) |
Take-off |
Landing |
Time (h) |
||
| VH-XKK | Heliport | 4 | 4 | 2.3 | 7 | 7 | 3.2 |
| Park pad | 0 | 0 | 0 | 0 | |||
| Pimpama | 4 | 4 | 3 | 3 | |||
| VH-XKQ | Heliport | 1 | 1 | 0.7 | 2 | 2 | 1.5 |
| Park pad | 2 | 2 | 0 | 1 | |||
| Pimpama | 0 | 0 | 1 | 1 | |||
Note: Pilot 1 was the pilot of XH9 and pilot 2 was another company pilot.
Figure 67: EC130 training flights

Source: Google Earth, annotated by the ATSB
Ground crew passenger loading and pre-departure procedures
Seating positions
Passengers were seated by the ground crew, and the ground crew had carriage of all aspects of passenger loading including helicopter weight and balance. The operator’s booking system created a manifest which provided ground crew with a schedule of flights that included the passengers’ names, measured weights, tour type and anticipated time of flight. The ground crew used that information to seat passengers in accordance with the operator’s documented helicopter loading chart. The chart provided options for the pilot’s weight and fuel load and gave a range of corresponding weight limits for the front and rear seats of the helicopter.
Remaining within the limits of the chart would keep the helicopter within its centre of gravity limitations. Any loading configurations outside of the limits of the chart required consultation with the pilot who would conduct a calculation to check that the proposed configuration was acceptable.
Weight and balance
For the loading of XKQ, the combined weight of the front seat passengers exceeded the usual limit as indicated by the operator’s loading chart. The ground crew member responsible for checking this spoke with the pilot who then manually calculated and confirmed that the passengers could be seated in the front (Figure 68).
Figure 68: XH9 and XKQ calculated longitudinal centre of gravity for accident flight
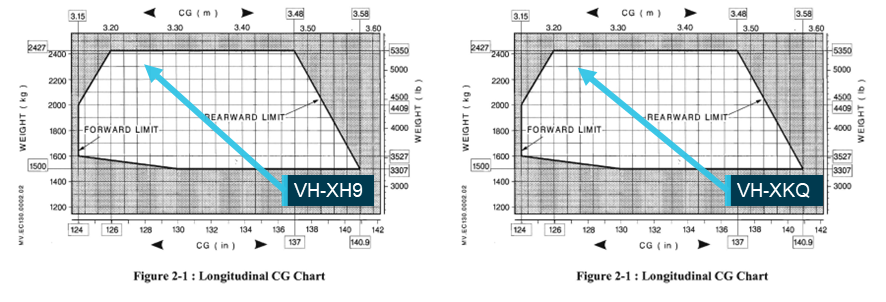
Source: Airbus Helicopters, annotated by the ATSB
Preparation for departure
Sea World Helicopters’ procedures in the Base Operating Procedures manual (SWH-BOP-SOP-75) outlining ground crew responsibilities in readying a flight for departure, stated (amongst other things):
12 Loading Procedures
12.1.11 Once all passengers are loaded and their seat belts secured, loaders should ensure that nothing is hanging outside the doors and that the doors are secured correctly before walking away from the helicopter.
12.1.12 The last loader should then visually check the doors are secured, check the area is clear behind the helicopter and on the adjoining helipads, and then give the pilot the thumbs up and signal for the flight, Tour 1, 2, 3 etc.
12.1.13 The loader should then exit the helipad.
12.1.14 Only loader should give the thumbs up to the pilot. This signal means, the doors are closed, no seat belts are hanging out and you are clear to depart. It is a very important signal and must not be given unless you are sure these things are correct.
Ground crew learned these procedures from each other. New crew members were teamed up with existing crew and shown the operation in on-the-job training. Interviews with ground crew and pilots revealed that practice met the procedure. Company pilots recalled that ground crew cleared the airspace then gave a thumbs up. Ground crew reported looking for obstacles on the water and in the air and drawing the pilot’s attention to any relevant obstacles before giving the thumbs up. They would then leave the helipad to attend to the next set of customers.
At the park pad, once the ground crew had exited the helipad, the briefing room would block their view of the airspace to the north.
One ground crew member reported following a different procedure, stating that they would watch the helicopter take off before attending to new customers. A review of tour videos from the park pad and the heliport showed that the crew would leave the pad between 20 s and 1 minute 30 s prior to departure. In interview one ground crew member stated that a 30 s gap was normal.
In interview with the ground crew of the accident flight they stated that that they had followed the departure procedure and had not heard or seen other aircraft or obstructions before giving the signal to the pilot of XKQ that indicated the helicopter was clear to depart.
Flight procedures
The operator did not have specific procedures for conduct of scenic flight operations at Sea World. However, some procedures for air transport flights applicable to the scenic flight operation were distributed throughout the operator’s exposition. Some elements more relevant to the scenic flight operation, such as approaches to overwater helipads, and routes in and out of the main heliport were also included. The below procedures were noted as relevant but not specific to the scenic flights at Sea World, and both pilots had signed and acknowledged the manuals.
Lighting use on the operator’s helicopters was stipulated in the Operator’s Flight Crew Operations Manual at 3.1.2
3.1.2 Unless stated otherwise in the FLM [the manufacturer’s Flight Manual] or specific circumstances are present, the following procedures shall be applied:
…
b) Anti-collision beacons shall be left ON at all times, even after shut down to warn of accidental battery activation;
c) Strobe lights and Nav lights are to be activated before start and deactivated after shut down;
d) Landing lights shall be ON prior to departure and OFF once aircraft has landed;
...
Lighting and lookout was in the Operator’s Aircraft Operations Manual at 7.15:
7.15 Maintenance of Look-out and use of external lights –
7.15.1 PIC’s [pilots in command] are to maintain a constant look-out at all times. Before departure, PIC’s will ensure strobes and landing lights are switched on.
Collision avoidance procedures were also carried in the Operator’s Aircraft Operations Manual at 7.6:
7.6 Collision Avoidance
7.6.1 The responsibility for collision avoidance, sequencing, and knowledge of local procedures lies solely with the PIC.
Later in the Aircraft Operations Manual traffic collision avoidance devices (TCAD) were discussed:
7.10 TCAD
7.10.1 Pilots are to use the TCAD equipment where supplied for collision avoidance in all phases of flight. Pre landing checks should include reference to the TCAD to ensure path clearance.
Radio procedures were discussed in the Flight Crew Operations Manual at 2.3.5:
2.3.5 The pilot in command shall ensure that a listening watch is maintained at all times from immediately prior to the time at which the helicopter commences to move for a flight until the helicopter stops on the apron after a flight, or in the case of communicating with an ATC [air traffic control] unit, the pilot shall personally maintain a listening watch at all times the helicopter is under control of that ATC unit. Pilots shall use the radio telephony procedures and phases detailed in the AIP.
Radio procedures were also detailed in the Aircraft Operations Manual at 9.2 and 9.3:
9.2 Position Reporting
9.2.1 The PIC should make a Position Report including location-altitude and intentions, at each turning point, reporting point of when in the vicinity of a high traffic area. This call should be made on the relevant area frequency.
The call at Porpoise Point was a call of this type, made in that location because Porpoise Point was a designated VFR reporting point.
Communications at Non-controlled Aerodromes[54]
9.2.2 When at or near a non-towered aerodrome the PIC shall check that the radio is on the correct frequency and listens to broadcasts. Under CAR166C, a radio broadcast is required whenever it is reasonably necessary to avoid a collision or the risk of a collision.
a) For minimum compliance, the PIC should broadcast their intentions:
• Before or during taxiing;
• Immediately before entering a runway, whether active or not;
• Inbound 10nm or earlier from the aerodrome immediately before joining the circuit;
• On a straight-in approach, on final, by 3nm from the threshold;
• On a base-join approach, before joining on base when flying near, but not intending to land at, a non-towered aerodrome, where the PIC intends to fly through the vicinity but not land;
b) When making radio calls state the name of the aerodrome, your aircraft’s type, call sign and position, and your intention;
• Repeat the name of the aerodrome;
• Use standard phraseology and don’t chat;
c) When flying VFR, identify yourself if you hear an IFR PIC intending to make an instrument approach;
d) As needed, make other broadcasts such as:
• Turning downwind base and final;
• Clear of runway.
Approach and landing procedures for the park pad were documented in the Aircraft Operations Manual at 13.2:
13.2.2 Approach to Overwater Helipads
As the park helipads at SWH are a raised platform over salt water, it is imperative that approaches are conducted in a manner to allow as safe autorotation onto the sandbar, shallow water or during final stages of approach onto the helipad.
a) Plan for a slightly steeper than normal approach, into wind if possible.
b) “Arm” floats at 500 feet. See Flight Manual for float activation procedures.
c) Terminate the approach at approx 10 feet over the helipad, allow the aircraft to sink while monitoring the ROD [rate of descent]. Cushion the touchdown and minimise hovering time.
d) A well performed approach should result in minimal salt spray on the windscreen.
13.2.3 Steep or Vertical Approach
a) Steep or Vertical approaches should only be used when absolutely necessary, extreme care must be taken to avoid Vortex Ring State.[55]
There was no radio or separation procedure specific to the scenic flight operations. Videos of previous flights and interviews with pilots showed that a taxi call prior to lifting off, a departure call over Sea World grass, and an inbound call at Porpoise Point were standard calls for the operator’s scenic flights. Longer flights made additional calls at appropriate reporting points.
Calls on short final[56] or passing behind other helicopters were not standard or mandated by the written procedures. The operator’s pilots reported using calls passing behind another helicopter on an as-required basis, based on the passing pilot’s assessment of the requirement.
With respect to ensuring calls could be made and heard, the operator’s Aircraft Operations Manual carried instruction on a pre-flight radio check.
9.3 Pre-flight Radio Check
9.3.1 Refer to FLM.
The helicopter manufacturer’s Aircraft Flight Manual for the EC130 B4 made no reference to a pre-flight radio check. Operator pilots reported that on their first flight of the day they would check that other stations were receiving their transmissions by calling other aircraft or ground crew with access to an office‑based VHF radio.
The operator published approach and departure tracks for Sea World Heliport in an annex to their Aircraft Operations Manual (Figure 69). Paths for approach and departure from the park pad were not included.
Figure 69: Operator’s declared Sea World Heliport approach and depart paths
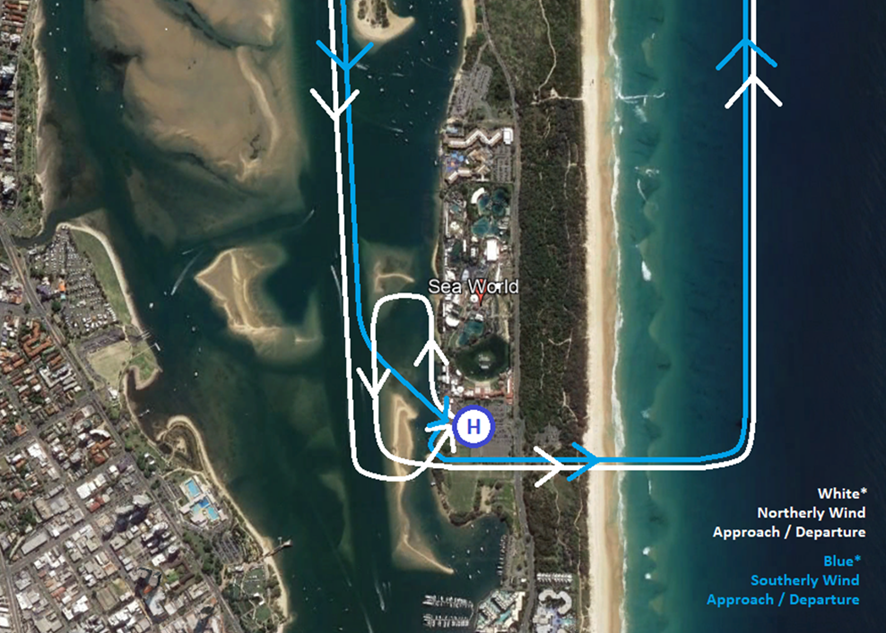
Source: Operator
See-and-avoid
Helicopters used for scenic flights generally have excellent visibility from the cabin. Pilots reported that the area was very busy, and they would commonly visually acquire aircraft either aided by radio calls or lookout alone. This activity was observable in tour videos supplied by the operator.
Unalerted see-and-avoid describes the concept of pilots of aircraft avoiding collisions by seeing another aircraft and avoiding it. While it sounds simple there are several complexities. It requires effective scanning, knowledge of the limitations of vision, and depends upon weather and conspicuity of targets against the background (CAA, 2011) (see also Flight path and cockpit visibility reconstruction (Visibility study). It is a very important strategy for managing the risk of midair collision because not all aircraft in uncontrolled airspace are required to carry radios (CASA, 2021), and those that do may experience issues with them.
There is extensive literature (also available via an internet search) for the limitations of see‑and‑avoid stretching back over 30 years and the importance of an ‘alert’ component to make it more effective.
An ATSB research report (Hobbs, 1991) stated that (unalerted) see-and-avoid is:
Last resort separation if other methods fail to prevent a confliction, regardless of the nature of the airspace.
The research report further detailed the issues associated with unalerted see-and-avoid, stating:
See-and-avoid can be considered to involve a number of steps. First, and most obviously, the pilot must look outside the aircraft.
Second, the pilot must search the available visual field and detect objects of interest, most likely in peripheral vision.
Next, the object must be looked at directly to be identified as an aircraft. If the aircraft is identified as a collision threat, the pilot must decide what evasive action to take. Finally, the pilot must make the necessary control movements and allow the aircraft to respond.
Not only does the whole process take valuable time, but human factors at various stages in the process can reduce the chance that a threat aircraft will be seen and successfully evaded. These human factors are not ‘errors’ nor are they signs of ‘poor airmanship’. They are limitations of the human visual and information processing system which are present to various degrees in all pilots.
Alerted see-and-avoid supplements the process by directing pilots to the location of other aircraft to concentrate a visual search and aid in detection of the other aircraft. It is typically achieved through radio communications or aircraft-based alerting systems. It requires no familiarity with location or other aircraft and is successfully employed for traffic to self-separate.
Citing Andrews, Hobbs (1991) found that an alerted search is likely to be 8 times more effective than an unalerted search, as knowing where to look greatly increases the chances of sighting traffic. Similarly, an FAA research report (Andrews, 1977) suggested that unalerted pilots may take 9 times longer to react than alerted pilots:
A traffic search in the absence of traffic information is less likely to be successful than a search where traffic information has been provided because knowing where to look greatly increases the chance of sighting the traffic (Edwards and Harris 1972). Field trials conducted by John Andrews found that in the absence of a traffic alert, the probability of a pilot sighting a threat aircraft is generally low until a short time before impact. Traffic alerts were found to increase search effectiveness by a factor of eight. A traffic alert from ATS or from a radio listening watch is likely to be similarly effective (Andrews 1977, Andrews 1984, Andrews 1987).
Alerts can be provided in a range of ways. Most commonly in the form radio calls from other aircraft sharing the airspace. CASA in advisory circular 91-14 (2021) lists a series of additional alert tools:
4.1.4 Other tools of alerted see-and-avoid include:
− Airborne Collision Avoidance System (ACAS)
Note: ACAS relies on transponder information from other aircraft for its pilot alerting and collision avoidance function. TCAS is one type of airborne collision avoidance system.
− Automatic Dependent Surveillance - Broadcast (ADS-B)
− Electronic Conspicuity devices
− FLARM— a traffic awareness and collision avoidance system developed by FLARM Technology Ltd and originally designed for gliders
− Electronic flight bag (EFB) applications that receive traffic information through the mobile phone network or an ADS-B or ADS-C receiver
− Ground-based ATS [air traffic service] surveillance system (with traffic information being relayed back to pilots via radio).
While alerted see-and-avoid is a great improvement on see-and-avoid, it is still known to be fallible, as described by an ATSB (2010) research report AR-2008-044 Safety in the vicinity of non-towered aerodromes. It evaluated separation occurrences and found:
See-and-avoid conflicts where situational awareness errors were involved (also contributed to by inadequate or no communications in some cases) made up about one-seventh of all occurrences [meaning incidents, serious incidents and accidents]. These types of conflicts led to almost all of the six accidents recorded in the vicinity of non-towered aerodromes between 2003 and 2008, four of which were mid-air collisions, and two of which were runway incursions leading to a collision on the ground…
Taxi call
The Sea World Helicopters Aircraft Operations Manual stated:
For minimum compliance, the PIC should broadcast their intentions… Before or during taxiing.
The procedure was not specific to the helipads, and at the helipads the pilots were not required to taxi to reach their lift-off area. However, they still needed to advise aircraft in the area of their intentions. A pilot advised that at the heliport or in the original configuration of helipads, if a pilot made a taxi call after lifting, an inbound helicopter could disrupt control of the helicopter with downwash. Therefore, taxi calls were ordinarily made before lifting. Video footage from previous flights showed that pilots consistently made a taxi call shortly before departure. The taxi call was:
Traffic Southport, helicopter [registration] taxiing Sea World. For departure to the [heading]. Southport.
Procedures did not require pilots to respond to a taxi call made by departing pilots, and pilots would not expect a response unless there was potentially conflicting traffic. The operator’s stated expectations were for inbound company pilots to coordinate with a departing pilot following the receipt of a taxi call. Pilots would arrange for the inbound pilot to slow their approach or for the departing pilot to delay their departure.
The pilot of XH9 did not hear the pilot of XKQ make a taxi call prior to departing, and 2 other pilots from another company for whom the call would have been relevant did not recall hearing a taxi call on the CTAF either.
A passenger on XKQ who could hear the intercom recalled the pilot of XKQ advising the passengers to ‘talk amongst yourselves’ and did not hear anything else from the pilot. The pilot’s instruction for the passengers to talk among themselves is indicative of the pilot intending to temporarily cease communication with the passengers. Commonly this would be for sterile cockpit conditions or for external communication.
Passengers could be isolated with a switch on the audio panel or a collective mounted button. The audio panel switch position noted on wreckage inspection could not be used to determine switch position on departure, and the cyclic button leaves no record of activation. If the pilot had isolated the passengers on departure, they would not hear the pilot make a radio call or hear any external radio communication.
Due to shielding from buildings on the opposite foreshore, broadcasts made below 200 ft were not expected to be recorded on the Southport Airfield CTAF. No taxi calls from any Sea World Helicopters pilots were captured on the CTAF recording.
Video footage recorded by a passenger on board XKQ showed the pilot from the rear right side immediately prior to take-off. The timing coincided with the timing of taxi calls from 2 other videos of the pilot performing scenic flights. The pilot was not engaging with passengers and the pilot’s cheek and jaw showed movement consistent with talking. However, helicopter noise drowned out the audio track and their mouth was not visible, meaning any speech from the pilot could not be isolated or discerned.
Departure call
The departure call was not specifically detailed in the operator’s Aircraft Operations Manual though all current pilots reported that it was a standard call that they all made, and the CTAF recording supported that. The call was made around 1 minute after take‑off and the CTAF recording showed that the structure of the call was:
Southport traffic, helicopter [registration] we’re airborne crossing the coast at Sea World grass, north bound over water not above 1,000, Southport traffic.
Inbound call
The Sea World Helicopters Aircraft Operations Manual required pilots to broadcast their intentions:
…on a straight-in approach, on final, by 3nm of the threshold
and to:
make a Position Report including location-altitude and intentions, at each turning point, reporting point of [or] when in the vicinity of a high traffic area.
There was a VFR reporting point[57] called Porpoise Point about 1.5 NM north of Sea World helipads. Videos from previous flights showed that pilots routinely made an inbound call for a landing at the helipads when approaching that location, which was around 2 minutes before arriving in the vicinity of the helipads. Procedures did not require other pilots to respond to an inbound call made by inbound pilots, and inbound pilots would not expect a response unless there was potentially conflicting traffic.
Calls followed the standard format of position, height, intention, and were typically:
Southport traffic, helicopter [registration], Porpoise Point, inbound for Sea World via the Broadwater with a left turn, Southport traffic.
The pilot of VH-XH9 was recorded making an inbound call, near Porpoise Point, and the call was clear and accurate.
Flight preparation procedures
The Sea World Helicopters Aircraft Operations Manual described the pre-flight actions required by company pilots. These included that the pilot must ensure that the aircraft was correctly loaded and:
shall ensure that all occupants have their seatbelts or harnesses fitted and correctly adjusted during all stages of flight.
There were no procedures supporting the use of a sterile cockpit in the scenic flight operation. A sterile cockpit environment is one whereby pilots restrict activities to only those required for the safe operation of the aircraft. While this could include directing and assisting passengers to fit seatbelts and headsets, the business owner stated that they wanted the scenic flights to be a premium experience for customers and expected company pilots to act as the host while on board the helicopter. There were no procedures which described the role of company pilots to greet and facilitate the guest experience of passengers, though the owner stated that it should not be at the expense of pilot duties.
The ATSB conducted 12 interviews with 8 pilots. All were current or prior pilots of Sea World Helicopters with experience of operations there. All the pilots stated that part of their job was to provide commentary and talk with passengers. They were all consistent in their appraisal of passengers creating a noisy environment, to the extent of creating a difficult workplace for a pilot at times.
For example, 2 pilots reported passengers attempting to talk over radio calls as the pilots were making them and 2 pilots reported that it was not uncommon to occasionally miss radio calls due to noise from passengers. While the tolerance for noise differed among the pilots, they all stated that the best way to mitigate the problem was to isolate passengers from the intercom, and all stated that they would.
All pilots stated they would interact with passengers while they were being loaded into the helicopters and awaiting departure, and footage from prior flights which started after passengers were seated showed that interaction with passengers to settle them in was normal. There was however, a spectrum of involvement, with one pilot stating they would have minimal interaction with passengers to attend to radio calls, and one pilot stating that they would concentrate on passenger unloading and loading then establish situation awareness before departing. Another pilot was very clear to point out that missing a call due to passenger activity would not be followed by a departure without further communication with other helicopters.
At the time the pilot of XH9 made their inbound call, passengers were boarding XKQ and took photographs and video capturing aspects of the passenger‑loading process. The pilot of XKQ was wearing a headset which allowed them to hear radio calls and converse with passengers. As expected by the operator and as shown in previous flights, the pilot of XKQ was seen to interact with passengers during the loading process.
The Sea World Helicopters Aircraft Operations Manual stated that company pilots were required to make radio broadcasts announcing their position and intentions ‘whenever it is reasonably necessary to avoid a collision or a risk of collision.’ The CEO described an understanding that pilots would negotiate separation with each other using radio communication as required.
There was inconsistency among the operator’s pilots with respect to the use of additional inbound calls. Of the 8 pilots interviewed, 3 pilots had worked for the previous owner and described a constant proactive communication over UHF between inbound and outbound pilots at that time. All 8 pilots interviewed flew under new ownership. They reported that proactive calls on the CTAF were encouraged and used, when necessary (if an outbound helicopter looked ready to depart).
Five current company pilots reported different practices. Two pilots stated they would wait for a taxi call to initiate contact, and 3 pilots described using an informal procedure whereby if they identified another helicopter preparing to depart, they would make an additional ‘short final’ call when approaching to land whether it was assessed as being required or not.
After passing Porpoise Point and making the inbound call, the pilot of XH9 did not make an additional broadcast. The pilot recalled observing XKQ on the park pad and, having seen the helicopter doors close, expected VH-XKQ would soon depart. The pilot of XH9 reported that they expected to hear a taxi call prior to XKQ taking off.
The pilot of XH9 reported being aware that the ability of a departing pilot to clear their airspace was limited and recalled being alert to a taxi call as a trigger to arrange separation. They stated that if they heard a taxi call from the pilot of XKQ they would have responded to announce their position and arranged separation.
Non-procedural radio calls
The operator’s AS350 helicopters were fitted with UHF radios for company communication. The ground crew and office were also equipped with radios and operated on the same UHF frequency. The EC130 helicopters were not utilising UHF.
While the CEO described an understanding that pilots would negotiate separation, they stated that the previously implemented UHF channel was not used for that purpose. They advised that the UHF was primarily for ground crew communications. While that matched use at the time of the accident, it did not match UHF use under VRTP ownership.
Several pilots recalled that the operating procedures used, while the helicopter operations were part of the VRTP business, included regular use of a private UHF channel for non-procedural radio communication to identify their position and intentions. According to these pilots, it was typical for pilots to use UHF radios for ‘chatter’ with other nearby helicopters, and with ground personnel.
Former pilots recalled that UHF radio was used to coordinate movements of concurrently operating helicopters, by maintaining a high level of awareness of the position and intentions of nearby helicopters. They recalled that this included coordinating the timing of flights with pilots and ground crew and communicating with company pilots regarding their position in the sequence.
In circumstances where a UHF radio was not available, company pilots would revert to using alternative VHF channels (operating ‘on numbers’), and that they would not operate without a ‘chatter’ capability. It was typical for the frequency 123.45MHz to be used for this purpose. Records showed that:
- A job hazard analysis for the commencement of operations from the car park helipad, conducted in August 2019, identified that pilots would ‘maintain comprehensive situational awareness regarding the movements of both company and CTAF traffic employing effective communication via both VHF and UHF radios’. The document also stated that it was not permitted to simultaneously approach and depart from the helipad, and pilots would ‘effectively coordinate their movements via UHF’.
- A job hazard analysis was conducted in October 2018 for the cross-hiring of an AS350 helicopter, which was not equipped to communicate on the company UHF channels. The Job Hazard Analysis stated that pilots were to configure the helicopter secondary radio channel to 123.45MHz ‘for the purpose of communicating with other company aircraft and ground staff.
- A job hazard analysis for an expected high volume of flights over Chinese New Year, conducted in February 2016, identified that all aircraft would monitor 123.45MHz ‘for general chit chat’. This was listed as a control against the risk of midair collision during take-off and landing.
Use of electronic flight bags
The operator stated that the primary use of the electronic flight bag (EFB)/iPads was for display of manifest[58] data from a tour booking system called Rezdy. The pilot of XH9 confirmed this and added that they also used the OzRunways EFB to support their awareness of location of company traffic and other aircraft when preparing for departure in the AS350s. Additionally, it was reported that the iPads were introduced by the previous owner, and before the implementation of the Rezdy system, for the sole purpose of using the OzRunways EFB.
Three pilots who flew for the previous owner, VRTP, reported using the map and traffic display on the OzRunways EFB to support their awareness of location of company traffic and other aircraft when preparing for departure. They stated that the live traffic display was not their primary means of separation but was used to support their awareness of nearby traffic.
Regulatory guidance and research identified that in-cockpit displays of traffic information can support pilots in maintaining situation awareness of nearby aircraft, including by informing a visual scan. As summarised by Howell and King (2019):
… [Display of live traffic information] improves the pilot's ability to visually acquire traffic so that the see-and-avoid principle can be more effectively applied...
The CASA advisory circular AC 91-23[59] makes similar observations on the utility of traffic displays, noting:
When a pilot is using any traffic awareness system, they should utilise the information it provides to aid in sighting other aircraft. Often, knowing where to look, both horizontally (direction) and/or vertically (up, down or at the same level) saves critical minutes compared with relying only on a full-sky scan
AC 91-23 emphasises that pilots should only use such systems to support a visual scan outside the aircraft, and to be mindful of distraction and minimise the amount of time spent ‘heads down’.
The Traffic awareness for general aviation study (DFS Deutsche Flugsicherung, 2003) compared the visual detection of aircraft by general aviation pilots in cruise, with and without the use of a cockpit display of traffic information. This study found that without the use of such displays, pilots detected 68% of traffic passing within 2.5 NM, and detection probability with a display was increased to 80%.
With respect to the non-carriage of EFBs in the accident flights, the CEO stated that ‘At that point they weren't mandatory to have’ and ‘they weren't using it that much anyway’. However, following review of the draft investigation report the operator stated the pilots could have used knee boards or carried the iPads in the seat webbing, and that the choice of helicopter and equipment was the sole responsibility of the pilots.
Minimising downwash and outwash effects
The take-off and approach paths of each helipad were subject to the passage of watercraft of various sizes. Small open top recreational vessels, susceptible to downwash, and sailboats with masts to around 18 m, tall enough to penetrate the obstacle free sectors of the flight paths, were common in the Broadwater and often passed the helipads. Maritime Safety Queensland (2020) published a chart of the Broadwater and south channel which passed to the west of the Sea World Theme Park (Figure 70). The historical hangar pad which closed in 2019 (see Organisational and management information) was marked on the chart with instructions for vessels to remain 30 m clear, and buoys were placed in the water near the park pad to mark a 30 m limit. The main heliport was not marked on the chart.
Figure 70: Boating instructions for navigation around Sea World Helicopters helipads
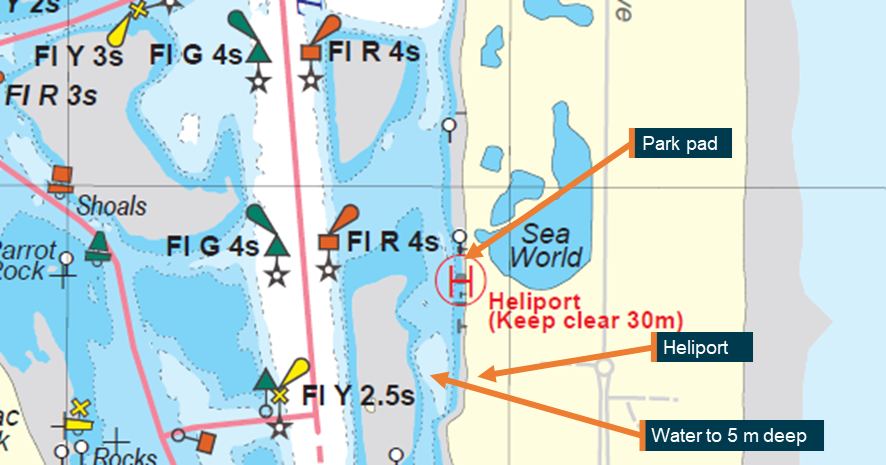
Source: Marine Safety Queensland annotated by the ATSB
The ICAO document 9261, Heliport Manual 5th Edition (2021) defined take-off and approach surfaces.
It stated in Part 2 Onshore heliports chapter 4 obstacle environment:
4.1.1.2 In order to safeguard a helicopter…it is necessary to establish a surface…through which no object is permitted to project….
4.1.1.4 …Mobile objects such as …boats…may be regarded as obstacles at certain times, in which case it would be necessary to delay helicopter operations until the obstacle is clear.
The ICAO guidance described a protected slope of 8% and first stage length of 245 m. A yacht with an 18 m mast could penetrate that slope at 30 m and create a slope of 60%. The departure slope of XKQ on the accident flight was around 10%.
Beneath a helicopter rotor system at a distance in the region of 3 rotor diameters, the downwash velocity is at its maximum, and downstream, more than 10 rotor diameters away, the downwash can be considered dissipated (DSAC, 2022). The rotor diameter of an EC130 is 10.69 m.
Small open top recreational vessels were susceptible to downwash and outwash from approaching and departing helicopters (Figure 71). Overflying vessels on the water risked causing damage or injury on board the vessel and foreign object damage[60] to the helicopter.
The operator’s pilots reported the practice of manoeuvring on approach or waiting on departure to avoid tall vessels and affecting others with downwash. Both helicopters involved in the accident encountered vessels in their vicinity on the accident flight (Figure 72).
Figure 71: Vessels on the departure path of XKQ and approach path of XH9
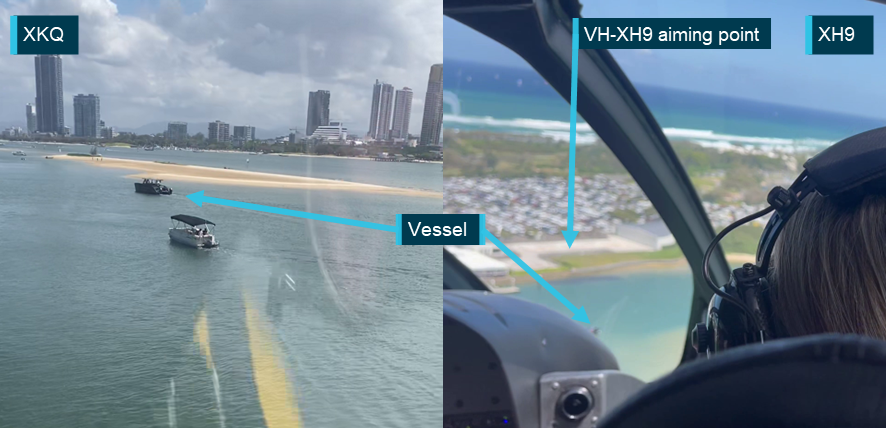
Source: passengers on board VH-XH9, annotated by the ATSB
Figure 72: Reconstruction showing vessels crossing the departure path of XKQ and approach path of XH9
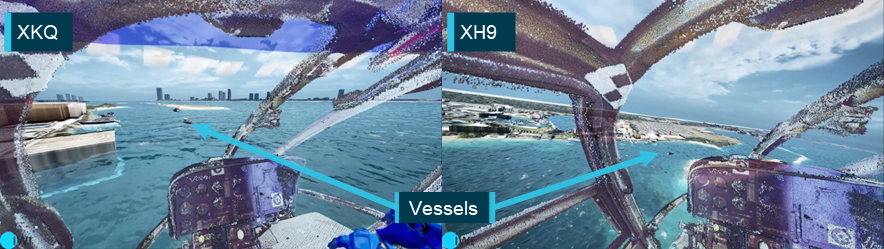
Source: iwiation GmbH and ATSB
Scenic flight operations information
Short duration, high frequency scenic flights are a popular tourism product commonly found in high density tourism locations around the world. The NTSB (1995) has long recognised that risk is elevated at tourism destinations in the United States and found that concentration of aircraft in scenic locations is a unique risk factor for midair collision in tourism flights. The NTSB has also recommended implementation of safety management systems (SMS) in that industry sector since 2016 (NTSB, 2022).
Sea World Helicopters scenic flight operations
The bulk of the operator’s business was high frequency short duration scenic flights. Operator data showed around 7,500 flights in 2022. These flights varied in duration though were concentrated in short duration flights. The volume of flights was seasonal, and the summer months were the busiest. From 1 December 2022 to 2 January 2023, the operator’s records showed 883 scenic flights were conducted, 536 of which were 5‑minute duration flights (Table 11).
Table 11: Flights from 1 December 2022 to 2 January 2023 (33 days)
| Duration | Main heliport flights | Park pad flights | % of total |
| 5 min | 387 | 149 | 60.7% |
| 10 min | 175 | 81 | 29.0% |
| 15 min | 50 | 12 | 7.0% |
| 20 min | 6 | 1 | 0.8% |
| 30 min | 8 | 0 | 0.9% |
| Other | 13 | 1 | 1.6% |
| Total | 639 (72.4%) | 244 (27.6%) | 100% |
Source: Operator
This volume of flights exceeded the number of movements found at some major airports with air traffic control services. In Table 12 below, total movements for airports are counted during tower hours and are the sum of arrivals and circuits multiplied by 2. The total movements for Sea World Heliport and park pad are number of scenic flights multiplied by 2 (one landing or take-off is a movement).
Table 12: Excerpts showing high, medium and low ranks of movements at Australian aerodromes December 2022
| Rank | Aerodrome | Code | Total |
| 1 | SYDNEY/KINGSFORD SMITH | YSSY | 27,312 |
| 2 | MELBOURNE/ MOORABBIN | YMMB | 19,296 |
| 3 | PERTH/JANDAKOT | YPJT | 19,176 |
| 13 | GOLD COAST | YBCG | 6,540 |
| 17 | SUNSHINE COAST | YBSU | 3,572 |
| 28 | SEA WORLD | YSWD | 1,640 |
| 29 | TAMWORTH | YSTW | 1,594 |
| 30 | ALICE SPRINGS | YBAS | 1,496 |
| 31 | HAMILTON ISLAND | YBHM | 594 |
| 32 | AVALON | YMAV | 492 |
Source: Airservices Australia and Sea World Helicopters
While they are managed under the same rules, high frequency short duration flights at tourism centres have a different risk profile to normal charter flights. On one hand, the flights are ordinarily conducted in good weather during daylight hours, and navigating the route requires little effort. On the other, there is a higher concentration of aircraft, rapidly changing airspace, and high levels of interaction with passengers.
The high frequency of short duration scenic flights necessarily meant that a greater proportion of the flights conducted by SWH helicopters spent time below 500 ft in the stages of take-off and landing. Research has shown that pilots experience greater levels of workload during the take-off and landing phases of flight, and less during the cruise phase of flight (Di Nocera and others 2007).
There was no evidence of complacency among pilots at Sea World Helicopters. Videos showed the pilots were active in managing their flights. In interviews, 4 current Sea World Helicopters pilots also expressed a high level of awareness of the level of risk associated with operating around Southport, and recalled the pilot of VH-XKQ as a diligent pilot who placed a high value on taking time to ensure flights were conducted correctly.
However, there is an extensive body of research demonstrating that repeated practice, as found in highly repetitive scenic flights, leads to increased automaticity where attention and control shifts from deliberate action to less effortful performance (Charlton & Starkey, 2013). Dismukes and colleagues (2017) identify the susceptibility of professional pilots to errors when conducting highly practiced procedural tasks:
It is not surprising for a pilot occasionally to inadvertently omit an item of a checklist performed thousands of times previously, often several times a day. When individuals perform a simple task in the same way many times the action often becomes automatic, requiring only a minimum of conscious supervision… (This) automaticity is vulnerable to error under some circumstances.
Organisational and management information
Village Roadshow Theme Parks ownership prior to December 2018
Village Roadshow Theme Parks (VRTP) was a large company with around 3,000 employees. The helicopter operations were a small part of that company and had been a feature at Sea World for over 40 years. In December 2018, VRTP sold the helicopter operations to the current owner. Until that time, VRTP had its own Air Operator’s Certificate (AOC) and key position holders including a HOFO and safety manager. The HOFO and safety manager were reported to be well resourced and supported by various departments within the company, such as finance, human resources, marketing, facility management and a safety team. It was also stated that as part of the company’s safety oversight, external aviation specialists were engaged to audit[61] the helicopter operation on a biannual basis.
Under VRTP ownership the scenic flight operation ran from 2 overwater helipads, the park pad and the hangar pad, which were sited 53 m apart (Figure 73). Although the park pad only had room to land one helicopter at a time, it was reported that in the peak season 2 helicopters would operate in sequence from the park pad. It was also common to operate from the hangar pad and the park pad at the same time. These configurations presented operational demands to manage.
Figure 73: Helipads as operated by previous owner
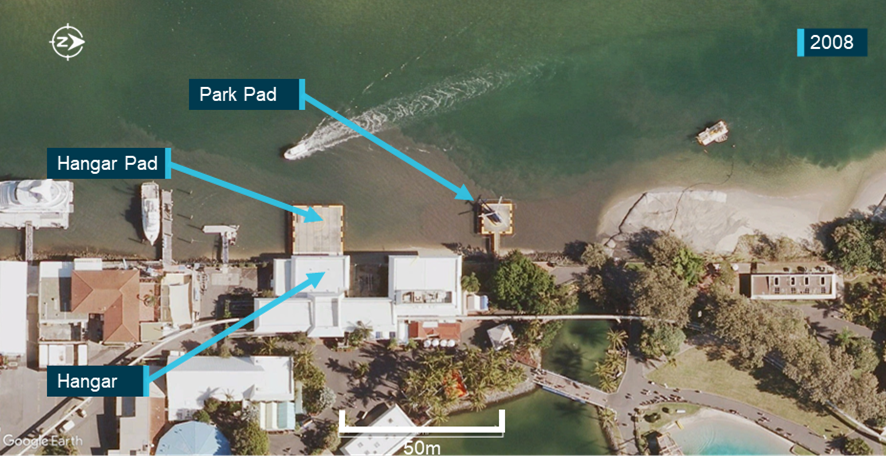
Source: Google Earth, annotated by the ATSB
With 2 helicopters operating from the park pad, timing of flights was important as the outbound helicopter would have to be clear for the inbound helicopter to land. When using the hangar pad and park pad at the same time, downwash from helicopters affected the upwind pad. This would result in high frequency low consequence events such as rotor wash and salt spray on the windows of the helicopter. Ground crew would then be delayed cleaning the windows before the next flight.
Interviews with 3 pilots of the previous operator revealed that the operator found that standard CTAF calls were not sufficient to provide the level of coordination required. To manage the timing of concurrent flights and prevent these downwash issues the operator used 2 further controls in addition to the standard radio calls. The pilots would communicate with each other over UHF to generate team situation awareness of where other helicopters were. That enabled them to slow down or speed up flights to fit into the pattern.
Additionally, prior to departure the pilots on the ground would also refer to an electronic flight bag (EFB) (an iPad with the OzRunways navigation and flight planning product), which included a traffic display that showed the pilots to within around 5 seconds where their company helicopters were. See also Operational procedures.
The enhanced communication controls were recorded in the operator’s safety management system (SMS) in a job hazard analysis for scenic flight operations from the theme park.
Historic use of the car park pad
The car park pad was 180 m south of the park pad and reportedly first became a pad for helicopter and hovercraft transfers for the world expo in 1988. It saw irregular use and for a few weeks a year, during Chinese New Year, the VRTP helicopter operation used it to expand capacity. They cross‑hired an additional helicopter and created a temporary facility at the car park pad (also known as the whale watch pad) to protect staff from the elements and manage customers at the site during use.
For cross‑hired helicopters and operation of the car park pad, a change management process was conducted and if existing operational controls could not be supported, alternative mechanisms were put in place.
Figure 74: Car park pad prior to redevelopment

Source: Google Earth, annotated by the ATSB
In summary, for most of their operations, to manage multiple helicopters, VRTP as the operator had:
- primary helipads in line of sight of each other for majority of approach
- limited use of car park pad
- UHF radios for chatter between pilots (VHF frequency 123.45 if no UHF in hired helicopters)
- EFB with traffic display.
The flow-on effect of using these controls to address high frequency low consequence events was to support and maintain a level of team situation awareness, which was also a defence against collision of company helicopters.
Sea World Helicopters change of ownership from December 2018
In December 2018, VRTP sold its interest in Sea World Helicopters to the new owners. Under a concession agreement, VRTP permitted Sea World Helicopters to use part of its site for its operations. At the same time, under an intellectual property licence, VTRP permitted Sea World Helicopters to use the Sea World trademark. From that point, Sea World Helicopters sold scenic helicopter flights at Sea World as an independent operator.
As part of the sale there was an understanding that the new owners would redevelop the car park pad and refurbish the park pad. While the new heliport was developed in the car park, operations were to continue from the hangar pad and the park pad. The new chief executive officer (CEO) of Sea World Helicopters reported that they implemented a change to fly the scenic flights in an oval racetrack pattern instead of a figure 8 to remove a crossing point and reduce the risk of midair collision.
The incoming CEO of Sea World Helicopters was familiar with the operation having conducted training and checking activities there around 30 years earlier. The new owners owned another helicopter business which included flight schools and a large tourism operation, and elements of that company were used to support operations at Sea World. This included internal quality audits, supply of helicopters and pilots and management support. VRTP stated that they continued external oversight of the operator through annual second‑party audits by external experts to comply with VRTP’s own WHS obligations.
Following the change in ownership, there was a turnover of staff. The team that implemented the SMS, including the safety manager, had left without replacement. Responsibility for the SMS was given to external parties. Pilots who had operated scenic flights for a number of years moved on, and the HOFO departed after handing over the role to the pilot of XKQ prior to the new heliport facility opening in August 2019. Additionally, all records of operation remained with the new owners.
On 15 August 2019 the new heliport (see Aerodrome information above) was opened on the grounds of the old car park pad. On 7 October 2019 the hangar pad in the theme park was closed, condemned and was not reopened. Very soon after, on 12 November 2019 the park pad was also condemned and operations there ceased. Sea World Helicopters’ operations were conducted from a single location. Operating the helicopters solely at that facility brought several benefits:
- all approaching helicopters had clear view of activity on helipads
- all departing helicopters had a clear view of the airspace they departed into
- reduced rate of downwash and salt spray issues
- no requirement for intersecting flight paths.
Changes to helicopter operations
Sea World Helicopters’ senior management stated that it was their intention to continue running the operation as it had been by the previous owners. They advised CASA that operations would continue unchanged. They also stated that they did not consider that anything had changed by the time of the accident. However, many changes had taken place, specifically:
- company size and structure
- senior management
- key personnel
- Head of Airworthiness and Maintenance Control
- Safety Manager
- Head of Flight Operations
- passenger handling facilities
- fuel and hangarage facilities
- helipad positioning
- pilots
- Approved Maintenance Organisation
- addition of EC130 B4 helicopters to the fleet.
Disruption due to global pandemic
During the COVID-19 pandemic, from March 2020, the state of Queensland declared an emergency and non-essential services were closed. International and interstate travel to Queensland was halted, and inbound tourism stopped. The number of flights, and therefore revenue, dropped dramatically. The number of annual flights dropped from over 20,000 to around 3,500. During the pandemic closure period the operator reported dropping from using 3 or 4 helicopters per day down to 1 and released all but 2 of their pilots.
During this period the company owners sought to change the product offering to make it a higher quality experience. This change in product offering meant replacing the AS350S D2 helicopters with EC130 B4 helicopters and a greater focus on customer service and add-on sales to customers. The operator also introduced a new booking system which integrated with the iPads used as EFBs in the helicopters to show booking and passenger manifests to the pilots.
At the end of June 2020, the theme park reopened to local tourists and in July 2020 border restrictions eased. State borders reopened with restrictions in December 2021, and a tourism industry recovery began. The operator stated that business hadn’t returned to pre-pandemic levels.
New heliport
The new heliport facility was considered to bring improvements in safety, aircraft management, and passenger experience over the previous facilities. The first flight from the new heliport was 15 August 2019. In summary, the facility brought improvements in:
- improved passenger flow and manifesting
- larger crew rest facilities
- larger operations management areas
- on shore helipads
- larger apron for manoeuvring
- improved hangar facilities
- new fuel facility.
Park pad refurbishment
In September 2021, prior to refurbishment, VRTP commissioned a report, for the stated purposes of VRTP complying with its WHS obligations, ensuring that aviation compliance issues were considered in the planned remediation works, and determining whether the facility was suitable to be operated as a helipad again. Aviation experts assessed the park pad using the guidance available at the time, ICAO Annex 14 Aerodromes Volume 2 Heliports (2020) and the Civil Aviation Advisory Publication (CAAP) 92-2 Guidelines for the establishment and use of helicopter landing sites (HLS) (CASA, 2014).
The review determined that the size of the helipad was appropriate and that use with the operator’s AS350 helicopters conformed to the guidance. The report concluded:
Once structurally repaired and approved, appropriately marked and with safety services such as first aid and others, a wind indicator and firefighting equipment upgraded, there would be an expectation that this HLS could successfully re-commence flights to support SWH and VRTP commercial operations.
Sea World Helicopters funded the refurbishment of the park pad and facilities, following the recommendations of the report. VRTP verified the implementation of the recommendations. The helipad was a 9 m square concrete helipad constructed over water and accessed by a footbridge. Pad markings conformed with CAAP 92-2. Improvements included a new briefing room and windsock, and it reopened on 12 March 2022. See also Aerodrome information – Park pad.
Helicopter landing site guidance
The helicopter landing sites at Sea World were not certified or required to be certified. Uncertified helicopter landing sites are not regulated by CASA. Any location that meets regulation 91.410 of the CASR (notwithstanding any applicable local laws) can be used as an aerodrome. CASA’s guidelines for helicopters in AC 91-29 v1.1 (2022) Guidelines for helicopters - suitable places to take off and land, stated that:
2.2.1 Regulation 91.410 authorises a place for use as an aerodrome if it is suitable for the landing and taking-off of aircraft and that the aircraft can land at or take off from the place safely, having regard for all of the circumstances of the proposed landing or take off including the prevailing weather conditions.
Essentially anywhere a pilot can land or take off safely can be used as an uncertified aerodrome. While there are no mandatory requirements for helicopter landing sites, CASA provided guidance based on ICAO Annex 14 and its supporting documents. Publications available throughout the development of the operator’s helipads are listed in Table 13.
Table 13: Guidelines on establishment and use of helicopter landing sites over time
| Source | Document | Date and edition | Guidance on conflict on approach and departure |
| ICAO | Heliport Manual (Doc 9261) – Heliport Manual | 3rd edition 1995 |
Provide adequate separation from aeroplane traffic patterns
|
| ICAO | Annex 14 Vol 2 – Heliports | 4th edition 2013 | Nil guidance – referred to ICAO Heliport Manual |
| CASA | CAAP 92-2 (2) - Guidelines for the establishment and use of helicopter landing sites (HLS) | February 2014 | Nil guidance |
| CASA | AC91-29 v1.0 - Guidelines for helicopters - suitable places to take off and land | October 2021 | Nil guidance - referred to ICAO Annex 14 |
| CASA | AC139.R-01 v1.0 - Guidelines for heliports - design and operation | April 2022 |
Assess impact on nearby certified aerodromes Minimise interactions between heliport traffic and pre-existing aerodrome traffic |
| CASA | AC91-29 v1.1 - Guidelines for helicopters - suitable places to take off and land | July 2022 | Referred to AC 139.R-01 |
While ICAO guidance on deconfliction and simultaneous use of nearby heliports was not directly applicable to the Sea World helipads at the time of the accident, the guidance in the ICAO Heliport manual outlining the concept of deconfliction was available for consideration.
Simultaneous operation of helipads for departures to the south
When Sea World Helicopters took over the operation in November 2018 it was operating from the hangar pad and park pad. The pattern of inbound and outbound flight paths changed twice during redevelopment of facilities. For the first year, during operation of the hangar pad and park pad there was a conflict point between outbound and inbound flights, near to and between the helipads (Figure 75).
Figure 75: Flight paths to the south in the first 9 months of operation
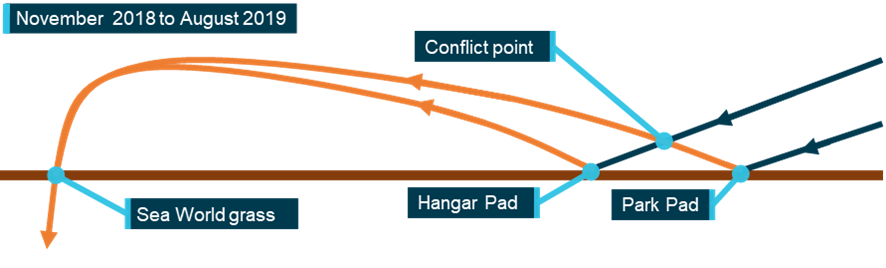
Note: horizontal axis represents a north (right) south (left). Orange paths represent outbound flight paths and blue paths represent inbound flight paths. Source: ATSB
Pilots inbound to these helipads were able to observe activity on the other pad for the majority of their approach (Figure 76).
Figure 76: Visibility of helipads in the original configuration

Source: Sea World Helicopters, annotated by the ATSB
In August 2019 the heliport opened and, for a 3‑month period, the heliport and the park pad were open together, matching the arrangement on the day of the accident. August to November is the period between low and high visitor numbers to South East Queensland. In October 2019 the hangar pad was closed, and in November 2019 the park pad was closed. For the next 2 years and 5 months, operations were solely from the heliport and there was no conflict point outside of operations at the heliport itself (Figure 77).
Figure 77: Flight paths to the south from November 2019 to March 2022
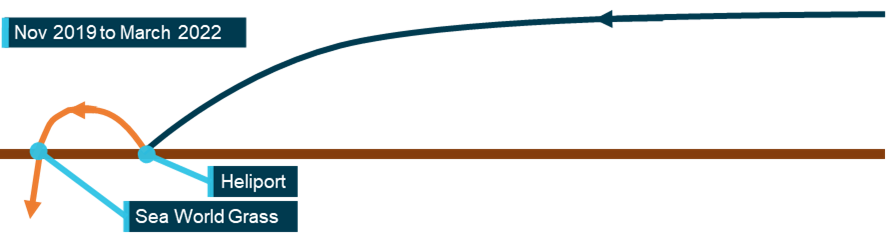
Note: horizontal axis represents a north (right) south (left). Orange paths represent outbound flight paths and blue paths represent inbound flight paths. Source: ATSB
In March 2022 the park pad reopened and operated simultaneously with the main heliport. This final configuration was the one intended at purchase of the company in late 2018. Once the park pad opened, a conflict point was created near to the main heliport between outbound flights from the park pad and inbound flights to the heliport (Figure 78).
Figure 78: Conflicting flight paths to the south from March 2022 onwards
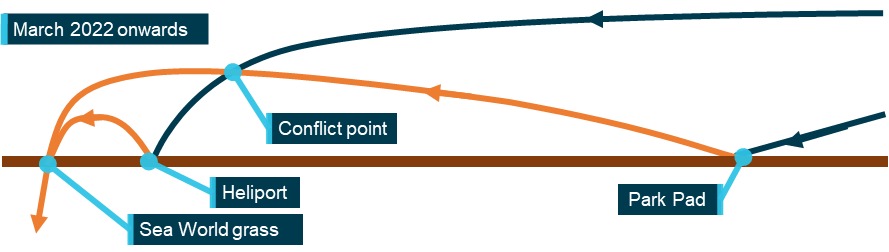
Note: horizontal axis represents a north (right) south (left) Orange paths represent outbound flight paths and blue paths represent inbound flight paths. Source: ATSB
Additionally, this configuration made it more difficult for a pilot approaching the heliport to observe activity on the park pad as it was now in the periphery or even outside of the pilot’s vision on approach (Figure 79).
Figure 79: Visibility of helipads in final configuration

Source: Sea World helicopters, annotated by the ATSB
The conflict point created can be seen in the visual representation below of all flight paths from 26 December 2022 to 2 January 2023 in XH9, XKQ and one of the operator’s AS350 helicopters (Figure 80). As can be seen, outbound flight paths from the park pad intersected with inbound flight paths to the helipad at the same height. This also corresponded with where the helicopters collided.
Figure 80: Traffic flow to and from the park pad (orange) and heliport (blue) 26 December 2022 to 2 January 2023
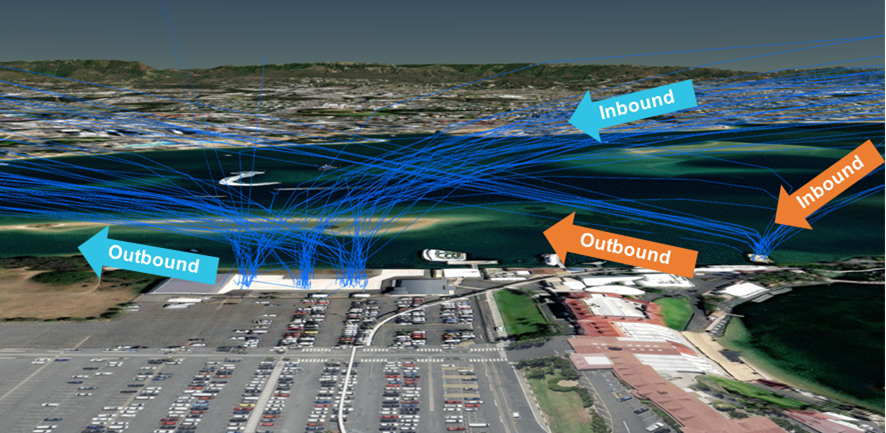
Source: ATSB
The operator was aware of the conflict point and stated that the intersecting flight paths used at Sea World were controlled through airmanship,[62] communication and rules of the air as at any aerodrome with intersecting runways.
Video and GPS data showed XKQ tracked directly from the park pad to the sandbar, which matched normal operations from the park pad. Taking off at the park pad and flying directly to the sandbar without a clearing turn appeared to be standard practice. Also, the track of XH9 was shown to be similar to previous flights. The flight paths of both helicopters prior to the accident were within the bounds of normal operation (Figure 81).
Figure 81: Accident flight trajectories with prior tracks
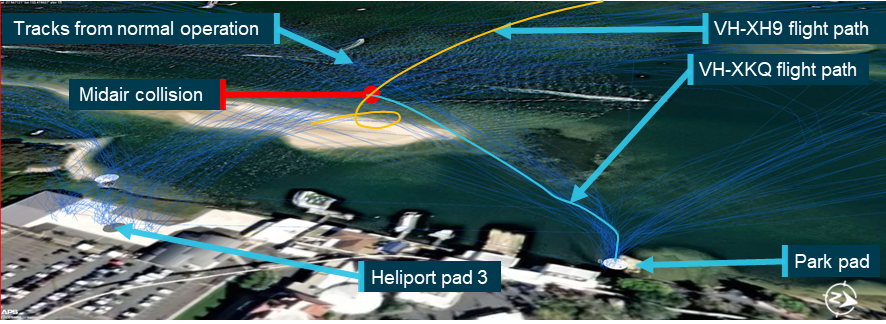
Source: ATSB
Addition of EC130 B4 helicopters to the fleet
As described in Sea World Helicopters fleet, the operator had begun to replace the AS350 helicopter fleet with EC130 B4 helicopters.
The timeline of implementation is detailed in Table 14.
Table 14: Sea World Helicopters implementation of EC130 helicopters
| Date | Activity |
| 5 December 2016 | First record of EC130 use in available documentation under previous ownership |
|
31 January 2018 to 27 April 2019 |
EC130 VH-EHY 7 instances of occasional cross‑hire |
| 12 September 21 | XKK added to fleet on cross‑hire |
| 12 September 21 | HOFO EC130 familiarisation flight |
| 15 December 21 | XKK used on scenic tours |
| 9 April 22 | Ground crew training on EC130 |
| 18 July 22 | HOFO EC130 pilot maintenance training |
| 22 July 22 | Ground staff identified that the briefing cards and pre-departure safety video do not show EC130 belts or doors, and raised this in a safety meeting |
| 09 September 22 | Briefing cards changed to include EC130 |
| 22 September 22 | EC130 seatbelts filmed for inclusion in passenger briefing video |
| 10 October 22 | Line pilot EC130 theory exams |
| 15 November 22 | Line pilot EC130 pilot maintenance training |
| 2 December 22 | XH9 completed certificate of airworthiness |
| 4 December 22 | Line pilot EC130 training |
| 4 December 22 | First use of VH-XH9 in scenic flights |
| 5 December 22 | Line pilot EC130 training |
| 9 December 22 | XKQ completed certificate of airworthiness |
| 26 December 22 | First use of VH-XKQ in scenic flights |
The HOFO of the previous owner (VRTP) stated they always conducted change management for new helicopters, and evidence existed to support that.
The current operator reported that none of the EC130 B4 helicopters in use at Sea World Helicopters at the time of the accident went through a change management process (see Safety management). Although none of the risk controls previously implemented relied on the type of the helicopter, the operator reported that change management was not necessary as the type certificate of the helicopters was the same as helicopters previously used and the type was listed on their AOC.
The operator stated that helicopters XH9 and XKQ were acquired to become the primary helicopters for scenic flights. A company pilot reported that ’the EC130s were pushed in before Christmas … to use them as a marketing tool’. That statement was supported by the meeting minutes from 30 December 2022 which read ’Need to push only EC130 on social media to push those machines’.
Both the CEO and owner of the organisation provided evidence that they spoke with the HOFO multiple times per day. The stated purpose of some of those calls was to assess how the pilots were settling into the new helicopters. For example, during these calls the CEO was made aware of problems with XH9’s transponder.
The operator trained the pilots and ground crew and made changes to procedures and operational documentation to allow the use of the helicopters in scenic flights. Helicopter XH9 started full time scenic flights on 16 December 2022 and XKQ started on 26 December 2022.
Following review of the draft report the operator stated:
The choice of which of the available aircraft to use was not influenced in any way by senior management.
Air operator’s certificate and structure
The Air Operator’s Certificate (AOC) for Sea World Helicopters was renewed by CASA on 21 July 2022. It covered Part 119 (air transport) and Part 138 (aerial work) and was valid until 31 July 2027. The organisation was authorised to perform helicopter air transport flights and was in the process of transitioning to Part 133 (air transport in rotorcraft).
Sea World Helicopters’ company strategy was to create an immersive experience with quality cues in the facilities and helicopters. The operator invested in facilities designed for smooth handling of a high volume of passengers. An external business consultant was used to reconfigure business functions and work with the owner on business strategy. Additionally, they employed experienced pilots and training and checking staff.
The structure of the organisation related in interviews did not match the structure depicted in the operator’s exposition (Figure 82 left). The operator reported that it was decided in consultation with CASA that just one CEO would be in place. The structure as described to the ATSB by participants in the company is described below (Figure 82 right).
Figure 82: Organisational structure
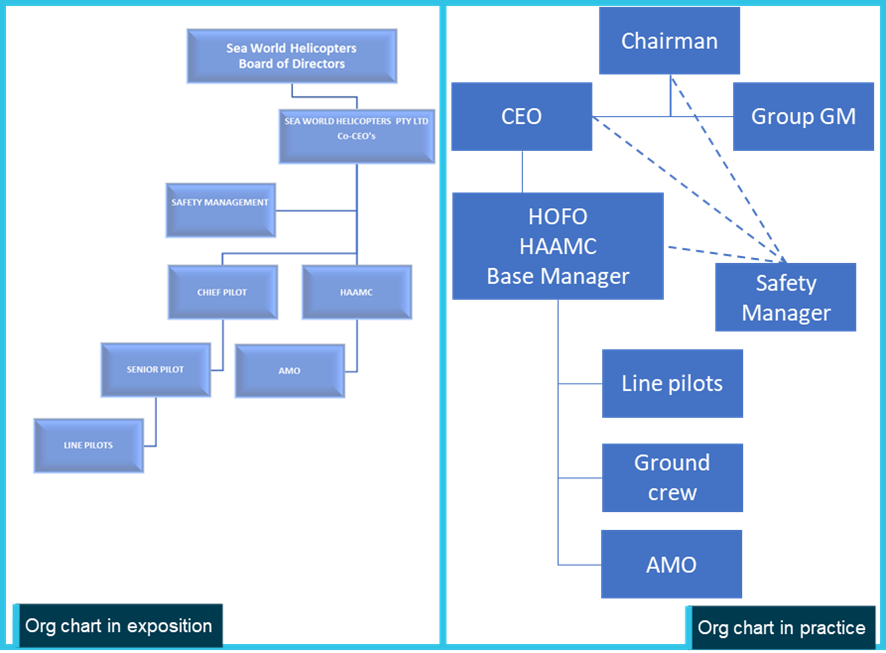
Source: Operator and ATSB
The owner held the position of chairman and employed a CEO and a general manager (GM). All 3 position holders lived interstate and would meet remotely or visit the operation and meet onsite.
The chairperson was accountable for directing investment and development of the business. The CEO was the accountable manager for all aviation operations and was also a training and checking captain for the pilots. The CEO also managed aviation operation decisions with the HOFO.
The GM employed by the owner was focused on the initial transition and setup of the business. That included creating business functions such as human resources, marketing and accounting. Once the business was operating the GM turned their attention to setting up functionality of the new facilities, setting-up reporting and supporting marketing processes. Their continued involvement was as a business development consultant and to conduct HR processes.
The pilot of XKQ, as HOFO, was tasked with the day-to-day running of the business. This meant they were involved in every facet of the business, including people management, line flying and fulfilling several key roles for the AOC.
An ATSB assessment of a sample of the HOFO’s communication for the previous 6 months showed that 19% of communication was related to their role as HOFO and 29% to their role as HAAMC. The remaining 52% was related to operation of the business. Additionally, following the draft review process the operator provided an analysis of 1,490 of the HOFO’s emails. Similarly, the operator found that 55.6% of the HOFO’s communication was related to operation of the business.
Colleagues of the pilot of XKQ at all levels were consistent in their description of the pilot as the cornerstone of the operation. Though there was support and contracts in place with external companies in various aspects of the business such as accounting and marketing, the pilot of XKQ remained involved in all activities, managing day‑to‑day operations and leading the team.
The pilot’s colleagues were also consistent in their assessment of the pilot of XKQ being a supportive and capable leader who ran the business well. The report of a second party audit conducted on behalf of VRTP published on 24 January 2022 stated:
The HOFO (head of flight operations) is a competent and proficient office-holder who has successfully combined the tasks of flying whilst managing the complexities of the operation during extraordinary times. However on occasion this workload comprises an excess of tasks, and his office could benefit with assistance from a post holder who is schooled in the SM’s (safety manager) role.
As a result, in May 2022 the pilot of XH9 was appointed as safety manager. Reporting lines for the safety manager were reported to be to the chairman, CEO, and HOFO. The safety manager had been in place for 7 months and had made progress towards re-establishing the operator’s safety management system.
The operator advised that at the time of the accident, they employed 7 full time or permanent part‑time staff, and 11 casual employees including office staff, ground handling staff, 3 permanent pilots (including the HOFO) and 3 casual pilots.
Regulatory oversight
In line with the Civil Aviation Act (1988) and within the resources available to the Civil Aviation Safety Authority (CASA), CASA oversighted authorisation holders, such as pilots, engineers, and commercial Air Operator’s Certificate (AOC) holders.
Planned surveillance was conducted under the National Surveillance Selection Process (NSSP). The NSSP commenced in the 2018–19 fiscal year. Under the NSSP CASA prioritised high volume air transport operators in their oversight of over 2,000 authorisation holders. The factors included in prioritisation were an authorisation holder’s:
- safety performance
- safety findings and findings history
- time since the last surveillance event
- specific safety-related risks.
Prior to the change in ownership, Sea World Helicopters was audited in 2016, and that audit made 4 observations. The next audit was on 22 October 2019. That audit was originally planned for June 2019 and was delayed to conduct the audit in the new heliport facility. That surveillance event made 4 administrative findings which were all subsequently acquitted.
For the fiscal year 2022–23, CASA reported that it did not audit any AOC’s. This was to minimise the burden both on industry and CASA as part of the transitional arrangements from the Civil Aviation Regulations to the Civil Aviation Safety Regulations.
CASA also had oversight over appointment of all key personal and acceptance of operational documentation. These activities included:
- appointment of pilot of XKQ as HOFO for Sea World Helicopters
- appointment of pilot of XKQ as HAAMC
- operator’s transition to Part 119 of the CASR
- operator’s ongoing transition to Part 133 (incomplete at time of the accident)
- operator’s transition to Part 138 of the CASR
- operator’s training and checking system transition
- operator’s fatigue system transition
- renewal of AOCs.
One month prior to the accident the operator had submitted an implementation plan to CASA for transition of their SMS to meet the requirements of Part 119 of the CASR. This application had not been assessed at the time of the accident.
Safety management
Introduction
A Safety Management System (SMS) is a structured approach to managing aviation safety risk. It supports operational crew by providing the means to design safer operations and manage hazards, incidents and emergent risks. It allows organisations to define their own tolerance for risk through establishment of procedures, training and assurance activities to ensure consistency and maintenance of risk controls.
CASA produced a resource kit which carried practical and accessible advice on the implementation and functioning of SMS for small operators in 2012 (CASA, 2022b). The SMS resource kit carries a particularly important definition (CASA, 2022b).
A key difference between WHS and an SMS is the intent. The intent of WHS is to meet legal and ethical obligations by fostering a safe and healthy workplace. Whereas an aviation SMS intentionally focuses on the safety management functions relating to, or in direct support of, the safe operation of aircraft. This means it goes beyond just legal obligations, and prioritises actions to address safety risks at all levels. Thus it more effectively manages organisational resources for the optimal benefit of aviation safety.
CASA (2022b) follows the ICAO SMS framework (2018) which consists of 4 components:
1. Safety policy and objectives
2. Safety risk management
3. Safety assurance
4. Safety promotion
Hudson’s culture ladder (CASA, 2017) describes 5 stages of maturity of an organisation’s culture as it relates to safety management. They range from:
Pathological - management believes accidents are caused by inattention on the part of employees
Reactive - safety becomes a priority after an accident
Calculative - calculative cultures have a process and use it
Proactive - use processes and systems to anticipate safety problems before they arise
Generative - a state where subject matter experts take responsibility and safety awareness is spread throughout the organisation
The aim is for organisations to transition along this ladder to a point whereby aviation safety risk management is an integral part of day-to-day activities.
The regulatory requirement for SMS in helicopter tourism operations in Australia was introduced by CASA in 2021. The requirement to comply with the regulation was deferred until 2 December 2024. Regulation 119.035 of the CASR stated:
An Australian air transport operator must have a safety manager.
And regulation 119.190 of the CASR stated:
An Australian air transport operator must have a safety management system that is appropriate for the size, nature and complexity of the operator’s Australian transport operations.
This section describes the path of safety management at Sea World Helicopters from inception to the day of the accident through the safety management framework described in CASA guidance.
Safety management before change of ownership
Records show that Village Roadshow Theme Parks (VRTP) and their HOFO had voluntarily implemented an SMS in their helicopter operations in 2014. In May 2017 they appointed a line pilot as safety manager to manage the system. Additionally, the helicopter operation had the support of VRTP’s operational safety team that managed safety at the theme parks. Hazard and incident reporting from the helicopter operations pilots went through the helicopter operations and VRTP’s theme park focused SMS and examples of proactive management of aviation safety risk were readily available. For example, an issue arose with fuel contamination and VRTP grounded the helicopter operation for around 90 days, until the issue was investigated, and alternative fuel supplies were implemented. The process could be followed through documentation in the SMS.
Senior management of that operation advised that as they were flying around 2,500 hours a year, they expected hazards to be reported. Evidence of SMS artifacts such as hazards and incidents raised by pilots, and job hazard analysis documents and change management documents were available and showed the system was used to gather information and manage aviation safety risk, including the risk of midair collision between company helicopters. Change management documents, interviews and records showed the system was well supported by VRTP and maturing in its application and acceptance. VRTP’s Management Risk and Compliance Committee governed and oversighted the helicopter operation. Oversight included the use of aviation consultants to conduct audits to ensure compliance with aviation regulations.
Senior management advised that while VRTP’s safety team was not involved in the sale of the helicopter business, they were able to meet with the new owners and advise of the kind of hazards they had in their system after the sale. They reported that the new owners retaining the HOFO and safety manager was a good sign that safety would continue being managed.
Safety management following change of ownership
Following the sale of the business in December 2018 and handover of hazard information, the VRTP safety team and management risk and compliance committee were no longer involved in the helicopter operation. VRTP did retain aviation consultants to maintain external auditing of the helicopter operator for their own WHS obligations. Incoming senior management stated that the SMS at the time of takeover was robust and that it supported a safe working environment.
The new owners reduced the number of full-time pilots by one, and the HOFO was involved in transfer of functions. The original safety manager/pilot engaged by VRTP remained on staff with the new owners of Sea World Helicopters. They reported they were not called on to discuss safety with the new owners and instead were returned mainly to line pilot duties, effectively ceasing the role in August 2019 without direct replacement or handover.
The COVID-19 pandemic impacted the operation in 2020. There was potential for disruption across all aspects of the operation including flight operations (Li and others, 2022) and aircraft maintenance. The operator had reduced operations to a single helicopter. Records showed that hazard and incident reporting was low, and no aviation safety risk was managed in the SMS in 2020. A third-party contractor was tasked with re-writing the safety management manual suite which was released 30 June 2020.
The operator stated that up until May 2022, safety at Sea World Helicopters was supported by part-time offsite management through their other helicopter company. Interviews with pilots and SMS records showed during the period of offsite management, which included COVID-19, little use of the SMS or its procedures was made for management of aviation safety risk (Figure 83). Though the other helicopter company had extensive and long running tourism operations, there was no evidence of either operation sharing hazards or risks or informing each other’s improvement of aviation safety risk via the SMS.
Figure 83: Rate of hazard and incident reporting
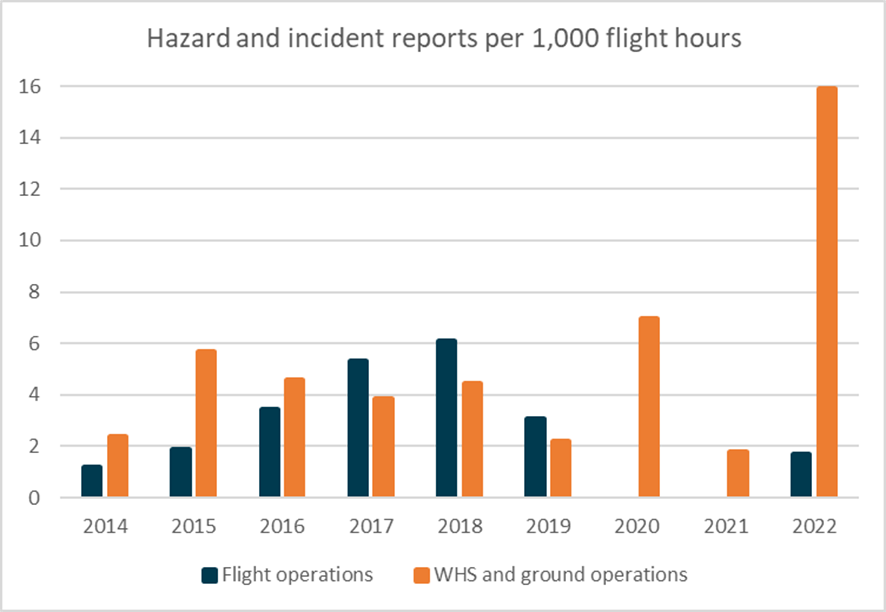
Note: Operator‑supplied flight and hazard reporting data has been normalised to a rate of reports per 1,000 flight hours. Source: ATSB from operator flight and reporting data
A review of contemporary evidence found some offsite support in the form of advice to the HOFO, generating forms, and an internal audit[63] for conformance with Sea World Helicopters’ exposition was carried out in August 2022. However, there was no evidence of day-to-day material support, and the SMS appeared to be effectively inactive during the period of offsite management.
Second‑party audits conducted on behalf of VRTP over the next 3 years (2020–2022) initially complimented the operator’s commitment to their SMS. An audit completed in January 2022 found that though new activities had been introduced, only one job hazard analysis had been created and no change management documents were created in the previous 12 months. Additionally, only 2 incident reports had been submitted and neither were concerned with aviation safety.
The external auditor noted the lack of reporting and found that there was no material support for the audits from the offsite safety manager over the last two years. The audit recommended that an onsite safety manager be appointed.
In interview, senior management reported to the ATSB that they disagreed with the VRTP audit that an onsite safety manager was required on the grounds that the operation was too small. Additionally, they reported that they did not agree that safety reporting should be at a higher rate. They stated that a well operated aviation organisation should not have any incidents or hazard reports. The operator did, however, accept the recommendation and appointed an onsite safety manager in May 2022. From that point, use of the operator’s SMS began to collect hazard and incident reports. The CEO reported that reports were mainly concentrated on ground handling and WHS hazards and incidents, and that was reflected in the data (Figure 83). The safety manager’s appointment was formally advised to CASA in November 2022.
External audits (Table 15) documented the changes within the SMS. The first report following the sale acknowledged that the safety manager put in place by VRTP was part of a team that was responsive to audit findings and willing to build on the system. The next report in early 2020 did not review hazard or incident reporting and noted the reason was that the previous safety manager had gone and was replaced by an offsite contractor who was not present for the audit.
The safety manager had changed again by the next audit in December 2020, and was not present for the audit due to COVID-19 travel restrictions. The audit did not record their presence by video or telephone call either, the HOFO was reported to be the only key person available to the auditors.
By January 2022 there was still no input from an external safety manager and the audit report stated that the HOFO was wearing most of the regulatory and functional hats, including safety. The auditors recommended a dedicated onsite safety manager.
|
ATSB observation The rate of reports related to flight operations safety risk dropped off significantly after change of ownership and did not recover after the pandemic. The operator asserted that well ran operations should not have hazard or incident reports. This indicates an incorrect understanding of the purpose of hazard and incident reporting. A fundamental element of accident prevention is the ability to understand risk (Hollnagel, 2016). Risk mitigation requires operators to collect the knowledge to understand the risk (Amundrud & Aven, 2015), and Reason (2016) states that safety systems rely on the input of the people in direct contact with hazards, and that requires a positive reporting culture. All operations are subject to disturbances of various types which lead to uncertain outcomes (Hollnagel, 2016). If an operator is not collecting hazard and incident reports, they cannot reasonably manage the risks that develop in the normal course of operation. |
Table 15: External party audit comments on safety management at Sea World Helicopters
| Date | Comment |
| 2018 | In the last year or so, the most significant change in this area has been the appointment of a Safety Manager (SM), whose prime task was to be the facilitation of the SMS…. The team should be applauded for their willingness to adopt the best practice recommendations from previous audits and improve on their existing achievements |
| Feb 2020 | The Safety Manager role has been taken over by a contractor to essentially overhaul the safety management of the organisation and observations of the progress to date was encouraging…. As the Safety Manager was not present for the audit, a review on the internal safety and reporting alert system was not conducted and will be examined further in the next audit. |
| Dec 2020 | The Safety Manager is a resident of Melbourne and is currently prohibited from travelling to Queensland thus not in attendance for this audit…. Despite the unprecedented changes due to the COVID-19 pandemic, it is noteworthy that there was no evidence of safety being compromised at SWH. This is largely attributed to the procedures and processes embedded in SWH’s SMS. |
| Jan 2022 |
Recommendations:
|
| Dec 2022 |
Progressive enhancements were evident in this Safety Compliance Audit, and these were not only because of external forces but also because of recommended internal improvements. The latter centred around stakeholder positions and documentary changes, and taken as a whole, Sea World Helicopters continues to create sound organisational structures which in turn will allow the organisation to concentrate on industry-leading best practices. Considerations for subsequent audits should therefore include an appraisal of any other areas that have yet to be investigated in detail, such as skydiving, or others as suggested by SWH staff. To that end, the auditors invite SWH to offer suggestions of areas in which they would like to improve and progress so that they may be proactively reviewed and incorporated into the 2023 audit. Overall, VRTP can be confident that because of SWH’s continued quality assurance and managerial commitment that the company is in step with regulatory requirements and with industry best practice. The managerial commitment observed during this audit provided reassurance that the process of change will continue in measured form. |
Source: VRTP
Resumption of the Safety Management System
After the appointment of the new safety manager the SMS was put to beneficial effect in managing hazards and risks in ground handling and work health and safety. The safety manager was successful in motivating ground crew to report and fix issues and use of the SMS was expanding.
Safety meetings restarted and documents showed 6 staff safety meetings were conducted in a 7‑month period between March 2022 and September 2022. Senior management did not attend these meetings either remotely or in person. The CEO was not present at the safety meetings, and the HOFO attended a portion of a single meeting. No records of safety meetings after September 2022 were provided.
Safety was a standing agenda item in management meetings attended by senior management. The safety manager reported that they would brief senior management on safety activities as the first item then leave the meeting.
The operator provided minutes covering management meetings from 30 September 2022 to the date of the accident where implementation of the new EC130 helicopters was discussed. A review of minutes of these meetings showed most of the safety items discussed concerned work health and safety, management of passengers and ground handling of helicopters. Of the minutes provided, the CEO was recorded to attend a single meeting.
An SMS was in place when the new owners took over in 2018, and it was rewritten in 2020 with additions in July 2021 and June 2022. On 13 December 2022, Sea World Helicopters submitted an implementation plan for its SMS to CASA. The operator advised CASA that it would complete implementation of their SMS from 31 March 2023 to 2 December 2024, the limit of the allowable period, to make their SMS compliant with the new regulations. Through the implementation plan the operator stated to CASA that the SMS was not currently functional. However, interviews with senior management, the operator’s documented procedures, audits, and outcomes of SMS activities demonstrated that within the organisation there was an expectation that the SMS was functional and in use.
Safety policy and objectives
Sea World Helicopters’ safety policy, endorsed by senior management, published in June 2020 and reconfirmed on 30 June 2022, carried conventional commitments to continuous improvement, best practice and provision of resources. For example, it committed the operator to, amongst other things:
Minimize the risks associated with aircraft operations to a point that is as low as reasonably practicable/achievable.
Establish and measure our safety performance against realistic objectives and/or targets;
Ensure that the application of effective aviation safety management systems is integral to all our aviation activities, with the objective of achieving the highest levels of safety standards and performance.
The objectives of a safety management system are intended to be practical achievable goals that describe the organisation’s priorities and address its most significant safety risks (CASA, 2022c). They are an opportunity for an operator to strategically focus its attention to their particular risks and guide the activities of their employees in reduction of aviation safety risk.
The operator’s SMS objectives were listed as:
a) Identify and eliminate hazardous conditions
b) Prevent aircraft accidents and reduce aircraft incidents
c) Prevent damage and injury to company property and personnel
d) Provide a safe, healthy work environment for all personnel
e) Incorporate awareness, compliance, inspection, investigation, and education by providing educational material and programs to employees
f) Prevent damage and injury to non-company property and personnel resulting from our operations
An internal audit on August 2022 had identified that the overarching elements of the SMS were too generic, and unsupported by policies that would ensure they were conformed to, stating:
Safety manual: too many “motherhood” statements. Needs policies in place and these need to be listed in the manual.
That recommendation had not been acted upon by the time of the accident. At the time of the accident, the objectives of the SMS were not specifically aligned with the operator’s primary business of high frequency low duration flights from the Sea World Heliport and overwater park pad. The objectives could be applied to any aviation activity. They did not account for frequency of flights, pilot interaction with passengers, overwater operations, or a number of other features unique to Sea World Helicopters’ operation.
A series of similarly generalised performance goals was listed in the SMS and included:
6.5.4 All proposed new equipment acquisitions, facilities, operations and procedures are reviewed to identify risks and potential hazards
and
6.5.8 When establishing and reviewing its goals and objectives, the company will consider… its hazards and risks….
Safety risk management – hazard identification
CASA (2022b) produced guidance on safety reporting within SMS. The guidance explained that effective safety reporting systems are crucial for preventing accidents by identifying hazards before incidents occur. Encouraging reporting fosters a supportive safety culture ultimately enhancing safety and reducing risks.
An electronic hazard and risk management system was initially introduced to the operation in 2018 and older hazards were transferred into it. That system allowed the operator to assess an individual hazard for current and post‑treatment risk, and to create a hazard register for holistic assessment of risk in their operation.
Hazards had been documented under different accountable managers and owners. Between 2 September 2014 and 25 April 2019, mainly under the prior owner, 14 collision risk reports were made, 10 of those were with drones operating in the vicinity of the park, 3 involved other aircraft, and 1 involved watercraft. No hazards involving conflict with other aircraft were recorded after April 2019, and no hazards were recorded until August 2022.
From 2022, incidents recorded were concerned mainly with ground handling events and passengers moving on the helipads. Of aviation safety incidents that were mandatory reportable matters to the ATSB, from August 2022[64] there was a birdstrike and an AS350 tail rotor strike on the park pad. Both were classified as high risk for management through the operator’s safety management system, mitigating actions were taken and pilots were briefed on those issues. On those 2 occasions the system worked as designed in a reactive fashion.
An internal audit completed in August 2022 identified that the hazard reporting system was being underutilised and that not all staff had access to it. The response was to increase licencing of the system to extend the system to all staff.
During interviews with the ATSB, while describing aspects of their job, pilots of the operator at all levels related various hazards to operation that had not been captured in procedures and not managed through reporting or more structured risk management activities. These included:
- limitations of visibility from park pad in EC130
- potential for conflicting company traffic
- passengers causing general disturbance and distraction during flight
- high volume of traffic on Common Traffic Advisory Frequency
- losing awareness of airspace changes while loading passengers on the ground
- limited understanding of traffic collision avoidance system by pilots
- traffic collision avoidance system nuisance alerts
- lack of availability of chatter frequency for pilots
- ambiguity in determining if park pad helicopter will depart and when.
|
ATSB observation Although it is unlikely any SMS will always capture all existing hazards, the hazards communicated to the ATSB in interviews, but not captured in the operator’s SMS, each represent a potential failure of the operator’s controls for managing safe scenic flight operations. Not managing hazards allows conditions to persist, making them part of the landscape of tolerable risk for an operator and their pilots. |
Safety risk management – risk management
Risk management is the process of identifying, assessing and controlling risk (CASA, 2022d). Risk management defines the overall context of an operation and prioritises risk for mitigation (Aven, 2016). The quantitative[65] element of the approach involves asking (Kaplan & Garrick, 1981):
- What can go wrong?
- What are the consequences?
- How likely is this to occur?
This quantitative approach is not a standalone activity; it should be supported by subject matter expert qualitative analysis and informed decision‑making. The same can be said for decision‑making, it should be supported by evaluation of data and evidence, otherwise decision‑makers can form unjustified beliefs (assumptions) (Aven, 2019).
The operator’s safety management system had an annex SWH-SMS-PRO-55 which dealt with hazard and risk management from 7 July 2021. It carried advice and instructions on the identification of hazard, management of risk and on monitoring and reviewing defences, but prompted people to use job hazard analysis forms for formal risk assessments.
A risk assessment is much wider in scope and assesses risks to prioritise mitigation by establishing the context of an operation (Aven, 2016). It would be expected that a risk assessment would take a systematic high-level approach to identifying unwanted events, measuring the risk through exposure and consequence across an activity such as scenic flights. It would be expected to consider elements such as infrastructure, environment, personnel, and aircraft. Then using risk matrices or probabilistic analysis, prioritise risk for implementation and communication of controls in a risk management plan.
A job hazard analysis would be expected to be conducted for one particular job. For example, a charter to an offsite location, or a series of scenic flights for a bus tour. A pilot would be expected to refer to the risk management plan while developing a job hazard analysis.
Risk assessment for the operator’s primary operations had not been conducted. Two risk assessments were conducted by a third party for parachute operations.
An internal audit in August 2022 identified that risk analysis was still to be carried out for operations. It stated:
Finding (16 August 2022): Risk Assessments to be completed for all identified activities.
Response (10 November 2022): Nil progress only currently conducted for off base landings
The response to the finding referred to a job hazard analysis, and not to risk assessments.
Job hazard analysis
Job hazard analysis (JHA), also known as a job safety analysis, is an important source of risk identification and management. JHA has a narrow view of a particular task. It is a process of defining the steps of a task and identifying hazards in each step, then defining controls for those hazards for implementation (Glenn, 2011).
Records of JHAs for scenic flight operations went back to 2014 and between then and August 2019, 28 JHA’s were conducted for various operations. The subjects of the JHAs included normal operations of scenic flights, refuelling and novel events including new facilities and offsite charter. Newer JHAs referred to older JHAs. For example, the hazard of midair collision in the cruise identified in JHA01 – Joy Flights, carried through to later documents involving similar operations.
A JHA for simultaneous operation of the park pad and the car park pad during Chinese New Year in 2016 was the first to consider midair collision between company helicopters. It identified ‘Mid-air collision during take-off and landing phases’ as a hazard. The recommended safe job procedure, in addition to calls on the CTAF was for ‘All aircraft to monitor 123.45 on second radio for general chit chat.’ The intent of that chit chat was reportedly to keep the pilots aware of each other’s position and intentions.
Three JHAs were later drafted for the inception of the new redeveloped heliport facility. They covered flight operations, passenger handling and refuelling. The flight operations JHA was dated 14 August 2019, (see Job hazard analysis for implementation of heliport). Following that hazard analysis there were no further additions or amendments to the documents, additionally, there were no hazard or incident reports relating to aviation safety risk at that location.
From November 2021 up to the time of the accident, 7 JHAs were conducted, mainly for offsite landings and charter operations. On 12 December 2021, the HOFO started a JHA for resumption of operations from the park pad (see Job hazard analysis for implementation of the park pad).
Safety assurance
Safety assurance is the systematic monitoring and assessment of an organisation’s safety performance, and includes activities such as continuous improvement, change management and measurement against safety performance indicators (CASA, 2022e).
Some safety assurance activities were conducted:
- external suppliers of fuel and maintenance services were audited
- internal facilities audits were conducted and findings were acted upon
- the operator’s larger sister company conducted an internal audit of Sea World Helicopters’ manuals and procedures.
- emergency response drills were conducted with Village Roadshow Theme Parks.
No safety performance indicators were selected or developed for the organisation. The operator’s documentation carried no advice on developing them. There was nothing documented for monitoring of scenic flight operations. In interview the CEO stated that assurance of separation relied on undocumented informal observation and reporting.
Change management
Change within aviation operations has the potential to introduce hazards which can defeat existing controls, or require implementation of new controls (CASA, 2022a). Change management while not yet matured was an evident practice before the sale of the business. Examples of basic change management practices went back to March 2018 whereby a change management process was used to implement an electronic hazard and risk register.
It was reported that ownership of the change management process was generally reserved for the person in charge of implementing the change, or their nominee. It was also reported that following the change of ownership pre-existing staff such as the HOFO and SM were not significantly involved in decision‑making around major changes, and changes were implemented without a change process.
For example, there was no evidence that an immediate change in the Approved Maintenance Organisation (AMO) used by the operator was subject to a change process (though a supplier audit was conducted). Another major change was the development of the heliport. Although planned for almost a year and under construction for 4 months, there was no evidence of change management for that process. Also, there was no change management conducted for the implementation of the new EC130 B4 helicopters, whereas it had been conducted for temporary use of helicopters under the old ownership.
The operator’s safety management system documents were submitted to CASA to evidence compliance with regulation 119.205 of the CASR Content of exposition, which requires aircraft operators to describe their processes for identifying change and especially significant change, as significant change must be advised to CASA.
Regulation 119.020 of the CASR carries the definition of a significant change and states:
A significant change, for an Australian air transport operator, means:
(a) a change in relation to any of the following:
(i) the location and operation of the operator's main operating bases, including the opening or closing of main operating bases;
(ii) the operator's key personnel; …
(vii) the operator's areas of operation or routes, including beginning to operate in a new area or on a new route (but not including ceasing to operate in an area or on a route);
(viii) the types and models of aeroplanes or rotorcraft used in the operator's Australian air transport operations, including the addition of a new type or model (but not including ceasing to operate a type or model); or
(b) a change in relation to any of the following that does not maintain or improve, or is not likely to maintain or improve, aviation safety:
(i) the plans, processes, procedures, programs and systems for the safe conduct and management of the operator's Australian air transport operations; …
(iii) any other aeronautical or aviation safety related services provided to the operator by third parties; …
(v) any leasing or other arrangements for the supply of an aeroplane or rotorcraft used in the operator's Australian air transport operations; or ….
Aside from the performance goal of reviewing all new equipment, facilities, operations and procedures to identify risks and potential hazards, the operator had a list of triggers for ‘increased vigilance’ during change in the safety management system manual from 22 November 2021, and triggers for change management in an annex of the SMS Management of change that was introduced on 28 June 2022 (see below).
For reference, the reopening of the park pad took place between those dates, and introduction of XKQ and XH9 took place after.
The operator’s SMS manual, relevant to the park pad refurbishment and introduction of the EC130 helicopters, stated:
7.2 Management of Change
7.2.1 While there should be constant vigilance to identify hazards, increased vigilance should be exercised during situations involving organisational or operational change or at other times such as those listed below:
a) When major structural changes are made to the company
b) Times of rapid growth
c) When many employees are inexperienced
d) When new equipment, procedures or processes are introduced
e) If financial problems start affecting operational decisions
f) Pre-assessment of any subcontracted services or equipment.
Within procedural documents, ‘should’ does not have the power of a mandatory requirement, though there is an expectation of implementation where considered relevant to do so. As a result, not all events in the list would result in concerted identification of hazards.
There was a process, but no advice on how to conduct the steps of change management or how increased vigilance should be implemented.
Additional change management annex
The focus of the annex to the SMS, Management of change, was continuous improvement, and it addressed the process for actioning changes to operations, policies and procedures, and identifying which were required to be notified to CASA as significant.
The term significant change can be easily misconstrued. It can be read as a major change that impacts various facets of an operation, or from a regulatory point of view it can mean any change that requires an amendment to the operator’s exposition.
It included a controlled document SWH-SMS-FOR-10 Change and Improvement for a change request. Change requests had been submitted for changes such as:
- updating references in exposition to match new regulations
- updating procedures for USB sales.
The annex captured recording of the need to act and called for risk analysis in planning the change, but it did not address implementation of change through change management processes. Further, while it mentioned post‑implementation evaluation of a change, it provided no procedure for monitoring a change.
With respect to identifying a need for a change management process the annex stated:
4.2.4 Need identified to change
When actioning a proposed change, the CEO, in consultation with the CP [chief pilot or HOFO] and Safety Manager, must follow the change management process flow Figure 1 in section 4.1 using the methodology outlined below.
verify the need for change with reference to the following change instigators:
- new regulatory requirements
- non-compliance notices (CASA)
- audit observations (CASA)
- CASA directions IAW CASR
- continuous improvement process
- new business opportunities or new or different kinds of aircraft
- internal audit results
- change of key personnel
assess the risks of the proposed change considering at least, but not limited to:
- resource requirements
- financial capability of the company
- compliance considerations
- urgency of change
- implementation implications and strategy
- impact on safety
The use of the word ‘must’ makes following the process mandatory to ensure compliance with the regulations. The flow chart taken from CASA guidance and presented in the operator’s manual (Figure 84) required that after the operator identified a need for change, they conduct an evaluation of that change. The manual described evaluation of the change as:
Assess the risks of the proposed change including any controls/mitigations being introduced with the change.
Figure 84: Operator’s change management flow chart copied from CASA guidance
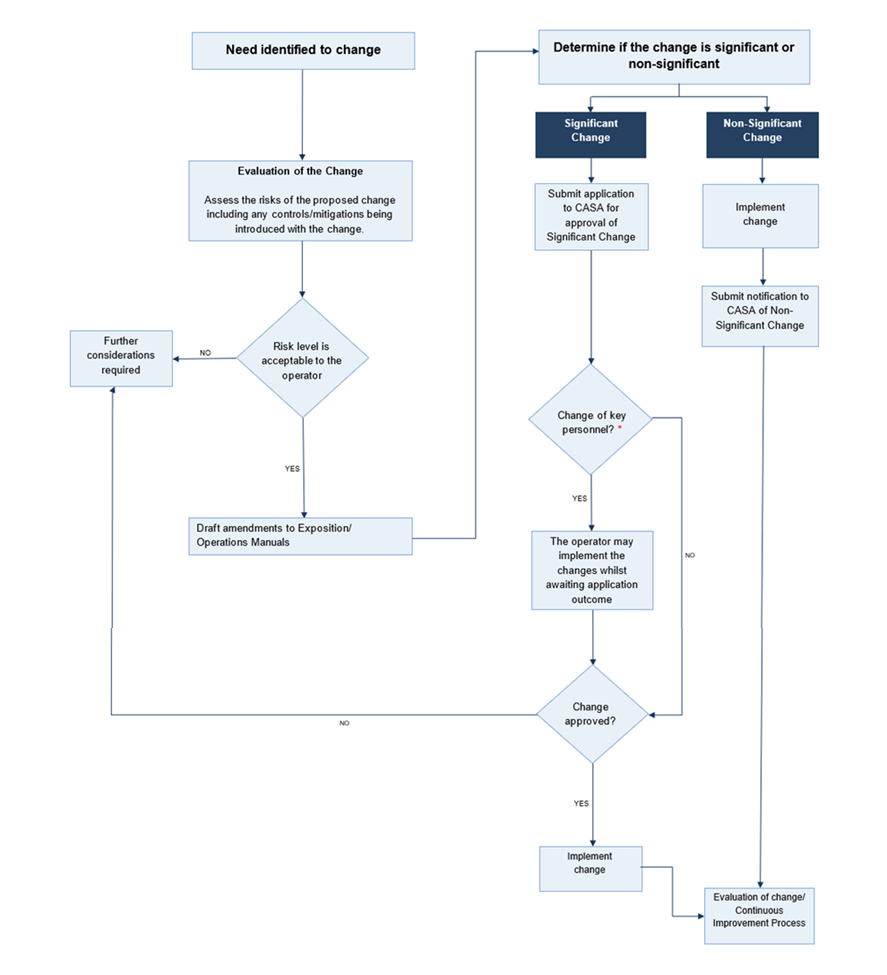
Source: Operator document SWH-SMS-MAN-04 Annex 3 Management of change
The operator stated that it did not consider some of the changes to be significant as they were improving aviation safety. Indeed, the implementation of the operator’s new heliport improved passenger handling and briefing facilities, and created an apron, hangar and fuel facility objectively safer than the previous hangar pad. However, without application of a change management process it cannot be reasonably determined that a change will not have unintended consequences that undermine aviation safety.
Job hazard analysis for implementation of heliport
In interview, the safety manager at the time stated that they were not involved in the development of the heliport from a safety management point of view, until Sea World Helicopters’ senior management requested draft JHAs at short notice to enable flying operations for the new site. A job hazard analysis was drafted on 13 August 2019 – Re-Fuelling and from car park bulk facility and 2 JHA’s were drafted on 14 August 2019, Commencement of Car Park Helipad Operations – Flight Ops and Commencement of Car Park Helipad Operations – Passenger Handling, the day before the first flight from that facility was made on 15 August 2019 (see Job hazard analysis for implementation of heliport below).
On commencement of operations from the new heliport facility, JHA 26 identified the following relevant hazards to aviation safety and listed mitigations (Table 16):
Table 16: Extracts from JHA 26 for the new heliport facility
| Potential Accident or Hazards | Recommended Safe Job Procedure |
|
In-ability to effectively communicate
|
Prior to the commencement of operations, pilots must ensure they have a serviceable UHF radio system for both aircraft to aircraft, and aircraft to ground communication. |
| Potential relevant Accidents or Hazards as described in SWH JHA-01- Joy flights | Pilots shall ensure they are familiar with all relevant potential accidents or hazards as described in SWH JHA – 01 – Joy flights |
| Traffic conflict | Pilots shall maintain comprehensive situational awareness regarding the movements of both company and CTAF traffic employing effective communication via both VHF and UHF radios. |
| Company traffic conflict | Simultaneous approaches and departures are not permitted and pilots shall effectively co-ordinate their movements by UHF. |
| Company traffic conflict | Pilots shall communicate on VHF or UHF radio their intent to taxi for departure. |
Change management for implementation of park pad
In December 2021, prior to reopening the park pad in March 2022 a change management process was commenced. The procedure for enacting the change was defined in steps on the change management form. The elements on the form broadly matched the process outlined in CASA advice on change management (CASA, 2022e) but truncated the intent and missed essential elements of the process. The difference is outlined in Table 17 below.
Table 17: CASA guidance and operator’s apparent process
| Guidance from CASA SMS 4: Safety Assurance | Operator’s change management process as derived from the SMS and park pad change management |
| Step 1: Understand and define the change; This includes a description of the change and why it’s being implemented. At this step you should be identifying if the change is occurring due to internal or external factors and what the overall objective for the change is. |
1 – identify the change / describe the change No advice existed in the SMS. At this stage the change was named “Recommence flights overwater helipad” and described as “Overwater helipad continued use after almost 2 years.” Details were listed as “Rectification of overwater helipad and resume of joy flight operations” |
|
Step 2: Understand and define who and what will be affected; When considering who will be affected, this may be individuals within the organisation across various departments, including contractors and even external parties to the organisation. Equipment, systems, and processes may also be impacted. A review of the system description and organisational interfaces may be needed to fully identify all areas and individuals that may be affected. This is also an opportunity to determine who should be involved in the change process. Changes may affect risk controls already in place to manage other risks, and therefore change could increase risks in areas that are not immediately obvious. |
No advice existed in the SMS. However, a list of team members was made on the change form. These team members included:
There was no evidence of assessment of risk controls already in place to manage other risks, and pilots conducting flights to and from the main heliport were not considered in the change. |
|
Step 3: Identify hazards and complete risk assessments; You need to identify any potential safety hazards related to the change and carry out a safety risk assessment. The impact on existing hazards and safety risk controls that may be affected by the change should also be reviewed. This step should use your already existing safety risk management processes. The most important part of the process is having all the people who are likely to be affected by the change, or who can add value to identifying potential risk, in the room to openly discuss the issues. |
3 – risk assessment y/n Advice on risk assessment was available in SWH-SMS-PRO-55 published 5 months prior to this change. A job hazard analysis (JHA) was conducted rather than a risk assessment as directed by procedures. The JHA was originated by the HOFO and signed only by the CEO. A risk assessment would be wider and address risks in other affected areas, such as operations at the main heliport. (See Park pad job hazard analysis) |
|
Step 4: Develop an action plan; Developing an action plan will define what is to be done, by whom and when, to ensure the change is implemented in such a way as to maintain or improve safety. There should be a clear plan describing how the change will be implemented and who is responsible for which actions, and the sequence and scheduling of each task. This includes not only the tasks required to implement the change itself but also any safety risk controls you identified in step 3 that would be needed to manage safety risks associated with the change. The critical feature of step 4 is the link back to the hazard identification and risk assessment in step 3. This is achieved by extracting the risk treatment strategies, or risk controls, identified in the risk assessments, and listing these items as tasks in the action plan. Each task will have a nominated timeline, responsibilities, and resources. |
4 – change plan No advice existed in the SMS. Project steps, ownership and completion date were recorded. Most steps were related to readying the infrastructure. There were steps for:
|
| Step 5: Sign off and implement Change; This step is done to confirm the change is safe to implement. The individual with overall responsibility and authority for implementing the change should sign off on the change plan. However, your accountable manager and safety manager should also sign off on the appropriateness of the risk assessment and action plan steps of the change as well |
There was nowhere for a change to be signed off, or for the accountable manager to accept the change was a safe thing to do. The accountable manager did sign off on the JHA, implying sign off for the recommencement of operations from the park pad. |
|
Step 6: Assurance planning and ongoing monitoring; The following should be monitored for changes or deviations, with revised actions taken accordingly:
|
5 – review the change (review required y/n) The form required the author to indicate if a review of the change was required and it was stated ‘No’. There was no declared intent on the part of the operator to conduct further reviews of the implementation of the park pad. |
Job hazard analysis for implementation of the park pad
A recommendation from the review of the park pad prior to rectification was the creation of a new risk management plan. The operator conducted a job hazard analysis for the park pad and did not review or amend JHA’s for the main heliport.
Additionally, the change form carried the question:
Step 3 – is a risk assessment (JHA) required?
The JHA accompanying the change management plan was written by the HOFO and accepted by the CEO on 12 March 2022. It dealt only with operations from the park pad and as such included risk of midair collision in cruise flight, but did not consider conflict with company traffic from the heliport on departure, nor did it consider conflict from the point of view of a pilot inbound for the heliport.
Following review of the draft report, the CEO stated that they did consider conflict with company traffic, and as a result checked pilots before they operated at the park pad and required them to look out for other helicopters. They stated that the new conflict point carried less risk than the prior operation, therefore enhanced communication was not required.
Table 18: Controls from park pad JHA
| Potential Accident or Hazards | Recommended Safe Job Procedure |
|
Midair collision in cruise flight
|
Pre-arranged flight paths Traffic collision advisory devices Monitoring and use of the CTAF channel. |
| Tail rotor contact with building or fence | Pilots were not to pedal turn past 90 degrees to fence |
| Engine failure on take off |
Steep profiles Emergency Floats Remaining outside of height velocity curve |
| Aircraft accident on or near pad | Sand bars and beaches to be used as alternate landing sites. |
|
Collision with watercraft Downwind take-off and approaches Excessive winds |
Only approved pilots to operate onto the overwater helipad |
Safety promotion
The pilot of XH9 (safety manager at this time) was aware that the nature of ground crew work, being both a seasonal job and a stepping stone into aviation, meant high turnover of staff. It was observed through interviews with the safety manager and ground crew, and examination of records that the safety manager successfully motivated the ground crew to be involved in improvement of safety in their workplace. In the areas of ground handling and general WHS, the crew was engaged in improving safety in their workplace and made 15 hazard and incident reports in 2022.
Records showed that the safety management system was not consistently applied across the operation. On the flying side of the business, in interviews company pilots reported they believed safety was well managed, citing the HOFO’s insistence on consistent and correct operation. However, current pilots reported that they had not sighted or signed risk documents for the scenic flight operations, and none reported sighting or signing the JHA for operation of the park pad. Additionally, only 2 aviation related hazard and incident reports had been made in more than 3 years. Reports of near collisions with aircraft, drones, and parasailers had dropped from 3.5 per year to zero following change of ownership.
Drug and alcohol management plan
The risk posed by alcohol and other drugs in civil aviation was managed through Part 99 of the CASR. This required certain organisations to implement drug and alcohol management plans (DAMPs) covering employees and contractors who performed safety sensitive aviation activities (SSAA). It also established a program for CASA to conduct no-notice (random) testing for alcohol and other drugs.
Sea World Helicopters Drug and alcohol management plan
Sea World Helicopters maintained a DAMP which met the requirements of Part 99 of the CASR. The DAMP manual included a description of the roles and responsibilities of specific personnel and described the organisation’s drug and alcohol education and testing programs.
The manual stated that the testing program involved testing for drugs and alcohol in circumstances including:
- Upon commencement of an SSAA role, unless the person had been tested within 90 days.
- Following an accident or serious incident. Drug testing was required to be conducted within 32 hours of an accident or incident.
- If a DAMP supervisor determined there was reasonable grounds to suspect the SSAA employee was affected by drugs or alcohol while performing or available to perform SSAAs.
The DAMP education program was delivered using CASA’s DAMP awareness eLearning modules for SSAA employees and supervisors, and the operators DAMP manual. All SSAA employees and DAMP supervisors were required to complete the course on commencement and to refresh the training every 30 months.
The education program consisted of topics including awareness of the potential risks to aviation safety from the use of drugs, and awareness of the operator’s DAMP and testing practices. The safety manager (pilot of XH9) and the HOFO (pilot of XKQ) had completed DAMP supervisor training and were documented as DAMP supervisors.
With respect to the pilots of XKQ and XH9, both pilots were tested upon commencement with the operator, and there were no records of either pilot being tested for drugs or alcohol due to suspicion of use, nor were there records of either of the pilots being involved in an accident or incident at the operator (prior to the day of the accident). As identified in Medical Information, the pilot of XH9 was not tested for drugs after the collision on 2 January 2023.
Another pilot who had been involved in a serious incident (tail rotor strike) in late‑December 2022 was not tested. The operator stated that this was because they didn’t believe the incident to be serious at the time. The operator stated that once it was determined how it occurred, they did categorise it as a serious incident, but by that time the window for testing had passed.
The DAMP manual stated that the operator contracted all alcohol and drug testing to Sea World medical and security departments. The manual stated that Sea World Helicopters had entered an arrangement with VRTP, for VRTP to breath test all Sea World Helicopters pilots prior to their shifts. The Sea World Helicopters Management System & Policy manual further stated that prior to commencing any operations, pilots were required to undergo breath testing for alcohol.
VRTP stated that while they would test Sea World Helicopters staff entering their theme park there was no formal agreement in place to provide drug and alcohol testing to Sea World Helicopters.
Drug and alcohol testing conducted by Village Roadshow Theme Parks
To meet its own WHS obligations, VRTP maintained an Alcohol and Other Drugs Policy, which was applicable to everyone working at a VRTP workplace including contractors. VRTP would conduct testing for the use of alcohol and/or other drugs in circumstances including:
- as part of pre-employment checks for roles identified as high-risk activities (which included Sea World Helicopters’ pilots)
- if a supervisor or manager formed a view that there was a reasonable suspicion of a VRTP team member or contractor being affected by alcohol or other drugs
- on a random basis, which may include daily drug or alcohol testing.
VRTP conducted daily breath testing for alcohol for specified classes of employees and contractors, including helicopter pilots. Daily breath analysis records from the weeks before the accident showed that all Sea World Helicopters pilots were tested by VRTP each day they conducted flight duties. On the day of the accident, both pilots were breathalysed to test for alcohol with nil alcohol detected.
VRTP stated that the VRTP with-suspicion drug and alcohol testing was applicable to Sea World Helicopters personnel, within the theme park, such that if an employee or guest raised concerns about a Sea World Helicopters employee being potentially affected by alcohol or drugs, VRTP would arrange for that employee to be tested. However, such concerns had never been raised.
VRTP conducted random testing for drugs which was also applicable to Sea World Helicopters personnel. A manager at VRTP estimated that about 40 people each month were selected to undergo drug testing. Records showed that the pilot of XKQ provided a sample for this testing on 1 August 2022, and that produced a negative result. The pilot of XH9 recalled that they had not been tested for drugs under the VRTP random testing program.
Sea World Helicopters ground staff who worked at the heliport and did not enter the theme park, would not be subject to VRTP’s random or with-cause testing. Sea World Helicopters stated that as pilots and ground crew worked inside the theme park on almost every shift, they would not be able to predict when they would not be subject to random drug tests.
Random testing by CASA
The ATSB obtained data from CASA regarding random (no-notice) drug and alcohol testing. This data recorded results from testing of 25,909 individuals from July 2018 to June 2023. Almost all individuals were tested for alcohol, and 10,327 were tested for other drugs.
CASA testing included initial and confirmatory field testing for alcohol and other drugs, followed by laboratory testing for positive readings from confirmatory field tests. There were 18 cases in which laboratory testing confirmed the presence of alcohol, and 11 cases where testing confirmed the presence of prohibited other drugs.
The data showed tests were conducted on 6 Sea World Helicopters personnel (4 helicopter pilots and 2 ground handlers) in September 2018 and September 2019. All tests were negative for alcohol (6 tests) and other drugs (2 tests).
Emergency response plan
The emergency response plan explained roles and responsibilities and provided guides for various emergency occurrences. Practice emergencies were conducted regularly with the VRTP emergency response team, the last scenario was conducted on 16 November 2022. The drills were well coordinated by VRTP and there was evidence of lessons learned being applied in operations.
On the day of the accident Sea World Helicopters initiated their response by calling VRTP and emergency services via a ‘000’ phone call. The conduct of the overall emergency response for which members of the public extended themselves as first responders before being joined by employees of VRTP, SWH, and emergency services, was out of scope of this investigation beyond information gathered for the purpose of survivability analysis.
Fatigue risk management
Flight crew rosters were designed to be compliant with the flight and duty time limitations described in CAO 48.1, and rostering evidence indicated that planned rosters were consistent with those limits.
Sea World Helicopters conducted its helicopter scenic flight operations in daytime hours only, and pilots were scheduled to work within the hours of around 0700 to 1830. The typical pattern for a line pilot roster was to work around 5 consecutive days, followed by 2 rest days. Considering the hours and timing of scheduled work, it was unlikely that rostering created a risk that pilots would be adversely affected by fatigue.
Flight crew were trained in issues of fatigue and fatigue management and completed an exam which was kept on their pilot file. All staff were required to review their fatigue through a series of questions when starting work each day. An adverse answer to any of the questions would trigger review by a senior staff member and if necessary, reassignment to tasks which did not carry risk associated with fatigue.
Records of these assessments were kept. On the day of the accident there was no record of assessment for the pilot of XKQ.
Related occurrences
Midair collision
The ATSB reviewed 25 investigation reports involving midair collisions and near collisions of 50 aircraft from Australia and overseas[66] (Table 19). Most of these events were fatal accidents, and the reports contained common findings and similarities around communication, visibility, conspicuity, and development of situation awareness.
Table 19: Midair collision and near collision investigations
| Agency | Investigation number | Occurrence title |
| JIAAC | 088/15 | Mid-air collision LQ-CGK / LQ-FJQ Villa Castelli, Province of La Rioja, 9 March 2015. |
| ATSB | AO-2007-065 | Mid-air collision Latrobe Valley Aerodrome, Victoria, 1 December 2007, Cessna 172 VH-EUI & Avid Flyer 28-0929 |
| ATSB | AO-2008-010 | Mid-air collision 53 km NNW of Gascoyne Junction, WA 13 February 2008 VH-OUS Piper Aircraft Corporation PA-18 Super Cub VH-ZDP Robinson Helicopter Company R44 Raven |
| ATSB | AO-2008-014 | Mid-air collision – 9 km NE Wee Waa, New South Wales – 26-Feb-08, VH‑CJK, Air Tractor, VH-ATB, Air Tractor |
| ATSB | AO-2008-059 | Mid-air collision 3 km NW of Moorabbin Airport, Vic 27 August 2008 VH‑UPY, Cessna Aircraft A150M and VH-CGT, Piper Aircraft PA-28-161 |
| ATSB | AO-2008-081 | Mid-air collision Cessna 152, VH-FMG and Liberty Aerospace Inc. XL-2, VH-XLY Casula, NSW, 18 December 2008 |
| ATSB | AO-2009-018 | Mid-air collision – 15 km SE Springvale Station, WA, 5 May 2009, VH-PHT, Robinson Helicopter Company R22 Beta II, VH-HCB, Robinson Helicopter Company R22 Beta II |
| ATSB | AO-2013-205 | Mid-air collision involving a Cessna 152, VH-TNV and a Jabiru J160, 19‑4430 Tyabb aerodrome, Victoria, 10 November 2013 |
| ATSB | AO-2015-023 | Collision after landing involving a Fletcher FU-24, VH-KXT and a Gippsland GA-200, VH-AGZ 13 km SW of Cootamundra, New South Wales, on 27 February 2015 |
| ATSB | AO-2015-036 | Collision on the ground involving a Piper PA-28, VH-TXH and a Cessna 172, VH-EUU, at Moorabbin Airport, Victoria, on 11 April 2015 |
| ATSB | AO-2020-012 | Mid-air collision involving Piper PA-44-180 Seminole, VH-JQF and Beech D95A Travel Air, VH-AEM, 8 km south of Mangalore Airport, Victoria on 19 February 2020 |
| ATSB | AO-2020-051 | Collision on runway between Extra EA-300 aeroplane, VH-EXR and Guimbal Cabri G2 helicopter, VH-LTO, Caloundra Airport, Queensland, on 18 September 2020 |
| ATSB | AO-2023-024 | Collision with terrain involving Magni M16C Tandem Trainer gyroplane, G1850, while avoiding Extra EA 300L, VH-IOG, Lake Macquarie Airport, New South Wales on 12 May 2023 |
| ATSB | AO-2023-025 | Near collision involving Piper PA-28-161, VH-ENL, and Bombardier DHC‑8‑315, VH-TQH, Mildura Airport, Victoria, on 6 June 2023 |
| ATSB | AO-2023-036 | Mid-air collision involving Jabiru J430, VH-EDJ, and Piper PA-25-235, VH‑SPA, Caboolture Airfield, Queensland, on 28 July 2023 |
| ATSB | AO-2023-057 | Mid-air collision involving SIAI Marchetti S-211s, VH-DZJ and VH-DQJ, 25 km west of Tyabb Airport, Victoria, on 19 November 2023 |
| TSB | A08A0147 | Mid-air collision Provincial Airlines Limited De Havilland DHC-6-300 Twin Otter, C-FWLG and Air Labrador De Havilland DHC-6-300 Twin Otter, C‑FGON, Natuashish, Newfoundland and Labrador 03 November 2008 |
| TSB | A07A0118 | In-flight collision between two helicopters. Newfoundland Helicopters Ltd Bell 206L LongRanger, C-GCHA and Universal Helicopters Newfoundland Ltd. Eurocopter AS 350 BA AStar, C-FHHH, Postville, Newfoundland and Labrador 03 October 2007 |
| TAIC | AO-2023-001 | Airbus Helicopters AS350B2 (ZK-IDB) and EC130B4 (ZK-IUP), Reported close air proximity Queenstown Aerodrome 27 December 2022 |
| AAIB | EW/C2017/11/02 | Cessna 152 G-WACG and Guimbal Cabri G2 G-JAMM ,17 November 2017 |
| AAIB | EW/C2017/09/05 | North American P-51D, Mustang, G-SHWN and North American P-51D-20 (Modified), Mustang, G-BIXL, 23 September 2017 |
| NTSB | LAX07MA231 | Midair Collision of Electronic News Gathering Helicopters KTVK-TV, Eurocopter AS350B2, N613TV, and U.S. Helicopters, Inc., Eurocopter AS350B2, N215TV Phoenix, Arizona July 27, 2007 |
| NTSB | ERA09MA447 | Midair Collision Over Hudson River Piper PA‐32R‐300, N71MC and Eurocopter AS350BA, N401LH Near Hoboken, New Jersey August 8, 2009 |
| NTSB | CEN19MA141 | Midair Collision over George Inlet de Havilland DHC-2, N952DB, and de Havilland DHC-3, N959PA Ketchikan, Alaska May 13, 2019 |
| NTSB | ANC20LA074 | Midair collision De Havilland DHC-2 N4982U; Piper PA 12 N2587M Soldotna, Alaska July 31, 2020 |
Almost all of these events took place in clear daytime conditions. In many cases the aircraft closing on each other had been obscured by aircraft structure (ATSB AO-2007-065, ATSB AO‑2008-010, JIAAC 088/15, TSB A08A0147, AAIB EW/C2017/11/02). TSB investigation A08A0147 found:
While they converged, the orientation of the two aircraft would have made it difficult for the PF [pilot flying] to see the other aircraft. Initially, LAL205 was above, to the right, and behind SPR961. LAL205’s approach was steeper and faster than SPR961, which created a blind spot under the belly of LAL205.
In other events, even unobscured traffic was difficult to see because of the limitations of the human eye and the relative size and closing speed of aircraft (NTSB investigation ERA09MA447, ATSB AO-2009-018, ATSB AO-2023-024). AAIB investigation EW/C2017/11/02 found:
The limitations of radar data are such that it was not possible to determine whether the pilots in G-WACG carried out any additional manoeuvring. Even if they did bring the helicopter into their field of view the chance of seeing it would have been limited; the conspicuity of a small helicopter against an unreflective background such as open fields and trees, is very low. The main rotor blades were of a uniform grey colour with yellow tips and would have been very difficult for the pilots of G-WACG to see against the land surface.
ATSB report AO-2023-024 stated:
The Extra pilot did not sight the gyroplane before entering the runway. The gyroplane pilots also did not sight the Extra at the start of their seventh and final wheel balance exercise, or while accelerating on the runway until a collision was imminent. While the reasons for this could not be determined, there were likely many common factors that reduced the ability of the pilots to identify each other such as the small angular size of each aircraft, the complex and cluttered background with reduced contrast difference, and the minimal relative movement between each aircraft.
The difficulty pilots face in detecting other aircraft in normal operation makes communication of vital importance. The TSB (AO7A0118) identified that uncontrolled aerodromes pose additional risks for users and that pilots should communicate even though it is not always mandatory to do so. A lack of communication is a feature in a number of fatal accidents (ATSB AO-2023-036, TSB A08A0147, TSB A07A0118). TSB report A07A0118 describes such gaps in communication:
No broadcast was heard stating the Bell 206L pilot’s intention to take off from the fuel-staging area. Had the Astar pilot known the Bell 206L was intending to take off, he could have possibly taken action in time to avoid a collision….
Although the Astar pilot made two position reports, it is probable that these broadcasts were not heard by the Bell 206L pilot. It is possible that the Bell 206L pilot had not yet donned his headset and/or that he had not yet powered the radios at the time the Astar pilot made his reports. The Astar pilot did not broadcast his aircraft’s position closer in on final approach or on short final to the fuel-staging area. Despite the fact that the Astar pilot saw the Bell 206L rotors turning and because the Bell 206L pilot had not broadcast his intentions to take off, the Astar pilot assumed he was not ready to do so or that he was shutting down. Also, the fact that the Bell 206L pilot had not responded to the Astar pilot’s position report when he was three nautical miles inbound would have indicated to the Astar pilot that the Bell 206L would not be a conflict.
In some accidents, correct and timely information that could have improved outcomes and aided in avoiding a collision, was not passed on (ATSB 2008-059, NTSB investigation ERA09MA447, ATSB AO-2020-012). These investigations show that traffic information is an important support for a pilot to sight other traffic or position their aircraft away from risk of conflict. NTSB investigation ERA09MA447 found that:
The Teterboro Airport local controller did not provide continual traffic advisories to the airplane pilot, as required; such advisories would have heightened the pilot’s awareness of traffic over the Hudson River.
ATSB report AO-2008-059 found that:
The aerodrome controller - west had been operating in a high workload environment in the period leading up to the midair collision. That increased the risk of traffic information not being able to be provided to flight crews.
The aerodrome controller - west did not provide the pilots of VH-CGT and VH-UPY with relevant traffic information about each other in sufficient time to assist self-separation.
The combination of difficulty seeing other aircraft with an absence of relevant information, leads many investigations to determine that pilots were operating with incorrect or incomplete mental models of their surrounding airspace (ATSB AO-2020-051, TSB A08A0147, NTSB CEN19MA141, NTSB ERA09MA447, ATSB AO-2007-065, ATSB AO-2008-010, ATSB AO-2008-081, ATSB AO‑2020-012, ATSB AO-2023-025, ATSB AO-2020-051, ATSB AO-2023-057, TAIC AO‑2023‑001).
ATSB report AO-2008-010:
The R44 pilot did not recognise the collision risk until there was insufficient time to prevent contact with the Super Cub.
TAIC report AO-2023-001:
The pilot of IDB did not positively identify the location of IUP before they commenced their departure and assumed that IUP had already departed.
ATSB AO-2023-025:
Both aircraft crews had incorrect mental models of local traffic at Mildura and neither crew spoke directly to the other to ascertain position and intentions before take-off.
Additional impediments to building accurate situation awareness exist in the operating environment. Pilots who have tasks onboard their aircraft other than safe conduct of flight are susceptible (NTSB AAR0902). NTSB investigation CEN19MA141 highlights the potential contribution of ancillary tasks to diminished situation awareness:
It is difficult to determine the extent that the channel 3 and 15 pilots’ reporting duties contributed to the breakdown in each pilot’s awareness of the other helicopter. The additional tasks of directly observing activities on the ground and providing narration could have affected the pilots’ ability to maintain their helicopter’s position or track the other helicopter’s positions. From about 1245:43 (channel 3) and about 1246:03 (channel 15) to the time of the collision, the pilots were continuously reporting the events as they unfolded, which narrowed the pilots’ attention to the ground and away from other tasks, such as maintaining the helicopters’ stated position and altitude and scanning the area for potential collision hazards.
Additionally, airspace and airport infrastructure can also make development of correct situation awareness difficult for pilots (TAIC AO-2023-001, ATSB AO-2023-025, NTSB ERA09MA447). TAIC investigation AO-2023-001 reported:
Complex and restrictive operating environments can impact a pilot’s ability to build an accurate mental model.
ATSB report AO-2023-025 found:
Due to topography and buildings at Mildura Airport, aircraft are not directly visible to each other on the threshold of runway 09, 27 and 36. The lack of a requirement for mandatory rolling calls increased the risk of aircraft not being aware of each other immediately prior to take-off.
A significant amount of ambiguity was recorded as being introduced through limitations in procedures for the areas of conflict. Investigations found a lack of procedures and guidance, and procedures without sufficient specification to support separation left gaps in support for pilots to develop accurate understanding of nearby traffic (JIACC 088/15, TSB AO8A0147, NTSB LAX07MA231, NTSB ERA09MA447, ATSB AO-2008-059, ATSB AO-2020-012). TSB report A08A0147 found that:
Neither company had formal policies, procedures, or training in place related to visual flight rules (VFR) radio communication and circuit-joining procedures at uncontrolled airports. This resulted in increased risk of collision due to flight crew uncertainty regarding ATF [aerodrome traffic frequency] procedures.
ATSB report AO-2008-010 found:
There were no formalised operating procedures detailing the conduct of multiple aircraft culling operations, including the assurance of aircraft separation, that would have assisted the pilots to maintain separation from each other.
Another common feature of these investigations was an absence of ancillary tools to support the pilots in identifying potential conflicts. Physical conspicuity devices such as strobes and high‑visibility main rotor blade paint schemes were discussed (NTSB LAX07MA231, AAIB EW/C2017/11/02), as were traffic displays and ADS-B (AAIB EW/C2017/09/05). The NTSB stated in their report:
A high-visibility paint scheme on the helicopters’ main rotor blades or high-visibility anticollision lights could have facilitated the detection of the impending collision risk.
NTSB investigation CEN19MA141:
Aural and visual alerts that draw the pilots’ attention to conflicting traffic presented on the cockpit display of traffic information can greatly increase the pilots’ awareness of potentially conflicting traffic and avoid a collision.
AAIB report EW/C2017/11/02:
As the separation between the two aircraft gradually reduced over several minutes, the use of compatible EC [electronic conspicuity] devices could have improved situational awareness such that avoiding action could be taken.
ATSB report AO-2020-012:
The student was using an EFB with the potential to provide enhanced traffic situational awareness, however due to the tablet not being equipped with an ADSB receiving device and data coverage limitations at Mangalore, it is unlikely that JQF ever appeared as traffic on the display.
Safety action undertaken by involved parties and detailed in the investigation reports took various forms. Most of the safety action was to introduce administrative controls. Administrative controls are known to have low levels of protection and reliability. These included:
- reminding pilots to look out
- mandating more frequent radio calls where collision risk exists
- mandating rolling calls
- implementation of 200 m separation minima
- introduction of job safety assessments prior to flight.
More substantial safety action was achieved in several cases. These actions were more robust and included:
- furnishing aircraft with visual conspicuity devices
- furnishing aircraft with electronic conspicuity devices
- establishment of dedicated radio frequencies
- change in airspace classification to provide better services
- relocation of facilities to minimise risk of conflict.
Seatbelt fitment
The ATSB reviewed numerous investigations from Australia, Canada and the United States involving injury due to incorrect seatbelt fitment or lack of restraint (Table 20).
Table 20: Investigations involving incorrect fitment or lack of restraints
| Agency | Investigation number | Occurrence title |
| ATSB | AO-2017-005 | Collision with terrain following an engine power loss involving Cessna 172M, VH‑WTQ, 12 NM (22 km) north-west of Agnes Water, Queensland, on 10 January 2017 |
| ATSB | AO-2018-031 | Collision with terrain, Garlick Helicopters UH-1H, VH-HUE, 24 km south-east of Talbingo, New South Wales, on 17 April 2018 |
| ATSB | AO-2018-057 | Collision with terrain involving BK117 helicopter, VH-JWB, near Ulladulla, New South Wales, on 17 August 2018 |
| ATSB | AO-2020-040 | Wirestrike and collision with terrain involving Robinson R44, VH-HNF, 69 km south‑east of Hay Airport (Steam Plains), New South Wales, on 31 July 2020 |
| ATSB | AO-2022-027 | Wirestrike and collision with terrain, involving Cessna 172, VH-REU, Coonabarabran Aerodrome, New South Wales, on 18 April 2022 |
| TSB | A01Q0166 | Loss of control and collision with water of de Havilland DHC-2 Mk 1, C-GPUO in Mollet Lake, Quebec, 8 October 2001 |
| TSB | A01W0261 | Controlled flight into terrain of Piper PA-31-350 Navajo Chieftain C-GIPB, at Fort Liard, Northwest Territories, 15 October 2001 |
| TSB | A08A0095 | Engine Failure and Collision with Terrain of de Havilland DHC-2 MK 1 (Beaver) C‑FPQC, 70 nm E of Schefferville, Quebec, 14 July 2008 |
| TSB | A11C0102 | Runway Overrun of Cessna 208B, C-FMCB, at Pukatawagan, Manitoba, 4 July 2011 |
| NTSB | WPR16FA055 | Loss of engine power (total) of Airbus EC130T2, N11VQ near Hanalei, Hawaii January 17, 2016 |
| NTSB | SEA05MA199 | Loss of control due adverse weather of Eurocopter AS350, N355NT, Haena Hawaii, 23 Sept 2005 |
Many accidents involved intentional or unintentional non-use of shoulder harness straps on multipoint restraints, often with demonstrated increased injuries compared to other occupants in the aircraft.
ATSB report AO-2018-031:
The pilot’s seat was fitted with a 4-point lap-belt and shoulder harness on an inertia reel, and the pilot was wearing a helmet. However, the shoulder harness (upper torso restraint (UTR) was not worn. The pilot stated that, due to the nature of the long-line operations, it was not possible to use the shoulder harness and lean left into the door bubble-window to view the long-line and maintain the helicopter position for load hook-up and unhook operations. The left side of the instrument panel and sunshade were damaged, consistent with being pushed forward from within the cabin. During the impact sequence, the pilot sustained serious injuries, including a fractured right eye socket and nose.
ATSB report AO-2022-027:
The pilot was wearing only the lap portion of the seatbelt during the accident flight, and not the sash-type upper torso restraint that was also fitted increasing the likelihood of serious injury in a collision.
TSB report A01Q0166:
Only the pilot and front passenger seats were fitted with shoulder harnesses, but the occupants of these seats were not wearing them. The pilot's and front passenger's heads struck the instrument panel. Their deaths resulted from cranial trauma and drowning.
The investigation found that the chances of surviving the impact would have been improved if the front seat occupants had been wearing their shoulder harnesses as prescribed by aviation regulations.
TSB report A01W0261:
The pilot and the passenger seated in the right cockpit seat were not wearing available shoulder harnesses. The pilot sustained severe head injuries and the passenger sustained fatal head injuries due to impact forces. These injuries may have been prevented or reduced in severity had the upper torsos of these occupants been restrained by the shoulder harnesses.
TSB report A08A0095:
The aircraft was equipped with both lap straps and shoulder harnesses. The pilot was wearing only the available lap strap because he was not in the habit of using the shoulder harness. The pilot suffered serious head injuries.
TSB report A11C0102:
The front left seat passenger, seated directly behind the pilot and the bulkhead separating the cabin from the cockpit , was wearing a seatbelt, but was not wearing the available shoulder harness. That passenger was severely injured to the head due to the impact and subsequently died of smoke inhalation.
Accident investigations have also shown that occupants restrained by shoulder harnesses are less likely to sustain serious injuries than those without.
ATSB report AO-2017-005:
In this accident, both rear-seat passengers suffered significant neck injuries, and the passenger on the left also received a significant cardiovascular injury and the passenger on the right received a significant head injury. Even though the rear bench seat had separated from the floor structure in overload during the impact sequence, UTRs [upper torso restraints], if fitted and worn, would still have provided some restraint to the passengers’ upper bodies. It is also noteworthy that the two front seats had also separated from the floor in overload, and the front-seat occupants, who were both wearing UTRs, had less serious injuries than the rear-seat passengers.
The aircraft was not fitted with upper torso restraints for the rear passenger seats, which very likely increased the severity of the injuries sustained by the two rear-seat passengers.
Additionally, incorrect positioning of occupants in seats due to poor safety harness positioning has been shown to contribute to injuries.
NTSB WPR16FA055:
Onboard video imagery recorded during the accident flight confirmed that the pilot's harness lap belt was positioned properly, low and tight across his hips. Of the six passengers onboard, four passengers' lap belt positioning were visible in recorded cabin imagery, and depicted that the lap belts were not tight across their hips and that the buckle was at or above their waists. … The loose and out-of-position seatbelts most likely allowed the passengers' bodies to shift out of position on the seat before and during the hard landing and did not restrain the occupants in the proper position for the seat to absorb the vertical landing loads for which it was designed.
Finally, seatbelts (and headsets) have been found to interfere with the donning of pouch‑style lifejackets.
NTSB SEA05MA199:
The passenger who was seated in the right rear seat stated that, after the helicopter rolled, the right side of the cabin was engulfed in water within about 3 seconds. He stated that he remembered the pre takeoff safety briefing and took off his headset and donned his PFD [personal floatation device] vest; however, he noted that the vest interfered with his ability to find and unlatch his seat belt and that it took him “precious seconds” to open the waist pouch to remove and don the vest.
Safety analysis
Introduction
The concurrent 5-minute scenic flights flown in EC130 B4 VH‑XKQ (XKQ) and EC130 B4 VH‑XH9 (XH9) on 2 January 2023 were conducted from the grounds of the Sea World Theme Park on the Gold Coast in Queensland, Australia. The scenic flights were part of a series flown simultaneously from the Sea World Helicopters heliport and the park pad inside the theme park. In bright clear conditions, the helicopters collided midair.
Following the collision, XKQ was severely damaged and broke apart, leading to a collision with terrain. Of 7 people on board, 4 were fatally injured and 3 were seriously injured. XKQ was destroyed. XH9 was substantially damaged, and the pilot made a controlled landing. Of 6 people on board 3 were seriously injured and 3 had minor injuries.
This analysis will describe the development of the collision initially from the perspectives of each helicopter pilot. It will explain how both pilots formed an incorrect understanding of the other’s position and intentions in the minutes before the collision.
Sea World Helicopters made changes to its operation which it intended to be positive in terms of customer experience and safety. The main heliport was developed and opened in August 2019, the park pad was refurbished and opened in March 2022, and in December 2022 the operator implemented 2 EC130 B4 helicopters as primary scenic flight helicopters.
The accident occurred one week after the operator started using 2 EC130 B4 helicopters for concurrent scenic flights from the 2 nearby helipads. Evidence collected in the investigation showed there were unintended consequences of the changes, which came about through limited use of safety management processes, which could have otherwise uncovered limitations in the operator’s risk controls.
The analysis will also examine the limitations in the systems that supported the operator’s approach to management of separation between aircraft, and the organisational approach to management of aviation safety risk.
The analysis will describe how gaps in knowledge regarding integration of safety equipment led to incorrect use of passenger restraints. Passenger safety was shown to be compromised not only in this event, but in scenic flights around the world.
This accident involved a combination of safety factors that either contributed to the accident, or increased aviation safety risk. The safety factors are discussed under the following:
- Occurrence overview
- Team shared mental model and awareness
- VH-XKQ departure from park pad
- VH-XH9 approach to the heliport
- Collision risk and risk controls
- Organisational approach to separation
- Organisational approach to safety management
- Survivability
Occurrence overview
Midair collision
Tracking data showed that operator’s helicopters routinely passed through the same point in space on approach to the heliport, and on departure from the park pad at Sea World. The helipads were 220 m apart and the point in space was around 155 m west-north‑west of the Sea World Heliport at around 130 ft high. Sea World Helicopters was aware that a conflict point had been created through reopening the park pad and that simultaneous operations from the park pad and the main heliport would require helicopters to converge on that point.
The operator’s main business of high frequency low duration flights meant that helicopters would be passing through that space frequently. In the 2 weeks prior to the accident, it was traversed over 200 times. Requiring the helicopters to converge on and pass through the same point in space created the conditions for a midair collision, and the frequency of operation increased exposure to that hazard.
The operator considered that this was not an unusual hazard given aircraft commonly pass through intersections at uncontrolled aerodromes. They did not identify a need to implement specific controls, and they relied upon alerted see-and-avoid. The alerts were designed to be broadcasts on the common traffic advisory frequency, and advice provided to departing pilots from ground crew. Alerted see-and-avoid, though a well-established defence against midair collision in uncontrolled airspace, is known to be fallible (CASA, 2021).
On the day of the accident, the operator’s controls which made up its system of alerted see‑and‑avoid broke down, and XKQ and XH9 collided at the established conflict point while conducting simultaneous operations from the park pad and main heliport.
|
Contributing factor VH‑XH9 and VH‑XKQ collided at an intersection created by simultaneous operation of the park pad and main heliport. Separation at the intersection relied solely upon alerted see-and-avoid. |
Landing of VH-XH9
The pilot of XH9 reported that their first indication of a collision was the main rotor blades of XKQ passing through the windscreen of XH9. This was a sudden destructive event. The pilot and passengers were peppered with penetrating shrapnel from the windows and window frames. The pilot was seriously injured and stated that their sunglasses were instrumental in protecting their eyes and maintaining an ability to fly.
Video of the event showed a short loss of control followed by an abrupt left turn around 1.5 s after the collision. The pilot reported continuing a left turn with the intention of descending and lining up on the long axis of the sandbar. The pilot also recalled that engine rpm began to decay, and all flight and engine instruments were lost. Additionally, the pilot noted a change in the sound signature of the main rotor blades, indicating damage. Later examination of XH9 showed that the blue main rotor blade of XH9 had a paint transfer and significant delamination, likely because of contact with one of XKQ’s main rotor blades.
The pilot continued the descending left turn through 270 degrees to land on the sandbar below them. The sandbar had featured in job hazard analysis for operations to and from the helipads and had long been planned for use in an emergency. The planned use of this site was instrumental in improving the outcome. Continued flight further than the sandbar may not have been possible.
From collision to landing took 28 seconds. During that time the pilot of XH9 assessed the flight controls through the turn and determined they were functional. The engine rpm started to recover, and the pilot made a controlled descent and landing on the sandbar. As soon as they had landed the pilot shut down the helicopter, checked their injured passengers, and went immediately to the aid of the occupants of XKQ.
|
Other finding Following the midair collision, the seriously injured pilot of VH‑XH9 landed the significantly damaged helicopter on a pre-selected forced landing site. Pre-planning and the pilot's positive control of the helicopter significantly reduced the consequences of the midair collision. |
Team shared mental model and awareness
The operation of the 2 scenic flight helicopters on the day was performed by a team of 2 pilots and 5 ground crew. This was a dynamic system which included:
- short notice changes to bookings and flights
- variability in passenger demographics
- nearby independent locations
- surface movement of vessels
- frequent movement of helicopters
- concurrent approaches and departures
- existence of a conflict point on approach and departure paths.
To manage the risk of midair collision and coordinate movements of the helicopters and passengers the team needed to have a shared understanding of the processes and procedures and a shared awareness of the current state of the system. Most importantly, with respect to the conflict point between the helipads, the pilots needed to know where the other helicopter was and what it was going to do.
Shared mental models are expected to affect team coordination by providing mutual expectations from which team members can know what their teammates are doing and predict future actions (Cannon-Bowers and others, 1993). Through situation awareness, a team has a better understanding of the current and future state of the system and is more likely to be successful (Endsley, 2015). This shared understanding is an essential component of how teams process information and perform (Salas & Fiore, 2004).
Communication is vital, and cooperative communication strategies are directly linked to positive outcomes for teams managing dynamic systems (Marks & Panzer, 2004; Roth et al., 2006). More effective teams have been demonstrated to engage in more communication and exchange of situation reports to develop situation awareness (Sorensen & Stanton, 2016).
This can be achieved through formal and informal communication and various technologies to provide relevant information and keep team members informed (Salas & Fiore, 2004). The mechanisms in use at the time of the accident were hand signals, ground crew look out prior to departure, radio calls, and see-and-avoid.
These mechanisms were examined in the context of the operator’s system and the need for pilots to form and maintain awareness of the position of company helicopters within that environment. This analysis will describe the breakdown of these procedural risk controls during the development of the accident. As a result of this breakdown, the pilots of XKQ and XH9 were unaware of each other’s position, intent and movement, leading up to the midair collision.
VH-XKQ departure from park pad
VH-XKQ radio problem
The ATSB analysed the Southport Airfield CTAF recording from 1–2 January 2023, alongside tracking data for XH9 and XKQ for the same period. The tracking data was used to determine the number of radio calls expected to be recorded at Southport for the flights made. It was not expected that any calls below around 250 ft would be recorded when broadcast from Sea World due to shielding by buildings.
Calls from XKQ were for the most part absent, and of 65 expected calls it was detected 17 times (26%) with an average readability of 2.5 (out of 5) for detected calls. Detected calls were noted to have a high frequency variation in volume.
The calls from XKQ had 4 calls of high (normal) readability on 1 January 2023 and the rest were broken and carried interference. All detected calls on 2 January 2023, except for a greeting to another pilot, averaged a readability of 1.
As the CTAF recording at Southport Airfield captured broadcasts from sport aircraft with 6 W radios at Heck Field 9 NM away, it could reasonably capture a radio of around 1 W from Porpoise Point.
The Com 1 radio from XKQ was bench tested and found to be slightly low on power at 9.5 W. This was lower than the original output, but still enough power to broadcast, and more than enough to be detected at Southport. The unit also displayed low modulation of 60% which would not have prevented broadcast, but slightly lowered strength and quality of transmission.
The Com 1 radio was connected to a Chelton 21-4B VHF whip antenna, mounted on the right side of the cabin roof. The antenna and installation hardware were inspected and found to have 3 significant faults:
- Corrosion at the helicopter’s mounting plate which could limit range and introduce noise into the system, reducing clarity of transmissions.
- Cracks in the solder joining from the BNC connecter to within the Chelton antenna itself, which could be unstable in an environment of vibration, and create intermittent operation.
- A stray wire in the helicopter’s coaxial cable BNC connector which could disrupt the signal path.
While it is certain that the Com 1 radio had defects, other pilots did not report any issue with receiving calls from XKQ and all stated that if they detected a problem, they would tell the pilot.
Low levels of expectancy can lead pilots to miss calls they didn’t necessarily expect to hear (Macdonald & Lavie, 2011). In a CTAF environment, calls are not addressed to specific aircraft, and there are no readback requirements. Unless there was a high expectancy of calls (Zhu et al., 2022), in the case of an intermittent fault, other pilots would likely not notice calls that were not transmitted.
Though there were other aircraft in the CTAF, they would not necessarily respond to calls from XKQ unless specifically asked to, or to arrange separation. Therefore, the pilot of XKQ would not necessarily expect a response to radio calls they made. The result of a successful transmission and a failed transmission can be the same, and the pilot would not know if a call they made was transmitted at low quality or subject to transmission failure.
However, if the CTAF at Southport detected a call it would ordinarily respond with a beep. It is not known how readily a pilot would notice no return. The faults described with XKQ’s radio system may not have been apparent to the pilot of XKQ, and there was no evidence that the pilot of XKQ suspected a radio failure.
|
Contributing factor The radio system used by pilots of VH‑XKQ for external communication had defects that limited transmission range and affected reliability of transmission. |
VH-XH9 inbound call
The pilot of XH9 followed Sea World Helicopters’ established convention, based on the procedure of making calls at designated VFR reporting points, and made an inbound call from Porpoise Point. The 8 second call was made 2 minutes 22 seconds prior to the collision, and it was recorded at Southport Aerodrome. The recording showed the call was clear, concise and correct.
The call was an alert to nearby traffic carrying the identity, position, height and intention of XH9 prior to tracking south along the Broadwater for the heliport. This was information the pilot of XKQ required to identify and manage the potential conflict for their future departure. The inbound call meant that XH9 would be somewhere between Porpoise Point and the heliport as XKQ departed.
If this information was received and retained by the pilot of XKQ it is almost certain that the pilot of XKQ would have sought to understand the location and intention of the pilot of XH9 prior to their departure to avoid conflict. As the position and intention of the pilot of XH9 was not factored into the departure of XKQ, it is likely that this information was either not received or not retained.
VH-XKQ radio ability to receive
At around 1145 on the day of the accident XKQ was flown into controlled airspace. Standard procedure would lead the pilot to listen to the automated terminal information service (ATIS), (found in the standby window of Com 1). It is almost certain that if Com 1 had a receipt problem the pilot would have used Com 2 for CTAF communications on exit from controlled airspace, and the CTAF frequency would have been found in both radios, which was not the case. Additionally, the pilot of XKQ had a short exchange with the pilot of a media helicopter on the CTAF around Porpoise Point. The pilot of XKQ responded to a greeting in kind, indicating they had received the transmission from the media helicopter.
Post-accident testing of radio equipment recovered from XKQ demonstrated Com 1 was tuned to the correct frequency and selected on the audio panel. Additionally, the antenna from Com 1 was tested on 2 different aviation band frequencies and found to receive without issue on both. Due to the issues with the antenna being intermittent, it was not possible to definitively rule out a technical element preventing receipt of the inbound call from XH9, however, there is no evidence to suggest this had happened previously and it is highly likely that Com 1 in XKQ was capable of receiving the call.
Activity on board VH-XKQ
While the operations manuals carried no specific written instructions for pilots accepting passengers, the operator stated that it expected pilots to be hosts aboard the helicopters. Pilots also reported instructing or assisting passengers in correct placement of restraints, hearing protection and microphones.
Videos and photographs showed that at the time the pilot of XH9 made the inbound call, passengers were being loaded into the front and rear seats of XKQ. The pilot of XKQ was shown in videos and photos to be wearing a headset and fulfilling the role of host and interacting with the passengers during the loading process. Additionally, at some point during that process, probably before the broadcast from XH9, the pilot engaged in conversation with ground crew at the door of the running helicopter, to conduct a weight and balance calculation for the passenger load on the flight.
The ATSB (2005) and the (UK) Civil Aviation Authority (2023) found that passenger interactions can distract pilots from duties and external events such as radio calls. The ATSB research advised pilots to ‘exercise discretion in engaging in conversation with other people on board the aircraft, particularly during pre-flight checks and critical phases of flight’.
The call was 1 minute 59 seconds prior to the departure of XKQ. A departing pilot who heard the inbound call would need to hold this information in memory while accepting passengers and completing their pre-flight procedures. This form of prospective memory task is known to be susceptible to error in the context of disruptions and routine tasks (Dismukes, 2008).
It is almost certain that the pilot of XKQ was not aware of the position and intent of XH9 when they departed. That means the pilot of XKQ had either not received, not heard or forgotten the inbound call. Given the inbound call carried significant information for the pilot of XKQ’s departure, it is less likely that the pilot of XKQ would forget the call once received.
While faults were discovered in the radio system in XKQ, there was evidence of the pilot receiving broadcasts on the CTAF, meaning it is unlikely that any radio system fault prevented receipt of the pilot of XH9’s inbound call. The most likely explanation for the pilot of XKQ being unaware of the position and intent of XH9 was that interactions with passengers and preparing for the flight interfered with the pilot’s ability to focus on the call.
The circumstances of this pre-flight sequence highlights limitations to the effectiveness of the inbound call as a reliable mechanism for supporting the situation awareness of departing helicopters for the position of company aircraft.
|
Contributing factor Due to the prioritisation of passenger loading and cabin preparation activities, it is unlikely that the pilot of VH‑XKQ focused on the inbound radio call made by the pilot of VH‑XH9. |
Ground crew pre-departure advice
The helipads were in a busy environment with traffic both on the waterway and in the air. Prior to departure, ground crew were required to communicate the status of the waterway and airspace behind the pilot, before leaving the pad so the helicopter could take off. Accordingly, on the day of the accident, after loading XKQ, one of the ground crew checked the security of the helicopter, checked the waterway and airspace behind the helicopter, found it to be clear and gave the pilot of XKQ the thumbs up. The ground crew immediately left the pad to attend to the next set of customers. The ground crew reported not seeing or hearing any other helicopters at that time.
It is highly likely that XH9 was not reasonably detectable by the ground crew. At the time the ground crew conducted their check, XH9 almost certainly presented a visual angle less than 0.4° (the size considered necessary of reasonable chance of detection) and was likely around 0.2° (the minimum level where detection is possible). Additionally, XH9 moved relatively slowly (around 0.4 deg/s) relative to the ground crew. This low apparent motion further reduced detectability.
However, from the time the ground crew departed to the time XKQ took off, XH9 had closed to a position behind XKQ of around 425 m. XH9 was now 3 times the previous visual angle with more apparent relative motion and was significantly more likely to be detected by an observer. (As discussed below, the pilot was not in an orientation on the pad at this time to see XH9).
The airspace information provided to the pilot of XKQ by ground crew was not relevant by the time XKQ took-off. If XH9 was detected by ground crew, and the pilot of XKQ had relevant traffic information, it is almost certain that their attention would have been drawn to XH9 and they would have waited to make visual contact with that helicopter prior to departure.
Adding the ground crew advice that the airspace was clear, to the distraction likely preventing focus on XH9’s inbound call, the pilot of XKQ was highly likely forming the impression that the airspace was clear for their departure.
|
Contributing factor The airspace information provided to the pilot of VH‑XKQ by ground crew was not relevant by the time VH‑XKQ took-off. As per the operator's procedures, after giving the thumbs up the ground crew member ceased monitoring the water and airspace behind the helicopter. |
VH-XKQ taxi call
The operator’s procedures stated that a taxi call was required before take-off. It was an alert to nearby traffic carrying the identity, location, and intended departure path of a helicopter. Seven pilots from Sea World Helicopters and a nearby operator, including the pilot of XH9, stated that they used a departing helicopter’s taxi call to identify potential conflict risk, and as a prompt to actively manage separation. This was a critical control for management of separation with other traffic.
The performance of these flights was frequent and repetitive, making the taxi call a habitual task. While it is uncommon, pilots can omit habitual tasks particularly when interrupted or if the normal cues to perform them are absent (Dismukes & Nowinski, 2007). There was no evidence that the pilot was interrupted or distracted prior to the departure. A passenger from XKQ recalled that after boarding and the pilot had settled the passengers in, the pilot told the passengers to talk amongst themselves. The pilot’s instruction indicates they took proactive steps to reduce the likelihood of distraction or interruption.
The pilot of XKQ was a highly experienced pilot and as Head of Flight Operations (HOFO), instructed company pilots in procedures, and conducted check and training of other company pilots. Company pilots all related that the pilot of XKQ impressed upon them the importance of the radio calls from the helipads. Tour videos of company pilots including 2 of the pilots of XKQ, showed the taxi call to be a consistent feature around 6 s to 10 s prior to departure.
A passenger’s video showed the pilot of XKQ for a few seconds prior to departure for the accident flight. Movement of the pilot’s cheek and jaw were consistent with the pilot speaking at a time consistent with the timing of taxi calls for previous flights, and the pilot was not interacting with passengers or ground crew at the time. While it is highly likely the pilot was talking it was not possible to determine which words were being formed.
There was however, a limited number of people the pilot could have been taking to. They were not communicating with ground crew because there was no UHF, and that was done through hand signals. They were unlikely to be talking with passengers as the pilot was not engaging them the way they were seen to do in tour videos, and the passengers had been told at some point to ‘talk amongst yourselves’. It is highly likely that the pilot of XKQ was intending to communicate with other helicopter traffic on the CTAF and at that time the procedurally correct call was a taxi call.
Three pilots for whom the taxi call would have been relevant reported that they did not hear the call. Components of the avionics system of one of those helicopters (XH9) were inspected and the pilot of XH9 provided an assessment of the general radio activity on the day that matched the CTAF recording, indicating that XH9 was transmitting and receiving radio calls normally on the day. The other 2 pilots reported talking to each other post-accident indicating an ability to transmit and receive.
It is almost certain that a radio call from XKQ was not successfully transmitted. The stray wire in the BNC housing of the Com 1 antenna on XKQ could cause the transmitted signal to leak into the aircraft structure rather than radiate outward from the antenna. Leakage would weaken the overall output and reduce the effective range, leading to potentially degraded or intermittent communication.
Combined with a cracked solder joint within the antenna base, and potential corrosion on the antenna mounting plate, transmission efficiency and stability would be further reduced. The cumulative effect would be to cause a significant reduction in the effective range and strength of transmitted signals, leading to intermittent or weaker communications with other aircraft.
Given the existence of radio system faults in XKQ, and the pilot’s proactive step to reduce distraction, it is likely that the pilot of XKQ made a taxi call that was subject to transmission failure.
It is almost certain that the pilot of XKQ was unaware of this failure, and almost certain that the pilot of XKQ would expect any conflicting traffic to respond to a taxi call to arrange separation. Making a taxi call and receiving no response would further strengthen the pilot of XKQ’s mental model of having clear airspace for departure. This also meant the pilot of XH9 had no trigger to attend to XKQ’s departure.
|
Contributing factor It is almost certain that a taxi call was not successfully broadcast from VH‑XKQ. It is likely that the pilot made a taxi call, and that it was subject to transmission failure. |
VH-XKQ blind spots and no visual contact with VH‑XH9
Parking position
On the day of the accident winds were forecast and measured from the south‑east and at the time of departure the windsock at the park pad displayed wind from the east. Therefore, prior to departure XKQ was parked with its nose facing south‑east to the corner of the helipad. XH9 would approach Sea World Helicopters’ heliport by tracking south along the Broadwater, the waterway to the west of the theme park, behind XKQ.
The operator had recently replaced its AS350 helicopters with EC130s. In an EC130 the pilot was seated front left as opposed to front right in an AS350.
Following review of the draft report, Sea World Helicopters provided statements from 2 of its pilots that stated that the visibility was better from the left of the EC130 than on the right of the AS350. Immediately after the accident, 2 different company pilots had stated the opposite.
The evidence showed that if the pilot had been on the right of the helicopter, they would be more likely to have seen XH9, and a video taken by a passenger seated on the right-hand side of XKQ showing XH9 on approach demonstrated this. From their position on the park pad, the pilot’s view of the Broadwater was demonstrably more restricted in an EC130 than it was in an AS350.
Limitations on manoeuvring
The operator’s procedures for departures from the park pad documented in its aircraft operations manual and in a job hazard analysis (JHA) restricted manoeuvring in the hover at the park pad to reduce the risk of an accident through tail rotor strike. Manoeuvring was also limited by surrounding structures and the pad’s position over water. The jellyfish house, and to a lesser extent the briefing room adjacent, were bluff objects and mechanical turbulence could affect stability of the helicopter (ICAO, 2021). Pilots familiar with operation at the park pad stated that additional manoeuvring on or around the park pad or over water was unadvisable, as it would create a separate set of risks including loss of control and ditching.
Departures to the south were more common due to prevailing winds in the area. Prior to and during southerly departures, pilots of EC130 helicopters operating at the park pad had limited visibility and limited opportunity to visually detect helicopters inbound for the main heliport from the Broadwater behind them.
The operator stated that training and checking activities encouraged pilots to look and ensure the area was clear on every departure. However, reconstruction of the event showed that pilots could not reliably clear the airspace from the left seat of an EC130 facing south‑east and departing to the south. Video and GPS data showed XKQ tracked from the park pad to the sandbar without deviation. Video analysis, mapping and tracking data, demonstrated that the profile flown on the day matched normal operations from the park pad. Taking off at the park pad and flying directly to the sandbar without a clearing turn appeared to be standard practice.
The ATSB’s adjoining Visibility Study showed that from the position and orientation of XKQ and the pilot’s eye position within it, XH9 was not realistically perceptible. XH9 was too far away and its visual angle was too small to be reliably detected during the earlier stage of its approach above the Broadwater. As it drew closer it was shielded by the cockpit structure of XKQ from the pilot’s eye position of XKQ.
The landing and approach lights of XH9 were not on during the accident flight. Had these lights been on, it is unlikely they would have provided a reliable mechanism for improving the detectability of XH9 (visibility of aircraft lighting is discussed further, below. See Design of ground crew checks).
The actual position and orientation of the pilot of XKQ’s eyes and head were not fully known, and any obstruction experienced by the pilot may have been different than that described from the pilot’s eye position. The CEO stated that pilots were trained to pause to look out and clear the airspace to their right on departures to the south prior to transition to forward flight. However, the operator’s tour videos showed the majority of departures being made without a pause but with a smooth transition to forward flight. The operator showed 2 scanning actions in its vision test video. The first was to rotate the head to the right and the second was to lean forward and look right.
It is unlikely that either of those techniques would have revealed XH9 during the lift-off and transition to forward flight, and just rotating the head would not have revealed XH9 for the duration of the flight at all. Leaning forward and looking right and up may have provided the pilot a 7 s window for detection in time to avoid a collision. To sight XH9 would still require the pilot of XKQ to look in the direction of XH9 at the correct time, and the pilot’s cap may have still obscured XH9.
While it was possible to sight XH9 for a short time, it was still unlikely the pilot would see it. The pilot was not alerted to the presence of XH9 and had no expectation it would be there. They did not have a particular threat to target and their scan was likely to be based on previous experience (Wickens & McCarley, 2008). If the pilot shared the assumption of other company pilots that traffic would be visible ahead or to the right of them, they would have no reason to extend the scope of their search to the actual location of XH9.
CASA (2021) stated that a full external scan of 180° wide and 30° high would take at least 54 s. A methodical scan ahead and to the right could reasonably take up to 27 s. However, a look out to the right and an instrument scan on departure, an assessment of the vessels on the waterway and a check for conflicting traffic at Sea World grass, would all reduce the time available for additional searching from the 24 seconds available in the accident flight, and the 7 s window where detection of XH9 was possible and necessary to avoid collision.
Resulting departure
Video showed the pilot of XKQ had 2 vessels on the water ahead of them, which they were required to avoid, and their departure began as the vessels crossed their path. Witnesses on board one of these vessels stated that the pilot looked at them as they passed. It is reasonable that the pilot’s attention would be directed at some point to the vessels as avoiding them was associated with a reduction in risk in the departure of XKQ.
Aside from the witnesses on the boat, it was not possible to determine exactly where the pilot of XKQ was looking prior to and throughout the departure. In a visual search, people are guided by priorities driven by salience of objects and goals of the searcher (Wolfe, 2021). As there was nothing to alert the pilot of XKQ to the presence of another helicopter, and with other concerns such as vessels on the water and a probable search for traffic at Sea World grass to attend to, the pilot would be less likely to allocate attention to searching the area where XH9 was. If the pilot of XKQ scanned for traffic and didn’t find any, that too could strengthen their assessment that the airspace was clear.
The restrictions on manoeuvring at the park pad meant pilots took off to the south without conducting a clearing turn, as the pilot of XKQ did on the accident flight. The ability of the pilot of XKQ to sight XH9 before lifting into the hover at the park pad was limited by their location, position in the helicopter and restrictions on manoeuvring.
The pilot of XKQ had not been alerted to the presence of XH9. As the 2 EC130s did not carry suitable UHF radios and the moving map electronic flight bags (EFB) displaying company traffic were not fitted, no other supplementary information was available to the pilot. For management of separation the pilot of XKQ now relied solely on unalerted see-and-avoid.
Their next communication was planned to be a departure call which was ordinarily made around 1 minute after departure. That call would not be made as the helicopters collided before that time.
|
Contributing factor The ability of the pilot of VH‑XKQ to visually identify VH‑XH9 northwest of their position over the Broadwater was limited due to restrictions on manoeuvring and visibility from the operationally required parking position facing southeast on the park pad. |
|
Contributing factor Having to rely solely on unalerted see-and-avoid for separation, the pilot of VH‑XKQ almost certainly did not sight VH‑XH9 or manoeuvre VH‑XKQ to do so. |
VH-XH9 approach to the heliport
Inbound radio call and assessment
The operator’s procedures required the pilot of XH9 to make an inbound call on the CTAF. The pilot of XH9 made that call at Porpoise Point at 1353:44, 2 minutes 22 s prior to the collision. The CTAF recording showed the call was clear concise and accurate. The pilot of XH9 did not receive a response to that broadcast, and this was normal; a response would only come if another pilot needed to arrange separation with them.
Around 1 minute 20 seconds later, the pilot of XH9 observed XKQ on the park pad and pointed it out to their passengers. The pilot of XH9 could see that XKQ was being prepared for flight and would depart soon. The regulations stated that a radio broadcast was required whenever it is reasonably necessary to avoid a collision or the risk of a collision.
The pilot of XH9 made an assessment that there was no risk of collision and had an expectation that XKQ would make a taxi call before departing and then pass behind XH9. The pilot of XH9 assessed that coordination with XKQ was not yet required and could be arranged, if necessary, when a taxi call from XKQ was heard. This presented no concerns to the pilot of XH9, who had previously experienced similar situations.
The pilot of XH9 stated that as they assessed that there was no risk of collision, they made no further radio calls, and no calls after the inbound call were recorded from XH9. The CTAF recording showed the pilot of XH9 demonstrated conformance to the operator’s standard calls. The lack of additional calls meant that the pilot of XKQ was not alerted to the presence of XH9 to enable alerted see-and-avoid.
|
Contributing factor Although the pilot of VH‑XH9 made a procedural call to announce their position when approximately 2 minutes from the heliport, they made no further radio calls. Consistent with the operator's procedures, upon sighting VH‑XKQ on the park pad, the pilot of VH‑XH9 assessed the risk of collision and did not consider it necessary to make an additional radio call to alert VH‑XKQ to their presence. |
Taxi call not heard
The pilot of XH9 reported not hearing a taxi call from XKQ and as discussed in VH‑XKQ taxi call, it was found likely that a taxi call was attempted and almost certainly not successfully broadcast. The taxi call was a critical control which would have alerted the pilot of XH9 to the requirement to manage separation. Company pilots including the pilot of XH9 related that hearing a taxi call from another company helicopter while on final approach to the heliport would prompt them to look for the other helicopter at the park pad. They would then make a call in response, either asking them to hold or relating their own position.
As the pilot’s assessment was that XKQ would pass behind, and as they knew both pilots intended to pass the sandbar, it is highly likely that the pilot of XH9 expected to hear a taxi call at a later stage of their approach. However, given there was no expectation of exactly when a call would be made, the absence of a call would not be considered an anomaly by the pilot of XH9.
The pilot of XH9 was already concentrating on the landing phase of flight and needed a reason to look at and identify XKQ. Without hearing a taxi call from XKQ the pilot of XH9 did not expect that XKQ would be airborne, and so did not engage in any specific search behaviour to detect XKQ.
|
Contributing factor As the pilot of VH‑XH9 did not hear a taxi call they had no trigger to reassess the status of VH‑XKQ as a collision risk. |
Conflicting traffic undetected
The pilot of XH9 recalled that after watching ground crew close the doors of XKQ, they concentrated on landing. Aside from the primary task of landing, the normal approach to the heliport over water had other considerations. XH9 was not equipped with emergency floats, and the pilot of XH9 was required to make a steep approach to the heliport to maintain access to the sandbar as a forced landing site. Also, on this approach, the pilot of XH9 modified their approach to avoid affecting a vessel on the water with downwash.
In a dynamic situation, it is not possible to pay attention to every aspect of the environment (Osvalder & Alm, 2018) and a pilot must choose where to focus. Setting up the helicopter for landing reduced the time and attention the pilot of XH9 had available to monitor or detect cues related to the status of XKQ. As people are more likely to turn their attention to things they expect (Wickens & McCarley, 2008), the expectancy that XKQ would not depart without a taxi call decreased the likelihood that the pilot of XH9 would notice XKQ’s departure without one.
Video taken on board XH9 on final approach showed that the pilot was focusing on the landing phase, managing their flight path to pass behind a vessel, and not searching for a departing aircraft. Other company pilots including the CEO of the operator agreed that this was appropriate behaviour at this stage of flight, and the pilot of XH9 was not expected to direct attention to the park pad without a warning to do so.
To be detected, any signal must stand out sufficiently from the background and a sensor needs to be sensitive to it (Lehto & Landry, 2013). In this case, XKQ would have to stand out sufficiently for the pilot of XH9 to detect it. The Visibility study showed that as XKQ took off it was unshielded up to 11 s prior to collision, before being partially shielded behind the left cockpit pillar of XH9. While shielded, XKQ was not visible from the pilot’s eye position.
The Visibility study identified that 4 s prior to collision XKQ was unshielded. The virtual reconstruction of the event produced a slightly different prediction and indicated that XKQ was unshielded a second or so earlier, between 5–6 s prior to the collision. As passenger video showed the pilot remained focused on the direction of travel, the implications of this difference are not significant.
With the pilot of XH9 looking ahead, the park pad and XKQ as it took off was in the pilot’s peripheral vision. From the XH9 pilot’s perspective, XKQ would not have drawn attention as there was little suggestion of motion. It was a dark helicopter on a background of overlapping colours and shapes, it was not equipped with high‑visibility blades, and the approach light, though on, was not visible from XH9’s position above XKQ. As such, though XKQ was not shielded for the pilot of XH9 as it departed from the park pad, it was unlikely the pilot of XH9 would detect XKQ.
Research on midair collisions has demonstrated that identifying a collision risk, reacting and manoeuvring takes on average 12.5 s (FAA, 2022). Close proximity events can be resolved more quickly by pilots as the collision course is more readily apparent. With an estimated pilot reaction and calculation time of between 1.5 s and 3.5 s and an input and aircraft response time of 2.5 s,[67] it could take around 4 s to 6 s to recognise the hazard, take avoiding action and then for the helicopter to actually change direction.
The sensitivity analysis demonstrated that during the periods in which XKQ was shielded by the left cockpit pillar, had the pilot leaned forward and moved their eye position forward by 100 to 200 mm, XKQ would no longer have been obstructed. In the circumstances of the accident flight, however, the pilot was not expecting to need to attend to XKQ unless prompted by the taxi call, and did not receive any prompt to direct their attention towards their left side until 2 seconds before the collision.
In air transport operations, passengers are not trained in cockpit communication and are not expected to form part of the defences against collisions.[68] A passenger on board XH9 had seen XKQ and recognised the risk. Seven seconds prior to collision the passenger attempted a verbal warning which did not work. With 2 seconds remaining the passenger escalated contact by tapping the pilot on the shoulder. It is likely that from the time of the passenger’s first verbal alert, the time required for interpretation of the message, added to recognition and initiating avoiding action, meant that successful avoiding action was already unlikely.
|
Contributing factor Inbound for the heliport, the pilot of VH‑XH9 concentrated on their primary task of landing, directing their attention to their landing site and a vessel on the water. Consequently, the pilot did not maintain an active scan, and the left door pillar blocked the view of the park pad and VH‑XKQ at times during their approach. As a result, the pilot of VH‑XH9 did not sight VH‑XKQ airborne before the collision. |
Collision risk and risk controls
The evidence presented above shows that prior to the collision, both pilots held an incorrect understanding of each other’s movements. The cues the pilot of XKQ received at each step built a picture of clear airspace, and the assessment of the pilot of XH9 would only be updated on receipt of a taxi call. The evidence also shows how the operator’s baseline controls were breached and how company procedures permitted a reactive approach to management of separation. When the critical control of a taxi call failed, see-and-avoid was an unsuitable defence and the helicopters collided.
The procedural risk controls relied upon by ground crew and pilots were not as reliable as the operator expected. This section will examine the risk controls in the context of the normal operations at Sea World Helicopters’ park pad and heliport.
Utility of inbound call from Porpoise Point
Tracking data, tour videos and CTAF recordings show that helicopters typically made the inbound call just over 2 minutes prior to arriving in the vicinity of the helipads, and recordings show the call took about 8–10 s. For pilots ready to depart from the park pad, hearing an inbound call of the arriving helicopter would present no threat to their departure.
However, helicopters that departed the park pad about 2 minutes after the inbound call would be at risk of conflict with the inbound helicopter. Of the 62 flights on 1–2 January 2023, 9 flights (14%) landed within a minute of another taking off, it is highly likely that those inbound helicopters were making calls as the outbound helicopter prepared for flight.
For pilots whose departure profile from the park pad may conflict with the arriving helicopter (to the heliport), they would need to focus on the inbound call during passenger loading, then hold that information in memory, and remember to coordinate with the arriving helicopter after completing their pre-flight procedures (Dismukes & Nowinski, 2007).
Figure 85: Timing of inbound call relative to loading activities of conflicting helicopters
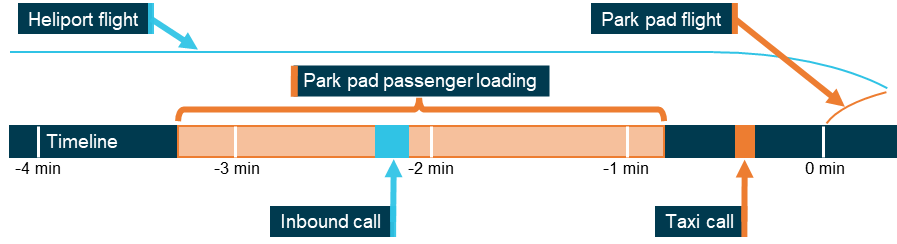
Source: ATSB
The operator’s scenic flights were booked with a 5-minute slot on the ground for loading and unloading passengers, this was consistent with ground crew recollections and tracking data showed this was ordinarily met with some variance of 1–2 minutes.
Sea World Helicopters’ pilots reported varied practices and mixed views on the ability of pilots to interact with passengers and attend to radios at the same time. Pilots reported different processes from turning down radios and focusing on passengers to monitoring radios and maintaining minimal interaction with passengers.
There were formal requirements for the pilots to engage with passengers with respect to cabin safety and informal expectations that pilots would interact and facilitate the passengers’ guest experiences. Videos showed that once the ground crew had closed the helicopter doors, pilots would continue settling-in customers while preparing for flight. During this process, many customers created noise, voicing their excitement in anticipation of the flight.
It is accepted that divided attention and distraction increase the risk of unintentional lapses in attention and perception, particularly during pre-flight checks and critical phases of flight (ATSB, 2005). Speaking and interacting with passengers in a noisy environment requires a pilot’s attention (Nagardaj, 2021), and inattentional deafness can occur, meaning critical signals can be missed (Dehais and colleagues, 2013).
Additionally, prospective memory tasks are susceptible to error in the context of disruptions (Dismukes, 2008). If a pilot heard the inbound call, there was still a chance that the passenger loading process would interrupt their intention to incorporate the call into their departure plan.
The timing of the inbound call was such that pilots of flights with the highest risk of conflict were highly likely to be engaged in passenger loading activities at the time an inbound call was made. Pilots on the park pad were highly likely to be in an environment of distraction and interruption that could prevent a pilot from attending to or incorporating the call. If a pilot missed that call, they could depart into occupied airspace without a full picture of relevant traffic.
|
Contributing factor Sea World Helicopters’ standard inbound call from Porpoise Point was not a reliable alert for a pilot on the ground while boarding and interacting with passengers. Where collision risk on departure existed, a pilot on the ground would highly likely be focused on cabin preparation at the time of that inbound call. |
Design of ground crew checks
To assist pilots with the limitations of visibility of the waterways and airspace behind the helicopters prior to take-off, there was a procedure for ground crew to follow. A ground crew member was to visually check the helicopters were secure and check the area behind the helicopter was clear, before signalling the tour type and giving a thumbs up that all was well for departure.
The ground crew was then to exit the helipad. Tour videos showed the crew leaving the helipad to attend to other tasks between 20 s and 1 minute 30 s prior to departure, and ground crew stated that 30 s was normal. Additionally, structures at the park pad blocked ground crew view of airspace to the north once they had left the pad, meaning changes in the airspace would be obscured from later casual observation, further reducing the opportunity for relevant hazard information.
Ground crew learned these procedures from each other. One ground crew member reported staying to watch the waterway and airspace behind the helicopter up to the point of departure.
Pilots had 4 main obstacle considerations departing the helipads:
- tall-masted vessels entering the take-off slope profile
- smaller vessels at risk of downwash
- immediate airborne threats such as birds and remotely piloted aircraft
- airborne threats requiring coordination such as other aircraft.
The obstacle environment behind a helicopter could change a great deal in the time between a ground crew giving the thumbs up and the pilot departing. In 30 seconds, common waterway traffic, such as parasailers, could travel around 300 m and so be visible to the ground crew at the time of the check, and therefore be provided as information relevant for departure. As discussed in ground crew departure advice, a helicopter can travel around 1,200 m in the same period.
At 1,200 m or more, the visual angle spanned by an inbound EC130 or similar sized helicopter showing a profile of 2 m wide would be around 0.2 degrees or less, on the boundary of perceptible size (NTSB 1988), and below the threshold at which an observer could be reasonably expected to detect it.
Company procedures required the use of strobes (not fitted to XH9 and XKQ) and landing and approach lights. Regarding the properties of lights, strobes are intended to be seen. They have wide arcs of visibility combined with various flash patterns to stand out and draw attention. Due to the bright daylight conditions that are normal in the operating environment for these helicopters, for an observer to see the strobes the lights need to be 5 to 10 times brighter than the background luminance (Bullough, 2011).
Conversely, landing and approach lights are designed for seeing with. They are higher powered and have narrower beams. For example, XH9 was fitted with a landing light of 15,000 candela (cd) with a 40° beam and an approach light of 310,000 cd with a 15° beam (these lights were not used on the day of the accident). To be visible these lights would have to be pointed at an observer and be brighter than the background.
As they are designed to illuminate the approach profile and landing site, forward of and below the helicopter, these lights are angled downwards from the body of the aircraft. XH9’s landing and approach lights were angled down at 30° and 15° respectively. Given the angle and spread of the lights, for the lights of a helicopter at around 500 ft above ground level to be visible to an observer on the ground the aircraft would need to be pointed towards them and less than 1 km away.
Tracking data showed that as company helicopters tracked along the Broadwater towards the heliport, the approach and landing lights would be directed towards an observer a maximum of 1% of the time. The locations where these lights would have been detectable were no more than 1 km from the observer, at which point the aircraft is above the lower threshold for visual detection and approximately 30–40 s from the conflict point.
Due to their intensity, where directed at the observer, active landing and approach lights would likely have aided in visual acquisition of the target aircraft even against a bright background. The illusion of movement created by a system such as Pulselite could also aid observer detection. However, detection at these times was still dependent on the position and orientation of the aircraft matching the visual scan of the ground crew member at the right time. As ground crew normally stopped observing about 30 s before departure (and up to 1 m 20 s), the use of landing or approach lights would still not guarantee that a conflicting inbound helicopter would be observed.
The designed procedures when correctly enacted by ground crew could not reliably provide pilots with suitably accurate and timely information. As a result, the ground crew check may not identify an approaching helicopter, yet one could be present at the time of departure.
|
Contributing factor Sea World Helicopters’ procedure did not require ground crew to monitor the airspace up to the time of departing the helipad. As the presence of hazards behind the helicopter could change significantly within a short space of time, helicopters routinely departed without current hazard information from ground crew. |
Flight path design and change in configuration of helipads
The original configuration of the helipads (used by the previous owner) with 53 m between the park pad and the hangar pad gave inbound pilots a continuous view of movement at both helipads for the majority of their approach. This configuration increased the opportunity for pilots to detect a change in the status of a helicopter on the other helipad. A pilot approaching either pad from the north could keep the other pad in sight, without effort.
At that time, the car park pad was used only for a few weeks at the height of the season, or infrequent ad-hoc use by third parties. Documents demonstrated that the use of the car park pad for high season scenic flights required positioning of temporary fences and briefing facilities. The operation of a third helicopter from there included implementation of enhanced communication on an air‑to‑air VHF frequency to ensure that new helicopters could communicate with other company traffic to manage separation.
Following change of ownership, on 15 August 2019 the new heliport opened. On 7 October 2019 the hangar pad closed, closely followed by the closure of the park pad on 12 November 2019. For the 2‑year 4‑month period of operation from just the main heliport there was no conflict point with company traffic beyond the bounds of the heliport itself. At the heliport, inbound pilots had a clear view of the helipads on approach and any change in the status of helicopters or movement of ground crew was readily noticeable.
The limitations for outbound pilots were improved over previous operation with the park pad as procedures prevented simultaneous operations at the heliport. Additionally, the stands were large enough that the pilots could turn the helicopter over the pad to look out and clear the airspace they were departing into. These features reduced the risk of midair collision between company helicopters over the previous configuration of helipads, and the requirement for enhanced communications between pilots was reduced.
When the operator reopened the park pad, the simultaneous use of the park and heliport pads 220 m apart created an area of interaction between helicopters operating from the 2 separate locations. Flight path analysis showed that a helicopter departing the park pad and tracking south and a helicopter approaching the heliport via the Broadwater would pass through the same point in space when flown on the tracks intended by the operator (see Midair Collision).
Issues at the designed conflict point
From the park pad and heliport, approaches and departures with a southerly component had a hazardous conflict point. An EC130 pilot inbound to the heliport had a clear view of the park pad, prior to beginning a final approach. However, as they passed abeam the park pad it would transition into their peripheral vision as they directed their attention to the heliport. This, combined with the complex background and limited relative movement of the departing helicopter, would impact the ability of a pilot to identify any changes to the status of an aircraft operating from the park pad.
As the pilots of both helicopters converge on the conflict area, they are both in higher workload phases of flight.[69] The inbound pilot must concentrate on landing the helicopter and managing their descent to maintain gliding distance to the sandbar or helipad throughout. The outbound pilot must monitor power use and systems and be prepared to enact an emergency response. Both pilots at this stage must also manage the effect of their downwash on surface vessels, altering their track and timing as required. The time and attention required by these tasks reduces the amount of time and attention available for looking for conflicting traffic.
Additionally, in this configuration, as both helicopters have a southerly component of heading, only the pilot of the inbound helicopter is on the preferred side of the cabin for visually acquiring the other. The outbound pilot must acquire any conflicting traffic across the cabin, and passengers and aircraft structure present obstacles to visual detection.
Making visual detection more difficult again, the helicopters in this configuration are closing on each other laterally and vertically. Lateral displacement puts another aircraft out to one side where door frames may occlude view or it will be in the far periphery of vision. Vertical displacement can put the other aircraft above or below normal lines of sight and outside of the frame of the windscreen. This means that for both helicopters a view of the conflicting traffic is more likely to be obstructed by aircraft structure, and in the cases where it is not obstructed it will be approaching from the top or bottom of the pilots’ field of view where it is less likely to be detected (see Visibility study for further detail).
As well as visual detection being limited, electronic detection would also be limited. The airborne collision avoidance systems as configured onboard the operator’s EC130 helicopters were not active below 380 ft and 400 ft, and they would provide no alerts of conflicting traffic below that height.
Without the conflict point created by using the park pad concurrently with heliport operations, the collision could not have occurred. However, it is not uncommon for airspace to exist where aircraft cross paths. The operator proceeded on the assumption that this conflict point was equivalent to any other intersection at an airport, while this intersection demonstrates unique and difficult features. The features of this intersection were demonstrated to be too complex for the operator’s baseline controls.
|
Contributing factor Reopening the park pad in March 2022 created an increased risk of collision with traffic operating from the existing heliport. The conflict point was placed at a location where:
(Safety issue) |
Reactive model of separation
While the operator’s standard inbound call was broadcast on the CTAF for the benefit of all nearby aircraft, it was particularly pertinent to helicopters departing the park pad. Inbound calls captured on the CTAF recording were consistent in accuracy and conformance with the operator’s procedures. As enacted on the day of the accident, this call could be the departing pilot’s only warning of potentially conflicting traffic but could fail to alert an outbound pilot.
For a pilot on the ground, the inbound call would not be immediately significant. It would be broadcast at a time when there was no immediate collision risk, and a pilot would have additional opportunity to manage separation with the inbound helicopter.
The regulations and the procedures only required an inbound pilot to make additional radio calls after assessing the risk of conflict. This commonly applied system is suited to operations at uncontrolled aerodromes. However, within the operator’s location and operation, limitations in visibility for outbound pilots, absence of systems to support situation awareness, frequency of flights and the conflict point helicopters passed through, reasonably demanded more robust communication.
The procedures were such that the departing pilot was only alerted to the presence of an arriving helicopter in circumstances where the arriving pilot identified a conflict risk, or through a response to their taxi call. This reactive model of communication between the pilots placed a reliance on the taxi call of a departing pilot and did not provide redundancy for situations where the taxi call was not made, not transmitted, or not heard. A proactive system including an additional call to a pilot on the ground would be more likely to highlight a failure. Being more salient, direct communication is more likely to elicit a response in return than a general broadcast (Vidulich et al., 2010).
A proactive strategy of separation would require pilots to update each other’s awareness even if a pilot assessed no risk of collision. A pilot tracking south along the Broadwater had a view of both landing sites, and a clear picture of the current (but not future) status of both helicopters. In contrast, a pilot on the park pad had limited ability to identify potentially conflicting helicopters. As previously discussed, the ground crew check and available visibility were unreliable mechanisms for identifying nearby traffic, and other means of information gathering were not present. If an inbound pilot did not coordinate with the pilot on the ground, the departing pilot may not have critical information regarding the proximity of the helicopters.
Interviews with company pilots showed they had differing views on the use of proactive calls. They stated that during training and checking activities they were taught that an additional call before joining ‘final’ when passing behind another helicopter on the park pad should be made. Some pilots reported routinely making additional ‘short final’ calls passing the pad. Other pilots indicated that normal practice was to make an additional call only if there was an assessment of potential conflict with the departing aircraft. However, they concurred that it was acceptable that if a pilot assessed no risk, they would not make a call.
The operator’s documented procedures allowed a reactive model of separation of the kind that was used by the pilot of XH9 on the accident flight. At Sea World, each approach to a helipad was made with the helicopters transitioning from cruise to a final approach. Though CASA recommended that aircraft making a straight in approach or joining a circuit should broadcast their intentions, Sea World Helicopters did not require their pilots to do so. The decision to make those calls was left to the individual pilots.
People within an organisation can view risk in very different ways (Reiman, 2011). This means pilots may not make the same decisions as each other. This introduces variability into the system at a critical phase of operation. Interviews showed company pilots had differing views on the interpretation of activities on the park pad and what they meant for the future status of that helicopter. Company procedures did not carry any advice on that matter. Pilots noted for example, that a helicopter with the doors closed and rotors turning may be loaded for departure or waiting for customers, presenting very different meanings for the same observation.
Also, pilots can develop very different assessment of risk based on their understanding of downstream controls (Orasanu, 2010). If they believe that there will be later opportunities to manage seperation, such as an outbound helicopter’s taxi call or an assumption that traffic would be visible, they may soften an assessment of developing risk.
The taxi call by a departing pilot was a general broadcast on the CTAF for the benefit of all nearby aircraft. As such there was no requirement for pilots to acknowledge or respond to the call. Within this open-loop undirected communication model, a pilot who transmitted their position would commonly not receive any indication of whether their message was received or understood.
Because of this, a departing pilot would perceive no distinction between a failed broadcast or a successful broadcast without conflicting traffic. Additionally, an inbound pilot would hear no distinction between a failed broadcast and no broadcast, carrying the inference that the other helicopter was not yet departing. This would leave both pilots without reliable cues to update their shared situation awareness.
Although training and checking activities encouraged proactive communication, procedures did not require it, stating that pilots should broadcast when turning final ‘as needed’. The operator’s procedures supported a reactive model of separation that provided limited cues for pilots departing the park pad to identify the location of inbound helicopters. At the same time, being based on open-loop communication, it left both pilots without an ability to detect communication failure. While this is a commonly applied system at uncontrolled aerodromes, and aligned with regulations, limitations of the operator’s system and environment made it insufficient for their location.
|
Contributing factor Sea World Helicopters' documented procedures for communication between inbound and outbound helicopters were not specific to their usual operation and location, and permitted a reactive model of separation, increasing the likelihood that an outbound pilot would not form awareness of relevant traffic. While some company pilots made proactive calls during final approach, this was not a standard practice. |
Organisational approach to separation
Assumptions on conflict
Interviews showed that senior management and pilots of the operator were aware of the potential for midair collision at the helipads and in the cruise phase of flight. Upon purchase of the company, the CEO changed flight paths of the scenic flights from a figure 8 to a racetrack pattern to remove a crossing point and reduce the risk of midair collision. Though this was not managed through the operator’s safety management system, it demonstrated that when a risk was identified, the organisation could take steps to reduce the risk.
Conversely, the conflict point at the helipads was a known consequence of the operator’s changes to the helipads. The operator stated that the intersection at Sea World is like that found at any airport. The operator further stated that separation was managed through airmanship, communication over the CTAF, and the rules of the air. These are baseline elements that could be expected to be employed for a day visual flight rules aircraft in uncontrolled airspace, and the operator relied on these controls being sufficient, and did not consider exploration of additional controls or further examination of the utility of these controls to be necessary.
While it is correct that the Sea World helipads were uncontrolled aerodromes, the number of movements at the helipads was in excess of the movements at some controlled aerodromes. In December 2022 Tamworth, New South Wales, Hamilton Island, Queensland, and Avalon Airport, Victoria, all controlled aerodromes, had less traffic than the uncontrolled helipads at Sea World (Airservices Australia, 2023). Being controlled aerodromes, those locations had a higher standard of protection for separation of aircraft through provision of air traffic control facilities.
At controlled aerodromes use of intersecting runways is generally avoided, and where intersecting runways are in use, controllers may ask pilots if they are endorsed to conduct ‘land and hold short operations’, that is to land without crossing the runway intersection. Additionally, if parallel runways are in use the traffic is ordinarily routed away from the other runway for separation and departure and approach paths do not cross.
Uncontrolled aerodromes often have intersecting runways to provide into wind approaches and departures for a variety of wind conditions. Ordinarily aircraft using the aerodrome would use the most into wind runway and depart from the same runway threshold. Inbound aircraft would listen to CTAF traffic and join the traffic pattern to land on the runway in use. Using an intersecting runway carries significant risk as demonstrated by 2 near collisions at Mildura, Victoria (see ATSB investigations AO-2023-025 and AO-2023-050) and a fatal midair collision at Caboolture, Queensland (see ATSB investigation AO-2023-036).
Where aircraft crossed the centre line of another runway additional radio calls were recommended by CASA, and the operator’s procedures required them. However, these calls were not taught or used in the scenic flight operation at Sea World, meaning the claimed equivalence with runway intersections did not extend to management of the risk of collision at the conflict point.
The heliport and park pad configuration at Sea World had several limitations when contrasted with uncontrolled aerodromes with intersecting runways:
- helicopters were instructed to depart from 2 active locations
- departures were commonly made crosswind and approaches into wind
- inbound and outbound tracks were not separated
- helicopters inbound for the heliport had to cross the departure path of an active helipad
- there were no procedural calls announcing crossing an active approach or departure path.
Pilots did not have the option, as pilots at uncontrolled aerodromes do, of selecting the best departure or approach point, and joining a common traffic pattern to avoid conflict with other airspace users. The heliport and park pad at Sea World were not an equivalent to intersecting runways at an uncontrolled aerodrome. In assuming they were, the operator missed the opportunity to examine the utility of the baseline controls for their location.
Rules of the air and airmanship
The rules of the air are a basic set of rules in Part 91 of the Civil Aviation Safety Regulations that govern right of way for aircraft. Regulation 91.325 of the CASR Basic Rule states that pilots must maintain vigilance during flight to see and avoid other aircraft.
Vigilance, meaning keeping careful watch for possible danger, could be considered an element of airmanship. This was impressed on pilots in training and checking activities conducted by the CEO. The CEO stated they instructed pilots to look for traffic and advised that given the high frequency of short duration flights, that pilots should assume there would be conflicting helicopter traffic.
Once an aircraft has been detected, Regulation 91.330 of the CASR Right of way Rules states among other things that if there is a risk of collision between 2 aircraft an aircraft must give way to another that is landing and give way to traffic on their right when converging at a similar altitude. To support these rules, detection of other aircraft and assessment of collision risk are both required. It is almost certain that the pilots would never intentionally contravene these regulations. Company pilots related examples of those rules being followed as a matter of course.
Instead, in this event, both pilots had formed an incorrect understanding of the status of the other aircraft and subsequently the need to apply those rules at that time. The pilot of XKQ had likely received convincing cues that pointed to there being no traffic and the pilot of XH9 was concentrating on landing and expected to hear a taxi call if that traffic was departing. Additionally, both pilots were adjusting their timing or flight path to avoid affecting vessels on the water with downwash. The short 24 s duration of converging flight did not offer much opportunity to correct either pilot’s understanding of the position of the other helicopter.
Rules of the air while providing direction, do not offer protection without the support of a reliable form of alerted see-and-avoid. In the EC130 helicopters at the helipads, below 400 ft, radios and hand signals were the only alert tools available to the pilots. Analysis has shown that the alerts available to the pilots and the radio equipment provided was unreliable.
Common traffic advisory frequency (CTAF) calls
The operator used standard CTAF calls at their helipads (see Operator’s flight procedures, and Reactive model of separation). Given the high volume of iterations it is not reasonable to expect radio calls to be infallible, and the reactive model of separation the operator accepted did not allow for redundancy in communications.
For example, the call made at Porpoise Point was because it was a VFR reporting point and operator’s procedures required calls at VFR reporting points in the vicinity of high traffic areas. That call was for the benefit of all nearby aircraft. It has been demonstrated the Porpoise Point call was of limited use to pilots on the ground at the park pad and some company pilots were aware of that. While training and checking encouraged further arrangement of separation, procedures did not require it. The operator’s management of the hazard concentrated responsibility for separation at the individual level and assumed that the controls would be suitable for the location and volume of traffic. It also made no allowance for a failure in any of the elements of the system.
The operator expected pilots to coordinate, with the only channel available to them being the CTAF. While quiet on the day of the accident, pilots commented that the CTAF was often busy, and pilots were reminded not to engage in chatter on it.
Assumptions on visibility
The operator’s routes in and out of the park pad had been tested and nominated as the safest routes by the CEO and HOFO on 13 March 2022 and were later shown to all the pilots operating from the park pad. Tracking data for scenic flight operations followed the same flight path as training and checking activities, showing that pilots were flying the approaches and departures as instructed by the company.
Helicopters in general have excellent visibility from the cabin. It was reported to be common for pilots to visually acquire aircraft either aided by radio calls or lookout alone. To identify a potential conflict means knowing where conflicting traffic is likely to be, having an uninterrupted view of that location, having a conspicuous target, and looking in that direction at the right time.
The general assessment of company pilots of conflicting traffic while departing the park pad was that the traffic would be in front or to the right, and readily visible to a pilot. The reconstruction of the event showed that this assumption that pilots would readily sight conflicting traffic was not correct.
The recreation of the event clearly shows that the helicopters on those flight paths on the day of the accident were obscured by airframe for most of the time, preventing visual contact. For XH9’s approach, XKQ was obscured by aircraft structure for 15 s and visible but outside of the pilot’s central vision for around 5 s before collision. For XKQ the other helicopter was above and to the right, shielded by structure while the pilot was seated on the left.
Moving to look around airframe structure would have improved each pilot’s chance of sighting the other helicopter. However, they would still need to look in the correct location during the short window the target was visible. In a situation where each pilot is not expecting the other helicopter to be there, an untargeted search may not significantly improve detection.
Acceptance of risk as tolerable
The operator asserted that the new configuration of 220 m distance between helipads, being built on pre-existing helipads, was the same that had existed without incident for almost 40 years. However, that assertion was incorrect as that configuration was previously seldom used and the main configuration was 53 m separation. Additionally, controls of enhanced communication and moving map traffic display were available to support pilot situation awareness at that time. This meant that the previous years of successful operation were not wholly representative of the new layout of facilities, and the operator could not rely on historical performance to determine that the new facilities would be safe.
Without any signs of formal assessment or testing, the operator considered traffic to be visible, communications to be reliable, enhanced communication to be unnecessary, and moving map displays and conspicuity devices to be of limited use (see Withholding of supporting risk controls below).
The operator’s safety management system had tools and the operator’s staff had the capability to assess these controls in the context of their operation and support that assessment with the benefit of decades of experience and knowledge within the aviation sector. However, there was no evidence to suggest that the operator had conducted any formal analysis of controls, or potential for conflict in that location to assure the operator that risk was as low as reasonably practicable (see also Implementation of the park pad). Additionally, if the conflict point was to be considered an intersection, no additional controls relevant to intersections had been applied. The operator’s informal, experience-based approach found the risk of collision near the helipads in the EC130 helicopters to be tolerable and their arrangements for managing it effective.
|
Contributing factor Sea World Helicopters was aware of the hazard of midair collision and assumed that any conflicting traffic would always be visible to pilots. Furthermore, the operator did not deem the collision risk to be unusual and considered its existing baseline controls to be effective. |
Withholding of supporting risk controls
Original arrangements
Following the change of ownership, helipad positioning underwent 2 significant changes (see Simultaneous operation of helipads for departures to the south). Under the previous owners, the original layout had 2 helipads close to each other, separated by around 53 m. Downwash and salt spray creating low consequence high frequency events at that location, combined with the operation of 2 helicopters from one helipad from time to time, required a high degree of coordination. That coordination was mainly in the form of radio communication ‘chatter’ between pilots.
The pilots would monitor the CTAF and a dedicated ultra-high frequency (UHF) radio channel, making calls on the CTAF for separation with aircraft outside of their company and chatter on the UHF for internal coordination. This provided a mechanism for pilots to send and receive information about each other’s position, without creating unwanted traffic on the CTAF. The chatter frequency used was a UHF frequency provided by the theme park. In circumstances where the UHF radio was not available, pilots would maintain their ability to communicate by using an alternate VHF channel in addition to the CTAF.
Pilots flying at that location at the time were aware of the limitations of visibility for outbound pilots and reported that the separation of these helipads meant that pilots on approach had a clear view of any traffic that may be taking off. Enhanced communication through the chatter frequency meant that proactive separation was the norm.
Additionally, the AS350 helicopters were fitted with electronic flight bags which showed a moving map and location of up to 18 of the nearest OzRunways equipped aircraft. This provided Sea World Helicopters’ pilots a visual representation of the local operating environment, including the location of other company helicopters currently airborne. Pilots from that era reported that they had accessed these displays while preparing to depart, to form awareness of nearby aircraft.
First change in location
The redevelopment of the car park pad by Sea World Helicopters’ new owner brought a custom designed 4‑helipad heliport to that location. Shortly after that site was open the hangar pad was condemned and operations there ceased. For a 3-month period outside of peak season the heliport was operated with the park pad. Once the park pad was closed for later refurbishment, the operator was left with a single location, their new facility on the grounds of the old car park pad. Operating the helicopters solely at that facility brought several benefits:
- all approaching helicopters had a clear view of activity on helipads
- all departing helicopters had a clear view of the airspace
- reduced rate of downwash and salt spray issues
- no requirement for intersecting flight paths.
The high frequency low consequence events were all but eliminated. There was still downwash to consider, but salt spray and the coordination of 2 helicopters for one pad were no longer an issue. Visibility for outbound aircraft was improved as there was room to manoeuvre on the pads and there was no intersecting flight path between inbound and outbound aircraft, as procedures at the helipad prevented simultaneous departures and approaches. This all combined to reduce the reliance on chatter for management of operations.
The operator also instructed pilots and ground crew to use the UHF less. Training files showed that this was to provide sterile cockpit conditions for the pilots operating the scenic flights. Additionally, a company pilot advised that it was also to reduce chatter in front of customers who could also hear the UHF. The UHF system was from that time reportedly used only for arranging refuelling and resolving questions about duration and load for flight booking purposes.
A change in staff also occurred around that time. The original HOFO and the safety manager had departed the organisation. The outgoing staff had many years of experience and while this represented a loss of operational knowledge there was a handover between HOFOs. However, though records of past procedures were retained, the safety manager was not directly replaced, and it was reported that there was no handover of the safety system.
Reduction in flights
In addition to operating from one location, the number of flights dropped dramatically in March 2020 with the onset of the global COVID-19 pandemic. Due to theme park, state border and international border closures, Sea World Helicopters operated just one helicopter. As a result of this reduction in business and frequency of flights the requirement for management of separation between company helicopters was further diminished.
Second change in location and introduction of new EC130 B4 helicopters
On 12 March 2022, following planned refurbishment, the park pad reopened. This created the conflict point between inbound and outbound helicopters where the midair collision took place. The separation between the helipads was now 220 m, the attendant issues in this configuration are discussed in Flight path design and change in configuration of helipads above. Essentially, the arrangement was a more hazardous situation than the original configuration, but without the controls previously employed to manage separation between company helicopters.
The operator was initially using the AS350 D2 helicopters from both locations. From the park pad for southerly departures (into prevailing winds) the AS350 D2 offered the outbound pilot an unobstructed view of the Broadwater as they were sitting on the right of the cabin. The use of UHF was limited and the use of EFBs with traffic display continued alongside use for displaying manifests.
From 1 December 2022 to 2 January 2023 99.5% of departures were made to the south and 0.5% to the north. The introduction of the EC130 helicopters reduced the ability of the pilot at the park pad making a southerly departure to ensure the airspace to the right and above them was clear of traffic, as they were on the left of the cabin and passengers and aircraft structure blocked their view. Additionally, EFBs had not been installed. The operator did intend to replace them, and the iPads arrived in late December 2022, yet mounts were still to be sourced and installation to be carried out. In addition, XKQ and XH9 had no ability to communicate on the theme park UHF frequency.
In summary, following changes in location and helicopter, at the time of the accident:
- reliance on controls was diminished by reduction in number of locations and volume of traffic
- chatter on UHF was reduced as utility declined, and its purpose changed
- traffic displays were unavailable and their utility was not recognised
- pilots with understanding of the previous need for controls had left the company
- a higher risk helipad configuration was introduced.
Following a period of decline in need and usage of these controls, their importance was not recognised to the extent that the operator imported and registered the new EC130 helicopters to be used in peak season, before the EFBs and mounts were purchased and installed. Those helicopters did not go through a managed process of change (see Implementation of aircraft), and there was no evidence that the withholding of the controls was subject to any other change or risk management process. By not using the processes that existed within the operator’s safety management system, it is likely that the operator did not recognise that the controls for the low consequence high frequency events also provided protection against midair collision.
The operator stated that the choice of helicopters to use and whether to carry EFBs was at its pilot’s sole discretion. However, with respect to the use of the helicopters, available evidence of interviews with the approved maintenance organisation, senior management and pilots, all pointed to these helicopters being the helicopters the operator intended to use and promote for the peak tourism season. This was further supported by flight records and meeting minutes, and documentary and procedural changes for ground crew.
With respect to the carriage of EFBs, senior management stated that the absence of the iPads in the EC130s was not a significant difference, and they weren’t mandatory to carry. Additionally, meeting minutes of 30 December 2022 which mentioned the arrival of iPads for XH9 and XKQ and the sourcing of suitable mounts made no mention of alternative means of carriage for the interim. It is highly likely that the operator did not expect or require the pilots to carry them.
Impact on team situation awareness
The previously employed additional risk controls of enhanced communications over UHF and in‑cockpit traffic displays supported the team situation awareness of the pilots. The use of UHF allowed pilots to broadcast their position and intention more frequently and to elicit position and intention information from other pilots. Therefore, pilots had more cues to maintain team situation awareness. The proactive flow of information between pilots created a better understanding of where other company aircraft were, in contrast to the reactive CTAF model the operator later adopted.
In situations where unloading and loading passengers could distract pilots from attending to standard CTAF calls, the in-cockpit traffic display showing company traffic provided useful cues. As described in Use of electronic flight bags, research and regulatory guidance support the utility of traffic displays for supporting pilot situation awareness, including by directing pilots where to look for traffic. Pilots reported using the display to re-establish their understanding of where company traffic was in the scenic flight circuit prior to departure. It provided a useful back-up for the standard inbound CTAF call from Porpoise Point. If the call was missed the pilot could reacquire traffic in the Broadwater via the display.
The role of communication in facilitating shared situation awareness cannot be overstated. Communication is the mechanism by which actions can be coordinated, and by which misunderstandings can be identified and corrected (Parush et al., 2011).
A feature of the development of this accident was removal of these controls reducing a pilot’s ability to maintain a working awareness of where other helicopters were. Team situation awareness was diminished, and this contributed to an incorrect mental model on the part of both pilots on the day of the accident.
|
Contributing factor Following the change in ownership of Sea World Helicopters, changes to the operation gradually degraded existing controls of enhanced communication and in-cockpit traffic display that informed team situation awareness, and the controls were eventually withheld without formal analysis of the change. This reduced opportunity for company pilots to form and maintain awareness of each other's position and intentions. (Safety issue) |
Reliance on alerted see-and-avoid
The defences-in-depth approach to safety seeks to ensure that risks with potentially catastrophic outcomes are controlled by overlapping risk controls with some redundancy. The failure of any given control should not result in a catastrophic outcome. If a control is the only thing standing between safe operation and catastrophe, that is a critical control. Critical controls must be supported, and early warning of their failure should be available in the system.
The concurrent operation of the EC130s at Sea World Helicopters had several complexities that meant it was not always possible for individual pilots to reliably observe and maintain awareness of all other aircraft operating nearby. The safety system used to manage concurrent helicopter operations employed 3 primary risk controls:
- The system was reliant upon pilots making the procedural CTAF calls, and these calls always being transmitted as intended. The taxi call by a departing pilot was sometimes a critical control used by an arriving pilot to arrange separation. There was no redundancy or warning in situations where the taxi call was not broadcast as intended.
- The ground crew pre-departure check was intended to provide an additional confirmation for the departing pilot that the local airspace and waterway were clear. As identified, due to the timing of these checks, ground crew could indicate the airspace was clear when an aircraft was arriving.
- The reduced ability for pilots to detect conflicting traffic visually at the park pad was limited by limitations on manoeuvring at the park pad, and by the angles of convergence of the helicopters at the conflict point.
Believing its operational environment to be equivalent to an uncontrolled aerodrome, the operator considered that CTAF calls, communication between ground and air crew, and see‑and‑avoid were an effective method of managing separation. As discussed above, the limitations of these controls, that could lead to pilots operating without critical information and an incorrect picture of company traffic, had not been assessed.
Without formal assessment and based on the operator’s assumption, multiple controls that were available to assist EC130 pilots in maintaining separation were not deemed to be required or of value and as such were not implemented, and included:
- UHF radios were not programmed or fitted.
- Electronic flight bags were not in place for the first peak season of operation.
- TCAS was not operational at the conflict point and pilots were not familiar with its use.
- Visual conspicuity devices such as strobes and high‑visibility paint schemes were not fitted.
- A pulse light system fitted to both helicopters was not operational in one and not used in the other.
|
Contributing factor Sea World Helicopters was reliant on CTAF calls, ground crew advice, and pilot visual detection of aircraft to ensure separation in VH‑XH9 and VH‑XKQ. Available additional controls for enhancing alerted see-and-avoid and reducing the risk of collision were not implemented. (Safety issue) |
Organisational approach to safety management
Introduction
An operator’s safety management system (SMS) is a structured and formal means to identify hazards, manage risk and develop risk controls to protect an organisation and its customers. It differs from work health and safety (WHS) in that it directly addresses aviation safety risk. In fatal accidents related to WHS matters, 3.8% involved multiple fatalities (Pierce, 2016). ATSB data for the period 2014–2024 showed much worse outcomes in aviation where 30% of fatal accidents involved multiple fatalities. While WHS is important, aviation safety risk must be specifically and wholly addressed in an aviation operation’s SMS.
The carriage of passengers increases the consequence of exposure to a hazard and must be considered when determining the adequacy of the risk controls used to prevent accidents. Uncontrolled aviation safety risk can cause catastrophic events. The operator’s SMS contained the tools to identify and control aviation safety risk. This section examines why Sea World Helicopters’ SMS was not used for effective management of aviation safety risk and concentrated instead for the most part on ground handling and WHS.
Safety management
Interviews and records demonstrate that when the operator took over the business, the SMS was well supported by staff and was being used to manage aviation safety risk. The HOFO and safety manager remained with the new owners for around 9 months, during the development of the new heliport facility. Initially, the new owner had the tools and people to expand and improve the use of the SMS, but the opportunity was not realised. Eventually, all the staff employed under previous ownership had left, and the COVID‑19 pandemic slowed tourism operations. The use of the SMS almost came to a halt.
The inclusion of safety management matters in the scope of the external audits demonstrated that the theme park owner expected safety management to be an element of the helicopter operation. The SMS was rewritten in 2020, bringing it in line with the new safety management requirements contained in regulation 119.190 of the CASR and other ancillary regulations for the functioning of an SMS. Without a safety manager, responsibility for the management of the Sea World Helicopters SMS was transferred to another of the owner’s companies and remained under external control until May 2022.
Records showed that the SMS was rarely used during the period of offsite management. Although the other company also had tourism operations there was no evidence of sharing of safety information between the operations, and there were no hazards related to flight operations raised. Some job hazard analyses (JHA) were raised locally for offsite charters; these jobs did not represent the bulk of the operator’s activities.
Following the second‑party audits of the operator conducted on behalf of VRTP, in which no safety management support was available, there was a recommendation to reinstate an onsite safety manager. The operator did not believe a safety manager was necessary, stating that the operation was too small. They did however recruit an onsite safety manager.
Aviation safety risk was not effectively managed within the context of the operator’s primary business. The operator advised CASA that it would complete implementation of the SMS by December 2024. The SMS was not applied to aviation safety risk despite being in place since 2014 and rewritten to comply with the regulations in 2020. Additionally, internal audit findings associated with hazard/occurrence reporting and risk assessments, and no recorded senior manager attendance at staff safety meetings, suggests a lack of organisational commitment to the SMS.
The safety discussion in management meetings reviewed carried a lot of activity that was heavily focused on WHS and ground handling. This likely provided a sense of security that the safety system was productive, but there was comparatively less focus on the operator’s flight operations, leaving aviation safety risk unmanaged.
Safety objectives
While the new safety manager was experienced and they motivated the ground crew to be involved in the SMS, the policies, objectives and goals of the SMS were vague and impractical. For example, there was a policy to:
Minimize the risks associated with aircraft operations to a point that is as low as reasonably practicable/achievable.
The operator’s primary business was short duration flights, operated at high frequency from 2 nearby facilities. The risk inherent in this operation was known to the operator. Guidance prompts operators to be specific with objectives, to identify aspects of aviation safety risk and set about measuring and managing them. Instead, the objectives were a collection of intangible aspirations such as prevent harm and provide a safe environment.
The unsuitability of the objectives was raised at internal audit in 2022 and noted in guidance from CASA when the operator’s SMS was submitted. The operator was advised to develop specific objectives; however, the objectives were not updated. None of the information so far gathered in the SMS between 2014 and 2019, or the operational experience of staff since then was used to determine what the SMS should be focused on.
During interviews, company pilots at all levels related hazards specific to that operation, that were not captured in the SMS. As a result of not reporting these hazards they were unavailable to the SMS to manage out of the system or for development of safety objectives. Without that information the objectives of the SMS were unfocused. For example, all the operator’s pilots raised the issue of a busy CTAF impacting quality of communication. A relevant objective could be to collect data on congestion and communication over a certain period to inform an approach for management of company communications. Another could be an objective to analyse the impact of communication failure throughout various stages of flight and ensure risk controls or redundancy existed.
Without relevant input from the pilots and crew conducting the operations the value and focus of such activities to manage aviation safety risk cannot be determined, and untargeted activities can result. One such activity was conducted. The operator introduced a fatigue management self‑declaration form, though there was no evidence of any hazard reporting or an organisational objective to better manage fatigue risks. The rosters worked by the pilots at Sea World involved daytime work only, and it is unlikely that a process based on hazard reports would identify fatigue management as a priority in the context of other operational hazards.
Safety reporting
The operator had not systematically identified hazards related to its aviation operations at the theme park and therefore could not assess the risks in its operation. There were 2 incident reports and no hazard reports related to aviation safety risk from 7 December 2019 to 30 December 2022. When an audit noted a lack of engagement of the SMS, the operator stated that a well operated aviation organisation should not have any incident or hazard reports. This assumes unsafe conditions will not emerge and goes against the principles of safety management (CASA, 2022b).
Failure exists in all systems and the outcomes of failures are unpredictable (Perrow, 2011). With over 7,500 flights in 2022, it is reasonable to expect that given variability in conduct of operations, external influences, and changes over time, that failures or events requiring active management would arise in the normal course of operation and those hazards would be captured in the SMS. To avoid these hazards developing into disasters, organisations need to be motivated to remain vigilant and collect information on which to base decisions (Sheridan, 2008).
It is a challenge for operators for whom accidents are rare to remain cautious and apply the time and resources required to monitor aviation safety risk (Zimmermann et al., 2017). However, an organisation cannot design effective controls or ensure the reliability of existing ones without a clear understanding of changes and the continued suitability of existing processes (Leveson, 2004). This requires an organisation that is capable of learning about itself (Flin, 2017). That is to say, hazard and incident reporting is a fundamental cornerstone of maintaining safe aviation operations.
Hazard identification is intended to be a continuous activity. It is a critical part of the safety risk management process required to maintain an acceptable level of safety within aviation operations (CASA, 2022d). Hazard reporting enables continuous improvement of operations and early detection of issues due to changing conditions both internal and external to the operator. This was not supported by the operator’s application of its SMS.
For example, Airservices Australia analysis of flight data identified an increase in number of helicopters operated in close proximity at the operator’s helipads, after the introduction of the EC130 helicopters. If the operator was encouraging crew to record these instances alongside the level of coordination in place or level of coordination required, there would have been a tool which could reveal separation trends in the operation. That could have provided an opportunity to re‑evaluate existing controls.
The operator’s operation and location were unique to it. Analysis of the risk controls for managing separation at the helipads has shown that the controls were not as reliable as imagined. Aviation safety in the operation was essentially being run on experience without data. Under that policy, the organisation was not able to demonstrate that the risk in its operation was as low as reasonably practicable.
Hazards were related in interviews relating to specific aspects of the high-volume low duration flights conducted in that location. Those hazards were not managed through the SMS and without specific objectives there was nothing to guide an employee’s engagement with the SMS. As a result, it would be unlikely that any known hazards would be managed at an organisational level and these hazards would instead be accepted as business as usual.
Evidence of activities within the SMS showed that the organisation was not focused on meeting its policy of minimising the risks associated with aircraft operations. However, the objectives of the SMS were easily met by addressing WHS and ground handling issues. In that regard, the system ramped up quickly and addressed WHS issues at a rate higher than before. This demonstrated that the system was suitable and functional enough to prevent harm and provide a safer environment.
All that was required from that point was to apply the system to aviation safety risk. The operator had awareness and had acknowledged hazards within their operations, such as the potential for a midair collision. The capability to manage safety existed, yet the operator, for reasons that could not be determined, chose not to use the SMS to manage aviation safety risk.
The evidence of what was achieved in a short space of time using the SMS in ground handling and WHS indicates that, had targeted objectives been set, the aviation safety risk relating specifically to the operator’s scenic flights in that location could have been effectively addressed. Importantly 2 major changes to the operation, introduction of new helicopters and reopening of the park pad, were lacking in management of aviation safety risk. As a result, limitations in the operator’s risk controls were not discovered, and unintended consequences of change in the operation were allowed to persist.
|
Contributing factor |
Implementation of aircraft
There was evidence that in 2018, under previous ownership, use of a new helicopter was subject to a change management process. During that process existing job hazard analysis documents with relevant information were referred to, and where the new helicopter could not support existing risk controls, alternative controls were put in place. Similar systems were available to Sea World Helicopters for onboarding their EC130 fleet.
The owner of Sea World Helicopters stated that the decision to use EC130 helicopters was made to improve the tourism product. Following occasional cross‑hire of EC130s the first long‑term EC130 B4 (registered VH-XKK) (XKK) was introduced in September 2021 and used to conduct scenic flights on 15 December 2021.
At the time of the introduction of the first EC130 B4 (XKK), a performance goal of the SMS was stated as:
All proposed new equipment acquisitions, facilities, operations and procedures are reviewed to identify risks and potential hazards
Additionally, a requirement of change in the SMS was:
While there should be constant vigilance to identify hazards, increased vigilance should be exercised during situations involving organisational or operational change or at other times such as those listed below:
…
d) When new equipment, procedures or processes are introduced
However, there was no evidence in records or interviews of hazard identification or change management being conducted for the introduction of XKK.
At the time of implementation of XKQ and XH9 a new change management requirement had been added. It stated that:
When actioning a proposed change, the CEO, in consultation with the CP[70] and Safety Manager, must…
Assess the risks of the proposed change including any controls/mitigations being introduced with the change.
A relevant trigger was:
new business opportunities or new or different kinds of aircraft
While the language of the trigger and use of the word ‘new’ could be ambiguous, the EC130 B4s, and specifically XKQ and XH9, were purchased to support a change in product offering. The new helicopters were different to the AS350s ordinarily used for tourism flights. The EC130 did not provide for direct continuity in operations and required changes in procedures and training. A change management process was appropriate for the introduction of these helicopters, and especially for XKQ and XH9 which the operator intended to be used full time for scenic flights.
The operator stated that they did not recognise the replacement of their primary aircraft as a change, and no change management process was required for XKQ and XH9 as XKK was already in the fleet. (However, as mentioned above, there was no evidence of change management processes implemented for XKK either.) This circumvented the mandatory requirement of their documented procedures. As there was no recognition of the change, there was no evaluation of the change. The operator reported that no further consideration of risk was required, and the replacement helicopters were implemented. Consequently, the impact on aviation safety risk was almost certainly underestimated.
As well as there being a requirement for change mandated in the operator’s exposition, there was a regulatory requirement to address. Regulation 119.020 of the CASR defines significant changes and included ‘any leasing or other arrangements for the supply of an aeroplane or rotorcraft used in the operator's Australian air transport operations’ which are required to be notified to CASA if the change ‘does not maintain or improve, or is not likely to maintain or improve, aviation safety’.
The operator was unable to determine maintenance or improvement of aviation safety without assessing the change, and the investigation has demonstrated that the introduction of the EC130s did not maintain safety. The existing AS350 helicopters had been standardised and were set up specifically for the scenic flight operations. To meet the same level of utility to the operations, deliberate steps should have been taken with the new helicopters.
For example, within XKQ and XH9:
- Seatbelt standardisation would have reduced risk of incorrect fitment and improved ground crew flow.
- Timely sourcing of mounts and iPads for EFBs would have ensured they were available for use.
- Fitment and programming of UHF radios would have enabled intracompany communication.
- ACAS settings could have been understood and correctly configured to offer better protection.
- Pilot training on ACAS systems would have reduced distraction and improved protection.
Furthermore, issues which could have been identified through a change and risk management process persisted during the implementation of the helicopters and affected previously documented risk controls.
For example, faulty avionics were a known issue for XH9 which had a non-functional transponder. That was equipment used as a risk control for midair collision in the cruise, and the failure reduced the effectiveness of existing controls. Additionally, a pilot of an AS350 would have a much clearer view of traffic in the Broadwater than the pilot of an EC130. Controls to support an EC130 pilot to detect traffic were not considered.
Camera systems were fitted to the helicopters, and while the camera systems had the potential to add to customer experience, the delay of the aforementioned elements along with the absence of a fire extinguisher in XKQ and fitment of an inappropriate extinguisher in XH9, suggests that the organisation did not prioritise safety. Clearly, the introduction of newer and more capable helicopters was intended to maintain or improve safety. Also, some elements of the implementation of the EC130 were successfully managed. Pilot and ground crew training, and the passenger briefing system for example were updated and conducted before XKQ and XH9 were used in scenic flight operations.
However, a formal change management process with attendant job hazard analysis, risk management and implementation review would have reasonably captured and managed the issues which undermined existing risk controls and procedures. Without that process the operator was less prepared to ensure maintenance or improvement of aviation safety when embedding the new helicopters into their scenic flight operation.
A change process would have brought formal consideration of absent risk controls and unintended consequences to the fore. However, management of airworthiness issues shows it is highly likely that the operator would have used the helicopters before resolutions were in place. Therefore, not conducting a change management process cannot be said to have contributed to the event, and instead increases risk.
|
Other factor that increased risk Sea World Helicopters commenced operations with EC130 helicopters without a formal change management process. Implementation of the operator's documented procedures would have increased the likelihood of formal consideration of various risk controls, including controls that were previously applied for the introduction of aircraft. (Safety issue) |
Assessment of the park pad
Prior to approving refurbishment of the park pad, Village Roadshow Theme Parks (VRTP) commissioned an aviation consultant to assess the suitability of the helipad for renewal. The aviation consultant used the CASA guidance available at the time, Civil Aviation Advisory Publication (CAAP) 92-2 (2), Guidelines for the Establishment and Operation of Onshore Helicopter Landing Sites (2014), as a reference and scope for the work. CAAP 92-2 (2) was derived from ICAO Annex 14 Volume II, which gave advice to nation states on the planning, design, and operation of heliports.
In a report provided to VRTP and Sea World Helicopters, the consultant found that refurbishment could restore the park pad to meet the requirements of a secondary helicopter landing site under CAAP 92-2 (2), and that it could accommodate the operator’s helicopter types. They made further recommendations about safety equipment at the helipad and recommended the creation of a new risk management plan.
The ICAO Heliport manual (ICAO, 2021)was produced to provide guidance to ICAO Annex 14 Volume II. That Heliport manual was not used and was not required to be used in this assessment. However, it did carry guidance on deconflicting heliport traffic with large aerodromes to eliminate or manage flight interaction with aerodrome traffic. While there were no large aerodromes to deconflict with in this case, taking the step to extend the concept of deconfliction to small aerodromes would have been a useful element to raise.
New guidance from CASA was published in April 2022, just a few weeks after the park pad was reopened. That document Advisory Circular 139.R-01 v1.0 – Guidelines for heliports - design and operation echoed the ICAO Heliport manual in providing guidance to assess impact on nearby certified (as opposed to large) aerodromes, to minimise interactions between heliport traffic and pre-existing aerodrome traffic.
However, none of the nearby landing sites were certified. While conflict with traffic at certified aerodromes would ordinarily involve larger air transport flights and collision alerts could cause significant disruption, operators would also benefit from prompts to deconflict with smaller landing sites and aerodromes to avoid flight below safe margins of separation.
At the time of the assessment the available guidance did not discuss flight paths or conflict with other helipads. If that guidance did advise deconfliction with nearby facilities it is likely to have featured within the scope of considerations of the assessment and subsequently appeared in recommendations to the helipad owner and the helicopter operator. However, the outcomes are likely to have remained the same as given the operator’s assumptions about the conflict point, it is highly likely that the operator would have considered their baseline controls to be effective.
|
Other factor that increased risk At the time of park pad assessment, the Civil Aviation Safety Authority's guidance documents for establishment of helipads did not prompt assessment of flight path interaction with other already established traffic. (Safety issue) |
Implementation of the park pad
There is ample freely‑available guidance provided by CASA for any aviation operation to conduct a change management process (CASA, 2022e). The first step of that guidance is that a change process should begin with establishing the objective and drivers for change. This was not captured in the operator’s process.
Interviews showed that there was an intent to refurbish the park pad from the inception of the contract following the sale of the helicopter business. It was also apparent through analysis of flights that the park pad, having easy access to park patrons, provided 27.6% of the scenic flight volume conducted by the operator. The intent of the change could be reasonably inferred to be to increase the number of flights conducted at the Sea World location.
The next step is to identify who will be affected. An important part of this step is to introduce people who could identify impact on existing risk controls that may affect aviation safety risk. The guidance states that it is critical that the broader impact of that change is considered on the system as a whole, and that existing safety risk management processes should be used (CASA, 2022e). However, the step of identifying hazards and completion of risk assessments appeared to be narrow in scope of assessment and in breadth of input.
Park pad hazards assessed in isolation
The most consequential deficiency of this process was that there was no formal consideration of existing flight operations and risk analysis of how this new facility would integrate with the pre‑existing one. The operator understood the helicopters would pass through the same point in space on approach and departure, and did not consider that the risk of collision with company traffic was something that required specific analysis or management. While the company advised pilots to look-out in all departures, the risk was not formally examined through this or any other process.
An appropriate group of people had been brought together, representing capabilities in all necessary aspects of the change from initial investment through to ticket sales, passenger handling and flight operations. However, there was no evidence of their input into management of risk for the new facility and expansion of flights. While existing risk controls were written down in older documents and experience existed in the team, there was no evidence existing risk controls were considered.
Specifically, there was no evidence of reference to a similar assessment conducted in 2019 for operations at the main heliport. That assessment discussed collision risk at the heliport with attendant mitigating controls. The park pad job hazard analysis was conducted by considering operations from the park pad in isolation. There was no evidence of requiring or considering additional risk controls or procedure changes for flights inbound for the heliport which were also impacted by the change. Examining relevant past documents would have revealed useful risk and procedure information.
That lack of consideration of the wider operation may have been due in part to the operator conflating risk management and job hazard analysis. The change form for this activity, and previous responses to audit findings, gave the impression that the distinction between job hazard analysis and risk management was not well understood within the operator.
While the JHA was written by the HOFO and approved by the CEO, no other change team members or pilots had signed it and interviews showed that other company pilots were not aware of that document. The development of the JHA document in isolation and remaining uncirculated suggests that this was a perfunctory activity as opposed to an exploratory one. Additionally, there was no evidence that the operator had conducted any assessments of the reliability of the CTAF calls, ground crew calls or visual lookout.
The CEO stated that the risk controls of CTAF, pilot visual lookout and rules of the air, were the same as any other operation in Australia. For that reason, the operator did not find it necessary to examine those controls and their suitability or consider additional controls for their specific operation. It is correct that these are standard controls, successfully implemented for operations at uncontrolled aerodromes. However, the operator’s intended implementation of high frequency short duration flights from co-located helipads could not be considered as a normal operation at an uncontrolled aerodrome.
The scenic flight operation at Sea World would reasonably require controls in excess of the baseline standard. Indeed, additional controls had been in place before the reopening of the park pad and the implementation of new helicopters. By considering the task of operation from the park pad in isolation, the operator overlooked the unique aspects of their operation. Specifically, the conflict point created by the implementation of the park pad, and the frequency of helicopters from both nearby locations passing through it.
No ongoing review of park pad operations
The operator stated on the change form that no review of the implementation of park pad operations was required. When combined with the low level of hazard reporting this meant that assumptions about the effectiveness of baseline controls at the site would be unlikely to be revisited or tested. Additionally, updated helipad guidance would be less likely to be incorporated without a review procedure. In a similar fashion to the implementation of the new heliport, there was no evidence of lessons learned at the park pad being incorporated into procedures or operational documents.
While the operator was aware of the existence of the conflict point, they did not consider introduction of the conflict point to present an unusual risk. Had they included analysis of the impact of the park pad change on the whole of operations in their change management process, it is highly likely that they would have seen that additional controls were justifiable. Without risk analysis, the circumstances surrounding this conflict point were not formally considered and the limitations of the operator’s controls to prevent midair collision could not be demonstrated to manage the risk to be as low as reasonably practicable. This resulted in unmanaged risk remaining in the system.
|
Contributing factor Sea World Helicopters' change management process, conducted prior to reopening the park pad, did not encompass the impact of the change on the operator's existing scenic flight operations. Crucially, the flight paths and the conflict point they created were not formally examined, therefore limitations of the operator’s controls for that location were not identified. (Safety issue) |
Drug and alcohol management
The Sea World Helicopters drug and alcohol management plan (DAMP) described a delegation of drug and alcohol testing to Village Road Show Theme Parks (VRTP). However, interviews showed that this delegation was inconsistent with the understanding of VRTP management. There was no formal agreement in place for VRTP to provide drug and alcohol testing to, or on behalf of, Sea World Helicopters. The testing provided by VRTP was reportedly only for their own WHS obligations.
Sea World Helicopters staff were tested on employment, and the DAMP allowed nominated DAMP supervisors (the HOFO and the safety manager) to require pilots and other personnel to undergo testing for drugs if they considered there was a reasonable suspicion of drug impairment.
Records showed that Sea World Helicopters pilots were breath tested for alcohol each day. All Sea World Helicopters employees working inside the theme park were subject to random and with-cause testing for drugs. Sea World Helicopters’ ground crew working at the main heliport would not be subject to testing by VRTP if they were not working within the confines of the theme park itself.
Regardless of the intentions of the program, the testing of Sea World Helicopters personnel for alcohol and drugs was in excess of CASA’s regulatory requirements and the practices of many air transport operators, and as such the absence of this testing for some ground personnel was not considered to be a safety risk.
Toxicology
There was no evidence that on the day of the accident anyone suspected that the pilot of XKQ was affected by illicit substances. Indeed, toxicological analysis indicated the pilot was unlikely to have been directly affected by cocaine at that time.
Post‑mortem examination and subsequent toxicological analysis showed that that the pilot of XKQ used cocaine between 1 and 4 days prior to the accident. The reasons for the pilot’s drug use, when or how the drug was ingested and the quantity that was ingested was not within scope of the investigation.
Toxicological analysis indicated that quantities of illicit substances present were very low, and that it was unlikely that the pilot’s psychomotor skills were impaired during the accident flight. The analysis further indicated it was unlikely the pilot was experiencing withdrawal phase effects on the day of the accident, and unlikely to be fatigued as a result of drug use. As such, the pilot’s consumption of cocaine was not found to have contributed to the development of the accident. While not contributory to the accident, the use of illicit drugs by the pilot of a passenger‑carrying aircraft is contrary to regulatory requirements, and to the expectations of fare-paying passengers.
The nature of uncontrolled substances is such that there is limited ability to control the content, quality or dosage of the substance. The cocaine ingested by the pilot of XKQ was contaminated with a veterinary pharmaceutical which mimicked the effects of cocaine and is known to be harmful to human health. The pilot of XKQ was almost certainly not aware of this adulterant and could not anticipate the short‑ and long-term effects it may have had on health and performance. For these reasons consumers of uncontrolled substances cannot accurately assess the ongoing effects of an uncontrolled substance on their ability to safely manage a flight.
No system for detecting drug use is likely to be able to identify all drug use. There is a shared responsibility for managing the aviation risks associated with drug impairment, and individual pilots must abstain from any drug use which may impair their ability to operate aircraft.
|
Other factor that increased risk It is very likely the pilot of VH‑XKQ used cocaine around one and a half days prior to the accident. While the pilot was unlikely to have been directly affected by the drug at the time of the accident, the actual effect of illicit substances and associated adulterants on safety of flight cannot be predicted by users and periods of impairment beyond the anticipated effects can occur. |
Survivability
Overview
The actions of the pilot of XH9 and to some extent the crash performance of XKQ has led to the survival of passengers in an accident that would not normally be survivable. Though the contribution to outcomes for passengers could not be determined, there were several factors from a survivability perspective that had the potential to lead to increased injury. These factors related to the performance of the occupant restraints and the lack of research, testing and guidance on how to fit constant wear lifejackets and multipoint restraints while maintaining the intended performance of each device. The investigation also found that the pre-flight safety information provided to passengers did not provide comprehensive, consistent, or correct information.
Fitment of multipoint restraints with constant wear lifejackets
The manufacturer’s instructions for the fitment and use of constant wear lifejackets covered only those actions required to use that piece of equipment independently. In Australia, in a helicopter tour context, when lifejackets are required to be carried, they must be worn. This is to ensure that passengers can access this piece of equipment in a timely manner. If the helicopter lands on or impacts water, helicopters are known to invert causing significant disorientation, making the retrieval of a lifejacket prior to egress almost impossible.
Helicopters used for scenic flight operations, like the EC130, are likely to be fitted with multipoint restraints. In this case, the operator had aircraft with both 3- and 4-point restraints. Given the requirement to wear a lifejacket with multipoint restraints, it is reasonably foreseeable that the 2 pieces of equipment would be used together.
Manufacturers of constant wear pouch‑style lifejackets provided instructions that required them to be fitted around a person’s waist and positioned in the middle of their body. This allows the lifejacket to be removed from the pouch and placed over the head, using only one hand. The problem that arises as a result, when fitting a multipoint restraint, is the position of the lifejacket interferes with the proper fitment and tightening of the restraint. Social media documented a significant number of examples of this interference in Australia and internationally. Commonly, the buckle of the restraint is placed above or over the lifejacket, causing the restraint webbing to be slack and off the occupant’s hips.
In an accident, incorrectly fitted restraints will not perform as designed and can cause injury to the person (from the restraint itself) and allow more serious injury to occur through submarining and excessive flail resulting in contact with aircraft structure. Incorrect fitment has also been shown to lessen the effectiveness of energy attenuating seats. These seats are designed to stroke and absorb energy that would otherwise be transferred to the occupant. If a person is not correctly restrained this feature may not work as designed, resulting in more serious injury.
Having access to a lifejacket in the case of ditching is important and reduces the risk of drowning. However, occupants must survive an impact and exit the aircraft before the lifejacket will be required. Correct fitment of restraints is vital to allow the restraints and energy‑attenuating seats to work as designed. This will provide the greatest opportunity to survive an accident to the extent that further actions can be taken to ensure survival through any post-crash factors.
There was no evidence of research or testing to validate the correct fitment of constant wear lifejackets and multipoint restraints together, nor was there any guidance from lifejacket manufacturers or regulatory authorities that could be used to assist operators. For the reasons listed above, research and/or testing that leads to guidance on integration of constant wear lifejackets with multipoint restraints is required so that operators and passengers in this sector and others can use these 2 pieces of equipment together without increased risk of harm. Further, while generic guidance was available, manufacturer guidance about the correct method of operation for specific seatbelts was not readily available. Making this information easily accessible would increase the likelihood that operators are clear about correct use of this equipment.
|
Other factor that increased risk Due to the lack of research, there was no validation to determine fitment of multipoint seatbelts with constant wear lifejackets to ensure correct function. Consequently, there was no readily available guidance for aircraft operators, and fitment of multipoint seatbelts with constant wear lifejackets across helicopter tourism operations worldwide was inconsistent and frequently incorrect. This created a risk of the equipment (including aircraft seats) not performing as designed in the event of an accident, increasing risk of injury. |
Operator integration of lifejackets with multipoint restraints
Ground crew members were given the responsibility of fitting lifejackets and restraints to passengers. Documentary evidence and interviews showed that the operator’s pilots and ground crew did not know how to integrate the constant wear lifejacket with restraints so that the fitment of the restraint would not be affected. As there was no operator guidance or procedures, ground crew would learn the incorrect fitment during their on-the-job training and through reference to the operator’s safety briefing video.
|
Other factor that increased risk Sea World Helicopters did not have documented procedures or guidance on the correct fitment of aircraft seatbelts in conjunction with constant wear lifejackets. As a result, on the job training provided to ground crew included incorrect fitting practices, leading to passengers being routinely incorrectly restrained. This increased the risk of injury to passengers in the event of an accident. (Safety issue) |
As a result, the ground crew were inadvertently assisting passengers to fit seatbelts incorrectly in everyday operations. Videos and photos confirmed that this was the case on the accident flight. Passengers on both helicopters variously had loose and twisted seatbelts with the buckle over the lifejacket or placed on the sternum.
|
Other factor that increased risk Although secured by ground crew, the restraints of most passengers aboard VH‑XKQ and VH‑XH9 were incorrectly fitted. |
VH-XKQ restraint performance
How well an occupant is restrained and supported by their seat and restraint system, and the degree to which the loads experienced in an impact are distributed over the body’s structures, is critical in ensuring human tolerance. This factor is one of the primary determinants of lack of survival in a survivable accident (Shanahan, 2004). Incorrect fitment of restraints was a feature of this accident, though the extent of passenger injuries because of incorrect fitment could not be determined.
The right side of the helicopter impacted the ground first and passengers on that side were seen to flail outside of the helicopter as it bounced then rolled over. Flail injuries sustained to several passengers were influenced by incorrect positioning of their restraint system.
Video taken prior to departure showed that the right rear outboard seat passenger’s restraint was fitted over their lifejacket creating slack. That passenger submarined and flailed outside the helicopter held by the lap belt under their arms. First responders rescued this passenger from the helicopter without the need to undo the passenger’s seatbelt.
Additionally, during the accident sequence, there was inadvertent partial or full release of 2 safety harnesses. One of these passengers was positioned front right. Video from inside XKQ showed the front right passenger’s shoulder harness was no longer connected during the rollover following the impact with terrain, and that passenger, restrained only by their lap belt, flailed outside the helicopter.
Reports and photographs of the emergency response showed that first responders found the rear left outboard passenger underneath the helicopter cabin, away from their seat. This passenger was also removed from the helicopter without making any cuts to their restraint, indicating that at some point this passenger had moved enough to have created slack in, or been completely released from their restraint.
In addition, a first responder reported releasing the rear left inboard passenger’s restraint buckle to extract them however, the buckle was subsequently found completely detached from the seatbelt. Testing of the restraints revealed that all restraint systems on XKQ functioned as expected and the reason for the release of the shoulder strap tangs on the front right passenger’s seatbelt and detachment of the rear left inboard passenger’s buckle could not be explained.
It was shown that those passengers whose restraint performance was sub-optimal flailed significantly, were more likely to have unrestricted movement, and potentially struck other objects or the aircraft structures. However, it could not be determined to what extent that the injuries received by those passengers would have been different if they had been correctly restrained. Nevertheless, research consistently shows that wearing restraints correctly (securely, low and tight across the hips, without slack) can reduce the risk of injury.
|
Other factor that increased risk The effectiveness of most of the passengers' 4-point restraints in VH‑XKQ were compromised due to incorrect positioning and loose lap belts. Additionally, during the accident sequence, there was inadvertent partial or full release of 2 safety harnesses. These issues resulted in improper restraint and/or excessive flail for those passengers. |
Passenger safety briefing
Passengers are often heavily reliant on instructions provided to them if an emergency occurs, and safety information differs across aircraft types and configurations. For example, the brace position that passengers may be familiar with from travelling on large transport aircraft is not the recommended position for use while utilising a 4-point restraint in a helicopter.
The operator had a system for briefing passengers that encompassed a safety briefing video, a briefing card and advice from their ground crew. Evidence showed that the primary method of communicating safety information to passengers was the safety briefing video played prior to departure. Aside from information about headsets, there was no other information provided to passengers once they had boarded the helicopter. Passengers on the day of the accident reported that they had not been referred to a briefing card and were unaware of its location.
The safety briefing video gave passengers incorrect information about how to correctly fasten their seatbelt, showing the buckle of the harness positioned on the person’s abdomen. As passengers are likely to be unfamiliar with an aviation 4-point restraint, they would not know the video was incorrect. Additionally, the safety briefing video did not include any information about the brace position, the location or operation of the doors on the EC130 or the location of the briefing card leaving passengers without knowledge of these key pieces of information.
The operator’s safety briefing card did contain information about the EC130 doors, the brace position and showed a more correct method of the operation of the seatbelt, although the image showed the seatbelt fitted to a seat and not a person. However, research conducted by the National Transportation Safety Board (2000) and the ATSB (2006) found that passengers tend not to read the safety briefing card, and if they do, not all of them will understand the instructions provided. Consequently, as supported by CASA guidance, safety briefing cards should only be used as a supplement to an audio visual or oral briefing.
Research has shown that more knowledgeable passengers perform better in an emergency. It is therefore important that passengers are aware of how to fasten their seatbelt correctly, how to brace, how to operate the exits in an emergency and if flying over water, what to do in the event of a ditching. However, in the context of helicopter tour operations and in this case, there may be limited time available to provide emergency instruction which means that passengers need to be as informed as possible prior to departure.
Importantly, because there is no longer a regulatory requirement to assign a crew member to check that seatbelts have been fastened correctly, it is now a passenger responsibility. This reinforces the need for passengers to be provided with complete and correct information so that they are as prepared as possible to take appropriate action in the event of an emergency.
|
Other factor that increased risk Sea World Helicopters' passenger safety briefing system, comprising of a passenger safety briefing video supplemented by safety cards and ground crew advice had limited, inconsistent and incorrect information about correct fitment of seatbelts, location and emergency operation of the EC130 doors, and the emergency brace position. (Safety issue) |
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the midair collision involving Eurocopter EC130 B4, VH‑XH9, and Eurocopter EC130 B4, VH‑XKQ at Main Beach, Gold Coast, Queensland, on 2 January 2023.
Contributing factors
- VH‑XH9 and VH‑XKQ collided at an intersection created by simultaneous operation of the park pad and main heliport. Separation at the intersection relied solely upon alerted see-and-avoid.
- Due to the prioritisation of passenger loading and cabin preparation activities, it is unlikely that the pilot of VH‑XKQ focused on the inbound radio call made by the pilot of VH‑XH9.
- The airspace information provided to the pilot of VH‑XKQ by ground crew was not relevant by the time VH‑XKQ took off. As per the operator's procedures, after giving the thumbs up the ground crew member ceased monitoring the water and airspace behind the helicopter.
- The radio system used by pilots of VH‑XKQ for external communication had defects that limited transmission range and affected reliability of transmission.
- It is almost certain that a taxi call was not successfully broadcast from VH‑XKQ. It is likely that the pilot made a taxi call, and that it was subject to transmission failure.
- The ability of the pilot of VH‑XKQ to visually identify VH‑XH9 north‑west of their position over the Broadwater was limited due to restrictions on manoeuvring and visibility from the operationally required parking position facing south‑east on the park pad.
- Having to rely solely on unalerted see-and-avoid for separation, the pilot of VH‑XKQ almost certainly did not sight VH‑XH9 or manoeuvre VH‑XKQ to do so.
- Although the pilot of VH‑XH9 made a procedural call to announce their position when approximately 2 minutes from the heliport, they made no further radio calls. Consistent with the operator's procedures, upon sighting VH‑XKQ on the park pad, the pilot of VH‑XH9 assessed the risk of collision and did not consider it necessary to make an additional radio call to alert VH‑XKQ to their presence.
- As the pilot of VH‑XH9 did not hear a taxi call they had no trigger to reassess the status of VH‑XKQ as a collision risk.
- Inbound for the heliport, the pilot of VH‑XH9 concentrated on their primary task of landing, directing their attention to their landing site and a vessel on the water. Consequently, the pilot did not maintain an active scan, and the left door pillar blocked the view of the park pad and VH‑XKQ at times during their approach. As a result, the pilot of VH‑XH9 did not sight VH‑XKQ airborne before the collision.
- Sea World Helicopters’ standard inbound call from Porpoise Point was not a reliable alert for a pilot on the ground while boarding and interacting with passengers. Where collision risk on departure existed, a pilot on the ground would highly likely be focused on cabin preparation at the time of that inbound call. (Safety issue)
- Sea World Helicopters’ procedure did not require ground crew to monitor the airspace up to the time of the helicopter departing the helipad. As the presence of hazards behind the helicopter could change significantly within a short space of time, helicopters routinely departed without current hazard information from ground crew. (Safety issue)
- Reopening the park pad in March 2022 created an increased risk of collision with traffic operating from the existing heliport. The conflict point was placed at a location where:
- there was a higher workload for both pilots
- both pilots needed to consider the effect of helicopter downwash on surface traffic
- it was less likely that an inbound pilot would notice a change in the status of a helicopter on the ground
- it was more difficult for an outbound pilot to acquire traffic
- helicopters would close on each other vertically and laterally, decreasing likelihood of detection
- the operator's airborne collision avoidance systems would not provide traffic advisories (Safety issue)
- Sea World Helicopters' documented procedures for communication between inbound and outbound helicopters were not specific to their usual operation and location, and permitted a reactive model of separation, increasing the likelihood that an outbound pilot would not form awareness of relevant traffic. While some company pilots made proactive calls during final approach, this was not a standard practice. (Safety issue)
- Sea World Helicopters was aware of the hazard of midair collision and assumed that any conflicting traffic would always be visible to pilots. Furthermore, the operator did not deem the collision risk to be unusual and considered its existing baseline controls to be effective.
- Following the change in ownership of Sea World Helicopters, changes to the operation gradually degraded existing controls of enhanced communication and in-cockpit traffic display that informed team situation awareness, and the controls were eventually withheld without formal analysis of the change. This reduced opportunity for company pilots to form and maintain awareness of each other's position and intentions. (Safety issue)
- Sea World Helicopters was reliant on CTAF calls, ground crew advice, and pilot visual detection of aircraft to ensure separation in VH‑XH9 and VH‑XKQ. Available additional controls for enhancing alerted see-and-avoid and reducing the risk of collision were not implemented. (Safety issue)
- Sea World Helicopters' implementation of their SMS did not effectively manage aviation safety risk in the context of the operator's primary business. Additionally, their objectives were non-specific, and the focus of safety management was primarily ground handling and WHS issues. This limited the operator's ability to ensure that aviation safety risk was as low as reasonably practicable. (Safety issue)
- Sea World Helicopters' change management process, conducted prior to reopening the park pad, did not encompass the impact of the change on the operator's existing scenic flight operations. Crucially, the flight paths and the conflict point they created were not formally examined, therefore limitations of the operator’s controls for that location were not identified. (Safety issue)
Other factors that increased risk
- Sea World Helicopters commenced operations with EC130 helicopters without a formal change management process. Implementation of the operator's documented procedures would have increased the likelihood of formal consideration of various risk controls, including controls that were previously applied for the introduction of aircraft. (Safety issue)
- At the time of park pad assessment, the Civil Aviation Safety Authority's guidance documents for establishment of helipads did not prompt assessment of flight path interaction with other already established traffic. (Safety issue)
- It is very likely the pilot of VH‑XKQ used cocaine around one and a half days prior to the accident. While the pilot was unlikely to have been directly affected by the drug at the time of the accident, the actual effect of illicit substances and associated adulterants on safety of flight cannot be predicted by users and periods of impairment beyond the anticipated effects can occur.
- Due to the lack of research, there was no validation to determine fitment of multipoint seatbelts with constant wear lifejackets to ensure correct function. Consequently, there was no readily available guidance for aircraft operators, and fitment of multipoint seatbelts with constant wear lifejackets across helicopter tourism operations worldwide was inconsistent and frequently incorrect. This created a risk of the equipment (including aircraft seats) not performing as designed in the event of an accident, increasing risk of injury.
- Sea World Helicopters did not have documented procedures or guidance on the correct fitment of aircraft seatbelts in conjunction with constant wear lifejackets. As a result, on the job training provided to ground crew included incorrect fitting practices, leading to passengers being routinely incorrectly restrained. This increased the risk of injury to passengers in the event of an accident. (Safety issue)
- Although secured by ground crew, the restraints of most passengers aboard VH‑XKQ and VH‑XH9 were incorrectly fitted.
- The effectiveness of most of the passengers' 4-point restraints in VH‑XKQ were compromised due to incorrect positioning and loose lap belts. Additionally, during the accident sequence, there was inadvertent partial or full release of 2 safety harnesses. These issues resulted in improper restraint and/or excessive flail for those passengers.
- Sea World Helicopters' passenger safety briefing system, comprising of a passenger safety briefing video supplemented by safety cards and ground crew advice had limited, inconsistent and incorrect information about correct fitment of seatbelts, location and emergency operation of the EC130 doors, and the emergency brace position. (Safety issue)
Other findings
- Following the midair collision, the seriously injured pilot of VH‑XH9 landed the significantly damaged helicopter on a pre-selected forced landing site. Pre-planning and the pilot's positive control of the helicopter significantly reduced the consequences of the midair collision.
Safety issues and actions
|
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Limitations of inbound call as a risk control
Safety issue number: AO-2023-001-SI-01
Safety issue description: Sea World Helicopters' standard inbound call from Porpoise Point was not a reliable alert for a pilot on the ground while boarding and interacting with passengers. Where collision risk on departure existed, a pilot on the ground would highly likely be focused on cabin preparation at the time of that inbound call.
Limitations of ground crew airspace check as a risk control
Safety issue number: AO-2023-001-SI-02
Safety issue description: Sea World Helicopters' procedure did not require ground crew to monitor the airspace up to the time of the helicopter departing the helipad. As the presence of hazards behind the helicopter could change significantly within a short space of time, helicopters routinely departed without current hazard information from ground crew.
Flight path design
Safety issue number: AO-2023-001-SI-03
Safety issue description: Reopening the Park Pad in March 2022 created an increased risk of collision with traffic operating from the existing heliport. The conflict point was placed at a location where:
- there was a higher workload for both pilots
- both pilots needed to consider the effect of helicopter downwash on surface traffic
- it was less likely that an inbound pilot would notice a change in the status of a helicopter on the ground
- it was more difficult for an outbound pilot to acquire traffic
- helicopters would close on each other vertically and laterally, decreasing likelihood of detection
- the operator's airborne collision avoidance systems would not provide traffic advisories.
Safety recommendation description: The Australian Transport Safety Bureau recommends that Sea World Helicopters formally considers the design of conflict points within its operation and identifies opportunity for mitigation of risk, with a view to eliminating conflict points, or ensuring administrative controls give pilots the best opportunity to identify conflicting traffic and ensuring that the risk is as low as reasonably practicable.
Reactive model of separation
Safety issue number: AO-2023-001-SI-04
Safety issue description: Sea World Helicopters' documented procedures for communication between inbound and outbound helicopters were not specific to their usual operation and location, and permitted a reactive model of separation, increasing the likelihood that an outbound pilot would not form awareness of relevant traffic. While some company pilots made proactive calls during final approach, this was not a standard practice.
Withholding of risk controls
Safety issue number: AO-2023-001-SI-05
Safety issue description: Following the change in ownership of Sea World Helicopters, changes to the operation gradually degraded existing controls of enhanced communication and in-cockpit traffic display that informed team situation awareness, and the controls were eventually withheld without formal analysis of the change. This reduced opportunity for company pilots to form and maintain awareness of each other's position and intentions.
Reliance on alerted see-and-avoid
Safety issue number: AO-2023-001-SI-06
Safety issue description: Sea World Helicopters was reliant on CTAF calls, ground crew advice, and pilot visual detection of aircraft to ensure separation in VH-XH9 and VH-XKQ. Available additional controls for enhancing alerted see-and-avoid and reducing the risk of collision were not implemented.
Focus of the SMS
Safety issue number: AO-2023-001-SI-07
Safety issue description: Sea World Helicopters' implementation of their SMS did not effectively manage aviation safety risk in the context of the operator's primary business. Additionally, their objectives were non-specific, and the focus of safety management was primarily ground handling and WHS issues. This limited the operator's ability to ensure that aviation safety risk was as low as reasonably practicable.
Safety recommendation description: The Australian Transport Safety Bureau recommends that Sea World Helicopters Pty Ltd develops appropriate policy and actionable objectives within its safety management system to bring the focus of the safety management system to the management of aviation safety risk.
Change management for reopening park pad
Safety issue number: AO-2023-001-SI-08
Safety issue description: Sea World Helicopters' change management process, conducted prior to reopening the park pad, did not encompass the impact of the change on the operator's existing scenic flight operations. Crucially, the flight paths and the conflict point they created were not formally examined, therefore limitations of the operator’s controls for that location were not identified.
Safety recommendation description: The Australian Transport Safety Bureau recommends that Sea World Helicopters Pty Ltd improves change management processes by ensuring assessments are expanded beyond the area of change to the wider organisation. Additionally, the operator should test assumptions and perform risk analysis to support risk‑focused decision‑making, to ensure new opportunities to control risk are identified and existing risk controls are maintained.
Implementation of helicopters without change management
Safety issue number: AO-2023-001-SI-09
Safety issue description: Sea World Helicopters commenced operations with EC130 helicopters without a formal change management process. Implementation of the operator's documented procedures would have increased the likelihood of formal consideration of various risk controls, including controls that were previously applied for the introduction of aircraft.
Helicopter landing site guidance
Safety issue number: AO-2023-001-SI-10
Safety issue description: At the time of park pad assessment, the Civil Aviation Safety Authority's guidance documents for establishment of helipads did not prompt assessment of flight path interaction with other already established traffic.
Ground crew restraint fitment training
Safety issue number: AO-2023-001-SI-12
Safety issue description: Sea World Helicopters did not have documented procedures or guidance on the correct fitment of aircraft seatbelts in conjunction with constant wear lifejackets. As a result, on the job training provided to ground crew included incorrect fitting practices, leading to passengers being routinely incorrectly restrained. This increased the risk of injury to passengers in the event of an accident.
Passenger safety briefing content
Safety issue number: AO-2023-001-SI-13
Safety issue description: Sea World Helicopters' passenger safety briefing system, comprising of a passenger safety briefing video supplemented by safety cards and ground crew advice had limited, inconsistent and incorrect information about correct fitment of seatbelts, location and emergency operation of the EC130 doors, and the emergency brace position.
Safety advisory notice to manufacturers and certification authorities of constant wear lifejackets
| SAN number: | AO-2023-001-SAN-001 |
| SAN release date: | 20 September 2023 |
The ATSB encourages manufacturers of constant wear lifejackets to provide operating instructions and/or guidance material to operators of aircraft on how to wear and use a constant wear lifejacket with a seatbelt (of any configuration) such that it does not interfere with the performance of the seatbelt during an accident.
Further, the ATSB encourages certification authorities to modify lifejacket standards to include the requirement for instructions on how to wear constant wear lifejackets while seated and wearing a seatbelt.
Safety advisory notice to aviation research and testing organisations
| SAN number: | AO-2023-001-SAN-002 |
| SAN release date: | 9 April 2025 |
The ATSB encourages those organisations capable of research to determine a correct method of wearing a constant wear lifejacket with a multipoint seatbelt, while ensuring the correct function of each.
Safety action not associated with an identified safety issue
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Additional safety action by Civil Aviation Safety Authority addressing fitment of seatbelts
In August 2024 CASA released version 1.3 of their multi-part advisory circular about passenger safety information, which had incorporated information about fitment of multipoint restraints and the problems identified when fitting those restraints with constant wear lifejackets. The information included content from the ATSB’s Safety Advisory Notice AO-2023-001-SAN-001 Fitment of constant wear lifejackets with seatbelts in aircraft. The guidance did not contain information about the correct combined fitment, and instead directed operators to consult lifejacket manufacturers.
Civil Aviation Safety Authority airspace review
The Civil Aviation Safety Authority (CASA) initiated a review of airspace around Southport which received 87 submissions from airspace users. CASA published the results of that review in March 2025.
Glossary
| AC | Advisory Circular |
| ACAS | Airborne Collision Avoidance System |
| ADS-B | Automatic dependent surveillance - broadcast |
| AFRU | Airborne frequency response unit |
| AHRS | Attitude and heading reference system |
| AIP | Aeronautical information publication |
| AMO | Approved maintenance organisation |
| AOC | Air operator certificate |
| ATAS | ADS-B traffic advisory system |
| ATIS | Automatic terminal information service |
| ATS | Air traffic services |
| BNC | Bayonet Neill-Concelman |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| CAO | Civil Aviation Order |
| CAR | Civil Aviation Regulations |
| CCTV | Closed-circuit television |
| CT | Computed tomography |
| CTA | Controlled airspace |
| CTAF | Common traffic advisory frequency |
| DAME | Designated aviation medical examiner |
| DAMP | Drug and alcohol management plan |
| EFB | Electronic flight bag |
| EMI | Electromagnetic interference |
| ERSA | En route supplement Australia |
| FATO | Final approach take-off area |
| FAA | Federal Aviation Administration |
| GNSS | Global navigation satellite system |
| HAAMC | Head of aircraft airworthiness and maintenance control |
| HLS | Helicopter landing site |
| HOFO | Head of flight operations |
| HOO | Head of operations |
| ICAO | International Civil Aviation Organization |
| IFR | Instrument flight rules |
| JHA | Job Hazard Analysis |
| LAME | Licenced aircraft maintenance engineer |
| MOS | Manual of standards |
| MR | Maintenance release |
| NSSP | National Surveillance Selection Process |
| NTSB | National Transportation Safety Board |
| PIC | Pilot in command |
| PTT | Push to talk |
| QPS | Queensland Police Service |
| RF | Radio frequency |
| SAN | Safety advisory notice |
| SMS | Safety management system |
| SSAA | Safety sensitive aviation activity |
| SWH | Sea World Helicopters |
| TA | Traffic advisory |
| TAS | Traffic advisory system |
| TCAD | Traffic collision avoidance device |
| TCAS | Traffic collision avoidance system |
| TLOF | Touch-down and lift-off area |
| TTIS | Total time in service |
| TSO | Technical Standards Order |
| UHF | Ultra high frequency |
| UTC | Coordinated universal time |
| VEMD | Vehicle and engine multifunction display |
| VFR | Visual flight rules |
| VHF | Very high frequency |
| VRTP | Village Roadshow Theme Parks |
| VSWR | Voltage standing wave ratio |
| WHS | Work health and safety |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot of the accident flight and other pilots who conducted flights for the operator
- the pilots of other companies who conducted flights in the area
- ground crew of the operator
- Sea World Helicopters
- owner and senior managers of Sea World Helicopters
- Village Roadshow Theme Parks
- employees of other companies under the same ownership as Sea World Helicopters
- Civil Aviation Safety Authority
- Queensland Police Service
- Queensland Fire and Emergency Services
- Gold Coast Health
- Children’s Health Queensland
- Queensland Coroner
- Airservices Australia
- Gold Coast Safety Camera Network
- flight track data
- accident witnesses
- video footage of the accident flight and other photographs and videos taken on the day of the accident
- recorded data from the GPS unit on the aircraft
- Airbus Helicopters
- Geoscience Australia
- Bureau of Meteorology
- Telstra Ltd
- Australian National University: The National Laboratory for X-ray Micro Computed Tomography (CTLab)
References
Airservices Australia. (2023). Movements at Australian Airports Between 01/12/2022 and 31/12/2022. Airservices Australia. https://www.airservicesaustralia.com/wp-content/uploads/Airport_Movement_Snapshot_December2022.pdf
Amundrud, Ø., & Aven, T. (2015). On how to understand and acknowledge risk. Reliability Engineering & System Safety, 16. https://doi.org/10.1016/j.ress.2015.04.021
Aven, T. (2019). The science of risk analysis: Foundation and practice. Routledge.
Bahl, I. (2009). Fundamentals of RF and microwave transistor amplifiers. John Wiley & Sons.
Balanis, C. A. (2016). Antenna theory: analysis and design. John wiley & sons.
Brooks, C. (1989). AGARDograph No.305(E). N. A. G. f. A. R. Development.
Bullough, J. D. (2011). Aviation signal lighting: impacts of lighting characteristics on visibility.
CAA. (2011). Safety Sense Leaflet 13 - Collision Avoidance.
CAA. (2022). Ditching light aircraft on water. (SS21). Crawley, UK: Civil Aviation Authority
CASA. (2017, 7 August). Safety in mind: Hudson’s culture ladder. Flight Safety Australia.
CASA. (2022b). SMS 1 Safety management system basics (3 ed.). Civil Aviation Safety Authority.
CASA. (2022c). SMS 2 Safety policy and objectives (3 ed., Vol. 2). Civil Aviation Safety Authority.
CASA. (2022d). SMS 3 Safety risk management (3 ed., Vol. 3). Civil Aviation Safety Authority.
CASA. (2022e). SMS 4 Safety assurance (3 ed., Vol. 4). Civil Aviation Safety Authority.
CASA. (2022f). SMS 5 Safety promotion (3 ed., Vol. 5). Civil Aviation Safety Authority.
CASA. (2022g). SMS 6 Human factors (3 ed., Vol. 6). Civil Aviation Safety Authority.
CASA. (2022i). SMS 8 SMS resource kit (3 ed., Vol. 8). Civil Aviation Safety Authority.
CASR Part 133 (Australian Air Transport Operations—Rotorcraft) Manual of Standards, (2021) Cth.
Civil Aviation Regulation, (1988) Cth.
Civil Aviation Safety Regulation (1988) Cth.
Collin, R. E. (1992). Foundations for microwave engineering (2 ed.). John Wiley & Sons.
DFS Deutsche Flugsicherung. (2003). TAGA - Traffic Awareness for General Aviation [Presentation]. Eurocontrol. https://www.eurocontrol.int/care-asas/gallery/content/public/docs/act0/tn_ws2/taga-or.ppt
Endsley, M. R. (2015). Situation Awareness Misconceptions and Misunderstandings. Journal of Cognitive Engineering and Decision Making, 9(1), 4-32. https://doi.org/10.1177/1555343415572631
Glenn, D. D. (2011). Job Safety Analysis its role today. Professional Safety(March), 49-57.
Hollnagel, E. (2016). Barriers and accident prevention. Routledge.
ICAO. (2007). Manual of Radiotelephony.
ICAO. (2020). Annex 14 Aerodromes. Montréal, Canada: Internation Civil Aviation Organization
ICAO. (2021). Doc 9261 - Heliport Manual (5 ed.). International Civil Aviation Organization,.
Macquarie Dictionary Online. In. (2024).
Parush, A., Kramer, C., Foster-Hunt, T., Momtahan, K., Hunter, A., & Sohmer, B. (2011). Communication and team situation awareness in the OR: Implications for augmentative information display. Journal of Biomedical Informatics, 44(3), 477-485. https://doi.org/https://doi.org/10.1016/j.jbi.2010.04.002
Pierce, B. (2016). How rare are large, multiple-fatality work-related incidents?, . Accident Analysis & Prevention,, 96, 88-100. https://doi.org/https://doi.org/10.1016/j.aap.2016.07.014.
Pozar, D. (2017). Microwave engineering (4th ed.). Wiley India.
Reason, J. (2016). Managing the risks of organizational accidents. Routledge.
Solomon, N., & Hayes, J. (2017). Levamisole: A High Performance Cutting Agent. Acad Forensic Pathol, 7(3), 469-476. https://doi.org/10.23907/2017.039
Technical Standard Order C13e Life Preservers, (1986 ).
Volakis, J. L. (2019). Antenna engineering handbook (Vol. 1755). McGraw-Hill New York.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Sea World Helicopters
- Jetpoint
- Airbus Helicopters
- Chelton
- Village Roadshow Theme Parks (VRTP)
- Key personnel of previous owner’s AOC
- Civil Aviation Safety Authority (Australia)
- Bureau d'Enquêtes et d'Analyses (France)
- Transport Accident Investigation Commission (New Zealand)
- Air Accidents Investigation Branch (United Kingdom)
- National Transportation Safety Board (United States)
- Airservices Australia.
Submissions were received from:
- Sea World Helicopters
- Chelton
- Village Roadshow Theme Parks (VRTP)
- Key personnel of previous owner’s AOC
- Civil Aviation Safety Authority (Australia)
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Antenna examination
Recovery of the antenna
Due to the identification that the radio transmission recordings from VH‑XKQ were of reduced quality, portions of the antenna system were electrically tested and physically examined. The components removed from the airframe were:
- the VHF antenna (manufactured by Chelton, part number 21-4B, serial number 9906)
- the airframe mounting blister panel for the antenna (manufactured by Airbus, part number 350A 65 25 28.59)
- a short length of radio frequency (RF) coaxial cable (manufacturer unknown, part identifier 1RCA23E) and its BNC connector (manufacturer unknown) (Figure A1).
Figure A1: Removal of antenna components from XKQ
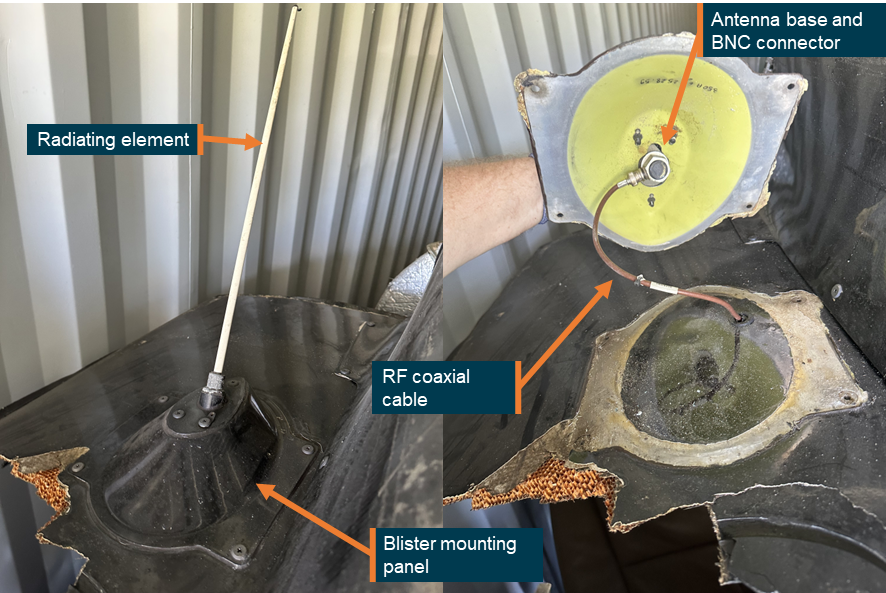
Source: ATSB
Antenna history
Maintenance records from when the helicopter was operated in New Zealand (2008–2019) showed no entries that the antenna or coaxial cable had been subject to unscheduled maintenance and/or replacement. Maintenance records from 2019–2022 while being operated in Indonesia consisted of scheduled maintenance requirements only, for example ‘150 hr’ and ’12 mth’, without showing the exact content of each inspection. Further, unscheduled maintenance and/or component replacement records from the time in Indonesia were not available to the ATSB.
Antenna testing and examination
Functional
Following its removal from the airframe, the antenna was tested at a CASA-authorised avionics maintenance facility, observed by the ATSB. A new BNC terminal was fitted to the cut end of the existing cable to enable connection to the test equipment. The testing identified that the antenna received on two different frequencies without issue, however, the transmission tests on those frequencies failed.
A voltage standing wave ratio (VSWR)[71] test was then conducted. A VSWR value under 2 is considered acceptable, as at 2 the antenna reflects 11% of power (Bahl, 2009). In the absence of an antenna the VSWR test unit read 2.8. With the coaxial cable and antenna attached to the unit they read 2.6. Application of fingertip pressure to the exterior of antenna coax connection caused VSWR to vary between 2.6 and 1.8 and at one point showed 1.1.
The ATSB conducted a further functional check of the antenna using 2 handheld receivers. The radios were positioned at a location over water, with an open line of sight about 500 m apart. This approximated the conditions and distance between XKQ and XH9 at the time a taxi call would have been made. As the VSWR test showed improvement with slight side pressure on the coaxial connection, this field test was conducted with slight pressure from 4 different points. Looking forward as the antenna would be mounted to the airframe of XKQ, gentle pressure was applied to the RF coaxial via manipulation in the fore, aft, up and down directions. The test identified nil transmission when pressure was applied fore, aft and up, with a broken transmission with downward pressure.
ATSB laboratory examination
The antenna was subsequently sent to the ATSB’s technical facility in Canberra for detailed examination.
A general visual examination identified that the antenna displayed evidence of minor physical damage where slight bending, scuffing and abrasion had occurred to the radiating element. There was no damage visually apparent to either the BNC connector, or to the antenna base (Figure A2 and Figure A3).
Upon removal from XKQ, the sealant between the blister panel and the airframe was found degraded and absent at several locations around the bond line. Sealant between the blister mount and the antenna ground plate was complete yet had low adherence (very easy to remove), including nil adherence at several locations, likely due to deterioration over time and/or poor surface preparation. The sealant between the antenna radiating element and the antenna base had gaps.
The ground plate from the antenna and the mounting blister had sustained extensive corrosion/oxidation to the exposed aluminium surfaces at each fixing hole location and to the antenna plate and mount surface.
Figure A2: The VHF Com 1 antenna removed from VH‑XKQ
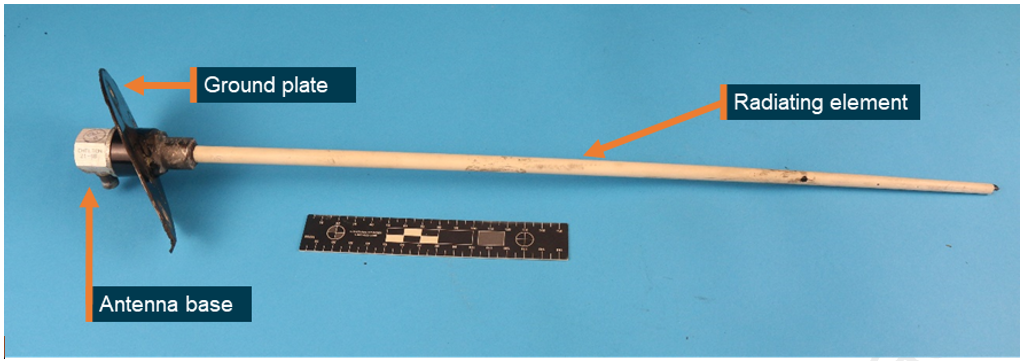
Surface corrosion was identified to the underside mounting holes of the ground plate. Source: ATSB
Figure A3: Corrosion damage to the fix hole surfaces surrounding where the antenna mounting plate (left) was attached to the blister panel (right)

Source: ATSB
Non-destructive examination – X-ray computed tomography
Prior to the conduct of any destructive processes, on 18 June 2024 and again on 30 August 2024, the antenna and the short length of RF coaxial cable containing the BNC connector were submitted for X-ray computed tomography (CT) at the CTLab within the Australian National University. For ease of scanning, the blister panel was removed from the antenna and ground plate assembly. During disassembly, it was noted that the 3 attachment screws between the ground plate and the blister mounting panel were of sufficient torque, however, the lockwire between the antenna and rear screw was not present.
The micro-CT imaging enabled high-resolution non-destructive evaluation of the internal condition of the antenna and BNC connector. The micro-CT imagery did not identify any defects to the entire length of the radiating element, however a crack indication was identified within the soldered joint between the circuit board and the link wire within the antenna base (Figure A4). Additionally for the BNC connector, a potential defect was indicated where a single wire strand was not contained within the centre pin and was protruding sufficiently to be in contact with the connector body (Figure A5 and Figure A6).
Figure A4: Micro-CT of the antenna base (inset) showing a crack in the soldered joint to the link wire (main)
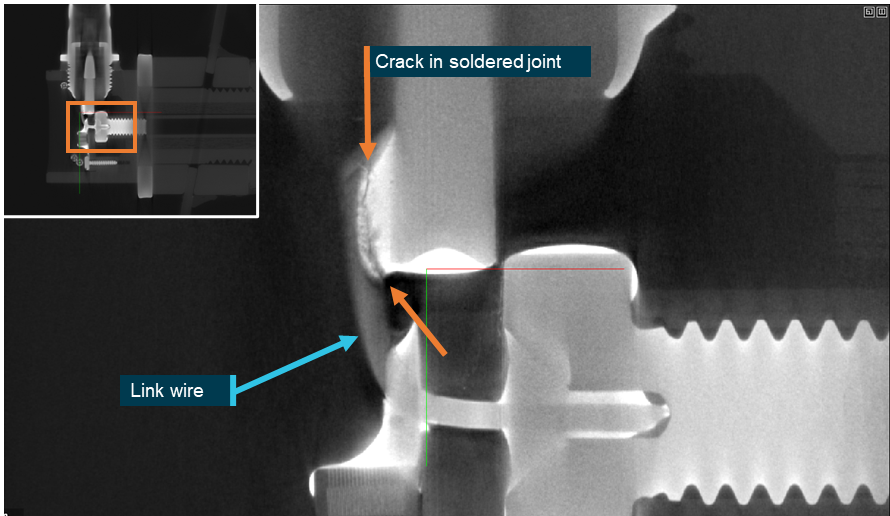
Source: CTLab, annotated by the ATSB
Figure A5: Micro-CT of the helicopter’s RF cable BNC connector: a protruding wire was identified from the crimped region of the central contact pin
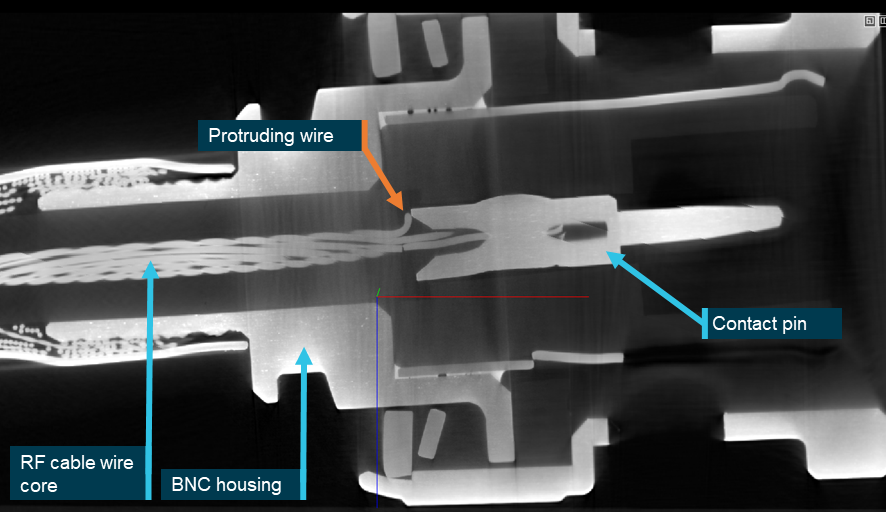
Source: CTLab, annotated by ATSB
Figure A6: Micro-CT of the helicopter’s RF cable BNC connector: close view of the protruding wire showing it was contacting the BNC housing
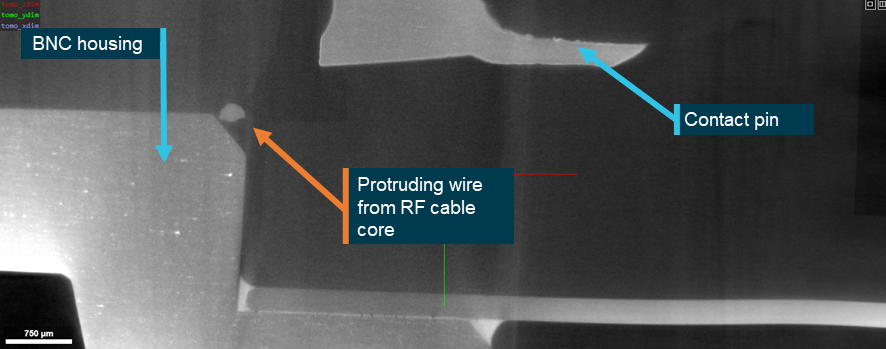
Source: CTLab, annotated by ATSB
Electrical testing and findings
At the request of the ATSB, Chelton (the antenna manufacturer) completed a physical assessment and electrical testing of the recovered antenna components at its facilities in the United Kingdom. The testing was completed on 16 August 2024 and witnessed by an Accredited Representative from the UK Air Accident Investigations Branch.
Through a review of their production records, Chelton confirmed that the part number 21-4B antenna from XKQ had been manufactured in 2008. It further advised that of the 2,166 part number 21-4B antennas that had been produced in the last 10 years, 18 were returned, however no specific electrical faults were identified with those returned units.
Chelton reported that return loss testing was completed in various configurations on the antenna, the RF cable, and the blister mounting panel. The testing was completed in accordance with its production test schedule. On initial connection to the network analyser, all power was reflected back from the antenna. The flat-line response indicated an open circuit and a fault to the RF connection within the antenna. It further noted that the VSWR response of the antenna was variable and could be affected by slight manipulation (or pressure) on the BNC connector.
Direct-current bonding resistance tests were also performed to assess the effect of surface corrosion between the helicopter antenna components. The results identified that there was electrical connectivity from the BNC connector outer through to the metallic radiating element mount. However, measurements suggested that there was no electrical grounding from the antenna to the small ground plate and mounting blister.
In its report of the testing, Chelton found that:
- the antenna had sustained physical damage and demonstrated intermittent performance
- the helicopter’s RF coaxial cable containing the BNC connector displayed corrosion damage and highly intermittent behaviour
- they were unable to determine if the physical damage on these parts was present pre-accident or produced from the accident.
Destructive examination – antenna base
Following completion of Chelton’s electrical testing, the antenna was returned to the ATSB for destructive examination to assess for the internal defects that led to the intermittent electrical behaviour. Because irreversible changes were to be introduced to the antenna components, representatives of the directly involved parties to the investigation were invited to witness the destructive aspect of the examination.
On 10 September 2024, the potting compound was removed from within the antenna base with the view to closely examine the internal circuit board. Once the potting material was removed, high magnification optical examination confirmed that cracks had developed where the link wire had been soldered to the circuit board. The cracks were in the same location identified from the micro-CT imagery. During the dissection and removal of the potting compound, it was noted there was no apparent degradation of that polymeric potting material, nor any evidence of corrosion to the circuit board or within the alloy antenna housing.
From the internal examination, it was established the link wire was able to be manipulated because it had fractured off the solder pad of the circuit board. The fracture surfaces of the solder pad were discoloured from oxidation, which provided evidence that the cracking and fracture of the joint had not recently occurred. Additionally, when examined at high magnification, a portion of the link wire displayed an absence of remnant solder (Figure A7 and Figure A8).
Destructive examination – BNC connector
After identification that an intermittent electrical fault existed within the BNC connector to the antenna coaxial cable, the ATSB completed a destructive examination to further understand that fault. The BNC connector was destructively cross‑sectioned to expose the constituent parts. Indents along the length of the contact pin identified that a crimping method had been used to encapsulate and secure the central coaxial cable wires within the contact pin of the BNC connector. The crimping was conducted as part of the BNC connector and coaxial cable assembly process.
Close visual examination of the centre pin confirmed that a single wire from the core of the coaxial cable was confirmed to be uncontained and looped outside of the contact pin (Figure A9 and Figure A10). Chelton indicated that an electrical fault could develop in the connector of the RF cable installed on the aircraft if that wire contacted the main body of the BNC connector. Because the wire was found protruding and wrapped within the BNC connector body, it is considered highly likely to have been introduced during the assembly process and was not an artefact from the accident sequence.
Figure A7: Antenna base: removal of the potting compound from within the antenna base confirmed the soldered joint containing the link wire had cracked and fractured from the circuit board
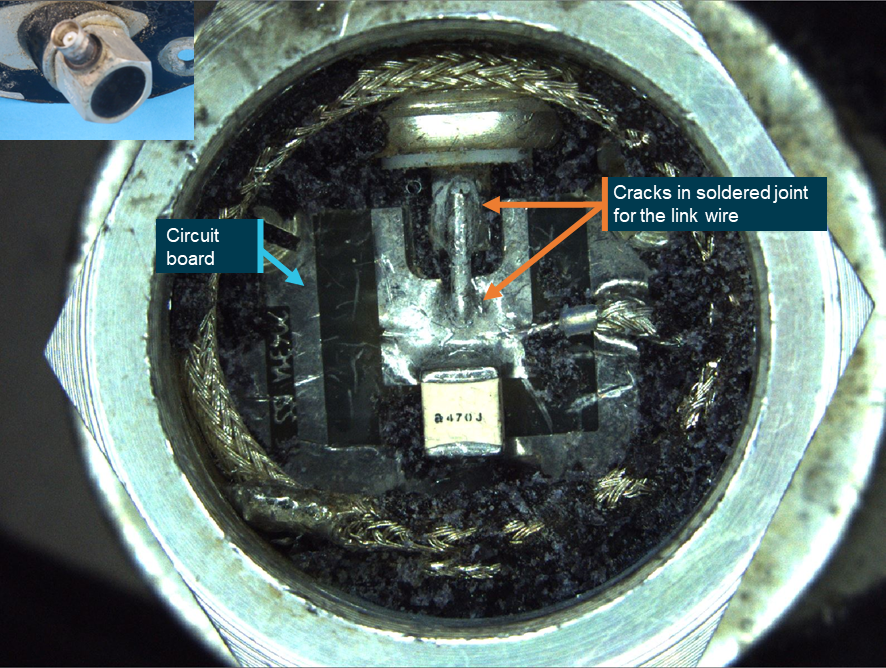
Source: ATSB
Figure A8: Antenna base: close view of the crack in the soldered joint between link wire and circuit board
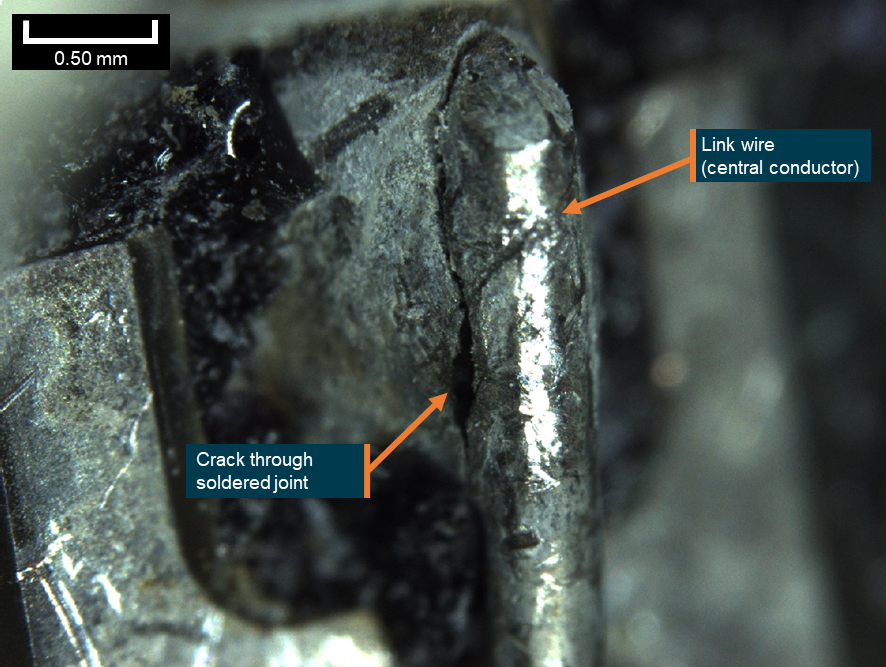
Source: ATSB
Figure A9: Helicopter RF cable BNC connector: cross-section through the connector (inset) from the radio frequency coaxial cable confirming that a stray wire was external to the contact pin
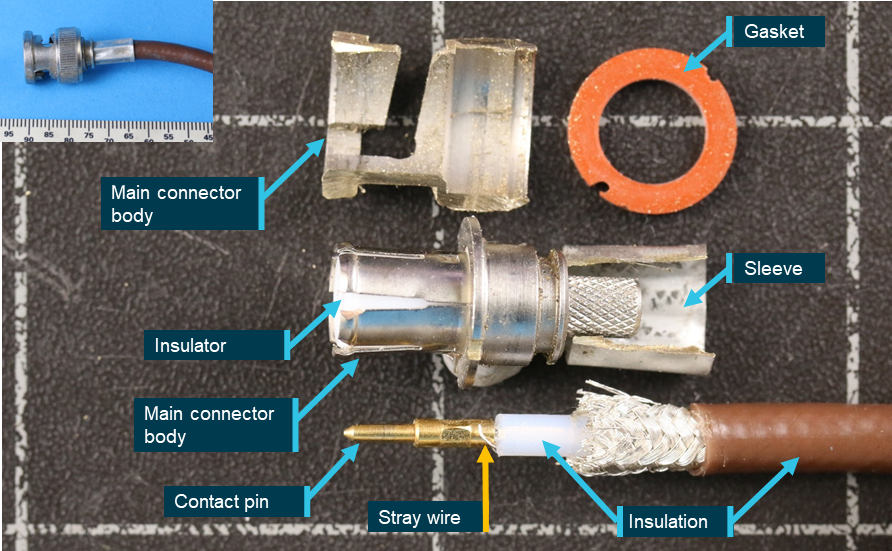
Source: ATSB
Figure A10: BNC connector: close-up showing a stray wire was not contained within the crimping of the contact pin
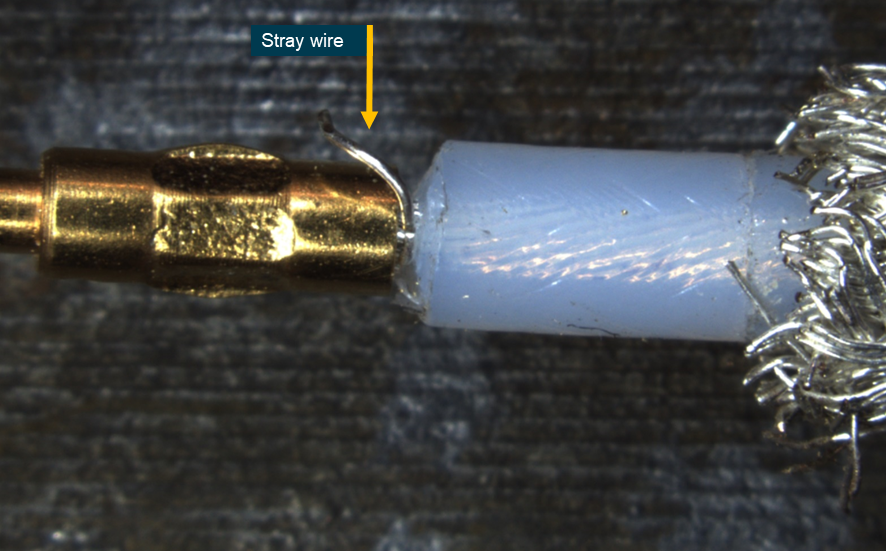
Source: ATSB
Appendix B – Survival analysis
Due to an unprecedented level of visually recorded media, both internally and externally to the helicopters, substantial information about survival factors were determined for the accident flights. This appendix looks at the midair collision mechanics, damage sequence, ground impact forces for XKQ, aspects of the cabin features of the EC130 B4, the injuries sustained, and rescue details for one of the occupants.
Midair collision
VH-XH9
As evidenced by the damage to VH‑XH9, the main rotor blades of VH‑XKQ made 4 passes through the cabin of VH‑XH9 (Figure B1). Debris and damage signatures along with injuries sustained by the occupants of VH‑XH9 correlate to the right-to-left main rotor blade path (clockwise rotating main rotor system) through the cabin of VH‑XH9. The initial impact was captured in video taken by the rear left outboard passenger of VH‑XH9 (Figure B2), and the vertical and lateral position of VH‑XKQ at the point of first contact aligns with the purple dotted line in the figure below.
Figure B1: VH-XKQ main rotor blade passes through the cabin of VH‑XH9
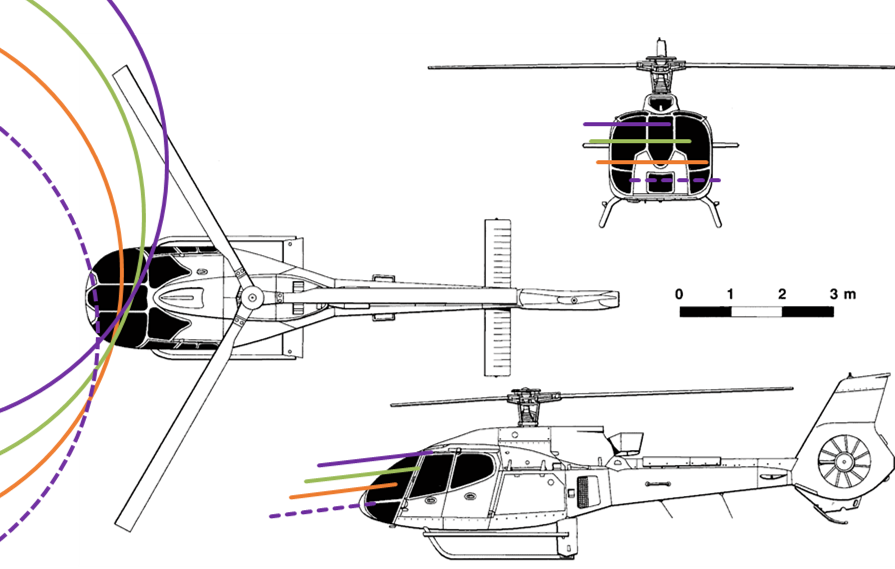
The orange, green and purple circles represent the blade tip path, which is not circular but rather moving in an elliptical and eccentric motion. The blade tip path is represented in the above image as blade discs at one third rotation intervals. Source: Drawingdatabase.com, modified by the ATSB
Figure B2: VH-XKQ initial main rotor blade strikes to VH‑XH9
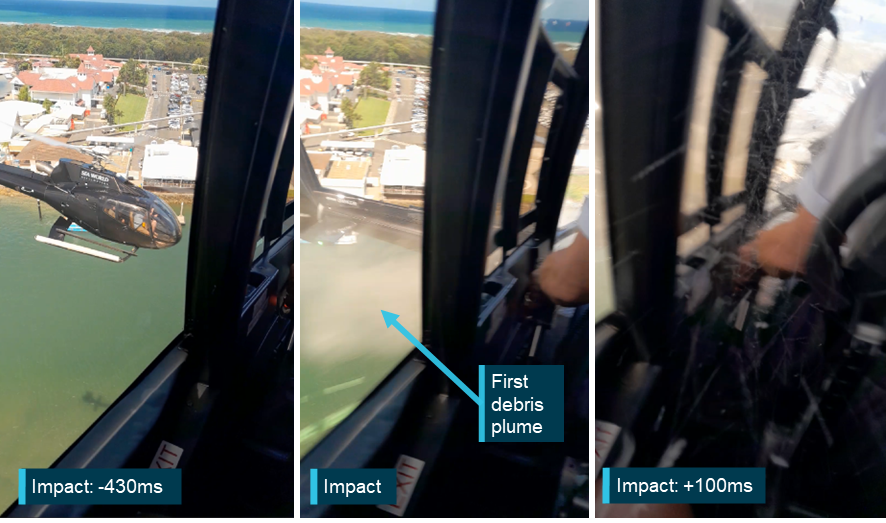
Source: Passenger video, annotated by the ATSB
From Spidertracks position data recovered after the accident, the closing vertical velocity of the 2 helicopters was 6.2 m/s (1,220 fpm). Additionally, the relative (closing) horizontal velocity was determined to be 21.9 m/s (42.6 kt) crossing paths at 73°. Assuming the nominal main rotor blade rotation rate of 400 revolutions per minute (rpm), the relative incremental change in height equated to approximately 0.31 m and a horizontal position change of 1.10 m per blade pass. This aligned closely with the vertical spacing of the cut marks identified in the cabin of VH‑XH9 and the projected relative horizontal paths (Figure B3).
Figure B3: VH-XKQ main rotor blade passes through cabin of VH‑XH9

Source: ATSB
Projecting the relative paths of the helicopters, it was determined that the blade discs of each aircraft passed through each other. At this point, the blade tip of each helicopter crossed the blades of the other at approximately half blade span.
A skin delamination along with a witness mark was identified around half span on the lower surface of VH‑XH9’s blue blade (Figure B4). No associated marking could be identified on VH‑XKQ’s blades.
Figure B4: Paint removal mark in VH‑XH9 blue blade (dashed blue pen mark denotes delamination edge)
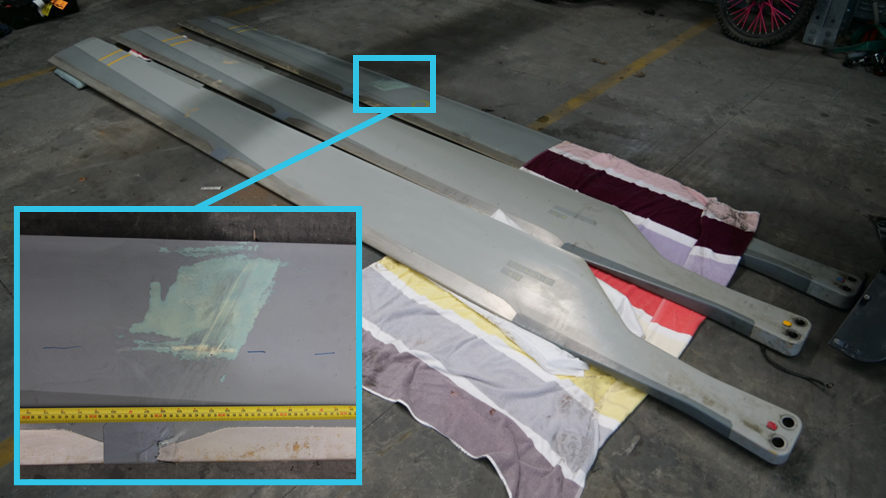
Source: ATSB
The air-conditioning cockpit evaporator unit and mount at the front of the cabin centre console was found bent in the opposite direction to other damage signatures (Figure B5). This was evidence of the damaged front cabin of VH‑XH9 then colliding with the tail of VH‑XKQ as it continued to pass left to right in front of VH‑XH9.
Figure B5: VH‑XH9 air-conditioning cockpit evaporator unit distorted in the direction of VH‑XKQ's travel

Source: ATSB
VH-XKQ collision analysis
The first part of VH-XKQ to strike VH‑XH9 was the main rotor system, which passed through the forward extremities of VH‑XH9’s cabin. Video evidence taken from within the cabin showed these strikes to the main rotor blades damaged 2 of the blades visibly, with trailing edge outboard sections detaching. The damage was more substantial as each successive blade passed deeper into the cabin and structure. Approximately 0.2 seconds later, VH‑XH9’s nose structure collided with VH‑XKQ’s tail. The Fenestron flailed briefly before separating completely when the main rotor system struck the tail boom after approximately another 2 seconds. This tail strike then dislodged the main rotor system, engine and transmission from the airframe which fell uncontrolled to the ground.
Little is known about any cabin intrusion into VH‑XKQ during the collision due to its subsequent destruction upon impact with the ground but evidence from onboard cameras and CCTV recordings at the time, and assessment of the wreckage indicated the cabin was likely contained and structurally intact until it hit the ground. Survivability was severely reduced due to the physical loss of engine, transmission, main rotor system, horizontal stabiliser and Fenestron. CCTV footage of the freefall depicted the fuselage pitching to 90° nose down before pitching up almost level while rolling right to 80° at a roll rate of close to 120° per second before impacting the sandbar.
VH-XKQ ground impact analysis
At the time of collision with terrain, the fuselage was slightly nose down and rolled substantially to the right travelling in the direction of the right side and belly, relative to the fuselage body axis. The fuselage impacted gently sloping wet sand at the water’s edge. The ground impact was captured by CCTV from multiple angles. Figure B6 shows the CCTV frame before VH‑XKQ made contact with the ground.
Figure B6: VH‑XKQ impending impact with ground
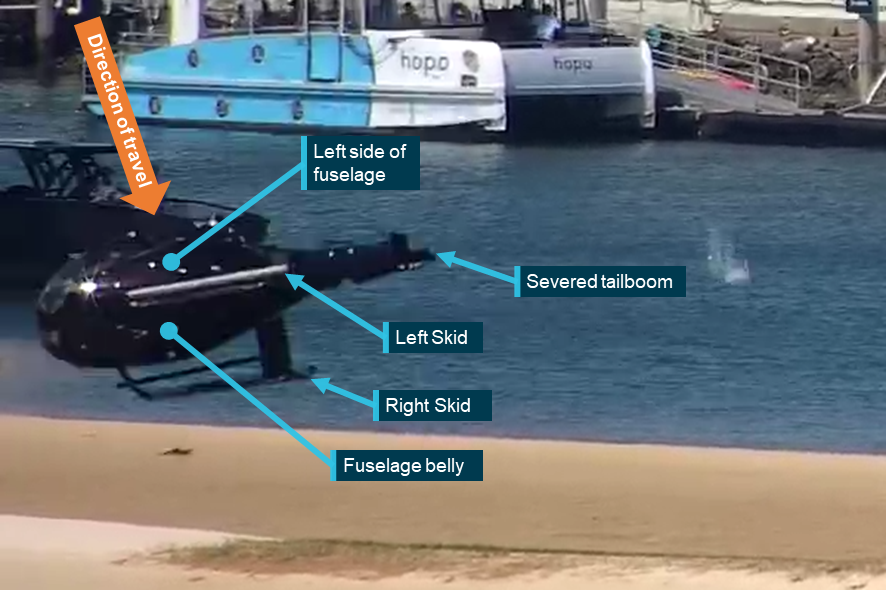
Source: Gold Coast Safety Camera Network, annotated by the ATSB
The fuselage struck the sand and compressed, fracturing the door frames, the floor and undercarriage skids. The polymer fuel tank fractured into many pieces under the hydraulic loading, releasing fuel in multiple directions. The fuselage then bounced very little (0.5–1.0 m) indicating the wet sand and fuselage absorbed considerable energy before rolling through 270° to the left stopping upside down approximately 5 m away.
Immediately after the impact, no occupants were able to self-evacuate. All occupants were partially or fully unconscious, or fatally injured. It was reported by first responders that at some time later (within minutes) the rear left outboard and rear right outboard occupants were conscious and responsive, however the rear left outboard passenger was trapped under the wreckage.
All windscreens, windows and door pillars were fractured, allowing the roof to compress towards the floor, reducing the available space within the cabin, particularly for front row occupants. Complete reduction in space was prevented by the floor and roof, bearing onto all the seat backs.
The floor was fractured but remained substantially attached around the front right seat with the floor bent upward 20° laterally and 7° fore/aft. This was the first section of the fuselage to strike the ground.
Impact velocity
Three separate and independent methods were used to determine ground impact velocities (and where able, attitudes) of VH‑XKQ onto the sandbar. Assumptions were also used to estimate peak deceleration.
The first method used simple acceleration logic based on the height of the collision and freefall to determine a vertical velocity. The other 2 methods used features to scale the movement of the fuselage in CCTV vision of the ground impact. One angle was from the Sea World helipad CCTV looking west-south-west. The other angle was from the Gold Coast Safety Camera Network (GCSCN) Australia Fair Shopping Centre CCTV looking north-east (Figure B7).
Figure B7: CCTV vision angles

Yellow lines mark the extremities of Sea World CCTV vision. Orange lines mark the extremities of the Gold Coast Safety Camera Network Australia Fair CCTV vision. Dashed red lines indicate the lateral position of the ground impact in each frame. Source: Google Earth, annotated by the ATSB
Simple freefall analysis
The height of the collision was estimated to be 39.6 m (130 ft) above ground level. Using a simple equation of motion, the vertical component of impact velocity was estimated to be 27.9 m/s. This does not consider drag or lift forces on the descending fuselage or any other components like the rotor/transmission system that did not disconnect immediately.
The helicopter was climbing at the time of impact and would have continued upwards for a short period. Due to the angles that all footage of the collision were taken from, it was not possible to determine how much further climb occurred other than it was small (likely less than 3 m).
It also does not inform horizontal velocities or angles of impact.
Sea World Helicopters CCTV
A CCTV camera on Sea World Helicopters’ property recording at 25 frames per second (fps) overlooking some of the main heliport complex caught the moment of ground impact and 0.6 seconds prior (Figure B8). Due to the angle of vision and an awning, the midair collision was not captured.
Using motion tracking software, buildings were identified in the background for which height data was available from the internet. Motion tracking software tracked and accurately determined the 2‑dimensional position in the frame of the building and a part of the helicopter skid. Relative distances to the buildings and the impact site were used to scale the vertical and horizontal movement across the frame of the skid/fuselage over the last 0.6 seconds.
Figure B8: Sea World CCTV (with buildings used to scale from)
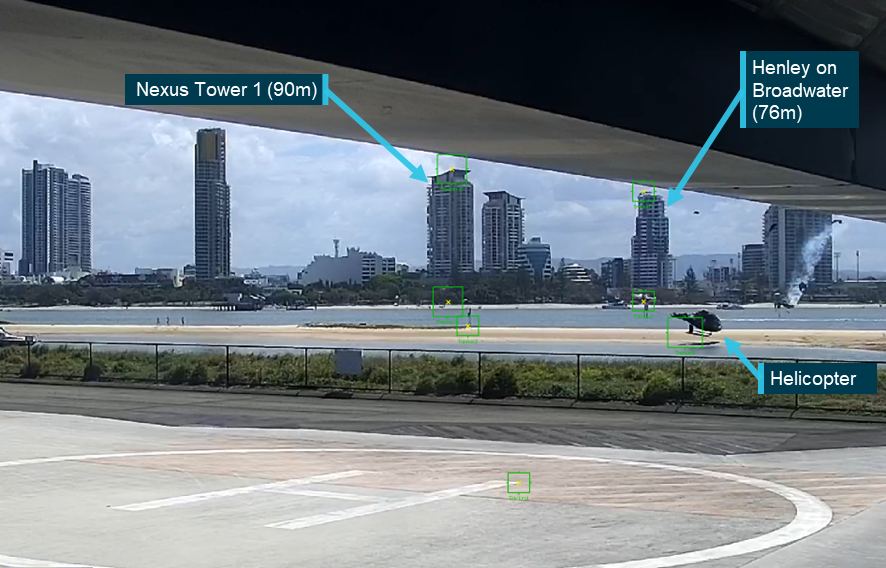
Source: Sea World Helicopters modified by ATSB
Given the relative distance to the aircraft, the fuselage was determined to be 0.084 metres/pixel. The position of the fuselage (skid) was determined over the last 11 frames and gave an average vertical velocity of 24.3 m/s.
This was more accurate than the previous method given it measured the actual velocity just before impact. It could also measure the horizontal motion across the frame. From flight tracking data, an angle of travel relative to the camera was estimated to be 56° off the camera axis (Figure B7). Correcting for this angle gave the total horizontal velocity of 17.1 m/s, resulting in an absolute velocity of 30.2 m/s. The true flight path angle at impact with the ground was determined to be 55°.
Additionally, due to the field of view and small number of pixels making up the image of the helicopter, the motion was averaged over the last 0.4 seconds to reduce errors in tracking between frames, over which time the helicopter would have accelerated vertically by around 4 m/s. Therefore, the calculated final impact velocities were likely slightly low.
Gold Coast Safety Camera Network Australia Fair CCTV
A Gold Coast Safety Camera Network (GCSCN) CCTV camera on the Australia Fair shopping centre rooftop, zoomed in on the Sea World ferry jetty complex, recording at 25 fps caught the moment of ground impact and 0.7 seconds prior. Due to the framing of the vision, the midair collision was not captured (Figure B9).
Figure B9: View of VH-XKQ just prior to impacting the sandbar
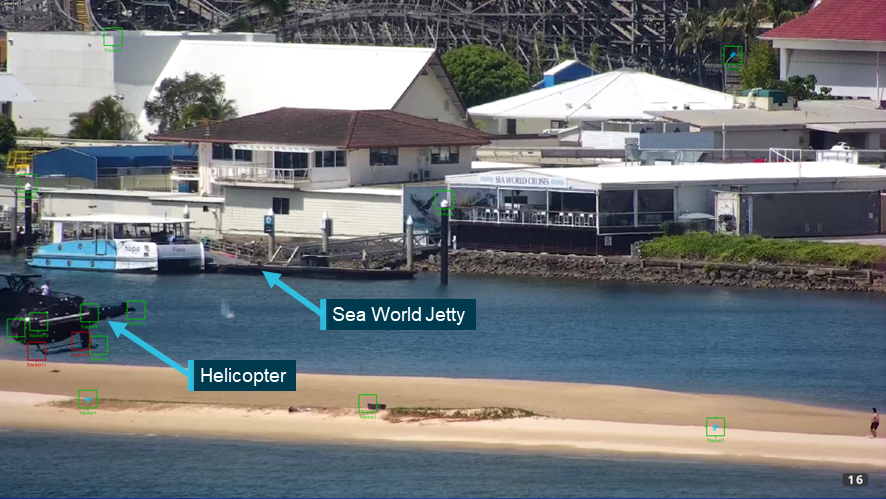
Source: Gold Coast Safety Camera Network, modified by the ATSB
Using motion tracking software, the right skid step was identified as a stable and visible source to scale off. The length of the step was used to scale the vertical and lateral movement of the landing skids and steps over the last 0.28 seconds (8 frames) and the nose and tail over the last 0.12 seconds (4 frames).
The right skid step was determined to be 0.026 metres/pixel, approximately 3 times better resolution than provided by the Sea World CCTV camera. Given the measurement was obtained from the vehicle itself, no scaling was required. The skid was not perpendicular to the camera and consequently slightly over calculated the speed of the vehicle, however, given the rate of right roll, the average skid vertical velocity would be slightly lower than the centre of mass of the cabin. The average position of 4 points on the fuselage skid were determined over the last 8 frames and the average position of the nose and severed tail were determined over the last 4 frames. The combined measurements gave an average vertical velocity of 24.8 m/s.
Horizontal motion across the frame was also determined although it was known that the helicopter was travelling more toward the camera than the Sea World CCTV. From Figure B7, the angle of travel was estimated to be 23° off the camera angle. A total horizontal velocity of 17.4 m/s was determined from the video and corrected for the camera angle. The final absolute velocity was calculated to be 30.3 m/s with an absolute flight path angle of 55°.
It is evident from the video that the helicopter impacted a rising sandbar at an oblique angle. The slope of the sandbar and the angle of the waterline relative to the helicopter’s motion could not be determined however this will have increased the angle of impact. Additionally, it was unknown how the soft sand would resist the impact of a large blunt object.
Due to the field of view and small number of pixels making up the image of the helicopter, the motion of the skid was averaged over 0.32s, over which time the helicopter would have accelerated vertically by around 3.1 m/s because of gravity. Again, the calculated final impact velocities were likely slightly low.
Peak deceleration
Excluding the freefall analysis result that only gave vertical velocity and was known to be non‑conservative, the remaining vertical and horizontal velocity calculations were averaged to give 24.5 m/s and 17.3 m/s respectively. This gave an absolute velocity at impact of 30.3 m/s.
An estimation of the deceleration of the ground impact was similarly made in a simplified form due to the lack of known terrain properties. CCTV footage captured the impact of the fuselage with the sandbar. The peak compression of the fuselage appeared to occur 2 frames after the fuselage first touched the sandbar and was calculated to be 31.2g (this is estimated because the actual contact is obscured by a small ridge of sand).
This is an average deceleration over the entire velocity change and does not consider the non‑linear response of the impact nor the rebound component. The deceleration pulse shape of a blunt object into the wet sand could not be estimated. Helicopter certification standards for occupant seating systems assume a triangular deceleration pulse and do not consider rebound. A triangular shaped deceleration pulse would result in an acceleration peak twice that compared to a constant deceleration over the same time period. Therefore, peak deceleration would appear to have been 31–62g.
Severity analysis
Given the variability and limitations of the analysis, the absolute velocity at impact was determined to be a minimum of 30.3 m/s and the flight path angle with the ground around 55°.
The orientation of the fuselage relative to the impact vector was difficult to determine due to the long focal length of the cameras and consequent lack of depth of field. It was noted from both camera angles that the fuselage rolled about its longitudinal axis after impact and only pivoted about the nose or tail. This indicates that, relative to the fuselage, there was very little longitudinal velocity.
Using the GCSCN CCTV which gave the clearest view of the fuselage orientation, the fuselage was determined to be rolled 75°–80° to the right and increasing at ~120 deg/s. The fuselage was also yawed 10° right which, given the vertical orientation, meant approximately 10° vertically down. However, it was rotating left (upwards) at 60 deg/s.
Unlike vertical velocity, the horizontal component of velocity was not completely arrested during the initial impact with the ground. While the incoming horizontal velocity components were determined from the absolute velocity and flight path angle at impact, outgoing velocity was assumed to be purely horizontal and a linear deceleration until it came to a stop. This is conservative as in actuality the helicopter rebounded (and decompressed) 0.5–1.0 m. The aircraft was observed to traverse approximately 5 m over 1 s until it stopped.
Using these assumptions and simple linear calculations, this gave a calculated velocity change during the initial impact (felt by the occupants) of 24.5 m/s vertical and 7.3 m/s horizontal, with a total velocity change of 25.6 m/s.
From this, the velocity change vector with the ground surface was estimated to be 73° and assuming the downward body axis of the fuselage was 10° off the horizon, the velocity change vector relative to the fuselage was 63° from upwards to the left (Figure B11).
The average vertical impact acceleration was determined to be approximately 31.2g. The horizontal acceleration cannot be effectively measured from the video. However, if it is assumed the horizontal velocity change occurred over the same period as the vertical deceleration, it equated to 9.3g.
Table B1 summarises the estimated velocity and accelerations for VH‑XKQ:
Table B1: VH-XKQ global velocity change and average acceleration
| Absolute | Vertical component |
Horizontal component | |
| Velocity (m/s) | 25.6 | 24.5 | 7.3 |
| Acceleration (g) | 32.6 | 31.2 | 9.3 |
Rotating these component velocities and accelerations through the same 63° about the longitudinal axis gives the following body axis components.
Table B2: VH‑XKQ body axis velocity change and average acceleration
| Source | Absolute | Downward component | Right component | Longitudinal component |
| Velocity (m/s) | 25.6 | 11.6 | 22.8 | ~0 |
| Acceleration (g) | 32.6 | 14.8 | 29.0 | ~0 |
Human tolerance to impact
Crash Survival Design Guide, Volume II, Aircraft Design Crash Impact Conditions and Human Tolerance (1989) states that human tolerance to lateral accelerations is not well understood but the limit is probably around 20 g for 100 milliseconds (ms). However, for severe lateral impacts, it is known there is an increased risk of injury for right side impacts compared to left side due to increased severity of damage to the liver (Klinich et al., 2008).
Human tolerance to vertical up acceleration (or vertical down deceleration) in a multipoint harness is better understood due to more exhaustive testing. The limit between moderate and severe injury is likely up to 45g but starts to decline higher than a 50 ms pulse duration to around 30 g for a 100 ms pulse. From video evidence, the pulse duration was likely closer to the latter of these periods.
However, comment is made that human skeletal structures, which must support most of the upper torso load, make the lumbar vertebrae susceptible to compression fracture. Additionally, spinal alignment is necessary to permit carriage of the maximum load. In this accident, the compressive load was complemented by an even larger side load likely reducing tolerance to spinal compression.
Further, vertical acceleration allows for greater displacement of the viscera[72] within the body cavity thereby increasing the susceptibility of the viscera to injuries.
Therefore, it could be concluded that while the vertical component of acceleration was probably under the limit of human tolerance, the lateral component exceeded the estimated human limit with the complication of destabilising the spine with respect to vertical compression. Hence, due to the impact vector, both axes were likely beyond tolerable limits. Limited relief would have been provided by shear distortion of the seats collapsing sideways.
Historical comparison
Analysis of Rotorcraft Crash Dynamics for Development of Improved Crashworthiness Design Criteria, (Coltman et al., 1985) provided a comprehensive analysis of impact angles, accelerations, and survival statistics of 311 helicopter accidents in the 1970s. Of those accidents, 40.1% were into soft terrain (sandy, ploughed, for example) and 9.6% had a roll angle between 76° and 90°. It should be noted that this accident did not fit the 6 principal impact scenarios identified in the analysis.
Coltman et al. (1985) plotted vertical, longitudinal, and lateral components of determined impact velocities for all accidents and noted which were survivable, partially survivable, or non-survivable. The relevant values determined by the analysis for VH‑XKQ (Table B2) were 11.6 m/s (38.1 ft/s) downward and 22.8 m/s (74.8 ft/s) lateral, with longitudinal velocity change being negligible. For lateral velocity components, data suggested that the 95th percentile survivable level is 3 m/s (10 ft/s) which is associated with typical rollover velocities, which reinforces that the VH‑XKQ impact is extraordinary. Coltman et al. (1985) coded a three-dimensional survivability velocity envelope. The lateral vertical plot is provided in Figure B10 with the impact velocity components for VH‑XKQ also plotted. The calculated impact velocity for VH‑XKQ was at least 3 times more extreme than the next most severe partially survivable accident documented. By comparing the values of the plotted point to the 95th percentile survivable accident curve, it can be argued that the VH‑XKQ ground impact was at least 7 times more severe than the 95th percentile survivable accident.
It should be noted that this data is based on aircraft accidents when lap belts were prevalent for passenger seats in helicopters and that the 95th percentile survivable curve would be expanded if it only considered accidents with occupants restrained by 4-point restraints. This is also suggested by Coltman et al. (1985).
Figure B10: Lateral vertical survivability envelope of helicopter accidents (VH‑XKQ identified by red triangle)
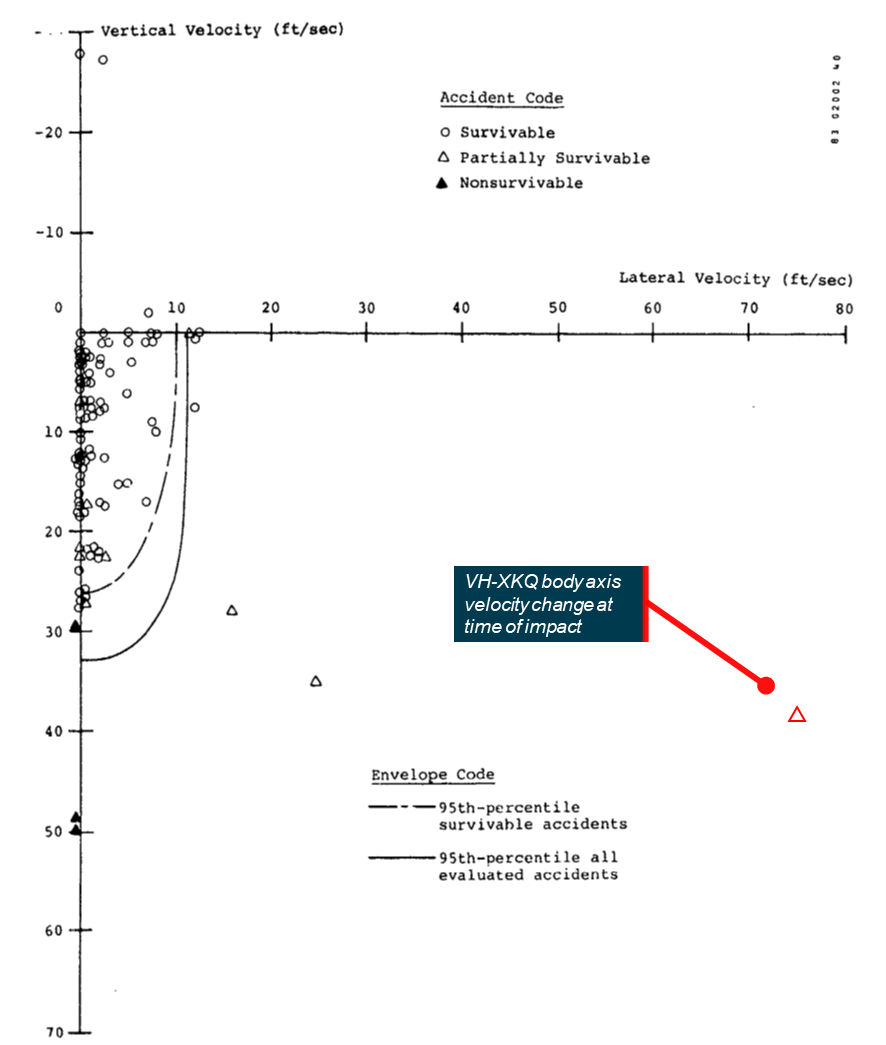
When VH‑XKQ impacted the ground, the lateral vertical velocity was at least 7 times more severe than the 95th percentile of historical survivable accidents. The accident was at least 3 times more extreme than the next most severe partially survivable accident documented. Source: Analysis of Rotorcraft Crash Dynamics for Development of Improved Crashworthiness Design Criteria, 1985, annotated by the ATSB
Summary of VH‑XKQ impact analysis
Three methods were used to estimate final vertical and absolute velocities. There was some correlation between methods, or where there wasn’t, the difference was readily explainable. The absolute final velocity could not be determined outright but a reasonable estimate was derived.
The vertical impact velocity was estimated to be approximately 24.5 m/s and the absolute impact velocity was estimated to be over 30.3 m/s (99 ft/s, 109 km/h). The flight path angle at impact was around 55° into a slightly upsloping sand bank. Peak vertical deceleration was likely to be around 50–60g in a highly lateral direction with average deceleration above 30g.
Table B3: Calculated velocity of VH‑XKQ at impact
| Source | Vertical velocity (m/s) |
Absolute velocity (m/s) | Angle of impact (deg) |
| Freefall analysis | 27.9 | - | - |
| Sea World CCTV | 24.3 | 30.2 | 55 |
| GCSCN Australia Fair CCTV | 24.8 | 30.3 | 55 |
The impact was obliquely into a gently up sloping wet sandbar that caused the fuselage to dig in with minimal rebound. It bounced to a height of roughly 0.5–1.0 m and rolled over approximately 270° traversing only around 5 m.
Orientation was determined visually to be approximately 80° rolled right with the longitudinal axis less than 10° nose down. The impact/direction vector relative to the body axis is complicated by the lack of precise measurements and by the fact the horizontal velocity did not immediately reduce to zero (Figure B11). However, it could be observed to be predominately laterally right followed by a not insignificant down (z axis) component. Any longitudinal component was minimal in comparison.
Figure B11: Visualisation of the impact vector (red), reaction vector (green) and components relative to the helicopter body axis

Source: 3dcadbrowser.com, annotated by ATSB
The impact was compared to historical data on rotorcraft crashworthiness and survivability. The impact was determined to be at least 7 times more severe in magnitude than that considered to be 95th percentile survivable.
Seat and seatbelt damage
The following is a record of assessed damage to the seats.
VH-XH9 seats damage
Apart from minor shrapnel damage, all seats were serviceable. All safety harnesses were functional.
VH‑XKQ seats damage
The impact deceleration for VH‑XKQ was determined to be 50–60 g peak, with the largest component being a dynamic lateral (sideways) loading averaging about 29 g which was much higher than the 8 g static certification load case.
All seats sustained similar amounts of damage (Figure B12). Typical features of the seat post‑accident included:
- the seats had substantial shear distortion to the right
- the seat legs were mostly undeformed
- the seat pan linkages on each side of the seat were bent to the right
- all seat legs remained attached to the seat tracks
- all seat tracks remained attached to the floor (front row) or plinth (second row)
- seat legs and integrated track slots rolled right with the seat track permanently set
- the seat bucket in the right leg slot fully stroked[73]
- the seat bucket in the left leg slot not stroked or partially stroked
- the composite seat bucket was intact and undeformed (except for right seats)
- seat pan and seat back cushions were in place and undamaged
- seatbelt harnesses attached to the seat
- 6 buckles were attached to right lap belt, 1 was free
- buckles released the webbing tangs when rotated
- inertia reels freely retracted and locked if pulled sharply (except as noted below in Injury assessment).
- the cabin ceiling had compressed onto the seats.
- the floor structure around the front right seat, and to a lesser extent around the rear right outboard seat, had failed longitudinally due to lateral compression.
Figure B12: Composite picture of typical seat damage

Source: ATSB
Seatbelt damage
All safety harnesses were removed from the helicopter and disassembled and analysed in the ATSB’s laboratory. Apart from some stiffness/binding due to post-accident corrosion, all harnesses were found to be serviceable and functional.
The seatbelt webbing of the right rear inboard seat was cut at the right lap belt adjuster. However, it did not fail completely (Figure B13) and was possibly caused by being caught between the seat bucket and that of the adjacent seat as they moved relatively.
Figure B13: Rear right inboard seat right lap belt
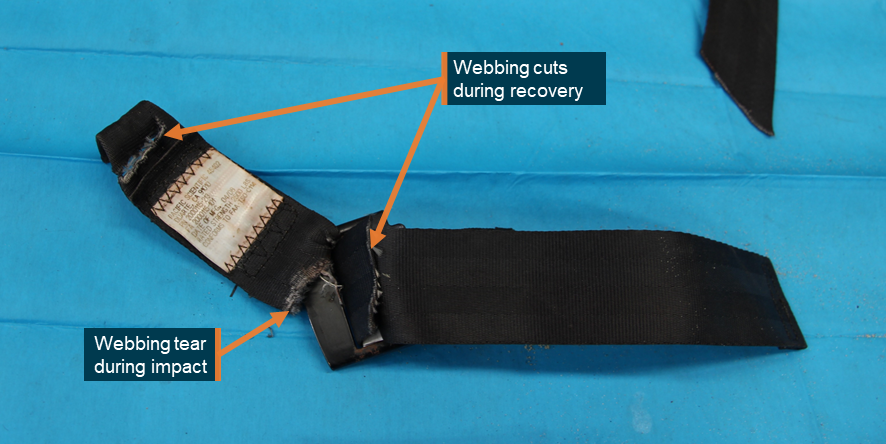
Source: ATSB
Injuries
Data provided
A full autopsy report was received for the pilot of VH‑XKQ while coronial certificates were provided for deceased passengers. Hospital discharge reports for surviving passengers of VH‑XKQ were reviewed along with progress notes for the pilot of VH‑XH9.
Assessment methodology
All medical reports were reviewed for key details and a simplified plain English summary generated. Additionally, all reports were assessed against the Association for the Advancement of Automotive Medicine’s Abbreviated Injury Scale and Injury Severity Score systems. Finally, the Glasgow Coma Score was noted where it was recorded.
Injury assessment
Of the occupants of VH‑XH9, the pilot and 2 front row passengers received serious injuries, principally peppering skin damage from flying acrylic, which required hospitalisation for more than 48 hours. In interview the pilot advised that their sunglasses had been instrumental in ensuring that their eyes were protected from the flying acrylic.
For VH‑XKQ, the injuries to the pilot, front middle, and rear right inboard fatally injured passengers were consistent high right lateral deceleration and right-side blunt force trauma. The pilot and front middle passenger injuries were likely exacerbated by the partial collapse of the roof structure providing reduced survivable space.
The fatal injuries to the passenger seated in the front right seat were different to the other fatalities and are not consistent with a high right lateral deceleration. Injuries were to the left side of the torso and fore/aft compression of the pelvis.
The injuries of rear right outboard and front right passengers were likely exacerbated by excessive flail permitted by ill-fitting or partially released harnesses and the lack of cabin protection when the doors came off the fuselage. The front right passenger, retained only at the waist, flailed completely outside the fuselage during rollover. A mobile phone video recording during this time confirmed the occupant’s shoulder harness had disconnected (Figure B14).
Figure B14: Front right seat shoulder harness disconnected during rollover
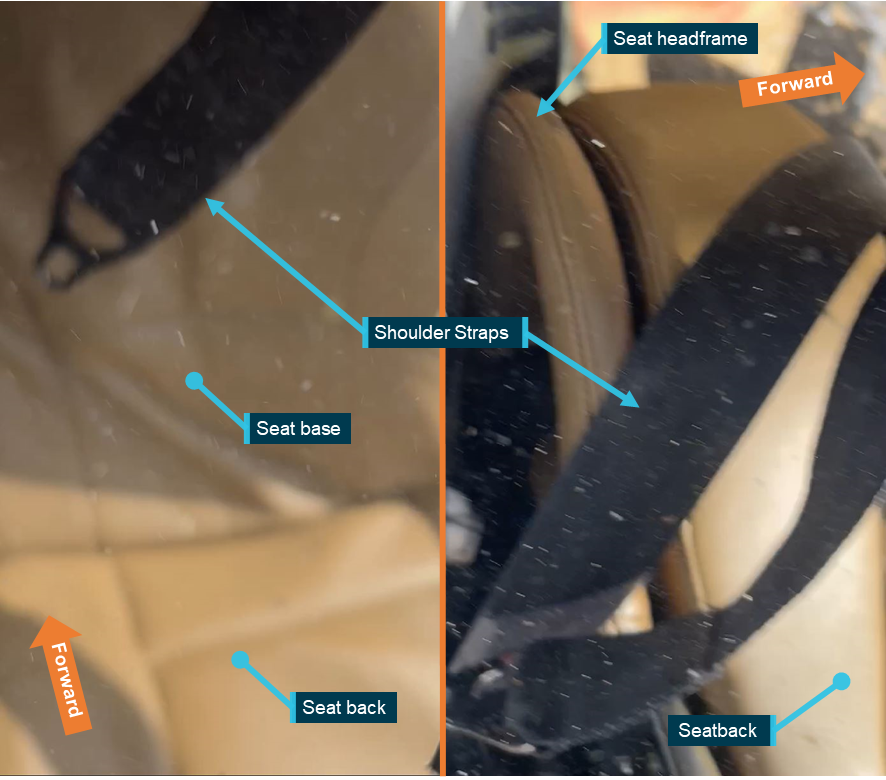
Source: Passenger video on board VH-XKQ, annotated by the ATSB
At the same time, the rear right outboard passenger, who was seriously injured, appeared to be restrained by the chest with no waist level restraint evident. Their legs, but not their torso, flailed outside of the fuselage. That passenger received a burst lumbar vertebra and abdominal injuries which may be the result of forced flexion about the abdomen. This passenger also received numerous severe open leg fractures.
The rear left inboard passenger received no injuries below chest level. Given the severity of the impact, with no pelvis level bruising or fractures, a possibility is the right lap belt disconnected from the buckle. This belt is normally permanently attached to the buckle but was found separated post-accident and remains unexplained after buckle examination. It was observed through internal video that this passenger at the beginning of the flight had a poorly fitted restraint with the buckle not down low across the pelvis. The child passenger, who was seriously injured, was sat between 2 adults which likely limited their ability to flail.
Based on reports from first responders, the rear left outboard passenger, who was seriously injured, was found external to and under the fuselage when it came to rest. The fuselage resting in soft sand may have conformed to the passenger’s body, thereby relieving some of the pressure from the fuselage. Additionally, structures would appear to have not borne directly onto the passenger’s chest, the weight of which would have severely restricted the ability to breathe.
Location and extrication of the injured rear left outboard passenger
A Queensland Fire and Emergency Services (QFES) response and extrication report identified the extraction of a person subsequently identified as the rear left outboard passenger (described above). The passenger was located outside and underneath the helicopter wreckage, when they should have been restrained by their harness and seat and remained within the cabin (Figure B15).
Figure B15: VH-XKQ – location of the rear left outboard passenger

Source: QFES, annotated by QFES and the ATSB
QFES extricated the passenger towards the rear after cutting a door frame (Figures B16 and B17). Specialist equipment was required to access the passenger and their extrication ‘was impeded by what appeared to be the top of a door frame protruding up from beneath the top of the overturned airframe in the sand’. The door was subsequently identified as being the rear left passenger cabin door that the passenger was sitting next to.
Additionally, the QFES report indicated the constant wear lifejacket had to be cut away using a rescue knife (Figure B16). The passenger in interview recalled their safety harness being cut. The passenger’s safety harness was found to be undamaged and could not have extended to the position where the passenger was found trapped. Therefore, it was likely the passenger had recalled the lifejacket strap being cut as opposed to their safety harness. This also meant the safety harness likely inadvertently released at some time during the accident sequence.
Figure B16: VH-XKQ – site of rear left outboard passenger
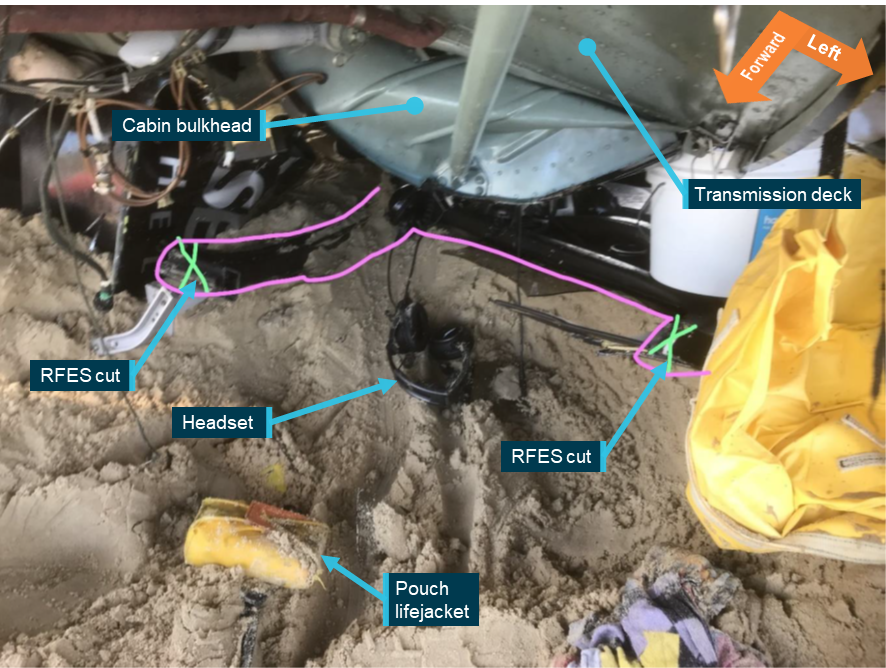
Source: QFES, annotated by QFES and ATSB
Figure B17: VH-XKQ rear left cabin door

Source: ATSB
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Eurocopter became Airbus Helicopters in 2014. The Eurocopter EC130 series is now sold as the Airbus Helicopters H130.
[2] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[3] Constant wear lifejacket: an uninflated lifejacket worn about the person in a pouch or harness for the duration of the flight.
[4] Sea World grass: an open area to the south of the Sea World theme park, used by local helicopter operators to cross the coast without overflying buildings.
[5] En Route Supplement Australia is published by Airservices Australia and contains vital operational information for pilots operating in Australian airspace.
[6] Sea World Helicopters nominated their flights Tours 1 and 6 – 5 minutes, Tours 2 and 7 – 10 minutes, Tours 3 and 8 – 15 minutes.
[7] Sleep opportunity: a period of time during an off-duty period when a pilot is not meeting the reasonable requirements of bodily functioning such as eating, drinking, washing or dressing, and has access to suitable sleeping accommodation without being interrupted by any requirement of their employer.
[8] Psychomotor skills refer to the coordination of perception and action and require either complex perceptual discrimination or a complex motoric response (Chaiken and others, 2000).
[9] Air transport replaced the term charter and is conducted for hire or reward.
[10] A maintenance release (MR) (CASA Form 918) is required to be carried on an aircraft as an ongoing record of the aircraft’s time-in-service. It is also used to record and communicate the airworthiness of an aircraft between registered operators, pilots, and engineers. It included a section (Part 2) for defects and/or maintenance activities, to be recorded (and cleared), and a section (Part 3) to record daily inspections and flight hours. Subject to conditions, the MR for the EC130 is valid for a set period, 150 hours in service or 12 months from issue.
[11] Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[12] One camera was located on the left horizontal stabiliser and looking forward. Three cameras inside the cabin, one looking forward through the windshield, one looking forward and slightly to the side from pilot’s chin window and one facing aft to capture the pilot and passengers.
[13] OzRunways base map can display a range of layers including various aeronautical charts, maps and satellite imagery depending on user preference.
[14] An Airworthiness Bulletin (AWB) is an advisory document that alerts, educates and makes recommendations about airworthiness matters. Recommendations in these bulletins are not mandatory. https://www.casa.gov.au/aircraft/airworthiness/airworthiness-bulletins
[15] The button switch does not latch and is therefore only selected when the button is depressed.
[16] Salience: the quality of being prominent or noticeable.
[17] Foveal region: the area of maximum visual acuity and where objects are most likely to be detected.
[18] The candela (cd) is the unit for luminous intensity of the International System of Units (SI). It measures the luminous power emitted by a light source. One candela is roughly equivalent to the luminous intensity of a wax candle.
[19] Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[20] Flicker vertigo: Disorientation or nausea caused by low frequency flickering.
[21] Mode C: A transponder mode that encodes the radar response to include aircraft pressure altitude.
[22] Whisper-shout: A method of controlling synchronous garble from Mode A/C transponders through the combined use of variable power levels and suppression pulses (ICAO document 9863).
[23] From 12 August 2022 the Australian government provided grants to increase the uptake of ADS-B equipment in Australian-registered aircraft to improve safety and efficiency for Australian airspace users (ADS-B rebate program).
[24] Flight information service broadcast (FIS-B): A service that provides pilots with free weather and flight information directly to their cockpit via ADS-B, enhancing situational awareness.
[25] Traffic information service broadcast (TIS-B): A service that relays traffic information to ADS-B equipped aircraft which helps pilots to identify nearby aircraft not broadcasting ADS-B signals.
[26] Automatic dependent surveillance rebroadcast (ADS-R): A service that retransmits ADS-B position data between aircraft on different ADSB frequencies, ensuring all aircraft have traffic information regardless of frequency differences.
[27] Rotor disc is the area or plane being swept by the main rotor blade system at any point in time.
[28] The transponder can be selected to STBY (standby), where the transponder will not respond to any interrogations, ON, where the transponder replies to interrogation but with no altitude information or ALT (altitude) where interrogation replies include altitude information.
[29] A BNC (Bayonet Neill-Concelman) connector is a quick connect/disconnect radio frequency connector used for coaxial cables and is designed to maintain the same impedance of the cable.
[30] Mathematical principle used to estimate the actual value of a variable based on a noisy data set.
[31] Published as a separate report – Cockpit visibility study supporting AO-2023-001 – Midair collision involving Eurocopter EC130 B4, VH-XH9, and Eurocopter EC130 B4, VH-XKQ, Main Beach, Gold Coast, Queensland, on 2 January 2023 (AS-2023-001).
[32] ICAO Annex 13 establishes the standards and recommended practices for accident investigations by states (countries) and coordination between them.
[33] An equirectangular image is where a 360-degree image is projected onto a flat 2D surface with equal azimuth and elevation angle.
[34] fpm – feet per minute.
[35] Antenna components were removed from XKQ on 26 February 2024.
[36] VSWR is ratio that measures how efficiently radio frequency power is transmitted from a power source, through a transmission line (in this case the coaxial cable), to an antenna.
[37] BNC: Bayonet Neill–Concelman is a coaxial cable connector commonly used in radio applications.
[38] Sealant is typically applied over the join between external components and provides a flexible barrier to prevent moisture ingress across variable environmental and operational conditions. This barrier protects against the formation of corrosion.
[39] Micro-computed tomography (CT): a non-destructive technique for producing high-resolution 2- and 3-dimensional cross-sectional images of an object from flat x-ray images. Characteristics of the internal structure of an object such as dimensions, shape, internal defects, and density can be obtained from micro-CT images.
[40] Micro-CT examination of the VHF Com 1 antenna components was initially completed at the ANU CTLab on 17 June 2024, and then repeated on 30 August 2024 at the conclusion of Chelton’s electrical testing.
[41] Destructive examination of the antenna base was completed on 10 September 2024.
[42] Potting compound: the base of the antenna was filled with an insulating plastic which sealed and protected the circuit board.
[43] Impedance is opposition to a current, and matching balances the source and load to maximise power transfer.
[44] Shanahan DF. Human tolerance and crash survivability. RTO HFM Lecture Series on Pathological Aspects and Associated Biodynamics in Aircraft Accident Investigation. Madrid, Spain. 2004.
[45] Tang: a long and slender projecting strip, tongue, or prong forming part of an object and serving as a means of attachment to another part, as commonly found in automotive seatbelts for insertion into the buckle.
[46] Stroked: the complete movement of a moving part in one direction.
[47] Pacific Scientific Co was purchased by Meggitt PLC in 2011.
[48] Federal Aviation Authority. Technical Standard Order TSO-C114, Torso restraint systems. Retrieved from Cabin Safety Technical Standard Orders | Federal Aviation Administration (faa.gov)
[49] Airbus Helicopters Safety Information Notice (SIN) 3444-S-25 Correct use of restraints to minimise the risk of injury
Civil Aviation Safety Authority Multi-Part Advisory Circular (AC) AC 133-10 – Passenger Safety information
Federal Aviation Administration Advisory Circular 91-65 Use of shoulder harnesses in passenger seats
Federal Aviation Administration Seatbelts and shoulder harnesses – smart protection in small aircraft (2020)
Transport Canada AC 605-004 (3) Use of safety belts and shoulder harnesses on board aircraft
Transport Canada AC 700 036 (1) Brace for impact positions for all aircraft occupants
[50] The solar position calculator gives azimuth and elevation angles relative to a position on the earth’s surface, the minor variation with aircraft altitude can then be trigonometrically accounted for.
[51] Aeronautical Information Package: A document produced by Airservices Australia, which consolidates the rules and requirements of piloting aircraft in Australian airspace.
[52] Mandatory Broadcast Area: A defined airspace volume in Class G airspace within which certain mandatory radio broadcasts are required on a common frequency, and within which all operations must be monitoring the published common frequency. (CASA: AC 91-10v1.2)
[53] Forced landing area: An area of ground is a suitable forced landing area for a flight of a rotorcraft if the rotorcraft could make a forced landing in the area with a reasonable expectation that there would be no injuries to persons in the rotorcraft or on the ground (CASR 133.010).
[54] In line with CASR 91.410(3) the heliport and park pad at Sea World meet the definition of non-controlled aerodromes.
[55] Vortex ring state: a condition of powered helicopter flight that causes a loss of lift in the rotor system if the helicopter descends into this downwash.
[56] Short final: a phrase which describes an aircraft’s position in the circuit as on the final approach path and near to the touchdown point.
[57] VFR approach point: a specified geographical location in relation to which the position of an aircraft can be reported.
[58] Manifest: a record of passengers and baggage required to be carried on air transport flights.
[59] Civil Aviation Safety Authority. (2023). Advisory Circular AC 91-21, ADS-B for enhancing situation awareness. Accessed from casa.gov.au.
[60] Foreign object damage (FOD): damage caused to an aircraft by contact with loose items. Helicopters are susceptible to ingesting items lifted by rotor wash through the rotor system.
[61] External audit: often referred to as a 2nd party audit. It is ordinarily for an organisation to oversee their suppliers and service providers.
[62] Airmanship: in advisory circular AC 91-14v1.0 Pilots’ responsibility for collision avoidance the Civil Aviation Safety Authority defines airmanship as the consistent use of good judgement and well-developed knowledge, skills and attitudes to accomplish flight objectives.
[63] Internal audit: often referred to as a 1st party audit. It is ordinarily conducted by the organisation itself to manage conformance to its own processes.
[64] Safety occurrences reportable to the ATSB are outlined in the Transport Safety Investigation Regulations.
[65] Quantitative risk assessment is also known as probabilistic risk assessment and risk is calculated by computing probabilities of events, scenarios and outcomes (Aven, 2019).
[66] JIACC refers to the Argentina Civil Aviation Accident Investigation Board.
TSB refers to the Canadian Transport Safety Board.
NTSB refers to the US National Transportation Safety Board.
TAIC refers to the New Zealand Transport Accident Investigation Commission.
AAIB refers to the UK Air Accident Investigation Branch.
[67] Various control inputs are possible for avoiding action, 2.5 s was chosen as a reasonable input and aircraft response time to result in avoidance.
[68] In some operations and especially aerial work, trained and briefed passengers can form part of the defences against collisions.
[69] Research has shown that pilots experience greater levels of workload during the take-off and landing phases of flight, and lower levels during the cruise. During take-off and landing, pilots have been found to engage in more frequent eye movements (Di Nocera and others, 2007), and experience greater levels of neurological activity (Di Stasi and others, 2015).
[70] CP: Chief pilot, otherwise referred to as head of flight operations (HOFO)
[71] VSWR is a measure of how efficiently radio-frequency power is transmitted from a power source, through a transmission line (in this case the coaxial cable), to an antenna.
[72] Viscera – the internal organs in the main cavities of the body, especially those in the abdomen.
[73] Stroke: seats fitted to EC130 helicopters have a mechanism that allows the seat pan to move (stroke) in a controlled manner relative to the seat frame during a vertical (upright) impact with the ground thereby decelerating the occupant over a greater distance reducing peak forces on the occupant’s spine.