
Executive summary
What happened
On the morning of 19 December 2021, a Rockwell Commander 114, registered VH-WMM, departed Redcliffe aircraft landing area, Queensland for a private flight. On board were a pilot and 3 passengers. Shortly after take-off, the engine lost power and the pilot elected to return to the airfield. During the return, the aircraft lost altitude and impacted the ocean before becoming inverted. The occupants were unable to escape the aircraft and were fatally injured, and the aircraft was destroyed.
What the ATSB found
The ATSB found that during preparation for the flight, a perceived engine problem distracted the pilot during the conduct of pre-take-off checks. After rectifying the issue, the pilot did not complete the remaining pre-take-off checks (including fuel tank selection) before departure. Before take-off when there was no time pressure (and during the inflight emergency when there was), checks and action items were only done by memory rather than using the pilot operating handbook or third‑party checklists also on board.
While stored in the hangar, most of the fuel moved into the right wing tank. The pilot would have been aware of the fuel imbalance from measuring fuel in both tanks via a dipstick before flight. However, it was likely that the fuel tank selection prior to take-off was to the left fuel tank only, which led to fuel starvation and engine stoppage soon after take-off.
The pilot, likely experiencing the effects of stress and time pressure following the engine power reduction and then stoppage, did not conduct initial emergency actions and attempted to return to the runway for landing. However, the pilot did not maintain glide speed, and the aircraft impacted shallow water prior to reaching the airfield. During the return to the airfield, the pilot had extended the undercarriage for the intended landing. This contributed to the aircraft inverting when it collided with water. This likely resulted in occupant disorientation and added difficulty in operating the exits, reducing their ability to escape.
It is very likely that the passengers did not receive information about the brace position or actions to be taken in the event of a ditching as part of the pre-flight briefing. In the limited time available inflight after the power loss, the pilot also did not provide an emergency briefing or any instructions to passengers prior to impact with the water.
While the pilot was primarily responsible for the operation of the aircraft exits in an emergency, seating a child, who may require assistance, adjacent to an exit instead of an adult meant that a less suitable passenger was available to operate the exit.
Safety message
Use of the approved aircraft checklists, taken from the pilot operating handbook, provides pilots with the appropriate checks to be conducted for the aircraft type. Having these readily available in a written form, for the preparation and conduct of a flight, provides pilots with the detailed normal and emergency checks specific to the aircraft type without having to rely on committing these to memory. This ensures that aircraft are operated in a way that meets aircraft flight manual requirements and limitations.
Distraction can impact proper procedural processes and lead to interruption and omission of safety critical elements before take-off. The habit of restarting an interrupted checklist from the beginning is a means of ensuring that all steps to be performed are done so in order and the checklist is complete.
Proper fuel management will ensure fuel supply to the engine(s) remains uninterrupted at all stages of flight. The ATSB publication, Avoidable Accidents No. 5 - Starved and exhausted: Fuel management aviation accidents (AR-2011-112) outlines strategies and key messages for fuel management.
Thorough pre-flight briefings of passengers on how to operate exits, the brace position and actions that might be required in a ditching or other forced landing are essential to increase post‑impact survivability. Additionally, as supported by guidance, pilots should consider who might be best to assist in the case of an emergency, and brief and seat them accordingly.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is: Reducing the severity of injuries in accidents involving small aircraft.
The investigation
| Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On the morning of 19 December 2021, at the Redcliffe aircraft landing area, Queensland, a Rockwell International 114 aircraft, registered VH‑WMM, was being prepared for a local private flight under visual flight rules.[1] On board for the flight were the pilot and 3 passengers. The weather conditions and visibility were good, with light winds from the east.
Closed circuit television (CCTV) showed the pilot conducting a pre-flight inspection of the aircraft. This included draining a small amount of fuel from each fuel tank drain to check for any water contamination and using a dipstick to check the fuel tank quantity of each tank.
A passenger video (see Appendix - Sequence of events) was recovered from a mobile phone which showed portions of the taxi, before take-off checks, and the accident flight. Several witnesses at the airfield, in boats near the airfield, and in other aircraft also observed the flight of VH-WMM (Figure 1).
Before the take-off, passenger video showed the pilot conducting before take-off checks (from memory) and did not show the use of any written checklists. While conducting the engine run-ups, the pilot perceived a technical difficulty with the aircraft, and the checks were paused. After notifying a ground crew member by phone, the pilot taxied back toward the ground crew who was walking towards the aircraft on the taxiway. The ground crew member recalled that through hand signals, the pilot identified the issue as misidentification of the mixture control for the propeller pitch control and communicated that they had identified and corrected the problem.
The pilot then taxied again for runway 07 without continuing or restarting the interrupted before take-off checks and continued direct to the runway holding point. The occupants of VH-WMM then discussed where other traffic was in the circuit, before entering and backtracking to the end of the runway. VH-WMM then turned and commenced the take-off at 0908 local time.
After take-off from runway 07,[2] the aircraft’s undercarriage and flaps were retracted, and 62 seconds later, while in a left climbing turn, the engine RPM started to fluctuate, followed by a large drop in engine power 3 seconds later. The (adult) passenger, seated on the rear-right side of the aircraft then asked the pilot about fuel coming out of the top of the right wing; however, the pilot did not respond to the question. The video also did not indicate the pilot conducting any engine troubleshooting activities. The pilot made 2 further left turns, which were consistent with manoeuvring the aircraft back toward the western end of runway 07 (Figure 1), and the stall warning sounded twice. About 17 seconds after the power reduction (1 minute 31 seconds after take-off), the engine stopped.
Four seconds later, the video recorded the undercarriage warning bell followed by the stall warning. Based on the recorded sounds, it is likely the pilot responded by lowering the landing gear. Another pilot who was on final approach for runway 07 heard the pilot of VH-WMM broadcast on the radio that they were returning to the airfield.[3]
Figure 1: Redcliffe aircraft landing area and VH-WMM approximate flight path and accident site
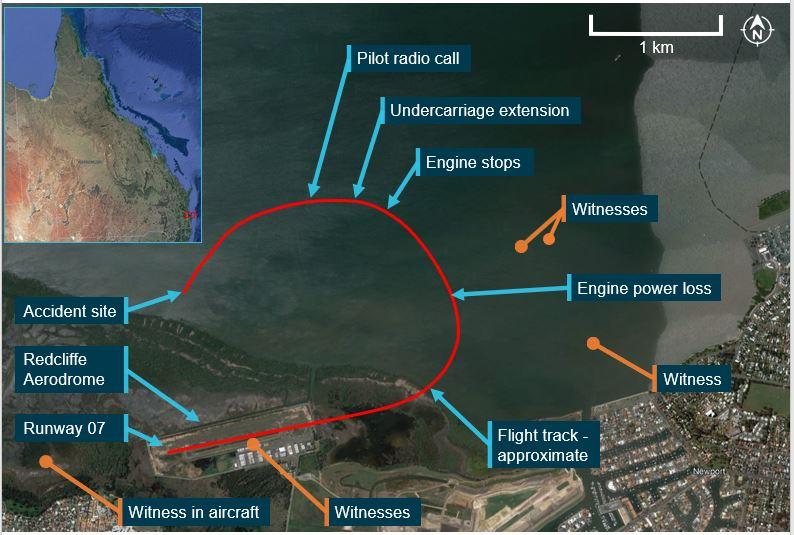
Source: Google Earth, annotated by the ATSB
Over 24 seconds, the stall warning sounded another three times, followed by a turn directly toward the runway and then further stall warnings, two successive drops of the right wing and then the sounding of the ‘stall’ voice alert.
Three seconds later, as the aircraft neared the mangrove tree line to the north of the airfield, it contacted the water, about 170 m from the shoreline. The aircraft overturned and came to rest inverted in about 2 m of water.
The pilot of another aircraft that was inbound to Redcliffe who had also heard the pilot of VH‑WMM make the returning to the airfield call, was alerted to the possibility of an accident from an unknown person on the radio upon arrival. After observing an aircraft in the water, the pilot contacted Brisbane air traffic control (ATC) to advise them of the accident. The pilot remained overhead the accident site while boats arrived at the scene and continued relaying information to ATC.
Witnesses at the airfield and on nearby boats contacted emergency services and the Australian Volunteer Coast Guard. After being notified by a witness on a kayak, a nearby vessel made its way to the aircraft, arriving about 5 minutes after the accident. Following the impact with water, the inverted orientation of the aircraft meant that the door handles were submerged. First responders reported that it was difficult to locate the handles to open the doors from the outside. When inverted on the seabed in mud and silt, the upper door latches were also unable to be located. The disturbance of the mud/silt further reduced visibility of the exits and their operating handles.
A coast guard vessel arrived onsite; however, the crew were also unable to gain access into the aircraft’s cabin. Queensland Police Service divers arrived at the aircraft about 2 hours after the accident. They observed the water to be about 1.5 m deep. Upon entering the water, police observed that visibility was very poor. The pilot’s door was shut and could not be opened. The right door was unlocked and slightly ajar, and police were able to open the door with some difficulty. The pilot and 3 passengers were fatally injured, and the aircraft was destroyed.
Context
Pilot information
The pilot held a valid Private Pilot Licence (Aeroplane) and a Class 2 aviation medical certificate, valid until February 2023. The pilot held single and multi‑engine aeroplane ratings and endorsements for manual propeller pitch control, retractable undercarriage, and formation flying. At the time of the accident, the pilot had logged 334.3 hours in VH-WMM and had about 505 hours total aeronautical experience.
The flight instructor who conducted the pilot’s last flight review in July 2021 stated that the pilot was assessed on engine failure after take-off. They also described that the assessed procedures on that review were similar to the accident flight, insofar as location of engine power loss and the actions that were to be taken as a result. During the flight review, the pilot had performed all actions to a satisfactory level.
Pilot medical history
A review of the pilot’s Civil Aviation Safety Authority (CASA) medical file identified that the pilot had disclosed a hypertension condition and that they had been prescribed medication for it but did not list any other health issues or concerns.
Discussion with the pilot’s next-of-kin and general practitioner (GP) identified that the pilot was a long term, type 2 non-insulin dependent diabetic. The pilot had been prescribed medication for at least 10 years with medical records indicating tracked blood glucose readings back to January 2003, and an immediate family history of non-insulin dependent diabetes. The pilot had also been diagnosed with high cholesterol and had been prescribed medication for its treatment. The GP was also aware of a family history of heart disease.
Of the last 3 CASA aviation medical examinations, the pilot had not declared their high cholesterol, diabetic status, and diabetes medication to their CASA designated aviation medical examiner (DAME), however had disclosed family history of both diabetes and heart disease to the DAME. Regarding the question in relation to diabetes on the pilot’s pre-examination medical history, the pilot indicated ‘unsure’, which was later changed by the DAME to ‘no’ during the examination.
Toxicology reports showed that the pilot of VH-WMM had detectable quantities of several substances, including a prescribed medication, paracetamol, and an over-the-counter sedating antihistamine. A carbon monoxide concentration of less than 5% was also detected in the analysis.
The ATSB sought advice from a specialist toxicologist regarding the potential effects the detected substances may have had on the pilot during the accident flight. The advice indicated that the level of antihistamine detected in the samples was low and suggested the drug had been used between 12 and 24 hours prior to the accident. They also reported that although the medication the pilot had been prescribed may have increased the sedating effects of the antihistamine, given the low levels detected it was unlikely there was any significant impairment of the psychomotor skills[4] required to fly an aircraft.
The specialist toxicologist also identified that there may have been an interaction between the multiple antihypertensive medications that the pilot had been prescribed[5] to lower blood pressure. However, from the passenger video it was noted that the pilot did not appear to be physically incapacitated, so it is very unlikely the pilot experienced any form of incapacitation prior to the accident.
Aircraft information
General information
The Rockwell International 114 is a 4-seat, single-engine aeroplane with fully retractable, trailing link undercarriage. It is powered by a 6-cylinder Lycoming IO-540 fuel-injected engine and is fitted with a 3-blade constant-speed propeller. Passenger and pilot access is by a door on each side of the aircraft cabin (Figure 2).
VH-WMM was manufactured in the US in 1977 and was first registered in Australia in May 2013. The last periodic inspection was conducted on 7 July 2021. At the time of the accident, VH-WMM had accrued a total time in service of 3,431.4 hours and had flown about 11 hours since the last inspection.
Figure 2: VH-WMM

Source: Nathen Sieben, annotated by the ATSB
Fuel system
The Rockwell 114 fuel system consists of 2 integral (wet wing)[6] fuel tanks, 1 in each wing, with a fuel gauge for each tank located in the cockpit. The fuel capacity is 132.5 L for each tank, with 128 L considered usable. Both fuel tanks supplied the engine through the fuel selector, gascolator,[7] electric fuel pump and an engine driven fuel pump. The fuel selector valve had 5 positions, which allowed the pilot to select OFF, LEFT, BOTH, RIGHT and OFF positions.
The last refuelling of VH-WMM occurred before a flight on 16 October with an uplift of about 120 L of AVGAS, taking the total quantity to about full tanks. VH-WMM was then operated for about 2.2 hours over 2 flights, prior to the accident flight. On the day of the accident, the ATSB calculated that about 115 L of fuel remained on board, equivalent to about half tanks.
CCTV at Redcliffe airfield showed that prior to the flight, the wings of VH-WMM were not level while parked on the tarmac. The right wing at the tip was about 60 cm lower than the left, indicating a fuel imbalance, where the right wing contained a greater fuel quantity than the left wing. The right-wing low condition indicated that fuel crossflow from the left to right fuel tanks may have occurred while VH-WMM was hangered.
It is a known issue with the Rockwell International 114 that when the fuel selector is not placed in the OFF position when parked, fuel can flow from one tank to the other. Once a crossflow has started, the increasing fuel weight will also increase the lean of the aircraft, further promoting the fuel crossflow. This results in further uneven fuel distribution, and sometimes an overflow of fuel through the wing tank fuel vents when this imbalance fills one tank completely. The ‘local fix’ amongst the Rockwell 114 community to prevent the crossflow was to set the fuel selector to OFF when the aircraft was parked for an extended period of time. The possibility of fuel crossflow in VH-WMM was also known to the pilot.
A review of the aircraft’s logbooks showed that in April 2011, a maintenance intervention was performed on the fuel system due to a crossflow defect occurring when the fuel selector was set to BOTH fuel tanks. The fuel selector position of VH-WMM was unknown prior to the day of the accident, however it is likely that it was not selected to the OFF position.
Undercarriage system
The Rockwell 114 is equipped with a hydraulically operated undercarriage. The aircraft is fitted with an undercarriage warning system. A switch is mounted on the throttle quadrant which connects to an undercarriage warning bell, activating whenever the throttle is brought to idle while the undercarriage is retracted.
Stall warning
The Rockwell International 114 is fitted with an aural stall warning system, that provides an audible tone to indicate that the aircraft speed is slowing to a speed that it can no longer produce lift in flight.
On board video recorded the stall warning sounding 13 seconds after the engine experienced the large drop in power. The stall warning continued sounding intermittently throughout the remainder of the flight, indicating that the aircraft was only marginally maintaining airspeed above the stall speed. The stall warning horn activated multiple times during the final approach until impact with water. This indicates that the aircraft would have been within 3-4 kt of the straight and level flapless stall speed of about 63 kt.
VH-WMM was also fitted with a voice alert system. This unit was an electronic device which detected the activation of the existing aircraft stall and undercarriage warning systems. It was configured to place a voice warning directly into the pilot headset and through a built-in speaker in the unit itself. In this situation, a pilot who may not hear the aircraft-generated stall warning horns because of noise cancelling headsets, will have an electronic voice annunciation of the warning.
A witness who had flown with the pilot previously described the system as functional and that it was an effective warning tool. The passenger video detected one annunciation of ‘stall’ from the built-in speaker, just prior to impact. It is unknown if the system was alerting the pilot through the headsets during the flight, however it is likely that the system was functioning, as other pilots who had been on board for previous flights had observed its operation.
Engine information
The engine fitted to VH-WMM was last overhauled in July 1998 and had accrued about 988 flight hours in operation. The overhaul schedule as listed in Lycoming Service Instruction SI 1009BE was 12 years or 2,000 hours, whichever occurred first.
Although the engine had exceeded the calendar schedule of the manufacturer’s time between overhaul, this was permissible when the engine was maintained in accordance with the CASA on‑condition[8] requirements. At the last annual inspection in July 2021, the maintenance organisation had completed a piston engine condition report verifying the engine serviceability, which then permitted the engine to continue in service.
Site & wreckage information
Onsite examination
The wreckage was located about 1 km north of the Redcliffe airfield, on a tidal flat (Figure 3). The accident occurred about 40 minutes before high tide, and the water depth at the time of the accident was about 2 m. The aircraft impacted the water on a heading of about 218° in an upright, slight right-wing low, nose-down attitude, with the undercarriage in the extended position, and with the wing flaps retracted.
Ground scars observed on the tidal flat indicated that after entering the water, the aircraft nose wheel and propeller contacted the seabed leading to the aircraft overturning, resulting in sudden deacceleration and the aircraft coming to rest inverted. Witnesses described the water directly around the aircraft to be murky due to the mud and silt seabed having been disturbed by the aircraft impact. The left door (pilot door) was in a closed and latched condition when the ATSB arrived onsite. The right door was found by police divers to be slightly ajar, and difficult to open during the recovery operation.
Figure 3: VH-WMM accident site at low tide

Source: ATSB
The aircraft fuselage underside and right wing showed evidence of hydraulic[9] compression from impacting the water surface, and the engine had separated from the aircraft. The impact to the fuselage underside damaged the fuselage skins forward and aft of the wing main spar carry‑through, resulting in a large hole. The engine firewall had been punctured by the engine and the left rear side window was broken. The identified damage would have allowed water ingress into the fuselage. Fuel was visibly leaking from the right underwing fuel vent, and a strong fuel smell was evident at the site.
Wreckage examination
The wreckage was recovered to a secure storage facility for a detailed examination. ATSB investigators established flight control continuity before the rear of the fuselage and empennage were separated to facilitate transport from the recovery point.
A further flight control examination was performed with no defects noted. All components of the aircraft were identified and accounted for, and no pre-existing defects were noted with the airframe or engine.
Fuel system examination
Examination of the aircraft fuel system was carried out and found that the fuel selector was set to the LEFT tank at the time of the accident, and the auxiliary fuel pump was switched OFF. The gascolator was disassembled and contained water. After recovery of the wreckage, the fuel tanks’ contents were drained and consisted of:
- right wing: about 85 L of AVGAS recovered, with no visible water
- left wing: about 25 L of water, with no visible AVGAS.
Engine & propeller examination
The engine and propeller displayed no pre-existing damage. The propeller damage was indicative of low rotational energy at the time of impact and exhibited damage to the blades and spinner due to impact with the seabed. The engine was externally examined, all components were accounted for, and the engine was able to be rotated. The engine was disassembled and examined at a CASA-approved engine overhaul facility under the supervision of the ATSB. The engine showed no evidence of pre-impact mechanical discontinuity or defects which would inhibit normal operation.
Examination and testing of the engine fuel system was performed at a separate CASA-approved overhaul facility under ATSB supervision. Some system components had internal corrosion; however, this was most likely due to saltwater immersion. After removal of the corrosion, the system components tested correctly for operation.
The fuel control unit (FCU) initially could not be tested. A disassembly of the FCU found internal corrosion within the regulating system and the centre body seal was found to be separated. The centre body seal was examined at the ATSB’s technical facilities in Canberra. ATSB determined that the internal seal separation had occurred when the FCU was disassembled for examination and was not a prior defect.
Rockwell 114 procedures
Before take-off checklist
At each critical phase of aircraft operation, pilots refer to checklists to guide them through specific items to configure the aircraft for the next planned phase of the flight. The Rockwell 114 pilot’s operating handbook (POH) [10] stated in 3 separate checklists, ‘interior’, ‘before starting engine’, and ‘before take-off’ checklists, that the fuel selector valve is to be set to the BOTH position before the aircraft is ready for take-off.
Figure 4 shows the Rockwell 114 ‘before take-off’ checklist as detailed in the POH. Annotations highlight where the interruption occurred at the beginning of the accident flight, and the steps not completed as identified in the passenger video. The POH was located at the accident site at the rear of the pilot seatback, and passenger video showed that it was not accessed during the before take-off checks or during the flight.
Figure 4: Before take-off checklist
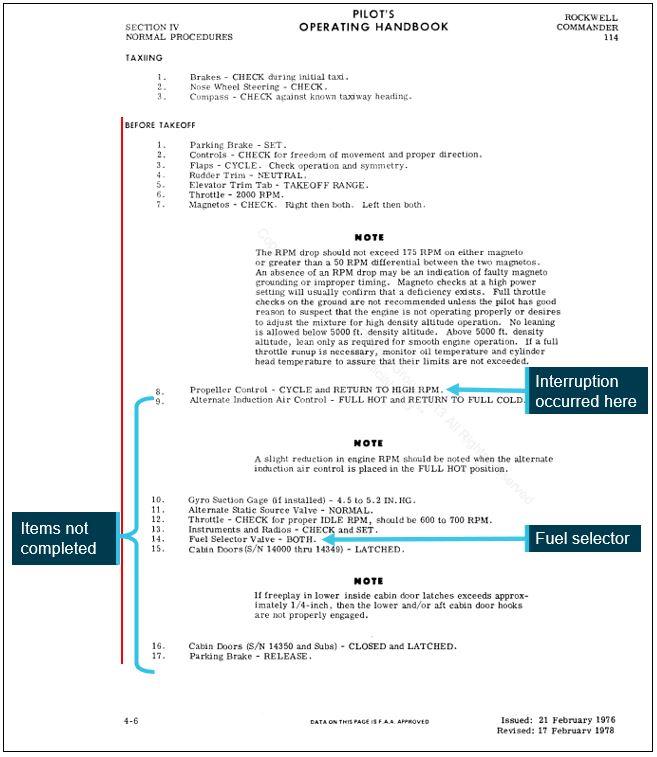
Source: Rockwell 114 pilot’s operating handbook, annotated by the ATSB
Third-party checklists
CCTV footage showed the pilot passing a folder to the adult passenger who placed it into the rear of the pilot seatback prior to engine start. This folder was found on-site in the rear of the pilot seatback pocket and contained the third-party checklists inside. Both of these checklists had interpretations of the Rockwell 114 POH checklists and had differences to the approved manufacturer’s documentation. This included changes in the checklist sequence, and omissions of some elements including the absence of one of the fuel selector checks.
CASA issued AC 91-22v2.0 Aircraft checklists, in November 2021 to provide guidance on establishing and using aircraft checklists and is derived from Civil Aviation Safety Regulation 91.095 Compliance with flight manual. This stated that any third-party checklists ‘must concisely convey each procedural step in correct sequence’ to ‘ensure aircraft are operated in a way that meets flight manual requirements and limitations.’
The US Federal Aviation Administration released a safety alert for operators (SAFO) 17006, in April 2017, warning pilots and operators of the risks of using commercially available and personally derived, third-party checklists.
An acquaintance who had regularly flown with the pilot reported that the pilot would also use generic mnemonic checklists that had been committed to memory, instead of the POH or the third‑party checklists. The commonly used mnemonic covered some, but not all of the checks required by the POH checklist.
Engine failure management
The Rockwell 114 POH emergency procedures checklist for an in-flight engine failure stated that the glide speed of 82 kt should be adopted, the auxiliary fuel pump selected on, mixture full rich, and the fuel selector be placed on the fuller tank to rectify possible fuel starvation.
Maintaining the published glide speed in flight gives the optimal amount of lift for the least amount of drag, thereby giving the greatest glide distance for the amount of height lost during the descent.
Rockwell 114 ditching procedure
A ditching is a controlled emergency landing on water. The Rockwell 114 POH ditching procedure identified that on approach to a ditching, the airspeed should be maintained at 82 kt.
The procedure followed on to list: transponder (if installed) set to 7700, and a mayday call should be made. The emergency locator transmitter should be activated if installed, seats, seatbelts, shoulder straps and loose objects should be secured, flaps should be up, cowl flaps closed, and the undercarriage retracted.
On final approach, flaps should be set to 20°, airspeed reduced to 74 kt, the undercarriage should remain retracted, and propeller set to high RPM. On touchdown, the elevator should be full aft, and the fuel selected to OFF.
Ditching guidance
In 2004 the ATSB made recommendation R20010258 which stated:
The Australian Transport Safety Bureau recommends that the Civil Aviation Safety Authority educate industry on procedures and techniques that may maximise the chances of survival of a ditching event. Part of that education program should include the development of formal guidance material of the type contained in the UK CAA General Aviation Safety Senses leaflet 21A Ditching.
In response to the recommendation CASA published CAAP 253-1(1) Ditching. This guidance was reissued in the form of AC 91-09 v1.0 and included but was not limited to the following safety advice about conducting a ditching:
For an aeroplane, it is likely to end up in a nose down vertical position after impact. Opening a forward door in these circumstances to escape may cause rapid water entry. Planning for this circumstance should include consideration of which exit might be opened prior to and after impact and briefing passengers on precautions when releasing seat belts. Any briefing should consider the prospect that the pilot may not be able to assist due to their prominent position where impact forces may be concentrated. An able-bodied passenger near an accessible exit would be the best resource for survivability in this situation.
The guidance also recommended unlatching a door prior to impact and providing passengers with a briefing, which included the brace position.[11]
Survival aspects
Passenger seating, exit location, and operation
The pilot (P) was seated in the front left seat location. The 3 passengers consisted of an adult and 2 children.[12] One child (C) was seated in the forward right seat next to the pilot and another child (C) was seated in the left-rear behind the pilot. The adult (A) passenger was seated in the rear‑right (Figure 5). Both aircraft doors were at the front row.
Figure 5: Seating positions
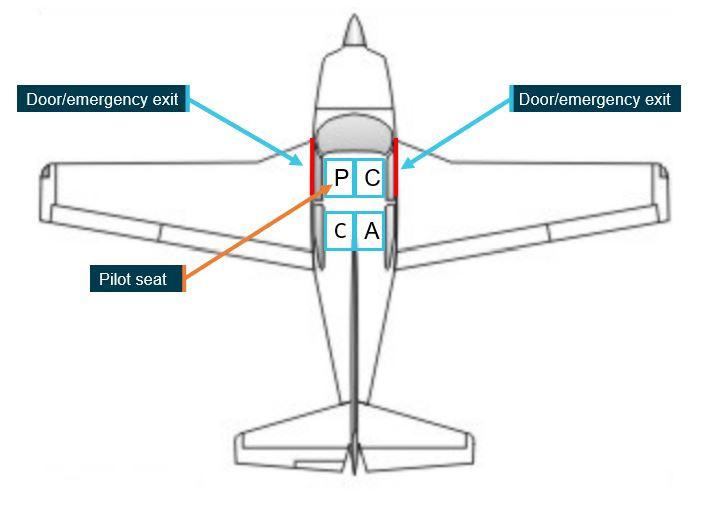
Source: Rockwell annotated by the ATSB
Figure 6 shows the aircraft doors, which were designed as both normal and emergency exits. Both doors had the same operation, which required 2 opening mechanisms to be manipulated, both when operating from inside or outside. One handle was located above the passenger/pilot head that needed to be rotated downwards to unlatch. The second handle was fitted to the forward lower part of the door and was a lever type arrangement, which was required to be pulled inwards to unlatch the 2 lower latches. Each door needed to be pushed outwards to open. There was no emergency jettison mechanism.
Figure 6: Location of door interior operating handles
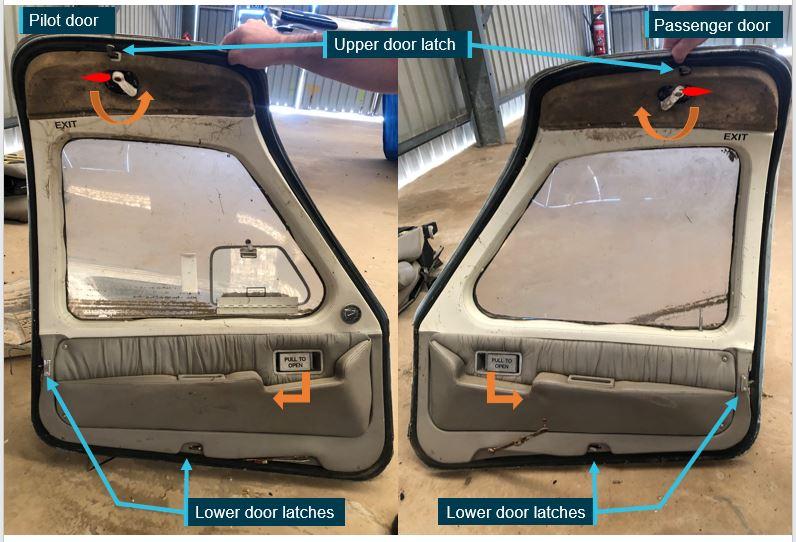
Source: ATSB
CASA produced guidance for the allocation of passengers to exit row seats in multi-part advisory circular (AC) Passengers seated in emergency exit row seats for parts 121, 133 and 135 operators, however this AC was not applicable to private flights.
In addition to passenger suitability, the AC identified risks associated with seating inappropriate persons at exits and recommended that operational procedures should be used to address this risk.
Applicable risks included:
- exits being opened when they should not be e.g., a passenger opens the exit without assessing the outside conditions
- operation of exits by passengers who are not aware of the instructions specific to that exit e.g. how to open, remove and discard the exit
- passengers seated in an emergency exit row having an adverse reaction to the emergency due to inadequate briefings
- passengers that are not suitably able-bodied, lacking the strength and ability to remove the exit, attempting to open the exit, and delaying or impeding an evacuation process.
In addition, CASA guidance[13] identified that pilots should consider the possibility of incapacitation, and seat and brief an able-bodied person accordingly. However, passenger composition and operational considerations such as weight and balance must always be considered to determine passenger seat allocation.
Pre-flight, exit and emergency briefings
Civil Aviation Safety Regulations (CASR) 1998 Part 91 (General Operating and Flight Rules) manual of standards, Division 20.3 Passenger safety briefings and instructions which came into effect just prior to the accident on 2 December 2021,[14] required, among other things, that passengers be briefed on:
(f) how and when to adopt the brace position;
(g) where the emergency exits are, and how to use them;
(p) the requirement that:
(i) passengers seated in emergency exit rows must be willing and able to operate the exit in the event of an emergency; and
(ii) such passengers must not have a condition that will cause them to obstruct the exit or hinder an emergency evacuation
While they had to be briefed, there was no legislative requirement to assess the suitability of a person[15] in an exit row for a private flight.
Guidance[16] on passenger safety briefings relevant for small aircraft operators included:
- to include the brace position in the pre-flight safety briefing
- to advise passengers to adopt the brace position in an emergency
- if the flight involves overwater operations, passengers are briefed on ditching procedures.
Briefings in practice
A witness who the accident pilot regularly flew with reported that the pilot would normally provide a briefing about the seatbelts and the operation of the aircraft exits. The instructor who assessed the pilot in their most recent flight review provided confirmation of consistent elements normally included in the pilot’s briefing.
The ATSB was unable to determine what information was provided to the passengers prior to flight on the day of the accident. Video footage captured during the emergency showed that the pilot did not provide an in-flight emergency briefing to passengers about the nature of the emergency or what actions to take.
Occupant injuries
A post-mortem examination of the pilot and passengers was conducted on behalf of the Queensland Coroner. The examination found all occupants had sustained injuries which may have caused some incapacitation but were insufficient to have been fatal. The reports found that the deaths were consistent with drowning. The report also detailed evidence of injuries consistent with being caused by wearing a harness or seatbelt.
Other information
Pilot medical requirements
As outlined above, of the last 3 CASA aviation medical examinations, the pilot had not declared their diabetic status or diabetes medication to their CASA designated aviation medical examiner (DAME).
The disclosure to DAMEs was required due to the nature of type 2 non-insulin dependent diabetes and its effect on aviation participants. The CASA Clinical practice guidelines for type 2 diabetes website stated their concerns:
Effect of aviation on [diabetes] condition:
- Difficulty with regular blood-sugar monitoring
- Irregular meal and sleep times
- Sedentary occupation
- Access to emergency sugar
Effect of [diabetes] condition on aviation:
- Overt incapacitation
- Cardiovascular event
- Cerebrovascular event
- Subtle incapacitation - end-organ damage
- Visual impairment (fields, low contrast sensitivity, colour)
- Impaired motor and sensory nerve function
- Impaired autonomic function (hypoglycaemia awareness).
Pilots are permitted to hold a licence after a diabetes diagnosis. The CASA website further stated:
Type 2 diabetes is an aeromedically significant medical condition. Pilots and [air traffic] controllers who have been diagnosed with Type 2 Diabetes are required to ground themselves and notify this condition to their DAME.
In cases where the condition can be managed appropriately, and once cleared by the DAME, in accordance with the CASA guidelines, ongoing monitoring of the diabetes must be provided to CASA to prove that it is able to be managed and does not affect the pilot’s ability to fly.
Safety analysis
Introduction
Shortly after take-off, VH-WMM likely experienced fuel starvation leading to a complete loss of engine power. During the attempted return to the airfield without power, the pilot did not maintain an adequate glide speed, and the undercarriage was extended, thereby reducing glide range, which resulted in the aircraft colliding with water before it reached the airfield and becoming inverted about 170 m from shore.
This analysis will explore the power loss on take-off, flight planning and decision making of the pilot in command, and post impact survivability factors.
Checklist use
The passenger video identified that the pilot became distracted with a perceived engine problem during the before take-off checks and taxied back towards the groundcrew member. However, after realising that they had mis-identified the wrong engine control, the pilot then proceeded to the runway and conducted the take-off, without further completion of the required checks.
One essential aspect of the POH checklist stated that the fuel selector was to be set to BOTH. This ensures a positive supply of fuel can be delivered to the engine from both fuel tanks during take-off. There were two versions of the checklists on board the aircraft: the official aircraft POH included this item in 3 separate checklists, while the third-party checklists included it twice. While it is likely that the distraction affected the pilot’s completion of the ‘before take-off’ checklist items, the fuel selector was also not set to BOTH on the ‘interior’ or ‘before starting engine’ checks.
Should a third-party checklist be used, it must be checked to ensure that it contains the correct information that is applicable for the aircraft being operated and that the checklist is verified against the approved POH checklists. The ATSB was advised that the pilot sometimes referred to the third-party checklists, however it is unlikely that the third-party checklists were referred to on the day of the accident as the folder containing the checklists were located in the pilot seat back pocket and not readily at hand.
The POH was carried on board the aircraft on the day of the accident, and the passenger video showed it was not referred to during the flight.
On this basis, it is likely the pilot performed the before take-off checks from memory or used a mnemonic checklist to perform the before take-off checks which were ultimately interrupted. Before take-off, there is no time pressure (as there was inflight after the engine power loss), so there was opportunity to consult the written checklists to ensure all steps were completed. Conducting aircraft checks from items committed to memory can lead to checks being skipped or an assumption that a check has been completed when it has not. Also, when a checklist is interrupted, the habit of restarting from the beginning is a means of ensuring that all steps to be performed are done so in order and the checklist is complete.
Fuel imbalance
Analysis of CCTV imagery indicated it was likely that VH-WMM had a substantial quantity of fuel in the right wing, and that the pilot would have been aware of the imbalance after physically using a dipstick to check the aircraft fuel tanks during the pre-flight checks on the ground outside the hangar.
The fuel selector was found to be on the left tank after the accident and there was no video evidence of the pilot changing it during the flight. Therefore, the fuel selector was likely on the left tank during take-off. Due to the fuel imbalance, the left tank likely had minimal fuel to sustain engine operation during the climb out, which would result in the engine being starved of fuel, lose power, and begin to surge, and eventually stop. This is consistent with no fuel being found in the left tank after the accident.
If the fuel selector was placed on BOTH tanks, then it is likely, even with one fuel tank having most of the fuel and the other almost empty, that fuel supply to the engine would remain unaffected. Excess fuel in the right tank may have led to the observed fuel coming from the right wing during the flight.
Therefore, with the aircraft’s remaining fuel supply most likely in the right tank, and with the fuel selector likely set to LEFT prior to take-off, the engine became starved of the available fuel supply in the aircraft’s right fuel tank, leading to the engine stopping.
Engine power loss management
ATSB found that few, if any, initial emergency actions took place in response to the loss of engine power to rectify a possible fuel starvation as per the Rockwell 114 procedures. The aircraft had sufficient fuel for flight in the right wing, but the fuel selector was found to be selected to the now empty left tank, and the auxiliary fuel pump was off during the emergency.
In addition, the pilot did not maintain the published glide speed of 82 kt as demonstrated by the numerous stall warnings that sounded repeatedly, indicating a speed within 3-4 kt of the straight and level flapless stall speed (63 kt). Airspeed management was made more difficult by the extension of the landing gear, which may have been an automatic reaction by the pilot in response to hearing the undercarriage warning bell sound while the pilot was managing the emergency.
Not maintaining the glide speed and the landing gear extension increased the vertical rate of descent and reduced the glide range of the aircraft. However, video evidence suggests the pilot continued with their initial plan to glide to the runway. In addition, the extended landing gear was an unfavourable configuration for the subsequent collision with water.
There was no available evidence to indicate that the pilot’s response (actions and inactions) to the emergency was affected by a medical issue, or similar factors. However, the pilot was making decisions during the emergency under a high level of stress and time pressure. A substantial amount of research has shown that people often do not make optimal decisions in such situations.
Some commonly reported effects of stress and/or time pressure include attentional narrowing, with people searching fewer information sources (Staal 2004) and focusing on cues that are perceived to be the most salient or threatening (Burian and others 2005, Wickens and Hollands 2000). Working memory and the ability to perform complex calculations is impaired (Burian and others 2005), and the ability to retrieve declarative knowledge (or facts) from long term memory is affected (Dismukes and others 2015). In addition, a person under stress and time pressure will generally consider fewer alternatives, and not be as systematic when evaluating alternatives (Dismukes and others 2015, Staal 2004).
Collision with water
It is likely that the pilot never intended to ditch the aircraft. Rather, the reduced speed of the aircraft below the glide speed, exacerbated by the undercarriage extension, led to a reduced glide range and inability to reach the runway at Redcliffe. The sounding of the ‘stall’ alert just before the collision indicates the aircraft could no longer maintain lift and the aircraft collided with water 3 seconds later.
It is likely that under the stress of the situation, the pilot’s attention narrowed and their focus on landing back on the departure runway likely hampered their ability to consider a forced landing on water (ditching). Had the pilot recognised that the aircraft would not be able to glide to the runway, there was a brief opportunity (about 30 seconds) to attempt a controlled landing on water before the aircraft’s speed reduced to the stall speed.
If this had been the case, there were several actions the pilot would have had to remember (due to the limited time remaining) and complete to ensure a safe ditching. From the Rockwell 114 POH procedure, key actions were to ensure the undercarriage was retracted and the flaps were selected to 20° on the final approach to land on the water.
Use of flap in the final stages of the ditching would have provided a reduced stall speed, therefore allowing the aircraft to touch down at a lower, controlled speed. Touching down on the water while not at the appropriate speed, and with the undercarriage extended, contributed to the aircraft inverting after colliding the water.
Further, although there was no reference in the POH to the pre-impact position of emergency exits (cabin doors) prior to a ditching, unlatching of cabin doors can allow quick egress from the aircraft after ditching. In this accident, given the brief opportunity available for such considerations, it was not considered feasible that all actions were possible.
Due to the inverted orientation of the aircraft during the crash sequence and its submersion in murky water, the aircraft occupants were probably panicked, confused, and disorientated following the collision. Once the cabin filled with water, visibility would have been extremely low, which would have further reduced the likelihood of occupants being able to visually locate and operate the aircraft door handles. With the aircraft inverted, it is likely the occupants would have also been disoriented to the extent that it made opening the closed doors more difficult, reducing their ability to escape.
Pre-flight and emergency briefings
Research has shown that more knowledgeable passengers perform better in an emergency (Meng-Yuan, 2014). It could not be determined what information was provided to the passengers prior to flight, however based on accounts from persons who had flown with the pilot previously, including their flight instructor, it is likely that any briefing given did not include any information about the brace position or what to do in the event of a ditching. This meant that the passengers were likely unaware of actions that may assist survival such as opening the aircraft door or adopting a brace position.
Video footage recorded during the accident sequence showed that the pilot also did not provide passengers an in-flight emergency brief or instruct them on any actions they should take. This accident highlights the importance of providing instructions to passengers before a flight commences as often emergency situations are time limited and there may not be an opportunity to do so once something occurs.
Providing information on the adoption of the brace position or how to, and when to open an emergency exit in a ditching situation will increase the likelihood of passengers taking appropriate action in an emergency.
Passenger seating and emergency exit operation
Post-mortem examinations identified that the occupants of the aircraft were not fatally injured during the accident sequence. There was no readily available assistance nearby the accident site, and therefore the occupants would have had to extricate themselves from the aircraft.
The 2 emergency exits available to the occupants were more accessible to persons seated in the front of the aircraft. The exits required manipulation of both a handle on the door and a latch at the top. For the rear passengers, it is likely that they would have had difficulty (particularly with their seatbelt on) to reach the latch at the top of the door if required to operate the exit. The rear seat occupants would have also been restricted in accessing the doors and exiting the aircraft due to the presence of the front seat occupants.
After the accident, police divers were unable to open the pilot’s left door, and only opened the other (right) door with difficulty. For the injured pilot and right front seat occupant of VH-WMM, who was a child, it is highly unlikely they would have had the post-accident capability to open the doors. The right door was observed unlocked and ajar by police divers following the collision, suggesting the possibility that an attempt had been made to open the door.
Guidance suggests that pilots should determine the most appropriate person to assist in an emergency and to brief that person accordingly, therefore, in this case, seating a child who has less physical and mental capability rather than an adult next to an exit, meant that the most suitable person (the adult) was not in the best position to assist themselves and others in the event of an emergency.
Diabetes
The pilot had been diagnosed with type 2 non-insulin dependent diabetes which was managed with prescription medication by the pilot’s GP. A review of the pilot’s CASA aviation medical information indicated that this significant medical condition was disclosed in the pilot medical history as ‘unsure’ to the CASA DAME in the previous 3 aviation medical renewals, all of which were changed to ‘no' at the DAME examination prior to submission to CASA.
It was important to note that having type 2 non-insulin dependent diabetes did not mean that this condition would be an immediate disqualification of the pilot’s licence. However, due to the aeromedically significant nature of diabetes, it was important for this to be fully disclosed with the pilot’s DAME and to CASA. Without this interaction, it was a missed opportunity for the pilot’s condition to be monitored at a safe level required to exercise the privileges of a pilot’s licence.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the fuel starvation and collision with terrain involving a Rockwell International 114, VH-WMM, 1 km north of Redcliffe aircraft landing area, Queensland, on 19 December 2021.
Contributing factors
- An unsafe condition was created by not referring to the approved checklists in the pilot operating handbook. Checklists located in the pilot operating handbook would have prompted the pilot on 3 occasions to set the fuel selector to BOTH prior to take-off.
- A perceived engine problem distracted the pilot during the conduct of pre-take-off checks. After rectifying the issue, they did not complete the remaining pre-take-off checks (including fuel tank selection) before departure.
- A fuel imbalance and likely an incorrect fuel tank selection prior to take-off, led to fuel starvation and engine stoppage soon after take-off.
- The pilot, likely experiencing the effects of stress and time pressure following the engine power reduction and then stoppage, did not conduct initial emergency actions and attempted to return to the runway for landing but did not maintain glide speed, and the aircraft impacted shallow water prior to reaching the airfield.
- During the return to the airfield, the pilot extended the undercarriage, contributing to the aircraft inverting when it collided with water. This likely resulted in occupant disorientation, difficulty in operating the exits, and reduced their ability to escape.
Other factors that increased risk
- It is very likely that the passengers did not receive pre-flight information about the brace position or what to do in the event of a ditching. In the limited time available inflight after the power loss, the pilot also did not provide an emergency briefing or any instructions to passengers prior to impact with the water.
- While the pilot was primarily responsible for the operation of the aircraft exits in an emergency, seating a child, who may require assistance, adjacent to an exit instead of an adult meant that a less suitable passenger was available to operate the exit if required.
- The pilot had a diagnosed type 2 diabetic condition and did not directly declare this to the DAME during multiple medical renewals.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Civil Aviation Safety Authority
- Queensland Police Service
- Australian Volunteer Coast Guard
- accident witnesses
- CCTV footage
- passenger mobile phone recordings
- the pilot’s general practitioner
- the pilot’s designated aviation medical examiner
- the flight review instructor
- maintenance organisation
References
Australian Government 2021, AC 91-22 Aircraft checklists v2.0, Civil Aviation Safety Authority, Canberra, ACT, viewed 18 December 2023, < AC 91-22 v2.0 - Aircraft checklists (casa.gov.au)>
Australian Government 2022, Type 2 Diabetes - Non-insulin dependent - Low risk of hypoglycaemia, Civil Aviation Safety Authority, Canberra, ACT, viewed 7 February 2022, < Type 2 Diabetes - Non-insulin dependent - Low risk of hypoglycaemia | Civil Aviation Safety Authority (casa.gov.au)>
Australian Government 2023, Avoidable Accidents No. 3 - Managing partial power loss after take-off in single-engine aircraft, Australian Transport Safety Bureau, Canberra, ACT, viewed 8 February 2022, < Avoidable Accidents No. 3 - Managing partial power loss after take-off in single-engine aircraft | ATSB>
Australian Government 2023, AC 91-09 Ditching v1.0, Civil Aviation Safety Authority, Canberra, ACT, viewed 25 January 2022, < AC 91-09 v1.0 - Ditching (casa.gov.au) >
Australian Government 2023, Part 91 (General Operating and Flight Rules) Manual of Standards 2020, Civil Aviation Safety Authority, Canberra, ACT, viewed 25 January 2022, Part 91 (General Operating and Flight Rules) Manual of Standards 2020 (legislation.gov.au)>
Australian Government 2023, Passenger safety information, Civil Aviation Safety Authority, Canberra, ACT, viewed 25 January 2022, < Multi-Part AC 91-19, AC 121-04, AC 133-10, AC 135-12 and 138-10 - Version 1.1 (casa.gov.au)>
Australian Government 2023, Passenger safety information, Federal Register of Legislation, Canberra, ACT, viewed 24 January 2022, <Civil Aviation Order 20.16.3 - Air service operations - Carriage of persons (02/12/2004) (legislation.gov.au)>
Burian BK, Barshi I & Dismukes K 2005, The challenge of aviation emergency and abnormal situations, National Aeronautics and Space Administration Technical Memorandum NASA/TM-2005-213462.
Casner SM, Geven RW & Williams RT 2013, ‘The effectiveness of airline pilot training for abnormal events’, Human Factors: The Journal of the Human Factors and Ergonomics Society, vol. 55, pp.477-485.
Chaiken, S. R., Kyllonen, P. C., & Tirre, W. C. (2000). Organization and components of psychomotor ability. Cognitive Psychology, 40(3), 198-226.
Dismukes RK, Goldsmith TE & Kochan JA 2015, Effects of acute stress on aircrew performance: Literature review and analysis of operational aspects, National Aeronautics and Space Administration Technical Memorandum NASA/TM-2015-218930.
United States Government 2017, Safety Concerns with Using Commercial Off-the-Shelf (COTS) or Personally Developed Checklists, Federal Aviation Administration, Washington, DC, viewed 10 January 2024, < SAFO 17006: Safety Concerns with Using Commercial Off-the-Shelf (COTS) or Personally Developed Checklists (faa.gov)>
Kahneman D 2011, Thinking, fast and slow, Allen Lane London.
Klein G 1998, Sources of power: How people make decisions, Massachusetts Institute of Technology.
Landman A, Groen EL, van Passen VV, Bronkhorst AW & Mulder M 2017, ‘The influence of surprise on upset recovery performance in airline pilots’, The International Journal of Aviation Psychology, vol. 27, pp.2–14.
Lycoming Engines 2021. Service Instruction No 1009BE Time Between Overhaul (TBO) Schedules, viewed 7 December 2021, Lycoming Engines <Service Instruction No. 1009 BE | Lycoming>.
Meng-Yuan, L. 2014, An evaluation of an airline safety education program for elementary school children. Evaluation and Program Planning, Science Direct, viewed 21 January 2023, < An evaluation of an airline cabin safety education program for elementary school children - ScienceDirect>
Precision Airmotive Corporation 20200, Training Manual RSA Fuel Injection System, viewed 6 June 2023, <15-812_b.pdf (precisionairmotive.com)>
Precision Airmotive Corporation 2020, RSA Fuel Injection system schematic wallchart, viewed 24 March 2022, < precisionairmotive.com/wp-content/uploads/2019/06/WALLCHART_rsa.pdf>
Staal MA 2004, Stress, cognition, and human performance: A literature review and conceptual framework, National Aeronautics and Space Administration Technical Memorandum NASA/TM-2004-212824.
Wickens CD & Hollands JG 2000, Engineering psychology and human performance, 3rd edition, Prentice-Hall International Upper Saddle River, NJ.
Wikipedia 2023, Rockwell Commander 112/114 family, viewed 14 January 2022, Wikipedia < Rockwell Commander 112 - Wikipedia>
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the Civil Aviation Safety Authority
- the National Transportation Safety Board
- the pilot’s last flight review flight instructor
- the pilot’s ground crew member
- medical subject matter experts.
Any submissions from those parties was reviewed and, where considered appropriate, the text of the draft report was amended accordingly.
Appendix
Sequence of events
The sequence of events below lists the key activities and audio from the passenger recorded video. This recording was started at 0902 and 25 seconds. The time listed in the table below is added to this time stamp. The video began during the taxi back toward the ground crew after the perceived engine problem.
Table 1: Sequence of events from accident flight video
| Time (m:ss) from recording start | Time (m:ss) after take-off commencement | Activity | Comment |
| 1:50 | Stop at holding point | Discussing location of other traffic | |
| 2:18 | WMM enters and backtracks runway 07 | ||
| 3:00 – 3:21 | Take-off | ||
| 3:30 | 0:09 | Undercarriage retracts | Motor heard during gear retraction |
| 3:56 | 0:35 | Left turn | Aircraft over water |
| 4:05 | 0:44 | Engine RPM decrease | Pilot reduces power after take-off |
| 4:09 | 0:48 | Flaps seen retracting | Captured on video |
| 4:15 | 0:54 | Left turn | WMM now about 90° to runway heading |
| 4:32 | 1:11 | Engine RPM fluctuating | Distinct rise and fall of engine RPM |
| 4:35 | 1:14 | Large drop in engine RPM | |
| 4:38 | 1:17 | Passenger asks pilot about fuel coming out of right-wing fuel cap | |
| 4:38 & 4:42 | 1:17 & 1:21 | Two left turns | WMM now on downwind leg to airfield |
| 4:48 & 4:51 | 1:27 & 1:30 | Stall warning sounds | |
| 4:52 | 1:31 | Engine stops | Distinct ‘whomp’ sound from engine, usually heard when a piston engine stops |
| 4:56 | 1:35 | Undercarriage warning bell followed by stall warning | ‘Click’ sound, followed by a wind noise. Gear extension most likely set here. |
| 5:02 | 1:41 | Pilot speaking | Radio call for return to runway |
| 5:18, 5:20 & 5:24 | 1:57, 1:59, & 2:03 | Stall warning sounds | |
| 5:25 | 2:04 | WMM turns directly toward runway | |
| 5:26 to 5:40 | 2:05 to 2:19 | Stall warning multiple sounds | |
| 5:40 | 2:19 | Right wing drops | |
| 5:42 | 2:21 |
Right wing drops Electronic voice calls “stall” Aircraft stall warning remains on |
Electronic voice is an alert from the Voice Alert System – heard only once |
| 5:45 | 2:24 | Aircraft impacts water |
Source: ATSB based on passenger mobile phone recording
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2] Runway number: the number represents the magnetic heading of the runway. In this case, 07 equates to 70°.
[3] Radio communications on the common traffic advisory frequency at Redcliffe Aerodrome were not recorded.
[4] Psychomotor skills refer to the co-ordination of perception and action and require either complex perceptual discrimination or a complex motoric response (Chaiken and others, 2000).
[5] Records showed that the pilot had been prescribed 4 antihypertensive medications and had regularly been dispensed these medications in the months before the accident. Only 1 of these medications was detected in the toxicology analysis, however the type of analysis conducted would not detect the other 3 medications.
[6] Wet wing – the wing structure forms an integral fuel tank instead of a bladder or metal fuel tank.
[7] Gascolator – a fuel filter fitted at the lowest point of the fuel system.
[8] On-condition: Performed only when the condition of an item demands, instead of at scheduled intervals.
[9] Hydraulic: in this context is the deformation of the aircraft skin around its structural members (such as ribs). This deformation occurs by the action of water on the aircraft skin during the accident sequence.
[10] While Rockwell uses the term pilot’s operating handbook, other manufacturers, and generic terms may include aircraft flight manual, flight manual, owner’s handbook, operating manual, or owner’s manual.
[11] Brace position – adopted for ditching or crash-landing; shoes removed, bent forward with arms protecting head.
[12] A child as defined by CASA is a person who has turned 2 but has not turned 13.
[13] Civil Aviation Advisory Publication (CAAP) 253-1(1) Ditching (2004) now AC Ditching (2021).
[14] The previous CAO 20.16.3 Air service operations - carriage of persons required that passengers be briefed to determine if they were willing and able if seated in emergency exits and CAO 20.11 Emergency and life-saving equipment and passenger control in emergencies required briefing on the location of the emergency exits, but not how to use them and did not include the brace position.
[15] A suitable person has been defined in the CASA dictionary as someone that is reasonably fit, strong, and able to assist with the rapid evacuation of the aircraft in an emergency; and would not, because of a condition or disability, including an inability to understand oral instructions, hinder other passengers during an evacuation of the aircraft in an emergency or the aircraft’s crew in carrying out their duties in an emergency.
[16] CASA guidance publications Cabin safety bulletin 12 - General aviation passenger briefings (2018), Civil Aviation Advisory Publication (CAAP) 253-1(1) Ditching (2004) now AC Ditching (2021), and Multi-part AC Passenger Safety Information (2021).



