
Executive summary
What happened
On 19 November 2023, 2 SIAI Marchetti S-211s, operated by Jetworks Aviation and registered VH-DQJ (Viper 1) and VH-DZJ (Viper 2), departed Essendon Airport, Victoria on a formation flight to undertake in-flight filming of both aircraft over Port Phillip Bay, Victoria.
During the flight, Viper 2 was manoeuvred to pass beneath an inverted Viper 1. As Viper 2 approached Viper 1, the vertical separation between the 2 aircraft reduced. Viper 2 then passed beneath and began to pitch up and bank left, away from Viper 1, with the right wings of each aircraft colliding.
After the collision, and with the right wing significantly damaged, Viper 2 continued to climb and began rolling right, passing above and behind Viper 1. Viper 2 rolled to an inverted attitude and quickly assumed a near‑vertical, nose-down flight path and impacted the water at high speed. Both occupants were fatally injured. Viper 1 was not significantly damaged and returned to Essendon.
What the ATSB found
The ATSB found that prior to the accident manoeuvre, Viper 2 was manoeuvred to pass directly beneath Viper 1 for a filming opportunity. This specific manoeuvre had not been briefed before the flight and increased the risk of collision. A subsequent in-flight discussion of the manoeuvre did not allow for full consideration of associated risks before a second attempt was commenced. During the second attempt of the manoeuvre, the right wings of each aircraft collided. The damage sustained by Viper 2 resulted in an immediate loss of control, and soon after, the aircraft’s collision with water.
The ATSB also found that the pilot of Viper 1 had a medical restriction which required them to only operate an aircraft with a side-by-side cockpit configuration and a qualified safety pilot to be present. These requirements were not being followed during the accident flight.
Furthermore, the operator did not hold the required operating certificate to undertake the filming flight and the aircraft were not permitted to be used for that purpose. This resulted in a lower level of safety assurance for the flights.
Safety message
The conduct of in-flight filming work introduces several risks to a flight including a potential increase in pilot workload and distraction. Additionally, efforts to maximise filming opportunities may conflict with the safe operation of the aircraft, in particular for aircraft operating in formation, which can further increase risk. Minimising the risk of these flights requires that the pilots prioritise operational safety, in particular through in-depth briefings, pre-flight planning of manoeuvres, and strict adherence to procedures and the agreed plan.
In addition, this investigation highlights the importance of adhering to operational restrictions to minimise risk. The pilot of Viper 1 had a medical restriction preventing them from operating the aircraft and regulatory restrictions were in place preventing the aircraft from being used for the filming. These limitations mitigated the known risks of the pilot's medical condition and the civil operation of ex-military aircraft. Operating outside of these limitations removed the in-built safety defences and organisational structures designed to identify and mitigate these risks.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On 19 November 2023, the crews of 2 SIAI Marchetti S-211s, operated by Jetworks Aviation and registered VH-DQJ and VH-DZJ, prepared to conduct a formation flight from Essendon Airport, Victoria. The flight operated using the callsign ‘Viper Formation’ and intended to undertake in-flight filming of both aircraft over Port Phillip Bay. VH-DQJ was the formation leader, operating as ‘Viper 1’, with a pilot and safety pilot (see the section titled Pilot details) on board. VH-DZJ was operating as ‘Viper 2’ with a pilot and camera operator on board.
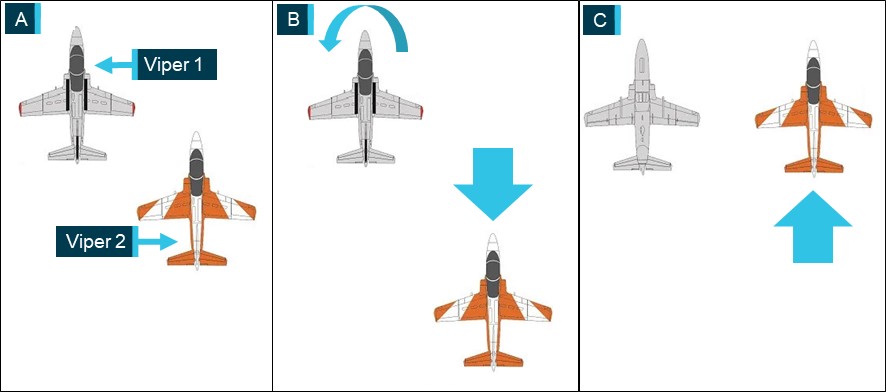
Prior to commencing the flight, the crews conducted a brief of the planned manoeuvres. The first of the manoeuvres involved Viper 1 flying inverted, straight and level, while Viper 2, flying upright, moved to the right line abreast position for filming (panel C in Figure 1). From that position, Viper 2 would move as required for the filming while maintaining separation from Viper 1. The crews planned to conduct this manoeuvre with Viper 2 starting in the right echelon position (panel A in Figure 1) before moving rearward to allow Viper 1 sufficient room to roll inverted (panel B in Figure 1). After Viper 1 rolled inverted, Viper 2 was to move forward and climb or descend as needed to reach the line abreast position at the same altitude, for filming (panel C in Figure 1). During the manoeuvring, the pilots would communicate on a discrete radio frequency.
Figure 1: Planned manoeuvre sequence
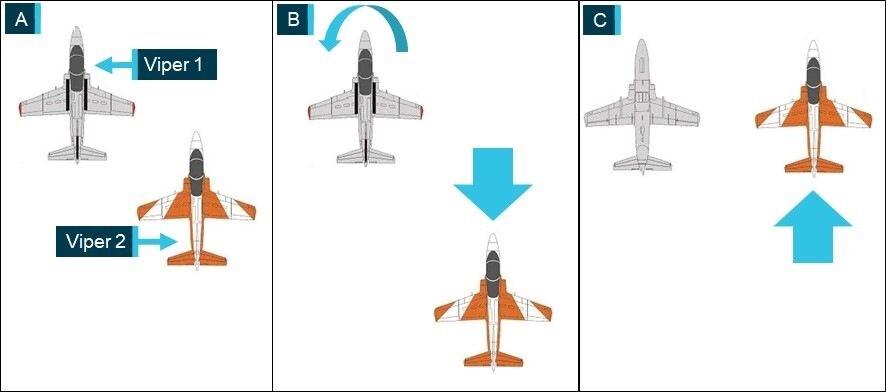
Source: Kovozavody Prostejov, modified and annotated by the ATSB
The crews completed the brief and, at 1324 local time, the aircraft departed Essendon towards Port Phillip Bay. About 6 minutes later, while the aircraft were operating at about 3,000 ft above mean sea level and at a speed of about 200 kt, the crews began manoeuvring for the planned sequence. Viper 2 moved rearward (panel A in Figure 2) and Viper 1 rolled inverted (panel B in Figure 2). From a low right echelon position, Viper 2 then moved forward and climbed toward the line abreast position while also moving laterally closer to Viper 1 (panel C in Figure 2). The rate of closure between the aircraft increased and before Viper 2 could stabilise in the line abreast position, the pilot banked away and moved out of the formation (panel D in Figure 2). Viper 1 then rolled upright.
Figure 2: Recorded images from Viper 1 of first manoeuvre
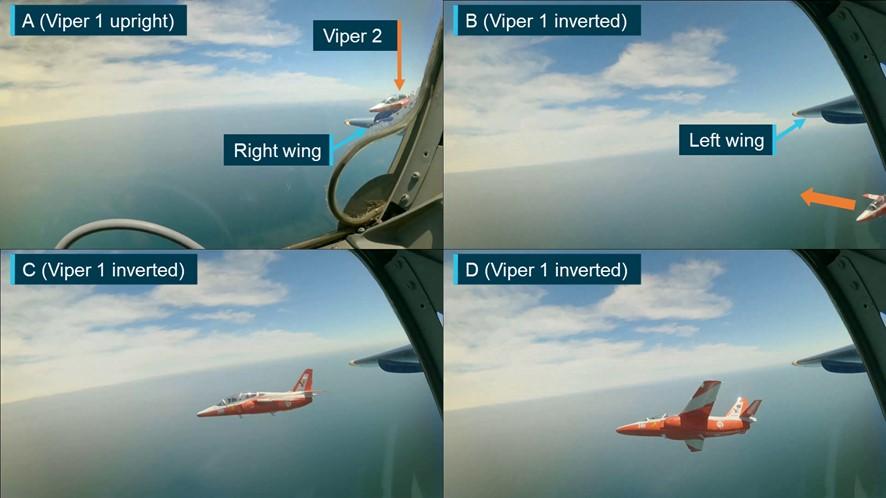
Note: For ease of interpretation some images have been inverted to present all footage in an upright orientation.
Source: Recorded video from Viper 1, modified and annotated by the ATSB
Viper 2 rejoined the formation in the right echelon position (panel A in Figure 3) and shortly after, Viper 1 rolled inverted for a second attempt (panel B in Figure 3). On this occasion, instead of moving toward the line abreast and level position as planned, the pilot of Viper 2 manoeuvred to pass below (panel C in Figure 3) and across to the left of Viper 1 (panel D in Figure 3).
Figure 3: Recorded images from Viper 1 of second manoeuvre
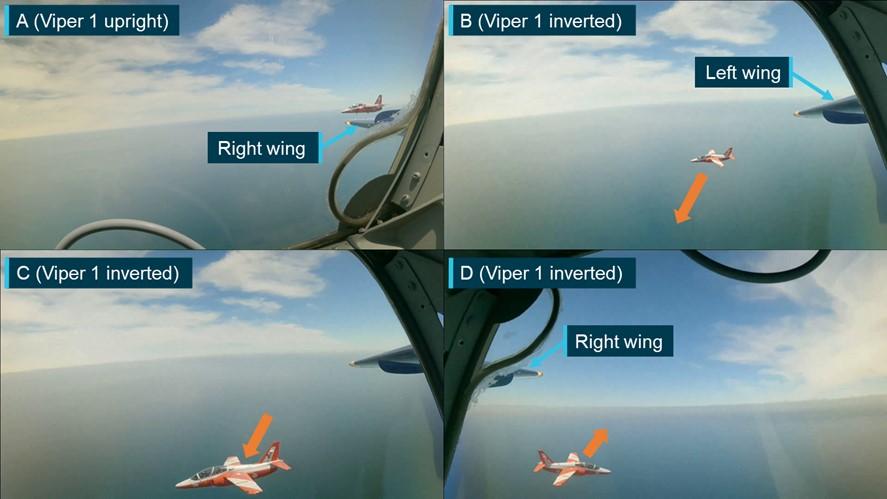
Note: For ease of interpretation some images have been inverted to present all footage in an upright orientation.
Source: Recorded video from Viper 1, modified and annotated by the ATSB
The safety pilot in Viper 1 observed Viper 2 pass beneath and alerted the pilot of Viper 1 to the manoeuvre. The pilot of Viper 1 then rolled upright and contacted the pilot of Viper 2 to discuss the manoeuvre. The pilot of Viper 2 advised that passing underneath Viper 1 provided a good filming opportunity and requested to repeat the manoeuvre. After discussing the manoeuvre, the pilots decided to attempt it again, and Viper 2 moved to the right echelon position to recommence the manoeuvre.
As with the previous attempt, Viper 2 moved rearward to allow Viper 1 to roll inverted. Before Viper 1 stabilised in the inverted attitude (panel A in Figure 4), Viper 2 began manoeuvring to pass beneath Viper 1 (panel B in Figure 4) and the safety pilot noted that Viper 2 moved in and underneath ‘quite quickly’. Viper 1 then stabilised in the inverted attitude and as Viper 2 approached, the vertical separation between the 2 aircraft reduced. Viper 2 passed beneath and began to pitch up and bank left, away from Viper 1 (panel C in Figure 4). At 1333, as Viper 2 climbed and banked left, the right wings of each aircraft collided (panel D in Figure 4).
Figure 4: Recorded images from Viper 1 of third manoeuvre and collision
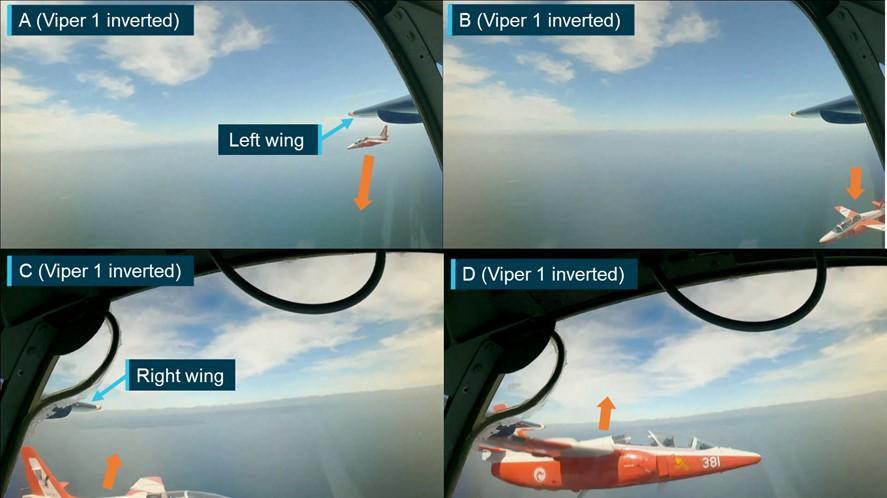
Note: For ease of interpretation the images have been inverted to present all footage in an upright orientation. The occupants of Viper 2 have been obscured in panel D.
Source: Recorded video from Viper 1, modified and annotated by the ATSB
After the collision, and with the right wing severely damaged (Figure 5), Viper 2 continued to climb and began rolling right, passing above and behind Viper 1. Viper 2 rolled to an inverted attitude and quickly assumed a near‑vertical, nose-down flight path toward the water and commenced a slow right roll until impacting the water at high speed. Both occupants were fatally injured.
Figure 5: Recorded image from Viper 1 showing the collision damage to Viper 2

Note: For ease of interpretation the image has been inverted to present an upright orientation.
Source: Recorded video from Viper 1, annotated by the ATSB
The pilot of Viper 1 felt the collision but did not observe it while the safety pilot observed Viper 2 pass underneath, climb and collide with Viper 1. The collision deflected Viper 1 right 35° from the level inverted attitude to an angle of left bank of about 145° from upright and slightly nose down. The pilot rolled the aircraft fully upright, checked the control response and assessed that the aircraft was controllable. The pilot then attempted to contact the pilot of Viper 2, but no response was received.
The pilot of Viper 1 turned the aircraft back towards the location of the collision where the safety pilot observed a splash mark and debris from Viper 2 on the water’s surface. The pilot of Viper 1 contacted air traffic control (ATC) to advise of the mid-air collision and broadcast a ‘MAYDAY’.[1] Viper 1 then orbited the location of the splash mark to assist ATC in marking the location for search and rescue purposes (Figure 6).
Figure 6: Recorded flight path of Viper 1
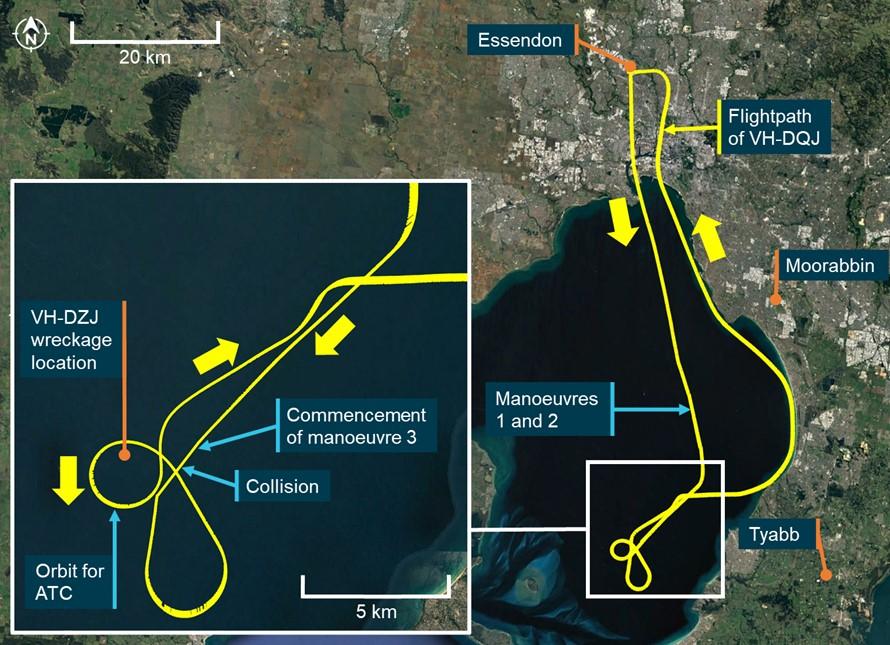
Note: As is normal procedure for formation flights, only the formation leader (Viper 1) had the transponder active. Surveillance data was only recorded for that aircraft.
Source: Airservices Australia, Google Earth and ATSB
The pilot of Viper 1 then turned north‑east and conducted further controllability checks of the aircraft in both the cruise and landing configurations.
The pilot considered diverting to the planned alternate airport of Moorabbin but assessed the aircraft to be fully controllable and not significantly damaged and elected to return along a coastal route to Essendon Airport (see the section titled Return to Essendon), landing at 1349.
Context
Aircraft details
The SIAI Marchetti S-211 (Figure 7) is a mid-wing aircraft designed for military flying training, with full dual controls and 2 tandem configured ejection seats fitted with 5-point restraint harnesses. The ejection seats were deactivated in VH-DQJ (Viper 1) and VH-DZJ (Viper 2). The aircraft were each powered by a Pratt and Whitney Canada JT15D-4C turbofan engine mounted in the rear fuselage. Fuel system limitations restricted inverted manoeuvres to periods not exceeding 30 seconds.
Figure 7: VH-DQJ (left) and VH-DZJ (right)

Source: ATSB and Phil Vabre
VH-DQJ and VH-DZJ were built in Italy in 1985 and delivered to the Republic of Singapore Air Force (RSAF), where they operated in the military flight training role. From 1996, until 2009, the aircraft were based at Royal Australian Air Force Base Pearce, Western Australia, after which the S-211 fleet was retired from RSAF service. Following retirement from military service, several RSAF S-211s, including VH‑DQJ and VH-DZJ, were sold in Australia to civilian owners.
Under the Civil Aviation Safety Regulations (CASRs), pilots operating the S-211 were required to complete flight training and undertake flight reviews for the aircraft type.[2] Pilots were also required to hold a single engine aeroplane class rating and applicable design feature endorsements.
At the time of the accident, VH-DQJ had accumulated about 6,363 hours in service and had a maintenance release valid until 10 November 2024, or 6,458 hours in service. The aircraft was certified for day visual flight rules flight only. VH-DZJ had about 5,595 hours in service and had a maintenance release valid until 28 July 2024 or 5,678 hours in service. The aircraft was certified for instrument flight rules operations.
Limited category operations
Ex-military aircraft or ‘Warbirds’, can be operated in Australia under a Limited category Certificate of Airworthiness (CoA) and in accordance with CASR Part 132. These operations were administered by the Australian Warbirds Association Limited. The Limited airworthiness category differs from the Standard category or other categories and includes restrictions on where and how these aircraft can be flown.
In 2011, VH-DQJ and VH-DZJ were entered onto the Australian Civil Aircraft Register and issued with special CoAs in the Limited category. The special CoA was subject to several conditions, including limitations on the permitted uses of the aircraft. For both aircraft, the permitted uses were:
- adventure style operations
- exhibition
- aerobatics
- mock combat.
The Civil Aviation Safety Authority (CASA) advised that the flights constituted an aerial work operation (see the section titled Operator details). Limited category aircraft were not permitted to be used for aerial work operations.
The carriage of passengers in these aircraft was permitted provided the person operating the aircraft ensured that each passenger was made aware that:
- the design, manufacture, and airworthiness of the aircraft were not required to meet any standard recognised by CASA
- the aircraft was not required by CASA to be operated to the level of safety normally associated with a commercial passenger flight
- that persons fly in the aircraft at their own risk.
Where paying passengers were carried for experience flights in ex-military aircraft (subject to a Limited category CoA), the passenger was required to read and acknowledge the following warning prior to payment for the flight being made:
Warning
When you fly in this aircraft, you do so at your own risk.
Any safety equipment provided by the operator of this aircraft must be worn at all times. The operator will provide you with information regarding its purpose and directions for its use.
The design, manufacture and airworthiness of the aircraft are not required to meet any safety standard recognised by CASA.
The aircraft is not required by CASA to be operated to the same safety standards as an aircraft used for regular public transport or charter operations.
Similar information was also included on a placard on the rear (passenger’s) instrument panel (Figure 8).
Figure 8: Rear instrument panel placard in Viper 1

Source: ATSB
Pilot details
The ATSB found no indicators that any of the flight crewmembers were experiencing a level of fatigue known to affect performance.
The crew of both aircraft were not wearing parachutes[3] or life jackets.
Viper 1 (VH-DQJ) pilot
The pilot of Viper 1 held an Air Transport Pilot Licence (Aeroplane) along with the required ratings, endorsements, and type training to operate the S-211 as pilot in command. In addition, the pilot held flight activity ratings and instructor training approvals for formation flying, formation aerobatics, low-level aerobatics (minimum height of 500 ft above ground level) and spinning. The pilot also held several type ratings in transport category turbine engine aircraft.
The pilot had recorded over 20,700 hours of flying time before the accident flight of which 10.8 hours were in the S-211. The pilot’s flying experience included military service operating aircraft of similar performance and handling to the S-211 and formation aerobatics displays. The pilot also had significant experience in civil formation aerobatic displays.
The pilot held a Class 2 aviation medical certificate valid until 21 August 2024 with a restriction that required them to fly with a safety pilot.
Safety pilot medical restriction
The safety pilot restriction was applied to the pilot’s medical certificate as the pilot was assessed to be at an elevated risk of distraction or incapacitation (subtle, partial, or full) resulting from a medical episode. This restriction provided a risk mitigation, where a suitable safety pilot could quickly take over control of the aircraft, in the event medical symptoms occurred in flight.
The restriction required that any aircraft flown by the pilot be configured with side-by-side seating in the cockpit and have a full set of dual flying controls. This requirement facilitated better communication between the pilot and safety pilot and allowed the safety pilot to directly observe the pilot to identify incapacitation symptoms. It also allowed the safety pilot to physically move the pilot should an incapacitation result in interference with the aircraft controls.
The restriction also required that the safety pilot:
- be endorsed and current on the aircraft type being flown
- be appropriately rated for the in-flight conditions
- have a medical certificate not restricted to multi-crew flight operations
- be aware of the type of incapacity the pilot may suffer in flight
- be prepared to take over the aircraft controls during critical phases of flight
- be competent and capable of concluding the flight safely from the control seat.
The pilot was also required to ensure that the safety pilot had read the requirements associated with the restriction.
The pilot of Viper 1 was aware of the medical restriction but had not read all the documentation detailing the specific requirements associated with the medical certificate restriction. Although they were not aware of the specific requirements for selecting a safety pilot, the pilot applied an informal assessment that satisfied them that the selected safety pilot was suitable to act in the role.
Viper 1 (VH-DQJ) safety pilot
The safety pilot in Viper 1 held an Air Transport Pilot Licence (Aeroplane) along with the required ratings and endorsements to operate the S-211. The safety pilot had commenced but had not yet completed the required training in the aircraft type to be qualified to operate the aircraft as pilot‑in‑command.
The safety pilot also held flight activity endorsements for formation flying, formation aerobatics, and spinning, as well as type ratings in several transport category turbine engine aircraft.
The safety pilot had recorded a total of 12,276 hours before the accident flight, including a previous training flight of 1 hour in the S-211. The safety pilot’s experience also included military service operating aircraft of similar performance and handling to the S-211 and formation aerobatic displays.
The safety pilot held a Class 1 aviation medical certificate valid until 22 February 2024 and was not restricted to multi-crew flight operations.
The safety pilot was aware of the pilot’s medical restriction and requirement for a safety pilot but was not aware of the specific requirements associated with the restriction, including the requirement to be endorsed and current on the aircraft type. To fulfil their role, the safety pilot carried S-211 checklists and operational documentation sufficient for the flight. With the exception of completing training in the aircraft type, the safety pilot held all other required qualifications for the aircraft and flight activities planned for the flight and felt well prepared to fulfil the role and take control should the pilot become incapacitated.
Viper 2 (VH-DZJ) pilot
The pilot of Viper 2 held a Commercial Pilot Licence (Aeroplane) along with the required ratings, endorsements, and type training to operate the S-211 as pilot in command. In addition, the pilot held formation flying, formation aerobatics, low-level aerobatics (minimum height of 500 ft above ground level) and spinning flight activity endorsements.
The pilot had recorded a total of 1,542 hours before the accident flight, including 489 hours on the S-211 aircraft type.
The pilot held a Class 1 aviation medical certificate valid until 28 February 2024.
Operator details
The aircraft were operated by Jetworks Aviation and the purpose of the accident flight was to produce footage to promote a proposed television program using the aircraft. The television program was envisaged by the pilot of Viper 2, who owned Jetworks Aviation and both S-211s as well as a Pacific Aerospace CT/4E that was also to be used for the program. The pilot of Viper 2 had also coordinated the filming activity with the production company.
CASA advised that the filming of a formation flight, with a dedicated camera operator for the purposes of producing footage for a television program involving those aircraft, constituted a task specialist operation.[4] This operation type was defined as an aerial work operation by CASR 138.010. To undertake such an operation, the operator required an aerial work certificate in accordance with CASR 138.030.
The operator did not hold an aerial work certificate and Limited category aircraft were not permitted to be used for aerial work operations.
Approved aerial work operations required several organisational risk mitigations not found in Limited category operations under CASR Part 132, including:
- aerial work aircraft were required to hold a Standard CoA, meeting airworthiness standards for at least one of the following categories:
- Transport, Commuter, Normal, Restricted and Utility
- aerial work passengers could only be carried in Transport, Commuter and normal category aircraft
- a requirement for identified key personnel with defined experience requirements and responsibilities
- an approved operations manual for all proposed operations, including risk assessment requirements and for non-propeller turbine aircraft, a safety management system[5]
- prescribed training and checking requirements.
Following the accident, the operator ceased operations.
Recorded data
Neither aircraft was fitted with a flight data recorder or cockpit voice recorder, nor were they required for the type of aircraft and operation.
The camera operator in Viper 2 carried a hand-held camera for filming and several video cameras were also mounted within the cockpit of both aircraft. None of these were able to be located during recovery operations or in the recovered wreckage.
There were 4 cameras fitted to Viper 1, of which 3 recorded video and audio during the flight (Figure 9), including the collision. The cameras were mounted on each side of the front seat headrest, looking left and right, on the glareshield looking forward and one mounted on the instrument panel facing the control column. The camera facing the control column stopped recording before departure while the cameras facing forward and left stopped filming during the return flight to Essendon. The right facing camera stopped filming after the flight as the crew exited the aircraft.
Figure 9: The recorded views of the cameras fitted to Viper 1

Source: Recorded video from Viper 1, annotated by the ATSB
The elapsed time between Viper 2 passing directly beneath Viper 1 and the collision occurring was about 2 seconds. The recorded footage showed that during this time, and just prior to the collision, the pilot of Viper 2 was looking up toward Viper 1.
Airflow and engine noise dominated the audio recorded by the cameras. ATSB analysis of the recorded audio, including using voice enhancement programs, was unable to recover intelligible voices from the audio data.
Recorded surveillance and communications audio data was provided by Airservices Australia. The discrete radio frequency used by the crews during the manoeuvres was not recorded.
Formation flying
Formation flying is when more than one aircraft, by prior arrangement between the pilots, operate in close proximity and as a single aircraft with regard to navigation, position reporting and air traffic control management. In Australia, to undertake formation flying, a pilot must have completed formation flying training and hold a formation flying flight activity endorsement.
The Formation and Standards Team Australia (FASTA)[6] Formation Fundamentals manual provided guidance on formation flying. That manual stated:
Within the formation, each pilot has a defined position and responsibilities. In a formation of 2 aircraft, these positions are defined as the lead and wingman. The lead pilot’s responsibilities include:
- briefing the flight
- safely conducting the flight
- manoeuvring smoothly and predictably.
The wingman’s responsibilities include:
- maintaining formation integrity
- always keeping the lead aircraft in sight
- maintaining separation from the lead aircraft.
When moving between formation positions, a wingman should always use small flight path changes to ensure that the closure rate between the aircraft remains manageable. When changing formation position, the wingman should also be focused on looking toward the intended direction of flight while maintaining awareness of the lead’s position and not focus on looking toward the lead aircraft. Looking toward the lead aircraft may result in the wingman inadvertently applying control inputs in the direction they are looking (‘hands following head’) and inadvertently manoeuvring their aircraft toward the lead aircraft.
Briefings
Pre-briefing of in-flight manoeuvres is critical to safe formation flying. Conducting this briefing on the ground prior to flight provides opportunity for all crewmembers to focus on the briefing, make a full assessment of considerations and risks associated with the planned manoeuvres, and ensure that everyone has similar understanding of the intended manoeuvres.
Pre-briefing of a manoeuvre can also be conducted in-flight. When compared to a face‑to‑face pre-flight briefing, an in-flight briefing, using radio and while also flying the aircraft, limits a pilot’s ability to articulate and understand intended manoeuvres and fully consider associated risks. In‑flight briefings can also reduce the lead’s ability to assess that there is mutual understanding before approving a manoeuvre.
The accident flight was the second filming flight of the day involving the 2 aircraft and pilots. A pre‑flight briefing had been completed prior to the first flight, but during that flight, the camera equipment stopped working before all planned manoeuvres were completed. Therefore, after landing, a second flight was planned, and another full pre-flight briefing conducted, addressing the manoeuvres that were not completed during the first flight.
During this additional pre-flight briefing, the crews briefed several manoeuvres, the first of which involved Viper 2 moving into a line abreast position to the right of an inverted Viper 1 for filming. The pilots of the 2 aircraft agreed that while Viper 1 was inverted, Viper 2 had freedom to manoeuvre as desired for filming with a restriction to remain behind the 9 o’clock to 3 o’clock line (an imaginary line running laterally through the wingtips of Viper 1).
During the second filming flight, Viper 2 passed beneath and to the left of Viper 1 without first advising the crew of Viper 1. Subsequently, the pilots of each aircraft conducted an in‑flight briefing of the manoeuvre and decided to attempt it again. The pilot of Viper 1 understood that the second attempt at the manoeuvre would be flown like an aborted formation rejoin (overshoot), but with Viper 2 passing directly beneath.
In this scenario, when an approaching wingman assesses that their manoeuvring to rejoin the formation is unstable or unsafe and wishes to abort the rejoin, an overshoot is conducted. In an overshoot from the right echelon position, the wingman’s aircraft is manoeuvred below and behind the lead aircraft, passing across to the other side of the formation before positioning to attempt another rejoin. To minimise the risk of collision during this manoeuvre, the wingman must ensure that no part of their aircraft passes directly beneath the lead aircraft.
Meteorology
The flights and filming manoeuvres were conducted in clear and smooth flying conditions.
At 1330, 3 minutes before the collision, the Bureau of Meteorology (BoM) weather station at South Channel Island, 12 km south‑west of the collision location, recorded the surface wind as southerly at 11 kt.
At the same time, the BoM weather station at Avalon Airport recorded the surface wind as easterly at 9 kt, no cloud and the visibility as greater than 10 km.
Collision damage and wreckage examination
At the time of the collision, Viper 2 was pitched slightly nose up, in a left bank, rolling left and had slightly higher speed than Viper 1. The first contact during the collision occurred when the forward right wingtip of Viper 2 impacted the right wing of Viper 1. The impact to the wing of Viper 1 was distributed across both the front and rear spars and 2 main outboard wing ribs.The impact to the wing of Viper 2 occurred in the relatively weaker area of the front spar and 2 of the outermost wing ribs (Figure 10).
Figure 10: Cutaway drawing of the S-211 right wing structures in the primary impact areas
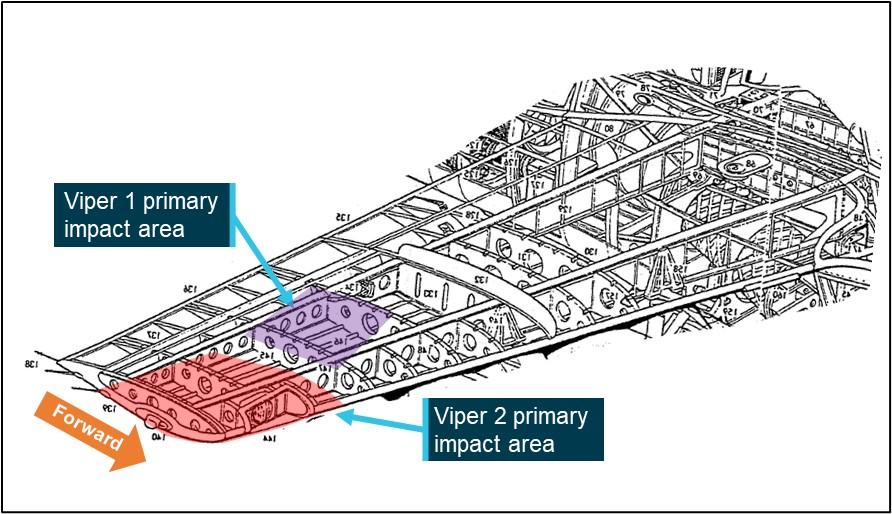
Source: Leonardo S.p.A., modified and annotated by the ATSB
Viper 1 (VH-DQJ)
Following the accident, Viper 1 was examined by the ATSB at Essendon Airport. Impact marks, including marks consistent with the wingtip fairing screws and wingtip light housing from Viper 2, along with paint transfers, were visible on the upper surface of the right wing. The upper wing skin was deformed, and the landing light cover broken (Figure 11).
Figure 11: Viper 1 collision damage
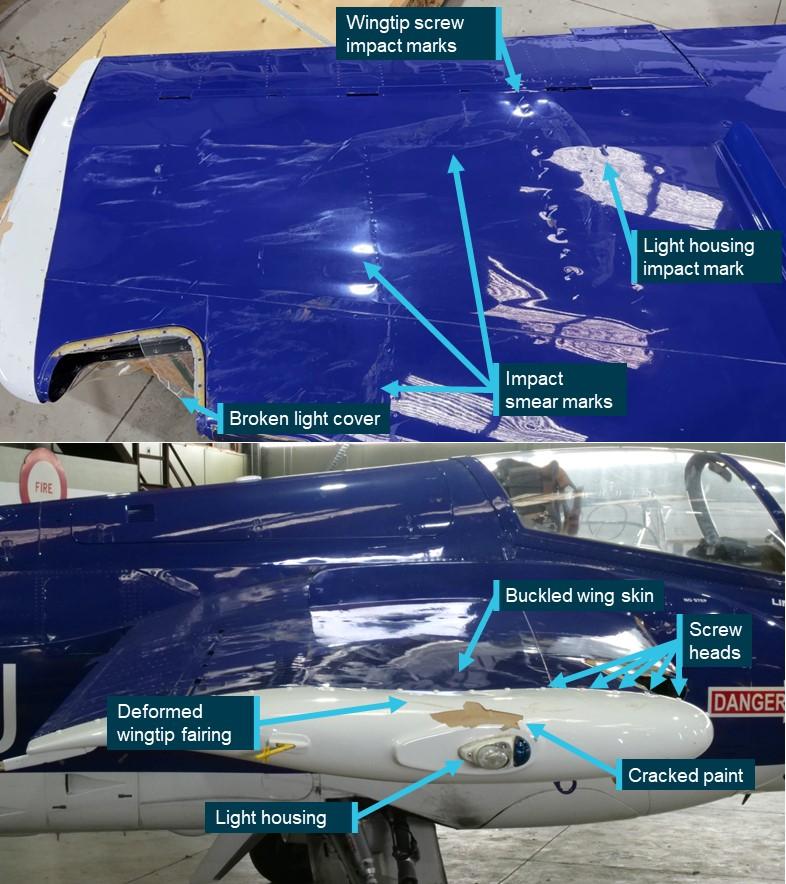
Source: ATSB
Viper 2 (VH-DZJ)
Witnesses observed Viper 2 impact the water in a near-vertical, nose‑down attitude at high speed. The aircraft was extensively damaged and came to rest on the floor of Port Phillip Bay at a depth of 24 m.
The wreckage was located the day after the accident and, on 25 November, Victoria Police recovered most of the fuselage, including the engine. The wing structures and most of the empennage were unable to be located and were not recovered. In the following days, the police conducted further diving operations to retrieve other aircraft debris and associated items.
The ATSB examination of the recovered wreckage did not identify any pre-impact faults, although the scope of the examination was limited by the extensive damage to the aircraft. Damage to the engine was consistent with the engine operating at the time of the collision with water. Examination of the recorded imagery indicated that there were no pre‑collision faults with either aircraft.
The recorded video showed that upon impact, the outboard section of the right wing of Viper 2 bent downward and the lower wing skin separated from the wingtip toward the wing fence[7] along a rivet line immediately aft of the leading edge (Figure 12). The wing tip, leading edge skin and forward wing spar were all deformed by the impact. Once the wing structure of Viper 2 started to fail, it redistributed the load across the wing of Viper 1, lessening the local effects and reducing the overall loads to that aircraft. The right aileron of Viper 2 was also deflected downward in both the normal plane of movement and also the spanwise direction, likely due to the outboard wing section and rear wing spar also being deformed downward.
Figure 12: Right wing of Viper 2 immediately after the collision
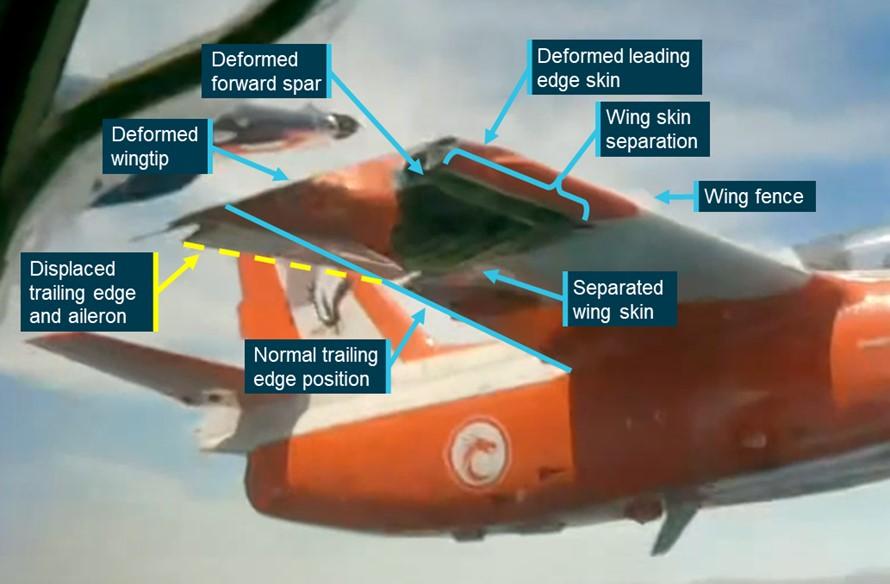
Note: For ease of interpretation the image has been inverted to present the footage in an upright orientation.
Source: Recorded video from Viper 1, modified and annotated by the ATSB
Return to Essendon Airport
Following the collision, Viper 1’s return to Essendon passed over built-up areas. The ATSB examined whether a diversion to another airport would have significantly reduced the risk to persons on the ground from falling debris or a loss of control.
Several airports were available to the crew of Viper 1 for landing. Of these, Avalon Airport presented the most suitable alternative as it was equipped with fire and rescue facilities, a suitable runway, was located away from built up areas and weather conditions at the time were suitable for its use.
Avalon was located 23 NM north‑west of the position of the collision, less than the 39 NM return flight flown by the crew to Essendon, but a direct flight to Avalon would have required flight over water beyond the gliding capability of the aircraft, exposing the crew to elevated risk in the event of a ditching. Following the coast to Avalon (as the crew of Viper 1 did during the return to Essendon) required a 52 NM (northern route) or a 38 NM (southern route) flight (Figure 13).
Figure 13: Flight paths to Avalon Airport

Source: Airservices Australia, Google Earth and ATSB
Following the collision, the crew of Viper 1 conducted controllability checks in both the cruise and landing aircraft configurations. These checks satisfied the crew that the aircraft was not significantly damaged, was fully controllable and that there were no indications that components would detach from the aircraft.
The crew had pre-briefed Moorabbin (also surrounded by built up areas) as the diversion airport but were not prepared for a diversion to Avalon. Therefore, when compared with the return to Essendon that the crew were prepared for and had already undertaken earlier that day, a diversion to Avalon would have introduced additional operational complexities that would have further increased the crew’s workload.
The ATSB assessed that, while a diversion to Avalon would have presented a lower risk to people on the ground than the crew’s decision to return to Essendon, it did not unduly increase risk and was reasonable given the information and resources available to the crew at the time.
Similar occurrences
Argentine Junta de Investigacion de Accidentes de Aviacion Civil investigation 88/15 (LQ‑CGK and LQ-FJQ)
On 9 March 2015, 2 Eurocopter AS350-B3s registered LQ-CGK and LQ-FJQ were operating an aerial filming flight for a French television programme near Villa Castelli, Rioja, Argentina. During the filming flight, the helicopters collided with each other and subsequently with terrain. The pilot and 4 passengers on board each helicopter were fatally injured.
United States National Transportation Safety Board investigation WPR14FA174 (N4962U and N20SF)
On 27 April 2014, a Cessna 210E registered N4962U and Hawker Sea Fury registered N20SF were being flown from Half Moon Bay Airport, California, United Sates of America, to Eagle’s Nest Airport. During the flight, the faster Sea Fury approached the Cessna from behind and the pilot contacted the pilot of the Cessna advising that they intended to pass below and to the left of the Cessna. The Cessna pilot acknowledged and advised that they wanted to take a photograph, the Sea Fury pilot replied that there would probably not be time due to the speed differential. The Sea Fury pilot then observed the Cessna abruptly roll left and attempted to avoid collision by pitching their aircraft’s nose down. The 2 aircraft collided, and the Cessna then collided with terrain fatally injuring the pilot. The Sea Fury landed safely.
United States National Transportation Safety Board investigation CHI06FA077A (N3735W and N372AC)
On 5 February 2006, 2 Shorts Brothers SD360-300 aircraft registered N3735W and N372AC were operating on a formation flight to undertake filming of each aircraft. While flying in formation, the pilot of N3735W advised the pilot of N372AC via radio that they would turn right, toward N372AC while descending. During the turn, the left wing of N3735W collided with the left wing and engine of N372AC. After the collision, N3735W collided with terrain fatally injuring the flight crew and passenger. N372AC made an emergency landing at a nearby airport. The occupants of that aircraft were not injured.
Safety analysis
Accident manoeuvre
Before the flight, the crews briefed and prepared for a manoeuvre that involved Viper 2 moving up to the line abreast position to the right of an inverted Viper 1. It had also been agreed that Viper 2 had some flexibility to move as desired to maximise filming opportunities, while also being responsible for maintaining separation between the 2 aircraft. The pilot of Viper 2 subsequently performed a manoeuvre to pass underneath Viper 1 without pre-briefing the manoeuvre and without advising the crew of Viper 1. During this manoeuvre, Viper 2 passed directly underneath Viper 1 at a close distance, increasing the risk of collision. This manoeuvre had not been specifically briefed prior to the flight and therefore a full assessment of the associated risks was not made at that time.
Following this manoeuvre, there was an in-flight discussion between the pilots. The pilot of Viper 2 advised that the manoeuvre provided a good filming opportunity and asked to repeat it. The pilots discussed the manoeuvre before agreeing to a second attempt. However, the in-flight discussion using the radio, while also flying the aircraft, likely limited the ability of the pilots to ensure there was a full consideration of the associated collision risks and that all participants had a similar mental model.
The recorded video showed that during the accident manoeuvre, Viper 1 maintained stable and level inverted flight. As Viper 2 passed underneath, that aircraft began to climb toward Viper 1 and continued to climb as it passed across to the left side of Viper 1. During this period (about 2 seconds), the pilot of Viper 2 was looking at Viper 1. Just before the collision, the pilot of Viper 2 banked the aircraft away from Viper 1 and the wings collided. It is possible that as Viper 2 passed beneath Viper 1, the pilot inadvertently applied control inputs moving the aircraft closer to Viper 1 (hands following head), but there was insufficient evidence to confirm whether that occurred.
The safety pilot observed Viper 2 pass underneath and begin climbing toward Viper 1, but the collision occurred before the safety pilot could recognise the collision risk and take any avoiding action.
The impact loading on Viper 1 occurred further in-board on the wing, to relatively stiffer and heavier structures, and with impact loads distributed more evenly across the front and rear spar (the primary load carrying structure). In addition, once the structure on Viper 2 started to fail, it redistributed the load over the wing of Viper 1, lessening the local impact effects. As a result, Viper 1 was not significantly damaged and landed safely at Essendon.
Conversely, the primary impact loading on Viper 2 was further outboard near the wingtip to relatively weaker structure, with the loads primarily absorbed by the front spar, resulting in failure of the spar and substantial deformation to the outboard wing section.
The damage to Viper 2 was substantial, created a significant amount of drag, and reduced both lift and aircraft controllability. The video showed that immediately after the impact, control of Viper 2 was lost and soon after, it collided with water, fatally injuring the pilot and camera operator.
Medical restrictions not followed
The pilot of Viper 1 was subject to a medical restriction which prevented them from operating an aircraft with the tandem cockpit configuration of the S-211. However, when the pilot received their medical certificate, they did not fully read the associated requirements and were not aware of that restriction.
This restriction was applied to reduce the risk of any distraction or incapacitation (subtle, partial, or full) to the pilot resulting from a medical episode. By not following this restriction and operating a tandem configured aircraft, the pilot reduced the ability of the safety pilot to identify any early indications of incapacitation and to manage them if they progressed. Given the precise nature of the manoeuvres required in the flight, even a subtle distraction or partial incapacitation could have significantly increased risk to both aircraft. Furthermore, if the pilot were to become fully incapacitated, the safety pilot would not have been able to reposition the pilot if the controls were obstructed or to take control of the aircraft in a timely manner.
The recorded video showed that the during the filming manoeuvring, Viper 1 was manoeuvred as intended with no indication of any pilot incapacitation. Therefore, while this aspect of the medical restriction not being followed increased risk to the flight, it did not contribute to the accident. Furthermore, the risk of control obstruction was reduced by the comprehensive pilot restraints fitted to the S-211.
Having not fully read the medical restriction requirements, the pilot of Viper 1 was also not aware that the safety pilot needed to be fully qualified on the aircraft type to act in that role or that the safety pilot was also required to read the medical restriction requirements. As a result, the safety pilot was not made aware of these requirements.
The safety pilot had not completed the required training to operate the S-211, and therefore was not qualified to act in the safety pilot role. While an unqualified pilot operating an aircraft that they are unfamiliar with can significantly increase risk to a flight, in this case, the safety pilot had commenced S-211 training and was familiar with the aircraft. Furthermore, the safety pilot had significant experience in similar aircraft and operations and carried all required checklists and documentation to operate the S-211 for the flight. Therefore, while the safety pilot was not qualified to meet the requirements of the role, they were prepared and capable of taking control of the aircraft should they have been required to do so. For those reasons, the ATSB assessed that risk to the accident flight was not unduly increased by this mitigation not being followed completely.
Operation type
Ex-military aircraft operated in the Limited airworthiness category are not required to meet civilian airworthiness standards and are operated in Australia with a special certificate of airworthiness. These aircraft can be operated under Civil Aviation Safety Regulation (CASR) Part 132. The framework of these regulations acknowledges the higher risk associated with the operation of these aircraft and mitigates this risk, in part, through limitations on their use.
The purpose of the accident flight was to produce footage of the aircraft to promote a proposed television program. However, the limitations placed on the operation of Limited category aircraft did not permit them to be used for that purpose.
The filming flights were required to be conducted as an aerial work (task specialist) operation. Aerial work operations under CASR Part 138 include several organisational and operational risk mitigations intended to increase safety assuredness that are not required under CASR Part 132. Operating outside of this established framework removed the built-in safety defences of the regulatory structure, thereby increasing operational risk. However, while the reduced airworthiness requirements of Limited category aircraft increased operational risk more generally, these did not contribute to the aircraft handling or decision-making that led to the collision and subsequent loss of Viper 2. Furthermore, it could not be determined if the application of the aerial work regulatory structure to the flights would have introduced a risk control that may have prevented the accident. Therefore, while overall risk assuredness was reduced by the unpermitted operation, using the aircraft in this way could not be shown to have contributed to the accident.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the mid-air collision involving SIAI Marchetti S-211s, VH-DZJ and VH-DQJ, 25 km west of Tyabb Airport, Victoria on 19 November 2023.
Contributing factors
- During a formation flight for the purpose of in-flight filming, Viper 2 was manoeuvred directly beneath Viper 1 for a filming opportunity. This manoeuvre had not been briefed before the flight and increased the risk of collision. An in-flight discussion of the manoeuvre did not allow full consideration of the associated risks before a second attempt was commenced.
- During the second attempt of the manoeuvre, Viper 2 passed beneath, and climbed toward, an inverted Viper 1 and the right wings of each aircraft collided.
- The damage sustained by Viper 2 during the collision led to an immediate loss of control and soon after, a collision with water. Viper 1 was not significantly damaged, and that aircraft landed safely.
Other factors that increased risk
- The pilot of Viper 1 had a medical restriction which required them to only operate an aircraft with a side-by-side cockpit configuration and a qualified safety pilot to be present. These requirements were not being followed during the accident flight.
- The operator did not hold the required operating certificate to undertake the filming flight and the aircraft were not permitted to be used for that purpose. This resulted in a lower level of safety assurance for the flights.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot and safety pilot in VH-DQJ
- Civil Aviation Safety Authority
- Australian Warbirds Association Limited
- Victoria Police
- the aircraft manufacturer
- the maintenance organisation for VH-DZJ and VH-DQJ
- Airservices Australia
- accident witnesses
- video footage of the accident flight
- a formation flying subject matter expert
- Argentine Junta de Investigacion de Accidentes de Aviacion Civil
- United States National Transportation Safety Board.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- pilot and safety pilot in VH-DQJ
- the next of kin of the pilot and camera operator of VH-DZJ
- Civil Aviation Safety Authority
- Australian Warbirds Association Limited
- a formation flying subject matter expert
- aircraft manufacturer
- engine manufacturer.
Submissions were received from:
- pilot and safety pilot in VH-DQJ
- the next of kin of the pilot and camera operator in VH-DZJ
- Civil Aviation Safety Authority
- Australian Warbirds Association Limited.
- the formation flying subject matter expert
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance. A mayday call can also made on behalf of one aircraft by another.
[2] Civil Aviation Safety Regulations 61.062: Prescription of types of aircraft for additional limitations on class ratings, and 61.747: Limitations on exercise of privileges of class ratings in certain aircraft—flight review
[3] The S-211 was not designed to facilitate bailing out and the canopy design made this form of egress impractical.
[4] CASR 138.010 (4) defines a task specialist operation as carrying out a specialised activity using an aircraft in flight and includes training for such an activity.
[5] A Safety Management System is an organised approach to managing safety and includes defined organisational structures, accountabilities, policies and procedures.
[6] The Formation and Safety Team is a worldwide, educational organisation teaching safe formation flying in restored, vintage military aircraft and civilian aircraft. FASTA is the Australian division of this organisation. The FASTA Formation Fundamentals manual is not approved or endorsed by CASA for training and operational purposes.
[7] Wing fences are flat plates fixed to the upper surfaces of an aircraft wing in line with the airflow which increase the aerodynamic efficiency of the wing.
 Source: Kovozavody Prostejov, modified and annotated by the ATSB
Source: Kovozavody Prostejov, modified and annotated by the ATSB







