
Executive summary
What happened
In August 2021, during the COVID-19 pandemic, Formosabulk Clement diverted to Brisbane, Queensland for crew change, to be completed to/from a launch via the combination pilot ladder. At the time, Queensland was the easiest jurisdiction in Australia for ships to conduct crew change due to the State’s extensive quarantine arrangements for transporting and accommodating seafarers. By 1833 on 9 August, 8 persons and their luggage had been successfully transferred from the launch PT Transporter to the ship located at an outer anchorage. The launch skipper then drove the launch a short distance off the ship for a short break.
By this time, the ship had turned about the anchor and the boarding side of the ship came under the influence of the forces of wind and sea. After receiving supervisor advice to attempt the transfer again, the launch skipper took the launch back toward the boarding area to assess whether the conditions were suitable. On board Formosabulk Clement, the departing chief mate (dCM) saw the approaching launch and went down the access ladders and onto the vertical pilot ladder in anticipation of boarding. At about 1838, as the dCM waited on the ladder and the launch came close alongside, a large wave passed down the side of the ship and lifted the launch higher than expected. The dCM was struck by the launch and knocked into the sea. Despite being quickly recovered on board, they received fatal injuries.
What the ATSB found
The investigation found that the open water conditions at the anchorage were marginal but, within a lee created by the ship, they were suitable for the transfer to occur. However, as the skipper brought the launch alongside to assess conditions, the transfer area was no longer in a lee and waves were acting against the ship’s side, increasing in height as they passed along it.
Coincident breakdowns in communications between, and within, the ship and the launch resulted in the ship’s master, the dCM, the launch skipper and the launch deckhand having different understandings of the significance and intent of the launch returning alongside the ship.
In addition, the dCM went down the boarding ladders in preparation to board the launch without the knowledge or agreement of either the ship’s master or the launch skipper. The dCM was then in a vulnerable position when the launch was lifted on the higher than expected wave.
The investigation also found that plans and details of how the transfer was to be controlled and progress when the launch was alongside were not adequately shared between all parties in the time available as the launch approached the ship. Neither the shipping company nor the launch company had in place procedures to ensure that such information was shared before the ship arrived at the anchorage.
As a consequence, different interpretations and misunderstandings of the plan and expectations of the people involved in the transfer, particularly those in positions of influence over the progress of the transfer, were not identified and addressed.
What has been done as a result
Following the accident:
- the launch service provider (Pacific Tug) ceased crew transfer operations until an investigation into the accident and assessment of transfer operations were completed
- Maritime Safety Queensland (the State’s regulator) amended the COVID crew change procedure for vessels at anchor including limiting crew changes to risk assessed conditions and daylight hours only
- Formosabulk Clement’s operator, Formosa Plastics Marine Corporation, completed investigations and held multiple safety meetings and training exercises to share details of, and lessons learned from, the accident.
Subsequently, Pacific Tug updated personnel transfer arrangements and procedures. This included developing and implementing a traffic light system (red, amber and green statuses) for operational assessment and control. The system set operational requirements and limits, including weather, against which the conduct of the transfer task was continually assessed. Light sets, mounted on the launch, are used to show the status of the transfer to all involved, on the launch and the ship. A red status requires cessation of the transfer operation and complete reassessment prior to any further attempt to complete the task.
Safety message
All parties are reminded of the importance of maintaining active and adaptable communications before and during the planning, co-ordination and control of a complicated task.
Further, where possible, all parties should share plans and information well before undertaking a task so as to allow all involved to have a common and complete understanding of the planned activity.
The occurrence
During the COVID-19 pandemic, the international maritime industry struggled to comply with requirements for the maximum continuous period that a seafarer could serve on board a ship without taking leave.[1] Following a period of grace during which the continuous service period was relaxed to 14 months, in November 2020, the Australian Maritime Safety Authority (AMSA) notified ship owners, operators and seafarers that it would resume enforcing the 11‑month continuous service limitation from 28 February 2021.
On 25 July 2021, Formosabulk Clement (Figure 1) departed Mailiao, Taiwan, in ballast, bound for Newcastle, New South Wales to load coal. The ship’s trade routes for the preceding 6 months had provided no opportunity for change of crew and 14 of the 25 crew on board had been on board for more than 11 months.
At that time, pandemic-related restrictions on crew changes varied considerably between different States in Australia with Queensland offering the most convenient opportunities. Hence, in early July, Formosabulk Clement’s manager, Formosa Plastics Marine Corporation (FPMC), engaged its local shipping agents in Australia to arrange a crew change off Brisbane, Queensland. The arrangements would involve the ship calling at Brisbane anchorage to rendezvous with a crew change vessel (launch). Eleven crewmembers were to join the ship and 15 were leaving.
Figure 1: Formosabulk Clement at anchor, PT Transporter alongside

Source: AMSA, Pacific Tug with modifications and annotations by ATSB
Arrival to anchor and preparations
At 0912[2] on 9 August, Formosabulk Clement anchored in the port of Brisbane outer anchorage, about 6 miles[3] east of Point Cartwright. Ashore, pandemic protocols had been completed for the joining crew and arrangements for transfer by launch had been made. The launch service provider (Pacific Tug) notified all parties that, to satisfy requirements, the transfer would require 2 trips by the launch PT Transporter. The launch was to collect the passengers and depart from the quarantine facility at Brisbane Rivergate marina and shipyard.[4]
Figure 2: Starboard side boarding site and ladder arrangement

Source: AMSA, FPMC and Pacific Tug annotated by ATSB
Pacific Tug requested that Formosabulk Clement be relocated further south in the anchorage area to assist the transfer, and with Brisbane vessel traffic service (VTS) approval, the ship was moved south. During this same information exchange, the ship’s master was requested to have the boarding arrangements (Figure 2) located on the opposite side of the ship to the deployed anchor and to provide a good lee for the transfer.
At 1436, Formosabulk Clement’s port anchor was let go and at 1500 ‘finished with engines’[5] was rung. The ship was now anchored about 5 miles east of Caloundra Head, about 7 miles south of the original anchor location. It was riding easy on the anchor, 7 shackles in the water in a fresh breeze and moderate seas, from the south-east.[6] Throughout the afternoon, the ship yawed about the anchor, at the whim of the conditions, its heading varying between about 140° and 80° in about 30-minute cycles.
At 1448, PT Transporter departed the Rivergate marina and shipyard with 2 crewmembers (skipper and deckhand) and 8 Formosabulk Clement joining crewmembers on board. At 1530, it passed to the west of the entrance beacons, 30 miles from the ship, heading north-east making better than 15 knots across Moreton Bay. The passage across the bay toward the ship remained uneventful other than for several of the passengers becoming seasick in the choppy conditions.
At 1600, on board Formosabulk Clement, the departing chief mate (dCM) completed handover of rank to the trainee chief mate who had been on board since early May and was now taking over the position. The new chief mate then took the navigation watch from the second mate.
The dCM was to leave the ship on the first launch after supervising the embarkation of the 8 joining crew (and their luggage) and the disembarkation of 7 other crewmembers. In agreement with the master, the plan was for the dCM to be the last person to disembark. The dCM and the master (on the bridge) would be using handheld UHF radios to communicate.
After the evening meal, crewmembers assembled and arrangements for the departure were finalised. At the boarding area on the starboard side, the bosun, one ordinary seafarer and one deck cadet were to be assisted with conducting the transfers by the departing, and then joining, crewmembers, overseen by the dCM. The personnel gathered on deck, with their luggage, and prepared to assist the boarding crewmembers.
At 1725, as PT Transporter approached Formosabulk Clement, the skipper called the ship on the port’s working channel (VHF channel 12) and advised that the launch was 15 minutes away. The skipper confirmed the transfer would be done on the ship’s starboard side and requested that a lee be provided. The ship’s new chief mate confirmed the boarding side and the lee. Subsequent communications generated confusion between the launch and the ship regarding the lee. The launch skipper then requested assistance from the launch passengers and from 1730 communications between the launch and the ship commenced in Chinese. At about 1740, the launch slowed and manoeuvred along the starboard side of the ship.
Transfer to the ship
At 1745,[7] Formosabulk Clement was at one extreme of yaw about the anchor with the starboard side exposed to the weather (heading 089° with weather from 100°— Figure 3). The launch skipper recalled there was a little bit of sea from the east-south-east and that it ‘wasn’t the calmest of conditions’ (noting that several of the launch passengers had been sick during the journey). The ship’s master recalled observing similar conditions at the time with 2 to 2.5 m wave heights. The ship’s stern began to swing to port and conditions along the starboard side began to ease.
Figure 3: Ship yaw leading up to the accident

Source: ATSB analysis of AIS data from AMSA
On board the launch, the skipper manoeuvred alongside, keeping parallel to the ship’s side with little if any force applied to the hull while keeping the boarding ladder in position on the foredeck of the launch. As the conditions allowed, the transfer commenced with each person guided, one at a time, forward and onto the ladder by the deckhand. Baggage was transferred by line from the after deck.
The weather conditions began pushing the ship’s stern to starboard and the master requested standby on the main engine and at 1806 the engine was ready for manoeuvring. The stern continued to swing to starboard and by 1810 the ship had swung back to heading 095°. The master used dead slow ahead commands in conjunction with rudder movements to drive the stern around and turn the port side of the ship against the weather, thereby providing shelter to the boarding area.
By 1825, the ship had been manoeuvred to heading 167°, creating calm conditions at the transfer site. The transfer continued. At about 1820, the ship’s main engine was stopped and the ship continued to yaw under the influence of the weather. The main engine was used again for a short period and by 1833 the transfer on board was complete and the ship had swung back to 097°.
The skipper then manoeuvred PT Transporter alongside Formosabulk Clement with the intention of assessing the suitability of conditions at the boarding ladder for continued operations.
The accident
Following the brief rest period, the launch was taken back in toward the boarding ladder. The skipper intended to see how the launch sat alongside as the ship yawed and the boarding area became more exposed to the conditions. The skipper also expected to provide approval to the ship before anyone left the deck and did not anticipate that someone would be on the ladder.
Onboard Formosabulk Clement, the master confirmed via radio with the dCM that the boarding phase was completed. At this time, the master could see the dCM on deck and expected that disembarkation would not commence until approval was given. The boarding area on the starboard side was now exposed to the weather and the master was aware that a lee would have to be made on that side. This required the master to manoeuvre the ship to make a lee and then convey this plan to the launch and to the dCM. However, while attempting to communicate with the launch, the master could see it returning.
As the launch approached, the dCM went down the accommodation ladder and onto the pilot ladder. One of the departing able seafarers (AB1) followed onto the accommodation ladder. The dCM was wearing multiple layers of clothes, including a jumper, along with a small document wallet type backpack under a self-inflating buoyancy vest and was carrying a ship’s hand-held radio.
As the launch closed in, the dCM began climbing down the pilot ladder. The master was preoccupied with contacting the launch and remained unaware that the dCM (or AB1) had left the deck and gone onto the ladder(s).
As the launch closed on the ship, the deckhand saw the dCM several rungs down the pilot ladder and descending. As the launch was not yet safely alongside, the deckhand directed the dCM to climb back up. The dCM climbed up until adjacent to the accommodation ladder lower platform.
Soon thereafter, the launch came close alongside and the dCM began to descend the pilot ladder a second time. The deckhand felt the conditions were suitable and did not direct the dCM away. The launch skipper was unaware of the presence of the dCM on the pilot ladder or of the interactions between the deckhand and the dCM.
At about 1838, suddenly a larger wave lifted the launch higher than had to that time been experienced (Figure 4). The skipper sighted the dCM on the ladder as the launch rose, but with insufficient time to take any avoiding action. The deckhand shouted a warning for the dCM to get clear, however, the launch rose up, trapping the dCM between it and the side of the ship. As the launch then came down on the wave, the dCM fell into the water. The dCM’s lifejacket inflated, keeping them afloat.
On board Formosabulk Clement, the master was still attempting to communicate with the launch when notified by the bosun that the dCM had fallen into the sea.
The skipper manoeuvred the launch clear of the ship and the dCM. Once clear, the skipper and deckhand went about rescuing the dCM who was soon retrieved on board PT Transporter. The dCM was seriously injured and the launch crew administered first aid, including CPR. The skipper notified the ship’s master that the dCM had been retrieved but was unconscious.
In the following minutes authorities including VTS, the harbour master and the shipping agents were notified. The emergency authorities were called and police and ambulance personnel were deployed. The launch was directed to take the dCM to Mooloolaba, about 10 miles to the north-west, to meet with the emergency services.
At 1905 PT Transporter departed the area for Mooloolaba. The launch arrived there at 1955 and met paramedics. The dCM was examined and provided treatment but was pronounced deceased soon thereafter.
Figure 4: Approximate positioning of the launch and personnel at 1838

Source: AMSA, Pacific Tug with modifications and annotations by ATSB
Post-accident
All further operations were ceased and both vessels were directed by AMSA to remain in their existing locations pending an accident investigation. During the following days, Formosabulk Clement was detained by AMSA on the grounds that the required boarding arrangements for safe means of access were defective and did not comply with regulations. This notice, along with action by the port authority, prevented personnel from boarding the ship from the water.
Consequently, alternative arrangements were made to complete the still outstanding crew change, which was completed by helicopter on 13 August. The detention order was subsequently lifted and the direction notice closed. At 1530 that day, standby was called and Formosabulk Clement departed the anchorage and continued its onward voyage to Newcastle.
Context
Formosa Plastics Marine Corporation
Formosa Plastics Marine Corporation (FPMC) commenced operations in 1980 with 2 chemical tankers to service the needs of its parent company Formosa Plastics Group. By 2022, FPMC operated a fleet of 48 vessels, including 18 bulk carriers, with total deadweight of 5.9 million tonnes. FPMC ships regularly traded to Australia, calling at ports including Brisbane and Newcastle.
Formosabulk Clement
At the time of the accident, Formosabulk Clement was owned by Pilot Maritime Company (Liberia) operated by the Formosa Plastics Marine Corporation (FPMC, Taiwan) and registered in Liberia. The ship was classed with Bureau Veritas.
Formosabulk Clement had regularly visited Newcastle, with 5 port calls in the 12 months prior to trading between Taiwan and Russia between the period of April 2021 and the accident voyage. The ship had completed one previous crew transfer off Brisbane, by launch, in December 2020. On that occasion, 4 persons had disembarked (none boarded).
Following this accident, Formosabulk Clement was sold and renamed Goody.
Crew details
Formosabulk Clement had a multi-national crew of 25, including the relieving chief mate (scheduled to take over during this crew change), 3 deck cadets and 2 engineer cadets. The master and departing chief mate (dCM) were from China and the remaining crewmembers were from China, Taiwan and India.
The master first went to sea in 1986 and obtained their master’s seagoing qualifications in 1999. They had worked for FPMC since 2003 as master within the bulk carrier fleet. This was the master’s first time on board Formosabulk Clement, having joined in June 2020.
Of the 15 crewmembers scheduled to depart Formosabulk Clement during the call to Brisbane, 14 had joined the ship in June 2020 and had been on board for 409 days.
All crewmembers interviewed reported having used a pilot ladder previously. The least experienced had joined the ship by pilot ladder and stated that more experienced crewmembers gave advice and reassurance when preparing on this occasion. More experienced persons had used pilot ladders multiple times on many different ships. All stated that training was given and discussions held prior to the transfer. Training was also provided at shore-based marine schools.
Crew change procedures
The FPMC fleetwide safety management system (SMS) included several procedures which related to conducting personnel transfer between a ship and another vessel while at anchor in open waters.
Personnel transfer at sea procedure
The ‘Personnel transfers procedure at sea’ advised that crew change at sea was to be undertaken as far as possible in favourable weather conditions, with good visibility, and preferably during daylight. Transfer activities were to be suspended and reported to the superintendent if the weather deteriorated.
The procedure required that, prior to the transfer, a risk assessment and a briefing meeting for the task were to be conducted. The briefing meeting was to include discussion of:
- the launch company’s risk assessment for personnel transfers. The documentation to be received was to include details of the suitability of the launch, details of its life-saving equipment and confirmation of the responsible officer on board the launch
- limiting weather conditions: wind <17 knots, swell <1.25 m, visibility >5 miles
- the requirement for approval by the masters or skippers of both vessels and the persons being transferred, for the transfer to take place.
Personnel to be transferred were to be fully aware of and understand the sequence of events including that only one person was allowed on the ladder at a time. They were also to understand the requirements for and use of any equipment including personal protective equipment (PPE) and clothing, including lifejacket, footwear and safety harness.
The procedure also advised that the responsible officer should not be one of the departing or joining crew.
Furthermore, the procedure advised that good communications be established with the launch and that during the transfer ‘There should also be a clear understanding of the meaning of all terms used in the transfer’.
Risk assessment
A risk assessment for ‘Transfer of personnel to and from small vessels’, involving 14 crewmembers, was authorised and dated 9 August 2021.
The assessment included the risk of personal injury due to a fall. This was mitigated by measures including not transferring in heavy weather (not defined in this document), that all crew were to be briefed on the transfer with the sequence explained, step-by-step, and ensuring good communication with the launch to co-ordinate the task.
The risk of crush injury due to the launch or other equipment was to be mitigated by briefing and training of the crew including confirmation of the sequence of activities.
Also identified was the risk that the gap between the ladder and the launch combined with the motion of the launch may lead to a person falling into the sea. This risk was to be addressed by good communications and co-ordination of the task along with sufficient lighting and personnel wearing the required PPE.
The assessment concluded that the level of risk was tolerable and no ‘additional measures’ to reduce risk or further assessment were required.
Crewmember training—pre-transfer briefing
A record (on FPMC form titled ‘Training Record’) was kept of a meeting held a week before arrival to discuss the transfer. Dated 2 August and signed by all crewmembers, the subject of the training record was ‘Personnel transfers procedure at sea’.
This one-page record included some of the points raised in the personnel transfer at sea procedure, such as providing a lee, having clear communications, completing a risk assessment, and details of lighting and safety equipment. However, no mention was made of the launch company’s documentation or expectations, limiting weather conditions or of signals and terms to be used.
Permit to work overside
A permit to work overside was completed on 9 August 2021, valid from 1530 that day. The permit identified the dCM as the person assigned to the work with the bosun as the team leader at the worksite. Twelve others, including those scheduled to depart, were signed-on to the permit as other persons.
This permit contained general applicable items such as PPE, communications, lighting and consideration of the weather conditions. The permit indicated that all requirements were in place, including that the weather was considered suitable for safe work. However, it did not make specific mention of limiting conditions, personnel transfer activities or communication and signalling protocols.
FPMC risk assessment procedures
The FPMC SMS risk assessment procedures document was to be a source of information and guidance for the use and implementation of risk assessments. The document outlined risk assessment philosophy and the company process. Guidance and suggestions were provided for each stage of the process. The procedure also advised that any person had the authority to stop the work should a condition or behaviour be perceived as unsafe.
The procedure required that all personnel performing a risk assessment on board were to be appropriately trained in the process.
FPMC permit to work procedures
The FPMC ‘Permit to work procedures’ required that, as part of the risk assessment process, a permit to work (PTW) was to be issued before any work was commenced. FPMC had a suite of 13 PTWs for use on board. A permit for work overside was required for any work which required crewmembers to work outboard of the ship’s railings, including preparation of the combination pilot ladder.
The PTW procedures also required that a toolbox talk be completed for all tasks. This was to be held by the person in charge, at the worksite, with all involved, before the work began.
FPMC crew change logistics
The ATSB sought advice from FPMC regarding crew change issues and requirements during the pandemic and the plan to change crew off Brisbane. The response received included:
- Joining personnel were to complete any special requirements before departing crew ended their contracts. This included visa requirements as well as pandemic requirements such as PCR[8] testing and quarantining.
- COVID-19 pandemic restrictions meant that, in the preceding 6 months, crew were denied entry into Russia or Taiwan. AMSA enforcement of MLC time on board limits meant that crew change needed to occur prior to or at Newcastle.
- Approval for crew change was not obtained from New South Wales (NSW) Health, and, FPMC had found, on previous occasions, that crew change in NSW was difficult.
- Queensland had put in place a COVID-safe plan which allowed crew changes to be completed and Brisbane was selected for the crew change on this basis.
- Crew change arrangements were made by a local Brisbane agent. At that time, arrangements included COVID-safe transport, accommodation and testing, in addition to the usual logistics of launch provision, notification of the required agencies for port, customs, immigration and biosecurity requirements.
- Earlier crew change operations for FPMC vessels had showed launch transfers to be significantly more cost-effective than other means, such as helicopters. In addition, the need to disembark 15 persons and embark 11 made launch transfer the preferred choice for Formosabulk Clement.
- FPMC also advised, that at the time, there were no restrictions on timing for the crew change with limitations only due to weather. The vessel position was guided by the port and advice from the launch company.
Boarding arrangement
At the time of the accident, freeboard at the boarding location was about 16 m (Figure 2). The combination pilot ladder was arranged with the accommodation ladder section at maximum angle leaving more than 5 m from the bottom of the ladder to the waterline. The vertical, rope pilot ladder was deployed from deck with the bottom step positioned about 1.4 m above the water.
Following the accident, PSC inspection found the pilot ladder defective, as, among other issues, the lower spreader was cracked (possibly due to contact from the launch during the transfer). The ship was detained by AMSA under the Navigation Act 2012, in part, due to deficient safe means of access to the vessel. The rope pilot ladder was replaced prior to the ship sailing from Australia and the deficiency was closed.
Lighting for the boarding area was provided by a portable floodlight mounted over the side at deck level and floodlights mounted on the ship’s starboard bridge wing (Figure 5). Deck lighting was also used to illuminate the work area on deck. Sunset was at 1723, and the ship’s crewmembers reported that there was sufficient lighting for the task.
Figure 5: Ship lighting for the starboard boarding area
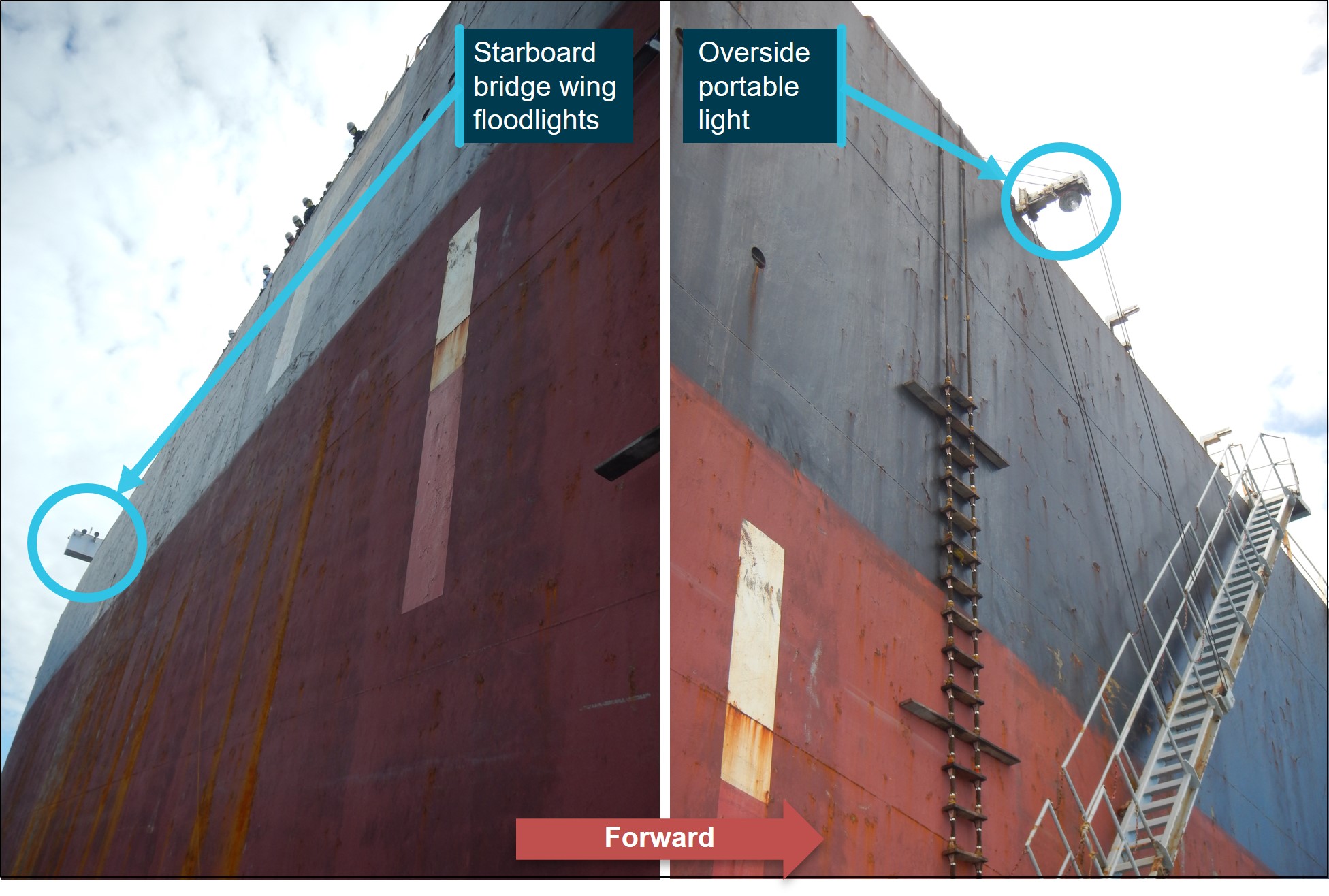
Source: AMSA with annotations by ATSB
Recorded data
Formosabulk Clement was fitted with a simplified voyage data recorder (S-VDR)[9] designed to collect and store data from various shipboard systems in compliance with regulations.
This system required crew action to ensure the data was saved following an incident where power was not lost. However, this procedure was not followed on this occasion and consequently the recorded data was not available to the ATSB. Bridge audio, radar data and rudder orders were not recorded.
Engine orders were recorded via the telegraph logger and printer fitted in the bridge console.
Pacific Tug
Pacific Tug (Aust) was a family owned and operated Australian registered company based in Victoria Point, Queensland, with operations in the Brisbane River and around Australia. The company began in 1965 and provided marine services including towage, salvage and personnel transfer. In 2022, the company had a fleet of 25 tugs, barges, support and crew transfer vessels.
Procedures
Pacific Tug maintained a company-wide operations manual within an integrated management system. This system included multiple procedures relevant to personnel transfer between vessels.
Risk assessment
The purpose of the risk assessment document was to provide clear and defined processes for the preparation and execution of a risk assessment at Pacific Tug workplaces. All workers involved in a task were required to actively participate in a risk assessment.
Risk assessments were required for activities which included new or non-routine tasks and prior to any complex task as required by legislation, regulations, standards and codes of practice.
Two types of risk assessments were described:
- A job safety environment analysis (JSEA) which detailed step-by-step how a task was to be carried out safely. The analysis considered:
- tasks—a step-by-step list of the basic activities of the task
- hazards—a list of potential hazards at each step of the task
- control measures—step-by-step instruction on how to safely carry out the task by controlling each identified hazard.
- A safe work method statement (SWMS) was also available. This statement detailed step‑by‑step how a task was to be carried out safely. It differed from a JSEA in that the SWMS was required, under Australian safety regulations, for all high-risk construction work.
In addition to other activities, Pacific Tug utilised PT Transporter for construction activities and both types of risk assessment were completed for the vessel. Personnel transfer between vessels was an activity for which a risk assessment was required.
Vessel transfers
The Pacific Tug fleet operations vessel transfers procedure aimed to provide clear and defined processes for boarding and disembarking from a vessel. The procedure outlined the master’s responsibilities and then provided guidance on transfer of personnel, including the importance of maintaining 3 points of contact and movement of personnel between a vessel and fixed wharf.
The master (skipper) was to ensure the safety of personnel during the transfer to and from the vessel. If the transfer was between vessels, the masters were to discuss and reach agreement beforehand regarding the person in charge of the activity (and on which vessel), with one person in charge at any one time.
Workers being transferred were to be briefed prior to the transfer and were to be familiar with the method of transfer. The procedure also advised, among other things, that:
- Before the transfer operation, the master was to designate who was responsible for the transfer. This designated crewmember was to be in charge of the actual transfer of the worker. No worker was to transfer onto, or off, the vessel until that crewmember considered it safe to do so and indicated that transfers may take place. Any doubt was to be resolved in consultation with the master before the transfer proceeded.
- A clear understanding of the meaning of all terminology used in the transfer should be established between all those taking part.
- Clear communications were to be established and maintained between the person conning the vessel and those assisting in the transfer.
- Only one person was permitted to transfer at a time.
- The vessels (where appropriate) should be manoeuvred to create a suitable lee and provide protection to the transfer site.
Permit to work
The Pacific Tug permit to work (PTW) procedure was to provide clear and defined processes for each type of activity requiring a PTW. A PTW was required for any non-routine activities and any activity deemed high risk (defined in the procedure as ‘An activity that is deemed to have potential risk or has hazards that may injure a worker or the potential to injure workers.’). Permits existed for work aloft or over the side and for lifting people, but not specifically for personnel transfer.
The PTW system was to identify, plan and control any hazardous tasks and promote worker accountability and responsibility for the task to be undertaken. Each PTW was to describe the high-risk work to be done and the precautions to be taken while doing it. It also highlighted the conditions to be met for the PTW and hence for the work to proceed.
The risk assessment completed for personnel transfer by launch did not identify that a separate permit to work was required.
COVID safe plan
In compliance with relevant legislation, Pacific Tug completed requirements put in place to respond to the COVID-19 pandemic. This included being a Queensland Government endorsed transport provider with an approved transport plan in place and Statement of Compliance for PT Transporter.
Customer interaction
Pacific Tug had processes in place for corresponding with customers (in this case this was via the agent) which included providing a package of standard information. This package included a schedule of rates, vessel specifications sheet and pandemic response requirements. It did not include Pacific Tug procedures or operational requirements relating to details of the transfer of persons from one vessel to another.
PT Transporter
PT Transporter (Figure 6) was an aluminium catamaran, built in 1996 and refurbished in 2019 with machinery and fit out changes and upgrades, including main engines and generator. The vessel had a cruising speed of 20 knots and was 11.9 m long, with a breadth of 4.80 m and draught of 1.20 m. It was an Australian domestic commercial vessel (DCV) regulated under the Marine Safety (Domestic Commercial Vessel) National Law Act 2012.
PT Transporter was in survey to class 1C,[10] certified to carry 2 crew and 23 passengers. It was designed, and predominantly used, for personnel transfer with the foredeck purpose-built for such. Since October 2019, PT Transporter had completed 51 personnel transfer operations, 39 of which were to outer anchorages.
Figure 6: PT Transporter
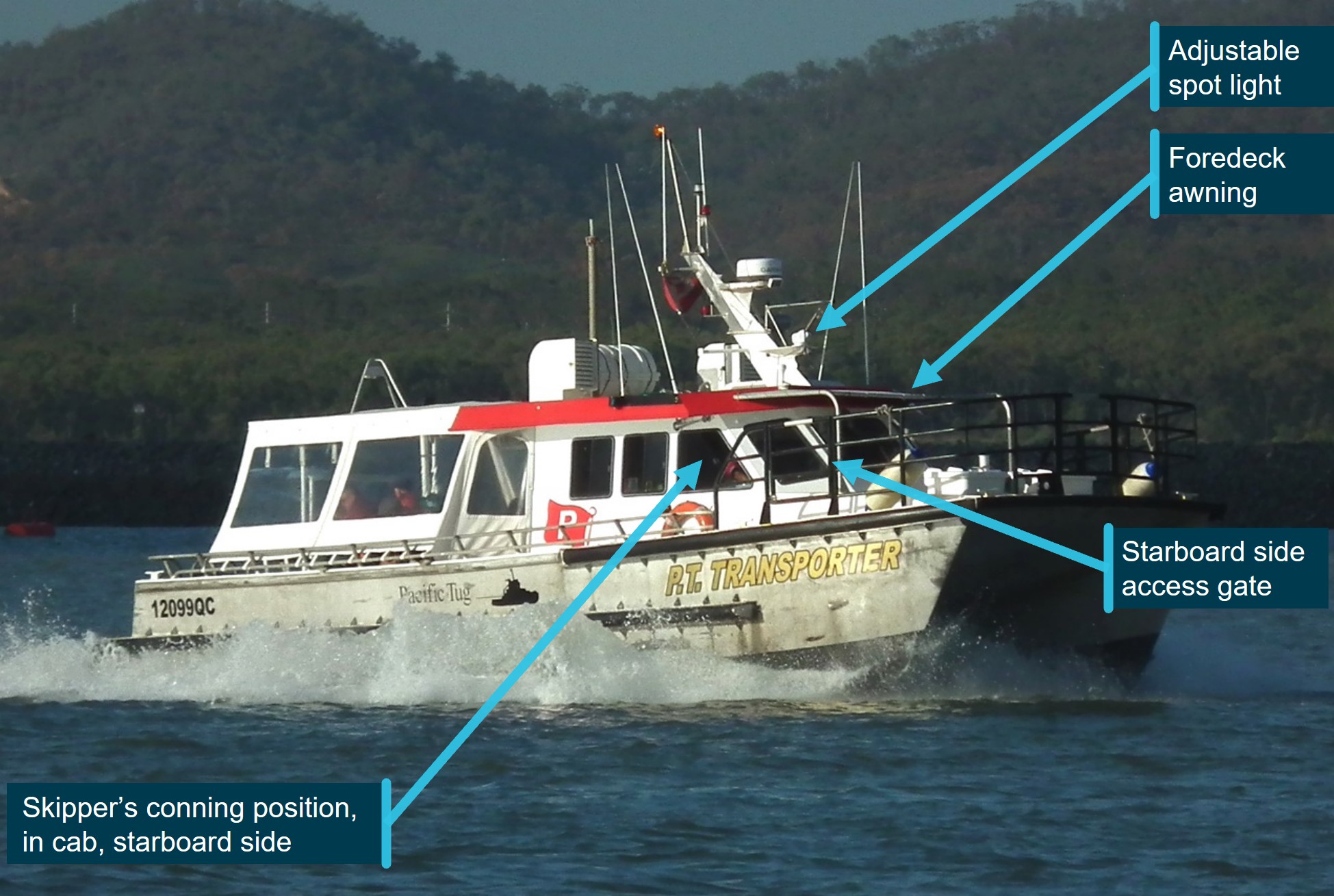
Source: Pacific Tug, annotated by ATSB
The vessel’s helm position was located to starboard of the centreline. The cabin layout combined with the foredeck awning limited the skipper’s view upwards, especially in close quarters such as when the launch was alongside the ship (Figure 7).
Crew
PT Transporter was certified with a complement of 2: master with minimum coxswain grade 1 certificate and an uncertificated deckhand.
PT Transporter’s master (skipper) had more than 15 years’ small boat experience in various locations around the coast of Australia. They had worked on several major construction projects as a crew boat skipper. At the time of this accident, they held valid certification as master <35 m near coastal and marine engine driver grade 2 NC (near coastal).
The skipper was employed with Pacific Tug on a contract/casual basis beginning in 2010 as a general-purpose deckhand with short periods as master of PT Transporter. In 2019, after time away, they were re‑employed as master of PT Transporter with stints in other vessels as deckhand and mate.
The deckhand commenced casual employment with Pacific Tug in June 2021 and had served in 4 vessels (total 8 days service), including the day of the accident. On 3 previous occasions the tasks had involved personnel transfer, all on board PT Transporter. The deckhand held a valid AMSA certificate of proficiency as an integrated rating.
Both crewmembers held a valid AMSA certificate of safety training. This was the first time they had worked together.
Figure 7: The view from PT Transporter’s skipper’s position at the helm

Source: Pacific Tug annotated by ATSB
PT Transporter specific procedures
The Pacific Tug operations manual included several procedures specific to the operation of PT Transporter.
Transfer of personnel job safety and environment analysis (JSEA)
A job safety environment analysis (JSEA) was completed in April 2020 for PT Transporter for the task of personnel transfer. This document identified that no permit to work was required and then identified hazards and risk control measures for steps within the task. Users were directed to the fleet procedure relating to personnel transfer.
Identified risk control measures included:
- clear communications
- assess vessel movement before commencing a transfer
- ensure sufficient lighting
- maintain communication between vessels at all times
- both launch personnel to monitor the sea conditions at all times
- the transfer was to proceed only after the skipper had given the ‘all clear’
- a lee was to be provided as necessary.
Both the skipper and deckhand of PT Transporter had signed multiple times that they had read and understood this document, with the most recent sign-offs less than 2 weeks before the accident.
General vessel operations job safety and environment analysis
This JSEA was for PT Transporter general operational activities. The risk assessment covered 14 identified activities, several of which were relevant on 9 August. In addition to general considerations, this included arrive at / depart another vessel, transiting, pushing up to another vessel, and transfer of personnel and belongings.
Hazards for each activity were identified, as were control measures. Common to the control measures were ensuring effective communication and ensuring all personnel understood the activity and their role in it.
The JSEA advised that for all vessel activities an ‘Operational Risk Assessment’ was required.
Safe work method statement (SWMS) for letting go / making fast—wharf or vessel
A SWMS risk assessment was completed in April 2020, for PT Transporter operations associated with construction activities identifying hazards and control measures related to the launch making fast to, or letting go from, another vessel. While not expressly applicable to the launch being manoeuvred alongside the ship, this risk assessment showed that relevant risk control measures were considered and applied to operations of this vessel. These included ensuring clear communication and instruction on the task sequence and between vessels, consideration of weather and sea conditions, and proceeding with the task under instruction of the master (skipper) and as per the planned sequence.
PT Transporter vessel safety training manual
This manual focussed on vessel‑specific safety training, equipment and firefighting arrangements with few references to operational procedures. Users were advised that this manual was in addition to the fleet operations manual which contained fleet standards and operating procedures including permits to work, work planning and hazard analysis.
PT Transporter Wellbeing Plan
This document outlined actions Pacific Tug would take to provide a consistent approach for the management of Safety, Health and Environmental (SHE) requirements. The document included details of crewmember responsibilities along with guidance on addressing the COVID-19 requirements at the time. To comply with Queensland Health guidelines, PT Transporter could accommodate 9 passengers and 2 crew.
PT Transporter COVID safe transport of quarantined persons plan
The Queensland Government’s Public Health Directions required that quarantining persons were moved to and from nominated quarantine premises by dedicated modes of transport. This required that the transport provider was endorsed by a government authority, with a Transport Plan in the form approved by the State’s Chief Health Officer. This was in addition to the in-house PT Transporter wellbeing plan.
Under PT Transporter’s approved transport plan, the vessel could safely transport 2 crew (housed in the cabin) and 13 passengers separately accommodated in the after deck seating area.
Daily pre-shift work plan
A daily pre-shift work plan for the vessel was completed on 9 August for a ‘crew run at the outer anchorage’. The work planned was for 8 persons on, 8 off Formosabulk Clement at the outer anchorage, departing from Rivergate Marina. This plan did not expand on this information or make mention of any related risk assessments or permits to work in the columns provided for such. Both crewmembers had signed the plan.
Provisional Pacific Tug procedures
As part of the company continuous improvement programme, at the time of the accident, an operational risk assessment procedure was being trialled for PT Transporter general operations. This provisional procedure included:
- A ‘Traffic light assessment’ system and criteria for operations. This system set the conditions used to determine the state of operations—safe, stop and assess, stop immediately and for re‑starting. This included environmental limitations:
- Operational requirements, which were separated into when the launch was approaching the ship and when alongside. Both situations mentioned communications between vessels and personnel. While approaching the ship the transfer process was to be communicated to and understood by transferring persons.
Weather
From arrival off Brisbane and throughout the day and into the evening of 9 August, the ship’s navigation watch officers recorded weather conditions as winds from the south-east at force 5[11] (17 to 21 knots, fresh breeze), moderate seas (1.25 to 2.5 m) on 3 m swell with good visibility and overcast conditions.
At the time of the transfer, the master observed that conditions were as above with waves about 2 to 2.5 m and a lee would have to be made for a safe transfer. Testimony of crewmembers on deck at the time was that conditions were windy and that the launch was noticeably moving.
Earlier in the day, as the launch skipper took command, the departing skipper reported that conditions on the bay were ‘not very nice’. Transit across the bay to the ship was made at better than 15 knots and while several of the passengers were sick, the launch crew were not and attributed this to the passengers’ being less experienced in small boats.
Once at the ship, the skipper observed that, with the boarding area exposed to the weather, the conditions were choppy and uncomfortable. The skipper requested the ship (master) provide a lee for the area. As the ship moved and when manoeuvred about the anchor, the conditions at the boarding site improved dramatically. The skipper was satisfied that the conditions, though not dead calm, were sufficiently smooth and comfortable to allow persons to board the ladder and went ahead with the personnel and luggage transfer onto the ship.
The deckhand stated that while choppy, the conditions on the bay and at the ship were similar to other times they had been out and that once in the shelter of the ship, the seas calmed and the launch moved up and down comfortably less than a metre.
Several government agencies, and others, maintain weather and sea monitoring equipment in the area around Moreton Bay and the port of Brisbane. Recordings obtained for locations nearby the anchorage position showed no abnormally high waves were recorded at this time. In the hour preceding the accident, significant wave heights varied from 1.1 m to 1.3 m with maximum wave height of less than 2.4 m recorded. The wave direction varied from 97° to 103°.
Winds were recorded as 10 to 20 knots from about 100° (varying from 70° to 120°).
COVID-19 pandemic
The first human case of a new (novel) coronavirus was identified in December 2019 and on 20 January 2020 the World Health Organization (WHO) issued the first situation report in relation to what was to become known as COVID-19. In response, countries implemented strict measures on the movement of people, including quarantine, isolation and lockdown requirements.
The escalating situation had a profound effect on the maritime industry and seafarers. By July 2021, the IMO estimated that some 250,000 seafarers remained on board commercial vessels, unable to be repatriated and past the expiry of their shipboard contracts. A similar number of seafarers urgently needed to join ships to replace them.[12]
Requirements of the MLC[13] limited the maximum continuous period of service on board ship to 11 months. However, as a consequence of the pandemic, in June 2020 AMSA issued a marine notice[14] allowing for extension of this period of service to 14 months maximum.
In November 2020, AMSA notified vessel owners, operators and seafarers that this extension would end on 28 February 2021.[15] At this time, crew change hubs were available in several major Asian ports including Hong Kong and Singapore. AMSA considered that industry had had sufficient time to adjust to the challenges of repatriation, and did not consider difficulties in finding a flight as an appropriate reason for an extension of a seafarer’s service onboard. Consequently, AMSA advised that from that date, the 11-month continuous service limitation as outlined in Marine Notice 17/2016 would be enforced.
The first case of the virus in Australia was reported on 25 January 2020, and on 20 March the international borders were closed to all non-residents and non-citizens and tight restrictions applied to movement of citizens.
Queensland
On 29 January 2020, Queensland recorded its first COVID-19 case. From 30 January, Maritime Safety Queensland (MSQ), via the vessel traffic service (VTS), increased vetting of vessels prior to pilot boarding. Then, on 25 March, border access restrictions were imposed which limited movement between States. In accordance with emergency powers arising from the declared public health emergency, the Queensland Chief Health Officer issued the first Border Restrictions Direction. Under these restrictions, anyone arriving into Queensland from another State or Territory had to self-quarantine for 14 days, unless they were an exempt person.
In July 2020, Queensland implemented the requirement for a maritime crewmember to comply with a comprehensive ‘Protocol for maritime crewmembers joining or signing off a vessel in Queensland’. The protocol contained instructions and requirements for crew joining or leaving a vessel including testing, quarantine and transport. The protocol required that a crew changeover checklist, endorsed by the regional harbour master (RHM), be completed for the joining crew and another for the departing crew. By June 2021 the protocol had been amended and updated to be version 10.
Also, in July 2020, MSQ established a liaison role to work with the Queensland State Health Emergency Co-ordination Centre to manage, among other roles, interaction between the health and shipping requirements. By mid-2021, a network of persons to assist and oversee crew change on behalf of RHMs and health authorities was in place. This included 2 full-time crew change assistants (CCA) based in Brisbane, 2 in regional ports and a hotel liaison officer based in Brisbane to manage accommodation and quarantining requirements.
In Brisbane, a 230-room hotel was designated for the primary use of maritime crew quarantine. From May 2020 to the end of July 2021, more than 9,000 mariners, from almost 1,500 ships, had changed through Queensland ports. About 4,500 had been through the port of Brisbane with less than 500 changed by launch to vessels at anchor.
At the time, a major Australia-based shipping industry representative body considered that crew changes were most easily conducted in Queensland and had provided that advice to members.
Quarantine corridor—crew changes in Queensland
To complete a crew change in Queensland, the shipping company’s representative (usually the local agent) applied to Queensland Health via a ‘Crew changeover checklist’ form. The form was submitted to the RHM who was acting on behalf of health authorities in this regard. In Brisbane, the CCA then assessed the application and the RHM approved the plan. The CCA responded to the applicant with information outlining the requirements to be met prior to, during and after the crew change.
Following the response from the CCA, communication followed in which the details of the crew change were revised, updated and approved as circumstances required. This included all travel and accommodation arrangements regardless of when these occurred—the first joining personnel for Formosabulk Clement arrived into quarantine in Brisbane on 13 July, almost 4 weeks before the ship arrived.
In this way, a ‘quarantine corridor’ was set up and maintained about any ship personnel travelling through Queensland. The CCAs kept oversight of the planning and progress. They ensured that plans were in place which ensured that a person remained quarantined from the point of arrival into Queensland until they boarded the ship, and vice versa. All steps within the corridor were assessed and approved. This extended to the CCA ensuring that all requirements were in place (for example, PCR testing and quarantine periods) to enable a departing person entry into their destination country.
This system thereby provided the flexibility and security to enable continuing crew changes within the dynamic circumstances created by the pandemic.
COVID safe transport plan
Queensland Government’s Public Health Directions required that quarantining persons were moved to and from a nominated quarantine premises by dedicated modes of transport. In certain circumstances, quarantined persons were required to travel with a transport provider endorsed by a government authority, with a Transport Plan in the form approved by the Chief Health Officer. To fulfill this requirement, transport providers developed a Transport Plan using a template and sought endorsement to operate from the Department of Transport and Main Roads (DTMR).
The purpose of the Transport Plan was to document the practices that would be applied by transport providers to keep themselves and the community ‘COVID safe’. It contained the minimum standards of practice that must be met by transport providers when offering a service to quarantined persons.
Pacific Tug was a Queensland Government endorsed transport provider with an approved transport plan in place and Statement of Compliance for PT Transporter.
Safety analysis
Introduction
In 2021, the COVID-19 pandemic and the response of international shipping to manage it created challenges for ship crew changes. In the case of Formosabulk Clement, this resulted in the ship diverting to Brisbane to conduct a change of long‑serving crewmembers on 9 August 2021. With the ship at anchor, the crew change was being conducted via a combination pilot ladder from the crew transfer launch, a much smaller vessel about 16 m below the ship’s deck.
The transfer was conducted in the early evening on the ship’s starboard side, the leeward side from time to time as the ship yawed at anchor in the rough sea conditions. The ship’s main engine was also used to maintain a lee and, by 1833, the 8 joining crewmembers (and their luggage) had safely boarded the ship.
Meanwhile, the ship’s master was expecting the launch, having moved off, to wait until the ladder was in the ship’s lee again and the master had asked the launch to return. The master knew the starboard side was exposed to the weather and that making a lee using the ship’s engine would take some time and planned to resume the crew transfers once there was a good lee. However, the language difficulties experienced combined with other tasks in this busy period resulted in the master not being able to communicate this plan to the skipper of the returning launch.
At the same time, the departing chief mate (dCM) climbed onto and down the pilot ladder in anticipation of boarding the launch. Neither the ship’s master nor the launch skipper was aware that the dCM had descended the ladder. In addition, the deckhand did not know that the skipper only intended to assess conditions, not to embark anyone. The deckhand saw the dCM on the ladder, directed them clear of the approaching launch and anticipated signalling readiness when it was safe to board.
However, neither the skipper nor the deckhand nor the dCM recognised the significance of the rough seas and swell running along and against the ship’s starboard side resulting in larger and higher waves. Consequently, they did not expect the launch to be lifted higher than previously experienced while alongside. A large wave, however, lifted the launch high and it struck the dCM, who fell into the water. The dCM was recovered but had been fatally injured.
Weather and making a lee
While the weather conditions at the time with rough, choppy seas exceeded limits defined in both ship and launch procedures for operations in open waters, conditions in the lee of the large ship were sufficiently benign to allow safe personnel transfers. The ship’s main engine was also used to effect to make a lee on the starboard side as the anchored ship’s heading swung through its natural yaw. This provided 15-minute windows for safe transfers, and the accident occurred outside one of these windows while the master was attempting to make a lee.
Communications
Clear, unambiguous communications within and between workgroups are essential for the safe completion of any task. Specifically, this ensures that all participants:
- have a shared understanding of the task, of what is expected and what is about to happen
- know and understand their input into that task as well as their individual, and team, roles and responsibilities.
Formosabulk Clement’s personnel transfer required active and adaptable communications at all stages of the planning, co-ordination and control of the high-risk task. Difficulties maintaining optimal communications can arise with personnel who have not previously worked together, increased workgroup size, multiple workgroups of differing skill sets, multiple worksites, and different languages. These factors complicated the task on 9 August.
The personnel transfer operation comprised crew with roles and responsibilities in 4 closely linked, but distinct locations:
- ship’s bridge
- ship’s deck
- launch cabin
- launch deck
The crew in these locations were central to the co-ordination and safe management of the transfer, and safe completion of the task required clear communication between all of them. They were all aware of the overall objective and sequencing for the transfer but details of their individual and common plans for each step were not shared and agreed.
Multiple communication breakdowns occurred, resulting in the responsible crew at each location being unaware of the intentions or expectations of those at the other locations.
For example:
- On the ship’s bridge—the master intended to manoeuvre the ship to re-create the lee and did not expect the launch to return alongside and did not know its skipper’s intentions.
- On the ship’s deck—the dCM changed the departure plan, without informing others, including the master, and left the deck first. The intentions and expectations of the dCM were not known to anyone on the ship or the launch.
- In the launch cabin—the skipper planned to bring the launch alongside and assess conditions before allowing anyone to board. They did not expect anyone to be on the pilot ladder.
- On the deck of the launch—the deckhand was unaware of the skipper’s intention to only assess conditions. The deckhand expected boarding to take place once the launch was alongside and stable.
The opportunity to discuss the next phase of the operation while the launch was stood off from the ship was not taken. Had that time been utilised by the various participants to discuss and agree the next phase, the conditions would likely then have been favourable due to a lee and the dCM would have probably not been in the position they were at the time of the accident.
On this occasion, key personnel misinterpreted the actions and intentions of other parties. Both ship and launch crew assumed those on the other vessel understood what was happening and about to happen and were experienced in the transfer operation from each other’s perspective.
Pre-task information sharing and task understanding
The decision to conduct the personnel transfer was made several weeks before the event. There were explicit procedural requirements to seek and discuss operational requirements prior to the transfer, at least on the part of Formosabulk Clement. However, neither Formosa Plastics Marine Corporation (FPMC) nor Pacific Tug (PT) had specific guidance in place regarding the content of, or timing for, information to share with third parties regarding the specifics involved in the transfer of personnel to or from company vessels.
As a consequence, other than information related to the procedures and protocols required by shore agencies to prevent transmission of the COVID‑19 virus, only generic particulars such as time, location and boarding ladder positioning were exchanged in the lead up to the event. This in turn led to a situation where misunderstandings in, and differences between, plans could only be clarified while the transfer task was underway.
English is the international language for ship-to-shore communications[16] and masters and mates are required to demonstrate competence in its use.[17] Problems with language, translation and interpretation are known risks in international shipping that were not adequately mitigated on this occasion. Limitations of the ship’s officers’ English language ability were exposed when attempting to communicate complicated details of a dynamic situation, over radio, in a busy, noisy environment. In this case, the launch skipper resorted to enlisting the passengers to assist communications with the ship’s master in their native language. However, this removed the skipper from the communication loop and from developing a proper understanding about what the ship’s master and crew would do.
In general, standard procedures on both the ship and the launch emphasised the importance of establishing and maintaining effective communications, including communicating plans, requirements and expectations for the activity. However, the evidence indicates that there was no common or complete understanding of how the transfer would be conducted either within, or between, the crew of either vessel.
Formosabulk Clement
Multiple procedures on board Formosabulk Clement were in place for crew change operations. Crewmembers completed risk assessments and held meetings to share details, roles and responsibilities of the task. This provided the opportunity to reduce misunderstanding or miscommunication between those involved on board the ship.
Procedures also required a toolbox talk prior to the task and the crewmembers involved in the transfer recalled discussions prior to arrival and commencing the task. However, their different versions and details of those discussions did not indicate that the required distinct, formalised toolbox talk took place, potentially reducing its effectiveness.
Procedures also required that the launch’s risk assessment be obtained and discussed on board but this was not done. Consequently, the plans and discussions relating to the task were imprecise and did not include detail of how an individual was to safely transfer between the vessels and how this was to be controlled and co-ordinated. This contributed to the master losing understanding of what was happening on the ship’s deck and what the launch was doing and why. Most significantly, the dCM left the deck first and climbed down the pilot ladder without the master’s knowledge or approval.
Pacific Tug
Pacific Tug (PT) had considerable experience in conducting personnel transfers with procedures to support these operations. However, PT had not ensured that all involved personnel, within the company and external parties (such as ship masters), had an agreed, clear and complete knowledge and understanding of how this process would occur and progress.
- the approaching launch was probably mistaken by the dCM as a signal to climb down the ladder in preparation to disembark
- the master did not understand why the launch was returning before a lee had been provided and before being requested to return
- the deckhand took it as confirmation that crew transfers were resuming.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
The following findings are made with respect to a crewmember’s fatal fall from Formosabulk Clement’s pilot ladder during crew transfer operations with the launch PT Transporter on 9 August 2021.
Contributing factors
- Formosabulk Clement’s departing chief mate climbed down the vertical pilot ladder intending to board the crew transfer launch. They did this without the knowledge of the ship’s master or the skipper of the launch.
- After the ship's master had manoeuvred the ship to create a lee and embark the joining crew from the launch, the ship yawed about the anchor, which exposed the transfer area to the prevailing weather.
- Immediately before the accident, there were difficulties in communicating between the ship’s bridge and the launch. As a consequence, the main engine was not used to re-create a lee before the launch came back alongside the ship, and the transfer location was exposed to the weather.
- A wave, larger than previously encountered, lifted the transfer launch higher than expected and sufficient to make contact with the departing chief mate, knocking them into the water.
- On board Formosabulk Clement, communications plans and protocols for the crew transfer operation had not been sufficiently well implemented and agreed to ensure that deck and bridge personnel maintained awareness and understanding of what was occurring and what was about to occur.
- On board PT Transporter, communications arrangements had not been sufficiently well implemented to ensure that events occurring as the crew transfer process progressed were clearly understood and agreed between its skipper and deckhand.
- Neither vessel’s managers had ensured that the involved personnel had a common and complete understanding of how the personnel transfer would be conducted with respect to aspects including:
- outlining task steps, limits and triggers such as agreed permissions for vessel movements
- setting operational limits
- defining terminology for key transfer-related communications.
The opportunity was not taken to share information well beforehand, which would have allowed differences to have been addressed and a single plan developed and agreed before the task was underway.
Safety action
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Pacific Tug
Pacific Tug (PT) informed the ATSB that the company immediately ceased personnel transfer operations after this accident until a comprehensive review of such operations was conducted. PT sought a system of communication less constrained by language and amenable to being shared beforehand to assist in achieving the shared mental model of the task among all participants.
To that end, PT designed and implemented a traffic light system (red, amber and green states) for control of 2 separate aspects of the transfer process:
- operational status—through the updated ‘operational risk assessment for personnel transfers to/from a PT vessel’ a range of preconditions were set which need to be met before the planned operation could commence. These preconditions included the setting of weather limits for each state as well as requirements on all involved vessels and crewmembers. The weather parameters are set prior to the launch leaving the wharf and then assessed against at the transfer location.
- transfer status—indication of the status of the transfer as it is occurring and controlled by the crew of the transfer launch.
- Green—transfers can occur as guided by launch crew
- Amber—transfers to stop, personnel make safe, reassess conditions to determine next steps
- Red—the transfer operation is stopped and not to recommence until the operational status preconditions are reassessed and met.
Transfer of personnel can only commence when both statuses are green, and masters of both vessels have agreed on the process and given permission.
PT procedures required that the operational risk assessment and a ‘personnel transfer procedure poster’ were shared with the vessel requiring the transfer of personnel. The poster outlined the traffic light system and actions to take in each situation. The masters of involved vessels, all personnel transferring and anyone assisting in the transfer were to provide confirmation that they understand and agree to the transfer protocols.
It was also emphasised that the master of the crew change vessel was to be in ultimate control for all transfers.
These procedural changes were supported by modifications to the launch (PT Transporter) through the fitting of red, amber and green indicator light sets: one in the passenger area and a second on the main mast. These light sets were designed to show the status of the transfer to persons on board both vessels. The launch crew (master and deckhand) each have remote controls for the lights.
During an extended transfer (many persons), the status was able to alternate between amber and green only. Red required a complete termination of the operation.
This personnel transfer process was further supported by updating of procedures including those for:
- Risk assessment
- Operational risk assessment for personnel transfers to/from a PT vessel
- Personnel transfers
Formosa Plastics Marine Corporation
Following this accident, Formosa Plastics Marine Corporation (FPMC) notified the ATSB that the company had:
- completed on board training and reassessment of risks relating to transfer of personnel to and from small vessels, including pilots
- conducted investigations via a third party and internally
- shared lessons learned throughout the FPMC fleet including a fleet circular outlining precautions for crew change at anchorage
- amended the ‘personnel transfers procedure at sea’
- held company safety meetings, including to senior shore management, to discuss the accident and outcomes.
Maritime Safety Queensland
Maritime Safety Queensland (MSQ) amended the COVID crew change procedure for vessels at anchor following the accident. The changes included that:
- all crew transfers were to be conducted during daylight hours only, commencing after sunrise, completing before sunset
- weather conditions were to be appropriately risk assessed by those involved prior to conducting the transfer
- both the ship and the transfer vessel were to be provided a copy of the Maritime Safety Awareness Bulletin September 2019 – Safe Access to Vessels.
- the transfer operations were to be appropriately risk assessed considering the competency and ability of all involved personnel (ship and launch) to complete transfers between vessels.
These conditions remained in place until COVID restrictions were eased in 2022.
Glossary
| Beaufort scale | The Beaufort scale of wind force, developed in 1805 by Admiral Sir Francis Beaufort, enables sailors to estimate wind speeds through visual observations of sea states. |
| COVID-19 | Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus. (World Health Organisation—WHO) |
| Freeboard | The vertical distance between the waterline and the ship’s main deck. |
| ILO | International Labour Organisation. (www.ilo.org) |
| IMO | International Maritime Organization. (www.imo.org) |
| Lee | this side or part of the ship that is sheltered or turned away from the wind |
| MLC | Maritime Labour Convention. The Maritime Labour Convention, 2006, as amended, (MLC), was adopted on 23 February 2006. and became binding international law on 20 August 2013. By December 2019 it had been ratified by 96 countries. |
| SMS | Safety management system. A systematic approach to organisational safety encompassing safety policy and objectives, risk management, safety assurance, safety promotion, third party interfaces, internal investigation and SMS implementation. |
| SOLAS | The International Convention for the Safety of Life at Sea, 1974, as amended. |
| STCW Code | Seafarer’s Training, Certification and Watchkeeping Code, International Maritime Organization, 1995. |
| VTS | Vessel traffic service. A VTS is any service implemented by a competent authority, designed to maximise the safe and efficient movement of water borne traffic within the jurisdiction. In Brisbane, VTS was the principal system by which the Regional Harbour Master managed the safe and efficient movement of vessel traffic approaching, departing and operating within the Brisbane VTS area. |
| Yaw | The ship’s head swinging from one side to the other. |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the master and crewmembers of Formosabulk Clement
- the skipper and deckhand of PT Transporter
- Formosa Plastics Marine Corporation
- Pacific Tug
- Wave Shipping
- LBH Australia
- Maritime Safety Queensland
- Australian Bureau of Meteorology
- Queensland Police Service
- Australian Maritime Safety Authority
- Marine Investigation Department of the Liberian Registry
- Queensland Department of Environment and Science
- Aus Ship P&I
- Wilhelmsen Ships Service
- Bhagwan Marine
- Citizens Radio Emergency Service Teams
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the skipper and deckhand of PT Transporter
- Pacific Tug
- Formosa Plastics Marine Corporation
- the master of Formosabulk Clement
- Maritime Safety Queensland
- Australian Maritime Safety Authority
- Marine Investigation Department of the Liberian Registry
Submissions were received from:
- the skipper of PT Transporter
- Pacific Tug
- Formosa Plastics Marine Corporation
- Maritime Safety Queensland
- Australian Maritime Safety Authority
- Marine Investigation Department of the Liberian Registry
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Limited to 11 months by the Maritime Labour Convention, 2006 (MLC), Regulation 2.4—Entitlement to leave and Regulation 2.5—Repatriation. The MLC provides the basic requirements for seafarer’s welfare regarding working and living conditions during employment. (www.ilo.org)
[2] All times referred to in this report are local time, Coordinated Universal Time (UTC) + 10 hours.
[3] A nautical mile (mile) of 1,852 metres.
[4] Rivergate marina and shipyard is located in the Brisbane River about 10 miles upstream from the entrance beacons.
[5] A signal from the bridge to the engine room (usually via the engine telegraph and verbally confirmed) that the main engine is no longer required and it and its ancillary systems can now be shut down and cooled as required.
[6] Bridge logbook recorded weather throughout the afternoon and evening as fresh south-easterly breeze (force 5—17 to 21 knots) and moderate seas (waves to 3 m, swell to 4 m)
[7] Sunset was at 1723 local time.
[8] Polymerase chain reaction testing or PCR testing was the type of test done most often in Queensland when testing for COVID-19. PCR testing looked for the genetic material of the virus in a sample taken from the person. As this test looked directly for the virus, it was the most accurate test for seeing whether a person was infected with the virus at the time the test was taken. (Queensland Health)
[9] The voyage data recorder for a cargo ship larger than 3,000 gross tons, constructed before July 2002 may be an S‑VDR.
[10] DCV class 1C—vessel use 1: Passenger vessel (13 or more passengers), operational area C: Restricted offshore operations: within 30 miles or 50 miles depending upon the area of Australia in which the vessel operates.
[11] The Beaufort scale of wind force, developed in 1805 by Admiral Sir Francis Beaufort, enables sailors to estimate wind speeds through visual observations of sea states.
[13] MLC 2006 Regulation 2.4—Entitlement to leave and Regulation 2.5—Repatriation
[14] AMSA marine notice 04/2020, superseded by MN 10/2020.
[15] AMSA marine notice 10/2020 issued 11 November 2020.
[16] SOLAS Chapter 5: Safety of Navigation, Regulation 14: Ships’ manning
[17] STCW Code Part A, Chapter II: Standards regarding the master and deck department