Executive summary
What happened
On the afternoon of 24 January 2024, a Cessna 172S, registered VH‑CPQ, was being used for pilot training by AltoCap Flight School at Camden Airport, New South Wales.
At 1431 local time, the student commenced circuits with the instructor on board, completing the normal, flapless, glide and missed approaches as briefed. Determining that the student was competent to complete the first solo in the Cessna 172 (and having flown a light sport aircraft previously), the instructor contacted the air traffic control tower stating they would complete ‘a full stop and taxi for a student first solo’ at 1456:50 and this was acknowledged by the controller.
At 1504:39 the student was cleared for take-off and commenced the flight. Towards the end of the downwind leg of the circuit, the aircraft rapidly descended and collided with terrain. The pilot was fatally injured, and the aircraft was destroyed.
What the ATSB found
The ATSB found that prior to turning onto base the aircraft departed level flight and collided steeply with terrain. There was no evidence of any in-flight failure of the airframe structure or flight control system and the engine appeared to have been producing significant power at impact.
In the absence of an identified problem with the aircraft, and in combination with the aircraft manufacturer’s assessment, continual nose-down control input was almost certainly applied to the flight controls throughout the increasingly steep, accelerating descent. The reason for the continued control input could not be determined.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On the afternoon of 24 January 2024, a Cessna 172S, registered VH-CPQ, was being used for pilot training by AltoCap Flight School at Camden Airport, New South Wales.
At 1300 local time the student pilot commenced a lesson with an instructor from the flight school. The instructor conducted a briefing with the student outlining the plan for the lesson. This included outlining the 4 types of landing approaches that would be completed: normal, flapless, glide, and missed approaches.[1] If deemed competent by the instructor, the student would complete their first solo flight (for that aircraft type).[2]
Before the flights, the instructor obtained the weather and the automatic terminal information service (ATIS)[3] data and asked the student to interpret the weather that would be encountered during flight.[4] The instructor then completed an internal company checklist and risk assessment relating to student solos, which indicated an acceptable risk score, in anticipation that the student would be ready for a solo flight after the flights with the instructor on board.
At approximately 1400, the instructor and student completed a pre-flight inspection of the aircraft and commenced the practical aspect of the lesson.
At 1420 the aircraft was taxied to the run-up bay, where pre-flight checklists and a safety briefing were conducted. At 1431, the student commenced circuits with the instructor on board, completing the normal, flapless, glide and missed approaches as briefed. The student requested to complete a fifth approach as the student was, according to the instructor, ‘not happy’ with their original attempt of the flapless approach.
Recorded automatic dependent surveillance–broadcast (ADS-B) data and secondary surveillance radar data was not available for these flights due to the aircraft’s transponder setting.[5] According to the instructor, the student had not set the transponder to ALT mode prior to the first circuit, which the flight school teaches students to do before beginning lessons, and this was noticed by the instructor prior to the first circuit. After noting the transponder had not been placed in ALT mode, the instructor did not turn on ALT mode and had intended to use it as a discussion point after the pilot’s solo flight.
Determining that the student was competent to complete the first solo, the instructor contacted the air traffic control tower stating they would complete ‘a full stop and taxi for a student first solo’ at 1456:50 and this was acknowledged by the controller.
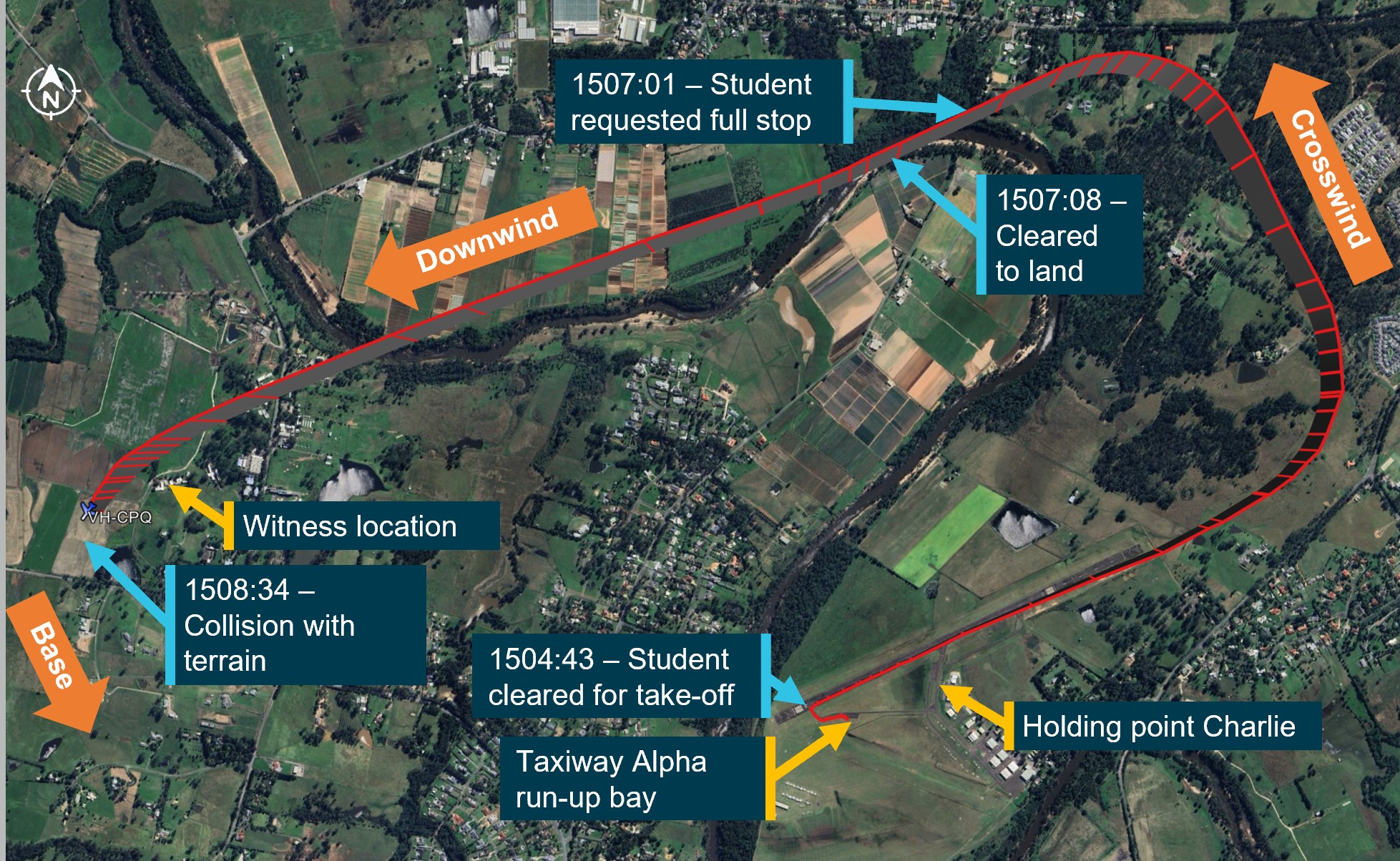
The student landed the aircraft and taxied clear of the runway to the run-up bay just prior to holding point Alpha (Figure 1). The instructor selected the ALT mode on the transponder to allow a viewing of the flightpath of the aircraft online and then exited the aircraft. The instructor informed the student they should complete the take-off checklist again and do everything required to feel comfortable to go solo.
At 1503:41 the student contacted the tower, requesting to taxi to holding point Alpha for runway 06. This was cleared by the tower and the pilot taxied to holding point Alpha.
At 1504:39 the student was cleared for take-off. There were no other aircraft in the area relevant to the occurrence.
The instructor recalled watching the student take off, turn onto the crosswind leg of the circuit and then onto the downwind leg (Figure 1). The instructor walked towards holding point Charlie which was the preferred viewpoint for the entire circuit. The student made a radio call stating ‘Charlie Papa Quebec downwind full stop’ and the instructor recalled hearing this before losing sight of the aircraft behind an obstruction. The pilot sounded normal during all recorded radio transmissions.
The controller issued the student pilot clearance to land 7 seconds later which was acknowledged by the student. No further calls were transmitted from the aircraft.
Figure 1: Flight path overview
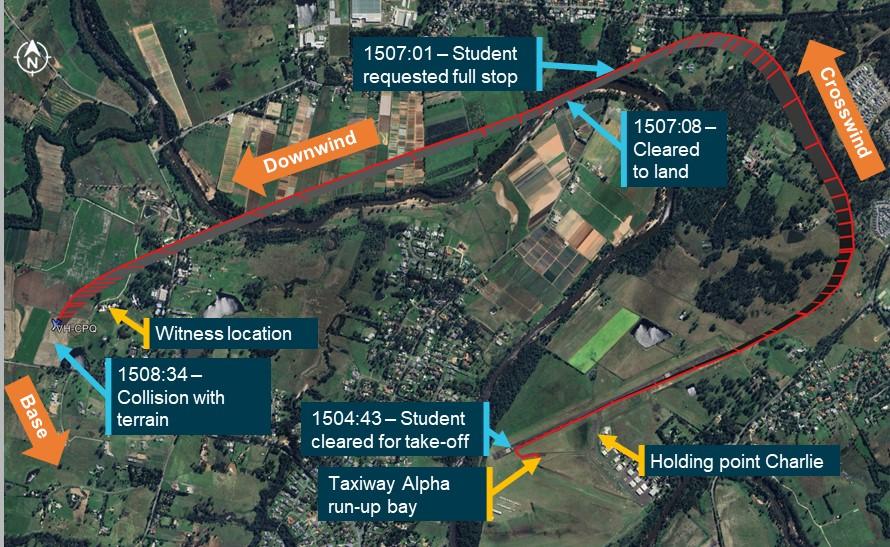
Source: Google Earth, annotated by the ATSB
Upon reaching holding point Charlie, the instructor expected to see the aircraft turning onto the base leg or on base but was unable to see it.
ADS-B data showed the aircraft in level flight at 1,400 ft[6] throughout the downwind leg, initially at about 100 kt groundspeed and decelerating to about 90 kt. The pilot’s target airspeed for the base leg was 75 kt. From abeam the landing threshold, where the instructor had taught the student pilot to reduce power, the aircraft decelerated again to 79 kt groundspeed and an estimated airspeed of 78 kt. At this airspeed, at about the location the aircraft would have been expected to turn onto base, the aircraft descended until it impacted the ground (see Recorded data). The descent and impact were not seen by the controller.
Two witnesses near the airport observed the aircraft descending in a nose-down, wings level attitude and described hearing a ‘whirring’ noise, that they described as an engine over‑revving, before losing sight of the aircraft behind a building. CCTV footage showed the aircraft collided with terrain at 1508:34 at high speed and with an attitude of about 60° nose-down (see Closed-circuit television). The impact was not survivable; the student pilot was fatally injured and the aircraft was destroyed.
Context
Pilot information
Flying history
The student pilot, who at the time of the accident was 16 years old, held a Recreational Aviation Australia (RAAus) pilot certificate[7] issued late June 2023. The student pilot had accumulated 51.3 hours experience on this certificate, including 37.1 hours in a Skyfox Gazelle.[8] The pilot had also completed 4.1 hours of solo flight under the RAAus certificate.
The student commenced flying training with AltoCap Flight School on 17 December 2023 and had completed a total of 6 lessons (Table 1) with the flight school prior to the lesson on the day. In addition to the time accumulated on the RAAus certificate, the pilot had 6.1 hours dual time on the Cessna 172.
The pilot completed a written pre-solo flight exam at AltoCap Flight School on 20 January 2024.
Table 1: Pilot training file
| Lesson date | Topic | Lesson cover | Instructor notes (paraphrased) |
| 16 December 2023 | Straight and level | C172 checklists and pre-flight. Normal, slow fast, and safe slow straight and level. Angle of climb and cruise climb. Cruise descent and glide. | Everything handled well by the pilot. Focus for future is maintaining heading. |
| 23 December 2023 | Climbing and descending, turning | Straight and level, climbing and descending, and turning | Minor assistance in managing the landing sequence. Impressed with the pilot’s progression on GA aircraft. |
| 4 January 2024 | Stalling, steep turns | Demonstration and application of stall and recovery. Steep turns at 45 and 60 degrees. | All sequences well managed |
| 6 January 2024 | Circuits | Initial session of circuits. | Focus is needed on managing airspeed on base and final. |
| 16 January 2024 | Circuits | Normal circuits, flapless, and go-arounds. | Airspeed control not effective on base and final. Glide approaches to be covered next lesson. |
| 20 January 2024 | Circuits | Normal circuits, flapless, and glide approaches. | More practice needed on glide approaches. Pleased with pilots’ performance to date. |
The pilot’s usual instructor recalled that they thought the pilot was ready to fly solo after the previous lesson, although the pilot had not demonstrated an adequate glide approach and they provided that information to the instructor for the pilot’s 24 January lesson.
Up until 24 January 2024, the student’s flight training had been carried out by a grade 3 instructor, who deemed the pilot competent. Due to an initial first solo requiring a check by a minimum grade 2 instructor, the student flew with a new instructor on the accident day.
The flights immediately preceding the accident flight was the first time that this instructor had flown with the student. The instructor reported that, during these flights, the student pilot demonstrated exceptional aircraft handling proficiency and the instructor assessed them as competent and ready for their first solo in the Cessna 172.
Medical information
The pilot held a valid Class 2 aviation medical certificate, received on 25 July 2023. The Civil Aviation Safety Authority’s medical records indicated no known medical issues or medication. Medicare records indicated there had been no medical treatment in the two years prior to the accident.
The pilot’s family reported the pilot to be in good health generally, although sometimes experienced severe migraines that lasted a few hours. The pilot had fainted once, while standing for a long period during an outdoor ceremony, and on another occasion was unable to stay afloat while swimming. In both situations, the pilot had not eaten breakfast. After this, the pilot reportedly understood that it was important to have food and water prior to driving or flying. In December 2023, the pilot had cancelled a lesson due to feeling unwell.
It was reported that the pilot had eaten on the morning of the accident and during a phone conversation with a family member at about 1400 seemed normal.
The pilot’s family and high school reported the pilot was not known for risk-taking behaviour and had no known, significant personal, psychological or social concerns. The instructor recalled the pilot was excited to fly the aircraft prior to the lesson. A witness who was with the pilot just prior to the lesson stated the pilot was in a good mood and seemed excited at the prospect of completing their first solo in the Cessna 172.
As part of a standard safety assessment prior to the accident flight, the student self-assessed against IMSAFE criteria (illness, medication, stress, alcohol, fatigue, eating/hydration) and obtained the lowest possible score.
A post-mortem carbon monoxide and drug screening was clear. A post-mortem examination report stated that 'the presence and/or significance of any natural disease could not be assessed’.
Aircraft information
The Cessna 172 is a high-wing, 4-seat, all-metal aircraft with fixed landing gear. It is powered by a single 4-cylinder Lycoming IO-360-L2A piston engine driving a fixed-pitch propeller. It is commonly used for basic flight training, in part due to its docile flying characteristics. The aircraft has a conventional flight control system with a yoke connected to a tube that passes through the instrument panel (Figure 2) and rudder pedals.
Figure 2: Cessna 172 control yoke

Source: Aircraft Owners and Pilots Association
The pilot and passenger seats were fitted with a 3-point harness. This included a lap belt and a single diagonal shoulder harness with inertia reel. The instructor reported the pilot was wearing both portions of the harness when they sent the pilot on the solo flight.
VH-CPQ was manufactured in 2000 and first registered in Australia in 2000. The aircraft had been registered with the current operator since January 2023, and at the time of the accident had accumulated 11,342.9 hours total time in service.
The aircraft was fitted with a Honeywell KAP 140 single axis digital autopilot system. This autopilot only controlled the roll axis of the aircraft via an electric servo on the aileron cables. The autopilot could not control the pitch and yaw of the aircraft, these had to be controlled by the pilot.
To engage the autopilot, the pilot must press and hold the AP button for 0.25 seconds. When engaged the autopilot will roll the wings level using the electric aileron servo. To enable heading mode, the pilot must then select HDG, this will turn the aircraft, at a rate one turn[9], using the aileron servos, to a heading selected by the pilot on the directional indicator. Further functions of the autopilot are a navigation mode, an approach mode, and a back course mode. All of these modes aid the pilot in conducting instrument approaches by providing heading assistance. Any activation of these modes will have no effect on the pitch and yaw of the aircraft. Due to the heavy disruption of the aircraft, the ATSB was unable to determine if the autopilot was active at the time of the accident.
The last periodic inspection was conducted on 15 December 2023. The most recent maintenance was performed on 23 January 2024, to investigate high engine oil temperature indications. This was rectified and the aircraft was released to service.
The aircraft was flown on lessons for other pilots on the day of the accident flight, accumulating 2.9 hours from the completion of maintenance to the commencement of the accident flight.
The ATSB performed weight and balance calculations based on the flight card,[10] pilot and aircraft weights, and estimated cargo weight. The calculations showed that the aircraft's weight and balance were within limits.
Site and wreckage
Accident site examination
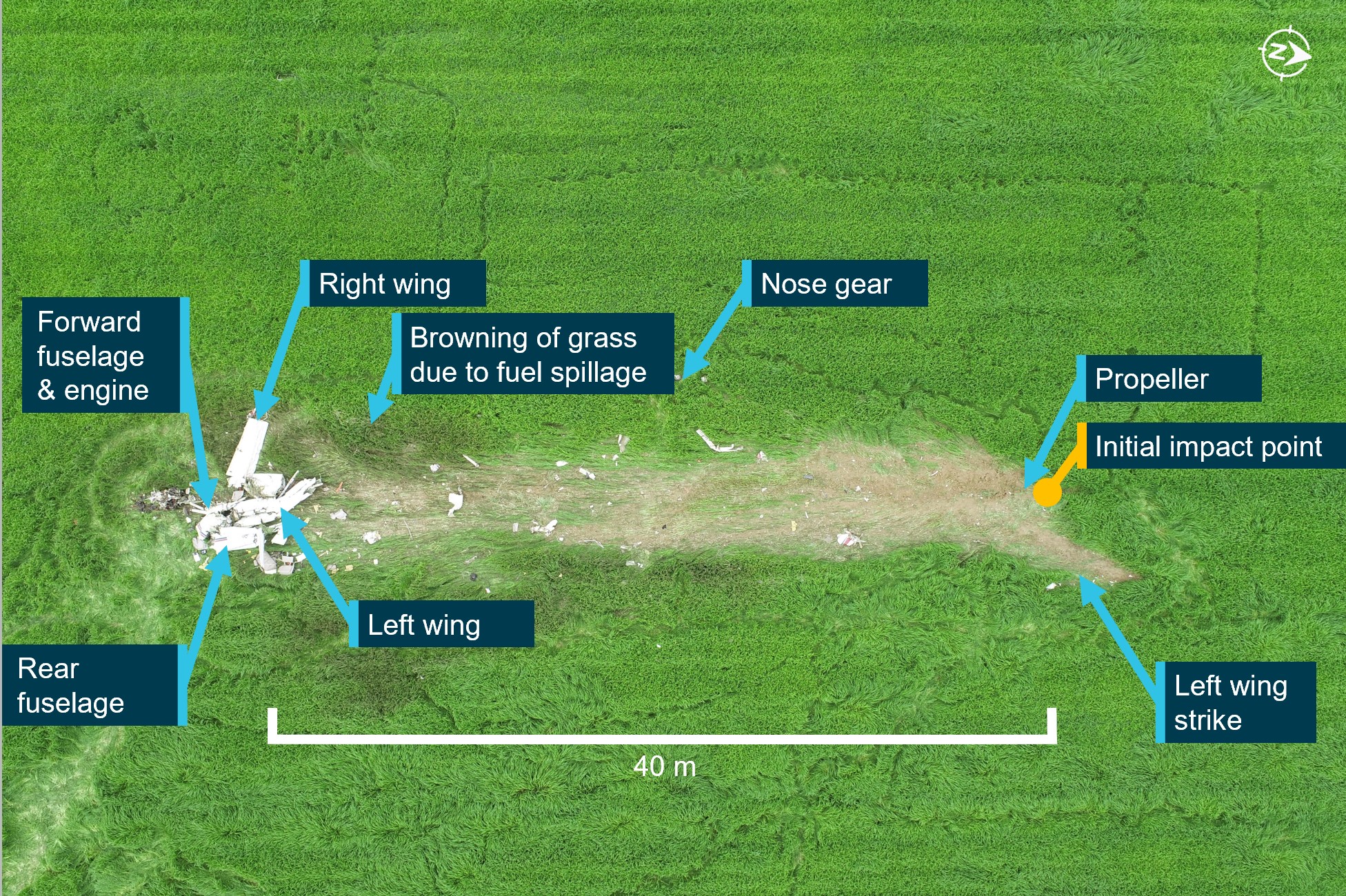
The accident site was approximately 1.6 NM west of the runway 06 threshold, in a paddock. The wreckage trail extended in a direction consistent with the flight path on the downwind leg of a circuit, about 40 m from the initial impact point to where the main wreckage, including the wings, empennage, and engine had come to rest (Figure 3). The propeller detached and was embedded in the soil at the point of initial impact. All components necessary for flight, including all major sections of the aircraft’s structure and control surfaces, were accounted for at the accident site.
Figure 3: Overview of VH-CPQ accident site

Source: ATSB
Ground impact marks and damage to the airframe indicated that the aircraft impacted the terrain in a slightly left wing-low, steep nose-down attitude at high speed. The airframe was heavily disrupted. Pre-impact flight control continuity was established and wing flaps[11] were assessed to have been extended but set at less than 10° at the time of impact. There was no evidence of an in-flight break-up or other pre-impact airframe or control defects.
On-site examination of the engine did not reveal any pre-impact mechanical issues, while damage to the propeller and marks in the soil at the impact indicated that the engine was producing power at impact. The engine control positions were unable to be confirmed due to the extensive damage.
Browning of the grass around the impact site was consistent with contact with fuel being released during the impact sequence. No fuel was obtainable from the aircraft and fuel quantity was unable to be determined at the accident site. However, records indicated the aircraft had 125 litres of fuel onboard prior to the lesson beginning, sufficient for approximately 3 hours of flight. There were no reported issues with the fuel source, which was used for other aircraft.
Aircraft component examination
The wreckage was moved to a secure location where further examination was conducted of the:
- flight control cables
- flight control yoke assembly
- elevator trim cables
- seats and rails.
The flight control cables were in good condition with no visible corrosion or broken strands. It was found that the elevator trim cables were routed correctly and there was free and easy movement of the trim tab actuator and subsequent movement of the trim tab. The trim setting could not be determined. There was no indication of a pre-impact failure of the flight control cables.
Both front seats were removed from the aircraft for further inspection. No pre‑impact damage was evident on the seat base or rails. There was significant impact damage to the forward inboard seat foot where it had slid forward and struck the stop bolt. This indicates the bolt was in place during ground impact and is consistent with the stop bolt being impacted by significant force from the seat sliding forward on rails during impact.
Recorded data
Automatic dependent surveillance–broadcast
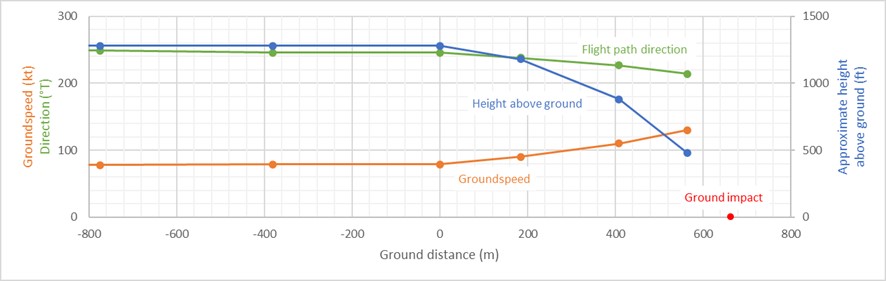
Recorded ADS-B data, which was validated by the ATSB, showed the aircraft travelling at 90nbsp;kt just prior to the descent. The data showed a steepening descent, consistent with the ground impact location, and groundspeed increasing to 130 kt before impact and a very high descent rate (about 10,500 ft/min).[12] Accounting for wind speed and descent angle, the airspeed was almost certainly above 150 kt. The descent from level flight lasted approximately 6 seconds until impact.
Figure 4: Recorded ADS-B data for the descent
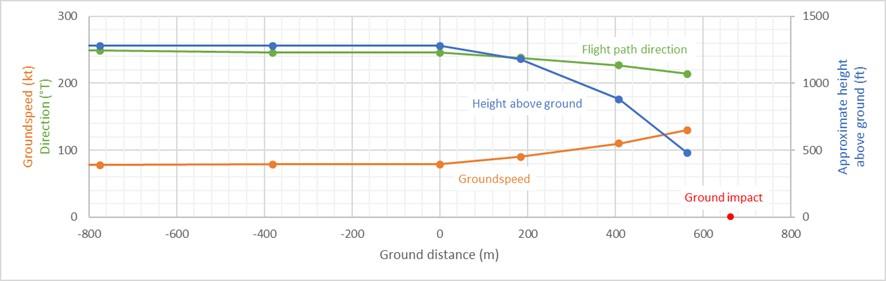
The height and distance axes are scaled 1:1. Ground distance is relative to the last recorded data point before the descent. Recorded altitude has been converted to height above the elevation at the point of ground impact. This was about 10 ft below the airport elevation.
Source: ATSB
Recordings of previous flights the pilot had conducted were also collected from ADS-B Exchange[13] (Figure 5). When comparing the occurrence flight to previous circuits, the location of the accident was in a similar location to the start of the turn onto base with the aircraft at a similar initial height and speed.
Figure 5: Previous circuit flights flown by the accident pilot

Training flights are indicated in pink. Occurrence flight is indicated in blue.
Source: Google Earth, annotated by the ATSB
Closed-circuit television
The ATSB obtained recordings from 3 CCTV cameras in the local area that had the potential to capture part of the accident flight (Figure 6). Cameras A and B were located on a building 340 m from the accident site. Both cameras recorded in 25 frames per second and captured the aircraft at various stages in its descent to impact.
Figure 6: CCTV locations

Source: Google Earth, annotated by the ATSB
Camera A faced southwest and captured the collision with terrain in a small part of the background. The footage indicated the aircraft was in a steep, nose-down descent on impact.
Figure 7: Camera A

Source: University of Sydney, annotated by the ATSB
Camera B faced west-southwest and captured the descent of the aircraft over 7 frames (at 25 frames/sec) before losing sight of the aircraft behind terrain. The aircraft was in a steep descent, with the flight path being about 60° from level, with the aircraft’s nose about 60° down and wings approximately level.
Figure 8: Camera B

Source: University of Sydney, annotated by the ATSB
Camera C was located 800 m north-east from the accident site. It did not capture the descent of VH-CPQ.
Analysis of the CCTV recordings from the 2 cameras resulted in an estimated airspeed above 150 kt and a descent impact angle of approximately 60⁰. There was no evidence of a spin or loss of control.
Air traffic control recordings
The airspace around Camden Airport is class D during towered hours when all aircraft are provided with an air traffic control service. During the accident flight the tower was active. Frequent ATC radio communications are required to conduct circuit operations. These include taxi, take-off, and landing clearances.
At the time of the occurrence there were 3 aircraft in the controlled airspace. One aircraft was turning downwind behind VH-CPQ at the time of the accident, and the pilot stated they did not see the aircraft in the circuit at the time of the accident. Another aircraft was heading away to the south-east, using runway 10.
The landing call was made with the correct phraseology and sounded like the pilot’s other broadcasts.
Flight path analysis
The recorded data of the downwind leg indicated that the pilot was maintaining a constant altitude consistent with the expected altitude of the circuit. The aircraft was tracking at 246° at 79 kt at the start of the descent. When calculating the vertical track of the aircraft, the airspeed increased significantly from the start of the descent until impact. Detailed analysis of the ADS-B, CCTV and other data indicated a descent rate of over 10,000 ft/min at impact with an airspeed 2-3 times the level flight stall speed (calculated to be about 48 kt at the time).
In response to a request for advice on what circumstances would be required to produce the observed steep, high-speed impact, the aircraft manufacturer advised:
Based on the recorded ground speed, reported winds, and aircraft track it appears the drop of the aircraft's nose was not brought about by a stall. Additionally, as no disconnected flight controls were found, indicating the aircraft was serviceable, it is unlikely the aircraft's nose would suddenly drop in an uncontrolled manner.
Once established in level flight, a pilot usually adjusts elevator trim to minimise constant control forces and leaves it set until a climb or descent is needed. The trim wheel requires 2 full turns from the middle position to the full nose-up or nose-down position. If a pilot does not adjust trim, they will need to maintain (usually) a small amount of forward or aft control force. With constant trim, configuration and power settings, an aircraft trimmed for level flight at a particular speed will tend to return to level flight at the same speed. The aircraft manufacturer advised:
…Assuming the elevator trim stays the same in a dive with the speed increasing, the pilot would have to push harder and harder on the yoke to keep it in a nose down position… more pressure would be needed to keep the same angle of dive.
The aircraft manufacturer also advised:
…If a 172S is properly trimmed and flying straight and level with the autopilot off the aircraft will most likely begin to roll before it begins to change pitch attitude. The rate of roll would depend on airspeed and power setting. However, how the aircraft moves with the pilot's hands off the controls also depends on the air currents/turbulence it is moving through along with how the aircraft is rigged.
In summary, to sustain a constant pitch attitude in an accelerating dive requires an increasing forward force on the control yoke, and a steepening dive requires additional pressure to overcome the increasing control yoke force.
Related occurrences
There have been a small number of accidents where there were no identified anomalies with the airframe, flight control systems, engine, or propeller that could be associated with a pre-impact malfunction.
Collision with terrain involving Cessna 172, VH-WLF, 10 km west of Wentworth Airport, NSW on 28 May 2012 (ATSB AO‑2012-072)
The ATSB found that shortly after departure from Wentworth Airport the aircraft collided steeply with terrain at high speed and that the accident was not survivable. There was no evidence of any in-flight failure of the airframe structure or flight control system and the engine appeared to have been producing significant power at impact.
Based on advice from the aircraft manufacturer following their consideration of on-site evidence, and in the absence of an identified problem with the aircraft, the ATSB concluded that continual pilot input was probably applied to the flight controls immediately before the impact with terrain. However, the possibility that the pilot may have applied that input as a result of incapacitation could not be discounted.
Collision with terrain involving Cessna 172P, N65698, Eagle River, Alaska, United States on 26 July 2021 (National Transportation Safety Board ANC21FA065)
The pilot and flight instructor departed on a 2-hour discovery flight and did not return. The wreckage was subsequently located nearly 9 hours after the airplane’s scheduled return time in an area of rocky, mountainous terrain. The airplane sustained substantial damage to the fuselage and left wing. No pre-accident engine or airframe mechanical malfunctions or anomalies were found that would have precluded normal operation.
The NTSB found that the aircraft collided with terrain under unknown circumstances.
Collision with terrain involving Cessna 172L, N3599F, Webster, Wisconsin, United States on 12 August 2004 (National Transportation Safety Board CHI04FA223)
The pilot was cruising at 5,500 ft when they reported a ’severe vibration’ and that they were diverting to a nearby airport. A plot of the radar data indicated that the aircraft made a course reversal to a southerly heading just prior to the accident. During the final 38 seconds of aircraft radar track data, the aircraft’s calculated ground speed increased from 130 kt to 218 kt while established on the southerly heading. The aircraft's maximum structural cruising speed was 121 kt and the never exceed speed was 151 kt. All primary airframe structural components, flight control surfaces, engine components, and propeller blades were located within the debris field. No anomalies were noted with the airframe, flight control systems, engine, or propeller that could be associated with a pre-impact malfunction.
The NTSB found the airplane was destroyed during a high velocity impact with terrain.
Safety analysis
Introduction
Evidence from the accident site, aircraft wreckage, and flight path data identified that the aircraft collided steeply with terrain at high speed and that the accident was not survivable.
The weather was clear with low winds. There were no pre-accident defects identified on the airframe or engine and no evidence of a bird or drone strike.
Departure from level flight
The data shows that the aircraft was towards the end of the downwind leg and had not yet commenced the base turn when it departed from level flight, the slight flightpath deviation to the left did not necessarily indicate that a turn had been commenced or established at that time.
The aircraft’s weight and balance were within limits. The stall speed was estimated to be about 48 kt, and the airspeed was estimated to be 78 kt at the point where the descent began. This airspeed is inconsistent with a low-speed stall.
The departure from level flight occurred in a location consistent with an expected trim adjustment by the pilot for the approach, however, there would be no operational reason for a pilot to make large trim adjustments in level flight, and an excessive trim adjustment or one in the wrong direction would likely be quickly detected and reversed.
The aircraft was not fitted with an electric elevator trim system. The Honeywell KAP 140 single axis digital autopilot system only gave the pilot the option of holding a heading and had no control over the elevators, elevator trim, or rudder. Should the autopilot have been inadvertently activated, the aircraft would have rolled wings level with no direct effect on its pitch. If the autopilot was selected in any further modes, dependent on the heading selection on the directional indicator, the aircraft would have commenced a rate one turn towards that heading. There was no indication of a turn prior to the descent of the aircraft.
Furthermore, the small flightpath deviation during the descent, along with the increasing groundspeed, increasing airspeed, the high rate of descent and impact speed was inconsistent with that of an incipient or established spin.
It is possible for the aircraft to stall above the stall speed with a rapid pitch-up movement or a banked turn; this is called an accelerated stall. However, it would not be possible for the aircraft to conduct such a manoeuvre without a significant change in altitude or direction that would have been visible in the recorded data.
It is likely, therefore, that in the absence of an identified problem with the aircraft, and in combination with the aircraft manufacturer’s assessment, that continual nose-down control input was almost certainly applied to the flight controls throughout the descent. The increasing airspeed throughout the descent would have meant that the forward pressure would have to be sustained throughout the descent and the control force required to maintain or increase the pitch-down attitude would have also increased.
Potential reasons for the sustained forward pressure on the control yoke were considered and are discussed in the following sections.
Seat slide
An inadvertent forward seat slide could result in the pilot’s torso or hands pushing forward on the control yoke, resulting in a nose-down control input.
However, significant disruption to the bottom of the occupied front seat and impact damage on the remaining stop bolt indicate that the seat slid forward on the rail and impacted the stop bolt during the accident sequence. This indicated that the seat was not in its forwardmost position at impact. Further, there was no longitudinal deceleration immediately prior to the descent that would be required to create a force for the seat to slide forwards. A forwards control input would also have had to be maintained for much of the descent, or the aircraft would have lifted the nose and reduced the descent rate or begun to climb.
A rearwards seat slide was considered less likely, as there was no longitudinal acceleration, and would result in a neutral or nose-up control input (not down), such as if the pilot attempted to prevent the slide by pulling on the control yoke.
Control jam
A control jam in the aircraft would have limited the pilot’s ability to manoeuvre the aircraft. If a primary flight control surface, such as the ailerons, elevator, or rudder, becomes jammed or partially restricted, the pilot may have difficulty controlling the aircraft's attitude and direction. Depending on the severity and type of jam, the pilot may need to rely on secondary or alternative control methods, such as trim adjustments or differential power, to maintain control and safely land the aircraft.
Most forms of flight control failure would not result in a rapid, steep, smooth descent. The only exceptions would be elevator trim which would fail in the most recent position, or the elevator getting stuck or broken.
If the elevator or controls had become stuck in a significant nose-down position, there would have to be a movement to put it in that position first. There was no reason for it to be in a strong nose‑down position as the aircraft was not in a phase of flight where the pilot would require that position (the possibility of an attempted evasive manoeuvre is discussed in Pilot action). If the elevator was broken the aircraft would trim to roughly level flight.
There was no indication that any of the flight controls or cabling were misrouted, had corrosion, any pre‑impact failure, nor any limitations to normal movement.
Medical event
The pilot had no recorded or reported pre-existing medical conditions, and the available evidence suggests that the pilot was in good health on the day of the accident. Although the pilot had experienced 2 medical events in the past, these were associated with physical exertion after omitting meals. The pilot had likely changed habits after this and had eaten breakfast on the day of the accident. In any case, the pilot had previously cancelled a lesson when not feeling well.
The flight path leading up to the descent was normal, and the pilot’s radio calls, the last being 1 minute and 26 seconds before the descent, were also normal.
Although extremely rare, a sudden unexplained medical event can never be completely excluded. However, given the relative positions between the pilot and control yoke, the horizontal movement of the control yoke required to initiate and maintain a nose-down control input (as shown in Figure 2), and the pilot’s use of the shoulder harness, the ATSB considered it very unlikely that a significant forward pressure on the control yoke would result from such an event. Rather, an incapacitation would more likely result in a significant roll input which did not occur. A pilot who ‘froze’ at the controls would not be likely to maintain a significant forward yoke pressure.
Pilot action
Analysis of the recorded ADS-B data showed that, other than the descent itself, there was no abnormal, rapid deviation from the flight path that might be expected if the pilot was attempting to avoid a hazard. Had this been the reason for the descent, it is unlikely that the pilot would have maintained a constant nose-down input. No other operational reason for the steep, accelerating descent could be identified, and there were no reports of previous risk-taking behaviour or significant personal, psychological, or social concerns.
Conclusions
Based on the available evidence, no mechanical, operational, or medical factors contributing to the accident could be determined. On this basis, the descent and absence of recovery were likely the result of a sustained forward control yoke movement, for reasons that could not be determined.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision with terrain involving Cessna 172S, VH-CPQ, 1.9 NM west of Camden Airport, New South Wales on 24 January 2024.
Contributing factors
- At about the time the pilot would have been expected to turn onto the base leg of the circuit, the aircraft commenced an increasingly steep, accelerating descent, almost certainly due to a sustained forward control yoke movement, until it impacted terrain.
Other findings
- No pre-existing aircraft defects could be identified.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- AltoCap Flight School
- Civil Aviation Safety Authority
- NSW Police
- Recreational Aviation Australia
- GB Aviation
- Medicare
- CCTV footage of the accident flight.
References
US Department of Transportation Federal Aviation Administration (2023). Pilot’s handbook of aeronautical knowledge. FAA-H-8083-25C. Oklahoma City, OK, USA.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- both instructors of the pilot
- AltoCap Flight School
- Civil Aviation Safety Authority
- NSW Coroner
- Textron Aviation.
Submissions were received from:
- Textron Aviation.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Flapless approach: Landing approach without deploying flaps to simulate a flap failure.
Glide approach: The controlled descent toward a landing area without engine power to simulate engine failure on landing.
Missed approach: A manoeuvre that involves an aircraft discontinuing its approach to the runway when landing.
[2] Solo: when a student pilot flies an aircraft alone for the first time without an instructor on board. Consists of a single take-off, circuit and a full stop landing.
[3] Automatic terminal information service: An automated service that provides current aerodrome information to departing and arriving aircraft.
[4] Conditions were clear, and the meteorological aerodrome report stated the wind was from the NNW at 4 kt.
[5] In ALT (altitude) or ON mode, a transponder responds to secondary surveillance radar interrogations and broadcasts ADS-B signals. In OFF and STBY (standby) modes no signals are transmitted.
[6] The circuit height at Camden Airport is 1,300 ft AMSL. Camden Airport has an elevation of 230 ft.
[7] An authorisation for individuals to fly RAAus registered recreational aircraft in Australia under specific regulations set by Recreational Aviation Australia.
[8] A sport aviation aircraft with 2 seats, smaller than a Cessna 172.
[9] Rate One Turn: rate one or standard rate turn is accomplished at 3°/second resulting in a course reversal in one minute or a 360° turn in two minutes.
[10] A log carried onboard the aircraft to capture fuel totals, hour meter and air switch readings.
[11] A movable surface on the trailing edge of a wing that, when extended, increases both lift and drag and reduces the stall speed. Flaps are extended to improve take-off and landing performance. At this point in the circuit a pilot would be expected to be extending the flaps to 10° while setting up the aircraft for landing.
[12] In highly dynamic situations, the internal processing of data can result in erroneous outputs. Therefore, this data should be treated as indicative only.
[13] ADS-B Exchange is an online repository of recorded ADS-B data: https://www.adsbexchange.com/