Safety summary
What happened
On the night of 14 March 2018, Heli-Aust Whitsundays Pty Ltd was operating a twin-engine EC135 P2+ helicopter, registered VH-ZGA, on a flight from its base at Port Hedland, Western Australia. This flight, conducted under the night visual flight rules, was to position the helicopter for a marine pilot transfer (MPT) from an outbound bulk carrier.
The pilot in command was a company instructor who was supervising line training with a recently recruited pilot. Earlier in their rostered shift, the pilot under supervision had passed a line check for day MPT and, having a total of 10 MPT flights, was approved for day operations. The instructor then introduced the pilot under supervision to night MPT operations and they completed 2 night MPT flights.
At 2330 local time, the helicopter was lifted off and climbed on track to the outer markers of the shipping channel (C1/C2), about 39 km from the port. Although the weather was suitable for the flight, there was no moonlight, and artificial lighting in the vicinity of C1/C2 was limited. Consequently, the approach to the ship was conducted in a degraded visual cueing environment that increased the risk of disorientation.
From a cruise altitude of 1,600 ft, the pilot under supervision descended the helicopter to join a right circuit around the carrier at the specified circuit height of 700 ft. During the base segment the helicopter’s altitude started to increase, reaching 850 ft soon after completing the turn onto final at an airspeed of about 70 kt. Although the helicopter was higher than the target height of 500 ft, a consistent descent was not established, and the helicopter remained above the nominal descent profile.
When the helicopter was about 300 m from the landing hatch, it was descending through 500 ft at a rate of about 900 ft/min. At about this point, a go‑around was initiated, but the helicopter descended to about 300 ft before a positive climb rate was achieved.
The helicopter was turned downwind for another approach and subsequently reached 1,100 ft. A descent was then initiated without coupling a vertical navigation mode of the autopilot. This was not consistent with standard operational practices and significantly increased the attentional demands on both pilots and associated risk of deviation from circuit procedure.
During the downwind and base segment of the circuit, the pilots did not effectively monitor their flight instruments and the helicopter descended below the standard circuit profile at excessive rate with decaying airspeed. Neither pilot responded to the abnormal flight path or parameters until a radio altimeter alert at 300 ft.
The instructor responded to the radio altimeter alert, reducing the rate of descent from about 1,800 ft/min to 1,300 ft/min. This response was not consistent with an emergency go-around and did not optimise recovery before collision with water.
After the unexpected and significant water impact in dark conditions, the helicopter immediately rolled over, and the cabin submerged then flooded. The instructor escaped through an adjacent hole in the windscreen and used flotation devices until rescued; however, the pilot under supervision was unable to escape the cockpit and did not survive.
What the ATSB found
In the context of a line training flight carried out in a degraded visual cueing environment, the ATSB found that a combination of factors contributed to the abnormal flight path and ineffective go-around. Firstly, the instrument panel was configured for single-pilot operation, which had a detrimental effect on the capacity of an instructor or training/check pilot to monitor the flight path and take over control if required.
In addition, the instructor had not been able to ensure that previous circling approaches flown in degraded visual cueing environments were consistent with the operator's standard operating procedures (SOPs), which probably limited the support provided to the pilot under supervision on the occurrence flight. As a related risk factor, the instructor did not report the previous deviations from SOPs or take other preventive/corrective action.
These limitations on the instructor’s capacity were coincident with the introduction of the pilot under supervision to night MPT operations without any day MPT consolidation or preparatory night flying. Given the pilot under supervision was transitioning from a different helicopter type and operational environment, this contributed to high cognitive workload for both pilots and increased the risk of sustained flight path deviations.
The ATSB also identified a number of other factors that increased the risk of the MPT operation. This included the pilot under supervision probably experiencing a level of fatigue known to adversely influence performance, due to a combination of limited sleep in the 48 hours prior to the accident and extended wakefulness on the day of the accident.
In addition, the operator's fatigue risk management system (FRMS) relied extensively on a sleep reporting spreadsheet (sleep log), and multiple pilots on multiple occasions had entered unrealistic or inaccurate sleep times, and there were limited effective controls in place to assure that the sleep times being entered by pilots was accurate. The ability of pilots to identify fatigue risks was also undermined by coding errors in the sleep log. At a higher level, the operator's FRMS did not describe the roster pattern or night shifts worked by line pilots based at Port Hedland, and the operator did not conduct a formal risk assessment of the roster prior to commencing MPT operations at Port Hedland.
In relation to the operator’s processes and procedures for MPT, the ATSB found there was a lack of assurance that personnel proficiency and helicopter equipment were suitable for the conduct of training at night in degraded visual cueing environments. In addition, the circuit and approach procedures for MPT did not minimise pilot workload or specify stabilised approach criteria with a mandatory go-around policy.
The operator rostered the pilot under supervision for MPT flying without ensuring that helicopter underwater escape training (HUET) had been completed in accordance with the operations manual. Although the pilot under supervision had completed HUET in 2009 and 2011, the lack of recency reduced their preparedness for escaping the helicopter following submersion.
The installed emergency locator transmitter (ELT) was not secured to the required primary load carrying structure of the helicopter, which increased the risk of non-activation during an accident.
Finally, although the operator’s primary helicopter activity was conducting MPTs, regulatory oversight activity by the Civil Aviation Safety Authority had not specifically examined the operator’s procedures and practices for conducting approaches and landings to ships at night in degraded visual cueing environments.
What has been done as a result
The operator carried out a safety investigation and introduced revised:
- training and checking specifications for MPT to address flight instrumentation, instructor/training/check pilot assurance, and pilot induction process
- MPT circuit procedures with defined stable approach criteria
- a fatigue risk management system for pilots, including modified tools.
The operator also:
- added emergency breathing system to pilot life jackets
- introduced a requirement for HUET every 2 years
- ensured ELT mounting conformance in its helicopter fleet.
The Civil Aviation Safety Authority (CASA) checked that MPT operators were complying with their own requirements for HUET recency and assessed the operator’s arrangements for crew scheduling and fatigue management at Port Hedland. As part of the new regulations introduced in December 2021, CASA clarified the guidance material regarding equipment requirements for training, checking and testing in aircraft designed for single pilot operation.
Safety message
The risks associated with marine pilot transfer operations in a degraded visual cueing environment are generally higher than conventional passenger-carrying activities and may require additional measures for safety assurance. Operators who conduct specialised flying are advised to assess the suitability of their pilot training/checking system and procedures for critical phases of flight. These should address flight path management, including the use of automation, stabilised approach criteria, and mandatory go-around requirements.
Flight crew fatigue is an insidious problem that is difficult to predict for each individual on an ongoing basis and can have subtle effects that undermine performance of critical tasks. Management of fatigue risk is a shared responsibility between operators and pilots and relies on sound principles, effective systems, and accurate recording.
Although the crashworthiness of helicopters is improving, there is an inherent tendency to roll and invert after a ditching or collision with water. Helicopter underwater escape training (HUET) provides familiarity with a crash environment and confidence in an emergency. Interviews with survivors from helicopter accidents requiring underwater escape frequently mention they considered that HUET had been very important in their survival. Training provided reflex conditioning, a behaviour pattern to follow, reduced confusion, and reduced panic.
From a regulatory perspective, the operator had demonstrated compliance with the standard requirements. However, if regulations do not have specific applicability to specialised operations, any safety-related audit of operators should assess the management of mission-specific hazards.
During the evening of 14 March 2018, a Eurocopter Deutschland GMBH[1] EC135 P2+ (EC135) helicopter, registered VH-ZGA, was being operated by Heli-Aust Whitsundays Pty Limited [2] on a series of marine pilot transfer (MPT) flights at Port Hedland, Western Australia. The helicopter was being operated from the heliport located at the port and the flights flown under the visual flight rules (VFR) in the charter operational category.[3]
These flights were normally conducted as a single-pilot operation. However, in this case, a pilot recently employed by the operator (pilot under supervision), who had not previously conducted MPT flights at night from Port Hedland, was flying the helicopter under the supervision of a company instructor pilot. Both pilots had been rostered for the night duty period (1800–0600 Western Standard Time).[4]
A total of 5 MPT flights were scheduled that evening and into the early morning of the next day. The first 2 flights were to transfer marine pilots from the port onto inbound bulk carriers[5] at the anchorage pilot boarding ground, about 9 NM (17 km) north of the heliport. The first transfer was completed during daylight and the helicopter landed back at the heliport just before sunset. The second transfer departed for the pilot boarding ground just after sunset. The 3 subsequent flights were to transfer marine pilots back to port from outbound bulk carriers near the end of the shipping channel at marine navigation beacons Charlie 1 (C1) and Charlie 2 (C2), about 21 NM (39 km) north-north-west of the heliport (Figure 1).
The first 3 MPT flights were completed without any reported incident. During the fourth scheduled transfer and on approach to the bulk carrier Squireship at C1/C2 to pick up the marine pilot, the helicopter crew initiated a go-around because the approach path had become too steep and began positioning the helicopter for another approach. During that manoeuvring, the helicopter descended and collided with the water.
The helicopter capsized immediately on impact and the cockpit flooded with water. The wreckage floated for a short time before sinking. The instructor pilot escaped from cockpit and was rescued a short time later. The location of the other pilot was unknown, and a search continued throughout the night and into the following days. On 17 March 2018, the helicopter wreckage was located on the seabed and the missing pilot was found inside the cockpit.
Figure 1: Chart showing relevant features at the seaport of Port Hedland

Source: Port Hedland electronic navigational chart produced by The Australian Hydrographic Office, modified by the ATSB
Departure from Port Hedland and transit to C1/C2
After completing the third transfer, the pilots did not shut down the helicopter due to the short turnaround prior to departing for the fourth transfer. At about 2330, the pilot under supervision lifted off from the heliport, set course for C1/C2 and climbed to an altitude of 1,600 ft.
At 2337, the helicopter was about 7 NM (13 km) south-south-east of the bulk carrier and the pilot under supervision established radio contact with the marine pilot on board the vessel. The marine pilot provided operational information to the helicopter crew, which included the direction and speed of the relative wind[6] across the vessel’s deck, which was 90° left of the bow at 15 kt (28 km/h) and clearance was provided for the helicopter to land. That wind direction necessitated an approach to the bulk carrier’s landing hatch from its starboard (right) side.
The marine pilot on board the bulk carrier recalled that the wind was light and there was no moon. Stars were visible and the lights of helicopter were seen as it approached the vessel. Data broadcast by the helicopter’s Automatic Dependent Surveillance Broadcast (ADS-B) equipment[7] and the bulk carrier’s Automated Identification System (AIS)[8] indicated that descent from cruise altitude commenced about 1,500 m from the vessel.
The instructor recalled[9] that as the helicopter approached the vessel, it was well-lit, with floodlighting of the deck and accommodation quarters. The weather conditions were described as fine, with no cloud, rain or obstructions to visibility.
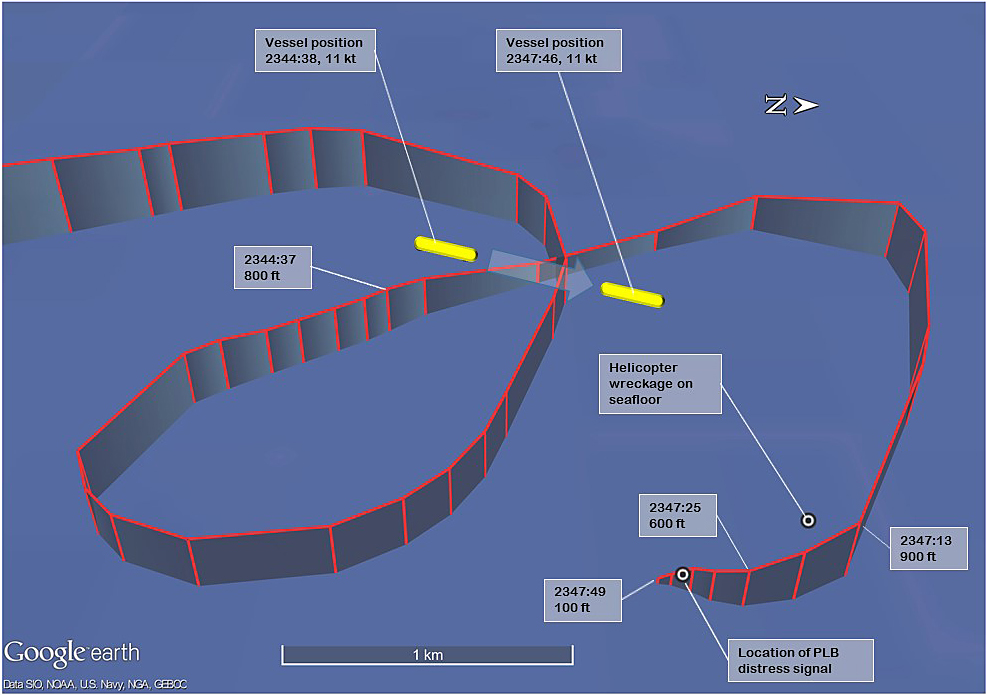
Figure 2 depicts the track of VH-ZGA as it was manoeuvred in the vicinity of the bulk carrier. ADS‑B and derived data at the alphabetically labelled points ‘A’ to ‘L’ is summarised in Table 1. Figure 3 graphically depicts the ADS-B and derived data while VH-ZGA was being operated in vicinity of the bulk carrier.
Figure 2: Manoeuvring of VH‑ZGA in the vicinity of Squireship

 This figure shows a representation of the flight path derived from ADS-B data recorded while VH-ZGA was being operated in the vicinity of Squireship. The white helicopter track is derived from positions recorded by Airservices Australia ADS-B receivers. Where that data was not available, positions recorded by the FlightRadar24 internet server were utilised and represented as the yellow flight path.[10] Data relevant to the annotated labels A to L is presented in Table 1 and marked as labelled index points in Figure 3. The light blue dots represent the AIS position of the bulk carrier recorded by the Australian Maritime Safety Authority receiver at corresponding times during the approaches of VH‑ZGA. The bulk carrier was 288 m in length, with the AIS position 248 m from the vessel’s bow.
This figure shows a representation of the flight path derived from ADS-B data recorded while VH-ZGA was being operated in the vicinity of Squireship. The white helicopter track is derived from positions recorded by Airservices Australia ADS-B receivers. Where that data was not available, positions recorded by the FlightRadar24 internet server were utilised and represented as the yellow flight path.[10] Data relevant to the annotated labels A to L is presented in Table 1 and marked as labelled index points in Figure 3. The light blue dots represent the AIS position of the bulk carrier recorded by the Australian Maritime Safety Authority receiver at corresponding times during the approaches of VH‑ZGA. The bulk carrier was 288 m in length, with the AIS position 248 m from the vessel’s bow.
Source: ATSB
Table 1: ADS-B and derived data, associated with the flight path of VH-ZGA depicted in Figure 2
|
Position |
Time (WST) |
Estimated range to landing hatch (m) |
Derived airspeed (kt)[1] |
Groundspeed (kt) |
Altitude (ft)[2] |
Geometric altitude rate of change (ft/min) |
|
A |
2341:37 |
- |
83 |
91 |
1,200 |
-513 |
|
B |
2342:21 |
- |
85 |
98 |
722 |
-576 |
|
C |
2343:02 |
2,300 |
78 |
82 |
722 |
-64 |
|
D |
23:43:44 |
2,075 |
68 |
62 |
825 |
+194 |
|
E |
23:44:29 |
925 |
50 |
48 |
775 |
-256 |
|
F |
23:45:05 |
275 |
31 |
30 |
525 |
-894 |
|
G |
2345:27 |
- |
78 |
78 |
325 |
0 |
|
H |
2346:13 |
- |
59 |
72 |
1,100 |
+831 |
|
L |
2347:13 |
1,775 |
77 |
83 |
822 |
-896 |
|
[1] Airspeed has been derived from ADS-B recorded groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. Where significant, the airspeed calculation has been adjusted for the effect of the descent flight path vector. [2] Altitude is either geometric altitude or pressure altitude reported in the ADS-B data set, corrected for atmospheric pressure. Geometric altitude is reported in increments of 25 ft, pressure altitude in increments of 100 ft. |
Figure 3: VH-ZGA derived airspeed, altitude and geometric altitude rate of change in vicinity of C1/C2

Graphical summary of aggregated ADS-B and derived data, while VH-ZGA was in the vicinity of the bulk carrier during the accident flight. The airspeed of the helicopter is derived from the ADS-B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The helicopter altitude is derived from the ADS-B geometric altitude and the independently measured pressure altitude, adjusted for surface pressure. The geometric altitude is reported in 25 ft increments, the pressure altitude is reported in 100 ft increments. The geometric altitude rate of change was broadcast by the helicopter’s ADS-B equipment, in increments of 6.25 ft/min. Breaks in the continuity of the data indicate periods where ADS‑B broadcasts were not being received. The labelled time markings correspond with the positions depicted in Figure 2 and Table 1.
Source: ATSB
First approach
The pilot under supervision positioned the helicopter for the approach and landing by flying a circuit around the vessel in a clockwise direction. The helicopter passed about 600 m astern of the bulk carrier while descending through a geometric altitude[11] of about 1,400 ft, at about 450 ft/min and at an airspeed estimated to be reducing through 87 kt.[12]
During the descent, the geometric altitude rate of change reported by the helicopter’s ADS-B equipment was about 500 ft/min, consistent with the upper mode of the automatic flight control system (AFCS - see the section titled Autopilot and stability augmentation system) being engaged in the altitude acquire (ALT.A) mode. After passing astern the vessel, the helicopter was turned right to circle around and position for the final approach.
The ADS-B data indicated the pilot under supervision levelled the helicopter at about 700 ft above the water during the downwind leg of the circuit, before it climbed slightly during the base leg of the circuit. The instructor recalled that the pilot under supervision completed the pre‑landing checklist, which included the arming the helicopter’s emergency flotation system.
At 2343:44, the helicopter was still climbing slightly as it was being turned onto final approach, with the airspeed reducing gradually through about 68 kt. The geometric altitude was increasing through 825 ft and the helicopter was about 2,000 m from the bulk carrier’s landing hatch. During the initial stages of final, the wind drift angle was estimated to be about 6° right. As the airspeed reduced, the size of the drift angle increased. ADS-B data indicated that, soon after the final track was established, the helicopter reached 850 ft then started to descend on the final approach. At this time, the helicopter was approximately 1,600 m from the landing hatch at an airspeed of about 60 kt.
The instructor recalled that the AFCS remained engaged until the helicopter was aligned on the final approach. The ‘upper’ autopilot modes were then decoupled, and the helicopter passed through the ‘entry gate’ with an airspeed of 50–60 kt at 500 ft.
The ADS-B data indicated that during the first 45 seconds of the descent, the helicopter’s geometric altitude reduced by 125 ft (commencing from 850 ft), before the descent rate gradually started to increase. At 2345:05, the helicopter was about 275 m from the landing hatch on the deck of the bulk carrier, descending through a geometric altitude of about 525 ft at a rate of about 900 ft/min. The airspeed gradually reduced to about 31 kt with a wind drift angle of about 19° right.[13]
The airspeed then began to increase, which was consistent with the recollection of the instructor that a missed approach (go-around) was commenced because of the steepening approach angle to the vessel. During the initial stages of the go-around, the airspeed continued to increase but the helicopter continued to descend, at a gradually reducing rate. The change in the ADS-B pressure altitude during this period was broadly consistent with the changes indicated by the ADS‑B geometric altitude and geometric altitude rate of change.[14]
Second approach
At 2345:14, the instructor radioed the marine pilot and said, ‘We’ll just have a second go at that, be with you shortly’. The ADS-B data indicated that, at that stage, the helicopter was passing overhead the deck of the vessel at about 375 ft, descending at about 500 ft/min and the airspeed was increasing through 60 kt. Soon after, the airspeed increased to about 80 kt and a positive rate of climb was established (325 ft altitude) and within a further 10 seconds, the geometric altitude rate of change was greater than +1,000 ft/min. The instructor recalled that a standard missed approach was flown, the AFCS upper modes were recoupled, and preparations commenced to make another approach. The helicopter was climbing through 700 ft when the crew turned the helicopter right, to position for another approach.
The available ADS-B data indicated that the helicopter reached an altitude of about 1,100 ft early on the downwind leg of the circuit. The airspeed reduced to about 60 kt during the final stages of the climb but started to increase again to about 75 kt as the helicopter flew downwind and commenced a descent. The instructor advised that the helicopter’s emergency flotation system remained armed from the previous approach, and that with the floats armed, the maximum airspeed limitation was 80 kt. Figure 4 depicts the track of VH-ZGA as it was repositioned for another approach. The ADS-B and derived data at the alphabetically labelled points ‘H’ to ‘R’ is summarised in Table 2. Figure 5 graphically depicts the ADS-B and derived data while VH-ZGA was being repositioned for the second approach.
Figure 4: VH-ZGA flight profile during the second approach

This figure shows a representation of the flight path derived from ADS-B data recorded while VH-ZGA was being operated in the vicinity of Squireship. The white helicopter track is derived from positions recorded by Airservices Australia ADS-B receivers. Where that data was not available, positions recorded by the FlightRadar24 internet server were utilised and represented as the yellow flight path. Data relevant to the annotated labels H to R is presented in Table 2 and marked as labelled index points in Figure 5.
Source: ATSB
Table 2: ADS-B and derived data, associated with the flight path of VH-ZGA depicted in Figure 4
|
Position |
Time (WST) |
Derived airspeed (kt)[1] |
Groundspeed (kt) |
Altitude (ft)[2] |
Geometric altitude rate of change (ft/min) |
|
H |
2346:13 |
59 |
72 |
1,100 |
+831 |
|
I |
2346:23 |
61 |
73 |
1,122 |
+704 |
|
J |
2346:45 |
74 |
86 |
1,122 |
-512 |
|
K |
2346:51 |
77 |
89 |
1,022 |
-832 |
|
L |
2347:13 |
77 |
83 |
822 |
-896 |
|
M |
2347:19 |
67 |
69 |
722 |
-1,088 |
|
N |
2347:25 |
53 |
50 |
522 |
-1,024 |
|
O |
2347:30 |
40 |
32 |
475 |
-1,344 |
|
P |
2347:36 |
34 |
22 |
300 |
-1,794 |
|
Q |
2347:45 |
30 |
21 |
75 |
-1,406 |
|
R |
2347:49 |
30 |
22 |
22 |
-1,280 |
|
[1] Airspeed has been derived from ADS-B recorded groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The airspeed derived from ADS-B groundspeed can slightly under-read at high rates of climb/descent due to the extra distance flown by the helicopter through the air, when compared to the horizontal distance used by the GPS receiver to calculate the speed across the ground. The size of that error increases as the rate of change in altitude increases and/or the groundspeed reduces. For this table, the derived airspeed has been adjusted for any effect of that climb/descent vector. [2] Altitude is either geometric altitude or pressure altitude reported in the ADS-B data set, corrected for atmospheric pressure. Geometric altitude is reported in increments of 25 ft, pressure altitude in increments of 100 ft. |
The airspeed started reducing again on late downwind and the descent continued. As the crew commenced the base turn, the airspeed was reducing through about 77 kt and the helicopter was passing through about 800 ft. Flight data also indicated that the rate of descent increased and exceeded 1,000 ft/min.
At 2347:25, the helicopter was part-way through the base turn and about 1,900 m east of the bulk carrier. The ADS-B data indicated that both the helicopter’s altitude and airspeed continued to reduce, while the rate of descent remained about 1,000 ft/min (see Table 2 and Figure 5).
Figure 5: VH-ZGA derived airspeed, altitude, geometric altitude rate of change and derived heading during second circuit

Graphical summary of aggregated ADS-B recorded data and parameters derived from that dataset, during the second circuit of the bulk carrier and during the final descent. The airspeed of the helicopter is derived from the ADS-B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The helicopter altitude cross-references the ADS-B geometric altitude and the independently measured pressure altitude, adjusted for surface pressure. The geometric altitude is reported in 25 ft increments, the pressure altitude is reported in 100 ft increments. The geometric altitude rate of change was broadcast by the helicopter’s ADS-B equipment, in increments of 6.25 ft/min. Breaks in the continuity of the data indicate periods where ADS‑B broadcasts were not being received. The labelled time markings correspond with the positions depicted for the helicopter in Figure 4 and Table 2.
Source: ATSB
The instructor recounted the following events on the second approach:
- the helicopter was turned inbound on the final approach
- the AFCS upper modes were decoupled
- they again passed through the ‘entry gate’
- the deck of the bulk carrier was in sight[15]
- the pilot under supervision reduced power/torque to commence the descent and again soon after.
The instructor recalled pointing out the descent rate to the pilot under supervision, requested an increase in power and was satisfied that the necessary correction was being made.
By contrast, a review of ADS-B data identified that, at about this time (2347:30), the helicopter was still about 1,900 m east of the bulk carrier, on a south-westerly track and not turning towards the vessel. On that track, the bulk carrier was to the right of the helicopter’s nose, with the lights of Port Hedland and the vessels at anchor to the left. The altitude and airspeed continued to reduce, and the rate of descent was about 1,300 ft/min and increasing.
From the deck of the vessel, the marine pilot could see the helicopter’s anti‑collision strobe light[16] and the green navigation light on the right side of the helicopter. The marine pilot did not recall seeing the red navigation light on the left side of the helicopter, nor any light from the helicopter’s steerable searchlight which was normally used during the final stages of the approach to illuminate the landing area. The marine pilot became concerned about the helicopter’s approach path and assessed that the helicopter was descending low on the horizon compared to observations of other flights.
The instructor recalled hearing the radio altimeter annunciating ‘check altitude, check altitude’. The radio altimeter was programmed to make this annunciation when the radio altitude reached the preselected altitude. The operator’s standard procedure was to set a radio altitude of 300 ft prior to take-off. The instructor recalled immediately taking over control of the helicopter and announcing to the pilot under supervision that they were conducting a missed approach (go‑around). The instructor did not remember hearing any alarms or other alerts from the helicopter’s warning systems.
The ADS-B data indicated that at a geometric altitude of 300 ft, the rate of descent was between 1,725 and 1,794 ft/min, the derived airspeed was about 34 kt and the altitude derived from the ADS-B reported pressure altitude was about 322 ft.
Soon after, the helicopter collided with the water surface. The ADS-B data indicated that about 12 seconds elapsed between the radio altimeter alert at 300 ft and the water contact. In that time the rate of descent reduced to about 1,280 ft/min while the airspeed remained about 30 kt.
The marine pilot watched the helicopter as it descended and recalled seeing a splash of water lit by a flash from the helicopter’s strobe light. Returning immediately to the bridge of the bulk carrier, the marine pilot alerted the port authority.
Post-accident
The instructor recalled that the cockpit immediately flooded with water and being submerged before being able to take a full breath of air. While still strapped in the seat, the instructor tried to operate the emergency door jettison, but had difficulty recalling the jettison action and did not believe that the door had released. The instructor then felt around and identified an alternative exit pathway through a break in the left front windscreen and kept hold of that opening using their left hand.
The instructor unsuccessfully attempted to unplug the helmet communications cord from the overhead console. Consequently, the instructor released the chinstrap and removed the helmet before releasing the seat belt. As recounted by the instructor, both hands were used to pull through the opening in the windscreen to escape the cockpit.
After vacating the cockpit, and while still underwater, the instructor identified and pulled one of the 2 inflation toggles on their personal flotation device. The chamber inflated normally and assisted the instructor to reach the surface. The instructor had no recollection or awareness of the other pilot’s location, movement, or actions in the cockpit after the water collision.
After reaching the surface, the instructor saw the helicopter was still afloat but inverted and then clung onto the helicopter’s left landing skid. The instructor could not see the pilot under supervision and was unsure of their location. The helicopter’s emergency flotation system had not automatically deployed on collision with water and inversion of the fuselage.
After a short time, the instructor remembered that the helicopter’s 2 life rafts[17] could be deployed using handles mounted on the underside of the rear cross-tube of the helicopter’s landing skids. The instructor pulled one of those handles and a life raft inflated and deployed from each landing skid. The life raft deploying from the left landing skid was trapped under the skid and unusable. The life raft from the right landing skid deployed normally and the instructor boarded that raft. The instructor recalled that the helicopter floated for a period of time before sinking, with the pilot under supervision still unaccounted for.
The crew of a surface vessel recovered the instructor from their life raft about 1 hour after the accident. The instructor had sustained only minor injuries.
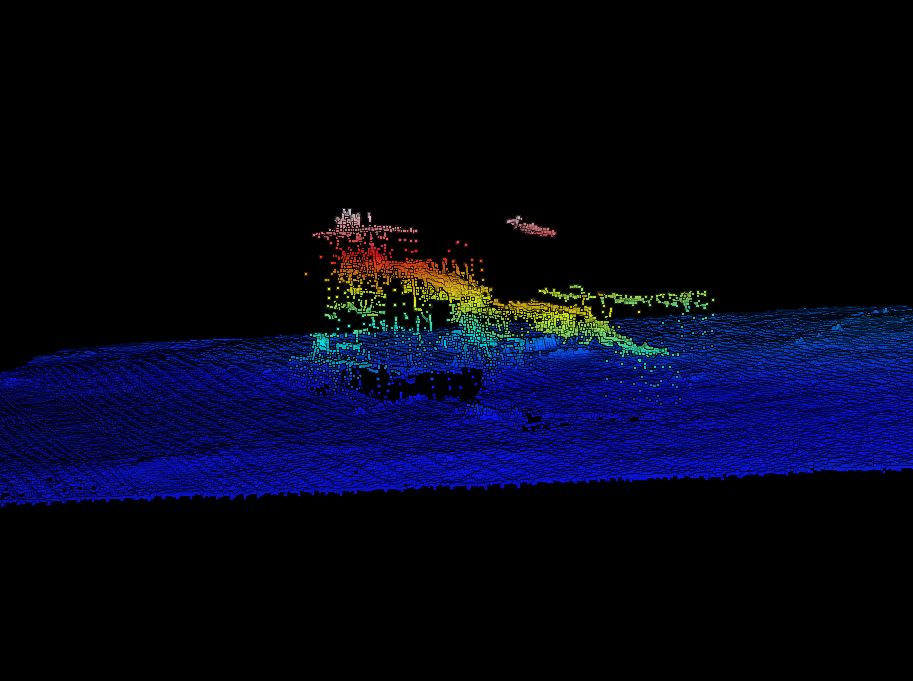
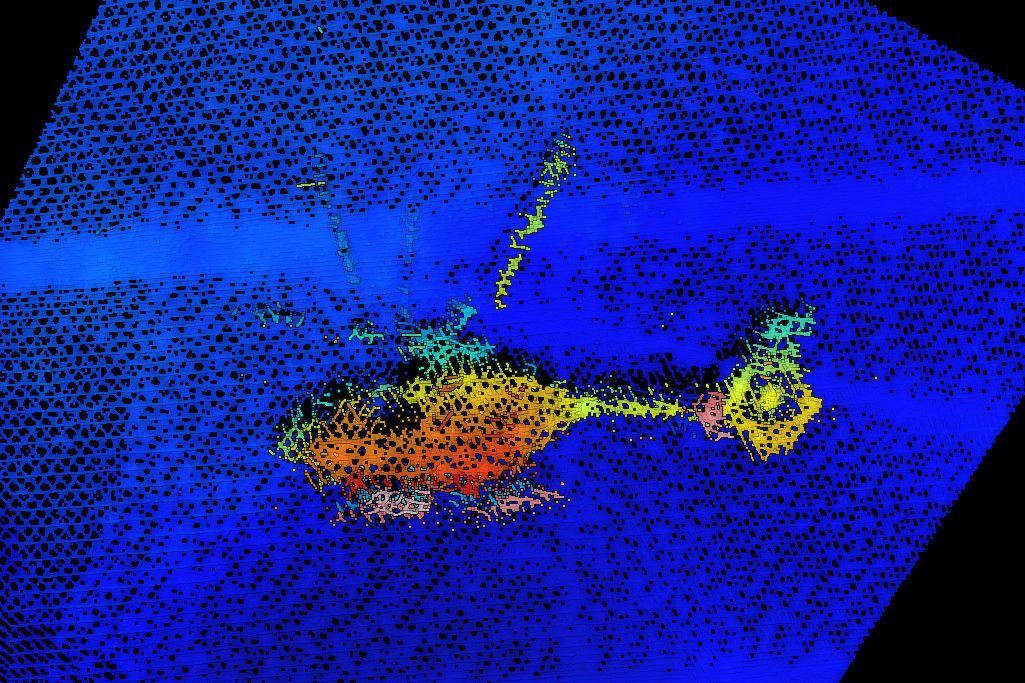
The search for the missing pilot and wreckage continued during the night and over the next 2 days. A vessel mobilised by the port authority commenced a sonar search of the seabed. On 17 March 2018 that vessel located the helicopter wreckage, approximately 675 m north-north-west of the last received ADS-B position. The helicopter was substantially intact and resting on its right side on the seabed in about 20 m of water. Divers from the Western Australia Police Force located the missing pilot in the helicopter cockpit.
- The holder of the type certificate is now Airbus Helicopters.
- Heli-Aust Whitsundays Pty Limited was the holder of the Air Operator Certificate issued by the Civil Aviation Safety Authority. The operator’s trading name for their Port Hedland operations was Port Hedland Helicopters.
- The operator did not operationally differentiate between flights carrying a marine pilot and flight sectors where there was no marine pilot on board. The Civil Aviation Safety Authority indicated that MPT flights were only charter category when a marine pilot was carried and at other times those flights would be categorised as positioning flights (in the aerial work category).
- Western Standard Time (WST): Coordinated Universal Time (UTC) + 8 hours.
- On bulk carriers, a cargo hatch cover was usually designated for use as a helicopter landing area.
- The relative wind reported by the marine pilot was the result of the surface wind velocity in that vicinity combined with the wind velocity due to the vessel’s motion. .
- The ADS-B equipment transmitted flight data that enabled air traffic service providers to track aircraft. Airservices Australia recorded the transmissions received by their network of ground-based ADS-B receivers. That data could also be received by other aircraft with suitable equipment and privately-operated ground-based equipment feeding information to flight tracking websites.
- The departing vessel was equipped with the maritime Automated Identification System (AIS) that transmitted data, including GPS position. That data was recorded by the Australian Maritime Safety Authority (AMSA).
- Instructor recollection at interview with the ATSB, a few days after the occurrence.
- In all of the figures that show ADS-B data, the line representing the flight path is a series of straight lines between successive data points. When the helicopter is in stable flight and the time interval between data points is short, the derived flight path is a close approximation of the actual flight path. As the time interval between data points increases, it is possible that the derived path does not closely reflect the actual flight path, although the trend over a series of points should be taken into account.
- The geometric altitude was calculated by the helicopter’s global positioning system (GPS) receiver using the GPS satellite constellation and is the height of the helicopter above the WGS-84 earth ellipsoid. The geometry of the satellite constellation and acceleration of the helicopter can affect the accuracy of the geometric altitude calculation.
- Airspeed was not a parameter transmitted by the helicopter’s ADS-B equipment. All airspeeds expressed in this report are derived from the ADS-B groundspeed and track, using the 10-minute average wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature.
- That is, to maintain the track across the ground indicated by the ADS-B data with the C2 recorded wind velocity and the derived airspeed, the nose of the helicopter would be pointing into wind, 19° left of the actual ground track.
- The pressure altitude transmitted by the helicopters ADS-B equipment was measured independently from the other parameters calculated by the helicopter’s GPS receiver. The correlation between the change in pressure altitude and the geometric altitude/geometric altitude rate of change is an independent verification of the altitude-related data trends identified in the GPS calculated data.
- This implies that the helicopter was tracking towards the bulk carrier on final approach.
- VH-ZGA was equipped with a red anti-collision beacon strobe light, that was mounted on top of the top of the Fenestron housing at the tail of the helicopter. Examination of the helicopter wreckage found the switch for this anti-collision beacon in the ON position. The switch for the white anti-collision strobe lights was found in the OFF position. .
- The life rafts were fitted to the helicopter’s landing skids and were stowed under protective covers, together with the bags for the emergency flotation system. When activated, the emergency flotation system or life raft inflated from under their protective covers.
Personnel information – pilot under supervision
Licence, rating, and general operating experience
The pilot under supervision obtained a commercial pilot licence (helicopter) in 2005 and air transport pilot licence (helicopter) in 2014. When these licences were transitioned to the equivalent Civil Aviation Safety Regulations (CASR) Part 61 qualifications in August 2015, they included a helicopter night VFR rating and helicopter multi-engine helicopter instrument rating, endorsed for conduct of 2-dimensional (2D) instrument approach operations and limited to non‑pilot in command duties.[18]Table 3 provides an outline of the pilot’s operating history.
Table 3: Pilot under supervision operating history
|
Year |
Operating history |
|
2005 |
Flight training for commercial pilot’s licence with R22, R44 and Bell B206 type endorsements |
|
2006–2009 |
Aerial work and charter operations with associated entity of occurrence operator; primarily in remote areas, including some tourist flights to/from ships |
|
2010 |
Transferred to predecessor of occurrence operator [1] at Mackay, Queensland – endorsed on Bell 222 (co-pilot) and EC135 types |
|
2010–2011 |
Marine pilot transfer (MPT) flying as co-pilot on BH222/430 night/IFR and pilot in command on B206 and EC135 day/VFR. Last EC135 flight of this period was in October 2011.[2] |
|
2012–2014 |
Joined a different operator at an inland base - remote area flying in B206L helicopters in support of the resource industry. |
|
2015 |
Overseas travel seeking flying work. Nil recorded flight time. |
|
2016 |
Re-joined B206L operator for inland remote area operations. Night vision imaging system (NVIS) rating issued in B206L type. |
|
2016–2018 |
Tours of duty at inland base – on standby to operate medical evacuation flights from remote areas at night in B206L helicopters utilising NVIS. |
|
2018 |
Recruited to operate EC135 on MPT flights from Port Hedland (non-NVIS) |
|
[1] Although this was the same air operator’s certificate (AOC) held by the occurrence operator, it was held by a different corporate entity. [2] The flight reviews for the EC135 type rating and BH222/430 type rating expired on 31 August 2014. The flight review for the co‑pilot multi-engine helicopter instrument rating (2D) expired on 31 May 2012. |
According to the operator’s electronic flight crew records, the pilot under supervision had logged a total experience of 4,057 flight hours, consisting of 3,666 hours single engine and 391 hours multi‑engine. Most of the multi-engine experience was co-pilot with 85 hours as pilot in command of EC135 helicopters. When dual and supervised flying was taken into account, the pilot’s total EC135 experience was 106.4 hours. The only night flying in the EC135 was 1.9 hours on the night of the accident.
Total night experience was recorded as 318 flight hours, which included 269 hours as co-pilot. Total instrument flying time was 117 hours consisting of 112 hours as co-pilot and 5 hours in a simulator.
In the 12 months prior to re‑joining the MPT operator, the pilot under supervision operated B206L helicopters for a total of 27.5 hours. This included 22.9 hours of night flying with 18.4 hours using a night vision imaging system (NVIS). The last night flight of this period was an NVIS proficiency check on 15 February 2018.
The operator’s chief pilot recruited the pilot under supervision in mid-February 2018 to fill a short‑notice vacancy in the pilot group operating from Port Hedland. This selection process was informal and based in part on the pilot under supervision holding an EC135 endorsement with sufficient experience to satisfy the contract requirement for a minimum 100 hours flying experience on the EC135 type. Other considerations for the chief pilot were previous MPT flying for the operator in 2011 and recent night flying experience in remote areas using NVIS. The chief pilot was aware that the pilot under supervision had been engaged in an emergency response role for the previous 3 years, which limited hours flown during that period.
Between 5 and 7 March 2018, the pilot under supervision was at the operator’s base in Mackay, Queensland for the initial induction and ground training process. Then, on 8 March 2018, the pilot under supervision travelled to Port Hedland for EC135 operational training.
Proficiency check and flight review status
All of the CASR Part 61 ratings were subject to periodic operational proficiency checks or flight reviews. Operator records and Civil Aviation Safety Authority (CASA) flight crew licencing data indicated that the pilot under supervision had completed the proficiency checks and reviews in Table 4.
Table 4: Previous operator checks or reviews with pilot under supervision
|
Date |
Proficiency check or flight review |
Expiry |
|
4 September 2016 |
Night VFR flight review – B206L |
30 September 2018 |
|
15 February 2018 |
NVIS rating Grade 2 proficiency check – B206L |
28 February 2019 |
Immediately following the night VFR flight review conducted by the previous operator on 4 September 2016, training started for the NVIS rating. Most of the subsequent flying for this operator utilised NVIS.
The flight instructor (for the previous operator) who supervised the pilot under supervision on a practice NVIS flight the night before the proficiency check on 15 February 2018 recorded that instrument flying (when required) was well flown but some procedures, such as radio broadcasts, downwind checks, and airspeed versus groundspeed checks, were not consistently applied. Overall, the standard of NVIS operations was considered to be improving. No comments were recorded for the successful NVIS check conducted by a company flight instructor/examiner the following night.
The instructor on the accident flight supervised 3.5 hours of EC135 flying by the pilot under supervision at Port Hedland on 10 and 11 March 2018 as revision for type-specific normal and emergency procedures. A helicopter type knowledge examination was also completed. For the combined EC135 flight review and VFR base check on 12 March 2018, the pilot under supervision operated to the pilot boarding ground, C1/C2 and Port Hedland Airport for 2.5 hours. The instructor recorded that normal circuits and various emergency procedures were conducted to a satisfactory standard. Having completed 6 hours of EC135 flying, the pilot under supervision was considered by the instructor to be ready for line training (supervised MPT) operations, starting the next day (13 March). No practice instrument or night flying was carried out during this pre-line training phase.
The operator was required to carry out periodic emergency procedures training in accordance with Civil Aviation Order (CAO) 20.11 and they also carried out initial and recurrent non-technical skills (NTS) training. The chief pilot assessed the pilot under supervision’s knowledge of emergency procedures applicable to the EC135 on 5 March 2018 and found it to be suitable.
According to the operator’s operations manual, pilots engaged in MPT were required to complete helicopter underwater escape training (HUET) at 3-year intervals. The pilot under supervision completed initial HUET in February 2009 and a second course in May 2011, with the training organisation recommending that training was valid through to 2013. Survival aspects associated with HUET are addressed in section Helicopter underwater escape training.
Marine pilot transfer experience
According to the operator’s electronic flight crew records, the pilot under supervision had conducted 253 deck landings by day and 76 deck landings by night. These figures included legacy data from 2010 and 2011 when deck or ship landings and offshore experience was recorded by a different method or not recorded at all. As such, the actual number of ship landings might have been higher.
It is likely that the pilot’s night deck landings were carried out while operating as co-pilot for BH222/430 MPT flights. One of the captains for this operation advised the ATSB that these night flights were to ships about 110 NM (204 km) offshore from Mackay. The co-pilot was required because the helicopters were not equipped with an autopilot.
The standard practice was for the captain to carry out the ship landing with the co-pilot in a supporting role. If the conditions were suitable, captains might allow the co-pilot to carry out a ship landing to gain experience, though these were generally not recorded.
The pilot under supervision commenced line training for Port Hedland MPT day operations on 13 March and night operations on 14 March 2018. Information about those activities and the relevant associated events are contained in the section Preliminary activities at Port Hedland in March 2018.
Medical information
The pilot under supervision held a Class 1 civil aviation medical certificate that was issued without restriction, valid to 18 April 2018. A review of CASA medical records did not identify any pre-existing condition or underlying health issue potentially relevant to the circumstances of the accident. The CASA records did not indicate the use of any prescription or over the counter medications. The pilot under supervision’s partner also indicated that the pilot was not experiencing any significant medical issues.
Police divers recovered the pilot under supervision from the cockpit of the helicopter. At the time of recovery, the pilot was not secured by the seat belt or wearing a helmet (see Survivability aspects - Helmets, communication cords and seat belts).
A post-mortem examination conducted by a forensic pathologist on behalf of the South Hedland Coroner did not identify any preceding pathology or injury. The pathologist’s post-mortem report indicated that it was not possible to ascertain the cause of death due to the elapsed time between the accident and location of the helicopter wreckage; only limited toxicology analysis was able to be performed.
Recent history
The pilot under supervision’s partner said the pilot normally slept about 9 hours each night, from about 2100 to 0630–0700. The operator’s pilots were required to record their hours of sleep and duty (in 1-hour blocks) in a sleep log (described in section Sleep logs). To develop a timeline of the periods the pilot was probably working and had opportunity to sleep,[19] the ATSB reviewed the pilot’s sleep log and other available information. This included the recorded times of phone calls and text messages, the content of text messages, and the recorded times that the pilot accessed the operator’s Port Hedland facility.
Based on the available information, key points included:
- The pilot under supervision woke early on 8 March to travel from Mackay to Port Hedland. A text message[20] indicated check-in for a flight at Mackay by 0500 Eastern Standard Time (0300 Western Standard Time).[21] Another text message indicated the pilot obtained a small amount of sleep during the day.
- The pilot under supervision performed various tasks (with no flying duty) on 9 and 10 March and then various tasks including some flying on 11 and 12 March. The available evidence indicated normal sleep periods during the nights of 8 to 11 March.
- During the morning of 12 March, the pilot under supervision received a night VFR flight planning assessment to complete prior to conducting planned night flying on 14 March. In text messages, the pilot expressed some concern regarding the completion of the assessment as their personal study notes were not in Port Hedland. There were indications the pilot did some reading for the assessment during the evening of 12 March.
- On 13 March, the pilot under supervision was rostered on a day shift (that is, from 0600–1800) to conduct MPT operations with the instructor. The first flight was scheduled for 0615 and, as indicated in text messages, the pilot under supervision planned to start work at 0430. Building access records indicated arrival at the operator’s premises at 0417, which correlated with a wake time of 0330. At 0413 the pilot sent a text message indicating they did not have a good sleep. The estimated sleep opportunity on the night of 12 March was about 5.5 hours.
- Text messages indicated the pilot under supervision left work at 1820 on 13 March, which meant completion of a duty period up to 14 hours duration.[22] The content of text messages indicated it had been a long day and the pilot was feeling ‘stuffed’. Flight records indicated that 9 MPT flights were conducted.
- On 14 March (the day of the accident), the pilot under supervision was rostered for a night shift (1800–0600) to conduct the second session of MPT operations with the instructor. Text messages indicated that, ‘as expected’ the pilot was awake at 0600 (with a weary face emoticon) and had slept well but wished it was for a longer period. The estimated sleep opportunity on the night of 13 March was 9 hours.
- Later on 14 March, the pilot under supervision indicated an intention to rest that afternoon, ‘if I get this flight plan done’, referring to the night VFR flight planning assessment. Other text messages indicated a degree of stress or frustration associated with completing the assessment. That afternoon, there were further messages stating that the assessment was completed and an attempt to sleep was unsuccessful. Another text message indicated that the last (and third) scheduled flight that night was at 0130, which was accompanied by a grimacing emoticon. Building access records and text messages indicated that the pilot returned to the operator’s port facility at 1609, prior to the start of the night shift.[23]
- The instructor recalled that, after completing the first 2 flights on the evening of 14 March, the pilot under supervision was advised to refuel the helicopter, conduct a daily maintenance inspection, and then take advantage of a break in the MPT schedule to retire to the nearby accommodation. Building access records and text messages showed the pilot under supervision left the operator’s premises at about 2000 and returned at about 2152. The instructor described this arrangement to the ATSB as providing the pilot under supervision with an opportunity to relax and did not believe the pilot under supervision needed to, or would, sleep in this time.
In summary, the available information indicated that the pilot under supervision obtained significantly less than their normal amount of sleep on the night of 12 March and, although they slept longer on 13 March, this was not as much sleep as they would have liked. At the time of the accident on 14 March (2348), the pilot under supervision had probably slept for at most 6 hours in the previous 24 hours and 12.5 hours in the previous 48 hours and had been awake for about 18 hours.
The instructor recalled that the pilot under supervision appeared ‘normal’ on the day of the accident and held no concerns about the pilot under supervision’s fitness for duty. There were no other available reports about the pilot under supervision’s alertness on the day of the accident.
The pilot under supervision’s partner recalled that the pilot was happy to be working for the operator and was feeling good about their performance on the initial flights and the feedback provided by the instructor. The partner also recalled that the pilot was concerned about having enough time to complete the night line check prior to the instructor leaving Port Hedland on 16 March. The partner recalled the pilot saying their hotel accommodation was noisy, including at night, and there were some difficulties with sleep.
Personnel information – flight instructor
Licence, rating, and general operating experience
The instructor held an air transport pilot licence in the aeroplane and helicopter categories with a multi-engine instrument rating and night VFR rating in both categories. Additional ratings included a grade 1 flight instructor rating for aeroplanes and helicopters and flight examiner rating for helicopter licences and ratings, including night VFR and EC135 ratings. Table 5 provides an outline of the instructor’s licences and ratings.
Table 5: Sequence of the instructor’s licence and rating issue
|
Year |
Licence and rating issued |
|
1992 |
Commercial pilot licence (aeroplane)[1] |
|
2000 |
Commercial pilot licence (helicopter) |
|
2006 |
Grade 1 aeroplane instructor rating[1] |
|
2007 |
Air transport licence (aeroplane)[1] |
|
2009 |
Air transport licence (helicopter) |
|
2009 |
Grade 1 helicopter instructor rating |
|
2012 |
Multi-engine helicopter instrument rating |
|
2014 |
EC135 type rating |
|
2015
|
Started with EC135 operator |
|
2016 – 2018 |
EC135 MPT and flight training/assessing |
|
[1] At the time of the occurrence the instructor was not maintaining the aeroplane licences and ratings. |
Prior to starting with the operator in 2015, the instructor was chief pilot and chief flying instructor of a flying school that provided CASR Part 61 flight training and reviews for the operator.
According to the operator’s electronic flight crew records, the instructor had logged a total of 6,285 hours experience consisting of 2,114 hours aeroplane and 4,171 hours helicopter. Most of the helicopter experience was light single-engine helicopters ranging from R22 to AS350 Squirrel types.
Total multi-engine helicopter experience was 758 hours consisting of 41 hours AS355 twin squirrel and 717 hours EC135. As pilot in command of EC135 helicopters, the instructor logged 467 hours by day and 188 hours by night. A further 62 hours were training or checking under the supervision of an instructor.
Of the total 703 hours night experience, 100 hours were aeroplane and 603 hours were helicopter. Most of this helicopter time was various single-engine types with 200 hours EC135.
Total instrument time was 499 hours, consisting of 234 hours in a simulator and 265 hours flight time. That instrument flight time was divided into 93 hours aeroplane and 172 hours helicopter, including 54 hours EC135.
The instructor’s pilot’s logbook showed total instructional experience of nearly 4,000 hours consisting of 1,700 hours aeroplane and 2,250 hours helicopter. Instructional experience included EC135-specific instruction of 164 hours by day and 48 hours by night.
Proficiency check and flight review status
All of the CASR Part 61 ratings were subject to periodic operational proficiency checks or flight reviews. Based on CASA records, the instructor had completed the checks and reviews that were relevant to the occurrence (see Table 6).
Table 6: Instructor’s proficiency checks and flight reviews
|
Date |
Proficiency check or flight review |
Expiry |
|
24 May 2016 |
Night VFR flight review – EC135 |
24 May 2018 |
|
24 May 2016 |
Flight instructor proficiency check – EC135 |
31 May 2018 |
|
27 October 2016 |
Multi-engine helicopter/EC135 type flight review (with IPC) |
31 October 2018 |
|
7 June 2017 |
Instrument proficiency check (IPC) |
30 June 2018 |
|
8 June 2017#rgbrgb |
Flight examiner proficiency check (EPC) |
30 June 2019 |
Based on records and interviews with flight examiners, the instructor had demonstrated compliance with the requirements of the various Part 61 proficiency checks and flight reviews. The ATSB noted that the recent EPC in June 2017 was carried out in a company EC135, VH‑ZGP, which was configured with an instrument panel that allowed for 2-pilot IFR operation.
The instructor advised that the flying and knowledge assessments were carried out in a wide variety of environments and flight regimes by experienced and qualified personnel. According to the instructor, at no stage was any significant deficiency identified and there was no evidence of inconsistent flying or varying commitment to flight safety.
The instructor’s logbook indicated that the flight instructor proficiency check (May 2016) was completed in VH-ZGZ. That helicopter did not have flight instruments at the instructor’s seating position. The logbook entry indicated the flight was flown by day and included multi-engine operations and emergencies.
The operator reported that it had not checked the instructor’s proficiency flying from the left seat of an EC135 equipped with a single set of flight instruments situated diagonally across the cockpit from the instructor seating position, in degraded visual environments.
Operator-managed training and assessing status
In addition to the CASR Part 61 checks and reviews, the following flight training and checks were recorded as carried out on behalf of the operator. All except the first check were within expiry dates at the time of the occurrence (see Table 7).
Table 7: Instructor’s additional checks and assessments
|
Date |
Training, proficiency check or flight review |
Expiry |
|
9 September 2015 |
Helicopter underwater escape training |
9 September 2018 |
|
6 March 2017 |
Instructor standardisation check – EC135 (day) |
6 March 2018 |
|
15-17 March 2017 |
Refresher training in emergencies – EC135 simulator (day)[1] |
Not applicable |
|
17 March 2017 |
Base check – EC135 (day)[2] |
17 March 2018 |
|
5 April 2017 |
MPT line check – EC135 (night) |
5 April 2018 |
|
25 May 2017 |
Human factors flight operations refresher training |
25 May 2019 |
|
17 July 2017 |
CAO 20.11 emergency procedures assessment – EC135 |
17 July 2018 |
|
16 August 2017 |
CFIT/ALAR recency |
16 August 2018 |
|
[1] This refresher training was conducted by the helicopter manufacturer at their factory simulator centre in Germany. [2] Recorded in the operator’s recency database. |
Based on records and interviews, the instructor had demonstrated conformance to the requirements of the various training and assessments. However, there was anomalous information about the MPT line check flight conducted on 5 April 2017.
That flight was a night flight to Pacific Treasure at the pilot boarding ground then to Shandong Zheng Tong at C1/C2. The chief pilot recorded this flight as a line check of the instructor, but the instructor recorded the same flight as fulfilling the requirements of a night VFR flight review of the chief pilot. The ATSB queried both pilots about the anomaly about 3 years after the occurrence.
Neither pilot could recall any specific details about the flight and could not definitively account for the anomaly. In retrospect, the chief pilot considered it was a line check of the instructor (as pilot controlling the helicopter from the right seat) and the flight review certified by the instructor was based on the chief pilot as pilot in command of that night VFR flight. The instructor advised the ATSB that applicants for a night VFR flight review were required to demonstrate helicopter handling, including manoeuvring with reference to instruments, before the review could be certified complete.
To resolve this anomaly, the ATSB obtained and analysed the ADS-B data for the flight on 5 April 2017. This was compared to ADS-B data for all MPT flights conducted at night by the chief pilot and instructor, respectively, at Port Hedland in January 2018. The ADS-B data for the flight on 5 April 2017 is presented in graphical and tabular form at Appendix C.
Data for the flight on 5 April 2017 showed that circling to both ships was conducted at about 1,000 ft, which was higher than the specified circuit height of 700 ft. Additionally, on both approaches the derived airspeed through 500 ft was about 40 kt, which was lower than the specified 60 kt for the ‘finals gate’.
When that data was compared with data for previous night flights conducted by the chief pilot and instructor at Port Hedland in January 2018, there was a higher correlation with the flights conducted by the instructor. Given the data for the flight on 5 April 2017 was consistent with a typical MPT operation and had a higher correlation with flights conducted by the instructor, the ATSB assessed that the flight was more consistent with a line check than a night VFR flight review. Based on the available information, ATSB was unable to further resolve the anomalous records for this flight.
Marine pilot transfer experience
The instructor was inducted into the marine pilot operation in August 2015 and received EC135 revision training with a flight review. After a month of operating a B206 helicopter and supervising some IFR training on a flight training device, the instructor completed further EC135 revision flying and began EC135 MPT operations under supervision. Over a 3-month period, the instructor conducted a mix of MPT as pilot in command under supervision, flight reviews and other training with company pilots.
On 4 January 2016, the chief pilot conducted a day line check with the instructor from the Mackay (Hay Point) base. The chief pilot recorded the instructor completed 6 ship landings and flew the EC135 well. Based on a satisfactory standard, the instructor was cleared to line for day MPT from Hay Point.
After being cleared to line, the instructor conducted 42 ship landings in daylight conditions, including 7 as pilot in command under supervision. From 11 February 2016, night line training started.
On 8 March 2016, the chief pilot conducted a night line check with the instructor from Hay Point. The chief pilot recorded in the check report that the instructor achieved a sound standard, with comments about lift-off technique, standard call‑outs, ship overflight, and positioning for into-wind approaches. The instructor was also reminded to keep the approach to the vessel relatively steep in case of an engine failure. On completion of the check the instructor had conducted 13 night ship landings and was cleared to line for night MPT.
After being fully checked to line, the instructor was engaged in MPT operations and continued to conduct some flight training and assessments under the approval of the associated flying school.
A review of the operator’s electronic flight crew records and the instructor’s logbooks covering the period 1 January 2017 to the date of the accident, indicated about 370 hours had been flown, mainly in the EC135 type. Of those hours, about 270 were completed in the role of instructor/examiner, which would have been consistent with operations from the left seat.
During that same period, about 180 ship landings were recorded, with about half of those being conducted on night operations. Of the night ship landings, about 30 were in the role of instructor/examiner, consistent with operations from the left seat.
The operator’s electronic flight crew records indicate that the instructor had completed a total of about 450 ship landings. Those records also indicated for the EC135, a total of about 160 hours of day instructing and about 50 hours of night instructing.
For operations at Port Hedland, a total of 10 night flights to C1/C2 were identified, with 3 flown from the right (command) seat in January 2018 and the 7 remaining flights in the role of instructor/examiner from the left seat during April 2017 and March 2018.
Previous night operations at Port Hedland
The ATSB obtained the ADS-B data for the instructor’s transfer flights conducted in January 2018. In addition to the 3 night flights to C1/C2, the instructor conducted 2 night flights to the pilot boarding ground. The data for the 5 night approaches, all in the early morning of 8 January 2018, is presented in graphical, and tabular form at Appendix B.
Moonrise on 7 January 2018 was at 2314 and moonset at 1131 the next day with about 60% of the moon’s visible disc illuminated. For the 5 flights, the moon would have been above the horizon and moving in an arc between 34° and 64° altitude.
An analysis of satellite imagery and meteorological data conducted by the Bureau of Meteorology indicated a large area of scattered to broken stratus cloud (covering between a quarter to almost all of the sky) offshore from Port Hedland with a cloud base estimated to be about 1,200 ft.
With broken stratus cloud and the moon still relatively low in the eastern part of the sky, conditions below the cloud base would have been generally dark, with some patches where the moonlight may have penetrated the cloud layer to illuminate the sea surface. Depending on the angle of approach, the reflection of moonlight on clouds may have been visible. If the stratus cloud was scattered, there would have been better illumination of the sea surface.
The ATSB noted the following:
- On each arrival the instructor conducted a circuit of the vessel to position for final approach.
- Other than the first approach, altitude on downwind was inconsistent and non-conforming with the operator’s procedures. Analysis of the ADS-B data indicated that an autopilot upper mode was not used for vertical navigation during operation in the circuit.
- Other than the first approach, the rate of descent on base was higher than industry practice.
- Other than the first approach, when established on final approach the helicopter height and airspeed did not conform to the operator’s final gate parameters.
- The final approach profile was not consistent and on the fourth approach, the rate of descent exceeded the operator’s limit for continuing the final approach below 300 ft.
- On the second and fourth approaches, the final approach profile was corrected soon after 300 ft, which correlated with the radio altimeter warning.
- Although there was a partial moon, surface illumination was probably attenuated by cloud.
- Operations above 1,200 ft, during climb, cruise and descent, might have been affected by cloud.
The ATSB noted that the chief pilot was also carrying out leave relief flying in Port Hedland at the same time and was not advised of any anomalies. Additionally, no report was submitted to the operator’s safety management system.
Medical information
The instructor held a Class 1 civil aviation medical certificate that was valid until 2 October 2018. The certificate required the instructor have reading correction available while exercising licence privileges. Consistent with this restriction, the instructor was wearing prescription spectacles for reading correction.
The instructor said that glasses were always worn when flying. These were bifocal with a focal point customised to the distance from the right-side pilot seat to the instrument panel of the EC135.
There were no other restrictions on the instructor’s medical certificate and the instructor said that there had been no recent illness.
Recent history
The instructor travelled to Port Hedland on 5 March 2018 and was nominally rostered from 0900–1700 between 6 and 15 March. These shifts primarily related to the instructor’s role as head of training and checking and included training and checking flights for other pilots based at Port Hedland. Conducting those tasks would require both day and night operations and the instructor was expected to manage their duty activities during that period and comply with the operator’s fatigue risk management system (FRMS). Information about the operator’s FRMS is discussed in the section Operator’s fatigue risk management system.
The ATSB reviewed the instructor’s sleep log and other available information to determine likely hours of duty and sleep opportunity in the days leading up to the accident. The ATSB observed numerous anomalies when comparing the recorded sleep times in the instructor’s sleep log against other information (see section Review of data in sleep logs). Based on the available information, key points included:
- The instructor had a sleep opportunity of about 7–8 hours during each night from 5 to 8 March.
- On 9 to 11 March, the instructor conducted work tasks, including training flights, in the afternoon and evening. There were sleep opportunities of about 5 hours, 6.5 hours and 7.5 hours over those 3 nights.
- On 12 March, the instructor conducted work tasks from about 1200 to 1900 and recorded sleep in the sleep log from 2200 on 12 March to 0600 the following morning. However, building access records indicated the instructor arrived at the operator’s premises at 0430 and, therefore, had probably been awake before 0400. It is likely there was a sleep opportunity of about 5.5–6 hours, assuming sleep from 2200 as recorded.
- On 13 March, the instructor was rostered for MPT operations with the pilot under supervision from 0600–1800. The instructor arrived at work at 0430 and was still onsite until at least 1917. The sleep log indicated a sleep period from 2200 until 0600 on 14 March (8 hours), though it was unclear whether the instructor had recorded these times (as these were the default values included in the sleep log tool). Phone records indicated the instructor was awake from about 0530 on 14 March, and probably had an overnight sleep opportunity of about 7.5 hours.
- When interviewed a few days after the accident, the instructor recalled sleeping well on the night of 13 March and waking late in the morning of the day of the accident. The instructor followed their normal routine and advised of sleeping in bed from about 1400–1600 in preparation for the night shift starting at 1800. Phone records showed no activity from about 1100 to 1600, although a draft email was saved at about 1500 in the afternoon.[24] Accordingly, it is possible the instructor obtained some sleep in the afternoon. The instructor arrived at work at 1648.
In summary, the available information indicates that the instructor had restricted sleep opportunity (5–6.5 hours) on the nights of 9, 10 and 12 March. There were opportunities for 7.5 hours sleep on each night of 11 and 13 March, with a reported 2 hours additional sleep during the day on 14 March. At the time of the accident on 14 March (2348), the instructor had probably slept at most 7.5 hours in the previous 24 hours, and 13.5hours in the previous 48 hours, assuming 2 hours sleep during the day of 14 March as reported.
None of the pilots the ATSB spoke to described seeing the instructor on the night of the accident, although one pilot recalled seeing the instructor on the day before the accident and being concerned about their level of fatigue. According to that pilot, the instructor had red, tired-looking eyes with the appearance of ‘burning the candle at both ends.’ The instructor recorded a relatively high fatigue evaluation at or near the end of the day on 13 March (see section Pilot self-assessments of fatigue).
When interviewed by the ATSB a few days after the accident, the instructor reported feeling alert prior to starting work on the day of the accident. A self-rated fatigue level at the time of the accident was between 2 and 3 out of 7[25]. Immediately prior to the accident flight, the instructor was not feeling completely fresh but did feel rested due to the sleep achieved during the day.
The chief pilot at the time of the occurrence advised that the 14‑hour duty period on 13 March was not normal and was not in accordance with the operator’s FRMS. Pilots were expected to start duty about 30-45 minutes before a scheduled lift-off and to complete their duty within 12 hours unless there was a split shift. The chief pilot noted that it was common for pilots to stay at the office for social reasons after a shift finished, so all the time at the office did not necessarily correspond to duty time.
Helicopter information
General information
The EC135 P2+ helicopter is a light multi-purpose twin-engine helicopter manufactured by Eurocopter Deutschland GMBH. The occurrence helicopter (serial number 777) was built in 2009 and imported into Australia from the United States (US) and registered as VH-ZGA in early 2017. The helicopter was maintained in accordance with the manufacturer’s continuous maintenance program.
At the time of the occurrence, the total time in service of the helicopter was 3,739 hours and time in service since last maintenance was 24.2 hours. Although the maintenance release was not with the helicopter when it was recovered from the seabed, there was no report of any defects prior to the occurrence. Furthermore, a general review of the maintenance records did not identify any anomalies.
The helicopter was powered by 2 Pratt & Whitney PW 206 B2 engines that were equipped with full authority digital engine control (FADEC) systems. When both engines were operating, the 5‑minute take-off torque limit[26] for each engine was 78% and maximum continuous was 69%. Adherence to these limits was dependent on pilot inputs (through the collective control). In an engine inoperative situation, up to 128% torque was available from the operating engine for up to 30 seconds, followed by 125% torque for 2 minutes.
Torque from the engines was transferred by the main transmission to a hydraulically-controlled 4‑bladed rigid main rotor. Antitorque was provided by a Fenestron-type system.
For maintenance purposes, data was transmitted by the electronic engine control (EEC) unit to the data collection unit (DCU) for each engine. Data was only recorded by the DCUs when parameter thresholds were exceeded.
The operator’s 2 EC135 helicopters based at Port Hedland were fitted with aftermarket single-pilot IFR kits in accordance with a supplemental type certificate (STC) approved by the US Federal Aviation Administration. This STC was generally installed to optimise the utility of the helicopter for special mission operations such as aeromedical. The STC was not required for the MPT operation and had no significant effect on the conduct of routine MPT flights. The helicopter was fitted with dual flight controls.
The helicopter cabin incorporated a hinged door adjacent to each pilot seating position and a sliding door on either side of the rear cabin for passenger access. An optional door jettisoning kit was installed that allowed the pilot door hinge pins to be released in an emergency. To jettison the door in accordance with the placard, the pilot was required to open the door (via normal open/close handle) then push the jettison lever downwards.
The helicopter was also equipped with an emergency flotation system[27] that comprised skid‑mounted inflatable floats. The floats could be either manually or automatically activated. Manual activation used a mechanical handle mounted on the pilot’s cyclic control. Automatic activation was via operation of a water immersion switch. Electrical power was required to initiate inflation of the automatic inflation mechanism. The helicopter was also equipped with 2 life rafts that could be manually deployed using a cockpit handle or external handles fitted to either side of the rear cross‑tube of the landing skids.
VH‑ZGA and other EC135 helicopters in the operator’s fleet were not fitted with a helicopter terrain awareness and warning system (HTAWS). An enhanced ground proximity warning system (EGPWS) was available from the manufacturer as an option. At the time of the occurrence, and writing, HTAWS was not required for the category of helicopter and type of operation.
Autopilot and stability augmentation system
The helicopter was equipped with an automatic flight control system (AFCS) supplied by the manufacturer as an option. This system enabled single-pilot operations in instrument meteorological conditions.
The AFCS consists of 3 independent elements: stability augmentation system (SAS), pitch damper, and 3-axis autopilot system. Each element operated as part of an integrated system according to programmed control laws and pilot selectable modes. The AFCS was selected ON for normal operations.
Stability augmentation was provided by a yaw SAS and pitch and roll SAS. These systems computed yaw rate and used attitude sensor data to drive actuators connected in series or parallel to the pedal and cyclic flight control circuits. In the default condition, feedback was provided to each pilot’s cyclic control.
Pitch damping utilised computed rate data to control an actuator within the cyclic pitch circuit. When the autopilot was operative, it directly commanded movement of the pitch damping actuator.
The autopilot system comprised the autopilot module (APM) and autopilot mode selector (APMS), which was located on the centre console panel. The APM was interfaced with multiple flight state data sources, SAS sensors and actuators.
In typical operation, the pilot selected the autopilot ON before take-off, which engaged the default automatic trim mode (A.TRIM). This basic autopilot function provided attitude hold that allowed ‘hands-off’ operation for reduced pilot workload. If A.TRIM was selected off, the system entered an autopilot SAS mode requiring ‘hands-on’ operation and some autopilot modes were not available.
When operating in the A.TRIM mode, the pilot could make adjustments to pitch and roll attitude by manipulating the cyclic control (Figure 6) in one of 3 ways. First, the pilot could simply override the A.TRIM control inputs to move the cyclic as required. On pilot release of cyclic input, the (unchanged) trim forces would return the cyclic and associated attitude to the pre-input values. This method could be used for short term attitude adjustments.
Second, the pilot could press and hold the force trim release (FTR) switch on the cyclic grip while moving the cyclic as required. Actuation of the FTR switch opened the actuator clutches and removed resistance to cyclic movement. When the switch was released, the actuator clutches closed and the A.TRIM was synchronised to the current cyclic position and associated attitude. Use of this method for significant and sustained attitude adjustments was common.
Finally, the pilot could manipulate the 4-way BEEP TRIM switch to ‘slew’ the attitude reference at 2–4° per second (depending on airspeed and axis). Without further pilot input, the helicopter would change attitude smoothly to the new reference. This was the preferred method for small attitude changes or fine adjustments.
Figure 6: Cyclic grip switch arrangement (side and front view)

Source: EC135 Approved Rotorcraft Flight Manual
In addition to the basic autopilot mode, when the helicopter was at or above 65 kt airspeed, the AFCS allowed the pilot to engage ‘upper’ modes:
- altitude (ALT), to maintain the current barometric altitude
- heading (HDG), to select, intercept, and maintain a magnetic heading
- airspeed (IAS), to maintain the airspeed at the reference value
- altitude acquire (ALT.A), to acquire and perform an automatic level-off to capture a selected barometric altitude
- vertical speed (V/S), to maintain the vertical speed at the reference value
- various other modes used during en route navigation and instrument approaches.
The active upper mode(s) were displayed to the pilot on the primary flight display (PFD) by a green upper axis mode label and illumination of the corresponding push-button on the APMS panel.
Another mode, go-around (GA), could be selected on the collective grip. Depending on the software version, this acquired and maintained an airspeed of 75 kt or acquired and held a vertical speed of 1,000 ft/min. In VH-ZGA the installed software had a vertical speed target parameter.
When operating in upper modes other than IAS, the minimum height limit was specified as 500 ft above ground level (AGL). If an upper mode was engaged and airspeed reduced below 60 kt, all upper modes of the AFCS were inhibited except IAS mode (minimum airspeed 40 kt). When this occurred, an amber DECOUPLE caution illuminated on the cockpit cautions and advisories display (CAD) and the label on the PFD was replaced by a flashing green box for 10 seconds before extinguishing. There was no audible warning to indicate decoupling of upper modes.
For complete disengagement of the SAS and AFCS, the pilot could select the SAS/AP CUT switch on the cyclic grip. To re-engage SAS and pitch damper functions, the pilot could manipulate the 4-way P&R/P-D/YRST switch on the cyclic grip. If the pilot wanted to cancel all upper modes, actuation of the APMD DCPL switch on the cyclic grip resulted in reversion to A.TRIM mode.
Instrument panel configuration
One of the features of the single-pilot IFR STC was modification of the instrument panel to extend the panel to the right of the helicopter with variation to type and location of avionics and instrumentation. The panel of VH-ZGA is shown in Figure 7 and for comparison an exemplar of the standard instrument panel fitted to the operator’s other EC135 helicopters is shown in Figure 8. Note: although the avionics and instrument layout for the 2 Port Hedland-based EC135 helicopters was similar, the panel in VH-ZGA retained panel area to the left of the centre console and the panel in VH-ZGZ was truncated to the left of the centre console.
In both non-standard instrument panels, the PFD and navigation display (ND) were both offset to the right (relative to the standard location) by the width of the displays. A further variation was installation of an integrated standby attitude module in place of the set of analogue standby instruments in the standard configuration.
Figure 7: Single-pilot IFR instrument panel fitted to VH-ZGA

Source: Helicopter operator
Figure 8: Operator’s EC135 standard instrument panel

Source: Reproduced with permission
Primary flight display
The PFD and ND fitted to each of the Port Hedland-based EC135s were SMD 45H multifunction colour displays designed for helicopters. These units were described as a high resolution, 4 x 5 inches (102 x 127 mm), active-matrix liquid crystal display. Brightness of the display was pilot adjustable. A typical display layout is shown at Figure 9.
As shown below, all of the critical flight information was presented on the PFD with conventional representation of attitude and digital representations of airspeed and altitude as scrolling vertical tapes. Other information such as AFCS mode and navigational data was usually presented with cautions/warnings related to non-normal equipment status.
An airspeed trend indicator aligned with the airspeed value predicted in 5 seconds. Vertical speed was indicated by the position of a white bar relative to an analogue scale and an associated numerical value to indicate the vertical rate in hundreds of feet. Above 2,000 ft/min in either climb or descent, the white bar was at full-scale deflection and did not provide an accurate analogue indication. In that circumstance and with the white bar at full-scale deflection, the numerical value correctly indicated the vertical rate.
Radio altimeter height information was depicted relative to ground/water level on the altitude tape, by a brown coloured terrain symbol (radio height zero). Radio height was displayed as a digital readout on the lower part of the attitude ball when within 500 ft of the surface. Above 500 ft of the surface, the radio height was also displayed within 500 ft of the selected decision height. The radio height was also displayed as a tape style readout on the right side of the ND. Magnetic heading was shown at the bottom of the PFD on a linear scale, which represented the arc of a circle.
Figure 9: Typical SMD 45H configured as primary flight display

Typical depiction of flight parameters on a SMD 45H configured as primary flight display. The information displayed indicates the helicopter is in a slight nose-up pitch attitude, descending through an altitude of 6,900 ft at 300 ft/min and an airspeed of 129 kt. The green symbols at the top of the display indicate that the AFCS IAS and HDG upper modes are active. The radio altimeter decision height has been set to 300 ft. The decision height flag is displayed on the on the attitude ball, with the radio height (220 ft) displayed below. The level of terrain relative to the helicopter’s current altitude is depicted on the altimeter scale.
Source: Eurocopter EC135 training manual, modified by the ATSB
A range of guidance material for the design and certification of aircraft states that key flight parameters (such as attitude, altitude and airspeed) should be placed within a pilot’s primary field of view, which is normally defined as being within 15° horizontally each side of straight ahead. This area corresponds to the highest visual acuity and can be searched with minimal or no head movement, and information placed outside of the primary field of view may not be detected as quickly (Yeh and others 2016).
Aircraft certification requirements for normal category rotorcraft stated that each flight and navigation instrument must be ‘easily visible’ to the pilot. Accordingly, the Federal Aviation Administration (FAA) Advisory Circular 27-1B (Certification of normal category rotorcraft) have recently defined this as meaning that high priority information and primary flight information should be displayed in the primary field of view (defined as 15° each side of straight ahead).[28]
The PFD’s location on VH-ZGA was in the primary field of view for a right-seat pilot and was located at about 57° to the right of straight ahead for a left-seat pilot. The PFD was located about 800 mm away from a right-seat pilot and about 1,120 mm away from a left-seat pilot.
A range of factors can affect the readability of alphanumeric characters, including their size. Various sources recommend a minimum height of 24 minutes of visual angle for aircraft environmental conditions (Yeh and others 2016). This equated to a minimum height on a right-side PFD of about 5.6 mm for a right-seat pilot and 7.8 mm for a left-seat pilot. The size of the numerals on the altitude display were about 8 x 4 mm for the major numbers (to indicate the thousands of feet) and 6 x 3 mm for the minor numbers (to indicate the hundreds of feet). When viewed from a significant angle, the width of the numerals would also appear smaller. Significantly, when operating below 1,000 ft, the major number displayed zero and the minor number indicated the helicopter’s altitude, in hundreds of feet. Consequently, for a pilot sitting in the left seat and using the PFD on the right side of the cockpit, the altitude indication when operating below 1,000 ft was smaller than the minimum size commonly recommended for readability.
During the initial interview with the ATSB a few days after the accident, the instructor said the standby flight instruments in VH-ZGA were small, and the primary flight instruments were the best for flying. The instructor said that the primary instruments were clearly visible from the left seat, but there was an increase in workload associated with looking outside, looking inside, and looking across the cockpit. In that context, the instructor preferred to have their own set of primary flight instuments. When interviewed again in early 2020, the instructor advised of difficulty viewing vertical speed information, including at night over water while trying to transition to a missed approach. To the instructor, this was because the vertical speed indicator was at the far side of the right-seat pilot’s PFD.
The ATSB spoke to other EC135 pilots who had experience flying from the left seat, but in helicopters equipped with a single set of primary flight instruments. The chief pilot from the time of the accident said that a pilot in the left seat had a good view of the primary flight instruments to preform the task of monitoring the helicopter’s flight path, but that in an emergency recovery situation, it would be difficult not having your own instruments to use. The head of training and checking appointed to the operator after the accident said that you could not read the displayed information (such as airspeed, rate of descent and altitude) as clearly with the primary flight instruments across the other side of the cockpit. The operator no longer conducted training and checking in helicopters that were not equipped with primary flight instruments at the instructor’s seating position. Other EC135 pilots with experience flying from the left seat considered that for night operations, and at other times when operating in degraded visual environments, it was important to have primary flight instruments at the instructor’s seating position.
Standby attitude module
The 2 helicopters based at Port Hedland were each equipped with a MD302 standby attitude module mounted in a central location relative to both pilots. The 2-inch (51 mm) format digital displays (Figure 10) presented an attitude indicator with heading numerals and an adjacent set of scrolling tape indicators with windows for airspeed and altitude data. This module was installed to satisfy the night VFR and IFR requirement for a backup set of flight instruments. Note: the arrangement of the instrument display screens in VH-ZGA and VH-ZGZ were transposed, with the attitude indicator displayed on the right screen and the airspeed and altimeter on the left screen.
Figure 10: MD302 standby attitude module

Source: Mid-Continent Instruments and Avionics Pilot’s Guide MD302 Standby Attitude Module
On the right edge of the module, rate of climb/descent was represented by a magenta altitude trend bar adjacent to the moving altitude scale. The trend bar was anchored to the central fixed altitude pointer and expanded up if climbing (as per example) or down if descending, by an amount proportional to the rate of vertical change. At the upper or lower end of the bar, respectively, the adjacent increment/figure was the projected altitude if the current vertical trend was maintained for a 6-second period.
For 500 ft/min rate of descent, the trend bar would expand downward to indicate 50 ft less than the indicated altitude, which was equivalent to 25% of the lower-half scale. Those parameters would double for 1,000 ft/min. In this occurrence, when VH-ZGA was passing 300 ft with a descent rate of 1,700 ft/min, the trend bar would have extended down by 170 ft (85% of the lower-half scale) to be adjacent to 130 ft.
The standby attitude module was located about 840 mm from a left-seat pilot, about 38° to the right of straight ahead. The instructor reported difficulty viewing the vertical speed information, describing the standby vertical speed information as tiny and badly lit.
Standard standby instrumentation
The standby instruments installed in the operator’s standard EC135 helicopters were an airspeed indicator, attitude indicator, and altimeter (Figure 11). These were conventional analogue instruments classified as 3 1/8 inch (80 mm). Note there was no vertical speed indicator (VSI).
Figure 11: Typical EC135 standby instrument configuration

Source: Helicopter operator
Central panel display system
The central panel display system (CPDS) comprised a vehicle and engine multifunction display (VEMD) and CAD. On the upper screen of the VEMD, the first limit indicator (FLI) page was normally selected to display key engine parameters digitally and represent the limiting parameter as an analogue pointer (Figure 12). Other data such as mast moment[29] and messages was also presented.
Operationally, the FLI provided an easily interpreted scale and guide for engine/torque settings.
Figure 12: Typical first limit indicator page

Typical depiction of the helicopter’s FLI page on the CPDS, extracted from the helicopter manufacturer’s EC135 P2+ flight manual. In this example, the digital readout indicates that the left and right engines are producing 78% torque and the adjacent solid white rectangles denote that these are the first-reached limits being displayed by the analogue FLI needles. Although the small split in needle indication illustrates the existence of 2 needles (indicating the torque produced by each engine), the position of the needle for the right engine is not representative of the torque indicated by the corresponding digital readout. For a normal-indicating situation where both engines were producing 78% torque, the 2 needles would both be aligned and pointing to the index mark at 10 and the corresponding red line radial denoting the 5-minute, 2 engine take-off power limit. Operation of the engines within in the yellow arc was limited to 5 minutes. A countdown timer on the face of the FLI indicated the time remaining at the relevant limit. The bottom of the yellow arc (index mark 9) denotes the 2-engine maximum continuous power (69% torque).
Source: Eurocopter EC135 P2+ flight manual
Internal lighting
Instrument lighting
The helicopter was equipped with instrument lighting for night operation. A 3-position switch on the overhead console panel controlled the lighting with selections for DAY, NIGHT and NVG [night vision goggle], together with an adjacent dimmer rheostat control. When selected to NVG, the lighting was modified to minimise the amount of NVG-sensitive illumination (such as near infrared) for optimum imaging in low-light environments.
After recovery of the wreckage to Port Hedland, the overhead console switch for instrument lighting was found in the NVG position and the dimming rheostat set close to fully dimmed. Although the instrument lighting selector was set to the NVG position, there was no evidence that the visible light range of the instrument lighting was insufficient for unaided night operations.
The SMD 45H primary flight display, VEMD, and CAD displays were fitted with brightness dimmer controls. All of these displays were compatible for use with NVIS.
Helicopter emergency egress lights
The helicopter was not fitted with helicopter emergency egress lights (HEEL). Although the cockpit overhead switch panel was fitted with a switch position and markings for that system, there was no switch installed at that location. There was no regulatory requirement for provision of emergency exit egress lighting.
When installed, the HEEL system was designed to automatically activate and assist occupants in an emergency to locate the door opening/jettison handles and exits, using illuminated markings and lighting for the emergency exits and operating handles. Green strip lights surrounded the doors used as emergency exits, green strip lights at the corners of the emergency exit windows and orange lights near the door opening/jettison handles.
Although there was no HEEL system installed, each exit and the relevant operating handles displayed the required placards and markings.
External Lighting
Controllable search/landing light
A steerable search/landing light was installed on the helicopter’s lower front fuselage and retracted flush with the fuselage when not in use. Switches on each collective control enabled either pilot to select the light ON/OFF and control the direction of the beam.
After recovery of the wreckage to Port Hedland, the right search/landing switch was found in the ON position and the left in the OFF position. Pilots conducting MPT operations reported that the controllable searchlight was effective during the later stages of final approach and was used to illuminate the landing area/hatch.
Nose-mounted traffic identification light
The helicopter was fitted with a nose-mounted traffic identification light that could be selected to ON (steady illumination) or PULSE (flashing illumination). This light was controlled by a switch on the overhead panel. After recovery of the wreckage to Port Hedland, the selector switch was found in the OFF position.
Position lights, anti-collision light and strobe lights
The helicopter was equipped with position, anti-collision and strobe lights. The position lights were steady red, green and white lights. The white light was mounted on the tail of the helicopter, the red light was mounted on the left horizontal stabiliser and the green light mounted on the right horizontal stabiliser. The anti-collision light was a flashing red light on the tip of the helicopter’s tail and the strobes were flashing white lights on the tip of each horizontal stabiliser.
After recovery of the wreckage to Port Hedland, the position and anti-collision lights were found in the ON position and the strobes were OFF. That configuration was consistent with a night VFR operation when operating close to reflective surfaces, to reduce potential disorientation.
Although the marine pilot who witnessed the accident advised that the water impact was partially illuminated by a strobe light, the as‑found position of the steerable search/landing light and strobe switches could indicate the light flash at impact was water being illuminated by the downward-pointing search/landing light.
Communication
The instructor and pilot under supervision were both wearing flight helmets, equipped with a boom microphone and headphones. The pilots and any passengers wearing a headset could communicate with each other using an intercom system. The intercom system could be either voice or push-button activated, with the mode selected on each audio controller panel located in the centre console between the seats.
The communication jack on the left (instructor) side of the cockpit was fitted with a quick-release, short-length break-away connector. Although that connector was still plugged into to the cockpit jack following the helicopter’s recovery from the water, the instructor’s flight helmet had been recovered from the search area the morning after the accident.
After recovery of the helicopter to Port Hedland, the ATSB noted the switch positions on the audio controller panels. Both intercom selectors were found selected to voice activation and the instructor’s audio switch was selected to NORMAL. However, the pilot under supervision’s audio switch was selected to ISO/EMERG.
Each audio switch was toggled between the 2 positions with a simple forward/rearward movement. Given the location of the panel and the switch being unguarded, the ATSB considered that the switch could have been unintentionally moved during the accident sequence or prior to recovery. However, there was no damage to the audio controller panel and no significant variations between the other switches on each respective panel to indicate that this had occurred.
If the audio switch had been selected to ISO/EMERG during the flight, from that point onwards there would have been no intercom communication between the instructor and pilot under supervision. The instructor did not advise of any communication difficulties; so, in this scenario, the instructor might have issued instructions to the pilot under supervision that were not heard or complied with.
Helicopter manufacturer’s operating procedures
The helicopter manufacturer’s aircraft flight manual (AFM) for the EC135 specified operational limitations and checks to ensure that systems were properly configured for normal flight and a selection of emergency and malfunction conditions.
The AFM specified pre-landing checks of instruments, warnings, and cabin security and recommended landing procedure from 50 ft AGL. No procedures were provided for circling approaches or night operations, and none were required by regulation.
Simulator training provided by Airbus Helicopters to the instructor was oriented to general operation of the EC135 and the management of emergencies.
Meteorological and environmental conditions
Meteorological information
The Bureau of Meteorology (BoM) reported light, variable winds, generally below 10 kt (19 km/h) during the day and night of the accident. There was little to no cloud present and no rain.
The port operator’s meteorological equipment and hydrographic sensors recorded that the surface wind conditions in the vicinity of the pilot boarding ground (PBG) and the C2 channel marker, were generally westerly flows, with the wind strength increasing slightly as the evening progressed. The maximum wind gust recorded during each of the 10-minute intervals was less than 3 kt (6 km/h) above the average wind for the period. The BoM grid point wind and temperature (GPWT) forecast for 2300 predicted similar wind speeds at the 1,000 ft and 2,000 ft levels, with a minor change in wind direction. The GPWT wind direction and speed forecast for 1,000 ft, were generally consistent with the 10-minute average winds recorded at the channel markers (Table 8).
Table 8: Average recorded wind velocity and GPWT forecast
|
Time (WST) |
10-minute average W/V recorded near PBG (deg True/kt) |
10-minute average W/V recorded at C2 (deg True/kt) |
2300 WST GPWT forecast wind, 1,000 ft (deg True/kt) |
2300 WST GPWT forecast wind, 2,000 ft (deg True/kt) |
|
2300 |
245/08 |
251/08 |
270/08 |
300/06 |
|
2310 |
246/08 |
247/08 |
- |
- |
|
2320 |
243/09 |
250/10 |
- |
- |
|
2330 |
194/10 |
256/10 |
- |
- |
|
2340 |
237/12 |
255/10 |
- |
- |
|
2350 |
230/12 |
253/11 |
- |
- |
Data from a Waverider buoy in the vicinity of C2 around the time of the accident indicated a swell wave height of 0.29 m at 10 second intervals and a sea wave height of 0.19 m at 8.3 second intervals.[30] The combined result of swell and sea height would have produced total wave heights of less than 0.4 m. The sea temperature was 30.6 °C.
Hydrographic data from the port authority’s equipment at C2 recorded a near surface current of 0.2 kt (370 m/hr) running in a north-north-westerly direction.
Sunset and moon information
Sunset at Port Hedland on 14 March 2018 was 1822 and the end of civil twilight[31] (last light) was 1845. Civil nautical twilight[32] was 1910 and astronomical twilight[33]1936. The moon was a waning crescent, rising at Port Hedland at 0356 on 15 March, with about 0.14% of the visible disk illuminated. As a result, dark night conditions existed after civil nautical twilight for all flights away from sources of artificial lighting.
Artificial/cultural lighting
In the vicinity of Port Hedland there were significant areas of flood lighting associated with ground infrastructure, which included industrial facilities, port infrastructure and lighting associated with suburban areas. During offshore operations, this lighting would have been in the distance, to the south of the pilot boarding ground and to the south-south-east of the C1/C2 channel markers.
Overall, the location of the C1 and C2 channel markers, about 21 NM (39 km) north-west of Port Hedland, meant there was very little environmental lighting in the vicinity. Pilots who were experienced in MPT operations from Port Hedland said C1/C2 was very dark at night.
Vessels at anchor
At the time of the accident, there were 17 vessels anchored at the eastern anchorage, awaiting access to the port. At night, those vessels were illuminated by their deck flood lighting. The anchorage was just over half-way between the C1/C2 channel markers and Port Hedland. Figure 13 depicts the relationship between the flight path of VH-ZGA, vessels at anchor and another vessel underway (Ormond) at the time of the accident.
The instructor told the ATSB that the visual environment made the approach to vessels at C1/C2 very challenging, and the channel marker lights did not assist with navigation. The instructor said that, other than lights on the target ship (Squireship), there were no visual references and the ship effectively appeared as a single light source.[34]
Following the go-around, the instructor may not have been able to sight the target ship for brief periods, due to the location of the other pilot and window posts.
Figure 13: ADS-B flight path for VH-ZGA, including relative position of Port Hedland, vessels at anchor and vessels underway at the time of the accident.
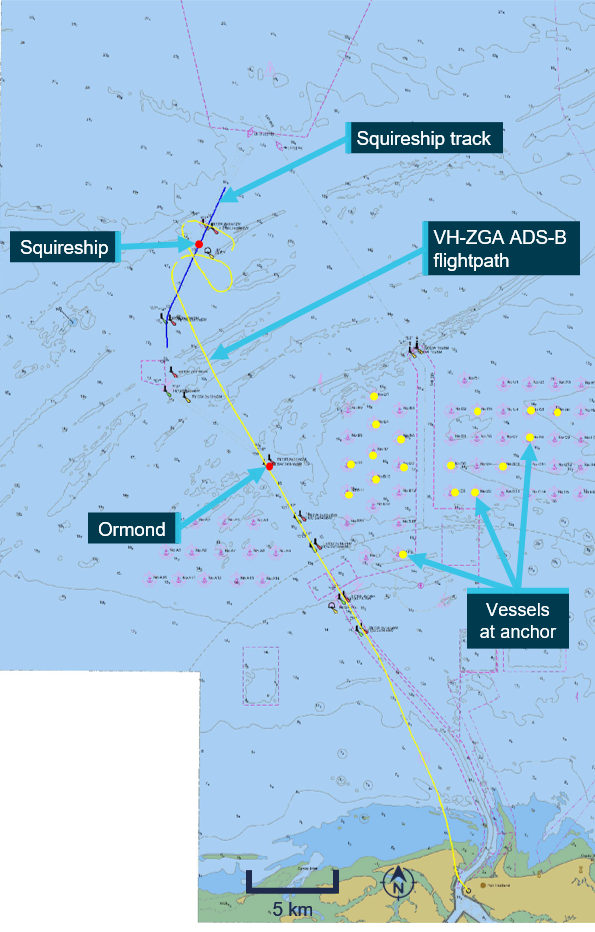
This image shows the helicopter flight path during the accident flight and the surface track of the departing bulk carrier in vicinity of C1/C2. Also shown is the position of the bulk carrier, Ormond underway along the shipping channel at the time of the accident, together with the vessels at anchor.
Source: Port Hedland electronic navigational chart produced by The Australian Hydrographic Office, modified by the ATSB
Wreckage recovery and examination
Wreckage disposition
The helicopter was found on the seabed, on the right side of its fuselage in about 20 m of water (Figure 14). Video recorded by police divers showed all doors in the closed position. Almost all the left main cockpit windscreen was missing, with some perspex remaining in the lower section behind the instrument panel and around the sides of the frame. The left chin window had also broken. The right main cockpit windscreen and right chin window were intact.
Figure 14: Sonar image of helicopter resting on its right side

Source: Pilbara Ports Authority and contractors working on their behalf
The left cockpit door (adjacent to the instructor) was visible in the initial police dive footage (Figure 15). The door’s operating handle was in the closed position and the latch pins were holding the rear edge of the door flush with the fuselage. The front of the door was slightly ajar from the door frame and the 2 hinge pins had been retracted, consistent with the position of the door’s emergency jettison handle that appeared to be in the DOWN position.
The right cockpit door (adjacent to the pilot under supervision) was not visible in the initial police dive footage because of the disposition of the helicopter on the seabed. After the first attempt to lift the helicopter, the orientation of the helicopter changed, and subsequent dive footage showed the door was securely attached with the door operating handle in the closed position.
Figure 15: Image of instructor’s cockpit door captured from police dive video, showing deployment of the door’s emergency jettison system and a partial door release

This image shows the helicopter as found on the seabed, on the right side of its fuselage. The instructor’s cockpit door (left) is shown with the forward hinge pins retracted and the door’s front edge slightly ajar from the fuselage. The door operating handle used for normal door operation is still in the closed position and the latching mechanism is holding the rear edge of the door closed.
Source: Western Australia Police Force dive video, annotated by the ATSB
Wreckage recovery
The Pilbara Ports Authority and their contractors recovered the helicopter wreckage from the seabed during 18 and 19 March 2018 (Figure 16). The wreckage was moved into secure storage where it was examined by the ATSB.
Figure 16: VH-ZGA being lifted onto the dock

Source: ATSB
Wreckage examination
The helicopter was substantially intact, although the main rotor head and transmission gearbox separated from the airframe during the recovery.
Three of the main rotor blades sustained significant damage near their blade roots during water impact and one of the main rotor blades had struck the upper surface of the helicopter tail boom. The flexible coupling of the main gearbox drive output shaft had sheared. The Fenestron blades exhibited evidence of rotational damage.
A review of police dive footage indicated that the main rotor transmission deck was damaged during the initial water impact, with the main gearbox and main rotor assembly tilting in a forward‑of‑centre position and tearing through the surrounding cowling panels. The disrupted transmission deck structure was most probably the result of reactive forces during the water impact of a powered main rotor system. Additional damage to the helicopter transmission deck, gearbox and rotor assembly and associated systems was sustained during the wreckage recovery.
Figure 17: Main rotor blades and main transmission, showing damage in vicinity of the blade roots

Source: ATSB
Damage to the engine compressors and associated housings indicated that both engines were rotating at impact. To the extent possible, due to the nature of the accident damage and wreckage recovery, continuity of the flight controls was established.
The left cockpit door (adjacent to the instructor) detached from the fuselage during the recovery operation and was not located. It was confirmed that the emergency door jettison handle was in the DOWN (release) position and the safety wire to the instructor’s handle was broken.
The right cockpit door (adjacent to pilot under supervision) had been opened during the recovery operation, indicating that there was no defect with the latching mechanism. It was confirmed that the door’s hinge pins were engaged, and the emergency door jettison handle was in the UP (secured) position with intact safety wire.[35]The emergency jettison for that door was functionally tested and found to operate normally.
The helicopter’s emergency flotation system had not deployed. Examination of the panel-mounted cockpit arming switch was consistent with the switch being in the armed position. The immersion switch for the automatic inflation system was functionally tested and found to operate normally. The immersion switch required to be submerged in water for several seconds before the circuit closed to enable the automatic deployment of the flotation system. Electrical continuity was demonstrated between the circuit breaker panel, the immersion switch and the linear actuator. Inspection of the actuator indicated that neither an automatic nor manual inflation had been initiated. The linear actuator was functionally tested and found to be capable of normal operation.
Electronic component examination
The ATSB recovered various electronic components from the helicopter engines and airframe to assess the data stored in their non-volatile memory. This data included information about system conditions and faults, typically used for maintenance and troubleshooting purposes. The units recovered included the:
- electronic engine control (EEC) for each engine
- data collection unit (DCU) for each engine
- cockpit warning unit (WU)
- cautions and advisories display (CAD)
- vehicle and engine multifunction display (VEMD).
ATSB investigators removed the required logic boards from the WU, CAD and VEMD at the ATSB technical facilities. Arrangements were then made for the French Bureau d’Enquêtes et d’Analyses (BEA) to complete the specialised cleaning and drying of components, prior to attempting the data recovery on behalf of ATSB.
The logic boards for the WU,[36] CAD[37] and VEMD[38] were dispatched from Canberra on 29 May 2018 as an international air freight consignment but were lost in transit. Extensive checking and investigation by the freight provider to locate the tracked consignment was unsuccessful. Consequently, any information stored on these components could not be retrieved for analysis.
The DCU and EEC for each engine were shipped to the Transport Safety Board (TSB) of Canada on 28 March 2018 to enable specialised desalination, cleaning and drying of components in preparation for the data download attempt. The data recovery task was successful, and data was obtained from each of the components.
Analysis of the data stored in the DCU indicated that both engines were coupled to the main transmission and operating when the DCU recordings were made. The recordings were associated with events occurring to the helicopter engines as a consequence of the water impact. The recorded values for some parameters may have been affected by structural integrity or system degradation due to the impact forces. The speed of the main rotor was not a parameter provided to the DCU.
The first event recorded to the left engine’s DCU was because of the engine control governing on the maximum fuel flow rate. At this time, the left engine torque was at 61.4% and the ‘cross-talk’ torque for the right engine was 48.9%. The split between the torque recorded for the left and right engines can be attributed to the variability in the events happening to the engines, the main rotor, and the engine to transmission connections. At the time of that recording, the power turbine was rotating at 99.1%, the gas generator at 81.6%, measured gas temperature 615.3 °C and the collective lever raised to 33.8°.[39]
The first event recorded to the right engine’s DCU was a consequence of the engine control governing on the minimum fuel flow rate. At that time, the right engine torque was at 38.2% and the ‘cross-talk’ torque for the left engine was 43.7%. At the time of that recording, the power turbine was rotating at 93.1%, the gas generator at 81.7%, measured gas temperature 605.8 °C and the collective lever at 82.6°.
Relevant engine limitations specified in the AFM indicated that for 2 engine operation, take-off power was 78% torque each engine, for a limit of 5 minutes and maximum continuous power 69% torque each engine. The maximum speed for the gas generator was 98.7% for take-off power and 97.4% maximum continuous maximum power. The relevant limit for the power turbine outlet temperature was 869 °C and 835 °C respectively.
Those limits would be indicated on the first limit indicator (see the section titled Central panel display system) as ‘10’ for the 5-minute take-off power setting and ‘9’ for maximum continuous power.
Although the data stored in the DCU indicated engine power significant to demonstrate the operation of both engines, that data did not represent a power setting consistent with a go-around or emergency application of power.
Operator organisational information
Operator history
In 2016, the helicopter operator successfully tendered to provide helicopter services for the transfer of marine pilots at Port Hedland, Western Australia. The contract required provision of helicopters and pilots commencing 1 April 2017. For the contracted services, the operator based 2 EC135 P2+ helicopters at Port Hedland and 8 helicopter pilots, who operated on a rotating 3‑week fly-in/fly-out touring roster.
The initial staffing for the Port Hedland contract comprised 4 pilots recruited from the outgoing helicopter contractor, 3 pilots transferred from the operator’s other bases and a recently re‑recruited pilot. The previous contractor had conducted MPT operations using single‑engine EC120 helicopters. As part of their induction at the new company, the 4 pilots from the previous contractor were provided ground school training and an endorsement to operate the EC135.[40]
Air Operator’s Certificate
At the time of the accident, the operator held an air operator’s certificate (AOC) issued by the Civil Aviation Safety Authority on 18 December 2017 and due to expire on 31 August 2019. This certificate authorised airwork and charter operations utilising a variety of helicopters including the EC135 type and flying training in accordance with CASR Part 142 for EC135 type ratings. An approval certificate issued in accordance with CASR Part 141 allowed for flight training for various licences and ratings.
Chief pilot information
As the holder of an AOC authorising aerial work and charter, the operator was required to appoint a chief pilot subject to approval by CASA. The chief pilot at the time of the occurrence had been in that role since nomination and approval in 2013.
At the time of nomination, the chief pilot held an air transport pilot licence (helicopter) and multi‑engine helicopter instrument rating. Total helicopter flying experience was recorded as 3,957 hours including 1,832 hours multi-engine and 1,365 hours multi-crew. Total night experience was recorded as 1,072 hours and total instrument flight as 440 hours. The chief pilot did not have any flight instructing qualifications or experience and this was not a requirement.
The assigned CASA inspector completed the internal checklist for approval of a chief pilot. This recorded that the desktop assessment, interview, and briefing were conducted with a satisfactory result. As part of the interview process, the CASA inspector assessed knowledge of applicable regulations and observed a MPT flight.
The ATSB noted that as part of the CASA assessment, the chief pilot was requested to outline the induction process for a new pilot including the type of proficiency check conducted prior to releasing a new pilot to line operations. There was no requirement for an assessment of the chief pilot’s capability to conduct a proficiency check or flight training and none was conducted during the approval process.
Safety management system
At the time of the occurrence, charter operators were not required to have a formalised safety management system (SMS). In this case the operator had voluntarily implemented a SMS, so the ATSB carried out a limited-scope review for context.
The operator issued version 5 of their SMS manual in November 2017. This outlined the safety function and defined the policy, activities, and assessments that were aimed at proactive and reactive management of risk. A group safety manager was employed to maintain the system with support from base safety officers and the participation of all company personnel. Reporting and recording could be done through operational management software.
According to the SMS manual, the operator intended to identify areas of vulnerability to human performance limitations and address these with non-technical skills training. This included external computer-based courses: controlled flight into terrain/approach-and-landing accident reduction, crew resource management, and human factors for helicopter flight crews and internal training on fatigue risk management.
Overall, the SMS records showed that safety meetings were taking place regularly and matters were being reported and generally addressed. Development of fatigue risk management and fatigue concerns were a consistent theme. Safety investigations had been conducted in response to damage from heliporter[41] use (initially undetected) and in‑flight detachment of an engine cowling.
A hazard and risk register was maintained to record the risk of a number of potential events before and after mitigation were assessed. This addressed flight operations and other aspects of the operation such as engineering and work health and safety. As a ‘living’ electronic document, a version history was not recorded.
The SMS specified annual safety surveys,[42] which were completed in February 2015, January 2017, and January 2018. As the survey methodology changed after 2015, only the results of the 2 later surveys were considered. There were 16 respondents in 2017 and 35 in 2018 but the number of potential respondents for each survey was not recorded.
Both surveys comprised questions that addressed the operator’s management of safety and effectiveness of safety reporting. The responses in both surveys were consistently positive for all of the questions except for the question about confidence that staff would report events and actions with potential for damage or injury/death. In 2017, all of respondents recorded ‘Yes’ but in 2018, 66 % of the respondents recorded ‘Yes’ and 34 % recorded ‘No’. Some of the ‘No’ responses were associated with the heliporter damage incident that was initially unreported.
There were no records kept of the following activities specified in the SMS manual or referenced in safety meetings:
- flight operations audit
- risk assessment for helicopter operations (recorded as ongoing)
- data trend analysis.
The operator maintained a change log with reference to various plans for the transition into the Port Hedland operation by April 2017. In relation to MPT, there was nothing to indicate that night VFR operation in a degraded visual cueing environment (see the section titled Flightpath management) or the offshore environment was recorded as a specific threat and subject to formal risk assessment and mitigation. There was also no recorded risk assessment as to the suitability of the single-pilot IFR helicopters (VH-ZGA and VH-ZGZ) for night VFR training and checking at Port Hedland.
External audits
In May 2017, an aviation consulting organisation conducted an operational and technical safety audit of the operator’s Port Hedland base on behalf of a mineral resource company. Audit scope included organisational, operational, and engineering elements defined by the resource company. No major non-conformances were reported by the auditors.
For flights at night and/or under the IFR that carried resource company personnel, it was recommended that the operator conduct the flights with 2 pilots or request a dispensation from the company. Given the helicopters based at Port Hedland were not equipped with weather radar, it was recommended that the operator seek a dispensation. The ATSB noted that the recommendation for 2 pilots for flights at night and/or under the IFR in helicopters was based on the resource company requirement for a safety pilot rather than for a 2-pilot operation.
In June 2018 (3 months after the occurrence), the operator contracted an aviation consulting company to carry out an audit in accordance with the basic aviation risk standard (BARS)[42] offshore helicopter operations safety performance requirements. This was the inaugural BARS offshore audit for the operator and was conducted at Mackay Airport. Further information related to the BARS audit is provided in the section titled Non-regulatory guidance – Flight Safety Foundation.
The BARS audit did not identify any Priority-1 safety critical findings, although a number of Priority-2 findings were reported. One of those findings related to an inappropriate policy for use of automation and another related to absence of a mandatory go‑around requirement for unstabilised approaches. Another finding related to the absence of a documented procedure for radio altimeter alerts.
Surveillance audits carried out by CASA are detailed in a following section.
Operations manual guidance
Regulatory guidance for operations manuals
The Civil Aviation Safety Authority was empowered to provide directions as to operations manual content and provided guidance to industry in the form of civil aviation advisory publication (CAAP) 215-1, as revised. Operators were required to ensure that operations manuals contained the necessary information, procedures, and instructions for safe conduct of operations. This included provision of standard operating procedures (SOPs) and a framework for training and checking.
For each section of a manual, CASA set out a typical structure with headings to be addressed by the operator and explanations of the required information. Under the sub-heading of VFR flight at night, CASA noted that in conditions of no visual horizon or insufficient visual cues (ground lighting), aircraft should be equipped for instrument flight and flown by an IFR-qualified pilot.
In the approach and landing section, operators were advised to provide general approach and landing precautions, including stabilised approach criteria. Operators were then advised to set out the company policy and procedures relating to joining and flying in the circuit, airspeed and altitude limitations and operations with strong crosswinds.
Marine pilot transfer was listed as a special operation that required procedures and specifications in accordance with CAO 95.7.3. This was an exemption to allow single-engine helicopters to be engaged in charter at night for the purpose of transferring marine pilots, subject to equipment, crewing, and training conditions.
Guidance relating to training and checking was referenced to Civil Aviation Regulation (CAR) 217 and CASR Part 61 (for flying schools). Operators were required to describe the selection, recent experience and completion standards for training and checking personnel.
Regulator guidance and recommended practices for night VFR operations
As part of the transition to CASR Part 61 flight crew licencing, CASA published an advisory circular to provide advice and guidance to illustrate a means, but not necessarily the only means, of complying with the regulations related to the night VFR rating. The ATSB identified the following extracts that were relevant to this occurrence:
Night visual flight rules (NVFR)
CASA strongly recommends that NVFR operations take place only in conditions that allow the pilot to discern a natural visual horizon or where the external environment has sufficient cues for the pilot to continually determine the pitch and roll attitude of the aircraft.
Even if visual reference is available at night, it can often be misleading and can further disorient a pilot attempting to fly visually. Integrating visual and basic instrument flying is essential when flying at night under VFR.
Aeronautical and underpinning knowledge - Instrument flying
Night operations require proficiency in instrument flight (IF).
Instrument flying skills are intrinsic to night flying; therefore, it is also desirable that IF proficiency be demonstrated before commencing actual night flying.
Hazards and risks
The ability to discern objects and terrain, together with their availability, is referred to as the ‘visual cueing environment’ and is related to the amount of natural and manmade lighting available, and the contrast, reflectivity, and texture of surface terrain and obstruction features.
A degraded visual cueing environment exists when high visual cueing conditions are not present (i.e. in conditions where the ability to discern objects and terrain is compromised).
Operations in a degraded visual cueing environment result in a perceived degradation in the effective rotorcraft handling qualities. The degraded handling qualities result in a substantial increase in pilot workload just to control the rotorcraft, leaving little excess workload capacity to maintain adequate situational awareness. This workload can easily exceed 100 percent of the pilot’s capacity, a situation which significantly increases the probability of a serious error.
In order to conduct operations safely and legally at night in a rotorcraft, the visual cueing environment must be accounted for in the planning and execution of NVFR rotorcraft operations.
The primary defence against sensory illusions during instrument flight in an aeroplane is to ignore the physical sensations and to maintain orientation by reference to the flight instruments. Attempting to use external visual reference at night can cause further confusion. Correct instrument scanning technique uses the flight attitude indicator (i.e. artificial horizon) in place of the natural horizon as the primary source of attitude information. Performance instruments, air-speed indicator (ASI), altimeter (ALT) indicator and vertical speed indicator (VSI) are used to confirm that the attitude being maintained is providing the desired aircraft performance.
Controlled flight into terrain is the result of a loss of situational awareness and is a significant problem worldwide both in NVFR and IFR operations. The common factor in this type of accident is that, due to the pilot's lack of awareness of either the horizontal or the vertical position of the aircraft, it is flown into the ground or water under full control.
The advisory circular also addressed threat and error management (TEM), risk management, human fatigue, situational awareness, task management, and decision-making.
Non-regulatory guidance – Flight Safety Foundation
Introduction
The Flight Safety Foundation produced BARS documents that specified a framework of safety performance goals necessary to assure safe offshore helicopter operations. This framework supplemented national and international regulations and was applied to contract specifications. The following standards have been extracted from the documents issued in May 2021, and slightly edited.
This information has been included to present industry best practice at the time of writing the investigation report for comparative analysis and safety education purposes.
Competency
To ensure safety critical personnel are competent to fulfill their duties by having appropriate training, qualifications, knowledge, skill and experience:
The aircraft operator must have an appropriate procedure for the initial selection of flight crew that considers aptitude and compatibility.
Where agreed by the company, the aircraft operator may use Competency Based Training in lieu of minimum experience requirements if the training program has been evaluated and meets the requirements of Flight Safety Foundation Offshore Safety Performance Requirements Flight Crew Competency Based Training Framework.
Flight crew must receive annual training to the standards of the responsible regulatory authority with two flight checks annually (or every six months for long term contracted operations). The flight checks must include an annual instrument rating renewal (where applicable), proficiency or base check (non-revenue) and a route check (revenue-flight permissible).
Flight crew members are to conduct training in suitable Flight Simulation Training Devices (FSTD) every 6 months.
Before commencing flight duties in a new location on long-term contract, all flight crew must receive a documented line check that includes orientation of local procedures and environment when these differ from their previous operating location.
Check and training procedures should include the syllabuses and procedures for initial training and approval and the processes for conducting periodic training, evaluation and ongoing standardization of check and training personnel, supported by appropriate training records.
Continuous monitoring of stabilized criteria should be required during all approaches.
Flight path management
To ensure a safe flight path with early identification of deviations and timely corrective action:
Aircraft operators must define procedures for critical phases of flight operations (inclusive of taxi, takeoff, cruise, approach and landing). This must include applying stabilized approach procedures that consider energy state for all flights. Aircraft operators must include no-fault, mandatory go-around requirements in the operations manual.
The Aircraft operator should conduct a gap analysis between its procedures and each revision of the HeliOffshore Flightpath management [recommended practice], identifying and justifying any differences to the [recommended practice].
Aircraft operators are encouraged to develop and implement a policy for mandatory, internal reporting of occurrences involving aircraft destabilization and any go-around. Tracking of such reports, alongside FDM analysis, within the aircraft operator’s SMS will assist with the identification of possible specific risks or considerations that may exist in the conduct of approaches.
Information from the HeliOffshore Flightpath management [recommended practice] is presented in the next section.
Effective use of automation
To ensure the maintenance of controlled flight:
An autopilot or automatic flight control system must be fitted. This must be a four-axis system for multi-engine helicopters unless risk assessed and endorsed by a competent aviation specialist.
The aircraft operator must have an automation policy that ensures the appropriate use of automation to reduce cockpit workload. Specific consideration should be given to automation training requirements to ensure all protection modes are fully understood.
Surface/obstacle conflict
To prevent an airworthy helicopter in the control of flight crew flying into the ground (or water):
All offshore helicopters must be equipped with at least one radio altimeter (RADALT) with dual displays (including analogue indication), with a visual alert and automated voice alerting device (AVAD) capability. The aircraft operator must have procedures for any user adjustable AVAD features and for actions to be taken by the flight crew in the event of an alert.
Non-regulatory guidance – HeliOffshore
Flightpath management
HeliOffshore is a global association of the offshore helicopter industry and a forum for expert collaboration about safety. One of their publications is Flightpath Management (FPM) Recommended Practice for Oil and Gas Passenger Transport Operations (Version 2). The FPM guidance is intended to eliminate offshore helicopter approach incidents by expanding on the airline industry’s adoption of stabilised approach principles. The content in this section is adapted from the FPM and has been included to present industry best practice at the time of writing the investigation report for comparative analysis and safety education purposes.
The recommended practice incorporates the key elements considered fundamental for stabilised helicopter approaches, including energy state, monitoring procedures, and use of automation.
The guidance notes that the use of standard repeatable approach profiles enhances the ability of crews to monitor and detect deviations. Three examples of standardised offshore approaches (when established on the final approach track) were provided:
- A defined 5° profile from 500 ft circuit height to landing decision point (typically 40 ft above deck height) with simple distance-height calculations at 0.2 NM/100 ft increments (Figure 18)
- Stabilisation criteria for 0.5 NM (926 m) from destination then up to committal point with crew call-outs
- A fully coupled approach at a consistent approach speed to 300 ft, maintained while reducing speed by selection of a suitable nose up attitude. Stabilised point was 0.5 NM (926 m), with further descent initiated when the final descent profile was intercepted (Figure 19).
Figure 18: Example 1, defined 5° profile

Source: HeliOffshore, Flightpath Management (FPM) Recommended Practice for Oil and Gas Passenger transport Operations, Version 2.0. September 2020
Figure 19: Example 3, day DVE (degraded visual (cueing) environment) or night offshore approach

Source: HeliOffshore, Flightpath Management (FPM) Recommended Practice for Oil and Gas Passenger transport Operations, Version 2.0. September 2020
In day visual meteorological conditions (VMC, see the following section), any of the above approaches can be flown with primary reference to a standard ‘sight picture’. However, offshore approaches at night or in a day DVE may require a more formalised structure of gates and checkable parameters. Operators were advised to consider 0.5 NM (926 m) as the stabilised gate for an offshore approach and to define criteria that required a go-around if the approach became unstable between the gate and committal point. As this was a relatively high-risk phase, continuous monitoring of energy state parameters - power setting, airspeed, and rate of descent – with standardised call-outs for multi-crew operations was necessary.
HeliOffshore considered that crews have a strong tendency to continue approaches despite deviations, and missed approaches are often mismanaged. In that context, operations manuals should have clear simple guidance on how to conduct go-arounds. This should be supported by training, so crews are prepared to apply take-off power, adjust pitch to accelerate to VTOSS[43] then VY,[44] and track to avoid obstacles. As flight in instrument meteorological conditions (IMC) can be more difficult at low airspeeds, training for these conditions with consideration of automation is good practice.
The guidance for monitoring procedures related to the use of detailed briefings and standard call‑outs in a multi-crew environment. An approach briefing was recommended for every landing to address the details of the approach and management of the helicopter. A discussion of the possibilities that may lead to a go-around and briefing of the procedure was recommended. Pilots were advised to make deviation calls as soon as one was observed, and all such calls should be acknowledged and acted upon immediately.
Safe and effective use of automation is an important principle. For offshore approaches at night or in a DVE, a straight-in approach and landing is preferred. If a circling approach is unavoidable, it shall be flown coupled in 4-axes/3-cue automation with the pilot adjusting ALT, HDG and IAS through beep trims while maintaining visual cues until the committal point. The use of automation should be integrated in the specified approach profiles.
As previously outlined, the autopilot/AFCS in VH-ZGA was designed for 3-axis function above 60 kt and was not approved for operations below 500 ft AGL. While, the autopilot could be used for the downwind and base phases of circling, it was not recommended for a constant-angle decelerating final approach from 500 ft.
Stabilised approach guidance
In accordance with revisions to legacy guidance, the last suitable point to ensure that final landing configuration was selected and verified was 1,000 ft AGL. From that point, the helicopter should be transitioned to the specified speed and power settings to be stabilised by 500 ft. Although 500 ft was a suitable point to verify stable approach criteria, a go-around was not mandatory if the helicopter was not yet stable when attaining this altitude.
For offshore approaches, the final gate was defined as 0.5 NM (926 m) from the installation or 300 ft above the landing site elevation. The approach criteria should be checked just before reaching the gate and if identified as ‘stabilised’ the approach could continue. If the helicopter was ‘Not stabilised’ by this point (or later became unstable), the response was to ‘go-around’ immediately.
An approach was considered stabilised when the following conditions existed:
- the helicopter was in the correct landing configuration
- the helicopter was on the correct flight path within tolerances that could be maintained using angles of bank and rates of descent within stabilised limits
- airspeed was fixed for an instrument approach or appropriate to the distance to go for visual approaches
- rate of descent was no greater than 700 ft/min
- steady power setting relative to conditions
- bank angle variation was less than 20°
- within navigational tolerances for an instrument approach.
Regulatory framework for night operations
General conditions
In Australia, night flying could be conducted under the night visual flight rules (night VFR) or instrument flight rules (IFR). Some operators conducting specialised operations also had approval to utilise night vision imaging systems (NVIS) for enhancement of pilot vision at night.
To operate a helicopter under the night VFR in uncontrolled airspace, the following conditions applied:
- visual meteorological conditions (VMC) – flight visibility of 5,000 m or greater and clear of cloud (below 3,000 ft above mean sea level)
- when at or below 2,000 ft above the ground or water, navigation by reference to ground or water
- forecast conditions indicate that the flight can be conducted in VMC at not less than the lowest safe altitude (LSALT) - defined as 1,000 ft above the highest obstacle within 10 NM (19 km) either side of the planned track
- provision for an alternate aerodrome or helicopter landing site if:
- more than scattered cloud below 1,500 ft and visibility less than 8 km was forecast for the destination
- approved navigation not available.
On arrival, descent below the LSALT was permitted when the aircraft was established within 3 NM (5.5 km) of the destination and the approach for a landing was predicated on visual manoeuvring in continuous VMC.
Pilot qualification and experience requirements
To operate a flight under the night VFR, the pilot is required to hold a night VFR rating. This is granted when a pilot meets the following requirements:
- holds a private, commercial or air transport pilot licence
- meets the requirements for granting of at least one night-VFR endorsement
- records 10 hours of aeronautical experience at night in an aircraft or approved flight simulation training device (including 5 hours dual cross-country flight time at night under the VFR in an aircraft)
- passes the night-VFR flight test.
The requirements for a helicopter night VFR endorsement were similar to the associated rating and specified 3 hours of dual flight, 1 hour of solo night circuits, and at least 3 hours of dual instrument time.
A flight test for a night VFR rating included an approach and landing at an aerodrome remote from ground lighting and a go-around procedure. In addition, the candidate was required to perform instrument flying in full panel and limited panel configurations, including recovery from 2 different unusual attitudes in either configuration.
The holder of a night VFR rating was authorised to conduct a flight under the VFR at night if the following recency conditions were satisfied:
- successful completion of an applicable flight review, flight test, or operator proficiency check in applicable aircraft within the previous 24 months
- one take-off and landing at night or competency assessment in previous 6 months
- if flight involves carriage of passengers – 3 take-offs and landings in applicable aircraft with previous 90 days.
Night flying competency standards
The competency standards for night VFR ratings were specified in the CASR Part 61 manual of standards. These included instrument flying, visual approaches, and go‑arounds (missed approaches).
A night VFR rated pilot required the skills and knowledge to perform normal flight manoeuvres and recover from unusual attitudes with reference to both full and limited instrument panels. Essentially, pilots were required to apply their knowledge of scan techniques and attitude/power requirements to interpret the instruments and carry out various normal manoeuvres such as descending and turning. For full instrument panel manoeuvres, pilots were expected to achieve, and maintain, a specified flight path while operating within defined flight tolerances.
Limited instrument panel manoeuvres were defined as non-normal situations without reference to the primary attitude indicator/display, the primary heading indicator/display, or reliable airspeed indications. In those cases, pilots were expected to use secondary (standby) instruments to carry out normal manoeuvres to achieve the nominated performance.
Recovery from upset and unusual attitudes in simulated IMC was a requirement with a full instrument panel and a limited instrument panel. Unusual attitude training and assessment conducted in aircraft was limited to daylight conditions for safety reasons.
A visual approach in the night VFR context was primarily the conduct of a traffic pattern around a runway for a landing. The circuit entry and pattern were required to be performed visually with reference to the runway environment and a safe altitude maintained by reference to aircraft instruments and runway lighting. Helicopter operation was specifically addressed in relation to take-off only.
The night VFR competency standards included the conduct of an approach and landing at an aerodrome remote from extensive ground lighting.
Discontinuation of an approach in the night VFR context was known as a go-around and in the instrument rating context as a missed approach. During a visual approach at night, the pilot was required to recognise the need for a go-around and to conduct it from any point on base and final approach legs.
Flight review
An applicant for a night VFR rating flight review is required to demonstrate relevant knowledge, including the use of instrument systems and operations below lowest safe altitude. For the flight assessment, the applicant was required to conduct an operation at night under the VFR and perform manoeuvres within specified tolerances. At a professional level, the general helicopter tolerances for altitude was +/- 100 ft and for airspeed was +/- 5 kt.
The practical flight standards referenced the competency standards as described in the previous section and specified that some elements were not required for a flight review. These non‑required items included operations to an aerodrome remote from ground lighting and engine failure after take-off. Some other elements such as flight planning and ‘manage hazardous weather conditions’ were not required if addressed in a flight review within the previous 24 months.
Helicopter equipment requirements
At the time of the occurrence, CASA specified the minimum equipment requirements for helicopters in CAO 20.18. The instruments required for night VFR included the basic VFR flight instruments plus an attitude indicator (with redundancy), heading indicator, and vertical speed indicator. For operations onto vessels or platforms at sea by night, an instantaneous vertical speed indicator was also required.
If a night VFR flight involved flights over land or water where the helicopter attitude could not be maintained by use of visual external surface cues (such as ground or celestial lighting), an approved autopilot system/stabilisation system or a qualified 2-pilot crew was required. For all IFR operations, an approved autopilot system/stabilisation system was required.
At the time of the occurrence, there were no requirements for helicopters to be equipped with an EGPWS or HTAWS.
Revised regulatory framework for marine pilot transfer (night operations)
From December 2021, MPT operations were authorised under a CASR Part 138 aerial work certificate and conducted under the general operating and flight rules contained in CASR Part 91, with addition or variation of those rules according to Part 138.
For night VFR operations under CASR Part 91, the general conditions such as VMC, navigation, and minimum altitude requirements remained the same as the previous regulations. The pilot qualification and experience requirements for a night VFR rating (CASR Part 61) also remained unchanged.
CASR Part 91 and Part 138 stated that any required equipment must be visible, and usable, from the pilot’s seat. The equipment requirements for rotorcraft night VFR and IFR were essentially the same as those specified in CAO 20.18. This included an ongoing requirement for an autopilot/stabilisation system for all IFR or single-pilot night VFR in conditions where the attitude could not be maintained by use of visual external cues (ground lighting and/or celestial illumination).
All operators conducting aerial work under CASR Part 138 were required to manage crew fatigue in accordance with existing rules and conduct risk assessment and mitigation processes. An operator who conducted MPT flights was also required to have a training and checking system and safety management system if currently required or according to deferral criteria.
The holder of a CASR Part 138 aerial work certificate could carry 1 or 2 passengers on VFR flights at night in multi-engine rotorcraft such as the EC135 type, subject to certain conditions. Carriage of 3 to 9 aerial work passengers in VFR flights at night was conditional on the use of multi-engine rotorcraft with equipment for flight under the IFR and/or in an approved NVIS operation. If marine pilots were winched to and from ships at night, the pilot in command was required to use NVIS for the operation.
An EGPWS or HTAWS was not required for CASR Part 138 aerial work operations.
Operator’s standard operating procedures
Introduction
As an AOC holder, the operator produced an operations manual to promulgate general policy and standardised procedures for EC135 MPT flights from bases at Gladstone, Mackay (Hay Point), and Port Hedland. The version of the operations manual current at the time of the accident was issued by the operator on 28 February 2018.
For operations to ships at sea, the operator specified requirements for flight planning, helicopter performance, shipboard landing areas, with instructions for various phases of an MPT flight. The standard operating procedures (SOPs) relevant to the occurrence are addressed in the following section.
The operator referred pilots to the respective Aircraft Handbook and Approved Flight Manuals for normal and emergency procedures. If any procedures required clarification these were addressed in the operations manual.
Circuit, approach, and landing procedures
Ships were generally underway when helicopter landings and take-offs occurred and there were no guidance systems to assist the helicopter pilots make their approaches to the ship. As such, pilots were required to descend, approach and land in visual meteorological conditions.
The SOPs for day and night approaches to ships at sea were essentially the same and both were conducted as visual manoeuvres. The following extract from the operations manual pertained to offshore night approaches:
Once the ship has been identified and the aircraft is established within the circling area, an approach may be commenced.
An approach to the ship will be made using normal circuit flying techniques (downwind 700 ft at 70‑80 kts). Aim to roll out on ‘final’ - with a headwind component at 500 ft AMSL with a 60 kt ground speed, and so as to position the ship upwind and within a sector 30°–45° degrees either side of the aircraft (the final ‘window’), so a normal (7°) approach sight picture is obtained.
For the EC135 type specifically:
Position the helicopter at a finals ‘gate’ of 500 ft above the landing site at 65 kt.
From this position, carry out a constant angle reducing speed sight picture approach to an [out of ground effect] hover position abeam the ship.
The extract pertaining to offshore night approaches continued:
In the event that visual reference with the ship is lost during the approach, the aircraft shall be established in the climb and a go-around within the circling area to LSALT/MSA initiated. The aircraft should be navigated so as to remain clear of other ships. Once at LSALT/MSA and visual reference has been re-established, an approach may be recommenced.
Further instructions were provided for the downwind, base, and final segments of the circuit without differentiating between day and night operations:
Downwind is to be flown at 700 ft AMSL and 70/80 kt. Judicious use of the aircraft’s navigational instruments should be employed to help maintain situation awareness. For example, the OBS/CDI in combination with the HDG bug may be particularly useful for circuit orientation.
On the base leg descent from downwind altitude to the final gate altitude of 500 ft should be achieved. The aircraft should be turned so as to position the ship in the final ‘window’. Descent below 500 ft should not commence until the aircraft is established into wind and aligned on the final approach path. In two-pilot operations, the pilot not flying was to assist the pilot flying.
Aim to roll out on ‘final’ with a headwind component at 500 ft AMSL with a 60 kt ground speed. On achieving the final ‘gate’, a constant angle approach is made to the over water termination area or FATO. The pilot is to ensure that the aircraft’s radar is in standby mode, the landing light is switched on and the floats are armed.
The operator also provided the following general advice for pilots conducting approaches to ships:
Turns below 500 ft AGL are not permitted while the pilot flying (PF) is controlling the aircraft by reference to flight instruments.
The chief pilot advised that circuit procedures for MPT operations were developed from past practice and the 700 ft circuit height provided a terrain clearance buffer at one of the locations. For operations at Port Hedland, the chief pilot had no objection to a local practice that abbreviated the circuit pattern (such as straight-in approach) according to the inbound track and final approach alignment based on relative wind at the ship.
Ship night approach and landing
The chief pilot advised that ship night approaches and landing were challenging and prospective MPT pilots required training to develop their judgement of descent profiles. Once pilots were established on the final approach track (not below 500 ft or above 60 kt groundspeed), they were expected to commence a descent according to the guidelines summarised in Table 9.
Table 9: Nominal descent parameters on final approach
|
Altitude |
Groundspeed |
Rate of descent |
|
500 ft |
60 kt reducing |
500 ft/min |
|
400 ft |
40 kt |
400 ft/min |
|
300 ft |
30 kt |
300 ft/min |
|
200 ft |
20 kt |
Reducing |
|
100 ft |
Reducing |
Reducing |
The chief pilot advised that the approach angle gradually steepened so that at 300 ft the helicopter was basically beside the ship and the helipad was visible in the chin bubble (lower window). From 300 ft, indicated by the radio altimeter, the pilot would generally be committed to carry out the landing. The EC135 could be operated with assured one engine inoperative performance that allowed a go-around in almost all phases.
For night approaches where there was no moon and no local illumination (black-hole approach), the chief pilot expected MPT pilots to maintain a continuous scan pattern of ‘airspeed/height/rate of descent/ship’ to ensure that all of the parameters were reducing. The chief pilot stated that, in general, it was better to be slower rather than faster to avoid a flare that could result in an overshoot. However, there had been occasions during training when pilots had been affected by night visual illusions and slowed the helicopter to no forward speed while still descending.
Stabilised approach criteria
Under the operations manual heading of ‘Stabilised approach criteria’, the operator specified the following:
(a) Broadcast your intentions on the appropriate frequency;
(b) Complete the downwind checks …;
(c) A normal sight picture to the landing area shall be established below 500 ft;
(d) The approach shall be stabilised below 300 feet with a decelerating disc attitude and airspeed …;
(e) The PIC shall ensure that obstacle clearance is maintained and compliance with CASR’s in relation to occupied buildings;
(f) A lookout shall be maintained throughout the approach;
(g) Curved approaches are permitted, however all approaches shall be terminated with a headwind component.
In the context of final approach in day or night conditions, the operator provided the following guidance for offshore operations:
When airspeed is below 30 kt, rates of descent in excess of:
(a) 500 ft/min should be avoided; and
(b) If a 700 [ft]/min (or higher) ROD should occur, a go-around should be conducted.
No guidance was provided for airspeeds above 30 kt or other parameters such as bank angle, pitch angle or engine torque. The chief pilot advised that pilots were expected to go-around when a landing was not feasible. In most cases pilots could recover from a below-profile approach but a go-around was necessary when high and close to the ship.
Missed approach/go-around
In the context of offshore operations, the operator provided the following guidelines for missed approaches:
Circumstances may arise in which an approach must be discontinued. In these circumstances, either pilot may call “Missed Approach” and issue the following instructions to the PF:
“Pull in climb/cruise power”
“Establish positive ROC”
“Maintain Vy until above 500 ft”
“At 500 ft adjust attitude for 80 knots”
“Level out at LSALT”.
The PF will then re-adjust for climb power and speed and fly the missed approach procedure. The PIC will re-assess the next approach.
If at any stage there is a requirement for the pilot in command to take over the controls, he/she will call “taking over” and the co-pilot will confirm “handing over”. The pilot in command will take control of the aircraft.
Use of automation
The operator specified that the EC135 flight director or upper modes of the 3-axis autopilot may be engaged at the pilot’s discretion after take-off above 500 ft AGL. No guidance regarding use of the autopilot in the circuit was provided in the operations manual.
The chief pilot advised the ATSB that for MPT operations in degraded visual environments, including at night, pilots were trained to use the upper modes of the autopilot until established on final approach at 500 ft and not below 60 kt. The autopilot interface was considered easy to use and capable of reducing pilot workload. From the chief pilot’s perspective, unless large and rapid flight path changes were required, there was higher risk and no benefit when operating without the autopilot (above 500 ft) in degraded visual cueing environments.
For manoeuvring in a normal circuit, the chief pilot expected pilots to use the beep trim as the primary means to command the autopilot. The use of force trim release was usually limited to momentary activation to quickly reset trim references. Based on initial and recurrent training and assessing conducted by the chief pilot, pilots were using the automation to manage the flight path without difficulty.
The instructor advised that, in general, ‘the autopilot needs to be on from 500 ft after take-off to 700 ft established in final approach’ and they were ‘very strict on use of the autopilot, especially in low visibility conditions’. However, the instructor also advised that, in benign conditions, if pilots chose to select the ‘autopilot off as they got to the circuit area, that’s a decision that they would make but would be accountable for.’
Night VFR
The operations manual specified that the pilot in command of a company helicopter operating under the night VFR shall hold a current night VFR rating and meet the standard recency requirements. This comprised 3 circuits or a flight test at night within the previous 90 days.
There was no other substantive content applicable to MPT operations at night.
Two-pilot operation
The occurrence flight was conducted as a single-pilot operation under supervision of a second pilot. Extracts of the operator’s SOPs for 2-pilot operations are provided for comparison and reference.
For operations that required 2 pilots, the operator specified roles, coordination protocols, and deviation criteria. One of the pilots operated as the flying pilot (FP) to manipulate the controls or manage the autopilot while the other pilot was the non-flying pilot (NFP). The NFP was required to assist the FP in any way necessary to allow the FP to concentrate on physically flying the helicopter.
At any stage of the flight if the FP failed to maintain control of the helicopter within accepted tolerances the NFP was required to bring the deviation to the attention of the FP. If corrective action was not initiated by the third call, the NFP was to take over control saying, ‘Taking Over’ and the other pilot would then relinquish control saying ‘Handing Over’.
In the context of offshore operations, on downwind the NFP should at all times maintain visual reference with the ship and should assist the FP by calling out any required HDG or speed changes. Then, on base, the NFP was to assist the FP by calling out the required final HDG. During final approach, the NFP was to concentrate on the helicopter’s instruments and call out airspeed, altitude, and vertical speed.
The operator specified significant deviation call outs during flight in IMC including the following:
- IAS +/- 10 KIAS
- altitude +/- 100 ft (+50 ft, -0 ft on final)
- rate of descent greater than 1,000 ft/min on final approach.
Absent procedures
Without implying any non-conformance, the ATSB noted that the operator did not specifically address the following topics in the operations manual:
- operations in degraded visual cueing environments
- use of radio altimeter
- unusual attitudes/energy states
- spatial disorientation
- controlled flight into terrain (CFIT)/Approach and landing accident reduction (ALAR) considerations.
The chief pilot advised that the risk of operating in degraded visual environments at night was controlled by the VMC requirements, use of automation, and application of instrument flying skills. Pilots were also trained to set the radio altimeter warning to 300 ft for approaches to ships. As these controls applied to all operations at night in VMC, there was no specific reference to degraded visual cueing environments in the operations manual.
The chief pilot also considered that the identification of, and recovery from, unusual attitudes was part of CASR Part 61 training and assessment and was therefore not addressed in the operations manual. Spatial disorientation and CFIT/ALAR were addressed in periodic online training provided by the operator.
Operator pilot training and assessing
Overview of pilot competency requirements
As the holder of a certificate that authorised charter and aerial work operations, the operator was subject to a number of general conditions. Some of these related to establishing and maintaining the competence of flight crew.
The operator provided charter and aerial work services and was not required to provide a CASA‑approved training and checking organisation. Nevertheless, CAO 82.0 and CAO 82.1 imposed obligations on the operator in relation to the competence of flight crew.
Before a pilot could operate a helicopter type and model, there was a requirement for the chief pilot to be satisfied that the pilot was competent to operate in accordance with the specific instructions provided in the operations manual and pilot operating handbook or AFM. Stated CAO 82.0 responsibilities of a chief pilot included monitoring operational standards, maintaining training records and supervising the training and checking of flight crew. A chief pilot was not allowed to delegate training and checking duties without the written approval of CASA.
Additional requirements applied to operators that conducted training and assessment related to licences, ratings, and endorsements issued in accordance with CASR Part 61. For flight training up to commercial pilot level (other than integrated training), an approval in accordance with CASR Part 141 was required. For other types of flight training, such as granting of a type rating, an approval in accordance with CASR Part 141 or 142 was required.
Management of line pilot competence
The operator specified training and checking requirements to ensure that company pilots met and maintained a high standard of knowledge and expertise in the overall operation of company operated helicopters. These specifications in part 4 of the operations manual were intended to satisfy the regulatory and corporate requirement to carry out internal operational checking of pilots within the guidelines of CAO 82.0. Extracts from Part 4 of the operations manual included:
Duties and responsibilities
The chief pilot is responsible to higher management to ensure appropriate training and checking procedures are in place.
As authorised by CAO 82.0 Appendix 1 the Chief Pilot is responsible for: …
Ensuring that all Company employed pilots undergo training and checking at intervals not exceeding 12 months;
The training and checking requirements are to be used to induct pilots for Company operations.
Selection and experience requirements for training and checking personnel
Training and checking personnel will be selected and approved by the Chief Pilot after consultation with the General Manager.
The Chief Pilot shall ensure that any instructor designated for training and checking duties has the appropriate operational experience, endorsements (including winch and sling) and ratings prior to being approved for training and checking duties.
Training and Checking duties on Company helicopters, both multi-engine and single engine, for pilots involved in MPT operations, may only be conducted by Check Pilots who have received the specific approval of the Chief Pilot. These pilots shall hold a current instructor rating with multi-engine training approval as well as a current command instrument rating.
Training and approval of training and checking personnel
Additional training for qualified instructors approved after selection should not be necessary.
The Chief Pilot or his/her delegate shall conduct the routine Base and Line Checks on all Company approved training and checking pilots conducting multi-engine or MPT operations.
Induction and training requirements
A pilot on joining the Company, will be briefed by the Chief Pilot on Company operating and administrative procedures. The pilot shall also be checked on the type/types of aircraft he/she will be rostered to fly.
All pilots employed by the Company will undergo air training or flight evaluation prior to commencing normal line operations.
Training syllabi and checking programs
Training Syllabi are located in “Air Maestro”[45]at the Forms Register under the control of the Chief Pilot.
All company pilots are to undergo two proficiency checks in each calendar year. The two checks shall be:
(a) Base check which may include the renewal of a Command Instrument rating, and
(b) Line check.
The base check will be directed to basic flying skills, aircraft handling, knowledge, and practice of emergency procedures.
The line check will be a normal revenue flight of at least two sectors, one of which should be at night if the pilot’s duties include night operations. The Initial Line Check shall be completed at the conclusion of ICUS (in command under supervision) flying.
Ship operational training
Multi-engine helicopters by day: Ten ICUS landing and take-offs
Multi-engine helicopters by night: Ten ICUS landing and take-offs
Demonstrate competence in all aspects of offshore operations to the satisfaction of the Chief Pilot or his/her delegate or an approved Check Pilot.
The forms in Air Maestro listed criteria for different phases of flight with provision to record the applicable assessment and comments.
The chief pilot, who did not hold an instructor rating, advised that the qualifications, experience, and approvals of the head of operations (as defined in CASR Part 141/142) and other instructors was considered to be suitable for the conduct of operator-specific training and assessing.
Flight training and assessment activity
From 1 November 2017, the operator held authorisations to conduct flight training in accordance with CASR Part 141/142 and the CASA-approved exposition,[46]This included flight training for night VFR ratings, instrument ratings, and EC135 type ratings.
In a parallel structure to the charter/airwork operation, the instructor in this occurrence was the head of operations (HOO) for the CASR Part 141/142 organisation and reported to the chief executive officer. Any flight instructors and examiners operating under the approvals reported to the HOO. The chief pilot was nominated as the operations officer to liaise with the HOO for rostering of instructors, helicopter allocation, and program changes.
To ensure that standardised training was delivered safely by competent and qualified instructors, the HOO managed an internal training and checking system. This system provided for annual refresher training for human factors/non-technical skills (HF/NTS) training and annual standardisation and proficiency (S&P) checking.
The S&P checks included a review of each instructor’s competency to deliver long and pre-flight briefings and flight instruction in accordance with the applicable syllabus and lesson plans. Between CASR Part 141/142 approval and the occurrence, the instructor conducted S&P checks on a line pilot/instructor and an external flight instructor/examiner. There was no record of the instructor undergoing a S&P check in the previous 12 months.
According to the pilot’s logbook, the last instructor standardisation check was carried out by an external instructor on behalf of the contracted flying school on 6 March 2017. This expired on 6 March 2018, 8 days before the occurrence. The last standardisation check was carried out in an EC135 equipped with dual flight instruments.
A key function of the CASR Part 141/142 organisation was to conduct flight reviews and proficiency checks with company pilots for maintenance of their Part 61 licences and ratings. For that function, reference was made to the CASR Part 61 manual of standards. There was no reference to base or line training/checks in the Part 141/142 exposition.
Summary observations
Although the CAO 82.0/82.1 and CASR Part 141/142 processes operated in parallel with different functions and accountabilities, in practice the chief pilot relied on the HOO and other instructors from the CASR Part 141/142 organisation to carry out type-specific base checks and some line training/checks.
Outside of CAR 217, there were no standards or guidance in support of the requirements for the chief pilot to be satisfied that the pilot was competent and for monitoring of operational standards. In the absence of training and checking system requirements, the operator mimicked aspects of CAR 217 and CAO 82.1 manual requirements without addressing training schedules, management of ICUS, or instructor competency in relation to supervision of MPT operations.
Although it was just over 12 months since the instructor’s last recorded S&P check (required annually), that check was oriented to generic CASR Part 61 requirements and was not considered to be significant.
To differentiate the operator’s management of pilot competence from a CAR 217 training and checking system, the term ‘training/assessing’ is used throughout the report.
Preliminary activities at Port Hedland in March 2018
Based on the arrival date at Port Hedland following initial training at the operator’s Mackay base, 10 consecutive days were available to complete the pilot under supervision’s operational EC135 training followed by a couple of non-rostered days. From that point (21 March), the pilot under supervision was rostered for day and night MPT operations for the balance of the 3‑week roster cycle.
The instructor travelled to Port Hedland on 5 March 2018 to conduct scheduled flight reviews and proficiency checks with the established line pilots, along with operational induction of the pilot under supervision. Although the chief pilot had allowed nearly 3 weeks overall for the instructor to complete those tasks, the roster showed the instructor had leave scheduled for the weekend at the end of the second week. As the training and assessing progressed, the instructor discussed the possibility that if the tasks could be completed by the end of the second week, a return to Port Hedland after weekend leave would not be required.
On the first duty day at Port Hedland, the instructor utilised the operator’s flight training device at the heliport for 1.3 hours of instrument time that included various instrument approaches. Between 6 and 11 March, the instructor conducted various flight reviews and proficiency checks with 5 of the established line pilots.
One of the line pilots did not meet the requirements of a night VFR flight review conducted by the instructor on Saturday 10 March. In consultation with the chief pilot, that pilot was withdrawn from rostered night duties. To fill the resulting roster gap, the instructor was rostered for a day duty on Tuesday 13 March and the next vacant night duty starting on evening of Wednesday 14 March.
For the remainder of the day (10 March) and during the 2 following days the instructor supervised some local EC135 flying by the pilot under supervision. That included general familiarisation flying, a helicopter type flight review, and base check. No practice instrument or night flying was carried out during this pre-line training phase.
On the afternoon of Monday 12 March, the instructor emailed the chief pilot in Mackay, Queensland with a plan to complete training and checking commitments at Port Hedland by Friday morning. To accomplish this, the instructor intended to fly with the pilot under supervision in accordance with the following schedule:
- Monday (12 March): completion of EC135 refresher training including base check and helicopter (EC135 type rating) flight review
- Tuesday (13 March): normal day shift line operations including any remaining helicopter flight review items
- Wednesday (14 March): night line operations on normal roster
- Thursday (15 March): night line check and night flight review
The chief pilot replied shortly afterwards with affirmation of the plan.
Based on recent experience and flight reviews/checks with the previous operator, the pilot under supervision met the regulatory requirements for night VFR operations. The ATSB noted that the flying for the previous operator was carried out in single-engine B206L helicopters equipped with analogue instrumentation and was conducted with the assistance of night vision imaging systems. As the previous operator’s B206L helicopters were not equipped with an autopilot or stabilisation augmentation system, the flight path was managed directly through continuous pilot control inputs.
Line training – session 1
Consistent with the schedule advised by the instructor to the chief pilot on 12 March, line training for day operations started early on 13 March 2018 with flight to a ship with a landing and take-off, possibly demonstrated by the instructor. A further 8 landings to a mix of inbound and outbound ships were conducted by the pilot under supervision of the instructor.
As recorded by the instructor, the pilot under supervision improved significantly with practice to consistently operate to a ‘good solid standard’ and was competent and safe. The instructor considered that at that stage, the pilot under supervision ‘just needs practice doing the transfers so the process was more automatic.’ Total flight time was recorded as 6.4 hours and the pilots were on duty for about 14 hours.
Line training – session 2
The instructor and pilot under supervision were rostered for the normal night duty on 14 March 2018 to continue line training. Although night duty nominally started at 1800, the pilot under supervision was at the operator’s port facility at various times during the day to complete induction-related tasks. The pilot under supervision then returned to the port facility at about 1610 to prepare for the flights scheduled that evening followed by the instructor at about 1650.
Five transfer flights were scheduled for the shift: the first 2 with marine pilots to the pilot boarding ground then 3 to pick up marine pilots from outbound ships near C1/C2. The first flight departed at 1753 and returned to the heliport at 1813. This flight, in daylight, was counted as the tenth MPT operation for the pilot under supervision, who was assessed by the instructor as performing to a solid standard and was recommended for day VFR MPT approval.
The second flight of the shift departed the heliport at 1859 (about 15 minutes after last light) and returned to the heliport at 1924. Operator records indicated that, following this flight, the pilot under supervision fully refuelled the helicopter. The instructor recalled that the pilot under supervision also conducted a daily inspection on VH-ZGA, preparatory to certifying the daily inspection for the next day’s flying.
After completion of those activities, the instructor suggested the pilot under supervision return to the nearby accommodation for a break prior to the next flight. The instructor remained at the heliport, to complete administrative tasks.
The third flight departed the heliport at 2252 and picked up a marine pilot from an outbound ship near C1/C2. During the flight back to Port Hedland, another marine pilot scheduled to be picked up from the next bulk carrier radioed the crew of VH-ZGA and amended their pick-up time to 2345. Consequently, on arrival at Port Hedland at 2327, the marine pilot was disembarked with the engines running to enable a quick turnaround.
Flight data review
For context and comparative analysis, the ATSB obtained the automatic dependent surveillance broadcast (ADS-B) and automatic identification system (AIS) data for the line training flights preceding the occurrence flight. A preliminary review of the data for the 9 ship approaches during the day on 13 March 2018 and first flight (during daylight) on the accident day did not identify anything that was inconsistent with the instructor’s assessment.
Data for the second and third line training flights on 14 March, both conducted at night, is presented in graphical and tabular form at Appendix A.
Meteorological conditions for both flights were similar to the occurrence flight. Although the second flight (of the shift) departed about 15 minutes after last light, the transit, circuit and landing on the carrier was completed before nautical twilight. As such, some scattered and diminishing light might have been evident on the western horizon.
The second flight departed the heliport at 1859 to transfer a marine pilot to an inbound bulk carrier (Anangel Explorer) at the pilot boarding ground. The initial descent from cruise altitude appeared to have been initiated using an upper vertical navigation mode. However, as the descent continued and the helicopter approached to pass abeam the bulk carrier, the rate of descent increased above 1,000 ft/min before an abrupt transition to level the helicopter at 700 ft. The helicopter was then manoeuvred around the ship at about 700 ft until established on final approach about 1,700 m from the landing hatch at 55 kt. In general, the final approach was conducted at a consistent angle with steady deceleration and a rate of descent varying between 0–450 ft/min.
The third flight departed the heliport at 2252 and tracked to C1/C2 to pick up a marine pilot from an outbound bulk carrier (Cape Aster). Descent was conducted at about 500 ft/min and continued as the helicopter circled the ship until it was levelled at 550 ft. While the helicopter was turning onto final approach about 1,500 m from the landing hatch, it started descending again and the airspeed reduced through 60 kt. The descent and reduction in airspeed continued to about 275 ft at 38 kt, about 700 m from the landing hatch.
As the approach continued, the helicopter climbed to 375 ft, with airspeed reducing through 35 kt about 300 m from the ship. The helicopter then descended to 150 ft at up to 1,000 ft/min with airspeed reducing to 15 kt. This descent rate then reduced to 300 ft/min while maintaining about 15 kt. The helicopter landed on the bulk carrier at about 2307.
Summary observations
- The pilot under supervision was involved in 10 MPT operations during daylight and was assessed by the instructor as competent.
- The instructor transitioned the pilot under supervision from day to night line training without any further day flying or preparatory night or instrument flying.
- The second flight of the shift, and first line training conducted at night, was to the pilot boarding ground. Although the transition to circuit height was abrupt, the base turn and final approach generally conformed to the operator’s procedures and parameters for ship approaches.
- The third flight of the shift was to C1/C2. Circuit height and descent profile on final approach did not conform to the operator’s procedures and parameters for ship approaches. Additionally, the conduct of the 2 night circuits was not consistent with use of a vertical upper mode of the autopilot.
Fatigue risk management
Operator’s fatigue risk management system
The operator managed the risk of fatigue-related incidents and accidents using a fatigue risk management system (FRMS) as an alternative compliance method for the flight and duty limitations prescribed in CAO 48.1 (Flight time limitations – pilots). The use of the operator’s FRMS as a compliance method was based on a CASA-issued exemption under subsection 4 of CAO 48.0. The exemption was issued by CASA in September 2014 and, in April 2017, it was extended to 30 April 2018.[47] The conditions applicable to the exemption required the flight and duty limits to be included in the company operations manual. The exemption also required the operator and each flight crew member to comply with the fatigue limits specified in the FRMS manual. The change record in the FRMS manual showed no updates since April 2014.
The operator’s FRMS described a system of shared responsibility, with pilots required to ensure they had sufficient sleep and were not impaired by fatigue prior to commencing flying duties. A key component of the operator’s FRMS was the requirement for each pilot to maintain a sleep log, which tracked the extent to which their sleep and duty time was within specified limits (see below).
The FRMS also prescribed rostering rules including a maximum duty period of 12 hours, a maximum flying time of 10 consecutive hours, a maximum 4 consecutive night shifts, and a maximum 100 duty hours in a 14-day roster period. A duty period could be extended by the chief pilot if a task was underway, although that was limited to 1 hour for day VFR operations and 2 hours for 2-pilot crews.
As part of the FRMS, pilots received fatigue awareness training and training regarding the operation of the FRMS. The fatigue awareness training included a description of the causes of fatigue and advised that fatigue was very difficult to self-diagnose and could only be prevented by achieving sufficient sleep.
Roster pattern at Port Hedland
The roster for line pilots at Port Hedland included days that were allocated as duty, off duty or standby. The FRMS defined duty as any task that a pilot was ‘required to carry out associated with the business of the operator’. Off duty was defined as time ‘free of all duties associated with any type of employment’, and standby was defined as periods where a pilot was required to be available for a duty period.
The rosters for Port Hedland pilots typically followed a set pattern, beginning with travel to Port Hedland followed by a series of 4-day blocks comprising:
- a day of standby
- a day shift (0600–1800)
- a night shift (1800–0600, commencing 24 hours after the end of the day shift)
- a day off duty.
Pilots were rostered on for 3 weeks, in which they would normally have about 4 or 5 day shifts and 4 or 5 night shifts. Time during a day shift, night shift or standby period was only considered as duty time if the pilot conducted a flight duty or other task associated with their employment.
The operator’s FRMS was produced prior to the commencement of MPT work at Port Hedland, with the manual stating that all operations would normally be based in Mackay and Gladstone. The manual also showed rosters for IFR and day VFR operations that were conducted at those bases. These roster patterns involved 14-day periods containing blocks of 4.5 days continual 24‑hour standby for IFR pilots (commencing at 0600), and 5 days continual day shifts for VFR pilots (from 0600–1800).
The roster worked by the Port Hedland base pilots was not described in the FRMS manual. There were no updated fatigue management procedures for any of the operational differences between Port Hedland and the other bases. The operator had suitable air-conditioned rest facilities at its Port Hedland base where pilots could sleep during a day shift or night shift. In addition, the residential units generally used by the pilots were situated only a short distance from the operator’s facility at the port. Each pilot would typically have access to their own 2-bedroom unit during their tour.
The FRMS manual included a discussion of the assessment of risk associated with different types of tasks. For MPT tasks, there was a discussion of risk for IFR tasks (2 pilots at night, single pilot by day) and day VFR tasks (single pilot), but no discussion of single pilot night VFR tasks. In terms of IFR tasks, the manual stated:
The route is fixed and the location of the ship and the base are also fixed, the details of the ship (nationality, size, hatch number for landing and weather) are known and communication with the ship exists. The major risk may be fatigue impairment leading from consecutive night operations, particularly those flown between the times of 10 PM to 6 AM which conflict with the circadian rhythm. The task is assessed as an M category task [moderate risk] …
The company does not expect a Pilot to fly for more than four consecutive late night operations …
Sleep logs
Under the FRMS, pilots were required to obtain the sleep necessary for flight duties. The manual stated:
A flight crew member will require between 6 and 8 hours sleep per night to satisfy his needs. The exact amount of sleep is dependent on the individual’s physiology. While it is desirable that the flight crew member has had that sleep before undertaking duty he may undertake duty in accordance with the PSWR …
PSWR is a rule that sets out the minimum sleep requirements before any duty may be performed. Duty may be performed in accordance with this rule with less than the normal sleep for a forty eight hour period. The rule states that the amount of ‘useful wakefulness’ that occurs is equal to the amount of sleep in the preceding 24 hours and the 24 hours before that. The minimum sleep needed prior to starting duty in a twenty four hour period is 5 hours and in a forty eight hour period 12 hours ...
During night operations it is unlikely that flight crew will gain all their normal sleep-in daylight hours. Flight crew members should therefore consider extending their normal sleep in a duty period between the hours of 6 PM and 6 AM in one of the following ways. They should gain a duty-free period of four hours in which they have some sleep or alternatively a nap, preferably for up to two hours, while remaining on duty. It is up to the flight crew member to ensure that in a period of night duty he has the sleep required for the duty to be performed and if this does not occur, he is to inform the tasking officer.
Further information regarding the prior sleep wake rule (PSWR) and prior sleep wake model (PSWM) is provided in Appendix E.
Pilots recorded their hours of sleep and duty using a Microsoft Excel spreadsheet known as a ‘sleep log’. The sleep log was developed by a consultancy group and was programmed to identify fatigue risk based on the PSWR as well as the operator’s maximum duty period of 12 hours. Pilots coded each hour of every day (or each cell) as either sleep (S, coloured grey), duty (D, coloured light blue) or flying (F, coloured dark blue). Other time awake but not on duty or flying was left or recorded as blank (light yellow). A separate spreadsheet in the same Excel file also required pilots to record their actual flight and duty times after each shift.
The FRMS manual stated that the sleep logs should be ‘maintained in an up-to-date state on a daily basis’. It also stated:
The sleep to be recorded is any sleep. That means dozing for ten minutes to a sleep break of five hours. The period that is recorded is entirely up to you, for example if you wake up and make a toilet visit this period should not be detracted from the sleep period. On the other hand, if you are lying in bed with your eyes closed and your mind in neutral that should not be recorded as sleep …
The sleep log tool provided some additional guidance. It instructed pilots to record times as duty from ‘notice to move’ (for a flying task) until back in resting accommodation (after a flying task), and record flight times using the engine operating time from the helicopter flight log, rounded to the nearest full hour.
The sleep log pre-loaded the hours of 2200–0600 each day as sleep, and pilots had to overwrite these times if they intended to record them as awake (blank), duty or flying.
When data was being entered, the sleep log automatically highlighted cells in various colours if a relevant rule was breached. More specifically:
- If a pilot recorded less than 5 hours sleep in the 24 hours prior, or less than 12 hours sleep in the previous 48 hours, cells would highlight red.
- If a pilot recorded being awake for more than the sleep in the sum of the previous 24 hours and 48 hours, cells would highlight orange (see also later this section).
- If a pilot recorded 9 or more hours consecutive duty, the 13th and subsequent hours after the start of the duty period would highlight yellow.[48]
Figure 20 shows 2 examples of simulated sleep and work information recorded in the sleep log. In the top image, the pilot recorded 4 hours sleep in the 24 hours to 0600 on 21 March, and 10 hours in the 48 hours to that time. As a result, all cells after 0600 highlighted red. In the bottom image, the addition of 1 hour sleep between 0600 and 0600 removed the red alerts, since the pilot now had recorded 5 hours sleep in the previous 24 hours.
Figure 20: Exemplar sleep log

Using simulated data, the ATSB observed that the sleep log tool was highly transparent and easy to modify. When entering sleep, duty and flying into the sleep logs, it was obvious when a rule had been breached or would be breached. Similarly, it was obvious what a pilot could do to change the recorded data to remove or prevent cells being highlighted.
The ATSB also determined that the rule embedded in the sleep log associated with extended wakefulness (and orange highlighting) contained a coding error; it counted both the sleep in the previous 24 hours and the total sleep in the previous 48 hours, and therefore it double-counted sleep in the period 25–48 hours prior to the relevant point in time. As a result, a pilot sleeping 8 hours a night would need to be awake for over 24 hours before this rule identified a fatigue risk, whereas the intended function of the rule was to identify fatigue risk after 16 hours. In other words, it was very unlikely that pilots could trigger an orange alert when entering in their normal range of sleep and other times.
Review of data in sleep logs
Sleep log information recorded by pilot under supervision
The ATSB reviewed the sleep log information recorded by the pilot under supervision and compared it to other information, including phone records and the operator’s building access records. Table 10 shows the sleep and duty times reported by the pilot under supervision in their sleep log for the period 8 March to 14 March 2018. Table 10 also shows times where the ATSB identified the pilot was probably sleeping and working, based on other sources of information.
The recorded sleep times were considered accurate unless other information indicated that the pilot was not asleep. However, it is noted that recorded sleep times are in 1-hour blocks, and sleep could have commenced any time within the first 1-hour block and ceased any time within the last 1-hour block.
Table 10: Pilot under supervision recorded sleep log and related information (click for larger image)
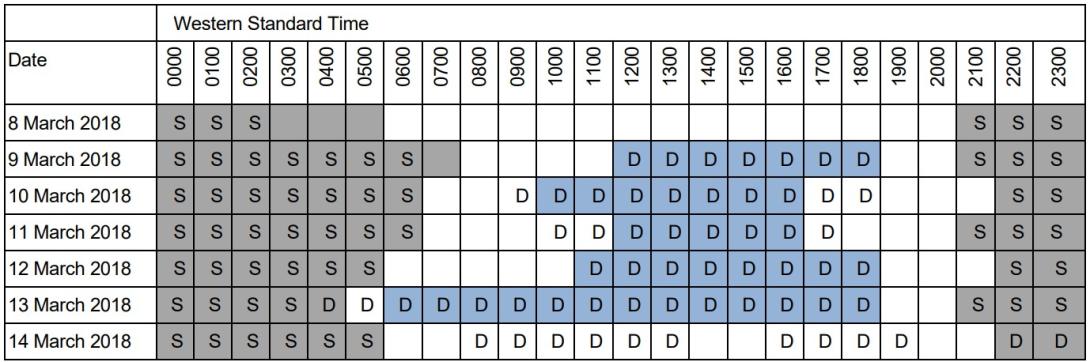
Colour-shaded cells show sleep and wake recorded by the pilot under supervision. Periods of sleep are shaded grey, periods of work (including flying) are shaded blue and other periods of wakefulness are shaded white. The pilot under supervision did not record any work for 14 March and the reported sleep time probably reflected the sleep log pre-filled sleep periods. Text-filled cells show the times of sleep and work determined by the ATSB based on various sources. Periods of potential sleep are shown by the letter ‘S’, and work-related duty are shown by the letter ‘D’.
The pilot under supervision commenced recording data in the sleep log for the night of 8 March (after arriving at Port Hedland). The most notable anomaly between the recorded times in the sleep log and other information occurred on 13 March. The pilot recorded sleeping until 0500, before working from 0600 to 1800. However, building access records showed the pilot arrived at work at 0417 and would have awoken before 0400. Text messages indicated the pilot left work at 1820.
The pilot under supervision’s sleep log showed recorded sleep from 2100 on 13 March until 0600 on the day of the accident, with no entries for duty that day and sleep recorded from 2200 that night. This was consistent with the pre-loaded default hours of sleep. It is probable the pilot did wake at about 0600 given text messages sent that morning and had not yet updated the sleep log during 14 March. The pilot under supervision was doing additional work for an assessment during the day on 14 March (included in Table 10). There was probably additional study on the night of 12 March, but this has not been included in the table as the time involved is unknown.
Given the sleep recorded on the 12, 13 and 14 of March, had the sleep logs been configured correctly for the PSWR extended wakefulness rule, any non-sleep times after 2200 on 14 March would have produced an orange alert. As the pilot had not removed the pre-loaded default sleep from the night of 14 March, no alert would have been produced even if the sleep log tool had been coded correctly.
Sleep log information recorded by instructor
Sleep log information recorded by the instructor was also compared to other sources of information (Table 11). The instructor’s phone records showed several calls made and messages sent during the hours recorded as sleep, and the building access records showed a number of instances where the instructor was at work after the reported duty finish time. Overall, this showed the instructor probably obtained less sleep and worked more than was recorded in the sleep log.
Table 11: Instructor recorded sleep log and related information
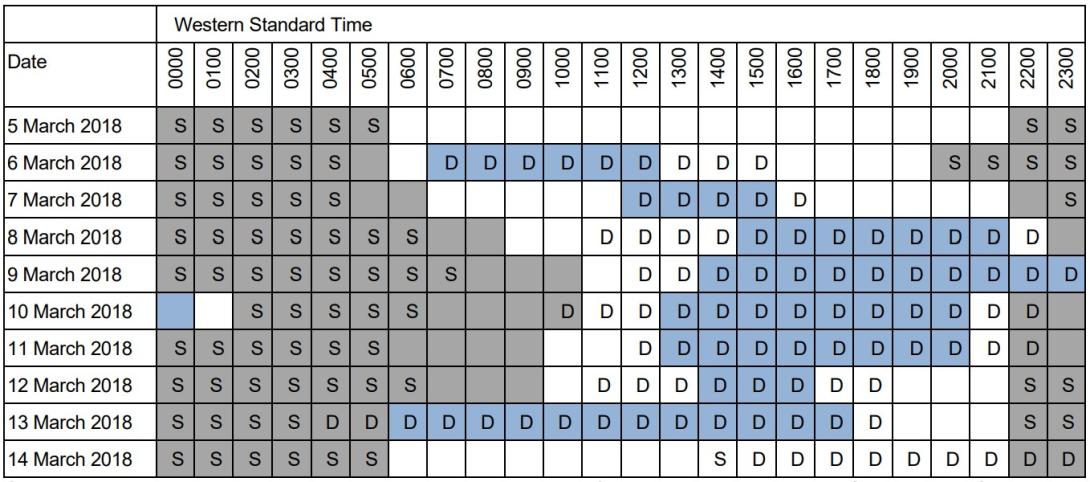
Colour-shaded cells show sleep and wake recorded by the instructor. Periods of sleep are shaded grey, periods of work (including flying) are shaded blue and other periods of wakefulness are shaded white. Text-filled cells show the times of sleep and work determined by the ATSB based on various sources. Periods of potential sleep are shown by the letter ‘S’, and periods of work are shown by the letter ‘D’.
On the nights starting 8, 10 and 11 March, the instructor recorded a period of 12 hours sleep[49] and on the night of 7 March recorded a period of 11 hours sleep. Available information from phone records indicated that the instructor woke significantly earlier than recorded on these and other days. More specifically, on the 5 nights of 7 to 11 March, the recorded sleep period extended until 0900, 1100, 1100, 1000 and 1000, and phone records indicated the instructor was awake at 0630, 0900, 0700, 0600 and 0700 respectively. On another trip to Port Hedland in January 2018, the instructor recorded one period of 14 hours sleep and one period of 16 hours sleep. On each of these occasions phone records indicated the sleep period was much less than recorded.
As with the pilot under supervision, there was inconsistency between the sleep log and other information on 13 March. The instructor reported sleeping to 0600 then working from 0600 until 1800. However, building access records showed the instructor entered the operator’s premises at 0430 and remained at work until at least 1917, longer than the 1800 recorded. The instructor had not yet recorded any information in the sleep log for 14 March.
The analysis of the instructor’s activities was complicated due to the nature of some of the recorded phone information. There were instances of very long phone calls between the instructor and their partner, including late at night. For example, one recorded phone call started at 1907 on 12 March and ended at 0400 on 13 March. The ATSB asked the instructor (in late 2020) about the long phone calls. The instructor explained that, around the time of the accident, they sometimes fell asleep while on the phone with their partner. Although unable to recall if this had occurred on 12 March, the instructor said they would not have gone flying if awake all of the previous night. For the purpose of fatigue analysis, the ATSB assumed the phone call on the night of 12 March ended prior to the instructor’s recorded sleep time start of 2200.[50]
Information recorded by other pilots
The ATSB reviewed the sleep logs completed by the operator’s other pilots based at Port Hedland from late 2017 through to the date of the accident (14 March 2018). There were no instances of pilots recording flight or duty times when the sleep logs identified a fatigue risk (that is, there were no flight or other duties reported in highlighted cells).
The ATSB recalculated the data for the extended wakefulness rule, to correct the coding error in the sleep log tool. After this correction, there were 55 instances of pilots reporting either flying or other duties when they had been awake for longer than the sum of their recorded sleep in the prior 48 hours.
The ATSB compared the sleep, work and rest times reported by pilots with other information about pilots’ probable activities. Operational records from the company’s 2 helicopters showed which pilot flew each flight and building access records showed when each pilot opened doors to the operator’s premises at Port Hedland. This analysis showed pilots recorded sleep on their sleep logs when they could not have been sleeping. Excluding data associated with the pilot under supervision and the instructor:
- There were 32 instances when a recorded sleep period significantly overlapped (greater than 10 minutes) with times the pilots were recorded entering the operator’s premises. Of these, 7 instances involved a probable sleep loss of 1 hour or more, and the maximum sleep loss was 8 hours.
- There were 11 instances of pilots recording a sleep period when flight records showed they had been flying a helicopter.
- There were 23 instances involving 6 different pilots where a continuous period of 12 or more hours sleep was recorded.
If the pilots had not recorded these periods as sleep, in some instances the sleep logs would have highlighted subsequent duty times as being a fatigue risk. In other instances, no fatigue risk would have been identified due to the problem with the coding of the extended wakefulness rule.
The ATSB did not obtain phone records of the operator’s pilots, apart from the 2 pilots involved in the accident. It is possible that there were other instances of sleep misreporting that were not identified in the building access and operational records.
The ATSB reviewed pilot rosters for March 2018 and compared the rostered shifts with the times of duty and non-duty recorded in the pilots’ sleep logs. This showed that pilots sometimes worked during their standby days. The sleep logs also showed that pilots often recorded having sleep during the first few hours of a rostered shift, finished duty prior to the end of the rostered shift, or obtained a mid-shift nap, presumably depending on the operational requirements as dictated by the shipping schedule. It was unusual for pilots to record 12 hours of consecutive duty
Pilot self-assessments of fatigue
The FRMS manual stated that pilots should self-assess their levels of fatigue and:
If when asked to perform duty a flight crew member feels that he is unable to do so in that he does not comply with the standards set out in this FRMS or he does not feel rested enough to undertake duty he is to inform the tasking officer of the situation. In doing so he is to recognise that his decision is totally supported by the CEO [chief executive officer] in that it complies with the procedures of the FRMS.
In addition, pilots were required to record self-assessments of fatigue in the Excel file (in a separate spreadsheet to the sleep log). These evaluations were based on a scale from 0% to 100%, as summarised in Table 12. They were required to be completed at the end of a shift (termed a ‘mission’ in the sleep log).
Table 12: Fatigue ratings used in sleep logs
|
Fatigue evaluation |
Description |
|
0% |
Just awake and well rested |
|
>33% |
Tired but feel ok to take on a new mission |
|
>66% |
Too fatigued to accept another mission. Assessed as bearing too much risk on fatigue related errors. |
|
100% |
Dead tired. Very fatigued. Need sleep. |
Following the duty on 13 March, the instructor reported a fatigue rating of 60%, which was higher than recorded on previous days (previous highest being 40%). The pilot under supervision reported a rating of 30%, higher than the 10% recorded for all previous days. The instructor and the pilot under supervision recorded duty periods of 11.8 and 12.0 hours, respectively, however both records substantially understated the times the pilots were at work.
Between December and March 2018, there were several instances of pilots recording ratings of 70 to 90%. However, as these were recorded at the end of their shifts, the operational meaning of such ratings was unclear (as the pilots would not generally be assigned any additional tasks after the end of their assigned shift).
Fatigue occurrence reporting and monitoring
The FRMS manual stated:
A flight crew member is to inform the Chief Pilot of his inability to undertake duty because of illness, fatigue or because he has not met the requirements of this system…
In other words, if a pilot felt fatigued, they were to advise the chief pilot. In addition, if they had recorded less sleep than required by the PSWR, they were to inform the chief pilot and they were also, under the FRMS, ‘not available to undertake duty’.
In simple terms, if a pilot had a red or orange alert in their sleep log, they were not able to fly or conduct duty during that time. If this occurred, the chief pilot was required to ‘find a suitable flight crew member who can perform the duty, pass the task to another operator or cancel the task’.
The FRMS manual did not provide any allowance for exceedances of the PSWR and there was no guidance regarding types of mitigators to consider for different types or levels of exceedance of the PSWR.
The FRMS manual stated that the chief pilot was responsible for continually monitoring the operation of the FRMS, and was to ‘review and initial pilots’ sleep logs and flight and duty records at least once per week’. There were no records of any such review and approval having been conducted.
The FRMS stated that pilots should submit fatigue occurrence reports to the chief pilot after an ‘adverse event’, so the chief pilot could review factors such as recent sleep. The ATSB sought records for the operator for fatigue occurrence reports during 2016–2018. There was one report, which was submitted in September 2016 and related to a pilot based in Mackay being unable to achieve sufficient rest. This report was closed in January 2017 with no action taken. There was no indication in the records for this event that there were factors in common with the accident involving VH-ZGA.
Pilot perceptions of the roster and use of sleep logs
During discussions with the ATSB after the accident, some of the operator’s pilots expressed their opinion that the sleep logs were an insufficient tool that did not accurately capture fatigue risk. Pilots felt that a key deficiency in the sleep logs was how easy the system was to manipulate. Pilots could see in real-time the effects of adding and removing periods of sleep and duty, and therefore it was easy to identify how to prevent fatigue alerts (or violations of the PSWR) from being generated in the logs.
Several pilots described perceiving implicit and explicit pressures to adjust the data they recorded in sleep logs to prevent any fatigue alerts. One pilot told the ATSB that if they submitted a sleep log showing a fatigue alert, the chief pilot would tell them to ‘make it work’. Another pilot described adjusting their sleep log to appease management and described an anecdote of another pilot being pressured to do the same. Other pilots described similar implicit and explicit pressures for adjusting their sleep logs to prevent fatigue alerts, including feeling that if they reported as unfit for duty they could lose their jobs.
Some of the operator’s pilots told the ATSB they perceived that the line pilot roster at Port Hedland created difficulties for achieving sufficient restorative sleep. Pilots described finding it difficult to sleep following the end of a night shift at 0600, particularly later in the morning and into the early afternoon. Pilots said that they were sometimes only able to achieve a couple of hours sleep in these situations but reported longer sleeps in the sleep logs to avoid generating fatigue alerts. The pilots said that if they recorded their actual sleep following these night shifts, the sleep log would show fatigue alerts towards the end of a subsequent night shift (in cases where they were required to work 2 night shifts in a row due to limited pilot availability).
Some pilots also believed the fatigue (mission) evaluations were of limited value, explaining that they found it very difficult to put a percentage figure on their level of fatigue. These pilots perceived there was an expectation that they would ensure their self-assessed fatigue was below the threshold 66% value.
The chief pilot (at the time of the accident) advised the ATSB that pilot concerns about the operator’s rostering pattern related to comparisons with the pattern used by previous operator at Port Hedland. The pilots who had been employed by the previous operator wanted to return to a 12-12 (midnight to midday/midday to midnight) roster and the previous fatigue management system (using FAID, see next section). However, this was not compatible with the new operator’s systems, which continued to be utilised.
After 12 months, the new operator was going to trial 12-12 rosters and turned on the FAID function of the flight management software to evaluate it. The chief pilot advised the ATSB that, before the trial, pilots were required to operate in accordance with the operator’s FRMS and that was the context for telling pilots ‘to make it work’. The chief pilot advised that pilots were not pressured (implicitly or explicitly) to adjust their sleep logs or given any indication that they could lose their jobs if they were fatigued.
The chief pilot advised that they did an evaluation of the 12-12 roster and noted various concerns, including:
- If pilots did not get any significant sleep before midnight, they were rostered until midday, working in the Port Hedland heat.
- Every flying shift was within the core hours of sleep 2200–0600.
- With the existing roster, the pilots were doing a normal day shift, then a night shift finishing at 0600, then a day off. This seemed to be less fatiguing than every shift within the core hours of sleep.
- Towards the end of the shift, the pilots would have been operating in the window of circadian low. If they were doing 12-12 they still would have been operating within this period but with sunrise and morning heat to work through.
Use of a biomathematical model of fatigue
A biomathematical model of fatigue (BMMF) uses mathematical algorithms to predict the effect of different patterns of work on measures such as subjective fatigue, sleep or the effectiveness of performing work. Each model uses different types of inputs and produces different types of outputs, and each model is based on many assumptions and has limitations. The models are designed to be one element of a system for evaluating and comparing work rosters (see Civil Aviation Safety Authority 2014, Dawson and others 2011, Gander and others 2011).
Many transport organisations include a BMMF as part of their FRMS, and the FAID [51] BMMF has been widely used in the Australian rail and aviation industries since the early 2000s. It uses hours of work (start time and end time) as its inputs, and it produces a score based on an algorithm that considers the effects of the length of the duty periods, time of day of the duty periods, and the amount of work over the previous 7 days (Roach and others 2004). The higher the FAID score, the higher the potential for fatigue.[52]
The operator’s FRMS did not include the use of a BMMF to evaluate roster patterns or recorded duty times. However, pilots reported that, up until a few months prior to the accident, the operator provided them with access to FAID scores associated with their recorded duty times and predictions for future shifts. Some pilots advised the ATSB that they believed the FAID scores provided them with a more objective indication of fatigue risk, and were less easy to manipulate, than the sleep and duty times recorded in the sleep log.
Some pilots recalled some FAID scores showed a high level of fatigue exposure associated with the Port Hedland roster, particularly when there was reduced pilot numbers. These pilots told the ATSB that access to the FAID scores was removed when concerns about the scores and the implication of excessive fatigue associated with the roster were brought to the attention of the operator’s management.
The operator advised that access to FAID was provided for ‘comparison information to test relevance of predicted work practices ...’, which some of the Port Hedland pilots were requesting. The operator rejected the implication that removal of FAID was intended to hide fatigue risk.
The ATSB used FAID to analyse a standard Port Hedland pilot roster (including a 12-hour day shift, a 12-hour night shift and then 2 days with no duty assigned over multiple weeks). This analysis predicted a FAID score of 79 towards the end of each night shift, with the scores being above 60 from about 0300 each night shift and above 70 from about 0430 each night shift.[53] This analysis assumed a pilot was on duty for the full length of their shifts (which would be very rare), and it also assumed that a pilot was not allocated work tasks on their standby day (which occurred to some extent).
The ATSB conducted further FAID analysis using the reported hours of duty from all line pilots based at Port Hedland during March 2018, which incorporated self-reported napping and shift start and finish times as recorded in the sleep log. With one exception, this analysis did not indicate that there were systemic issues in the fatigue exposure associated with the patterns of work of the line pilots.
In October 2021, the ATSB received documents relating to the operator’s application for CASA approval of an FRMS trial under CAO 48.1 Instrument 2019. These documents included a ‘scientific safety case’, which stated
Recently, a whole year of flight duty and flight time data were subjected to analysis for the Gladstone and Port Hedland operations ... For the Port Hedland operation there was a median of 4 flights per flight duty period and a total of 2.99hrs of actual duty time (including all flight time and an allowance for daily pre-flight and end of shift activities).
These flight and duty data were subjected to bio-mathematical modelling using the FAID Quantum software. Across both datasets there were no instances of a FAID score greater than 60 in either operation, suggesting an overall low level of inherent fatigue-related risk. The FAID Quantum model indicated that for less than two percent of duty periods flight crew were predicted to have obtained less than five hours sleep in the prior 24 hours. This predicted exposure to instances of restricted sleep is less than observed in datasets from objective monitoring of flight crew internationally and again demonstrates an inherently low level of fatigue-related risk.
The ability to obtain sleep during the 12-hour duty periods is an important consideration that significantly lowers the inherent risks associated with long duty periods, especially at night. Within the Heli-Aust Whitsundays operation, all flight crew have access to suitable sleeping accommodation when on duty, and evidence suggests that this is utilised during breaks between taskings.
The ATSB notes that the duty times included in this analysis were only associated with flying activities and did not include other duty. The analysis was also based on duty times from a different period of time and may not have reflected the situation that existed in March 2018.
FRMS internal reviews
The FRMS manual stated that the chief pilot should produce a written review of the FRMS every 12 months. The ATSB sought records of internal reviews of the FRMS over the period 2016–2018; the operator advised that no review had been conducted.
Records from the operator’s safety meetings noted the following:
- In October 2017, concerns were raised about the consistency of pilots recording of duty times across the helicopter records, Air Maestro and the sleep logs.
- In December 2017, the deputy chief pilot noted that they had received feedback about the duty period and sleep cycle ‘one pilot is following’ and stated that they had adjusted the roster and would continue to monitor. The deputy chief pilot also said that ‘pilots are reminded that if they are fatigued, then they should not fly and ensure they notify the General Manager’.
- In January 2018, the deputy chief pilot said the operator was trialling a new roster at Port Hedland.
- In February 2018, the chief pilot noted ‘Fatigue concerns with the roster for Port Hedland was closed out and has now reopened due to ongoing feedback. A risk assessment is being carried out on the current PH roster.’
The ATSB sought clarification from the operator about the roster trial and risk assessments alluded to in the safety meeting minutes from early 2018. The operator advised that, although there was consideration of a roster pattern of shifts starting at 0000 and 1200, no trial was commenced.
Other occurrences
Introduction
As a standard practice, ATSB investigations research other occurrences with similar themes as a reference for analysis and, in particular, identification of risk factors and assessment of safety issues. A search for this type of occurrence – inadvertent descent during a visual approach at night in a degraded visual (cueing) environment (DVE) involving a helicopter – did not yield any results in the ATSB database.
The ATSB has investigated occurrences involving VFR operations at night in a DVE, including the loss of control involving AS355F2 (Twin Squirrel), VH-NTV, in outback South Australia on 18 August 2011.[54] During departure, the pilot became spatially disoriented[55] for reasons that included workload and absence of an autopilot. Following this event, CASA enhanced guidance for night VFR operations and required an autopilot or second pilot for air transport operations at night.
Three occurrences outside of Australia, detailed below, were identified that featured a visual approach or visual element of an instrument approach in a DVE. Although these were 2-crew IFR operations and 2 involved larger helicopters, the same hazards were present in the operating environment.
Nova Scotia, Canada Sikorsky S-92A
The Transportation Safety Board of Canada (TSB) investigated an inadvertent descent during a visual approach involving a Sikorsky S-92A on 24 July 2019 in the Nova Scotia region. This was a 2‑pilot operation under the IFR carrying 11 passengers from Halifax to a fixed offshore facility. The following information is adapted from TSB safety investigation report A19A0055. Instrumental to the investigation was data recovered by the TSB from multi-purpose flight recorders (including voice), health and usage monitoring system, and flight management system computers. This data was integrated with ADS-B and satellite-based flight-following services.
On arrival at the facility the crew attempted 2 instrument approaches, but low cloud and poor visibility prevented a landing. During the second missed approach, the flight crew exited cloud at about 300 ft and sighted the helideck above the fog layer. The crew levelled at 500 ft and after assessing the conditions manoeuvred for a visual approach.
The helicopter rolled out on final approach 0.6 NM (1.1 km) from the facility at 500 ft, which was above the cloud layer with forward visibility of about 5 km. Shortly afterwards, the pilot flying disengaged altitude hold and held the cyclic trim release button to manually fly the approach. At about the same time the pilot flying lowered the collective to descend. (The angle to the helideck was 7.1°, which was steeper than the company’s standard 4.7° approach angle.)
As the approach progressed, the pitch attitude increased to 17°, the airspeed decreased below 40 kt, and the rate of descent was 670 ft/min and increasing. Although the pilot monitoring called the pitch attitude through 15°, neither pilot was aware of the increasing rate of descent, low engine torque setting, or increasing sideslip.
By 250 ft, all forward motion had been lost and the rate of descent was 1,200 ft/min and increasing with a large sideslip angle (lateral groundspeed of 18 kt. The pilot flying realised the helicopter was getting low and applied moderate then high engine torque. At the same time the rate of descent increased to 1,800 ft/min and helicopter descended below helideck elevation (174 ft). Both pilots recognised the helicopter was in fog and a go-around was initiated.
As the helicopter descended through 100 ft the water was sighted and by 70 ft the collective was raised to the full up position. A significant over-torque occurred accompanied by low main rotor RPM (with alert) and when the helicopter was at 40 ft it yawed uncontrollably to the right for 2 rotations. Due to the low rotor RPM, the main generators dropped offline and various electrical systems including the AFCS and some flight displays were depowered.
The crew arrested the descent within 13 ft of the water in reduced visibility due to fog.
Under control of the captain, the helicopter was then climbed and accelerated with high power settings and increasing main rotor RPM. The helicopter reached 1,350 ft then began descending and accelerating while the crew were trying to engage the AFCS. Initially unnoticed by the crew, the airspeed increased to 148 kt while descending through 650 ft at 1,700 ft/min. This descent was arrested at about 500 ft and the helicopter climbed for a return to Halifax where conditions would allow a visual approach.
Of the 18 findings issued by the TSB, the following were of particular relevance:
[The operator’s] standard operating procedures provided flight crew with insufficient guidance to ensure that approaches were being conducted in accordance with industry-recommended stabilized approach guidelines.
The pilots experienced attentional narrowing due to increased workload while attempting a non‑standard offshore visual approach in a degraded visual environment. This led to a breakdown in the pilots’ instrument cross-check, which prevented the timely recognition that the approach had become unstable.
Depressing and holding the cyclic trim release button, while operating in a degraded visual environment, increased pilot workload and contributed to control difficulties that resulted in an unstable approach that developed into vortex ring state.
If manufacturers’ flight manuals and operators’ standard operating procedures do not include guidelines for the use of the cyclic trim release button, it could lead to aircraft control problems in a degraded visual environment due to the sub-optimal use of the automatic flight control system.
Prerow, Germany BK117
The German Federal Bureau of Aircraft Accident Investigation (BFU) investigated an accident during night hoist training to a sea rescue vessel at sea near Prerow, Germany, involving a BK117 C-1 helicopter on 28 February 2014. This was a 2-pilot operation under the night VFR with a hoist operator and emergency physician onboard. The following information is adapted from BFU investigation report 3X006-14.
The sea rescue vessel was a relatively small ship with minimal lighting and there was no cultural lighting in the vicinity. It was a dark night due to light rain and no moonlight.
On arrival, the first approach was terminated because of low visibility and late identification of the ship. The co-pilot (in the left seat) then conducted a tight left circuit to the ship. That circuit and all of the subsequent manoeuvring in the vicinity of the ship was conducted manually.
After 3 hoist exercises to the ship were completed, the pilot in command (in the right seat) flew away from the ship and conducted a left circuit for another approach. During the approach the crew lost sight of the ship and by the time it was resighted the helicopter had inadvertently climbed. The pilot in command discontinued the approach and manoeuvred for another left circuit at 500 ft.
Based on directions from the co-pilot, the PIC turned onto base, decelerated, and descended. As the helicopter descended through 150 ft with an airspeed about 35 kt, the co-pilot advised the PIC to turn. The PIC called ‘150’ and at the same time the radio altimeter annunciated ‘decision height’ (pre-selected to 100 ft). The co-pilot acknowledged ‘150’ then the PIC called ‘100’ followed by an exclamation from the hoist operator. Within 3 seconds the helicopter impacted the water. The co-pilot was the only survivor.
The helicopter was equipped with a combined cockpit voice recorder (CVR) and flight data recorder (FDR). A plot of the FDR data showed that in the 20-second period before impact, the airspeed reduced from about 45 kt to less than 10 kt while the aircraft turned through 60° and descended 200 ft.
The BFU identified the following factors as immediate causes:
- little experience of the crew regarding the applicable procedures at night over sea
- the approach deviated from the described approach procedure
- in regard to the altitude, the airspeed, and the rate of descent, the approach was not stabilised
- the descent was commenced prior to being on final approach and without visual contact with the ship
- insufficient monitoring of the flight instruments
- loss of situational awareness in combination with loss of control
- non-reaction to visual and audio altitude warnings of the radio altimeter.
The BFU also identified 6 systemic causes including:
- insufficient company specifications for the use of the flight attitude stabilising functions of the autopilot system during approaches and departures and in traffic circuits above sea
- lack of go-around criteria for a non-stabilised approach
- lack of aviation regulations for offshore helicopter flight operations in Germany
- insufficient assessment of the operator’s procedures by the responsible supervising authority.
Based on the operator’s implemented and planned safety actions, the BFU refrained from issuing safety recommendations to the operator. When the report was published in March 2016, the following safety recommendation (BFU 25/2015) was still in effect:
The LBA (German Civil Aviation Authority) should ensure that Operators conducting VFR-Night approaches to sparsely lit landing sites should specify practical and detailed procedures in their handbooks that are appropriate to the special demands of this type of operation, and which specify systematic, consistent and comprehensive use of the resources available to the conduct of the flight.
Sumburgh, United Kingdom Super Puma
The United Kingdom (UK) Air Accidents Investigation Branch (AAIB) investigated an accident during an instrument approach in the Shetland Islands region of Scotland involving a Eurocopter AS332 L2 Super Puma on 23 August 2013. This was a 2‑pilot operation under the instrument flight rules carrying 16 passengers from an offshore platform in the North Sea to Sumburgh Airport for a refuelling stop. The following information is adapted from AAIB aircraft accident report 1/2016.
On arrival at Sumburgh, the crew conducted a non-precision approach in cloud that at the airport was reported to have a base of 300 ft with reduced visibility in mist. The approach was flown with the autopilot in 3-axes with vertical speed (V/S) mode, which required the pilot flying to operate the collective pitch control manually to control the helicopter’s airspeed. The role of pilot not flying was monitoring the helicopter’s vertical flight path against the published approach vertical profile and seeking the external visual references necessary to continue with the approach and landing.
The procedures permitted the crew to descend to a height of 300 ft, the minimum descent altitude (MDA) for the approach, at which point a level-off was required if visual references had not yet been acquired.
Although the approach vertical profile was maintained initially, insufficient collective pitch control input was applied by the pilot flying to maintain the approach profile and the target approach airspeed of 80 kt. This resulted in insufficient engine power being provided and the helicopter’s airspeed reduced continuously during the final approach. Control of the flight path was lost, and the helicopter continued to descend below the MDA. During the latter stages of the approach the helicopter’s airspeed decreased below 35 kt and a high rate of descent developed.
The decreasing airspeed went unnoticed by the pilots until a very late stage, when the helicopter was in a critically low energy state. The pilot flying’s attempt to recover the situation was unsuccessful and the helicopter struck the surface of the sea approximately 2 NM (3 km) west of Sumburgh Airport. It rapidly filled with water and rolled inverted but was kept afloat by the flotation bags which had deployed. Four of the passengers did not survive.
Of the 6 causal and contributory findings issued by the AAIB, the following were relevant:
The helicopter’s flight instruments were not monitored effectively during the latter stages of the non‑precision instrument approach. This allowed the helicopter to enter a critically low energy state, from which recovery was not possible.
The operator’s SOP for this type of approach was not clearly defined and the pilots had not developed a shared, unambiguous understanding of how the approach was to be flown.
The operator’s SOPs at the time did not optimise the use of the helicopter’s automated systems during a Non-Precision Approach.
The AAIB advised that the commander’s decision to fly the non-precision approach using a reducing airspeed meant that there were 2 parameters changing during the approach. These were: a) the vertical speed, controlled through the autopilot, and b) the airspeed, controlled through manual collective pitch adjustment. This method increased the risk that any significant period of inattention to either parameter would lead to an undesired approach profile.
In relation to the finding that the appropriate flight instrument displays were not being monitored adequately in the latter stages of the approach, the AAIB advised that improved pilot training may be beneficial, and several research projects have been undertaken which have identified a need for revised training in pilot instrument scan techniques.
A number of recommendations were issued by the AAIB to address safety issues associated with the findings and other themes such as provision of operational information, flight data monitoring, helicopter terrain awareness warning systems (HTAWS), onboard image recording, and survivability.
Research and additional occurrences associated with night operations
Research has shown that pilots engaging in simulated ship-borne landing operations experienced significantly degraded visual cues during night conditions, with a reduced ability to make corrections to attitude and horizontal and vertical translational rates. Pilots experienced higher workload and more control inputs were needed to perform the task than in good visual conditions (Wang and others, 2013).
Perceptual difficulties posed by navigation to single-source maritime lights have also been described in investigations of accidents involving night approaches to oil platform helidecks. Excerpts from these include:
- A difficulty which is relevant to approaches to platforms and ships at night, is that these may be the only light source in an otherwise totally dark environment. A single light source phenomenon has long been recognised by the aviation community as one which contributes nothing to the pilot's judgement of distance. …The usual effects of this phenomenon are that the pilot is deprived of the visual cues normally associated with daylight vision. These are: the relationship of the object to the horizon; the relationship to other objects and the surface texture between the aircraft and the object in view, and the use, for ranging, of the angle subtended at the viewer's eye by the object, because: (a) the absolute size of the object is uncertain, and (b) the judgement of this angle when it is very small is difficult.[56]
- In dark, overcast conditions, it is likely that some cues were degraded or absent. For example, without a distinct horizon the assessment of pitch attitude and approach angle (by reference to the depression of the deck below the horizon) would be compromised. Without textural cues in the ground plane (in this case the sea surface), judgement of pitch attitude and approach angle by inference from textural perspective would also be compromised, as would the appreciation of the range to the deck. The illuminated deck would have provided limited cues to roll attitude and, by reference to its apparent size, to range. The crew’s judgement of range and rate of closure to the platform would have improved as they approached the platform, but, initially, this would be relatively insensitive.[57]
Survival aspects
Helicopter underwater escape training
Helicopter underwater escape training (HUET) has been in use around the world since the 1940s and is considered best practice in the overwater helicopter operating industry. HUET is designed to improve survivability after a helicopter ditches or impacts into water. Research of such accidents has shown that occupants who survive the initial impact will likely have to make an in-water or underwater escape, as helicopters usually rapidly roll inverted post-impact due to the position and mass of the engine/s, transmission and main rotor system. The research has also shown that drowning is the primary cause of death following a helicopter accident into water.
Fear, anxiety, panic and inaction are the common behavioural responses experienced by occupants during a helicopter accident. In addition to the initial impact, in-rushing water, disorientation, entanglement with debris, unfamiliarity with seat belt release mechanisms and an inability to reach or open exits have all been cited as problems experienced when attempting to escape from a helicopter following an in-water accident.[58]
HUET involves a module (replicate of a helicopter cabin and fuselage) being lowered into a swimming pool to simulate the sinking of a helicopter. The module can rotate upside down and focuses students on bracing for impact, identifying primary and secondary exit points, egressing the wreckage and surfacing. HUET is normally part of a program of graduated training that builds in complexity, with occupants utilising different seating locations, exits and visibility (via the use of ‘blackout’ goggles). This training is conducted in a controlled environment with safety divers in the water.
HUET is considered to provide individuals with familiarity with the crash environment and confidence in their ability to cope with the emergency situation.[59] Interviews with survivors from helicopter accidents requiring underwater escape frequently mention they considered that HUET was very important in their survival. Training provided reflex conditioning, a behaviour pattern to follow, reduced confusion, and reduced panic.[60]
Like other highly procedural and complex skills, if underwater escape is infrequently practiced, skill decays rapidly.[61] In a UK Civil Aviation Authority (2014) safety review of offshore public transport in helicopters for the oil and gas industries, it was noted that although the frequency of refresher HUET is presently every 4 years in the UK, this is widely regarded by experts as being inadequate.[62]
In Australia, CAO 95.7.3 required all flight crew engaged in MPT operations in single-engine helicopters to have completed a HUET course. The CAO had no requirement for recurrent training and there was no regulatory requirement for multi-engine flight crew conducting MPT to complete HUET.
CASA advised the ATSB that updates to CAO 95.7.3 (made in 1992) were delayed a number of years in anticipation of new flight operations regulations that eventually became effective in December 2021. According to CASA, in the intervening period, it assessed the operations manual content of operators who conducted overwater operations to assess how effectively they were addressing the risks associated with the operation. If required, CASA could issue directions to an operator utilising CAR 215 or an operator could elect to include those requirements in its operations manual.[63]
Operator HUET requirements
Part 4 of the operator’s operations manual (Training and Checking) required all pilots engaged in overwater (offshore) operations to have completed a HUET course with an approved provider during the previous 3-year period. The manual indicated that the chief pilot could extend that period for an individual pilot if circumstances arise which preclude that training being done within the 3-year period. In that situation, the period of extension was to be specified at the appropriate time and would normally not exceed 6 months. The training was to be rescheduled as soon as practicable and a note was required to be made in the pilot’s records.
The pilot under supervision had last completed HUET in May 2011, which was outside the operator’s 3-year recurrent training period. On 6 March 2018, the operator’s chief pilot booked a HUET course for the pilot under supervision but did not make any note of the extended interval in the pilot’s records. The training, scheduled for 24 April 2018, was a full-day course with a Brisbane-based training provider.
The chief pilot reported that there was pressure from the operator’s management to replace a pilot (assigned to Port Hedland) that had recently resigned. As the chief pilot considered this was not a normal circumstance, and the operations manual allowed for an extension (not normally more than 6 months), the chief pilot applied the extension until the next available HUET course. (This was equivalent to an extension of 3 years and 11 months.)
The instructor had completed HUET within the last 3 years. The operator also provided the ATSB with records of HUET course information for 24 other company pilots, all of who had completed their HUET training within the required period.
There were also procedures included in Part 3 of the operator’s operations manual (Aerodromes and Routes) that specified HUET requirements for various bases. At the operator’s Hay Point base, a HUET course was required every 2 years, but could be extended to 3 years at the discretion of the chief pilot. Other bases included the requirement for a HUET course before conducting night transfers of marine pilots but specified no other requirements in terms of recurrency or training requirements for day operations. The operations manual required all pilots and marine pilots at the Port Hedland base to have completed a HUET course before conducting night transfers.
The conflicting information contained in the operations manual had potential to confuse personnel as to the operator’s requirements for HUET. That ambiguity could result in a situation where personnel were complying with the requirements contained in one part of the operations manual, but inadvertently breaching a requirement contained in another part of the manual.
Emergency breathing systems
Underwater escape from a flooded cabin is a recognised hazard after an accident or ditching on water and where the cabin becomes submerged. In that situation, occupants of the helicopter typically have a very short timeframe to complete the necessary actions to assure their survival. Those actions include orientating themselves in the cabin relative to their emergency exit pathway, correctly operating and opening the emergency exit, releasing their seat belt, escaping cabin and swimming to the surface.
The time available to escape a flooded cabin can be extended using a compressed air emergency breathing system (EBS). These systems vary in design and capacity but are usually carried on the occupant’s life jacket/personal flotation device and provide a small quantity of supplemental air for use during their escape.[64]
EBS are critical for survival in situations where the occupant’s likely escape time exceeds their breath hold capability/capacity. Factors affecting breath hold capability includes the temperature of the water and the suddenness of immersion, particularly when the occupant does not have opportunity to take a full breath as the cabin floods. EBS are commonly used in larger passenger-carrying transport category helicopters operating over-water in hazardous environments, where there are a relatively large number of passengers to evacuate the cabin through the available emergency exits.[65]
In 2013, the United Kingdom’s Civil Aviation Authority published a report on the experimental work conducted in support of developing a technical standard for helicopter EBS.[66] The draft technical standard identified ‘Category A’ EBS for use in water impact accidents with little or no warning and which could be deployed underwater. Those systems should be capable of being fully deployed with one hand in less than 12 seconds following submersion.
In 2020, the European Union Aviation Safety Agency published a literature review relating to helicopter evacuation and underwater escape and identified gaps in research and provided recommendations for future research.[67] The literature review noted various research studies measuring time for occupants to escape from a helicopter cabin to vary from 15 to 25 seconds, depending on conditions. In addition, the literature review identified a study of offshore workers that measured breath holding times in air and water. In water at 25°C, the overall breath-hold time ranged from 6 to 120 seconds, with a median time of 37 seconds.
There were no Australian regulatory requirements that specified EBS as emergency equipment for occupant use in an underwater escape from a helicopter cabin.
Requirement for recurrent training in emergency procedures at the time of the accident
At the time of the accident, CAO 20.11 specified requirements for crews to complete periodic training in emergency procedures and specific to the type of aircraft being operated. As discussed in the Pilot information section, both the instructor and pilot under supervision had completed this training within the required period.
Relevant to the pilot under supervision was the CAO 20.11 check completed during their company induction 5 March 2018. Although this training included operation of the emergency exits, that training did not include any actual activation of the emergency exits using the door jettison system. However, having recently competed that training the pilot under supervision should have been familiar with the location of the door jettison handle and the correct sequence for operating the door.
In addition to the CAO 20.11 training, the chief pilot had completed the company induction checklist with the pilot under supervision. That checklist included a section titled survival at sea and the item titled HUET procedures had been ticked. The application of that item would have been limited to a check of theoretical knowledge and discussion of the HUET procedure and not an application of the practical skills and/or procedures.
Revised regulatory requirements
New flight operations regulations introduced in December 2021 authorised MPT operations under a CASR Part 138 aerial work certificate, to be conducted under the general operating and flight rules in CASR Part 91 with addition or variation of those rules according to CASR Part 138.
The CASR Part 138 manual of standards (MOS) specified that for flights in helicopters where life jackets and life rafts were required to be carried, flight crew members were required to have training, including an in-water practical component, in:
- ditching procedures
- use of life jackets and life rafts (as required)
- underwater escape.
The MOS specified that training in relation to life jackets, life rafts or underwater escape was to occur at intervals of not more than 3 years.
At the time of the accident, there was no regulatory standard that required crews of multi-engine helicopters flying over water to have completed underwater escape training. However, a requirement existed in the company operations manual for this training to be completed.
Helmets, communication cords and seat belts
Minutes from an operator safety meeting in October 2017 documented that VH‑ZGA and VH‑ZGZ required helmet/headset communication cords to be connected directly to the airframe connector jacks. The meeting minutes identified that in a ditching scenario, those communication cords could impede occupant egress unless they were pulled directly to disconnect the helmet from the airframe. To address this potential issue, short connector leads were to be provided to connect headsets/helmets to the airframe and improve the cord’s breakaway capability.
The instructor recalled being unable to disconnect their helmet communication cord from the overhead console after the water impact, so had unfastened their helmet chinstrap and discarded the helmet during their cockpit escape. This helmet was recovered with the communications cord still attached. Inspection of the helicopter wreckage found that the short breakaway connector remained connected to the instructor’s connector jack in the overhead console.
Police divers located the pilot under supervision in the cockpit of the helicopter, with the 4‑point seat belt unfastened. The pilot’s helmet was located in the cockpit with the chinstrap unfastened. The helmet’s communication cord was plugged into an extension connected to the overhead console. Although there was no short breakaway connector fitted at the overhead console, the extension cord provided similar functionality.
Lifejackets/personal flotation devices
The instructor and pilot under supervision were each wearing a lifejacket/personal flotation device equipped with survival equipment that included a 406 MHz personal locator beacon (PLB) and distress flares. Inflation of the lifejacket/personal flotation device was via a toggle pull that activated a compressed gas cylinder for inflation. The lifejacket/personal flotation device was equipped with 2 gas cylinders and 2 separate buoyancy chambers.
The instructor activated their PLB about 10-minutes after the accident, and that signal was detected by the satellite detection system at 2358. Encoded with the distress signal was the identification of the PLB, together with a GPS distress location. That information was received by the Australian Joint Rescue Coordination Centre (JRCC) at 0000 on 15 March 2018.
The instructor also used several flares from their lifejacket/personal flotation device to signal their position to the responding surface vessels. Two flares were initially deployed and were followed by a third when a bulk carrier appeared to be turning towards their direction. The instructor recalled deploying a fourth flare to mark their position as a launch got closer to their position. The port authority’s daily log included an entry at 0010, with vessels at the scene sighting 2 distress flares.
The lifejacket/personal flotation device worn by the pilot under supervision was uninflated and the inflation system had not been activated. That was consistent with procedures used for escaping underwater, where the lifejacket/personal flotation device is not activated inside the cabin due to the potential for the increased buoyancy to prevent escape.
Emergency locator transmitter
The helicopter was fitted with a battery-operated Artex 406-N HM emergency locator transmitter (ELT) capable of transmitting a unique digitally-encoded distress alert signal from an external antenna on the upper fuselage. On this model of ELT, the unit’s GPS position was also encoded in the signal. The ELT was designed to activate automatically when the helicopter was subjected to g-forces consistent with an accident.[68] It could also be manually activated using a switch mounted on the lower left side of the cockpit centre instrument panel.
About 50 seconds after activation, the ELT would transmit its first 0.5 second burst of digital data on 406 MHz and then repeat a transmission of data approximately every 50 seconds. Those signals could be detected by Cospas-Sarsat satellites, which would then be processed to the relevant search and rescue agency to coordinate a rescue response.
The Cospas-Sarsat satellites did not detect any post-impact transmissions from VH-ZGA, which indicated that the ELT did not activate, or activated without transmitting an effective signal. Examination of the ELT found that the battery compartment and internal electronics had been affected by water ingress and it was not possible to measure battery voltage as an indicator of ELT status. It was however noted that the ELT’s batteries were not due for replacement until August 2018 and the ELT was not waterproof or designed to operate under water. Irrespective of ELT activation, the almost immediate immersion of the ELT antenna would have attenuated any transmission.
The ATSB also identified that the ELT was mounted on the PELICAN[69] rack attached to the avionics deck in the rear passenger cabin. Guidelines issued by the Radio Technical Commission for Aeronautics (RTCA)[70] indicated that for proper operation in an accident, ELTs shall be installed to primary aircraft load carrying structures, such as trusses, bulkheads, longerons, spars, or floor beams.
The helicopter manufacturer advised the ATSB that the PELICAN rack was not an integral or primary load carrying structure and, as such, was not a suitable location for installing an ELT. The helicopter manufacturer confirmed that ELTs at airframe manufacture would be installed to the load carrying structures on the cockpit floor, adjacent to the pilot seat. A review of the available VH-ZGA’s maintenance documentation did not identify any supplemental type certificate, field approval or similar engineering assessment that approved the installation of the ELT to the PELICAN rack.
During the investigation, the ATSB advised the helicopter operator of the potential issue associated with the PELICAN rack mounting method of the ELT. A check of other helicopters in their fleet identified one other helicopter with a similarly mounted ELT, which was subsequently relocated to the cockpit floor, adjacent the pilot seat.[71]
A review of the helicopter’s maintenance records identified that the ELT was installed in July 2009, as part of emergency medical service modifications while the helicopter was on the United States’ aircraft register.[72]
In addition to the airframe mounted fixed ELT, a portable GME MT403G Emergency Position Indicating Radio Beacon (EPIRB) was fitted in the rear passenger cabin. The EPIRB unit activated automatically on water immersion or if not water immersed, it could be manually activated. This model of EPIRB would also transmit a distress signal encoded with the units GPS position. The battery expiration date was September 2023. This unit was found in its cabin mount and had activated on water immersion. The JRCC did not receive any distress signal from this EPIRB during the night of the accident.
Regulatory oversight and approvals
Regulatory framework
The Civil Aviation Safety Authority (CASA) was responsible, under the provisions of Section 9 of the Civil Aviation Act 1988, for the safety regulation of civil aviation in Australia and of Australian aircraft outside of Australia. Section 9(1) stated the means of conducting the regulation included:
(c) developing and promulgating appropriate, clear and concise aviation safety standards;
(d) developing effective enforcement strategies to secure compliance with aviation safety standards…
(e) issuing certificates, licences, registrations and permits;
(f) conducting comprehensive aviation industry surveillance, including assessment of safety‑related decisions taken by industry management at all levels for their impact on aviation safety
The 2 primary means of oversighting a specific operator’s aviation activities were:
- assessing applications for the issue of or variations to its AOC and associated approvals (including approvals of key personnel)
- conducting surveillance of its activities, including level 1 surveillance events (such as systems audits) and level 2 surveillance events of shorter duration and narrower scope (such as site inspections and ramp checks).
Previous occurrences and regulatory oversight
Detailed discussion of CASA’s processes for oversighting passenger charter operators for the period up to 2017 was provided in an ATSB report into a fatal Cessna 172 accident.[73] That report (released in October 2019) identified that, although the Cessna 172 operator’s primary activity since July 2009 was passenger charter flights to beach aeroplane landing areas (ALAs), regulatory oversight by CASA had not examined the operator’s procedures and practices for conducting flight operations at these ALAs. The ATSB investigation also identified the following safety issue:
The Civil Aviation Safety Authority’s procedures and guidance for scoping a surveillance event included several important aspects, but it did not formally include the nature of the operator’s activities, the inherent threats or hazards associated with those activities, and the risk controls that were important for managing those threats or hazards.
The ATSB issued a safety recommendation (AO-2017-005-SR-026) to CASA in October 2019 to address the safety issue, and this recommendation was closed in March 2020 after CASA outlined the safety actions it had taken, and was taking, to address the issue. A similar safety issue had been previously identified in another ATSB investigation.[74]
CASA oversight processes were also addressed in the ATSB investigation of a loss of control and collision with water involving a Eurocopter EC120B at Hardy Reef, Queensland on 21 March 2018.[75] The ATSB found that although the operator’s primary helicopter activity was conducting charter flights to pontoons at Hardy Reef, regulatory oversight activity by CASA had not specifically examined the operator’s procedures and practices for conducting operations to these helicopter landing sites.
Pre-occurrence audits
As part of this investigation, CASA provided records of regulatory activities carried out in relation to the operator during the 5-year period prior to the occurrence and up to the end of 2019. The ATSB reviewed these records with a focus on flight operations.
CASA conducted 5 audit or check events between 25 July 2013 and 21 February 2018. The 2 events conducted in 2013 were not applicable to the contemporary operating entity so were not considered.
The most recent audit prior to the occurrence (21 February 2018) was a Level-1 health check of the operator within a defined scope, including crew scheduling, operational standards, authorised activities, and operational support systems. It involved sampling documentation, interviewing key personnel, and reviewing some of the operator’s systems and processes at the operator’s main office in Mackay.
The auditors found that both the chief pilot and head of operations demonstrated adequate control of the flying operations and a high operational standard was expected and maintained. Crew scheduling appeared to be operating and effective. For operational standards, the auditors assessed the system that tracked qualification expiry dates and sampled induction records. They identified that the chief pilot was not licenced for one of the helicopter types on the operator’s approval and this type was subsequently removed from the approval.
The surveillance report noted that crew scheduling ‘appeared to be operating and effective’. CASA advised that this activity did not raise any concerns regarding the operator’s rostering practices or its flight and duty periods. It also noted that the Port Hedland base roster and flight and duty records were not specifically examined. There was no indication in the surveillance report that the operator’s FRMS manual was reviewed.
Prior audits/checks in 2016 and 2017 identified 2 non-compliances that were not directly related to flight operations. An observation issued in September 2016 noted that the level of control the operator had over its functions was limited in the area of chief pilot duties as there was no management process followed to support the chief pilot’s working practices. The operator was not required to respond to observations.
Post-occurrence audits
Following the occurrence, CASA conducted a national desktop audit of helicopter underwater escape training (HUET) for AOC holders conducting MPT operations. On 22 August 2018, CASA recorded that the operator was compliant with their 3-year HUET requirement for all of their MPT pilots.
Between 18 and 20 September 2018, CASA carried out a Level-2 operational check of the operator with a site inspection at Port Hedland in response to concerns raised by pilots about crew scheduling and fatigue management. The surveillance report stated that ‘the surveillance focussed on safety, training and scheduling practices’ of flight crew, and concluded that the operator’s ‘crew scheduling and safety management procedures were found to be suitable and effective in managing fatigue’. The surveillance report also stated that key management personnel were interviewed and the operator’s FRMS manual was referenced. CASA advised that the surveillance activity involved reviewing pilot rosters for the previous 3 months and next 2 months and copies of reported and identified flight and duty breaches in the past 6 months.
Three further Level-2 events were maintenance related or administrative.
Other surveillance events
During the Level-1 health check conducted on 21 February 2018, the auditors compiled an authorisation holder performance indicator (AHPI) questionnaire with input from the chief pilot and the head of operations. This form listed standard questions about scope of operations, organisational stability, and exposure to 2 risks - challenging environments and extension of working hours beyond limits. Based on the responses, the overall risk was recorded as low.
As noted by the auditors, the respondents advised that the 3 highest risks were vessel landings, drones (collision), and weather. There was no further reference to MPT operations and no provision for the associated risk controls to be identified and assessed.
The preceding AHPI in August 2017 produced a similar result. No other preceding AHPIs were available for the contemporary operating entity.
Post-occurrence AHPI results varied in the first 12 months with some higher risk scores associated with maintenance control concerns. Subsequent AHPI scores were lower with notes indicating organisational stability and CASA’s confidence in operational personnel.
Following the occurrence, CASA carried out a regulatory and safety review with reference to the regulatory posture to the operator and any safety action or learning derived from the occurrence. This did not identify any requirements for immediate action or significant learnings. Some minor improvements to processes were identified and a national sector campaign to audit HUET compliance in the MPT sector was initiated.
Application for approvals under CASR Part 141/142 and CAR 217
In September 2016, the operator submitted applications to CASA for flying school activities under CASR Parts 141/142 and training and checking approval under CAR 217.
The operator developed the various elements of their CASR Part 141/142 exposition/manual during 2017 with feedback and guidance from the assigned CASA personnel. In October 2017, CASA personnel assessed that the operator was compliant with the applicable requirements. The AOC was re‑issued (effective 1 November 2017) with approval to conduct CASR Part 142 flying training activities for the singe-engine helicopter class and EC135 type ratings.[76] The operator was also granted a CASR Part 141 flight training certificate for the single-engine class and various ratings such as night VFR and instrument ratings. CASA assessed that the instructor was acceptable for the position of head of operations for the CASR Part 142.
From a CASA perspective, the operator did not develop the CAR 217 application during 2017. In January 2018, the operator applied to CASA for a permission under CAR 217 to train and check aircrew and flight crew that would be involved in EC135 winch operations for MPT. The operator followed up with a proposed training manual based on the existing volume-4 of the operations
- Although the pilot under supervision held a Part 61 multi-engine helicopter instrument rating restricted to non-pilot in command duties on the basis of their co-pilot multi-engine helicopter instrument rating, a proficiency check had not been completed since the issue of the Part 61 licence in August 2015.
- The term ‘sleep opportunity’ is distinct from the amount of sleep obtained. Sleep opportunity in the context of this report’s analysis of the pilots’ recent histories refers to periods in which the pilots reported sleep in their sleep logs and no other data indicated they were awake. The actual sleep obtained by the pilots was probably less than the sleep opportunity.
- The text messages referred to in this section were sent from the pilot under supervision to close personal contacts, including the pilot’s partner. Those contacts provided the content of relevant text messages to the ATSB.
- All times in this report are Western Standard Time (WST) unless otherwise stated. WST is UTC + 8 hours and Eastern Standard Time is UTC + 10 hours.
- Flight records indicate engine shutdown at 1714 on return from the last flight. Post-flight activities would have included a debriefing with the instructor and general housekeeping/administrative duties, including refuelling of the helicopter.
- Flight records indicate engine start at 1743 for the first MPT flight. Prior to this, the pilot under supervision would have needed to complete various sign-on tasks. Those tasks include attending the security gate to perform a routine alcohol screen, a review of weather forecasts for the night’s flying, completion of a pre-flight briefing with the instructor and a pre-flight inspection of the helicopter.
- The investigation was not able to obtain a record of all of the instructor’s work-related email activity.
- The Samn-Perelli rating scale was used for the self-evaluation of fatigue. The scale ranges from 1 (fully alert) to 7 (completely exhausted). A rating of 2 indicates ‘very lively, responsive, but not at peak’ and a rating of 3 indicates ‘okay, somewhat fresh’.
- The specification of engine torque limits was to avoid an over-torque condition causing damage to, or failure of the helicopter’s main transmission.
- Emergency floatation system: inflatable bags to provide water buoyancy in an emergency.
- The EC135 helicopter was certified by the European Aviation Safety Agency as a small rotorcraft under Joint Aviation Requirements 27 (JAR 27). The certification specifications indicated FAA advisory circular AC 27-1B provided the acceptable means of compliance to the certification specifications. The definition for the primary field of view was included in Change 7 of the advisory circular, published April 2016.
- Rigid rotor systems can generate large bending forces to the rotor shaft with cyclic movement or a change in the rotor’s plane of motion while the helicopter is in contact with the ground/deck. To monitor those forces and warn of an exceedance, the helicopter was equipped with a mast moment indicator (MMI).
- Sea waves are generated by the local prevailing winds. Swell waves are the regular, longer period waves, generated by distant weather systems. Total wave height is the combined height of the sea and swell waves on open water.
- Geoscience Australia (GA) defines the ending of civil twilight as the instant in the evening, when the centre of the Sun is at a depression angle of 6° below an ideal horizon. At this time in the absence of moonlight, artificial lighting or adverse atmospheric conditions, the illumination is such that large objects may be seen but no detail is discernible. The brightest stars and planets can be seen and for navigation purposes at sea, the sea horizon is clearly defined.
- GA defines the ending of evening nautical twilight as the instant in the evening, when the centre of the Sun is at a depression angle of 12° below an ideal horizon. At this time in the absence of moonlight, artificial lighting or adverse atmospheric conditions, it is dark for normal practical purposes. For navigation purposes at sea, the sea horizon is not normally visible..
- GA defines the ending of astronomical twilight as the instant in the evening, when the centre of the Sun is at a depression angle of 18° below an ideal horizon. At this time the illumination due to scattered light from the Sun is less than that from starlight and other natural light sources in the sky.
- The bulk carrier Squireship was about 288 m long and had deck floodlighting at the bow and on the accommodation quarters, which were about 260 m apart. The extent to which the lights would be seen as one light or multiple lights would depend on the distance away, orientation of the vessel relative to the helicopter’s position, meteorological conditions and factors such as diffraction when viewing through a windscreen. Even if multiple light sources were discernible, these would still provide very limited cues for orientation until the helicopter was in close proximity.
- The safety wire used has low tensile strength and is easily broken when operating the emergency door jettison handle. A break to the safety wire indicates that the handle has been moved from the secured position and, potentially, the door jettison system may have been partially activated. The emergency door jettison handles on VH-ZGZ, the other EC135 at Port Hedland, were secured by plastic tie wraps (cable ties). Those tie wraps had higher tensile strength than the normal safety wire and would make the handle more difficult to operate in an emergency. The tie wraps fitted to VH-ZGZ were replaced by safety wire a short time after the accident.
- The non-volatile memory of the WU retains snapshot data of the last 32 changes to the unit’s visual and audible warnings, typically covering the last 2 to 3 flights.
- The non-volatile memory of the CAD retains the last 256 failures, cautions and advisories, associated with a contextual snapshot of parameters such as engine torque, fuel flow and fuel quantity.
- The non-volatile memory of the VEMD retains flight report summaries for the last 32 flights and fault codes for the last 256 faults. Any failures and overlimit conditions are associated with the flight report and contextual parameter snapshots are recorded. On EC135 helicopters, the parameter snapshots related to main rotor RPM, torque and turbine outlet temperature.
- The position of the collective lever was measured in degrees, from zero at a ‘flat pitch’ rotor position, to about 100° when commanding maximum rotor pitch
- Although the helicopter operator did not have the necessary CASA approvals to conduct endorsement training under their own air operator’s certificate (AOC) at this time, the training was provided by qualified instructors operating under an appropriate AOC.
- Heliporters are battery operated transporters to assist personnel with helicopter ground handling.
- These surveys utilised an online survey development application.
- VTOSS: Take-off safety speed. For a rotorcraft, this is the minimum speed at which climb of the rotorcraft is achieved with 1 engine inoperative and the remaining engines operating within the operating limits specified in the rotorcraft’s flight manual for a take off.
- VY: Best rate of climb speed. Flying at this speed achieves the greatest increase in altitude over a given time period.
- Air Maestro is an online safety and operational tool with various features including for records management and rostering.
- This term is used in some regulatory domains for a document or set of documents that describe how an organisation will comply with all applicable legislative requirements, and how they will manage the safety of their operations. An exposition is broadly equivalent to an operations manual in other domains.
- The associated CASA instrument extended the FRMS approval of a number of operators at the same time for the same period.
- Due to a coding error, if the duty period was extended beyond 12 hours, the cells recorded as duty or flying would remain their normal colour.
- That is, 12 consecutive hours in the sleep log recorded as sleep. It should be noted that consecutive hours of sleep could legitimately be recorded on a sleep log even if a person awoke for brief periods.
- A phone call on the night of 13 March started at 1908 and lasted about 2 hours.
- FAID was initially known as ‘Fatigue Audit InterDyne’. It was subsequently renamed the Fatigue Analysis Tool by InterDynamics.
- FAID documentation stated scores of 40–80 were broadly consistent with a safe system of work. However, the threshold for deciding the acceptability of a roster needed to be set by an operator based on a fatigue hazard assessment, taking into account the fatigue-related hazards specific to the role or task, and determining the acceptable level of fatigue tolerance for that role or task. Without this assessment, the FAID program defaulted to a fatigue tolerance level (FTL) of 80.
- The ATSB notes that FAID scores (and the scores from any BMMF) need to be interpreted with caution. The Independent Transport Safety Regulator of New South Wales (2010) stated that, due to various factors associated with the model, ‘a FAID score of less than 80 does not mean that a work schedule is acceptable or that a person is not impaired at a level that could affect safety’. In addition, the US Federal Railroad Administration (2010) concluded that in some situations FAID scores between 70 and 80 can be associated with ‘extreme fatigue’.
- ATSB investigation AO-2011-102, VFR flight into dark night involving Aerospatiale AS355F2 VH-NTV, 18 August 2011.
- Spatial disorientation occurs when a pilot does not correctly sense the position, motion and attitude of an aircraft relative to the surface of the earth. Although not a requisite condition, spatial disorientation is much more frequently encountered in a degraded visual environment, when pilots are unable to establish their spatial position through external visual cues.
- Air Accidents Investigation Branch, Air Accident Report 5/88. Report on the incident to Sikorsky S-76A helicopter G BHYB near Fulmar ‘A’ Oil Platform in the North Sea on 9 December 1987.
- Air Accidents Investigation Branch, Air Accident Report 7/2008. Report on the accident to Aerospatiale SA365N, registration G-BLUN near the North Morecambe gas platform Morecambe Bay on 27 December 2006.
- Rice E,V. and Greear J.F. (1973) Underwater escape from helicopters. In Proceedings of the Eleventh Annual Symposium, Phoenix, AZ: Survival and Flight Equipment Association, 59-60. Cited in Brooks C. (1989) The Human Factors relating to escape and survival from helicopters ditching in water; AGRAD.
- Ryack, B. L., Luria, S. M., & Smith, P. F. (1986). Surviving helicopter crashes at sea: A review of studies of underwater egress from helicopters. Aviation, Space, and Environmental Medicine, 57(6), 603-609.
- Hytten K (1989) Helicopter crash in water: effects of simulator escape training. Acta Psychiatrica Scandinavica, Suppl. 355: 73-78. Cited in Coleshaw S (2010) Report for the Offshore Helicopter Safety Inquiry. Report No SC176.
- Summers F (1996) Procedural skill decay and optimal retraining periods for helicopter underwater escape training. IFAP; Willetton, Western Australia. Cited in Coleshaw S (2010) Report for the Offshore Helicopter Safety Inquiry. Report No SC176.
- Civil Aviation Authority (2014) Safety review of offshore public transport helicopter operations in support of the exploitation of oil and gas. CAP1145.
- The requirement for an operator to conduct their operations in accordance with an operations manual was contained in the Civil Aviation Regulations 1988, Regulation 215.
- The extra time available for emergency escape depends on the design of the system and other variables such as water temperature, water depth and the user’s breathing rate. A user would typically have somewhere between 10 to 20 breaths before the supplemental supply was exhausted.
- Those flights are typically conducted in support of the oil and gas offshore industry and during which, the operating environment also requires the use of survival (immersion) suits.
- CAP 1034, Development of a Technical Standard for Emergency Breathing Systems, UK Civil Aviation, 2013.
- Research Report Underwater Escape from Helicopters, European Union Aviation Safety Agency, 2020.
- This model of ELT was designed to activate using a 4.5 ft/sec impact operated g-switch, together with a 5-way g-switch detecting +12.5g along any of the ELT’s 6 orthogonal axes. Operation of either switch would activate the ELT.
- PELICAN is an acronym used by the helicopter manufacturer to describe the packing equipment line for integrated concept of avionic nouvelle (new avionics).
- RTCA DO-204, Minimum Operational Performance Standard for Aircraft Emergency Locator Transmitters 406 MHz
- This helicopter was the other EC135 based at Port Hedland (VH-ZGZ), which had been imported to Australia in 2008 from the United States.
- The ELT was not fitted at airframe manufacture but was installed soon after customer delivery.
- ATSB AO-2017-005, Collision with terrain following an engine power loss involving Cessna 172M, VH WTQ, 12 NM (22 km) north-west of Agnes Water, Queensland, 10 January 2017.
- ATSB AO-2009-072 (reopened), Fuel planning event, weather-related event and ditching involving Israel Aircraft Industries Westwind 1124A, VH-NGA, 6.4 km WSW of Norfolk Island Airport, 18 November 2009 (Released in November 2017).
- ATSB AO-2018-026, Loss of control and collision with water involving Eurocopter EC120B, VH-WII, 72 km north-north-east of Hamilton Island, Queensland, 21 March 2018.
- The Prescription of Type Ratings Excluded from CASR Part 142 Flight Training (Edition 6) Instrument 2018, signed 4 June 2018, directed that a number of type ratings including the EC135 type rating was not Part 142 training but was Part 141 training. This did not have any implications for the occurrence.
Introduction
The operator was contracted to provide helicopter transfers of marine pilots to and from ships at any time of the day or night according to the Port Hedland shipping schedule. These marine pilot transfer flights (MPT) were carried out as charter flights under the day/night visual flight rules (VFR) in twin-engine EC135 helicopters equipped for single-pilot instrument flight rules (IFR) operations. Night vision imaging systems were not required, nor utilised by the operator.
In this occurrence, VH-ZGA descended into the ocean during a positioning flight at night to Squireship, about 20 NM (37 km) offshore. This flight was the third line training flight at night as part of the operator’s process to induct a recently employed pilot into day and night operations at Port Hedland. This pilot was acting as pilot in command under the supervision of a company instructor pilot.
As was standard for this helicopter type, the EC135 was not equipped with a flight data recorder or cockpit voice recorder. In the absence of that data, the ATSB sought data from other sources, including GPS-based automatic dependent surveillance broadcast (ADS-B) data and the surviving pilot. When the ADS-B data was processed and analysed, it indicated that during circling and before final approach, the vertical component of the flight path and airspeed was abnormal for a period leading up to the accident. The surviving pilot was unable to recall specific details of the pre‑accident sequence.
Based on the derived flight path and contextual information such as environmental conditions, operator procedures, and operational capability, the ATSB identified 8 safety factors that contributed to the occurrence and 10 factors that, while not influential in the development of the accident, increased operational risk. These included 5 safety issues that related to helicopter equipment and operator processes, including fatigue management.
Safety issues not related to fatigue management were identified and addressed by the operator soon after the occurrence. Additionally, regulatory changes introduced following the occurrence, although not in response to it, imposed further requirements on MPT operations that will be categorised as aerial work carrying passengers.
This part of the report presents the evidence and arguments that relate to the identified findings. It also details consideration of concerns about aspects of the MPT operation reported to the ATSB that did not have any direct links to the occurrence or any related safety issues.
Local operational conditions
To operate a helicopter at night in accordance with the night visual flight rules (night VFR) while below 3,000 ft above mean sea level (AMSL), pilots were required to be clear of cloud and in sight of ground or water with visibility greater than 5 km. In addition, the Civil Aviation Safety Authority (CASA) strongly recommended that night VFR operations only take place in conditions that allowed the pilot to discern a natural visual horizon, or where the external environment had sufficient cues for the pilot to continually determine the pitch and roll attitude of the helicopter. This was actually a requirement unless the helicopter was equipped with an autopilot/stabilisation system or was a 2-pilot operation.
For the approach and landing to Squireship, there was no cloud or other atmospheric factor to reduce visibility below night VFR minima, but the visual cueing environment was degraded by the dark night conditions (low celestial lighting) and the scarcity of cultural lighting in the offshore environment. In preparation for arrival of the helicopter, the external lighting of Squireship would have been maximised and provided local illumination greater than a single point light source. Although this was useful as a visual reference point for a circuit and as a sight picture for profile management on final approach, it would not have provided sufficient visual cues to determine the helicopter’s pitch and roll attitude throughout the circuit.
Although Squireship was being operated near low intensity lighting associated with marking of the shipping channel, this would have provided only limited visual cues. Furthermore, as Squireship was underway at 12–13 kt, the relationship between the channel markers to the ship landing area was not constant and therefore of limited value as references for a circuit. Similarly, while there were a number of other illuminated ships in the Port Hedland area, these would have provided little to no visual assistance to the pilots.
Operations in a degraded visual cueing environment increases the difficulty of a pilot’s task in terms of continually maintaining awareness of the helicopter’s position, and therefore increases workload. Research by the FAA (Hoh, 1990) has shown that operations in a degraded visual environment result in a degradation of the effective handling qualities … due to a loss of the ability of the pilot to adequately perceive fine-grained detail in the visual environment. The degraded handing qualities result in a substantial increase in pilot workload simply to control the helicopter. This leaves very little excess workload capacity to maintain situational awareness (i.e., awareness of distances and rates with respect to obstacles and the ground)
As the helicopter was equipped with an integrated autopilot/stabilisation system, and the pilots held the appropriate ratings, the circuit and approach to the ship in a degraded visual cueing environment was within the allowable operational parameters. However, manoeuvring safely in this environment at low altitudes was highly demanding and required a high level of instrument flying proficiency integrated with visual flying skills, adherence to procedures, and effective use of automation.
Although pilot workload was generally high in these conditions, it was probably higher for both pilots during the occurrence flight because this was the third flight in the planned sequence of 10 line training flights at night and it was only the second night MPT to C1/C2. In the operational context, as the pilot under supervision had not yet passed a line check, the instructor was required to monitor the helicopter flight path and provide guidance/support as required. Additionally, there were factors discussed later that negated the effectiveness of the instructor.
|
Contributing factor During the positioning flight for the third supervised marine pilot transfer at night, circling in the vicinity of outbound bulk carrier Squireship was conducted in a degraded visual cueing environment, with associated increases in pilot workload and risk of disorientation. |
Management of automation during visual circling
Introduction
The helicopter was equipped with a stability augmentation system (SAS) and 3-axis autopilot that provided basic attitude hold and pilot-selectable ‘upper’ modes to control airspeed, heading/track, altitude, and vertical speed. In the default SAS mode, the system would hold the last commanded attitude until the pilot made an adjustment by moving the cyclic - with or without force trim release (FTR) - or using the BEEP TRIM switch. If the helicopter was above both an airspeed of 60 kt and 500 ft above the ground or water, the pilot could engage an upper mode(s) to achieve a flight path within specified parameters.
Although the operator did not have a documented procedure for the management of automation during MPT operations, the chief pilot advised pilots to operate with an upper mode engaged during circling at night until the helicopter passed the ‘finals gate’ (500 ft and 60 kt) on final approach. The instructor similarly advised the ATSB that such use of automation was standard practice and would have been implemented on the occurrence flight.
However, as there was no recorded data of automation selections and the instructor recalled limited specific detail of its use, the ATSB sought to characterise the management of automation by analysing the ADS-B data.
First circuit and go-around
Analysis of the ADS-B data identified that the first inbound descent to Squireship was at a steady rate of 500 ft/min and the helicopter levelled at 700 ft in the vicinity of the ship. This was consistent with engagement of the autopilot in a vertical upper mode. Due to a gap in the data, it was not possible to characterise autopilot use in the first part of the downwind segment of the circuit.
By about mid-downwind, data points indicated that the circuit altitude was steady. During the base segment, the helicopter climbed slightly and was about 825 ft turning onto final approach, which was contrary to the SOPs that required a descent from circuit height and join final approach at 500 ft. This indicates that an upper vertical mode was probably no longer engaged, and pilot control inputs were not effective to manage the flight path of the helicopter.
Provided airspeed was maintained above 60 kt, the ALT.A (altitude acquire) autopilot mode was capable of managing the descent from 700 ft to 500 ft during the base turn, and this was the operator’s recommended method until the helicopter was through the ‘finals gate’ and positioned for a continuous descent on the nominated descent profile.
Although the helicopter was about 300 ft higher than the target for commencing the final approach, an effective descent rate was not achieved, and the helicopter remained high on profile. When the helicopter was 275 m from the landing hatch (at about 500 ft and 31 kt), the airspeed started to increase, consistent with initiation of a go-around. However, a further 175 ft was then lost over a 22-second period before a positive rate of climb was established. This height loss in the early stages of the go-around was not consistent with recommended practices that prioritised a climb to a safe altitude. The instructor advised the ATSB that the autopilot was engaged during the climb phase of the go-around and the data supported that recollection.
Sustained deviations from the specified flight path on final approach and height loss in the go‑around can be associated with decrements in visual perception, instrument scan, and/or helicopter handling. The human factors aspects of these potential factors are addressed in a later section.
On final approach, handling of the helicopter by the pilot under supervision would have been influenced by the ongoing transition from a different type of helicopter, including interaction with the SAS. Any of the 3 available methods to adjust the helicopter’s attitude could have been applied on final approach depending on operational imperatives such as the rate, magnitude, and duration of the intended attitude change. Given there was no recorded data or applicable observation, it was not possible to establish the method of attitude adjustment used.
Despite that, as the Transportation Safety Board of Canada found in relation to the S‑92A occurrence in Nova Scotia, use of FTR in a degraded visual environment can increase pilot workload and contribute to control difficulties and an unstable approach. If that occurred, it would have compounded the high workload of the pilot under supervision that was associated with transition from a different helicopter type without the benefit of automation.
Second circuit
By the time the helicopter reached 1,100 ft in the go-around, the helicopter was being turned onto the downwind segment of a circuit to position for another approach in the same orientation to the ship as the first approach. About 30 seconds later the helicopter was on descent. The rate of descent developed quickly to 800–900 ft/min, steadied at about that rate for about 30 seconds, then increased further as the helicopter turned onto a base segment and descended through 500 ft.
Assuming the target circuit altitude was 700 ft in accordance with the operator’s standard operating procedures (SOPs) and consistent with the first circuit, the descent below circuit altitude and the high descent rate (above 500 ft/min) were not consistent with use of ALT.A or other vertical upper mode. This was contrary to the instructor’s recollection that the autopilot was used for circling. However, the ATSB also noted that the instructor did not advise of any confirmatory details, such as specific mode selection and annunciation or conforming flight path. It is therefore possible that the instructor assumed that the expected operator’s autopilot practices were implemented.
In the context of high workload associated with the transition from a go-around to another circuit in a degraded visual cueing environment, it is possible that operating in the default SAS mode rather than making upper mode selections was considered to be easier. Another possibility is that the vertical autopilot mode might have been perceived as unsuitable to manage the intended flight path due to the required higher than usual rate of descent. A further possibility is that either or both pilots incorrectly thought that a vertical mode had been engaged but did not identify the contrary indications such as mode annunciation and abnormal flight path.
The observed general practice during the circuits of previous line training flights (10 by day and 2 by night) was to manage vertical navigation in the pre-final phases with autopilot rather than pilot control inputs. However, it was also noted that the instructor conducted 5 night circuits in January 2018 without apparent use of an autopilot vertical mode to manage the flight path in the circuit prior to joining final approach.
If an autopilot vertical mode such as ALT.A had been used to capture and hold the circuit altitude of 700 ft then descend to 500 ft, the accident would almost certainly have been averted. While there was insufficient evidence to determine why a vertical mode was not selected during the final descent, the potential influence of pilot fatigue and the operator’s circuit procedures are considered later in the analysis.
|
Contributing factor Following a circuit, missed approach, and climb to 1,100 ft, a descent was initiated without coupling a vertical navigation mode of the autopilot. This was not consistent with standard operational practices and significantly increased the attentional demands on both pilots and the associated risk of deviation from circuit procedure. |
Inadvertent descent below 500 ft
Abnormal flight path and associated parameters
As the helicopter descended through 500 ft, the descent rate increased above 1,000 ft/min while the airspeed reduced below 50 kt. This occurred while the helicopter was turning right from the downwind onto base segment of the circuit, about 1,950 m from Squireship.
The descent rate continued to build rapidly, and the airspeed reduced further, but neither of these significantly abnormal parameters appear to have been detected by either the pilot under supervision or the instructor. According to the instructor, activation of the radio altimeter alert at 300 ft was the first prompt to take over control and initiate a go-around. At about this time the ADS-B data showed the rate of descent was about 1,700 ft/min and the airspeed was just above 30 kt.
Although the instructor advised the ATSB that the helicopter was on final approach before the descent into water, this was not consistent with the position and heading/track of the helicopter as it descended below 500 ft during the base turn. Based on the orientation of the helicopter relative to Squireship, it is likely that the instructor’s view of the ship (from the left seat) was obstructed as it was in the approximate 2‑o’clock position relative to the helicopter nose. The disparity between the instructor’s recollection of helicopter position and the flight data indicates a level of disorientation during the sequence and/or mis‑remembering after the event.
The instructor did not recall any communication with the pilot under supervision regarding the relative position of Squireship during the second circuit. Seated on the right side of the helicopter, the pilot under supervision had relatively unobstructed views of the ship during the right circuit and could be expected to periodically reference Squireship for circuit position information. It is possible to detect changes in height and vertical trend by observing movement of the ship relative to cabin features. For example, during a descent with a consistent attitude, the vertical position of Squireship would have moved up relative to the windscreen or cockpit windows. This, however, would have been low resolution information, disrupted by changes to pitch/roll attitude and attenuated by distance from the ship. Seated on the left side of the helicopter, the instructor’s view of the ship would probably have been obstructed for brief periods.
Irrespective of how the 2 pilots perceived the relative position of the helicopter, it was not tracking toward the ship at any stage of the second circuit. In that context, the SOP was to not descend below 500 ft and not reduce airspeed below 60 to 65 kt. Both pilots were presumably aware of the importance of these limits, especially for night operations, but seemingly did not identify the deviation.
When the descent rate exceeded 500 ft/min and continued to increase, it was outside the industry practice for circling at night over water below 1,000 ft. The descent rate of 1,000 ft/min when the helicopter was passing 500 ft was double the rule-of-thumb amount for descent rate proportional to height. At the maximum descent rate of 1,700 ft/min, passing 300 ft, the helicopter was descending at 5 times more than the rule-of-thumb figure (300 ft/min). As discussed further in a later section, the operator did not specify rate‑of‑descent parameters for operations above 30 kt.
Operational requirements
After the missed approach and climb to 1,100 ft, a descent was required to circuit height and the pilots might have intended a relatively high rate of descent to ensure they were not high on final approach. In that context, the physical (vestibular) sensations associated with the very high descent rates would not have provided a reliable cue for detection of the abnormal flight path.
To manoeuvre an aircraft in a degraded visual cueing environment, the pilot must consistently scan the flight instruments and assimilate pitch and roll information, combined with reference to other instrument indications - airspeed, altitude, rate of descent, heading – according to operational priorities. Visual circling also requires periodic reference to the landing area and any visible terrain features for position information, possibly supplemented by GPS data. These actions are required whether the pilot is controlling the aircraft manually or through autopilot selections. This is a complex information processing task that generally requires a high level of aircraft handling skill and instrument flying proficiency.
To manage the flight path of a helicopter through control inputs, the pilot manipulates power/torque (main rotor thrust) through the collective control in combination with selection of attitude (pitch and roll) through the cyclic control. In simple terms, for a given power/torque, the cyclic input will influence airspeed and rate of climb/descent (see Appendix D for further detail).
Role of pilot under supervision
While the pilot under supervision had held an EC135 type rating for a number of years, experience on that type was not substantial and none of it was recent. This was addressed by refresher training and a type rating flight review on arrival at Port Hedland. After 10 ship landings by day, the pilot under supervision was approved by the instructor for day MPT operations.
As the holder of a night VFR rating and current flight review, the pilot under supervision was considered competent to operate at night in visual meteorological conditions. Although this was a necessary qualification for the MPT operation, further training was required to prepare pilots for the inherent challenges and risks of ship landings and take-offs in an offshore environment at night.
In recent night flying for a previous operator using night vision imaging systems (NVIS), the pilot under supervision had demonstrated instrument flying proficiency as part of normal NVIS flying and simulated system failure conditions. However, due to the enhancement provided by NVIS, the previous flying provided relatively fewer opportunities to maintain proficiency in the integration of instrument and unaided visual data while operating in degraded visual cueing environments.
Since leaving the previous operator, the only night or instrument flying conducted by the pilot under supervision was on the night of the occurrence. The ADS-B data showed that the pilot under supervision was able to conduct the circuits on the previous 2 night flights and on arrival at Squireship, but was having difficulty maintaining the helicopter on a constant-angle final approach.
In the early stages of the transition from previous night operations over land using NVIS to unaided night VFR over water, the relative absence of visual cues might have had a disorienting effect during circling and approach with associated increase to workload. The pilot under supervision was also transitioning from previous operation with analogue instruments to an integrated digital display, which required a different type of scan and more effort (initially) to interpret the data. In addition, considering the pilot was now operating a helicopter with different handling characteristics and equipped with a complex autopilot/stabilisation system, manoeuvring the helicopter was likely demanding during the transition period.
In combination, these factors probably led to a relatively high workload associated with the transition to night operations that would have affected the capability of the pilot under supervision to manage the flight path and monitor critical parameters. Significantly, in a degraded visual cueing environment, a high level of attention to the primary flight display is required to detect and correct abnormal operation.
In addition to high workload, diversion of attention or inattention might have occurred for the following reasons:
- disproportionate attention to the limited visual cues
- lower intensity monitoring of flight instruments on the (incorrect) basis that an autopilot vertical mode was engaged
- instructor communication about the first approach, go-around, and next approach.
During the process of adapting to unaided night VFR it is possible that the pilot under supervision was seeking visual cues that were not available without the enhancement provided by NVIS. Alternatively, the lack of visual cues might have reinforced the need for reliance on instrument flying in the circuit. The pilot under supervision’s successful manoeuvring of the helicopter with reference to the ships in the 2 preceding night flights and first approach to Squireship supports that latter as circling would have required the use of flight instruments.
From the ADS-B data it is apparent that the autopilot was not engaged in a vertical upper mode but could have been engaged in a lateral mode. If that was the case, the pilots might have associated this with a fully coupled condition and not been aware of the mode status. Complicating identification of an uncoupled upper mode is the default SAS mode that will hold the last commanded attitude. Although there is a mode annunciation on the PFD, this might not be a specific item of the routine instrument scan and was not in the primary field of view of the instructor.
Given the lack of detail in the instructor’s recollection, it is not clear if the instructor provided feedback to the pilot under supervision after the first approach and go-around with advice for the next approach. Such feedback would be consistent with the instructor’s training role and the operational imperative to land off the second approach. However, the as-found intercom selection would have isolated the pilot under supervision from the attentional demands of any feedback, depending on when that selection was made.
From the available information it was not possible to determine if any of these elements diverted the attention of the pilots during the second approach to the ship.
Role of flight instructor
The instructor held an instructor rating, night VFR rating and instrument rating with CASA approvals to train and examine pilots for those ratings. In regard to the EC135 helicopter, the instructor held the type rating and CASA approval to issue the rating. As such, the pilot was qualified to conduct, instruct, and assess night and instrument flight from the right or left seat of EC135 helicopters. Based on these qualifications and MPT experience, the instructor met the operator requirements for a training and checking pilot.
In addition to CASR Part 61 requirements, the operator required a base check and line check every 12 months to ensure that pilots were able to operate the EC135 type and conduct MPT in accordance with SOPs. Based on the operator’s pilot records, the instructor was within the validity periods of both checks but there was contradictory information about the last line check. The ATSB analysed all of the available information and concluded that the instructor was probably line checked on 5 April 2017 but there were variations from SOPs that were not recorded.
Since that check the instructor had been operating EC135 helicopters in a mix of line flying and flight training/assessing, including a number of ship landings by day and night. The ATSB analysed the ADS-B data for the instructor’s previous night MPT flights at Port Hedland in January 2018 and identified deviations from SOPs by the instructor.
Having operated EC135 helicopters for about 2.5 years, the instructor was familiar with the format of the integrated digital displays. Although this was an advantage, the 2 EC135 helicopters at Port Hedland were single-pilot variants with modified instrument panel/consoles and flight instrument configuration. For the instructor in the left seat, this could undermine monitoring effectiveness, especially at night. The instrument panel configuration is addressed further in a later section.
During line training for a single-pilot operation, the instructor was the pilot in command but generally not directly involved in operation of the helicopter. This role is primarily to support a pilot with the appropriate licences, ratings, and experience to acquire the knowledge and develop the skills specific to the operation. To do that effectively, the instructor needed to monitor the flight path and critical parameters, alert the pilot under supervision to any sustained deviations from SOPs, and provide advice before, during, and after the flight. Critically, if the pilot under supervision was unable to operate the helicopter within acceptable parameters, the instructor was expected to intervene and take over control before a dangerous situation developed.
As outlined previously, conduct of the line training role in the context of the non-conforming first approach, go-around, and descending transition into the second approach was intrinsically high workload for the pilot under supervision. For the Grade 1 instructor and flight examiner it should have been significantly less so, especially in the context that their role provided the key assurance of safety.
Diversion of attention or inattention might occur in this operational context for the following reasons:
- disproportionate attention to, or over reliance on, limited visual cues
- lower intensity monitoring on (incorrect) basis that autopilot vertical mode engaged
- communication with pilot under supervision about go-around and next approach
- lower intensity monitoring on basis that pilot under supervision was controlling the helicopter.
In the context of higher workload associated with reference to the primary flight display, the instructor might have prioritised visual cues over instrument data. This might be correlated with the instructor account that the helicopter was on final approach when the water impact occurred. Additionally, when the instructor was flying at Port Hedland in January 2018, altitude maintenance at night was less consistent when the pilot lost sight of the ship during circling.
The instructor advised the ATSB that it was standard practice to use the autopilot including vertical mode until reaching the final ‘gate’. However, as the flying at Port Hedland in January 2018 showed, this does not appear to have been consistently applied. For the instructor in the left seat, the autopilot mode annunciation was also not salient and probably not part of a normal scan.
As discussed in the previous section, it is not clear when the instructor might have been providing feedback on the first approach and go-around with advice for the next approach. If there was difficulty communicating with the pilot under supervision as a result of the intercom selection, this would have been distracting and possibly delayed corrective action.
From the instructor’s perspective, the pilot under supervision was controlling the helicopter until the radio altimeter alert at 300 ft. On that basis and given the pilot under supervision had conducted the 3 previous downwind/base segments at night without apparent problems, the instructor might have been less attentive to the primary flight display or standby instruments during this phase of flight.
Consideration of influence
It is apparent from the right turn onto base late in the sequence that lateral control inputs were being applied. Some reference to the primary flight display or standby attitude indicator might be expected during this manoeuvre but neither pilot identified the excessive descent rate. This suggests a loss of situation awareness and possibly some level of disorientation that also had implications for the recovery actions discussed in the next section.
In line training for a single-pilot operation, the pilot under supervision operates the helicopter as if in command and the supervisory pilot (as pilot in command) monitors, advises, and intervenes as required. When circling at night in a degraded visual cueing environment during a line training flight, both pilots were required to apply instrument flying skills integrated with reference to any relevant visual cues.
If the operational roles for line training were maintained down to 300 ft, as related by the instructor, the implication is that there was a breakdown in the instrument scan of both pilots. For this analysis, this is considered as the default scenario (1).
As discussed, the workload was high for both pilots in their default roles, but their individual qualifications and experience should have been sufficient for either pilot to detect the abnormal flight path. Given their qualifications and experience, this was especially true of the instructor. This infers that both pilots were diverted from, or otherwise inattentive to the primary task of instrument flying, for reasons that could be independent or interrelated. Fatigue as a factor potentially affecting the performance of both pilots is considered later.
In an alternative scenario (2), if the instructor had taken over control of the helicopter after the first approach, the pilot under supervision would not be obligated to monitor the primary flight display. As such, management of the flight path would rely on the instructor, and 2 of the factors to be considered later – instrument panel configuration and capability in degraded visual cueing environments – might have affected the capacity of the instructor to control the flight path.
The ATSB acknowledges that the instructor recalled taking over 300 ft and the ADS-B data shows a partial recovery from that point. However, the instructor did not recall the sequence of events in detail, and recollection of circuit position before the impact was incorrect. Given memory of an event can be distorted by various factors, the ATSB considered the conditions that related to scenario 2.
In principle, the scenario in which the instructor takes over control to relieve the pilot under supervision after the go-around has instructional advantages. By taking over, the instructor can provide feedback with a demonstration of technique and desired outcome while allowing the pilot under supervision to rest, observe and assimilate information.
A further consideration for the instructor is the time available to transfer the marine pilot from Squireship to the port then return to C1/C2 to pick up the marine pilot from the following outbound ship. The shipping schedule did not allow for any additional flying time so after the missed approach, there was an operational imperative to land off the next approach. In that context, it would generally be an advantage for an MPT-qualified instructor to take over control. However, on this occasion the instructor might have considered that workload associated with cross-cockpit instrument scanning, and prior experience in a degraded visual cueing environment nullified the advantages of taking over. And, if the instructor felt fatigued, the monitoring task might have been considered less risk than controlling the helicopter.
The ATSB noted a correlation between the second circuit around Squireship and the instructor’s previously observed actions when flying at Port Hedland to not use a vertical upper mode in the circuit with high descent rates developing during the base turn. This suggests that instructor might have been flying the helicopter during the second circuit but was inconclusive.
The ATSB considered that the evidence related to who was flying the helicopter during the second circuit was ambiguous. Irrespective of who was controlling the helicopter, the prime responsibility of the instructor as pilot in command was to ensure the safety of the flight.
|
Contributing factor During the downwind and base segment of the circuit, the pilots did not effectively monitor their flight instruments and the helicopter descended below the standard circuit profile at excessive rate with decaying airspeed. Neither pilot responded to the significantly abnormal flight path or parameters until the radio altimeter alert at 300 ft. |
Radio altimeter alert and pilot response
When the radio altimeter alert activated at 300 ft the rate of descent was about 1,700–1,800 ft/min and the airspeed was about 34 kt. As related by the instructor, that alert was the prompt to take over control and conduct a missed approach (go-around). Despite that, by 200 ft, the descent rate was still about 1,700 ft/min then reduced to about 1,300 ft/min at water impact.
Without intervention, the rate of descent would have continued to build and the impact with water may not have been survivable. Although the action reported by the instructor had a positive effect by reducing the rate of descent, the ATSB considered the range of potential actions and outcomes in the accident scenario.
Setting the radio altimeter alert to 300 ft for every approach was intended to be an aural and visual cue for a nominal committal height. Initiation of a missed approach as reported by the instructor implied an awareness that the flight path was abnormal and outside the operator’s stabilised approach criteria (rate of descent exceeding 700 ft/min when operating below 30 kt airspeed). However, the instructor was unable to recall any critical details that might have been derived from the flight instruments or external reference during this phase and the collision with water was unexpected.
The time interval from the radio altimeter alert at 300 ft to water impact was about 12 seconds. From 300 ft, if a nominal reaction time of 4 seconds and descent rate of 1,700 ft/min was applied, the helicopter would have descended an additional 100 ft before pilot inputs were made. This was not reflected in the data, which showed the descent rate stabilised by 200 ft. As such, the pilot response time was shorter, or the helicopter response was almost instantaneous. In either case, the instructor was able to make further inputs during the 7-second period between 200 ft and the water surface.
The ATSB considered the potential for vortex ring state (see Appendix D) to have prevented recovery prior to water contact. However, a review of ADS‑B data identified that the application of collective reduced the rate of descent, so that was considered unlikely.
With both engines operating, the EC135 had a significant surplus of engine power/torque that could be applied through the collective to reduce the descent rate. At the request of the ATSB, Airbus Helicopters replicated the accident scenario in an EC135 simulator and found that the helicopter could be recovered from as low as 100 ft if the appropriate go-around procedures were carried out.
The data collection units (DCUs) for each engine recorded a set of parameters in response to the main rotor impact with the water and engine ingestion of water. Given the high descent rate and rapid inversion of the helicopter, it is likely that the data was recorded early in the accident sequence and is an indicator of engine operation immediately before the impact.
The data indicates that both engines were operating normally up to the collision with water and were not operating at or near maximum power/torque when those parameters were recorded. This is not consistent with optimisation of the performance of the helicopter, as would be expected for a go-around, especially in an emergency situation. This could have reflected the instructor’s disorientation at the time and/or missed approach technique.
The ATSB did not have any comparative data that included a missed approach conducted by the instructor but the missed approach immediately preceding the accident was supervised by the instructor. Although the ADS-B data indicates a missed approach was initiated at 500 ft, the helicopter descended to 325 ft over a period of 22 seconds before a climb was achieved, contrary to standard practice that prioritised obstacle clearance. If that technique was applied to the subsequent missed approach, recovery was unlikely.
It is instructive to look at the flight data from the 5 January 2018 night flights - where the instructor was flying during line operations - for 2 related reasons. Firstly, on 2 of those approaches, the rate of descent exceeded the specified parameters and the instructor recovered without conducting a go-around. Secondly, the data suggests that initiation of some flight path corrections and recoveries were coincident with the routine radio altimeter alert at 300 ft.
It is therefore possible that the instructor responded to the radio altimeter alert in a manner consistent with the pattern evident in the comparison flights in January 2018. That is, collective input was consistent with a profile correction rather than a go-around. The ATSB also identified that the instrument layout in the helicopter probably hampered the instructor’s response following the radio altimeter alert. This is discussed further in a following section.
The radio altimeter alerting function is recognised as an effective risk control for controlled flight into terrain/water. By setting the alert for 300 ft, the operator was conforming to a standard industry practice that appeared to be effective in almost all cases. The ATSB is unaware of a safety case for increasing the height of this alert, although some operators prescribed an additional alert at 500 ft.
|
Contributing factor The instructor responded to the radio altimeter alert, reducing the rate of descent from about 1,800 ft/min to 1,300 ft/min, but this response was not consistent with an emergency go-around and did not optimise recovery before collision with water. |
Survival scenario and outcomes
Survival scenario
Both pilots were equipped with the standard safety equipment including flight helmets and inflatable personal flotation devices with distress flares and personal locator beacons. At the time of the occurrence the operator did not provide emergency breathing system (EBS) for MPT pilots and was not required to do so. The helicopter was equipped with an emergency floatation system and life rafts.
The instructor advised the ATSB that the collision with water was unexpected, and there was no indication that the pilot under supervision was aware of the helicopter trajectory and impending collision with water. As such, there was no opportunity to attenuate the impact forces (abrupt pitch and/or power changes) and the pilots were not mentally or physically prepared for immersion in the sea.
Although the helicopter descended into the water in a relatively level attitude, it immediately inverted as a consequence of its trajectory at impact, reaction to the main rotor blades striking the water, and its inherently high centre of gravity. The distortion to the transmission deck and the force of water during the impact sequence fractured the left main cockpit windscreen and left cockpit chin window, which flooded the cockpit.
The helicopter was fitted with an emergency flotation system, that was capable of both automatic and manual inflation. Although the system was armed in accordance with the SOPs, the floats did not automatically inflate when the helicopter entered the water. There were no system defects and non-activation was attributed to rapid inversion of the helicopter. Float inflation was not manually selected and it is unlikely that post-impact inflation would have altered the survival outcomes as, even without activation, the helicopter remained afloat for a time period in excess of that required to exit the cabin.
Immediately following the impact sequence, the pilots were strapped in their seats within the inverted helicopter cabin that had quickly flooded with sea water. The helicopter was not equipped with emergency egress lighting and electrical power was probably lost during the accident sequence. Consequently, the pilots were in total darkness and probably experiencing shock from the sudden and unexpected onset of the dynamic impact sequence. In a very challenging survival situation, the initial flotation of the helicopter, sea state, and relatively warm water were advantageous.
However, without air to breathe in the flooded cabin, survival was dependent on escaping the cabin in a critically short time period. Pilots (and passengers) engaged in offshore operations are generally trained to do this by:
- orienting themselves in the cabin relative to their emergency exit
- operating the emergency exit
- releasing their seat belt while retaining a fixed reference point
- exiting the cabin and swimming to the surface.
Both pilots were seated next to access doors that functioned as their respective emergency exits. These doors could be fully released from the fuselage by operating the door handle then pushing the jettison lever downwards. The seat belt was released by rotation of the latch.
Neither of the pilot doors had been opened and the left door (instructor side) jettison lever was the only door handle/lever that had been operated to release the hinges. Both seat belts were undamaged and unlatched. The ATSB found that the door mechanisms and seat belts were capable of normal operation.
Instructor escape
Although aware of the jettison lever and door release process, following immersion the instructor was unable to operate the door and did not recall operating the jettison lever. This was not consistent with the recommended practice to identify then operate the emergency exit but was not critical on this occasion.
The instructor advised that the hole in the windscreen was located and the seat belt was released while holding onto the edge of the opening. After being initially restrained by the helmet cord, the instructor managed to swim out and to the surface. The sequence of identifying the exit then releasing the seat belt was consistent with the recommended practice.
From the instructor’s perspective, helicopter underwater escape training (HUET), last carried out in September 2015, helped with the escape and previous diving experience at night probably helped with orientation in the flooded cabin. One of the elements of the annual Civil Aviation Order (CAO) 20.11 check carried out with the instructor in July 2017 was operation of the emergency exits.
Pilot under supervision non-survival
The pilot under supervision did not escape and was later recovered from the cockpit area of the submerged helicopter. As the instructor did not recall any awareness of the pilot under supervision post‑impact, there was limited information about the pilot’s non-survival.
Based on the unfastened seat belt and helmet, and absent any intervention by the instructor, the pilot under supervision was conscious post-impact and had attempted to escape. Non-operation of the door handle or jettison lever for the adjacent exit door indicated that the pilot under supervision was probably disoriented and/or unable to recall or carry out the first 2 steps of the recommended escape sequence. Locating and operating the door handle and jettison handle before releasing the seat belt is essential for maintaining orientation.
At some point, the pilot under supervision might have realised that the instructor had escaped and attempted to follow the same exit path. If the pilot under supervision found the left door on the instructor’s side was still closed, it would have been disorienting, and might account for operation of the jettison lever.
The pilot under supervision had last completed a HUET course in 2011, which was well outside the operator’s requirements for MPT pilots to complete the course at 3-year intervals. This was identified as a safety factor and is addressed later in this section. Having completed the CAO 20.11 check conducted by the chief pilot on 5 March 2018, the pilot under supervision should have been familiar with operation of the EC135 emergency exits and been reminded of recommended underwater escape practices.
|
Contributing factor After the unexpected and significant water impact in dark conditions, the helicopter immediately rolled over and the cabin submerged then flooded. The instructor escaped through an adjacent hole in the windscreen and used flotation devices until rescued but the pilot under supervision was unable to escape the cockpit and did not survive. |
Helicopter underwater escape training
The chief pilot was aware that the pilot under supervision had not completed HUET in the previous 3 years and had arranged for a course as soon as possible. This was scheduled in the month following the planned line training at Port Hedland. Although the training and checking section of the operations manual allowed the chief pilot to extend the period between HUET courses, any extension was not expected to be more than 6 months. The ATSB noted that the operator’s requirements for HUET varied according to the base of operations, which was potentially confusing, but not a factor in this occurrence.
Marine pilot transfer operations are predominantly over water and often conducted in challenging offshore conditions. By utilising multi-engine helicopters, the operator reduced the risk of a ditching but as this occurrence shows, it did not preclude an inadvertent descent into the water and underwater survival scenario. The ATSB noted that the operator only required HUET for night MPT at Port Hedland, which reflected a higher risk profile than day MPT.
To ensure that pilots were able to manage emergencies in the EC135 type, the operator provided periodic CAO 20.11 checks that included operation of the emergency exits. These checks were primarily knowledge assessments and did not provide opportunities to practice skills in simulated emergencies. Although the recent CAO 20.11 check would have beneficial to the pilot under supervision and provided an opportunity to rehearse HUET procedures with touch drills, this was not considered to be sufficient to reduce the risk of offshore operations.
HUET is widely accepted as a necessary and effective risk control for offshore operations. Through exposure to simulated underwater escape scenarios including an inverted cabin in darkness, pilots (and passengers) are better prepared to implement the recommended procedures in adverse conditions.
Having completed HUET on 2 occasions, the pilot under supervision would have been aware of the principles and challenges of underwater survival. However, the ability to recall the procedures and carry them out after a sudden and unexpected impact sequence and in adverse conditions would been diminished by their lack of recency.
Given the lack of information about the post-impact capability and actions of the pilot under supervision, it was not possible to establish if HUET conducted with the preceding 3 years would have made a difference to the outcome. Despite that, based on the value ascribed to HUET by the offshore industry and the benefit claimed by the instructor in this occurrence, the lack of HUET recency was a factor that increased the risk of disorientation and non-survival.
This issue was discussed in the ATSB preliminary report and a safety advisory notice was issued.
|
Other factor that increased risk The operator rostered the pilot under supervision for marine pilot transfer flying without ensuring that helicopter underwater escape training (HUET) had been completed in accordance with the operations manual. Although the pilot under supervision had completed HUET in 2009 and 2011, the lack of recency reduced preparedness for escaping the helicopter following submersion. |
Instrument panel configuration
Context
In the context of this occurrence, development of the abnormal flight path was associated with insufficient attention to key parameters displayed on the primary flight display (PFD) or standby flight instruments. One of the factors that could have affected the pilots’ capacity to monitor the flight path and parameters in a degraded visual cueing environment was the instrument panel configuration of the 2 EC135 helicopters based at Port Hedland.
Instead of a centrally-oriented instrument panel with duplicated PFDs/navigation displays (NDs), the instrument panels of VH-ZGA and VH-ZGZ were oriented asymmetrically to the default pilot‑flying position (right seat) with the single set of displays offset to the right of the forward-view centreline. As a related variation from a standard EC135, the standby flight instruments were not the standard analogue set but a digital MD302 standby attitude module.
For the pilot under supervision in the right seat, the offset PFD/ND was adjacent to the standard position and not considered to be a disadvantage for instrument flying. However, when flying a visual approach, the pilot in the right seat had a more restricted external field of view relative to the typical panel. Although pilots generally adjusted to this and there was no evidence it was non‑compliant with certification guidance, it could have contributed to the inconsistent descent profiles of the 2 previous approaches. However, given the abnormal flight path occurred in the phase of flight where instrument reference rather than visual cues required most attention, the panel/console configuration was not considered to have affected the pilot under supervision.
The instructor advised that when operating from the left seat in VH-ZGA and VH-ZGZ, the PFD was the preferred source of flight information because of the relative size and brightness of the digital display. From instructing and assessing in the left seat of the standard EC135s and flying from the right seat of all of the operator’s EC135s, these displays were familiar. The instructor advised that the PFD in VH-ZGA was clearly visible from the left seat and allowed the monitoring role to be performed but cross-cockpit scanning increased workload and duplicate displays in a co-pilot panel were preferred. The instructor also advised of experience with cross-cockpit monitoring of instruments during earlier flying as an aeroplane instructor.
After further consideration, the instructor emphasised the high workload associated with addition of the cross-cockpit scan and their inside/outside scanning pattern. The instructor recalled that on the second approach to Squireship (after the radio altimeter alert occurred at 300 ft), the transition to the PFD and assessment of vertical speed was very difficult. For the instructor, opportunities to identify the rate of descent were limited by the ‘unreadability’ of the altitude trend bar on the standby instrument indication and location of the vertical speed indicator on the far (right) side of the PFD.
Overall, the instructor considered the instrument configuration to be compliant with regulations, consistent with industry practice, and suitable for most operations. However, in the context of the occurrence flight, the instructor found the operation to be difficult and considered that the outcome would probably have been averted if a primary flight display had been located in a co-pilot panel.
Use of the primary flight display
An advantage of cross-cockpit reference to the PFD as advised by the instructor was access to a large format attitude indicator. Even if this advantage was attenuated by higher workload associated with cross-cockpit scanning, operationally significant changes to helicopter attitude were probably detectable from the left-seat position.
Although the digital integrated presentation of primary flight information with other parameters is generally an advantage, this was not necessarily the case for cross-cockpit scanning. The ATSB considered contextual and explanatory factors that might have undermined the advantages of a PFD.
Firstly, the presentation of airspeed and altitude information on digital flight displays differs from analogue displays by utilising a scrolling-tape scale and a fixed pointer rather than a fixed scale and a radial-action pointer. In relative terms, the digital indications provide less salient visual cues to airspeed and altitude trends with more reliance on reading of figures. Although the instructor was familiar with this presentation, in the cross-cockpit scanning and high workload context, the airspeed and altitude information might have been less accessible to quick-glance interpretation.
Secondly, the ability of the instructor to read the airspeed and altitude indicators on the primary flight display from the left seat would have been affected to some extent by the luminosity of the display. Given the general instrument lighting was found on the lowest setting, it is likely that the PFD luminosity was also on a low setting, consistent with standard practice in dark night conditions. This might have further affected the readability of the presented data.
Finally, the instructor’s previous instructional experience in light aeroplanes was not equivalent to the complexity of the EC135 MPT operation and the instructor had limited experience in the left seat at night in VH‑ZGA or VH‑ZGZ. Of those 7 flights, in 2017 there were 2 MPT check flights to the anchorage and 2 non-MPT rating-related flights. In 2018, as part of the current Port Hedland roster period, there were 2 MPT check flights at night with experienced pilots then the line training flights prior to the accident flight.
If those 7 flights are filtered according to MPT operations in a degraded visual cueing environment, the result is one flight – the one before the accident flight. On that basis, the capability of the instructor to monitor the offset primary flight display from the left seat had not been fully exercised until the night of the accident. The risk management and organisational aspects of this is addressed in a later section.
Alternative source of primary flight information
Given the challenges inherent in monitoring the offset PFD from the left seat, the ATSB considered the utility of the MD302 standby attitude module as an alternative source of flight information for the instructor.
Consistent with its purpose, the module provided the critical flight information required for instrument flying in case the PFD failed. An advantage of this module in the context of this occurrence was the relatively accessible position within a secondary field-of-view reference either seat.
The main disadvantage of the module was the size of the 2 adjacent displays relative to a PFD, Given the module was certified for use as standby instrumentation and the instructor advised that their prescribed vision correction was suitable for EC135 panels, there was no apparent reason for the information to be inaccessible. However, the instructor described the indication of vertical speed (altitude trend bar) as unreadable.
Although increased workload and slower interpretation of detailed information might be expected with reference to smaller displays, the rate of movement of the altitude tape and extension of the altitude trend indicator would have been salient cues to the abnormal flight path. As with most instrument flying skills, assimilation of information is improved by familiarity with the representation of normal and abnormal conditions on a particular display.
With duplicated primary flight instrument displays in the standard EC135s, the instructor did not have any reason to refer to the standby instruments during training and assessment conducted in those models. And from the limited instructing or assessing experience at night in VH-ZGA and VH-ZGZ, it can be inferred that the instructor had limited opportunity to become familiar with this type of standby instrument.
Instrument and night‑rated pilots are required to periodically demonstrate their capability to operate in normal and abnormal conditions with reference to a ‘partial panel’, which are generally the flight instruments that continue to function after a primary system failure. As these exercises had been carried out by the instructor in standard EC135s and in an artificial checking environment, they were not representative of the occurrence conditions and it is unlikely that partial panel exercises had any relevant effect.
In the context of this occurrence, it is unclear if the outcome would have been different if the instructor had referenced the standby instrument module instead of the offset primary flight display.
Influence and risk
The instructor assessed that the configuration of the instrument panel and workload associated with cross-cockpit reference to the PFD was a factor in the abnormal flight path and recovery actions. For additional perspectives on the potential influence of the instrument panel configuration, the ATSB conducted a comparative analysis with reference to various certification and regulatory criteria and consulted expert pilots.
The ATSB consulted a range of certification criteria and industry association advice that applied to the positioning of flight instruments relative to the seat positions approved for flight crew. As the EC135 variant was configured for single-pilot IFR operation from the right seat, it was not required to satisfy any instrumentation standards for the left seat occupant. For the comparative analysis, the ATSB considered the extent to which the left cockpit seat conformed to the certification criteria or industry association advice for essential flight crew.
In general, the certification guidance advised that primary flight information was to be in front of each pilot so that it was readily or easily visible. Based on measurements of the other EC135, VH‑ZGZ, the angle between the left‑seat centreline and the primary flight display was 57°. This was not within or near the primary field of view (15° each side of straight ahead), although allowed the instructor to view the primary flight display with a moderate head turn to the right.
Although not addressed directly by certification guidance, viewing distance was considered by comparison with recommendations for the size of characters on displays. When viewed from the left seat position, the smaller numerals on the altimeter tape indicating 100 ft increments were below a commonly recommended height. This was critical when the helicopter was below 1,000 ft.
From an Australian regulatory perspective, VH-ZGA was suitably equipped for the night operation in visual conditions being conducted and for single-pilot IFR. In the absence of a second 5-inch attitude indicator (or other CASA-approved attitude indicator for primary use), it was not equipped for IFR helicopter operations requiring 2 pilots.
Practically, line training for offshore ship landings in a degraded visual cueing environment required both pilots to exercise a high level of instrument flying skill. Those demands were exacerbated by transitioning the pilot under supervision from day to night line training without a consolidation period. Given the similarities between IFR helicopter operations requiring 2 pilots and the line training scenario, the single-pilot panel configuration probably increased relative risk.
Further to the certification/regulatory aspects, the ATSB sought the perspectives of experienced EC135 pilots who had conducted training and assessing in VH-ZGA or VH-ZGZ. The only person with substantive experience was the chief pilot who advised that night line training and assessment was carried out in those variants before the occurrence without any perceived high risk. The chief pilot added that although the instrument panel configuration was considered suitable for monitoring line operations from the left seat, it was not suitable for controlling the helicopter from the left seat. The ATSB noted that after the accident the operator discontinued training/checking in the remaining EC135 variant, VH-ZGZ.
In summary, the ATSB considered that the configuration of the EC135 variant instrument panel disadvantaged the instructor and increased the risk of ineffective monitoring. When occurrence‑specific factors were taken into account, the lack of an accessible high-resolution integrated display of primary flight information probably exacerbated the effect of those factors and contributed to the abnormal flight path and water collision.
|
Contributing factor The instrument panels fitted to VH-ZGA and the operator's other EC135 helicopter at Port Hedland were equipped for single-pilot operation under the instrument flight rules. When used for flight training or checking in a degraded visual cueing environment, this configuration has a detrimental effect on the ability of an instructor or training/check pilot to monitor the helicopter's flight path and take over control if required. (Safety issue) |
The ATSB considered the CAO 20.18 equipment requirements as a risk control related to this contributing factor.
To be operated at night in visual conditions but without external cues for pitch and roll, the helicopter was required to be equipped with an autopilot or be operated by 2 pilots. The occurrence flight was a supervised single-pilot operation, and the helicopter was equipped with an autopilot. As such, if the pilot controlling the helicopter had utilised the autopilot to advantage while circling the ship, consistent with the CAO 20.18 requirement, the risk of an inadvertent descent would have been greatly reduced. The occurrence flight was not a 2-pilot operation in the conventional sense, so there was no procedural crew coordination and, in normal operation, no requirement for the instructor to control the helicopter from the left seat. As such, there was no regulatory requirement for the helicopter to be equipped with co-pilot flight instruments.
Although the absence of a PFD in the instructor’s primary field of view was an influential factor in this occurrence, the ATSB was not aware of any similar occurrences where this was identified as a factor. As helicopters are often equipped with suitable instrumentation for 2-pilot operation and the relative risk of operations varies, the exposure of the helicopter industry to this risk was difficult to quantify.
The ATSB considers that although CAO 20.18 did not address the equipment requirements for the pilot in command of line training for single-pilot operations, there was insufficient evidence to find that this was a safety issue.
Irrespective of specific regulations, operators are required to identify and mitigate risks, as the operator did after the occurrence. As such, the ATSB makes the following safety observation.
|
Safety observation For any operation that relies on the instrument flying skills of a second pilot, consideration should be given to the adequacy of flight instrumentation for that pilot. |
Instructor role
Introduction
As previously stated, since the pilot under supervision had not received any preparatory night flying and was conducting the third of 10 planned MPT operations at night, conformance and safety of the operation was heavily reliant on the instructor as pilot in command.
The ADS-B data for flights on the night of the accident indicated that the first 2 approaches to ships at C1/C2 and the go-around were not conducted in accordance with the operator’s SOPs. This indicated that both pilots were having difficulty in their respective roles with respect to flight path management.
The instructor held the necessary qualifications for MPT operations at night in the EC135 type and held a multi-engine helicopter instrument rating. Although the instructor’s proficiency had been checked at the applicable intervals, and no significant deficiencies were identified, the scope of these checks did not include specialist skills such as MPT.
To manage line training generally, the instructor was required to apply knowledge of instructional technique, helicopter systems, and SOPs. For the purpose of training pilots for MPT operations, the instructor also required skill to manage flight paths in degraded visual cueing environments both manually and via the helicopter’s automation. In the early stages of training, the instructor was typically required to apply the requisite knowledge and skill from the left seat to provide pre-emptive advice and feedback to the pilot under supervision with intervention as required for safety.
The Grade-1 instructor had substantial training and assessing experience from the left seat of helicopters and there was no indication of any significant deficiencies related to the knowledge requirements of line training. For the EC135 specifically, the instructor had recorded 164 hours of day instructing and 48 hours of night instructing.
Although instructional qualifications and experience are generally beneficial, these are oriented to the competency standards for CASR Part 61 licences and ratings rather than conduct of specialist operations. Line training and assessing was also carried out by the chief pilot who was not an instructor. As such, flight instructing qualifications and experience was by itself neither necessary nor sufficient for the line training role.
Marine pilot transfer experience
The instructor had been operating EC135 helicopters on MPT operations and flight training/assessing for 2.5 years. This was initially in the Hay Point and Gladstone areas, with the addition of Port Hedland in the year prior to the occurrence. By the time of the occurrence, the instructor had recorded 450 ship landings in day and night conditions. Most of those ship landings were conducted as pilot in command, controlling the helicopter from the right seat.
Given the occurrence was to an outbound ship at Port Hedland and this offshore operation was relatively more demanding at night than some of the other MPT flying conducted by the instructor, the ATSB reviewed the instructor’s experience at night in the Port Hedland area.
The ATSB found that the instructor had limited experience at Port Hedland, having been involved in 10 landings to outbound ships near C1/C2 at night, including 3 single-pilot operations as pilot in command (flying the helicopter from the right seat). These 3 landings were conducted during a night shift in January 2018, along with 2 ship landings to inbound ships at the pilot boarding ground. Although there was moon illumination on those occasions, due to cloud the flights were probably conducted in degraded visual cueing environments.
A review of ADS-B data for the 5 flights in January 2018 identified inconsistent altitude maintenance with varying rates of descent in the circuit. When the helicopter developed abnormal rates of descent on some of the (final) approaches there was a correction towards the nominal 7° flight path, in some cases this correlated with the radio altimeter alert at 300 ft. This indicated that the instructor was finding it difficult to maintain a stable flight path and conform to the SOPs. The ATSB noted that the instructor was controlling the helicopter from the right seat with a PFD in the primary field of view, which might account for the flight path corrections.
In the normal course of line flying or line training/assessing, the instructor did not conduct ship landings from the left seat. There was no record of this occurring, although the instructor indicated that the first line training flight by day and first line training flight by night with the pilot under supervision might have been such occasions. As a training/assessing pilot, the instructor had the opportunity to observe landings to ships at night conducted by experienced MPT pilots.
Line check and flight review/check
The primary means for the operator to ensure that the instructor was proficient at night MPT operations was via initial and ongoing annual night line checks. As MPT pilots were required to hold a night VFR rating and some pilots also held an instrument rating, the flight review and proficiency check for those ratings were also important risk controls for night operations.
According to operator records, the instructor had completed the initial line check at night on 8 March 2016 and a subsequent check at night on 5 April 2017. The chief pilot who conducted both checks recorded that the instructor’s flying was satisfactory on both checks involving a total of 3 ship landings at night.
There was contradictory information about the flight on 5 April 2017 that was recorded by the chief pilot as a line check at night of the instructor and by the instructor as a night VFR flight review of the chief pilot. Although there was insufficient information to conclusively resolve the discrepancy, the ATSB considered it more likely that the instructor was controlling the helicopter, and the flight was probably a line check as recorded by the chief pilot.
Given the line check in 2017 was the most recent check and was carried out at night from Port Hedland with an approach to ships at the pilot boarding ground and near C1/C2, this was considered to be a relevant indicator of the instructor’s MPT proficiency at the time of the accident, noting there may have been some change in the intervening 12 months.
For the flight conducted by the instructor and chief pilot on 5 April 2017, the conditions were suitable for night VFR and there was substantial moonlight (elevation 53° with 68 % of the visible disk illuminated). ADS-B data showed that the approach profiles were generally consistent but circling to both ships was conducted at about 1,000 ft, which was higher than the specified circuit height of 700 ft. And on both approaches the airspeed through 500 ft was about 40 kt, which was lower than the specified 60 kt for the ‘finals gate’.
Based on the flight data review, the ATSB considered that the instructor (as the likely pilot controlling the helicopter) did not demonstrate a capability to operate in accordance with the SOPs at night in relatively favourable night VFR conditions. The chief pilot advised there were no concerns about the instructor’s ability to conduct night MPT operations, and there was no evidence that the instructor identified or addressed those variations. Although a link between the demonstrated level of SOP conformance and a prospective inadvertent descent, such as in the occurrence, was not clear at the time, this check did not provide any assurance that the instructor was proficient at night MPT, especially in a degraded visual cueing environment.
Having completed a night VFR flight review in May 2016 and instrument proficiency check in June 2017, the instructor was within the respective validity period of both ratings. To satisfy either review/check the instructor was required to demonstrate instrument flying capability and recovery from unusual attitudes with full and partial panel. There were no indications of any performance decrements in these areas.
While the night VFR rating was necessary and the instrument rating was advantageous for night MPT, the data review of the instructor’s flight on 5 April 2017 indicated that those qualifications alone were not sufficient to ensure that the instructor was proficient at visual circling at night in degraded visual cueing environments. The ATSB also noted that the flight review and proficiency check were oriented to conventional helicopter operation with circuits and instrument approaches at aerodromes.
|
Contributing factor When operating at Port Hedland in degraded visual cueing environments, the instructor had not been able to ensure that circling approaches were consistent with the operator's standard operating procedures. This probably limited the support provided to the pilot under supervision on the occurrence flight and, in combination with other factors, probably contributed to the abnormal flight path and partial recovery. |
Safety reporting
Following analysis of the ADS-B data from the night flights conducted by the instructor in January 2018, the instructor was presented with the data and asked about any recollections about those flights. Noting that it was 3 years since those flights, the instructor did not recollect anything about flights from Port Hedland during that roster period.
The chief pilot advised the ATSB that the instructor did not report any significant variations from SOPs or seek any related training. Similarly, no report was identified in the operator’s reporting system. Assuming that the instructor was aware of the SOPs and related variations on those flights in January 2018, it is not clear why a report was not made, or a remedy was not sought. The instructor advised that if those flights had been knowingly flown out of tolerance, they would have been reported and remedial training would have been sought.
According to the safety management system manual, safety hazards and deficiencies such as deviation from SOPs were to be reported through the electronic system accessible via the internet. It was intended that these hazards and deficiencies would be investigated, corrected, and discussed by the safety committee. A key feature of the operator’s ‘Just Culture’ policy was the differentiation of various types of normal human error from intentional non-compliances, with guidance that implied, but did not guarantee, nil disciplinary action for the former.
Over the 3 years the safety management system was operating, there was evidence that the reporting of occurrences and safety hazards was improving, and issues were being addressed. None of these reports involved pilots self-identifying concerns about their proficiency so there was no comparative example. A safety survey reportedly conducted in February 2018 would have been a useful reference for safety culture, but the results could not be located. There was no record of a safety survey in 2017 or 2016.
As the head of operations for the CASR Part 141/142 organisation and nominal head of training and checking, the instructor was partly accountable for the flight standards of the operator’s pilots. As such, it was presumably difficult to self‑report any performance issues or to objectively assess the associated risk.
Over the 3 years the safety management system was operating, there was evidence that the reporting of occurrences and safety hazards was improving, and issues were being addressed. None of these reports involved pilots self-identifying concerns about their proficiency so there was no comparative example. The ATSB considered the safety surveys conducted in 2017 and 2018 as indicators of the operator’s safety culture. Although the surveys did not indicate any systemic issues, the lack of information about survey response rates, and the survey methodology, did not allow a conclusion to be reached.
|
Other factor that increased risk Although the instructor was flying when significant deviations from standard operating procedures occurred during night approaches in January 2018, these were not reported to the operator or otherwise addressed by the instructor. |
Pilot training and assessment
Line training arrangements
Prior to line training, the instructor provided the pilot under supervision with refresher flying on the EC135 type and assessed this satisfied the requirements of a type rating flight review. This review of normal and abnormal procedures was consistent with the operator’s requirements for a new pilot.
On the first day of line training (the day before the accident), the pilot under supervision was involved in 9 ship landings and was controlling the helicopter for at least 8 of those. At the end of the session, the instructor assessed that the pilot under supervision was competent and safe, and just needed practice for more familiarity in MPT operations.
Line training continued the next day with a ship landing/take-off in the early evening. The instructor counted this as the tenth ship landing/take-off by day and a conforming line check. At this point, the instructor considered the pilot under supervision complied with the operator’s requirement for 10 landing/take-offs as pilot in command under supervision and was competent for line operations by day. There were no contrary indications in the related ADS-B flight data.
Consistent with the schedule emailed to the chief pilot 2 days before, the instructor then transitioned the pilot under supervision into night MPT operations on the next flight. Given the instructor considered that the pilot under supervision was competent for day MPT, there was no policy or procedural impediment to proceeding with the night line training. As such, continuation of the training was at the discretion of the instructor and chief pilot, who did not identify this as a significant risk.
The first landing/take-off at night was to a ship inbound from the pilot boarding ground near the anchorage. It is possible that the instructor conducted this approach. After a 2‑hour rest period, the next flight was to an outbound ship nearing C1/C2 at the end of the shipping channel followed by a quick turnaround for the occurrence flight to the outbound Squireship.
It is apparent from the ADS-B data that the pilot under supervision had been progressively adapting to day MPT operations in the EC135 but was having some difficulties with the introduction of night approaches. This could be anticipated, given the pilot under supervision was transitioning from the Bell 206L to the EC135 helicopter with different handling characteristics, more complex systems with automation, and digital presentation of flight data.
Although these factors were present during day operations, the increased reliance on flight instruments and the higher workload associated with a degraded visual cueing environment would have exacerbated their effects. The transition from flying at night using night vision imaging systems to unaided night VFR in an offshore environment was an additional challenge and potentially disorienting.
Although previous MPT and EC135 experience was an advantage for the pilot under supervision, this was attenuated by the 7-year time interval, relatively low EC135 hours, and limited ship landings/take-offs as pilot flying at night. Overall flying experience in the previous 3 years was predominantly at night but consisted of a relatively low amount of flying hours.
In that context, and consistent with training for pilot licences, it is advisable for instruction to be provided in stages with intervening consolidation periods. That allows the trainee to practice a defined set of unfamiliar skills and reach a certain level of expertise before further complexity and workload is introduced. As a precaution, exposure to more demanding environmental conditions can be controlled to further manage the risk.
As a Grade 1 instructor, the instructor would have been familiar with the principles of training consolidation. The instructor was aware that these principles had been applied to the MPT operation because the chief pilot had arranged for the instructor (after joining the operator) to consolidate day MPT before being introduced to night MPT.
With a deficit of 2 pilots representing 25% of the normal roster group, there was an operational imperative for the pilot under supervision to be trained and cleared for line flying as soon as practicable. In the short term, there was also a requirement for the operator to assign a substitute pilot to the duties originally assigned to a suspended pilot, until that pilot was cleared back to line operations. It is likely that the short notice scheduling of night line training that included the occurrence flight was influenced by both of these factors.
There was another incentive for the pilot under supervision to be trained and cleared for line flying as soon as practicable. If the instructor completed the line training before flying out of Port Hedland for leave over the weekend, there would be no need to return for the remaining days of the rostered duty.
Commercial imperatives and personal incentives are an unavoidable element of the operational environment. In general, operators manage the risks associated with these potential influences by establishing an operational framework that includes SOPs and a safety management system. To ensure conformance and safe outcomes, operators will select and train suitably qualified personnel, then assign duties according to experience level, with an appropriate level of support and ongoing supervision.
If the pilot under supervision was given the opportunity to consolidate day MPT operations after the requisite 10 ship landings, night operations could then have been introduced with lower cognitive workload for both pilots and reduced risk of abnormal flight paths. In the context of this occurrence, this would have provided roster relief for the 0600 to 1800 day period and released an experienced pilot to carry out night flights. As another benefit, in the short term at least, the risk of fatigue for the pilot under supervision would have been lower.
A period of general night flying prior to starting night line flying would also have allowed the pilot under supervision to become more familiar with the digital instrumentation and practice instrument flying in that helicopter type. A pilot will typically learn more effectively from a graduated introduction to more demanding environmental conditions and complex procedures with the added benefit of lower operational risk.
Line training was a key element in the operator’s management of the risks associated with offshore ship landings/take-offs in day and night conditions. Although line training is often carried out on an opportunity basis and requires adjustment to individual capabilities, the specification of a staged training schedule with competency criteria assists the effective management of risk.
|
Contributing factor The pilot under supervision was introduced to line flying at night in a degraded visual cueing environment immediately after completion of the minimum-required 10 ship landings by day and without any preparatory night flying. Given the pilot under supervision was transitioning from a different helicopter type and operational environment, the lack of consolidation contributed to high cognitive workload for both pilots and increased the risk of sustained flight path deviations. |
Management of pilot training and assessing
Prior to joining the operator, the instructor was chief flying instructor for a flying school associated with the operator and held an EC135 type rating with minimal operational experience. Between August and November 2015, the instructor was inducted into the operation and completed EC135 familiarisation training and a multi-engine instrument proficiency check.
The instructor then operated as an EC135 line pilot for MPT operations on the east coast and carried out some rating proficiency checks and flight reviews as Grade-1 instructor or flight examiner. In March 2017, an external instructor conducted an EC135 instructor standardisation related to licences/ratings and instructors from Airbus helicopters provided further type-related training.
In April 2017, the chief pilot carried out a night line check at Port Hedland with the instructor in the command seat. The chief pilot recorded that the check including one ship landing/take-off carried out satisfactorily near C1/C2. It should be noted that the conditions were not challenging.
In June 2017, a CASA flight examiner evaluated the instructor’s EC135 type and instrument proficiency as the pilot controlling the helicopter in the right command seat then flight examiner proficiency as supervising pilot from the left seat. These were found to be satisfactory and the ratings were renewed/revalidated.
None of the proficiency checks to renew the various CASR Part 61 ratings were oriented to MPT operations and were not intended for that purpose. The function of the line check was to assess proficiency in MPT operations from the right command seat. As a result, the capability of the instructor to supervise MPT operations from the left seat had not been assessed. Also, when training or supervising qualified pilots, there was generally limited need for the instructor to take over control from the left seat.
The appointment of pilots to conduct training or checking was at the discretion of the chief pilot. A company pilot who held an instructor rating with multi-engine training approval, command instrument rating, other applicable endorsements/ratings, and with appropriate operational experience could be approved for training/checking duties. No further training/checking of the instructors was considered necessary by the operator unless the chief pilot identified a specific requirement.
At the time of the occurrence, the operator was approved to conduct flight training and reviews or checks for licences/ratings in accordance with CASR 141/142. The instructor was the nominated head of operations, which was equivalent to the prior role of chief flying instructor in the previous regulatory regime and was on the same organisational level as the chief pilot.
The operator did not maintain a CASA-approved training and checking organisation in accordance with CAR 217, which was not a requirement for charter operations such as MPT. Any flight training or assessment other than CASR 141/142 was carried out as a function of the air operator’s certificate as determined by the operator. Although CAR 217 only applied to the operator if CASA issued a direction, the guidance provided for training and checking organisations is a useful reference.
One of the key components of a CAR 217 organisation is the selection, training, and maintenance of continued competency of training and checking personnel. This is closely related to another component that addressed quality assurance audits and the over-sight of the standards of check pilots.
Although the operator prescribed minimum qualifications, applicable experience, and chief pilot discretion for pilots selected to carry out the AOC-related training and assessment, there was no process to train or assess the initial or ongoing role-competency of those pilots. In an environment where the instructor was the CASA-approved head of operations for the operator’s CASR Part 141/142 organisation and a CASA-approved flight examiner, expertise in those domains was presumed to be sufficient for related elements in similar domain.
|
Other factor that increased risk The operator's training and assessing procedures for marine pilot transfer operations did not provide assurance that pilot under supervision experience, helicopter instrumentation, and instructor capability were suitable for line training at night in a degraded visual cueing environment. (Safety issue) |
Circuit and approach procedures
Circuit profile and parameters
For operations to ships by day or night, the operator specified a downwind segment at 700 ft above the water and 70–80 kt airspeed, then a turn through 180° on the base segment with combined descent and deceleration to intercept final approach at 500 ft and 60 kt groundspeed ('final gate'). Further descent and deceleration were contingent on the disposition of the helicopter relative to the ‘sight picture’ for a nominal 7° profile.
To carry out a descent while decelerating and turning requires a high rate of information processing with skilful coordination of controls. If that manoeuvre is carried out at night in a degraded visual cueing environment, the processing and skill demands increase further. Compared to a level constant-speed turn, this pilot workload increases the likelihood of an abnormal flight path. When this manoeuvring is in the vicinity of 500 ft (above water), the consequences of any attentional or skill deficits are likely to be significant.
For airspeeds above 60 kt, the upper modes of the autopilot were available to manage the altitude, vertical speed, and heading of the helicopter. However, the pilot was still required to closely monitor the airspeed and rate of descent and could expect to adjust the power/torque as the airspeed varied and the target altitude was reached. By nominating 60 kt as the ‘final gate’ airspeed, the operator did not provide a buffer for any inadvertent airspeed loss during the turn. If the airspeed decayed below 60 kt, the upper modes disengaged, and the helicopter would not necessarily hold the selected altitude (subject to power/torque).
In the company’s east coast operations, there was a contract requirement to overfly the ship on arrival to allow the pilot to inspect the landing site and was the default procedure when the Port Hedland operation started in March 2017. To conduct this arrival procedure in a degraded visual cueing environment at night, the pilot transitions from instrument flying for the ship overflight and visual inspection then back to predominantly instrument flying for the circuit with reference to the ship lights for positioning. Transitions between instrument and visual flying contribute to pilot workload and increase the risk of disorientation.
Straight-in approaches minimise manoeuvring at low level prior to final approach and were preferred by the experienced line pilots at Port Hedland and the chief pilot as more efficient with less risk at night. For offshore approaches at night, HeliOffshore recommended a straight-in approach and landing rather than a circuit (see the section titled Non-regulatory guidance – HeliOffshore).
Although straight-in approaches were allowed by the operations manual, the description of the circuit procedure in the manual suggested that it was the default method. The instructor considered that to be the case and had generally conducted circuits when operating at Port Hedland in January 2018. It is acknowledged that a circuit may be required for various reasons, such as a transition from inbound track to landing direction and after a go-around so related training and assessment is required.
No specific risk assessment was carried out for the Port Hedland operation and the operator did not perceive that it was significantly different to the existing operations.
Automation procedures and practices
One of the contributing factors to this accident was operation of the helicopter on the second circuit without a vertical navigation mode engaged. This was not consistent with standard or expected practice and was an absent risk control for inadvertent descent and controlled flight into terrain/water.
The chief pilot advised that pilots were trained to keep the upper modes engaged until passing the ‘final gate’ and descending below 500 ft on the nominal 7° profile to the ship. From that point onwards, the pilot was required to make manual inputs as the upper automation modes were unavailable below 60 kt. Although this was considered to be the default practice, use of the autopilot and mode selection was effectively at the discretion of the pilot in command.
Following the occurrence, the instructor advised that use of the autopilot upper modes in the circuit was standard practice but did not recall any detail about autopilot use in the circuits around Squireship prior to the occurrence. As noted earlier, when the instructor was flying at Port Hedland in January 2018 the variation in circuit altitude indicated that a vertical upper mode was not used.
Although engagement of the upper modes of the 3-axis autopilot could reduce workload, the pilot was still required to adjust engine power/torque to control parameters such as airspeed or rate of descent. This is a complex coordination task when manoeuvring in accordance with the operator’s circuit procedure in a degraded visual cueing environment. If the pilot is not familiar with the autopilot interface and/or the helicopter is in a dynamic flight state, the high short-term workload associated with managing the autopilot modes might be perceived as a disadvantage.
That said, it is in high workload conditions that the autopilot provides significant safety benefit. The regulatory requirement for the helicopter to be fitted with an autopilot/stabilisation system when operated single-pilot in a degraded visual cueing environment underscores this point.
In addition, the Flight Safety Foundation and HeliOffshore provided standards and guidance to the helicopter offshore industry that specified the provision of a 4-axis (or 3-axis if risk assessment allowed) autopilot with policies/procedures to ensure appropriate use. This included integration of automation in specified approach profiles with coupling of approaches until the committal point. Although the autopilot in VH-ZGA was not usable below 500 ft, it could be used in a circling approach until visual cues were available on final approach.
Another consideration for EC135 operations is pilot interaction with the stabilisation system when the upper modes are not engaged. One advantage of the system is reduced pilot workload because the helicopter will hold an attitude that is selected by the pilot. Although this provides an element of autopilot operation, the pilot was required to manipulate engine power/torque and modulate attitude through movement of the cyclic with/without force trim switch or beep trim.
In their investigation of a Sikorsky S-92A accident in the Nova Scotia region, the Transportation Safety Board of Canada (TSB) addressed use of the cyclic trim release button, which is equivalent to force trim release. It found that depressing and holding the cyclic trim release button, while operating in a degraded visual environment, increased pilot workload and contributed to control difficulties that resulted in an unstable approach that developed into vortex ring state.
Although any use of force trim release in this occurrence was not recorded and was undetermined, this was a potential factor that increased risk. The ATSB noted the TSB caution that: if manufacturers’ flight manuals and operators’ standard operating procedures do not include guidelines for the use of the cyclic trim release button, it could lead to helicopter control problems in a degraded visual environment due to the sub-optimal use of the automatic flight control system. HeliOffshore recommended that when flying a circling approach in a coupled autopilot mode, adjustment of the flight path should be through beep trim until the committal height.
By not specifying that the autopilot upper modes were to be used in the circuit as a standard procedure, the operator did not minimise the risk of disorientation.
Stabilised approach criteria
As the helicopter descended during the second circuit to Squireship, the rate of descent developed to be about 1,700–1,800 ft/min passing 300 ft and the airspeed had reduced to about 30 kt at 75 ft. This was an unstabilised aircraft state that was well outside industry practices.
Specification of stabilised approach criteria is an important risk control for prevention of controlled flight into terrain. It provides clear guidance as to operational boundaries and is designed to assist a pilot or crew to identify and correct unsafe conditions or carry out a go-around. At the time of the occurrence, CASA guidance for operations manuals (CAAP 215-1(3.2) Operations Manuals) simply listed stabilised approach criteria as an item to be addressed.
According to recommended practices developed by HeliOffshore, pilots should select the final landing configuration by 1,000 ft and aim to be stabilised by 500 ft. If the helicopter was not stabilised by 0.5 NM (926 m) or 300 ft above the landing site, an immediate go-around was required. To be stabilised, the helicopter was required to be on the correct flight path at an appropriate speed with rate of descent no greater than 700 ft/min.
In the operations manual under the heading of stabilised approach criteria, the operator provided general advice for conducting an approach and conditions to be avoided when the airspeed was below 30 kt. If the rate of descent exceeded 700 ft/min (when the airspeed was below 30 kt), the pilot was expected to conduct a go-around.
Although this maximum rate of descent was consistent with the HeliOffshore figure, the correlation with low airspeed and lack of other criteria provided limited utility as the decision point for a go‑around. In MPT operations the ships were generally moving, and pilots were required to judge distance to the ship from visual cues. As such, 300 ft above the landing site could be used as the decision point for continuation of the approach or a go-around.
Given the helicopter was not on final approach and the pilots did not detect the exceedance of the operator’s descent rate/airspeed criteria, the absence of criteria recommended by HeliOffshore was not considered to a contributing factor in this occurrence. However, without such criteria it is more difficult for pilots to identify and avoid unsafe conditions or to respond appropriately.
This could be a factor in the deviations from normal procedures observed in ADS-B data when the instructor was flying at Port Hedland in January 2018, and the non-reporting of these to the operator.
In this occurrence, the deviations from normal practices were significant and it is unlikely that either pilot would have attempted to continue the approach if they had been aware of the abnormal flight path. Nevertheless, the provision of stabilised approach criteria would have conditioned pilot attention and response to critical parameters.
|
Other factor that increased risk The operator’s circuit and approach procedures for marine pilot transfer operations did not minimise pilot workload or provide the recommended stabilised approach criteria with mandatory go-around policy. These procedures could allow a combination of conditions that increased the risk of a sustained abnormal flight path and collision with terrain/water. (Safety issue) |
Fatigue and fatigue management
General background
As discussed in Task requirements, there were elements of the crew’s performance during the accident flight that related to their monitoring of flight parameters such as altitude, vertical speed and airspeed. The helicopter’s deviation from the intended flight path and target parameters was not identified or corrected by the pilots.
The accident occurred during the late evening and at a time when the pilot under supervision had been awake for an extended period, which followed-on from a long duty period involving both pilots the previous day. In that context, the investigation considered the potential effect of fatigue on the performance of the pilots.
Instructor fatigue level
Most people need at least 7 hours of sleep each day to achieve optimum levels of alertness and performance, and research has shown that restricting sleep to 6 hours or less a night over several nights will result in significant performance decrements (Banks and Dinges 2007, Watson and others 2015b).
Based on the available information, the instructor probably had a restricted sleep opportunity (5–6.5 hours) during the nights of 9, 10 and 12 March (and only 7.5 hours on 11 March), and may have achieved less sleep than the available opportunity. There was also an early start on 13 March then a long work day (at work from 0430 to 1917). Overall, at times during this period the instructor was probably experiencing a level of fatigue known to adversely influence performance.
On the night of 13 March, the instructor had a maximum sleep opportunity of 7.5 hours, reported 2 hours sleep during the day on 14 March, and felt rested prior to commencing work that afternoon. Although the workload involved in the MPT tasks at night would have been significant, the instructor had an opportunity for rest breaks between each of the tasks during the evening of 14 March. The time of day of the accident flight was not during the window of circadian low, though also was not during a time of day associated with maximum levels of alertness.
The ATSB analysis of the instructor’s sleep times was complicated by inconsistencies between the recorded sleep times in the instructor’s sleep log, and other information which indicated the instructor was awake when sleep had been recorded. Although the ATSB was able to construct a probable timeline for some of the instructor’s sleep opportunities, for other times (including the sleep on the night of 13 March), the analysis was more reliant on the sleep times recorded by the instructor.
Based on the available information, there was insufficient evidence to establish whether the instructor was affected by fatigue at the time of the accident, though it is likely they were experiencing a level of fatigue in previous days.
Pilot under supervision fatigue level
It was reported the pilot under supervision typically slept for 9 hours per night. Although there appeared to have been sufficient sleep opportunity for the period from 8 to 11 March, there was only 5.5 hours sleep opportunity on the night of 12 March. There was also an early start on 13 March then a long work day. Although the pilot under supervision had 9 hours sleep opportunity on the night of 13 March, no sleep was obtained during the next day. So, at the time of the accident, the pilot under supervision had probably slept for at most 6 hours in the previous 24 hours and 12.5 hours in the previous 48 hours, and had been awake for about 18 hours.
A significant amount of research has shown that a person’s performance starts to decline after 16–18 hours of extended wakefulness (Dawson and others 2021). According to the prior sleep wake rule (PSWR) threshold for extended wakefulness used by the operator, the pilot under supervision should not have conducted any work after 2100.
The quality of sleep will also influence the risk of fatigue and reduced alertness. A text message indicated the pilot under supervision did not sleep well on the night of 12 March. Although the pilot indicated sleeping well on the night of 13 March, they also indicated they did not get sufficient sleep. Sleep quality and quantity are also affected by stress and anxiety (Kim and Dimsdale, 2007), including the stress associated with completing exams (Zunhammer and others 2014). The pilot had reported being concerned about completing the night VFR flight planning assessment. Although there was not sufficient evidence to determine the degree to which the pilot was worried about this, and therefore its potential impact on their sleep, it possibly affected the quality and quantity of the actual sleep obtained on 12 and 13 March
Given the pilot under supervision’s restricted sleep in the previous 48 hours, and the significant time awake before the accident, combined with evidence the pilot was sometimes not sleeping well, the ATSB determined that the pilot under supervision was probably experiencing a level of fatigue known to adversely influence performance.
Although the pilot under supervision was probably experiencing fatigue, it was not possible to reliably determine the extent to which this fatigue contributed to the accident. As described in Inadvertent descent below 500 ft, the ATSB could not establish to a satisfactory standard of certainty which pilot was controlling the helicopter after the go-around. If the pilot under supervision was not flying, the effects of any fatigue-related impairment may not have significantly contributed to the occurrence, given the responsibilities then assumed by the instructor.
If the pilot under supervision was controlling the helicopter after the first circuit go-around, then the fatigue they probably experienced would have reduced their ability to cope with and respond to the conditions encountered during the accident flight. However, other factors, including the dark night conditions and the pilot under supervision’s low level of experience and recency in dark night MPT operations, and the associated workload, would also have affected the pilot under supervision’s ability to manage the go-around and subsequent circuit. Although fatigue increased the risk of the pilot making errors, the extent to which the errors could have occurred even without fatigue was difficult to determine.
|
Other factor that increased risk Due to a combination of limited sleep in the 48 hours prior to the accident and extended wakefulness on the day of the accident, the pilot under supervision probably experienced a level of fatigue known to adversely influence performance. |
Sleep log recording discrepancies
Although there was insufficient evidence to conclude whether fatigue contributed to this accident, the ATSB’s analysis did identify patterns of work and sleep associated with an increased risk of fatigue. These included the restricted sleep both pilots had on the night of 12 March, and the long day both pilots worked on 13 March.
It is acknowledged that these problems occurred during the context of training a new pilot rather than routine line operations. However, neither of the pilot’s sleep logs accurately reflected their sleep or work on these days. During the course of the investigation, other pilots raised concerns about the effectiveness of the operator’s fatigue risk management system (FRMS) and the validity of the sleep log approach based on the prior sleep wake model (PSWM). The ATSB therefore examined the effectiveness of the FRMS and, in particular the design and usage of the sleep log.
The operator’s FRMS required pilots ensure they had sufficient sleep prior to commencing a duty period, with sufficient sleep being defined in terms of the rules described by the PSWR. Pilots were required to record sleep and duty in a sleep log, which was designed to help pilots identify if they had achieved sufficient sleep by highlighting circumstances where a pilot would not meet the requirements of the PSWR. In essence, the sleep log provided the primary means of ensuring that pilots were sufficiently rested prior to conducting an MPT task.
It is understandable that knowing how much sleep a pilot had in the previous 24 and 48 hours can play a very useful role in determining their fatigue level and fitness for duty. This information can be particularly relevant for rosters involving night shifts and with no pre-defined hours of duty but with some duty likely to be required each allocated shift. It is relatively simple information to record and tailored to each individual’s circumstances.
There are some general caveats to consider when using prior sleep wake information within an FRMS (see also Appendix E). For example, individuals have different sleep needs, and sleep patterns prior to the last 48 hours can influence a person’s level of fatigue. As well as the quantity of sleep and hours awake, a range of other factors can also influence fatigue and alertness, such as the quality of sleep, time of day, type of work and frequency of rest breaks, all of which need to be monitored and/or managed.
In addition, there were significant problems associated with the implementation of the PSWR by the operator. These included:
- The PSWR values used by the operator were the standard thresholds proposed by Dawson and McCullough (2005). These authors also stated that different thresholds would be appropriate depending on the risk profile of the tasks being performed or their susceptibility to fatigue-related error. However, the operator’s FRMS did not discuss the risk profile of single pilot night VFR MPT operations. It would be reasonable to expect that such operations have a higher risk profile than many other types of work tasks.
- The operator’s guidance for using the sleep logs encouraged pilots to record any sleep. Given that sleep and duty was only recorded in 1-hour blocks, this effectively resulted in pilots rounding sleep up and over-estimating the amount of sleep they had obtained.
- According to the FRMS manual, any exceedance of the PSWR (as recorded in a pilot’s sleep log) meant that a pilot could not undertake any duty. Depending on a range of factors, there can be some cases where small exceedances of PSWR thresholds may have minimal effect, and could be managed with the use of appropriate mitigators.
- There was no explicit means of recording sleep quality, or at least noting problematic sleep quality, in the sleep log.
- The operator also (and reasonably) encouraged pilots to sleep before and between MPT tasks when on shift. However, there was no discussion in the FRMS manual.[77]
More importantly, the major limitation of applying the PSWR as the primary means of determining a pilot’s fitness for work is that it relies upon accurate sleep information. Inaccurate recording of sleep would fundamentally devalue the potential of the approach to manage fatigue, and when pilots are recording the sleep information there are a range of potential factors that can affect how this information is recorded.
In this case, the instructor (and to some extent the pilot under supervision) over-reported their hours of sleep and under-reported their hours of duty in the days before the accident. The ATSB also observed multiple other pilots misreporting hours of sleep and duty on multiple occasions. This primarily included many instances of pilots recording long sleep periods of 12 hours or more, which research would suggest should be rare, even when workers have significant breaks between shifts (for example, Roach and others 2003). In addition, there were many cases where pilots recorded sleep when other information indicated they were awake. The effect of the misreporting was that the sleep logs did not show the increased fatigue risk associated with problematic hours of work and sleep.
The operator’s FRMS stated that pilots were to report if they felt fatigued and unable to fly, or if their recorded sleep and duty within the sleep log did not meet the requirements of the PSWR. The FRMS also stated that such reporting would be ‘totally supported’ by management. Evidence from some of the operator’s pilots, however, indicated that they perceived implicit and explicit pressure to ensure that they recorded sleep and duty that did not exceed the PSWR thresholds. Pilots reported feeling pressured to ‘make the roster work’, by recording incorrect information.
The simplicity of the PSWR rule set and the design of the sleep log meant it was obvious to pilots what they needed to do to clear fatigue alerts, and when they had reported enough sleep to enable them to conduct a task. Pilots could simply adjust the sleep log values until fatigue alerts disappeared, and pilots reported doing exactly that. In this way, the nature of the sleep logs facilitated any pilot who was motivated to record a pattern of sleep that allowed them to complete the duty allocated to them.
These experiences and perceptions of the operator’s pilots are consistent with the results of an ATSB survey on the fatigue experiences of Australian commercial pilots.[78] This survey showed that most pilots never removed themselves from duty due to fatigue, and that most pilots who did remove themselves from duty perceived this left a negative impression with management. The results also showed that almost half of the pilots surveyed said they were either ‘not comfortable’ reporting as unfit for duty due to fatigue or were only ‘rarely’ comfortable to make this assessment.
It is apparent that problems with inaccurate sleep recording had been occurring for some time prior to the accident. Although the FRMS required the chief pilot to review sleep records, there was no evidence available to show that this had occurred, nor any other oversight activity undertaken to determine the accuracy of the sleep and wake data recorded in the sleep logs. Had the operator compared recorded sleep times with flight records, or queried any sleeps longer than 12 hours, this may have provided an opportunity to identify inaccurate sleep recording and address fundamental issues associated with the operator’s application of the PSWR within its FRMS.
The use of the operator’s FRMS as an alternative method to comply with the flight and duty time limitations prescribed in CAO 48.1 was based on a CASA-issued exemption under subsection 4 of CAO 48.0. The operator’s FRMS did not include the use of a biomathematical model of fatigue (BMMF), which is often used as a key component in many FRMSs that do not include restrictive flight and duty time limits. Instead, the FRMS primarily relied on pilots using the PSWR and recording sleep information to determine their own fitness for duty.
As evidenced by this investigation, an FRMS that fundamentally relies on the PSWM has challenges than need to be carefully managed. Such an approach also fundamentally relies on the fidelity of sleep information. Unless the FRMS can facilitate accurate recording of sleep information, and actively assure that the information is accurate, then additional means of managing fatigue risk will also be required.
|
Other factor that increased risk The operator's fatigue risk management system relied extensively on a sleep reporting spreadsheet (sleep log) that was based on the prior sleep wake model, and the spreadsheet had a transparent rule set that made the recorded data easy to modify to achieve results that met the operator’s minimum sleep and wake requirements. In the context of perceived pressure to present as fit for duty, multiple pilots on multiple occasions had entered unrealistic or inaccurate sleep times and there were limited effective controls in place to assure that the sleep times being entered by pilots was accurate. (Safety issue) |
Sleep log coding error
The sleep log spreadsheet contained a coding error for the PSWR ‘extended wakefulness’ rule. In effect, it double counted the sleep in the period 25–48 hours prior to the specific time, and therefore increased the allowed period of extended wakefulness for several hours in most situations. The consequence of this error was that the sleep log would not highlight circumstances where a pilot was awake for greater than their sleep in the previous 48 hours.
The spreadsheets also pre-loaded the hours of 2200 to 0600 as sleep for all days. A pilot anticipating a night shift would need to clear the pre-loaded sleeps from that night to identify the times in which they would not have sufficient rest.
The ATSB considered the influence of the sleep log coding error and pre-loaded sleep on the fatigue experienced by the pilot under supervision. A correctly coded spreadsheet may have provided the pilot under supervision with an additional prompt that they would not have sufficient rest when operating late on the night of the accident, which may have further encouraged them to attempt to sleep prior to the accident flight. However, messages sent to the pilot’s partner indicate that, even without this prompt, the pilot wanted to have a nap on the day of the accident, but was unsuccessful in their attempt to rest.
|
Other factor that increased risk The sleep log tool used by the operator contained a coding error and it also pre-loaded sleep periods of future nights by default. This combination of factors reduced the likelihood pilots would identify fatigue risks associated with insufficient sleep and extended wakefulness. (Safety issue) |
Port Hedland pilot roster change management
The operator’s FRMS had not been updated since 2014, prior to the start of undertaking MPT contract work at Port Hedland in April 2017. Consequently, the rosters described in the FRMS manual were not directly applicable to the work conducted in Port Hedland. That is, they did not include a roster pattern involving a day shift (0600–1800) followed by a night shift (1800–0600), with the potential for additional day or night shifts as required. Because the FRMS did not describe the rosters worked by Port Hedland pilots, this limited the ability of the operator to identify and manage the attendant fatigue-related risks.
In addition, as already discussed, the night shifts at Port Hedland involved single pilot operations under the night VFR. This risk profile for single pilot night operations was not discussed in the FRMS manual. The only night operations with assessments were those involving 2-pilot crews under IFR.
The timing of the Port Hedland night shifts meant that, towards the end of the shift, pilots would be operating in the window of circadian low, or the time of day associated with the lowest level of alertness. In addition, if pilots conducted 2 night shifts in a row, they would potentially be sleeping during the day between the shifts, which was likely to result in restricted sleep quantity and quality.
Analysis of the hours worked by Port Hedland line pilots indicated that, in most cases, they were not associated with significant risks due to the nature of the MPT schedule. Nevertheless, there were risks that needed to be carefully assessed and managed, with relevant controls outlined in the FRMS manual.
A new operational environment with a different roster pattern would generally meet the criteria for a significant change that required risk management. However, there was no evidence of the operator having used a biomathematical model or other means for assessing the roster, or during ongoing oversight of the suitability of that roster. The absence of a formal consideration of the fatigue implications the Port Hedland contract work significantly impaired the ability of the operator to identify and mitigate any attendant risks.
|
Other factor that increased risk The operator's fatigue risk management system did not describe the roster pattern or night shifts worked by line pilots based at Port Hedland, and the operator did not conduct a formal risk assessment of the roster prior to commencing marine pilot transfer operations at Port Hedland. |
Installation of emergency location transmitters
During the investigation the ATSB noted that the ELT was mounted to the PELICAN rack in the rear of the cabin. The helicopter manufacturer did not mount the ELT in that position and did not consider the PELICAN rack to be structural or load carrying. As such, the installation was inconsistent with the Radio Technical Commission for Aeronautics (RTCA) guidelines.
The ELT was installed as part of the emergency medical service modifications before the helicopter was imported into Australia. The ATSB did not locate any documentation to show that the PELICAN rack had been assessed and approved as a suitable location for installation of crash activated equipment such as an ELT.
An ELT is designed to automatically activate when the unit is subjected to forces in excess of threshold values. If the ELT is not mounted to primary structure, impact forces can be attenuated by mechanisms such as distortion or separation of the secondary structure.
In this occurrence, the vertical impact forces were almost certainly within the range for automatic activation of the emergency locator transmitter (ELT) but the Cospas-Sarsat satellites did not receive any transmissions from the helicopter. However, if the ELT had activated, the transmissions would have been attenuated by the rapid inversion of the helicopter and submersion of the antenna so non receipt of transmissions was not necessarily indicative of ELT non-activation. Due to water ingress damage to the ELT, the ATSB was unable to measure battery voltage as an indicator of ELT operation.
Given the ATSB was unable to establish if the ELT activated, the ATSB was also unable to determine if the mounting of the ELT on non-primary structure had a negative effect on ELT activation. Nevertheless, the ATSB is concerned about the potential for incorrectly mounted ELTs to not activate during accidents with associated delays to search and rescue.
Consequently, the ATSB advises operators of aircraft with a non-standard ELT installations to verify conformance with RTCA guidelines to ensure the maximum probability of automatic activation in an accident.
|
Other factor that increased risk The ELT was mounted to the PELICAN rack in the rear of the EC135 cabin rather than to primary load carrying structure, which increased the risk of non-activation during an accident. |
Regulatory oversight
Previous ATSB reports have noted that regulatory oversight processes will always have constraints in their ability to detect problems such as restricted time and limited resources. Due to resource constraints, regulatory surveillance by CASA is by necessity sample‑based and cannot examine every aspect of an operator’s activities, nor identify all the limitations associated with these activities.
Nevertheless, in 3 investigation reports released in the last 4 years, the ATSB noted that CASA’s processes for scoping surveillance events did not formally include the nature of the operator’s activities, the inherent threats or hazards associated with those activities, and the risk controls that were important for managing those threats or hazards.
In the 3 years prior to this occurrence involving VH-ZGA in March 2018, CASA recorded 3 surveillance events related to the operator without identifying any significant operational safety concerns. As the surveillance event in 2017 was a desktop assessment of a limited range of airworthiness documentation, MPT operations were out of scope.
The defined scope of the ‘Level 1 Health Check’ carried out 3 weeks before the occurrence included operational standards and authorised activities, but there is no indication that the auditors considered the efficacy of risk controls for MPT operations. This was similarly the case for the ‘Level 1 Systems Audit’ in 2016.
The ATSB noted that the CASA auditors in 2016 had observed there was no management process to support the chief pilot’s working practices. There was no requirement for the operator to address this observation and no indication that the operator responded. In any event, CASA auditors in February 2018 noted that the chief pilot and head of operations demonstrated adequate control of the flying operations.
Post-occurrence, CASA checked that MPT operators were complying with their own requirements for HUET recency and assessed the operator’s arrangements for crew scheduling and fatigue management at Port Hedland. No safety concerns were identified. The regulatory and safety review carried out by CASA in response to the occurrence did not identify any requirements for immediate action or significant learnings.
In addition to time and resource constraints that inhibit scope and sampling, auditing is generally carried out with reference to criteria such as regulatory material and operator manuals. As there were no specific regulations for twin-engine MPT operations, the operator’s manuals were the primary references for any audit of the MPT operation. An assessment of the suitability of the operator’s procedures could be referenced to best practice guidelines.
The German Federal Bureau of Aircraft Accident Investigation (BFU) investigated a BK117 helicopter accident that occurred during circling for an approach to a vessel on a dark night. The BFU found that in the context of no regulations for offshore helicopter flight operations in Germany, the operator’s procedures and assessment by the supervising authority were insufficient.
BFU safety recommendation 24/2015 stated that the German Civil Aviation Authority should ensure that operators conducting night VFR approaches to sparsely lit landing sites should specify practical and detailed procedures in their handbooks that are appropriate to the special demands of this type of operation, and which specify systematic, consistent and comprehensive use of the resources available to the conduct of the flight.
In relation to this occurrence, the operator’s process for line training was not under CAR 217 or CASR Part 141/142 and there was limited criteria for CASA assessments of that process. However, with the introduction of new regulations applicable to MPT operations, the operator will be required to provide a training and checking system with defined standards.
Another element of regulatory oversight was application of the authorisation holder performance indicator (AHPI) questionnaire. Although the operator responded that ship landings were one of its highest risks and they operated in challenging environments, this had no apparent effect on surveillance priorities or risk assessment.
|
Given that the underlying problem associated with the scoping of surveillance events was extensively discussed in recent ATSB investigations (AO-2017-005 and AO-2018-026), further discussion was not considered necessary in this report. As part of the earlier investigation, the ATSB issued a safety recommendation (AO-2017-005-SR-026) to CASA in October 2019, and this recommendation was closed in March 2020 after CASA outlined the safety actions it had taken and was taking to address the issue. In addition, the Australian National Audit Office (ANAO) commenced an audit in April 2021 into planning and conduct of CASA’s surveillance activities. Other factor that increased risk Although the operator’s primary helicopter activity was conducting marine pilot transfers, regulatory oversight activity by the Civil Aviation Safety Authority had not specifically examined the operator’s procedures and practices for conducting approaches and landings to ships at night in degraded visual cueing environments. |
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision with water involving EC135 P2+ helicopter, VH-ZGA, 37 km north-north-west of Port Hedland, Western Australia, on 14 March 2018.
Contributing factors
- During the positioning flight for the third supervised marine pilot transfer at night, circling in the vicinity of outbound bulk carrier Squireship was conducted in a degraded visual cueing environment, with associated increases in pilot workload and risk of disorientation.
- Following a circuit, missed approach, and climb to 1,100 ft, a descent was initiated without coupling a vertical navigation mode of the autopilot. This was not consistent with standard operational practices and significantly increased the attentional demands on both pilots and associated risk of deviation from circuit procedure.
- During the downwind and base segment of the circuit, the pilots did not effectively monitor their flight instruments and the helicopter descended below the standard circuit profile at excessive rate with decaying airspeed. Neither pilot responded to the significantly abnormal flight path or parameters until the radio altimeter alert at 300 ft.
- The instructor responded to the radio altimeter alert, reducing the rate of descent from about 1,800 ft/min to 1,300 ft/min, but this response was not consistent with an emergency go-around and did not optimise recovery before collision with water.
- After the unexpected and significant water impact in dark conditions, the helicopter immediately rolled over and the cabin submerged then flooded. The instructor escaped through an adjacent hole in the windscreen and used flotation devices until rescued but the pilot under supervision was unable to escape the cockpit and did not survive.
- The instrument panels fitted to VH-ZGA and the operator's other EC135 helicopter at Port Hedland were equipped for single-pilot operation under the instrument flight rules. When used for flight training or checking in a degraded visual cueing environment, this configuration has a detrimental effect on the ability of an instructor or training/check pilot to monitor the helicopter's flight path and take over control if required. (Safety issue)
- When operating at Port Hedland in degraded visual cueing environments, the instructor had not been able to ensure that circling approaches were consistent with the operator's standard operating procedures. This probably limited the support provided to the pilot under supervision on the occurrence flight and, in combination with other factors, probably contributed to the abnormal flight path and partial recovery.
- The pilot under supervision was introduced to line flying at night in a degraded visual cueing environment immediately after completion of the minimum-required 10 ship landings by day and without any preparatory night flying. Given the pilot under supervision was transitioning from a different helicopter type and operational environment, the lack of consolidation contributed to high cognitive workload for both pilots and increased the risk of sustained flight path deviations.
Other factors that increased risk
- The operator rostered the pilot under supervision for marine pilot transfer flying without ensuring that helicopter underwater escape training (HUET) had been completed in accordance with the operations manual. Although the pilot under supervision had completed HUET in 2009 and 2011, the lack of recency reduced preparedness for escaping the helicopter following submersion.
- Although the instructor was flying when significant deviations from standard operating procedures occurred during night approaches in January 2018, these were not reported to the operator or otherwise addressed by the instructor.
- The operator's training and assessing procedures for marine pilot transfer operations did not provide assurance that pilot under supervision experience, helicopter instrumentation, and instructor capability were suitable for line training at night in a degraded visual cueing environment. (Safety issue)
- The operator’s circuit and approach procedures for marine pilot transfer operations did not minimise pilot workload or provide the recommended stabilised approach criteria with mandatory go-around policy. These procedures could allow a combination of conditions that increased the risk of a sustained abnormal flight path and collision with terrain/water. (Safety issue)
- Due to a combination of limited sleep in the 48 hours prior to the accident and extended wakefulness on the day of the accident, the pilot under supervision probably experienced a level of fatigue known to adversely influence performance.
- The operator's fatigue risk management system relied extensively on a sleep reporting spreadsheet (sleep log) that was based on the prior sleep wake model, and the spreadsheet had a transparent rule set that made the recorded data easy to modify to achieve results that met the operator’s minimum sleep and wake requirements. In the context of perceived pressure to present as fit for duty, multiple pilots on multiple occasions had entered unrealistic or inaccurate sleep times and there were limited effective controls in place to assure that the sleep times being entered by pilots was accurate. (Safety issue)
- The sleep log tool used by the operator contained a coding error and it also pre-loaded sleep periods of future nights by default. This combination of factors reduced the likelihood pilots would identify fatigue risks associated with insufficient sleep and extended wakefulness. (Safety issue)
- The operator's fatigue risk management system did not describe the roster pattern or night shifts worked by line pilots based at Port Hedland, and the operator did not conduct a formal risk assessment of the roster prior to commencing marine pilot transfer operations at Port Hedland.
- The ELT was mounted to the PELICAN rack in the rear of the EC135 cabin rather than to primary load carrying structure, which increased the risk of non-activation during an accident.
- Although the operator’s primary helicopter activity was conducting marine pilot transfers, regulatory oversight activity by the Civil Aviation Safety Authority had not specifically examined the operator’s procedures and practices for conducting approaches and landings to ships at night in degraded visual cueing environments.
Other findings
- There was insufficient evidence to establish whether the instructor was affected by fatigue at the time of the accident, though it is likely they were experiencing a level of fatigue in previous days.
- There was no evidence of any helicopter defects or anomalies.
- When the helicopter was recovered, the right audio controller was found in the pilot isolate configuration and it was not possible to establish if this occurred before, during, or after the impact sequence. If pre-impact, this would have prevented effective communication between the pilots and potentially influenced the occurrence.
|
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Configuration of instrument panel for instructor or training/check pilot in degraded visual cueing environments
Safety issue number: AO-2018-022-SI-03
Safety issue description: The instrument panels fitted to VH-ZGA and the operator's other EC135 helicopter at Port Hedland were equipped for single-pilot operation under the instrument flight rules. When used for flight training or checking in a degraded visual cueing environment, this configuration has a detrimental effect on the ability of an instructor or training/check pilot to monitor the helicopter's flight path and take over control if required.
Operator’s training and assessing procedures for marine pilot transfer operations in degraded visual cueing environments
Safety issue number: AO-2018-022-SI-005
Safety issue description: The operator's training and assessing procedures for marine pilot transfer operations did not provide assurance that pilot under supervision experience, helicopter instrumentation, and instructor capability were suitable for line training at night in a degraded visual cueing environment.
Operator’s circuit and approach procedures for marine pilot transfer operations and criteria for achieving a stabilised approach
Safety issue number: AO-2018-022-SI-04
Safety issue description: The operator’s circuit and approach procedures for marine pilot transfer operations did not minimise pilot workload or provide the recommended stabilised approach criteria with mandatory go-around policy. These procedures could allow a combination of conditions that increased the risk of a sustained abnormal flight path and collision with terrain/water.
Use of sleep reporting spreadsheet and potential for modification of data input to meet operator’s minimum requirements
Safety issue number: AO-2018-022-SI-02
Safety issue description: The operator's fatigue risk management system relied extensively on a sleep reporting spreadsheet (sleep log) that was based on the prior sleep wake model, and the spreadsheet had a transparent rule set that made the recorded data easy to modify to achieve results that met the operator’s minimum sleep and wake requirements. In the context of perceived pressure to present as fit for duty, multiple pilots on multiple occasions had entered unrealistic or inaccurate sleep times and there were limited effective controls in place to assure that the sleep times being entered by pilots was accurate.
Risk controls associated with pilots identifying fatigue risks associated with insufficient sleep and extended wakefulness
Safety issue description: AO-2018-022-SI-01
Safety issue description: The sleep log tool used by the operator contained a coding error and it also pre-loaded sleep periods of future nights by default. This combination of factors reduced the likelihood pilots would identify fatigue risks associated with insufficient sleep and extended wakefulness.
Additional safety action
Additional safety action by Heli-Aust Whitsundays Pty Limited
The operator advised the ATSB of the following additional safety actions taken following the accident:
- The operator has equipped all personal flotation devices (life jackets) used by pilots with an emergency breathing system (EBS).
- The operator relocated the emergency locator transmitter installed in VH-ZGZ from the PELICAN rack to primary load carrying structure (cockpit floor, adjacent the pilot seat).
- Newly recruited pilots are required to complete training in helicopter underwater escape (HUET) and use of EBS prior to commencing flight training/operations.
- All pilots are required to complete recurrent HUET and proficiency using EBS every 2 years, with an extension of up to 6 months in accordance with the operations manual.
- With the support of its customer, the operator has introduced night vision imaging systems (NVIS) to the Port Hedland marine pilot transfer operation.
- With the support of their customer, the operator has supplied the Port Hedland base with 2 Airbus Helicopters H135 equipped with the Helionix avionics suite. This includes terrain avoidance capabilities and a 4-axis autopilot.
Additional safety action by the Civil Aviation Safety Authority
The Civil Aviation Safety Authority advised the ATSB of the following additional safety actions taken following the accident:
- CASA conducted a national desktop audit of helicopter underwater escape training (HUET) for AOC holders conducting MPT operations.
- In September 2018, CASA carried out a Level-2 operational check of the operator with a site inspection at Port Hedland in response to concerns raised by pilots about crew scheduling and fatigue management. The surveillance report concluded that the operator’s ‘crew scheduling and safety management procedures were found to be suitable and effective in managing fatigue’.
Previously issued safety advisory notice
Safety advisory notice to all helicopter operators engaged in overwater operations
In May 2018, concurrent with the publication of the preliminary report, the ATSB issued the following safety advisory notice to all overwater helicopter operators.
|
SAN number: |
|
|
SAN release date: |
3 May 2018 |
The Australian Transport Safety Bureau advises helicopter operators involved in overwater operations of the importance of undertaking regular HUET for all crew and regular passengers to increase their survivability in the event of an in-water accident or ditching.
|
°C |
Degrees Celsius |
|
2D |
Two-dimensional instrument approach procedure |
|
AAIB |
Air Accidents Investigation Branch (UK) |
|
ADS-B |
Automatic dependent surveillance broadcast |
|
AFCS |
Automatic flight control system |
|
AFM |
Aircraft flight manual |
|
AGL |
Above ground level |
|
AHPI |
Authorisation holder performance indicator |
|
AIS |
Automated identification system (marine shipping) |
|
ALA(s) |
Aeroplane landing area(s) |
|
ALT |
Altitude |
|
ALT.A |
Altitude acquire |
|
ALAR |
Approach and landing accident reduction |
|
AMSA |
Australian Maritime Safety Authority |
|
AMSL |
Above mean sea level |
|
ANAO |
Australian National Audit Office |
|
AOC |
Air operator’s certificate |
|
APM |
Autopilot module |
|
APMS |
Autopilot mode selector |
|
ASI |
Airspeed indicator |
|
ATC |
Air traffic control |
|
A.TRIM |
Automatic trim |
|
ATSB |
Australian Transport Safety Bureau |
|
AVAD |
Automated voice alerting device |
|
AWB |
Airworthiness bulletin |
|
BARS |
Basic aviation risk standard |
|
BEA |
Bureau d’Enquêtes et d’Analyses (France) |
|
BFU |
Bundesstelle für Flugunfalluntersuchung (Germany) |
|
BoM |
Bureau of Meteorology |
|
BMMF |
Biomathematical model of fatigue |
|
C1 |
Charlie 1, marine navigation beacon |
|
C2 |
Charlie 2, marine navigation beacon |
|
CAAP |
Civil aviation advisory publication |
|
CAD |
Cautions and advisories display |
|
CAO |
Civil Aviation Order |
|
CASA |
Civil Aviation Safety Authority |
|
CAR |
Civil Aviation Regulation |
|
CASR |
Civil Aviation Safety Regulation |
|
CEO |
Chief executive officer |
|
CFIT |
Controlled flight into terrain |
|
Cospas-Sarsat |
Space system for the search of vessels in distress - Search and rescue satellite-aided tracking |
|
CPDS |
Central panel display system |
|
CVR |
Cockpit voice recorder |
|
DAR |
Digital aircraft recorder |
|
DCU |
Data collection unit |
|
DVE |
Degraded visual (cueing) environment |
|
EBS |
Emergency breathing system |
|
EEC |
Electronic engine control |
|
EFIS |
Electronic flight information system |
|
EGPWS |
Enhanced ground proximity warning system |
|
ELT |
Emergency locator transmitter |
|
EPC |
(Flight) examiner proficiency check |
|
EPIRB |
Emergency position indicating radio beacon |
|
FAA |
Federal Aviation Authority (US) |
|
FADEC |
Full authority digital engine control |
|
FAID |
Fatigue audit InterDyne |
|
FATO |
Final approach and take-off area |
|
FCOM |
Flight crew operations manual |
|
FDR |
Flight data recorder |
|
FLI |
First limit indicator |
|
FP |
Flying pilot |
|
FPM |
Flightpath management (HeliOffshore publication) |
|
FRMS |
Fatigue risk management system |
|
FSAG |
Fatigue safety advisory group |
|
FSTD |
Flight simulation training device |
|
FTL |
Fatigue tolerance level |
|
FTR |
Force trim release |
|
ft |
Feet |
|
ft/min |
Feet per minute |
|
FO |
First officer |
|
GA |
Go-around |
|
GA |
Geoscience Australia |
|
GAMA |
General aviation manufacturers association |
|
GPS |
Global positioning system |
|
GPWT |
Grid point wind and temperature |
|
HDG |
Heading |
|
HEEL |
Helicopter emergency egress lights |
|
HF/NTS |
Human factors/non-technical skills |
|
HOO |
Head of operations |
|
HTAWS |
Helicopter terrain awareness and warning system |
|
HUET |
Helicopter underwater escape training |
|
IAS |
Indicated airspeed |
|
ICAO |
International Civil Aviation Organization |
|
ICUS |
In command under supervision |
|
IF |
Instrument flight |
|
IFR |
Instrument flight rules |
|
IMC |
Instrument meteorological conditions |
|
IPC |
Instrument proficiency check |
|
JAR |
Joint Aviation Requirements |
|
JRCC |
Joint Rescue Coordination Centre (Australia) |
|
KIAS |
Knots indicated airspeed |
|
kt |
Knot |
|
LBA |
Luftfahrt-Bundesamt (Germany) |
|
LSALT |
Lowest safe altitude |
|
MDA |
Minimum descent altitude |
|
m |
Metres |
|
mm |
Millimetres |
|
MMI |
Mast moment indicator |
|
MOS |
Manual of Standards |
|
MPT |
Marine pilot transfer |
|
MSA |
Minimum safe altitude |
|
ND |
Navigation display |
|
NFP |
Non-flying pilot |
|
NM |
Nautical mile |
|
NTS |
Non-technical skills |
|
NTSB |
National Transportation Safety Board (United States of America) |
|
NVFR |
Night visual flight rules |
|
NVG |
Night vision goggle |
|
NVIS |
Night vision imaging system |
|
PBG |
Pilot boarding ground (marine) |
|
PELICAN |
Packing equipment line for integrated concept of avionic nouvelle (new avionics) |
|
PF |
Pilot flying |
|
PFD |
Primary flight display |
|
PIC |
Pilot in command |
|
PICUS |
Pilot in command, under supervision |
|
PLB |
Personal locator beacon |
|
PSWM |
Prior sleep wake model |
|
PSWR |
Prior sleep wake rule |
|
RADALT |
Radio altimeter |
|
ROD |
Rate of descent |
|
RPM |
Revolutions per minute |
|
RTCA |
Radio Technical Commission for Aeronautics |
|
S&P |
Standardisation and proficiency |
|
SAN |
Safety advisory notice |
|
SAS |
Stability augmentation system |
|
SMS |
Safety management system |
|
SOP(s) |
Standard operating procedure(s) |
|
STC |
Supplemental type certificate |
|
TEM |
Threat and error management |
|
TSB |
Transport Safety Board (Canada) |
|
US |
United States (of America) |
|
UTC |
Universal coordinated time |
|
V/S |
Vertical speed |
|
VEMD |
Vehicle and engine multifunction display |
|
VFR |
Visual flight rules |
|
VMC |
Visual meteorological conditions |
|
VSI |
Vertical speed indicator |
|
VTOSS |
Take-off safety speed |
|
VY |
Best rate of climb speed |
|
WST |
Western standard time |
|
WU |
Warning unit |
Sources of information
The sources of information during the investigation included the:
- instructor pilot of the accident flight
- pilot under supervision’s next of kin and pilot under supervision’s partner
- helicopter operator (Heli-Aust Whitsundays Pty Limited), including management personnel, safety personnel and flight crew
- Bundesstelle für Flugunfalluntersuchung (BFU), the German Federal Bureau of Aircraft Accident Investigation
- helicopter manufacturer (Airbus Helicopters Deutschland GmbH)
- Transportation Safety Board of Canada (TSB)
- engine manufacturer (Pratt & Whitney Canada)
- Bureau d’Enquêtes et d’Analyses (BEA)
- Civil Aviation Safety Authority (CASA) and personnel who worked for CASA during the period prior to the accident
- Airservices Australia
- Australian Maritime Safety Authority (AMSA)
- flight examiners and flight instructors who had flown with the flight crew of the helicopter
- Pilbara Ports Authority (PPA) and their contractors
- marine pilots who flown with the helicopter crew and/or witnessed the accident
- Bureau of Meteorology (BoM)
- Western Australia Police Force
References
Dawson D and McCulloch K (2005) ‘Managing fatigue: it's about sleep’, Sleep Medicine Reviews, 9:365–80.
Dorrian J, Sweeney M and Dawson D (2011) ‘Modeling fatigue-related truck accidents: Prior sleep duration, recency and continuity’, Sleep and Biological Rhythms, 9:3–11.
Hoh R (1990) The effects of degraded visual cueing and divided attention on obstruction avoidance in rotorcraft, Technical report DOT/FAA/RD-90/40, Federal Aviation Administration.
Kim EJ and Dimsdale JE (2007) ‘The effect of psychosocial stress on sleep: a review of polysomnographic evidence’, Behavioral Sleep Medicine, 5:256–78.
National Transportation Safety Board 2011, Airbag performance in general aviation restraint systems, Safety Study NTSB/SS-11/01.
Rupert A, McGrath B, Mortimer B and Brill JC (2020) Multisensory cueing to resolve helicopter drift detection in DVE. Paper presented at the Vertical Flight Society’s 76th Annual Forum and Technology Display.
Sprajcer M, Thomas MJH, Sargent C, Crowther MW, Boivin DB, Wong IS, Smiley A and Dawson D (2022) ‘How effective are fatigue risk management systems (FRMS)?’, Accident Analysis and Prevention, 165:106398.
Thomas MJW and Ferguson SA (2010) ‘Prior sleep, prior wake, and crew performance during normal flight operations’, Aviation, Space, and Environmental Medicine, 81:665–670.
Van Dongen H, Maislin G, Mullington JM and Dinges DF (2003) ‘The cumulative cost of additional wakefulness: dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation, Sleep, 26:117–126.
Wang Y, White M, Owen I, Hodge S, and Barakos G (2013) ‘Effects of visual and motion cues in flight simulation of ship-borne helicopter operations’, CEAS Aeronautical Journal, 4:385–396.
Watson NF, Badr MS, Belenky G, Bliwise DL, Buxton OM, Buysse D, Dinges DF, Gangwisch J, Grandner MA, Kushida C, Malhotra RK, Martin JL, Patel SR, Quan SF and Tasali E (2015a) ‘Recommended amount of sleep for a healthy adult: A joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society’, Sleep, 38:843-844.
Watson NF, Badr MS, Belenky G, Bliwise DL, Buxton OM, Buysse D, Dinges DF, Gangwisch J, Grandner MA, Kushida C, Malhotra RK, Martin JL, Patel SR, Quan SF and Tasali E (2015b), ‘Joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society on the recommended amount of sleep for a healthy adult: methodology and discussion’, Journal of Clinical Sleep Medicine, 11:931-952.
Williamson A, Lombardi D A, Folkard S, Stutts J, Courtney TK and Connor J L (2011) ‘The link between fatigue and safety’, Accident Analysis and Prevention, 43:498–515.
Yeh M, Swider C, Yong JJ and Donovan C (2016) Human factors considerations in the design and evaluation of flight deck displays and controls, Technical report DOT/FAA/TC-16/56, Federal Aviation Administration.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- instructor pilot of the accident flight
- helicopter operator (Heli-Aust Whitsundays Pty Limited)
- chief pilot of the helicopter operator at the time of the accident
- Civil Aviation Safety Authority (CASA)
- Airservices Australia (ASA)
- Australian Maritime Safety Authority (AMSA)
- Bundesstelle für Flugunfalluntersuchung (BFU), the German Federal Bureau of Aircraft Accident Investigation and their advisers (including the helicopter manufacturer, Airbus Helicopters Deutschland GmbH)
- Transportation Safety Board of Canada (TSB) and their advisers (including the engine manufacturer Pratt & Whitney Canada)
- United States’ National Transportation Safety Board (NTSB).
Submissions were received from:
- CASA
- BFU
- TSB
- the instructor pilot
- the helicopter operator, incorporating comments also from the chief pilot at the time of the accident
- the family of the pilot under supervision (as a party with an involvement).
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendix A - 14 March 2018, flights preceding the accident flight
First night flight
The first night flight was to embark a marine pilot to the inbound bulk carrier Anangel Explorer at the pilot boarding ground. The helicopter departed the heliport at about 1859. This was about 15 minutes after last light and the sun’s illumination of the nautical horizon was decreasing.
The flight was conducted under night visual flight rules (night VFR) procedures and helicopter was flown to the pilot boarding ground at about 1,600 ft. This was consistent with procedures for night operations, flying en route at or above the lowest safe altitude[79] (LSALT).
The crew of VH-ZGA initiated descent from cruise altitude when the helicopter was about 2 NM (3.7 km) south of the bulk carrier. The rate of change of geometric altitude broadcast by the helicopter’s ADS‑B equipment indicated an initial descent rate of about 400 ft/min at an estimated airspeed [80] of about 85 kt. After about 30 seconds, the descent rate progressively increased, accompanied by a slight reduction in the airspeed. The descent rate continued to increase and exceeded 1,000 ft/min when the helicopter was about 1 NM (1.9 km) south of the bulk carrier, descending through 1,250 ft at an airspeed of about 80 kt.
Figure 21 depicts the flight path flown in vicinity of the bulk carrier. ADS-B and derived data at the alphabetically labelled points ‘A’ to ‘F’ is depicted in Table 13. Figure 22 graphically depicts the ADS‑B and derived data during the approach.
Figure 21: ADS-B data for VH-ZGA, during a night approach to Anangel Explorer at the pilot boarding ground, during the early evening of 14 March 2018

Representation of recorded track data during the first night flight, to transfer a marine pilot to Anangel Explorer at the pilot boarding ground. This flight was conducted at night, under night VFR procedures. The white track is positions of VH-ZGA recorded by the ASA ADS-B receivers, the yellow track is positions recorded on the FlightRadar24 internet server. The annotated labels A to F correspond to the ADS-B helicopter position relative to the bulk carrier’s landing hatch, as derived from shipping data recorded by the Australian Maritime Safety Authority. Data relevant to the annotated labels for VH-ZGA is presented in Table 13 and marked as labelled index points in Figure 22. The bulk carrier was 289 m in length.
Source: ATSB
Table 13: ADS-B and derived data, associated with the flight path of VH-ZGA depicted in Figure 21
|
Position |
Time (WST) |
Estimated range to landing hatch (m) |
Derived airspeed (kt)[1] |
Groundspeed (kt) |
Altitude (ft)[2] |
Geometric altitude rate of change (ft/min) |
|
A |
1905:25 |
2,238 |
84 |
87 |
1,400 |
-831 |
|
B |
1906:04 |
740 |
82 |
87 |
725 |
-1,344 |
|
C |
1907:03 |
1,957 |
65 |
77 |
684 |
- |
|
D |
1907:25 |
1,894 |
53 |
52 |
684 |
- |
|
E |
1908:12 |
788 |
49 |
44 |
450 |
-381 |
|
F |
1908:42 |
375 |
32 |
26 |
300 |
-319 |
|
[1] Airspeed has been derived from ADS-B recorded groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. [2] Altitude is either geometric altitude or pressure altitude reported in the ADS-B data set, corrected for atmospheric pressure. Geometric altitude is reported in increments of 25 ft, pressure altitude in increments of 100 ft. |
The ADS-B data indicated that the helicopter was levelled out at about 700 ft as it passed approximately 450 m abeam the bulk carrier on the downwind leg. The helicopter was about 1,200 m astern of the vessel at an altitude of about 700 ft, when it was turned right to make the base turn and position for final approach.
The turn onto final approach was completed about 1,900 m from the bulk carrier’s landing hatch at an altitude of about 700 ft and an airspeed of about 55 kt.
Figure 22: VH-ZGA derived airspeed, ADS-B reported altitudes and geometric altitude rate of change during the first night approach at the pilot boarding ground

Graphical summary of aggregated ADS-B and derived data during the evening of the accident, while VH-ZGA was being operated in vicinity of Anangel Explorer as it approached the pilot boarding ground, in night conditions under the night VFR. The airspeed of the helicopter is derived from the ADS-B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The helicopter altitude cross-references the ADS-B geometric altitude and the independently measured pressure altitude, adjusted for surface pressure. The geometric altitude is reported in 25 ft increments, the pressure altitude is reported in 100 ft increments. The geometric altitude rate of change was broadcast by the helicopter’s ADS-B equipment, in increments of 6.25 ft/min. Breaks in the continuity of the data indicate periods where the ADS‑B broadcasts were not being received. The labelled time markings correspond with the positions depicted for the helicopter in Figure 21 and Table 13.
Source: ATSB
After embarking the marine pilot to the bulk carrier, the crew flew VH-ZGA back to the heliport and landed at about 1924 and the pilot under supervision refuelled the helicopter. Due to the break in the shipping schedule, the pilot under supervision went back to their nearby accommodation, the instructor remained at the heliport to complete administrative tasks.
Second night flight
The second night flight was to disembark a marine pilot from the bulk carrier Cape Aster at C1/C2. The pilot under supervision arrived back at the heliport at about 2150 to prepare for the flight. The crew departed in the helicopter from the heliport just after 2250, set course for C1/C2 while climbing to 1,600 ft.
At 2257 the pilot under supervision made a radio transmission to the marine pilot on-board the departing bulk carrier. The marine pilot provided operational information relevant for the helicopter’s landing, which included the relative wind direction 60° left of the vessel’s bow at 8 kt and cleared the helicopter to land.
Recorded ADS-B data indicated that the crew of the helicopter established a descent from cruise altitude about 1.3 NM (2.4 km) from the bulk carrier and the rate of descent was about 500 ft/min.
Figure 23 depicts the flight path flown by the crew of the helicopter in vicinity of the bulk carrier. ADS-B and derived data at the alphabetically labelled points ‘A’ to ‘G’ is depicted in Table 14. The ADS-B and derived data is graphically depicted in Figure 24.
Figure 23: ADS-B data for VH-ZGA, during a night approach to Cape Aster as it approached C1/C2, which was the flight immediately prior to the accident flight

Representation of recorded track data during the second night flight, to disembark a marine pilot from Cape Aster at C1/C2. This flight was conducted at night, under night VFR procedures. The white track is positions of VH-ZGA recorded by the ASA ADS-B receivers. The annotated labels correspond to the ADS-B helicopter position relative to the bulk carrier’s landing hatch, as derived from shipping data recorded by the Australian Maritime Safety Authority. Data relevant to the annotated labels for VH-ZGA is presented in Table 14 and marked as labelled index points in Figure 24. The bulk carrier was 292 m in length.
Source: ATSB
Table 14: ADS-B and derived data, associated with the flight path of VH-ZGA depicted in Figure 23
|
Position |
Time (WST) |
Estimated range to landing hatch (m) |
Derived airspeed (kt)[1] |
Groundspeed (kt) |
Geometric altitude (ft) |
Geometric altitude rate of change (ft/min) |
|
A |
2303:39 |
- |
81 |
90 |
1,000 |
-513 |
|
B |
2304:15 |
- |
78 |
87 |
750 |
-194 |
|
C |
2304:46 |
1,478 |
83 |
83 |
550 |
0 |
|
D |
2305:23 |
1,603 |
60 |
56 |
500 |
-381 |
|
E |
2306:00 |
805 |
40 |
46 |
300 |
-194 |
|
F |
2306:29 |
421 |
36 |
39 |
375 |
+319 |
|
G |
2306:54 |
155 |
21 |
22 |
200 |
-1,025 |
|
[1] Airspeed has been derived from ADS-B recorded groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. |
The helicopter passed about 600 m astern of the bulk carrier descending through an altitude of about 1,200 ft, at a descent rate of about 500 ft/min and the airspeed was reducing through 100 kt. The helicopter was then turned right to orbit the vessel and position for the final approach. During the orbit of the vessel, the crew levelled the helicopter at about 550 ft.
The helicopter was turned onto final approach, approximately 1,500 m from the bulk carrier. During that turn, the helicopter’s altitude reduced, and the airspeed decreased below 60 kt. Over the next minute, the altitude continued to reduce. The helicopter descended to about 275 ft, at a range of approximately 700 m from the bulk carrier’s landing hatch, then the helicopter’s altitude started to gradually increase. Over the next 25 seconds, the helicopter’s altitude increased 100 ft while the range to the landing hatch continued to reduce.
When the helicopter was about 300 m from the landing hatch, the helicopter’s altitude was about 375 ft with the airspeed reducing through 35 kt. However, as the airspeed reduced through 30 kt, the geometric altitude rate of change then began to increase. As the airspeed continued to reduce the descent rate then increased, and during a 10-second period the altitude of the helicopter reduced from 300 to 150 ft at a rate of descent exceeding 700 ft/min and the airspeed reducing from 20 to 15 kt.
The descent towards the landing hatch was continued and by about 125 ft, the indicated geometric altitude rate of change had reduced below 300 ft/min, with an airspeed of about 15 kt. The helicopter landed on the bulk carrier about 2307 and the marine pilot was disembarked from the vessel.
Figure 24: VH-ZGA derived airspeed, ADS-B reported altitudes and geometric altitude rate of change during a night approach to Cape Aster at C1/C2

Graphical summary of aggregated ADS-B and derived data during the evening of the accident, while VH-ZGA was being operated in the vicinity of Cape Aster as it approached the C1/C2 channel markers, in night conditions under the night VFR. The airspeed of the helicopter is derived from the ADS-B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The helicopter altitude cross-references the ADS-B geometric altitude and the independently measured pressure altitude, adjusted for surface pressure. The geometric altitude is reported in 25 ft increments, the pressure altitude is reported in 100 ft increments. The geometric altitude rate of change was broadcast by the helicopter’s ADS-B equipment, in increments of 6.25 ft/min. Breaks in the continuity of the data indicate periods where ADS‑B broadcasts were not being received. The labelled time markings correspond with the positions depicted for the helicopter in Figure 23 and Table 14.
Source: ATSB
Appendix B – Night flights conducted by instructor at Port Hedland during January 2018
The following flights were conducted by the instructor while providing a period of leave relief during early January 2018. During the early morning of 8 January 2018, a series flights were flown at night under visual flight rules (night VFR) procedures and during which 5 marine pilot transfer (MPT) flights were conducted.
For the first transfer, the helicopter departed from the heliport at 0152 and transited to Shandong Ren He at the pilot boarding ground. Figure 25 depicts the flight path flown by the helicopter in vicinity of the bulk carrier. ADS-B and derived data at the alphabetically labelled points ‘A’ to ‘E’ is depicted in Table 15. The ADS-B and derived data is graphically depicted in Figure 26. On arrival, the helicopter flew past the ship and then circled at 800 ft to join final approach at 600 ft and 60 kt. The descent profile on final approach was not constant, with the descent rate varying between 0 and 1,000 ft/min (Figure 26).
Figure 25: ADS-B data for VH-ZGA, during a night approach to Shandong Ren He at the pilot boarding ground (first transfer)

Representation of ADS-B data (FlightRadar24) while VH-ZGA was being operated by the instructor at night under the night VFR in vicinity of Shandong Ren He as it approached the pilot boarding ground. Data relevant to the annotated labels A to E is presented in Table 15 and marked as labelled index points in Figure 26.
Source: Google Earth, annotated by the ATSB
Table 15: ADS-B and derived data, associated with the flight path of VH-ZGA depicted in Figure 25
|
Position |
Time (WST) |
Estimated range to landing hatch (m) |
Derived airspeed (kt)[1] |
Groundspeed (kt) |
Derived altitude (ft)[2] |
Geometric altitude rate of change (ft/min) |
|
A |
0204:28 |
- |
99 |
99 |
1,013 |
-512 |
|
B |
0204:55 |
- |
84 |
106 |
813 |
-192 |
|
C |
0205:29 |
1,450 |
60 |
53 |
713 |
-512 |
|
D |
0206:09 |
700 |
54 |
38 |
513 |
-512 |
|
E |
0206:25 |
475 |
43 |
26 |
313 |
-640 |
|
[1] Airspeed has been derived from ADS-B recorded groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. [2] Altitude has been derived from ADS-B recorded pressure altitude using the atmospheric pressure recorded by meteorological equipment at a nearby channel marker. |
Figure 26: Derived airspeed, ADS-B reported altitudes and geometric altitude rate of change during a night approach to Shandong Ren He at the pilot boarding ground (first transfer)

Graphical summary of FlightRadar24 ADS-B and derived data while VH-ZGA was being operated by the instructor at night under the night VFR in vicinity of Shandong Ren He as it approached the pilot boarding ground. The airspeed of the helicopter is derived from the ADS‑B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The helicopter altitude cross-references the ADS-B geometric altitude (where available) and the independently measured pressure altitude, adjusted for surface pressure. The geometric altitude is reported in 25 ft increments, the pressure altitude is reported in 100 ft increments. The geometric altitude rate of change was broadcast by the helicopter’s ADS-B equipment, in increments of 6.25 ft/min. Breaks in the continuity of the data indicate periods where ADS‑B broadcasts were not being received. The labelled time markings correspond with the positions depicted for the helicopter in Figure 25 and Table 15.
Source: ATSB
The flight to conduct the second transfer departed from the heliport at 0230 to pick up a marine pilot from the departing vessel Hebei Triumph, near C1/C2. Late in the transit the helicopter climbed to 2,200 ft then descended at up to 2,000 ft/min to circuit height. Late downwind it climbed to 900 ft then descended in the base turn at up to 1,500 ft/min with reducing airspeed to turn final below 500 ft and 30 kt. The descent profile on final approach was not stable, with the descent rate and airspeed decay moderating after 300 ft (see Figure 27, Table 16 and Figure 28).
Figure 27: ADS-B data for VH-ZGA, during a night approach to Hebei Triumph at C1/C2 (second transfer)

Representation of ADS-B data (ASA) while VH-ZGA was being operated by the instructor at night under the night VFR in vicinity of Hebei Triumph as it approached C1/C2. Data relevant to the annotated labels A to G is presented in Table 16 and marked as labelled index points in Figure 28.
Source: Google Earth, annotated by the ATSB
Table 16: ADS-B data and derived data, associated with the flight path of VH-ZGA depicted in Figure 27
|
Position |
Time (WST) |
Estimated range to landing hatch (m) |
Derived airspeed (kt)[1] |
Groundspeed (kt) |
Geometric altitude (ft) |
Geometric altitude rate of change (ft/min) |
|
A |
0242:00 |
- |
75 |
96 |
725 |
+319 |
|
B |
0242:27 |
- |
64 |
67 |
950 |
+575 |
|
C |
0242:46 |
- |
63 |
46 |
700 |
-1,600 |
|
D |
0242:58 |
- |
44 |
26 |
450 |
-1,150 |
|
E |
0243:09 |
975 |
28 |
14 |
300 |
-638 |
|
F |
0243:37 |
725 |
35 |
31 |
475 |
+256 |
|
G |
0244:01 |
475 |
28 |
21 |
300 |
-450 |
|
[1] Airspeed has been derived from ADS-B recorded groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. Where relevant, the airspeed calculation has been adjusted for any effect of the descent flight path vector. |
Figure 28: Derived airspeed, ADS-B reported altitudes and geometric altitude rate of change during a night approach to Hebei Triumph at C1/C2 (second transfer)

VFR in vicinity of Hebei Triumph as it approached C1/C2. The airspeed of the helicopter is derived from the ADS-B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The helicopter altitude cross-references the ADS-B geometric altitude and the independently measured pressure altitude, adjusted for surface pressure. The geometric altitude is reported in 25 ft increments, the pressure altitude is reported in 100 ft increments. The geometric altitude rate of change was broadcast by the helicopter’s ADS-B equipment, in increments of 6.25 ft/min. Breaks in the continuity of the data indicate periods where ADS‑B broadcasts were not being received. The labelled time markings correspond with the positions depicted for the helicopter in Figure 27 and Table 16.
Source: ATSB
The third and fourth transfers were conducted consecutively during the third flight that morning. A marine pilot was transferred to an inbound vessel (Stella Tess) at the pilot boarding ground and the helicopter was then flown to collect a marine pilot from a departing vessel (China Fortune) at C1/C2.
The helicopter departed the heliport at 0305 and the transit to the pilot boarding ground was flown at 1,100 ft, which was below the lowest safe altitude (LSALT) for conducting flight at night under the VFR. After flying past the inbound vessel at 1,100 ft, the helicopter entered a climb (of maximum 900 ft/min) for about 30 seconds then descended in the circuit at between 400–500 ft/min. The entry into the climb would have occurred soon after the instructor lost visual reference with the vessel (see Figure 29, Table 17 and Figure 30).
Late in the base turn, the helicopter was still at 1,000 ft with rate of descent of about 900 ft/min and a derived airspeed of about 85 kt. The descent profile on final approach varied between 9–18° (short final) with a variable descent rate moderating from mid-final.
Figure 29: ADS-B data for VH-ZGA during a night approach to Stella Tess at the pilot boarding ground (third transfer)

Representation of ADS-B data (ASA) while VH-ZGA was being operated by the instructor at night under the night VFR in vicinity of Stella Tess as it approached the pilot boarding ground. Data relevant to the annotated labels A to G is presented in Table 17 and marked as labelled index points in Figure 30.
Source: Google Earth, annotated by the ATSB
Table 17: ADS-B data and derived data, associated with the flight path of VH-ZGA depicted in Figure 29
|
Position |
Time (WST) |
Estimated range to landing hatch (m) |
Derived airspeed (kt)[1] |
Groundspeed (kt) |
Geometric altitude (ft) |
Geometric altitude rate of change (ft/min) |
|
A |
0312:11 |
- |
92 |
106 |
1,050 |
0 |
|
B |
0312:27 |
- |
87 |
111 |
1,200 |
+575 |
|
C |
0312:47 |
- |
96 |
111 |
1,200 |
-450 |
|
D |
0313:12 |
1,800 |
84 |
70 |
1,000 |
-894 |
|
E |
0313:32 |
1,350 |
75 |
59 |
700 |
-831 |
|
F |
0313:46 |
975 |
58 |
42 |
500 |
-575 |
|
G |
0314:40 |
325 |
38 |
21 |
300 |
-513 |
|
[1] Airspeed has been derived from ADS-B recorded groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. Where relevant, the airspeed calculation has been adjusted for any effect of the descent flight path vector. |
Figure 30: Derived airspeed, ADS-B reported altitudes and geometric altitude rate of change during a night approach to Stella Tess at the pilot boarding ground (third transfer)

Graphical summary of aggregated ADS-B and derived data while VH-ZGA was being operated by the instructor at night under the night VFR in vicinity of Stella Tess as it approached the pilot boarding ground. The airspeed of the helicopter is derived from the ADS-B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The helicopter altitude cross-references the ADS-B geometric altitude and the independently measured pressure altitude, adjusted for surface pressure. The geometric altitude is reported in 25 ft increments, the pressure altitude is reported in 100 ft increments. The geometric altitude rate of change was broadcast by the helicopter’s ADS-B equipment, in increments of 6.25 ft/min. Breaks in the continuity of the data indicate periods where ADS‑B broadcasts were not being received. The labelled time markings correspond with the positions depicted for the helicopter in Figure 29 and Table 17.
Source: ATSB
After disembarking the marine pilot to the vessel at the pilot boarding ground, the helicopter departed and climbed to 2,000 ft for the transit to China Fortune, which was approaching C1/C2. The helicopter commenced descent as it approached the vessel, joining the circuit at an altitude of about 900 ft mid downwind. Before and during the base turn there was a slight climb then descent increasing to 1,350 ft/min turning finals. This transitioned into a climb of 500 ft/min then a descent at 1,100 ft/min at around 300 ft and about 40 kt airspeed. The descent profile on final approach continued to be unstable (see Figure 31, Table 18 and Figure 32).
Figure 31: ADS-B data for VH-ZGA, during a night approach to China Fortune at C1/C2 (fourth transfer)

Representation of ADS-B data (ASA) while VH-ZGA was being operated by the instructor at night under the night VFR in vicinity of China Fortune as it approached C1/C2. Data relevant to the annotated labels A to H is presented in Table 18 and marked as labelled index points in Figure 32.
Source: Google Earth, annotated by the ATSB
Table 18: ADS-B and derived data, associated with the flight path of VH-ZGA depicted in Figure 31
|
Position |
Time (WST) |
Estimated range to landing hatch (m) |
Derived airspeed (kt)[1] |
Groundspeed (kt) |
Geometric altitude (ft) |
Geometric altitude rate of change (ft/min) |
|
A |
0327:23 |
- |
87 |
80 |
1,000 |
-638 |
|
B |
0327:44 |
- |
78 |
86 |
875 |
+194 |
|
C |
0328:15 |
1,575 |
60 |
77 |
950 |
-513 |
|
D |
0328:29 |
1,275 |
55 |
56 |
700 |
-1,344 |
|
E |
0328:38 |
1,100 |
46 |
45 |
500 |
-1,088 |
|
F |
0329:02 |
800 |
37 |
36 |
450 |
+575 |
|
G |
0329:29 |
425 |
41 |
25 |
300 |
-1,088 |
|
H |
0329:43 |
300 |
21 |
19 |
150 |
0 |
|
[1] Airspeed has been derived from ADS-B recorded groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. Where relevant, the airspeed calculation has been adjusted for the effect of the descent flight path vector. |
Figure 32: Derived airspeed, ADS-B reported altitudes and geometric altitude rate of change during a night approach to China Fortune at C1/C2 (fourth flight)

Graphical summary of aggregated ADS-B and derived data while VH-ZGA was being operated by the instructor at night under the night VFR in vicinity of China Fortune as it approached C1/C2. The airspeed of the helicopter is derived from the ADS-B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The helicopter altitude cross-references the ADS-B geometric altitude and the independently measured pressure altitude, adjusted for surface pressure. The geometric altitude is reported in 25 ft increments, the pressure altitude is reported in 100 ft increments. The geometric altitude rate of change was broadcast by the helicopter’s ADS-B equipment, in increments of 6.25 ft/min. Breaks in the continuity of the data indicate periods where ADS‑B broadcasts were not being received. The labelled time markings correspond with the positions depicted for the helicopter in Figure 31 and Table 18.
Source: ATSB
The fourth flight (transfer 5) departed the heliport at 0355 to pick up a marine pilot from Iron Pilbara near C1/C2. The helicopter overflew the ship at 1,375 ft on descent and joined the circuit to be 1,250 ft by mid downwind. As the helicopter descended in the base turn the descent rate briefly reached 1,700 ft/min at about 700 ft then reduced back to level flight to be established on final approach at 375 ft and airspeed below 40 kt. The descent profile flown during base and final was unstable (see Figure 33, Table 19 and Figure 34).
Figure 33: ADS-B data for VH-ZGA, during a night approach to Iron Pilbara at C1/C2 (fifth transfer)

Pilbara as it approached C1/C2. Data relevant to the annotated labels A to G is presented in Table 19 and marked as labelled index points in Figure 34.
Source: Google Earth, annotated by the ATSB
Table 19: ADS-B and derived data, associated with the flight path of VH-ZGA depicted in Figure 33
|
Position |
Time (WST) |
Estimated range to landing hatch (m) |
Derived airspeed (kt)[1] |
Groundspeed (kt) |
Geometric altitude (ft) |
Geometric altitude rate of change (ft/min) |
|
A |
0409:10 |
- |
92 |
113 |
1,275 |
-381 |
|
B |
0409:48 |
- |
51 |
36 |
1,000 |
-1,025 |
|
C |
0410:02 |
- |
54 |
34 |
700 |
-1,600 |
|
D |
0410:12 |
- |
49 |
32 |
500 |
-1,088 |
|
E |
0410:38 |
1,075 |
36 |
19 |
375 |
-63 |
|
F |
0411:20 |
525 |
36 |
27 |
300 |
-381 |
|
G |
0411:40 |
350 |
24 |
16 |
150 |
+256 |
|
[1] Airspeed has been derived from ADS-B recorded groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. Where relevant, the airspeed calculation has been adjusted for any effect of the descent flight path vector. |
Figure 34: Derived airspeed, ADS-B reported altitudes and geometric altitude rate of change during a night approach to Iron Pilbara at C1/C2 (fifth transfer)

Graphical summary of aggregated ADS-B and derived data while VH-ZGA was being operated by the instructor at night under the night VFR in vicinity of Iron Pilbara as it approached C1/C2. The airspeed of the helicopter is derived from the ADS-B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The helicopter altitude cross-references the ADS-B geometric altitude and the independently measured pressure altitude, adjusted for surface pressure. The geometric altitude is reported in 25 ft increments, the pressure altitude is reported in 100 ft increments. The geometric altitude rate of change was broadcast by the helicopter’s ADS-B equipment, in increments of 6.25 ft/min. Breaks in the continuity of the data indicate periods where ADS‑B broadcasts were not being received. The labelled time markings correspond with the positions depicted for the helicopter in Figure 33 and Table 19.
Appendix C – Line check flight or night VFR rating flight conducted 5 April 2017
Figure 35: ADS-B data for VH-ZGA, during a night approach to Pacific Treasure at the pilot boarding ground

Representation of ADS-B data (ASA) while VH-ZGA was being operated at night under the night VFR in vicinity of Pacific Treasure as it approached the pilot boarding ground. On board the helicopter was the instructor and the operator’s chief pilot. The flight was recorded as either a line check for the instructor or a night VFR flight review for the chief pilot. Data relevant to the annotated labels A to F is presented in Table 20 and marked as labelled index points in Figure 36.
Source: Google Earth, annotated by the ATSB
Table 20: ADS-B and derived data, associated with the flight path of VH-ZGA depicted in Figure 35
|
Position |
Time (WST) |
Estimated range to landing hatch (m) |
Derived airspeed (kt)[1] |
Groundspeed (kt) |
Geometric altitude (ft) |
Geometric altitude rate of change (ft/min) |
|
A |
1923:04 |
- |
92 |
97 |
1,075 |
+63 |
|
B |
1923:48 |
- |
72 |
73 |
1,050 |
0 |
|
C |
1924:15 |
2,150 |
78 |
82 |
900 |
-256 |
|
D |
1924:39 |
1,275 |
59 |
62 |
725 |
-706 |
|
E |
1924:57 |
850 |
38 |
40 |
500 |
-769 |
|
F |
1925:36 |
275 |
27 |
29 |
300 |
0 |
|
[1] Airspeed has been derived from ADS-B recorded groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature.
|
Figure 36: Derived airspeed, ADS-B reported altitudes and geometric altitude rate of change during a night approach to Pacific Treasure at the pilot boarding ground

Graphical summary of aggregated ADS-B and derived data while VH-ZGA was being operated at night under the night VFR in vicinity of Pacific Treasure as it approached the pilot boarding ground. On board the helicopter was the instructor and the operator’s chief pilot. The airspeed of the helicopter is derived from the ADS-B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The helicopter altitude cross-references the ADS-B geometric altitude and the independently measured pressure altitude, adjusted for surface pressure. The geometric altitude is reported in 25 ft increments, the pressure altitude is reported in 100 ft increments. The geometric altitude rate of change was broadcast by the helicopter’s ADS-B equipment, in increments of 6.25 ft/min. Breaks in the continuity of the data indicate periods where ADS‑B broadcasts were not being received. The labelled time markings correspond with the positions depicted for the helicopter in Table 20 and Figure 35.
Source: ATSB
Figure 37: ADS-B data for VH-ZGA, during a night approach to Shandong Zheng Tong at C1/C2

Representation of ADS-B data (ASA) while VH-ZGA was being operated at night under the night VFR in vicinity of Shandong Zheng Tong as it approached C1/C2. On board the helicopter was the instructor and the operator’s chief pilot. The flight was recorded as either a line check for the instructor or a night VFR flight review for the chief pilot. Data relevant to the annotated labels A to E is presented in Table 21 and marked as labelled index points in Figure 38.
Source: Google Earth, annotated by the ATSB
Table 21: ADS-B data and derived data, associated with the flight path of VH-ZGA depicted in Figure 37
|
Position |
Time (WST) |
Estimated range to landing hatch (m) |
Derived airspeed (kt)[1] |
Groundspeed (kt) |
Geometric altitude (ft) |
Geometric altitude rate of change (ft/min) |
|
A |
1936:01 |
1,575 |
105 |
109 |
1,250 |
-575 |
|
B |
1937:14 |
2,425 |
77 |
77 |
1,000 |
-319 |
|
C |
1937:39 |
1,550 |
65 |
67 |
700 |
-575 |
|
D |
1938:13 |
725 |
40 |
39 |
500 |
-513 |
|
E |
1938:54 |
325 |
28 |
25 |
300 |
-256 |
|
[1] Airspeed has been derived from ADS-B recorded groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. |
Figure 38: Derived airspeed, ADS-B reported altitudes and geometric altitude rate of change during a night approach to Shandong Zheng Tong at C1/C2

Graphical summary of aggregated ADS-B and derived data while VH-ZGA was being operated at night under the night VFR in vicinity of Shandong Zheng Tong as it approached C1/C2. On board the helicopter was the instructor and the operator’s chief pilot. The airspeed of the helicopter is derived from the ADS-B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for temperature. The helicopter altitude cross-references the ADS-B geometric altitude and the independently measured pressure altitude, adjusted for surface pressure. The geometric altitude is reported in 25 ft increments, the pressure altitude is reported in 100 ft increments. The geometric altitude rate of change was broadcast by the helicopter’s ADS-B equipment, in increments of 6.25 ft/min. Breaks in the continuity of the data indicate periods where ADS‑B broadcasts were not being received. The labelled time markings correspond with the positions depicted for the helicopter in Table 21 and Figure 37.
Source: ATSB
Appendix D – Principles of helicopter operation
Basic helicopter aerodynamics
Acting on any aircraft in flight are the primary forces of thrust/drag and lift/weight. For helicopters in powered forward flight, the upward force generated by the main rotor (rotor thrust) simultaneously provides the vertical lift component and propulsive component in varying ratios according to the tilt angle of the main rotor. The degree to which the vertical component exceeds weight (and any g‑loading) will influence the rate of climb/descent and the extent to which the propulsive component exceeds drag will influence acceleration. Figure 39 depicts the 4 primary forces acting on a helicopter in flight.
Figure 39: Four primary forces acting on a helicopter in forward flight

Source: FAA Helicopter Flying Handbook (FAA-H-8083-21B)
The pilot (or autopilot in some cases) controls the total quantity of main rotor thrust by raising or lowering the collective control to increase/decrease blade pitch with associated increase/decrease of engine power (measured as torque in turbine helicopters). At the same time, the pilot controls the tilt angle of main rotor thrust by moving the cyclic control to selectively change blade pitch and consequently helicopter attitude and direction. Rotation of the main rotor produces a torque reaction which is controlled by the pilot through pedals that alter the pitch of the tail rotor or output of alternative anti-torque mechanism.
Basic helicopter performance
In normal operation, helicopter performance can be limited by high gross weight (mass) and low air density (high altitude and/or high temperatures). Given these factors were not present in this occurrence, the primary influence on in-flight performance was airspeed, manoeuvring, and applied engine power/torque. Although wind is a potential effect on performance, this was generally not a significant factor in the approach phase for this occurrence.
Airspeed is a function of the attitude of the helicopter and applied engine power/torque. The amount of engine power/torque required to maintain a specific airspeed or accelerate/decelerate is related to total drag that varies according to airspeed. (Figure 40) At the lowest point of the total drag curve, the power required is at a minimum and the corresponding airspeed is defined as best rate of climb speed (Vy). Therefore, as a helicopter decelerates through Vy, the power required will progressively reduce then start to increase.
Figure 40: Representative drag curves

Source: FAA Helicopter Flying Handbook (FAA-H-8083-21B)
Manoeuvres can have 3 inter-related effects on performance with relatively higher power requirements. Any increase to g-loading is equivalent to an increase in weight and tilting of the rotor will reduce the lift component of main rotor thrust. An increase in anti-torque demand requires additional engine power/torque.
To manage the flight path of a helicopter effectively, the pilot anticipates the engine power/torque requirements for that phase of flight, coordinates the flight control inputs (or commands the autopilot), and monitors performance in case further adjustments are required. If engine power is insufficient, the adverse effect on airspeed and vertical speed (rate of descent) can be compounding.
Vortex ring state
If the flight path, airspeed, and rate of descent of a helicopter is mismanaged, an abnormal condition known as vortex ring state (VRS) can develop. When this occurs, the helicopter descends into air already affected by the main rotor downwash, which significantly impairs main rotor efficiency and thrust. In VRS flight conditions, any further application of power/torque will accelerate the downwash and increase the rate of descent with uncommanded pitch and roll.
Main rotor design
The twin-engine EC135 helicopter was designed with a 4-bladed hinge-less and bearing-less main rotor known as a ‘rigid’ system. Rotor blade movement in all axes is enabled by an inboard flexbeam.
The single-engine B206L helicopter was designed with a 2-bladed teetering‑head main rotor system known as a ‘semi-rigid’ system. This allows the main rotor to flap (move up/down) as an assembly.
As a consequence, the handling characteristics of the 2 helicopters were different. In general terms, the EC135 type was relatively more sensitive to control inputs than B206 types.
Appendix E – Research relevant to the prior sleep wake model
Introduction of the prior sleep wake model
Dawson and McCullough (2005) outlined a series of levels associated with fatigue-risk trajectory (Figure 41). To effectively manage fatigue risk, they stated that a fatigue risk management system (FRMS) should develop appropriate controls at each of the levels. In particularly, they noted that, in addition to prescribing hours of service (HOS) limits, an organisation should also specify controls in terms of prior sleep and wake.
Figure 41: Fatigue-risk trajectory from Dawson and McCullough (2005)

Dawson and McCullough stated:
… we would suggest that knowledge of the frequency distribution of prior sleep and wake could form a rational basis for determining the level of fatigue an individual is likely to experience within a given shift. Furthermore, there is potential for both individuals and organizations to use this information as the basis for rational decision making with respect to fatigue-related risk …
As a starting point for this decision, we suggest that a rational FRMS should be based on prior sleep and wake rules, linked to an evaluation of the adequacy of prior sleep and wake. The reasons for this are straightforward:
Unlike subjective estimates of fatigue, prior sleep and wake are observable and potentially verifiable determinants of fatigue;
Prior sleep and wake provide a way of integrating individual and organizational measures of fatigue (levels 1 and 2) since systems-based approaches can deal with probabilistic estimates of sleep and wakefulness, and individual employees can make clear determinations of individual amounts of actual prior sleep and wakefulness; and
Prior sleep and wake measures can be set or modified according to the risk profile associated with specific tasks or workgroups.
The authors also proposed an algorithm, known as the prior sleep wake model (PSWM), which stated that fitness for work could be determined by specifying appropriate values for sleep obtained in the last 24 hours, sleep obtained in the last 48 hours, and the length of time awake until the end of work.
With regard to sleep within 24 hours, Dawson and McCullough (2005) stated:
Following a single night of sleep loss, it would appear that there is little evidence of a clinically significant reduction in any measure of sleepiness/ alertness until TIB [time in bed] is reduced below 6 h. Most measures show significant clinical levels of sleepiness once TIB is reduced to 4 h. Between 6 and 4 h there is some debate based on the measure used (i.e. psychomotor vigilance, reaction time or more complex cognitive tasks); and the degree to which the task is engaging or boring ...
…it is unlikely that individuals would be significantly impaired at most common work tasks until obtained sleep fell below 5 h in the preceding 24. There are a number of caveats to this conclusion …
With regard to sleep over longer periods, the paper reviewed several studies involving multiple nights of sleep restriction. These included studies by Belenky and others (2003) and Van Dongen and others (2003) that demonstrated a dose-response relationship; as the extent of sleep restriction per day increased and as the number of days of sleep instruction increased, then the extent of the performance deficits increased.
Overall, based on their review of relevant research available at the time, Dawson and McCullough (2005) concluded:
We can extrapolate from this data to conclude that it is unlikely that prior to commencing work an individual obtaining less than 5 h sleep in the prior 24 and 12 h sleep in the prior 48 h and who is awake for longer than the amount of sleep in the prior 48 h is likely to be unimpaired at a level consistent with a safe system of work.
In defining this threshold we caution readers that particular occupational tasks may well be more susceptible to fatigue-related error or the consequences of fatigue-related error are so severe as to require threshold values greater than we have specified. Furthermore, these initial values should be viewed as a starting point and subject to revision in the light of actual workplace experience.
Subsequent research
In 2015, the American Academy of Sleep Medicine and Sleep Research Society developed a consensus recommendation for the amount of sleep needed by adults (Watson and others 2015a). It stated that adults should sleep 7 hours or more per night on a regular basis to promote optimal health. It also stated that sleeping less than 7 hours per night was associated with impaired performance, increased errors and greater risk of accidents.
In further discussion, Watson and others (2015b) stated:
Research findings show two consistent cognitive performance dynamics relative to 8 hours TIB for sleep: (1) The shorter the sleep duration, the greater the cognitive performance deficits; and (2) the longer the exposure to sleep restriction, the greater the cognitive deficits. Thus, the less sleep obtained, and the longer this continues, the more quickly cognitive deficits become evident. Self-reported sleepiness does not show the latter dynamic and therefore cannot be used to track increasing performance deficits. In addition, total sleep duration per 24 hours is the critical factor relative to performance, since split-sleep schedules also show the same sleep dose-response effects. Finally, the adverse effects of limited sleep time are especially severe at circadian times when sleep propensity is high …
In summary, Level I evidence demonstrates that cognitive performance involving vigilance attention, cognitive processing speed and working memory, as well as physiological sleep propensity and drowsy driving are all sensitive to sleep duration below 7 hours.
Although less than 7 hours sleep can have a adverse effect on performance (for most individuals), determining exactly how much sleep is necessary to achieve a minimum or appropriate level of alertness and performance has been a subject of debate. As stated above, Dawson and McCullough (2005) proposed 5 hours sleep in 24 and 12 hours sleep in 48 as minimum operational limits. Other research has indicated that more sleep may be appropriate.
For example, Thomas and Ferguson (2010) found the occurrence of crew errors was higher, and performance at managing threats was poorer, during flights when a flight crew included a captain with less than 6 hours sleep or a first officer with less than 5 hours sleep. Road safety research has also shown that 5–6 hours sleep is associated with significantly more risk of an accident than 7–8 hours sleep (Williamson and others 2011).
One study specifically examined the most suitable PSWM values to predict involvement in fatigue-related truck accidents (Dorrian and others 2011). This study found that using the standard PSWM values (5 hours in 24 / 12 hours in 48) correctly classified 65% of accidents. However, using a modified model (6.5 hours / 8 hours) provided a slightly better prediction (71%), and a model using only sleep in the last 24 hours (6.5 hours) provided even better results (75%). The authors noted that, based on their results, the 5-hour value for the last 24 hours may not be conservative enough.
Dawson and others (2021) reviewed relevant laboratory research studies into the effects of restricted sleep in the previous 24 hours conducted since the Dawson and McCullough (2005) paper. It concluded:
While it appears that there are some effects of 6 h sleep and/or sleep opportunities on next-day cognitive performance, these differences tend to be small in magnitude and are inconsistent in the literature. When sleep is restricted to five hours during a laboratory-based protocol, findings are very consistent. Significant performance decrements after ~5 h prior sleep have been seen in measures such as distractibility …, reaction time, and sustained attention…, and increases in both errors of commission and omission ... This is in line with much of the pre-2005 literature, which demonstrates heightened performance decrements with one night of ~5 h sleep ...
Research into sleep duration of 4 h has indicated that there is a very significant likelihood that all individuals will be impaired in a number of cognitive domains…
The paper also noted some road safety research which indicated that drivers who had obtained 5–6 hours sleep had increased accident risk or poorer driver performance compared to drivers who obtained more sleep.
Dawson and others (2021) also reviewed extended wakefulness research, noting there was limited research available to support the PSWM rule for extended wakefulness when it was developed in 2005. They noted that several studies since 2005 had shown cognitive performance begins to degrade after 16–18 hours of wakefulness, with performance deteriorating further as the duration of wakefulness increased.
Additional information
Although specifying minimum levels of prior sleep before conducting work has significant merit, there are a range of other aspects to consider when applying risk controls based on the PSWM. For example, individuals vary in terms of their sleep needs. In addition, restricted sleep prior to the previous 48 hours can also have some influence on a person’s level of alertness (albeit not as much as the previous 24 or 48 hours).
A range of factors other than the quantity of sleep can also influence fatigue, such as the quality of sleep, time of day and the extent to which rest breaks during work tasks are available and used. The type of work tasks being performed is also critically important and, as indicated by Dawson and McCullough, some types of safety-critical tasks should probably use different PSWM thresholds.
In terms of the time of day, the adverse effects of limited sleep are exacerbated at times of day when sleep propensity is higher, such as during the window of circadian low (Watson and others (2015b). In addition, most of the research into the effect of restricted sleep is based on sleep occurring during the night. The extent to which the same PSWM rules should apply to sleep occurring during the day is unclear. As noted by Dawson and McCullough (2005):
While it is true that when sleep is attempted at an inappropriate circadian time it is typically reported as more disrupted and shorter and subjects report the sleep to be less satisfying, the relationship between neurobehavioral performance recovery and sleep duration and quality are typically confounded.
Another key aspect to consider when applying the PSWM is the accuracy of sleep information. Some research has shown that people generally overestimate the amount of sleep they obtain (Lauderdale and others 2008, Jackson and others 2018). People also underestimate the impact of several days of sleep restriction (Banks and Dinges 2007, Watson and others 2015b), and therefore may not recognise the importance of accurately reporting sleep information.
More importantly, within a work context, there are many factors that can influence how people will report information such as their amount of sleep. Depending on the consequences of what they report, employees may be more likely to overestimate the amount of sleep they obtain. The ATSB is not aware of any published research that has examined the accuracy of reported sleep information in the context of an FRMS that uses the PSWM.
Applications of the PSWM
Prior sleep and wake information is used in by many organisations as part of an FRMS (Sprajcer and others 2022), and the ATSB is aware of many aviation and rail organisations who have integrated the PSWM into their fatigue management processes. This has generally been as an additional type of risk control to the use of minimum hours of work requirements and a biomathematical model of fatigue (BMMF) to evaluate planned work schedules. In some cases, the use of the PSWM has only been required when considering an extension or change to a planned work schedule. In other cases, the PSWM information has been provided to employees as educational information for them to evaluate their own fitness for work.
In many cases, the application of the PSWM involved allocating points depending on the extent of any exceedance of the 24-hour, 48-hour and extended wakefulness rules. This individual fatigue likelihood score (IFLS) was then compared with a table of listed score ranges that specified likely fatigue-related symptoms and, more importantly, mandatory and/or optional risk controls to implement to manage the risk associated with the overall score. This approach typically allocated more points for every hour of exceedance of the 24-hour rule than the other rules.
Most applications of the PSWM use the default values stated by Dawson and McCullough (2005). However, some applications use higher thresholds, such as 6 hours sleep in the last 24 hours and 13 hours sleep in the last 48 hours.
Prior to the current investigation, the ATSB had not encountered an FRMS which required operational personnel to record their sleep and wake information and for an organisation to use that information to determine fitness for duty in accordance with the PSWM. The ATSB is not aware of any published research evaluating the effectiveness of an FRMS based primarily on using the PSWM to determine whether operational personnel are fit for duty.
- LSALT is 1,000 ft higher than the highest obstacle 10 NM (19 km) either side of planned track.
- The estimate of airspeed was derived from ADS-B groundspeed and ground track using the wind velocity and atmospheric pressure recorded by meteorological equipment at a nearby channel marker and corrected for tem
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2022
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |