
Investigation summary
What happened
On the morning of 12 August 2024, a Fairchild SA227-DC was being operated by Skippers Aviation on a non-scheduled air transport passenger flight from Forrestania to Perth, Western Australia. Close to the top of descent into Perth, the crew experienced a complete loss of pressure in the aircraft’s hydraulic system. The crew coordinated with air traffic control for a holding pattern to allow for time to troubleshoot the failure and prepare for an appropriate approach and flapless landing. Ground inspection vehicles were requested to ascertain post-landing if fluid was visibly leaking onto the runway and a tow vehicle was requested to recover the aircraft after landing.
After successfully landing and stopping on the taxiway, the captain was unable to establish contact with the tow vehicle and then decided to continue to taxi to the operator’s apron. As the aircraft approached the operator’s apron, a slight downhill slope caused an increase in speed. However, when the crew applied the brakes, they were ineffective. In an effort to avoid collision with a hangar, the captain applied reverse thrust. However the aircraft continued to roll forward, the captain shut down the engines and feathered the propellors before impacting the hangar. The aircraft sustained damage to the right-side wingtip and propellor, there were no injuries to crew or passengers.
What the ATSB found
During the flight, the captain was supervising the cadet-entry first officer’s flying when a crack in a hydraulic line led to a hydraulic fluid leak and in-flight failure of the hydraulic system.
Consistent with the first officer’s minimal experience, their ability to contribute to the in-flight emergency management was limited, requiring the captain to manage the emergency. The captain was required to take on both the pilot flying and pilot monitoring roles, which reduced their ability to effectively manage the emergency.
The first officer's inexperience limited their ability to contribute to managing the hydraulic system failure. This negatively impacted crew resource management and increased the captain's workload.
After stopping on the taxiway, the captain mistakenly assumed the brakes were functioning. Unable to locate or contact the tow tug, and influenced by self-imposed pressure, they continued the taxi to the apron.
On arrival at the operator’s apron, the aircraft had minimal braking capacity and the crew was not able to stop the aircraft. Due to the proximity of the hangar, the captain had limited opportunity to take corrective action and a collision occurred.
What has been done as a result
The operator has advised it is reviewing maintenance practices for tube repairs and replacements for the fleet. In addition, the following actions have been advised to the ATSB by the operator:
- The flight crew received refresher training in human factors, standard operating procedures, workload management and decision‑making. Additionally, the captain has completed remedial training on decision‑making.
- The captain has completed a series of simulator exercises to confirm all procedures are followed in accordance with the aircraft quick reference handbook (QRH) and company standards.
- During their fleet meeting, all fleet pilots were made aware of the incident and the lessons learnt to prevent reoccurrence.
- All fleet pilots have completed theory training and examination on the hydraulic system.
Safety message
This occurrence highlights the necessity for accurate assessment of system functionality following an in-flight system failure and the need to follow standard operating procedures. Vigilance when assessing aircraft performance and an objective assessment of system status are vital to minimise opportunities for error and avoid relying on potentially misleading indicators.
Flight crews are advised to prioritise procedural compliance in uncertain circumstances, especially when perceived pressure is heightened to continue to operate an aircraft in non‑normal situations.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
At about 0900 local time on 12 August 2024, a Fairchild SA227-DC Metroliner (Metro) aircraft, registered VH-WAJ and operated by Skippers Aviation, was conducting a non‑scheduled air transport flight with 2 crew and 4 passengers on board from Forrestania to Perth, Western Australia. The first officer (FO), who was completing supervised line flying, was the pilot flying and the captain was in the pilot monitoring role.
At about 1000, the aircraft was close to the top of descent into Perth (Figure 1), when the right hydraulic system low-pressure annunciator light flickered and then subsequently remained solid, which indicated a system failure.
Figure 1: Flightpath and location of VH-WAJ at the time of hydraulic failure

Source: Google Earth and QAR data, annotated by the ATSB
The flight crew consulted the aircraft quick reference handbook (QRH) and followed the standard checklist procedures to manage the indicated hydraulic system failure. The crew identified that the hydraulic pressure remained between 1,700 and 2,100 psi and as per the QRH instruction, the flight should be continued as originally planned. The crew reported following the planned route until, a short time later, the left hydraulic low-pressure annunciator light illuminated. The captain checked the main pressure gauge which displayed 0 psi and identified that there was a total failure of the hydraulic system.[1] The captain requested vectors[2] from air traffic control (ATC) for a holding pattern to allow time to determine the appropriate speed and extra distance required to conduct a flapless landing. This also provided time for the captain to instruct the FO on how to conduct a manual extension of the landing gear using the hand pump, as this was the first time the FO had undertaken this task.
ATC provided vectors for holding, while the captain recalled trying to contact the company maintenance watch directly, however, was unable to find the correct frequency and instead was able to advise other company representatives of the situation.
The captain considered but elected not to broadcast a PAN PAN[3] call to ATC, instead advising them that a tow vehicle (tug) would be required to tow them from the runway to the apron. The captain also requested ATC to provide a vehicle to follow the aircraft after landing for an inspection of any fluid visibly leaking onto the runway.
After finalising details for landing, the captain and first officer swapped ‘pilot flying’ roles due to the limited experience of the FO. The captain then took control of the aircraft and conducted the flapless landing on runway 24 at Perth Airport.
After a successful landing, they exited the runway and stopped on taxiway ‘A’. The captain reported looking for the tow vehicle but could not visually locate it and was unable to establish direct communication with the tug. The captain recalled that at this time the hydraulic system pressure gauge showed a positive pressure and so they elected to test the brakes and found that some braking pressure was evident.
An airport vehicle following the aircraft reported to ATC that no fluid was observed on the runway. ATC requested the crew’s intentions, and the captain informed them that they would continue the taxi back to the operator’s apron without the assistance of a tug.
As the aircraft approached the operator’s apron and turned toward the hangar, the aircraft’s speed increased due to a slight downhill gradient. The captain and FO applied full braking, but neither of their systems responded.
Figure 2: VH-WAJ shown stationary after collision with operator’s hangar

Source: Operator
In an attempt to avoid collision with the hangar, the captain momentarily used reverse thrust, then shut down the engines and feathered[4] the propellers. However, the aircraft’s right wingtip collided with the hangar at low speed, before the right propeller made contact. The impact resulted in minor damage to the right propeller and wingtip (Figure 2). All of the occupants disembarked safely, with no injuries to the crew or passengers.
Context
Aircraft information
VH-WAJ, a Fairchild Industries SA227-DC Metroliner was manufactured in the United States in 1995. The 19-seat aircraft was fitted with 2 Garrett TPE331-12 turboprop engines.
The flight log for the morning of the incident showed that the aircraft was considered serviceable. Maintenance documentation identified the successful repair of a hydraulic leak in April 2024, with no known hydraulic deficiencies prior to the incident flight.
Flight crew
The crew was composed of a training captain and FO. Each pilot held a commercial pilot licence (aeroplane) and a class 1 medical certificate.
The captain had about 3,620 hours total flying experience of which about 1,120 hours were on the Metro.
The FO had 325 hours total flying experience and was a cadet in training, with about 34 hours experience on the Metro.
Cadet training
Skippers Aviation partnered with a training organisation, accepting cadets with little prior aviation experience and providing a training captain for them while conducting Part 121 operations.[5] For this scheme, the operator had identified that new cadet FOs may have little prior aeronautical experience and so may be near capacity in normal operations of the aircraft and possibly unable to effectively handle emergency situations or support other crew during such an event.
The operator confirmed that significant training is conducted with training captains to ensure that pilots’ skills are developed in live operational environments while ensuring safety through operational oversight. Supervised line flying, line training and line checks were used to expose cadets to the operator’s procedures and to enable them to gain real time experience conducting authorised activities on the aircraft over the operator's network. Additional training requirements for cadet FOs included increased simulator training sessions and expanded line oriented flight training to 100 hours from 50 hours to improve preparedness for both routine and emergency scenarios.
Civil Aviation Safety Regulation 119 (Australian air transport operators, certification and management) Subpart 119.E (Training and checking for operational safety‑critical personnel) details how an approved company exposition assesses the competence of a flight crew member and the training and checking system.
Airport information
Perth Airport is the major international aerodrome in Western Australia. The main runway 03/21 is 3,444 m in length and the secondary runway 06/24 is 2,163 m in length; both runways are 45 m wide (Figure 3).
A system of interconnected taxiways connects runways with terminals, aircraft aprons and hangars. The captain reported using asymmetric power to taxi (as nose wheel steering was not functional due to the hydraulics failure) at walking pace via taxiways D and H to the operator’s apron.
Figure 3: Aerial view of Perth Airport showing the route used by VH-WAJ after landing

Source: Google Earth and QAR data annotated by the ATSB. Metro model not to scale.
Meteorological conditions
The terminal forecast for Perth Airport on the day of the occurrence was for intermittent rain showers and scattered low cloud. The wind was mainly from the west at 15–25 kt and visibility was reduced to 5,000 m at times with low cloud down to 1,500 ft.
Recorded information
The aircraft was fitted with a Fairchild model A200S cockpit voice recorder (CVR) which was transported to the ATSB technical facilities in Canberra for download. The recovered audio data contained 5 channels of high-quality audio with about 32 minutes recorded which included the descent, landing and taxi.
The recorded audio is consistent with the crew’s recollection at interview of the event and their discussions with ATC for the descent, landing and taxi.
Hydraulic system
The main hydraulic system on the Metro provides hydraulic pressure for actuation of the landing gear, flaps and nose wheel steering. Without the hydraulic system, the flaps, nose wheel steering and landing gear were inoperable and aircraft braking had limited functionality.
The nose wheel steering system provides directional control while taxiing, however the nose wheel casters move freely when the system is not engaged. Additionally, there is a self‑contained hydraulic power system for brake operation.
The main hydraulic system is pressurised by two engine‐driven hydraulic pumps (EDPs) and there is one manually‑operated hand pump. The hand pump draws reserve hydraulic fluid from the same reservoir as the EDPs and provides pressure for the emergency landing gear extension.
Normal system pressure is 2,000 psi. Two warning lights on the annunciator panel warn of low pump pressure or pump failure and a pressure gauge on the instrument panel is used to monitor the hydraulic system.
The brake hydraulic system is completely independent of the main hydraulic system used for landing gear and wing flap actuation. The power brake system includes master cylinders, brake accumulators and a pressure gauge. The brake accumulators, pre-charged with nitrogen (to 650 psi) and hydraulic fluid (from the aircraft main landing gear extension lines to 2,000 psi), provide back-up to the main hydraulic system in case of hydraulic pressure loss. The brake accumulators allow multiple brake applications without anti-skid protection until the pressure depletes to a minimum level. A pressure gauge monitors the hydraulic pressure in the accumulators showing normal levels during operation and residual pressure in the case of hydraulic fluid loss. When the accumulators bleed down to their minimum pressure, the brakes become unavailable.
If an emergency manual extension of landing gear is needed, the main hydraulic pressure gauge will continue to indicate approximately 2,000 psi system pressure (Figure 4). The captain recalled identifying that the hydraulic pressure read about 2,100 psi after landing.
Figure 4: Extract from operator’s QRH describing the pressure reading after landing gear emergency extension
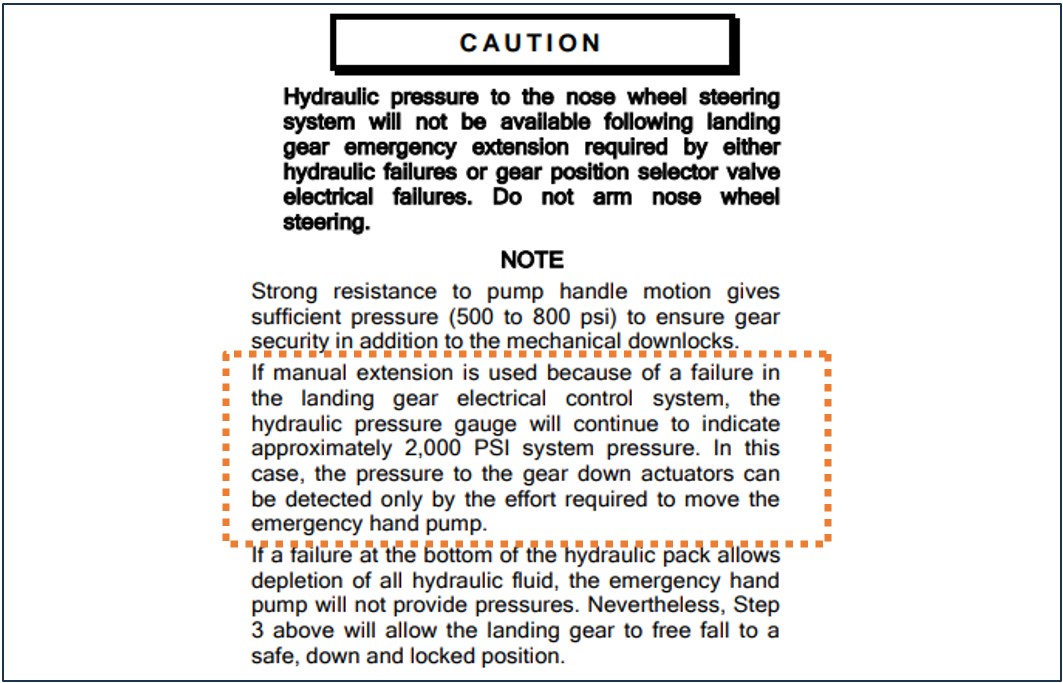
Source: Operator’s Quick Reference Handbook, annotated by the ATSB
QRH procedure for hydraulic pressure loss
The crew reported that they followed the checklist procedures from the operator’s QRH to manage the hydraulic system failure. Figure 5 shows extracts from the QRH detailing the procedure for management of a hydraulic system failure.
Figure 5: Partial extracts from the operator’s QRH for hydraulic failure management
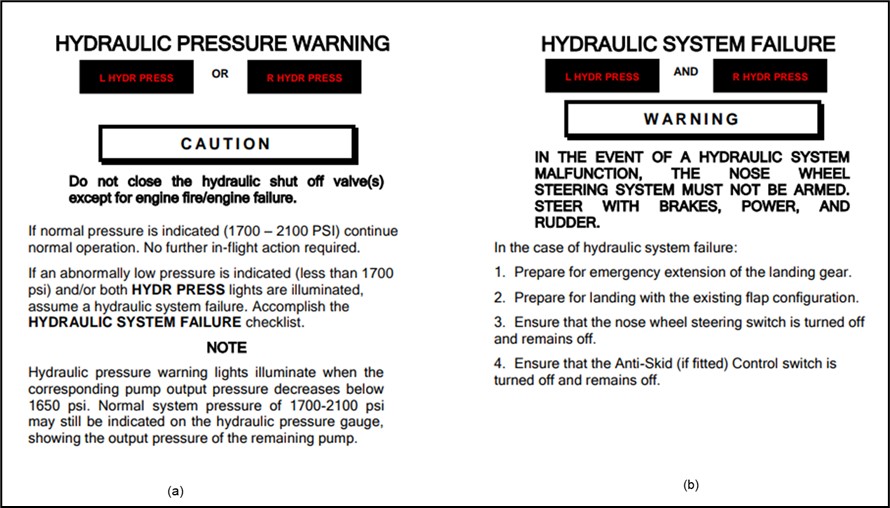
Source: Operator’s Quick Reference Handbook
The QRH also indicated that after landing with hydraulic system failure, the aircraft should have sufficient accumulator pressure to taxi clear of the runway.
Post‑event maintenance inspection
A post‑event maintenance inspection, conducted by the operator, indicated that the hydraulic system failure was due to a stress crack in the hydraulic pipe's union flare (located in the left landing gear wheel well). This crack allowed fluid loss, which then depleted the remaining hydraulic fluid and caused the warning lights to illuminate.
Flight crew workload
Descent, approach and landing phases are periods of high workload during normal operations due to the increase in task demand. In non-normal operations, such as equipment malfunction, workload levels escalate significantly for the crew who must assess and manage the abnormal conditions, complete additional tasks and make timely decisions under pressure.
At interview, the crew reported that the captain’s workload was very high at the time.
Research that has examined unexpected changes in workload during flight indicate that pilots who face abnormal or emergency situations experience a higher workload and increased number of errors, compared to pilots who do not encounter the same scenarios (Johannsen and Rouse, 1983).
During this time the captain was trying to involve the FO in the handling of the emergency situation by instructing them on the manual release of the landing gear.
Crew resource management
Crew resource management (CRM)[6] plays an important role in workload management and communication in the cockpit, particularly during non-normal situations. For the captain, who had to monitor the FO’s actions and provide instruction, this dual role led to task saturation and increased the likelihood of errors. The normal benefits of CRM to load-shed and delegate tasks can be unrealised when supporting flight crew have minimal experience in the aircraft type and low aeronautical experience.
Confirmation bias
Cognitive biases are mental shortcuts used to aid decision-making. Research points to most incidents of cognitive bias in flight operations happening during landing and at the end of their journey, with over 55% of incidents occurring in this phase (Nadri and others, 2024). A common bias is confirmation bias which describes a tendency for people to seek information and cues that confirm a tentatively held belief and not seek (or avoid) information that supports an opposite conclusion (Wickens & Hollands, 2000). Under high cognitive load this is amplified and individuals tend to focus on familiar or expected information reducing their openness to consider all relevant information (Liden, 2023).
Self-imposed pressure
Pilots may experience self-imposed pressure, for a range of reasons, that can form a desire to meet operational expectations. This pressure can manifest as a feeling to expedite tasks to avoid impacting schedules or inconveniencing other operators. The captain described that, after landing and bringing the aircraft to a stop on taxiway A, there was self-imposed pressure to clear the taxiway for incoming and outgoing aircraft.
Safety analysis
During a non-scheduled air transport flight from Forrestania to Perth, the crew of VH-WAJ experienced a complete loss of pressure in the hydraulic system. Without the hydraulic system, the flaps, nose wheel steering, and landing gear were not functional, however limited braking was available from a reserve pressure accumulator. The captain conducted a flapless landing and after stopping on the taxiway for a short moment, opted to continue the taxi to the operator’s hangar, mistakenly believing the hydraulic pressure had returned and that the brakes were functioning. In close proximity to the operator’s hangar, the crew applied the brakes to stop the aircraft while on a slight slope, but they were ineffective and the aircraft collided with the hangar, damaging the right wingtip and right propellor.
The complete loss of hydraulic pressure was identified post-flight as a result of a fluid leak from a hydraulic pipe crack in the union flare in the left main landing gear wheel well.
The training captain ordinarily had an increased physical and cognitive workload due to oversight of the aircraft and providing guidance for the novice FO. However, their workload surged considerably when the illumination of both hydraulic system warning lights required immediate management of the in-flight emergency. In addition to conducting the checklist procedures, the captain had the added responsibilities of all the radio communications and guiding the FO through the emergency task of the manual extension of the landing gear. Additionally, the captain assumed the role of pilot flying from the FO for the approach and landing at Perth. This contributed to the captain’s decision to continue taxiing to the apron after exiting the runway, as the demands of the emergency likely disrupted the typical task prioritisation for post-landing procedures after this event, which would have been to have the aircraft towed.
The FO’s inexperience and low number of hours on the Metro, while completing supervised line‑flying, reduced their capacity to contribute to decision-making, workload and task‑sharing in the same manner as a more experienced FO during the emergency. The FO’s unfamiliarity with non-normal procedures outside of the simulator meant that they were unable to anticipate the needs of the captain to help distribute the workload after the hydraulic system had failed. As a result, this limited their ability to fully support the captain, which negatively impacted CRM and further increased the captain’s workload.
The captain reported that they did not check the brake accumulator gauge after landing. It was likely that after using the brakes during landing, the reserve accumulator pressure became depleted, although this was not obvious based on the feel of the brakes when tested after stopping.
Both the in-flight positive pressure indication observed on the main hydraulic pressure gauge (due to the manual extension of the landing gear) and the report of no fluid on the runway mistakenly supported the captain‘s understanding that the pressure had returned to the aircraft and that the brakes were functional. The absence of establishing contact with a tow vehicle and being aware of other traffic requiring access to the taxiway, it is likely that the captain felt self-imposed pressure to continue to move the aircraft. This likely influenced the captain’s decision to continue to taxi to the hangar.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the hydraulics system failure involving Fairchild SA227-DC, registered VH-WAJ, at Perth Airport, Western Australia, on 12 August 2024.
Contributing factors
- A crack in a hydraulic line in flight resulted in a loss of hydraulic pressure and required the crew to manage the emergency.
- Following the hydraulic system failure, the captain was required to take-on both the pilot flying and pilot monitoring roles. This reduced the ability to effectively manage the emergency.
- The first officer's inexperience limited their ability to contribute to managing the hydraulic system failure. This negatively impacted crew resource management and increased the captain's workload
- After stopping on the taxiway, the captain mistakenly assumed the brakes were functioning. Unable to locate or contact the tow tug and influenced by self-imposed pressure, continued the taxi to the apron. Approaching a hangar, the crew applied the brakes, but they were ineffective and resulted in the right wingtip and propellor colliding with the hangar.
Safety actions
|
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence. Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence |
Safety action by the operator
- The flight crew received refresher training in human factors, standard operating procedures, workload management and decision‑making. Additionally, the captain has completed remedial training on decision‑making.
- The captain has completed a series of simulator exercises to confirm all procedures are followed in accordance with the QRH and company standards.
- During their fleet meeting, all fleet pilots were made aware of the incident and the lessons learnt to prevent reoccurrence.
- All fleet pilots have completed theory training and examination of the hydraulic system.
- Skippers Aviation is carrying out a review of maintenance practices for tube repairs and replacements for the fleet.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the captain and first officer
- Skippers Aviation safety manager
- video footage of the accident flight and other photographs taken on the day of the accident
- cockpit voice recorder.
References
Johannsen, G & Rouse, WB, (1983). Studies of planning behaviour of aircraft pilots in normal, abnormal, and emergency situations. Systems, Man and Cybernetics, IEEE Transactions on, (3), pp.267-278.
Nadri, C., Regalado, J., Ferris, T., & Zahabi, M. (2024). Cognitive Biases in Commercial Aviation: Empirical Review of Accident Reports. Proceedings of the Human Factors and Ergonomics Society Annual Meeting.
Wickens, C. D., & Hollands, J. (2000). Engineering psychology and human performance
(3rd ed.). Upper Saddle River, NJ: Prentice Hall.
Liden, M. (2023). Confirmation bias in criminal cases. Oxford University Press.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- captain and first officer
- Skippers Aviation (the operator)
- the Civil Aviation Safety Authority
- Airservices Australia
There were no submissions received.
[1] The hydraulic system controls movement of external components including flaps and landing gear.
[2] Specific directions to sequence an aircraft for the safe and efficient movement of aircraft in controlled airspace.
[3] PAN PAN: an internationally recognised radio call announcing an urgency condition, which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[4] Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[5] Part 121 of Civil Aviation Safety Authority (CASA) regulations cover air transport rules for larger aeroplanes.
[6] Crew resource management (CRM) refers to the effective use of all available resources: human resources, hardware, and information to achieve safe and efficient operation.