Safety summary
What happened
On 30 May 2017, a twin‑engine Cessna 441 Conquest II (Cessna 441), registered VH-XMJ and operated by AE Charter (trading as Rossair) departed Adelaide Airport, South Australia for a return flight via Renmark Airport, South Australia.
On board the aircraft were:
- an inductee pilot undergoing a proficiency check, flying from the front left control seat
- the chief pilot conducting the proficiency check, and under assessment for the company training and checking role for Cessna 441 aircraft, seated in the front right control seat
- a Civil Aviation Safety Authority (CASA) flying operations inspector, observing and assessing the flight from the first passenger seat directly behind the inductee pilot.
Each pilot was qualified to operate the aircraft.
The flight departed Adelaide at about 1524 local time and flew to the Renmark area for exercises related to the check flight, followed by a landing at Renmark Airport. After a short period of time running on the ground, the aircraft departed from runway 25 at about 1614.
A distress beacon broadcast was subsequently received by the Joint Rescue Coordination Centre and passed on to air traffic services at 1625. Following an air and ground search the aircraft was located by a ground party at 1856 about 4 km west of Renmark Airport. All on board were fatally injured and the aircraft was destroyed.
What the ATSB found
The ATSB determined that, following a simulated failure of one of the aircraft’s engines at about 400 ft above the ground during the take‑off from Renmark, the aircraft did not achieve the expected single engine climb performance or target airspeed. As there were no technical defects identified, it is likely that the reduced aircraft performance was due to the method of simulating the engine failure, pilot control inputs or a combination of both.
It was also identified that normal power on both engines was not restored when the expected single engine performance and target airspeed were not attained. That was probably because the degraded aircraft performance, or the associated risk, were not recognised by the pilots occupying the control seats. Consequently, about 40 seconds after initiation of the simulated engine failure, the aircraft experienced an asymmetric loss of control.
The single engine failure after take‑off exercise was conducted at a significantly lower height above the ground than the 5,000 ft recommended in the Cessna 441 pilot’s operating handbook. This meant that there was insufficient height to recover from the loss of control before the aircraft impacted the ground.
While not necessarily contributory to the accident, the ATSB also identified that:
- The operator’s training and checking manual procedure for simulating an engine failure in a turboprop aircraft was inappropriate and increased the risk of asymmetric control loss.
- The CASA flying operations inspector was not in a control seat and was unable to share the headset system used by the inductee and chief pilot. Therefore, despite having significant experience in Cessna 441 operations, he had reduced ability to actively monitor the flight and communicate any identified problem.
- The inductee and chief pilot, while compliant with recency requirements, had limited recent experience in the Cessna 441 and that probably led to a degradation in the skills required to safely perform and monitor the simulated engine failure exercise.
- The chief pilot and other key operational managers within Rossair were experiencing high levels of workload and pressure during the months leading up to the accident.
- The Civil Aviation Safety Authority’s method of oversighting Rossair in the several years prior to the accident increased the risk that organisational issues would not be identified and addressed.
Finally, a lack of recorded data from this aircraft reduced the available evidence about pilot handling aspects and cockpit communications. This limited the extent to which potential factors contributing to the accident could be analysed.
What's been done as a result
Following the accident, CASA issued a temporary management instruction to provide higher risk protection around operations involving CASA flying operations inspectors. However, at the time of writing these instructions had not been permanently incorporated into regulation.
Safety message
Conducting a simulated engine failure after an actual take-off is a high-risk exercise with little margin for error. For that reason, Cessna recommended practicing this sequence in the 441 aircraft at a height of 5,000 ft above ground level to allow the opportunity for recovery in the event that control is lost.
A review of past accidents indicates that, while accidents associated with engine malfunctions are rare, training to manage one engine inoperative flight (OEI) after take‑off is important. The ATSB recommends that such training should follow the manufacturer’s guidance and, if possible, be conducted in an aircraft simulator. If the sequence is conducted in the aircraft close to the ground, then effective risk controls need to be in place to prevent a loss of control as recovery at low height will probably not be possible. Such defences include:
- defined OEI performance criteria that, if not met, require immediate restoration of normal power
- use of the appropriate handling techniques to correctly simulate the engine failure and ensure that aircraft drag is minimised/OEI performance is maximised
- ensuring that the involved pilots have the appropriate recency and skill to conduct the exercise and that any detrimental external factors, such as high workload or pressure, are minimised.
What happened
On 30 May 2017, a Cessna 441 Conquest II (Cessna 441), registered VH-XMJ (XMJ) and operated by AE Charter, trading as Rossair, departed Adelaide Airport, South Australia for a return flight via Renmark Airport, South Australia.
On board the aircraft were:
- an inductee pilot undergoing a proficiency check, flying from the front left control seat
- the chief pilot conducting the proficiency check, and under assessment for the company training and checking role for Cessna 441 aircraft, seated in the front right control seat
- a Civil Aviation Safety Authority flying operations inspector (FOI), observing and assessing the flight from the first passenger seat directly behind the left hand pilot seat.
Each pilot was qualified to operate the aircraft.
There were two purposes for the flight. The primary purpose was for the FOI to observe the chief pilot conducting an operational proficiency check (OPC), for the purposes of issuing him with a check pilot approval on the company’s Cessna 441 aircraft. The second purpose was for the inductee pilot, who had worked for Rossair previously, to complete an OPC as part of his return to line operations for the company.
The three pilots reportedly started their pre‑flight briefing at around 1300 Central Standard Time.[1] There were two parts of the briefing – the FOI’s briefing to the chief pilot, and the chief pilot’s briefing to the inductee pilot. As the FOI was not occupying a control seat, he was monitoring and assessing the performance of the chief pilot in the conduct of the OPC.
There were two distinct exercises listed for the flight (see the section titled Check flight sequences). Flight exercise 1 detailed that the inductee pilot was to conduct an instrument departure from Adelaide Airport, holding pattern and single engine RNAV[2] approach, go around and landing at Renmark Airport. Flight exercise 2 included a normal take‑off from Renmark Airport, simulated engine failure after take-off, and a two engine instrument approach on return to Adelaide.
The aircraft departed from Adelaide at 1524, climbed to an altitude about 17,000 ft above mean sea level, and was cleared by air traffic control (ATC) to track to waypoint RENWB, which was the commencement of the Renmark runway 07[3] RNAV-Z GNSS approach. The pilot of XMJ was then cleared to descend, and notified ATC that they intended to carry out airwork in the Renmark area. The pilot further advised that they would call ATC again on the completion of the airwork, or at the latest by 1615. No further transmissions from XMJ were recorded on the area frequency and the aircraft left surveillance coverage as it descended towards waypoint RENWB.
The common traffic advisory frequency used for air-to-air communications in the vicinity of Renmark Airport recorded several further transmissions from XMJ as the crew conducted practice holding patterns, and a practice runway 07 RNAV GNSS approach. Voice analysis confirmed that the inductee pilot made the radio transmissions, as expected for the check flight. At the completion of the approach, the aircraft circled for the opposite runway and landed on runway 25, before backtracking and lining up for departure. That sequence varied from the planned exercise in that no single-engine go-around was conducted prior to landing at Renmark.
At 1614, the common traffic advisory frequency recorded a transmission from the pilot of XMJ stating that they would shortly depart Renmark using runway 25 to conduct further airwork in the circuit area of the runway. A witness at the airport reported that, prior to the take‑off roll, the aircraft was briefly held stationary in the lined‑up position with the engines operating at significant power. The take-off roll was described as normal however, and the witness looked away before the aircraft became airborne.
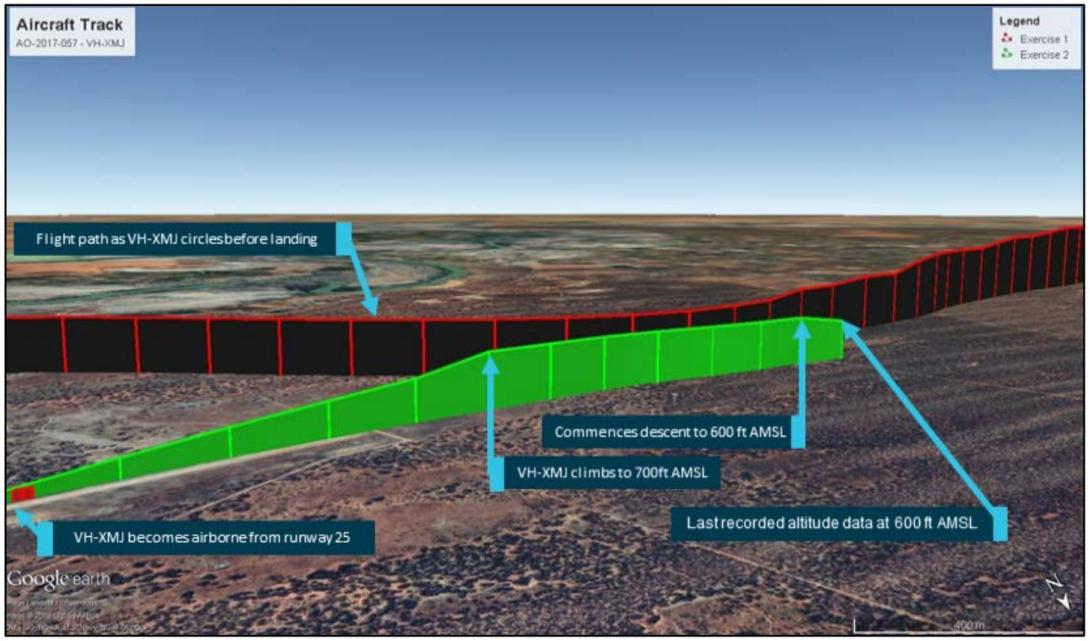
The aircraft maintained the runway heading until reaching a height of between 300‑400 ft above the ground (see the section titled Recorded flight data). At that point the aircraft began veering to the right of the extended runway centreline (Figures 1 and 15). The aircraft continued to climb to about 600 ft above the ground (700 ft altitude), and held this height for about 30 seconds, followed by a descent to about 500 ft (Figures 2 and 13). The information ceased 5 seconds later, which was about 60 seconds after take-off.
Figure 1: Position information of VH-XMJ as the aircraft circled and landed on runway 25 (depicted in red), before backtracking and departing (depicted in green).
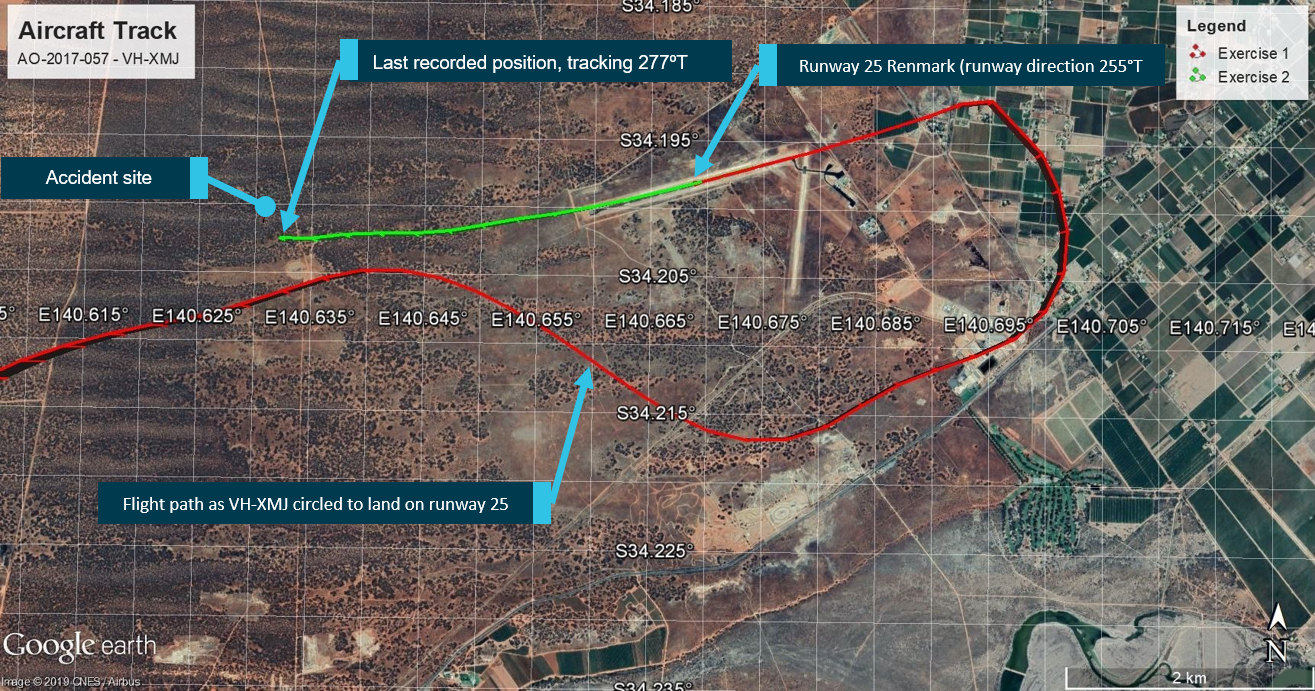
Source: Google and OzRunways, annotated by the ATSB
Figure 2: Altitude information of VH-XMJ (each vertical line represents 5 seconds)
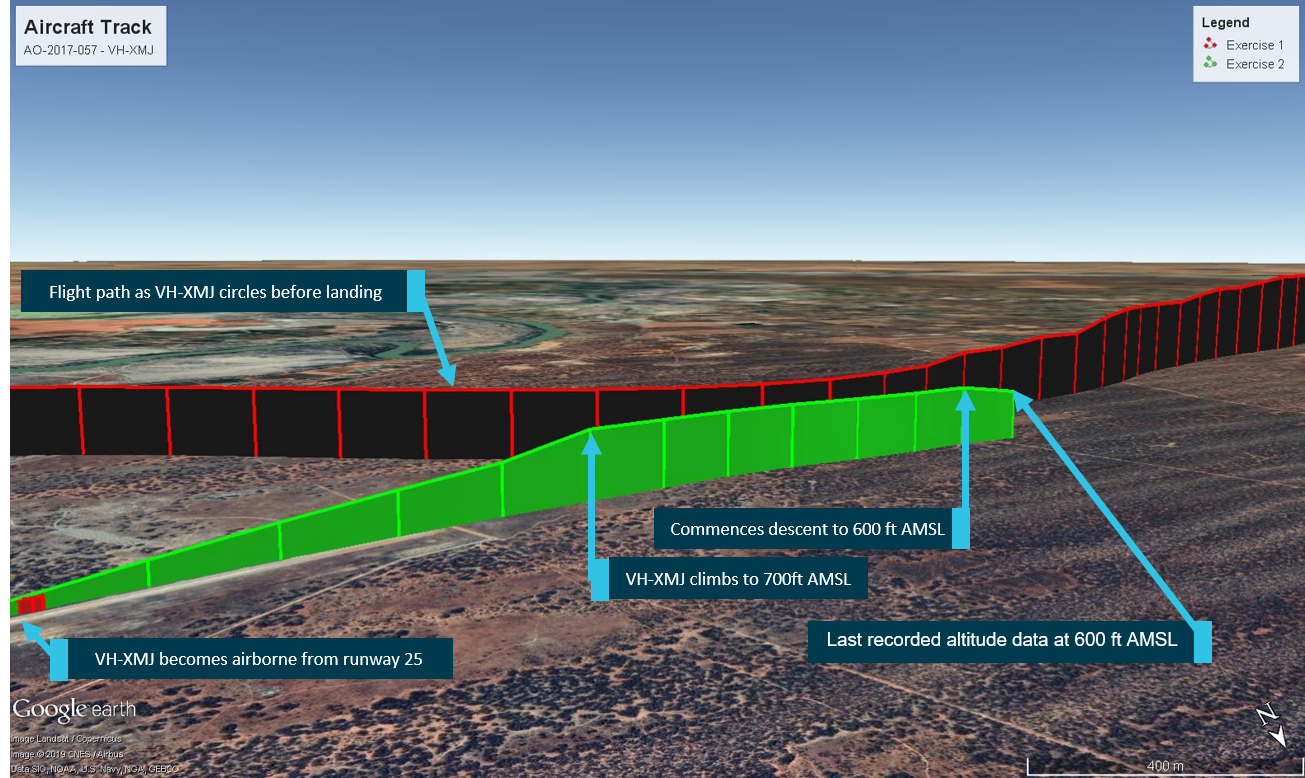
Source: Google and OzRunways, annotated by the ATSB
A distress beacon broadcast was received by the Joint Rescue Coordination Centre and passed on to ATC at 1625. Following an air and ground search the aircraft was located by a ground party at 1856 about 4 km west of Renmark Airport. All on board were fatally injured and the aircraft was destroyed.
__________
- Central Standard Time (CST): Coordinated Universal Time (UTC) + 9.5 hours.
- An RNAV approach is a method of navigation utilising GPS that enables a pilot to guide his aircraft to a landing in low visibility situations. It is often practiced during check flights to ensure proficiency.
- Runway number: the number represents the magnetic heading of the runway.
Pilot information
There were three pilots on board VH-XMJ (XMJ). A summary of the role of each pilot, and their relevant training, qualifications and experience is provided below. The intention of the flight was to allow a Civil Aviation Safety Authority (CASA) flying operations inspector (FOI) to observe the Rossair chief pilot conduct an operator proficiency check (OPC), for the purposes of issuing him with a Conquest II (Cessna 441) check pilot approval (see the section titled Check pilot training). The pilot undertaking the OPC was being inducted into the company. The inductee pilot was seated in the left-hand control seat, the chief pilot in the right-hand control seat, and the CASA FOI in the first row passenger seat behind the left-hand seat pilot.
Inductee pilot
Flight role
The inductee pilot was the planned pilot flying. He was an experienced Cessna 441 pilot who had previously flown for Rossair from May 2010 to August 2014. Undertaking the OPC was part of his induction back into the company.
Qualifications and experience
The inductee pilot held an Air Transport Pilot (Aeroplane) Licence (ATPL), issued in December 1991, and Commercial Pilot (Aeroplane) Licence (CPL) issued in January 1979. He also held an ATPL from the Netherlands. He held a current class 1 aviation medical certificate (valid to 24 June 2017), which required reading correction to be available when flying, but placed no other restrictions on operation.
The pilot’s logbook showed a total flying experience of 14,751.1 hours, with 3,293.7 hours on single engine aircraft and 11,427.4 hours on a range of type-rated and class-rated multi-engine aircraft (see the section titled Pilot licencing). This included 987.7 hours on Cessna 441 aircraft. With the exception of the accident flight and an associated practice flight the week before, all of the inductee pilot’s Cessna 441 experience was gained prior to August 2014.
A review of the pilot’s licence and associated documentation identified that he held the relevant endorsements and ratings to fly the Cessna 441. In addition, he held a current grade 1 instructor rating for multi‑engine class rating training.
In the previous 90 days, the inductee pilot had logged 22.2 hours flying as pilot in command, all on multi-engine class rated aircraft, including 3.5 hours in XMJ the week prior to the accident.
Proficiency checks and flight reviews
The inductee pilot last completed an instrument rating proficiency check (IPC) during his multi‑engine class aircraft flight review in a Beechcraft Baron 95-B55 on 13 February 2017. This check required the pilot to demonstrate conducting a one-engine inoperative instrument departure, which was marked on his proficiency check form as completed satisfactorily. His IPC was valid at the time of the accident.
Chief pilot
Flight role
The pilot in the right-hand seat was appointed as the Rossair chief pilot in January 2016. On this flight, the chief pilot was being observed by the CASA FOI in order to assess his competence to perform operational proficiency checks on Rossair Cessna 441 pilots.
In accordance with the Rossair operations manual, as this was a checking flight, the chief pilot, in the check captain role, was the pilot in command (PIC) for the flight.
Based on the planned exercises for the flight the chief pilot’s role was to observe and monitor the inductee pilot’s proficiency. In addition, he was responsible for setting the power controls to simulate asymmetric flights when required and recover the aircraft if it deviated from safe flight.
Qualifications and experience
The chief pilot held an ATPL (Aeroplane), issued in June 2001, a CPL (Aeroplane) issued in August 1998, as well as an ATPL (Helicopter) issued in November 2013, and a CPL (Helicopter) issued in April 2007. He also held an ATPL (Aeroplane) from the United States of America. The pilot held a current class 1 aviation medical certificate, valid until 3 August 2017, which required reading correction to be available while flying, but placed no other restrictions on operation.
The chief pilot’s logbook history was sought by the ATSB, but the complete record could not be located. A review of available records for the pilot indicated the pilot had around 5,000 hours experience operating aeroplanes, including over 3,200 hours of turbine‑powered aeroplane experience. This included over 1,000 hours on a Cessna 441 aircraft, accumulated during the period between September 2001 and September 2004 and since March 2016. The pilot also had around 1,300 hours experience operating helicopters.
The pilot’s licence showed that the chief pilot held the ratings and endorsements required for the flight, as well as for operation of the company Embraer EMB 120 (EMB 120) aircraft. Additionally, he had previously held a grade 2 instructor rating for aeroplanes with night visual flight rules, design features (for example, retractable undercarriage and manual propeller pitch control), and single engine aircraft class rating endorsements.
In the previous 90 days, flight and duty records for the chief pilot recorded 128.1 hours of flight time, including 99.6 hours as a captain on the EMB 120 aircraft, and 16.6 hours in the Cessna 441, including a previous flight with the inductee pilot on 22 May 2017. The pilot’s flight and duty records had not been updated since 12 May 2017, so some of these times are based on planned flight times rather than actual flight times.
Proficiency checks and flight reviews
The chief pilot was inducted into Rossair Cessna 441 operations in April and May 2016 by the Cessna 441 fleet manager. The chief pilot successfully completed his line check and OPC on the Cessna 441 on 30 May 2016. As part of that flying, the chief pilot also completed training to become a check pilot on the aircraft. Following the flight on 30 May 2016, a recommendation was submitted to CASA that he be assessed as a Cessna 441 check pilot.
The chief pilot’s last IPC was completed as part of a type rating flight review in the EMB 120 simulator on 22 October 2016. Under CASA exemption 97/16 current at the time of the accident, this flight review conducted on a type‑rated aircraft, also satisfied the requirements of a flight review on the multi-engine class rated Cessna 441 aircraft.
The chief pilot had not completed an OPC or line check on the Cessna 441 aircraft since 30 May 2016. However, he had completed an OPC in the EMB 120 simulator on 1 February 2017, which was conducted under CASA observation. That 2017 check, although not conducted in the Cessna 441, met the required regulatory and operator proficiency checking requirements (see the section titled Operational proficiency check).
CASA flying operations inspector
Flight role
The CASA FOI was sitting in a non-control seat behind the inductee pilot, and therefore had no flying role on this flight. The role of the CASA FOI on the flight was to observe and assess the chief pilot’s skills in conducting an OPC on the inductee pilot.
Qualifications and experience
The CASA FOI held an ATPL (Aeroplane) issued in December 1990 and a CPL (Aeroplane) issued in February 1987. He also held a grade 1 instructor rating, with endorsements, among others, in instructor training, multi-engine class rating, and multi-engine aeroplane class rating instructor training. He held a class 1 aviation medical certificate, valid until 15 December 2017, which required reading correction to be available while flying, but placed no other restrictions on operation.
The CASA FOI had been in the role since 2008, and at the time of employment with CASA had 12,725 hours, including over 5,100 hours as a Cessna 441 pilot. The FOI role did not involve significant flying, but in the last 90 days he had completed 2.5 hours aircraft flight time, as well as simulator time.
Among a variety of flying and management roles prior to joining CASA, the FOI previously held chief pilot and head of training and checking roles at Rossair, with approval to conduct initial training on the Cessna 441.
Proficiency checks and flight reviews
The FOI completed a flight review and IPC in the Saab 340 simulator on 18 April 2017, and in the Bombardier Dash 8 simulator on 9 May 2017. He completed a flight proficiency check for his grade 1 instructor rating in a Beechcraft Baron 95-B55 on 24 May 2017. Additionally, the FOI had logged a 2.7 hour flight in the Cessna 441, with the FOI as PIC flying with the previous Rossair check pilot, in August 2016.
Aircraft information
General information
The Cessna 441 Conquest II is a pressurised, low‑wing, twin-engine turbopropeller (turboprop) aircraft with seating for up to 2 pilots and 9 passengers. Both pilot seats are equipped with flight controls however single‑pilot line operations are flown from the left seat. The right pilot seat would normally only be occupied by a second pilot for training and checking flights.
The accident aircraft, serial number 441‑0113, was manufactured in the United States by the Cessna Aircraft Company in 1980, and registered in Australia as XMJ in February 1989. The Cessna 441 is certified as a normal category[4] aircraft under the United States Federal Aviation Regulations Part 23, and issued with type certificate data sheet number A28CE by the United States Federal Aviation Administration in 1977. At the time of the accident, Textron Aviation Inc. was the Type Certificate holder[5] for the aircraft and as of March 2020, there were 39 Cessna 441 aircraft registered in Australia.
Notable modifications to the aircraft were the incorporation of supplemental type certificates to replace the three blade propellers with four blade propellers, replace the -8 engines with more powerful -10 engines and the installation of vortex generators[6] to increase the aircraft’s maximum take-off weight. Other than an associated increase in the aircraft’s maximum take-off weight, these modifications did not require any changes to the procedures and airspeed limitations in the aircraft’s pilot’s operating handbook (POH).
Aircraft records
XMJ had a current Certificate of Registration, Certificate of Airworthiness and maintenance release, all of which were recovered from the accident site. The maintenance release was due to expire on 10 March 2018 or upon 13,859.0 hours total time-in-service, whichever came first. The maintenance release indicated that XMJ was equipped to be operated under the instrument flight rules and in the charter operational category. The maintenance release indicated that there was no maintenance due on the aircraft or open defects at the time of the accident. Prior to the departure from Adelaide, the aircraft had accumulated a total time in service of 13,845.3 flight hours.
Part 1 of the aircraft’s Logbook Statement specified that the aircraft was to be maintained in accordance with the AE Charter Services system of maintenance and all applicable airworthiness directives. The following summarises the maintenance activities conducted on XMJ leading up to the accident.
- On 31 August 2016 a number of parts, including both the left and right engines were removed for use on other company aircraft. These engines were reinstalled on 24 November 2016 and had operated for 385.2 hours on XMJ since this time.
- On 30 April 2017, the installed fuel control unit (FCU) from the aircraft’s left engine was replaced by an FCU borrowed from a third party maintenance organisation.
- On 4 May 2017, the aircraft was erroneously released to service prior to in-flight FCU set-ups having occurred, with an endorsement in the deferred defect list that the left engine had to be operated in manual mode until the FCU set-up had been completed but could continue in service until no later than 14 May 2017 without the set-up being completed.
- The Rossair chief pilot raised a concern on 8 May 2017 about the aircraft being released into service without the in-flight set-ups being completed, as the aircraft was more difficult than normal to operate with one engine in manual mode. Further maintenance work was performed on the aircraft, and, on 10 May, the aircraft was released into service, with both engines operating in normal (automatic) mode.
- The aircraft subsequently flew 28 flights, totalling 32.6 hours with no reported issues.
- On 26 May 2017, the original FCU that was removed on the 30 April 2017 was reinstalled onto the left engine of XMJ following removal, cleaning and reinstallation of the FCU’s manual mode control valve.
- A certification regarding a wing de-icing system unserviceability was made on 26 May 2017. It stated ‘No action was carried out at this time. Aircraft unavailable due to flying requirements. Customer notified.’ There was no entry in the defect field of the current maintenance release Part 3.
- Between 26 May and 30 May, the aircraft flew 6.9 hours without reported issue, including 4.5 hours across five sectors on the morning of the accident.
Aircraft systems information
Flight control overview
The Cessna 441 is fitted with conventional flight controls connected to the aircraft’s primary flight control surfaces. The primary flight controls consist of the rudder, elevators, and ailerons, which control the aircraft about the yaw, pitch and roll axes respectively.
The pilot controls an aircraft by manipulating the control wheel and rudder pedals, which deflect the ailerons, elevators and rudder. Deflection of an aircraft’s primary flight control surfaces changes the aerodynamic shape and therefore the amount of lift generated by the associated part of each wing, vertical stabiliser or horizontal stabiliser. These local variations in lift result in changes to the aircraft attitude and consequently flight path.
Any deflection of the primary flight control surfaces into the adjacent airflow produces aerodynamic forces on the surface and corresponding loads on the control wheel or rudder pedals. The magnitude of the aerodynamic force is principally related to the amount of flight control surface deflection, airspeed and trim tab deflection.
On the Cessna 441, adjustable trim tabs are attached to the trailing edge of the primary flight controls. These tabs are used to ‘trim’ or counteract the aerodynamic forces felt by the pilot on the control wheel or rudder pedals. During flight, deflection of an aircraft’s trim tab produces an aerodynamic force on the aft part of the associated primary surface. The tabs have the capacity, when adjusted in the opposite direction to the deflection of the primary control surface, to modify the aerodynamic force on the surface and correspondingly, reduce the load felt by the pilot on the control wheel or rudder pedals. The effectiveness of a trim tab is principally related to the amount of deflection and the aircraft’s airspeed.
Flap system description
The aircraft has four flaps, one inboard, and one outboard per wing. The flaps are normally in the fully retracted position. They are extended to slow the aircraft and allow it to land at a lower airspeed. They can also be used to improve take-off performance in the ‘T.O.’ position. The flaps are operated using a sliding selector. Flap travel is registered on an indicator adjacent to the selector. There are four detents in the selector assembly as follows:
- UP – fully retracted, 0⁰ of travel
- T.O. – 10° of flap down travel
- APPR – 20⁰ of flap down travel
- LAND – full extension, 30⁰ of flap down travel.
Engine and propeller controls
Each engine is controlled by two levers located in the engine controls section of the centre pedestal (Figure 3).
The power levers provide control input to the engine for the power necessary throughout the entire operational envelope. The power lever has the following positions:
- MAX
- AIR START
- FLIGHT IDLE
- GROUND IDLE
- REVERSE
The power levers can be moved freely forward of FLIGHT IDLE. A hard stop is provided at the FLIGHT IDLE position to prevent inadvertent selection of reverse thrust in flight (Figure 4). Finger latches located on each power lever must be pulled up to allow movement of the power levers rearward of the FLIGHT IDLE position.
The condition levers are used to set the engine revolutions per minute required for flight as well as acting as the control for propeller feathering and emergency fuel shut-off. The condition lever quadrant has the following positions:
- TAKEOFF, CLIMB and LANDING
- CRUISE
- START AND TAXI
- EMER SHUT-OFF
The condition levers can be moved freely forward of CRUISE. A hard stop is provided at the CRUISE position to prevent inadvertent selection of START AND TAXI speed in flight (Figure 5). Each condition lever must be pulled up to allow movement rear of the CRUISE stop. Another stop is provided at the START AND TAXI position. Rearward movement past this position allows the respective engine to be shut down and its propeller feathered.
Figure 3: Engine control levers
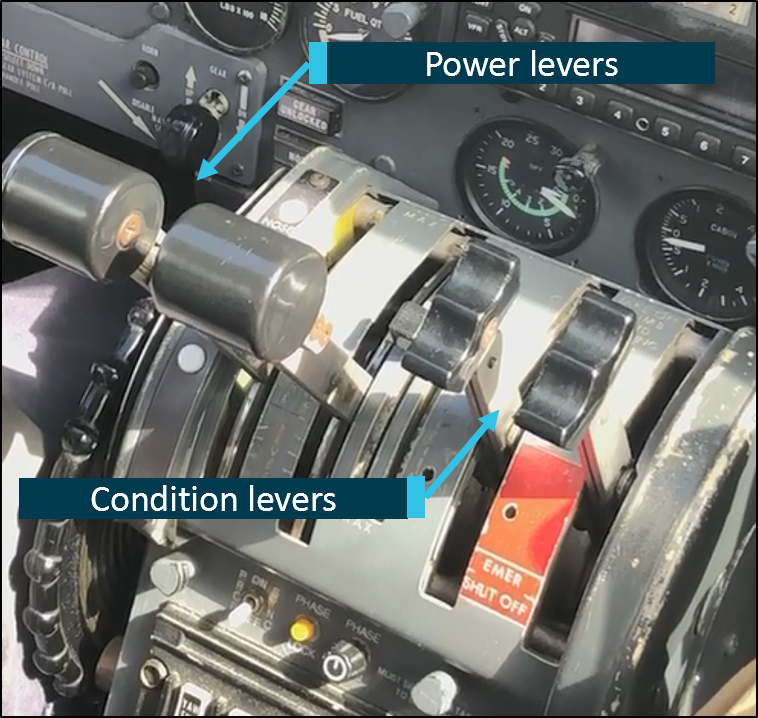
Source: ATSB
Figure 4: Power lever

Source: Textron Aviation Inc.
Figure 5: Condition lever

Source: Textron Aviation Inc.
Negative torque system
The aircraft’s engines are equipped with a negative torque sensing (NTS) system that activates under conditions of low propeller pitch (see the section titled Multi‑engine aeroplane propellers) when air loads drive the propeller instead of the engine. This can occur during normal operation at high airspeed and low power settings but will also happen following an engine failure. When NTS activates, the propeller blades are automatically driven towards the feathered[7] position to reduce both the air load and the significant associated drag. NTS will only activate while negative torque is detected so, unlike an auto‑feather system fitted to other aircraft, the blades will only automatically move to a high pitch position rather than fully feathered. Consequently, in the event of an engine failure the pilot is required to move the condition lever to the emergency shut off position to feather the propeller.
With regard to functioning of the NTS, the POH noted that:
NTS operation, as evidenced by a cycling sound of the engine(s) can occur at high airspeed with the power levers at FLIGHT IDLE; this is particularly true when operating in manual mode. NTS operation occurs when the propeller is driving the engine, rather than the engine driving the propeller. During normal mode operation, NTS can indicate the fuel flow is insufficient for existing conditions.
There is a POH requirement to confirm operation of the NTS prior to flight. Normal operation of the NTS on the ground is accompanied by illumination of an amber light on the cockpit annunciator panel for the respective engine being checked. The light was for check purposes only and would not illuminate during in‑flight activation of the NTS. Activation of the NTS on an operative engine in flight can be overcome by advancing the power levers slightly.
Manual mode operation
Manual mode refers to the engine power output being directly controlled by the power lever position rather than by a signal sent to the engine by the electronic engine control unit (EEC). The power system is designed so that fuel scheduling is lower in manual mode than it is in normal (automatic) mode.
Higher power lever positions are therefore required to maintain engine power when in manual mode compared to normal mode. This means that if a fault is detected in the EEC and the engine operation automatically reverts to manual mode the engine will have a reduction in power for that particular power lever setting. If that occurs the power can be restored by advancing the power lever as required.
Weight and balance
The ATSB determined the likely fuel on board at the time of the accident and the weight and location of people, baggage and ballast. From this information, it was calculated that the aircraft was within the weight and balance limitations specified in the aircraft’s POH and relevant supplements. The aircraft’s weight at the time of the accident was estimated to be about 3,950 kg. The aircraft’s maximum take-off weight was 4,690 kg.[8]
Meteorological information
The forecast weather conditions at Renmark Airport on the afternoon of the accident were benign with a southerly wind at 14 kt, visibility in excess of 10 km and scattered[9] cloud at 4,000 ft above the airport.
Weather observations recorded at one‑minute intervals by an automatic weather station at the airport were obtained from the Bureau of Meteorology (BoM). Consistent with the forecast, in the 20 minutes preceding the accident the wind strength varied between 8‑13 knots, and the direction varied between 188‑205° magnetic. The cloud cover was consistently seven oktas at about 6,500 ft above the airport and the ambient temperature was 13°C.
The ATSB also sought the assistance of the BoM to assess the likely wind strength and direction at the operating altitude of the aircraft immediately prior to the loss of control. This was done to enable an assessment of the airspeed during the final flight segment using recorded groundspeed data (see the section titled Recorded flight data).
Airport information
Renmark Airport is at an elevation of 115 ft above mean sea level and has one sealed runway, 07/25, and one gravel runway, 18/36.3 As there is no air traffic control tower at the airport, traffic at the airport broadcast on a common traffic advisory frequency to advise intentions and arrange separation with other traffic.
The terrain west of the airport, along the extended runway centreline in XMJ’s departure direction, slopes upwards, with an elevation gain of about 60 ft between the runway and the accident site location.
Circuit operations
In order to assure a safe and orderly traffic flow into and out of an airport, a standard circuit traffic pattern is used. The circuit consists of four legs: crosswind, downwind, base and final as shown in Figure 6, with standardised methods for joining the pattern to avoid traffic conflicts.
Figure 6: Standard circuit pattern
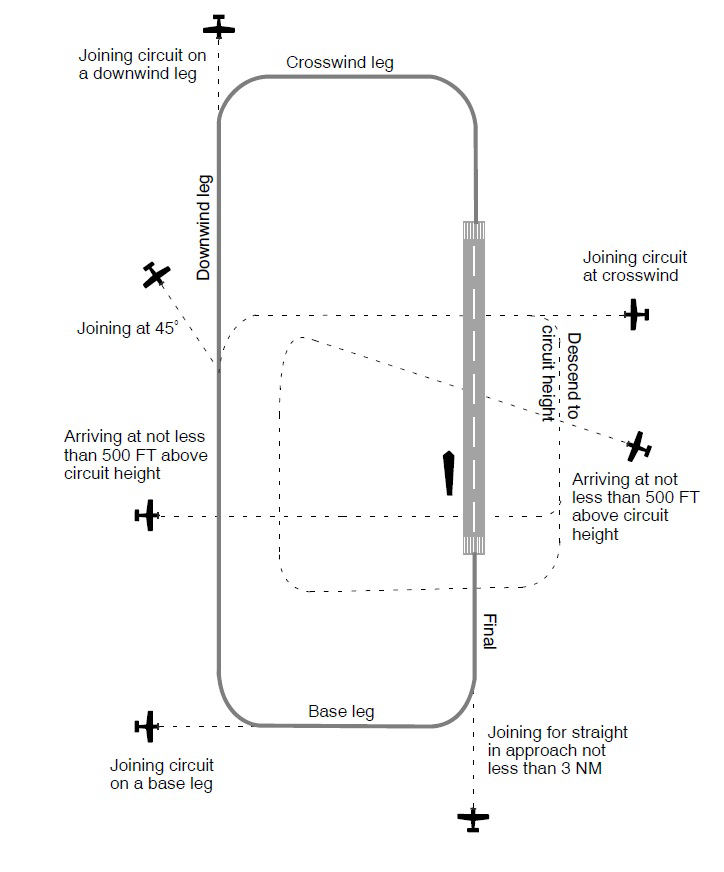
Source: Airservices Australia
Asymmetric flight
Multi-engine aeroplanes
In a discussion of small[10] multi-engine aeroplane operations, the United States Federal Aviation Administration (FAA) Airplane Flying Handbook FAA‑H‑8083‑3B, stated:[11]
The basic difference between operating a multiengine airplane and a single-engine airplane is the potential problem involving an engine failure. The penalties for loss of an engine are twofold: performance and control. The most obvious problem is the loss of 50 percent of power, which reduces climb performance 80 to 90 percent, sometimes even more. The other is the control problem caused by the remaining thrust, which is now asymmetrical. Attention to both these factors is crucial to safe OEI [one engine inoperative] flight. The performance and systems redundancy of a multiengine airplane is a safety advantage only to a trained and proficient pilot.
The importance of maintaining one engine inoperative performance and control was further emphasised in the handbook as follows:
In OEI flight at low altitudes and airspeeds such as the initial climb after takeoff, pilots must operate the airplane so as to guard against the three major accident factors: (1) loss of directional control, (2) loss of performance, and (3) loss of flying speed. All have equal potential to be lethal. Loss of flying speed is not a factor, however, when the airplane is operated with due regard for directional control and performance.
Multi-engine aeroplane propellers
In the event of an engine power loss, the inoperative engine may windmill - continue to rotate due to the airflow acting on the propeller. The FAA handbook described the hazard of a windmilling propeller as follows:
The propeller windmilling at high speed in the low range of blade angles can produce an increase in parasite drag, which may be as great as the parasite drag of the basic airplane.
In order to minimise this significant source of drag on single engine controllability and climb performance, the propellers of multi-engine aeroplanes are capable of aligning the blades with the airflow (Figure 7).
Figure 7: Multiengine aeroplane propeller
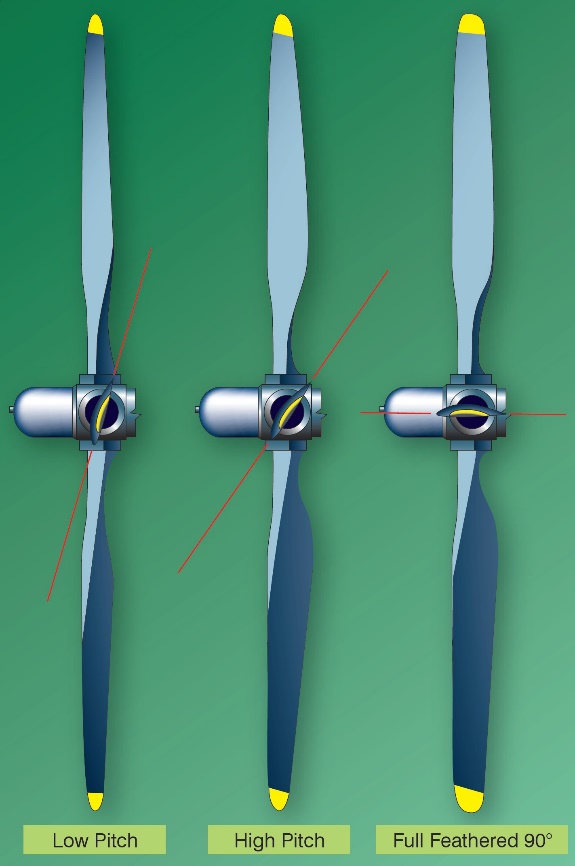
Source: United States Federal Aviation Administration
This ‘feathered’ configuration stops the rotation of the engine and propeller and significantly reduces the parasite drag compared to that associated with a windmilling propeller (Figure 8).
Figure 8: Propeller drag
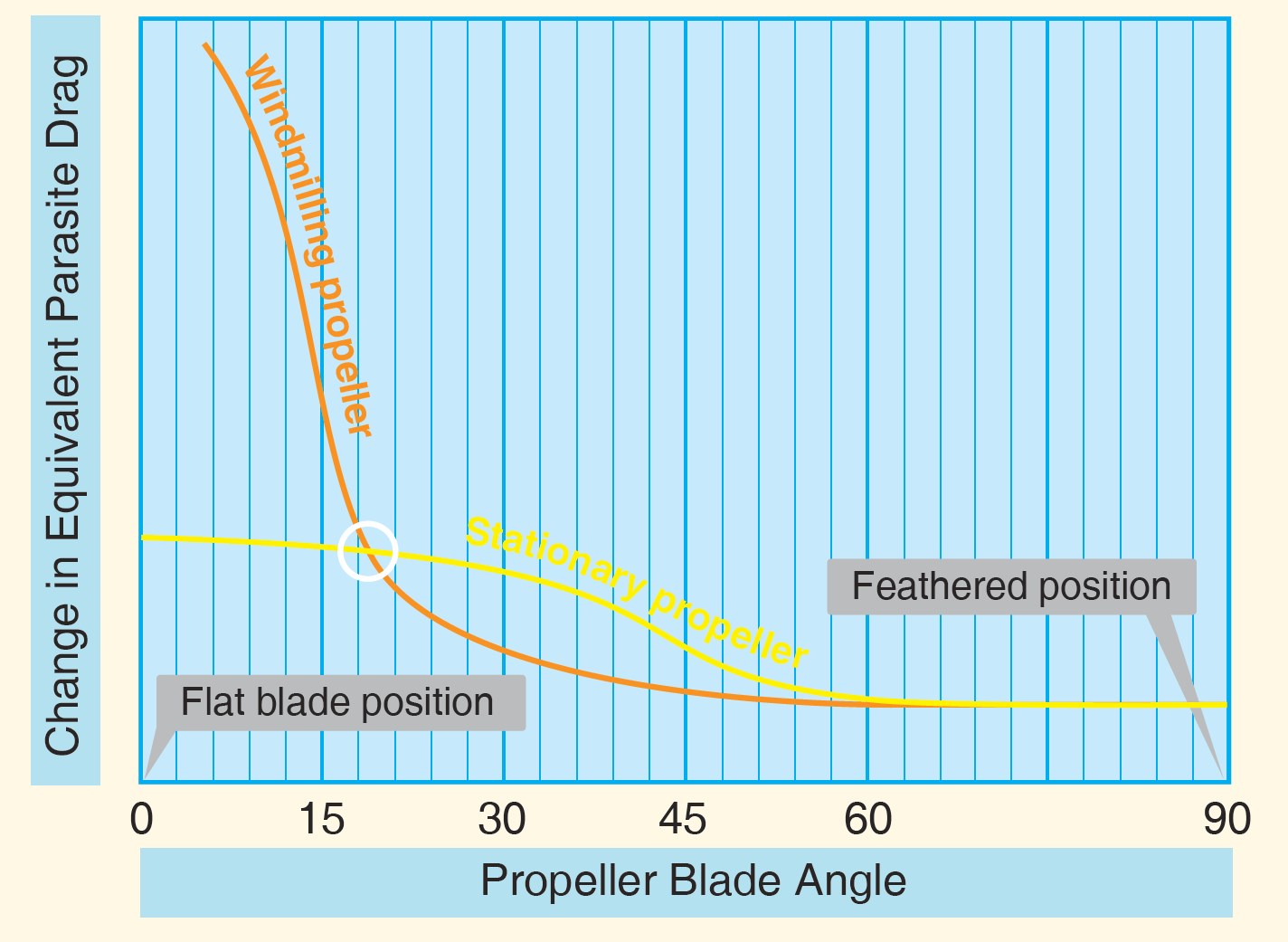
Source: United States Federal Aviation Administration
Asymmetric control
The majority of small, multi-engine aeroplanes like the Cessna 441 have two wing‑mounted engines that produce symmetrical propeller thrust during normal operation. One engine inoperative (OEI) flight in these aeroplanes results in asymmetric thrust and drag due to the offset position of the engines from the aeroplane’s centreline. The result is a tendency for the nose of the aeroplane to turn in the direction of the inoperative engine. The extent of the yaw may vary depending on which engine becomes inoperative, with the inoperative engine that produces the greatest degree of asymmetry being termed the ‘critical’ engine.[12]
The asymmetric yawing tendency may be countered through the application of rudder and aileron control inputs. As the effectiveness of an aircraft’s control surfaces generally decreases with decreasing airspeed, sufficient airspeed must be maintained while operating OEI to ensure that the rudder and aileron retain sufficient control authority to maintain directional control of the aeroplane.
The minimum control airspeed with the critical engine inoperative (VMCA) is established by test pilots during aircraft certification under a specific set of conditions, and is marked on the air speed indicators of most multi-engine aeroplanes with a red radial line. VMCA is influenced by a large number of factors, including an aircraft’s configuration/loading, operating altitude and pilot control inputs and is therefore likely to vary from the stated value.
The VMCA published in the Cessna 441 pilots operating handbook (POH) was 91 kt indicated airspeed. The POH further stated that:
The airplane must reach the air minimum control speed (VMCA) before full control deflections are able to counteract the roll and yaw tendencies associated with one engine inoperative and full power operation on the other engine. VMCA with wing flaps in take-off position is indicated by a red radial on the airspeed indicator. VMCA with wing flaps in the UP position and the airplane in an en-route climb configuration will be buffet limited and occur at a higher speed.
In addition to the published VMCA the POH also listed an ‘intentional one engine inoperative’ indicated airspeed of 98 kt with advice that:
Although the airplane is controllable at the air minimum control speed, the airplane performance is less than optimum. A more suitable speed with wing flaps positioned in take-off is 98 KIAS [kt indicated airspeed]. This speed is identical to the normal rotation speed, thus the pilot can direct more of this attention to determining and securing the inoperative engine than to achieving a speed not normally associated with take-off. This speed also provides additional safety for controllability and allows easier maintenance of altitude during the period of gear retraction and securing the inoperative engine.
As detailed in the FAA handbook, maintaining directional control following an engine failure during take‑off and initial climb is especially critical:
The first consideration following engine failure during takeoff is to maintain control of the airplane. Maintaining directional control with prompt and often aggressive rudder application and STOPPING THE YAW is critical to the safety of flight. Ensure that airspeed stays above VMC [VMCA]. If the yaw cannot be controlled with full rudder applied, reducing thrust on the operative engine is the only alternative. Attempting to correct the roll with aileron without first applying rudder increases drag and adverse yaw and further degrades directional control.
Asymmetric performance
Optimum single-engine climb performance is obtained by flying the aircraft at the published OEI best rate of climb speed (VYSE), 120 KIAS for the Cessna 441, with maximum available power and minimised drag. Minimum drag is achieved by:
- retracting the flaps and landing gear
- feathering the propeller of the inoperative engine
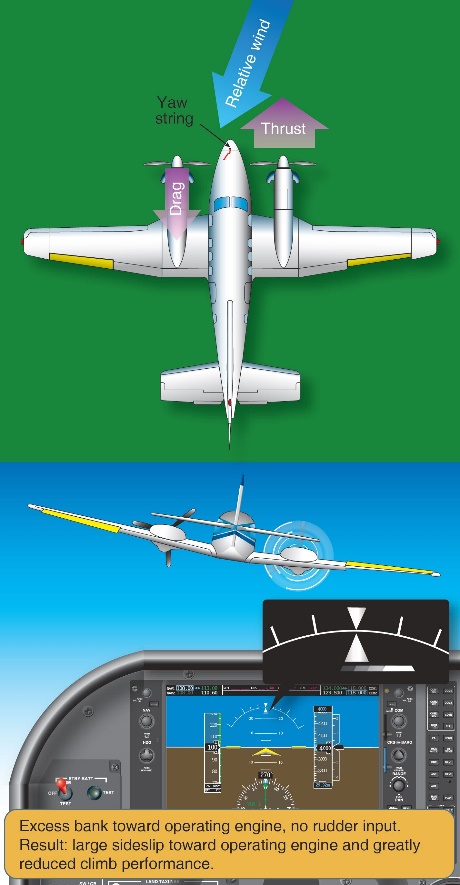
- minimising sideslip by presenting the smallest aircraft profile to the relative wind.
During symmetrical flight in a single-engine airplane, or a multiengine airplane with both engines operating, zero sideslip occurs when the balance ball[13] is centred. However, in the case of asymmetric thrust, zero sideslip requires a combination of bank angle and non‑centred ball position. That is, a combination of rudder and aileron inputs (Figure 9).
As it related to the Cessna 441, the POH provided the following information on the required combination of rudder and aileron inputs to minimise sideslip:
Best single-engine climb is attained with the wings banked approximately 3° to 4° and with a ⅔ to ¾ ball slip into the operative engine when the airplane is at low airspeed and heavy weight. As airspeed increases and/or airplane weight is significantly reduced, the ⅔ to ¾ ball slip becomes less important.
Figure 9: Zero sideslip

Source: United States Federal Aviation Administration
While it is possible to counteract asymmetric thrust using only rudder or only aileron, this results in significant performance and controllability penalties. Specifically, countering asymmetry with level wings and the ball centred (large rudder input towards the operative engine) results in moderate sideslip towards the inoperative engine that reduces climb performance (Figure 10). It also significantly increase VMCA as there is no horizontal component of lift to assist the rudder to counter the asymmetric thrust. In discussing this increase in minimum control speed as it related to the Cessna 441, the Civil Aviation Advisory Publication (CAAP) 5.23‑1(2) Multi-engine aeroplane operations and training stated:
…Flight tests in an instrumented Cessna Conquest showed that with a published VMCA [VMCA] of 91 kts, if the aircraft was flown in asymmetric flight with full power applied and the wings held level with the rudder balancing the aircraft, minimum control speed increased to 115 kts, an increase of 24 kts.
Figure 10: Rudder‑only input
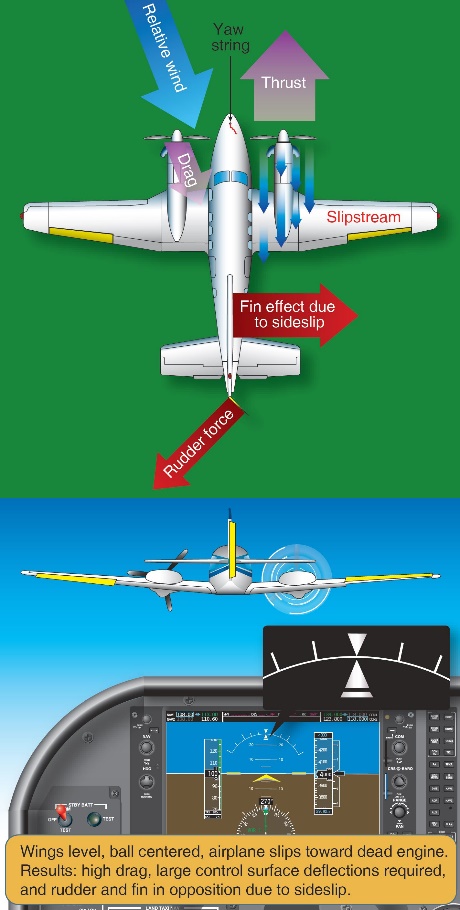
Source: United States Federal Aviation Administration
Opposing asymmetric thrust using only aileron input results in a large sideslip towards the operative engine that also significantly reduces climb performance (Figure 11).
Figure 11: Aileron‑only input
Source: United States Federal Aviation Administration
OEI rate of climb performance for given operating conditions can be determined using data published in the POH/flight manual. Achieving the published performance relies on use of the zero sideslip technique and configuring the aircraft for minimum drag.
Considering the configuration and approximate weight of the aircraft at the time of the accident (see the section titled Weight and balance), the calculated OEI climb rate over a range of indicated airspeeds is shown in Table 1.
Table 1: One engine inoperative climb performance for Cessna 441 at 3,950 kg
| Indicated airspeed (kt) | Excess Thrust Horse Power (HP) | Calculated climb rate (ft/min) |
| 90 | 115.7 | 438 |
| 100 | 185.1 | 701 |
| 110 | 205.4 | 778 |
| 120 | 213.4 | 809 |
| 130 | 211.7 | 802 |
Source: ATSB analysis from aircraft certification data
The OEI performance data indicated that XMJ was capable of achieving a positive rate of climb following departure from Renmark if sideslip and other sources of drag were minimised.
Engine failure simulation
Zero thrust
Demonstration of OEI flight often involves simulating a failed engine by moving the power lever to a low power level rather than actually shutting down the engine and feathering the propeller. This method of simulation allows rapid normal power restoration. However, as detailed in the section titled Multi-engine aeroplane propellers, at low power settings the propeller will rotate due to the airflow rather than the engine, creating much higher drag than a feathered propeller. For that reason, a zero thrust power level is commonly set to overcome the drag associated with windmilling and more accurately simulate the low drag associated with a feathered propeller.
Zero thrust varies depending on the engine type, airspeed, altitude and temperature. In a piston engine aircraft zero thrust is normally achieved by setting a manifold pressure that results in a specific propeller rpm. In a turbine propeller engine zero thrust is expressed as an engine torque, and in some cases rpm, for a particular airspeed (normally VYSE).
Aircraft manufacturer’s procedures
The Cessna 441 POH detailed two procedures for simulating an engine failure, however neither procedure involved the use of a zero thrust power setting.
The first POH procedure was designed to practice management of an engine failure during the cruise phase of flight. The procedure involved retarding the power lever to the AIRSTART position and then shutting the engine down. In discussing the AIRSTART power lever position, the POH stated:
The AIRSTART position does provide some forward thrust. This position is recommended as it allows the best exhaust gas temperature stabilization before shutdown and it is the lowest position which will prevent the fuel computer from tripping to manual mode during an airstart.
If the power lever is retarded below the AIRSTART position and the fuel computer trips to manual mode, normal mode may be regained by advancing the power lever slightly and cycling the fuel computer switch to OFF then back to ON.
The second procedure was designed to train pilots to handle an engine failure in the take-off configuration. This involved using a fuel interruption process to actually shut the engine down. This was achieved by momentary selection of the engine stop button which activated a solenoid within the fuel control unit and cut off the fuel supply to the engine. In order to also simulate representative control forces during the exercise, the set up for the sequence involved:
- extending the landing gear
- extending the wing flaps to the take‑off position
- trimming the aircraft for a speed greater than the intentional one engine inoperative speed of 98 kt.
This procedure directly referenced related guidance in the POH, applicable to the demonstration of VMCA, which stated:
One engine inoperative procedures should be practiced in anticipation of an emergency. This practice should be conducted at a safe altitude (5000 ft AGL), with full power on both engines, and should be started at a safe speed of at least 98 KIAS. As recovery ability is gained with practice, the starting speed may be lowered in small increments until the feel of the airplane in emergency conductions is well known. It should be noted that as the speed is reduced, directional control becomes more difficult. Emphasis should be placed on stopping the initial large yaw angles by the IMMEDIATE application of rudder supplements by banking slightly away from the yaw. Practice should be continued until: (1) an instinctive corrective reaction is developed and the corrective procedure is automatic, and (2) airspeed, altitude and heading can be maintained easily while the airplane is being prepared for a climb.
The POH did not contain any procedure relating to simulation of an engine failure during the actual take‑off phase.
Additionally, for Cessna 441 aircraft with the serial number 0173 onwards (not applicable to VH‑XMJ) the POH, in reference to the ‘engine shutdown to simulate engine failure in takeoff configuration’ procedure (second procedure), explicitly stated
“This procedure must not be practiced at an altitude below 5,000 ft AGL”
Some of Rossair’s other Cessna 441 aircraft operated under this later POH, but the operators manual did not note a difference between the two handbooks.
With respect to the change in the POH procedures applicable to serial number 0173 and onwards, the aircraft manufacturer advised that:
- there was no material difference between the aircraft from serial numbers 0173 and onwards and the earlier serial numbers (0172 and prior) that necessitated a different method of simulating an engine failure in the take-off configuration
- the statements in the earlier POH procedure that referenced the demonstration of VMCA have the same intent as the warning note in the POH for aircraft with serial numbers 0173 and onwards, which states this procedure must not be practiced at an altitude below 5,000 feet above ground level.
Operator’s procedures
Rossair’s operations manual contained information relating to simulated engine failures in both Part A (general operations) and Part C (training and checking). Part A of the manual stated:
Simulated asymmetric flight is not to be carried out unless specifically authorised, and then only when accompanied by an authorised person. Asymmetric flight shall not be carried out when passengers are being carried and shall only be conducted on a designated training flight.
Any engine failure simulation shall be conducted by closing the power lever to a position equivalent to zero thrust (Turbine) in accordance with Part C, or moving the mixture lever to the idle cut off position (Piston).
For the purpose of training, simulated engine failures and the feathering of aircraft propellers shall only be conducted in VMC conditions. In addition, the aircraft shall be operating above 3000 ft AGL, unless the simulation or feather practice is specifically required during the approach and landing phase.
Following any practice engine shut-down in flight, the engine controls must be set for an immediate restart.
At no time are stalling or Vmca demonstrations to be made with the aircraft propeller feathered.
Part C contained detailed information on the procedure for simulating engine failures in the Cessna 441 (Figure 12). However, the procedure varied from that outlined in Part A with regard to initial power settings and the height at which the simulation could be initiated.
Part A detailed that engine failure simulation for training purposes was to occur above 3,000 ft above ground level unless specifically required during the approach and landing phase. Part C permitted the simulation of engine failure ‘After attaining the higher of 400’ or acceleration altitude’. The reference to ‘acceleration altitude’ was not applicable to the Cessna 441.
Figure 12: Rossair training and checking manual

Source: AE Charter/Rossair
The Part C procedure involved retarding power to flight idle (power level to minimum) and then advancing the power to zero thrust (to represent a feathered propeller) on completion of the engine failure drills. This is the normal technique used for simulating the failure of a piston engine aircraft, where the pilot must manually feather the propeller.
It is not necessary to select less than a zero thrust setting to simulate failure of a turboprop engine equipped with auto feather or negative torque sensing systems (such as the Cessna 441). More importantly, setting the power lever below the zero thrust setting will increase propeller drag. As detailed previously, selection of less than the AIRSTART power lever position in the Cessna 441 can also affect automatic operation of the fuel computer.
An earlier version of the company operations manual detailed simulation of a failed engine on a turboprop engine by only moving the power lever to zero thrust. The ATSB could not determine how the procedure involving moving the power to below zero thrust was introduced into the 2016 version of the manual (in use at the time of the accident). However it may have occurred during the merger of Rossair with another company (see section titled Overview of the operator). Additionally, this section of the operations manual was approved by the Civil Aviation Safety Authority without detection of the error (see section titled Regulatory services processes).
Finally, the propeller manufacturer advised that for the four‑bladed propellers fitted to XMJ, the required zero thrust setting was about 234 ft.lbs of engine torque, 116 ft.lbs less than stated in Part C of the operations manual.
Regulatory guidance
CAAP 5.23‑1(2) Multi-engine aeroplane operations and training, provided comprehensive guidance on the operation of multiengine aeroplanes. With regard to the simulation of engine failures, it stated:
Before simulating engine failures in multi-engine aircraft, instructors must be aware of the implications and be sure of their actions. Consult the aircraft flight manual or POH for the manufacturer’s recommended method of simulating an engine failure.
The CAAP also provided guidance on setting power to simulate a failed engine. Specifically, it was recommended to initially close the throttle of a piston engine to replicate a windmilling propeller and then set zero thrust once the trainee had simulated propeller feathering. In the case of a turboprop engine, replication of an engine failure only required selection of zero thrust. Guidance was also provided on a method to establish zero thrust if it was not specified.
The CAAP also detailed a number of risks associated with multi-engine training, including:
- inappropriate management of complex aircraft systems
- conducting flight operations at low level (engine failures after take-off)
- conducting operations at or near VMCA or VSO [stall speed with undercarriage and flap selected] with an engine inoperative
- asymmetric operations.
With regard to flight operations at low level, the CAAP further stated:
Any flight operation at low altitude has potential dangers. Trainers have debated over the decades on the value of practicing engine failures after an actual take-off, near the ground. The general consensus is that despite the risks, pilots must be trained to manage these situations in multi-engine aircraft.
…Instructors should consider not simulating engine failures below 400 ft above ground level (AGL) to provide a reasonable safety margin.
Accident flight procedure
There was insufficient information and recording devices to determine the specific procedure used to simulate the engine failure after take‑off from Renmark Airport. However, the electronic briefing developed by the chief pilot in preparation for the occurrence check flight provided specific guidance on how engine failures were to be simulated as follows:
All failures will be preceded by the phrase “simulated”
• Once the memory items have been carried out, zero thrust will be set
• The instructor will handle the ‘failed’ engine
• Pilot is to use other power lever as required
• When landing, pilot may retard both levers as required
Any failure not preceded with the phrase “simulated” is real and shall be treated as such.
In preparation for the occurrence check flight, a practice flight covering similar sequences was conducted in XMJ the week before with the chief pilot and inductee pilot. That flight also had an observer on board with extensive Cessna 441 check pilot experience. The practice flight was not conducted as a training flight, but rather a private flight with two licenced and experienced pilots on board, preparing for their respective roles during the CASA check flight.
The observer advised that during the practice flight, the engine failure was simulated by the chief pilot reducing the power lever but not all the way to the flight idle stop. He further recalled that once the inductee pilot completed the initial response actions, the chief pilot partially advanced the power lever. The observer stated that, based on his experience, zero thrust in the occurrence aircraft was about 150 ft.lbs of torque and lower than other company Cessna 441 aircraft. He also recalled that the chief pilot set a power lever position at or slightly above that torque value during the simulation.
Stall speed
The calculated stall speed depends on the weight of the aircraft, as well as the gear and flap configurations, and the angle of bank. For XMJ, at the ATSB calculated take-off weight from Renmark Airport (3,950 kg), with:
- gear and flap retracted
- power at the flight idle,
the calculated stall speed with wings level was 85 KIAS. At 20° angle of bank, the stall speed increased to approximately 88 KIAS.
Flight recorders
XMJ was not equipped with a flight data recorder or cockpit voice recorder. Requirements relating to the fitment of flight recorders is detailed in Civil Aviation Order (CAO) 20.18 as follows:
An aircraft of maximum take-off weight:
a) In excess of 5,700 kg and which is:
i. turbine powered; or
ii. of a type first certificated in its country of manufacture on or after 1 July 1965;
shall not be flown (except in agricultural operations) unless it is equipped with an approved flight data recorder and an approved cockpit voice recorder system;
b) Less than or equal to 5,700 kg and which is:
i. pressurised; and
ii. turbine powered by more than one engine; and
iii . of a type certificated in its country of manufacture for operation with more than eleven places; and
iv. issued with its initial Australian Certificate of airworthiness after 1 January 1988;
shall not be flown unless it is equipped with an approved cockpit voice recorder system.
The Cessna 441 has a maximum take‑off weight of 4,468 kg so CAO 20.18(a) was not applicable. Additionally, although meeting a number of the criteria detailed in CAO 20.18(b), the Cessna 441 is certified for a maximum of eleven seats (two crew and nine passengers). The aircraft was therefore not required to be fitted with either a flight data recorder or a cockpit voice recorder.
Recorded flight data
As part of the investigation, data broadcast by the automatic dependent surveillance broadcast (ADS-B) equipment fitted to the aircraft was obtained from various web-based providers. Depending on the provider, this data recorded the following parameters at intervals of either 6 or 15 seconds:
- latitude and longitude
- time of the logged position
- pressure altitude
- groundspeed
- track.
A review of the data identified that the aircraft descended outside ADS-B coverage as it approached the circuit area at Renmark Airport. Consequently, no ADS-B flight data was available for the departure of XMJ from Renmark.
However, GPS data transmitted from an on board mobile device with the OzRunways application installed was able to be sourced. This data was available at 5 second intervals with the GPS altitude truncated to the nearest 100 ft and accurate to about -30/+130 ft of the recorded value. The OzRunways data parameters were compared with ADS‑B information from earlier stages of the flight and was found to be consistent. That provided assurance that the OzRunways data was valid and could be relied upon for analysis of the final flight segment. Although the recorded parameters were considered representative of the actual flight profile, it was not possible to determine how they varied between sample points.
Using the GPS groundspeed, and wind information obtained from the BoM, the aircraft’s true airspeed (TAS) was calculated. The TAS values were then converted to a calculated indicated airspeed (IAS) using altitude and temperature data. Given the relatively low operating altitude, the IAS varied only slightly from the calculated TAS. The airspeed and height above the ground variation over the final 1 minute of the flight, referenced to the elapsed time from take‑off, is shown in Figure 13.
Figure 13: Indicated airspeed and altitude variation over the final minute of flight

Source: ATSB
The data showed a steady increase in airspeed up to about 132 kt, followed by loss of airspeed, brief stabilisation around 110‑115 kt, then a further decrease to about 107 kt before the data ended. The maximum recorded airspeed was about 10 kt higher than published OEI best rate of climb speed VYSE (120 kt, see the section titled Asymmetric performance) and occurred at a height of about 300 ft above ground level.
That height was derived from the recorded GPS altitude of 400 ft less 100 ft for the approximate runway elevation (see the section titled Airport information). Noting that the GPS altitude was truncated to the nearest 100 ft and had an accuracy of about ‑30/+130 ft, a height of 300 ft above the ground was indicative of an actual height range between 270‑420 ft above the ground.
Analysis of the indicated airspeed and height profiles indicated that, on attaining the minimum operator‑specified conditions for initiation of a simulated engine failure, the variation in airspeed and altitude was consistent with a reduction in performance associated with OEI flight.
The airspeed subsequently decreased below the target airspeed of VYSE and remained below that airspeed for the final 35 seconds of the data. The final airspeed value of 107 kt was above both the calculated stall speed (see the section titled Stall speed) and the published minimum control airspeed VMCA. However, it was below the VMCA range established during flight testing in the Cessna 441 (see the section titled Asymmetric performance).
Figure 14 illustrates the difference in the calculated IAS and height (above ground level) profiles between the departure from Renmark Airport and the earlier departure from Adelaide Airport.
Figure 14: Departure profile comparison

Source: ATSB
In addition to the airspeed variation, the aircraft’s rate of climb was derived from the GPS altitude data and is shown, together with the aircraft’s track deviation from the runway heading in Figure 15. The data indicated that the aircraft initially climbed at greater than the expected OEI rate of climb before levelling and maintaining approximately level flight for 30 seconds until the data ended. A review of the airspeed over the same time period identified that it reduced during the peak increase in the rate of climb, suggesting that the aircraft was pitched up to reduce airspeed.
Analysis of the track variation identified that the aircraft deviated to the right of the runway centreline during the final minute of the flight. That movement was consistent with both the prevailing left crosswind component during the departure and a reduction in power on the right engine.
Figure 15: Rate of climb and track variation over the final minute of flight

Source: ATSB
Operational information
Pilot licencing
Each of the three pilots on board held a Civil Aviation Safety Regulations 1998 (CASR) Part 61 licence. CASR Subpart 61E requires that pilots meet a series of ongoing requirements in order to exercise the privileges of their licence. Relevant requirements are discussed below.
Pilot recency requirements for carriage of passengers
CASR Part 61.395 outlines the recent experience requirements that pilots must have in order to carry passengers. By day, this includes at least three take-offs and three landings within 90 days in the aircraft. A pass in a flight check meets this requirement.
The Rossair operations manual (Part A) reflected the Part 61 requirements for landings and included the company recency requirements for conducting instrument approaches.
Both of the pilots in the control seats met the recency requirements for the flight they were conducting.
Class and type rated aircraft
Under the regulations prior to CASR Part 61, particular aircraft required a pilot to be trained, endorsed and checked on that aircraft type in order to operate that specific type. Under Part 61, there are still some aircraft which come under this requirement (‘type rated aircraft’), such as the Embraer EMB 120, but other aircraft are included in a class rating (‘class rated aircraft’). This means that a check on any aircraft in the class rating covers all other aircraft in that class rating. Pilots must complete a flight review for the class rating every two years to continue operating aircraft in that class.
The Cessna 441 is in the multi-engine class rating. However, the complexity of the aircraft is recognised by CASA, who requires that pilots that wish to operate the Cessna 441 first complete flight training and a flight review in this aircraft type, before it becomes covered by the class rating in subsequent years. Other complex twin aircraft covered by this legislation include the Beechcraft King Air C90, King Air B200 and the de Havilland DHC-6 Twin Otter.
As discussed previously (see the section titled Pilot licencing), the CASA FOI renewed his class rating in a Rossair Cessna 441 with the Cessna 441 fleet manager in late 2016. The inductee pilot completed his multi-engine class rating renewal along with his instrument proficiency check in a Beechcraft Baron 95-B55 in February 2017.
The chief pilot had not been checked on a class rated aircraft, since his check pilot training was completed in the Cessna 441 (see the section titled Pilot licencing). In October 2016 he completed his instrument proficiency check (IPC) and type rating renewal in the EMB 120 simulator, which, at that time, under CASA exemption 97/16 satisfied the requirements for the multi-engine class rating renewal. Despite the EMB 120 being a two crew aircraft, and the Cessna 441 being a single pilot operation, the chief pilot was not required to demonstrate on‑going competency in the Cessna 441, as long as he continued to be checked in the EMB 120.
General competency
CASR Part 61.385 ‘Limitations on exercise of privileges of pilots licences – general competency requirement’ states:
1) The holder of a pilot licence is authorised to exercise the privileges of the licence in an aircraft only if the holder is competent in operating the aircraft to the standards mentioned in the Part 61 Manual of standards for the class or type to which the aircraft belongs, including in all of the following areas:
• Operating the aircraft’s navigation and operating systems;
• Conducting all normal, abnormal and emergency flight procedures for the aircraft;
• Applying operating limitations;
• Weight and balance requirements;
• Applying aircraft performance data, including take-off and landing performance data, for the aircraft.
(1A) Subregulation (1B) applies if the holder of a pilot licence also hold an operational rating or endorsement
(1B) The holder is authorised to exercise the privileges of his or her pilot licence in an activity in an aircraft under the rating or endorsement only if the holder is competent in operating the aircraft in the activity to the standards mentioned in the Part 61 Manual of standards (if any) for:
a) The class or type to which the aircraft belongs; and
b) The activity.
In assessing personal competency under this regulation, CASA recommended that ‘pilots should seek advice and consider refresher training or practice before commencing an operation they haven’t carried out for a while’. Although the pilot is already licenced and current on the class of aircraft, training for general competency can only be given by a pilot who holds an instructor rating and appropriate training endorsements.
The check flight briefing (see the section titled Check flight sequences) prepared for the flight had a series of questions at the end of the briefing for the inductee pilot to answer, consistent with the areas of competency identified above. Additionally, the practice flight conducted by the two pilots the week prior was an opportunity to practice the handling skills in this aircraft rather than other aircraft flown by each of the pilots.
Operational proficiency check
A proficiency check is ‘an assessment of your skills and knowledge in a particular operational area. Pilots are required to undertake proficiency checks to ensure they continue to be competent conducting particular kinds of operations’ (CASA Proficiency checks information sheet, 2018). CASA recognises that skill decay occurs over time, and that these checks are an on-going measure to ensure that the licence competencies specified in the CASR Part 61 Manual of Standards continue to be met (see the section titled Skill decay).
Operational proficiency checks are carried out by an operator and may also include the elements required for an instrument proficiency check (IPC), provided the check pilot is authorised to conduct both types of check. The chief pilot in this case was being checked only for approval to conduct OPCs. Operational proficiency checks can only be conducted on pilots employed by that company.
Operating under Civil Aviation Regulations 1988 (CAR) Regulation 217 (see the section titled Organisational structure) Rossair pilots had to pass two proficiency checks per year (listed in the operations manual as alternating between an IPC and OPC), with at least four months between checks, in order to exercise the associated privilege. As the inductee pilot was re-joining the operator, this was his first OPC in the Cessna 441 in over three years. The chief pilot had completed an:
- OPC in the Cessna 441 in April 2016 in the left seat, and in May 2016 from the right seat, as part of his Cessna 441 check pilot training
- IPC in the EMB 120 in October 2016, and an OPC in the EMB 120 simulator in February 2017.
This met the regulatory and operator requirements for proficiency checking, but did not permit assessment of the chief pilot’s on-going competency in the particular area of single pilot operations.
Practice engine failure after take‑off check requirements
The chief pilot was the pilot primarily being checked during the flight and he had to conduct the inductee pilot’s operational proficiency check in line with the company procedure to be approved as a check pilot.
When a proficiency check is conducted under a CAR 217 approval, the exercises conducted are set by the CAR 217 holder rather than CASA. The Rossair operations manual Part C stated that proficiency checks were to be conducted in accordance with their own check assessment form and the CASA instrument proficiency check form. The company guidance was for check pilots to reference the section of the CASR Part 61 manual of standards for the instrument rating flight test.
When an operator proficiency check is conducted without an instrument proficiency check, there is no CASA requirement for the candidate to demonstrate management of a simulated engine failure after take-off. The Rossair check assessment form however, had a required flight component to ’deal with a simulated engine emergency after take-off requiring an immediate re-landing’.
There are a number of CASA checks which require demonstration of an engine failure after take‑off in a multi-engine aircraft, both for initial issue of a licence or endorsement and during specific types of proficiency checks. The wording of the specified activity varies slightly between checks, for example ’conduct instrument departure (one engine inoperative)’ for the multi-engine class rating; or ’manage an engine failure after take-off (simulated)’ in the multi-engine class rating.
While the wording varied, the competencies are all similar in intent: requiring the pilot to manage the simulated failure while maintaining the aircraft within specified tolerances; and configuring and flying the aircraft to achieve the best performance.
While the manual of standards does not specify a height at which these activities should be conducted, CAAP guidance stated that they should not be conducted below 400 ft above ground level. The requirement of managing an engine failure during an instrument departure or after take‑off, could be interpreted as meaning that these activities should to be conducted at low altitude. However, there was no direct comment in any CASA guidance that this is required.
The flight
Background
The chief pilot’s approval instrument had a conditional requirement that an additional pilot had to be either employed or contracted to Rossair as a fleet manager on the Cessna 441 (see the section titled Organisational structure). Due to an unexpected temporary loss of his medical approval, the fleet manager became unable to conduct flying duties for Rossair, and was therefore unable to fulfil the full fleet manager role, which included check flight responsibilities.
To resolve this issue, the chief pilot wrote to CASA to request a variation to his chief pilot instrument of approval, to remove the requirement for a Cessna 441 fleet manager. It was intended that the fleet manager would continue in an administrative fleet manager role, and a contract Cessna 441 pilot would be used for on-going check and training responsibilities, with the chief pilot maintaining oversight responsibilities only. The proposed contract pilot was known to CASA, and had been given permission to carry out two OPC checks for Rossair in April 2017 while there was no company check pilot.
In response to this request, CASA proposed that the chief pilot should be checked in the aircraft conducting an OPC on a company pilot. This check would give the chief pilot approval to conduct OPCs and line checks. The approval would then allow him to undertake the Rossair induction process with the contract Cessna 441 pilot, before the contract pilot began all checks on company pilots.
Check flight sequences
The chief pilot developed an electronic briefing, in preparation for the occurrence check flight, which included specific detail of the ground and flight components to be conducted. The briefing detailed the following two flight exercises:
Flight exercise #1
• Normal departure via SID [standard instrument departure from Adelaide Airport]
• Fly to
• Holding pattern, engine failure
- Conduct memory items then checklist
- Radio calls, passenger brief
• RNAV approach
- Single engine
• Visual then go around on final
- Single engine
• Single engine circuit and landing
Flight exercise #2
• Normal take-off [from Renmark Airport]
- Engine failure above 400’
› Conduct memory items and checklists
› On base,[14] engine will be restored
- Climb to 8000’
- Steep turns
- Partial panel
- Stall
› Clean
› Approach configuration
- Two engine instrument approach at Adelaide.
While the pre-check briefing was not witnessed by anyone other than the participants, surveillance data and radio transmissions indicated the accident flight was conducted as per the briefed flight exercises, except that no single‑engine go around was performed on arrival at Renmark. An observer on board the aircraft during the preparatory practice flight the week before reported that the briefed sequences, including a practice engine failure after take‑off from Renmark Airport, were undertaken.
With regard to that sequence, the second flight exercise detailed that following a normal take‑off and simulated engine failure above 400 ft above ground level, ‘memory items and checklists’ were to be conducted. These memory items, also known as ‘phase one’ checks, were detailed in the company operations manual for the Cessna 441 as follows:
| 1. Engine power | ADJUST as required |
| 2. Inoperative engine | DETERMINE |
| a. Condition lever | EMERGENCY SHUT OFF |
| b. Firewall shut of | PUSH to close |
| 3. Landing gear | UP |
| 4. Flaps | UP above 115 knots |
The memory checks duplicated the initial response actions detailed in the POH checklist for an engine failure above the minimum control airspeed, VMCA (see the section titled Asymmetric flight) (Figure 16).
Figure 16: POH engine failure checklist
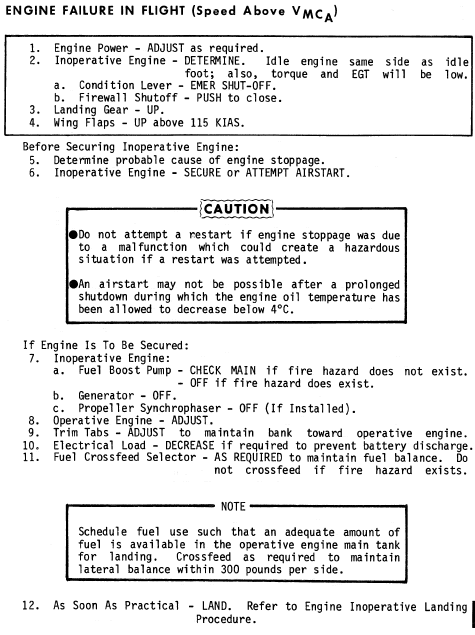
Source: Cessna 441 Pilot’s operating handbook
In the event of an actual engine failure, the briefing detailed that the ‘[inductee] Pilot is to continue operating the aircraft unless the instructor [check pilot] elects to take over with the phrase “Taking Over”.’ and that the check would then be terminated and the aircraft landed at an appropriate airport.
The briefing also outlined the following process for transitioning control of the aircraft between the chief pilot and inductee pilot:
• Control over aircraft is to be conducted with the “handing over, taking over” phrase.
• If at any time, the instructor announces “taking over”, the pilot shall:
- Remove hands and feet from all controls’
- Respond “handing over”.
• To pass control of aircraft to pilot, instructor shall announce “handing over”. The pilot shall:
- Place hands and feet on the controls,
- Respond “taking over”,
- Be responsible for operation of the aircraft.
The briefing also specified the required test flight tolerances from the Civil Aviation Safety Regulations 1998 Part 61 Manual of Standards, including for asymmetric flight (Figure 17). In detailing the objectives of the proficiency check, with regard to flight tolerances the briefing also stated:
“a sustained deviation outside of the applicable flight tolerance is not permitted”.
Figure 17: Required flight accuracy tolerances

Source: Rossair
Carriage of passengers during practice emergency procedures
Regulation 249 of the Civil Aviation Regulations 1988 prohibited the carriage of passengers on board an aircraft during the practice of emergency procedures, such as simulated engine failures. CASA issued exemption EX74/15 which, under certain circumstances, permitted a passenger to be carried if the pilot in command - being either a check pilot, approved testing officer of flight examiner - carried out a proficiency check or flight test on another pilot. This exemption permitted the chief pilot to be carried as an observer on three check flights during his Cessna 441 check pilot training (see the section titled Check pilot training).
The exemption at the time did not explicitly refer to carriage of CASA FOIs, outside permitting them to be carried during their training in connection to become a flight examiner or inspector. Following this accident, CASA issued exemption EX58/19 – Carriage of passengers on proficiency check and flight test flight instrument 2019 - which clarified the previous exemption, clearly stating that a CASA officer could be carried as a passenger for duties directly relating to the conduct of the flight test or proficiency check. The explanatory statement for this exemption stated ’the pilot in command must ensure that the passenger does not interfere with the conduct of the proficiency check of flight test. The passenger must not occupy a control seat’.
Flying operations inspector seated in non-control seat
During the accident flight, two checks were being conducted simultaneously – the OPC on the inductee pilot, and the check pilot approval on the chief pilot. Therefore, the CASA FOI was not occupying a control seat for the flight.
The CASA flying qualification and training handbook (2016) stated the conditions with which a CASA FOI may sit in an observation seat:
A CASA inspector may conduct an assessment from an observation seat where that seat is in the immediate vicinity of the operating crew (e.g. a jump seat). The observation seat must have a reasonably unrestricted view of the flight crew and instrumentation.
Where an assessment from an observation seat occurs, suitable communication facilities must exist to permit the inspector to both monitor and communicate with the flight crew.
Where an inspector has a general exposure level of capability and is conducting an assessment from an observation seat, the inspector must have sufficient general exposure to ascertain that the operational activity is being planned and conducted safely and within the performance capabilities of the aircraft; and the competency of the person(s) being observed.
When making an assessment from an observation seat, the inspector must ensure (prior to flight) that the person acting as pilot in command is qualified and meets recency requirements (i.e. is qualified and proficient to conduct the activity required)
When conducting an inflight assessment a CASA inspector must wear a seatbelt where required by the regulations to do so.
A CASA inspector conducting an assessment from an observation seat shall conduct a pre-flight brief.
There is no jump seat[15] in a Cessna 441 aircraft, so the CASA FOI sat in the first row passenger seat, on the left side of the aircraft, behind the inductee pilot (Figure 18). From the seated position, he should have had some visibility of the chief pilot, and the controls and instruments, but was not likely to be able to read the instruments precisely.
Figure 18: Exemplar Cessna 441 in a similar configuration to the accident aircraft

Source: Rossair, annotated by ATSB
The aircraft intercommunication system did not allow the FOI to share communications or monitor exchanges between the pilots via headset. A briefing sheet found in the FOI’s documents indicated that if he had a safety concern he would tap the chief pilot on the shoulder, with the chief pilot responding when ready. While the noise within the aircraft is relatively high, it was reportedly not prohibitive to communication. However, as both of the other pilots were using headsets, this may have affected their ability to hear any verbal intervention by the FOI. Additionally, the volume of any spoken communication between the inductee and chief pilot would not have taken account of the ambient cabin noise and that may have increased the difficulty for the FOI to monitor communication between them.
Reports from other Cessna 441 pilots indicated that it was not unusual to have an FOI or other check pilot sitting in the front row passenger seat. This was the same seating positions as the practice flight conducted by the inductee pilot and chief pilot, along with the former Cessna 441 company check pilot, the week prior.
The FOI likely knew that the two pilots had conducted a practice flight the week before the test flight, and therefore considered that they were prepared for the planned flight. The practice flight and the planned flight were relatively similar, with the main difference between the flights being the presence of the FOI rather than the former Rossair Cessna 441 check pilot.
Of the three occupants, the CASA FOI had the most experience on the Cessna 441 overall, both in flying and in a check pilot role. He was the pilot on board with the most recent operational proficiency check in the aircraft type, albeit not with the most recent operational experience. In the investigation into the in-flight uncontained engine failure of QF32 in 2010 (ATSB report AO-2010-089), it was stated ’the additional flight crew that were present on the flight deck during the accident flight were resources available to provide support to the primary flight crew of the captain and the first officer...’. While the set-up of this flight was different from that on QF32, the FOI was an available resource knowledgeable about the aircraft type, had a problem arisen with the aircraft.
Following this accident, CASA issued an exemption instrument EX83/18 – Occupation of flight control seat (certain flight instruction and examination activities) Exemption 2018 - which permitted the FOI to conduct the flight examination activity while not occupying a control seat, as each of the pilots in the control seats were licenced to fly the Cessna 441. Some points in this exemption were:
- In relation to a flight in an aircraft that is not a single-place aircraft, an authorisation holder conducting a relevant flight examiner activity, when occupying a seat that is not a flight control seat:
- Must be located at a place on the aircraft that enables the authorisation holder to observe all the matters to be demonstrated by each flight crew member occupying a flight control seat; and
- Must not manipulate any aircraft control or system accessible from a flight control seat
- An authorisation holder conducting a relevant simulator instructor activity or a relevant flight examiner activity, when not occupying a flight control seat must ensure that at all times during the activity they can:
- Monitor flight crew member use of radio communications systems; and
- Maintain 2-way communications with the flight crew members.
Cessna 441 simulator
At the time of writing, there was no Cessna 441 simulator in Australia, or any foreign Cessna 441 simulator approved by CASA for use by Australian pilots.
In assessing the availability of simulators in Australia, the only CASA-approved simulator which fell into the same multi-engine class rating as the Cessna 441 was the King Air B200 simulator. However, as the B200 is another aircraft like the Cessna 441 which requires an initial type rating (under Part 61 Schedule 13) before it becomes covered by the multi-engine aircraft class rating, it cannot be used directly without training. Additionally, there are significant differences with the B200 aircraft such as auto-feathering (compared to the Cessna 441 negative torque sensing system) and rudder boost. Those differences may affect the training effectiveness between the aircraft types and introduce an adverse response to an emergency situation.
In February 2020, CASA identified the absence of an available simulator as a factor which increased risk in this accident.
Check pilot training
Role of a check pilot
A check pilot is defined by Civil Aviation Orders 82.0 as ‘a person approved by CASA to conduct flight training and proficiency checks’. A check pilot approval is the company equivalent of a flight examiner operating under the CASR Part 61 regulations. Part C of the Rossair operations manual required company check pilots to meet the same standards as flight examiners.
Under CASR Part 61 flight examiners must hold a flight instructor rating, whereas under CAR 217 (see the section titled Organisational structure) – ‘a pilot may conduct tests or checks for the purposes of an approved training and checking organisation without being the holder of a flight instructor rating’. This means that a company check pilot is not required to demonstrate the same skills in instructing as a flight examiner, but they are expected to have similar competencies.
The reason for this difference is that ‘the primary role of the CAR 217 organisation is the maintenance of competency for flight crew members’ (CASA CAAP 217, 2015), rather than the initial issue of a rating or endorsement for flight crew. In this case, all pilots on board held, or had held, some level of instructor rating.
The chief pilot’s check pilot training
The Rossair manual stated the phases required in the training of a check pilot:
1. Flight training in the handling of engine failures and other emergencies while operating from the right hand seat. The training/check pilot undergoing training shall reach a standard whereby he/she can safely handle engine and propeller malfunctions while in the right hand seat
2. A minimum of 6 line flights (sectors) under the supervision of the check pilot. 2 sectors shall be operated with the training/check pilot under training in the left hand seat and 4 sectors with him/her in the right hand seat. The training/check pilot under training shall reach a standard whereby he/she can adequately demonstrate normal line flying techniques from either seat/
3. Receipt of a thorough briefing from the nominated check pilot or the chief pilot on all aspects of training and checking on the particular aircraft type
4. Ground and flight training in the methods of simulating engine failures including the assessment of a student’s performance following a simulate engine failure and control of student errors.
The training / check pilot under training shall be able to satisfactorily demonstrate from the right hand seat, the following:
- Rejected take-off
- Engine failure after take-off
- Single engine circuit and landing
- Singe engine circling approach
- Singe engine missed approach
5. Pass a type specific proficiency check from the right hand seat.
The chief pilot underwent training as a check pilot on the Cessna 441 during April and May 2016. Training records confirmed that he completed all training in accordance with the operations manual procedure. Comment made on the training records indicated the chief pilot achieved a ‘high standard with simulated engine failures’.
At the time, the intention of this training was not for the chief pilot to become a main Cessna 441 check pilot, but rather to be a secondary check pilot available to check the primary Cessna 441 check pilot. This is a recommended practice, included in the CASA Air Operator’s Certificate handbook (Volume 2 – Flying operations) as it is the minimum number which allows each pilot to maintain competency checks.
CASA recognised the training the pilot undertook as sufficient for undertaking an assessment to conduct OPCs. As confirmed by CASA to the chief pilot via email prior to the flight, approval to conduct IPCs would require a separate approval under CASR Part 61.040, which would need to be applied for and assessed separately.
The chief pilot submitted his self-recommendation for CASA assessment as a Cessna 441 check pilot, on 30 May 2016. This recommendation was not formally assessed at the time of submission (see the section titled Regulatory services processes).
CASA observations of the chief pilot’s flying
In June 2016, the same CASA FOI was on board the aircraft with the chief pilot and the Cessna 441 fleet manager, for the fleet manager’s OPC. This was listed in the CASA regulatory services records for Rossair. The proficiency check paperwork for the fleet manager was completed by the chief pilot, listing himself as check captain. The CASA FOI also made observational comments and signed the document. Flight and duty records indicate that the chief pilot and the fleet manager were in the two control seats for the flight. However, there is no indication that the FOI reviewed or assessed the chief pilots check pilot skills at this time.
The chief pilot was also recommended by the EMB 120 fleet manager as competent in the check pilot role in January 2017. Unlike the Cessna 441 recommendation in May 2016, this recommendation accompanied an official request for regulatory approval from CASA.
While not being an official assessment by CASA, a CASA FOI observed the chief pilot completing an OPC in the EMB 120 simulator in February 2017. The chief pilot passed the OPC, however the CASA FOI raised a concern with another CASA staff member and the chief pilot about his performance, which was considered below his previous observed performance, and not of a suitable standard to monitor and assess a trainee candidate. The FOI expressed the opinion that the known high workload of the chief pilot was affecting his personal flying skills and potentially his ability in the assessor role.
The accident assessment flight was reported by CASA to also be a follow up observation of the chief pilot’s performance.
Time period between training and assessment
In Australia there is no limit on the elapsed time between a pilot being trained in an activity, and testing for licencing in that activity. For the chief pilot, there was a year between his assessment by the fleet manager as ready for assessment, and when the assessment with CASA occurred. He had not completed any more Cessna 441 check pilot specific training in this time. The chief pilot completed two flights as a check pilot in the year since being judged ready for assessment (Cessna 441 fleet manager’s OPC and a line check) and the practice test flight the week prior. All other flying he conducted in the Cessna 441 was in the role of line pilot, and conducted as single pilot operations.
By contrast, in the United Kingdom, pilots being assessed for class, type, instrument rating, or proficiency checks in single pilot aircraft must complete their skills test ’within a period of 6 months preceding the application for the issue of the class or type rating training course and with a period of 6 months preceding the application for the issue of the class or type rating’ (CAA, 2014).
As part of the temporary management instruction issued after the accident (see the section titled Safety issues and actions) CASA implemented a 28 day maximum between the recommendation for checking post training and checking.
Skill decay
The CASA CAAP 5.23-1(2) (see the section titled Regulatory information) stated:
Any pilot qualified to operate a multi-engine aircraft may shutdown an engine in flight. However, CASA strongly recommends that this only be done with a qualified flight instructor present, as there is a likelihood for errors and engine mismanagement. Flight instructors regularly practice this procedure and are less likely to cause problems
Furthermore, the CAAP added that:
Recency may not be an issue for a pilot who is operating a multi-engine aeroplane on a regular basis and receives ongoing training, but could be a significant problem for a pilot who flies infrequently, or has not practiced asymmetric operations in recent time.
Other than during the practice flight the week prior, the inductee pilot had not managed an engine failure in the Cessna 441 in over two and a half years, and the chief pilot had not had the opportunity to set an engine failure in almost a year. It is unclear from the chief pilot’s training records if he had ever been required to demonstrate a recovery from a mishandled engine failure after take‑off in a Cessna 441.
The Cessna 441 check pilot observer who was present on the practice flight the week before described that flight as ‘messy’, with the inductee pilot appearing to be ‘rusty’. Specifically he recalled that the inductee:
- had to make reference to the checklist as he was unfamiliar with the memory items and was therefore ‘well behind’ the aircraft
- adopted a steep pitch attitude that resulted in a lower than normal climb airspeed.
The observer further advised that there were also omissions by the chief pilot during the flight including that the:
- pre-flight briefing did not cover the procedure for transferring control of the aircraft between the two pilots
- incorrect use of the engine anti‑ice system was not identified.
He also stated that the practice engine failure simulation after take‑off from Renmark was ‘quite safe’ and that he debriefed both pilots on his observations.
Previous ATSB reports, such as the 2011 VFR flight into dark night involving an Aérospatiale, AS355F2 (Twin Squirrel) helicopter VH-NTV (ATSB report AO-2011-102), have identified the risk that limited recent experience can have on a pilot’s performance. Limitations in experience can relate to both total hours, and exposure to a particular exercise.
Arthur et al (1998) defined skill decay as ’the loss or decay of trained or acquired skills (or knowledge) after periods of non-use. Skill decay is particularly salient and problematic in situations where individuals receive training on knowledge and skills that they may not be required to use or exercise for extended periods of time’. Their research identified that there is a negative relation between skill retention and the length of non-use, starting from the day of training, and with participants showing a 92 per cent reduction in performance when there are more than 365 days between training and performing the skill again.
Research studies have identified a variety of factors which can affect skill retention. There is a general consensus that skill-retention is generally better for perceptual-motor skills than for procedural tasks, or tasks that require a sequence of steps to be completed.
Wreckage and impact information
Accident site
Examination of tree damage, ground scars and damage to the aircraft identified that the aircraft collided with terrain in an inverted near‑vertical attitude. Following the initial impact the aircraft travelled a further 20 meters in a west-north-westerly direction (Figure 19). All of the major aircraft components were accounted for at the accident site, indicating that an in‑flight structural failure of the aircraft or its components did not occur.
First responders reported a strong smell of fuel and evidence of extensive fuel soaked soil was found on-site consistent with a significant amount of fuel on board the aircraft.
Aircraft wreckage
The aircraft was destroyed as a result of the ground collision. There was no subsequent fire, however, damage to the aircraft precluded a complete examination of a number of the aircraft systems. On-site examination of the wreckage and later examination of recovered components did not identify any pre-impact faults that could have contributed to the accident.
Figure 19: Accident site and wreckage of VH-XMJ

Source: News Corp Australia, annotated by the ATSB.
Flap and undercarriage
The landing gear and flaps were found to have been in the retracted position at impact. Due to the disruption to the cockpit the ATSB was unable to determine the position of the flap and landing gear selector levers and position indicators.
Flight controls
A complete examination of the flight control systems was not possible due to the extent of the damage to the aircraft. However, the majority of the components were able to be examined in detail and no pre-impact defects were noted that could have contributed to the accident.
Rudder trim
The rudder trim actuator screw jack was found in a slightly over extended position which equated to a full nose‑left trim position. The actuator displayed evidence of having been alternately driven toward the retracted and extended positions by impact forces. The ATSB could not determine the extent to which impact forces affected the screw jack’s pre-impact position.
The rudder trim indicator was found in the full nose left position. Although it is possible that impact forces may have affected the position of the indicator, it was considered that crushing, evident in the cockpit area probably captured the indicator in its pre-impact position.
On balance, the evidence supported the rudder trim being in the full nose‑left position at impact. That position was consistent with pilot response to a simulated failure of the right engine.
Engines
Both engines were recovered from the accident site and sent to the engine manufacturer for examination. Following disassembly and examination under the supervision of the United States National Transportation Safety Board (NTSB) it was determined that both engines were operating prior to impact with terrain. The power output of each engine could not be established however, no defects were found that would have prevented normal operation.
Engine components
The aircraft’s fuel control units, electronic engine control units and propeller governors were inspected and, where possible, tested by the units’ manufacturer or approved facility under the supervision of the ATSB, NTSB or the United States Federal Aviation Administration. Those examinations did not identify any pre-impact faults that would have prevented normal engine operation.
Propellers
Both propellers were disassembled and examined by the ATSB. Assistance in interpreting the damage was provided by a Hartzell Propeller accident investigator. Damage to the propeller assembly was found to be consistent with both engines operating at comparable low power settings prior to impact with terrain. No defects were found that would have precluded normal operation.
Aircraft instruments
Instruments recovered from the accident site were examined in an attempt to determine their position at impact from contact marks between moveable and fixed parts of the instruments. Most of the instruments did not retain reliable information, however, the following instruments had contact marks indicating:
- engine revolutions per minute indicator at 94 per cent
- engine torque indicator at 50 ft.lbs
- exhaust gas temperature (EGT) indicator at 450° Celsius.
Due to the disruption of the aircraft instrument panel it was not possible to determine which engine/s these gauges had been monitoring. However, with respect to the last two gauges, it is not possible for an engine to be operating simultaneously at such a high EGT and close to minimum torque. As such, either those two instruments were from different, unidentifiable engines or the contact marks were unreliable. In either case, they did not assist in the assessment of likely engine power levels.
Medical and pathological information
Due to the estimated airspeed and angle of impact with the ground following the loss of control, the accident was not considered survivable.
Autopsies were conducted on all three pilots on the flight. There were no medical conditions of note identified in either the chief pilot or the CASA FOI.
The autopsy conducted on the inductee pilot identified evidence of coronary artery disease, however did not note any change associated with a heart attack.
The inductee pilot’s autopsy report also referenced an audiologist’s report from January 2017 in which it was noted that he had hearing loss, with a referral to a hearing specialist recommended. This was also noted during his aviation medical examination in December 2016, and while follow‑up specialist examination was required, the inductee pilot was assessed as fit to exercise the privilege of his licence.
It was not possible to discount the possibility of a temporary medical event affecting the pilots’ response to handling the simulated engine failure.
Organisational information
Overview of the operator
Rossair, based in Adelaide, had operated continually since 1963, making it Australia’s second oldest air operator. Over many years it primarily conducted ad hoc passenger charter operations using Cessna 441 aircraft.
In 2011, Adelaide Equity Partners purchased Rossair, which at that time operated five Cessna 441 aircraft. The owners and managers in Rossair were interested in expanding to operate larger aircraft, and in 2013 the owners purchased Air South, another Adelaide-based operator. Air South operated two Beechcraft 1900 (19 seat, two pilot turboprop, greater than 5,700 kg maximum take‑off weight) aircraft and a Beechcraft King Air B200 (9 seat, single pilot turboprop) aircraft. Air South had a contract to conduct flights for a resources company using the Beechcraft 1900 aircraft, and Rossair had also acquired a similar contract using Cessna 441 aircraft.
Soon after the two operations were merged under the Air South air operator’s certificate (AOC). This involved integrating Rossair’s Cessna 441 operations into the Air South operations manual. During 2014, the combined operator obtained approval to operate the Embraer EMB 120 (30 seat, two-pilot turboprop) aircraft to fulfil a new contract. The EMB 120 required a cabin crew member and flight crew training and checking to be conducted in a simulator.
The AOC was reissued to AE Charter Services, operating both as Rossair Charter and Air South Charter, in July 2015 until the end of August 2018. It authorised passenger and cargo charter operations in Australia using Cessna 441, EMB 120, Beechcraft 1900, Beechcraft King Air B200 and Cessna 402/421 aircraft.
During 2015, there was a significant downturn in the resources industry. Ultimately the Beechcraft 1900s were leased to a Perth-based operator, and the number of serviceable aircraft reduced to two Cessna 441 and one EMB 120, with three other Cessna 441 and another EMB 120 still owned by the operator but requiring significant maintenance to be able to return to operations.
In late 2016, the operator was awarded multiple new contracts. According to the chief executive officer (CEO), at that time it did not have sufficient serviceable aircraft and pilots to conduct all the work, and it therefore had to cross-hire aircraft from other operators.
The owners of the operator also acquired a Perth-based operator, which was conducting operations under its own AOC using AE Charter’s two Beechcraft 1900 aircraft, and conducting operations on behalf of AE Charter. In February 2017, the operator applied for an AOC variation to integrate the Perth-based operation into the AE Charter AOC, but as of the end of May 2017 this variation had not been approved.
As of May 2017, the operator’s business focused primarily on fly-in-fly-out operations for the resource industry. The operator had a head office and terminal at Adelaide Airport, and also operated regularly from the nearby Parafield Airport. It owned two EMB 120 aircraft, two Beechcraft 1900 aircraft, and four Cessna 441 aircraft. However, it was still only operating two of the Cessna 441 aircraft (including VH‑XMJ) and one EMB 120, with two other Cessna 441 and one other EMB 120 aircraft still requiring maintenance and the two Beechcraft 1900s being used by the Peth-based operator.
At the time of the accident, the Cessna 441 aircraft were registered with Rossair Charter as the registered operator. The operations manuals were all under the ‘Rossair’ name, and company marketing and media reflected the use of this branding as the common use name for the operator.
The organisation also held a Certificate of Approval, in the name of Rossair Engineering, permitting limited maintenance on their aircraft. Rossair Engineering had been formed from another company which held a Certificate of Approval; the operations were based at Adelaide Airport and Parafield airports. The majority of Rossair’s aircraft maintenance for the Cessna 441 was outsourced to a third-party organisation.
Organisational structure
The Civil Aviation Act 1988 legislates the requirements around the issue of an AOC. Section 28(1) specified that CASA must be satisfied that an organisation can meet a number of requirements, including that:
The organisation has a sufficient number of suitably qualified and competent employees to conduct or carry out the AOC operations safely; and
Key personnel in the organisation have appropriate experience in air operations to conduct or carry out the AOC operations safely.
Further, section 28BF stated:
The holder of an AOC must at all times maintain an appropriate organisation, with a sufficient number of appropriately qualified personnel and a sound and effective management structure, having regard to the nature of the operations covered by the AOC.
Section 28(3) identified the key personnel for an aviation organisation as the:
• chief executive officer (CEO)
• head of flying operations (or chief pilot)
• head of aircraft airworthiness and maintenance control (HAAMC)
• head of training and checking
• any other position prescribed.
Each of these key post-holders was required to be assessed by CASA as suitable to hold the position. Civil Aviation Order (CAO) 82.1 Conditions on Air Operator’s Certificates authorising charter operations and aerial work operations also outlined additional requirements for the operator’s organisation and facilities, and CAO 82.0 Air Operators’ Certificates – applications for certificates and general requirements outlined additional requirements, particularly in regard to the role of the chief pilot.
In addition to the AOC, Rossair held an approval under Civil Aviation Regulations 1988 (CAR) regulation 217(3) to operate a training and checking organisation, in accordance with the procedures outlined in the operator’s training and checking manual. The operator was required to have a CAR 217 approval as it operated aircraft with a maximum take-off weight greater than 5,700 kg. The CAR 217 approval required the employment of check pilots, which also had to be approved by CASA.
As of May 2017, the operator had a CEO, chief pilot (who also acted as the head of training and checking), HAAMC, cabin crew manager, chief financial officer and operations manager. The chief pilot, HAAMC and cabin crew manager were responsible for the conduct of the operator’s activities, whereas the chief financial officer and operations manager were responsible for the commercial aspects of the operator. A contractor conducted the role of safety manger and quality manager on a part-time basis. All the managers reported to the CEO, who in turn reported directly to the board.
The operator had fleet managers for each aircraft type, who reported to the chief pilot (see the section titled Key personnel).
Flight and duty records for May 2017 indicated that the operator had three full-time Cessna 441 pilots, one casual Cessna 441 pilot, two full-time EMB 120 pilots and two other full-time pilots (including the chief pilot) who were primarily operating the EMB 120 but were also qualified to operate Cessna 441. In 2017, the Cessna 441 pilots were working close to maximum duty hours (see section titled Manager workloads) whereas the operator’s single EMB 120 aircraft was only conducting about 4–5 flights per week.
The operator’s personnel advised that there had been significant difficulties in obtaining additional pilots, both in terms of getting approval from the owners and also in terms of the availability of suitable pilots in the industry. As of the time of the accident, the operator had recruited two Beechcraft 1900 pilots (to be based in Adelaide) and was in the process of acquiring additional EMB 120 pilots, in addition to the inductee Cessna 441 pilot on board the accident flight.
Key personnel
Chief executive officer
The CEO at the time of the accident was approved by CASA in February 2017. The Rossair operations manual specified the role as having ’overall responsibility for the management of AE Charter and the formulating of company policy’. The CEO had previously lived in Perth, and up until the time of the accident worked two weeks a month in the Adelaide office and two weeks remotely from Perth.
The CEO reported that, since starting in the role, he had implemented a number of changes to increase organisational efficiency. He advised that he had received approval from the board for additional staffing of both pilots and office-based staff to facilitate the growth. He also advised that the operator’s aim was to move resources from the smaller Cessna 441 operations into the larger Beechcraft 1900 and EMB 120 operations. This plan had not been actioned at the time of the accident.
Some former Rossair personnel advised that the directors often directly interacted with personnel other than the CEO over the years, which had been problematic for some former managers. However, the CEO appointed in February 2017 advised that he had made it clear that the directors were to communicate with him on all operational matters, and other personnel advised that they had minimal interaction with the directors during 2017.
Chief pilot
CAO 82.0 listed the responsibilities of a chief pilot as follows:
The Chief Pilot for an operator is to have control of all flight crew training and operational matters affecting the safety of the flying operations of the operator.
The responsibilities of a Chief Pilot must, unless CASA otherwise specifies in writing, include the following responsibilities:
a) ensuring that the operator’s air operations are conducted in compliance with the Act, the Civil Aviation Regulations 1988, the Civil Aviation Regulations 1998 and the Civil Aviation Orders;
b) arranging flight crew rosters;
c) maintaining a record of licences, ratings, and route qualifications held by each flight crew member, including:
(i) validity; and
(ii) recency; and
(iii) type endorsements and any applicable licence restrictions;
d) maintaining a system to record flight crew duty and flight times to ensure compliance with duty and flight time limitations in accordance with Part 48 of the Orders;
e) ensuring compliance with loading procedures specified for each aircraft type used by the operator and proper compilation of loading documents, including passenger and cargo manifests;
f) monitoring operational standards, maintaining training records and supervising the training and checking of flight crew of the operator;
g) conducting proficiency tests in the execution of emergency procedures and issuing certificates of proficiency as required by section 20.11;
h) training flight crew in the acceptance and handling of dangerous goods as required by the Civil Aviation Regulations 1988 or the Orders;
i) maintaining a complete and up-to-date reference library of operational documents as required by CASA for the class of operations conducted;
j) allocating appropriate aircraft.
The Rossair operations manual described the role of the head of flying operations, or chief pilot, as ‘a full time management position with a component of line flying duties in order to maintain competency and currency on the most complex company aircraft type.’
The chief pilot started at Rossair in late 2015 and CASA issued his chief pilot approval instrument in January 2016. This was his first chief pilot role. Although meeting all the experience requirements to be chief pilot under CAO 82.0 Appendix 1, CASA placed a condition on his approval instrument that a fleet manager was to be appointed for each type of aircraft the company operated. CASA identified that this was due to the chief pilot not having a Beechcraft 1900 type rating, limited EMB 120 experience, and no substantial recent experience on the Cessna 441.
The operator’s previous permanent chief pilot (and previous chief pilot of Air South) resigned from the operator in mid-2015. At that time, the EMB 120 fleet manager, who was a contract check pilot, acted as chief pilot until a new permanent chief pilot could be appointed.
Head of training and checking
The role of the head of training and checking was defined in the operations manual as follows:
The Head of Training and Checking is the nominated head of the training and checking organisation in accordance with CAR 217 and CAO 82.1 and is a member of the Safety/Management committee.
The head of training and checking is required to monitor general flying standards, supervise route familiarisations, ensure compliance with operating procedures and techniques and ensure that all records for each training or check are completed promptly and accurately and placed in the pilot’s file. Appropriate advice must be given to the chief pilot as required.
In organisations operating under CAO 82.1, and with a CAR 217 approval, the chief pilot is also the head of training and checking. In addition to the experience requirements to become a chief pilot, the CASA AOC handbook volume 2 (2016) stated that, if the chief pilot is to hold both roles, the chief pilot should also have, or demonstrate the equivalent of:
- 1000 hours flight time in operations substantially similar to those proposed
- 500 hours in command of aircraft of a type substantially similar to the major type of aircraft proposed to be operated
- 12 months experience as a check pilot in operations substantially similar to those proposed.
However, the CASA guidance contained within the AOC handbook also stated:
If the operator is of a size that would cause high workload for one person, CASA should encourage or require to operator to appoint a separate person to the head of training and checking position.
The chief pilot did not have any prior experience as a check pilot, or formally hold any check pilot approvals, and therefore did not meet the recommended requirements to hold the head of training and checking role. As these were recommended requirements only, this did not prevent him from holding the role, as long as CASA made an assessment and assessed him as suitable given any other control measures imposed.
CAO 82.0 stated that:
A Chief Pilot, in exercising any responsibility, may delegate duties to other members of the operator’s staff, but may not delegate training and checking duties without the written approval of CASA.
There was evidence in internal Rossair paperwork naming the EMB 120 fleet manager as the head of training and checking, and a CASA document in November 2015 indicated that ‘new chief pilot candidate to be interviewed shortly, but with current temporary chief pilot being retained as the head of training and checking’ (see the section titled Key personnel). However, no instrument approving a specific or separate head of training and checking to Rossair could be located by CASA following the accident. Therefore, according to CASA’s post-accident assessment, the chief pilot was filling the role of both the chief pilot and the head of training and checking.
Fleet managers
The requirement for fleet managers was a method used by CASA, and the operator, to manage the chief pilot’s limited check pilot and aircraft type experience, while he gained that experience with the operator. The use of nominated fleet managers or similar appointments on a chief pilot’s approval instrument was not uncommon.
The responsibilities listed for the fleet managers in the operations manual were:
- Ensuring that air operations undertaken are conducted safely and in compliance with the Company operations manual and regulatory legislation applicable to the aircraft fleet
- Provision of advice to the chief pilot on specific fleet operations and AOC matters
- Briefing the CEO on all incidents, accidents and surveillance reports, along with proposed corrective actions, as applicable to the fleet
- Conduct research, as directed by the chief pilot on existing and future flight crew procedures, aircraft equipment and systems development to enhance operational safety and efficiency.
The Cessna 441 fleet manager listed on the chief pilot’s instrument from January 2016 until the time of the accident was a permanent employee of the operator. He was previously the chief pilot and head of training and checking for Rossair prior to the merger with Air South, and had considerable check pilot experience on the Cessna 441 aircraft.
The fleet manager conducted all the operator proficiency checks (OPCs) and instrument proficiency checks (IPCs) for the operator’s Cessna 441 pilots, as well as conducting line flying for the operator, until mid-April 2017 (he was also acting operations manager between March and April 2017). At that time he developed a medical condition, which meant he temporarily lost his medical certificate and was unable to exercise the privileges of his licence for 12 months. He continued to work for the operator in an administrative role to support the chief pilot.
The EMB 120 fleet manager named on the chief pilot’s instrument was a contractor who did not conduct line flying for the operator. He had assisted the operator getting the EMB 120 onto its AOC, and conducted all of the training and checking for the operator’s EMB 120 flights. He had also acted in the position of chief pilot (and head of training and checking) for several months up until January 2016, during which time he conducted line flights for the operator.
The Beechcraft 1900 check pilot listed on the chief pilot’s instrument was a contractor check pilot. However, because the operator had ceased operating its Beechcraft 1900 aircraft, he had not conducted any work for the operator after the chief pilot commenced in January 2016. A new Beechcraft 1900 fleet manager was to be assessed and appointed to support the integration of the Perth-based operator into Rossair during 2017.
Each of the fleet managers was an approved check pilot, capable of conducting OPCs and IPCs on the pilots in their fleet. CASA recommended in its AOC Handbook Volume 2 that ‘the minimum number of check pilots acceptable to CASA would generally be two, as this will allow each check pilot to maintain competency.’ There were no other instructor, check, or supervisory pilots on any of the fleets, other than the fleet managers. Check pilot redundancy was not needed on the EMB 120 fleet, where the fleet manager was a contractor pilot, but was needed for the Cessna 441 fleet. It was for this reason the chief pilot initially underwent training to be a Cessna 441 check pilot in April and May 2016 (see section titled Check pilot training), so that he could conduct OPCs on the Cessna 441 fleet manager.
Head of aircraft airworthiness and maintenance control
The HAAMC was defined in the operations manual as the person ‘with the responsibility for all airworthiness matters relating to aircraft operated by the company’.
More specifically, the HAAMC’s responsibilities listed in the operations manual were:
- Supervision of the maintenance co-ordinator who carries out our compliance with airworthiness directives
- Investigation and reporting of defects
- Monitoring the continued effectiveness of the aircraft’s maintenance program
- Monitoring and assessment of aircraft trends
- Engaging and monitoring the performance of the nominated maintenance provider
- Maintenance and security of aircraft and aircraft component records
- Liaising with CASA and complying with CASA directions.
The HAAMC was appointed in October 2015, but had worked for Rossair previously in a variety of roles, including HAAMC and CEO. The HAAMC was also filling the roles of maintenance controller and technical records controller, as well working as a licenced aircraft maintenance engineer (LAME) operating under the Rossair Engineering Certificate of Approval. The HAAMC was nominated as deputy CEO to perform that role on an ad hoc basis if the CEO was away.
The HAAMC worked with one other LAME employed by Rossair Engineering, as well as in close liaison with the third party maintenance providers used for on-going maintenance on the EMB 120 and Cessna 441 aircraft.
Cabin crew manager
The cabin crew manager was responsible for training and standardisation of the cabin crew for the EMB 120 fleet. The current cabin crew manager was appointed in December 2015, and at the time of the accident the operator had two other cabin crew members in addition to the cabin crew manager.
The responsibility for the training of all flight and cabin crew in CAO 20.11 Emergency and life saving equipment and passenger control in emergencies training lies with the chief pilot. However, this training can be delegated, with the approval of CASA. This occurred in April 2016, with the cabin crew manager receiving approval after an initial assessment and operational line check.
The cabin crew manager reported that during her time with the operator her role had expanded from a cabin crew management role to also include operational and business development roles.
Organisational change
In the four years since the 2013 merger, there was almost a complete staff turnover, including:
- three CEOs (last appointed February 2017)
- three chief pilots (last appointed January 2016)
- two cabin crew managers (last appointed April 2016)
- new HAAMC (last appointed October 2015)
- multiple people in the chief financial officer and operations manager roles (with the last appointed in 2017)
- numerous pilot and cabin crew changes.
The biggest change to operations during this time was the introduction of the EMB 120 fleet, and fleet rationalisation, by ceasing operations on smaller piston aircraft and focusing on the three aircraft types owned.
Table 2 outlines some of the important events that occurred following the employment of the chief pilot.
Table 2: Overview of changes in the operator's organisation and activities following recruitment of the chief pilot
| Date | Event |
| August 2015 | Chief pilot application submitted to CASA. |
| October 2015 | Chief pilot cleared through company induction and checked to line on EMB 120. |
| November 2015 | First chief pilot interview conducted with CASA (unsuccessful). |
| January 2016 | Second chief pilot interview conducted (successful), check flight conducted and chief pilot instrument of approval issued by CASA. |
| February 2016 | Beechcraft 1900 fleet manager left and was not replaced. |
| April 2016 | Chief pilot commenced Cessna 441 line training. |
| May 2016 | Chief pilot completed Cessna 441 check pilot training and submitted recommendation to CASA for assessment as check pilot (to check the fleet manager). |
| June 2016 |
Operations manual part A (general operations manual) updated. Cessna 441 fleet manager renews OPC, signed off by chief pilot, and with the same CASA FOI as in the accident flight on board |
| July 2016 | Operations manual part E (cabin crew) updated. |
| September 2016 | Cessna 441 wirestrike occurrence (see section titled Surveillance events for Rossair). |
| October 2016 | Operations manual part C (training and checking) updated. |
| November 2016 | CASA Level 1 systems audit scheduled. Opening meeting occurred, but audit not conducted (see section titled Surveillance events for Rossair). |
| January 2017 |
Chief pilot received recommendation for EMB 120 check pilot approval from EMB 120 fleet manager. Check pilot training records submitted to CASA, as application for the chief pilot to conduct proficiency checks on the EMB 120. |
| February 2017 |
Chief pilot observed by CASA in the Embraer EMB 120 simulator undergoing OPC (as a captain). Concerns raised about his performance being below that required for a check pilot, potentially due to workload (see section titled CASA awareness of Rossair workload). New CEO begins in role. Application submitted to CASA for AOC variation to include Perth-based Beechcraft 1900 operator’s operations. |
| March 2017 |
Chief financial officer leaves and is replaced on temporary basis. Flight operations manager leaves and is replaced. Application for deputy maintenance controller submitted to CASA. |
| April 2017 |
Board approved recruitment for additional Beechcraft 1900 and EMB 120 pilots. Cessna 441 fleet manager loses medical certificate, affecting operator’s ability to conduct checks on operator’s Cessna 441 pilots. Contractor Cessna 441 check pilot given approval to conduct proficiency checks for two Cessna 441 pilots. Inductee Cessna 441 pilot employed on part-time basis and begins preparation to be checked to line. HAAMC takes 3 weeks unscheduled leave due to work-related stress issues. Returns mid-May. |
| May 2017 |
Check flight arranged for chief pilot to check inductee pilot. CASA internal email suggests conducting ‘some sort of audit in the next week or two’ due to concerns about maintenance and the HAAMC and chief pilot’s workload. Operations manual part B (Beechcraft 1900) submitted by chief pilot to CASA for AOC variation. |
Manager workloads
Workload is defined by Orlady and Orlady (1999) as ‘reflecting the interaction between a specific individual and the demands imposed by a particular task.’
Chief pilot workload
The ATSB interviewed the chief pilot’s fiancée, several other current and former management personnel within the operator and CASA personnel who had interacted with the chief pilot in the weeks and months leading up the accident. Many of these people reported that the chief pilot was very busy and was working long hours to conduct all the tasks associated with his responsibilities.
According to CAO 48.1 Flight time limitations – pilots:
An operator shall not roster a pilot to fly when completion of the flight will result in the pilot exceeding 90 hours of duty of any nature associated with his or her employment in each fortnight standing alone. For the purpose of this paragraph, duties associated with a pilot’s employment include reserve time at the airport, tours of duty, dead head transportation, administrative duties and all forms of ground training.
The CAO applied to chief pilots as well as other pilots conducting flight duties.
The chief pilot’s flight and duty records indicated, in the six months leading up to the accident on 30 May 2017, he was working an average of 71 hours of duty per 14-day period. However, email records indicated that the chief pilot regularly conducted work-related tasks outside of the times which he officially logged duty time. That was consistent with the observations of his fiancée and indicated that his average duty time was higher than reported.
As defined in the operations manual, the role of chief pilot was primarily a management role, with a small component of flying on the predominant operated aircraft. In the previous year, he recorded an average of 59 hours flight time per 28-day period, although that had reduced to 30 hours in the most recent 28-day period. The maximum permissible flight time was not more than 100 hours per 28 days in two-pilot operations, or 90 hours per 28 days for single-pilot operations. In comparison to the chief pilot, the full-time Cessna 441 pilots were logging around 80–90 hours flight time per 28 day period, and 88-90 hours of duty time per 14 days. There was an increase in flight and duty times for Cessna 441 pilots since February 2017.
These flight and duty hours meant that, for most of 2017, the chief pilot was flying more than the ‘component of flying duties’ expected of a full time management position associated with the chief pilot role. In addition to this, the chief pilot was carrying out many training and checking responsibilities, other than the checks themselves.
As detailed in Table 2, the chief pilot was responsible for managing many of the recent changes that had occurred in the organisation, such as the updates to the operations manuals in 2016–2017, reviewing investigations of incidents, managing the current pilots, and recruiting new pilots. The chief pilot also had preparation work for further assessment in the check pilot roles on both the Embraer EMB 120 and the Cessna 441.
In terms of other ongoing work, email evidence showed that the chief pilot was preparing to fly an increased number of flight hours in June 2017 to cover a pilot who was taking annual leave. In addition, there was a continuing evolution of the operations manuals underway, a review of the safety management system manual, work towards applying for CASR Part 141/142 training approval with CASA for the organisation, and further work for the AOC variation associated with integrating the Perth-based operator into the organisation.
Reports from a number of the chief pilot’s colleagues indicated they had full confidence in him and thought that he was doing a good job. However, some people expressed concern that he was taking on too many responsibilities and spreading himself too thin. Several also described him as being a confident and/or positive individual who just got on with his job, to the point of taking on more work that he should have.
The CEO advised the ATSB that he wanted the chief pilot to do less flying and focus more on his management tasks. He had arranged to provide the chief pilot with some administrative support to help him manage his tasks.
Some people who interacted with the chief pilot in the weeks prior to the accident reported that they did not think he appeared any different than normal. However, a similar number indicated that he appeared to be stressed or tired (see also CASA comments in CASA awareness of Rossair workload). Some noted that he had not had an extended period of leave between joining Rossair in late 2015 and the accident on 30 May 2017, and that he was greatly looking forward to some leave planned in September 2017. Some also reported that the chief pilot had indicated at various times during 2017 that he was looking for another job elsewhere.
The chief pilot’s fiancée reported that the chief pilot was tired, and had a lot of work commitments, but had good sleep the night before, and appeared in good spirits before leaving for work.
Other managers’ workload
The HAAMC reported that the increase in flying hours, as well as having aircraft operate out of both Parafield and Adelaide airports, increased the workload associated with his roles. He also had limited support in the multiple roles being covered, although had recently recruited a second LAME. The HAAMC stated that he and other managers (including the chief pilot) were dealing with a high level of pressure associated with ensuring that they could conduct all of the required operations associated with the new contracts and related tasks.
In April 2017, the HAAMC required an unscheduled period of three weeks leave associated with work-related stress. An alternate HAAMC had to be brought in from the Perth operation to cover this period, as there was no one else in Rossair with approval to cover this role.
Other managers interviewed by the ATSB also reported high levels of pressure and workload within the operator during 2017, coming from a variety of sources, including the training of new staff due to the staff turnover, the nature of communications between staff, and differing goals from a commercial standpoint to what had been previously experienced. Despite that, it was also reported that the management and staff were working supportively together.
Regulatory oversight
Overview
The stated mission of the Civil Aviation Safety Authority (CASA) is ‘To promote a positive and collaborative safety culture through a fair, effective and efficient aviation safety regulatory system, supporting our aviation community.’
CASA was responsible, under Section 9 of the Civil Aviation Act 1988, for the safety regulation of civil aviation in Australia, including by:
(c) developing and promulgating appropriate, clear and concise aviation safety standards;
(d) developing effective enforcement strategies to secure compliance with aviation safety standards…
(e) issuing certificates, licences, registrations and permits;
(f) conducting comprehensive aviation industry surveillance, including assessment of safety‑related decisions taken by industry management at all levels for their impact on aviation safety…
CASA had documented a regulatory philosophy that included maintaining a risk-based approach to decision making, and being consultative and collaborative with industry, while balancing consistency with flexibility in its work.
CASA had two primary means of oversighting a specific operator’s aviation activities:
- regulatory services, by assessing applications for the issue or variations to its AOC and associated approvals (including approvals of key personnel)
- conducting surveillance of its activities.
CASA used a scale of prioritisation based on risk to determine where to focus resources. This prioritisation was based on a number of factors, such as the sector of operation, organisational changes and challenges.
In order to maintain oversight across Australian operators, CASA had a number of certificate management teams (CMTs), made up of CASA officers, including flying operations inspectors (FOIs) and airworthiness inspectors (AWIs), in different regions of Australia. Each of these teams oversighted a number of AOC holders. The majority of the oversight of Rossair was conducted by an Adelaide-based team.
Regulatory services processes
Regulatory services include changes to the AOC, key personnel approvals, maintenance personnel approvals, and check pilot approvals and renewals. Depending on the assessed risk, some of these regulatory services required a CASA FOI to conduct in-flight or simulator checks with the Rossair pilots, such as for operational proficiency checks (OPCs) for key personnel.
CASA’s procedures and guidance for assessing an application for the issue of, or variation to, an AOC and other approval processes were contained in the Air Operator’s Certificate Process Manual and the Air Operator’s Certificate Handbook.
Regulatory services provided by CASA for Rossair (AE Charter) in 2015–2017 (and their start dates) included:
- approval of a system of maintenance for the EMB 120 (January 2015)
- CAR 217 approval for the EMB 120 type rating training (April 2015)
- renewal of the operator’s AOC (June 2015)
- approval of temporary chief pilot (August 2015)
- initial issue of a maintenance controller approval (September 2015)
- chief pilot assessment (October 2015)
- check pilot assessments and renewals (Beechcraft 1900 fleet manager - October 2015, Cessna 441 fleet manager - March 2016)
- CAO 20.11 assessment for approved person (April 2016)
- OPC on the Cessna 441 fleet manager (June 2016)
- Observation of OPC for EMB 120 fleet manager (June 2016)
- flight check system approval for the EMB 120 (July 2016)
- operations manual part E revision (August 2016)
- authorisation for a person to carry out maintenance (various times for different types of maintenance)
- renewal of maintenance controller approval (December 2016)
- variation from the system of maintenance on VH-XMJ (January 2017)
- check pilot approval for the chief pilot on the EMB 120 (January 2017)
- AOC variation to add Beechcraft 1900C aircraft (March 2017)
- initial issue of a maintenance controller approval (March 2017)
- CAR 217 temporary approval for check pilot, to allow a contractor check pilot to conduct checks on two of the operator’s Cessna 441 pilots (April 2017).
Recent approvals of key personnel
Key personnel in an organisation must be approved by CASA in accordance with the process outlined in the Air Operator’s Certificate Handbook volume 2.
The chief pilot was issued with his instrument of approval following two interviews and a check flight in the EMB 120 in January 2016. This application was all processed, documented and assessed in accordance with the handbook procedure. Following his first interview in November 2015, CASA indicated that he needed more time to prepare for the interview. No problems were noted in his second interview in January 2016.
CASA’s assessment process of the chief pilot identified the need for the fleet managers to continue in an on-going role to support the chief pilot, while he gained additional experience in the chief pilot role. Notes made during the assessment identified the chief pilot as having a good attitude, and having sound systems and managerial skills. Regarding the chief pilot’s assessment flight, it was noted that he was ‘confident and accurate at ease with EMB 120 and unflustered by last minute changes.’ The assessment also noted that the chief pilot ‘would benefit from more exposure to line operations before any involvement in training beyond CAO 20.11’. The recommendation made for the chief pilot approval stated that ‘ongoing surveillance is essential’.
The approval for the CEO position, in February 2017, did not follow the documented formal key personnel assessment process. The procedure outlined in the handbook stated that CASA would conduct both a desktop assessment of a CEO application form and, once the assessment considered the application successful, an interview. There was no regulatory services task raised by CASA for this key personnel assessment, neither was there evidence recorded of a CEO application form being received or a desktop assessment being conducted. An email to the CEO confirming his successful application following an interview was sent on 22 February 2017, with a list of the issues discussed during the interview. This email was the only documented evidence of the assessment being conducted.
Approval process for chief pilot as check pilot
As with the key personnel assessments, the Air Operator’s Certificate Handbook volume 2 required CASA approval of check pilots to:
- Conduct conversion training (CASR Parts 141/142) and proficiency checks
- Conduct recurrent and remedial training including abnormal and emergency operations
- Conduct competency checks and instrument proficiency checks
- Conduct emergency procedures proficiency checks.
The documented procedure for applying for a check pilot approval was to submit the required CASA form, which was then to be subject to a desktop assessment, including a review of the candidate’s training records, and then completion of a flight test assessment.
Following submission of the form, the handbook stated CASA would assess the application, verifying that it contained:
- Details of the nominee
- The training and checking approval requested
- The nomination is recommended by the head of training and checking
- The nominee has successfully completed a syllabus of training conducted in accordance with procedures outline in the operators training and checking manual
- Log book copies of the training flight
- The nominee’s training and assessment records
- The nominee’s resume or CV.
The self‑recommendation made by the chief pilot on his training records was for CASA to assess him in checking other check pilots, that is, just the Cessna 441 fleet manager, rather than checking all line pilots. Following that recommendation, a CASA FOI (who was on the accident flight) observed the Cessna 441 check pilot’s OPC, which was conducted by the chief pilot in the right‑hand seat.
The Cessna 441 fleet manager believed that this check gave the chief pilot approval to conduct the fleet manager’s OPCs from then on, in line with the recommendation made on the chief pilot’s training form. Although the chief pilot submitted his training records to CASA following successful completion of his check pilot training in May 2016, no formal application form for check pilot approval was submitted to CASA at that time, and no regulatory services task was raised by CASA. The June 2016 flight was processed as a regulatory services task as a check pilot OPC, with no CASA documentation to support the chief pilot’s approval as a check pilot in this capacity. Following the accident, CASA verified the chief pilot did not hold any formal check pilot approvals.
In January 2017, a regulatory services task was raised for the chief pilot to be assessed as an EMB 120 check pilot. As noted in the section titled CASA awareness of Rossair workload, another CASA FOI observed the chief pilot undergoing an OPC (as captain/in the left seat), and made comments about his performance and CASA needing to observe his personal proficiency again before considering any check pilot privileges. Some of the operator’s personnel and staff within CASA interviewed by the ATSB recalled that CASA had observed the chief pilot again in the EMB 120 simulator, and they were under the impression that the chief pilot’s check pilot approval for the EMB 120 had progressed. However, CASA advised that no further observations of the chief pilot’s flying performance had been undertaken prior to the day of the accident and as of May 2017 the assessment for the EMB 120 check pilot approval had not been completed.
On 2 May 2017, the chief pilot sent an email to CASA noting that the Cessna 441 fleet manager’s loss of a medical certificate presented an ongoing challenge. He noted that the contractor Cessna 441 check pilot, who had recently conducted two checks on two of operator’s Cessna 441 pilots with CASA approval, would be conducting checks on behalf of the operator in the future. However, the chief pilot requested that he would like to conduct an OPC and line check on the contractor check pilot to induct him into the operator. Alternatively, he requested approval to conduct OPCs on another experienced Cessna 441 pilot. The chief pilot noted that he had been undergoing training as a backup to the fleet manager, and had conducted the fleet manager’s OPC in June 2016 under CASA observation. He also noted that he had since gained further experience on the Cessna 441 and had observed the fleet manager conduct other checks on the operator’s pilots.
On 4 May 2017, CASA responded to the chief pilot, and advised that it could arrange for an FOI to observe him conducting another OPC which, if successful, meant that it could issue him with an approval to conduct OPCs and line checks. CASA subsequently varied the EMB 120 check pilot task to become a Cessna 441 check pilot task. No formal application form was received (as requested by CASA), and therefore the normal pre-flight assessment verification process, as per the CASA AOC handbook, was not recorded as having been conducted.
In subsequent correspondence, the inductee pilot was nominated by the chief pilot as the person he would conduct the OPC on. The flight was to be observed by the CASA FOI who was a Cessna 441 specialist and had previously observed the chief pilot during the June 2016 flight. CASA personnel advised the ATSB that, following the chief pilot’s request on 2 May 2017, they had discussed the request among themselves (including the CMT manager) in the Adelaide office. They believe they had considered all the risk factors involved with the proposed flight, and had sufficient mitigators in place. However, there was no written record of these considerations.
Approval of changes to the operations manual
Under CAR 215(1):
an operator shall provide an operations manual for the use and guidance of the operations personnel of the operator
Furthermore, CAR 215(5) required the manuals to be updated where necessary, and CAR 215(6) required these manuals to be provided to CASA. The record of interview during the chief pilot assessment in January 2016 indicated he was aware of the regulatory process for updating parts of the operations manual, including requiring a draft to be submitted to CASA before an amendment was incorporated.
The list of regulatory services tasks conducted by CASA in the preceding years did not reflect the 2016 updates to part A (general operations) and part C (training and checking) of Rossair’s operations manual. The only regulatory services tasks raised for a manual revision for the year was to part E (cabin crew).
There were a number of draft versions of each of the revised manuals located on the chief pilot’s computer, including iterations labelled ‘draft for CASA’. Although a record of the chief pilot submitting these to CASA could not be found, CASA confirmed that the version of part C current on 26 June 2016 was the version that it held.
Some operations manual parts are ‘accepted’ by CASA, while some are ‘approved’ by CASA. The operations manual part C, the training and checking manual, which contained the incorrect procedure for simulating an engine failure in a turboprop aircraft (see the section titled Engine failure simulation), was an example of a part that must be approved by CASA.
Surveillance processes
CASA Surveillance Manual
CASA developed a surveillance program to determine whether aircraft operators and other organisations were meeting the regulatory requirements. CASA’s surveillance policies, processes and procedures from July 2012 were outlined in the CASA Surveillance Manual (CSM). With the introduction of the CSM, CASA also started using Sky Sentinel, an information technology tool designed to help manage surveillance activities.
The CSM stated:
Surveillance is the mechanism by which CASA monitors the ongoing safety health and maturity of authorisation holders. Surveillance comprises audits and operational checks involving the examination and testing of systems, sampling of products, and gathering evidence, data, information and intelligence. Surveillance assesses an authorisation holder’s ability to manage its safety risks and willingness to comply with applicable legislative obligations…
CASA conducts surveillance on all authorisation holders with its principal obligation being to detect and mitigate threats to aviation safety as they manifest themselves in an authorisation holder…
CASA’s surveillance program uses a systems and risk-based approach. Surveillance events are recorded and tracked in a supporting IT system [Sky Sentinel] and the results analysed, which allows CASA to evaluate the authorisation holder’s safety performance. The Surveillance Program is dynamic, regularly reviewed and updated, taking the following issues into consideration:
• significant changes that could affect an authorisation holder, including changes to management or organisational structure, policy, technology; special projects; changes to authorisation holder’s service providers; global and/or local threats and regulatory requirements
• application of the authorisation holder’s Safety Management System (SMS) where applicable
• results of previously conducted surveillance and/or investigations
• surveillance resource requirements
• the authorisation holder’s willingness and ability to identify and control its aviation safety-related risks.
Types of surveillance
The CSM outlined the following types of surveillance events:
- systems audits (or audits based on a defined scope to take into account the specific activities conducted by the authorisation holder ensuring their compliance with regulations and the use of effective control of risks)
- health checks (which were similar to systems audits but reduced in scope and duration)
- post-authorisation reviews (conducted within 6–15 months after initial authorisation)
- operational checks (such as site inspections, ramp checks, en route checks, manual reviews, key personnel interview, desktop investigation of an occurrence and on-site investigation of an occurrence).
System audits, health checks and post-authorisation reviews were described as level 1 surveillance events, which meant they were structured, forward-planned and larger in nature. Systems audits would generally done by multi-disciplinary teams, whereas health checks could be done by teams or a single inspector as required. Operational checks, known as level 2 events, were significantly shorter in duration, and were described as generally being compliance assessments used to verify the process in practice.
A key personnel interview was described in the CSM as ‘an interview (phone or face to face) with a person with a key role in an authorisation holder’s operation during which matters of significance are discussed which can be constituted as surveillance’.
Frequency of surveillance activities
The recommended frequency of surveillance activities in the CSM for a passenger charter operator using air transport aircraft above 5,700 kg (such as the Beechcraft 1900 or EMB 120) and for an operator with a CAR 217 organisation was as shown in Table 3.
Table 3: Flight operations surveillance frequency guide
| Type of operation | Level of surveillance | Recommended frequency | Last conducted |
| Large charter (greater than 5,700 kg)[16] |
Level 1 – Systems Audit | 1 per year | March 2012 |
| Level 2 – Operational check | 1 per year |
Ramp check – August 2015 En-route check – April 2014 |
|
| CAR217 | Level 2 – Operational check | 1 per year |
CAO 20.11 assessment – April 2016 En-route check – March 2014 |
Source: CASA, modified by ATSB
In discussing the scheduling of surveillance activities, the CSM stated:
CASA’s surveillance program scheduling is driven by the risk to safety posed by authorisation holders and is based on an assessment of a number of factors. These factors include the assessment of an authorisation holder’s safety performance, taking into account assessment factors indicated by the Authorisation Holder Performance Indicator (AHPI) assessment results and time since the last assessment, outstanding NCNs and findings history, time since the last surveillance event and safety‑related risks specific to each authorisation holder. Based on this consolidated information, CASA has the ability to prioritise surveillance activities commensurate with resources available.
CASA personnel interviewed during a number of ATSB investigations have advised that the recommended frequency of surveillance tasks was not achievable with their current resources. The Adelaide CMT members reported that workload for the team was high, due to the 52 AOC holders they were required to oversight, as well as the level of industry support required for regulatory changes at the time, particularly in relation to the CASR Part 61 and Parts 141/142.
In addition, CASA personnel advised the ATSB that its policy in recent years was to ensure that it was regularly interacting with operators and their key personnel, through regulatory services tasks and other means. These interactions could assist in forming an understanding of the operator, and help in assessment of when surveillance events where required.
Authorisation holder performance indicator (AHPI)
The authorisation holder performance indicator (AHPI) assessment is a tool used by CASA CMTs to assess ’the apparent risk to safety presented by an authorisation holder’. An AHPI assessment was required to be conducted at least every 6 months, and the results discussed either monthly, or 6 monthly, depending on the category of the operator.
Using the AHPI, the AOC holder was assessed on 19 parameters, using a word picture-based one to five scoring system, where one was a good score, and five was a bad score. A weighting based on risk was given to each of these parameters to give an overall score. The score itself did not have a particular meaning in terms of further action required, but it assisted the CMT to assess whether any risk-based surveillance of an organisation was required, and scope the areas for that assessment.
Conduct of surveillance events
The CSM outlined requirements for planning, scoping, conducting and reporting (and recording) of surveillance events. In terms of surveillance event reporting, the CSM outlined a number of different forms that could be used to document the nature and results of a surveillance event. The manual stated:
The Surveillance Report provides an official record of the surveillance event as well as information for CASA’s own ongoing analysis and risk management. The role of the report is to give CASA enough information to be satisfied that either an authorisation holder can continue to operate in a safe and effective manner, or is not operating safely and appropriate action should be taken. The report also provides context to the authorisation holder about any findings.
Authorisation Holder Performance Indicator scores for Rossair
A summary of the overall scores and comments made during AHPI assessments for Rossair in recent years are shown in Table 4.
Table 4: AHPI assessments on Rossair during July 2015 to May 2017
| Date of AHPI assessment | Overall score | Selected comments |
| 13 July 2015 | 94 | [Discussion about regulatory services tasks being undertaken.] |
| 19 August 2015 | 115 | Significant changes to AOC holder. [Additional comments in Sky Sentinel at this time noted that ‘new CEO appointed after previous CEO… was terminated. Chief pilot resigned then withdrew resignation… will leave organisation on 24 August 2015…’. |
| 9 November 2015 | 97 | Organisation has new CEO with limited experience, and a temporary but very experienced chief pilot. Limited coverage of check pilots on B1900 fleet, which is being addressed. New Chief Pilot candidate to be interviewed shortly, but with current temporary [chief pilot] being retained as [head of training and checking]. Continued close oversight required. |
| 8 February 2016 | 113 | Concerns include new and inexperienced chief pilot, a new cabin services manager (awaiting training). B1900 fleet manager has resigned. New HAAMC. New CEO. |
| 18 July 2016 | 85 | New Chief Pilot becoming effective in role and implementing positive improvements in safety culture, IT and training. New [Flight Attendant] Manager also providing continual improvement. Good communication links with [Adelaide] CASA office with regular informal meetings and updates. Possible expansion and additional recruitment needs ongoing monitoring due to limited (but good) training resources. |
| 9 September 2016 | 95 | Recent wire strike may indicate issues with flight planning and preparation for [Cessna] 441 ad hoc operations. |
| 3 February 2017 | 122 | Limited personnel available with rapid turnover of crew, new CEO has been appointed and is awaiting interview. Chief pilot and [Flight Attendant] Manager have very high workloads. |
| 4 May 2017 | 130 | Change of CEO. Corporate owners have purchased another AOC… and the degree of separation is sometimes vague due to cross hiring of aircraft. Both [chief pilot] and HAAMC are reporting increased stress levels and commercial pressures. |
Source: CASA, modified by ATSB
In the assessments in 2015 and early 2016, there had been some variation in the scores, reflecting the changes in the organisation. The same FOI conducted all five assessment since February 2016, and was conducting them at a higher frequency than was required. The trend of the last four AHPI scores was negative. These assessments had the organisation moving from its best score to its worst. It is not possible to compare the longer term trends, as CASA changed the AHPI scoring method in early 2015.
Some factors that were trending negatively in the 2017 assessments included:
- Stability of the company, which had reached the highest risk score possible in May 2017, indicating that the authorisation holder was experiencing five or more of the following issues: changes to operation; expansion or contraction beyond capability and capacity; political issues; merger/take-over activity; management and staff turnover; financial concerns; and industrial relations tensions.
- Between September 2016 and May 2017, the score for senior management attitude indicated a move from senior managers having cultivated a strong safety culture with a proactive attitude towards regulatory compliance and safety to senior managers having an accepting attitude towards these issues.
- Management control, with a score which indicated that many and/or major aspects of the organisation’s operations were outsourced or leased and/or some suppliers/third party providers were considered as a medium to high risk.
There were also some positive changes noted in the scores, including:
- Safety assurance had improved to a score indicating that proactive and reactive processes exist and are tied to safety outcomes or regulatory compliance (but only partially implemented)
- Human resources was rated at a level indicating that ‘human resources and data meet minimum standards; personnel are generally available, although availability may be limited at peak times; human resource data systems are adequately maintained and available for all parts of the organisation and are used effectively.’ This score had deteriorated in early 2017, but improved to the previous level.
- The training and competency rating had deteriorated in February 2017, but by May 2017 had returned to a score indicating that competency (including technical and non‑technical skills) of all personnel is actively managed through established training programs and assurance. This was the highest score possible.
At the time of the accident, Rossair had the eighth highest AHPI assessment score for the 52 AOC holders the CMT had responsibility to oversight. CASA advised that this was due, in part, the nature of the operator’s operations and the size of the aircraft involved.
Surveillance events for Rossair
The last audit conducted on the operator was in March 2012. This audit was conducted on Air South as a separate operator, before the merger with Rossair took place. The audit issued three non-compliance notices and 11 observations.
There had been no follow up systems audit on the merged AE Charter operation, or on the EMB 120 operation since its introduction.
A level 1 systems audit was scheduled for November 2016. There were 25 elements that could be assessed in a systems audit, and the scope selected was based on the information gathered by CASA during AHPI assessments and from other sources (including previous surveillance). The scope of the planned audit on Rossair included:
- Aircraft – airworthiness control
- Aircraft – line servicing
- Cargo and passengers – fuel load control
- Cargo and passengers – non dangerous goods / baggage system
- Cargo and passengers – passenger control
- Operations – authorised activities
- Operations – operational support systems
- Safety management – safety risk management
- Training – flight testing
- Training – qualifications and authorisations (instructor, examiner and support staff)
- Training – training infrastructure
- Training – training management.
This audit was postponed on the day it was scheduled to begin, following the opening meeting of the audit, reportedly due to both CASA FOI and operator availability.
In March 2017, the scope was updated to include ‘Operational personnel – crew scheduling.’ The audit had not occurred by the time of the accident.
CASA had conducted a number of unscheduled level 2 desktop investigations based on occurrence or event reports. There had been seven of these started since the beginning of 2016, two events of which were also subject to ATSB investigations: AO-2016-110 Wirestrike involving Cessna 441, VH-NAX and AO-2016-143 Flight control system event involving EMB 120, VH‑YEI. Five of the seven investigations had been completed by the time of the accident, with no findings or action required. Level 2 desktop investigations were usually started following a notification from either the ATSB or Airservices Australia about an occurrence or event. Following the accident, CASA noted that the frequency of the occurrence reports received, although generally minor, was of heightened interest for CASA.
Other surveillance events planned or conducted on the operator following the 2012 systems audit until 2017 are summarised in Table 5. Neither of the planned operational checks, the route check and the en-route check had occurred within the 17 months since the chief pilot had been approved into the role in January 2016. The assessment of the cabin crew manager as a CAO 20.11 emergency procedures trainer, which was primarily a regulatory services task, was the only formal surveillance event that had occurred since the chief pilot had started at Rossair.
Table 5: Surveillance events on Rossair (and previous AOCs) 2012–2017
| Surveillance event | Date | Discussion |
| Level 2 unscheduled investigation | 12 February 2014 | Two incidents involved Cessna 441 aircraft at Marla aerodrome. Report completed and 4 non-compliance notices and two observations were issued. (Completed under Rossair AOC prior to merger with Air South AOC) |
| Level 2 operational check – CAR 217 | 14 March 2014 | Check pilot approval for multi-engine command instrument rating delegations. No findings issued. |
| Level 2 unscheduled investigation | 23 March 2014 | Beechcraft 1900 flight director anomaly. Investigated as ATSB investigation AO-2014-066. CASA lists no further action required. |
| Level 2 operational en-route check | 7 April 2014 | Three Cessna 441 flights were observed (two proficiency checks and a night currency flight, involving the then chief pilot and other check pilot in Rossair). Two non-compliance notices and four observations were issued. |
| Level 2 operational en-route check | 2 March 2015 | Post AOC issue – monitoring of operation. Approved but not carried out. |
| Level 2 operational ramp check | 24 August 2015 | Ramp check completed on Cessna 441 pilot. Weight and balance chart showed 11 passengers, and the manifest showed 9 passengers. The checklist was not completed and signed off as a satisfactory or unsatisfactory assessment, although items were marked as assessed. |
| Level 2 operational check – 20.11 | 11 April 2016 | CAO 20.11 approval granted for cabin crew manager (associated with a regulatory services event). CASA advised that no report was issued for this surveillance event. One observation was issued. |
| Level 1 systems audit | 21 November 2016 | Rescheduled |
CASA awareness of Rossair workload
CASA was, at least informally, aware of workload issues with the chief pilot and other key personnel. Indicators of this awareness include:
- Comments made in the authorisation holder performance indicator assessments conducted stated:
- ‘Chief pilot and flight attendant manager have very high workloads’ (February 2017)
- ‘Both chief pilot and HAAMC are reporting increased stress levels and commercial pressures’ (May 2017)
- The internal email regarding the chief pilot’s performance in the EMB 120 simulator in February 2017 possibly being affected by workload, as it was below what had been seen previously.
- An internal email in mid-May 2016, again identified concerns regarding workload of the HAAMC and chief pilot, regarding ‘Looks like we may need to do some sort of audit in the next week or two.’
After the accident, a CASA internal report stated ‘Interviews with CASA officers identified an awareness of under-resourcing and organisational stress within the operator, but no evidence of regulatory non-compliance.’
Additional information
The CASA FOIs maintained good links with the chief pilot, through regular informal meetings. While these meetings assisted the FOI in completing the AHPI assessment, in informing the FOI about changes in Rossair, and building a collaborative working environment between the regulator and the operator, there were no records kept of the conversations which could be used in later risk assessments and surveillance.
Rossair personnel reported that the lack of formal oversight placed them in a position where they did not always have the required support for safety related initiatives and, as a result, addressing commercial matters became a higher priority.
The risks of informal surveillance have been shown in previous accident investigations.
The reopened ATSB investigation into the 2009 Pelair Westwind ditching near Norfolk Island (AO-2009-072) identified a safety issue that:
Although the Civil Aviation Safety Authority (CASA) collected or had access to many types of information about a charter and/or aerial work operator, the information was not integrated to form a useful operations or safety profile of that operator. In addition, CASAs process for obtaining information in the nature and extent of an operator’s operations were limited and informal. These limitations reduced its ability to effectively prioritise surveillance activities.
CASA’s response to the safety issue referred to the introduction in 2012 of the CASA surveillance framework, including the surveillance manual and sky sentinel for logging information, and the use of AHPI assessments; and toward the National Surveillance Selection Process (NSSP) which was implemented in 2018.
In the 2017 investigation into the Collision with terrain following an engine power loss involving Cessna 172M, VH-WTQ, 12km north-west of Agnes Water, QLD on 10 January 2017 (ATSB report AO-2017-005), it was noted that there were limitations in the documentation associated with surveillance events, including ‘no scoping form, worksheets, or other documents that identified the specific aspects of each element that was being assessed in relation to flight operations elements.’ There were also further limitations with documented records about discussions held with the operator.
The New Zealand Transport Accident Investigation Commission (TAIC) investigation into a fatal AS350BA helicopter collision with terrain at Fox Glacier on 21 November 2015 (TAIC report AO-2015-007) found that ‘the operator had been allowed to continue providing helicopter air operations with little or no intervention from the CAA, in spite of the CAA having identified significant non-compliances with the operator’s training system and managerial oversight.’ More specifically:
The CAA auditors and inspectors had raised concerns at various audits since 2012 about the operator’s management oversight and training program. However, the CAA had not responded decisively to the information provided by its surveillance unit.
...
Without any formal findings having been raised during any audits at which this situation was observed, the CAA had not been able to address the continued non-compliance. Internal CAA processes had not ensured that higher-level CAA managers were made fully aware of the true situation. Without the correct information, the managers could not take the most appropriate action necessary to get the operator to comply with the requirements of its air operator certificate.
Furthermore, the report explained:
The CAA cannot reasonably be expected to ensure total compliance by all participants in the sector. However, its surveillance activity should ensure that where deficiencies are found they are formally recorded so that regulatory decisions can be informed. Appropriate action can then be taken to either cause change or remove the threat from the system before an accident occurs.
Unlike the TAIC investigation, there was no evidence collected in this investigation suggesting that CASA were aware of any regulatory non-compliances that had not been acted upon, however there is evidence, from both interviews and documents, that they did have concerns about the organisation only just meeting minimal regulatory compliance. The scope of the planned 2016 audit, which was expanded again following the February 2017 AHPI assessment, indicated some of the areas which CASA considered as necessary to audit.
Related occurrences
Training accidents 2008-2017
A review of the ATSB occurrence database revealed that in the 10 years between 2008 and 2017, there were 24 accidents for twin-engine, VH-registered, aircraft under 5,700 kg[17] conducting training or checking. Of these, in addition to this accident, two involved an asymmetric simulated engine failure on take‑off or climb. This accident was the only fatal training accident. The two other asymmetric training accidents were:
On 23 December 2010, a flight instructor and student pilot departed Camden Airport, New South Wales on an instrument training flight in a Piper PA-30 (Twin Comanche) aircraft. Shortly after take-off, the instructor simulated an engine failure by moving the mixture control on the right engine rearwards at 400 ft above the ground. In response, the student reduced the engine control/s on the left engine. Shortly after, the airspeed decayed and the aircraft stalled. The aircraft rolled abruptly, with the right wing dropping to a 120° angle and the aircraft entered a spin. The instructor regained control of the aircraft at about 10 ft above ground level, with the aircraft in a relatively level attitude. As the nose of the aircraft was raised the airframe began to shudder, indicating that a stall was imminent. Consequently, the instructor elected to reduce the throttles to idle and land the aircraft. The aircraft subsequently impacted the ground resulting in minor injuries to the instructor. The student was not injured. (ATSB investigation AO-2010-111).
- On 10 July 2009, a flight instructor and student were conducting asymmetric circuit refresher training in a Beechcraft Aircraft 76 at Bunbury Airport, Queensland. During a go-around from a practice asymmetric landing, the flying pilot flared too high and bounced on one wheel. While the instructor said ‘I have control’, the student pilot applied power on the good engine, and (under 50 ft above the ground) the aircraft yawed right then impacted the ground in a flat attitude. The aircraft was seriously damaged but there were no reported injuries (ATSB occurrence number 200904058).
Engine failure and malfunction occurrences 2008-2017
For the same 10 year period and types of aircraft, there were 405 actual engine failures or malfunctions reported to the ATSB. Of these, 43 per cent were in the take-off/climb phases of flight. Only 9 resulted in accidents (2%), but 78 per cent of accidents were in the take-off/climb phases of flight. Five accidents followed a single engine failure on take-off or climb that resulted in asymmetric thrust:
- On 6 February 2009, a Piper PA-31 aircraft was on a business flight departing from Darwin, Northern Territory. During the initial climb, the right engine gradually lost power. The aircraft failed to climb and the pilot shut the engine down and feathered the propeller. The aircraft did not maintain altitude and subsequently the pilot landed the aircraft on water. The pilot and five passengers walked to shore in knee deep water (ATSB occurrence number 200900366).
- On 23 March 2010, a Piper PA-30 was conducting a ferry flight to the United States. During the initial climb from San Francisco Airport, the left engine failed at 60 ft above the ground. The aircraft veered left and lost height until it struck the ground. The aircraft was seriously damaged but the pilot was not injured (ATSB occurrence number 201001978).
- On 15 June 2010, a Piper PA-31P aircraft, with a pilot and a flight nurse on board departed Bankstown Airport, New South Wales for a repositioning flight to Archerfield Airport, Queensland in preparation for a medical patient transfer flight. While the aircraft was climbing to 9,000 ft the right engine sustained a power problem and the pilot subsequently shut down that engine. Following the engine shut down, the aircraft’s airspeed and rate of descent were not optimised for one engine inoperative flight. As a result, the aircraft descended to a low altitude over a suburban area and the pilot was then unable to maintain level flight, which led to a collision with terrain. Both occupants were fatally injured and the aircraft was destroyed (ATSB investigation AO-2010-043).
- On 14 November 2010, a Piper PA-31 aircraft was being operated on a passenger charter flight from Marree, South Australia. During the climb, at 2,500 ft, the pilot detected an unusual noise in the right engine followed by a gradual decrease in engine performance. The pilot returned to Marree Airport, however during the turn back the aircraft was unable to maintain altitude and elected to conduct a forced landing about 22 km south-east of the airport. The pilot did not feather the right engine as he assessed that the right engine was still producing some power. The aircraft was substantially damaged, however, the passengers and crew were able to exit the aircraft safely (ATSB investigation AO-2010-094).
- On 8 March 2015, the pilot of an Aero Commander 500 aircraft taxied for a charter flight from Badu Island to Horn Island, Queensland, with five passengers. The pilot commenced rotation and the nose and main landing gear lifted off the runway. Just as the main landing gear lifted off, the pilot detected a significant loss of power from the left engine. The aircraft yawed to the left, which the pilot counteracted with right rudder. He heard the left engine noise decrease noticeably and the aircraft dropped back onto the runway. The pilot immediately rejected the take-off; reduced the power to idle, and used rudder and brakes to maintain the runway centreline. Due to the wet runway surface, the aircraft did not decelerate as quickly as expected and the pilot anticipated that the aircraft would overshoot the runway. To avoid a steep slope and trees beyond the end of the runway, he steered the aircraft to the right towards more open and level ground. The aircraft collided with a fence and a bush resulting in substantial damage. The pilot and passengers were not injured (ATSB investigation AO-2015-028).
Other related asymmetric training accidents
Two other notable training accidents, and one training serious incident, outside of the small twin‑engine aircraft (below 5,700 kg) data set and/or before than 2008 are described below. The two accidents (AO-2010-019 and 200300224) resulted in fatal and serious injuries and involved a simulated engine failure just after take-off, at less than 50 above the ground. The serious incident (200404589) involved a recovered loss of control after simulated engine failures at 2,200 ft above the ground.
Loss of control involving Embraer S.A. EMB-120ER Brasilia, VH-ANB, Darwin Airport, Northern Territory, 22 March 2010 AO-2010-019
On 22 March 2010, an AirNorth Embraer S.A. EMB-120ER Brasilia aircraft (EMB 120), registration VH-ANB, collided with terrain moments after take-off from runway 29 at Darwin Airport, Northern Territory, fatally injuring both pilots. The flight was for the purpose of revalidating the command instrument rating of the pilot under check and was under the command of a training and checking captain, who occupied the co‑pilot’s seat.
The take‑off included a simulated engine failure and a review of data from the aircraft’s flight recorders identified that the pilot in command (PIC) retarded the left power lever to flight idle to simulate an engine failure. That introduced a simultaneous failure of the left engine and propeller auto‑feathering system.
The increased drag from the ‘windmilling’ propeller increased the control forces required to maintain the aircraft’s flightpath. The pilot under check allowed the speed to decrease and the aircraft to bank toward the inoperative engine. Additionally, he increased power on the right engine, and engaged the yaw damper in an attempt to stabilise the aircraft’s flight. Those actions increased his workload and made control of the aircraft more difficult.
The PIC did not restore power to the left engine to discontinue the manoeuvre. The few seconds available before the aircraft became uncontrollable were insufficient to allow ‘trouble shooting’ and deliberation before resolving the situation.
Following this accident, the operator transitioned the majority of its EMB 120 proficiency checking, including asymmetric flight sequences, to simulator‑based training.
Loss of control involving SA227-AC Metro III, VH-TAG near Lake George, New South Wales on 21 March 2004 200404589
On 21 November 2004, the crew of a Fairchild Industries SA227-AC Metro III aircraft, registered VH-TAG, was conducting an endorsement training flight near Lake George, 33 km north-east of Canberra Airport. The flight included a planned in-flight engine shutdown and restart, conducted at an altitude below 4,500 ft (about 2,200 ft above ground level (AGL)).
During the engine restart preparation, the instructor departed from the published procedure by moving the power lever for the left engine into the beta range and directing the pilot to select the unfeather test switch. These actions were appropriate to prepare an engine for start on the ground with a feathered propeller, but not during an airstart. As a result, the propeller on the left engine became fixed in the start-locks position. The crew lost control of the aircraft and it descended 1,000 ft, to about 450 ft AGL, before they regained control.
The crew could not diagnose the source of the loss of control and proceeded to start the left engine while the propeller was fixed on the start-locks. As a result, the crew lost control of the aircraft for a second time and it descended 1,300 ft, to about 300 ft AGL, before they regained control.
The SA226 / SA227 aircraft contain no lockout system to prevent pilots from intentionally moving the power lever into the beta range during flight. It was the first time the instructor had given a Metro endorsement and he was subject to time pressure to complete the endorsement. Additionally, his ongoing difficulties in adapting to his employment tasks were not successfully dealt with by the operator. He had a limited understanding of the aircraft's engine and propeller systems, and had not practiced an airstart for 8 years as the Civil Aviation Safety Authority (CASA) check and training approval did not include an assessment of all flight critical exercises.
Collision with terrain involving Beechcraft Aircraft Corp 76, VH-JWX, Camden, New South Wales on 7 February 2003 200300224
A multi-engine command instrument rating flight test was being conducted in a Raytheon (Beechcraft Aircraft Corporation) BE76 Duchess aircraft at night. The Approved Testing Officer (ATO) simulated an engine failure shortly after take‑off (at 30 ft) from a touch and go approach during the test. The candidate could not achieve adequate climb performance from the aircraft, and called for the ATO to reset full power. Shortly after, the aircraft's right wing impacted a tree, and the aircraft descended, colliding with steel and concrete structures on the ground. The cockpit remained intact during the accident sequence, but was consumed in an intense post-impact fire.
The two occupants escaped from the aircraft, however the ATO did not survive his injuries. The investigation determined that a simulated engine failure was conducted from a height where it was not possible to ensure a safe flight path, unless visual reference with obstacles could be maintained. There was insufficient illumination to maintain that visual reference.
Regulatory documents provided guidance recommending against low level asymmetric operations at night. The flight test was a CASA flight test, being conducted by a CASA-approved testing officer. The flight was conducted as a private flight, without the oversight normally afforded by operating under the control of an air operators' certificate.
__________
- Normal category: an airworthiness categorisation that applies to aircraft which are intended for non-acrobatic operation, having a seating configuration (excluding pilot seats) of nine seats or less, and a maximum take-off weight (MTOW) of 5,700 kg or less, or 2,750 kg or less for rotorcraft.
- The Type Certificate holder is responsible for the design and continued airworthiness support of the aircraft.
- Small installed tabs that create vortices in the airflow just above the upper wing surface (boundary layer) that in turn keep it attached to the aerofoil for longer, improving aerodynamic performance.
- Feathering: the rotation of the propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in-flight engine failure or shutdown. See the section titled Multiengine aeroplane propellers for further information.
- The maximum take-off weight was increased over that of the basic aeroplane due to the fitment of vortex generators.
- When measuring cloud cover, the sky is broken up into eighths. Scattered cloud equates to 3 to 4 oktas of cloud.
- In this context, ‘small’ referred to a reciprocating or turbopropeller-powered airplane with a maximum certificated takeoff weight of 12,500 pounds or less. This included the Cessna 441.
- See www.faa.gov.
- The left engine was the critical engine in this occurrence.
- A cockpit instrument to assist with coordinating flight control inputs, especially rudder application.
- See the section titled Circuit operations.
- Extra seat in cockpit or on flight deck not required by flight crew, but possibly occupied by an authorised crewmember.
- The recommended frequency for a passenger charter operator of smaller aircraft was one level 1 health check each year and one operational check each year.
- The same ‘small’ multi engine aeroplane as the Cessna 441, with a maximum certificated takeoff weight of 12,500 pounds or less.
Introduction
Shortly after departure from Renmark Airport, control of VH‑XMJ was lost at low altitude and the aircraft collided with terrain fatally injuring the three occupants. The accident occurred at the point in the flight at which a simulated engine failure after take-off exercise was to be conducted as part of a planned check flight.
The extent of impact damage meant that it was not possible to verify the operation of every aircraft system. However, detailed examination of those systems that had the potential to effect performance and/or controllability did not identify any pre‑existing technical defects. Additionally, while the extent of propeller damage indicated that both engines were operating at comparable low power at impact, reducing power on both engines would be an expected pilot recovery action following a loss of control. As such, the propeller damage signature was not necessarily indicative of engine issues.
On balance, the ATSB assessed that the accident occurred after the simulation of an engine failure rather than following an aircraft malfunction. As such, the following analysis will consider the operational factors associated with the development of the accident. It will also discuss the organisational factors and related risk controls that were identified, including their potential to influence future operations. The investigative challenges created by having limited recorded flight data available will also be discussed.
Development of the accident
A comparison of flight data for the respective departures from Adelaide and Renmark airports identified that both profiles were similar until the aircraft reached about 400 ft above the ground. At that point the aircraft was above the briefed minimum height and airspeed for initiation of a practice engine failure in the Cessna 441. From that point on the two profiles diverged significantly due to commencement of the planned one engine inoperative (OEI) flight sequence. Analysis of the track variation indicated that the exercise involved reducing power on the right engine.
The flight data showed that, while the initial yaw associated with the simulated engine failure was controlled, neither the target airspeed or a positive OEI rate of climb were achieved over the last 30 seconds of the flight. Despite that, the exercise was not discontinued resulting in a subsequent loss of control.
The company operations manual contained a requirement to restore normal power if difficulty was experienced in maintaining aircraft control and there was a briefed check flight requirement that sustained deviation below the target airspeed was not permitted. Arguably these requirements related more to controllability of the aircraft than performance limits. In that regard they may not have provided a prompt to the crew to consider terminating the exercise. While the reason for persisting with the practice emergency despite not achieving the expected performance could not be determined, the increased risk of a control loss was presumably not recognised by the pilots occupying the control seats. Furthermore, if a risk of control loss was identified by the flying operations inspector, as he was not able to communicate using a headset, he may have been hindered in communicating this to the other pilots. This aspect is discussed further below.
Degraded aircraft performance
There was no evidence of any mechanical defect likely to have influenced the accident and the two‑pilot operation provided redundancy in the event of incapacitation. The ATSB also considered it unlikely that practice of an OEI sequence would have required any variation to the power level of the ‘good’ engine. As such, the recorded degraded aircraft performance was probably the result of the power setting of the ‘failed’ engine, aircraft handling or a combination of both.
Engine failure simulation
The in‑flight power lever positions could not be identified as they were not recorded and the as‑found positions were not considered reliable. However, the operator’s procedure for simulating an engine failure initially required reduction of power on the ‘failed’ engine to flight idle. Once the initial response actions were complete, the power lever was then to be reset to zero thrust. That method of simulating an engine failure was different to the procedures outlined in Civil Aviation Advisory Publication 5.23‑1(2) Multi-engine aeroplane operations and training and the pilot’s operating handbook (POH).
Despite the operator’s procedure being approved by the Civil Aviation Safety Authority (CASA), reducing the power to flight idle on a turboprop aircraft is not representative of the drag associated with a real engine failure as it does not take account of the beneficial effect of auto‑feather/negative torque sensing systems. Consequently, had flight idle been selected it would have created significantly more drag on the ‘failed’ engine, making it more difficult to control the aircraft and achieve the expected OEI performance. While the operator’s procedure only required use of this power setting during the initial ‘phase one’ checks (which would be expected to be completed in less than 30 seconds), it has been a contributing factor to previous asymmetric loss of control accidents (for example AO-2010-019 in the section titled Related occurrences).
The ATSB sought information from CASA regarding the circumstances under which the incorrect procedure was approved for use by the operator. Despite this request, no information was provided by CASA. Consequently, the ATSB was unable to determine whether the approval of incorrect information was an isolated human error or symptomatic of a systemic deficiency with the approval process.
In addition, the operator’s documented zero thrust value was different to the value calculated and provided to the ATSB by the propeller manufacturer in support of this investigation. Despite this, had the pilot used the value in the operations manual, it was unlikely to have contributed to the accident, because it would have provided positive thrust on the failed engine and reduced asymmetric yaw.
However, based on the documented flight briefing and reported power lever manipulation during the previous week’s practice flight, the ATSB considered that simulation of the engine failure during the accident flight probably involved:
- initial reduction of the power lever to a position short of the flight idle stop
- if the ‘phase one’ actions were completed, advancement of the power lever to a position less than the zero thrust setting determined by the propeller manufacturer.
Setting less than zero thrust would have increased the drag, yaw tendency and therefore increased the actual asymmetric minimum control airspeed, VMCA.
Additionally, the likely power setting was less than the AIRSTART lever position detailed in the POH and had the potential to allow the aircraft’s right fuel computer to trip from the normal automated mode to the manual mode. If that occurred it could have affected that engine’s power level and/or been a distraction to the crew. As switching of the fuel computer from normal to manual was not recorded, it was not possible to determine if this occurred.
Aircraft handling
As detailed in the United States Federal Aviation Administration (FAA) Airplane Flying Handbook, achieving asymmetric performance relies on minimising sideslip through the appropriate use of rudder and aileron. The failure of the aircraft to achieve the published OEI rate of climb, despite retraction of the landing gear and flaps, indicated that the required combination of these flight controls, as detailed in the POH, may not have been applied.
The FAA handbook outlined that using either the rudder or aileron in isolation to counter asymmetric thrust will result in OEI performance penalties. Given the rudder trim was found to be at an extreme limit it was considered unlikely that the flying pilot had used only aileron to oppose the asymmetric thrust. Conversely, that trim setting was consistent with the use of significant and sustained rudder input. Therefore the recorded lack of OEI performance may have been influenced by a disproportionate use of rudder. In that circumstance, not only would there be a performance penalty but, as identified during Cessna 441 flight testing, the actual VMCA could have been as high as 115 kt.
Summary
Although a lack of recorded information prevented identification of the precise reason/s that the aircraft failed to achieve the expected OEI performance, the ATSB concluded that the method of simulating the power loss and pilot control inputs, together or in isolation, probably increased the actual VMCA significantly above the published value of 91 kt. The aircraft then experienced an asymmetric loss of control when the airspeed reduced below that minimum control speed. The near‑vertical impact signature was consistent with that loss of control mechanism.
The ATSB also considered the potential that the loss of control was the result of an aerodynamic stall. However, given that the final recorded indicated airspeed was about 20 kt higher than the aircraft’s stall speed that was considered unlikely.
Simulating engine failures after take-off
A 2002 Flight Safety Australia article published by the Civil Aviation Safety Authority, which discussed engine failures after take-off, stated that:
Few pilots will ever face a higher-risk situation than a loss of engine power immediately after take-off in a twin-engine aircraft.
This type of emergency occurs at low altitude, low airspeed, and close to maximum available power on the operating engine. To make matters worse, other workload elements competing for the attention of the pilot include asymmetric control issues; after-take-off actions and checks, and in most cases, the requirement to observe standard instrument departure procedures.
For those reasons, it has long been accepted as essential that pilots be exposed to simulated engine failures after take-off.
However, the practice of a simulated engine failure after an actual take-off is also a high-risk flight activity. Every element needs to be conducted precisely and the only defences are preventative as there is limited opportunity to recover from a loss of control. The same Flight Safety Australia article noted that if a simulated engine failure is ‘not done properly, engine failure after take-off training can be more dangerous than the real thing.’
A review of the ATSB occurrence database identified that there were three accidents during asymmetric training/checking flights in the last 10 years, with this accident being the only one with a fatal outcome.
Over the same time period there were nine accidents associated with actual engine failures/malfunctions in ‘small’ aeroplanes like the Cessna 441, four of which followed a single engine failure on take-off/climb that resulted in asymmetric thrust but no injuries. One of the accidents was fatal and followed an engine failure at an altitude of about 7,500 ft. The nine accidents represented two per cent of the total number of engine failure/malfunction occurrences. However, 78 per cent of the accidents occurred during the take‑off/climb phase of flight despite only 43 per cent of the total engine failures occurring during that flight phase.
The data indicates that while accidents associated with engine malfunctions are rare, training to manage OEI flight after take‑off is important.
At present there is insufficient information available to accurately assess the accident rate associated with simulated engine failures, compared to the accident rate of actual engine failures occurring after take-off. Specifically, there is no data collected about the number of times asymmetric exercises are conducted in aircraft in Australia, in either flight training or company‑based training and checking, which means the exposure is unknown.
Without knowing the exposure rate and how the training exercises are being conducted, including whether they accurately represent the conditions of a real engine failure, the ATSB could not determine whether the benefits of conducting simulated engine failures at low level outweighed the risks. Further research in this area is required to answer that question.
Simulated engine failure after take‑off guidance
The Cessna 441 POH did not contain a procedure to simulate an engine failure during the actual take off phase. Instead, the manufacturer’s procedure for practising this emergency involved shutting the engine down while in the take-off configuration (extended landing gear and take off flap) at a safe airspeed and safe height, which Cessna considered to be 5,000 ft above the ground as directly referenced in related guidance, and as subsequently explicitly defined in the POH for Cessna 441 aircraft with later serial numbers.
In discussing the simulation of engine failures, Civil Aviation Advisory Publication (CAAP) 5.23 1(2) Multi‑engine aeroplane operations and training, recommended that those conducting the sequences ‘Consult the aircraft flight manual or POH for the manufacturer’s recommended method of simulating an engine failure’. The CAAP also contained detailed guidance on how to simulate an engine failure in the event the flight manual/POH did not.
This included detail on the height for initiating the exercise with advice that consideration should be given to not simulating engine failures below 400 ft above the ground in order to provide what CASA considered to be a reasonable safety margin. The CAAP also advised use of zero thrust to simulate a turbopropeller engine failure and provided a method to establish a torque value for zero thrust in the event that none was provided by the manufacturer. Recognising that the correct zero thrust setting will appropriately balance thrust and drag to simulate an engine failure in turboprop aircraft, it is important that zero thrust be derived and set accurately to ensure that it does not introduce additional drag. Cessna did not publish a zero thrust setting for the 441 aircraft and it did not form part of the procedure for simulating an engine failure.
Despite guidance in the CAAP to follow flight manual/POH recommended methods, on this occasion the exercise was conducted in accordance with the more general CAAP procedure at minimum practice height of 400 ft above the ground. The same procedure was also reflected in Part C of the company operations manual and, as such, had been approved by CASA. Practically, conducting the exercise in that manner resulted in it being conducted at a much lower safety height and via a different engine failure simulation method than detailed in the POH. That in turn reduced the overall safety margin for the activity.
Simulating an engine failure at low level affords very limited available height for recovery in the event of a real emergency or a loss of control. While there was no flight test data available regarding the height required for a Cessna 441 to recover from an asymmetric loss of control, the 5,000 ft safety height indicated that considerable height may be lost during recovery and that should it occur at 400 ft, the situation will be probably be unrecoverable. It is expected that an asymmetric loss of control at 400 ft would similarly be unrecoverable for many other small twin‑engine aircraft.
In that context, if a simulated engine failure is required to be demonstrated after an actual take‑off, it should be conducted in an aircraft simulator. If that is not possible then the sequence needs to be carefully risk managed to ensure that effective preventative risk controls are in place. In the case of this accident the safety defences included:
- a check flight requirement that the airspeed was not permitted to reduce below the target airspeed for any sustained period of time
- an operations manual requirement that normal power was to be restored if difficulty was experienced in controlling the aircraft.
Despite these requirements, the exercise was not discontinued when the airspeed and expected climb performance were not attained. However as discussed above, these requirements relate to controllability more than performance so may not have provided a prompt to the crew to consider terminating the exercise.
Continuation of the exercise
The aircraft did not achieve close to the expected OEI climb performance over the last 30 seconds of the flight. That should have been a clear indicator that the exercise wasn’t progressing as planned.
With the overall level of flight experience of the pilots on board, it was considered very unlikely that the pilots would have knowingly persisted with the exercise to a point where the aircraft was in danger. As such, the pilots probably didn’t recognise the degraded aircraft performance or the risk of continuing the exercise in the degraded state. The ATSB considered the following potential reasons why the exercise continued:
- Limited appreciation of the extent to which VMCA could increase if the simulated engine failure was not set-up or handled appropriately, and the risk that presented.
- The chief and inductee pilot’s limited training and recent experience on the Cessna 441. This could have increased the time taken and attention required to conduct the phase one checks following the simulated engine failure. That, in turn, may have affected the timely recognition of the need to discontinue the exercise.
- The check training completed by the chief pilot did not include recognition and recovery from abnormal situations that can develop from a mishandled simulated engine failure in a multi engine aircraft.
- Delayed intervention by the chief pilot in order to allow the inductee pilot more time to achieve the required flight parameters and pass the check flight. Successful completion of the two checks would have assisted the operator’s understaffing and provided an additional check pilot resource.
Due to limited evidence, it was ultimately not possible to determine to what extent any of these factors contributed to continuation of the exercise.
Skill decay
The two pilots in control seats had demonstrated handling of an engine failure in a Cessna 441 and other aircraft types numerous times previously. For the occurrence flight they both had specific roles to complete - either to handle, or to set and monitor the engine failure. Skill decay is known to occur when there is an extended time between training of a skill and needing to use that skill. This is reflected by the proficiency testing requirements for organisations holding a training and checking approval under Regulation 217 of the Civil Aviation Regulations 1988, which was to ensure safety critical perishable skills are checked at least every six months.
Although licenced, recent and current to operate aircraft included in the multi engine class rating, other than the practice flight the week before the accident, the inductee pilot had not flown the Cessna 441 since August 2014. Most of his recent experience was in lower‑performance piston engine aircraft in the same class rating. While these aircraft may have the same methods of handling a simulated engine failure, they also had lower target speeds, and different expected performance, following an engine failure. This could have influenced the way the pilot configured the aircraft, or his flight control inputs. Had the inductee pilot obtained further experience before undertaking the assessment, he may have been in a better position to manage the engine failure and developing emergency situation.
The chief pilot completed his training for the Cessna 441 check pilot role a year prior to this flight. The practice flight the week prior likely helped the chief pilot recover from that skill decay to some extent. Additionally, as the chief pilot was also preparing to conduct the same exercises on the EMB 120 aircraft, there was probably some level of transfer of training, although potentially negative, between the practice of initiating the engine failure, and the expected performance of the aircraft following that simulation.
Due to the chief pilot primarily flying on the EMB 120, as well as the permitted CASA exemptions, he had not had to demonstrate his own proficiency in flying the Cessna 441 aircraft, including the handling of a simulated engine failure, in the previous 12 months. This is outside the intent of the proficiency check guidelines, and may have allowed his skills to decay further than if there was a greater frequency of practice.
Therefore, while it was not possible to establish any influence in this occurrence, it was probable that the inductee’s limited recent experience in the Cessna 441, and the time between the chief pilot’s training and assessment, led to a degradation in the relevant skills required to safely perform and monitor this exercise. The observations of the experienced check pilot who was present during the practice flight the week before the accident flight supports that conclusion.
Communication within the aircraft
The CASA flying operations inspector (FOI) was the most experienced Cessna 441 pilot on board the flight, in terms of overall experience and instructing/checking on the type. In a crew resource management context he was therefore a valuable available resource during the flight. Despite this, the aircraft was not fitted with a communication system that permitted the FOI to have a headset with speaker or microphone to communicate directly with the inductee and chief pilot. That reduced his ability to engage with the pilots and actively monitor the exercise, including communication between the inductee and chief pilots.
If a situation developed where the two pilots were struggling to control the aircraft, or there was an issue causing a distraction, the planned process for identifying an unsafe situation was to tap the chief pilot on the shoulder and wait for a response. That means of communication involved probable delay and a requirement to talk over the ambient cockpit noise. As such, it was significantly less effective than speaking to the pilots directly via headset.
While there was insufficient information to determine the extent to which this situation influenced the development of the accident, better communication and visibility of the control inputs and instruments of both pilots would have assisted the FOI to identify the degraded performance and intervene.
Organisational workload and pressure
Rossair had undergone many changes since the merger in 2013 of the former Rossair operation, conducting primarily Cessna 441 charter operations, and the Air South operator, conducting primarily Beechcraft 1900 charter operations. There had been the introduction of the larger EMB 120 aircraft, a significant turnover of key personnel and pilots, and a period of growth as well as shrinkage in operations. Since late 2016, there had been a significant increase in the operator’s work and, according to many within the operator, it was struggling to conduct the required work with the number of aircraft and pilots available. The operator was in a process of expanding its operations to include more aircraft and pilots, as well as integrating another operator’s operations into the same AOC.
A chief pilot is a safety-critical and important role within an organisation. The chief pilot of Rossair was managing many responsibilities, as is normally associated with a chief pilot role in a charter operator of this size. However, based on the available evidence, the amount of work being completed by the chief pilot, in addition to flying duties, while preparing for check pilot roles on two aircraft types, was very high, and it had probably been high for a sustained period of time. He was likely exceeding the required duty limits to complete both the flying and management duties, in a time of growth, understaffing, little (if any) redundancy of personnel in key positions and to some extent uncertainty.
In addition to workload, the chief pilot also probably felt a significant degree of pressure to ensure that his tasks would be completed successfully, as not doing so could have affected the viability of some or all of the operator’s activities.
Sustained periods of high workload and pressure can lead to chronic fatigue and/or chronic stress, as well as potentially periods of acute fatigue or stress. All of these effects can influence performance and increase the likelihood of error, which is of concern for someone conducting a safety-critical role, including normal flying duties and also check pilot duties. The extent to which an individual’s performance would be affected by high workload and pressure is highly variable, depending on a range of personal and situational factors, including an individual’s coping mechanisms and available support processes. However, high levels of workload, pressure and or stress have previously been associated with accidents and serious incidents involving key personnel, such as chief pilots[18] and check pilots.[19]
The chief pilot’s workload and pressure would have been exacerbated in the weeks leading up to the accident with the unexpected absence of the head of aircraft airworthiness and maintenance control (HAAMC) due to work-related stress and, more importantly, the unavailability of the Cessna 441 fleet manager to conduct any proficiency checks or flying duties for an extended period. Despite his existing high workload, he took on the additional responsibility and workload of becoming a Cessna 441 check pilot.
In terms of the actual events on the day, there is undoubtedly a level of elevated workload, pressure and stress associated with any in-flight emergency in an aircraft, regardless of whether it is real or simulated. In addition, there is also workload, pressure and/or stress associated with undertaking a proficiency check, or being assessed for a particular role. A 2011 New Zealand Transport Accident Investigation Commission (TAIC) report[20] discussed the potential for ’evaluative stress’, or stress coming from a check flight, which creates a change in flight deck dynamics when pilots are having their performance assessed. Additionally, an ATSB report (AO2014189) identified the risk of a pilot sleeping poorly prior to a check flight.
However, there is insufficient evidence to conclude that the chief pilot’s performance during the accident flight was affected by the sustained workload and pressure in the preceding months, or the specific workload and pressure associated with conducting the check. He was reported to have been well rested the night before, and there were no reports to suggest that his behaviour or demeanour on the day of the accident was unusual or problematic.
In addition to the chief pilot, there was also evidence that other key management personnel within the operator had been experiencing sustained periods of workload and pressure in the months leading up to the accident. Although some level of workload and pressure is unavoidable in any organisation, the available evidence indicates that the levels of workload and pressure during 2017 were clearly problematic for the chief pilot and some other key personnel.
Regulatory oversight of Rossair
The purpose of regulatory oversight is to ensure operators are meeting regulatory compliance and to monitor the ongoing safety health and maturity of the operators. This oversight is comprised of both regulatory services activities and surveillance activities.
In the case of Rossair, the Civil Aviation Safety Authority (CASA) had conducted a significant number of regulatory approval activities on the operator in recent years. In addition, the Adelaide Certificate Management Team (CMT) had regular and frequent contact with Rossair management personnel, particularly its chief pilots but also to some extent the HAAMCs and chief executive officers. This included during the months leading up to the accident.
The informal approach to conducting surveillance is undoubtedly a useful engagement tool, and overall the significant level of interaction CASA personnel had with some of the operator’s key personnel enabled CASA to have a reasonable understanding of the operator’s activities and the effectiveness and suitability of its structure and processes. Based on this approach, it had not identified any regulatory breaches on the operator’s operations. However, there were two limitations or problematic aspects of its oversight approach.
Firstly, much of the informal interaction that occurred between CASA and the operator’s key personnel was not documented. Some observations were recorded, as required, in authorisation holder performance indicator (AHPI) assessments. However, this was general in nature. In addition, some of the regulatory services activities were also not fully or effectively documented, such as the operations manual approvals or flight observations. This limited amount of documentation restricted the sharing of information among CASA personnel, and increased the potential for subjectivity when making assessments. It also limited the ability for CASA to objectively and systematically understand trends or make assessments over time.
Secondly, there had been very little formal surveillance conducted on the operator in recent years. The last systemic audit conducted on the operator was in March 2012, conducted on Air South’s Beechcraft 1900 prior to the merger with Rossair’s Cessna 441 operation. CASA had conducted surveillance events in the first half of 2014 on the Cessna 441 operation, which had led to a number of findings regarding flight operations matters. However, since then, there had been little if any formal surveillance conducted on the operator’s activities.
The CASA Surveillance Manual (CSM) recommended that, for an operator such as Rossair, there should have been one systems audit every year. The ATSB accepts that this recommended frequency may not be achievable for many operators, and that the use of regulatory services tasks and informal communications can provide very useful insights to determine when more formal surveillance activities should occur.
Nonetheless, the context of Rossair suggested that more formal surveillance activities should have been conducted. Since early 2014, the operator had introduced passenger-carrying operations in EMB 120 aircraft, and there had been significant turnover of pilots and key personnel, including during 2016 and early 2017.
CASA had planned and initiated a systems audit in November 2016, and the scope of the planned audit appeared to be relevant and appropriate for an operator of Rossair’s size and complexity. However, the audit was discontinued shortly after it commenced, with limited information recorded, and the audit had not yet recommenced by the time of the accident on 30 May 2017. In the meantime, CASA personnel had documented concerns about high workload, stress and commercial pressures on key personnel. CASA was also aware of the operator’s plans to expand its operations.
In summary, the level of interaction CASA had with the operator was significant and commendable. However, its ability to fully understand the effectiveness or suitability of the operator’s processes based on this interaction was limited. Given the significant changes in the operator, and known problems with the workload and stress of key personnel, a more systematic review and assessment of its operations would have provided more assurance that its informal assessment of the operator and its key personnel was warranted.
With regards to the specific approval to conduct the check pilot observation on 30 May 2017, CASA personnel reported they had considered the risk factors and mitigators associated with the activity. They believed that, as:
- they knew the flying background of both the chief pilot and the inductee pilot
- had observed them fly previously, and
- knew that both pilots had completed flights recently with known instructors with no reported problems,
that both pilots had the skills for successful conduct of the flight.
Recorded data
Given the weight and seating configuration of the aircraft, neither a cockpit voice recorder or a flight data recorder were required to be fitted to the aircraft. Additionally, at low level, Renmark Airport is outside of surveillance coverage. Consequently, the data recovered for this flight was confined to information broadcast by a portable device carried by the FOI.
The limited recorded flight information available to the investigation prevented a full analysis of the handling aspects and cockpit communications, This in turn restricted the extent to which the factors contributing to the accident could be analysed and the potential for identification of safety issues and areas for safety improvement.
In 2008 The ATSB made a recommendation (R2006004) to CASA regarding the fitment of lightweight recorders. Specifically:
The Australian Transport Safety Bureau recommends that the Civil Aviation Safety Authority (CASA) review the requirements for the carriage of on-board recording devices in Australian registered aircraft as a consequence of technical developments.
CASA conducted a cost-benefit analysis with respect to mandating the carriage of on board recorders in smaller aircraft, but determined that priority be given to fitment of accident prevention technologies, such as airborne collision avoidance systems, terrain avoidance and warning systems and automatic dependent surveillance broadcast equipment. Based on that justification, the recommendation was accepted and closed.
Despite this, the ATSB continues to investigate accidents where the absence of on board recordings has limited the understanding of the occurrence. Notably, investigation AO-2017-118 (Collision with water involving a de Havilland Canada DHC-2 Beaver aircraft, VH-NOO, at Jerusalem Bay, Hawkesbury River, New South Wales on 31 December 2017) was similarly restricted by data availability. That investigation will re-examine the fitment of lightweight recording systems for passenger operations in aircraft with a maximum take-off weight of less than 5,700 kg in more detail.
__________
- NTSB Investigation AAR-11-04: Crash after encounter with instrument meteorological conditions during take off from remove landing site New Mexico State Police Agusta S.p.A. A-109E, N606SP
- ATSB investigation 200404589: Aircraft Loss of Control, Lake George, NSW; VH-TAG, SA227-AC Metro III
- TAIC investigation AO-2011-007: Descent below instrument approach minima, Christchurch International Airport, 29 October 2011
From the evidence available, the following findings are made with respect to the collision with terrain involving Cessna 441, registered VH-XMJ, that occurred 4 km west of Renmark Airport, South Australia on 30 May 2017. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
- Following a planned simulated engine failure after take-off, the aircraft did not achieve the expected single engine climb performance, or target airspeed, over the final 30 seconds of the flight.
- The exercise was not discontinued when the aircraft’s single engine performance and airspeed were not attained. That was probably because the degraded aircraft performance, or the associated risk, were not recognised by the pilots occupying the control seats.
- It is likely that the method of simulating the engine failure and pilot control inputs, together or in isolation, led to reduced single engine aircraft performance and asymmetric loss of control.
- Not following the recommended procedure for simulating an engine failure in the Cessna 441 pilot’s operating handbook meant that there was insufficient height to recover following the loss of control.
Other factors that increased risk
- The Rossair training and checking manual procedure for a simulated engine failure in a turboprop aircraft was inappropriate and, if followed, increased the risk of asymmetric control loss.
- The flying operations inspector was not in a control seat and did not share a communication systems with the crew. Consequently, he had reduced ability to actively monitor the flight and communicate any identified performance degradation.
- The inductee pilot had limited recent experience in the Cessna 441, and the chief pilot had an extended time period between being trained and being tested as a check pilot on this aircraft. While both pilots performed the same exercise during a practice flight the week before, it is probable that these two factors led to a degradation in the skills required to safely perform and monitor the simulated engine failure exercise.
- The chief pilot and other key operational managers within Rossair were experiencing high levels of workload and pressure during the months leading up to the accident.
- In the 5 years leading up to the accident, the Civil Aviation Safety Authority had conducted numerous regulatory service tasks for the air transport operator and had regular communication with the operator’s chief pilots and other personnel. However, it had not conducted a systemic or detailed audit during that period, and its focus on a largely informal and often undocumented approach to oversight increased the risk that organisational or systemic issues associated with the operator would not be effectively identified and addressed.
Other findings
- A lack of recorded data from this aircraft reduced the available evidence about handling aspects and cockpit communications. This limited the extent to which potential factors contributing to the accident could be analysed.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action taken by the Civil Aviation Safety Authority in response to this occurrence.
Following the accident, CASA issued temporary management instruction (TMI) 2017-004 to provide interim instructions to CASA officers tasked to conduct in-aircraft activity as a CASA employee. These instructions were issued with the caveat that CASA did not know the contributing factors to this accident. The instruction’s intent was to generally provide higher risk protection around operations involving CASA flying operations inspectors (FOIs).
The operating requirements differed, based on whether the CASA FOI was occupying a control or non‑control seat in the aircraft. For key personnel and check pilot assessments when the FOI was in a position other than a control seat, the TMI required:
- Emergencies were not to be simulated below 1000 ft above ground level and initiated at VYSE + 10 kt.
- The assessment could only be conducted if the non-control seat was in the immediate vicinity of the operating crew, suitable communication existed and a pre-flight briefing was conducted.
- The CASA FOI had to have evidence of each person at the controls meeting the requirements of Civil Aviation Safety Regulation 1998 Regulation 61.385 – General pilot competency requirements in relation to the manoeuvres intended to be conducted and recover from the above manoeuvres in the event of mishandling. For example, a person who does not regularly (and recently) operate the aircraft may be unable to demonstrate the general competency requirements to the satisfaction of a CASA officer.
- The FOI had to have evidence that the person under check had been trained and considered competent / recommended by someone other than themselves. The time between the competency recommendation and the assessment flight could be no more than 28 days.
The temporary management instruction published on the CASA website expired in June 2018. This was reissued as an amended internal document in June 2018 and November 2019, with an expiry of May 2020. One additional relevant inclusion in the amended versions was a requirement for CASA officers to ensure the requirements of the new CASA exemption 58/18 - Carriage of passengers on proficiency check and flight test flight instrument (updated to 58/19 in May 2019).
As of April 2020, the TMI conditions had not been incorporated into regulation.
Sources of information
The sources of information during the investigation included the:
- former aircraft operator and staff
- aircraft, engine and propeller manufacturers
- OzRunways flight data
- Bureau of Meteorology
- Civil Aviation Safety Authority
- South Australia Police and Coroner’s Court.
References
Arthur Jr, W; Bennett, Jr, W; Stanush, PL and McNelly, TL 1988, Factors that influence skill decay and retention: A quantitative review and analysis. Human Performance 11(1) 57-101.
Civil Aviation Authority 2014, Standards Document 14, version 7 – Guidance for Examiners and Information for Pilots of Single Pilot Aeroplanes. Civil Aviation Authority, United Kingdom.
Civil Aviation Safety Authority 2002, Even worse than the real thing. Flight Safety Australia, March-April 2002.
Civil Aviation Safety Authority 2015, Civil Aviation Advisory Publication 217-1(0): CAR 217 Flight Crew – Training and checking organisations. Civil Aviation Safety Authority.
Civil Aviation Safety Authority 2015, Civil Aviation Advisory Publication 5.23-1(2): Multi-engine aeroplane operations and training. Civil Aviation Safety Authority.
Civil Aviation Safety Authority 2016, Air Operators Certificate Handbook Volume 2 – Flying Operations. November 2016. Civil Aviation Safety Authority.
Civil Aviation Safety Authority 2016, Air Operators Certificate Process Manual – November 2016. Civil Aviation Safety Authority.
Civil Aviation Safety Authority 2016, Flying Qualification and Training Handbook – October 2016. Civil Aviation Safety Authority.
Civil Aviation Safety Authority 2017, CASA Surveillance Manual, Version 2.4 – April 2017. Civil Aviation Safety Authority.
Federal Aviation Administration 2016, Airplane Flying Handbook FAA-H-8038-3B. US Department of Transportation, Federal Aviation Administration, Flight Standards Service.
Orlady HM and Orlady LM 1999, Human Factors in Multi-Crew Flight Operations. Ashgate, Aldershot, England.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the former aircraft operator and staff that provided cited information to the ATSB, the aircraft, engine and propeller manufacturers, the United States National Transportation Safety Board and the Civil Aviation Safety Authority.
Submissions were received from the former aircraft operator, Textron Aviation Inc, Hartzell Propeller, Honeywell, the Civil Aviation Safety Authority, and some of the previous employees of the operator. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2020
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
Chief pilot details
| Licence details: | Air Transport Pilot (Aeroplane) Licence, issued April 2001 |
| Endorsements: | TWU, MPPC, GTE, PXS, RU |
| Ratings: | EMB 120, MEA, SEA, SEH |
| Medical certificate: | Class 1, valid to 3 August 2017 |
| Aeronautical experience: | Approximately 5,000 hours (Aeroplane) |
| Last flight review: | 22 October 2016 |
Inductee pilot details
| Licence details: | Air Transport Pilot (Aeroplane) Licence, issued December 1991 |
| Endorsements: | TWU, MPPC, MEAC, GTE, PXS, RU |
| Ratings: | FK 50, FK 70/100, FK 28, SA 226/227, SF 340, MEA, SEA |
| Medical certificate: | Class 1, valid to 24 June 2017 |
| Aeronautical experience: | Approximately 14,750 hours |
| Last flight review: | 13 February 2017 |