
Executive summary
What happened
Late evening 29 May 2021, a Leonardo Helicopters AW139, registered VH-TJK, operated by Toll Helicopters, was tasked as single-pilot helicopter emergency medical service (HEMS) flight ‘Rescue 208’. Onboard the helicopter were 2 aircrew and 2 medical crew.
During the later stages of the approach into an unimproved helicopter landing site, the aircraft’s tail rotor struck a small tree. The contact was not identified by the crew. Having assessed the landing site as unsuitable, the crew discontinued the approach and diverted to a landing site about 1 km away. After shutting down, the flight crew conducted a walkaround inspection of the helicopter and identified evidence of foliage contact on the vertical fin.
What the ATSB found
The ATSB found that while manoeuvring to land within a confined area, unintended yaw and drift of the helicopter was not identified by the crew and stopped prior to the tail rotor striking a tree.
What has been done as a result
The operator has completed the following proactive safety actions:
- amended their operational guidance on minimum clearances from terrain when operating in confined areas
- issued guidance on site selection during primary missions
- a final internal safety report was provided to the ATSB and proactively shared among the emergency helicopter network
- installed the A800 Trakkabeam high‑intensity searchlights onto the fleet of aircraft.
Safety message
This incident highlights the need for flight crew to have a heightened situational awareness when operating into a confined area and unfamiliar location in the vicinity of obstacles, as there is very little to no margin to recover from any unexpected event(s).
Crew coordination plays a vital role in HEMS operations and ensures improved situational awareness, reduced errors, and the fostering of effective teamwork. Effective coordination and communication (including of concerns) minimises the risk of misinterpretation, ensures accurate transmission of information, and reduces the likelihood of mistakes.
The investigation
The occurrence
On 29 May 2021, at about 2325 local time, a Leonardo Helicopters AW139, registered VH-TJK (callsign ‘Rescue 208’) and operated by Toll Helicopters, was tasked to conduct a helicopter emergency medical service (HEMS)[1] flight. The flight was planned under night visual flight rules (NVFR)[2] supplemented with the use of a night vision imaging system (NVIS).[3] The aircrew comprised a pilot and aircrew officer (ACO). The medical crew included a New South Wales health department (NSW Health) flight paramedic and an emergency specialist doctor.
The NSW Health aeromedical control tasked Rescue 208 to transit from Bankstown Airport to Shelly Beach (Figure 1) to assist with retrieval, stabilisation and transport of a patient to the Royal North Shore Hospital, NSW. After accepting the task, conducting pre-flight planning and briefing on the operation (including a planned winching retrieval), the pilot started the helicopter engines at about 2343.
Figure 1: Aircraft flight path
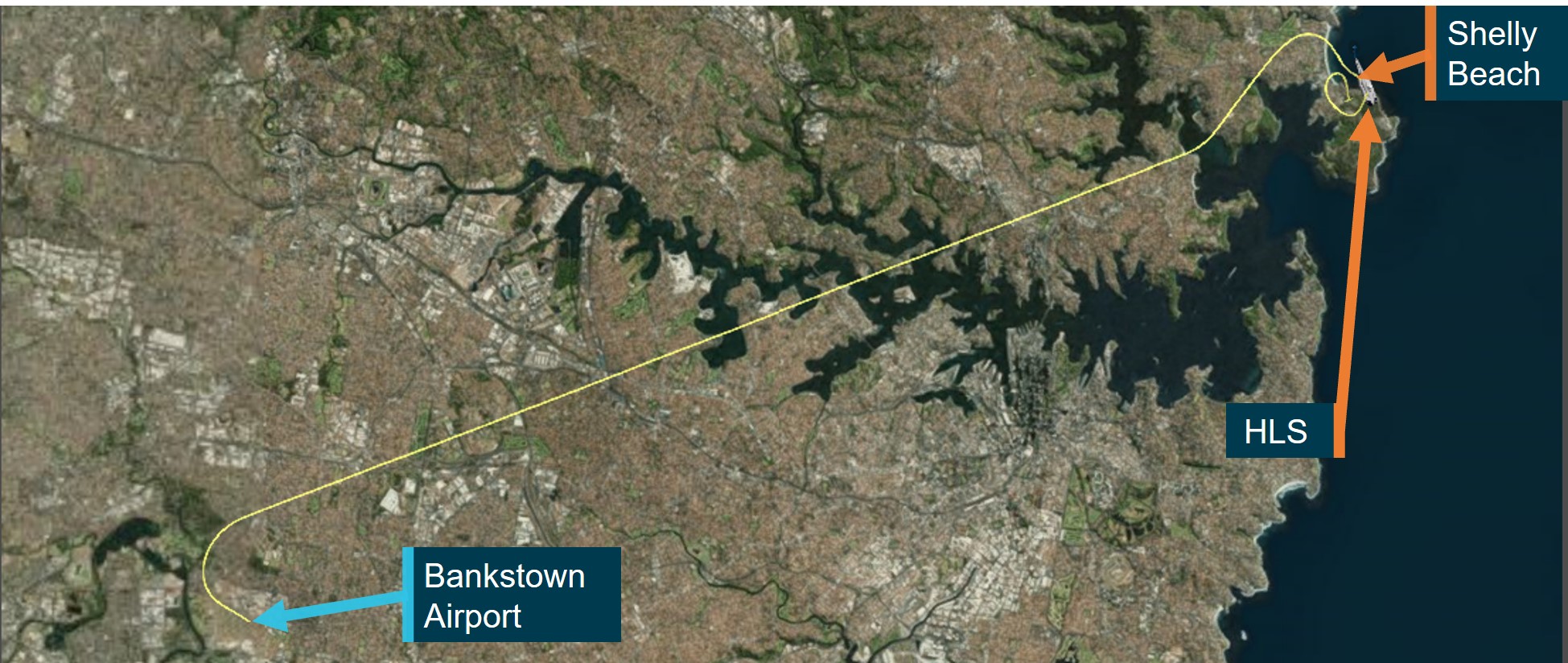
Source: Google Maps annotated by the ATSB
At about 2348, the aircrew and flight paramedic transitioned to using night vision goggles (NVG) and about a minute later, Rescue 208 departed Bankstown Airport, with the ACO in the rear cabin of the helicopter. While outbound at 1,500 ft, the paramedic was in contact the ground crew at the scene while the aircrew completed their checks. The aircrew had difficulties hearing the paramedic due to issues with the internal communication system.
The paramedic was informed by the scene commander on the ground at Shelly Beach that the plan had changed and was now for the crew to land in a playing field at Bear Cottage (Figure 2), instead of winching at the site. However, during that communication exchange, a second, closer landing option near the carpark at Shelly Beach was proposed, with the crew being advised that a HEMS helicopter had previously landed in the area (see the section titled Helicopter landing site).
Figure 2: Helicopter landing site options

Source: Google Earth annotated by the ATSB
Between 2352 and 2354, during the cruise, the doctor and flight paramedic discussed the equipment required for the rescue operation. A preparatory briefing was then conducted between the flight paramedic, the doctor and the ACO. At about 2355, the pilot acknowledged the briefing and subsequently briefed the crew on the weather, stating that there were light showers and the visibility was 5 km. Thirty seconds later, the pilot conducted the pre-landing checks, including lowering the landing gear, configuring and selecting the landing/search lighting system to ON (see the section titled Lighting and scan technique).
The aircraft arrived overhead Manly Beach at about 700 ft. The pilot then turned the helicopter south to parallel the beach and continued descent towards the proposed alternate landing area, while slowing the helicopter to an airspeed of 80 kt (Figure 3).
Figure 3: Aircraft flight path over Manly
Source: ATSB
At 2358, the pilot cleared the ACO to open the rear doors and continued descent while slowing to 60 kt. The ACO opened the right rear door and subsequently selected the winch power to ON, which also turned on the winch light. The pilot completed the pre-landing checks. The crew then received a radio call from the scene commander explaining the status of the patient, with a request that they land in the area near the Shelly Beach carpark if possible. The crew advised that they would assess that location and, if unable to land, they would reposition and land at Bear Cottage. About 30 seconds later, the helicopter was hovering at about 300 ft radio altitude (RA) adjacent to the proposed helicopter landing site (HLS).[4] From this position, the aircrew located the proposed landing area, primarily using the white search light rather than NVG.
At 0001, the pilot established the helicopter in a lower hover (between 100–130 ft RA) to assess the landing area. The ACO verbalised a description of the area, including the size, obstacles (advising that there were no power lines and that the trees were small), and available access. An approach plan was then discussed and the ACO then confirmed with the pilot and flight paramedic that they were happy to continue into the area. The pilot then handed over verbal control of the helicopter movement to the ACO, who then had responsibility for assisting the pilot by guiding them into the confined area HLS.[5]
The left rear cabin door was opened at about 0002 by the paramedic, who took up a position to ensure obstacle clearance to the left and rear of the helicopter. About 10 seconds later, the helicopter commenced an approach to the HLS on a heading of about 177°.
At 0003, as the helicopter descended, the ACO called ‘well clear of trees’ and guided the pilot through the movement of the tail through 20° right before stating ‘tail well clear’. The pilot then continued the descent, while undetected the helicopter yawed (see the section titled Helicopter movement) about 10° left to 145°. About 5 seconds later while at around 13 ft, the pilot asked the ACO about the slope of the site to which the ACO responded that it was ‘flat, or maybe a little bit nose to tail’. The flight paramedic responded to the comment of the slope stating it was ‘pretty heavy left’, this was not acknowledged by the other crew. During this conversation, the aircraft continued to gradually yaw further left.
Noticing the movement, the ACO told the pilot that they were drifting right and to move left. The ACO then advised that the tail was clear before again telling the pilot they were drifting to right. The ACO subsequently assessed that the helicopter was closer to the trees than they expected and called ‘climb climb climb’ and when the pilot did not respond, repeated the instruction. The pilot immediately responded to the second instruction and climbed the helicopter vertically to 100 ft (RA). Given the proximity of the trees, the ACO considered the possibility that the helicopter may have contacted them, however there had not been any indication of airframe contact (such as increased vibration).
Once out of the confined area, the pilot mentioned that they were happy to attempt another landing and the ACO agreed. The ACO did not mention the possibility the aircraft might have contacted the tree. However, the flight paramedic reiterated the increased slope on the left side of the aircraft and, after checking a second landing site in the car park, the crew diverted and landed at Bear Cottage.
After shutting down, the ACO and pilot conducted a walkaround inspection of the helicopter using hand-held torches. While inspecting the vertical fin, green material indicating contact with foliage was identified (Figure 4). The pilot then briefed the medical crew that the aircraft would be offline and notified the operator’s management of the incident.
Figure 4: Evidence of foliage contact on the vertical fin

Source: Toll Helicopters ACT/NSW
Context
Helicopter personnel
Pilot
The pilot had previously been employed by the operator for about 2 years from 2017–2019 and had recently returned to the role. They were cleared back to line flying on 29 April 2021. The pilot had a total of 4,594.8 flying hours, of which 1,219.7 were on the AW139. They had a total of 174.7 hours NVG flying time and since their return they had completed 16.1 NVG hours. An NVG/NVIS Capability Check Flight (CCF)[6] was completed 14 April 2021.
Aircrew officer
The ACO had 5,691 flying hours of which 2,001.1 were on the AW139. The ACO had 459 hours of NVG time at the time of the occurrence. They had completed an NVG/NVIS CCF on 19 May 2021.
Medical crew
The flight paramedic had previous experience in HEMS operations while working with another operator from mid-2015 to 2018. They started working with the operator in 2018 in road operations and in 2019 transitioned to flight paramedic. The flight paramedic was using NVG on the occurrence flight and had completed 3 hours of NVG flying within the last month.
The doctor had worked as an aeromedical doctor with another operator between August 2020 and February 2021 before joining the operator. At the time of the occurrence, they had about 10 months experience working in the HEMS operational environment. The majority of operations experienced during this time did not include night operations. The doctor was not using NVG on the occurrence flight.
Aircraft information
General
The Leonardo S.p.A AW139 is a medium-sized, multi-role helicopter, powered by two Pratt & Whitney Canada PT6C-67C turboshaft engines. The aircraft has a length of 16.66 m and a rotor diameter of 13.8 m. The AW139 aircraft is primarily used for emergency medical services (EMS) within Australia.
The tail rotor of the AW139 is a critical component of the aircraft’s flight control system, providing the necessary lateral force to counteract the torque generated by the main rotor system. Figure 5 outlines the aircraft dimensions and the area of foliage contact.
Figure 5: Area of impact with tree
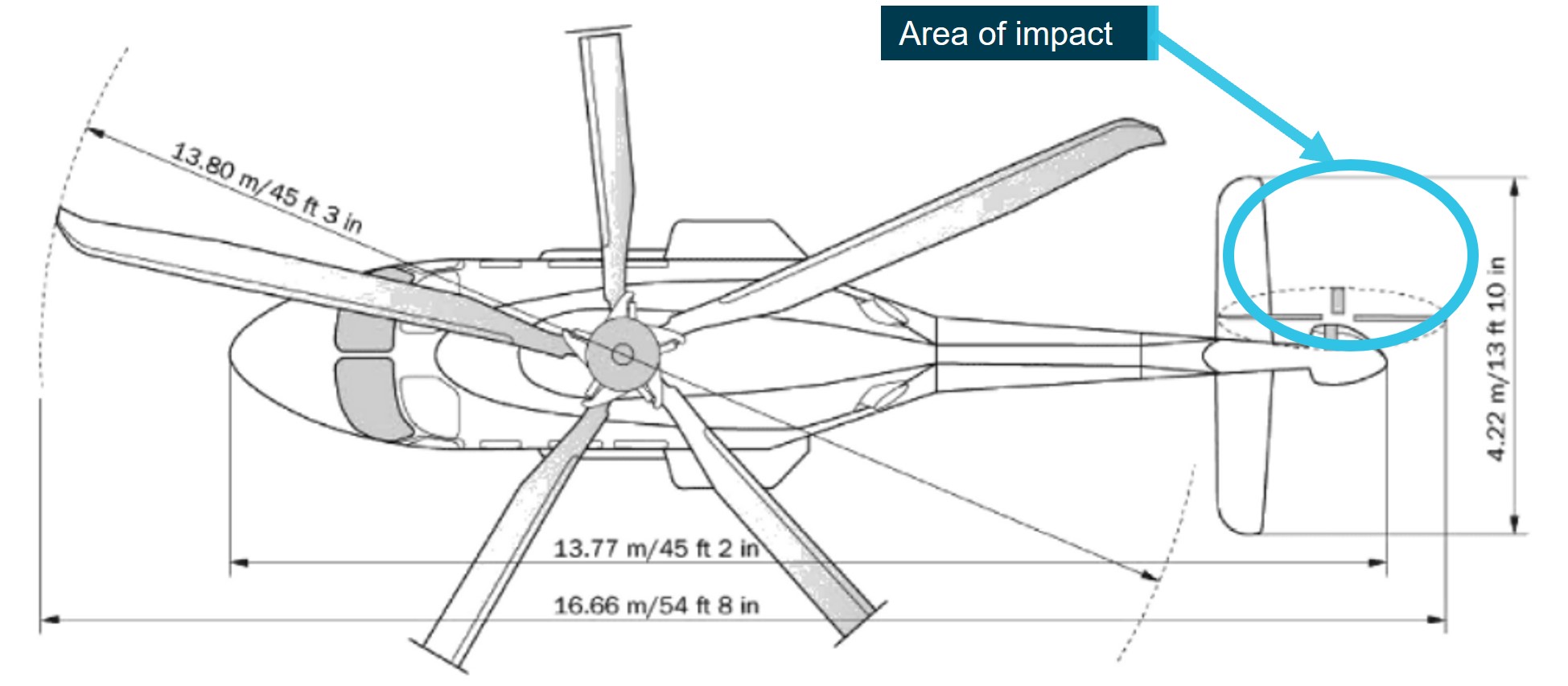
Source: Leonardo Helicopters (Augusta Westland 139), annotated by the ATSB
Helicopter movement
Two important aspects of helicopter movement, especially in the context of hover operations are yaw and drift. Yaw refers to the rotation of the helicopter around its vertical axis. This is controlled by input to the tail rotor, which generates a lateral force to counteract the torque produced by engine/s driving the main rotor. The amount of yaw is adjusted by the pilot using the anti‑torque (tail rotor) pedals, which control the pitch (and therefore thrust) of the tail rotor blades. Yaw is important for controlling the heading of the aircraft and for maintaining balance in forward flight.
Drift refers to the (usually) unintended lateral movement of the aircraft as a result of wind/turbulence, flight control inputs and lateral tail rotor thrust (particularly in hovering flight). Drift can occur without the aircraft yawing and vice versa.
The Federal Aviation administration (FAA) Helicopter Flying Handbook (2019) Chapter 2 - Aerodynamics of Flight emphasises the importance of understanding and controlling both yaw and drift.
Active Vibration Control System
VH-TJK was fitted with an active vibration control system (AVCS). The system worked by sensing vibrations of the aircraft rotor system and using advanced algorithms to automatically adjust the pitch of the main rotor blades to reduce the amplitude of the vibration. The system could adjust the pitch of the blades up to 20 time per second, allowing it to quickly respond to changes in vibration levels.
External lighting
The aircraft was fitted with two pilot-steerable landing (search) lights mounted on the underside of the helicopter. Additionally, the aircraft was fitted with an ACO-steerable hoist light and each crew member had handheld torches available.
At low level, the operator required crews to make use of the external lights (white light), to assist the detection of wires and other obstacles and maintain terrain separation. This required the crew to conduct their scan with both the use of NVG and without.
Visual scan technique
Pilot
The pilot advised that during the approach their NVG goggles were in position, however they were also looking underneath and around them to use the white light to scan, and then doing a general scan through their NVG. To ensure they had adequate reference points, the pilot had one light directed to the front of the helicopter, with the second directed in the 3 o’clock[7] position.
The pilot also reported using lit houses in front and to their right, as reference points. During the descent, they used a dead tree in front of the helicopter and another identifiable tree to their right. They then transitioned to using ground references visible through the helicopter’s clear chin bubble. The pilot identified that the ground was sloping and decided they would assess the magnitude of the slope when they got to a low hover. The pilot also stated that they thought the inadvertent yaw occurred during a reduction in power associated with lowering the collective. They assessed this most likely happened when they brought their gaze down to the ground and were not using the identified trees as references. They did not believe that the unintended yaw was due to inadequate illumination of the confined area.
Aircrew officer
The ACO advised they used both NVG and the winch light to identify visual cues when descending into the HLS. They reported keeping the closest obstacle, being the contacted trees, to their right so they could observe and avoid them. They estimated the helicopter was 15‑20 ft away from the trees during the initial descent. The ACO moved from the right to left inside the helicopter and also lay on the floor to check underneath for clearance from obstacles. While monitoring the ground clearance, the ACO looked up and identified that the tail of the helicopter was significantly closer to the trees than expected, assessing that they may have misinterpreted yaw as drift when lying on the floor.
The ACO stated that they did not observe an excessive ground slope and were surprised by the paramedic’s assessment. They also advised that they were not relying on the paramedic to give advice on the helicopter clearance from objects. Finally, the ACO advised they did not consider visibility of the HLS was an issue, assessing the conditions as a relatively high visibility night.
Paramedic
The paramedic advised they were positioned on the left side of the helicopter during the approach to the confined area and, while they had NVG, they had better vision using the white light and a handheld torch. They advised that the role of the paramedic was to give negative clearances when asked, and to identify and call out potential hazards in the area. On the night, the paramedic recalled having a large clearance on the left side of the tail and they could see the ground dropping off behind the tail in the white light. They recalled that due to the references outside the aircraft they thought the aircraft had drifted.
The paramedic assessed that the underbelly lighting of the aircraft was not ideal for landing into the HLS and that with more white light the crew might have been able to identify more of the terrain.
Briefings
The crew arrived at the base at approximately 1930, for an overnight shift. They completed a shift hand-over, checked the local weather conditions and conducted a pre-flight inspection of the helicopter. The crew then went to bed at about 2200.
At 2325, the paramedic received a phone call for a priority job and woke the pilot. The pilot conducted a pre-flight operational risk assessment considering the:
- weather that included moderate to strong winds, turbulence and showers
- time of night
- moon illumination
- possibility of a winch.
The pilot determined the risk was within the appropriate levels to conduct the operation and woke the doctor and ACO.
The ACO completed an online reconnaissance of the area, to assess possible landing locations. The pilot completed the aircraft’s weight and balance and performance calculations and confirmed they allowed for an out of ground effect hover and winch, without the need for internal configuration changes.
During the transit to the scene a brief was completed, which included the crew duties, available equipment, possible landing locations, and weather.
The operator’s operations manual outlined that when a crew was operating to an unknown HLS, NVIS crews were required to conduct a thorough reconnaissance of the landing area with a white light prior to committing to an approach. This could be done either while conducting an orbit over the area or during a high hover over the site.
The crew completed 2 hovers, a high hover at approximately 300 ft and a low hover at approximately 100 ft (Figure 6).
Figure 6: Hover heights prior to entry into HLS
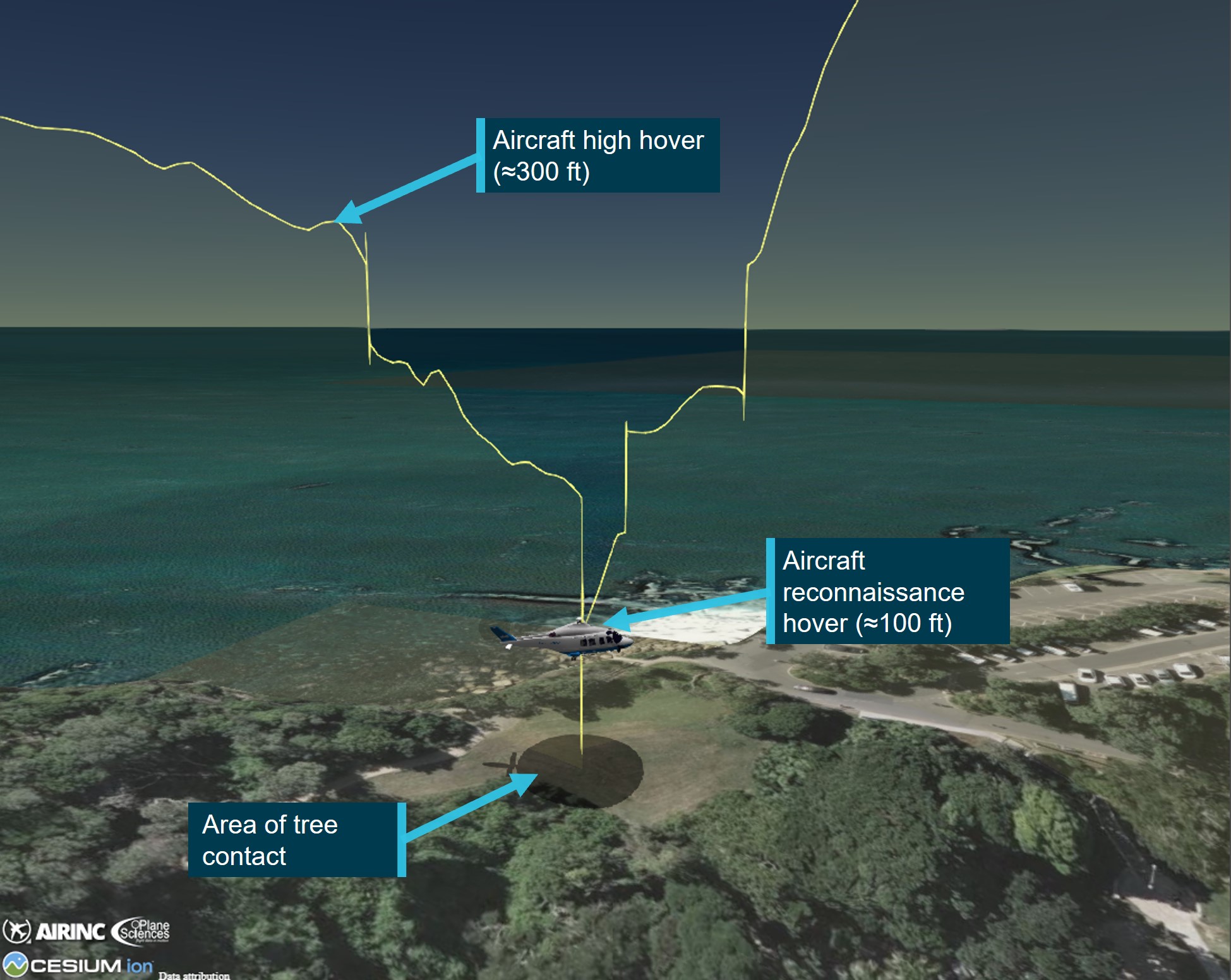
Source: ATSB
As a minimum, the reconnaissance and brief was required to assess the required power, wind, any obstacles and a plan for the approach and departure, typically based on the acronym PSWATP:
- P – Power available/required and therefore performance margin
- S – Size, shape, slope and surrounds
- W – Wind direction, strength and any turbulence
- A – Approach profile, departure and overshoot options
- T – Terrain, turbulence relevant to the area
- P – The plan, including crew duties, based on the reconnaissance
The pilot was to give a brief on the relevant information of the PSWATP briefing requirements and the ACO was expected to contribute to the reconnaissance.
Table 1 outlines the 6 sections of the PSWATP and at what point during the mission they were completed and by whom.
Table 1: Completion of Briefings
| Section of PSWATP | Prior to departure | During flight | During reconnaissance hover |
| Power available/required and therefore performance margin | Pilot – completed the aircraft’s weight and balance and performance calculations. They also analysed the hover out of ground effect and confirmed it was acceptable for the mission. | ||
| Size, shape, slope and surrounds |
ACO – discussed size, shape, and obstacles. Pilot and Paramedic – confirmed ACO observations. |
||
| Wind direction, strength and any turbulence | Pilot – conducted a pre-flight risk assessment based on the weather that included moderate to strong winds, turbulence and showers, time of night, moon illumination and a possible NVIS winch | Pilot – communicated information on wind and rain | Pilot – confirmed wind direction with crew |
| Approach profile, departure and overshoot options | Pilot and ACO – discussed initial approach into HLS | ||
| Terrain, turbulence relevant to the area | ACO – completed an online reconnaissance of the area, to assess possible landing locations | ACO – described the terrain to the crew | |
| The plan, including crew duties, based on the reconnaissance | Paramedic & Doctor – Discussed crew duties and what equipment would be brought based on a winching | The crew – discussed the planned approach and the revised plan for each crew member after receiving an update on the patient’s condition |
Helicopter landing site
The landing site was adjacent to Shelly Beach carpark and was an ‘unimproved’ or ‘non‑conforming’ HLS.[8] The open area was about 21.5 m wide and 41.5 m at its longest point (Figure 7).
The air crew and the flight paramedic recalled the area was a confined area and a ‘tight fit’, however after a low-level reconnaissance at 100 ft, they determined that although there were some obstacles (foliage and trees) in the area, it was a suitable place to land.
When manoeuvring into the landing site, the ACO did not communicate the proximity of the obstacles at the rear of the aircraft and as such both the pilot and the flight paramedic were unaware of the hazard they posed.
The HLS had a slope of 10° towards the west, which was undetected by the ACO (Figure 7). The pilot advised that slope was difficult to detect using both NVIS and white light. The operator’s operations manual indicated that the slope limitation for the helicopter was 10° in all directions. The pilot advised that they had intended to check the slope in a low hover and even if there had been no other concerns, they may not have landed in the HLS due to the slope.
The operator required a minimum safety distance of 10 ft laterally around the main and tail rotor disk, with aircraft fuselage to be maintained clear of obstacles however, 20 ft lateral separation was preferred. A minimum safety distance of 6 ft vertically below the rotor disk was recommended and landing with any obstacle under the rotor disk was to be avoided wherever practical. Under night operations, crews were asked to increase safety margins depending on the situation, aircraft configuration, operating crew and environmental conditions.
The operator stated that once the aircraft was in a low hover in a confined area, manoeuvring should be minimised as it was difficult to maintain adequate visibility and obstacle recognition in all directions, particularly rearwards.
Figure 7: HLS slope and obstacle location

Source: Toll Helicopters annotated by the ATSB
Figure 8 shows the approach and intended landing directions. The plan was that when the helicopter was established in a low hover over the landing site, the nose would be turned right so the tail would fit in the cut-out area.
The ATSB did not attend the site, however the operator’s report advised that:
The operator confirmed that the same confined area had been used for a task by day, in good conditions, on 26 January 2021, however it was approached from the reciprocal direction. The reciprocal direction allows a larger landing area with more obstacle clearance due to the reduced slope.
The pilot advised the operator that the decision to approach the HLS was influenced by the information that a company helicopter had landed at the site previously. However, they also advised the ATSB that they were not influenced by this information when assessing the HLS. The paramedic recalled that the information played a part in deciding to go to the HLS. The ACO, recalled there had been an aircraft in the HLS previously, however, they did not state if that affected their decision to whether to conduct the approach.
Figure 8: Approach and intended landing orientation

Source: Google Earth annotated by the ATSB
Weather
Prior to the flight, the pilot reviewed the weather using the Bureau of Meteorology (BOM) meteorological aerodrome report (METAR) and terminal aerodrome forecast (TAF) for Sydney Airport. At the time of the incident, the METAR showed the wind from the south-south‑west at 18 kt, 10 km visibility, showers of rain in the vicinity, few clouds[9] at 1,800 ft and broken cloud at 3,300 ft.
The astronomical conditions at the time of occurrence included moon illumination of about 87%. The moon angle was at 50.03°, which produced a shadow length of about 25 m when at 100 ft. There was a possibility of reduced moon illumination due to the extent of the cloud and localised light rain in the area. The low angle of a rising or setting moon may reduce contrast detail and create strong shadowing effects which can mask hazards when operating under NVG. The crew reported ambient lighting generated from surrounding residential properties was present on approach to the HLS.
The operator’s operations manual states the minimum visibility for NVIS flight was 5,000 m and there should be no more than scattered cloud below 2,000 ft above ground level (AGL) within a 2 NM corridor either side of track. The weather at the time of this occurrence was above the minimum requirements for NVIS flight.
Flight data
The aircraft was fitted with a multi-purpose flight recorder (MPFR).[10] The MPFR data was found to contain the occurrence flight from Bankstown Airport to Bear Cottage, however the audio recording of the occurrence had been overwritten. Additionally, the operator provided the ATSB recorded rear cabin footage and the associated audio.
The MPFR data indicated that in the 30 seconds prior to the ACO instructing the pilot to climb, the aircraft experienced a 30° yaw to the left, a 2 ft lateral drift to the right followed by an 8 ft drift to the left, and a 3.5 ft longitudinal drift rearwards before a slight forward movement of 1 ft, as outlined in Figure 9.
Figure 9: Aircraft flight data
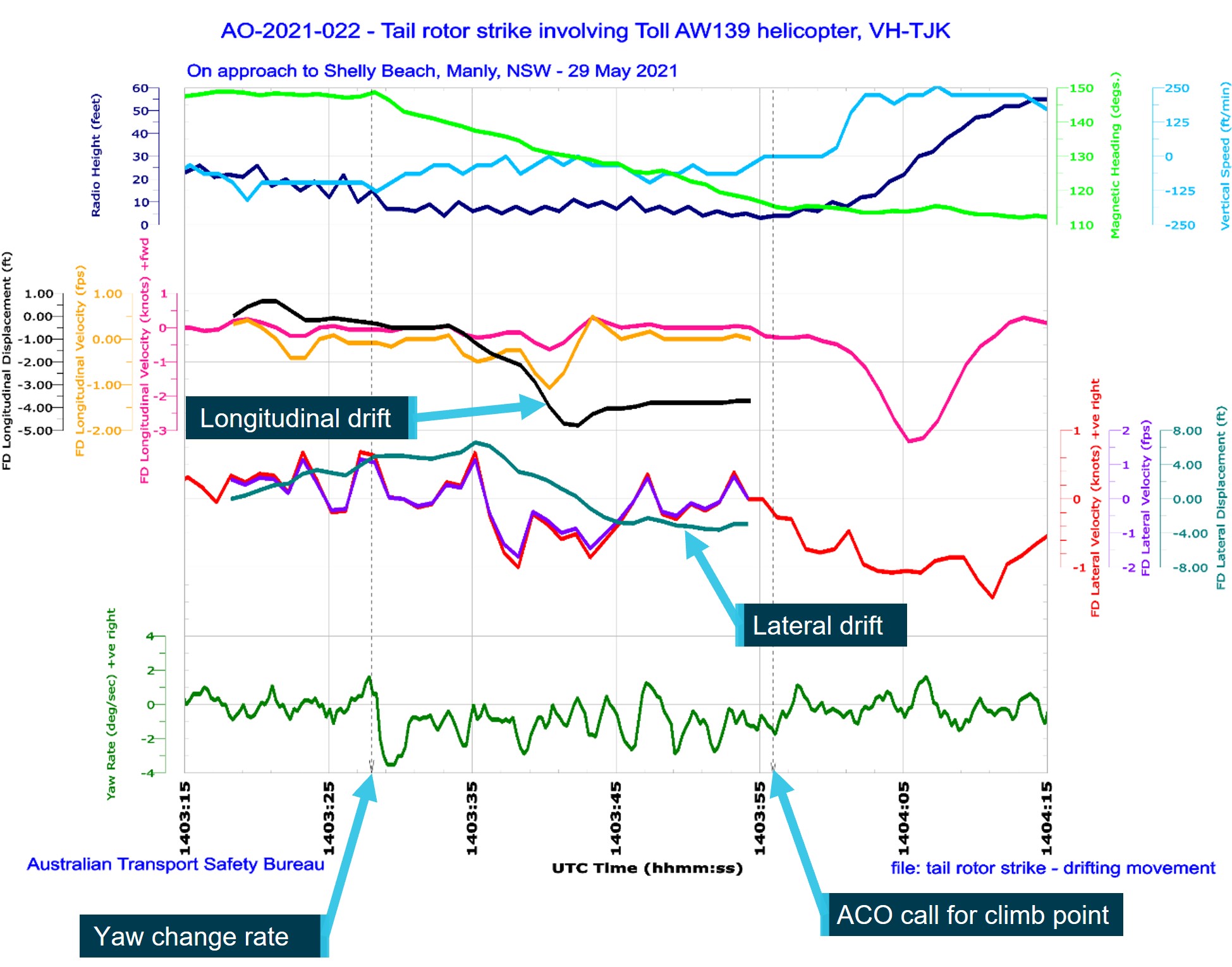
Source: ATSB
Training
Australian regulations required a minimum 6-month NVIS recency interval. However, the operator implemented a requirement for additional NVIS training, specifically ‘complex operations’ to confined areas, including winching in areas devoid of cultural lighting,[11] at least every 3 months. Further, 6-monthly recency flights were to be conducted with a training and checking pilot and/or ACO ‘to improve standardisation, enhance crews comfort levels and further develop the skills and knowledge required to operate on NVIS’.
The operator advised that the choice of NVIS training and checking locations was constrained by several factors, including proximity to the operator’s base (due required response time), the permission of various landowners, the presence of hazards, and to ensure sites were devoid of cultural lighting to maximise training effectiveness. As such, the operator also used simulators for recurrent pilot and ACO training and during clearance-to-line training. This included low level flying, winching, and manoeuvring into confined areas. Simulators were also used for ‘complex operations’ training for both pilots and ACOs.
Safety analysis
The crew completed a reconnaissance in a hover, however they did not conduct an orbit of the site. Although not required by the operator’s procedures, an orbit would have allowed the crew to view the site from different angles and may have enabled them to identify the sloping ground, which was on the limits of the slope allowed for the helicopter type. It would also have provided an opportunity to fully assess the extent of the obstacles/available clearances. However, the crew advised that due to the prevailing weather conditions and avoiding the residential area close‑by they did not conduct an orbit.
Following the reconnaissance, the crew completed a briefing in the hover before approaching the HLS. They discussed the size and shape of the proposed HLS, they also discussed the approach and obstacles, ensuring all members of the crew were consulted. Although the non-standard HLS met the requirements of the operators 10 ft obstacle clearance, the crew were aware it was tight. As such, only small, controlled helicopter movements were allowable once established within the confined area.
During the approach, the communication between the ACO and the pilot was continual and clear. Additionally, once established inside the confines of the landing area, the ACO actively moved within the rear cabin to assess the lateral and vertical clearance to obstacles. Despite that, unintended movement of the helicopter – both yaw and drift (lateral and rearwards) was not identified by the crew and stopped prior to the tail rotor contacting foliage.
The crew did not identify the tail rotor strike until after the helicopter was shutdown at the alternate landing site. This may have been due to the relatively light foliage that was contacted, with the active vibration control system also possibly dampening any rotor vibrations from the collision.
The ACO suspected that the tail may have contacted the tree during the initial approach however, there was no physical confirmation in the aircraft airframe of this occurring. Despite this, if the ACO had advised the rest of the crew that a strike may have occurred, it would have allowed discussion and informed decision making on subsequent actions.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the tail rotor blade strike involving Leonardo Helicopters AW139, VH-TJK.
Contributing factors
- While manoeuvring to land within a confined area, unintended yaw and drift of the helicopter was not identified by the crew and stopped prior to the tail rotor striking a tree.
Safety actions
Safety action by Toll Helicopters
The operator has completed the following proactive safety actions:
- The operator has amended their operational procedures stipulating aircrew maintain the following minimum clearances from terrain when operating in confined areas:
- 20 ft from the main and tail rotors
- by day only, 10 ft from main and tail rotors if operationally necessary
- for obstacles below the main rotors, 6 ft vertically
- 3 ft from aircraft fuselage including antennas and ancillary equipment.
- The operator issued guidance on site selection during primary missions outlining:
- aircrew to prioritise lower risk landing and winching sites (i.e. large open areas, playing fields, parks etc.)
- confined areas at or close to the scene should only be used if other options are not viable
- recommended or directed sites from emergency services on scene are not mandatory and should be regarded as guidance information only
- proximity to a scene should be regarded as secondary consideration.
- A final internal safety report was provided to the ATSB and proactively shared among the emergency helicopter network.
- Installed the A800 Trakkabeam high‑intensity searchlight onto the fleet of aircraft.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the crew of the occurrence flight
- Toll Helicopters (ACT/NSW)
- Bureau of Meteorology
- recorded data from the MPFR unit on the aircraft.
- cabin video and audio recordings
References
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Civil Aviation Safety Authority
- Toll Helicopters (ACT/NSW)
- Crew of VH-TJK
- Transportation Safety Board of Canada
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Helicopter Emergency Medical Service (HEMS): the use of helicopters to provide various kinds of medical care.
[2] Night Visual Flight Rules (VFR): a set of regulations that permit a pilot to operate an aircraft at night, in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[3] Night vision imaging system (NVIS): a system of internal and external lighting, combined with night vision goggles, which provides enhanced vision to crew for operation at night.
[4] Helicopter Landing Site (HLS): an area (not located on an aerodrome) wholly or partly used for the arrival or departure of helicopter.
[5] Confined area: an area where the operation of the helicopter is limited in some direction/dimension by terrain or the presence of obstructions or obstacles, man-made or natural.
[6] Capability Check Flight (CCF): periodic check (6-monthly) regarding the capability of an NVIS aircrew member in accordance with Civil Aviation Order 82.6
[7] O’clock: the clock code is used to denote the direction of an aircraft or surface feature relative to the current heading of the observer’s aircraft, expressed in terms of position on an analogue clock face. Twelve o’clock is ahead while an aircraft observed abeam to the right would be said to be at 3 o’clock.
[8] Unimproved helicopter landing site (HLS): a place that has not been prepared or supplemented with guidance infrastructure, identified for use as a temporary landing site for the purposes of landing and take-off.
[9] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that cloud is covering less than a quarter of the sky, if the sky is covered between 5/8 and 7/8 with clouds, it's reported as ‘broken’.
[10] Multi-purpose flight recorder (MPFR): includes a cockpit voice recorder (CVR) and flight data recorder (FDR)
[11] Cultural lighting: the illumination caused by the reflection of a major metropolitan area's lighting.