
Executive summary
What happened
Early on the morning of 2 March 2024, BHP Western Australia Iron Ore trains M05519A and M05519B were stopped 232 m apart, queued to be unloaded at BHP’s Finucane Island Balloon Loop, near Port Hedland, Western Australia. At about 0425 local time, the driver of M05519A slowly moved their train 325 m forwards to the handover point, where the train would be prepared for unloading.
As train M05519A came to a stop, the driver of train M05519B began to move their train forwards, intending to stop 200 m behind train M05519A. Over the next 6 minutes, train M05519B accelerated to a maximum speed of 12 km/h, and the driver acknowledged 4 audible alerts of the locomotive’s vigilance system. However, there was no brake application or reduction in throttle during that time, resulting in the train colliding with the rear of train M05519A. The driver was uninjured and there was no damage to the rollingstock.
What the ATSB found
The ATSB found that the driver of train M05519B had been experiencing stress, sleeping with the light on, and waking often, resulting in poor quality sleep. As a result, on their fourth consecutive night shift, during darkness and while experiencing low workload, the driver set the train in motion while in a degraded level of alertness, possibly associated with a microsleep, and did not detect the impending collision.
The ATSB also found that without awareness or memory of having done so, the driver acknowledged 4 audible vigilance alerts, which, by design, prevented a penalty brake application. This resulted in a low-speed collision with stationary train M05519A.
What has been done as a result
Following the collision, BHP undertook a series of actions to manage fatigue and the limitations of the vigilance systems in the SD70Ace/LCi locomotives.
BHP reviewed the fatigue risk periods for their fly-in fly-out (FIFO) rail operations driver rosters, and increased the number of fatigue assessments during each rotation. Fatigue assessments are now conducted on each of the first 5 night shifts and on the first and fourth day shifts of each rotation. These assessments are conducted face-to-face with the on-shift supervisor or coordinator at each depot location.
BHP is also implementing an additional check-in per shift, to be conducted with the rail crew team member either face-to-face or electronically via phone or radio. To support this activity, BHP employed additional resources to support existing operations supervisors and superintendents to identify and monitor fatigue concerns within the rostering environment.
Additionally, research was conducted into the viability of an interactive fatigue assessment tool (FAT), delivered through a mobile application, to improve the quality of fatigue assessments. A trial of the FAT was scheduled to commence at the end of November 2024.
BHP also proposed several changes to the vigilance system installed on their SD70Ace/LCi locomotives, including changing from fixed-time intervals to random intervals for the countdown, and limiting consecutive alerter resets to require different inputs and eliminate ‘muscle memory’.
Safety message
Adequate sleep duration is important, but sleep quality is also important. Of the factors that affect sleep, light has the most profound effect on the sleep-wake cycle. Exposure to light promotes wakefulness and darkness is necessary for deep restorative sleep. Exposure to sun or blue light, before and during sleep, also results in fragmented sleep and reduces the amount of deep restorative sleep. Stress also negatively affects sleep quality and creates hyperarousal that can mask symptoms of tiredness and fatigue. An increasing deficit of restorative sleep increases the body’s sleep drive and can result in reduced levels of alertness during waking hours, as well as napping, dozing, and microsleeps outside of planned sleep times.
Effective fatigue management includes self-reporting of fatigue or factors likely to contribute to fatigue. Conditions such as stress and interrupted sleep that affect sleep quality should prompt workers to assess and report an elevated risk of fatigue even if sleep quantity may be adequate. Use of fatigue reporting mechanisms is essential for an organisation to be able to apply mitigation strategies to address the associated risks.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
Late at night on 1 March 2024, at the Mooka staging facility (about 32 km south-south-east of Port Hedland, Western Australia) train M05519, operated by BHP Western Australia Iron Ore, was divided into 2 single-crew trains. The 2 trains, M05519A (train A) and M05519B (train B), were each about 1.4 km long, consisting of 2 Progress Rail EMD SD70Ace/LCi Locomotives, short-end leading, followed by 135 wagons loaded with iron ore. A flashing red LED light was secured on the last wagon of each train as an end-of-train marker.
Train A, followed by train B, proceeded towards BHP’s Finucane Island facility at Port Hedland, which consisted of a standard-gauge dual track balloon loop servicing 2 car dumpers (CDs), where iron ore wagons were emptied. Emptying occurred under the authority of a dumper operator, in a semi-automated process where wagons were rotated to dump their contents, and control arms progressed each rake through the dumper facility. As the emptying process could take up to several hours, drivers would secure and hand over the train, then head to the control room for a short break before being assigned a further task.
At about 2320 local time, train A entered Finucane Island yard limits.[1] Within the yard limits, drivers had authority to move their train up to the owner transfer point (OTP) board for the relevant CD (Figure 1). There were no signals and limited controller oversight of the section between the yard limits board and the OTP board, and train drivers were responsible for visually maintaining separation with other rail traffic. Train A slowly progressed, before coming to a stand between 28 points and the OTP board for CD4, where it remained between 0156 and 0425 on 2 March 2024.
Figure 1: Finucane Island facility showing car dumper 4 and its owner transfer point

Source: Google Earth, annotated by the ATSB
At about 0200, having been stopped by train control for one hour at an en route yard, train B was authorised to enter Finucane Island yard limits and, at 0220, came to a stand 260 m behind train A. The entirety of train B was stopped between 26 and 27 points, the section of track with the steepest uphill grade before the car dumpers. Train B remained stopped in that location from 0220 until 0327 (Figure 2).
Figure 2: Diagrammatic representation of train positions from 0220 to 0327
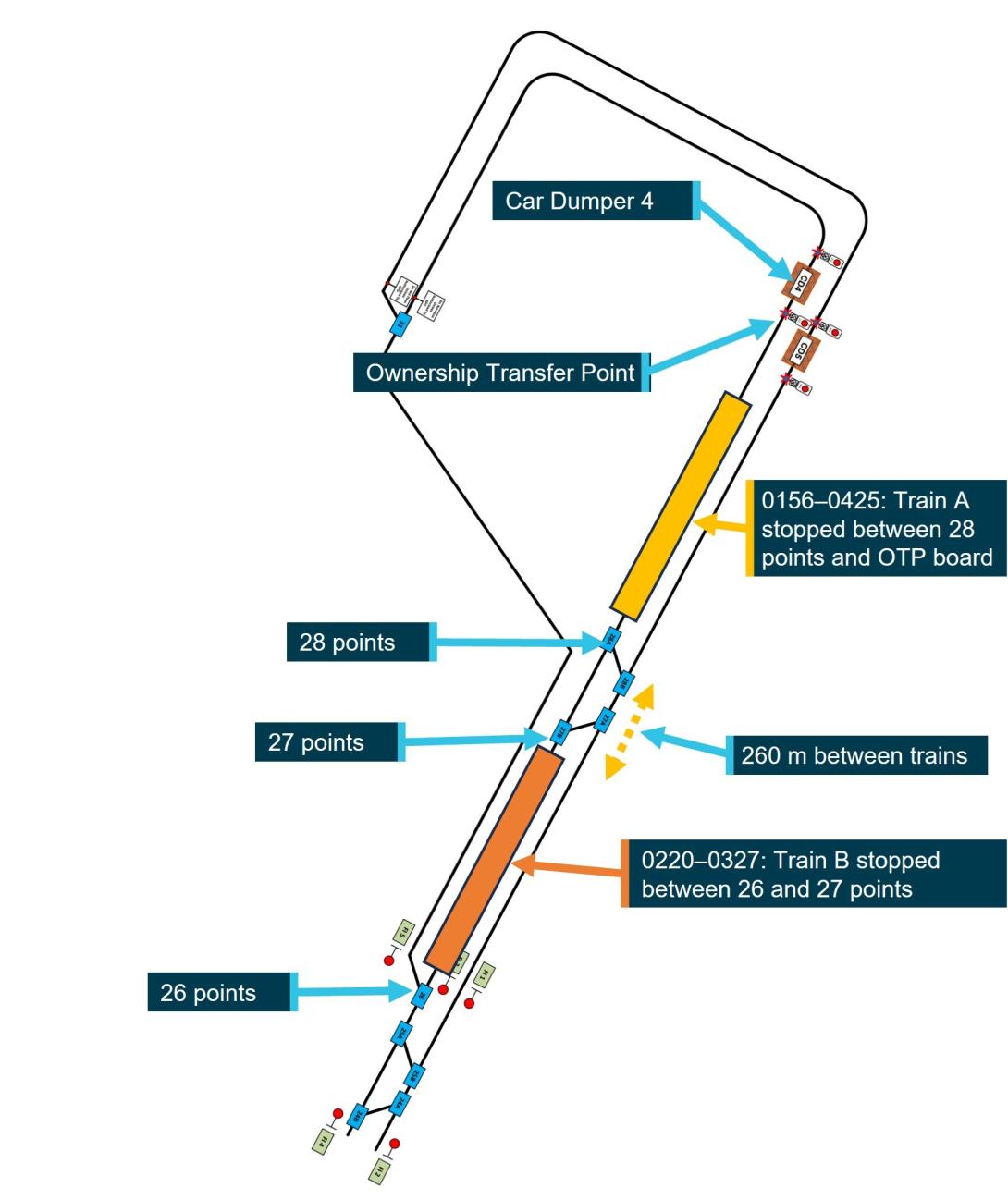
Not to scale
Source: BHP, annotated by the ATSB
Recorded locomotive data for train B showed that between 0327 and 0331, the driver moved the train forward 27 m before briefly coming to a stand. At 0334, the driver moved the throttle to 1 notch,[2] the train moved forward 1 m then stopped, and the driver applied the independent brake at 0340. Train B was then 232 m behind train A and remained there with the throttle in 1 notch and the brake on, which deactivated the vigilance system (see the section titled Locomotive vigilance system), until 0400 when the driver moved the throttle to idle.
The driver of train B reported that while waiting for the train in front to move, they monitored the radio, swept and cleaned out the cab and spent some time standing outside on the locomotive’s footplate. At that time, the half-moon was above the horizon, and it was a clear night.
At 0425, after the preceding train departed CD4, the driver of train A placed the throttle into 2 notch, applying sufficient tractive effort to slowly move the train 325 m to the OTP board, before coming to a stand at 0432 (Figure 3). Train A’s driver then awaited authority from the dumper operator to start the process for the train to proceed into CD4 and commence unloading.
Figure 3: Diagrammatic representation of train positions at 0432
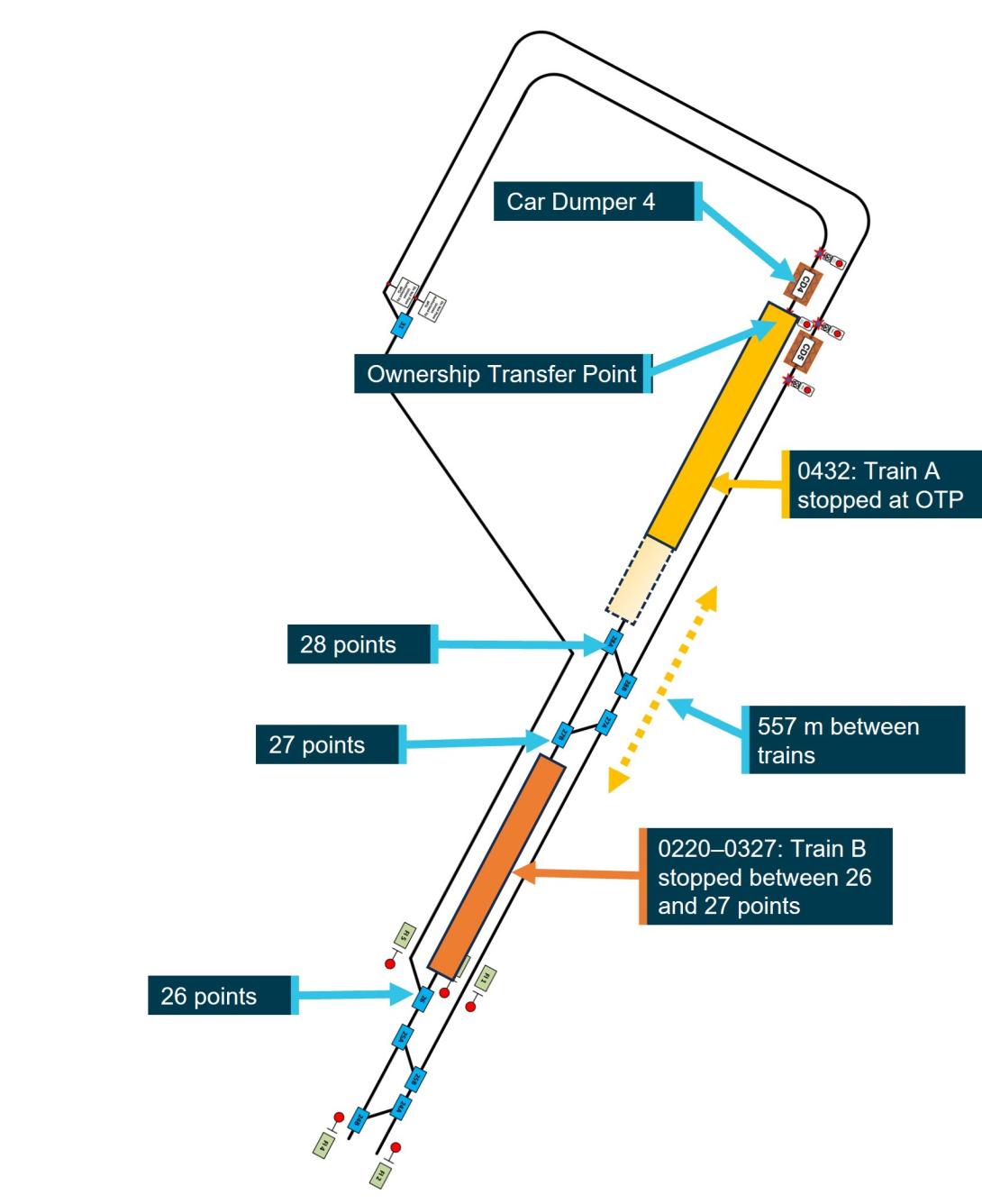
Not to scale
Source: BHP, annotated by the ATSB
After detecting that train A had moved ahead, the driver of train B applied power to move their train forward, intending to stop at least 200 m behind train A. At 0431:27, the driver placed the throttle to 1 notch, then 10 seconds later to 2 notch, and another 31 seconds later to 3 notch. At 0433:28, the driver responded to an audible alert from the vigilance system, the train started to move, and the driver placed the throttle into 4 notch.
Over the next 4 minutes, as the trained slowly accelerated to 12 km/h, the driver made 3 more responses to audible alerts from the vigilance system, the last of which occurred at 0437:28. At 0437:42, nearly one hour before first light,[3] train B impacted the rear of train A. The impact sequence lasted 38 seconds and, although the locomotive brakes were fully applied on train A from the point of contact, train A was pushed forwards about 40 m.
The driver of train B reported remembering moving the throttle to 1 notch, but had no awareness of hearing or responding to audible vigilance alerts in the lead up to the collision, and thought they must have had a microsleep. The driver reported being awoken by the impact, and immediately communicated with drivers on nearby trains and controllers to coordinate movements, maintain safe operations, and initiate post-incident protocols.
The driver also uncoupled the lead locomotive of train B from the rear of train A and checked for any damage. There was no damage to rollingstock (Figure 4) and the driver was uninjured.
Figure 4: Lead locomotive of train M05519B after the accident

Source: BHP
Context
Train driver information
Experience, qualifications, and training
The driver had over 30 years of experience driving trains and had worked in Western Australia for over a decade on a fly-in, fly-out (FIFO) basis, operating grain, container, and heavy bulk mineral trains. The driver joined BHP in 2022 and completed all relevant safeworking, locomotive, and in‑field training courses. The driver also held the required route knowledge and operational competencies for the tasks undertaken. The driver regularly operated trains around Finucane Island and last did so 3 days prior to the incident.
The driver successfully completed BHP’s fatigue management training course in 2022 as part of the induction process, but had not completed a refresher course that had been due since December 2023, due to an absence from work.
Medical information
The driver passed an annual category 1 rail medical assessment on 4 October 2023. The driver’s responses to the sleep-related questions in the medical assessment indicated no sleep issues, no tendency to doze, and the driver reported normally sleeping for 6 hours when on day or night shifts and at home.
On 29 November 2023, the driver presented to a medical centre at Port Hedland with a bite on their leg, which they had received while sleeping at night in the barracks.[4] The driver was given temporary pain relief and flew home to Sydney, New South Wales, where they subsequently underwent surgery for what was identified as a white‑tailed spider bite. The driver was subsequently cleared by their general practitioner to resume normal work duties from 16 January 2024 and, that day, flew from Sydney to Port Hedland.
Just over one week after returning to work, on the morning of 25 January 2024, the driver awoke at 0600 and noticed similar signs of a white-tailed spider bite, this time on their neck. On 29 January, the driver returned to Sydney, where they underwent surgery for the second white‑tailed spider bite, followed by a period of rehabilitation. The general practitioner then deemed the driver fit to return to duties, with no requirement for ongoing treatment or medication, and the driver returned to work on 27 February 2024.
Upon returning to Port Hedland, the driver began to experience panic attacks and stress, possibly associated with a response to the previous spider bites. The driver had been allocated the same room at barracks after returning to duty in January and February. BHP provided the ATSB with receipts confirming that the driver’s room and 3 adjacent rooms were fumigated on 1 February 2024. However, when the driver returned to their room 26 days later, they reported there were no obvious signs it had been fumigated as it did not appear to have been cleaned. As a result, the driver began frequently spraying their room and locomotive cab with insect spray. The driver reported that their sleep quality was affected as they woke often, including to spray the room, fearing they would be bitten again, and slept with the lights on to deter spiders.
Following the collision, BHP conducted standard post-incident drug and alcohol testing on the driver, with negative results for both drugs and alcohol, and no substance-related impairment was identified.
Rostering and recent history
Roster and fly-in fly-out arrangements
The driver’s FIFO roster involved 7 12-hour night shifts, followed by a minimum 24-hour changeover period, then 7 12-hour day shifts, followed by 7 days off duty. Drivers were expected to fly in on the day of their first shift (or the day prior, if their start time was at or after midnight), with an opportunity to rest for several hours at barracks prior to commencing their first shift later that night. At the end of each rotation, drivers would fly home on the first morning after their final day shift. The driver travelled from their home in Sydney to Port Hedland via Perth on scheduled airline flights.
Accommodation at Port Hedland
The accommodation barracks were located next to Port Hedland International Airport. The barracks were fully serviced with a dining area and recreational facilities, and all personnel were allocated a single occupancy room with an en suite and air-conditioning. The driver reported that, as a 24-hour facility, the barracks could be moderately noisy at times with the movement of cleaners and their equipment during the day, and the activities of other workers between shifts.
Adjusting to shift work and variable sleep patterns
The driver was experienced in shift work and reported that they adjusted well to variable sleep and roster patterns. The driver reported maintaining similar sleep habits at barracks in Port Hedland and at home. The driver also reported commonly having broken sleep, but no problems returning to sleep.
The driver reported that they would usually be in bed no later than 2 hours after the end of each shift, and aimed to wake at least 2–3 hours prior to commencing their next shift. The driver also reported that they could sleep for several hours on the flights to Port Hedland prior to commencing the first shift of a new rotation.
Fatigue mitigation strategies
BHP Western Australia Iron Ore had strategies aimed at mitigating fatigue risks associated with the FIFO roster. These included a fatigue assessment, which was required to be conducted at specific times in the roster and under certain other conditions. Individuals could also voluntarily complete the assessment at other times. If a driver reported being fatigued, they could be assigned rest or non-operational duties. Drivers could also request a fatigue break during a shift.
The ATSB assessed whether a safety issue relating to BHP’s rostering practices, which was identified during investigation RO‑2018‑018, was relevant to this occurrence. However, contrary to the circumstances associated with RO‑2018‑018, the driver had been off work for one month and during this first rotation back had 11–12 hours of sleep opportunity each day, during which they reported obtaining their normal sleep duration.
Recent history
The driver reported having had a good sleep at home in Sydney, before waking on the morning of 27 February 2024. The driver then obtained another 4–5 hours of sleep on the flights to Port Hedland with their first 12-hour night shift rostered to commence that night at 2200. The driver reported that, prior to arriving at Port Hedland, they had completed a fatigue assessment form, which based on their responses, indicated a low fatigue score.[5] The collision occurred on the fourth night of this rotation, after which the driver was relieved from duty and placed on leave. The driver reported that they generally felt most fatigued towards the end of the fourth shift of a rotation.
The driver reported that in the 72 hours prior to the collision, they followed their normal sleep pattern. They went to bed about 1130–1200, obtained about 6–7 hours of broken sleep, with a maximum continuous sleep period of about 4 hours. The driver rated the quality of their sleep in the days prior to the collision as being 1 out 10 (where 0 indicates the worst possible sleep and 10 indicates the best possible sleep), due to numerous sleep interruptions.
Despite that, the driver reported that before the incident shift, they felt well rested and did not consider completing a fatigue assessment. The driver assessed their perceived level of alertness at the time of the collision as ‘ok, somewhat fresh’, and reported feeling wide awake with no symptoms of tiredness.
Food and drink consumption
The driver maintained regular eating patterns, eating conventional breakfast foods in the morning and more traditional or substantial dinner-style meals in the evening. The driver was not taking medication, natural sleep aids or vitamin supplements, and they rarely consumed alcohol and did not drink caffeinated energy drinks.
After returning from the previous night shift mid-morning, on 1 March 2024, the driver consumed a light meal before going to bed, and, after waking, ate a full meal at around 1900. The driver made a coffee at the office when signing-on at 2100, which was the only caffeinated beverage they consumed prior to the collision.
Locomotive vigilance system
Locomotive vigilance systems monitor driver activity and responsiveness and apply the train’s brakes if the driver does not respond to vigilance alerts in a specified period. The vigilance alerts consist of an initial visual alert followed soon after by the addition of an audible alert. The system will initiate a penalty brake application, causing the train to stop, if no acknowledgement is made.
A limitation of such systems, as identified in an ATSB investigation into a collision between 2 freight trains in 2019 (RO-2019-022), was that drivers could acknowledge vigilance systems during periods of acute fatigue, and habituate to these systems, responding to alerts without conscious thought by pressing the reset button through a reflexive motor response. Vigilance systems could identify and intervene in cases of driver absence or total incapacitation but were less effective in detecting and responding when drivers were mildly incapacitated, inattentive, fatigued, or otherwise distracted.
The vigilance system installed on SD70Ace/LCi locomotives operated as a task/activity-based system with a fixed-time element. If the system detected inactivity in relation to control inputs or locomotive settings, the timer would commence a countdown with a visual alert displayed on the Functionally Integrated Railroad Electronics (FIRE)[6] system display screen and a warning light on the vigilance push‑button.
If the driver did not respond within a specified time, an audible tone would sound. The timer would automatically reset if the driver made control inputs such as throttle, brake, or directional controller settings, or operated items such as the locomotive horn or sanding[7] equipment. It would also reset if the driver pressed the vigilance acknowledgement push‑button or the reset button on the FIRE display screen.
The vigilance timer operated on a 90-second cycle with the following sequence:
- 0 seconds – system reset, commence silent countdown
- 70 seconds – flashing countdown and warning lights on the driver’s display, warning light illuminated on the FIRE alert reset button and vigilance pushbutton
- 75 seconds – commencement of audible tone increasing in volume and frequency to accompany visual alerts
- 85 seconds – rising audible tone reaches peak volume and continues to sound along with the visual alerts until the vigilance is reset or the timing cycle ends
- 90 seconds – full emergency brake application.
The alerts would not be generated while the train was idle or the independent brake[8] was applied, and only became active when at least one of the following conditions were met:
- locomotive speed was greater than 0.8 km/h (task-linked to the throttle)
- brake cylinder pressure was lower than 25 psi (task-linked to the independent brake).
- driver’s console (right side of the cab, on the right of the desk)
- driver’s control panel (left of the driver’s seat above the dynamic brake handle)
- observer’s console (left side of the cab)
- rear of locomotive cab.
The first 2 of these listed alerter reset buttons, together with the FIRE display screen, are shown in Figure 5.
Figure 5: Alerter reset button on control panel and driver’s console
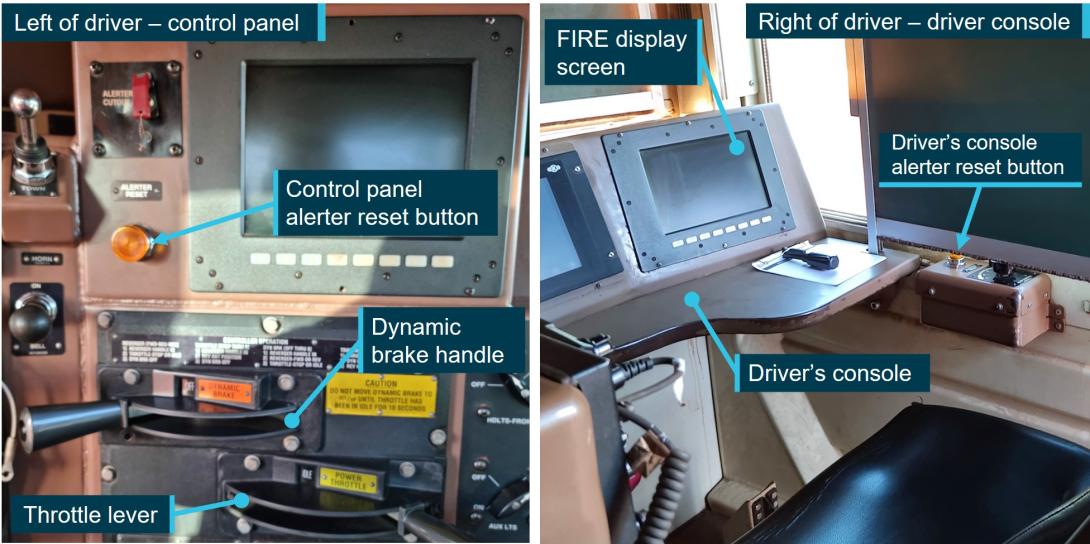
Source: BHP, annotated by the ATSB
Recorded information
The FIRE system also recorded data on a logger when an event occurred, or at an interval when no other triggers had caused an event recording. The events that triggered a recording included changes in analogue parameter values, and changes of discrete inputs, such as the movement of throttle or brake controls, activation of the horn, changes to light settings, and the acknowledgement of the vigilance system. There was no way to determine which specific button the driver pressed in the locomotive to reset the vigilance system, as the buttons were all in parallel through a single digital input/output channel in the locomotive.
Data from one locomotive per train – locomotives 4328 (train A) and 4480 (train B) – showed that both trains were operated below the track speed limits with both trains functioning within normal parameters and responding appropriately to driver inputs. The system recorded speed in whole km/h, and the following tables outline key events recorded on train B across 3 time periods.
Table 1 shows the sequence of events on train B between 0327 and 0332, when the driver applied power for over 2 minutes before releasing the independent brake. The driver responded to either the flashing reset button or the visual alert on the FIRE screen to acknowledge the vigilance system as train B moved forwards 27 m.
Table 1: Sequence of events recorded on train B (0327 to 0332)
| Time | Action by driver | Effect | Gap to train A (m) |
| 0327:44 | Throttle to 1 notch | Tractive effort increased | 260 |
| 0328:01 | Throttle to 2 notch | Tractive effort increased | 260 |
| 0328:12 | Throttle to 3 notch | Tractive effort increased | 260 |
| 0329:54 | Independent brake released | Train is able to move | 260 |
| 0330:00 |
Vigilance system activated (brake psi threshold met) |
Safety system in operation | 260 |
| 0330:18 | Throttle, brake settings maintained | Train starts to move | 259 |
| 0331:14 | Vigilance system acknowledged | Timer at 74 seconds: Visual alert | 244 |
| 0331:24 | Throttle to 2 notch | (Speed remains at 1 km/h) | 240 |
| 0331:33 | Throttle to 1 notch | Tractive effort reduced | 236 |
| 0331:39 | Independent brake applied | Train begins to slow | 235 |
| 0331:43 | Throttle to idle | Train comes to a stand | 233 |
Table 2 shows the driver released the independent brake at 0334. The driver then applied power, and responded to the audible alert tone when resetting the vigilance system on 4 occasions, during which time the train moved forward 1 m. At 0340, the driver reapplied the independent brake, deactivating the vigilance system but with power applied to the traction motors for the next 20 minutes. Due to the brakes, uphill grade, and tonnage, this setting was insufficient to move the train fast enough to reactivate the vigilance system. At 0400, the driver moved the throttle to idle.
Table 2: Sequence of events recorded on train B (0334 to 0400)
| Time | Action by driver | Effect | Gap to train A (m) |
| 0334:07 | Independent brake released | Reduction in brake pressure | 233 |
| 0334:08 | Throttle to 1 notch | Tractive effort increased | 233 |
| 0334:14 |
Vigilance system activated (brake psi threshold met) |
Safety system in operation | 233 |
| 0334:15 | Throttle to 2 notch | Tractive effort increased | 233 |
| 0335:32 | Vigilance system acknowledged | Timer at 78 seconds: visual alert and audible tone increasing in volume and frequency | 233 |
| 0335:50 | Throttle to 1 notch | Vigilance timer reset to zero | 233 |
| 0337:08 | Vigilance system acknowledged | Timer at 78 seconds: visual alert and audible tone increasing in volume and frequency | 232 |
| 0338:29 | Vigilance system acknowledged | Timer at 81 seconds: visual alert and audible tone increasing in volume and frequency | 232 |
| 0339:48 | Vigilance system acknowledged | Timer at 79 seconds: visual alert and audible tone increasing in volume and frequency | 232 |
| 0340:27 | Independent brake applied | Vigilance system deactivated | 232 |
| 0400:18 | Throttle to idle from 1 notch | Tractive effort stops | 232 |
Between 0400 and 0431, train B remained at a stand with idle throttle and brakes applied, before the driver made a series of control inputs as outlined in Table 3Table 4. The throttle was moved to 4 notch, which applied half the available power to the traction motors and the driver responded to the audible alert tone when resetting the vigilance system on 4 occasions.
Table 3: Sequence of events recorded on train B (0431 to 0438)
| Time | Action by driver | Effect on train | Gap to train A (m) |
| 0431:27 | Throttle to 1 notch | Tractive effort increased | 557 |
| 0431:34 | Independent brake released | Vigilance system activated | 557 |
| 0431:37 | Throttle to 2 notch | Tractive effort increased | 557 |
| 0432:08 | Throttle to 3 notch | Tractive effort increased | 557 |
| 0433:28 | Vigilance system acknowledged | Timer at 80 seconds: visual alert and audible tone increasing in volume and frequency | 543 |
| 0433:31 | Throttle to 4 notch | Train begins to accelerate | 542 |
| 0434:49 | Vigilance system acknowledged | Timer at 78 seconds: visual alert and audible tone increasing in volume and frequency | 472 |
| 0436:08 | Vigilance system acknowledged | Timer at 79 seconds: visual alert and audible tone increasing in volume and frequency | 304 |
| 0437:28 | Vigilance system acknowledged | Timer at 80 seconds: visual alert and audible tone increasing in volume and frequency | 47 |
| 0437:42 | Impact with Train 5519A at 12 km/h | Loss of data recording | 0 |
Human factors considerations
Workload
The driver described their workload on the night prior to the incident night as being ‘flat out’ with numerous locomotive and rolling stock movements. On the incident night, the driver’s workload was low, the train having been stationary first at Mooka, then stopped by train control for one hour, and again while waiting at Finucane Island. Low workload situations lack stimulation, leading to monotony and boredom, and this can reveal underlying sleepiness from inadequate sleep, and degrade performance (Williamson et al 2011). Limited stimulation of a task can also reduce attention (Young and Stanton 2002).
Sleep cycle
It is generally agreed that most adults need at least 7 hours of sleep each day to achieve maximum levels of alertness and performance (Hirshkowitz and others 2015). Getting enough sleep quantity is critical in mitigating fatigue. However, sleep quality is also important. Good quality, restorative sleep depends on obtaining sufficient deep and rapid eye movement (REM) sleep, which only occur after being asleep for some time (Carskadon and Dement 2017).
The sleep cycle comprises 4 stages – drowsiness, light sleep, deep sleep, and REM sleep. During sleep, adults normally cycle through these stages, with the duration of each stage and the proportions changing with age. Each stage is important, and waking frequently reduces the ability to obtain deep sleep and REM sleep, because after waking, the cycle begins again.
Sleep quality broadly refers to the capacity of sleep to restore waking function. Ohayon et al (2017) reviewed sleep-related research and identified characteristics consistent with poor sleep quality. These include 4 or more awakenings per night (for more than 5 minutes) or being awake for more than 40 minutes after falling asleep. While there is less research on the effect of sleep quality than of sleep duration on performance, it has been found that sleep fragmentation has been shown to degrade memory, reaction time, vigilance, and mood (Bonnet & Arand 2003).
Sleep-wake cycle
In addition to the sleep cycle, there is the daily sleep-wake cycle. The sleep-wake cycle, known as the circadian rhythm, is usually comprised of a single period of wake and a major sleep episode every 24 hours. This alternation of sleep and wake normally coincides with the daily light-dark cycle, such that sleep occurs at night and wake occurs during the day (Kosmadopolos 2023). The sleep-wake cycle is regulated by the circadian clock and sleep homeostasis – the longer a person is awake, the stronger the drive for sleep. A reduction in sleep quantity or quality, or extension of the time awake since sleep, produces a sleep debt and increases the drive to sleep (Williamson et al 2011).
Effects of light
Light affects both the sleep cycle and the sleep-wake cycle. The greatest influence on circadian rhythm is sunlight or blue light. Exposure to light promotes wakefulness and hinders sleep (Chellappa et al 2011). Light exposure before or during sleep times can reduce sleep quality, cause repeated awakenings and interrupt the sleep cycle.
Effects of stress
Psychological stress and worry are known to reduce the recuperative value of sleep and increase mental demands in waking hours (Kim & Dimsdale 2007). Being stressed or anxious affects multiple systems in the body and increases activation of the sympathetic nervous system and cortisol levels (Stanford et al 2015). This causes alertness, or hyperarousal, and can lead to sleep fragmentation and reduced deep sleep (Han, Kim & Shim 2012). The effects of stress and anxiety can result in a high state of alertness despite disrupted sleep, where a person feels ‘tired but wired’ (Ramlakhan 2010).
Stress responsible for prolonged sleep disruption in humans may be a cognitive and emotional phenomenon that is not necessarily always associated with an acute challenge. Humans may experience stress based on memories of past events as well as worries and expectations about the future. They can take a single acute stressor or life event that occurred in the past, or even one pending in the future, into a persistent and chronic stress state. Research has found that stress and worry experienced over successive days, particularly at bedtime, was shown to negatively affect sleep quality (Akerstedt et al 2012). In addition, poor sleep can result in people performing an action without any awareness or memory of having done so (Leschziner 2020).
Microsleeps
As sleep is a biological need, when it reaches a critical level, the brain will sleep regardless of any effort to remain awake. This may result in microsleeps, which are described as brief fragments of sleep shorter than 15 seconds (Malafeev et al 2021). They can occur due to sleep loss, where the propensity for sleep is increased (Durmer and Dingers 2005), or during periods of low workload. One consequence of a microsleep is when a person does not respond during cognitive performance demands (Kause et al 2017). Microsleeps can occur without conscious awareness and can occur in settings where automation is provided, such as through automatic train protection systems (Thomas et al 2023).
Safety analysis
Following multiple surgeries and medical leave because of 2 white-tailed spider bites, which occurred while the train driver was asleep in their accommodation at Port Hedland, the train driver returned to work at Port Hedland and commenced a week of night shifts. Experiences of acute stressors, such as spider bites, can result in persistent stress based on memories and associations of the past event and worries that a bite may occur in the future. Fearing another bite, the driver was frequently spraying insecticide in the locomotive and their bedroom, including waking from sleep to do so. In addition to impacting sleep, stress stimulates the sympathetic nervous system. This likely led to the driver feeling awake and alert, rather than experiencing symptoms of tiredness that would normally arise from a deficiency of deep restorative sleep.
In the 11–12 hours of sleep opportunity on each of the first 3 daytime off-duty periods, the driver reported having obtained the same total duration of sleep as normal. However, the disruption detail above inhibited their ability to obtain deep restorative sleep, reducing overall sleep quality. This was exacerbated by the driver sleeping with the light on (to deter spiders), which delays sleep onset and fragments sleep, reducing the amount of deep sleep. As the circadian rhythm is dependent on bright light for regulation, sleeping with the light on also likely affected the driver’s ability to adapt to sleeping during the day and being wakeful while on duty at night.
Between 0335 and 0340 on the incident morning, while applying some tractive effort with the brakes released, the driver acknowledged 4 audible alerts with no memory of having heard or acknowledged them. The driver then set the independent brake, deactivating the vigilance system, and both throttle and brakes were then engaged for about 20 minutes. This configuration was unlikely to have been conscious, given that the simultaneous application of power and brakes was not a normal operating mode and would almost certainly have resulted in the train moving either forwards or backwards but for the incline on which the train was stopped.
The unusual configuration was resolved at 0400 by the driver moving the throttle to idle, following which the train was stationary with no driver inputs for 31 minutes. That period was consistent with the driver’s recollection of standing outside on the footplate and cleaning the cab in preparation for the handover that would occur when the locomotive eventually reached the car dumper.
When the driver recognised that the train ahead had progressed, they set their train in motion. However, the driver had no recollection of subsequently hearing and acknowledging another 4 vigilance alerts. Vigilance systems are ineffective in detecting drivers who are mildly incapacitated, inattentive, fatigued, or otherwise distracted, and who can perform an automated task in acknowledging the alerts without conscious awareness.
Although the driver did not respond to visual alerts within the time required, and the vigilance system progressed to issuing audible alerts, the vigilance timer reset each time the driver acknowledged a vigilance alert, and consequently, the vigilance system did not activate the emergency brake. There was also no driver action to reduce the throttle or apply independent braking, or any other recorded control or system inputs by the driver. The pattern of slowed reaction times to the vigilance system alerts throughout the shift may indicate the driver was pre‑occupied or distracted. However, there was no evidence of any distraction.
As a result of poor-quality sleep, low workload, and dark conditions, after the driver set the train in motion it is probable that the driver was in a degraded level of alertness, possibly associated with a microsleep. During this period, the driver was unable to detect the risk posed by the stationary train ahead and identify the appropriate actions to be taken to stop the train.
As a result, about 5 minutes after the train started to move, and 14 seconds after the driver last acknowledged a vigilance alert, the locomotive impacted the rear of the stationary train ahead. The driver reported having no recollection of anything after setting the train in motion until the collision.
After the impact the driver was immediately able to perform normal and post-incident functions. This was consistent with being aroused from a degraded state rather than having suffered a medical incapacitation, and there was no evidence of any condition likely to result in incapacitation in the driver’s medical history or subsequent evaluation.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the low-speed collision between trains M05519A and M05519B at Finucane Island Balloon Loop, Port Hedland, Western Australia on 2 March 2024.
Contributing factors
- The driver of train M05519B had been experiencing stress, sleeping with the light on, and waking often, resulting in poor quality sleep. As a result, on their fourth consecutive night shift, during darkness and while experiencing low workload, the driver set the train in motion while in a degraded level of alertness, possibly associated with a microsleep, and did not detect the impending collision.
- Without awareness or memory of having done so, the driver acknowledged 4 audible vigilance alerts, which, by design, prevented a penalty brake activation. This resulted in a low-speed collision with stationary train M05519A.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Safety action by BHP
Following the collision, BHP undertook a series of actions to manage fatigue and the limitations of the vigilance systems in the SD70Ace/LCi locomotives.
BHP reviewed the fatigue risk periods for its FIFO rail operations driver rosters and increased the number of fatigue assessments during each rotation. Fatigue assessments are now conducted on each of the first 5 night shifts and on the first and fourth day shifts of each rotation. These assessments are conducted face-to-face with the on-shift supervisor or coordinator at each depot location.
BHP is also implementing an additional check-in per shift, to be conducted with the rail crew team member either face-to-face or electronically via phone or radio. To support this activity, BHP employed additional resources to support existing operations supervisors and superintendents to identify and monitor fatigue concerns within the rostering environment.
Additionally, research was conducted into the viability of an interactive fatigue assessment tool (FAT), delivered through a mobile application, to improve the quality of fatigue assessments. A trial of the FAT was scheduled to commence at the end of November 2024.
BHP also proposed several changes to the vigilance system installed on its SD70Ace/LCi locomotives, including changing from fixed-time intervals to random intervals for the countdown, and limiting consecutive alerter resets to require different inputs and eliminate ‘muscle memory’.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the driver of train M05519B
- BHP.
References
Åkerstedt T., Orsini N., Petersen H., Axelsson J., Lekander M., and Kecklund G. (2012). ‘Predicting sleep quality from stress and prior sleep–a study of day-to-day covariation across six weeks’, Sleep Medicine, 13(6):674–679. doi: 10.1016/j.sleep.2011.12.013.
Bonnet M.H. and Arand D.L. (2003). ‘Clinical effects of sleep fragmentation versus sleep deprivation’, Sleep Medicine Reviews, 7(4): 297-310, doi: 10.1053/smrv.2001.0245.
Carskadon M.A. and Dement W.C. (2017). ‘Normal human sleep: and overview’, in Kryger, M.H., Roth T. and W.C. (eds). Principles and practice of sleep medicine (6th edition), Elsevier.
Chellappa S.L., Gordijn M.C. and Cajochen C. (2011). ‘Can light make us bright? Effects of light on cognition and sleep’. Progress in Brain Research, 190:119 –133, doi: 10.1016/B978-0-444-53817-8.00007-4.
Durmer J.S. and Dinges D.F. (2005). ‘Neurocognitive consequences of sleep deprivation’. Seminars in Neurology, 25(1):117-129, doi: 10.1038/nrn.2017.55.
Han, K.S., Kim, L., Shim, I. (2012). ‘Stress and sleep disorder’, Experimental Neurobiology, 21(4):141-50. doi: 10.5607/en.2012.21.4.141. Accessed 5 September 2024: Stress and Sleep Disorder - PMC (nih.gov)
Hirshkowitz M., Whiton K., Albert S.M., Alessi C., Bruni O., DonCarlos L., Hazen N., Herman J., Katz E.S., Kheirandish-Gozal L., Neubauer D.N., O’Donnell, A.E., Ohayon, M., Peever, J., Rawding, R., Sachdeva, R.C., Setters B., Vitiello, M.V., Ware, J.C., and Adams-Hillard, P.J. (2015). ‘National Sleep Foundation’s sleep time duration recommendations: methodology and results summary’, Sleep Health, 1(1):40–43. doi: 10.1016/j.sleh.2014.12.010.
Krause A.J., Simon E.B., Mander, B.A., Greer S.M., Saletin J.M., Goldstein-Piekarski A.N. and Walker M.P. (2017). ‘The sleep-deprived human brain’, Nature Reviews Neuroscience, 18(7):404-418. doi:
Kim, E. J. and Dimsdale, J. E. (2007). ‘The effect of psychosocial stress on sleep: a review of polysomnographic evidence’, Behavioural Sleep Medicine, 5(4), 256-278.
Kosmadopolos A. (2023). ‘Sleep pressure and circadian rhythms’, in Rudin-Brown C. and Filtness, A.J., The handbook of fatigue management in transportation: waking up to the challenge, CRC Press, Boca Raton, Florida.
Leschziner, G. (2020). The nocturnal brain: nightmares, neuroscience, and the secret world of sleep. First St. Martin's Griffin edition. New York, NY, St. Martin's Griffin.
Malafeev A., Hertig-Godeschalk A., Schreier D.R., Skorucak J., Mathis J. and Achermann P. (2021). ‘Automatic detection of microsleep episodes with deep learning’, Frontiers in Neuroscience, 15:1-12. doi: 10.3389/fnins.2021.564098.
Ohayon M., Wickwire E.M., Hirshkowitz M., Albert S.M., Avidan A., Daly F.J., Dauvilliers Y., Ferri R., Fung C., Gozal D., Hazen N. (2017). ‘National Sleep Foundation's sleep quality recommendations: first report’, Sleep Health 3(1):6–19. doi:10.1016/j.sleh.2016.11.006.
Ramlakhan, N. (2010). Tired but wired: how to overcome sleep problems – the essential sleep toolkit. Souvenir Press; Main edition (3 May 2010). London, United Kingdom.
Sanford L.D., Suchecki D. and Meerlo P. (2015). ‘Stress, arousal, and sleep’. Sleep, Neuronal Plasticity and Brain Function, 25:379-410. doi:10.1007/7854_2014_314.
Thomas M.J.W., Sprajcer M. and Dawson D. (2023). ‘The effects of fatigue on performance in transportation operations’, in Rudin-Brown C. and Filtness, A.J., The handbook of fatigue management in transportation: waking up to the challenge, CRC Press, Boca Raton, FL.
Williamson A., Lombardi D.A., Folkard S., Stutts J., Courtney T.K. and Connor J.L. (2011). ‘The link between fatigue and safety’, Accident Analysis and Prevention, 43(2): 498–515. doi:10.1016/j.aap.2009.11.011.
Young M.S. and Stanton N.A. (2002). ‘Malleable attentional resources theory: a new explanation for the effects of mental underload on performance’, Human Factors, 44(3):365–375. doi:10.1518/0018720024497709.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the driver of train M05519B
- BHP
- the Office of the National Rail Safety Regulator.
Submissions were received from:
- BHP
- the Office of the National Rail Safety Regulator.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Yard Limits: a defined area of track where rail traffic movements are authorised and managed by a nominated network control officer or other suitably qualified employee, and whose boundaries are marked by trackside signage and, where relevant, labelling on signal panel displays. Train movements in these areas can be co-ordinated through fixed signal routes, hand signals, or verbal/written authorities.
[2] Notch: refers to engine power/RPM settings. Drivers apply or remove gradations of power by moving the throttle handle to the desired notch, which then provides a fixed percentage of the maximum power available to the traction motors.
[3] First light: when the centre of the sun is at an angle of 6° below the horizon before sunrise. At this time, the horizon is clearly defined but the brightest stars are still visible under clear atmospheric conditions. On 2 March 2024, first light at Port Hedland occurred at 0541 local time.
[4] Barracks: a place provided to railway personnel for rest between shifts. Usually consists of serviced accommodation located en route or in remote areas where staff are required to start and/or end their allocated shifts away from their home depot.
[5] Fatigue assessment tools rely upon an individual’s subjective reporting of factors that may contribute to the experience of fatigue. A low score indicates a low risk of fatigue, and the higher the score, the greater the severity or risk of fatigue.
[6] Functionally Integrated Railroad Electronics (FIRE): connected to the train’s onboard computer control system, this system monitors and measures train parameters and is linked to the vigilance device. Train information, control settings, and fault indications are presented to the driver on a digital display screen located in the driver’s console as well as recorded on an event/data logger.
[7] Sanding: a process where sand is applied to the railhead in order to improve overall traction and prevent wheel slip. This enables increased adhesion between the wheels and the rails to facilitate the smooth acceleration and braking of rollingstock, particularly when traversing slippery rails, tight curves, or steep grades. Excessive sand can have the opposite effect by reducing traction in certain circumstances.
[8] Independent brake: The independent brake solely controls air brakes within the locomotive(s) and works independently of a train’s other braking control systems. These brakes are controlled via the driver’s independent brake control handle and apply when the locomotive brake cylinder pressure is increased and release when the pressure is decreased.