
Investigation summary
What happened
On 16 July 2023, a Bell 206B‑1 helicopter, registered VH‑ZDI, was being operated on a private flight from a rural property near Tumbarumba to Khancoban, New South Wales, with the pilot and 3 passengers on board. Shortly after take‑off, the pilot brought the helicopter into a hover around 7 ft above the helipad located near a hangar. The pilot then initiated a hovering turn to the left and reported that they were able to complete around 90º of an intended 180º turn before they experienced a shudder, and the helicopter began to rotate to the right. While continuing to rotate to the right for around 2 full rotations, the pilot attempted several pedal control inputs and was unable to regain directional control. The pilot elected to lower the collective, reducing height, and later closed the throttle. As the helicopter descended, the left skid contacted the soft earth beside the pad and broke off. The helicopter rolled over. The occupants were uninjured, and the helicopter was substantially damaged.
What the ATSB found
The helicopter was hovering in ground effect near an obstacle, the hangar. The high all-up weight of the helicopter would have strengthened the recirculation of downwash from the main rotor blades generated by the proximity to the hangar. The hovering left turn, initiated by the pilot, brought the tail of the helicopter from its position away from the hangar, where recirculation would be less, closer to the hangar where recirculation would be greater. It was likely that the flow of air through the tail rotor was disturbed, resulting in a loss of tail rotor effectiveness, which manifested as a right yaw.
The ATSB found that a miscalculation of fuel led to the helicopter being operated about 15 kg above the maximum take-off weight.
The ATSB also noted that the occupants were wearing 4- and 5-point restraints, and a helmet was worn by the pilot. The use of such items reduces the risk of injury to occupants in the event of an accident.
Safety message
Helicopter pilots should remain cognisant of the factors that may induce unanticipated yaw (a loss of tail rotor effectiveness), and that helicopter performance can be adversely affected by the proximity to obstacles, including terrain, vegetation, and buildings. If unanticipated yaw is encountered, prompt and correct pilot response is essential.
This accident also illustrated the importance of operating within the weight and balance limitations prescribed in the flight manual. A weight and balance calculation tool, such as a mobile application, can be a useful way to check hand calculations, but it must be validated to ensure that it accurately reflects the flight manual limitations.
The investigation
The occurrence
The pilot completed pre‑flight checks and did not identify any defects or outstanding maintenance issues with the helicopter. Following this, the pilot assisted the passengers to board the helicopter and secure their seatbelts. The pilot then briefed the front left seat passenger regarding the seatbelt mechanism and emergency locator transmitter activation. The front passenger had been in the pilot's other helicopter on previous occasions and the pilot stated that the passenger knew not to touch the anti-torque control pedals.[1]
Following a normal engine start, the take‑off commenced at about 1300 local time. As per their normal procedure when departing from this location, the pilot brought the helicopter into a hover around 7 ft, in ground effect,[2] above the helipad facing the hangar. They then initiated a left turn, which initially progressed as the pilot expected. There was no evidence to suggest that the rate of yaw was rapid or deviated from normal. The pilot reported that they were able to complete around 90° of an intended 180° turn before they experienced a shudder, which could be felt through the flight controls and airframe. The helicopter then began to rotate to the right.[3]
In response, the pilot reported that they first applied left, and then both right and left pedal inputs, in an attempt to control the right rotation. They did not recall if either of the left or right pedal stops were reached, nor did they notice any unusual resistance associated with the pedals. The pilot was unable to regain directional control and recalled that ‘nothing could stop’ the right yaw, when describing the pedal control inputs. After about 2 full rotations, the pilot lowered the collective,[4] reducing height, and closed the throttle just prior to the helicopter touching the ground.
Initially, the left skid contacted the soft earth beside the helipad and broke off. The helicopter then rolled over coming to rest on the left side. The pilot reported that they switched the fuel valve into the ‘off’ position as the helicopter contacted the ground. The front passenger was able to exit the helicopter with the assistance of the pilot. They then assisted the rear passengers to exit, whereupon all occupants moved away from the helicopter. The pilot collected fire extinguishers and discharged them into the engine exhaust. There were no injuries. The helicopter was substantially damaged.
The pilot initially reported the accident as a loss of tail rotor effectiveness,[5] but later stated that they believed that there had been a mechanical issue with the helicopter.
Figure 1: VH‑ZDI in final resting position

Source: McClaren Aviation, annotated by the ATSB
Context
Pilot information
The pilot obtained a private pilot licence (helicopter) in 2018. Their flying experience totalled around 300 hours, with about 260 hours on Bell 206 variants. In the 90 days prior to the accident, the pilot had flown 20 hours, all on VH‑ZDI. The pilot’s latest flight review was on 15 March 2023. The pilot reported feeling fully awake immediately preceding the accident, so fatigue was not considered as a contributing factor to the accident.
Helicopter information
VH‑ZDI was a Bell 206B‑1 helicopter, manufactured in 1976, by the Commonwealth Aircraft Corporation Pty Ltd for the Australian Army, powered by a single-engine Allison Gas Turbines 250‑C20 engine. In 2020, a special certificate of airworthiness in the ‘limited category’[6] was issued for the helicopter. At the time of the accident, the total time-in-service was 9,856.5 hours.
The helicopter was maintained in accordance with the Australian Warbirds Association Limited[7] Bell 206B‑1 Kiowa maintenance program. The latest maintenance was performed 15.4 flight hours (20 days) prior to the accident, on 26 June 2023. An engine power assurance check[8] was performed at that time, but the conditions under which this check was conducted could not be validated by the ATSB. The maintainer conducting this check assessed that the minimum acceptable torque requirement was met. A previous engine power assurance check performed on 11 March 2022, 16 months prior to the accident, also indicated the engine was producing above the minimum acceptable torque. No defects were noted in the technical logs.
The helicopter was fitted with an anti-torque control pedal lock‑out kit on the left pedal assembly. The kit is designed to disconnect the passenger pedals without the use of tools, allowing pilots the ability to quickly isolate the pedals to prevent passenger interference with the tail rotor during flight.
Helipad information
The helipad (Figure 2) was a concrete pad, large enough to accommodate the helicopter. It adjoined a hangar, with the terrain sloping downwards to the west, away from it. The centre of the helipad was around 16 m from the hangar. The elevation of the pad was about 1,962 ft.
Figure 2: Helipad location

Source: Google Earth, annotated by the ATSB
The method used to conduct a take‑off from the helipad was to push the helicopter out of the hangar tail first (towards the west) and position it such that the tail was over the downhill slope, affording the helicopter the greatest possible clearance from the hangar. The pilot would initiate a hover while facing the hangar, rotate left 180º, before commencing forward flight.
The pilot described experiencing helicopter-building interference from the hangar on other occasions. They stated that they had only experienced interference when they came into land and did not position the helicopter on the ground quickly. They likened the experience to rotor-head shake, bad turbulence, and bad air.
The pilot also stated that, though there was a lot of wildlife around the property, they did not observe any at the time of the accident. Furthermore, they ensured that items were stowed away and clear of the helipad.
Meteorological information
The Bureau of Meteorology analysis of weather observations around the Tumbarumba area found that a large high‑pressure system commonly associated with light winds and clear skies was present. This was consistent with the pilot’s recollections that it was not a windy day, that the wind was barely registering on the windsock, and it was about 15 ºC.
The Bureau of Meteorology did not have observations for Tumbarumba, the nearest airport. Instead, they provided observations for Wagga Wagga and Albury with the note that these airports were located on the same side of the ranges as Tumbarumba and experienced similar weather. Winds were very light, tending to a light to moderate north to north‑easterly and QNH[9] pressure was between 1026 and 1027 hPa. Visibility was greater than 10 km and no significant cloud was detected. Both airports recorded the temperature to be 15 ºC.
Wreckage examination
The ATSB’s examination of the site photographs provided by the pilot and the insurer found that the damage to the helicopter was consistent with a heavy landing and rollover event. The relative locations of the major components were consistent with power being supplied to the main rotor just prior to, or during, impact. The proximity to the ground and integrity of the occupant space contributed to a high probability of occupant survival.
ATSB investigators did not deploy to the site but inspected the wreckage once it was transported to a storage facility. No mechanical issues were identified during that inspection and there was no indication of pre-accident failure. The tail rotor and associated controls were inspected and showed no signs of failure, no restriction of normal operation, and no contact marks indicating a strike with a foreign object or animal. The exception to this was the inspection of the tail rotor control rigging, where system functionality was unable to be confirmed due to the airframe disruption. As a result, the possible contribution of a tail rotor control rigging error could not be eliminated.
While the helicopter was fitted with a pedal lock‑out kit on the left pedal assembly, the kit was not configured such that the passenger was ‘locked-out’. The pilot stated that they had never used the pedal lock‑out kit and were unfamiliar with its use. The passenger side cyclic control[10] was not present and there was no cover. The pilot stated that they removed the cyclic and that there was no cyclic control stub cover available. The passenger side collective was present.
The insurer’s assessment reported that they were not able to confirm the pre‑event serviceability of the tail boom attachment bolts. The tail boom was attached to the fuselage by 4 bolts. Two of the bolts had fractured and laboratory examination conducted by the ATSB identified that the failure of the bolts was consistent with overstress. There was no evidence of pre‑existing flaws or fatigue. Overall, the insurer concluded that the tail boom exhibited damage consistent with impact from a main rotor blade on the left side.
Weight and balance
Limits
The flight manual included forward and aft centre of gravity limits and specified that the maximum take-off weight (MTOW) for the helicopter was 3,200 lbs (1,452 kg). A type‑specific weight and balance assessment was performed on VH-ZDI on 30 June 2020. The resulting load data sheet listed the MTOW as 1,452 kg, the forward centre of gravity limit as 2,672 mm and the aft limit as 2,901 mm (Figure 4).
Calculations by the pilot
The pilot performed a weight and balance assessment prior to commencing the flight. In their handwritten calculations, the pilot included the weight and position of the 4 occupants and 430 lbs of JetA1 fuel. Calculation of the weight and centre of gravity required converting the fuel amount from the indicated units of lbs to kg, as all other amounts were measured in kgs. When converting the fuel from lbs to kg, the pilot mistakenly substituted volume, L, for mass, kg, and believed they had converted 430 lbs to 195 L (with the conversion factor of ÷2.2) (Figure 3). They subsequently converted 195 L to weight (with the conversion factor x0.8), arriving at 156 kg of fuel. This resulted in the pilot calculating the weight of the helicopter to be 1,428 kg (Figure 4). The pilot also listed the MTOW for the helicopter as 1,455 kg. This led the pilot to believe the helicopter was 27 kg under its MTOW.
Figure 3: JetA1 fuel conversion chart

Source: Airservices Australia, the pilot, annotated by the ATSB
The pilot used a third‑party application (App), iBal Rotary, as a secondary check to ensure that the helicopter was appropriately loaded. The pilot had selected ‘Sample Bell 206B3 (Bell 206B3 Jet Ranger)’ from the available models and input the 4 occupant details and 156 kg for fuel. The pilot was aware that this model selection did not represent VH‑ZDI and, to compensate, included an additional centre aft passenger weighing 100 kg as an adjustment to account for the unrepresentative model selection. The App indicated that the weight and balance of the selected model, which did not reflect the limits specified in the flight manual, was within limits.
According to the developer of the App, a more representative model selection for VH‑ZDI was the ‘Bell OH‑58A/C’.[11] The weight and balance envelope for the App ‘Bell OH‑58A/C’ model was sourced from the Operator's Manual Army Model OH-58 A/C Helicopter (Department of the Army (United States), 1989). This differed to the weight and balance envelope specified in the VH-ZDI flight manual but more closely resembled the flight manual than the model selected by the pilot. When the 4 occupants and 156 kg of fuel was input into the App with ‘Bell OH‑58A/C’ selected, the App indicated that the loading was within MTOW, but that the forward centre of gravity limit was exceeded. When the 4 occupants and 195 kg (430 lbs)[12] of fuel was input into the App, the App indicated that the helicopter loading had exceeded the MTOW.
Calculations by the ATSB
The ATSB performed a weight and balance calculation with the information provided by the pilot and determined the take‑off weight to be 1,467 kg with an associated moment arm of 2,715 mm (Figure 4). This exceeded the MTOW of the helicopter by 15 kg.
Figure 4: VH‑ZDI weight and balance limits and calculations

Source: Flight manual, load data sheet, and pilot, annotated by the ATSB
Operational information
Engine torque required and available
From the flight manual, the minimum engine torque required to hover for the accident conditions was about 61.9 psi and the minimum acceptable torque that the engine should produce under those conditions was about 68.6 psi.
Factors affecting performance
According to the United States Federal Aviation Administration (2019) Helicopter Flying Handbook:
A helicopter’s performance is dependent on the power output of the engine and the lift produced by the rotors, whether it is the main rotor(s) or tail rotor. Any factor that affects engine and rotor efficiency affects performance. The three major factors that affect performance are density altitude,[13] weight, and wind.
An increase in density altitude can affect helicopter performance by reducing the hovering ceiling, operating margins, and rate-of-climb performance. The higher the gross weight, the greater the lift or rotor thrust required for hovering or climbing. Therefore, the margin between the engine power available and the power required to hover at higher weights and density altitudes may often be small for helicopters (Civil Aviation Authority of New of Zealand, 2020). The Helicopter Flying Handbook noted that, while more engine power was required during the hover than in any other phase of flight, if a hover could be maintained, a take-off could also be made.
Recirculation and helicopter-building interference
Recirculation is a type of interference between a helicopter and its surroundings (Royal Air Force (UK), 2010). According to the UK AP3456 Central Flying School (CFS) Manual of Flying, Volume 12 – Helicopters:
Whenever a helicopter is hovering near the ground, some of the air passing through the disc is recirculated and it would appear that the recirculated air increases speed as it passes through the disc a second time (Figure 5). This local increase in induced flow near the tips gives rise to a loss of rotor thrust.
Recirculation will increase when any obstruction on the surface or near where the helicopter is hovering prevents the air from flowing evenly away. Hovering close to a building, wire link fencing or cliff face may cause severe recirculation (Figure 6).
Figure 5: Helicopter hovering near the ground with recirculated air
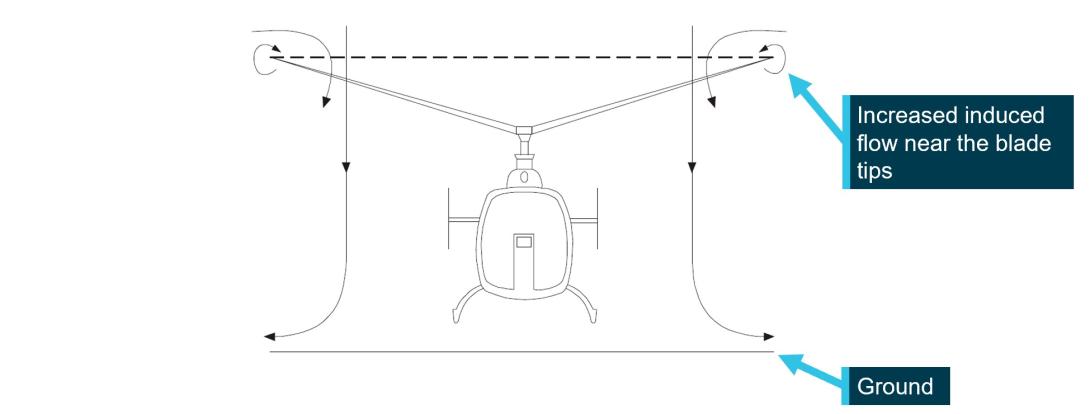
Source: Royal Air Force (UK) (2010), annotated by the ATSB
Figure 6: Recirculation near a building
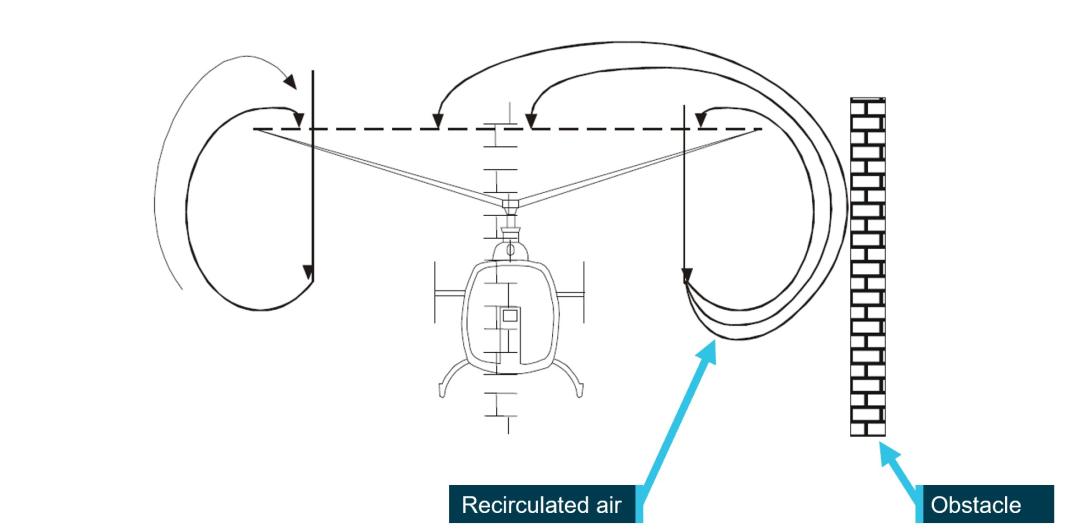
Source: Royal Air Force (UK) (2010), annotated by the ATSB
The section of the rotor disc largely affected by recirculation was the side closer to the obstruction (right side of disc in Figure 6). A tail rotor positioned on the far side of the helicopter relative to the obstacle would experience less recirculated air than a tail rotor positioned on the near side.
Łusiak et al. (2009) described wind tunnel testing of a model helicopter with surrounding elements (buildings). Their paper stated:
The phenomenon of interference between the helicopter and the surrounding elements appears with a visible intensity when the helicopter operates at a low speed in the near vicinity of objects with specific geometrical shapes, such as buildings or ship hulls.
All computational analyzes and experimental investigations which were performed in order to study the mutual helicopter-building interaction indicate that in the considered specific situations the phenomenon of aerodynamic interference can seriously disturb the flow around the helicopter and change the loading of some of its elements. Substantial changes in the value of the resulting loads can make the helicopter difficult to control.
Wagtendonk (2011) discussed recirculation within the context of confined area operations, which included the following points:
As rotor downwash strikes the surface it splits, and a large part diffuses horizontally. If obstructions such as buildings or trees interfere with the escaping airflow, it moves vertically up the obstruction and re-enters the disc from above, increasing the induced flow.
The greater the gross weight, the stronger the downwash and the greater the degree of recirculation.
The lower the hover height, the stronger the outbound flow and the greater the degree of recirculation.
The more solid the obstruction, the greater the recirculation. Hovering close to large buildings (such as hangars) creates more recirculation than hovering near trees.
The highest velocity of horizontal outflow escaping from beneath the helicopter occurs at a distance that is roughly 30 percent of the disc diameter beyond the disc tip. For example, with a 30-foot disc the highest velocity occurs about 10 feet away from the tips. Although the velocity beyond that distance decreases sharply, substantial horizontal velocity values can still be encountered.
Recirculation can occur when obstructions are reasonably far away from the disc tip, but in general, the shorter the distance, the greater the risk of recirculation.
Loss of tail rotor effectiveness
The emergency procedures section of the flight manual for VH‑ZDI identified loss of tail rotor effectiveness[14] as an anti‑torque system malfunction. As the main rotor rotated in the anti‑clockwise direction when viewed from above, in instances of anti-torque system malfunction the helicopter will most likely yaw to the right.
The flight manual stated:
The prime contributing causes of LTE[15] are:
a. Tail Rotor Vortex Ring. This condition may be encountered with wind azimuths caused by crosswinds, left sidewards flight, or right pedal turns.
b. Weather Cock Stability. Wind azimuths aft of the beam will cause the helicopter to weather cock.
c. Main Rotor Vortex Interference. Certain wind azimuths will cause the tail rotor to ingest main rotor vortices.
d. Tail Rotor Precessional Flapping. High yaw rates will cause the tail rotor to precess. This, coupled with the pitch change characteristics of the tail rotor flapping hinge, will reduce tail rotor thrust.
e. High Gross Weight. High gross weights require increased torque and reduce tail rotor operating margins.
f. High Density Altitude. High DAs[16] require increased torque and reduce tail rotor operating efficiency.
g. Ground Vortex Interference. Interaction between the main rotor vortex and the ground can reduce tail rotor efficiency.
h. Limited Directional Control Margin. Right relative wind azimuths reduce left pedal travel margins.
i. Governor Droop. Governor droop leads to main rotor RPM droop. This requires increased torque to accelerate the rotor and also reduces tail rotor efficiency.
j. Low Airspeed. The aircraft is dynamically unstable in the yawing plane at low airspeed.
The best recovery technique detailed for ‘Loss of Tail Rotor Effectiveness’ was:
1. Pedal – Full left.
2. Cyclic – Forward.
3. Collective – Reduce if altitude permits.
4. Adjust controls for normal flight as control is regained.
If yaw cannot be controlled and an uncontrolled landing is imminent:
5. Throttle – CLOSED.
6. Collective – Autorotate.
7. Pedal – Full left until yaw stops.
The United States Federal Aviation Administration has produced advisory circular 90-95 that related to loss of tail rotor effectiveness, which they also term ‘unanticipated yaw’. The recommended recovery techniques in the circular were:
a. If a sudden unanticipated right yaw occurs, the pilot should perform the following:
(1) Apply full left pedal. Simultaneously, move cyclic forward to increase speed. If altitude permits, reduce power.
(2) As recovery is effected, adjust controls for normal forward flight.
b. Collective pitch reduction will aid in arresting the yaw rate but may cause an increase in the rate of descent. Any large, rapid increase in collective to prevent ground or obstacle contact may further increase the yaw rate and decrease rotor rpm.
c. The amount of collective reduction should be based on the height above obstructions or surface, gross weight of the aircraft, and the existing atmospheric conditions.
d. If the rotation cannot be stopped and ground contact is imminent, an autorotation may be the best course of action. The pilot should maintain full left pedal until rotation stops, then adjust to maintain heading.
Survival aspects
Seatbelts
The helicopter was fitted with 5‑point turn‑to‑open restraints in the front seats and 4‑point lift‑latch‑to‑open restraints in the rear seats. Zimmermann and Merritt (1989) stated that:
- The overall probability of survival in an accident depends to a large extent on the manner of the restraint.
- The use of upper and lower torso restraints to prevent such critical body parts as the head and chest from striking surrounding structure can significantly reduce the probability of serious or fatal injury under given accident conditions.
- Studies have shown the addition of a shoulder harness greatly reduced injuries from head impacts and maintain proper spinal alignment. The further addition of a lab belt tie down strap (crotch strap on a 5-point harness) may nearly double the tolerance to impact forces.
Helmets
The Flight Safety Foundation (2022) stated that the primary purpose of a helmet was to provide impact protection and thereby reduce the risk of head injury in the event of an accident. The helmet worn by the pilot was damaged (Figure 7), indicating that the helmet sustained an impact during the accident sequence.
Figure 7: Top view of helmet worn by the pilot of VH‑ZDI showing damage

Source: Pilot, annotated by the ATSB
Similar occurrences
A search of the ATSB’s occurrence database for helicopter incidents, serious incidents, or accidents with the occurrence category ‘loss of control’ or ‘control issues’ from 2013 onwards returned 151 results. Eight of these occurrences contained sufficient information to be identified as unanticipated yaw or loss of tail rotor effectiveness. None of the occurrences related to helicopter‑building interference.
The 3 examples detailed below include an occurrence where the pilot was able to recover directional control, one that took place in a confined landing site with nearby obstacles, and an international event where helicopter-building interference was a probable factor.
ATSB investigation AO-2015-091
On 20 July 2015, the pilot of a Bell 206L3 (LongRanger) helicopter, registered VH-BLV, conducted a charter flight from Essendon Airport to Falls Creek, Victoria, with 5 passengers on board. The pilot refuelled at a property near Lake Eildon and departed close to its MTOW.
On approach to the helipad at Falls Creek, the pilot assessed that there was insufficient power available to continue to land and elected to abort the approach. The pilot pushed forward on the cyclic to increase the helicopter’s airspeed and conducted a left turn towards the valley whereupon the helicopter started to yaw rapidly to the right. The pilot applied full left pedal to counteract the yaw, but the helicopter continued to yaw. The helicopter turned through one and a half revolutions, as the pilot lowered the collective. Lowering the collective reduced the power demand of the power rotor system, thereby increasing the ability of the anti-torque pedals to stop the right yaw. The combination of lowering collective and applying forward cyclic to gain forward airspeed, allowed the pilot to regain control of the helicopter. The pilot then conducted a left turn towards the helipad and made an approach to the helipad from an easterly direction. The helicopter landed following the second approach without further incident.
ATSB investigation AO-2022-060
On 19 November 2022, the pilot of a Robinson Helicopter Company R44, registered VH-TKI, was conducting a private flight from a nearby property to a function centre at Forresters Beach, New South Wales with 2 passengers onboard. The proposed landing site was the carpark of the venue and was considered a confined area due to the proximity of roads, powerlines, and palm trees.
During the approach, the pilot reported an uncommanded yaw to the right, which was unable to be recovered. The ATSB found that, during the approach to a confined area landing site, the helicopter experienced a loss of tail rotor effectiveness and accompanying right yaw. The pilot’s response was ineffective at recovering control. The position of the helicopter on approach to the confined area was such that it could not be established if control of the helicopter could have been recovered before colliding with powerlines and terrain. The occupants received minor injuries and the helicopter was substantially damaged.
Federal Safety Investigation Authority (Austria) investigation reference: 2020-0.701.771
On 20 July 2018, a privately‑owned Airbus Helicopters AS350B, registered N36033, was destroyed while the pilot attempted to hover taxi closer to a fuelling station at Wolfsberg airfield in Austria (Aerossurance, 2020; Federal Safety Investigation Authority (Austria), 2020). The pilot, who did not hold a valid licence, sustained a minor leg injury. At the time the wind was 1 to 2 kt.
After lifting into a 1 m hover there were excessive pitching movements forwards and backwards and the helicopter yawed around 90° to the right. The pilot reported feeling turbulence from the side of the fuelling station building, which was a 5.2 m x 5.2 m, flat‑roofed building, 3.2 m high. The Austrian Federal Safety Investigation Authority determined the probable cause was a loss of lateral control during hover in ground effect. The probable factors were:
- excessive control inputs
- flight crew induced oscillations about the helicopter longitudinal axis
- lack of corrective action to stop flight crew induced oscillations
- proximity of obstacles
- formation of ground effect air vortices in ground effect.
Safety analysis
Loss of tail rotor effectiveness
The ATSB considered several reasons to explain the unanticipated right yaw. Although the pilot described a shudder immediately prior to the right yaw, which could have indicated a mechanical issue, examination of the helicopter and maintenance documents did not reveal any anomalies. A wildlife strike or contact with a foreign object was considered but there was no indication of strikes on the rotors, a strike on the hangar, or animal remains to support this hypothesis. Inadvertent interference from the front seat passenger was also explored. This possibility was unlikely as the pilot did not feel any resistance when manipulating the anti-torque pedals.
While the helicopter was loaded above the MTOW, at the estimated density altitude for the time of the accident, the helicopter likely had sufficient power available to sustain a hover in-ground effect. Additionally, the left turn was not likely to be at a rapid yaw rate, and the weather conditions were calm.
During the hover, the helicopter was in a position close to an obstacle, the hangar, where helicopter-building interference was known to have occurred in the past. As described by Wagtendonk (2011), the obstacle would have prevented downwash from the main rotor escaping and the air would have recirculated. This recirculation would have been strengthened by the high all-up weight of the helicopter.
The literature indicated that the side of the main rotor disc closest to the obstruction would be more affected than the side further from the obstruction. Furthermore, recirculation from obstacles, such as buildings, can disturb the airflow though the disc, which can result in random movements and controllability difficulties. The hovering left turn, initiated by the pilot, brought the tail of the helicopter from its position away from the hangar, where recirculation would be less, closer to the hanger where recirculation would be greater. This was a position where the air flow through the tail rotor was more likely to be disturbed. Disturbance to the flow through the tail rotor, to an extent that the anti-torque forces could no longer overcome, likely account for the unanticipated right yaw. The pilot had likened their previous experience to turbulence or ‘bad air’, which could potentially explain the shuddering.
Helicopter-building interference is a variation on one of the contributors to a loss of tail rotor effectiveness described in the flight manual, specifically, ground vortex interference. Instead of the interference being generated from the proximity to the ground, it is generated by close proximity to a building. Therefore, with insufficient evidence to support other potential reasons for the unanticipated right yaw, it was likely that, as the left turn brought the tail rotor closer to the hangar, with recirculation strengthened by the high all-up weight, the flow of air through the tail rotor became disturbed. As a result, a loss of tail rotor effectiveness occurred, and the helicopter began to yaw right.
Once the right yaw initiated, the pilot’s control input included both left and right pedals. This was not consistent with the recommended procedures in the flight manual and advisory circular 90-95 for loss of tail rotor effectiveness, which stated that full and sustained left pedal input was required. This did not give the pilot the best opportunity to regain directional control. Ultimately, the pilot reduced the throttle, but this did not prevent the helicopter from colliding with the terrain.
Maximum take-off weight (MTOW) exceedance
When manually calculating the weight and balance of the helicopter, the pilot inadvertently made an error when converting the fuel load from lbs to kg. Their calculation indicated that the helicopter weight was 27 kg under the MTOW.
When the hand calculation appeared to be acceptable, the pilot used the third-party App for verification. The pilot was aware that the model selected in the App did not represent VH‑ZDI and added an unverified correction factor. Under these conditions, the App confirmed that the loading of the helicopter was within limits. Had the pilot selected the model that the App developer stated more closely reflected VH‑ZDI, the App would have shown that the centre of gravity was beyond the forward limit, even with the fuel conversion error. It is worth noting that third‑party applications are not a controlled source of information, and the flight manual and manufacturer’s documentation is the authoritative source of information.
Applying the required conversion factor, the ATSB weight and balance calculation established that the helicopter was loaded in a way that exceeded the MTOW by around 15kg. Had the pilot not made the conversion error and instead identified that the MTOW was exceeded, it was unlikely that they would have proceeded with the planned flight.
Operation at higher helicopter weights can affect performance and controllability, and potentially exacerbate other conditions such as helicopter-building interference. It is not known what loading configuration would have been sufficiently conservative such that the helicopter-building interference would not have resulted in a loss of control for the conditions. Regardless, compliance with the limitations set out in the flight manual remains vital for safe helicopter operation.
Survivability
The front occupants of the helicopter were wearing 5‑point turn‑to‑open restraints, while the rear occupants were wearing 4‑point lift‑latch‑to‑open restraints. The pilot was also wearing a helmet, on which only minor damage was observed. There was no comparative evidence, such as, one occupant with a seatbelt and one without to determine whether the severity of the accident was such that the occupants would have sustained greater injury if they were not wearing seatbelts. Nevertheless, the literature indicated that the use of upper and lower torso restraints and helmets reduces the risk of injury.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision with terrain involving Bell 206B‑1, VH‑ZDI, 9.3 km south-south‑east of Tumbarumba, New South Wales, on 16 July 2023.
Contributing factors
- After lift-off and initiating a hover turn to the left, while operating at a high all-up weight, it was likely that the helicopter’s tail rotor encountered helicopter-building interference from the hangar, which resulted in a loss of tail rotor effectiveness, and a subsequent collision with terrain.
Other factors that increased risk
- Errors when calculating the weight and balance for the flight likely resulted in the maximum take-off weight being exceeded by 15 kilograms.
Other findings
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot
- the flight instructor of the pilot
- maintenance organisations for VH‑ZDI
- the weight and balance application developer
- Bureau of Meteorology
- Civil Aviation Safety Authority.
References
Aerossurance. (2020). Helicopter Destroyed in Hover Taxi Accident. Aerossurance. Accessed 26 September 2024. https://aerossurance.com/helicopters/hover-taxi-accident/
Australian Transport Safety Bureau. (2015). Loss of control involving a Bell 206L3, VH-BLV Falls Creek, Victoria, on 20 July 2015 [ATSB Transport Safety Report](Aviation Occurrence Investigation AO-2015-091). https://www.atsb.gov.au/publications/investigation_reports/2015/aair/ao-2015-091
Australian Transport Safety Bureau. (2023). Collision with terrain involving Robinson Helicopter Company R44, VH-TKI, Forresters Beach, New South Wales on 19 November 2022 [ATSB Transport Safety Investigation Report](Aviation Occurrence Investigation (Short) AO-2022-060). https://www.atsb.gov.au/publications/investigation_reports/2024/report/ao-2022-060
Civil Aviation Authority of New of Zealand. (2020). Helicopter Performance [Good Aviation Practice]. Accessed 9 January 2024. https://www.aviation.govt.nz/assets/publications/gaps/helicopter-performance.pdf
Civil Aviation Safety Authority. (2018). Limited category aircraft - operation [Advisory Circular](AC 132-01v1.1). File ref D17/105699.
Department of the Army (United States). (1989). Operator's Manual Army Model OH-58 A/C Helicopter [Technical Manual](TM 55-1520-228-10).
Federal Safety Investigation Authority (Austria). (2020). Accident involving the helicopter type AEROSPATIALE AS350B on 20.07.2018 at approximately 06:33 UTC at Wolfsberg airfield, A-9400 Wolfsberg, Carinthia [Investigation report](Reference: 2020-0.701.771).
Flight Safety Foundation. (2022). Basic Aviation Risk Standard Implementation Guidelines (Version 9). https://flightsafety.org/bars/the-bar-standards-and-manuals/
Łusiak, T., Dziubiński, A., & Szumański, K. (2009). Interference between helicopter and its surroundings, experimental and numerical analysis. Task Quarterly, 13(4), 379-392.
Royal Air Force (UK). (2010). AP3456 The Central Flying School (CFS) Manual of Flying (Volume 12 - Helicopters). Revised November 2013.
Royal Australian Navy. (n.d.). Bell Kiowa 206B-1 [Webpage]. Accessed 7 February 2024. https://www.navy.gov.au/aircraft/bell-kiowa-206b-1
United States Federal Aviation Administration. (1995). Unanticipated right yaw in helicopters [Advisory Circular: 90-95]. Accessed 3 October 2023. https://www.faa.gov/regulations_policies/advisory_circulars/index.cfm/go/document.information/documentid/23136
United States Federal Aviation Administration. (2019). Helicopter Flying Handbook (FAA-H-8083-21B). Department of Transportation (U.S.). Accessed 9 February 2024. https://www.faa.gov/regulations_policies/handbooks_manuals/aviation/helicopter_flying_handbook
Vietnam Helicopter Museum. (28 March 2016). OH-58C Kiowa Helicopter [Webpage]. Accessed 7 February 2024. https://www.vietnamhelicopters.org/oh-58c-kiowa/
Wagtendonk, W. J. (2011). Principals of Helicopter Flight (Second revised ed.). Aviation Supplies & Academics, Inc.
Zimmermann, R. E., & Merritt, N. A. (1989). Aircraft crash survival design guide: Volume I Design criteria and checklists [Final Report](AD-A218 434, TR 89-D-22A). Aviation Applied Technology Directorate.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the pilot
- the maintenance organisations for VH‑ZDI
- the weight and balance application developer
- Civil Aviation Safety Authority.
Submissions were received from the weight and balance application developer. The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Anit-torque control pedals: A primary helicopter flight control that changes the pitch of tail rotor blades and thereby affects thrust to provide heading control in the hover and balanced flight when the helicopter is in forward flight.
[2] When hovering within about one rotor diameter of the ground, the performance of the main rotor is affected by ground effect. A helicopter hovering in ground effect requires less engine power to hover than a helicopter hovering out of ground effect. That is, when hovering close to the ground, the air being drawn down through the rotor collects under the helicopter and provides a ‘cushion’ of air, requiring slightly less power than would otherwise be required.
[3] In a single main rotor helicopter, where the main rotor rotates in the anti-clockwise direction when viewed from above, the main rotor generates lift but also generates a torque that causes the body of the helicopter to turn in the nose right direction. A tail rotor is a common means to provide the anti-torque needed to counteract this effect, such that the heading of the helicopter can be controlled.
[4] Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[5] Loss of tail rotor effectiveness, also called unanticipated yaw, is a critical, low‑speed aerodynamic flight characteristic, which can result in uncommanded rapid yaw rate that does not subside of its own accord and, if not corrected, can result in the loss of control (United States Federal Aviation Administration, 1995).
[6] The ‘limited category’ permits the use of helicopters (ex-military) in a civil environment with regulations that prescribe how, where, and by whom these helicopters may be operated in order to ensure that public safety is not compromised by their civil operations. (Civil Aviation Safety Authority, 2018).
[7] Australian Warbirds is the administering body for all limited category (ex-military and historic) aircraft operations in Australia. Through delegations granted by the Civil Aviation Safety Authority, Australian Warbirds issues certificates of airworthiness, oversees maintenance systems for limited category aircraft, provides safety guidance, manages adventure flight operations, and facilitates permit index assessments.
[8] Power assurance checks compare the torque gauge reading with the minimum acceptable torque value for the particular power setting, pressure altitude, and temperature. If the torque achieved exceeds the minimum acceptable torque value, then the engine is producing sufficient torque.
[9] QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[10] Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[11] The Bell 206B‑1 Kiowa was a helicopter acquired by the Australian Army in 1971 (Royal Australian Navy, n.d.), whereas the OH‑58 Kiowa is a different model and was manufactured by Bell Helicopters for the U.S. Army (Vietnam Helicopter Museum, 28 March 2016).
[12] The 430 lbs fuel value was converted to 195 kg and used in the calculation.
[13] Density altitude: the altitude in the standard atmosphere corresponding to a particular value of air density.
[14] While loss of tail rotor effectiveness was included under the heading ‘anti‑torque system malfunctions’, the phenomena is not related to a maintenance malfunction (Federal Aviation Administration, 1995).
[15] Loss of tail rotor effectiveness.
[16] Density altitudes.