
Executive summary
What happened
At 0715 local time on 29 August 2022, a Cessna R182 Skylane RG (R182), registered VH-EHM, and operated by Executive Helicopters, departed a private property (Lighthouse) north-east of Roma, Queensland for an air transport flight under the visual flight rules (VFR) to Archerfield Airport. The aircraft departed with the pilot, 2 passengers, and a passenger’s pet dog on board.
As the aircraft attempted to cross a section of the Great Dividing Range, the pilot encountered forecast low cloud and reduced visibility, and was unable to find a way across. With limited fuel remaining, the pilot diverted to Dalby Airport and refuelled the aircraft before departing once again to find a different location to cross the elevated terrain.
After crossing a section of the Great Dividing Range at low level, the pilot tracked to the north of Amberley below low cloud towards an area adjacent to the D’Aguilar Range. While manoeuvring around the edge of this range, the aircraft collided with terrain during a turn, about 36 km north‑west of Archerfield. All occupants of the aircraft were fatally injured.
What the ATSB found
The ATSB found that the en route forecast available before departing Lighthouse predicted that the flight to Archerfield would be affected by low cloud, rain, fog and associated reduced visibility, particularly around the elevated terrain of the Great Dividing Range. After departing Lighthouse, the pilot encountered and manoeuvred at low level around forecast low cloud over elevated terrain of the range before diverting and landing at Dalby to refuel. An updated weather forecast available while at Dalby predicted similar conditions as previously forecast with additional periods of deteriorating weather around Amberley and Archerfield. However, the low cloud and deteriorating weather were expected to dissipate within the next 2-3 hours. The updated weather was not reviewed by the pilot while on the ground and, after refuelling, they subsequently departed once again toward forecast en route weather unsuitable for visual flight.
The pilot likely reviewed the updated weather forecast in-flight, shortly after take-off, but continued the flight at low level, and at normal cruise speed towards elevated terrain. After crossing a section of the Great Dividing Range below cloud and with minimal terrain separation, the pilot continued the flight in similar conditions toward the Lake Manchester VFR route adjacent to the D’Aguilar Range. While manoeuvring in this area, the aircraft very likely entered cloud resulting in the pilot losing visual reference with the ground and surrounding terrain, eventually leading to controlled flight into terrain.
There was no evidence of any conditions or circumstances likely to induce a medical problem or incapacitation for the pilot. There was also no evidence of any aircraft system or mechanical anomalies that would have influenced the accident. It was also considered unlikely that there was any direct or perceived organisational pressure on the pilot to continue the flight.
The pilot was probably influenced by plan continuation bias – an internal pressure or desire to get to the destination – to continue the flight, which probably became stronger as they got closer to Archerfield Airport. However, due to a lack of information, the ATSB was unable to determine the reasons why the pilot continued the flight at cruise speed and low level into unsuitable weather in the vicinity of known high terrain.
The investigation identified several other factors related to flight notification and fuel planning. Although these factors increased risk, they were not considered contributory to the accident.
Finally, the investigation found that the operator's hazard and risk register, which formed part of the organisation's safety management system, did not identify inadvertent entry into instrument meteorological conditions (IMC) as a hazard, which reduced the ability of the organisation to effectively manage the related risk.
What has been done as a result
The operator advised that they had removed aeroplane operations from their Air Operator's Certificate (AOC) and updated the hazard and risk register to include inadvertent entry into IMC. A risk assessment was conducted with the following risk controls planned to be implemented by February 2024 to minimise the risk of inadvertent entry into IMC for helicopter operations:
- the operations manual is to be updated to include a formal organisational policy for supporting pilots to land or return to a safe landing site if they assess that they will be unable to maintain visual meteorological conditions.
- annual operator proficiency checks will include inadvertent IMC avoidance and recovery techniques.
Safety message
The safety risks of visual pilots flying into non-visual conditions are well documented. This continues to be a recurring factor in aircraft accidents and has been the focus of numerous previous ATSB reports and publications.
A large amount of reference material is available to pilots for guidance on avoiding VFR flight into adverse weather as well as recovery should inadvertent IMC entry occur. The United States Aircraft Owners and Pilots Association Air Safety Institute website VFR into IMC provides an online course, videos and reference materials to assist pilots in avoiding and managing these scenarios. Additionally, the ATSB publication Avoidable Accidents No. 4, Accidents involving Visual Flight Rules Pilots in instrument Meteorological Conditions provides lessons learned from the analysis of various weather-related accidents and incidents.
Aviation safety risk management can be applied at all levels of aviation to enhance operational safety. For commercial operators, formalised risk management supports individual pilot decision making and provides a systemic approach to safety by introducing layers of controls to reduce single point of failure accidents.
As such, the ATSB strongly encourages operators to specifically assess the risk of inadvertent IMC and implement mitigation strategies commensurate to the level of risk it presents to their pilots and passengers.
The occurrence
On 28 August 2022 a Cessna R182 Skylane RG (R182), registered VH-EHM and operated by Executive Helicopters, flew from Archerfield Airport, Queensland to a private property (Lighthouse) north‑east of Roma, Queensland, with a pilot, 3 passengers, and a passenger’s pet dog on board.
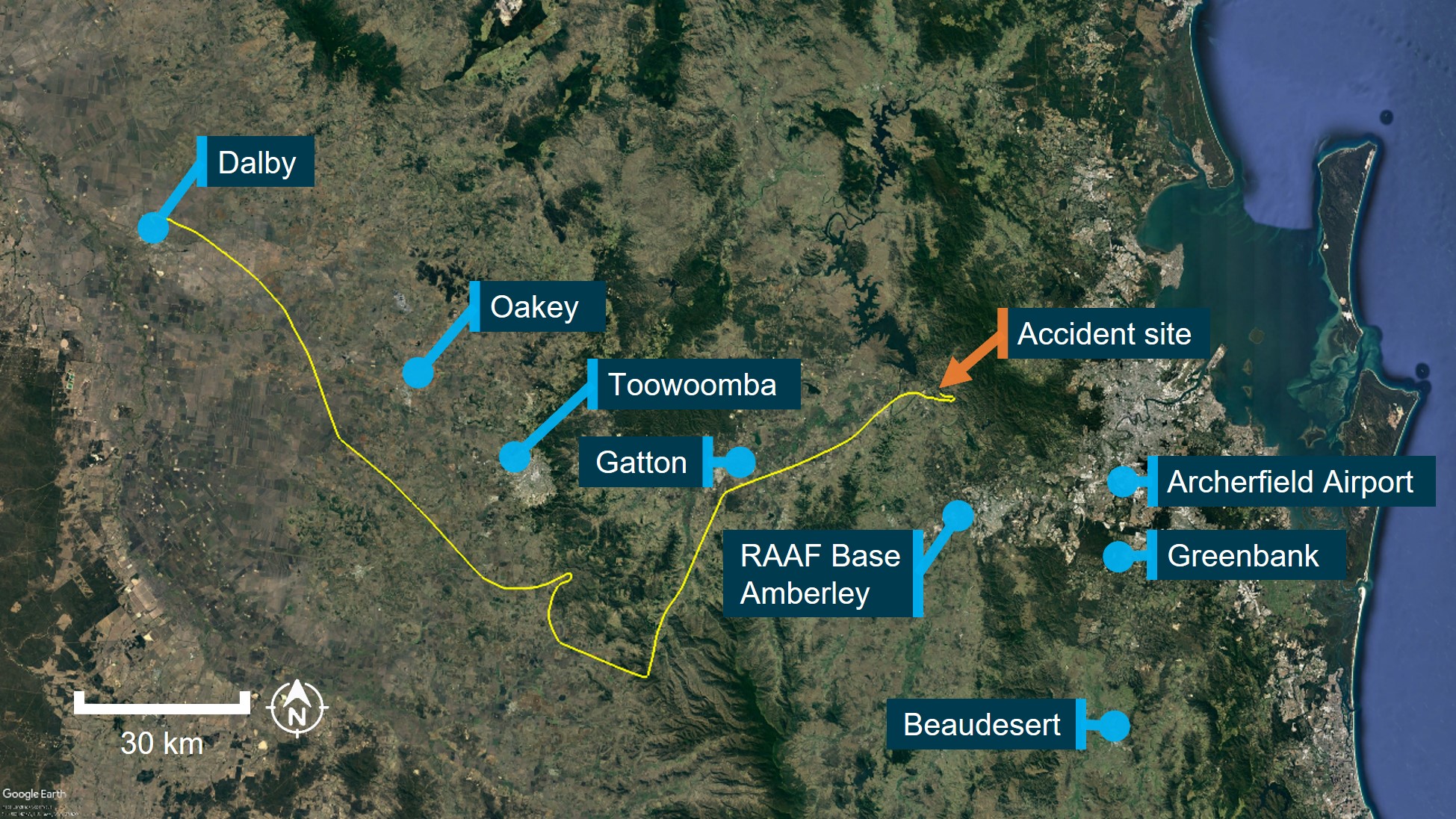
The following day, VH-EHM departed Lighthouse at 0715 local time with the pilot, 2 passengers, and pet dog, for an air transport[1] flight under the visual flight rules (VFR)[2] back to Archerfield (Figure 1). Recorded flight data showed the aircraft was initially established on a direct south‑easterly track towards Archerfield at cruise altitudes between 3,400 ft and 3,900 ft above mean sea level (AMSL).[3] The en route weather forecast valid at the time of departure indicated low cloud, rain, fog and associated reduced visibility (see the section titled Meteorological information).
At 0828, the pilot turned the aircraft left and descended to about 1,800 ft AMSL (about 600 ft above ground level (AGL))[4] before tracking north, then east towards the Biarra Range into a valley. The aircraft was then descended to about 1,200 ft (700 ft AGL), before the pilot completed a 180° turn at 300 ft AGL, climbed to 3,900 ft (2,000 ft AGL) and tracked towards Dalby Airport.
At about 0850, the pilot was contacted by a person via mobile phone. During the conversation, the pilot reported some weather on the range and their intention to refuel at Dalby before attempting to find another way to Archerfield. At 0901, the aircraft landed at Dalby and was refuelled with about 263 L of fuel.
Figure 1: Flight to Dalby Airport
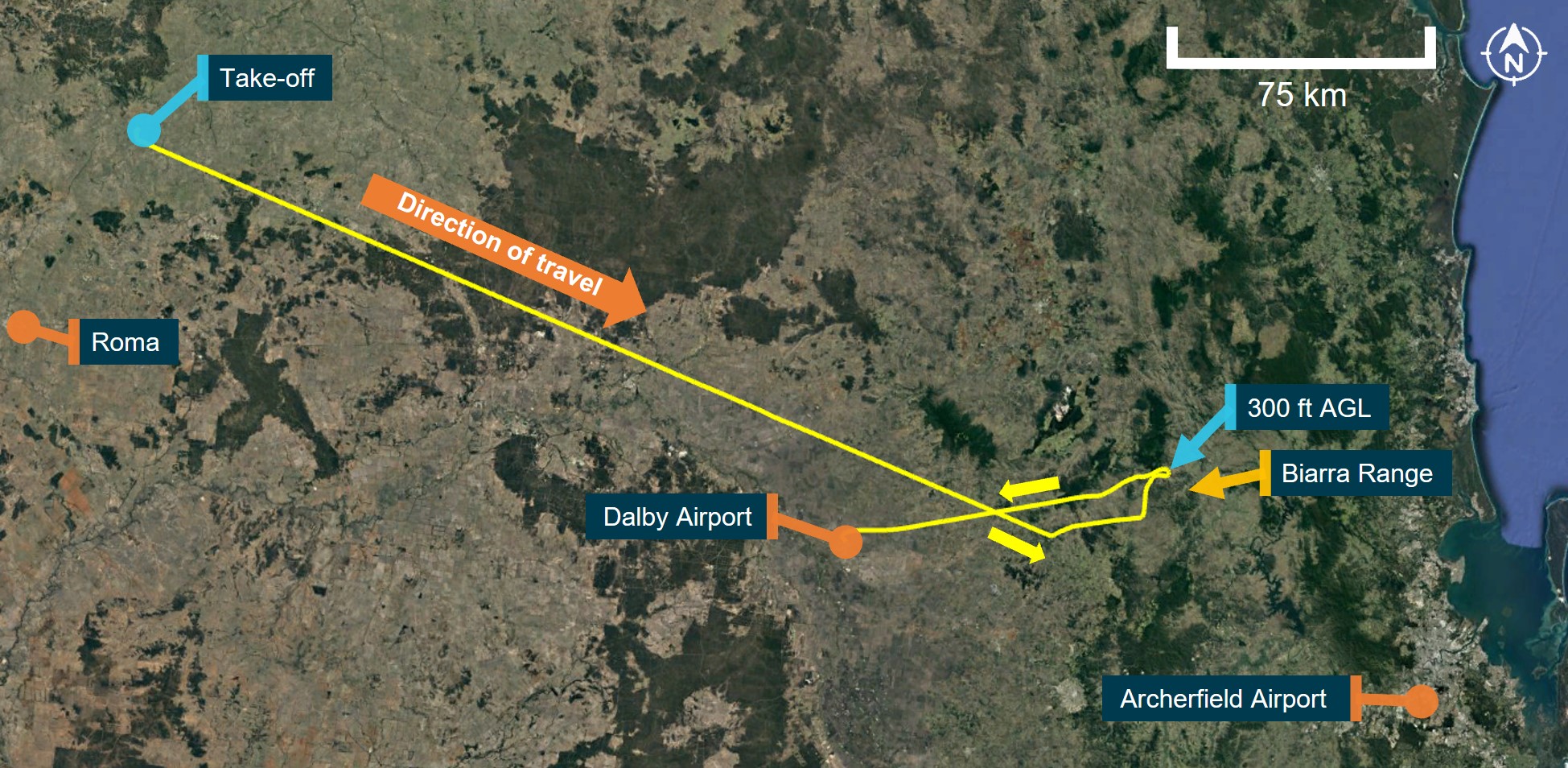
Source: Google Earth and OzRunways, annotated by ATSB
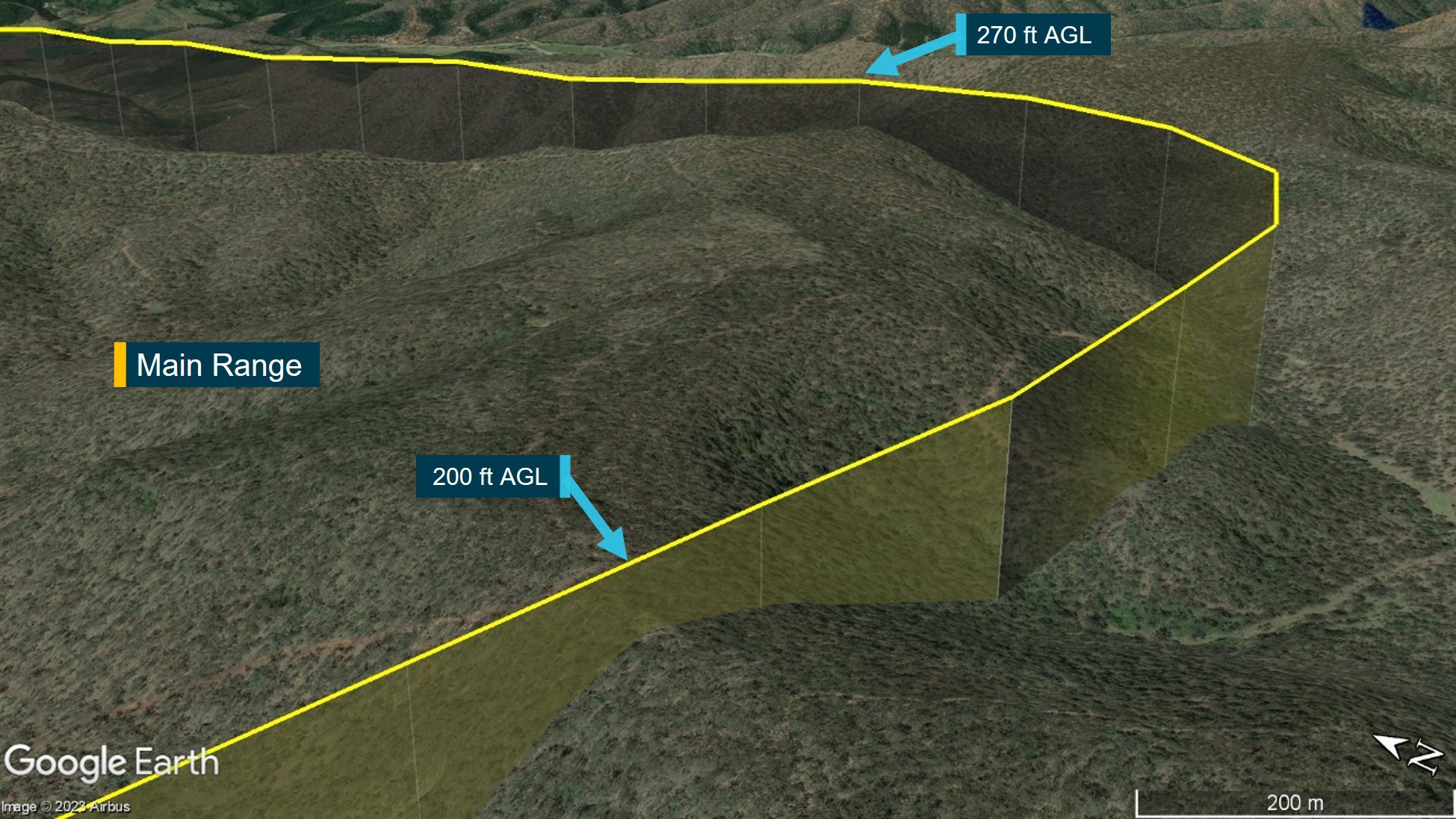
Recorded data showed that VH-EHM departed Dalby at about 0912 and tracked southeast before climbing to a cruise altitude of about 2,500 ft (1,300 ft AGL). By 0927, the flight had progressed over rising terrain and, about 3 minutes later, was operating at about 2,300 ft (400 ft AGL) (Figure 2). At 0935, the pilot turned left towards Main Range, and about 8 km later, completed a 180° turn between 300–500 ft AGL before tracking south-east and climbing to about 2,500 ft (1,000 ft AGL).
At 0946, the aircraft passed over a mountain ridge at about 2,800 ft (200 ft AGL) before conducting a 90° left turn over another ridge at about 2,900 ft (270 ft AGL). VH-EHM then tracked to the north‑east and descended down the range to an altitude of about 1,200 ft (700 ft AGL).
Figure 2: Accident flight
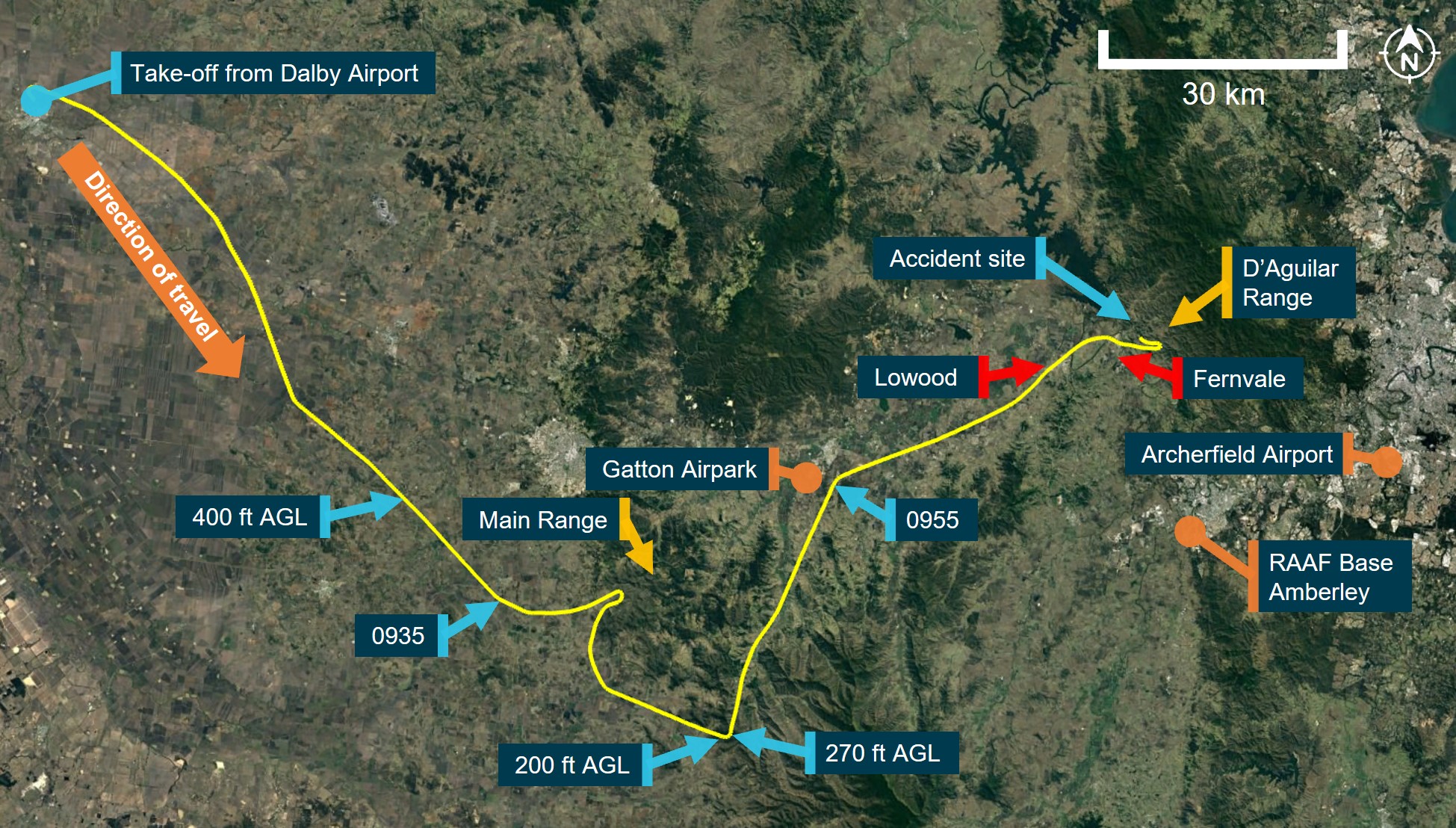
Source: Google Earth and OzRunways, annotated by ATSB
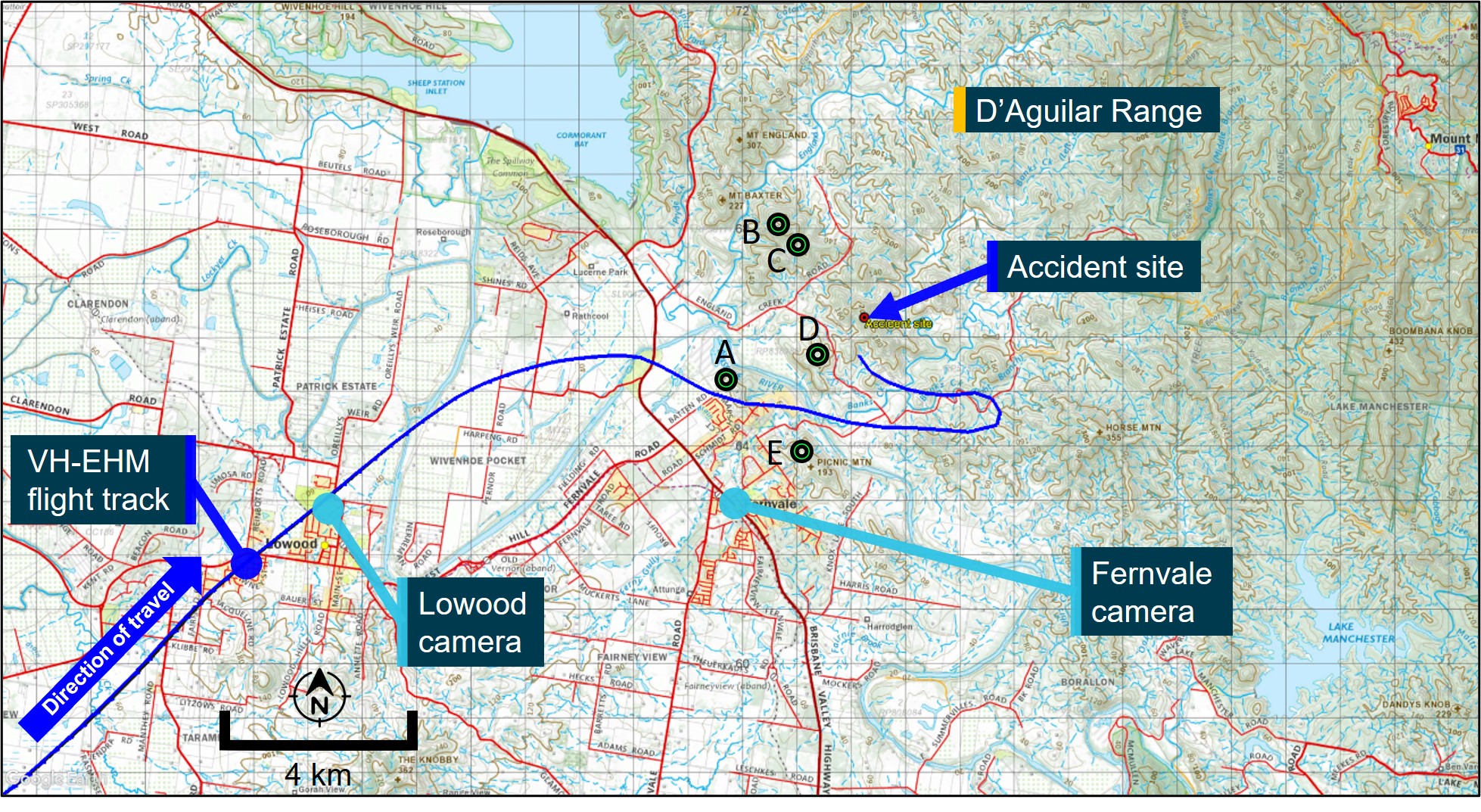
At about 0955, the aircraft passed to the east of Gatton Airpark before tracking towards Lowood. After passing overhead Lowood, VH-EHM descended to about 700 ft (500 ft AGL) before turning east towards Fernvale and the D’Aguilar Range. The flight data showed that at 1005, the aircraft passed over a hill at a height of about 200 ft AGL, before climbing to 900 ft (700 ft AGL).
After passing Fernvale, the flight progressed down a valley before completing another 180° turn while climbing to 1,200 ft (1,000 ft AGL). After completing the turn, the aircraft was then descended to 800 ft (600 ft AGL) before turning right, back towards the D’Aguilar Range (Figure 3) and towards observed low cloud. During this turn, at 1007, the aircraft impacted terrain at an elevation of about 650 ft. The aircraft was destroyed, and the occupants were fatally injured.
Figure 3: Final flight track segment and accident site
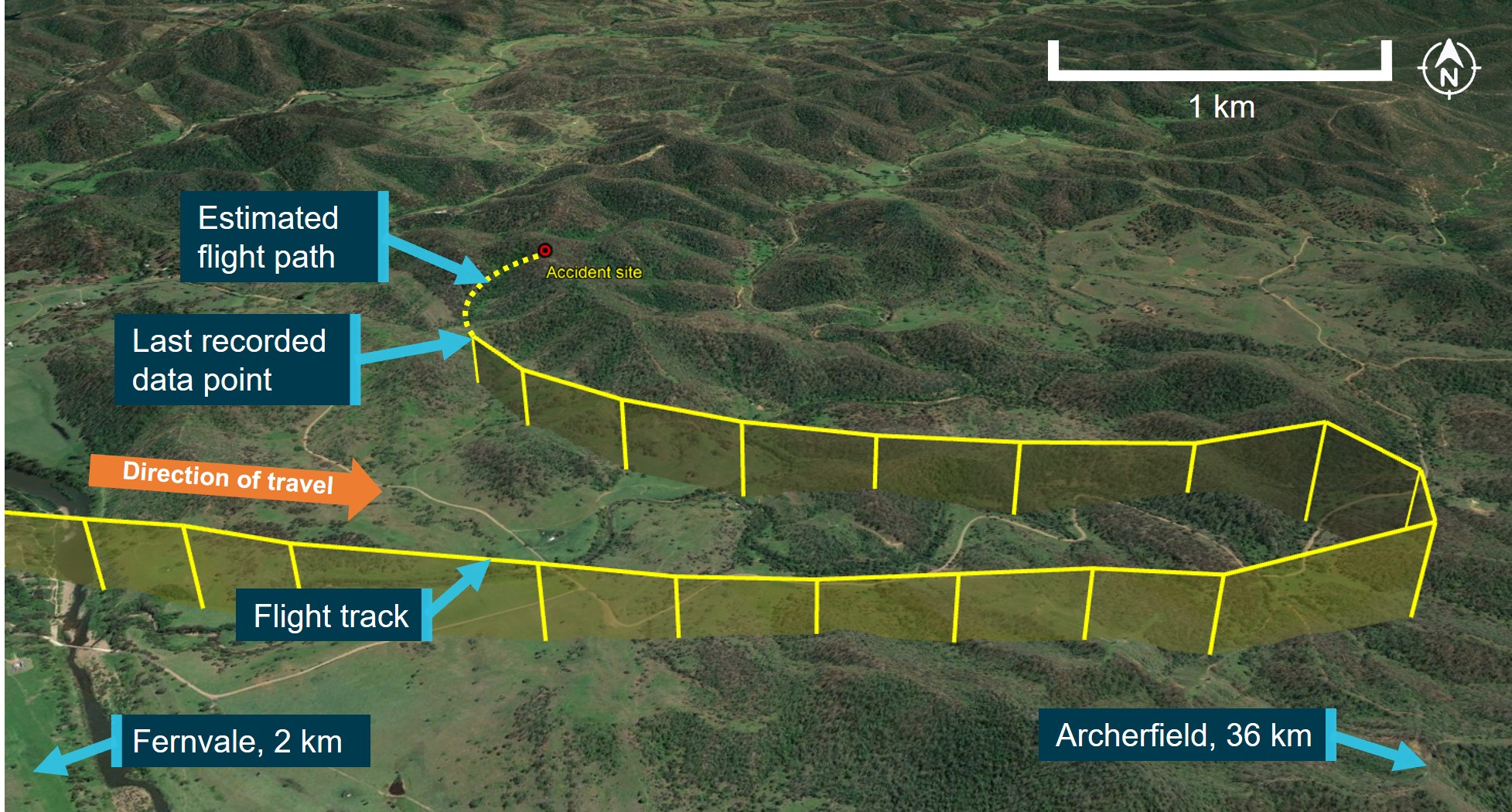
Source: Google Earth and OzRunways, annotated by ATSB
Context
Pilot information
Qualifications and experience
The pilot held valid aeroplane and helicopter commercial pilot licences first issued in 1986 and 1990 respectively. The pilot’s last aeroplane flight review was conducted in March 2021 (valid until March 2023) and an annual operator proficiency check was last completed in March 2022 (also valid until March 2023). The pilot obtained a multi-engine command instrument rating in 1992, which was renewed 8 times,[5] with the last renewal completed in October 2002 (valid until October 2003). The pilot also held a helicopter night VFR rating that expired in May 2021, a helicopter low‑level rating,[6] and had completed a flight review for this rating in February 2022 (valid until February 2024).
The pilot first obtained their private pilot licences (aeroplane and helicopter) in 1976 and 1985 respectively and had accumulated experience in both fixed and rotary wing operations. At the time of the accident flight, the pilot had accumulated about 13,900 hours of aeronautical experience with over 12,000 hours in helicopters and over 1,000 hours in aeroplanes, of which about 470 hours were in command of the Cessna R182.
The pilot had about 96 hours of instrument flying experience and about 85 hours of night experience, with the last night flight conducted in April 2018.
The pilot had operated VH-EHM for 32.7 hours in the 30 days before the accident, which included several return flights from Archerfield to Lighthouse.
The pilot had also conducted aerial firefighting tasks throughout their aviation career and in June 2018 reported the following flight hours for different activities and environments:
- air attack supervision, reconnaissance, and firebombing – about 200 hours
- agricultural mustering[7] – 1,500 hours
- low level flying – over 300 hours
- mountainous terrain – 500 hours.
Recent history
The pilot’s activities in the week before the accident, and on the day of the accident, were reported as being normal. The pilot’s next of kin stated that the pilot had been sleeping well with about 8–9 hours of sleep obtained each night. Other witnesses stated that the pilot was ‘very fit and healthy’ and not suffering any unusual personal or professional stress.
The day before the accident, the pilot woke at about 0530 and left for Archerfield Airport at about 0600. The pilot and passengers departed Archerfield in VH-EHM at 1055 and arrived at Lighthouse at about 1230. The pilot spoke to next of kin over the phone a few times during the day and had dinner at about 1800. The pilot sent a text message at 1945 indicating they were going to bed, however they also responded to an email at 2130. The next morning, a witness at Lighthouse did not notice anything abnormal during their interaction with the pilot before take-off at 0715. The pilot made and received some phone calls during the accident flight, including one after departing Dalby. The people who spoke to the pilot during the flight reported that they did not notice anything unusual or abnormal during these conversations.
The ATSB found no evidence to indicate that the pilot was experiencing a level of fatigue known to have an effect on performance.
Medical information
The pilot held a Class 1 aviation medical certificate, valid until October 2022. There were no indications of any significant medical problems in the pilot’s aviation medical records.
A post-mortem examination and toxicological analysis indicated no evidence of any pre-existing medical condition that could have contributed to the accident. The pilot’s toxicology report identified that carbon monoxide was present in the pilot’s system, but at a low level that was highly unlikely to cause impairment.
The pilot’s toxicology report also identified the presence of a medication in their system that was not documented on the medical examination questionnaires completed as part of their annual medical certificate renewals. This medication required approval for use by a designated aviation medical examiner (DAME) or by the Civil Aviation Safety Authority (CASA). The approval process required a 1-day ground trial of the medication, during which the pilot’s response to the medication would be assessed. The pilot was first prescribed this medication in 2019 by their DAME (who was also their general practitioner), who recalled that they likely advised the pilot to monitor for any symptoms or side effects. The DAME was unaware at that time that the medication required a ground trial and there was no evidence that this trial was conducted. The medication was not used on an on-going basis but was prescribed for a second time by the DAME in 2021.
The potential side effects of the medication were changes to colour vision, low blood pressure, dizziness, and blurred vision. The medication also had the potential to interact with another documented medication that the pilot had been taking regularly since 2010, although the potential interaction between them was classified as ‘minor’ with no significant interaction indicated by clinical studies. Nevertheless, patients had to be advised of the potential for interaction and were required to contact their doctor if they experienced symptoms such as dizziness, light‑headedness, or fainting.
The DAME reported that the pilot was health conscious and forthcoming in reporting any medical symptoms and that they had not reported any side effects from the use of the medication(s).
The ATSB considers it unlikely that the pilot was experiencing any side effects from the medication during the accident flight as they had probably used the medication previously (since 2019) and had not reported any adverse effects to their DAME. However, had the pilot been experiencing some of the medication’s known symptoms before the accident, it was probably insufficient to affect the ability of the pilot to fly the aircraft because:
- the aircraft was under control during the entire flight and very likely so at the time of the accident.
- radio calls made during the flight, and video footage of the pilot from Dalby Airport, did not indicate anything abnormal with the pilot.
Therefore, it was considered unlikely that the use of the medication adversely affected their performance during the accident flight. Additionally, while the medication was not documented on the pilot’s CASA medical records, its use was approved by the pilot’s DAME.
Relationship with passengers
There were 2 passengers on board VH-EHM on the day of the accident. The pilot’s next of kin and colleagues reported that the pilot and one of the passengers were close personal friends.
That passenger’s business had utilised the services of the operator (and accident pilot) for several years, and the pilot had flown the passenger to various private properties in Queensland numerous times. The passenger and their business were the operator’s most significant client at the time of the accident and had played a key role in the operator’s growth and success.
Passenger commitments
The passenger had a work-related meeting to attend at 0900 on the morning of the accident flight, however they notified a work colleague that they would not be able to attend the meeting due to the diversion to Dalby. The passenger’s next scheduled meeting was at 1530, which they communicated that they would likely be present for.
The work colleague reported that the passenger was generally not concerned about missing meetings if they could not get there in time. The passenger received business-related phone calls while on the ground at Dalby, and during the accident flight. People who spoke with the passenger during these calls reported that they did not notice anything unusual.
The other passenger on board had been communicating with friends during the flight using internet-based phone applications. Some messages sent by this passenger mentioned the poor weather encountered, the diversion to Dalby, and that they would be late for work. This passenger also contacted their employer at 0903 to advise that they would be late for work.
Aircraft information
The Cessna R182 Skylane RG is a 4-seat, high-wing, single-engine aircraft with retractable landing gear. The accident aircraft (Figure 4) was manufactured in the United States in 1978 and first registered in Australia in 1989. The aircraft was fitted with a Lycoming O‑540 piston engine driving a 3-blade Hartzell constant speed propeller and was equipped and approved for flight under both VFR and instrument flight rules (IFR).[8] The aircraft’s fuel tanks had a total maximum capacity of about 303 L, of which 284 L was useable.
Figure 4: VH-EHM

Source: Robert Frola
The aircraft was equipped with an autopilot with lateral and vertical modes capable of maintaining altitude, airspeed, track, and wings level. The pilot’s next of kin reported that the pilot was familiar with using the autopilot, including the various modes. The aircraft’s original avionics had been upgraded to include 2 Garmin G5 electronic flight instruments, which provided redundant attitude, altitude, and airspeed information. The original mechanical altimeter and airspeed indicator had also been retained and the aircraft was also fitted with a JP Instruments FS-450, which provided fuel flow, fuel used, and fuel endurance information (Figure 5).
At the time of the accident, the aircraft had accrued about 5,858 hours of time in service. The most recent periodic maintenance inspection (100-hourly) was completed on 15 July 2022 and the aircraft had accrued about 30 hours of flight time since. There were no defects recorded on the aircraft’s current maintenance release,[9] and no scheduled maintenance was due.
The ATSB performed weight and balance calculations for the flight from Dalby based on the fuel quantity from the fuel upload, occupant and aircraft weights, and cargo weight. The calculations showed that the aircraft's take-off weight and centre of gravity were within limits.
Terrain awareness
The aircraft was fitted with a Garmin GTN 750Xi, which operated as both a radio communications unit and Global Navigation Satellite System[10] unit (Figure 5). The GTN 750Xi could operate in different modes and display a significant amount of information relating to management of the flight such as maps, airspace, and terrain.
Figure 5: VH-EHM instrument panel

Source: VH-EHM avionics maintainer, modified by ATSB
While not required to be fitted with a certified terrain awareness and warning system,[11] VH-EHM’s GTN 750Xi unit had a non-certified[12] terrain awareness function capable of predicting hazardous terrain conditions and issuing alerts. Terrain information was advisory only and could include:
- display of altitudes of terrain and obstructions relative to the aircraft’s altitude
- pop-up terrain alert messages (visual/auditory) issued when flight conditions met parameters set within the terrain system software algorithms. For example, an alert would be generated when the aircraft was above terrain during en route level flight but projected to come within 700 ft vertically of any obstacle, terrain, or powerline below or ahead of the aircraft.
The system also included a ‘terrain inhibit’ mode to deactivate the terrain alert message system.
Alerts from certified or non-certified terrain warning systems can be a nuisance or distraction to pilots when flying at altitudes below the alerting threshold of the system. In March 2023, the United States Federal Aviation Administration advised operators ‘…about the risks associated with distraction and complacency brought about by routine use of the…terrain inhibit feature…[and to] ensure operators understand the importance of having procedures and training for the use of the terrain inhibit aural warning switches associated with nuisance alerts’.[13]
The operator did not have any procedures or training on the use of the terrain awareness and warning system for the Garmin GTN 750Xi. The pilot was reported to usually have the terrain awareness system enabled unless conducting low level visual aerial firefighting operations where the terrain alerts could be a nuisance.
The ATSB was unable to establish whether the terrain awareness function was enabled or inhibited at the time of the accident. Had the terrain awareness system been enabled during the accident flight, the system’s alerting thresholds, coupled with the low-level flying, would likely have produced multiple alerts, potentially distracting the pilot. These factors would have limited the effectiveness of the terrain awareness system in preventing this accident.
Flight following system
All the operator’s aircraft, including VH-EHM, were equipped with a Spidertracks[14] unit with a dash mounted device (Figure 5). The units were fitted primarily to support contracted aerial work and the system was not normally activated for other flights. When powered on, the system entered ‘normal mode’, which would automatically record and transmit the aircraft’s position at regular intervals. A ‘Watch’ function could be manually activated by the pilot so that an alert would be sent out if communication with the aircraft was lost after 10 minutes. The pilot could also manually enable the ‘SOS’ function to signal an emergency or to alert pre‑determined personnel. When the emergency ‘SOS’ function was activated, the system was programmed to send out text messages and emails to operator personnel.
The operator did not receive any Spidertracks alerts from VH-EHM during the accident flight.
Certificate of airworthiness
The aircraft’s certificate of airworthiness (CoA) was issued in 1989 when it was registered VH‑HZU. After purchasing the aircraft in late 2019, the operator requested a change of registration to VH‑EHM, which was approved by CASA in January 2020, effective from 7 February 2020. The CASA approval noted that the aircraft could not be operated beyond 7 February 2020, unless a new CoA bearing the new registration mark was issued.
An application and relevant aircraft documentation was required to be submitted by the operator to CASA for the issue of the new CoA. However, neither the operator, nor CASA possessed any records to indicate that the application for the new CoA had been submitted or that the new CoA was issued. The original CoA was found in the on-site wreckage and showed the old registration mark (VH‑HZU) amended by pen to reflect the new registration mark (VH-EHM).
Terrain
The flight’s planned track toward Archerfield Airport took the aircraft from the low-lying plains of inland Queensland across an area of the Great Dividing Range to the west of Brisbane. Elevations within the range were generally between 1,500–2,000 ft AMSL, with numerous peaks between 2,000–2,700 ft (Figure 6).
Figure 6: Visual navigation chart extract showing terrain along the flight path
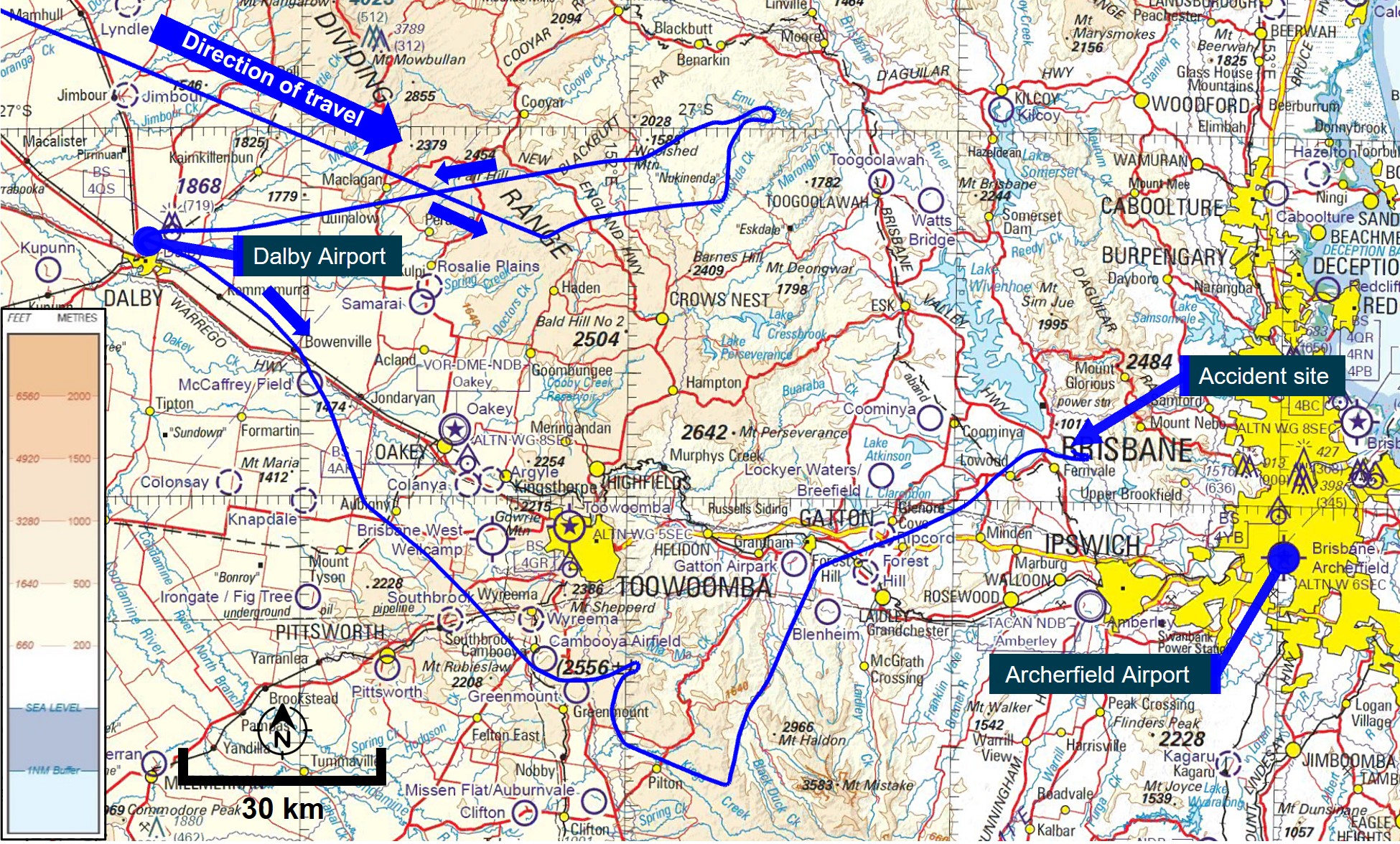
Source: Airservices Australia and OzRunways, modified and annotated by ATSB
Meteorological information
Pilot weather requests
CASA regulations[15] required the pilot to review weather forecasts and reports, within 1 hour of commencing a flight, covering the route to be flown, the departure aerodrome, and the planned destination aerodrome. If an authorised weather forecast/report was not available, and the weather conditions at the departure aerodrome would permit the aircraft to return and land safely within 1 hour of take-off, the pilot could take-off without reviewing the weather. However, they were required to obtain the relevant weather information within 30 minutes of take-off or return to the departure aerodrome. The available evidence indicated that the relevant weather forecast information would have been available to the pilot while at Dalby via the internet, or by radio from Brisbane air traffic control.
Data from Airservices Australia indicated that the pilot logged in to the National Aeronautical Information Processing System (NAIPS)[16] 3 times in the 24-hour period before the accident. These were recorded on 29 August 2022 at 0708 and 0709 (shortly before departing Lighthouse), and 0925 (about 13 minutes after departing Dalby).
The data accessed by the pilot in NAIPS included Terminal Area Forecast (TAF)[17] and METAR[18] for aerodromes relevant to the flight (Archerfield, Amberley and Toowoomba). Weather products, such as the graphical area forecast (GAF), and grid point wind and temperature, could also be viewed by the pilot, but access to these were not logged by NAIPS. Therefore, the investigation could not determine whether the pilot reviewed that information.
Forecast
Departure from Lighthouse
Two GAFs[19] issued by the Bureau of Meteorology (BoM) at 0225 on 29 August covered the planned direct route from Lighthouse to Archerfield and were valid from 0300–1500.
The weather forecast from Lighthouse towards the Great Dividing Range was generally suitable for VFR flight. However, from the Great Dividing Range to Archerfield, the forecast included broken[20] stratus cloud from 1,500 ft to 2,500 ft (becoming scattered from 1200), scattered cumulus cloud between 2,500 ft and 6,000 ft, and broken stratocumulus cloud from 5,000 ft to 7,000 ft. Visibility below the cloud layer was greater than 10 km.
Moderate isolated showers of rain were expected to reduce visibility to less than 3,000 m in broken stratus cloud between 1,000 ft and 2,500 ft, and in broken cumulus from 2,500 ft to 8,000 ft. The forecast predicted isolated fog over land areas which would reduce visibility to less than 300 m and was expected to dissipate after 0900. Isolated smoke below 3,000 ft was also forecast with associated reduced visibility of 4,000 m and extending up to 4,000 ft after 0900.
TAFs were also issued for relevant aerodromes along the planned route. Toowoomba had forecast broken cloud at 200 ft AGL (2,303 ft AMSL), mist with 2,000 m visibility, and a 40% probability of fog with 400 m visibility. Amberley had forecast light showers of rain, scattered cloud at 2,000 ft AGL (2,091 ft AMSL), broken at 4,000 ft AGL (4,091 ft AMSL), and greater than 10 km visibility below the cloud layer. Archerfield had forecast light showers of rain, few cloud at 2,000 ft AGL (2,065 ft AMSL), broken at 3,500 ft AGL (3,565 ft AMSL), and greater than 10 km visibility below the cloud layer.
The grid point wind and temperature chart for the region issued at 0359 and valid from 0700–1000 forecast:
- easterly winds between 9–13 kt at 1,000 ft, with temperatures of 12–14 °C
- easterly winds between 13–21 kt at 2,000 ft, with temperatures of 11–13 °C
- north-easterly winds between 8–20 kt at 5,000 ft, with temperatures of 7–10 °C.
Departure from Dalby
An updated GAF was issued at 0819 valid for the period from 0900–1500 with some differences to the previous forecast.
The updated forecast predicted that the previously forecast broken stratus cloud from 1,500 ft to 2,500 ft would reduce to scattered at 1100 and then dissipate by 1200, with broken cumulus and stratocumulus cloud between 3,000 ft and 7,000 ft. Visibility remained greater than 10 km below the cloud layer. The previously forecast moderate isolated showers of rain continued, as did the isolated smoke which extended up to 6,000 ft with an increased visibility of 6,000 m.
An amended TAF was also issued for Amberley at 0851, which included the same rain, cloud, and visibility forecast as the previous TAF but with an INTER[21] period between 0900 and 1100 where visibility reduced to 6,000 m in light showers of rain, with cloud broken at 1,500 ft AGL (1,591 ft AMSL). The Archerfield TAF was also amended at 0831 to include scattered cloud now forecast at 1,500 ft AGL (1,565 ft AMSL), broken at 3,000 ft AGL (3,065 ft AMSL), and an INTER period between 0900 and 1000 where visibility reduced to 4,000 m in moderate showers of rain.
The above forecasts were available when the aircraft was on the ground at Dalby and also when the pilot requested the weather at 0925 – 13 minutes after take-off. At this time, an amended TAF issued at 0914 (after departure from Dalby) was also available for Toowoomba which forecast broken cloud at 100 ft AGL (2,303 ft AMSL), and fog with 300 m visibility.
Observations
The following cloud and visibility observations were recorded or derived at weather stations along the aircraft’s flight path (Figure 7).
Table 1: Cloud and visibility observations
| Time | Location | Cloud base | Visibility (m) |
| 0900 | Dalby | 2,500 ft AMSL (2,500 ft AGL) [1] | - [2] |
| 0930 | Oakey | 2,531 ft AMSL (1,200 ft AGL) | >10 km |
| 0930 | Toowoomba | 2,203 ft AMSL (100 ft AGL) | 150 m |
| 1000 | Gatton | 1,542 ft AMSL (1,250 ft AGL) | - |
| 1000 | Amberley | 1,491 ft AMSL (1,400 ft AGL) | >10 km |
| 1000 | Beaudesert | 1,657 ft AMSL (1,500 ft AGL) | - |
| 1000 | Greenbank | 636 ft AMSL (500 ft AGL) | - |
| 1000 | Archerfield | 1,965 ft AMSL (1,900 ft AGL) | >10 km |
| 1022 | Amberley | 791 ft AMSL (700 ft AGL) | 4,000 |
[1] The automatic weather stations at Dalby, Gatton, Beaudesert and Greenbank did not have a ceilometer to record cloud base. The cloud base was estimated from the temperature‑dewpoint spread. Dewpoint is the temperature at which water vapour in the air starts to condense as the air cools. It is used, among other things, to monitor the risk of aircraft carburettor icing or the likelihood of fog.
[2] The automatic weather stations at Dalby, Gatton, Beaudesert and Greenbank did not have a visibility meter.
Figure 7: Weather station locations and flight track
Source: Google Earth and Bureau of Meteorology, annotated by ATSB
Video camera footage
Surveillance video cameras from Lowood and Fernvale provided information on the weather around the time of the accident. The field of view of each camera was determined (Figure 8), alongside identifiable mountain peaks (labels A to E).
Figure 8: Map showing camera field of views, identifiable points (A to E), and flight track
Source: Google Earth and Geoscience Australia, modified and annotated by ATSB
The surveillance video camera from Lowood, located about 10.5 km west-south-west of the accident site, captured the aircraft flying overhead below a low-level cloud layer about 4 minutes before the accident. No abnormal engine or propeller sounds were noted. A mountain peak (A) about 7.8 km from the camera location was just visible (Figure 9).
Figure 9: Image from Lowood towards D’Aguilar Range at the time of flyover

Source: Lowood Golf Course, modified and annotated by ATSB
Another surveillance video camera from Fernvale, located about 4.2 km south-west of the accident site, provided video observations of the weather conditions surrounding the accident site. An exemplar image from the video is provided to show identifiable peaks of the D’Aguilar Range and their elevations in clear conditions (Figure 10).
Figure 10: Image from Fernvale showing the D’Aguilar Range in clear conditions
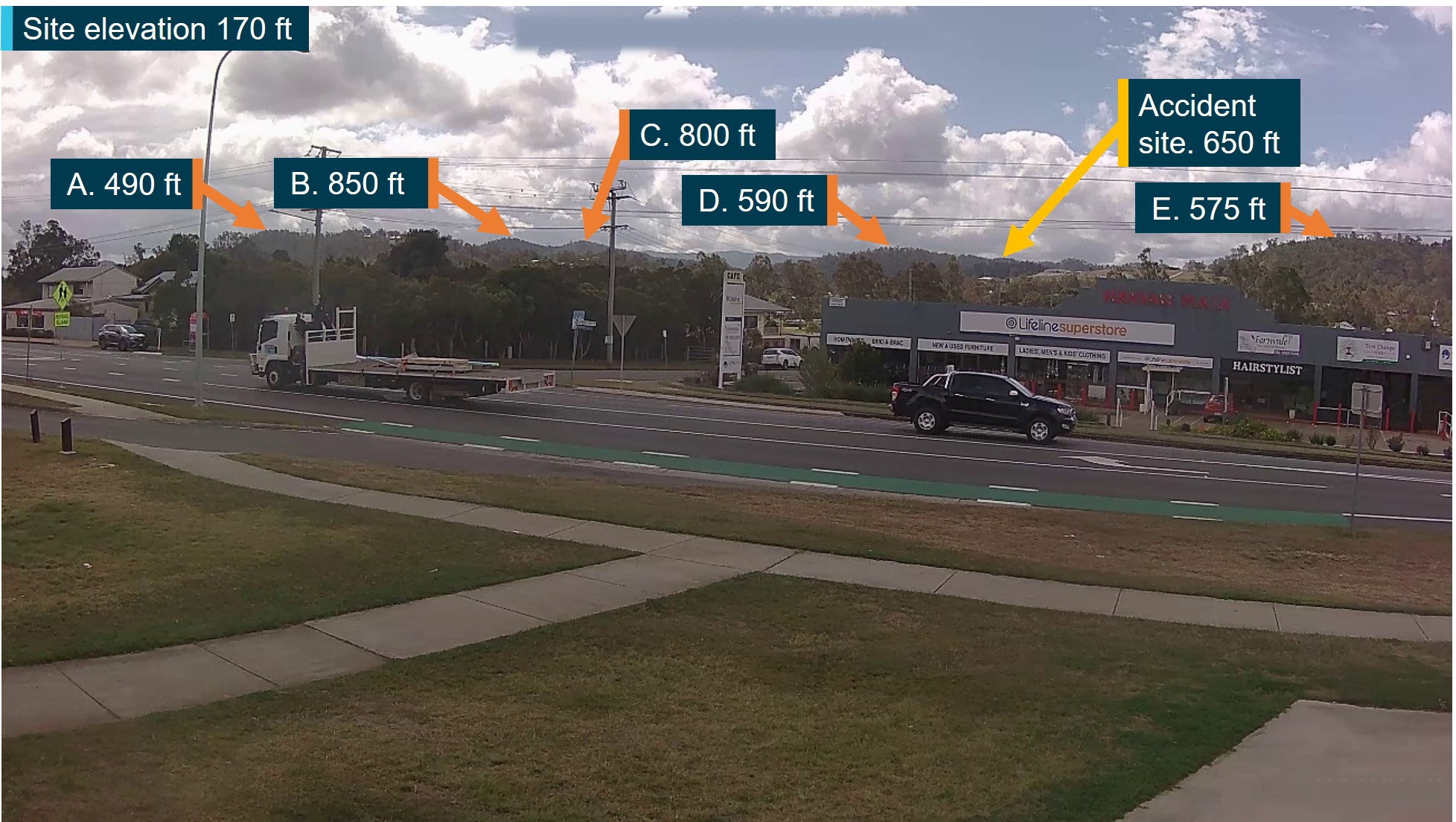
All heights AMSL.
Source: Fernvale Rural Fire Brigade, modified and annotated by ATSB
Video footage of the conditions around the time of the accident[22] (Figure 11) showed low level cloud over the area of the D’Aguilar Range, with mountain peaks B and C, and the accident site, obscured by cloud. The aircraft could not be seen in the footage.
Figure 11: Image from Fernvale around the time of the accident

All heights AMSL.
Source: Fernvale Rural Fire Brigade, modified and annotated by ATSB
Witness observations
Several witnesses along the aircraft’s route from Dalby to Fernvale recalled seeing the aircraft flying at low altitude below cloud. The witness closest to the accident site in Fernvale reported a low flying Cessna heading east towards the D’Aguilar Range with the wings level and undercarriage retracted. They recalled the aircraft banking left and disappearing from view due to cloud. The witness also reported heavy low cloud, light rain, and fog in the Fernvale area at the time.
Visual flight rules
CASA regulations[23] outlined that flight under the VFR could only be conducted in VMC with the criteria provided in the CASR manual of standards and the CASA Visual Flight Rules Guide.
The flight from Dalby, and the location of the accident, were in Class G (non-controlled) airspace. The following VMC were stipulated for flight under the VFR in Class G airspace at or below 3,000 ft or 1,000 ft above ground level (whichever was higher):
- clear of cloud and in sight of the ground or water
- a flight visibility of 5,000 m.
Amberley was in Class C (controlled) airspace. The following VMC were stipulated for flight under the VFR in Class C below 10,000 ft above ground level:
- 1,500 m horizontally from cloud
- 1,000 ft vertically from cloud
- a flight visibility of 5,000 m.
Archerfield was in Class D (controlled) airspace. The following VMC were stipulated for flight under the VFR in Class D (all heights):
- 600 m horizontally from cloud
- 1,000 ft vertically above cloud, 500 ft vertically below cloud
- flight visibility of 5,000 m.
Special VFR
By day, when VMC did not exist, pilots could request, and be issued, a ‘special VFR clearance’ from air traffic control responsible for a control zone (CTR) or control area (CTA). The clearance allowed for flight in a CTR, or in a CTA next to a CTR, for the purpose of entering or leaving a CTR, providing an IFR flight would not be unduly delayed. When operating under a special VFR clearance the pilot was responsible for ensuring that the:
- flight could be conducted clear of cloud
- visibility was not less than 1,600 m (for aeroplanes).
Requirements for maintaining visual conditions
VH-EHM was an IFR‑equipped aircraft and the pilot had previous instrument flying experience, although not current at the time of the accident. Additionally, passenger air transport flights conducted under CASR Part 135 in single-engine piston-powered aircraft were prohibited from operating under the IFR.[24] Despite that restriction, the aircraft was also in a radar coverage area with air traffic control support available to the pilot from either Amberley or Brisbane in the event emergency assistance due to flight in instrument meteorological conditions (IMC)[25] became necessary. The ATSB was unable to determine the extent to which compliance with the requirement to remain in VMC influenced the pilot’s decision to remain at low level, near terrain, in reduced visibility rather than climbing into cloud at higher altitudes above terrain.
The flight conduct section of the operator’s operations manual stated:
Similarly, the emergency procedures section of the operations manual stated:
Minimum height
In addition to minimum visibility and distance from cloud requirements, a pilot was also required to maintain a minimum height above the ground. Unless during take-off, landing or other approved low-flying operation, the CASR[26] detailed that a pilot in command must not fly an aeroplane over:
- a populous area or public gathering below 1,000 ft above the highest feature or obstacle within a horizontal radius of 600 m of the point on the ground or water immediately below the aeroplane
- any other area at a height lower than 500 ft above the highest feature or obstacle within a horizontal radius of 300 m of the point on the ground or water immediately below the aeroplane.
These minimum heights did not apply if it was essential, through stress of weather or any other unavoidable cause, that a lower height be maintained.
Recorded Data
Recorded data was obtained from various sources during the investigation, as follows:
- OzRunways[27] flight track data (altitude, ground speed, heading) was available for the entire flight up until about 8 seconds before the accident.
- The pilot made 3 radio broadcasts on the Dalby common traffic advisory frequency[28] during the flight — an inbound call at 0855, left base call at 0859, and a taxi/departure call at 0911. Review of this audio did not indicate anything abnormal with the flight or the pilot.
- While at Dalby, airport video footage captured the aircraft’s taxi to the refuel location, refuel, and taxi out to the runway. Once the aircraft had taxied and was stationary near the fuelling location, the pilot remained inside the cockpit for about 20 seconds before disembarking. The pilot spent the next 9 minutes refuelling the aircraft before re‑entering the cockpit, and 30 seconds later, the aircraft taxied back out to the runway.
- The aircraft made 4 significant turns during the accident flight including 2 course reversals. Based on flight data, the 2 turns around the Main Range (including a 180° course reversal) had estimated average bank angles of 35° and 39°. The 2 turns near the D’Aguilar Range (including the turn leading up to the accident) averaged 38° and 36° indicating they were made in the course of controlled flight similar to the previous turns (Figure 12).
- The aircraft was flown below 500 ft AGL[29] on several occasions during the accident flight, with the lowest being about 200 ft AGL (Figure 13). Since the terrain elevation data did not account for vegetation or structures, it was likely that there were lower vertical clearances during the flight.
- The flight track data indicated that the aircraft’s ground speed after departing Dalby was generally between 120–140 kt, about the normal cruise speed for the R182.
- Surveillance video footage from a private property in Fernvale, located about 2.3 km south‑west of the accident site, captured the sound of the aircraft as it flew over Fernvale, up to the time of impact with terrain. The sound of the engine and propeller could be heard up to the time of impact with no abnormal engine or propeller sounds noted.
Figure 12: Significant turns during flight
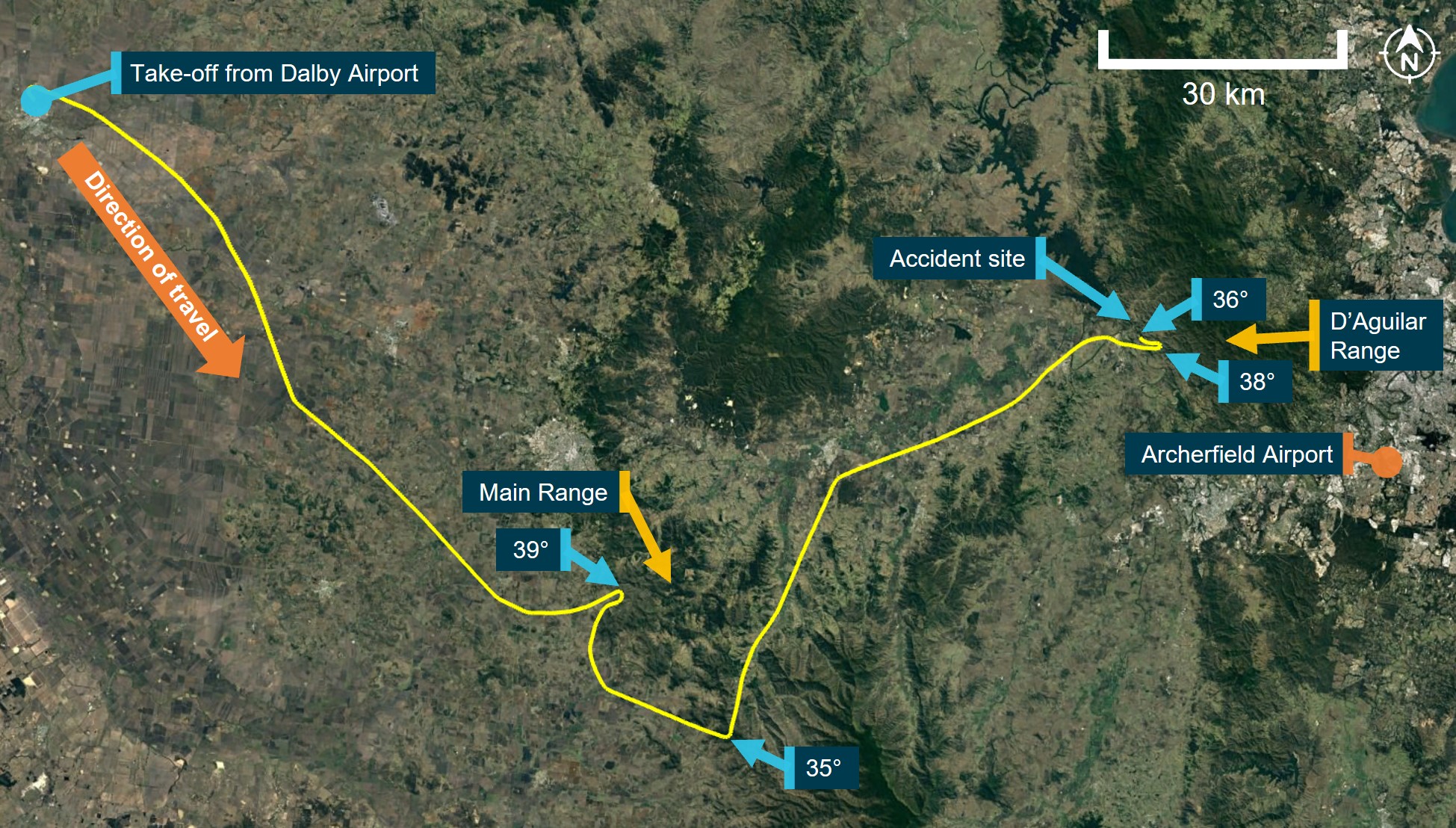
Source: Google Earth and OzRunways, annotated by ATSB
Figure 13: Low-level flight over Main Range
Source: Google Earth and OzRunways, annotated by ATSB
On-board recording devices
The aircraft was not fitted with a flight data recorder or cockpit voice recorder, nor was it required to be. There have been numerous investigations undertaken by the ATSB that would have been significantly assisted by the availability of recorded data. Such information would likely have provided additional detail about the events that led to the development of these accidents, and possibly allowed for timely identification and resolution of safety issues.
The ATSB investigation report AO-2017-118 into the collision with water involving de Havilland Canada DHC-2, in Jerusalem Bay, New South Wales in 2017 identified and directed the following safety issue to CASA:
In October 2021, the ATSB received advice from the International Civil Aviation Organization (ICAO) that the recommendation for fitment of lightweight and airborne image recorders in aircraft less than 5,700 kg used in passenger carrying operations will be referred to an ICAO Working Group for further study and consideration. In May 2023, the coronial inquest relating to the Jerusalem Bay accident recommended that CASA engage with the ATSB on the subject of mandatory fitment of on-board recording devices.
There have been several recent examples of investigations where the use of recording devices, although not required by regulations, has assisted in determining important safety factors related to the incident under investigation. A recent example was the VFR-into-IMC, loss of control, and collision with terrain involving Airbus Helicopters EC130 T2 near Mount Disappointment, Victoria in 2022 which resulted in 5 fatalities, including 4 fare-paying passengers.
The aircraft was fitted with a device that recorded video imagery and audio data from inside the aircraft cabin, as well as GPS inertial and positioning data, which assisted the investigation. Fitment of a similar device to VH-EHM may have been of value to this accident investigation to understand the specific environmental conditions faced by the pilot, insights into the pilot’s weather-related decision making, and any pilot-passenger interactions during the flight.
Site and wreckage information
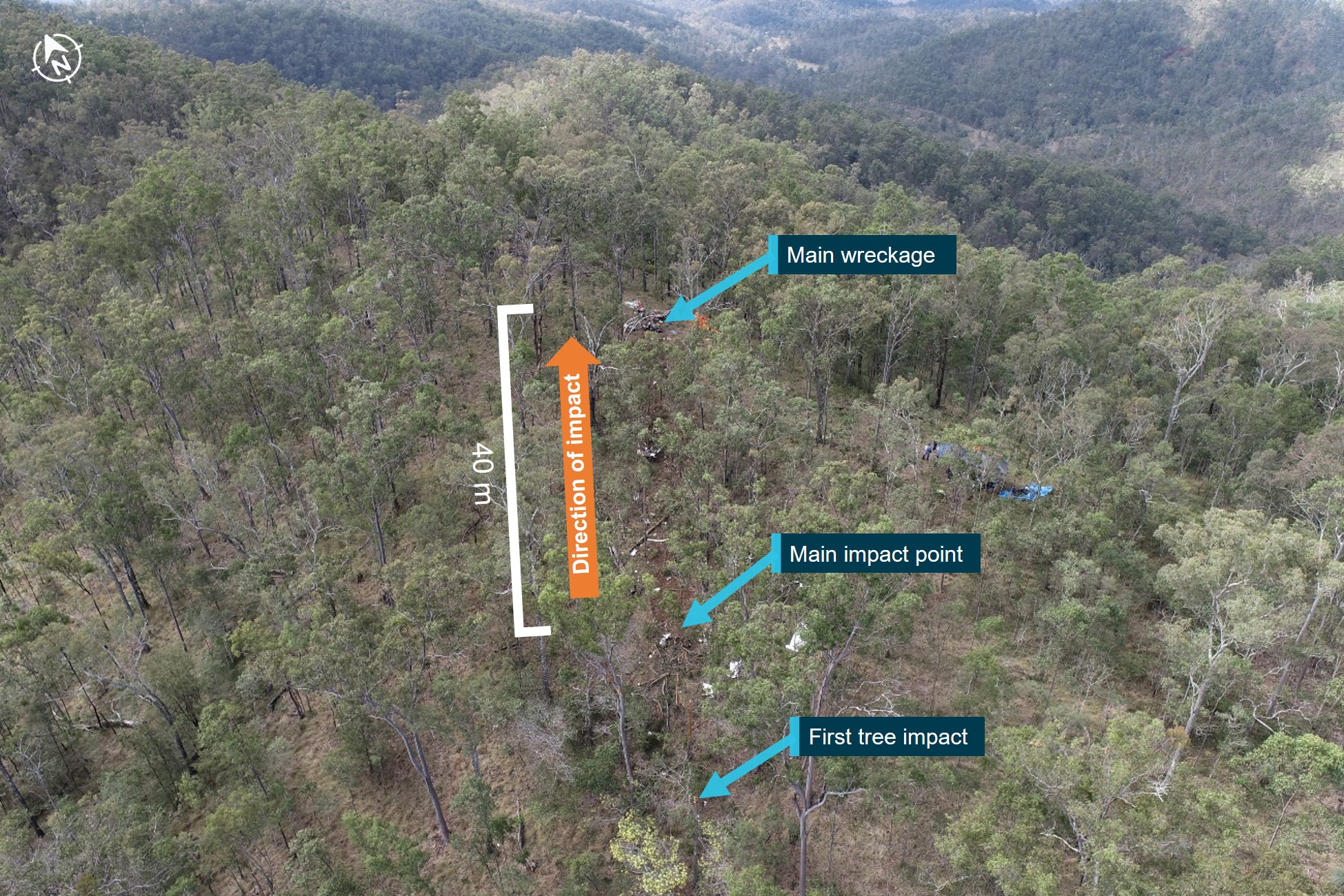
The accident site was located within the D’Aguilar Range on a steep section of mountainous terrain covered with trees (Figure 14).
Figure 14: Accident site
Source: ATSB
There were several initial impact points with numerous trees before the aircraft impacted the ground. These indicated a final flight path descent angle of about 2°, in about a 47° right bank (Figure 15).
Figure 15: Representation of the aircraft’s attitude at time of impact with trees

Source: ATSB
The aircraft impacted terrain at 650 ft AMSL, about 28 ft vertically below the top of the ridge. The wreckage trail extended about 40 m from the initial impact point to the top of the ridge where most of the wreckage, including the engine, was located. The propeller was located about 10 m forward of the main impact point.
On-site examination of the engine did not reveal any pre-impact mechanical damage, while damage to the propeller indicated that the engine was providing high power at impact. The landing gear and flaps were retracted and there was no evidence of an in-flight break-up or a pre‑existing defect with the aircraft. Due to extensive damage, the serviceability of the flight instruments, auto‑pilot, and associated systems could not be determined. The pressure altimeter subscale QNH[30] setting was appropriately set. The fuel tanks ruptured on impact, and an odour of fuel was present at the site. No fuel samples were available for recovery.
A tablet and 3 mobile phones were retrieved from the accident site, however the ATSB was unable to recover any data from these devices due to substantial damage to their internal components.
Survivability aspects
Examination of the aircraft wreckage indicated that the impact was at high speed into steep rising terrain and was not survivable.
Emergency locator transmitters
Emergency locator transmitters (ELT) and/or portable beacons are carried on aircraft so that in the event of an accident in a remote location, the aircraft wreckage and its occupants can be located quickly and efficiently by search and rescue (SAR) operations.
Under CASA regulations,[31] at the time of the accident, the aircraft was required to carry either:
- a portable ELT – an emergency position indicating radio beacon (EPIRB), or a personal locator beacon (PLB). These are handheld and usually require manual activation.
- an automatic ELT – usually mounted to the airframe and activated automatically during a crash, typically by a g-force[32] activated switch.
A review of the available maintenance documentation identified some inconsistencies regarding the aircraft’s ELT carriage requirements. As part of the aircraft’s maintenance schedule, the automatic ELT’s battery was periodically inspected by the avionics provider and was last replaced in 2019, with replacement due in 2024. The battery condition was last inspected by the avionics provider in July 2022 and was found to be serviceable. However, the aircraft’s maintenance organisation had annotated the aircraft’s current maintenance release to require the carriage of a portable ELT for flight.
The annotation for carriage of a portable ELT first appeared in a maintenance release in March 2020. Of the following 9 maintenance releases, the portable ELT annotation only appeared on 4, with one of those entries crossed out and signed by the maintainer indicating that it was likely annotated in error. The operator similarly understood the annotations on the maintenance releases requiring carriage of a portable ELT to be incorrect as the aircraft was fitted with an automatic ELT and that the pilot had previously spoken to the maintenance organisation to correct this.
During the on-site investigation, an automatic ELT and its antenna were observed to be physically fitted to the aircraft, but its serviceability and whether it was in the armed position was not determined. There were no signals received from the automatic ELT at the time of the accident and no portable ELT (PLB or EPIRB) was able to be located at the accident site.
Data from a 2013 ATSB research report indicated that ELTs function as intended in about 40% to 60% of accidents in which their activation was expected. Various factors can affect activation such as flat batteries, incorrect installation, not arming the ELT, lack of fire protection, and impact damage. The ATSB could not determine why the ELT did not function in this accident.
Flight notification
Requirements
Regulations[33] required pilots conducting VFR air transport flights to follow one of the following flight notification processes:
- submit a flight plan to Airservices Australia
- nominate a SARTIME[34] for arrival to Airservices Australia
- leave a flight note[35] with a ‘responsible person’.
A ‘responsible person’ was required to meet the following requirements:
- be over the age of 18 years
- have access to at least 2 operative and appropriate means of communicating with SAR (for example, 2 telephones)
- satisfy the pilot in command that the person:
- knows how to contact the Joint Rescue Coordination Centre (JRCC)
- will immediately do so if the pilot in command’s flight is overdue.
The operator’s procedures required that a flight notification be submitted via electronic, verbal or written means for all air transport flights. If the notification was not submitted to Airservices Australia, then a SAR form was to be completed and provided to the operator or a client (passenger) representative who was to be briefed on the SAR procedure.
The SAR form included information such as the route, SARTIME, and a ‘Next Call’ time. Pilots were required to contact the person holding the SAR form by the ‘Next Call’ time or by the SARTIME. If no contact was made within 15 minutes of these times, the person holding the SAR form would contact the operator’s head of flying operations (or their delegate) and the relevant procedures from the operator’s emergency response plan would be initiated, which included contacting JRCC after 30 minutes.
VH-EHM’s operator advised that the pilot would usually either leave the flight notification with the operator’s line pilot if they were on duty, or with a family member who was not associated with the operator. The line pilot was not on duty on the day of the accident.
Accident flight
The aircraft departed Lighthouse at 0715 on 29 August 2022. About 30 minutes after departing, the pilot contacted a family member and advised them to expect their arrival ‘late morning’. The family member was expecting the pilot to arrive at Archerfield between 1030 and 1100, and to receive a call from the pilot upon landing. They stated that they were not provided with any information about what actions to take if the aircraft became overdue.
The family member attempted to contact the pilot on several occasions between 1120 (one hour and 13 minutes after the accident) and 1240 but was unsuccessful. They subsequently raised concern about the flight by notifying the operator via email at 1309 that they were unable to contact the pilot. The operator then attempted unsuccessfully to contact the pilot, and subsequently checked publicly available ADS-B[36] data to check the aircraft’s last recorded position, which was over the Lowood Golf Club. The operator then made several calls to individuals at various nearby locations to see whether the aircraft had landed somewhere other than Archerfield.
At 1331, the operator notified Lowood police and at 1342, arranged for a helicopter from another Archerfield based operator to search for the missing aircraft near the last recorded location. At 1344, the operator notified Airservices Australia who coordinated a SAR effort with the JRCC.
At about 1427 (4 hours and 20 minutes after the accident), the helicopter arranged by the operator departed Archerfield and located the wreckage shortly after. The helicopter was landed near the wreckage and its pilot proceeded to the site on foot, reporting back to the operator that none of the occupants had survived. Shortly after, a SAR helicopter arrived at the site with paramedics confirming the previous report.
Operational information
Fuel planning
The CASR[37] prescribed the fuel requirements for air transport flights conducted under CASR Part 135 which were also reflected in the operator’s operations manual. At a minimum, the aircraft had to carry the following amounts of usable fuel before a flight commenced:
- taxi fuel – fuel used before take-off
- trip fuel – fuel for take-off, climb, cruise, descent, and landing
- contingency fuel – 10% of trip fuel for a piston engine aeroplane
- final reserve fuel – 45 minutes flight time for a piston engine aeroplane (between 24–30 L for VH‑EHM)[38]
- if required – destination alternate fuel, holding fuel, and additional fuel.
Also, the effect of operational conditions such as the aircraft’s weight, and relevant meteorological reports and forecasts had to be considered during fuel planning.
To determine the required quantity of usable fuel for a flight, fuel consumption data from either the operator’s fuel consumption monitoring system or aircraft manufacturer data could be used. Operators conducting air transport flights under CASR Part 135 were required to complete a ‘journey log’ before and after each flight and include information such as fuel on-board before the flight and after landing. The operator required the quantity of fuel on-board before each flight be determined using 2 independent means.
Fuel records were available for the operator’s helicopters, but no fuel records could be found for VH-EHM. Fuel was available at Lighthouse and was primarily used for filling up helicopters involved in cattle mustering. VH-EHM could be re-fuelled at the property but required some additional effort to set up the fuel drum and pump for fuel delivery. Prior to departure on the morning of the accident flight, VH-EHM was not refuelled at Lighthouse. No information was available about the pilot’s fuel planning for the flight from Lighthouse to Archerfield.
Fuel calculations
After departing Lighthouse and encountering weather on the range, the pilot diverted to Dalby to refuel. An assessment was undertaken to estimate the quantity of fuel on-board the aircraft when it departed Lighthouse, and if that quantity was sufficient for the intended flight to Archerfield (see Appendix – Fuel calculations).
Depending on the fuel flow data used for the calculations, the aircraft was estimated to have had between 100–125 L of useable fuel on‑board (of a total useable capacity of 284 L) before departing Lighthouse. Calculations showed that the aircraft had sufficient fuel on-board to complete the flight to Archerfield (taxi fuel and trip fuel) in ideal weather conditions but was required to land with between 31–39 L of useable fuel (contingency fuel and final reserve fuel). As a result, it was estimated that the aircraft would have landed at Archerfield with between 4–13 L below the minimum required useable fuel in ideal weather conditions.
In addition, even had this minimum required fuel been on-board, it would have been insufficient fuel to account for a weather-related diversion. Weight and balance calculations showed that the aircraft fuel tanks could have been filled completely with the available fuel at Lighthouse while remaining below the allowable maximum take-off weight.
Airspace
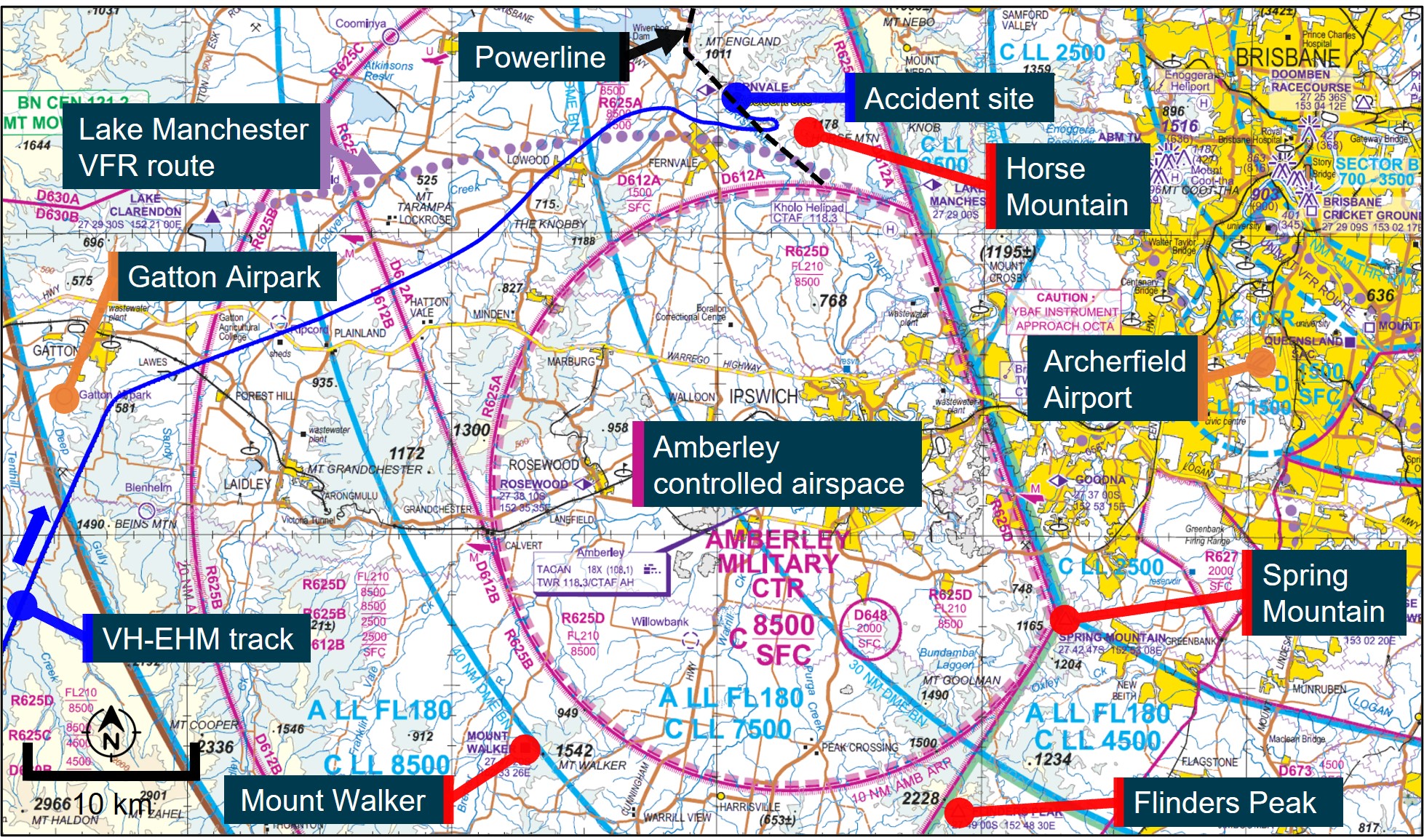
The Amberley military control zone extended from ground level up to an altitude of 8,500 ft surrounding Royal Australian Air Force Base Amberley (Figure 16). NOTAMs[39] applicable on the day of the accident established that the Amberley controlled airspace was active from 0800 to 2300 and required an airways clearance to transit. Transit through the Amberley control zone provided the lowest terrain elevations for flights between Archerfield and areas west of the controlled airspace.
In March 2021, Amberley air traffic control notified Archerfield operators that pilots needed to plan flights around the Amberley control zone and should not plan for, or expect to receive, a clearance when departing from or arriving into Archerfield. This was due to an increase in the volume and complexity of traffic in the area, in combination with Brisbane airspace changes.
Figure 16: Amberley control area
Source: Airservices Australia, annotated by ATSB
Flights bound for Archerfield from the west of the Amberley CTR generally tracked around Amberley controlled airspace, either from the north using the Lake Manchester VFR route or from the south using the points of Mount Walker, Flinders Peak, and Spring Mountain (Figure 16). These routes enabled pilots to fly visually under or around restricted airspace without requiring an airways clearance from Amberley air traffic control.
Lake Manchester VFR route
The Lake Manchester VFR route was a corridor under the restricted airspace from ground level to 1,500 ft AMSL (less than 1,000 ft AGL in some sections). The lateral separation from Amberley controlled airspace and elevated terrain reduced to about 1 km at some points, and there was a powerline that passed under a section of the route. Flying south via the mountain peaks required maintaining the aircraft below the 2,500 ft AMSL restriction (associated with the R612B restricted airspace), and above elevated terrain exceeding 600 ft AMSL.
The pilot’s next of kin and a former colleague reported that the pilot had flown the Lake Manchester VFR route, and the route south of Amberley airspace, numerous times in helicopters and aeroplanes and was very familiar with the terrain. The former colleague also reported that the pilot did not recommend using the Lake Manchester VFR route if the weather was poor around the D’Aguilar Range, due to the rising terrain and limited separation from controlled airspace. Transit through the low-lying terrain of the Amberley control zone was preferred in those circumstances.
The operator reported similar concerns associated with the use of the Class G airspace (uncontrolled) surrounding Amberley and the Lake Manchester VFR route, particularly in marginal weather conditions due to the:
- rising terrain to the north and east of the Lake Manchester VFR route
- limited lateral separation between controlled airspace and rising terrain in some areas of the route
- need for aircraft to remain below 1,500 ft while also remaining above the terrain and power lines, with potential for east and west bound traffic
- potential for the range to the north of the route to create problematic weather
- occurrence of regular airspace infringements in the area.
CASA Office of Airspace Regulation
The CASA Office of Airspace Regulation (OAR) advised that VFR routes, which were usually established following feedback from local airspace users, were only to be used in VMC and generally followed identifiable ground features to ease visual navigation. The OAR further stated that in non‑controlled airspace, pilots were responsible for aircraft separation, terrain clearance, and being appropriately briefed for the flight.
Aeronautical studies and airspace reviews undertaken by the OAR generally involved consultation with the aviation community as well as review of ATSB and Airservices Australia incident data. While there were several reported airspace infringements into the Amberley controlled airspace, in the period from January 2020 to May 2023 there were no CASA aviation safety incident reports recorded relating to the Lake Manchester VFR route, except for the accident involving VH-EHM.
A review of data by the Royal Australian Air Force concluded that infringements of the Amberley controlled airspace were primarily due to pilots not reviewing NOTAMs and an over reliance on electronic flight bags, which in some instances did not accurately display the activity status of military restricted areas.
The OAR considered that the risk associated with defence-related aircraft movements within the Amberley airspace and the segregation of these activities with civil aviation activities was appropriate. The OAR also noted that there was ongoing work by CASA, the Australian Defence Force, and Airservices Australia to reduce airspace infringements by educating pilots on the use of military airspace, including via the publication of guidance material. For example, an infringement from 2017 involved a VFR flight where the pilot was tracking along the Lake Manchester VFR route and requested clearance to transit the Amberley control zone. The clearance was denied by Amberley air traffic control due to other traffic in the area. Unknown to Amberley ATC, the pilot was deviating around weather and subsequently inadvertently entered the Amberley control zone. The Royal Australian Air Force advised pilots facing similar circumstances:
Conclusion
The ATSB concluded that there was insufficient evidence to indicate that the structure of the Amberley controlled airspace in relation to the Lake Manchester VFR route contributed to this accident. While acknowledging the narrow lateral and vertical separation between terrain and controlled airspace on the route, it was a published area of airspace intended for use only in VMC.
Furthermore, the route was known to the pilot as being an area to avoid in adverse weather, which existed at the time of the accident, when safety margins would be greatly reduced. In the event of encountering adverse weather along the route making it unsuitable, there remained an alternative in‑flight option of requesting an airways clearance to enter Amberley airspace to either land or transit.
The NAIPS login records indicated that the pilot requested NOTAM information during each NAIPS request and was tracking around Amberley controlled airspace towards the end of the flight. Therefore, the pilot was likely aware it was active at the time, and that it required an airways clearance to transit. However, a review of air traffic control recordings did not identify any radio communications or requests for an airways clearance between VH-EHM’s pilot and Amberley air traffic control.
A pilot previously employed by the operator between January 2021 and June 2022, reported that in their experience, requests to transit Amberley were usually denied. However, there was no information available on the accident pilot's past experience with requesting and being granted/denied Amberley transit clearance, or of their views on the 2021 Amberley notification to Archerfield operators regarding flight planning around the Amberley CTR. Therefore, the investigation was unable to determine whether these considerations influenced their decision not to request a transit clearance.
Organisational information
Executive Helicopters was an Archerfield based operator established in 2008. The pilot joined the operator as chief pilot in 2009 – later retitled head of flying operations (HOFO) – after which commercial helicopter operations commenced. Single-engine piston-powered aeroplane VFR charter[40] (air transport) operations were added to the AOC in 2020 after VH-EHM was purchased.
The operator held an Air Operator’s Certificate (AOC) issued by CASA which was valid at the time of the accident. The AOC authorised the certificate holder to operate various single-engine helicopters, as well as single-engine piston‑powered aeroplane types with a maximum take-off weight not exceeding 5,700 kg, on VFR air transport and aerial work operations.
From 2009 to 2021, the accident pilot was the only full-time pilot conducting operations under the AOC. Over this time, casual pilots were also contracted to undertake flying as required. A second full‑time pilot was employed from January 2021 to June 2022 and a third joined shortly before the accident.
At the time of the accident, the operator’s staff consisted of the HOFO (the accident pilot), one line pilot, an administrative compliance assistant, and the chief executive officer (CEO) who had been involved since the organisation was established in 2008. The accident pilot was also the head of aircraft airworthiness and maintenance control for the operator.
Safety management system
At the time of the accident, CASA regulations did not require the operator to have a safety management system (SMS).[41] However, the operator had voluntarily introduced an SMS in 2020.
ICAO defines an SMS as:
The operator’s SMS manual stated:
The SMS manual included several sources of information to aid hazard identification such as previous experience, accident investigations, audits, group discussions, and client feedback. The SMS incorporated a hazard register which included various hazards related to the operator’s flight operations, with the chief pilot being responsible for most of them. The register did not include any hazards related to the loss of visual reference, or inadvertent entry of a VFR flight into IMC.
Pilot training
As part of holding a commercial pilot licence (aeroplane), the pilot was required to complete a flight review every 2 years. The review included competencies related to knowledge of pre-flight weather assessment, maintaining situational awareness and decision making, as well as recognising and managing threats and undesired aircraft states. The review required pilots to perform basic flight manoeuvres using full instrument panel, and to recover from upset situations and unusual aircraft attitudes to straight and level flight while operating under simulated IMC. The pilot had successfully completed this review in March 2021. Biennial flight reviews for the commercial pilot licence (helicopter) could also include an instrument flying component but this was optional.
Operator proficiency checks were conducted annually and involved a ground review and flight review, as well as practical and theoretical components on emergencies. The proficiency check did not include any additional training related to instrument flying or VFR‑into‑IMC prevention and recovery, nor was such training required by CASA.
The operator also conducted annual aeronautical decision-making training based on the non‑technical skills theory within CASR Part 61 (flight crew licencing) although it was not required under CASA regulations at the time of the accident.[42] The training had a slightly different syllabus for each recurrent exercise and was intended to be self-paced, with an estimated duration of 2 hours. The subject matter was based on the CASA resource material – Safety behaviours: human factors for pilots: Resource booklet 7 Decision making. The pilot had completed the initial training in September 2020, which required reading the booklet, watching a CASA video on decision making, and completing a short multiple-choice quiz. The first recurrent training was completed in October 2021 and involved similar tasks.
Regulatory oversight
CASA’s surveillance manual outlined that the surveillance program for Authorisation Holders (AH), such as Executive Helicopters, used a systems and risk-based approach to obtain, record, and analyse results to evaluate safety performance. The scheduling of surveillance events was driven by many factors such as external intelligence, outstanding safety findings, time since the last surveillance event, and safety-related risks specific to each AH.
CASA last conducted a surveillance event on the operator in October 2018. That surveillance was classified as ‘Level 1’[43] and conducted on-site at the operator’s premises. The scope of the surveillance included a review of airworthiness assurance, crew scheduling, and flight operations. The surveillance event resulted in 3 findings regarding crew rostering, navigation logs, and operations manual document control.
The operator responded to each finding with satisfactory corrective action and CASA acquitted the 3 findings in January 2019. Another Level 1 scheduled surveillance event was planned for March 2022 but was not conducted as all CASA surveillance events were postponed due to the flight operations regulations transition.
CASA used an Authorisation Holder Performance Indicator (AHPI) tool to assist with surveillance. The AHPI tool was one of a number of factors used to determine the need for surveillance events. The AHPI tool was a questionnaire-based tool consisting of several factors and sub-factors associated with organisational characteristics and performance commonly thought to affect or relate to safety performance behaviour. The assessment would result in the AH being assigned to either category 1 (higher level surveillance focus required) or category 2 (normal surveillance level appropriate). Since January 2019, 3 AHPI assessments had been conducted on Executive Helicopters — in May 2019, May 2020, and November 2021 — with each resulting in the operator being assigned to category 2 indicating that the normal level of surveillance was appropriate.
VFR-into-IMC
Visual flight rules pilots flying into IMC (VFR-into-IMC) has been a worldwide challenge in aviation and continues to represent a significant portion of fatal accidents. VFR-into-IMC accidents usually involve either loss of control, spatial disorientation, or controlled flight into terrain. A significant number of studies have examined VFR‑into-IMC accidents, and a range of factors are usually involved, of which many are related to decision making.
Decision making
Pilot decision making is a cognitive process used to select a course of action between alternatives. Several factors, circumstances, and biases can affect decision making, including the flight objective or goal, and the pilot’s knowledge, experience, and training (Endsley, 1995).
The CASA Resource booklet 7 Decision making contained the following:
Air transport operations in smaller aeroplanes, such as that conducted by the operator, do not have the same sophistication of systems, processes, and procedures as larger airlines (Harris and others, 2022):
Recent research into general aviation pilots involved in the entry of VFR flights into IMC, noted a distinction between intentional and unintentional VFR-into-IMC (Stanton, 2022), which was normally not considered within previous research. Unintentional or inadvertent VFR‑into‑IMC flight were those where there was no deliberate intention to do so and occurred ‘…due to poor situational awareness or poor interpretation of weather cues whilst operating in a dynamic, sometimes subtly changing environment (Orasanu et al., 2001)’.
Intentional flights were those where the pilots were:
A systematic review of the available research into VFR-into-IMC accidents, with a focus on commercial pilots and operations where there was intentional continuation of flight into unsuitable conditions, found the following 2 overarching themes, each with associated personal, social and organisational factors (Harris and others, 2022):
- continuation influence
- acceptance of risk/normalisation of deviance.
Continuation influence
Research has shown that pilots often continue VFR flights despite deteriorating cues associated with adverse weather conditions. This ‘plan continuation bias’ is an internal pressure or desire to get to the destination and could result from various factors such as previous encounters with IMC or an inability to detect cues of gradually deteriorating conditions while getting closer to the destination.
The ATSB found that the chances of a VFR-into-IMC encounter for general aviation pilots increased until they reached a maximum during the final 20% of the flight distance (ATSB, 2005). This pattern suggested an increasing tendency on the part of pilots to ‘press on’ as they near their goal with a decreasing probability of turning back or diverting as the destination drew closer.
Practical reasons can also play a role, with pilots continuing because the alternative places them in a location with minimal facilities (accommodation, food, communications). Also, the way alternative options are framed can also have an impact (Harris and others, 2022):
The presence of passengers or customers on a flight can also directly, or indirectly, place pressure on a pilot to continue the flight, where the pilot does not want to disappoint the passenger(s) and to avoid social disapproval or failure. A review of United States general aviation aircraft accidents between 1990 and 1997 found a significantly greater percentage of VFR‑into‑IMC accident flights carried passengers on board (Goh and Wiegmann, 2001).
At the operator level, pilots can be influenced by time pressures, resource limitations or financial constraints and incentives. An organisation’s safety culture can also affect pilot motivations and decision making. For example, a safety conscious culture could lead to a pilot choosing a safe option (for example, diversion), while a pilot that fears punishment if they divert may lead them to press on into deteriorating weather.
Acceptance of risk/normalisation of deviance
Decision making under uncertainty involves the perception of risk (Harris and others, 2022). Pilots may detect deteriorating weather but perceive the risk of continuing differently based on factors such as personal experience and ability. Pilots that had lower risk perception, or were less risk averse, were more likely to have encountered adverse weather before:
These findings were supported by another recent study on VFR-into-IMC accidents, where a cycle of repeated and successful VFR-into-IMC encounters could create a pattern of deviation from the rules (Stanton, 2022):
This research also found that the perceptions pilots held about what other people, whose opinion they valued, might expect or think about conducting a VFR flight into IMC, and what these people would do in such a situation, was highly influential to forming an intention to conduct VFR flights into IMC (Stanton, 2022).
From an organisational perspective, pilots could become accustomed to risk-taking when instructed to take-off and ‘…see how bad the weather is…’ if it leads to no negative consequences (Harris and others, 2022):
Pilot decision making during the accident flight
The pilot was described as being diligent with weather-related decision making, knowledgeable and experienced with the local terrain surrounding Brisbane. The pilot’s next of kin and a former colleague reported that the pilot always had alternative options in case poor weather was encountered. On 2 separate occasions the pilot had reportedly landed after encountering poor weather, and either waited until the weather cleared, or sought a different method of travel to get to the destination. A review of the ATSB occurrence database did not identify any weather-related occurrences involving the pilot, nor did CASA hold any records of enforcement action taken against the pilot.
In the time leading up to the accident, the pilot was operating the aircraft in regions of elevated terrain at altitudes below the minimum height requirements. While the pilot had substantial experience flying at low level and in mountainous terrain, as well as previous IFR experience, the ATSB was unable to determine whether this previous experience lowered the pilot’s risk perception and influenced the decision to continue the flight.
While the pilot was also described as being very customer focused, a former colleague reported that the pilot never had any urgency to ‘get the job done’ and would not be pressured by anyone to do something they were not comfortable with. On the day of the accident, there was no evidence of schedule-related time pressure for the passengers’ return to Archerfield. Nevertheless, there was insufficient information to determine whether the pilot was under any real or perceived customer-imposed pressure, or self-induced pressure due to the presence of the passengers, to complete the flight.
From an organisational perspective, the accident pilot and the CEO were, for a significant period of time, the only personnel at Executive Helicopters with responsibility and accountability for the safe operation of aircraft. The full-time pilot who was employed by the operator from January 2021 to June 2022 described the CEO as ‘easy going’ with a friendly and open, professional and personal relationship with the accident pilot.
The CEO was not involved in the day to day flying operations of the operator but would receive regular communications from the accident pilot on these matters. The previously‑employed pilot stated that during their time with the organisation they felt 'very comfortable’ with all aspects of operations and did not experience any pressure to complete flights. Based on this information, it was considered unlikely that there was any direct or perceived organisational pressure on the pilot to continue the flight.
Intervention strategies
The commonly documented strategies to avoid entering IMC are appropriate pre-flight preparation and sound decision making. Initial instrument training required for a commercial aeroplane licence, and recurring training as part of biennial flight reviews, can also assist pilots in maintaining aircraft control in IMC and to recover to VMC. Some recent research and information on aspects related to VFR-into-IMC prevention and recovery are outlined below.
Prevention
The dangers of VFR pilots flying into IMC have been recognised for a very long time, yet VFR pilots still fly into deteriorating weather and IMC. Recent research, which applied the ‘theory of planned behaviour’[44] to intentional VFR-into-IMC flights, summarised the historical attempts at preventing these accidents (Stanton, 2022):
This research found that pilot’s ‘…beliefs related to the hazardous consequences of conducting VFR flight into IMC (i.e., behavioural beliefs) had limited influence on a pilot’s intentions’ which could explain ‘…why past attempts at intervention have been unsuccessful for so long’.
The research found that the distinction between inadvertent and intentional VFR-into-IMC was likely an important factor when considering intervention strategies:
For intentional VFR-into-IMC, the research indicated that ‘…beliefs associated with social pressures and those associated with a pilot’s perception of their skills and ability were the primary influences on behavioural intentions’. The research suggested that intervention strategies be developed by applying behaviour change theories to pilots to alter their beliefs, attitudes, and perceptions. This conclusion was also supported by other research that reviewed VFR-into-IMC from a behavioural economics[45] perspective, which also suggested more comprehensive weather training was required (O’Mahony et al., 2023). The research proposed 3 interventions to facilitate better pilot decision making in the context of VFR-into-IMC:
IMC recovery
The Cessna R182 pilot’s operating handbook[46] included an emergency procedure for inadvertently entering clouds. The procedure was to execute a standard rate 180° turn using the aircraft’s compass and clock, while maintaining altitude and airspeed.
The 180° turn may not be suitable for all IMC recovery situations and execution of this turn at low altitude has resulted in controlled flight into terrain (CFIT) accidents or a loss of control during the turn. A 2021 United States General Aviation Joint Steering Committee[47] (GAJSC) report into CFIT accidents recommended a task force be created to review IMC recovery events to ‘…make recommendations on revisiting how we teach and train the [IMC] escape response [manoeuvre] to include an initial climb before any heading change, should the data support such a change.’ An Aircraft Owners and Pilots Association (AOPA) article indicated that climbing, rather than turning, was a valid option to consider depending on the situation faced by a pilot:
Instrument training and flying, such as that conducted during flight reviews can assist in maintaining aircraft control and to recover to VMC conditions, although there are limitations to this approach (AOPA, 2022):
To resolve this limitation, the 2021 GAJSC report recommended ‘…to improve scenario-based training through the use of [available] advanced view-limiting device technology that simulates inadvertent IMC entry and/or through the use of flight simulators.’
Related Occurrences
Many similar occurrences have been summarised in the ATSB research report Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions as well as in ATSB accident reports, including AO‑2018‑078.
Safety analysis
Introduction
At 0715 local time on 29 August 2022, a Cessna R182 Skylane RG (R182), registered VH-EHM, and operated by Executive Helicopters, departed a private property (Lighthouse) north-east of Roma, Queensland for an air transport flight under visual flight rules (VFR) to Archerfield Airport, Queensland. The aircraft departed with the pilot, 2 passengers, and a passenger’s pet dog on board.
As the aircraft was crossing the elevated terrain of the Great Dividing Range, the pilot encountered forecast low cloud and reduced visibility, and was unable to find a way across that was clear of cloud. With limited fuel remaining, the pilot diverted to Dalby Airport and refuelled the aircraft before departing once again. About an hour later, the aircraft collided with terrain in the D’Aguilar Range about 36 km north-west of Archerfield. All occupants of the aircraft were fatally injured.
The ATSB did not identify any aircraft defects or anomalies that may have contributed to the accident. As such, the following analysis will examine the:
- pilot’s pre‑flight planning and decision making.
- continuation of the flight into adverse weather.
- operator’s risk management.
- search and rescue aspects.
Pre-flight planning and diversion to Dalby
Pre-flight weather assessment
While at Lighthouse, the forecast weather at the destination (Archerfield) was suitable for a VFR arrival. However, the en route forecast predicted low cloud, rain, fog and associated reduced visibility, particularly around the elevated terrain of the Great Dividing Range, with cloud down to ground level in some areas. Although the forecast predicted acceptable visibility below the cloud layers, the weather conditions around the elevated terrain of the range – which had to be crossed to reach Archerfield – were unsuitable for visual flight.
About 6 minutes before the flight departed Lighthouse, the pilot requested weather information through the National Aeronautical Information Processing System (NAIPS). This was the pilot’s first NAIPS weather request since their departure from Archerfield the previous day. The exact weather information reviewed by the pilot could not be determined, nor is it not known whether the pilot accessed other non‑approved sources of weather. Nevertheless, the information available as part of the NAIPS request was sufficient for the pilot to assess the weather en route and to inform the pilot’s pre-flight decision making. However, the minimal time between the NAIPS weather request and subsequent take-off (6 minutes), provided limited opportunity for a thorough review of the en route weather and was consistent with a strong motivation to conduct the flight despite the forecast weather conditions.
Fuel planning
Although fuel was available at Lighthouse, and there was sufficient fuel on-board to complete the flight in ideal conditions, there was insufficient fuel to account for weather-related diversions or meet contingency fuel requirements. Furthermore, depending on the fuel flow data used for the calculations, there was also insufficient final reserve fuel on-board.
The limited pre-flight planning information available meant that the investigation was unable to determine the factors considered by the pilot with respect to fuel planning prior to departure.
Flight notification and search and rescue
Civil Aviation Safety Regulations (CASR) required that, before undertaking the flight, the pilot leave details of the flight and arrival time with a ‘responsible person’ who knew when and how to contact the Joint Rescue Coordination Centre (JRCC) and would do so if the flight was overdue.
The operator's documented procedures reflected this requirement and stipulated that this ‘responsible person’ could be someone from the operator or a representative of a client onboard.
The operator reported that the pilot did not always follow this documented procedure and would sometimes provide flight details to a family member, as occurred on the accident flight. Providing the flight note to this family member was still sufficient to meet the regulatory requirement if they were aware of their obligations and expected actions. However, the investigation identified various deficiencies in relation to the pilot’s compliance with this requirement for the accident flight:
- The family member was notified about 30 minutes after departure from Lighthouse, limiting search and rescue (SAR) functions during that initial part of the flight.
- An unspecific arrival time of ‘late morning’ was provided which was not suitable for the purposes of timely SAR action.
- Although the flight diverted to Dalby, the pilot did not notify the family member when there was a change to the flight route and arrival timing.
- The pilot had not briefed the family member about the correct actions to take for an overdue flight, resulting in a delay of over 2 hours in notifying the operator that the flight was overdue. This substantially delayed the subsequent emergency SAR response and potential medical attention (in the event of a survivable accident).
The accident was non-survivable, and consequently, a timely SAR response and immediate medical aid would not have altered the outcome. However, in different circumstances, SAR notification and the carriage and use of manually activated emergency beacons would likely have played a key role in increasing the chances of post‑accident survival by facilitating rapid medical aid to treat injuries.
Departure and diversion to Dalby
While the forecast indicated that visual meteorological conditions (VMC) would probably not be maintained while transiting the elevated terrain of the Great Dividing Range, the decision to depart Lighthouse towards Archerfield was in itself reasonable. With adequate fuel on-board and escape routes planned, actual weather conditions could be assessed and managed in‑flight. However, doing so placed additional pressure on the pilot’s in‑flight decision making capabilities.
After encountering the forecast cloud, the pilot continued to manoeuvre to try to find a way through the Great Dividing Range with the aircraft’s fuel running low. The pilot then diverted to Dalby, landing with less than the required final reserve fuel. Although this may have been influenced in part by the aircraft being equipped with instrumentation capable of indicating the fuel state accurately, this indicated that the pilot’s planning before and during the flight was ineffective, and there was likely a motivation to complete the flight even though reduced safety margins existed.
Summary
The operator’s small size, limited flight operation personnel, and single-pilot operations, required the accident pilot to exercise a high level of pre-flight and in-flight decision-making autonomy.
The decision to depart into forecast weather that was not conducive to visual flight, with limited time for pre-flight weather review, insufficient required fuel on-board, and without an appropriate flight notification system, combined to reduce safety margins and presented an increased risk to occupants on board.
Although not contributory to the accident outcome, these factors were indicative of inadequate pre-flight planning. However, having attempted to cross the Great Dividing Range, the pilot did make an effective in-flight decision to return to Dalby to refuel. This provided an opportunity to re‑assess the weather and its suitability for continued flight, as well as providing an opportunity to identify alternative options for the passengers’ continued travel.
Departure from Dalby and continuation of flight
Pre-flight
The updated weather forecast information available to the pilot while at Dalby, predicted en route weather conditions similar to those already experienced but the forecast cloud between 1,500‑2,500 ft was expected to start dissipating within about 2 hours (by 1100), and clear completely by 1200. Also, the forecast deteriorating weather conditions with reduced visibility and low cloud cover at Amberley and Archerfield were also expected to clear by 1100. These deteriorating periods had forecast conditions that were less than the VMC criteria necessary to achieve the minimum height of 1,000 ft AGL required to transit Amberley and land at Archerfield. However, the conditions were within the special VFR criteria which meant that a transit and landing could have been possible had the pilot requested a special VFR clearance from air traffic control at Amberley and Archerfield.
As was the case before departing Lighthouse, although good visibility below the cloud layers was forecast en route, conditions around the elevated terrain of the Great Dividing Range were not suitable for visual flight.
The pilot spent about 10 minutes on the ground at Dalby, almost all of which was spent refuelling, and there were no NAIPS logins recorded during time on the ground. Therefore, it was unlikely that the pilot reviewed the updated forecast either from NAIPS or another source before take-off (for example, via radio), although the pilot likely reviewed it in-flight, shortly after take-off. This suggested that there was little consideration given to alternative means of getting the passengers to their destination (for example, ground transport or waiting until the weather improved as was forecast to occur within the next 2-3 hours). The short time spent on the ground provided further evidence of a motivation to complete the flight despite having already encountered the forecast cloud in-flight.
After departure
Across the Great Dividing Range
The flight track showed that, following departure from Dalby, the pilot attempted to find a different path across a section of the Great Dividing Range to get to the low-lying terrain west of Amberley, this time tracking south of Toowoomba. The pilot requested updated weather through NAIPS about 13 minutes after take-off. However, re-assessing the weather in‑flight removed the ability of the pilot to decide against taking off again. Research indicates that continuing with an initial plan or strategy despite indications that an alternative course of action may be safer can be stronger after take-off, making the decision to discontinue the flight more difficult.
The forecast and observed weather conditions, as well as the pilot’s flight track, indicated that a cloud layer was obscuring terrain on Main Range. The pilot’s first attempt to cross this range was unsuccessful, likely due to cloud, with a 180° turn performed to try to cross at a different location. The pilot then tracked south-east and between 2 peaks at low level, before heading down a long valley towards low-lying coastal terrain.
The flight track suggested familiarity and knowledge of the terrain with the pilot possibly heading towards known locations that presented the best chance of transit. However, the aircraft crossed over the terrain with minimal separation. This was likely indicative of the pilot’s intention and motivation to continue and complete the flight, despite the forecast and observed weather conditions.
Amberley and surrounding area
After crossing Main Range, the pilot descended the aircraft towards Gatton before tracking towards Lowood, following the low-lying terrain below cloud. Weather observations from Gatton, Amberley, and Lowood Golf Course indicated a low cloud base but with good visibility below the layer. However, a weather report about 15 minutes after the accident indicated the forecast deteriorating weather at Amberley had reduced the observed visibility to 4,000 m and lowered the scattered cloud to 700 ft. These conditions would have meant that the area was not suitable for visual flight at that time.
Lake Manchester VFR route
The Lake Manchester VFR route, intended to be used in VMC, had narrow lateral and vertical separation between the hilly terrain of the adjacent D’Aguilar Range and controlled airspace, which increased the difficulty of this route in poor weather. The flight track indicated that the pilot was trying to follow the route to get to Archerfield. However, the adjacent range was obscured by cloud, so it was likely difficult to orientate the aircraft with identifiable ground features to assist with navigation. In addition, the aircraft’s relatively high speed for the conditions reduced the time available for decision making.
After turning east over Fernvale, the aircraft tracked towards a mountain at an altitude below its peak before conducting another 180° turn at about 1,200 ft and less than 2 km from rising terrain. About 10 seconds later, the pilot conducted a right turn at about 140 kt ground speed towards the rising terrain of the D’Aguilar Range, which had low cloud cover obscuring some of the peaks, and shortly after, impacted terrain.
Evidence from the site of the accident and the sound of the aircraft up until the impact indicated:
- no abnormal engine or propeller sounds up to the time of impact
- no pre-impact issues with the aircraft, engine, or propeller
- a relatively high-speed impact
- a shallow descent at the time of impact with the trees and terrain
- an angle of bank at the time of impact similar to previous turns completed during the flight.
As a result, the ATSB concluded that the aircraft was likely under control during the impact with the pilot very likely unaware of the aircraft’s proximity to the terrain. Although the pilot was knowledgeable and experienced with the location of the D’Aguilar Range relative to Fernvale, the low cloud over the range and the flight track indicated the aircraft was very likely in instrument meteorological conditions (IMC) in the final stages of the flight. The pilot very likely lost visual reference with the ground, limiting the ability to geographically orient themselves and avoid the surrounding hills, eventually leading to a controlled flight into terrain. The high speed would also have limited the pilot’s ability to react and avoid any terrain identified in the final moments of the flight.
Pilot decision making
On the day of the accident, the pilot was conscious of the adverse weather forecast and encountered during the flight prior to landing at Dalby. The pilot then made a deliberate decision to depart Dalby and continue the flight into known unsuitable weather conditions at cruise speed, low altitude, and towards a known area of rising terrain obscured by cloud. This was inconsistent with the prudent judgement, behaviour and decision making capability attributed to them by others. Nevertheless, the available information suggests the pilot was probably influenced by plan continuation bias – an internal pressure or desire to get to the destination – to continue the flight, which probably became stronger as they got closer to Archerfield Airport. However, due to a lack of information, the ATSB was unable to conclusively determine the pilot’s motivations in choosing to continue the flight in unsuitable circumstances with reduced safety margins.
Operator risk management
Although inadvertent IMC was a well-known, high consequence risk, the operator's hazard and risk register, which formed part of the organisation's safety management system (SMS), did not identify this hazard. Consequently, there was no specific assessment of its risk to operations and no specific risk mitigation in place.
Although not documented in the operator’s SMS, the risk of inadvertent IMC was being managed by requiring that pilots not commence flights unless VFR conditions were forecast for the route and at the destination, and to monitor and plan alternative actions in-flight if weather deteriorated. In this accident, the pilot did not follow these procedural controls. The controls relied on an individual pilot’s pre-flight assessment of weather, and on in-flight weather-related decision making, neither of which were addressed by the operator through any specific training, procedures, or review.
In addition, the operator did not have any procedures or training in place beyond the minimum regulatory instrument flying component of fixed wing flight reviews for pilots to recover from an inadvertent IMC encounter. Historically, relying on pilots to avoid IMC has been the primary strategy in preventing inadvertent IMC accidents. However, the continuing occurrence of these accidents demonstrates that this strategy alone is insufficient.
As the hazard of inadvertent entry into IMC was not identified in the risk register, no conclusions could be drawn about the nature and effectiveness of the specific risk controls that might have been implemented, nor whether the pilot would have utilised them. Therefore, while important, the absence of the hazard being identified in the operator’s SMS was not considered contributory to the accident.
On-board recording devices
There was no regulatory requirement for the aircraft to be fitted with on-board recording devices. However, this and numerous other investigations have shown that the lack of such devices limits the ability to understand and determine all of the factors that contributed to an accident. In turn, important safety issues that present a hazard to current and future operations were potentially not identified. Conversely, other investigations where some form of recording device was on board, provided valuable information regarding the accident.
In this investigation, flight track data was available to identify the aircraft’s movement. However, the ATSB was unable to determine why a highly experienced commercial pilot continued the flight into a known area of high terrain obscured by cloud, nor could the circumstances of what was occurring in the cockpit, especially in the final minutes before the accident, be determined. Recorded information may have provided some insights into the pilot’s decision making during the flight and further detail on how the accident developed.
The use of lightweight recorders on smaller aircraft conducting commercial operations has the potential to provide a relatively simple and cost-effective way of achieving many of the benefits that are provided by traditional recorders fitted to larger aircraft.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the VFR into IMC and controlled flight into terrain involving Cessna R182, VH-EHM, 36 km north-west of Archerfield Airport, Queensland on 29 August 2022
Contributing factors
- After encountering and manoeuvring around forecast low cloud, insufficient fuel remained on board the aircraft to complete the flight and the pilot diverted to Dalby to refuel. After refuelling, the pilot departed toward forecast en route weather unsuitable for visual flight.
- The pilot continued the flight at low level, at cruise speed, into weather conditions unsuitable for visual flight. This very likely resulted in the pilot experiencing a loss of visual reference leading to controlled flight into terrain.
Other factors that increased risk
- Although in this instance the accident was not survivable, several deficiencies were identified that delayed a search and rescue response:
- Contrary to operator procedures, the pilot provided flight notification information to a family member not associated with the operator.
- The family member was not provided with any information on appropriate actions to be taken in the event of the aircraft being overdue.
- The pilot provided flight notification information to the family member about 30 minutes after take-off from Lighthouse which limited search and rescue functions for that time.
- The aircraft likely departed Lighthouse for the flight to Archerfield Airport with insufficient fuel to account for weather-related diversions and the required contingency and final reserve fuel.
- The operator's hazard and risk register, which formed part of the organisation's safety management system, did not identify inadvertent entry into instrument meteorological conditions as a hazard, which reduced the ability of the organisation to effectively manage the related risk. (Safety issue)
Other findings
- While flight tracking data was available, the aircraft was not fitted with an onboard recording device. This could have provided valuable information to better understand the pilot’s in-flight weather-related decision making.
Safety issues and actions
|
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Operator risk management
Safety issue number: AO-2022-041-SI-01
Safety issue description: The operator's hazard and risk register, which formed part of the organisation's safety management system, did not identify inadvertent entry into instrument meteorological conditions as a hazard, which reduced the ability of the organisation to effectively manage the related risk.
Glossary
| AGL | Above ground level |
| AMSL | Above mean sea level |
| AOC | Air Operator's Certificate |
| AOPA | Aircraft Owners and Pilots Association |
| ATC | Air traffic control |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| CEO | Chief Executive Officer |
| CoA | Certificate of airworthiness |
| CFIT | Controlled flight into terrain |
| CTA | Control area |
| CTR | Control zone |
| DAME | Designated aviation medical examiner |
| ELT | Emergency locator transmitter |
| EPIRB | Emergency position indicating radio beacon |
| GAF | Graphical area forecast |
| GAJSC | General Aviation Joint Steering Committee |
| HOFO | Head of flying operations |
| ICAO | International Civil Aviation Organization |
| IFR | Instrument flight rules |
| IMC | Instrument meteorological conditions |
| ISA | International Standard Atmosphere |
| JRCC | Joint Rescue Coordination Centre |
| NAIPS | National Aeronautical Information Processing System |
| PLB | Personal locator beacon |
| POH | Pilot’s operating handbook |
| SAR | Search and rescue |
| SMS | Safety management system |
| TAF | Terminal area forecast |
| TAS | True Airspeed |
| TAWS | Terrain awareness and warning system |
| VFR | Visual flight rules |
| VMC | Visual meteorological conditions |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot’s next of kin and former colleagues
- the passengers’ friends and colleagues
- Bureau of Meteorology
- Geoscience Australia
- Airservices Australia
- Executive Helicopters (operator)
- Civil Aviation Safety Authority
- OzRunways
- Avdata
- Fernvale Rural Fire Brigade
- Queensland Police Service
- witnesses
- CCTV video footage of weather near the aircraft’s flight path.
References
Australian Transport Safety Bureau. (2005). General Aviation Pilot Behaviours in the Face of Adverse Weather. B2005/0127
Australian Transport Safety Bureau. (2013). A review of the effectiveness of emergency locator transmitters in aviation accidents. AR-2012-128
Australian Transport Safety Bureau. (2019). Avoidable Accidents No. 4: Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions. AR-2011-050
Australian Transport Safety Bureau. (2021). Collision with water involving de Havilland Canada DHC-2, VH-NOO. AO-2017-118
Australian Transport Safety Bureau. (2021). VFR into IMC and controlled flight into terrain involving Pilatus Britten-Norman BN2A, VH-OBL. AO‑2018‑078
Australian Transport Safety Bureau. (2023). VFR into IMC, loss of control and collision with terrain involving Airbus Helicopters EC130 T2, VH-XWD. AO-2022-016
Civil Aviation Safety Authority. (2019). Safety behaviours: human factors for pilots: Resource booklet 7 Decision making (2nd edition)
Collins, J. (2022). Training and Safety Tip: Escaping the VFR-into-IMC Trap. Aircraft Owners and Pilots Association (AOPA).
Endsley M.R. (1995). Toward a theory of situation awareness in dynamic systems. Human Factors, Volume 37, No. 1, 32-64
Federal Aviation Administration. (2023). Information for Operators (InFO): Terrain Awareness and Warning Systems (TAWS) Nuisance Alerts
General Aviation Joint Steering Committee (GAJSC). (2021). Controlled Flight Into Terrain (CFIT) Working Group
General Aviation Joint Steering Committee (GAJSC). (2021). Controlled Flight Into Terrain (CFIT) Working Group: Appendix 6 — Detailed Implementation Plans for Safety Enhancements
Harris M.R., Fein E.C. and Machin M.A. (2022). A Systematic Review of Multilevel Influenced Risk-Taking in Helicopter and Small Airplane Normal Operations. Front. Public Health 10:823276. doi: 10.3389/fpubh.2022.823276
International Civil Aviation Organization. (2018). Safety Management Manual (4th ed). ICAO Doc 9859, Montreal
O'Mahony et al. (2023). VFR Into IMC Through the Lens of Behavioral Economics. Journal of Air Law and Commerce. Volume 88, Issue 1, Article 4 https://scholar.smu.edu/jalc/vol88/iss1/4
Smith, M. (2022). 178 Seconds: VFR into IMC is an Insidious Trap. Aircraft Owners and Pilots Association (AOPA)
Stanton A. (2022). 'Gathering Clouds' A Study of Plan Continuation, Risk, Rules, and Pilot Behaviour. https://doi.org/10.25904/1912/4844
Wilson, D.R., & Sloan, T.A. (2003). VFR Flight Into IMC: Reducing the Hazard. Journal of Aviation/ Aerospace Education & Research, 13(1). https://doi.org/10.15394/jaaer.2003.1567
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the aircraft operator and the Civil Aviation Safety Authority.
A submission was received from the aircraft’s operator.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix – Fuel calculations
Background
An assessment was undertaken to determine the likely quantity of fuel on-board the aircraft when it departed Lighthouse, and if that quantity was sufficient for the intended flight to Archerfield.
Calculations – Fuel on-board at Lighthouse
Using the maximum capacity of the fuel tanks and the fuel uplift data at Dalby, the useable fuel remaining in the tanks on landing at Dalby could be calculated (20.7 L). The total fuel used during the flight (taxi, climb, and cruise) from Lighthouse to Dalby was estimated using the pilot’s operating handbook (POH),[48] the operator’s operations manual, and the forecast weather.
Taxi
Total taxi fuel was calculated from the POH as the difference between the maximum ramp weight (1,411.6 kg) and maximum take-off weight (1,406.1 kg). The operator’s operations manual also provided an estimated taxi fuel amount.
Climb
Climb fuel consumption rate data in the POH was available for maximum aircraft weight, and International Standard Atmosphere (ISA) conditions and for normal climb performance. Similar temperature conditions to International Standard atmosphere (ISA) were forecast. The main cruise altitude from the aircraft’s OzRunways flight track data was 3,400 ft between Lighthouse and Dalby. The POH data provided fuel consumption for 3,000 ft and 4,000 ft so an interpolation calculation was conducted.
Cruise
Fuel consumption from Lighthouse to Dalby was calculated using data provided in the POH, operator’s operations manual, and forecast weather. As the cruise power setting for the flight was not known, cruise fuel consumption rates were calculated for 3 common engine power settings (75%, 65% and 55%). The POH data assumed maximum take-off weight and standard ISA conditions. The most relevant data for the 3,400 ft cruise altitude was contained in the performance chart for 4,000 ft altitude. For calculations conducted using the operations manual data, the provided ‘block fuel flow’ was used as the cruise and climb fuel flow.
Cruise time was based on the OzRunways flight track data after reaching cruise level until landing at Dalby. Although about two-thirds of the flight was at a similar cruise altitude, the remaining third was made up of 2 climbs and 2 descents along with heading changes. It was assumed that the fuel consumption rate during these phases averaged out to be similar to the cruise fuel consumption rate (since a higher fuel consumption rate would occur during climb with a lower rate during descent). Therefore, the cruise fuel consumption rate was used for the flight time between initially reaching cruise altitude and landing at Dalby.
The actual weight of the aircraft at the same power level and operating altitude can affect the cruise speed of the aircraft and thus flight time and total fuel consumption. POH fuel consumption and related true airspeed (TAS) data was provided at maximum weight but the aircraft during the flight was below this weight. The estimated aircraft departure weight based on the operations manual fuel usage was about 1,269 kg. However, the difference in TAS at this weight was considered minimal so no correction to the cruise time was applied.
The estimated fuel on-board at Lighthouse for each scenario is shown in Table 2.
Table 2: Estimated fuel on-board VH-EHM at Lighthouse
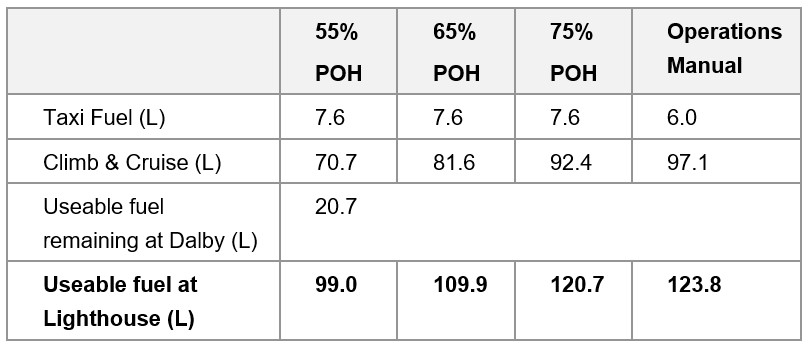
Calculations – Fuel required from Lighthouse to Archerfield
The Civil Aviation Safety Regulations defined the fuel requirements for Part 135 operators. The following fuel was required for a Part 135 flight:
- taxi fuel – fuel used before take-off
- trip fuel – fuel for take-off, climb, cruise, descent, and landing
- contingency fuel – 10% of trip fuel for a piston engine aeroplane to compensate for unforeseen factors
- final reserve fuel – 45 minutes flight time for a piston engine aeroplane and is useable fuel remaining on completion of final landing at the aerodrome
- Destination alternate fuel (if required)
- Holding fuel (if required)
- Additional fuel (if required)
An estimate on the fuel required to complete the flight from Lighthouse to Archerfield (taxi, climb, cruise) was determined using data available in the POH, operations manual and the forecast wind conditions.
The anticipated ground speed was calculated based on the TAS and forecast wind conditions. The Bureau of Meteorology grid point wind and temperature chart forecast 13‑21 kt wind from 70° at 2,000 ft and 14-20 kt wind from 50-80° at 5,000 ft for most of the planned flight which was on a 115° track. Therefore, an estimated 10 kt headwind was used for the calculations. For the different power settings, the ground speed was used along with the cruise distance to determine the total time and fuel consumption during cruise. For the operations manual fuel flow calculations, the total planned distance to Archerfield was used as the ‘block fuel flow’ accounted for climb, cruise, and descent fuel consumption.
Cruise fuel planning was conducted to overhead the destination aerodrome at cruise level. Manoeuvring and approach fuel consumption was not considered.
Contingency fuel
Contingency fuel was 10% of the calculated trip fuel.
Final reserve fuel
Final reserve fuel was 45 minutes at holding speed, ISA conditions and 1,500 ft. The POH provided a holding fuel of 23.8 L based on 45 minutes at 45 % engine power. The operations manual provided an expected ‘holding’ fuel flow of 40 L per hour (30 L for 45 mins).
Destination alternate fuel, holding fuel, and additional fuel
Either the ‘destination alternate fuel’ or ‘holding fuel’ was required if the destination forecast was below the alternate minima. The relevant Terminal Area Forecast (TAF) for Archerfield forecast conditions above the alternative minima, so no holding or destination alternate fuel was required for the flight. ‘Additional fuel’ was only required for multi-engine aircraft, or aircraft with pressurisation. Since VH‑EHM was a single-engine non-pressurised aircraft, ‘additional fuel’ was not required. The results are shown below in Table 3.
Table 3: Estimated minimum regulatory fuel required for planned flight to Archerfield
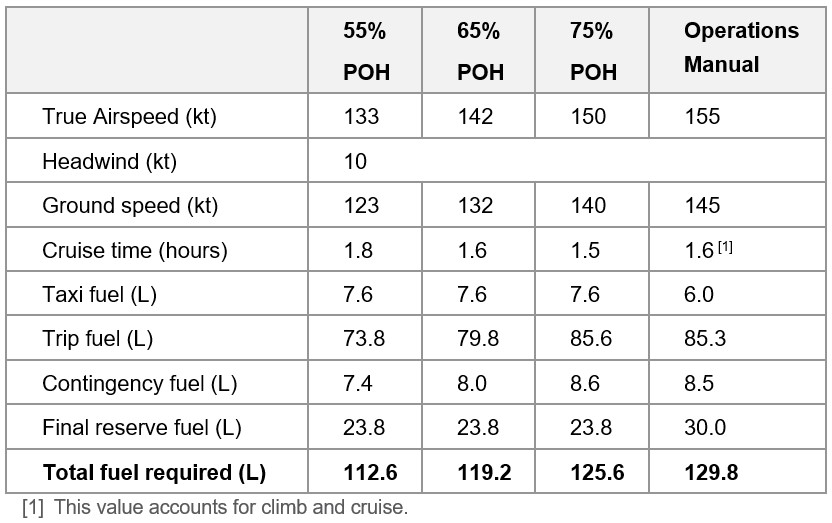
Estimated fuel margin
The results of the above calculations are shown below in Table 4 to determine the fuel margin between the useable fuel on-board and the minimum required fuel.
Table 4: Estimated fuel margin for the planned flight to Archerfield
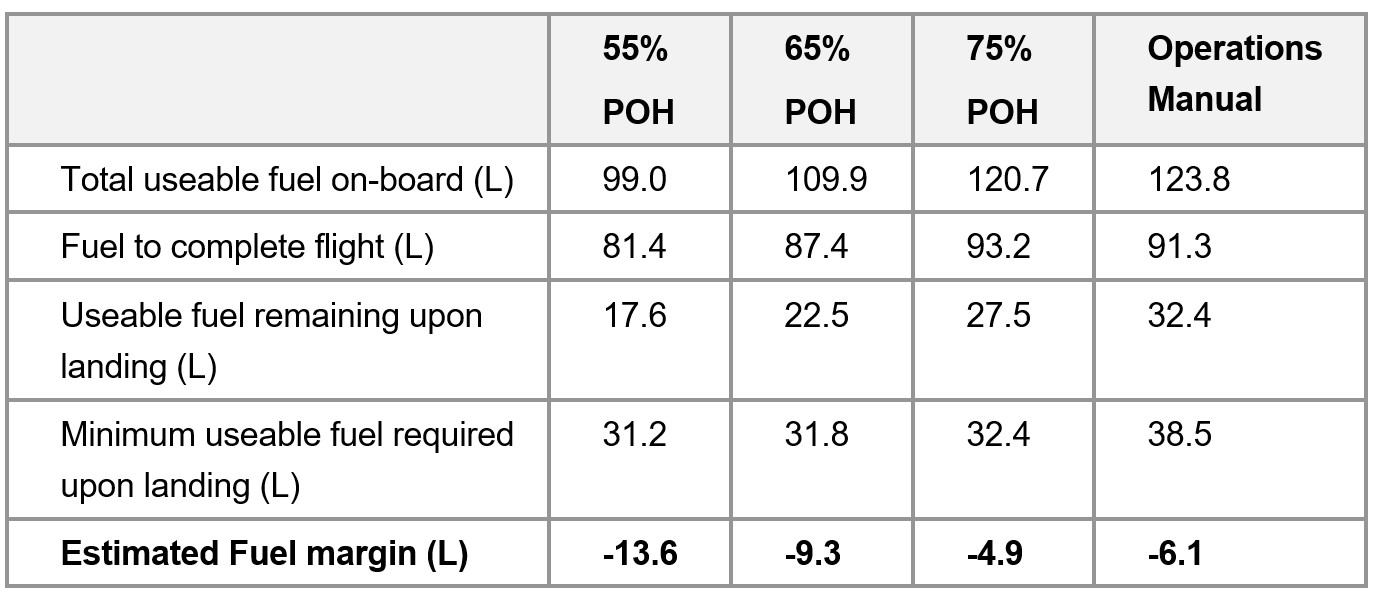
The results are based on forecast ideal weather conditions. As per the general fuel requirements in the CASR, in determining the quantity of useable fuel required, the pilot in command must also consider the effect of relevant meteorological reports and forecasts.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The flight was operated under Civil Aviation Safety Regulations Part 135 (Air transport operations – smaller aeroplanes).
[2] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[3] GPS altitude from OzRunways, which is truncated to 100 ft increments.
[4] Data used for terrain elevation does not account for vegetation or structures such as power lines, which may protrude some distance above the ground.
[5] Before the introduction of the Civil Aviation Safety Authority (CASA) Part 61 licencing regulations in 2014, under Civil Aviation Regulation 5, pilots maintained instrument currency by completing an instrument ‘renewal’. Under Part 61, pilots maintained this currency by completing an ‘instrument proficiency check’.
[6] A low-level (LL) rating is needed for a low-level flight operation (below 500 feet AGL including low-level aerobatics).
[7] Aerial stock mustering involving the direct use of aircraft for the movement of livestock.
[8] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[9] An aircraft’s maintenance release is a document that provides registered operators and pilots with evidence that an aircraft has had the required maintenance carried out, provides details of any defects that may require rectification before a flight can commence, and also provides essential information about any scheduled maintenance actions that may become due before completion of a planned flight.
[10] Global Navigation Satellite System: A satellite-based radio navigation system that uses signals from orbiting satellites to determine precise position and time.
[11] A TAWS provides visual and aural alerting including a look-ahead terrain function. TAWS is a generic term that also includes a ground proximity warning system (GPWS) with a forward-looking terrain avoidance function. A TAWS is an important tool to help minimise the risk of controlled flight into terrain (CFIT). It provides an independent and unambiguous warning of proximity to the ground or obstacles, regardless of any navigational uncertainty or error such as mis-setting or misreading the altimeter.
[12] The series of Technical Standard Orders (TSO) C151 stipulated the minimum operational performance standards that a terrain awareness and warning system (TAWS) must meet to comply with regulatory requirements for the fitment and use of those systems.
[13] Federal Aviation Administration, 2023, Information for Operators (InFO) - Terrain Awareness and Warning Systems (TAWS) Nuisance Alerts.
[14] Spidertracks is a subscription aircraft monitoring service that allows operators to track and monitor the location of aircraft at regular intervals. The location is recorded and transmitted by a unit that is fitted to the aircraft.
[15] CASR Part 91 Manual of Standards (MoS), section 7.02.
[16] The National Aeronautical Information Processing System (NAIPS) is a computerised, aeronautical information system. It processes and stores meteorological and NOTAM information as well as enables the provision of briefing products and services to pilots.
[17] A Terminal Area Forecast (TAF) is a statement of meteorological conditions expected for a specified period in the airspace within a radius of 5 NM of the aerodrome reference point.
[18] METAR: a routine aerodrome weather report issued at routine times, hourly or half-hourly.
[19] All cloud heights stated are AMSL.
[20] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[21] INTER: an intermittent deterioration in the forecast weather conditions, during which a significant variation in prevailing conditions is expected to last for periods of less than 30 minutes duration.
[22] The timestamp on the video footage was likely accurate within minutes based on comparison with other sources. In any event, the weather conditions shown in the video footage were similar for at least 15 minutes before and after the recorded accident time.
[23] CASR Part 91, Table 2.07 (3).
[24] CASR 135.230.
[25] Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under Instrument Flight Rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[26] CASR 91.265 and 91.267.
[27] OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[28] A common traffic advisory frequency is a designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled airport, or within a broadcast area.
[29] The height above ground level was based on GPS altitude available from OzRunways (truncated to 100 ft increments), and Geoscience Australia terrain elevation data.
[30] QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
[31] CASR Part 135 Manual of Standards (MoS), section 11.51.
[32] The force needed to accelerate a mass. G-force is normally expressed in multiples of gravitational acceleration (normal gravity = 1g).
[33] CASR Part 91 Manual of Standards (MoS), section 9.02.
[34] SARTIME: An abbreviation for ‘time search action required’. A SARTIME is the time nominated by a pilot for the initiation of Search and Rescue (SAR) action.
[35] Flight Note: Details of the route and timing of a proposed flight provided by the pilot in command of an aircraft, other than notification submitted to Airservices Australia, and which is required to be left with a person who could be expected to notify appropriate authorities in the event that the flight becomes overdue.
[36] Automatic Dependent Surveillance - Broadcast (ADS-B) is a system in which equipment on board an aircraft automatically broadcasts the precise location of the aircraft. The data can be used by other aircraft and air traffic control to identify the aircraft’s position and altitude without the need for radar.
[37] CASR Part 135 Manual of Standards (MoS), chapter 7.
[38] The Pilots Operating Handbook provided a value of about 24 L compared with 30 L from the operator’s operations manual.
[39] A notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[40] The AOC was issued before the CASA flight operation rules changed in December 2021, where the term ‘air transport’ replaced charter, regular public transport, and air ambulance when conducted for hire or reward.
[41] The operator was required to have a CASA-approved SMS by December 2024.
[42] The operator will be required to have a CASA approved program for training and assessing operational safety‑critical personnel in human factors principles and non‑technical skills by a future date to be specified by CASA.
[43] A structured, forward-planned, larger-type, surveillance event, which examined an authorisation holder’s systems, safety risk controls, and processes.
[44] The theory of planned behaviour posits that the most immediate cognitive antecedent to performing a distinct behaviour is the formation of an intention. The theory suggests that behavioural intentions are formed and can be predicted, predominantly from just 3 kinds of beliefs that a person holds in relation to the behaviour: attitude toward the behaviour, social norms, and perceived behavioural control (Stanton, 2022).
[45] Economics has traditionally assumed people always make decisions in their best interests. Behavioural economics challenges this view by providing a more realistic model of human behaviour. It recognises we are systematically biased (for example, we tend to satisfy our present self rather than planning for the future) and can make decisions that conflict with our own interests.
[46] The pilot’s operating handbook (POH) for the aircraft could not be located. Information from the POH of another Cessna R182 Skylane RG with a different serial number was used.
[47] The General Aviation Joint Steering Committee (GAJSC) is a United States based public-private partnership focused on improving the safety of the general aviation industry.
[48] As the aircraft’s POH was damaged during the accident, the POH for a different, but similar, 1978 Cessna R182 Skylane RG aircraft was used (serial number R18200450). The performance related data should be similar or identical to the data for VH-EHM.





