
This investigation was conducted under the Transport Safety Investigation Act 2003 (Commonwealth) by the Office of Transport Safety Investigations (NSW Government) on behalf of the ATSB in accordance with the Collaboration Agreement. Released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Safety summary
What happened
At approximately 0407 on 8 January 2021, freight train 5936, travelling in the up direction (towards Sydney) failed as a result of wheel slip, on the steep Cowan bank inside Boronia tunnel No. 3. To keep the up main line clear the train crew were directed by Sydney Trains network control to propel1the train backwards into Hawkesbury River up refuge siding.
Network rules for propelling trains require crew to direct the movement from the rear of the train via radio communication with the driver. Due to the terrain, the assistant driver and a trainee were required to walk to the rear of the train on the adjacent down main line, as there was no alternate pathway beside the track. To protect these workers from passing trains, the driver of 5936 requested track protection from the Sydney Trains signaller. This protection was provided in the form of rail signals placed to stop to prevent a train from entering the section of track where the workers were walking.
On arrival at the rear of the train the two workers and the driver of 5936 proceeded to propel the train back towards Hawkesbury River up refuge siding in accordance with procedures, with the two workers walking in advance of the train on the adjacent down main line. During the propelling movement the workers observed the lights of an oncoming train on the down main line on which they were walking. The two workers told the driver of 5936 to stop the propelling movement and the train was brought to a stand. The workers jumped clear of the oncoming train onto the adjacent cess area, with one of the workers suffering an injury. A passenger train, 247B, passed the workers, travelling around train 5936 in the up direction towards Sydney on the down main line.
The driver of 5936 contacted the Sydney Trains signaller and requested an explanation about why a train had been permitted to run on the down main while there was meant to be a signal block in place to protect the workers.
The Sydney Trains signaller told the driver the signal block had been removed once the propelling movement started, due to the signaller mistakenly thinking the workers were clear of the down main line. The incident was not reported at the time by the Sydney Trains signaller. The incident was reported by the driver of 5936 to their control centre, but it was not acted on at the time. The incident came to notice when the trainee worker reported an injury resulting from jumping out of the way of train 247B.
What the ATSB found
The Sydney Trains signaller and the driver of train 5936 did not observe the requirements of the relevant Train Working Network Rules and Procedures for protecting workers on track with in-service rail traffic, specifically rule NTR 432, Protecting activities associated with in-service rail traffic and associated procedure NPR 750. The Sydney Trains signaller and the driver of train 5936 did not observe the relevant safety critical communications requirements during the application and removal of the protection. The Sydney Trains signaller placed blocks on the signals manually as if protecting an emergency situation or Condition Affecting the Network and did not use the electronic forms as required under NTR 432 and NPR 750. The Sydney Trains signaller removed the signal block protection without confirmation from the driver of train 5936 that the workers were clear of the danger zone as required by NTR 432 and NPR 750.
The Sydney Trains signaller did not understand the details of the tasks required for propelling movements, was not familiar with the terrain, and assumed the workers were clear of the down main line once the propelling movement had commenced. Sydney Trains signaller safeworking refresher training, which may have identified a knowledge gap or non-compliance with procedures, has not been in place since 2009.
The application of signal blocks was not compliant with NTR 432 and NPR 750. Sydney Trains assurance and audit processes for signal box management did not detect the non-conformances. The signaller did not report the incident as per General Rule NGE 234, Responsibilities of Signallers. Cowan bank is a known problem area for failed freight trains. Rail lubricators were overactive and delivering too much lubricant to the rail surface, contributing to the likelihood of a train becoming disabled. Lack of breathing apparatus in train 5936 meant the driver was exposed to diesel fumes in Boronia tunnel 3 for a considerable time while organising and performing the propelling movement.
What has been done as a result
Sydney Trains delivered the following actions following the occurrence:
- Issued two Safe Tracks alerts to reinforce the requirements of Network Rule NTR 432, Protecting activities associated with in-service rail traffic, and related procedure NPR 750.
- Issued an Operating Instruction 02/2022 to staff who manage this type of incident that deals specifically with propelling movements on Cowan Bank.
- Adjusted the rail lubricators on Cowan Bank to provide optimum balance between lubrication of the rails while still permitting the train to retain traction on the rail surface.
- Reintroduced Safety Refresher Training for signallers.
- Delivered to all signallers an e-learning course on the use of NTR 432.
- Use of NTR432 will be added to Signaller Competency assurance scenarios and the next annual round of Safety Refresher Training commencing during 2023.
- Line managers have been required to focus safety engagements, undertaken with signallers, on ensuring signaller understanding of NTR 432. If non conformances are identified remedial coaching/training will be undertaken with the signaller.
- From 18 November 2022 all Signallers have been instructed to report each use of NTR432 to their line manager and line managers have been instructed to submit an audio compliance request for all reported uses of NTR432 for a compliance review.
- A communications cue card on use of NTR 432 for Signallers and Rail traffic crew was developed and distributed and is published on the RailSafe website.
- A review of the network hazard of instance of worker in path of rail vehicle (protecting activities associated with in service rail traffic) is currently being undertaken.
Transport for NSW delivered the following action following the occurrence:
- Assisted Sydney Trains through the provision of project support and vendor engagement for the design and development of safety refresher training.
Safety message
To provide confidence that rules and procedures are being followed and that they are effective in managing relevant risks, rail operator assurance processes need to detect non-conformances.
Training and competence management regimes for rail safety workers need to provide relevant and meaningful content, such as scenario-based training, and site based network familiarisation, to allow workers to perform safely and effectively.
The occurrence
Overview
At approximately 0407 on 8 January 2021, Pacific National (PN) freight train 5936, travelling in the up direction (towards Sydney) failed as a result of wheelslip inside Boronia tunnel No. 3 while travelling on the steep grade on Cowan bank. Following discussion between the Signaller Hornsby North (SHN) located in the Homebush Control Centre (HCC) and the Train Service Delivery Manager Central Coast (TSDMCC) located in the Rail Operations Centre (ROC), the train crew were directed to propel the train backwards into the Hawkesbury River Up Refuge siding in order to keep the up main line clear.
Two members of the train crew, the assistant driver and a trainee assistant driver were required under the network rules for propelling trains to walk back along the length of the train to the last vehicle in order to direct the propelling movement. Because of the terrain and lack of a safe place beside the track the two workers needed to walk on the adjacent down main line. In order to protect these workers, the driver of 5936 requested protection from the SHN. This protection was provided in the form of rail signals placed to stop to prevent a train from entering the area.
While the workers made their way to the rear of the train, the driver of 5936 reported at interview that they were suffering the ill effects of diesel exhaust inhalation as the leading locomotive was inside Boronia tunnel No. 3 and exhaust fumes had built up in the tunnel and entered the cab. There was no breathing apparatus available to the driver on board to assist with managing this situation.
Once the two workers were in position at the rear of the train, the driver of 5936 confirmed with the SHN that the route was set for the movement and proceeded to propel the train backwards, under the direction of the two workers, towards Hawkesbury River Up Refuge siding. As the two workers were walking in advance of the train on the adjacent down main line, they observed the lights of an oncoming train. The two workers told the driver of 5936 to stop the propelling movement and the train was brought to a stand. The workers jumped clear of the down main onto the adjacent cess area, with one of the workers suffering an injury.
A passenger train, 247B, passed the workers on the down main, travelling in the up direction around train 5936. The driver of 5936 contacted the SHN and requested an explanation from the signaller about why a train had been permitted to run on the down main while there was meant to be a signal block in place to protect the workers.
The SHN told the driver the signal block had been removed once the propelling movement started, mistakenly thinking the workers were clear of the down main line. The signaller was not familiar with either the propelling procedure or the network terrain and was not aware that the workers were still walking adjacent to and in front of the propelling freight train, as they are required to do under the Sydney Trains Network Rules. The incident was not reported at the time by the SHN. The incident was reported by the driver of 5936 to their control centre, but it was not acted upon at the time. The incident came to notice when the trainee worker reported an injury resulting from jumping out of the way of train 247B.
Context
Train information
Train 5936 consist
Train 5936 was a Pacific National freight train hauling grain from Moree Wheat Silo to Bomaderry. It consisted of four 82 class diesel electric locomotives (8214, 8213, 8244, 8232) hauling a consist of 52 loaded wheat hopper wagons (25 x NGKF wagons and 27 x NGPF wagons).
The train length was 831.6 m and the mass was 4134 t.
Figure 1: 82 class Pacific National locomotive

Source: Pacific National
Train 5936 journey
Train 5936 departed Moree Wheat Silo on Thursday 7 January 2021 at 1230. There was a crew change at Morandoo at 0030 on Friday 8 January 2021. The incoming crew consisted of a driver, an assistant driver and a trainee assistant driver.
Train 247B
247B was an eight car OSCar NSW TrainLink passenger service operating from Newcastle to Central.
Train crew information 5936
Driver
The driver was an employee of Pacific National with 21 years and four months experience. The driver possessed the requisite qualifications to operate the type of train and to operate over the route. They were trained in protection arrangements for in-service rail traffic in 2016.
Assistant driver
The assistant driver was an employee of RailTrain, a rail labour hire company with a contract with Pacific National, with four months experience. The assistant driver possessed the qualifications to be a second person but did not possess the requisite qualifications to operate the type of train over the route. The assistant driver was trained in protection arrangements for in-service rail traffic in September 2020.
Trainee assistant driver
The trainee assistant driver was an employee of RailTrain with three weeks experience. The trainee assistant driver did not possess the requisite qualifications to be a second person or operate the type of train over the route. The trainee assistant driver was trained in protection arrangements for in-service rail traffic in December 2020.
Signaller information
The SHN advised they were first qualified in signalling in 2002, however Sydney Trains could not locate any signaller training records for this worker until 2007. The SHN had worked at a variety of signal boxes and control centres including Penrith, Springwood, Auburn, Katoomba, Blacktown, and a number of control panels in the Homebush Control Centre.
Signaller performance
Between 2015 and 2021 the SHN had received coaching, counselling or retraining, post incident on 18 separate occasions. These incidents included:
- Faulty manipulation of signalling equipment that resulted in delays
- Misrouting of trains
- Incorrect setting of train route
- Delays in setting of routes.
The most serious incident involved an occurrence at Penrith where the SHN had allowed a freight train to enter a section that was subject to Block Working. Block Working is an operational method where rail traffic is not permitted to enter a section until previous rail traffic is reported as clear of the block ahead. In this case it was a set of track machines that do not operate signalling track circuits like a train. To secure their safety, these machines operate under Block Working conditions.
Allowing a following train to enter the section without ensuring the track machines were clear of the block ahead ran the risk of a collision.
Signaller training
The SHN held all the necessary safeworking qualifications to operate the Hornsby North panel at HCC. Sydney Trains manages the safeworking certification and qualifications arrangements for rail safety workers through two standards, the Network Rules and Network Procedures Certification Standard, and the Network Rules and Network Procedures Training Standard.
Each standard contains a matrix of information. The Certification Standard details those competencies applicable to each role and assigns a code to that role. The code is then expanded upon in the Training Standard that details the specific Rules and Procedures applicable to that role, and what must be contained in the training package for that role.
The code for a signaller is C105, Control Rail Traffic Movements level 1. For the code C105, a training package must contain instruction in 51 Network Rules, 39 Network procedures and how to complete 10 different Network Forms. The training package for signallers includes the Train Working Network Rules for propelling trains, NTR 424, and protecting activities associated with in-service rail traffic, NTR 432.
Each Rule, Procedure and associated forms may have several individual requirements, so the knowledge requirement for a signaller runs into several hundred individual steps, processes and tasks.
In addition to the Network Rules and Network Procedures, Sydney Trains has other operating requirements known as Operator Specific Procedures, Special Instructions and General Orders. The signaller role training requirements in these procedures, instructions and orders are not captured by the Network Rules and Network Procedures training process.
A signaller must have current knowledge and competency in a large array of rules, procedures, instructions, and orders to perform safely and efficiently.
Localised training and assessment
Each signal control panel in the Sydney Trains network has its own Localised Training and Assessment (LTA) process. The LTA for Hornsby North panel does not include scenario-based training to deal with a failed train on Cowan Bank, despite it being a common occurrence, nor any network familiarisation training to ensure that signallers can visualise the network they are managing.
Network Control
Rail Operations Centre (ROC)
Sydney Trains has a centralised control room called the Rail Operations Centre (ROC) where a number of functions are co-located. The functions include train control and supervision, incident management, customer information, security and infrastructure control. Working within the ROC are Train Service Delivery Managers (TSDM) and Network Incident Managers (NIM) who work with signallers, train crew and others to manage train operations, work on track and other functions.
Train Service Delivery Manager (TSDM)
TSDM is the Sydney Trains business term used for what is referred to in the Sydney Trains Network Rules and Procedures as the Network Controller. TSDM are responsible for train running, planned possessions and planned work on track authorities. There are five TSDM areas, Central Coast, North, Main, Illawarra, and South West.
The TSDM principally involved in this incident was the TSDM Central Coast. The TSDM Central Coast is described as the TSDMCC in this report.
|
ATSB observation The role description for the TSDM does not have mandatory requirements for rail safeworking or train operations qualifications or experience. These are listed as desirable criteria. However, the TSDMCC was responsible for train running, and safeworking decisions such as the train movement to Hawkesbury River Up Refuge. |
Figure 2 Rail Operations Centre (ROC) control room

Source: Sydney Trains
Signal box operations
Sydney Trains has a number of small signal boxes and larger control centres in the network where signallers control the trackside signals to give proceed authorities[1] for trains to operate. Signallers also provide protection for workers doing maintenance and other activities, such as train crew attending to their train while in service.
Signallers do this by putting signals to stop and applying blocking facilities[2] to prevent them from being cleared, thereby excluding trains from entering the area where work is occurring. There are several Network Rules and Procedures that govern this activity.
Assurance and oversight of signallers is undertaken by Signal Box Operations (SBO), who provide line management functions and ensure operational requirements are delivered safely and in accordance with the relevant rules, procedures and standards. This assurance activity can take the form of:
- review of recorded audio to check compliance with communications protocols and application of rules and procedures
- review of applicable forms and documents to ensure that details have been completed as required
- review of similar incident types to check on outcomes and application of standard requirements.
SBO is an operating section of the Sydney Trains Customer Operations Branch. SBO is responsible for managing all signallers and signal boxes in the network.
Location
Sydney Trains network – Cowan Bank
Cowan Bank is a steep and curving section of track that runs from Hawkesbury River up to Cowan station, a distance of approximately 9 km. The section consists of the Up and Down Main lines, features four tunnels and the signalling system is rail vehicle detection bi-directional.
Trains travelling in the up direction towards Sydney from Hawkesbury River encounter steep rising gradients as much as 1:37. A rising gradient refers to the graded rate of ascent. A 1:37 rising gradient means that for every 37 m travelled, the track rises 1 m.
The bi-directional signalling system means trains can operate in either direction on either track as there are signals provided to control movements in both directions. This type of signalling is a feature in areas on the network where there are steep grades and trains have a greater risk of being unable to continue due to mechanical faults, or as in the case with 5936, excessive wheel slip.
The rail line winds through a narrow corridor and access and space is limited. The line in the section from Hawkesbury River to Cowan station is formed of many cuttings made into the hillside to house the rail tracks.
Figure 3: Entry to Boronia Tunnel No. 3 in the up direction

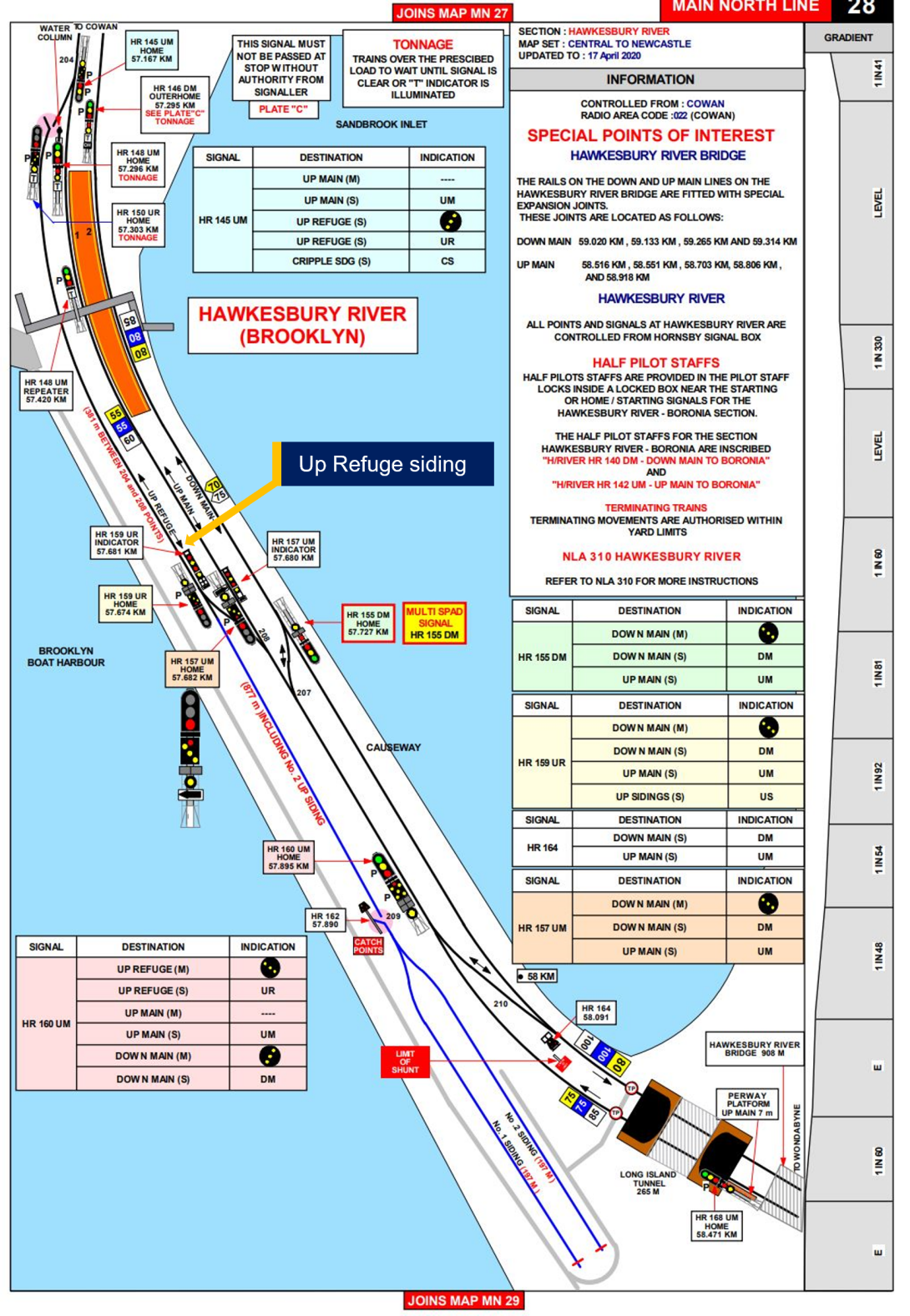
Hawkesbury River Up Refuge siding
The Hawkesbury River Up Refuge siding is located within the Hawkesbury River yard. The yard consists of the Up and Down Main lines, the Up Refuge siding, No. 1 and 2 sidings and various points and signals to permit trains to operate. The Up Refuge siding has a stowing capacity of 877 m including the use of No. 2 siding.
Figure 4: Diagram of Hawkesbury River
Rail lubricators
Rail lubricators are engineering devices designed to deliver rail lubrication to the wheel-rail interface to reduce wear and wheel squeal noise. Three rail lubricators were installed and active on the Up Main track between Hawkesbury River and Cowan at the time of the incident.
Delivery of excessive lubricant to the rail can induce wheel slip in a train, leading to a lack of adhesion between the rail and the wheel face and the train being unable to continue.
Rail safety systems and rules and application
Protecting activities for in service rail traffic
Sydney Trains describes their Train Working (NTR) Rules as prescribing the Network requirements for operating trains and track vehicles, including the maintenance of train integrity, and management of equipment defects by Operators, Train Crews and Track Vehicle Crews. Train Working Network Procedures (NPR) describe how particular actions are to be done to apply the Network Rules.
Sydney Trains has specific Train Working Network Rules (NTR) and Procedures (NPR) for protecting people when attending to trains which are in service on the network. The Network Rule is NTR 432 Protecting activities associated with in-service rail traffic and the associated Network Procedure is NPR 750.
The rule and procedure cover situations including where train crew leave their cab to get down on the track and conduct repairs or undertake other activities.
The activities that are undertaken by workers and subject to this form of protection include minor repairs to rolling stock, re-coupling burst air hoses, removing minor obstructions from the track and conducting roll by inspections.
This Train Working rule for protecting people when attending to trains in service and the associated procedure were introduced in 2016, after the SHN had received their foundation training and qualifications, to provide a greater level of prescription about how these on track activities were managed. Previously these activities were managed under the Work on Track (NWT) suite of rules using Absolute Signal Blocking rule NWT 308.
According to RailSafe, Work on Track (NWT) rules prescribe the Network requirements for undertaking activities in the rail corridor and mandate the ways to plan for and achieve the separation of rail traffic from people working on or about track. Principally aimed at maintenance and infrastructure repair, not in-traffic protection.
The new rule and procedure under Train Working (NTR) rules provided a level of assurance for both the signaller applying the protection and the in-traffic worker seeking the protection by compelling the parties to give and receive assurances about the location of the work and the type of work being done. It has similar assurances to the work on track requirements for other tasks like maintenance and infrastructure repair.
NTR 432 operational requirements
NTR 432, Protecting activities associated with in-service rail traffic, has very explicit instructions about what information must be exchanged between the Qualified Worker requesting the protection and the signaller.
Requesting protection
When requesting the protection of activities associated with in-service rail traffic, the Qualified Worker must:
- Provide the train number or track vehicle number
- Identify the lines on which the protection is required
- Nominate the activity location as being:
- between any two stations
- completely within a nominated dead-end siding, or
- completely within the limits of a platform.
Absolute Signal Blocking (ASB)
ASB is a network rule for working on track, Work on Track NWT 308, Absolute Signal Blocking. It works on the principle of rail signals being set to stop with blocking facilities applied to exclude rail traffic from the work area. Within the rule there are several options to provide protection, including:
- Having two controlled absolute signals set to stop with blocking facilities applied or
- Having one controlled absolute signal set to stop with blocking facilities applied and
- Removing an ESML/EOL key, or
- Securing points to prevent access, or
- There being an easily reached safe place available and providing a lookout.
In the case of protecting workers under NTR 432 and NPR 750 Protecting activities associated with in-service rail traffic, while signals are used to protect workers, similar to using ASB, the protection itself is not ASB, as the assurances and requirements are different to ASB and are contained in separate train working rules and procedures, NTR 432 and NPR 750. It is a subtle but important distinction.
ATRICS overview
ATRICS stands for Advanced Train Running and Information Control System, a bespoke system developed in-house by Sydney Trains. ATRICS is a computer-based control system that interfaces with signalling assets to control and monitor their status. It also has an interface with the timetable to automatically set routes for rail traffic.
A signaller will oversee rail traffic operating through the control area of each signalling panel, however in normal circumstances, ATRICS will set routes based on the timetable inputs. The signaller intervenes to control signals manually when there is a need, such as protecting work on track.
The signal control panel the SHN was operating was an ATRICS controlled panel within Homebush Control Centre.
Applying and removing blocks to signals
When a signaller applies blocks to signals on an ATRICS control panel, there are two methods to do so. Manually placing blocks on signals is done directly by the signaller in response to an incident or another circumstance such as a Condition Affecting the Network, where there may be a potential obstruction to the track or other hazard. In this circumstance, the signaller can place and remove signal blocks with no other intervention.
However, when placing signals to stop and placing blocks to protect work on track or workers attending to in-service trains, there are very specific requirements in the rules and procedures about how this is done.
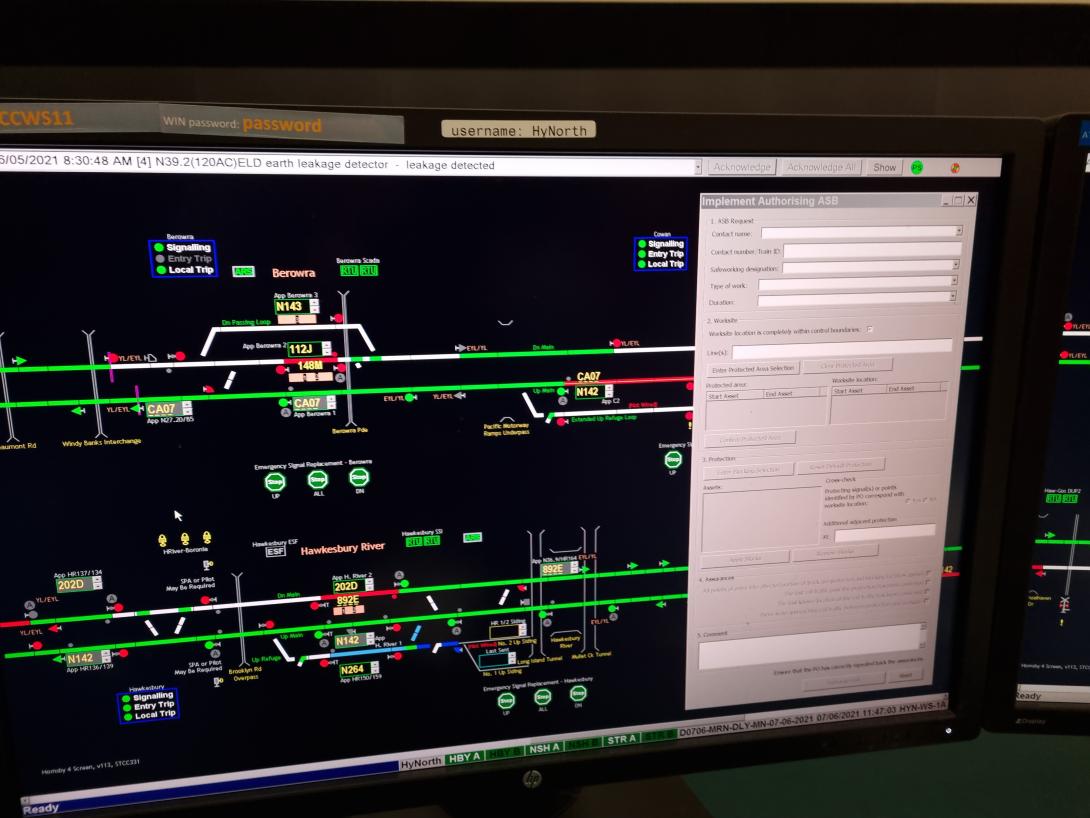
According to NTR 432, Protecting activities associated with in-service rail traffic, the signaller must use an electronic Absolute Signal Blocking (ASB) form to record the application of the signal protection. The extract of the rule is below:
The Signaller must:
- Use a system-generated ASB form, or if that is unavailable, an NRF 018 Absolute Signal Blocking (ASB) form to record the protection details
- Issue a unique protection number to the Qualified Worker requesting the protection.
When using the system-generated ASB form, ATRICS generates a unique code which is associated with the protection and is provided to the worker who has requested the protection. This code is used when ending the protection as an identifier of the correct protection.
NTR 432 requires the use of a system generated form, if it is available, to record the details of the protection. This form is the same as used when applying protection for ASB.
Figure 5: ASB form on ATRICS workstation
Propelling trains
Propelling trains under the network rule NTR 424, Propelling rail traffic, can be a dangerous activity, as a worker or workers may be walking in front of a moving train, and as the driver is not at the end of the movement in the direction of travel, they do not have visibility of the worker(s). There is no procedure that accompanies the network rule to identify and manage risks associated with this activity, unlike other activities that are governed by a rule and a procedure.
Network Communications
NGE 204 is the network General Rule (NGE) applicable to communications. NGE 204 says, in part:
Communication in the Network must be:
- Clear, brief and unambiguous
- Relevant to the task at hand
- Agreed to its meaning before being acted upon.
Communication between the SHN and the driver 5936
The driver of 5936 did not specifically request protection under NTR 432, Protecting activities associated with in-service rail traffic. They requested that a block be put on the signals, and that is what the signaller did. Neither party followed the requirements of NTR 432 in particular the required safety critical communication exchange. The transcript of the recorded audio between the SHN and the driver of 5936 at the time protection was requested is below.
SHN: OK um do you need any protection there for that?
Driver 5936: Yes, if he’s gotta walk on the ah on the opposite track, we definitely need protection. A block for the whole way over.
HNAC: Righto then …ok so …. I’m just putting some blocks on there now….. Just stand by while I do that.
DR5936: Roger that over.
HNAC: Righto I’ve done that there now, so um, I haven’t, so nothing can come up….on that line for ya there so, when you’re ready to walk back and get into position you’re able to do that for me now please.
DR5936: Roger that my mate will walk back now ah so his got the blocks, so his gotta walk back another 832 metres and then get ahead of me. Bit of a way. And then I will proceed down as safely as I can possibly can over.
HNAC: ok thank you for that driver.
Neither party to this conversation specifically mentioned protection being required under NTR 432, which is the relevant rule in this circumstance. All they refer to is “blocks”.
The driver of 5936 did not specify where and for how long the two crew members would be required to walk on the Down Main line while the propelling movement was taking place.
Fatigue management
The SHN was subject to the Sydney Trains rostering and fatigue management arrangements contained in the procedure Managing Shift Work and Rostering procedure, SMS-08-OP-3128 V1.2.
The Pacific National train crew were subject to fatigue management requirements that were derived from their labour management system. No issues of concern were discovered with the fatigue management requirements for the train crew.
The Sydney Trains rostering and fatigue procedure included eight rostering principles to be observed in order to reduce or manage the cumulative effects of fatigue. These eight rostering principles, and a description of these principles, are reproduced below from the Sydney Trains procedure:
| Principle | Description |
| Acclimatisation | Workers new to shift work and those returning after an extended period of annual or sick leave should not be rostered on night work or an early morning start for their first shift. When on leave, human circadian rhythms quickly re-establish a pattern of sleeping at night and being active during the day. Returning to night or early morning starts may be difficult, a bit like ‘Mondayitis’. |
| Shift length | The length of a shift should not exceed 12 hours including overtime, especially if it involves a night shift. Human performance declines significantly when people have been working for 12 hours or more, especially where work is done at night or in the early morning. |
| Total hours worked | Aim for no more than 48 hours per week including overtime, which can be averaged across the roster cycle. The risk of fatigue increases towards the end of a week/roster cycle. This is because a sleep debt has accumulated. Limiting the number of hours worked in a week or roster cycle, provides time off to recover and repay the sleep debt. |
| Limit night shifts and early morning starts |
Aim for no more than:
Working a series of night/early morning shifts disrupts circadian rhythms and leads to accumulation of a sleep debt. |
| Break during a shift | Schedule frequent breaks especially during a night shift or if the work involves sustained mental or physical activity, if local arrangements allow. Breaks during a shift provide workers with an opportunity to rehydrate and get a short rest. Breaks during a shift may be rostered or managed informally, depending on local arrangements and the nature of the work. |
| Break between shifts | Aim for at least 12 hours from the end of a shift and the start of the next shift. Industrial agreements may allow for less than 12 hours, however, to reduce the risk of fatigue, a minimum of 12 hours break is needed. Breaks between shifts need to allow enough time for recovery and sleep. Night shifts may need longer breaks between shifts. This is because workers will need to sleep during the day when it is difficult to get good quality sleep |
| Breaks between cycles |
Make sure there are adequate breaks between shift cycles. For example:
Days off should be a minimum of two consecutive days. Evidence indicates shift workers need at least two consecutive nights sleep per week to enable them to report to work feeling refreshed. |
| Shift cycles |
Schedule consistent start times where possible, or if rotating rosters are used, shift start times should move in a forward rotation i.e. morning-afternoon-night. Consistent start times can help shift workers get into a routine. Where rotating rosters are used, there is evidence that a forward rotating roster allows shift workers to delay sleep and wake up later. This is easier to do than going to sleep earlier or waking up earlier. |
The planned, or master, roster and shifts the SHN actually worked for the period from 28 December 2020 to 8 January 2021 is included in the table below.
| Date |
Planned shift times |
Actual shift times |
Hours worked |
Time until next shifts |
| 28 December 2020 | Rostered off | |||
| 29 December 2020 | Rostered off | |||
| 30 December 2020 | Rostered off | |||
| 31 December 2020 | 2200 - 0600 | 2200 - 0600 | 8 | 24 |
| 1 January 2021 | Rostered off | |||
| 2 January 2021 | 0600 - 1400 | 0600 - 1400 | 8 | 16 |
| 3 January 2021 | 0600 - 1400 | 0600 - 1400 | 8 | 32 |
| 4 January 2021 | 2200 - 0600 | 2200 - 0600 | 8 | 16 |
| 5 January 2021 | 2200 - 0600 | 2200 - 0600 | 8 | 16 |
| 6 January 2021 | 2200 - 0600 | 2200 - 0600 | 8 | 16 |
| 7 January 2021 (incident 0405 8 Jan) | 2200 - 0600 | 2200 - 0600 | 8 | 16 |
| 8 January 2021 | 2200 - 0600 | Off roster |
Environmental conditions
The Bureau of Meteorology (BOM) Terry Hills weather station (located approximately 12.0 km from Cowan Station) recorded a minimum temperature of 15.4˚C and maximum temperature of 20.6˚C. The weather station also recorded 2 millimetres of rain on the date of the incident. The track was wet and slippery and the driver of 5936 reported these conditions added to the degree of difficulty in conducting the propelling movement of a train in excess of 4000 t down a steep gradient. However, while the conditions made the propelling movement difficult, it did not contribute to the incident itself.
Breathing apparatus and welfare of the train driver
Train 5936 was stopped in Boronia tunnel no. 3 for over thirty minutes before the propelling movement commenced. The driver reported at interview suffering health effects from exposure to diesel fumes while stopped in the tunnel. Unlike their coal fleet, Pacific National bulk trains carrying products such as grain do not carry breathing apparatus as part of their standard on board kit.
Reporting incidents
NGE 234, Responsibilities of Signallers is the network rule applicable to the responsibilities of signallers and contains a requirement relating to reporting incidents. Specifically stating, Signallers must:
…..promptly report breaches of Network Rules and Network Procedures to the controlling officer and the Network Controller.
Related occurrences
On 2 March 2022 at 0121, Pacific National freight train CA80 failed on the Down main line at Wondabyne, NSW in the Sydney Trains network. The recovery process for this train, as determined by the Sydney Trains Network Incident Manager, involved attaching a following freight train, 1423, to the rear of CA80 and pushing it out of the section to Gosford.
A member of the crew of CA80 was on the track and attached the air hoses of 1423 to CA80. No protection was provided to this worker and as a result, a passenger train, 282L, passed by on the adjacent Up Main line as the worker was walking back to the crew cab of CA80. This worker had to take evasive action and move off the track to avoid being struck by 282L.
No protection was provided to this worker using the required network rules and procedures, NTR 432 Protecting activities associated with in-service rail traffic and related procedure NPR 750.
At approximately 0030 on 21 August 2019, freight train 4WM2 operated by Pacific National stopped at signal W26U near Waterfall, NSW. The train crew consisting of driver A and B were directed by the Waterfall Signaller at 0200 to remarshal the train. The train could not continue and was required to return to Coalcliff to clear the main line.
Remarshalling the train required one of the drivers to enter the danger zone to apply hand brakes on the wagons. Driver A requested safeworking protection from the Waterfall Signaller before entering the danger zone without incident.
The locomotives were detached and operated to Waterfall, before travelling to Helensburgh and returning to the stabled wagons near Waterfall.
On arrival at the stabled wagons, driver B requested safeworking protection again from the Waterfall Signaller. Driver B entered the danger zone to release the hand brakes from the stabled wagons. At about 0417, driver A signalled (hand signals and red marker lights) to the driver of an approaching passenger train (404A) to stop. The train was travelling on the adjacent track towards driver B in the danger zone and the driver of 404A made an emergency brake application to stop the train. The train stopped before arriving at the location of driver B and there were no physical injuries.
The safeworking network rule and procedure for protecting activities associated with in-service rail traffic, NTR 432 and NPR 750, were not used effectively to ensure workers were protected from rail traffic. The requests for protection were informal and did not detail the required activities or protection. Both drivers of 4WM2 unknowingly entered the danger zone without appropriate protection and were at risk of being struck by rail traffic.
Safety analysis
Introduction
Pacific National train 5936 failed inside Boronia tunnel No. 3 on Cowan Bank in the up direction as a result of wheel slip from excessive lubricant and was unable to lift its load up the grade. The driver of 5936 reported the train failure to the SHN. The SHN reported the incident to the Sydney Trains TSDMCC and their decision on how to manage the incident involved propelling the train backwards down Cowan bank and into the Hawkesbury River Up Refuge siding to clear the main line.
To undertake the propelling movement, a qualified worker needed to be located at the rear of the train, to supervise the movement backwards down the Cowan Bank. This was a standard requirement in the Sydney Trains Network rules for propelling trains. Under the rule, if there is not a designated safe place on the rear of the train, the worker must walk in advance of the movement in a safe place. Where the worker walks, depends on a few conditions, like the terrain, the availability of a safe place and the layout of the rail environment.
Train 5936 had three people in the driver’s cab, the driver, an assistant driver and a trainee assistant driver. The driver of 5936 intended to send the assistant driver and the trainee assistant driver to the back of the train to supervise the movement.
The driver of 5936 requested protection from the SHN in the form of signals put to stop and blocked on the Down Main line. This prevented trains from entering the area where the two workers needed to walk to reach the rear of 5936. Once confirmed, the assistant driver from 5936 and the trainee driver exited the driver’s cab and walked on the adjacent Down Main line to the rear of the train.
Once the two crew members were in place at the rear of the train, the driver advised the SHN that the propelling movement was about to commence and asked the SHN to confirm that the route was clear back to the Hawkesbury River Up refuge siding. The two workers continued to walk on the Down Main line adjacent to the rear of 5936, as there was no other safe place to walk.
As the propelling movement continued, the two crew members observed the lights of a train travelling towards them in the up direction on the Down Main line. The two crew members alerted the driver of 5936 of the presence of the oncoming train and to stop the movement, then they jumped clear of the Down Main into the Down Cess area.
Cowan Bank terrain and operational features
Cowan bank is known to have some challenging operational features. For example, access on the up side of Cowan Bank is problematic for a worker needing to walk along the rail line as the corridor is often butted up against the rock face of cuttings and there is no safe place.
To give a worker a continuous safe place to walk while supervising a propelling movement, a safe place is created on the adjacent track by applying protection in the form of setting rail signals to stop and blocking them to stop rail traffic entering the affected area.
Trains failing to make the steep grade on Cowan Bank is a regular occurrence and there are two main options to deal with the situation. In some cases, a rescue engine is brought in from Gosford or elsewhere north of the incident location to push the train up the grade.
The alternative is to propel the train back down the grade into the Hawkesbury River Up Refuge siding. This option can only work if the train is a suitable length to fit into the siding, which has a capacity of 877 m. 5936 was 831.6 m and therefore suitable to fit safely inside the siding, so the decision was made by the TSDMCC to propel the train back towards Hawkesbury River.
Rail lubrication on Cowan Bank
There were three operational rail lubrication devices installed on Cowan Bank to service the Up Main between Hawkesbury River Yard and the Cowan Station. Sydney Trains engineers had assessed that the rail lubricators should have similar settings as those used in the Blue Mountains in order to deliver optimal lubrication. These adjustments were made in February 2021.
Sydney Trains conducted an engineering review post incident into these devices and determined that excess lubrication contributed to the wheelslip. This led to the train becoming disabled and unable to continue up the Cowan Bank. This resulted in the need to propel the train backwards to the Hawkesbury River Up refuge siding.
Sydney Trains determined post incident and in response to a spate of similar events where freight trains were unable to lift their load due to loss of traction from excess lubricant on the wheel-rail interface that further adjustments were necessary to ensure the amount of lubrication provided did not adversely affect wheel adhesion to the rail head, particularly for loaded freight trains.
The decision to propel 5936 and run passenger trains using bi- directional signalling
Discussion between SHN and TSDMCC
When the SHN and TSDMCC became aware of the inability of 5936 to lift its load up the Cowan Bank, a discussion took place to determine what to do with the train. The discussion canvassed the option of using a rescue engine to assist, however, given the time and location, it was considered unlikely to result in a timely outcome. The TSDMCC determined that the best course of action was to propel 5936 backwards down Cowan Bank into the Hawkesbury River Up Refuge siding.
The TSDMCC checked reference documents to ensure the Up Refuge siding was long enough to contain 5936, and once confirmed, gave the instruction to SHN to direct the driver of 5936 to propel back into the siding.
The TSDMCC and SHN also discussed the need to run any AM peak passenger services via the Down Main using the bi-directional signalling. This discussion indicated there was a concurrent plan developing not only to remove 5936 from the main lines but also to facilitate the continued operation of passenger services in the up direction for the AM peak.
Implication of the decision to propel 5936
The TSDMCC and SHN knew that workers would have to walk to the back of the train to manage the propelling movement. The recorded audio indicated there was a suggestion that a passing train could be used to transport the workers via the Down Main, but there was no train due in that direction for nearly an hour so that was dismissed.
Both the TSDMCC and the SHN knew there would be a worker or workers out of the train and on the track at some point to facilitate and manage the propelling movement.
What the propelling decision meant to the driver of 5936
The degree of difficulty in making this manoeuvre was considerable. The driver had to slowly reverse a train of over 4000 t and nearly 900 m long down a steep gradient, in the dark and in the rain. The train also had to negotiate tunnels, and in the case of 5936, the leading locomotive was still within Boronia tunnel No. 3. The driver reported at interview suffering ill health effects from diesel exhaust whilst being stopped in the tunnel.
Recorded audio of exchanges between the SHN and the driver of 5936 indicated numerous calls were made during the movement, which likely disrupted the concentration of the driver during what was a high cognitive load due to a difficult manoeuvre under complicated circumstances. Other recorded audio of exchanges between the SHN and the TSDMCC indicated there was particular focus on continuation of passenger train services, especially in the up direction for the AM peak.
Protecting workers attending to in-service rail traffic
Compliance with the requirements of NTR 432 and NPR 750
In the case of the workers involved in propelling 5936, the driver needed to nominate the activity location as being between two points. This did not occur. They also did not describe that two workers would be walking all the way behind and adjacent to the train as it propelled backwards towards Hawkesbury River yard, past the station and into the Up Refuge Siding.
NTR 432 also stated that the signaller must:
- Use a system-generated ASB form, or if that is unavailable, an NRF 018 Absolute Signal Blocking (ASB) form to record the protection details
- Issue a unique protection number to the Qualified Worker requesting the protection.
The SHN did neither of these things in this circumstance.
Sydney Trains internal safety investigation into this incident found evidence that similar events of managing failed freight trains where the requirements of NTR 432 and NPR 750 were not applied. Recent ATSB investigations listed in the Related Occurrences section of this report also found this error in practice.
Suitability of NTR 432 to protect workers
NTR 432 is a Train Working rule about protecting workers while on the track, however it is not included in the suite of other rules devoted to the same purpose, specifically Work on Track (NWT).
NTR 432 is designed to protect people on the track when attending to their train while it is in service however is included in the suite of rules devoted to train working. This suite contains rules more specific to the operation and use of the train, rather than the protection of workers and includes rules such as:
- NTR 400 Protecting rail traffic,
- NTR 402 Inspecting trains,
- NTR 404 Using brakes
- NTR 406 Using lights.
The Work on Track (the NWT) series of rules, is more specific to protecting workers and includes rules such as:
- NWT 300 Planning work in the rail corridor
- NWT 302 Local Possession Authority
- NWT 304 Track Occupancy Authority
- NWT 306 Track Work Authority
- NWT 308 Absolute Signal Blocking.
NTR 432 appears out of place in the suite of train working rules given it is a rule devoted to protecting workers who are on the track performing rail safety work. In this case, the workers were attending to a train while it was in service however required protection while doing so because they were on the track. However, NTR 432 is not included in the Work on Track suite of rules which are devoted to protecting workers while on the track.
Evidence from the Sydney Trains investigation report into the incident indicated that rule NTR 432 was not applied in other cases where it should have been. It is possible that NTR 432 was not applied correctly because rail safety workers were not familiar enough with it as a rule to be followed while working on track. As rule NTR 432 is contained in a suite of rules devoted to train operations, and not within the suite devoted to protecting people while on track (the NWT suite). It is possible that its importance and application may not be understood by rail safety workers.
Suitability of NTR 432 to manage propelling movements
NTR 432 Protecting activities associated with in-service rail traffic includes a number of requirements which must be met through satisfying the assurances contained within the rule. One of the assurances relates to the mobility of the rolling stock and reads:
Unless conducting a roll by inspection, the Qualified Worker must make sure that the associated rail traffic will not be moved until the activity is completed.
If the intention of NTR 432 was to protect workers attending to in service rail traffic, then this rule may not be suitable for use during a propelling movement. NTR 432 contains a prohibition on rolling stock movement, except when conducting a roll by inspection. That being the case, there are no approved measures available under the current set of rules to protect workers supervising a propelling movement.
Signaller operational assurance
The Sydney Trains investigation examined the assurance regime for signallers relating to the application of the requirements of NTR 432 and NPR 750 - Protecting activities associated with in-service rail traffic. The investigation found that the SBO group did not undertake assurance activity related to the correct application of relevant rules and procedures for protecting workers attending to in-service rail traffic.
The investigation identified other similar incidents that were also not managed in accordance with the requirements of NTR 432. Examples of where the requirements of NTR 432 and NPR 750 were not applied are listed in the Related Occurrences section of this report.
ATRICS and the application of signal protection
Applying and removing blocks to signals
The SHN did not apply blocks to the protecting signals in accordance with NTR 432 and NPR 750 and did not use the ATRICS generated form to record the placement of the protection. The SHN applied the blocks to the protecting signals manually and removed them without the authority of the person requesting the protection, the driver of 5936.
Communication between the SHN and the driver 5936
The driver of 5936 did not specifically request protection under NTR 432. They requested that a block be put on the signals, and that is what the signaller did. Neither party followed the requirements of NTR 432 or observed the assurances. The transcript of the recorded audio between the SHN and the driver of 5936 at the time protection was requested is below.
SHN: OK um do you need any protection there for that?
Driver 5936: Yes, if he’s gotta walk on the ah on the opposite track, we definitely need protection. A block for the whole way over.
HNAC: Righto then …ok so …. I’m just putting some blocks on there now….. Just stand by while I do that.
DR5936: Roger that over.
HNAC: Righto I’ve done that there now, so um, I haven’t, so nothing can come up….on that line for ya there so, when you’re ready to walk back and get into position you’re able to do that for me now please.
DR5936: Roger that my mate will walk back now ah so his got the blocks, so his gotta walk back another 832 metres and then get ahead of me. Bit of a way. And then I will proceed down as safely as I can possibly can over.
HNAC: ok thank you for that driver.
Neither party to this conversation specifically mentioned protection being required under NTR 432, which is the relevant rule in this circumstance. All they refer to is “blocks”.
The driver of 5936 did not specify where and for how long the two crew members would be required to walk on the Down Main line while the propelling movement was taking place.
Signaller training, performance, and competence management
Signaller knowledge of propelling trains
The SHN did not understand the requirements of NTR 424 - Propelling Trains. At interview, the SHN expressed a lack of knowledge about the activities of the workers on the ground directing the propelling movement. Specifically, the SHN did not understand that the two workers directing the propelling movement were still walking in front of, and adjacent to, train 5936 when it was propelled down Cowan Bank.
The SHN expressed some surprise that the workers were in that position and assumed they were riding on the freight rolling stock once the propelling movement started. The practice of riding on moving freight rolling stock has been prohibited since 2004.
Once the propelling movement started, the SHN removed the blocks on the protecting signals and allowed train 247B to run in the Up direction on the Down Main through use of the bi-directional signalling system.
During the conversation with the driver of 5936 after the near miss incident with 247B, it was apparent that the signaller was not aware that the workers were still on the protected track walking in front of the propelling movement.
Driver 5936 Yes Hornsby ah my ah mate down the back just said you just put a train up on the down around us over.
HNAC Yeah that’s correct.
Driver 5936 Ah I thought we had a block on over
HNAC Yeah that’s when you actually, when you weren’t moving, when you were actually on the (pauses) when you walking back over.
Driver 5936 He’s still walking back. He’s gotta walk me back to get into the siding over HNAC OK (speaks under their breath) well you’ve moved back.
Driver 5936 Yes ‘cause he was on the down calling me back, that’s the only safe place for him to stand over.
HNAC (12 seconds of silence and clears his throat) OK that trains trains gone and there are no other trains on the down. I have got blocks on on um up at Cowan (silence for a few seconds) just stand-by.
Driver 5936 Roger.
HNAC Yes so you’re right to proceed there driver um keep proceeding I’ve got the um all the routes and the signals set for you to go into the Refuge Loop there at Hawkesbury River driver. Thank you driver.
Driver 5936 5936 out.
HNAC (groans) Hornsby North Panel out.
Driver 5936 Roger that, we have everything set so there is nothing definitely going to come either way towards us now over.
HNAC That is correct driver.
Driver 5936 Roger so I can my mate to ah get back on the down in a safe place. HNAC That is correct.
Driver 5936 Roger that well we start again over.
This conversation, after the near miss happened, resulted in the incorrect re-application of protection required by NTR 432. The SHN reapplied the blocks manually with communication assurances not observed as required by the rules and procedures. The conversation revealed that the SHN did not understand the workers positioning during the propelling movement and had made an assumption that the signal blocks could be safely removed, without confirmation from the driver as required.
Safety Refresher Training
At interview, the SHN advised that the job of a signaller involves the use of many rules and procedures, and that signallers are expected to be current and competent with all these requirements all of the time. The SHN specifically stated that he did not know the workers were walking in front of train 5936 during the propelling movement because he was not familiar with the requirements of NTR 424 Propelling Trains, even though it was a mandatory requirement for signallers to know this rule.
The SHN also advised that they had not attended any refresher, or scenario-based training for several years. The SHN advised that the only safeworking training they received, other than initial training, was when there were rule changes, as there was in the case of the introduction of NTR 432 in 2016. A briefing session was provided to explain the new rule and procedure. The SHN advised that when they had enquired about receiving refresher training, their management’s response was they could not be released because of operational requirements.
The Sydney Trains investigation report into this incident identified that its Customer Operations Branch had not delivered any safety refresher training for signallers since 2009. Other rail safety workers such as Protection Officers on the other hand received a form of refresher training and competency assessment which included periodic recertification in safeworking rules and procedures along with formal assessment.
Following its investigation report finding, Sydney Trains advised that a pilot of a revised refresher training program for signallers was commenced in April 2021.
Network familiarisation
Signallers control the operation of signals, points and other infrastructure in a defined geographical area. What the signaller sees and understands of the network is what is represented on their signal display panel, which is a schematic array and does not depict the geography or topography or other features of the network.
The SHN advised at interview that they had never been to Hawkesbury River Yard or seen the Cowan Bank, or any other part of the network they had controlled during their career. Signallers are not provided the opportunity to visit their area of operation to make them familiar with the area of the network that they controlled. The mental model that the SHN reported they had of Cowan Bank did not include key features such as the steep grade, the winding rail corridor and the lack of safe places and access.
A review undertaken as part of this investigation of the Sydney Trains competence management system for signallers revealed that network familiarisation or route knowledge was not a feature of the initial or ongoing training requirements for signallers.
Sydney Trains commenced a trial program of network familiarisation for protection officers in December 2020 designed to provide awareness and knowledge of the layout and risks in the network, to help workers perform more safely and efficiently, but at the time of writing it was not being rolled out to signallers.
Signaller fatigue
The incident happened around 0430, which is a known time of the window of circadian low, or the time of maximum sleepiness, for most people.
Two of the eight rostering principles were not met in relation to the roster of SHN in the eight days leading up to the incident. The two principles, and the nature of the departure from these principles, are outlined below. The acronym HNAC stands for Hornsby North Area Controller, and is the term used by Sydney Trains to describe the signaller operating the Hornby North panel.
| Rostering principle | Departure from principle during this incident |
| 4. Limit night shifts and early morning starts | The HNAC was rostered for two consecutive early morning shifts on 2- 3 Jan 2021 and six consecutive night shifts on 4-9 Jan 2021 |
| 7. Breaks between cycles | The HNAC had single days off on 28 Dec 2020, 30 Dec 2020, and 1 Jan 2021—each time after a night shift before commencing the consecutive shifts leading up to the day of the incident. |
An extract of the Sydney Trains Investigation report into this incident relating to fatigue is reproduced below:
Rostering Principle #4: Limit night shifts and early morning starts. Aim for no more than six consecutive shifts where 8-hour shifts are worked. ‘
The Hornsby North Area Controller (HNAC) was rostered for two consecutive early morning shifts on 2- 3 Jan 2021 and six consecutive night shifts on 4-9 Jan 2021. While the incident occurred at the sixth consecutive shift (where HNAC signed in on 7 Jan 2021 at 10pm) and was just at the limit of this rostering principle, the increase in the FAID score over this period had reached 93 by this shift.
Although this FAID score had not reached the business unit threshold of 100, it was on the upper limits of approaching the threshold. Furthermore, it is difficult for humans to adjust from the two extremes of an early morning shift to a night shift without the opportunity to have an adequate break in between to prepare and adjust to the sleep impacts of night shift.
Rostering Principle #7: Breaks between cycles. Make sure there are adequate breaks between shift cycles. Days off should be a minimum of two consecutive days.
The HNAC had single days off on 28 Dec 2020, 30 Dec 2020, and 1 Jan 2021—each time after a night shift before commencing the consecutive shifts leading up to the day of the incident. Having less than 48 hours between shift cycles, especially after completing night shifts, does not provide an individual with enough opportunity to have restorative sleep to recover from any sleep debt that has accumulated from working night shifts. With the HNAC working single night shifts between these single days off, it is likely that the HNAC had accumulated an amount of sleep debt from only having the opportunity for restorative sleep during daytime, which is not as restorative as obtaining sleep during night time. The HNAC then commenced the sequence of consecutive early morning and night shifts, which would have further contributed to additional sleep debt leading up to the day of the incident.
According to the Managing Shift Work and Rostering procedure, when departures from these rostering principles occur, line managers must intervene and put in place measures to try and correct the situation. There was no intervention by the Sydney Trains line manager for SHN to adjust or amend the roster.
Sydney Trains acknowledged in their internal investigation report into this incident that the requirements for the procedure Managing Shift Work and Rostering were not being followed. Sydney Trains adopted a recommendation from their internal report as follows:
Review the business unit Fatigue Risk Management System / processes to ensure that there is an ability for the business unit to identify the fatigue risk associated with different rostering patterns and to detect adherence to rostering principles with mitigating fatigue risk controls to be implemented for these instances.
The issue of departures from the Managing Shift Work and Rostering procedure, and the subsequent lack of managerial intervention, have been raised previously in the ATSB investigation RO-2019-18 Westmead.
Signaller rest regime
At interview, the SHN stated that they were well rested for the shift prior to the incident. SHN recounted how they had an effective rest regime at home when working night shift and had obtained sufficient rest, had slept as usual from about 0730 to 1530, and felt fit and able to carry out their shift.
It is unknown whether the amount of sleep was sufficient to allow for recovery from the five consecutive shifts. It is possible that the SHN was affected by the cumulative effects of fatigue given the deviations from two rostering principles leading up to the day of the incident. However, the evidence is not definitive, and it is not possible to ascribe fatigue as a contributing factor with sufficient certainty.
Breathing apparatus and welfare of the train driver
Train 5936 came to a stand inside Boronia No. 3 tunnel and was there for around 30 minutes before the propelling movement commenced. According to the driver’s statement, the lead locomotive exited Boronia tunnel around 0441, therefore the driver was exposed to diesel fumes for around 35 minutes. The driver reported in their statement at interview that they were starting to feel unwell and had trouble seeing as their eyes had started to weep.
This physical discomfort existed while the driver undertook the difficult manoeuvre of propelling the train down the Cowan Bank.
Pacific National did not supply breathing apparatus or other mitigation measures to crews on its bulk trains, despite these trains operating through tunnels. Breathing apparatus was provided on locomotives that service the coal network in the Hunter Valley, as there were some long tunnels. The network manager specified that trains operating there must carry and use breathing apparatus in the case of train failure or some other mishap.
Safe Work Australia produces guidance on managing exposure to diesel fumes. The guidance says, in part:
Short-term (Acute) effects
Short term exposure to high concentrations of diesel exhaust can irritate the eyes, nose, throat and lungs and cause light-headedness, coughing, phlegm and nausea. Very high levels of diesel exhaust exposure can lead to asphyxiation from carbon monoxide poisoning.
The driver of 5936 reported feeling effects that were consistent with short-term effects of high concentration exposure to diesel exhaust listed above. The Safe Work Australia guidance does not provide any detail on the timeframes that these effects are likely to lead to more serious effects such as asphyxiation from carbon monoxide poisoning, as this would be subject to a range of factors, such as the health of the individual, the environment and ventilation and other factors.
However, based on the evidence of the driver, they indicated they were affected by diesel fumes, as they were on a disabled train in a tunnel for an extended period and were experiencing physical discomfort.
Once the two other crew members left the cabin to walk to the end of the train to supervise the propelling movement, the driver was alone. The Safe Work Australia guidance says that extended exposure to very high levels of diesel exhaust can lead to asphyxiation. If this were to happen while undertaking a propelling movement with a 4000 t freight train then there would be a risk of the movement becoming out of control.
While the effect of diesel exhaust on the driver did not directly contribute to this incident, it is a factor of increased risk in that it may have contributed to loss of control of the train in other circumstances.
Incident reporting
The SHN did not report the safeworking breach or the incident to the TSDMCC or anyone else. Signallers have clear accountabilities to report incidents in Network Rule NGE 234 - Responsibilities of Signallers.
Signallers must:
- Promptly report breaches of Network Rules and Network procedures to the controlling officer and the Network Controller.
The recorded audio of the conversation between SHN and the driver of 5936 clearly identified that a safeworking breach and a safety incident had occurred, i.e., the signals had been cleared without the authority of the driver and consequently, two workers had to jump clear of the track to avoid being struck by a train.
The incident was not reported until some days later when the trainee assistant driver reported an injury to Pacific National as a result of having jumped off the track. Pacific National then reported the incident to Sydney Trains who were then able to trace the events back to the original incident.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the near miss with train crew from train 5936 at Hawkesbury River on 8 January 2021.
Contributing factors
- The signaller did not apply or remove blocks to the protecting signals in accordance with NTR 432, Protecting activities associated with in-service rail traffic and NPR 750 and did not use the ATRICS generated form to record the placement of the protection.
- Sydney Trains’ internal safety investigation identified similar incidents i.e., where a freight train failed, that were not managed in accordance with the requirements of NTR 432, Protecting activities associated with in-service rail traffic. Recent ATSB investigations also identified examples where the requirements of NTR 432 and NPR 750 were not adequately applied. (Safety issue)
- Sydney Trains’ assurance and audit processes for signal box management did not routinely detect non-conformances with NTR 432, Protecting activities associated with in-service rail traffic. (Safety issue)
- Sydney Trains’ signaller refresher training, to keep signallers’ skills and knowledge up to date, had not been in place since 2009. (Safety issue)
- The driver of 5936 and signaller did not comply with the requirements of NGE 204, Network Communication as communications were casual, ambiguous, and unclear so did not conform to prescribed protocols.
- The Signaller Hornsby North did not understand that under the requirements of NTR 424, Propelling rail traffic, the worker(s) on track were walking next to or in front of the movement to direct the train.
- The Signaller Hornsby North did not receive advice from the driver to clear the protecting signals and remove the protection and did not receive confirmation that workers were clear of the danger zone as per the requirements of NPR 750.
Other factors that increased risk
- The Signaller Hornsby North did not report the incident as per NGE 234, Responsibilities of Signallers.
- Sydney Trains signallers were not provided with network or route familiarisation training for the area they controlled.
- Cowan Bank was a known problem area for failed freight trains however there were no local established procedures for managing such incidents in that area.
- Rail lubricators were overactive and delivered too much lubricant to the rail surface, which contributed to the likelihood of a train becoming disabled.
- Lack of breathing apparatus in train 5936 meant the driver was exposed to potentially dangerous levels of diesel fumes because they were in Boronia tunnel No. 3 for over 30 minutes while organising and performing the propelling movement.
- Network rule NTR 432, Protecting activities associated with in-service rail traffic was designed to protect workers while on the track but is not included in the suite of rules devoted to this purpose.
- Network rule NTR 432, Protecting activities associated with in-service rail traffic was not suitable to protect workers on track supervising a propelling movement as the rule prohibited the movement of rail traffic except for conducting a roll by inspection.
- Network rule NTR 424, Propelling rail traffic, does not cover protection arrangements for workers and there is no specific supporting procedure to provide guidance in how to do that.
Safety issues and actions
|
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the rail industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Requirements of NTR 432 and NPR 750 not applied
Safety issue number: RO-2021-SI-01
Safety issue description: Sydney Trains internal safety investigation identified similar incidents i.e., where a freight train failed, that were not managed in accordance with the requirements of NTR 432, Protecting activities associated with in-service rail traffic. Recent ATSB investigations also identified examples where the requirements of NTR 432 and NPR 750 were not adequately applied.
Assurance and audit process
Safety issue number: RO-2021-002-SI-02
Safety issue description: Sydney Trains assurance and audit processes for signal box management did not routinely detect non-conformances with NTR 432.
Signaller refresher training
Safety issue number: RO-2021-002-SI-03
Safety issue description: Sydney Trains Signaller refresher training, to keep signallers’ skills and knowledge up to date, has not been in place since 2009.
Glossary
| ASB | Absolute Signal Blocking |
| ATRICS | Advanced Train Running and Information Control System. |
| CAN | Condition Affecting the Network |
| ESML | Emergency switch machine lock |
| EOL | Emergency Operations Lock |
| FAID | Fatigue Audit Interdyne |
| HCC | Homebush Control Centre |
| LTA | Localised Training and Assessment |
| NGE | Network Rules General |
| NIM | Network Incident Managers |
| NPR | Network Procedures |
| NTR | Network Rules Train Working |
| PO | Protection Officer |
| PN | Pacific National |
| ROC | Rail Operations Centre |
| SHN/HNAC | Signaller Hornsby North |
| TSDMCC | Train Service Delivery Manager Central Coast |
| TSDM | Train Service Delivery Managers |
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- Sydney Trains Systemic investigation report
- Sydney Trains recorded audio from Homebush Control Centre and the Rail Operations Centre
- Rostering data for the Sydney Trains signaller
- Sydney Trains Network Rules and Procedures
- Pacific National investigation report
- Interviews with the Sydney Trains signaller and Pacific National train driver
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Sydney Trains
- Transport for NSW
- Pacific National
- The Office of the National Rail Safety Regulator
Any submissions from those parties will be reviewed and, where considered appropriate, the text of the draft report will be amended accordingly.
Submissions were received from:
- Sydney Trains
- Transport for NSW
- Pacific National
- The Office of the National Rail Safety Regulator
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2022
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] A propelling movement is a rail movement where the train is travelling in the reverse direction, with the locomotives pushing the train rather than hauling it.
[2] A proceed authority is defined in the RailSafe Glossary as: An Authority that allows rail traffic to enter and occupy a portion of line and proceed in the forward direction.
[3] Blocking facilities are defined in the RailSafe Glossary as: A facility or device used by a Qualified Worker to prevent either the unintended issue of an Occupancy Authority, or the operation of points or signalling equipment