
What happened
At about 1618 Eastern Standard Time on 8 July 2015, the pilot/owner of an amateur-built Pitts Model 12, registered VH‑JDZ, took off from Maitland Airport, New South Wales.
Witnesses reported hearing a loud engine noise at about 1630 that caught their attention. They then observed the aircraft at the top of what appeared to be a vertical climb. The aircraft slid backwards, tail first, before entering a horizontal spin. Shortly after, the witnesses lost sight of the aircraft below the tree line and some reported hearing a loud bang.
The aircraft was located by search aircraft and ground personnel who arrived at the site of the accident at about 1715. The aircraft had collided with terrain in thick bushland, fatally injuring the pilot. The aircraft was destroyed by impact forces and an intense post-impact fire.
What the ATSB found
Radar data and witness reports were consistent with the aircraft being used for aerobatic manoeuvres in the minutes prior to the accident.
The ATSB considered the results of the pilot’s post-mortem examination, which indicated the pilot had coronary artery disease that may have resulted in permanent incapacitation. However, while that remained a possibility, there was insufficient evidence to conclude that it influenced the development of the accident. The ATSB found that for reasons that could not be determined, VH‑JDZ entered a vertical manoeuvre from which the pilot did not regain control before colliding with terrain. Additionally, the aircraft was being flown at a height which reduced the time available to effect a recovery, if required.
The ATSB also identified instances of misinterpretation of a number of the regulations concerning the maintenance of amateur-built experimental aircraft. This has the potential to affect the safety of these aircraft and those on board.
Safety message
Aerobatic flying requires extensive training and ongoing commitment to maintain the skills necessary for safe operations. Unauthorised aerobatic manoeuvres increase the risk to the pilot, any passengers and third parties in the vicinity of the aerobatics.
Flying at low level reduces the safety margin available should something unexpected happen. The ATSB has issued a series of ‘Avoidable Accidents’ publications, the first of which details the risks involved in low-level flying and includes the following statement:
Low-level flying also presents fewer opportunities to recover from a loss of control compared to flight at higher altitudes. It takes time to react and to regain control of an aircraft, and the closer to the ground you are, the less time and distance you have. Flying at low altitudes is not only risky when things are going right; it becomes downright perilous when things are going wrong.
More information is available from the ATSB’s avoidable accident web page.
Finally, ongoing safety requires aircraft owners and maintainers to operate and maintain the aircraft in accordance with relevant regulations, including those specific to experimental aircraft. Aircraft operation and maintenance outside the regulatory requirements increases safety risk.
Amateur-built Pitts Model 12 registered VH-JDZ

Source: Supplied
At about 1618 Eastern Standard Time (EST)[1] on 8 July 2015, the pilot/owner of an amateur-built Pitts Model 12, registered VH-JDZ (JDZ), departed Maitland Airport, New South Wales on a local flight. The aircraft was being operated in the experimental category and the pilot was the only person on board.
JDZ was fitted with a transponder[2] however, the aircraft was not detected by secondary radar. The lack of a secondary surveillance radar return was consistent with either the transponder not being activated or, if activated, the equipment not operating correctly (see the section titled Radar and airspace information). However, primary surveillance radar detected an aircraft at about 1622, to the south of Maitland Airport. The location and movements of this aircraft were consistent with the area in which the pilot of JDZ was reported to regularly conduct aerobatics (see the following discussion).
The primary radar data indicated that the aircraft initially flew in a south-easterly direction, before heading west toward an area near Lovedale Road and Keinbah Quarry. The aircraft then tracked variously east and west, consistent with the conduct of aerobatic manoeuvres. The aircraft disappeared from radar before reappearing on two occasions during the flight. At about 1630 the aircraft disappeared from radar a third time and was not detected again.
Witnesses reported that the area in which they saw the aircraft leading up to the accident is regularly used for aerobatics. Several witnesses reported hearing a particularly loud engine sound at about 1630 that caught their attention. Witnesses described:
- the aircraft at the top of what appeared to be a vertical climb
- the aircraft sliding backwards, tail first, before entering a flat spin
- that the flat spin descent was slow and almost straight down, with little forward speed
- that the aircraft completed several rotations during the spin before sight was lost behind trees.
Three of the witnesses believed the aircraft had impacted terrain and contacted the police. At about 1650 emergency personnel arrived in the area and commenced a ground search. At the same time, a number of aircraft from Maitland Airport commenced an aerial search. A rescue helicopter was also dispatched.
The aircraft was located from the air at about 1712 and ground crews arrived at the site shortly after. The aircraft had collided with terrain in thick bushland in the area in which aircraft regularly conducted aerobatics and close to where the previously-discussed aircraft disappeared from primary surveillance radar. The pilot was fatally injured and there was an intense post‑impact fire. The fire could not be extinguished with the available resources and was monitored until it self‑extinguished (Figure 1).
Figure 1: Accident site viewed from the front of the aircraft and showing the surrounding thick vegetation and minimal structural damage to the wings and airframe (consistent with the reported vertical descent)

Source: ATSB
__________
- Eastern Standard Time (EST) was Coordinated Universal Time (UTC) + 10 hours.
- A radio device that, when triggered by the correct radio signal (called interrogation), transmits a pre-coded reply. Air traffic control ground equipment interrogates the aircraft’s transponder, identifies the aircraft by its reply code and displays the aircraft’s position on the controller’s radar screen.
Pilot information
The pilot commenced flying in December 2006 and was issued with a Private Pilot (Aeroplane) Licence in January 2008. In addition, the pilot was endorsed for single-engine aeroplanes not exceeding 5,700 kg maximum take‑off weight and category design features including retractable undercarriage and manual propeller pitch control.
The pilot had accrued about 750 hours flying experience, mostly in Piper PA32 and Eagle Aircraft 150-type aircraft. The pilot completed an emergency manoeuvre training course in a Pitts S2A in June 2010 and commenced aerobatic training in a similar aircraft in August 2012. In February 2014, the pilot was issued an endorsement to fly ‘tail wheel undercarriage aircraft’ and completed a flight review at the same time.
The pilot commenced dual familiarisation flying in VH-JDZ (JDZ) in December 2014. Basic aerobatic training was also conducted in JDZ from March 2015. At the time of the accident the pilot had accrued about 22 hours in JDZ, of which about 7 hours was solo. The pilot’s aerobatic flying experience, under instruction and in a Pitts S2A, a Yakovlev Yak 52 and JDZ, totalled about 21.5 hours.
The pilot had not yet achieved the required competency to be authorised for spinning or an aerobatic endorsement. In addition, the pilot was advised by his instructors to not conduct solo aerobatics.
The pilot held a current Class 2 Medical Certificate that was issued on 22 January 2015.
Aircraft information
General
JDZ was an amateur-built Pitts Model 12 two-seat tandem biplane, serial number 42. It was powered by a Vedeneyev M14P radial engine and had a two-blade composite constant speed propeller. The only special requirements to operate the Pitts Model 12 were an endorsement for tail wheel undercarriage and for manual propeller pitch control.
The pilot purchased JDZ from the builder on 11 November 2014 and became the registered operator on 11 December 2014.
Construction and certification
JDZ was purchased as a kit from the aircraft manufacturer in the United States and assembly commenced in Australia in 1999. The aircraft was issued with a Special Certificate of Airworthiness (SCOA) on 24 October 2006. An annex to the SCOA outlined a number of Phase I operational limitations and specific maintenance requirements. This included the requirement for at least 25 hours of flight testing within a 35 NM (65 km) radius of Wedderburn Airport, New South Wales. Unusually, the SCOA was not limited by an expiry date.
An entry in the aircraft logbook on 12 November 2014 stated that the required 25 flight test hours were complete. Manoeuvres recorded as tested included 'loops, rolls, spins, half‑cuban eights, roll off the top of a loop, wingover and snaps [snap rolls]’. The SCOA flight test area was amended on 12 December 2014 to include Maitland Airport.
On 12 June 2015, SCOA Phase II replaced Phase I, authorising operation of an amateur-built aircraft in accordance with the Phase II limitations. These limitations restricted the conduct of aerobatic manoeuvres to those that had been flight tested.
Airworthiness and maintenance
The aircraft logbook statement required JDZ to be maintained under Civil Aviation Regulation 1988 (CAR) Schedule 5 and in accordance with the additional requirements of the annex to the SCOA. An annual inspection was to be carried out every 100 hours or 12 months, whichever came first. The last annual inspection was completed on 16 March 2015, and the associated maintenance release was valid at the time of the accident.
Uncertified maintenance
Maintenance carried out on an aircraft is required to be certified complete in accordance with CAR 42ZE and CAR Schedule 6. However, there were multiple maintenance actions carried out on JDZ that were not certified complete in the aircraft logbook. These included:
- a weld repair to the tail wheel post structure, including fabric replacement and rudder system removal and re‑fitment
- replacement of the original wooden propeller blades with composite blades[3]
- replacement of engine oil and fuel delivery ‘flop tubes’[4]
- replacement of the fuel quantity indicating system
- replacement of the tail wheel
- adjustment of the flying wires during the aircraft ‘flight test phase’.
Pilot maintenance
CASA authorised the holder of a private pilot licence to conduct certain maintenance as specified in CAR Schedule 8 (Schedule 8). In addition, CASA Instrument 33/13 Authorisation of persons to carry out maintenance on certain amateur‑built, kit-built and light sport aircraft with a special certificate of airworthiness detailed that, in some circumstances, a person who builds or has previously built an amateur‑built aircraft of a similar type, may be authorised to conduct certain maintenance and issue a maintenance release for that aircraft.
All maintenance conducted by a pilot under CASA Instrument 33/13 and/or Schedule 8 was required to be certified as per CAR 42ZE.
The occurrence pilot was authorised to conduct maintenance on JDZ as specified in Schedule 8. However, the pilot was not authorised to conduct maintenance on JDZ under Instrument 33/13 as they did not build the aircraft.
It was reported that the pilot replaced the tail wheel of JDZ due to excessive wear and shimmy. This maintenance action was permitted if carried out in accordance with Schedule 8. In addition, it was reported that adjustment of the aircraft flying wires, which was not included in Schedule 8, was carried out by another pilot during the Phase I flight testing period. Neither the tail wheel replacement nor the flying wire adjustments were certified in the aircraft logbook.
Maintenance of amateur-built aircraft
This and other ATSB investigations have identified a degree of uncertainty amongst a number of pilots and engineers regarding the certification of maintenance performed on amateur-built experimental aircraft. When asked, CASA advised that, in accordance with CASA Instrument 33/13, a licenced aircraft maintenance engineer (LAME) is authorised to certify for maintenance of certain amateur‑built, kit‑built and light sport aircraft with a SCOA. This authorisation extends to the scope and privileges of the LAME’s licence. Additionally, a LAME may certify for maintenance ‘for and on behalf of’ a maintenance organisation, if the aircraft undergoing maintenance is within the scope of activities for that organisation.
CASA also advised that other than a number of specific exemptions, amateur-built aircraft are to be maintained in accordance with the regulations and any additional instructions detailed in a SCOA annex. Ultimately, as per CAR 42CB Experimental aircraft, the certificate of registration holder is responsible for ensuring the aircraft is maintained in accordance with the regulations. In addition, CAR 133 Conditions of flight requires the pilot in command to ensure that all the required maintenance has been completed and is appropriately certified.
Weight and balance
An initial weight and balance was carried out on JDZ on 19 October 2006.
The ATSB estimated the aircraft’s weight and balance for the accident flight based on the available data. This indicated that the aircraft was likely operating within limitations at the time and the ATSB concluded that weight and balance was unlikely to be a factor in the loss of control.
Meteorological information
Witnesses described the weather at the time they observed JDZ as being calm with a clear sky.
Weather observations were recorded by an automatic station at the Maitland Visitor’s Centre. Observations for 1500 on 8 July 2015 recorded a temperature of about 15 °C, relative humidity of 60 per cent and a southerly wind at 6 km/h (about 3 kt). This was consistent with the witness observations.
According to the Geoscience Australia website (see www.ga.gov.au/), at about 1630 the sun was at an elevation of 5° above the horizon and an azimuth of 300°.[5] The aircraft that was observed on primary radar, and the ATSB concluded to have been JDZ, was flying in an easterly direction just prior to disappearing from radar at about 1631 (see the section titled Radar and airspace information). The ATSB concluded that it was unlikely sun glare was a factor in the loss of control.
Communications
A review of the recorded Maitland common traffic advisory frequency[6] broadcast data determined that the pilot transmitted a departure call on that frequency at 1609 local time. No further transmissions from JDZ were recorded.
Radar and airspace information
Aircraft transponder equipment
The aircraft logbook indicated that during the assembly, the aircraft was fitted with a Mode C transponder that could be activated by the pilot. There was no subsequent logbook entry in respect of the transponder.
Aeronautical Information Publication Australia[7] EN ROUTE (ENR) 1.1 Section 56 OPERATING REQUIREMENTS FOR TRANSPONDERS, paragraph 56.1 stated that:
Pilots of aircraft fitted with a serviceable Mode 3A or Mode S transponder must activate the transponder at all times during flight, and if the Mode 3A transponder is Mode C capable, that mode must also be operated continuously.
In addition to the potential benefits to air traffic control of the activation of an aircraft’s transponder, aircraft traffic collision avoidance systems[8] rely on transponder information for their traffic alerting and collision avoidance functions.[9] These systems have the potential to enhance crews’ self separation, in particular in uncontrolled airspace.
Analysis of recorded radar data
The primary radar data for the aircraft that was manoeuvring in the area in which the pilot of JDZ was reported to regularly conduct aerobatics showed:
- an unidentified aircraft immediately to the south of Maitland Airport at about 1622
- from immediately south of the airport the aircraft tracked to the vicinity of the Keinbah Quarry
- the aircraft then tracked variously east and west for about 4 minutes
- the primary radar return for the aircraft was lost on two occasions and was reacquired after 23 and 10 seconds respectively
- the primary radar return for the aircraft was lost a third time at about 1631 and was not detected again.
Expert analysis of the aircraft’s radar data as it tracked variously east and west for 4 minutes indicated that the aircraft was manoeuvring consistent with the conduct of aerobatic manoeuvres.
In addition, the recorded flight path of a search aircraft with an operational transponder was also reviewed. The radar data from this aircraft showed that the:
- unidentified aircraft’s last detected location was consistent with the accident site
- primary surveillance radar could detect aircraft in that area down to an altitude of about 200 ft.
The ATSB concluded that, based on the analysis of the primary radar data, and its consistency with the witness observations, the unidentified aircraft was highly likely to have been JDZ. The ATSB could not determine whether the lack of a secondary surveillance radar return for JDZ was a result of the transponder not being activated or the equipment not operating correctly. Of note, secondary surveillance radar returns were observed for other aircraft in the area, indicating that terrain shielding was not a factor.
Airspace
- The Visual Terminal Chart[10] for the area showed that JDZ was operating in uncontrolled, Class G airspace. This airspace, which extended up to an altitude of 8,500 ft, provided ample altitude in which to conduct aerobatic manoeuvres.
Site and wreckage information
Witness information
Witnesses reported that a loud engine noise caught their attention and caused them to look up to see JDZ near the top of what appeared to be a vertical climb. The aircraft was then observed to slide backwards tail first, before entering a flat spin. The flat spin descent was described as slow. Sight of the aircraft was lost behind trees and, shortly after, an explosion was heard by some witnesses.
Table 1 provides a summary of the observations that were unique to each witness. Figure 2 shows the location of each witness with respect to the accident site. Of the witnesses, witness D had flying experience.
Table 1: Summary of specific witness observations
| Witness | Distance from the accident site | Witness-specific observations |
| A | 1.75 km south | Aircraft ‘swooped side to side’ as it slid backwards, before entering an inverted flat spin. |
| B | 2.9 km south | Observed in a nose-down attitude before sight was lost. |
| C | 1.5 km north-west | Heard a loud bang after sight was lost. |
| D | 1.75 km north-north-east | Reported that the engine sounded normal. The witness did not recall hearing the engine cut out or stall. After sight was lost, the witness heard a loud explosion, followed a few minutes later by a second explosion. |
Figure 2: Witness location with reference to the accident site

Source: Google earth, modified by the ATSB
The area was reported to be popular with aerobatic pilots. The witnesses advised that they regularly observed various aerobatic manoeuvres by these aircraft.[11] It was reported that the manoeuvres by the pilot of JDZ were, up to the point where sight was lost, consistent with the regularly-observed aerobatic manoeuvres.
The height of JDZ at the top of the vertical climb was estimated from the witness observations. While it could be expected that the accuracy of this estimation was affected by the witness’ limited visual references, observations from the three closest witnesses to the accident site suggested that the height of the aircraft at the top of the vertical climb was less than 2,000 ft above ground level.
Wreckage information
The accident site was about 8 km south-west of Maitland Airport and was located in thick bushland near the Hunter Expressway. Examination of the site and wreckage determined that immediately before colliding with terrain, the aircraft was inverted, slightly nose-down and in an almost vertical descent. An initial fuel-fed post-impact fire was followed by an intense oil-fed fire, which in combination destroyed most of the aircraft.
The aircraft structure was severely damaged by impact forces and the post-impact fire, limiting the evidence available and conclusions that could be drawn from an examination of the wreckage. However, that examination determined that:
- all components of the aircraft were located at the impact site
- there were no pre-accident defects with the aircraft and engine
- the cockpit canopy frame was consistent with it being in the closed position at the time of impact
- damage to the aircraft’s tubular structure was consistent with impact with trees and/or terrain
- what remained of the wooden wing spars showed little damage, consistent with little forward speed just prior to the impact with terrain
- the engine was partly submerged in the soft earth, at an angle of about 23° to the horizon
- continuity of engine controls was confirmed; however, the rest of the engine and its accessories were extensively damaged, or destroyed by the fire, preventing further assessment
- one propeller blade was torn from the hub and was wedged between the engine and the ground. The other blade was undamaged and had stopped in a vertical position. The positions of the propeller blades indicated that the engine rotated no more than a quarter turn following the impact with terrain.
Flight controls
The flight control system and cables were examined as far as possible. With the exception of the elevator control tube and hinge bolt, continuity of the flight controls was established on-site. A number of elevator and tail structure components were recovered for subsequent technical examination at the ATSB’s technical facilities in Canberra, Australian Capital Territory.
Technical examination of the recovered components determined that the fractures of the control tube and hinge bolt were consistent with overstress. No pre‑existing defects were identified and the failures were likely the result of impact with trees and/or terrain.
Seat harness and buckles
The webbing of both seat harnesses was almost entirely destroyed in the post-impact fire. Despite this level of damage, various buckles and harness adjust mechanisms were identified. Of these, one five-point harness buckle and one lap-belt harness buckle were found in the secured, or closed position. The other buckles were found unsecured (Figure 3). Refer to the section Test and research for more detail.
Figure 3: As-found five-point and lap-belt harness buckles. Of these four buckle sets, one of each type was secured (see the lower left and right images below)
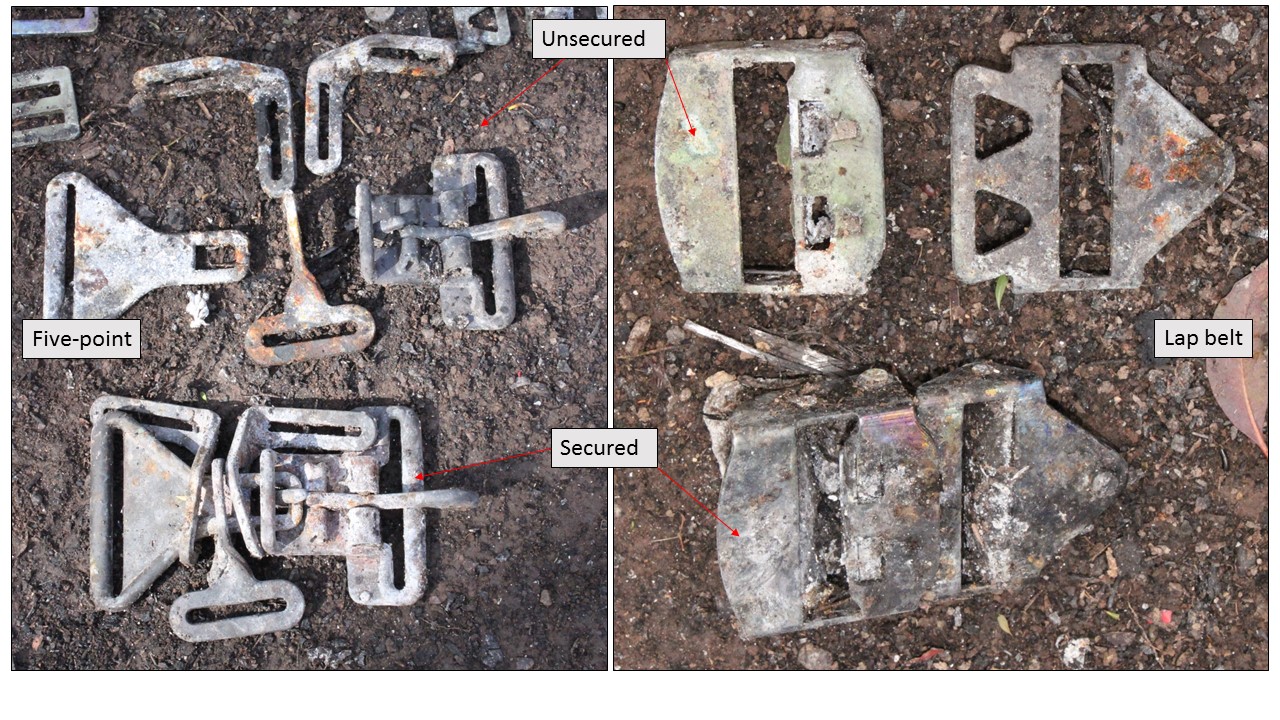
Source: ATSB
Medical and pathological information
Post-mortem examination
The post-mortem examination identified that the pilot was fatally injured as a result of multiple injuries, consistent with an aircraft accident, and was deceased at the time of the post‑impact fire. The examination also identified significant coronary artery disease. Toxicology results were negative for alcohol and commonly-tested drugs.
Medical information
CASA records showed that the pilot had been monitored for borderline high blood pressure (hypertension) by the same Designated Aviation Medical Examiner (DAME) since January 2007. In this regard, the pilot had been taking anti-hypertensive medication as prescribed by his general practitioner (GP) since August 2012.This medication was permissible in accordance with the International Civil Aviation Organization Manual of Civil Aviation Medicine and was reportedly effective in maintaining the pilot’s blood pressure within prescribed limits.
The DAME and the GP advised that the pilot had not reported any side effects to the medication.
It was reported that the pilot also regularly took various herbal tonics that were dispensed by a naturopath. Additionally, the pilot was reported to use over-the-counter herbal supplements for relief from allergies, sinusitis and colds. The pilot did not report the use of these herbal supplements to their GP or DAME.
Civil Aviation Safety Regulations 1998 (CASR) 67.155 stated the criteria for medical standards for the holder of a private pilot licence. In particular, item 2.3 of the regulation required a pilot to not use:
…any over-the-counter or prescribed medication or drug (including medication or a drug used to treat a disease or medical disorder) that causes the person to experience any side effects likely to affect the person to an extent that is safety-relevant
As part of the initial issue and/or renewal of a medical certificate, any prescribed or over‑the‑counter medications taken for greater than 2 weeks (including herbal or alternative therapies) are to be documented. A review of the pilot’s CASA medical file showed that the anti‑hypertensive medication was the only medication noted.
The pilot was reported to be active and healthy. The DAME and GP advised they had no indication to suspect the pilot had significant coronary artery disease, as was identified by the post‑mortem examination.
It was reported that the pilot had been suffering from a head cold for at least a week prior to the accident. However, the severity of the symptoms could not be determined. In addition, the pilot had been heavily involved in the Hunter Valley Air Show over the period 4–5 July 2015. Reportedly this included preparations over several weeks, activities over the weekend and assisting with the post-event clean-up.
The pilot was reported to be well rested and in good spirits in the 2 days prior to the accident. There was insufficient evidence to indicate fatigue was a factor in the loss of control.
Nausea during aerobatic flying
It was reported that the pilot was affected by nausea during certain flying activities. Low g Load (g)[12] tolerance and associated airsickness resulted in the pilot’s aerobatic training flights being kept brief or cut short on a number of occasions and with a number of instructors. Certain manoeuvres, such as spinning and negative g, reportedly affected the pilot more significantly than others. In addition, on more than one occasion during an aerobatic training flight, the nausea overwhelmed the pilot to the point where the instructor had to take control of the aircraft.
Civil Aviation Advisory Publication (CAAP) 155-1(0) Aerobatics provided detailed information on many aspects of aerobatics, including the physiological effects of g forces. Section 4.1 stated:
Aerobatic manoeuvres involve rapid changes in speed and direction which impose significant accelerative forces on the aircraft and pilot. The physiological effects of these G forces can range from minor discomfort to loss of consciousness.
Pilots beginning aerobatics may be adversely affected by airsickness, disorientation and discomfort but continued practice, and the use of appropriate methods of mitigating the physiological effects, will allow most pilots to adapt fairly quickly to standard aerobatic manoeuvres.
The CAAP also provided further and more-detailed information on the various g forces and their effects on the body. It described that pilots can build up their tolerance to g forces with practice but need to be aware that established tolerance levels can be significantly reduced by various factors that affect their physical condition. These factors included, but were not limited to, fatigue, illness, medication, low blood pressure and dehydration. In addition, lack of recent aerobatic practice will also reduce a pilot’s g tolerance and pilots returning to aerobatics after some time need to check and then gradually re-establish their tolerance level.
Section 4.20 Disorientation, included the following statement:
Sustained rapid rotation, such is in flick manoeuvres or spins, can also lead to disorientation because visual reference is made difficult due to the rapid rotation and there is no visual correction to the confused signals from the balance mechanism.
Recent ear, nose, throat infections may cause injury or pain, as well as disorientation, during aerobatics.
The pilot’s last recorded aerobatic training flight was 28 May 2015. Training notes for that flight indicated the pilot was unable to recover from a stable inverted spin. The pilot’s reported disorientation and nausea that day led to the decision to end the flight and return to the airfield.
Survival aspects
The pilot was not required to and did not notify a SARTIME,[13] or leave a Flight Note with a responsible person. In addition, consistent with there being no need for the carriage in the aircraft of an ELT,[14] the aircraft was not equipped with a permanent emergency locator transmitter (ELT). It was reported the pilot did carry a portable ELT but, only on extended cross‑country flights.
The pilot’s decision to not nominate a SARTIME or leave a Flight Note and not carry an ELT increased the risk of a delayed emergency response in the event of an accident or incident. However, in this case the accident was not considered survivable due to the magnitude of the impact forces and intensity of the post-impact fire.
Operational information
Low-level flying
The pilot in command must not fly the aircraft over non-built-up or –populous areas at a height lower than 500 ft unless it is within the exemptions detailed in CAR 157 (4) Low flying. Radar data showed JDZ below 200 ft on two occasions during the flight that day. There was no evidence to indicate any requirement, or authorisation for going below 500 ft during the flight.
Flying endorsements
The CASR Dictionary, Part 1 Definitions defined aerobatic manoeuvres as those that involve:
- bank angles that are greater than 60˚; or
- pitch angles that are greater than 45˚, or are otherwise abnormal to the aircraft type; or
- abrupt changes of speed, direction, angle of bank or angle of pitch.
A pilot was required to hold the appropriate aeroplane category and a spinning endorsement before an aerobatic endorsement was issued. In addition, the pilot was required to have received training and shown competency in all the course units mentioned in Part 61 Manual of Standards.[15] That training included performance criteria covering loops, rolls, stall turns, recovery from unusual attitudes and spins. The knowledge requirements included, but were not limited to an understanding of the definitions of negative and positive g and the associated effects on the pilot and the aircraft.
CASR 61.065 prohibited the conduct of any activity for which the licence holder was not authorised. In addition, CASR subpart 61.S stated the requirements for aerobatic endorsements. These included that:
- an initial aerobatic endorsement would authorise the pilot to conduct aerobatic manoeuvres in an aeroplane above 3,000 ft above ground level (AGL)
- subsequent endorsements were necessary for aerobatic activities at lower altitudes.
Aerobatic flying
It was reported by a number of Pitts Model 12 pilots and instructors that:
- loops in a Pitts Model 12 aircraft usually required 1,000 to 1,500 ft to complete
- loops with a vertical consistency of around 1,500 ft would be required by the student to achieve aerobatic training competency
- aerobatic manoeuvres during training were normally commenced at 5,000 ft
- in all cases the loop should be entered and exited at the same altitude.
The height required to recover from a spin varies with pilot competency and experience. Spin recovery within the number of turns normally required for the aircraft type is essential to achieve basic competency. Early identification of the spin and correct control inputs should result in a prompt recovery.
The Pitts Model 12 pilot operating handbook Aerobatic Flight included, in part, that the pilot should:
…
-Do be certain that you have ample altitude for the maneuvers [sic] that you want to perform.
-Do be sure that you are familiar enough with the maneuvers [sic], and the airplane, that a bad recovery will produce no worse result than embarrassment.
-Know the limitation on your PITTS Model 12 and yourself.
In addition, the pilot’s operating handbook identified the procedures for emergency spin recovery as:
- POWER OFF
- REMOVE YOUR HAND FROM THE STICK
- DETERMINE DIRECTION OF SPIN ROTATION
- APPLY FULL OPPOSITE RUDDER
- WHEN ROTATION STOP [sic], RECOVER
Finally, CAAP 155-1(0) Aerobatics provided pilots with:
- information and guidance on safety issues related to aerobatic flight, including in respect of the aircraft, pilot and regulations
- an explanation of spin recovery techniques
- advice on the importance of ensuring sufficient height to recover from an aerobatic manoeuvre by 3,000 ft AGL (or the lower limit of the pilot’s approval). In particular, section 7.3.2 of the CAAP stated:
It is highly probable that the consequence of an error or failure during low-level aerobatics will be fatal to the participants.
Test and research
Unsecured seat harness
CAR 155 (5) Aerobatic manoeuvres required an unoccupied seat harness to be secured by the pilot in command prior to conducting an aerobatic manoeuvre. In addition, CAAP 155‑1 (0) Aerobatics discussed the importance of securing unoccupied seat harnesses to prevent them fouling the controls. The ATSB was advised that this procedure had been demonstrated to the pilot and that the pilot was aware of the associated regulatory requirement.
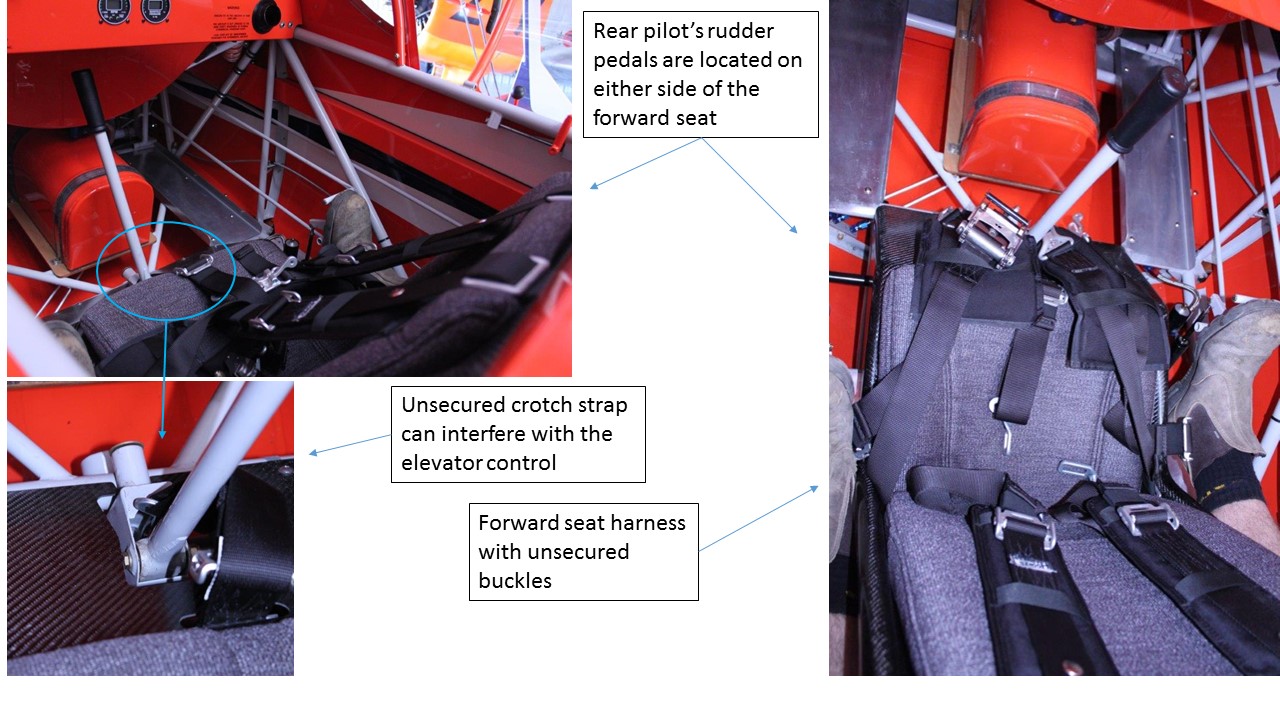
The ATSB determined that the pilot was secured in the rear seat harness and that the unsecured seat buckles were associated with the forward, unoccupied seat (see the previous discussion titled Site and wreckage information). Testing in a Pitts Model 12 aircraft determined that an unsecured forward seat harness had the potential to interfere with the aircraft’s flight controls. Figure 4 shows the orientation of the flight controls with reference to an unsecured forward seat harness.
Refer to appendix A Unsecured seat harness for more information.
Figure 4: Unsecured forward seat harness, showing the potential for the harness to interfere with the flight controls, in particular during aerobatic manoeuvres

Source: ATSB
ATSB research
ATSB research report AR-2007-043(2) Amateur-built aircraft, published 26 March 2013 and available at www.atsb.gov.au concluded the following in relation to amateur-built aircraft accidents:
- Between 1988 and 2010, amateur-built aircraft on the Australian VH-register had an accident rate three times higher than comparable VH-registered factory-built aircraft conducting similar flight operations.
- The fatal and serious injury accident rate was more than five-times higher in amateur-built aircraft than in similar factory-built aircraft.
- Loss of aircraft control led to 25 per cent of all amateur-built accidents, slightly more than for factory-built aircraft accidents. However, the loss of control accident rate was over four times higher. As compared to factory-built aircraft, serious injury was three times more likely after loss of control in amateur-built aircraft accidents.
- Loss of control accidents were more likely to arise from aircraft handling issues where pilots had comparatively lower levels of experience on the aircraft type.
- Loss of control was more likely to occur in the initial climb phase of flight.
- Amateur-built aircraft pilots were significantly more experienced overall than factory-built aircraft accident pilots. However, they were significantly less experienced on the amateur‑aircraft type being flown at the time of the accident when compared to pilots of factory-built aircraft accidents and amateur-built aircraft owners in general. Twenty per cent of amateur-built aircraft accident pilots had less than 10 hours experience on the accident aircraft type.
ATSB research report AR-2008-045 Improving the odds: Trends in fatal and non-fatal accidents in private flying operations, published in June 2010 and also available at www.atsb.gov.au identified that 44 per cent of all accidents and over half of fatal accidents between 1999 and 2008 were attributed to private operations. These figures far surpassed the proportions for any other flying category, even though private operations contributed to less than 15 per cent of the hours flown in that decade. The report also identified that:
- the three most common occurrence types in fatal accidents were collision with terrain, loss of control and wirestrike
- aircraft handling was a significant contributor to loss of control and collision with terrain fatal accidents
- compared with non-fatal accidents, fatal accidents were more likely to be associated with violations of rules and regulations. Violations of rules and regulations remove safety defences and, when coupled with an error, increase the likelihood of an accident.
Previous occurrences
ATSB investigations
The ATSB has investigated a number of fatal accidents involving the conduct of aerobatics. All are available via the ATSB website at www.atsb.gov.au.
199501051 – Collision with terrain involving Pitts S-2A, registered VH-IXY
On 8 April 1995 the pilot was observed practising aerobatic manoeuvres in a Pitts S-2A, registered VH-IXY. The early afternoon flight was observed from the ground by a number of other pilots, including a highly-experienced pilot and flying instructor. This pilot/instructor was in radio contact with the pilot.
The instructor reported a number of unusual manoeuvres by the pilot of VH-IXY and unsuccessful attempts by the instructor to contact the pilot. The aircraft then appeared to stabilise and the pilot responded saying he thought he might have blacked out. The aircraft landed normally and the pilot and instructor discussed g-induced loss of consciousness.
During a later aerobatic flight by the pilot of VH-IXY, after a period of standard aerobatic manoeuvres, the instructor on the ground observed the aircraft pitch up before commencing a continuous roll to the left. The instructor made several unsuccessful attempts to contact the pilot by radio. The nose of the aircraft dropped and the aircraft dived almost vertically into the ground.
The pilot was fatally injured and the aircraft destroyed.
AO-2014-114 - Collision with terrain involving DHC-1 Chipmunk, registered VH-UPD
The ATSB also investigated the collision with terrain involving a DHC-1 Chipmunk, registered VH‑UPD, which occurred near Coffs Harbour, New South Wales on 29 June 2014.The passenger and witness reports indicated that, during an attempted aerobatic manoeuvre, the aircraft entered a spin. The pilot had reportedly received some aerobatic training but had yet to receive an endorsement. Video footage taken by witnesses showed the aircraft established in a slow, upright spin. The on‑site evidence was consistent with the spin continuing until the impact with terrain. The ATSB found it was likely the pilot did not possess the necessary skills and judgement to conduct the manoeuvre safely and consistently.
AO-2014-163 - Collision with terrain involving amateur-built aircraft, registered VH-EGT
On 10 October 2014, the pilot of an amateur-built One Design DR-107 aircraft, registered VH‑EGT, was observed performing a series of low-level aerobatic manoeuvres. Each involved a vertical climb and tumbling manoeuvre followed by a vertical dive and a low altitude recovery. Witnesses reported that, during recovery from the last vertical dive, the aircraft collided with terrain. The aircraft was destroyed by the impact and the pilot was fatally injured.
There was insufficient evidence to determine why the recovery was not accomplished above the pilot’s minimum‑authorised aerobatics height. The accident highlighted the risks inherent in performing low-level aerobatics and the ATSB encouraged pilots to always maintain minimum approved heights above the ground when performing aerobatics.
United States National Transport Safety Bureau investigations
A review of the United States National Transportation Safety Board (NTSB) Aviation Accident Database identified two accidents involving Pitts Model 12 aircraft losses of control and one regarding possible pilot impairment that showed similar traits to the ATSB’s investigation of the accident involving JDZ. Below is a brief summary of the NTSB’s investigation reports into these accidents (available at NTSB website).
Loss of control accidents
NTSB investigation report MIA00LA149 involved a collision with terrain of a Pitts Model 12 on 9 May 2000, with both occupants fatally injured. It was reported the pilot had been flying in formation, but discontinued the return flight to practice aerobatics. Examination of the wreckage showed extensive damage consistent with the aircraft impacting the hard ground inverted, in about a 20°–25°nose‑low attitude. The NTSB determined the ‘probable cause’ of the accident as ‘the pilot’s loss of control in flight for undetermined reasons’.
NTSB investigation report ANC05LA033 found that a Pitts Model 12 collided with terrain while the pilot was performing low‑altitude aerobatic manoeuvres on 12 February 2005. Site and wreckage examination concluded that all damage was consistent with the aircraft impacting the ground in a near-vertical descent. The NTSB determined the ‘probable cause’ of the accident as:
The pilot’s failure to maintain control of the airplane while performing a low altitude, aerobatic maneuver [sic], which resulted in an uncontrolled descent, and an in-flight collision with terrain. A factor associated with the accident was the initiation of a low altitude aerobatic manoeuvre.
Pilot impairment
NTSB investigation report CEN11LA582 found that ‘the pilot’s impairment during an aerobatic airshow performance for reasons that could not be determined…resulted in an in-flight loss of airplane control’. The report identified the pilot had previously sought treatment for vertigo and nausea suffered while conducting aerobatics.
United Kingdom Air Accidents Investigation Branch investigation
The United Kingdom Air Accidents Investigation Branch[16] published investigation report EW/G2009/05/11 regarding a collision with terrain involving a Pitts S-12 that occurred on 14 May 2009. The pilot was the sole occupant and received serious injuries. The report ‘emphasised the importance of entering a manoeuvre at a height from which recovery was possible in the event of failure to complete it as planned’. Additionally the report referred to the summary of British Aerobatic Association Safety Sense Leaflet 19 Aerobatics, which stated:
…start with sufficient height to give plenty of margin if things go wrong
__________
- Replacement of the blades was entered in the aircraft logbook, but the entry did not include the associated release and traceability documentation required by CAR Schedule 6. In addition, the registration details and logbook statement had yet to be updated with the new propeller information.
- A flop tube is a flexible hose with a weighted end. The weight ensures the hose draw point remains submerged in the respective fluid whether the aircraft is in normal or inverted flight.
- The clockwise horizontal component of the sun’s or moon’s position from true north, measured in degrees.
- Common Traffic Advisory Frequency is the frequency on which pilots operating at a non-towered aerodrome should make positional radio broadcasts.
- A package of documents that provides the operational information necessary for the safe and efficient conduct of national (civil) and international air navigation throughout Australia and its Territories.
- An aircraft collision avoidance system that monitors the airspace around an aircraft for other aircraft equipped with a corresponding active transponder and gives warning of possible collision risks.
- AIP ENR 1.6 Section 7.1 Operation of SSR Transponders, paragraph 7.1.2.
- Visual Terminal Charts provide aeronautical and topographical information for operations under the Visual Flight Rules in the vicinity of major aerodromes. They also show controlled airspace.
- Witness simulations of their observations with an aircraft model were consistent, even when unsure of the correct manoeuvre terminology.
- g Load is the nominal value for acceleration. In flight, g load values represent the combined effects of flight manoeuvring loads and turbulence. This can be a positive or negative value.
- The time nominated by a pilot for the initiation of search and rescue action if a report has not been received by the nominated unit.
- Crash-activated radio beacon that transmits an emergency signal that may include the position of a crashed aircraft. Also able to be manually activated.
- The purpose of Part 61 Manual of Standards Instrument 2014 is to set out the standards relating to flight crew licensing.
- AAIB reports can be viewed via https://www.gov.uk/government/organisations/air-accidents-investigation-branch.
Background
The private flight in a Pitts Model 12, registered VH-JDZ (JDZ), was conducted in favourable weather conditions but ended in a collision with terrain, fatally injuring the pilot. The witness observations were consistent with the aircraft exiting a vertical manoeuvre in an uncontrolled state, with insufficient height for recovery before impacting terrain. Wreckage and accident site examination indicated that the aircraft collided with terrain inverted, slightly nose-down and with little or no forward speed.
Given the extent of the impact damage and intensity and effect of the post-impact fire, there was no evidence that any mechanical failure or aircraft unserviceability contributed to the development of the accident. In addition, the surrounding area contained cleared and open paddocks, which could have been used for a precautionary or emergency landing had that been required.
This analysis will consider the circumstances that preceded the loss of control.
Unauthorised flight manoeuvres
The pilot was appropriately licenced to fly JDZ solo and had been encouraged to fly the aircraft solo and with an instructor to increase familiarity and gain experience on type. The pilot did not hold the required authorisation to conduct aerobatic manoeuvres or fly at low altitude. The pilot’s instructors advised the pilot to not conduct solo aerobatic manoeuvres. However, radar surveillance data and witness reports were consistent with the pilot conducting aerobatic manoeuvres in the minutes preceding the impact with terrain. This included flight below 200 ft above ground level.
The pilot’s decision to conduct the aerobatic manoeuvres solo, and without authorisation, increased the risk of unintended departure from controlled flight. In addition, the pilot’s conduct of those manoeuvres at low altitude reduced the height, and therefore the time available in which to recover control of the aircraft should it depart from controlled flight.
The observed vertical manoeuvre, followed by the reported horizontal flat spin is consistent with a loss of control. The reason for the loss of control could not be determined.
Flight control fouling
The forward seat harness buckles were found unsecured during the wreckage examination. The post-impact fire hindered the ATSB’s ability to determine if the harness had been secured in a non-standard manner prior to the flight, increasing the risk that they might unbuckle. In addition, although unlikely, the possibility that if buckled correctly the buckles may have come undone as a consequence of the impact sequence could not be discounted. Despite these possibilities, the ATSB concluded that the as-found insecurity of the front seat harness buckles suggested that they were not secured correctly as part of the standard pre-flight preparation for solo flight.
Unsecured harnesses have the potential to interfere with the flight controls, in particular during aerobatic flight. The cockpit layout would have inhibited the pilot’s ability to clear such an interference in flight. Any interference could result in an unintended manoeuvre or inhibit the pilot’s ability to recover from a manoeuvre, whether the manoeuvre was intended or unintended.
While flight control fouling remains a possibility, there was insufficient evidence to determine if it was a contributor to the accident.
Pilot incapacitation and non-reporting of medication
Pilot incapacitation can impair a pilot’s performance to the extent that safe operation of the aircraft is adversely affected. It can be due to the effects of a medical condition or a physiological impairment and represents a potential threat to flight safety. It can have either a long- or short‑term effect on the pilot.
The pilot’s post-mortem examination indicated that the pilot had coronary artery disease that could have resulted in a permanent incapacitation event. In addition, reports of other flights indicated the pilot suffered from temporary incapacitation as a result of nausea caused by the onset of g forces. Further, the use of non-prescribed medical or herbal supplements or the effects of a cold or virus can increase the risk of pilot incapacitation. The conduct of aerobatic manoeuvres can exacerbate the effects of a number of these conditions and non‑prescribed ‘treatments’.
All of these factors were present during this occurrence and pilot incapacitation could have preceded the loss of control or influenced any recovery. However, while an incapacitating event remained a possibility, there was insufficient evidence to conclude probable contribution to this accident.
Many documents highlight the risks involved with various medications and their possible effects on pilot performance and flight safety. The Designated Aviation Medical Examiner reported being unaware of all medications and supplements reported taken by the pilot. Therefore, the medical examiner was unable to determine any possible interactions between the prescribed anti‑hypertensives and/or the non‑prescribed medication and herbal supplements. This removed a potential protection against the risk of pilot incapacitation as a result of those medicines and supplements.
Maintenance
The ATSB found that uncertified maintenance was conducted on JDZ by authorised and unauthorised persons. The registered operator is responsible for the airworthiness and maintenance control of the aircraft to ensure its safe operation. Additionally, the pilot in command must not commence a flight unless all required maintenance has been completed and certified.
This and other ATSB investigations have reiterated the importance of adhering to the regulations as they apply to aircraft maintenance and operation. However, there is evidence that some in the industry are unsure of, or are misinterpreting a number of the regulations concerning the operation and maintenance of amateur-built experimental aircraft. Authorised aircraft maintenance is mandated to assure a level of safety for aircraft operations. Unauthorised maintenance increases the risk of mechanical failure, in turn reducing the level of safety and increasing the risk of injury or death.
From the evidence available, the following findings are made with respect to the collision with terrain involving a Pitts Model 12, registered VH-JDZ, which occurred about 8 km south-west of Maitland Airport, New South Wales on 8 July 2015. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
- Control of the aircraft was lost during a vertical manoeuvre that was likely entered at an altitude lower than that required and the aircraft was not recovered before impact with terrain.
Other factors that increased risk
- The pilot conducted low-level flight and aerobatic manoeuvres despite not holding the appropriate authorisations, significantly increasing the risk of an accident.
- The pilot used non-prescribed medication and herbal supplements without informing their doctor and Designated Aviation Medical Examiner, removing a protection against pilot incapacitation.
- Uncertified and unauthorised maintenance was carried out on VH-JDZ, which increased the risk that a technical issue would affect the safety of the aircraft and those on board.
- Industry interpretation of the regulations regarding the maintenance of amateur-built experimental aircraft was varied, increasing risk associated with the maintenance of those aircraft.
Other findings
- The front seat buckles were found unsecured and, although unable to be determined if they were not secured correctly as part of the standard pre-flight preparation for solo flight, or they may have undone as a consequence of the impact sequence, any insecurity during aerobatic manoeuvres has implications for flight control fouling.
Sources of information
The sources of information during the investigation included the:
- Civil Aviation Safety Authority
- New South Wales Police and Coroner
- Department of Defence
- Airservices Australia
- Bureau of Meteorology
- a number of flight instructors and Pitts Model 12 pilots
- aircraft kit manufacturer and builder
- maintainers of VH-JDZ.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Civil Aviation Safety Authority, the United States National Transportation Safety Board, the aircraft kit manufacturer, a number of flight instructors, the Department of Defence and Airservices Australia.
No submissions were received from those parties.
Appendix A – Unsecured seat harness
Examination of seat harness components
The aircraft was fitted with two seats to accommodate a passenger forward and the pilot aft. Both seats had a five‑point harness and a lap-belt harness. The dual harness arrangement is typical for aerobatic aircraft. The five-point and lap-belt harnesses are secured to separate airframe attachment points. In addition, the buckles of each harness type operate in opposite directions to minimise the risk of accidental release. It was reported that VH-JDZ had the same type of harness in the forward and rear seats.
The various secured and unsecured harness buckles located on site were retained for further examination.
Forward five-point harness
The lever mechanism of the unsecured forward five-point buckle was observed to be in the closed position; however, it could not be determined if this lever was in the closed position during flight or as a result of the impact with terrain. It was noted, however, that all five buckle components were separate from each other, consistent with the buckle assembly not being secured or closed. Visual examination of the unsecured five-point buckle components did not identify any deformation or damage. In addition, when tested, the buckle mechanism was capable of operation and security.
Rear harness
The rear pilot shoulder harness restraint cable that connected it to the airframe structure had fractured in overload. The tubular structure to which the rear pilot crotch strap was secured had fractured at each end of the tube, where it is welded to the airframe structure. In addition, components of the ‘secured’ rear five-point harness buckle showed signs of deformation (Figure A1).
Figure A1: Deformation to rear seat buckle in comparison with the forward buckle, and fracture of rear seat crotch strap hard point

Source: ATSB
Conclusion
Damage to the airframe and the severed harness cable at the rear pilot position was consistent with the pilot being secured in the seat at the point of impact. Therefore, the open buckles of the five point harness and lap belt were associated with the unoccupied, forward passenger seat.
Unsecured harness testing
Civil Aviation Regulation 155 (5) Aerobatic manoeuvres required an unoccupied seat harness to be secured by the pilot in command prior to conducting an aerobatic manoeuvre. In addition, Civil Aviation Advisory Publication 155‑1 (0) Aerobatics indicates that unoccupied seats should have their harnesses secured to prevent them fouling the controls.
In the Pitts Model 12 the harnesses can be secured by connecting the buckles, pulling the adjustment straps tight, wrapping the adjusting lengths round the bundle and tucking in the loose ends. The ATSB was advised that this procedure was demonstrated to the pilot and that the pilot was aware of the need to secure the seat harnesses.
The ATSB conducted testing in a Pitts Model 12 aircraft to ascertain if unsecured forward seat harness components had the potential to interfere with the aircraft’s flight controls.
The rear pilot’s rudder pedals are positioned on either side of the forward seat base. A loose lap strap and associated buckle, from either the forward seat lap belt or five-point harness, were found to have the potential to interfere with rudder pedal operation. In addition, a buckle component could lodge between the rudder pedal and the diagonal tubular bracing of the airframe (Figure A2).
Figure A2: Possible rudder pedal interference from an unsecured forward seat harness
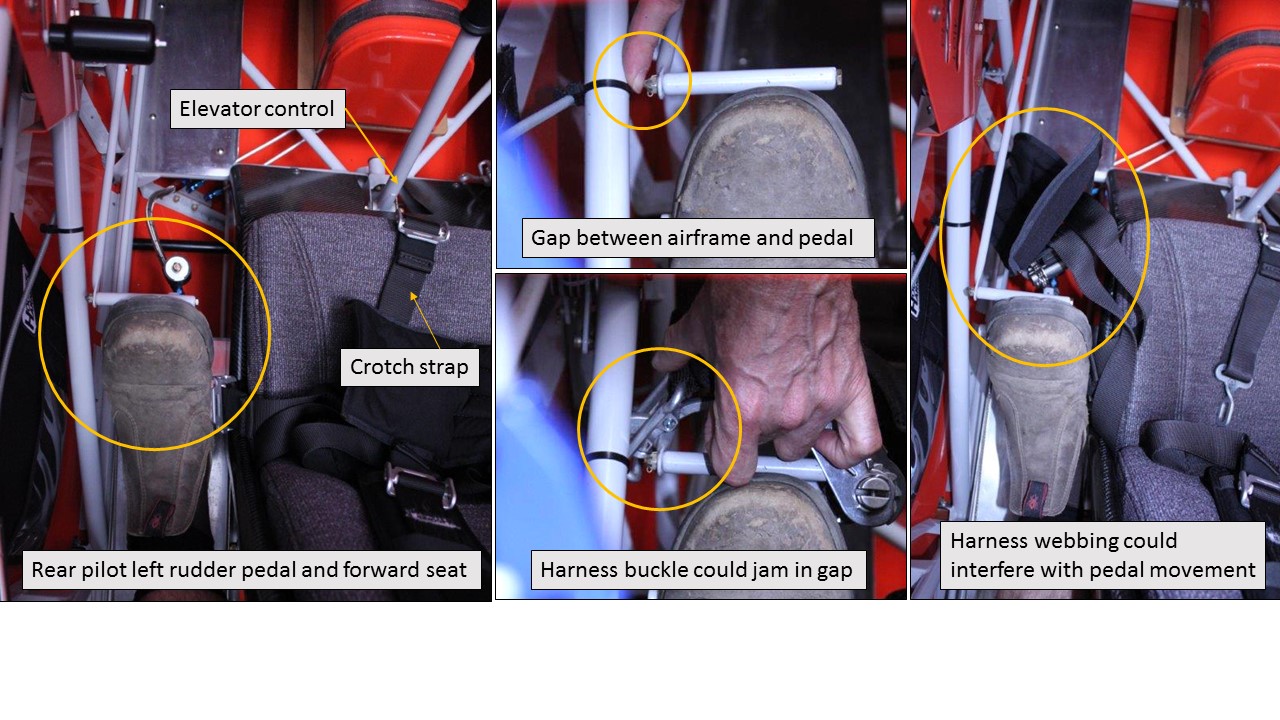
Source: ATSB
Access to the rudder pedals from the rear seat was limited and it would be very difficult to release a misplaced front seatbelt by hand. Also, due to the design of the rudder control system, rearward movement of one rudder pedal does not naturally impart a forward movement of the opposite pedal.[17] Therefore, the cockpit layout and rudder design may inhibit the pilot’s ability to free an obstructed rudder pedal in flight.
It was also noted that it was possible for the forward seat crotch strap and associated buckle to interfere with the forward seat elevator control stick (Figure A3). It would not be possible for a rear‑seat pilot to remove this obstruction by hand during flight operations.
Figure A3: Possible elevator control interference from an unsecured forward seat harness
Source: ATSB
__________
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2016
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |