
Executive summary
What happened
On the evening of 24 October 2022, a Link Airways Saab 340, registered VH-VEQ, was being operated on an air transport flight from Canberra, Australian Capital Territory to Sydney, New South Wales. As the aircraft approached Sydney, in cloud and at night, with the autopilot engaged, air traffic control cleared the aircraft for the instrument landing system (ILS) approach to runway 34 left.
The aircraft intercepted the ILS localiser at an altitude and distance from the runway that positioned it close to being on the glideslope for the approach. However, as the approach continued, the crew observed that the aircraft did not commence descending as expected, with the cockpit instruments indicating that the aircraft remained on the glideslope. In response, the captain temporarily disengaged the autopilot and manually increased the descent rate. The approach continued until the ground proximity warning system generated a ‘glideslope’ alert. At about the same time, the crew assessed the approach as unstable and commenced a missed approach.
What the ATSB found
The ATSB found that, unknown to the crew and prior to commencing the approach, an unidentified instrumentation fault resulted in erroneous on‑slope indications being presented on the pilot’s instruments without any failure indication. Consequently, the autopilot did not descend the aircraft as expected, resulting in the crew initiating a manual descent. The crew subsequently re-engaged the autopilot as the aircraft descended at a rate exceeding that required for the approach.
The autopilot maintained the excessive descent rate rather than recapturing the glideslope. As the aircraft descended below about 1,000 ft above ground level, the ground proximity warning system activated due to the significant deviation below the glideslope.
What has been done as a result
Although maintenance action could not be linked to the incident, the operator developed and implemented several maintenance‑related safety actions following the occurrence. These included a standardised component reinstallation (re‑rack) procedure based upon aircraft manufacturer guidance. This procedure aimed to reduce faults possibly created during defect troubleshooting. The operator also issued an internal notice to maintenance personnel that provided guidance on the required items to be included in maintenance explanatory text.
Safety message
During this incident, the crew faced a complex scenario where, unknown to the crew, an instrumentation failure presented them with erroneous on-glideslope indications, without any failure indications, while conducting a precision approach at night and in cloud. The absence of any failure indications reduced the ability of the crew to identify the fault, which incorrectly showed the aircraft on the correct and expected approach path.
The incident highlights the importance of assessing all available indications and being ready to initiate a missed approach early should there be a significant exceedance from expected aircraft performance or instrument indications, such as the excessive descent rate during this occurrence.
The value of adherence to operational procedures to ensure safe aircraft operation is also underlined—upon recognising that the approach was unstable and in response to the glideslope alert, the crew correctly conducted a missed approach. The crew then identified the subsequent erroneous glideslope indications and completed a safe landing using a different approach type.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On the evening of 24 October 2022, a Link Airways Saab 340 registered VH-VEQ, was being operated on an air transport flight from Canberra, Australian Capital Territory to Sydney, New South Wales.[1] The captain was acting as pilot flying, and the first officer as pilot monitoring.[2]
The aircraft departed Canberra at 1910 local time. At 1944, as the aircraft approached Sydney in cloud and at night with the autopilot engaged, air traffic control cleared the aircraft for the instrument landing system (ILS) approach to runway 34 left via the waypoint SOSIJ.
As the aircraft tracked toward SOSIJ, the crew configured the aircraft’s instrumentation and navigation radios for the ILS approach. Unknown to the crew, an instrumentation fault resulted in erroneous glideslope indications (see the section titled Instrument landing system) being presented on the electronic attitude director indicators (EADIs) without any failure indication.
At 1946:11 the aircraft was 13.7 NM from the runway and descending through 5,357 ft above mean sea level (AMSL). Shortly after, the crew used the autopilot global positioning system navigation mode to commence a turn to intercept the localiser track and at 1947:19, the first officer announced that the EADI localiser course bar was active.
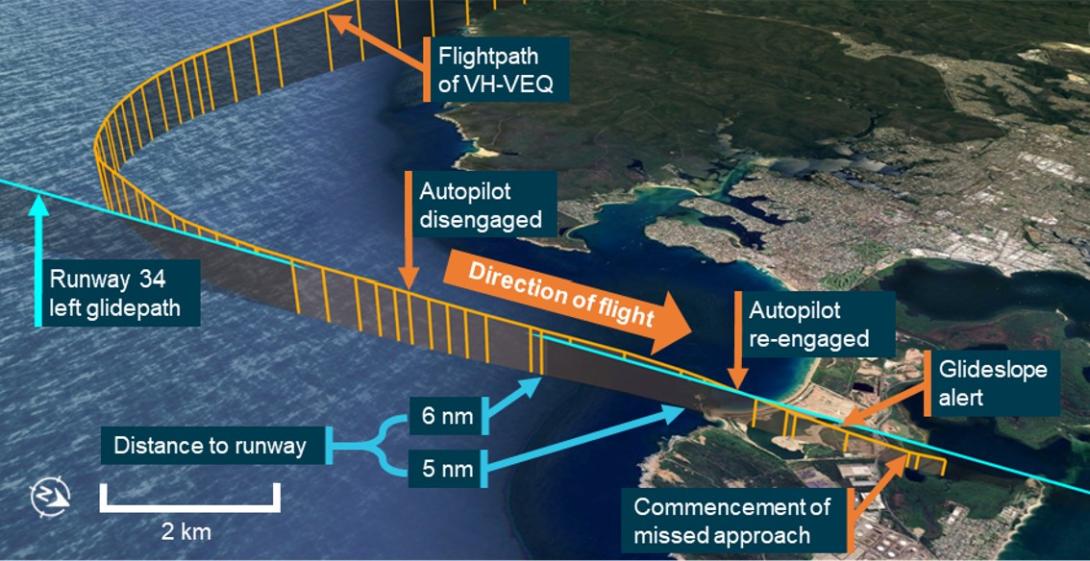
The aircraft continued descending and at 1947:58, as the aircraft tracked to intercept the localiser, the cockpit voice recorder captured the first officer asking, ‘What’s it doing with the glideslope?’ (Figure 1).
Figure 1: Flightpath of approach

Source: Recorded flight data and Google Earth, annotated by ATSB
As the descent continued, the autopilot switched automatically to localiser mode and captured the ILS localiser at an altitude and distance from the runway that positioned the aircraft close to being on the glideslope for the approach. The autopilot subsequently captured the glideslope and the crew continued the approach using the autopilot approach mode. The crew observed that the aircraft did not commence descending as expected to maintain the glidepath, despite the EADIs indicating that the aircraft remained on glideslope. The captain assessed that there was probably some lag in the glideslope indication and its input to the autopilot capturing of the glideslope. To progress the aircraft’s descent along the glideslope, the captain disengaged the autopilot and manually increased the descent rate.
The crew continued the approach and when 6 NM from the runway, as the aircraft descended past 2,205 ft AMSL at 1,759 feet per minute (ft/min) and with an indicated air speed of 184 kt, the captain requested a height and distance check. The first officer advised that they should be passing 1,930 ft AMSL and the captain commented that the glideslope indication was ‘way out’.
At 1949:39, the crew selected the landing gear down and 8 seconds later, when the aircraft was approaching 5 NM from the runway, the captain requested another height check. The first officer advised that at 5 NM, they should be passing 1,610 ft and the captain commented ‘It seems as though we’re coming back on’. As the aircraft approached within 5 NM from the runway, it was descending past 1,693 ft AMSL at 1,280 ft/min at a speed of 176 kt.
At 1949:58, the descent rate increased to 1,920 ft/min and 5 seconds later, the aircraft descended through the 3° approach profile at a speed of 171 kt. At about the same time, the crew re‑engaged the autopilot in the glideslope and localiser hold mode. The approach continued and the autopilot maintained the excessive descent rate and the aircraft descended significantly below the glideslope. At that time, the first officer observed that both the glideslope and the localiser indications were centred.
A few seconds later, at 1950:08, the first officer commented that their EADI glideslope indication had commenced moving and was ‘… going way off now’. At the same time, air traffic control cleared the aircraft to land.
The captain then called for the flaps to be extended, but the first officer did not complete the action as they were engaged in trying to resolve the conflicting glideslope indications. A second later, as the aircraft descended below 957 ft AMSL (about 380 ft below the glideslope – full-scale deflection), the ground proximity warning system generated a ‘glideslope’ alert (see the section titled Ground proximity warning system) (Figure 2) and 7 seconds later, the crew commenced a missed approach. At 19:50:36, 10 seconds after the missed approach was commenced, air traffic control issued a safety alert to the crew advising them to check their altitude. The minimum height recorded during the missed approach was 586 ft.
Figure 2: Flightpath of the descent below glideslope
Source: Recorded flight data and Google Earth, annotated by ATSB
After completing the missed approach, air traffic control repositioned the aircraft for another approach. During this repositioning, when the aircraft was 11.6 NM from the runway and flying level at 2,445 ft (1,259 ft below the glideslope – full-scale deflection), the crew re‑selected the ILS and commented that the EADI glideslope indication showed the aircraft to be on glideslope. The crew then completed a required navigation performance approach and landed without further incident.
After the aircraft had landed and the passengers had disembarked, the cockpit voice recorder captured the crew discussing the incident. During this discussion, the captain and first officer both stated that the EADI glideslope indications were constantly on glideslope until just before they commenced the missed approach when the first officer’s EADI indications moved rapidly up to show the aircraft as being very low. The captain’s EADI glideslope indication remained constantly on slope throughout and after the approach. Both crewmembers stated that no ILS or instrumentation failure indications were presented, and the captain also stated that the standby ILS indicator showed a constant on glideslope indication.
Context
Crew details
The captain held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. The captain had 6,277 hours of flying experience, of which 242 hours were on the Saab 340.
The first officer held a commercial pilot licence (aeroplane) and class 1 aviation medical certificate. The first officer had 455 hours of flying experience, of which 244 hours were on the Saab 340.
The ATSB found no indicators that the flight crewmembers were experiencing a level of fatigue known to affect performance.
Instrument landing system
An instrument landing system (ILS) is an instrument approach procedure that provides lateral (localiser) and vertical (glideslope) position information using angular deviation signals from the localiser antennas (located past the upwind end of the runway) and the glideslope antennas (located approximately 1,000 ft from the runway threshold). Aircraft systems detect these radio signals and provide instrument indications which, when utilised in conjunction with the flight instruments, enable an aircraft to be manoeuvred along a precise final approach path.
The Sydney runway 34L ILS approach included a 3° glideslope to the runway (Figure 3). During the incident approach, when the autopilot was re‑engaged, the groundspeed of the aircraft was 165 kt and the rate of descent required to descend along the glideslope at that groundspeed was about 876 ft/min.
Figure 3: Sydney runway 34 left ILS approach chart
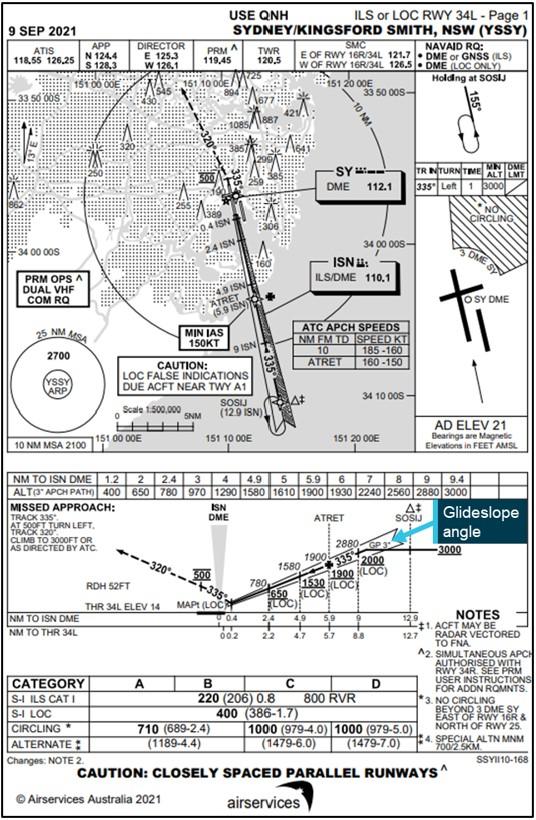
Source: Airservices Australia, annotated by ATSB
The ILS ground equipment can emit false glideslopes at steeper than normal glideslope angles. The lowest of these typically occurs at about 9° to 12°, well above the flightpath of VH-VEQ during the incident approach.
Before and after the incident, a number of other aircraft completed uneventful ILS approaches to runway 34L, with no unusual indications reported by the crews of these aircraft.
Aircraft instrumentation
VH-VEQ was equipped with the Rockwell Collins Pro Line 4 electronic flight instrument system. This system used cathode ray tube displays to present flight and navigation information on the left (captain) and right (first officer) electronic attitude direction indicators (EADIs) and electronic horizontal situation indicators (EHSIs) (Figure 4).
The data presented on each side’s EADI and EHSI was provided by a corresponding display processor unit (DPU). The DPUs received data from numerous aircraft systems, including the navigation radios[3] and used the data to generate the required text and imagery for each display.
Figure 4: Saab 340 left (captain’s) flight instrumentation
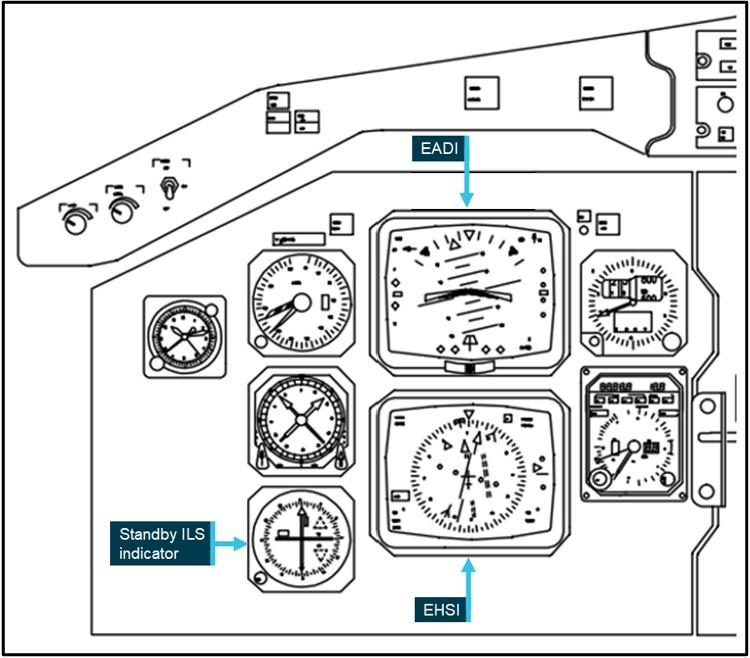
Source: Link Airways, modified and annotated by ATSB
The ILS glideslope indication was presented on the right side of each EADI as fly-up or fly‑down commands on the glideslope indicator. Glideslope deviation was displayed with a centre marker and deviation dots (Figure 5). Full-scale deflection equated to about 0.7° of angular deviation from the nominal glideslope.
If the aircraft receiver malfunctioned, or the glideslope or localiser signals were invalid, a red glideslope or localiser indication (flag) should be presented on the respective erroneous EADI and standby ILS indications. If the DPU failed, a DPU fail indication should be presented on the EADI. No failure flags were reported on either EADI or on the standby ILS indicator during this incident.
Figure 5: Electronic attitude direction indicator
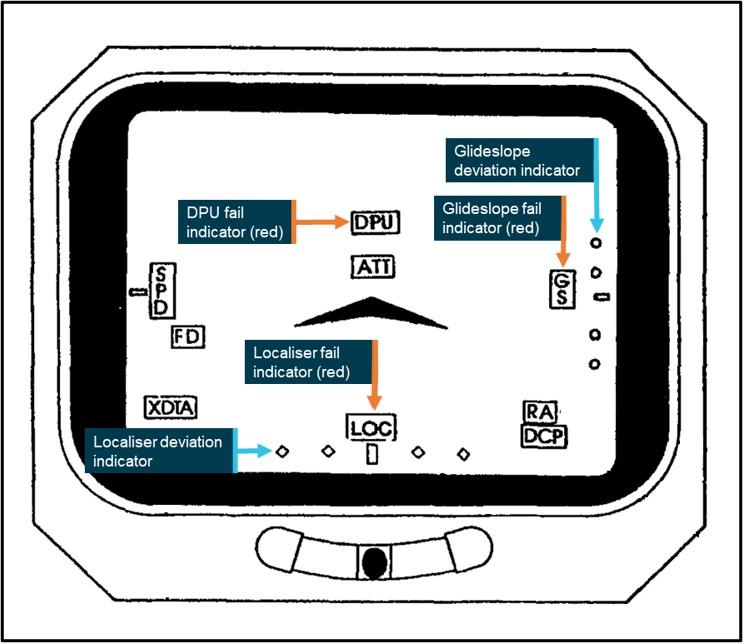
Source: Saab, modified and annotated by ATSB
Post incident examination and analysis
On the morning after the incident, an engineer tested the ILS instrumentation in VH-VEQ by simulating ILS data inputs to the DPUs. This testing found that the captain’s EADI presented a constant and erroneous on-glideslope indication while the standby and first officer glideslope indications were presented correctly. The captain and first officer’s DPUs were then removed and reinstalled in opposite positions and were again tested. This second testing found all 3 (captain, first officer and standby) glideslope indications were presented correctly.
Following the testing, the DPU found to be presenting faulty signals to the captain’s EADI during the incident was removed from service and sent to the manufacturer for examination. The examination found several damaged components within the unit, however it was not determined whether this damage contributed to the erroneous glideslope indications.
The manufacturer advised that, provided the signal from the navigation radio was valid, then information and indications derived from that signal would be displayed when that navigation radio was selected as the data source. The absence of any fault indications on the EADI indicates that the navigation radio was providing valid data, but that the data was likely outside of the normal data range scale. The manufacturer advised that the presentation of erroneous glideslope indications without any fault indication suggested an issue with the navigation radio.
Following the incident, the navigation radios were not tested or removed from the aircraft. No similar occurrences were reported in the subsequent operation of VH-VEQ.
The aircraft and avionics manufacturers advised that this incident was the first occurrence of its type on the Saab 340 or on any other Pro Line 4-equipped aircraft.
Ground proximity warning system
The aircraft was equipped with an enhanced ground proximity warning system (EGPWS). This system used aircraft inputs combined with internal terrain, obstacles, and airport runway databases to predict potential conflicts between the aircraft flight path and terrain or an obstacle.
The system also included a mode which detected excessive deviation below an ILS glideslope. The first level alert occurred when the aircraft was below 1,000 ft radio altitude with a deviation greater than 25% below the glideslope. In that case, a ‘glideslope’ aural alert was generated, and the caution light illuminated. Increases in deviation below the glideslope caused additional ‘glideslope’ alerts at increasing frequency. A second level alert occurred when the aircraft was below 300 ft radio altitude with a glideslope deviation of 40% or greater. This level generated a louder ‘glideslope’ alert every 3 seconds, continuing until the deviation was corrected.
Stable approach criteria
The operator’s flight crew operation manual stipulated that all flights must be stabilised by 1,000 ft above airport elevation in instrument meteorological conditions[4] and that flight crew must fly a stabilised approach to land at an aerodrome. The criteria to be met for an approach to be stabilised at 1,000 ft was:
- The aeroplane is either in level flight or on descent with less than 1,000 ft per min sink rate (unless required to meet specific approach criteria), and
- Below first stage flap and/or gear extension speed whichever is higher, and
- Not accelerating.
Note: To be considered stable, ILS approaches must be within one dot[5] of the glideslope and localizer and wings must be level below 300 feet AGL (except for minor corrections of less than 5 degrees angle of bank).
Despite the stabilised approach criteria and the advice on when a missed approach should be conducted, the PIC should go-around whenever they deem a missed approach is necessary.
Meteorology
At 1950, the time of the commencement of the missed approach, the Sydney Airport automated weather information service reported the wind as 7 kt from 330° magnetic. Cloud cover was reported as scattered at 821 ft above mean sea level (AMSL) and broken at 2,121 ft AMSL. Visibility was reported as 25 km.
Recorded data
Analysis of flight data from the flight data recorder showed the glideslope value indication presented on the captain’s EADI was fixed at 0.1 dots below glideslope throughout the occurrence. The glideslope indications presented on the first officer’s EADI and standby ILS indicator were not recorded.
As the aircraft descended below 1,000 ft radio altitude, the activation of the glideslope alert was recorded by the flight data recorder and cockpit voice recorder.
During the flight, no comment was made by either crewmember about the indications on the standby ILS indicator.
Safety analysis
Instrumentation fault
Following the incident, testing found the left (captain’s) display processor unit (DPU) to be faulty and it was removed from the aircraft and replaced. Since replacing the DPU, there have been no additional reports of erroneous glideslope indications on this aircraft. This indicates that the DPU was potentially the source of the false indications, although this could not be conclusively determined. The DPU was shipped to the manufacturer where a teardown of the unit was undertaken, and several failed components identified. However, when analysing the occurrence, the manufacturer reported that the failure indications were more consistent with an issue originating from the navigation radio. Both the aircraft and instrumentation manufacturers reported that this was the only known failure of its kind in the history of the aircraft type or on other aircraft equipped with the Pro Line 4 electronic flight instrument system.
While the precise source of the error could not be determined, it resulted in a constant on‑glideslope indication on the captain’s electronic attitude direction indicator (EADI) regardless of the aircraft's position relative to the glideslope. The indications were presented with no glideslope or DPU failure indication.
The first officer also reported similar erroneous indications on their EADI during the approach and made several comments about the glideslope that were recorded by the cockpit voice recorder. These comments often referred to a glideslope indication that differed from the recorded position of the aircraft. While the first officer’s glideslope indications were not recorded by the flight data recorder, these statements, the first officer’s reported observations and the recorded glideslope values indicated that the erroneous glideslope indications were also, at least intermittently, presented on the first officer’s EADI. However, as the aircraft descended below 1,000 ft, this EADI began presenting a correct fly‑up indication.
After the flight, the captain stated that the indications on the standby ILS indicator were also erroneous. The standby indicator’s input signals were not provided by the faulty DPU, and the glideslope indications displayed were not recorded by the flight data recorder. There was also no comment made by the crew referring to the standby ILS during the flight. Consequently, it could not be determined what indications were present.
Descent below glideslope and recovery
The erroneous on-glideslope indications were presented to the crew without any glideslope fault indications so the crew were not alerted to the instrumentation failure by the system. The aircraft commenced the approach at a position close to the glideslope. This positioned the erroneous indication close to the expected and correct glideslope indication. Furthermore, both EADIs very likely presented similar erroneous glideslope indications and the localiser indications were presented correctly. Therefore, when the autopilot did not descend the aircraft along the glideslope as anticipated, the crew were not immediately alerted to a potential instrumentation failure. Instead, the crew assessed that the autopilot was probably experiencing a lag in capturing the glideslope and the captain responded by disconnecting the autopilot and manually descending the aircraft to follow the glideslope.
The crew subsequently observed unusual glideslope indications and completed several altitude and distance checks in an attempt to understand the conflicting indications. As the aircraft descended close to the glideslope and with an on-glideslope indication, the captain re‑engaged the autopilot. However, this occurred when the aircraft was descending at an excessive rate for the approach, the implication of which did not appear to be recognised by the crew. As the aircraft continued the excessive descent rate, the instruments continued to show erroneous on-glideslope indications and the aircraft subsequently descended below the glideslope.
As the aircraft descended below 1,000 ft AMSL while significantly below the glideslope, the aircraft penetrated the ground proximity warning system warning envelope and a ‘glideslope’ alert sounded. At about the same time, the first officer’s EADI began showing correct glideslope indications. At that point the crew recognised the approach was unstable and immediately commenced a missed approach.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the flight instrumentation failure and descent below glideslope involving Saab 340, VH-VEQ on 24 October 2022.
Contributing factors
- During an instrument landing system approach, an undetermined instrumentation fault resulted in an erroneous on-glideslope indication being presented constantly on the left electronic attitude direction indicator and intermittently on the right electronic attitude direction indicator.
- The erroneous on-glideslope indications were presented without a fault indication and regardless of the aircraft's actual position relative to the glideslope. When the autopilot did not descend the aircraft along the glideslope as expected, the crew initiated a manual descent.
- The crew subsequently re-engaged the autopilot as the aircraft descended at a rate exceeding that required for the approach. The autopilot maintained the excessive descent rate, and the aircraft descended significantly below the glideslope.
Other findings
- As the aircraft descended below about 1,000 ft above ground level while about 380 ft below the glideslope, the ground proximity warnings system activated, and the crew recognised that the approach was not stabilised. In response, they commenced a missed approach.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Safety action not associated with an identified safety issue
Proactive safety action by Link Airways
| Action number: | AO-2022-050-PSA-01 |
| Action organisation: | Link Airways |
Following the occurrence, the operator developed and implemented a standardised component reinstallation (re-rack) procedure based upon aircraft manufacturer guidance. This procedure aimed to reduce faults possibly created during defect troubleshooting.
| Action number: | AO-2022-050-PSA-51 |
| Action organisation: | Link Airways |
The operator also issued an internal notice to maintenance personnel that provided guidance on the required items to be included in maintenance explanatory text. This notice also highlighted the importance of detailed explanatory information.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Link Airways
- the flight crew
- the aircraft manufacturer
- the instrumentation manufacturer
- Bureau of Meteorology
- Civil Aviation Safety Authority
- Airservices Australia
- recorded flight data and cockpit voice data from VH-VEQ.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Link Airways
- the flight crew
- Civil Aviation Safety Authority
- the United States National Transportation Safety Board
- the Swedish Accident Investigation Board
- the aircraft manufacturer
- the instrumentation manufacturer.
Submissions were received from:
- the first officer
- the United States National Transportation Safety Board
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The flight was operated under Civil Aviation Safety Regulations Part 121 (Air transport operations - larger aeroplanes).
[2] Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[3] The navigation radio is the aircraft instrument that receives the radio signals from the ILS ground stations. The navigation radio interprets the signal information and then provides data to the DPUs for presentation on the EADI and the standby ILS indicator.
[4] Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under Instrument Flight Rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[5] Each dot of glideslope deviation indication equals 20% of angular deviation.
