
Executive summary
What happened
On 15 August 2024, a Fairchild SA227-DC Metroliner 23, operated by Skippers Aviation, departed Perth Airport, Western Australia (WA) for a flight to Bronzewing Airport, WA, with 12 passengers and 2 flight crew on board. As the aircraft climbed, the crew noted high-temperature air and light smoke emanating from flight deck air vents.
As the smoke quickly increased, the crew commenced actioning the ‘smoke in aircraft’ checklist but required items of the checklist were not completed – the first officer did not don an oxygen mask due to difficulty with its usage, and the left bleed air system was not selected ‘off’. Instead, the crew commenced preparations for a return to Perth and subsequently, the left wing overheat light illuminated. The crew then actioned the ‘wheel well and wing overheat’ checklist and selected the left bleed air system ‘off’, which stopped the smoke ingress into the cabin, but elected not to complete the required action of extending the landing gear.
During the return to Perth, the aircraft deviated both above and below the altitude assigned by air traffic control including a descent to 639 ft below the lowest safe altitude. The crew then completed the ILS approach and landed without further incident. The aircraft was not damaged, and there were no crew or passenger injuries.
What the ATSB found
The ATSB found that a failure within the left air cycle machine prior to departure resulted in hot engine bleed air and smoke entering the cabin and that items on the ‘smoke in aircraft’ checklist were not completed. Consequently, the smoke ingress into the cabin continued and during the return, the left air conditioning duct overheated, and the wing overheat light illuminated. Furthermore, the first officer’s decision not to don an oxygen mask increased their risk of impairment or incapacitation. A later decision not to extend the landing gear, as required by the response checklist, had the potential to increase risk if the wing overheat indication had been associated with a brake fire or wheel well overheat.
The ATSB determined that the workload associated with the in-flight response to the smoke in the cockpit and wing overheat indication adversely affected the flight crew's performance, leading to errors in flight path adherence, checklist completion and decision making.
During the return to Perth, the first officer readback an air traffic control altitude instruction as 2,000 ft AMSL instead of 2,800 ft AMSL. The controller did not identify or correct the error however, following a query from the crew, this was later corrected. Finally, after the assigned altitude had been confirmed by the crew, the aircraft descended below the lowest safe altitude. While the crew were advised of the deviation by air traffic control, the required ‘safety alert’ wording was not used.
What has been done as a result
Following the occurrence, the operator conducted a refresher training course for flight crew on emergency response briefings and a theory examination for flight crew on bleed air, pneumatics, pressurisation and fire warning systems. Practical training sessions were also held for flight crew on revised emergency procedures and the use of the crew oxygen system.
The operator also changed the Metroliner 23 flight crew training program to include a revised Line Oriented Flight Training (LOFT) program including more comprehensive oxygen system training and a presentation on the Metroliner 23 oxygen system.
Safety message
This occurrence highlights the importance of careful and methodical checklist completion. In this case, not completing a checklist resulted in increased risk to the flight and an avoidable increase to an already high workload. This in turn led to later decision-making and flight path management errors.
Additionally, the incident also emphasises the importance of flight crew familiarising themselves with the operation and use of the onboard emergency equipment. When exposed to an environment of smoke and fumes, flight crew must ensure that emergency breathing equipment is correctly utilised.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On the morning of 15 August 2024, the crew of a Fairchild SA227-DC Metroliner 23 aircraft operated by Skippers Aviation, registered VH-WBQ and callsign ‘Skippy 5003’, taxied the aircraft to runway 24 at Perth Airport, Western Australia (WA) for a flight to Bronzewing Airport, WA. There were 12 passengers on board and the flight crew comprised the captain acting as pilot flying,[1] and the first officer acting as pilot monitoring.
As the aircraft taxied to the runway, the first officer noted that the cabin temperature was unusually warm and selected ‘full cold’ on the temperature selector.
At 0746, the aircraft departed runway 24 and turned left turn following the REPOK 1 standard instrument departure. As the aircraft climbed above about 1,500 ft above mean sea level (AMSL), the captain noted that the cabin temperature was warm and asked the first officer to select full cold on the temperature selector. The first officer responded by advising that full cold was already selected.
As the aircraft climbed above about 3,000 ft AMSL, the first officer attempted to reduce the high cabin temperature by selecting ‘auto’ on the temperature controller before then reselecting ‘full cold’. At about this time, the crew noted that vents on the captain’s (left) side of the flight deck (Figure 1) were blowing very hot air while the vents on the first officer’s (right) side blew the expected cool air.
Figure 1: Exemplar Metroliner 23 flight deck

Source: Matt Hayes, annotated by the ATSB
In response, the captain attempted to close the vent but found it too hot to touch. At the same time, they observed light smoke emanating from the vent. The smoke quickly increased, and the crew commenced the quick reference handbook (QRH) ‘smoke in aircraft’ checklist memory items.[2]
These memory items required the crew to don oxygen masks, establish communications (see the section titled Crew oxygen system) and consider donning smoke goggles. As the smoke was not impacting their vision, both flight crew members elected not to don smoke goggles. The captain donned an oxygen mask and made the required audio selections to establish communications using the mask.
The first officer encountered difficulties in adjusting the mask straps and could not get the mask to fit. They also did not make the required selections to establish communications using the mask, which resulted in the first officer hearing breathing noses through the headset and not being able to communicate using the oxygen mask microphone. As a result of these difficulties, the first officer elected not to wear the mask at that time.
The first officer retrieved the QRH ‘smoke in aircraft’ checklist to confirm the required memory actions had been completed and complete the remaining items of the checklist. For smoke emanating from a bleed air source, such as the air-conditioning system, the checklist required selecting the appropriate bleed air system ‘off’ (see the section titled Quick reference handbook). Before completing those checklist actions, the crew made a PAN PAN[3] broadcast advising air traffic control that there was smoke in the cockpit and that a return to Perth was required. The crew then began preparing for the return to Perth and did not complete the remaining items of the checklist at that time.
At 0751, the Perth Departures air traffic controller acknowledged the PAN transmission and instructed the crew to turn to a heading[4] of 360° and descend to 3,000 ft AMSL to commence the return. At this time, air traffic control also activated the Perth Airport emergency services.
Shortly after, the controller handed the crew over to the Perth Approach controller. One minute later, the approach controller instructed the crew to turn to a heading of 240° and descend to the lowest safe altitude of 2,800 ft AMSL. The first officer incorrectly read back the descent altitude as 2,000 ft AMSL, however the controller did not identify the error (Figure 2). The crew subsequently began descending the aircraft.
Figure 2: Flight path of VH-WBQ

Source: Airservices Australia and Google Earth, annotated by the ATSB
As the aircraft descended, the captain assisted the first officer with donning the oxygen mask and making the required audio selections to establish communications. From this time on, the use of the oxygen mask significantly reduced the intelligibility of the first officer’s radio broadcasts.
At 0756, the crew levelled the aircraft at 2,800 ft AMSL and contacted the controller to confirm the assigned altitude. The controller confirmed the altitude was 2,800 ft AMSL and the assigned heading as 180°. The first officer readback the altitude and heading instructions correctly.
At 0756, as the aircraft turned to the assigned heading, a descent commenced from 2,800 ft AMSL (Figure 3). About 50 seconds later, having observed the descent, the air traffic controller advised the crew to maintain 2,800 ft AMSL and that 2,800 ft AMSL was the lowest safe altitude. The crew immediately commenced climbing the aircraft, having descended to 2,338 ft AMSL (about 1,600 ft above ground level (AGL)).
Figure 3: Flightpath of VH-WBQ after the incorrect readback

Source: Airservices Australia and Google Earth, annotated by the ATSB
In response to the air traffic control instruction, the first officer replied stating ‘unable, Skippy 5003’ intending to convey that the crew were ‘unable’ to clearly hear the instructions. The controller interpreted the statement to mean that the crew were unable to maintain 2,800 ft AMSL and queried if the crew were in visual conditions. The first officer replied that the aircraft was not visual. At the same time, the air traffic control system generated a cleared level adherence monitoring (CLAM) alert for the aircraft. The controller, believing that the aircraft could not maintain altitude and aware that the Perth runway 24 instrument landing system (ILS) provided the lowest available minimum safe altitude, provided the crew with heading instructions directly to the ILS localiser.
While tracking toward the localiser, the aircraft continued climbing until 0757:57 when it reached 2,717 ft AMSL, before it once again commenced descending. At about this time, the crew returned to the ‘smoke in aircraft’ QRH checklist to complete the remaining items, but before these could be completed, the left wing overheat light illuminated continuously (see the section titled Quick reference handbook). The crew then actioned the relevant memory items of the ‘wheel well and wing overheat’ QRH checklist, including switching off the left bleed air system. Soon after switching off the bleed air, the crew noted that the smoke ceased. The checklist also required the crew to extend the main landing gear. As the aircraft was descending at a speed of over 220 kt (in excess of the 175 kt maximum landing gear extension speed), and wanting to expedite the return, the crew decided not to extend the landing gear at that time.
The aircraft continued descending and at 0758:23 reached 2,161 ft AMSL (about 1,200 ft AGL) before recommencing a climb. The air traffic controller observed the aircraft descend below the minimum safe altitude and, shortly after, a second CLAM alert was generated. The controller did not advise the crew of the low altitude as they believed the crew were unable to maintain altitude and that contacting them would only increase their workload.
At the same time, the crew commenced a right turn to intercept the ILS localiser and 12 seconds later, while still wearing the oxygen masks, the crew contacted the controller to request airport emergency services. The controller did not comprehend the broadcast and asked the crew to repeat the request. The crew repeated the request, but the controller again could not understand it. The controller did not query the crew further and commenced coordinating the handover of the aircraft to the Perth Tower controller. During this period, the left wing overheat light extinguished.
At 0758:41, the aircraft crossed the ILS localiser while climbing above about 2,800 ft AMSL. The climb and right turn continued until the aircraft levelled at about 3,000 ft AMSL for 7 seconds before recommencing a descent. The aircraft descended to 2,751 ft AMSL, before again climbing. The right turn continued for a further short period, followed by the aircraft commencing an intercept of the localiser from the left side. The aircraft climbed for a final time to 2,947 ft AMSL before again commencing a descent and levelling at 2,800 ft AMSL about 10 seconds later. The aircraft then maintained 2,800 ft AMSL until intercepting the localiser at 0800.
The crew completed the ILS approach and landed without further incident. The aircraft was not damaged, and there were no crew or passenger injuries.
Context
Crew details
The captain held a commercial pilot licence (aeroplane) and class 1 aviation medical certificate. The captain commenced flying with Skippers Aviation as a first officer in May 2022 before progressing to captain in April 2024 and had 1,484 hours of flying experience, of which 1,270 hours were accrued in the Metroliner.
The first officer held a commercial pilot licence (aeroplane) and class 1 aviation medical certificate. The first officer commenced flying with Skippers Aviation in April 2024 and had 509 hours of flying experience, of which 247 hours were obtained in the Metroliner.
The ATSB found no indicators that the flight crewmembers were experiencing a level of fatigue known to affect performance.
Aircraft details
The Fairchild SA227-DC Metroliner 23 is a twin-engine turboprop regional airliner and an enhanced version of the Metroliner series that initially entered service in 1972. The aircraft was fitted with an analogue cockpit and was not equipped with an autopilot or flight director. VH-WBQ (Figure 4) was configured with 2 crew seats and 19 passenger seats.
Figure 4: VH-WBQ

Source: Lloyd Cartwright
Crew oxygen system
The aircraft was fitted with oxygen masks for use by the flight crew during a smoke event. After donning the masks, the following steps were to be followed to establish communications between the crew members and when using the aircraft radios:
- select the microphone switch at the rear of the cockpit side panel from ‘boom’ to ‘mask’
- deselect the cockpit button on the audio panel
- to communicate with the other flight crew member, use the intercom push-to-talk button on the front side of the control column
- to transmit using the radio use the push-to-talk button on the reverse side of the control column as normal.
If these steps were not fully followed, breathing noises would be heard through the crew’s headsets that could distract from, and disrupt, normal communications.
Air conditioning system
The aircraft was fitted with 2 identical air conditioning systems, one associated with each engine, and feeding conditioned air to the associated side of the flight deck and cabin. Each air conditioning system was supplied with hot, high pressure bleed air from the engine compressor through a shut‑off valve to the air cycle machine. The air cycle machine used ambient air to cool the bleed air and incorporated a mixing valve (for cabin temperature control).
An engineering evaluation of the left engine air cycle machine, conducted after the flight, found that it had overheated and that the cooling turbine was expelling oil. The hot air mixing valve was also found to be operating intermittently and sticking in various positions.
Quick reference handbook
The operator’s Metroliner 23 Flight Operations Manual included quick reference handbook (QRH) checklists with memory items specified within red brackets. This manual provided the following guidance for usage:
In a situation where the PM has had to reference the QRH to cross check correct memory item completion they will then announce to the PF that he/she is “Standing by with the ……..checklist”…Both pilots will then silently carry out the circuit breaker check at this point after which the PF then commands “Continue” when he/she is ready, and the checklist is read from the beginning.
The checklist must be announced by title and checklist notes must be read before proceeding with the checklist. A checklist is not completed until stating, “…. checklist complete”.
QRH items shall be read and actioned (any memory items will just be checked for completion) by the PM (where practical). A self-challenge and response technique is required.
Most of the PF attention should be directed at flying the aircraft; however, he must also be kept informed with the management process of accomplishing the appropriate procedures/checklist.
It would be appropriate for the PM to delay reading of the checklist procedure until the PF is in a position to monitor and assist if required. Confusion is often a problem area when conducting QRH procedures. Checklist procedures must not be rushed. It is important crews conduct checklists in a careful and controlled manner.
To stop smoke ingress into the aircraft from a bleed air source such as the air conditioning system, the ‘smoke in aircraft’ checklist required the crew to select the affected bleed air system ‘off’ (Figure 5).
Figure 5: Smoke in aircraft QRH checklist

Source: Operator, annotated by the ATSB
The wing overheat annunciator illuminated with either a steady or flashing indication. A steady light indicated a brake fire, wheel well or air conditioning duct overheat condition. A flashing light indicated a wing leading edge bleed air line failure or an overheated generator wire. The QRH checklist for a steady indication (Figure 6) required the crew to extend the landing gear to reduce the risk of a brake or tyre fire, overheat condition or a tyre explosion.
Figure 6: Wheel well and wing overheat, steady light QRH checklist
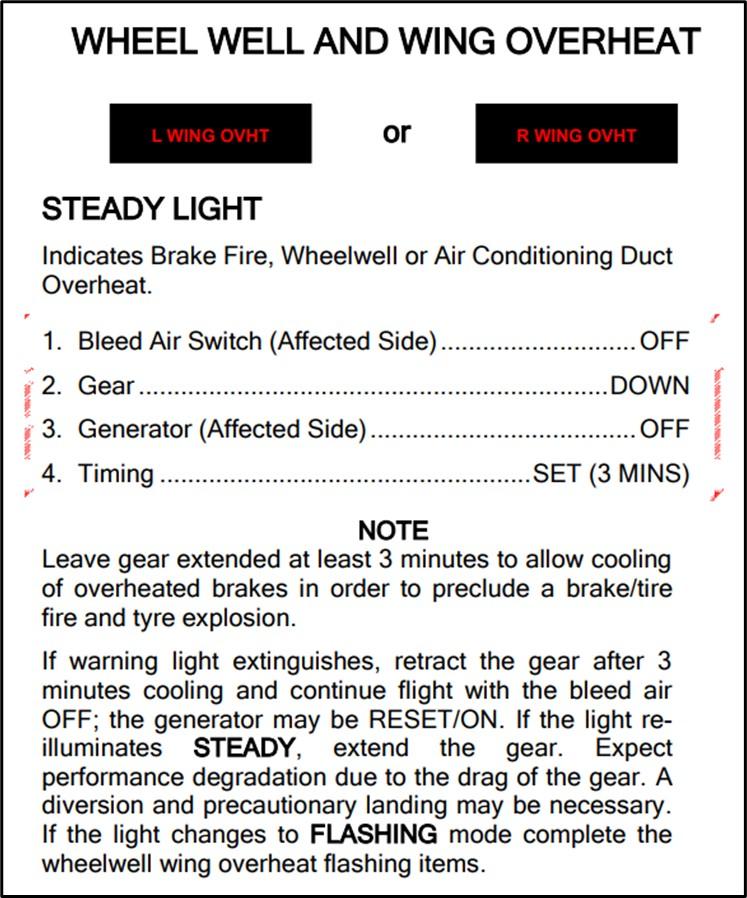
Source: Operator
Smoke and fumes exposure
The United States Federal Aviation Administration pilot safety brochure Smoke toxicity highlighted that smoke inhalation should be recognised as a very real danger. It also stated that ‘smoke gas levels do not need to be lethal to seriously impair a pilot’s performance’.
ATSB research report AR-2013-213 Analysis of fumes and smoke events in Australian aviation from 2008 to 2012: A joint initiative of Australian aviation safety agencies found that over 1,000 fumes/smoke events were reported to the ATSB and the Civil Aviation Safety Authority in the period from 2008–2012. The report highlighted that fumes associated with these events may have the potential to pose a health risk through eye/skin irritation, difficulty in breathing, incapacitation or illness. This was especially the case if the fumes were associated with particulates (smoke) or fire. However, while occurrences involving smoke were more likely to result in an outcome than a fumes‑only event, the research also found that ‘very few led to a serious consequential event (such as a forced landing) or outcome such as fire or crew incapacitation’.
Air traffic control safety alert
The air traffic control manual of air traffic services provided the following guidance for issuing a safety alert:
Unless the pilot has advised that action is being taken to resolve the situation or that the other aircraft is in sight, issue a safety alert prefixed by the phrase 'SAFETY ALERT' when you become aware that an aircraft is in a situation that places it in unsafe proximity to:
a) terrain;
b) obstruction;
c) active Prohibited/Restricted/Military Operating Areas; or
d) other aircraft.
As the crew prepared the aircraft for the return to Perth, it descended below the 2,800 ft altitude assigned by the air traffic controller. The controller identified the aircraft descending below the assigned altitude and contacted the crew stating, ‘maintain 2,800, 2,800 lowest safe’, but the broadcast was not prefixed by the required statement ‘safety alert’.
Meteorology
From soon after take-off until after the aircraft was established on the ILS approach, the flight was conducted in instrument meteorological conditions.[5]
At 0800, the Bureau of Meteorology (BoM) automatic weather station at Perth Airport recorded the wind as 5 kt from 222° magnetic. Cloud cover was recorded as few[6] at 1,267 ft above mean sea level (AMSL), scattered at 1,867 ft AMSL and broken at 3,067 ft AMSL. Visibility was recorded as 9,000 m in light rain showers.
Recorded data
Airservices Australia provided recorded air traffic control audio and surveillance data.
During maintenance actions following the occurrence, the aircraft electrical system was powered‑up and the cockpit voice recording of the incident flight was overwritten.
Flight data recorded by the aircraft’s flight data recorder, combined with recorded surveillance and audio data is presented in Figure 7.
Figure 7: Recorded flight data from 0756 to 0800

Source: ATSB
Safety analysis
Air conditioning pack failure and checklist error
The unusually high temperature noted by the first officer during the taxi to the runway, combined with the findings of the post‑event engineering examination, indicated that the left air cycle machine (ACM) failed prior to departure. This failure resulted in oil being expelled from the ACM cooling turbine and unconditioned hot bleed air entering the air conditioning system. This in turn resulted in the temperature control difficulties faced by the crew and, after take-off, smoke being emitted from the left side flight deck and cabin vents.
In response to the smoke, the crew actioned the memory items of the ‘smoke in aircraft’ checklist. This included donning oxygen masks however the first officer had difficulty in fitting the mask and establishing communications with the mask in use. As a result, the first officer elected not to wear the mask. This exposed the first officer to potentially harmful smoke and fumes. While the first officer reported no adverse effects from this exposure, it did increase the risk of impairment and incapacitation.
After completing the checklist memory items, the crew were required to action the complete ‘smoke in aircraft’ quick reference handbook (QRH) checklist to ensure all required actions had been completed. However, before completing the checklist, the crew commenced the actions required to return to Perth as they assessed that task was of higher priority. Had the QRH checklist been subsequently fully completed, the left bleed air would have been selected ‘off’ and this would have stopped the smoke ingress into the cabin. This action would also have likely prevented the later overheating of the air conditioning duct that triggered the ‘wheel well and wing overheat’ annunciation.
Workload and unsafe descents
The aircraft was equipped with analogue instrumentation with no flight automation to reduce flight crew workload and the smoke was detected immediately after take-off while the aircraft was operating in instrument flight conditions. These factors combined to create a high workload period for the relatively inexperienced crew.
Workload has been defined as ‘reflecting the interaction between a specific individual and the demands imposed by a particular task. Workload represents the cost incurred by the human operator in achieving a particular level of performance’ (Orlady and Orlady, 1999). A discussion of the effect of workload on the completion of a task requires an understanding of an individual’s strategies for managing tasks.
An individual has a finite set of mental resources they can assign to a set of tasks (for example, performing a take-off). These resources can change given the individual’s experience and training and the level of stress and fatigue being experienced at the time. An individual will seek to perform at an optimum workload by balancing the demands of their tasks. When workload is low, the individual will seek to take on tasks. When workload becomes excessive the individual must, as a result of their finite mental resources, shed tasks.
An individual can shed tasks in an efficient manner by eliminating performance on low priority tasks. Alternately, they can shed tasks in an inefficient fashion by abandoning tasks that should be performed. Tasks make demands on an individual’s resources through the mental and physical requirements of the task, temporal demands and the wish to achieve performance goals (Hart and Staveland, 1988, and Lee and Liu, 2003).
Examples of errors associated with excessive workload include:[7]
- Flight crew may mishear, misunderstand or miss setting an air traffic control clearance provided during a period of high workload, leading to:
- A deviation from assigned altitude (level bust)
- controlled flight into terrain (CFIT)
- loss of separation from other aircraft, or
- an unstabilised approach.
- The pilot becoming distracted from primary tasks resulting in an error in handling or managing the aircraft.
In response to the smoke and due to the high workload, the crew initially omitted or missed required checklist items (donning the oxygen mask and completing the ‘smoke in aircraft’ checklist). Had the checklist been completed with the left bleed air selected ‘off’ and the oxygen mask fitted, with communications correctly established, the additional workload associated with returning the aircraft to Perth would have been reduced. Furthermore, the increased distraction and workload associated with the response to the subsequent wing overheat annunciation would have been avoided.
Later, when the crew returned to complete the ‘smoke in aircraft’ checklist, they were interrupted by the wing overheat annunciator illuminating. The required response actions further compounded their workload and this likely influenced the decision error to leave the landing gear retracted. While the crew elected not to extend the gear due to their desire to expedite the return, the decision was not fully considered and would have exposed the aircraft to increased risk if the overheat condition had been associated with the landing gear.
The significant workload that the crew were subject to also adversely affected the crew’s management of the aircraft’s flight path. Without automation to reduce workload and support flightpath management, the aircraft deviated above and critically, twice considerably below the assigned and lowest safe altitude. The aircraft also passed through, and then deviated significantly left of, the localiser before the crew recovered and completed the approach.
Air traffic control factors
The clearance to descend to 2,800 ft was incorrectly readback as 2,000 ft by the first officer (who was not wearing the oxygen mask at that time), but this error was not identified by the air traffic controller. The purpose of a clearance readback is to ensure that the clearance has been correctly received and provides the controller an opportunity to correct any errors. As this error was not identified, there was increased risk of the crew descending the aircraft below the minimum safe altitude while still operating in instrument meteorological conditions. However, despite reading back the clearance incorrectly, the crew initially levelled the aircraft at 2,800 ft before querying and confirming the assigned altitude as 2,800 ft. Therefore, the non-identification of the readback error did not contribute to the aircraft descending below the lowest safe altitude.
Despite obtaining confirmation of the assigned altitude, very soon after, the aircraft began descending. The controller identified the aircraft descending below the assigned altitude and contacted the crew, advising them to maintain 2,800 ft as that was the lowest safe altitude. However, this broadcast was not prefixed by the required statement ‘safety alert’. Commencing such a broadcast with the phraseology ‘safety alert’ is designed to alert crews to safety critical information to ensure a response is prioritised and is particularly important during times of high crew workload. Despite the correct phraseology not being used, the broadcast achieved the desired crew response. The recorded data showed that immediately after the controller contacted the crew, the descent was stopped, and the aircraft commenced climbing. As such, the absence of a safety alert did not contribute to the occurrence.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the smoke in the aircraft and descent below lowest safe altitude involving Fairchild Industries SA227-DC, VH-WBQ, 25 km north-east of Perth Airport, Western Australia on 15 August 2024.
Contributing factors
- A failure within the left air cycle machine resulted in hot engine bleed air and smoke entering the cabin soon after take-off. In response, the crew elected to return to Perth.
- After commencing the ‘smoke in aircraft’ checklist memory items, the quick reference handbook checklist was not completed, and the left engine bleed air system was not selected off. As a result, during the return, the left air conditioning duct overheated, and the wing overheat light illuminated.
- The workload associated with the in-flight response to the smoke in the aircraft and wing overheat indication adversely affected the flight crew's performance, leading to errors in flight path adherence, checklist completion and decision‑making.
- On several occasions during the return to Perth Airport, the aircraft deviated above and below the assigned and lowest safe altitude. These deviations included a descent to 639 ft below the lowest safe altitude.
Other factors that increased risk
- Following the smoke entering the cabin, the first officer initially elected not to wear the oxygen mask due to difficulties in donning the mask and then establishing communications. This increased their risk of impairment or incapacitation.
- An incorrect altitude readback from the flight crew was not identified or corrected by air traffic control. Later, after the assigned altitude had been communicated, when the aircraft first descended below the lowest safe altitude, the crew were advised of the deviation by air traffic control, but the required ‘safety alert’ was not issued.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Safety action taken by Skippers Aviation
Line oriented flight training
| Action number: | AO-2024-048-PSA-01 |
| Action organisation: | Skippers Aviation |
In response to this incident, Skippers Aviation:
- revised the Line Oriented Flight Training (LOFT) program to include more comprehensive oxygen system training
- conducted the following refresher training for Metroliner 23 flight crew:
- emergency response briefings
- theory examination for the Metroliner 23 bleed air, pneumatics, pressurisation and fire warning systems.
- practical training of the crew oxygen system
- revised emergency procedures
- updated the aircrew initial and recurrent training to include a presentation on the Metroliner 23 oxygen system.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the flight crew
- the aircraft operator
- Civil Aviation Safety Authority
- Airservices Australia
- recorded data from VH-WBQ.
References
Orlady, HW & Orlady, LM 1999, Human factors in multi-crew flight operations. Ashgate, Aldershot, p. 203.
Hart, SG & Staveland, LE 1988, ‘Development of NASA-TLX (Task Load Index): Results of empirical and theoretical research’, In PA Hancock & N Meshkati (Eds.), Human Mental Workload. North Holland Press, Amsterdam.
Lee, YH & Liu, BS 2003, ‘Inflight workload assessment: Comparison of subjective and physiological measurements’, Aviation, Space, and Environmental Medicine, vol.74, pp. 1078-1084
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the operator
- the flight crew
- the air traffic controller
- Airservices Australia
- Civil Aviation Safety Authority.
A submission was received from Airservices Australia. The submission was reviewed and did not result in any amendment to the report.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] Memory items are checklist items required to be committed to memory to allow an immediate response to high priority abnormal events.
[3] PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[4] All headings used in the report are magnetic.
[5] Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under Instrument Flight Rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[6] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, and ‘broken’ indicates that more than half to almost all the sky is covered.