Safety summary
What happened
On 17 April 2018, the pilot of a Garlick Helicopters UH-1H, registered VH-HUE, was conducting long-line lifting operations near Talbingo in the Snowy Mountains region of New South Wales. While on approach to pick-up a load, the helicopter’s engine failed. During the subsequent forced landing, the helicopter collided with trees and a riverbed. The pilot sustained serious injuries and the helicopter was destroyed.
What the ATSB found
The ATSB found that the inner struts in the exhaust diffuser fractured leading to the engine failure. The fracture was the result of high-cycle metal fatigue, which had not been detected for at least 36 routine maintenance inspections prior to the accident. It was also established that the maintenance practices and processes were likely inadequate to detect the potential impending failure of safety critical components. These practices related to inspections, record keeping and trend monitoring.
Following the engine failure, the pilot had limited assurance that ground support personnel could vacate the clearing directly below the helicopter, necessitating a forced landing to a less suitable location. This was likely the result of a risk assessment for helicopter operations that did not consider the hazard of an emergency landing as the helicopter approached to hook-up a load.
The pilot was not wearing the upper torso restraint fitted to the helicopter during the flight. It was virtually certain that this resulted in the pilot sustaining serious head injuries when the aircraft collided with terrain. It was also identified that upper torso restraints were likely not routinely worn by a notable proportion of pilots conducting vertical reference flying operations in Australia. This was likely due to these restraints not being fit-for-purpose for the operations being conducted. The operations mainly related to aerial firefighting, and to a lesser extent, lifting operations.
Although not contributory, the ATSB also found that a screw-clamp was retrofitted to the firefighting retardant delivery hose, which likely prevented the release of the long-line during the forced landing. While this did not influence the outcome of the accident, this had the potential of becoming snagged in trees and increase the severity of the impact.
Further, the immediate response of the ground personnel to extinguish a small fire in the engine bay and assist the pilot with exiting the helicopter, likely reduced the risk of more severe injuries to the pilot.
What has been done as a result
Following the accident, the maintenance organisation was acquired by another company. They advised improvements were made to their maintenance procedures and processes. Those improvements included the implementation of a new computer-based maintenance system that was expected to provide greater assurance in maintenance performed and assist with trend monitoring for detecting anomalies. Further, vibration test equipment was purchased to allow greater ease in conducting required checks.
In addition, the company responsible for managing the site ground works convened a hazard assessment workshop with the helicopter operators where they reviewed the hazards and controls for mountain flying and lifting operations. This was to ensure alignment, and a common approach and understanding between all parties. A risk management plan was collated during this workshop for use in similar future operations.
Safety message
Purposeful visual inspections of safety critical components, and the routine review of documented maintenance records for trend monitoring and anomaly detection purposes provide a vital role in preventative aircraft maintenance. These aspects would have likely allowed anomalies to be identified and investigated prior to the engine failure occurring.
Helicopter lifting operations introduce additional risks to personnel working in their vicinity. In circumstances where there may be insufficient time to formulate a plan, such as an emergency landing from a low height and low speed, carefully considered and clearly communicated pre‑flight risk assessments provide an important mechanism to mitigate these risks.
Upper torso restraints provide an important defence to reduce the severity of injuries during an accident. This report highlights an elevated risk to pilots who are unable to effectively wear these restraints during some vertical reference operations, such as aerial firefighting and lifting. Further consideration of engineering innovations for these restraints could reduce the risk associated with this problem.
Preparation for lifting operations
On 17 April 2018, the pilot of a Garlick Helicopters UH-1H, registered VH-HUE (HUE), was to be conducting long-line lifting operations near Talbingo in the Snowy Mountains region of New South Wales. In the morning, the helicopter was prepared for flight at Tumut Airport, about 60 km north of the planned area of operation. Flight preparations involved a discussion between the pilot[1] and a contracted licenced aircraft maintenance engineer about the maintenance performed since the pilot had last flown the previous day. The pilot conducted a walk-around inspection of the helicopter, signed the maintenance release and conducted an engine run. Nothing abnormal was noted by the pilot or licenced aircraft maintenance engineer.
The helicopter departed Tumut Airport at about 0804 Eastern Standard Time,[2] for a positioning flight to a clearing 57 km south of Tumut, known as Lobs Hole, arriving at about 0837 (Figure 1). This location was used as the base of operations for the lifting work on the day, referred to as the ‘laydown area’. The operation was part of a proposed expansion of the Snowy Mountains Hydro‑electric Scheme, known as the Snowy 2.0 project. The planned work on the day involved using helicopters to relocate components of a de-constructed drill-rig used for geotechnical survey within the ‘area of operation’ shown in Figure 1.
Figure 1: Map showing morning repositioning flight and area of lifting operation

Source: Google Earth, annotated by the ATSB
The lifting operation involved HUE and two AS350 ‘Squirrel’ helicopters. HUE was to be utilised for heavier loads, and the Squirrels to be utilised for the lighter loads. Supporting the lifting operation on the ground at the drill site (location of the load hook-up) were two loadmasters, who had radio communications with the pilots. Three additional workers were also assisting with drill rig de-construction. Although these workers were not involved in the lifting operation, they remained at the drill site during lifting.
Conduct of lifting operations
Lifting operations involving HUE commenced at 1308. Each run involved lifting drill-rig components from the drill site to the laydown area, before returning for the next lift. Each lift run, and return, was completed in about 5 minutes, with ground personnel preparing the next load between lifts. HUE had completed 11 lift runs (Figure 2), which the pilot reported were ‘uneventful’. At about 1414, the pilot positioned HUE for the twelfth run (Figure 2 red flight path), in order to lift the drill rig motor.
As the helicopter approached for the twelfth lift, one of the loadmasters advised the pilot that more time was required to prepare the rigging and requested the pilot hold off for a short time. HUE entered a holding circuit about 700 m to the north-east prior to making a very slow approach toward the drill site (Figure 2 red flight path). The pilot recalled that the weather conditions were ideal, with a slight breeze and good visibility.
Figure 2: Map of lifting runs conducted

Source: Google Earth, annotated by the ATSB
While waiting for a radio clearance to lift the drill rig motor, the pilot recalled conducting a full system check, and that all instruments indicated the helicopter was operating in the normal range. At about 1415, the loadmaster requested the pilot approach the site in preparation for lifting the drill rig motor. As HUE approached overhead, the loadmaster informed the pilot that the rigging required re-checking. In order to minimise the rotor downwash on the people below, the pilot raised the collective to climb the helicopter, and the 100-foot long-line, above the tree canopy.
Engine failure and forced landing
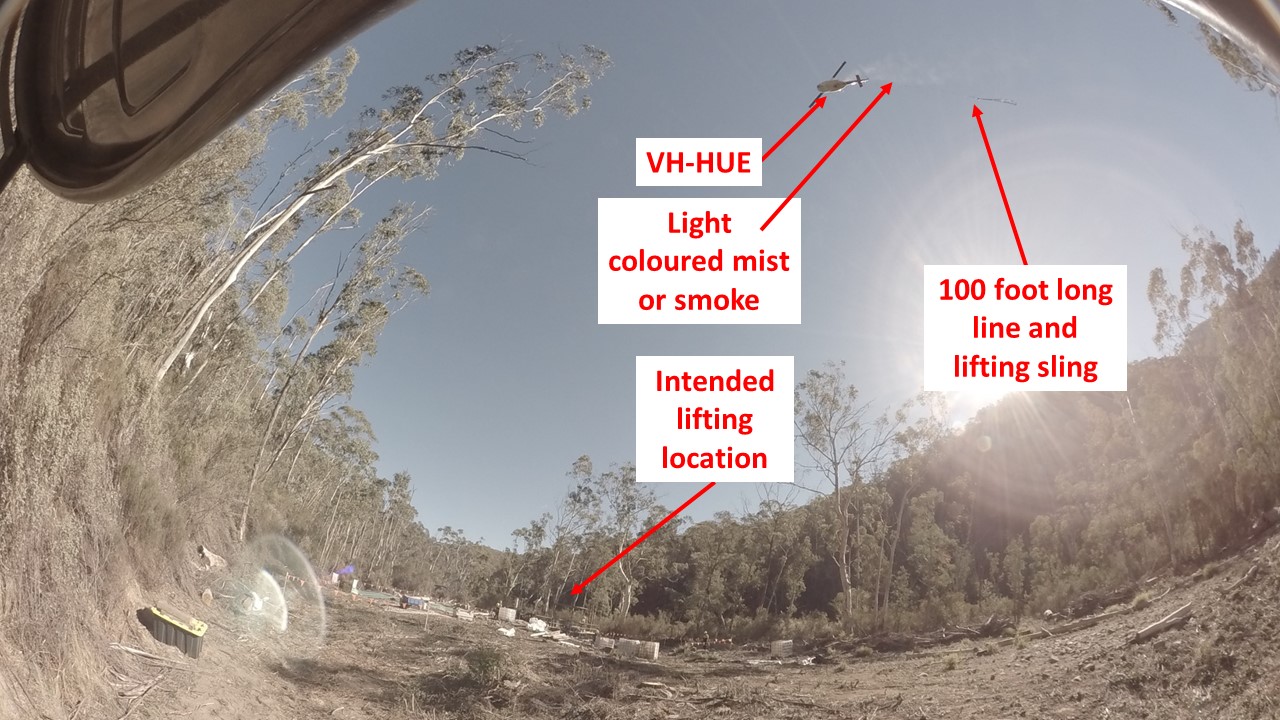
At about 1417, as the helicopter started to climb, the pilot heard a loud mechanical ‘screaming’ noise and started planning for a forced landing. Witnesses also reported seeing ‘smoke’ and some advised they heard a ‘bang’ at about the same time. Almost immediately, the pilot also heard an audible alarm, followed by a noticeable yaw and engine power loss. Time-lapse images from a camera mounted at the drill site showed a light-coloured gas or mist near the engine area of the helicopter (Figure 3).
Just prior to the engine failure, HUE was about 200 to 250 ft above ground level, with a forward airspeed of about 20 to 25 kt, based on global positioning system (GPS) data, eye-witness reports, and the pilot reporting flying into a slight headwind. From fuel-burn calculations by the ATSB, the weight of HUE was estimated at 2,900 kg at that time.
Figure 3: Light coloured gas or mist from the helicopter above the drill site

Source: GHD, annotated by the ATSB
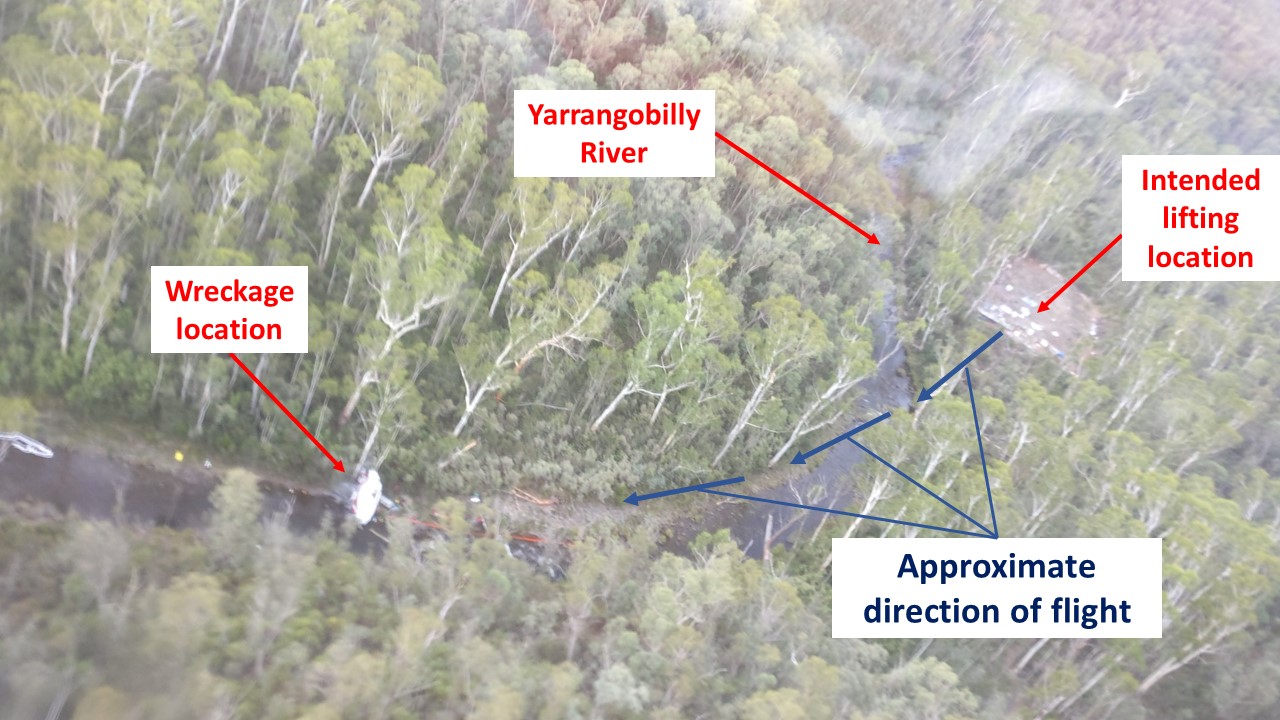
The pilot broadcast a ‘Mayday’[3] call and attempted to conduct the forced landing (autorotation) into the Yarrangobilly riverbed, south-west of the lifting area and the ground personnel. The workers observed the helicopter being turned to the south-west, away from the drill site.[4] They described the helicopter as appearing to ‘float’ over the trees, before descending quickly. Around this time, the pilot commanded jettison of the long-line and lifting strops. At interview, the pilot advised that the helicopter was flared prior to the impact with the second tree, but could not recall the remainder of the impact sequence until exiting the helicopter. The helicopter subsequently collided with trees and the riverbed (Figures 4 and 5). Ground personnel from the drill site immediately responded to the accident with fire extinguishers. They extinguished a small fire in the engine bay, removed the pilot from the wreckage, and performed first aid until emergency services arrived at 1520. The pilot sustained serious injuries and the helicopter was destroyed.
Figure 4: Forced landing flightpath showing drill site and helicopter wreckage

Source: New South Wales Rural Fire Service, annotated by the ATSB
__________
- The pilot was also the owner and operator of VH-HUE and is referred to hereafter as ‘the pilot’.
- Australian eastern standard time (EST): Coordinated Universal Time (UTC) + 10 hours.
- MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
- The drill site was a cleared area that included a helipad, and the drill rig to be lifted (at the lifting location).
Pilot information
The pilot held a Commercial Pilot Licence (Helicopter) and current Class 1 Aviation Medical Certificate. In addition, the pilot held a low-level operational rating, with endorsements for helicopter sling-load. The pilot had accumulated more than 9,000 hours total aeronautical experience, predominantly in helicopters. In the previous 30 and 90 days, the pilot had flown 43.4 and 154 hours respectively. The pilot reported being well rested for the day of the accident.
Meteorological information
The meteorological conditions from witness reports and drill site time-lapse camera footage throughout the period of lifting operations indicated clear sky and light winds. The wind conditions recorded by a Bureau of Meteorology automatic weather station about 45 minutes after the accident at Cabramurra (18 km away), were 11 km/h (6 kt) from the west, consistent with reports from the accident pilot.
Helicopter information
General
The UH-1H helicopter was developed by Bell Helicopters as a military utility helicopter for the United States (US) Army. The accident helicopter was manufactured in 1965. The helicopter had a two-blade main rotor and two-blade tail rotor and was powered by a military variant of the Honeywell Aerospace (formally Lycoming Engines) T53-L-13B turboshaft engine. Several organisations were authorised by the US Federal Aviation Administration (FAA) to convert surplus US military helicopters for civilian operations. Garlick Helicopters Inc. was the holder of the type certificate for this helicopter, which was US-registered as N2220Y, when it entered civilian operations.
VH-HUE (HUE) was first registered in Australia in December 2002 and was operated by one owner, until it was purchased by the current owner in January 2011. At entry in Australia, HUE had accumulated 8,017.3 hours and had ‘no record of accident’. In 2006, HUE was transferred to the restricted ‘special purpose’ category, due to the limited ongoing maintenance technical support. This category included agricultural operations, forest and wildlife conservation, and firefighting, and only persons who were ‘directly associated with the special purpose’ could be carried. HUE was issued with a special certificate of airworthiness[5] in July 2008.
Weight and balance
The ATSB calculated that HUE was very likely below the maximum take-off weight and within centre of gravity limits for all flights on the day of the accident. This included the 11 previous lift runs. Furthermore, fuel-burn calculations and the presence of a considerable amount of fuel at the accident site indicated there was sufficient fuel on board, about 270 kg, to conduct the lifting operations at the time of the accident.
Continued airworthiness
The logbook statement for HUE indicated that it was to be maintained in accordance with the Garlick Helicopters Inc. Instructions for Continued Airworthiness (ICA) Report GH-H13WE-CA1H. which stated:
FAA [Federal Aviation Administration] type certified civil engines and FAA approved civil appliances…must be serviced, maintained, inspected, and repaired in accordance with the applicable manufacturer’s maintenance manuals, or manufacturer’s Instructions for Continued Airworthiness or this TC Holder’s Instructions for Continued Airworthiness.
Therefore, HUE’s engine was to be maintained as per the US Army technical publications.
Wreckage and impact information
Examination of the trees on the side of the river opposite to the drill site revealed multiple broken branches resulting from the tips of the main rotor blades. Based on the path of broken branches and witness accounts, the helicopter’s descent path from this point became much steeper. The helicopter descended with the main rotor blades striking tree branches to the right of the helicopter prior to striking and severing a tree (the main impact tree) about 11 m up from its base, and 30 m from the initial tree strike. Audio analysis by the ATSB of the tree strikes from the phone of an eye‑witness was used to calculate a mean groundspeed of 45 kt, and vertical speed of about 2,000 feet per minute during this phase of flight. The flight path suggested that the pilot probably maintained control of the helicopter until one of the main rotor blades broke apart from impacting the tree.
Examination of the wreckage and ground impact marks indicated that the helicopter had impacted the ground in a nose high, slightly right side down attitude. The tail boom of the helicopter struck the ground during the impact, detaching from the fuselage. The landing gear assembly showed evidence of deflection during the main impact of the fuselage with the ground. The helicopter likely bounced off the skids, leading to the fuselage coming to rest in a nose low, slightly inverted position (Figure 5).
Figure 5: Helicopter wreckage showing nose of helicopter in Yarrangobilly River

Note: Wreckage of VH-HUE looking upstream toward the drill site, showing the nose of the helicopter and pilot’s seat.
Source: ATSB
For the lifting operations on the day of the accident, a 100 ft/30 m long-line was being used, with lifting strops attached at the remote hook. The site and wreckage examination revealed that, during the accident sequence, the long-line had detached from the belly hook, and the strops had released from the remote hook. This indicated that the long-line and strops were likely jettisoned during the accident sequence, as per emergency procedures. Although the pilot could not recall jettisoning the load, photographs confirmed that both the long-line and strops were attached to these hooks prior to the emergency, and the long-line did not appear to have snagged on any trees during the accident sequence. However, the long-line remained tethered to the fuselage due to the Sacksafoam hose line, which had failed to separate (refer to section titled Retention of the long-line) (Figure 6).
Figure 6: Failed to detach long line

Source: ATSB
During the examination of the wreckage, the ATSB identified cracking and material loss visible in the exhaust diffuser area (Figure 7 and Figure 8). In addition, the exhaust diffuser cover attachment bolt was not lock-wired, as required by the US Army maintenance manual applicable to HUE (Figure 8). Examination of the engine, including the exhaust diffuser assembly is discussed in the next section.
Figure 7: Visible cracking in the exhaust diffuser area

Source: ATSB
Figure 8: Diffuser area, unsecured cover plate, cracking and missing material

Source: ATSB
Engine examination and maintenance
Examination
Exhaust diffuser strut cracking
The engine was shipped to Honeywell’s facilities in Phoenix, Arizona, in the US and underwent a teardown examination under the supervision of a representative from the US National Transportation Safety Board. The purpose of the examination was to identify the technical failure mechanism, or mechanisms of the engine failure. This included a detailed examination of the exhaust diffuser assembly illustrated in Figure 9.
Figure 9: Exhaust diffuser assembly schematic and photograph (inset)

Source: Honeywell, modified by the ATSB
The Honeywell engine teardown identified extensive fatigue cracking in the exhaust diffuser inner struts (Figure 10 inset). The inner struts were a critical engine component that supported the rear of the power turbine assembly through the number 3 and number 4 bearings (Figure 10). Note for reference that Figure 10 (inset) shows missing material in the exhaust diffuser inner cone also shown in Figure 8. Honeywell identified the location of the cracking for each of the four inner struts:
- two of the four inner struts were separated around the full circumference of the inner strut flange welds
- another strut exhibited cracking around most of the circumference of the inner strut flange welds, although the inner strut remained attached to the inner cone by a small welded section
- one strut was separated through the strut with no visible weld separations.
The analysis by Honeywell determined that the cracking in the inner struts resulted in the complete loss of structural integrity of the four struts. This led to the power turbine assembly moving rearward, indicated by the arrow labelled ‘direction of PT movement’ in Figure 10. The rearward movement was sufficient for the rear tapered section of the power turbine drive shaft (labelled ‘PT drive shaft rear taper’) to contact the adjacent rear shaft of the compressor assembly, highlighted in blue. Due to the compressor and turbine assemblies rotating in opposite directions, the contact resulted in considerable friction, and deformation of the rear compressor shaft. This led to the compressor assembly contacting the walls of the engine case.
Figure 10: Illustration of T53 engine and exhaust diffuser inner cone (inset)

Source: Honeywell, modified by the ATSB
Considering the contact between the tapered section of the drive shaft and the compressor assembly, Honeywell reported that, ‘by design, this was the most critical section for inter-shaft clearance of the counter-rotating components. Rapid frictional heating is imminent once the rub condition is established. All damage, therefore, is considered secondary to the fatigue cracking of the exhaust diffuser struts’.
High-cycle fatigue
Regarding the material analysis of the exhaust diffuser housing, Honeywell identified that:
- the cracking in the strut/inner cone weld joints resulted from high-cycle fatigue emanating from multiple initiation sites along the inner edge of the weld bead, which was likely driven by power turbine vibration
- no material anomalies were observed
- the chemistry of the exhaust diffuser housing was indicative of the manufacturer’s specified material
- the measured hardness of the strut, inner cone, and weld bead indicated that the assembly was heat treated subsequent to welding, as specified.
Honeywell reported that ‘the exact initiation locations [of the fatigue cracks] were unable to be determined due to secondary smearing damage’. Further, due to the post-accident damage to the engine and airframe structure, the ATSB concurred that it was not possible to determine the source of the power turbine vibration.
Visible indications of cracking
Honeywell advised that they have had some previous experience with cracking on exhaust diffuser assemblies. Specifically, they indicated that:
Empirical evidence suggests that the cracking develops and propagates over a considerable period of time, i.e. hundreds of operational hours. Therefore, it is believed that the exhaust diffuser cracking and material loss from the inner cone would have been visible during the most recent Phase Inspection performed 20.8 hours before the accident. Visual indications of cracking were likely present during the preceding phase inspection(s) as well. An investigation to assess and rectify the exhaust diffuser cracking would have necessitated the removal from service of the exhaust diffuser.
This indicated that cracking and missing material on the inner cone of the exhaust diffuser, as observed by the ATSB after the accident, was likely visible during maintenance inspections prior to the accident. Further, Honeywell stated:
During the previous 40 years, this is only the third reported incident of exhaust diffuser strut cracking that developed sufficiently to cause an engine malfunction in Honeywell’s experience with the T53 series engine. Typical experience for the T53 is that removal of the exhaust diffuser for observed cracking will necessitate off-engine inspections and repairs to the inner struts, as required.
This indicated an expectation that if the visible cracking in the exhaust diffuser was identified, removal of the exhaust diffuser would be required. Subsequent inspections would have led to the identification of the cracking in the inner struts.
Maintenance arrangements for VH-HUE
HUE had been maintained by Encore Aviation (Encore) since March 2016. Encore was a CASA‑authorised maintenance organisation established in 2002 and provided maintenance to a variety of fixed and rotary-wing aircraft. Encore incorporated another maintenance organisation in 2017. The chief engineer of Encore at the time of the accident was from the organisation prior to incorporation. Encore was then acquired by another company in March 2019 (1 year after the accident). The role of chief engineer changed to another person at about this time, due to retirement.
Field maintenance
The services provided for HUE included field maintenance, when requested by the operator. The chief engineer at the time of the accident advised that, when a licenced aircraft maintenance engineer (LAME) was providing field maintenance for HUE, the LAME would perform the daily inspection. This arrangement was intended to relieve a pilot of extended duty, outside of their flying requirements.
With respect to daily maintenance performed by the pilot, the pilot reported doing ‘fuel and oils, so walk around doing all the inspections…normal stuff…but I don’t actually do any maintenance because I travel everywhere with an engineer [LAME]’. This included the expectation by the pilot that the daily inspection, which included the requirement for an inspection of the exhaust diffuser housing, was conducted by the LAME. The LAME who provided field support for HUE reported that ‘they generally completed the greasing requirements’[6] and the pilot conducted the daily inspection. This LAME also advised that they had carried out a daily inspection on occasion, when specifically requested by the pilot. A review of records identified the LAME’s signature on a maintenance release daily inspection for HUE, dated in November 2017. The pilot reported that the LAME had conducted a compressor wash and greasing prior to the flight on the morning of the accident.
Phase inspections
The two most recent phase inspections, in January and April 2018, were conducted in the hangar by different LAMEs at Encore. The chief engineer reported that HUE was maintained in accordance with the US Army technical publication requirements, which were last updated in 2010.
Exhaust diffuser inspections
Inspection requirements
The tailpipe and exhaust diffuser could be readily accessed via a ladder (Figure 11). Inspection of this area was typically carried out with the aid of a bright torch and mirror. A borescope could also be utilised if closer inspection was warranted.
Figure 11: Typical exhaust, showing accessibility for inspection

Source: Honeywell
The US Army technical publications included the following inspection requirements for the exhaust area, including the diffuser (Table 1).
Table 1: US Army exhaust area inspection requirements
| Technical publication | Inspection requirements | Frequency |
| Flight operations manual | Engine exhaust - check | Before the first flight of the day |
| Flight operations checklist |
Engine compartment - check Engine exhaust - check |
Before every flight |
| Preventative maintenance daily inspection checklist | Engine combustion chamber housing, exhaust diffuser, support cone, fire shield, firewall gaskets and seal, and tailpipe for cracks, dents and burned or buckled areas | Daily – prior to the first flight of the day |
| Phased maintenance checklist (‘phase inspection’) |
Engine exhaust tailpipe for cracks, dents and burned or buckled areas Perform a daily inspection at the completion of the phase check |
Every 150 hours |
Recent exhaust diffuser inspection opportunities
In consideration of Honeywell’s comment that the exhaust diffuser cracking was likely visible at the previous two ‘phase inspections’, the ATSB examined the potential opportunities for detection. In 2018, HUE underwent phase inspections on 11 January and 1 April. Following each of these inspections, a new maintenance release was issued. From 11 January 2018 to the accident flight, a review of the maintenance release records showed 34 daily inspections, certified by four different people. It was permissible for these certifications to be made by the pilot in command, another pilot licenced to fly the helicopter or an appropriately qualified LAME. In addition to the pre-flight and phased maintenance inspections, maintenance records indicated another eight separate maintenance visits to the maintainer had occurred in the 4 months prior to the accident. The helicopter had accumulated 171 flight hours in this period.
Vibration checks
Rotating components, in the airframe and engine, are the primary source of vibration in helicopters. Maintaining vibration levels within manufacturer-specified limits is essential in enabling components to be functional for their projected life limit. If excessive vibration continues over time, the wear on components will increase exponentially to the point of failure. In addition, this vibration can affect the fatigue life of stationary components.
US Army vibration requirements applicable to HUE
The US Army engine maintenance manual required an engine vibration test be conducted following certain maintenance actions, including:
- any maintenance that required removal and reinstallation of an engine for any reason
- when excessive engine vibration was suspected
- when more than 20 per cent of the total number of compressor blades were repaired to maximum limits.
Vibrations levels at specified engine revolutions per minute (RPMs) were to be recorded on the US Army Engine Vibration Test Data Sheet (vibration data sheet) applicable to the helicopter. The data sheet also detailed the maximum permissible vibration for each parameter. For HUE, a maximum vibration level of 2.5 inches per second applied to the majority of the tested parameters.
Maintenance records on vibration checks
Encore advised that, up to the time of the accident, they did not use the US Army vibration data sheet or keep physical records of vibration test data. Instead, they relied on the vibration test equipment internal memory storage for maintaining a record of the test results. However, during the investigation, Encore reported that their equipment suffered a major failure that required its return to the manufacturer for repair, resulting in a loss of all the stored data.
A review of the maintenance records identified that the engine had been removed from the helicopter for repairs from foreign object damage and re-installed on 12 November 2016, 417 hours prior to the accident. A vibration check had been conducted at that time. The certification indicated the vibration was ‘within limits’, however, no vibration data had been recorded. In addition, associated maintenance worksheets were not available as Encore did not retain these records beyond 24 months.[7] In accordance with the US Army engine maintenance manual, a re‑check of the vibration was required at 500 and 1,000 hours’ time-in-service. However, the engine had not accumulated 500 hours prior to the accident.
The engine logbook indicated that, on 1 April 2018, the top axial compressor half had been removed from the engine to repair minor foreign object damage to multiple compressor rotor blades. This was recorded as having been conducted in accordance with the US Army maintenance manual. However, there was insufficient information recorded by maintainers in HUE’s maintenance records to determine if a vibration check was required in this instance. Specifically, it was unclear if more than 20 per cent of blades required repair to maximum limits, which would have triggered the US Army requirement for a vibration test. Regardless, the engine logbook did not include any indication that a vibration check had been carried out.
Guidance for record keeping and trend monitoring
Trend monitoring in this investigation refers to the process of evaluating historical data to identify anomalies that may indicate an emerging technical failure of the engine. This process is generally considered to be in-line with industry best practice as a method to identify underlying problems before a safety incident occurs, such as the engine failure of HUE. This is supported by guidance produced by Civil Aviation Advisory Publication 30-04 Certificates of approval – Maintenance organisations, which set out the procedures that CASA would expect an authorised maintenance provider to have in place ‘to ensure that aviation safety is not compromised’. This publication stated that, part of an organisation’s quality system should detail ‘procedures for monitoring the other quality indicators such as facility malfunction reports, incidents, occurrences, maintenance errors, complaints and defects’.
The US Army engine maintenance manual, Section 1-73 General troubleshooting, provided a general statement with respect to identifying the source of failures, referred to as ‘general troubleshooting’, stating:
It is essential to have a thorough knowledge of specified fuel flow, oil pressure, exhaust gas temperature and other important specifications of normal engine operation to discover troubles. Having a record of prior trouble and work performed is essential when troubleshooting.
Although this advice did not specify requirements for vibration trend monitoring, it noted the general importance of recording prior work and ‘trouble’ encountered. In summary, these documents present ‘defect reporting’ and ‘record keeping’ as important sources of information for the effective management of continued airworthiness.
Review of Encore Aviation maintenance practices
VH-HUE replacement of engine related components
HUE’s maintenance records indicated that the power turbine (N2) tachometer generator[8] had been replaced four times: 29 August 2017 (10,060.0 aircraft hours), 27 November 2017 (10,146.4 hours), 11 January 2018 (10,200.3 hours) and 16 January 2018 (10,204.9 hours). The records did not detail the exact nature of each unserviceability. On 1 March 2018 (10,304.3 hours) the drive assembly for the tachometer generator was replaced, recorded in the maintenance logs as ‘suspect’. Again, there was no indication that further evaluation, such as a vibration check, had been conducted following any of these maintenance actions.
VH-HUE phase inspection documentation
The ATSB reviewed the worksheets and logbook entries for the phase inspections for HUE that were completed on 11 January and 1 April 2018. Inconsistencies were found in certification requirements including inspection items not certified as ‘completed’ or ‘not applicable’, and no indication of reference data. Therefore, it could not be established if these specific inspections were, or were not, performed.
Surveillance findings
From 24 October to 1 November 2018, CASA conducted a surveillance event of Encore and released a report documenting their findings. The surveillance was triggered by CASA becoming aware of a Cessna 172 (C172), maintained by Encore that had:
…significant defects and corrosion relating to inspections that should have been identified as part of SIDS [supplemental inspection documents] inspections.[9] The aircraft had been maintained by Encore Aviation and it was clear that significant anomalies related to execution of the mandatory inspections had occurred….
The CASA surveillance report noted that the C172 had been grounded while undergoing maintenance at another maintenance organisation to correct the ‘significant defects and corrosion’. This aircraft was operated by a company offering flight training, and it was expected that it was primarily used for this purpose. As a result of the surveillance, CASA issued three findings, applicable to the C172 and two Cessna 310 (C310) aircraft also maintained by Encore, which identified:
- maintenance releases had been issued for certain aircraft, when all required maintenance had yet to be completed
- tasks had been certified as complete when not all items within that task had been performed as per the maintenance instructions
- various examples of certifications not containing reference data: using a stamp rather than a signature and missing date information.
The certifications identified in the report had been made between June 2016 and April 2018. Findings documented for the C172 aircraft included significant corrosion found in the area of the forward spar of the horizontal stabiliser and trim bracket, with cracking identified in the trim bracket. The horizontal stabiliser is considered a single point of failure for the aircraft, with failure expected to lead to an unrecoverable loss of control. Furthermore, the aircraft maintenance release was issued without a required inspection on the wing root rib being certified in the worksheets or aircraft logbook. This inspection was for the purpose of corrosion detection using non-destructive testing. In addition, CASA identified that the aircraft maintenance release was issued without a required engine mount inspection being performed.
The two C310 aircraft were operated by a company providing charter and aeromedical flights. Findings on these aircraft indicated that inspections on critical aircraft components were not performed, specifically relating to the elevator torque tube, wing lower rear spar carry through, wing lower front spar root, horizontal stabiliser spar attachments and engine support beam. These are all areas representing potential single points of failure leading to loss of control if any of these components failed in-flight.
Alternate options for continuing airworthiness
The Honeywell Aerospace (Honeywell) type-certified equivalent engine is designated the T5313B. The T53-L-13B engine is the military variant, as denoted by the ‘L’ in the model designation. Honeywell advised both engine types are ‘very similar, if not the same. The difference is that Honeywell owns the design and ICA [Instructions for Continued Airworthiness] responsibility for the commercial / type certified version, whereas the US Army is responsible for the design and ICA for the military variant’.
In 2010, Honeywell published a service bulletin T53-0173 R1 to owner/operators, where military variants could be ‘upgraded’ at overhaul, to align with civil standards. Honeywell had identified that ‘maintenance of T53 engines under the US Army and foreign military systems are not equivalent to standards of Honeywell Aerospace. Differences between the maintenance concepts exist in cycle counting, parts procurement, engine assembly tolerances, and general maintenance practices’. While not required by regulations, this ‘upgrade’ would have enabled the engine fitted to HUE to be maintained to Honeywell technical publications, which were routinely updated to represent current best practices. In contrast, the US Army publications had not been updated since 2010, as far as could be determined.[10]
Honeywell vibration maintenance requirements
The Honeywell T53-L-13B engine maintenance manual required a vibration check to be conducted upon installation into the airframe and after ‘repair/replacement of major components’, including:
- after compressor blade replacement or compressor blade repair or blending
- when excessive engine vibration was suspected.
Honeywell advised that, in 2008, they ‘undertook some actions to ameliorate the risk of exhaust diffuser cracking. Specifically, the power turbine component balance process was enhanced and the vibration limits reduced’. This was initially incorporated at the engine overhaul level (from the factory). These reduced limits were subsequently incorporated in the maintenance manual (T53-L-13B) in 2015. The maximum permissible limits, at specified parameters, were now 1.3 and 1.7 inches per second. In contrast, as noted above, the US Army manual limits were 2.5 inches per second. In addition, the Honeywell maintenance manual required a vibration check after any compressor blade repair, in contrast to the US Army requirement of more than 20 per cent.
Compared to the US Army requirements applicable to HUE, the Honeywell maintenance requirements were more stringent with respect to engine vibration inspections. Although not required, upgrading HUE to this standard may have provided additional opportunities for the detection of emerging engine problems.
Conduct of the forced landing
Height-velocity diagram restrictions
A successful forced landing in a single-engine helicopter can only be achieved if the helicopter has sufficient energy to achieve its required landing deceleration and touch down configuration, and the pilot has sufficient time to initiate a recovery to this configuration. The height-velocity envelope shows the combinations of height above the ground and forward velocity (airspeed), which have been demonstrated by flight test to allow, and which are also predicted to not allow, the pilot to complete a safe landing after an engine failure. These combinations of height and airspeed are primarily for use during the take-off or landing manoeuvre or when manoeuvring at low level, such as in long-line operations.
For single-engine helicopters, the height-velocity envelope for complete power failure must be established by the manufacturer at the time of certification. When constructed in the aircraft flight manual, the height-velocity envelope typically delineates areas that represent safe combinations of airspeed and height, and areas that represent combinations of airspeed and height that should be avoided. The avoid areas are specific to the helicopter design and are normally associated with increasing height and slow or no airspeed flight (hover as is the case with long lining) and low height with high airspeed.
The US Federal Aviation Administration (2019) also stated that:
As the airspeed increases without an increase in height, there comes a point at which the pilot’s reaction time would be insufficient to react with a flare in time to prevent a high speed, and thus probably fatal, ground impact.
Conversely, an increase in height without a corresponding increase in airspeed puts the aircraft above a survivable un-cushioned impact height, and eventually above a height where rotor inertia can be converted to sufficient lift to enable a survivable landing. This occurs abruptly with airspeeds much below the ideal autorotative speed (typically 40–80 knots). The pilot must have enough time to accelerate to autorotation speed in order to autorotate successfully; this directly relates to a requirement for height.
The nature of the long-line operation required HUE to enter the avoid area during the load hook‑up and unhook sequences. Further, comparing the height, airspeed and weight to the height-velocity diagram applicable to HUE established that it was likely within the avoid area at the time of the engine failure. This indicated that the pilot had limited options to manoeuvre following the engine failure.
Pilot decision-making and forced landing
The pilot reported that there were personnel working in and around the drill site when the helicopter was on approach to hook-up the load (the drill site also included a helipad). This was supported by time-lapse images from the drill site, which confirmed ground personnel moving in and around the drill site, including this approach. Consequently, when the engine failed, the pilot attempted to autorotate[11] the helicopter clear of the drill site and towards the river to keep clear of ground personnel. When asked where the pilot would have conducted the forced landing if the drill site was assured to be clear of personnel, the pilot reported that the drill site (Figure 12) would have been used. Figure 12 also shows the high trees and generally inhospitable terrain surrounding the drill site.
Figure 12: Drill site looking in direction of flight

Source: ATSB
The GPS data, time-lapse images (location shown in Figure 12), supplied camera footage from eyewitnesses and witness statements were evaluated to determine the sequence of events from the engine failure to the collision with terrain. At 1417:33, the helicopter was observed approaching the drill site (indicated by Figure 13 ‘A’). Following the loss of engine power (Figure 13 ‘B’), the aircraft started descending and began to accelerate (Figure 13 ‘C’). As the helicopter approached the line of trees at the end of the clearing, the helicopter had accelerated to about 40 kt and was close to the height of the tree canopy (Figure 13 ‘D’ and ‘E’). Around this time, GPS flight data indicated a notable shallowing of the descent profile.
Figure 13: Time-lapse composite showing helicopter engine failure location and forced landing

Source: GHD, modified by the ATSB
The shallowing descent path was consistent with witness reports describing the helicopter as appearing to ‘float’ over the trees, and that it was not descending quickly until over the trees. Comparison of this glide performance with the published performance charts for HUE revealed this ratio was shallower than the autorotation range performance based on the speed and rate of descent. The pilot reported that, during this time the main rotor speed (RPM) became low. Audio analysis[12] by the ATSB using witness phone footage established that the main rotor speed was about 214 RPM as the helicopter passed over the first line of trees, about two-thirds below the optimal speed of 314 RPM. This suggested that the pilot increased collective pitch of the rotor system to avoid the line of trees prior to reaching the gap in the canopy created by the river below. The pilot stated during interview that the helicopter’s rotor system carried a lot of inertia, and as a result, elected to fly over the trees, knowing that the rotor speed would decay. The pilot’s response was consistent with guidance in the US Army operator’s manual, which stated that a ‘landing in trees should be made when no other landing area is available’. The reduction in rotor speed is a concern during an autorotation as this equates to energy available in the rotor system. As a result, the energy available to arrest the descent rate during landing or to cut through tree branches was reduced.
Lifting operations
Helicopter lifting operations were utilised to demobilise the drill site due to the remote location of the site and to minimise the environmental impact within the Kosciuszko National Park. Consequently, helicopters involved in the lifting operation were required to operate over terrain that was generally not suitable to make a safe landing.
Organisational information
There were four organisations working together during the lifting operation on the day of the accident. GHD Limited (GHD), another geotechnical company contracted by GHD, Heli Surveys and O’Driscoll Aviation. Ground-based geotechnical survey works at the drill site were coordinated by GHD Limited, in conjunction with the geotechnical company (geotechnical crew). GHD was contractually responsible to Snowy Hydro for the safety management of all works to be conducted at relevant sites.
Helicopter operations were led by Heli Surveys. They had a contractual arrangement with Snowy Hydro to provide helicopter services to support the drilling sites at the direction of GHD. In turn, GHD were contractually responsible for ‘liaison and coordination’ with Heli Surveys. As some loads exceeded the capability of Heli Surveys, they sub-contracted O’Driscoll Aviation (HUE) to lift these heavier loads.
GHD reported to the ATSB that they were responsible for safety management for works on the ground and Snowy Hydro were ultimately responsible for the risk management of all operations, both in the air and on the ground. Snowy Hydro reported that GHD were the principal contractor for all operations and therefore, it was their understanding that GHD were responsible for the risk management activities.
The works on the day of the accident followed the completion of a geotechnical survey at the drill site and involved helicopter lifting of all the main drill rig components to the laydown area. This involved three geotechnical workers deconstructing the drill rig and two load-masters from Heli Surveys, with GHD managing the aviation component of the operation. This included preparation of loads for helicopter lifting, providing direction to the helicopter pilots via radio communications, and hooking up loads.
Lifting operations risk assessment and toolbox talk
The pilot reported attending a meeting, referred to as a ‘toolbox talk’, that involved all ground personnel and pilots prior to the lifting operation. The toolbox talk was led by representatives from GHD and Heli Surveys. This discussion included the loads to be lifted by each helicopter and safety considerations. Heli Surveys reported that part of the safety considerations included discussion of a ‘sterile zone’. This sterile zone was reported as being:
…an area where all personnel on the ground are to avoid at all times. This is usually the area on the opposite side of the aircraft to where the pilot sits. The reason for this “zone” is to give the pilot an area to land in if a forced landing is required. Although the area might not be clear of obstacles, the pilot can be confident it is clear of people on the ground.
Further, as part of these discussions, all crew, including the pilot of HUE, signed a ‘pre‑work assessment’ form indicating attendance at the meeting and compliance with the Safe Work Methods Statement. Part of the purpose of the form was to:
…discuss the planned activities and hazards and modify [Safe Work Method Statements] (SWMSs) if required.
GHD, in consultation with Heli Surveys, developed a ‘helicopter operations hazard identification’ register, referred to hereafter as the ‘risk management plan’. According to GHD, this represented the safe work method statement referred to in the ‘pre-work assessment’ form, that applied on the day of the accident. GHD were reliant on Heli Surveys providing subject matter expertise to identify aviation related hazards, risks and controls. Neither of these documents were provided to the pilot before the day of the accident for review, however, the pilot was aware of the general procedures having previously worked with Heli Surveys. A sample of the risk management plan is reproduced in Table 2, noting that only an extract of one assessment is shown for illustrative purposes only.
Table 2: Reproduced sample from risk management plan
| Job step | Identified hazards | Mechanism /pathway of harm | Initial risk level (A-D) | Control measures | Residual risk level | Control measures/responsibility for implementation |
| General site works | Unfit for work |
No induction … |
B |
Project induction … |
D |
… Safety Management Plan All Personnel |
The risk management plan identified hazards that were assigned an ‘initial risk level’ (Table 2). The specific ‘mechanism’ or ‘pathway’ was also recorded. Control measures were then listed, in order of preference, before being assigned a ‘residual risk level’. The risk management plan consisted of key operational activities grouped into a ‘Job step’, which included general site works (shown in Table 2), driving to site, pre-flight actions, passenger embarkation/disembarkation, mountain flying, ground operations and aircraft refuelling. Some of the job steps identified several pathways of harm to ground personnel during load-lifting as:
- Ground operations: ‘Load not slung correctly’, ‘Load not correctly packaged’, and ‘Slung load out of control or not flying correctly’. Controls for this were related to having a lifting plan and ensuring the plan and long-line rigging was correct.
- Mountain flying:
- ‘Lifting loads over buildings/people and wires’, which involved the pilot ’determining the most appropriate flight path away from obstructions and people etc’. Falling trees/branches caused by downwash were also considered for the load drop-off site. However, these controls related to the helicopter with an attached load or at the drop-off site.
- ‘Aircraft collision with spectators, objects, animals, during take-off and landing’. This had the associated risk control of ‘spectators are to be kept clear by ground personnel. If no ground personnel are present and spectators cause undue risk, an alternative landing site must be found’.
The hazard of an ‘emergency situation’ was also included in the risk management plan. Controls for this stated:
Each emergency situation is different and requires a unique set of procedures. All procedures set out in the Pilots Operating Handbook and the Flight Manual must be followed.
However, there were no control measures that explicitly addressed the risk to people underneath the helicopter for that hazard.
Despite the above, there was no specific job step for load-lifting operations in the risk management plan. Further, the risk management plan did not consider the risks to ground personnel when the helicopter was on approach to pick-up a load, which was where the engine failure occurred.
Retention of the long-line
In the days prior to the accident flight, the pilot was involved in bush firefighting operations on behalf of the New South Wales Rural Fire Service (NSW RFS). Equipment utilised during firefighting operations consisted of a long-line, connected to the helicopter belly-mounted hook. A Bambi Bucket was connected to the remote hook, at the base of the long-line. The remote hook worked independently to the belly hook and was powered by an electrical cable attached to the long-line (depicted in Figure 6). A Sacksafoam kit, which was used to provide a precise quantity of fire-retardant foam to the Bambi Bucket, was also fitted.
The Sacksafoam kit used in HUE consisted of a case located in the helicopter, which delivered the foam to the bucket via a hose. The kit included a short hose and junction, that reached from the case, around the fuselage, to the aircraft hook area. The helicopter operator then supplied the remaining length of hose required to deliver the foam to the bucket itself. An orange protective sheath held the second length of hose, electrical cables, and long-line together along the length of the line.
It was identified that a screw clamp (Figure 14) and barbed fitting had been utilised at the Sacksafoam-to-operator hose junction, located near the aircraft hook assembly. This was in contrast with the installation manual, which required the hoses to be connected via a barbed connector, without the use of clamps. The purpose of the barbed connector was to allow the hose to disconnect in the event of the long-line and bucket being released by the pilot from the belly hook in an emergency. It was this ‘clamped’ hose that prevented the complete release of the long-line from HUE.
The pilot reported that the screw-clamp had been fitted (Figure 14), in addition to the barbed fitting, to prevent the hose from ‘popping’, and leaking corrosive foam from the hose junction.
Figure 14: Operator hose with screw clamp installed

Source: ATSB and SEI Industries, annotated by the ATSB
Survival aspects
Pilot injuries
The pilot was wearing a helmet and lap-belt on the accident flight. During the impact sequence, the pilot sustained serious injuries, including a fractured right eye socket and nose. In addition, the pilot also suffered ligament damage surrounding the ribs, and ligament and tendon damage around both ankles and left knee.
Post-accident response
After witnessing the accident, video footage showed four of the workers at the drill site gathering fire extinguishers and immediately moving in the direction of the helicopter before the sound of the impact. One of the loadmasters stayed at the drill site and called for help via satellite telephone and radio. Upon arrival at the accident site (Figure 5), the first responders noticed fuel leaking down the outside of the fuselage. Fire was also observed in the area of the engine bay and fire extinguishers were deployed toward this area to extinguish the fire. Meanwhile, two workers assisted the pilot, who was unable to exit the wreckage, with moving safely away from the helicopter before commencing first aid.
The pilot of another helicopter (supporting the Snowy 2.0 project), who heard the Mayday call, flew to the drill site and dropped off three additional workers to assist. These workers gathered additional first aid supplies and assisted with rescue coordination. A third helicopter (also supporting the project) arrived at the site about 24 minutes after the accident, with two medical personnel. About 2 hours after the accident, the injured pilot was winched from the site and transported to hospital.
Liveable space
Measurements of the floor pan against published dimensions revealed no detectable deformation in the area where the pilot was sitting. This included the area of the floor pan from the position of the rudder pedals to the rear of the pilot’s seat. Furthermore, the wreckage examination did not reveal evidence of any intrusions to the occupied area. Therefore, the area occupied by the pilot did not appear to have been compromised during the accident.
Cockpit interior damage
The left side of the instrument panel and sunshade were damaged, consistent with being pushed forward from within the cabin in front of the pilot’s seat (Figure 15). For comparison, the right-side dash panel was undamaged. Although the windscreen exhibited extensive cracking, a localised concentration of damage was present in front of the left pilot seat, the position occupied by the pilot. The damage to the cockpit and injuries sustained were consistent with the pilot’s upper torso flailing forward during the accident sequence, sufficient for the pilot’s helmet and face to strike the instrument panel sunshade and windscreen.
Figure 15: Interior instrument panel sunshade and windscreen damage adjacent to pilot

Source: ATSB
Occupant protection systems
The pilot’s seat was fitted with a 4-point lap-belt and shoulder harness on an inertia reel. However, the shoulder harness (upper torso restraint (UTR)) was not worn. The pilot stated that, due to the nature of the long-line operations, it was not possible to use the shoulder harness and lean left into the door bubble-window to view the long-line and maintain the helicopter position for load hook-up and unhook operations. The helicopter was not fitted with energy absorbing seats designed to minimise vertical accelerations during impact, although this did not appear to influence the pilot injuries.
Flail analysis
The ATSB estimated the extent of pilot upper torso movement while restrained by the lap-belt worn at the time of the accident. This was focussed on backward horizontal accelerations leading to the pilot flailing forward. Two independent methods were adopted. The first assumed a circular arc traversed by the pilot’s head. The second method, derived from an empirical study by Young, J.W. (1967), was scaled for the sitting height (94 cm) of the accident pilot. The second method also provided an assessment of the probable movement a UTR was worn by the pilot.
Figure 16 shows a head forward flail circular arc, which indicated that the pilot’s head could contact the instrument panel and windscreen if restrained only by the lap-belt. Projections indicated the middle third of the pilot’s head aligned with the instrument panel and sunshade.
Figure 16: Pilot seat and cockpit side view with circular arc based on pilot sitting height

Source: ATSB
Young’s (1967) study compared the effectiveness of lap-belts combined with various UTRs and lap-belt only. This study found that there was a significant difference in forward and downward motion between using any shoulder harness and lap-belt compared to wearing only a lap-belt. This was based on head kinematics recorded in the vertical plane for a dummy weighing 82 kg and a sitting height of 97 cm, on a sled travelling at about 45 km/h prior to impact. Using the results of this study, assessments were performed by the ATSB to indicate the range of forward movement of the accident pilot for two scenarios – with, and without the use of a UTR (Figure 17).
The left diagram of Figure 17 shows the empirical projections of the dummy wearing a lap-belt only (from Figure 4 of Young (1967)) intersecting the approximate location of the instrument panel and sunshade. In contrast, the right diagram shows considerable distance between all dummy projections and the instrument panel (Figure 11 of Young (1967)). These results were consistent with the instrument panel damage and injuries sustained by the pilot.
Figure 17: Comparison of lap-belt and UTR effectiveness, with approximate location of HUE instrument panel and sunshade

Source: Young (1967), annotated by the ATSB
Upper torso restraint use
Benefits of upper torso restraint use
When correctly worn, UTRs form an important part of the occupant protection system in aircraft, and the benefits in reducing the likelihood and severity of injuries is well established. A significant benefit of correctly fitted UTRs is the minimisation of body movement to prevent the body striking the aircraft structure in lateral and longitudinal impacts, as established by Young (1967). There is also evidence to suggest that UTRs may assist to align the spine in an anatomically ideal position during vertical impacts (Laananen, D.H., 1983, as cited in Coltman, 1985).
Research into previous helicopter accidents revealed no serious or fatal injuries in a sample of longitudinal-type impacts where occupants wore a UTR, ‘even at very high velocities’ (Coltman et al., 1985). In comparison, occupants not wearing a UTR were found to consistently sustain severe or fatal injuries at longitudinal impact speeds above 25 km/h, indicating the effectiveness of UTRs in preventing impact injuries to the head and torso. These findings are supported by accidents in fixed-wing aircraft, in which the US National Transportation Safety Board (2011) found that pilots who used lap-belts only were nearly 50 per cent more likely to be seriously or fatally injured compared with those who wore lap-belts with UTRs.
Vertical reference flying in Australia
Long-line operations, as was being conducted in this instance, require the pilot to rotate their upper torso so they can look out and down through a bubble-window, during the load hook-up and unhook stages of the flight. This type of operation is referred to as vertical reference flying.
The most significant proportion of vertical reference flying operations were expected in firefighting operations, with more than 20,000 firefighting flights conducted in Australia in 2018.[13] Some of these flights may not require vertical reference flying techniques, such as fire spotting, and firefighting using integrated tanks and a snorkel. However, a significant number of these flights are likely to be vertical reference flying. In addition, about three-quarters of firefighting flights were conducted using single-engine helicopters. Firefighting operations were the majority of the flying performed by the pilot of HUE.
Vertical reference flying techniques are also used for construction sling-load work, similar to the accident flight. About 3,000 flights per year were recorded for construction sling-load work in 2018, mostly involving single‑engine helicopters.
Utilisation of upper torso restraints
Investigated occurrences
To identify the state of UTR use during vertical reference flying operations, a review of investigated aviation safety occurrences was conducted. This involved searching the ATSB’s aviation occurrence database and for comparison, the website of the Transportation Safety Board of Canada (TSB). The TSB were selected due to Canada being known to have a considerable amount of vertical reference flying activity. Australian investigations were identified using a regular expressions-based[14] search for terms commonly indicating the conduct of vertical reference flying. Canadian investigation records were identified by a text search for ‘long line operations’. These records were then manually verified as vertical reference flying operations and reviewed for evidence of UTR use.
At least[15] 14 Australian and 9 Canadian investigations involved the conduct of vertical reference flying operations between January 2000 and June 2020 (Figure 18). From the 14 Australian investigations it was found that 4 pilots confirmed they did not wear their UTR (recorded as ‘No’ in Figure 18), 1 partially wore it (recorded as ‘Partial’), 1 did wear it, and 8 were unknown. For the partially worn case, it was found that the UTR provided no benefit due to it being incorrectly worn. Therefore, where the use of UTR was determined,[16] it was found that 67 per cent (4/6) of pilots were not wearing their UTR, and 83 per cent (5/6) when considering cases where the UTR was not effectively worn. This result was consistent with known cases in Canadian investigations. When considering all investigated occurrences (including unknown cases), at least one-third of pilots conducting vertical reference flying were not correctly wearing a UTR.
The confirmation from several pilots in Australian investigations that they were not wearing their UTR was consistent with the physical restriction it would impose on rotating the upper torso for vertical reference flying. This was supported by one of the TSB investigations that stated ‘as is typical with many pilots involved in vertical reference flying, the pilot did not use the shoulder restraint system provided’ (TSB report A08P0265).
Figure 18: Number of pilots in ATSB and TSB investigations involving vertical reference flying by upper torso restraint use, January 2000 to June 2020

Source: ATSB
Industry experiences
The ATSB held a meeting with the Australian Helicopter Industry Association (AHIA) to discuss the issue of UTR use for vertical reference flying in light of investigation findings.
In general, investigations identified factors such as cockpit dimensions and seatbelt design probably contributed to the lack of UTR use by pilots conducting vertical reference operations. For example, ‘Most helicopters are not designed or certified to accommodate vertical reference external load operations; however, these operations are very common and pilots fly in this higher‑risk environment without proper safety-restraint devices’ (TSB report A05P0103). When these findings were reviewed by the AHIA, it was generally agreed that this practice was probably adopted due to the sideways leaning required by the pilot during vertical reference flying, rather than for reasons of comfort.
During the meeting with AHIA, the limitations of the accident helicopter were discussed. Helicopters such as HUE were expected to present greater challenges to vertical reference flying due to the distance between the pilot seat and door, coupled with an older-style seat-belt webbing being fitted. This was despite having a number of modifications to assist leaning into the bubble‑window to look down, such as some of the cockpit instruments being duplicated and mounted on the door. It was reported that, despite these modifications, the design of the harness inertia lock release mechanisms were generally insufficient to allow pilots to lean outside without a work-around, even if fitted with modern harnesses. One such reported work-around was wearing the UTR, but slipping one strap underneath the arm to aid leaning out and prevent the belt pressing into the pilot’s neck.
The consensus from the AHIA representatives was that the previous and current investigation findings were generally consistent with their collective experience. It was agreed that lack of UTR use or wearing the UTR differently to that recommended, was a commonly adopted practice during vertical reference flying. Specifically, due to the UTR impeding a pilot’s ability to effectively conduct vertical reference flying operations. This was expected to affect multiple helicopter types frequently used in long-line operations that were not initially designed for this purpose. However, they also acknowledged there was no readily available market solution.
Solutions for restraint in vertical reference operations
A small number of helicopter models are specifically designed for vertical reference flying. These helicopters allow the pilot to conduct vertical reference flying while being fully restrained. However, these helicopters were expected to form a small proportion of vertical reference operations in Australia.
The ATSB was also aware of a number of innovations to assist in the conduct of vertical reference flying. These innovations were available to be retrofitted to helicopter models not specifically designed for regular vertical reference operations. For example, the fitment of light-weight webbing. It was reported that light weight and low friction webbing of these seatbelts would probably assist with vertical reference flying. However, these seatbelts were generally fitted within the existing guide mechanisms on the helicopter. As a result, it was expected that work‑around solutions, such as tucking the seat-belt under the arm were likely to still be required.
Reports have also been received about tilting seats fitted to some helicopters. These allow the pilot to remained fully harnessed, with the entire seat assembly tilting outside the helicopter structure to allow vertical reference flying. The accident pilot reported that these seats were limited for taller pilots. At the time of writing, it could not be ascertained how many, if any, of these systems were used in Australia.
Injuries associated with damaging vertical reference flying accidents
A short study was conducted by the ATSB to evaluate the possible influence of UTR use on accident-related injuries sustained during vertical reference flying operations. This involved comparing the proportion of accidents with injuries between vertical reference flying and the mean of all other helicopter aerial work, where the helicopter was substantially damaged or destroyed. These accidents were intended to represent scenarios where the flight crew would have experienced significant in-cockpit accelerations.
From the sample, it was found that flight crew were significantly more likely to receive an injury in a vertical reference flying accident where the helicopter was substantially damaged or destroyed compared to the mean of all other helicopter aerial work. It was identified that for two of these, including this accident, head injuries were likely sustained or made more severe due to improper, or lack of UTR use. While it was possible that these injuries contributed to the difference in the proportion of injuries between the two groups, this was unable to be determined as the nature of injuries or UTR usage in other aerial work was not known. This supports the need for further research in this area. Further results, including the methodology for this study can be found in Appendix A – Injuries associated with vertical reference flying compared to other aerial work operations.
__________
- According to Civil Aviation Safety Authority Advisory Circular AC-21.10 v4.2 (issued March 2019), some special certificates of airworthiness are issued to permit operations of aircraft that do not meet the requirements for a standard certificate of airworthiness, as was the case for VH-HUE, but are capable of safe operations under defined operating conditions and purposes. In recognition of the lack of compliance with some of the airworthiness standards, the aircraft is normally permitted to be operated under more restrictive operating conditions than in the case of a comparable aircraft operating on a standard certificate.
- ‘Greasing’ referred to the requirements in the maintenance manual of HUE for periodic lubrication of components at nominated time intervals.
- Civil Aviation Order 100.5 General requirements in respect of maintenance of Australian aircraft, Part 5 ‘retention of aircraft maintenance records’, generally required retention for a period of 1 year.
- The power turbine (N2) tachometer generator provides engine RPM, as a percentage, to the instrument panel. It is mounted to a drive assembly (shown in red in Figure 8), at the 10 o’clock position on the exterior of the inlet housing and is driven through shafts and gearing from the power turbine shaft.
- The supplemental inspection documents (SIDS) were developed by Cessna, and required by CASA, to provide additional inspection criteria, to certain aging aircraft. The SIDs identified areas of the aircraft that were most likely to experience a principal structural element component failure under extended life operations.
- The US Army retired the UH-1 from active service in 2005. Residual aircraft were used for training only and the final UH-1 was retired in 2016.
- Autorotation is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
- Helicopter RPM was calculated by counting the time between audible ‘beats’ created by the helicopter rotor blades. Comparative analysis was performed with earlier footage confirming nominal RPM during normal operations.
- Provided to the ATSB by the Bureau of Infrastructure, Transport and Regional Economics (BITRE).
- Regular expressions methods refer to the use of sequence of characters as a search pattern. These were used to provide a more robust mechanism to identify records than conventional text searches.
- Due to vertical reference flying not being formally categorised by the ATSB or Canada, it is possible that additional flights were not identified in the selection. This is not expected to impact on these results.
- Investigations with unknown UTR usage were not considered to impact results because of the focus on the existence of lack of UTR use.
Introduction
While conducting long-line lifting operations near Talbingo in the Snowy Mountains region of New South Wales, VH-HUE (HUE) experienced an engine failure. During the subsequent forced landing, the helicopter collided with trees and a riverbed. The pilot sustained serious injuries and the helicopter was destroyed.
This analysis will discuss the factors contributing to the engine failure, including the maintenance procedures and practices that were in place at the time and the opportunities to identify the developing engine issue. It will also examine the limited options available for the forced landing, increasing the severity of the impact, and the risk management planning for personnel working near or underneath the helicopter in the event of an emergency landing. The limited ability for pilots to wear an upper torso restraint (UTR) during long-line operations will also be reviewed. Further, the retention of the helicopter long-line during the accident sequence, and the positive influence of ground personnel in recovering the pilot and reducing the potential severity of injuries are also discussed.
Engine exhaust diffuser inner strut fractures
While on approach for the twelfth lifting operation of the day, the pilot heard a mechanical ‘screaming’ noise, followed immediately after by a complete loss of engine power. The ATSB’s wreckage inspection identified cracking and missing material in the engine exhaust diffuser housing. Further examination of the engine by the manufacturer revealed extensive fatigue cracking led to the failure of the exhaust diffuser inner struts, which position the power turbine shaft. The loss of internal support resulted in interference between the power turbine shaft and compressor shaft, and subsequent failure of the engine.
Engine inspections
Following their examination of the engine, the manufacturer concluded that the cracking in the exhaust diffuser area was likely visible in at least the previous two phased maintenance inspections, which was at least 171 flying hours before the accident. Furthermore, 34 daily inspections had also been certified during this period. Another eight separate visits to the helicopter maintainer had also occurred during this time.
The phased maintenance inspections were typically conducted in a hangar by a licenced aircraft maintenance engineer (LAME) and involved a detailed inspection of the engine, where a higher level of scrutiny was expected. The daily inspection could be conducted and certified by a LAME or a pilot. This required a visual examination of the exhaust diffuser area, generally conducted in the field using a ladder, torch and mirror, which should have been sufficient to identify the cracks. However, there was a difference in understanding between the pilot and LAME as to who was responsible for conducting the daily inspections on HUE when in the field. Therefore, it was likely that the exhaust diffuser area daily inspection was not completed for all, or part of the period they were operating together with HUE.
Had the missing material and cracking been identified in any of these inspections, it would be reasonable to expect that further investigation of the exhaust diffuser would have been conducted. This would have typically involved removal of the engine for examination at an overhaul facility. However, for reasons that could not be determined, the missing material and visible cracking in the exhaust diffuser area was likely present, but not identified in either the phased or daily inspections, prior to propagating to the point of failure.
Maintenance practices and processes
The engine manufacturer concluded that the cracking in the exhaust diffuser would have been visible at the last phase inspection about 20 hours prior to the accident and likely visible at the preceding inspection about 171 hours before. These inspections were performed at Encore Aviation by two different LAME’s, neither of whom detected the cracking or the missing material. Similarly, another aircraft maintained by Encore Aviation was found to have significant defects and corrosion in critical components, which were not identified during routine maintenance, but were detected by another organisation. Also, two other aircraft that were used for passenger-carrying operations did not have inspections performed on critical components.
In addition to routine maintenance inspections, trend monitoring provides another mechanism for identifying engine deterioration, and the malfunction of engine components and accessories. In this case, the United States Army technical publication detailed when vibration checks were to be conducted on the engine type fitted to HUE and the maximum permissible limits. When adhered to, these should enable a component to reach its expected service life.
A vibration check had been conducted when the engine was installed in late 2016 and was recorded as being ‘within limits’. However, the actual vibration levels were not documented. Rather, the maintenance organisation’s standard practice was to rely on the internal memory in the test equipment for retaining a record of these values, which were subsequently deleted when the machine failed. While compressor blade repairs were conducted in early 2018, there was insufficient information available in the maintenance documents to establish if a vibration check was required and/or if one was conducted. Irrespective, this data could have been used as a baseline figure for comparison with future vibration checks to assist with trend monitoring. This was particularly relevant in this case given that the cracking resulted from high-cycle fatigue likely from excessive vibration of the power turbine.
The investigation also noted that an engine component associated with the power turbine assembly supported by bearings in the exhaust diffuser was replaced four times over a period of about 150 flying hours. In addition, the drive between the same engine component and the power turbine was also replaced during this time. The maintenance records did not detail the exact nature of each unserviceability, which provided limited information for identifying trends to detect anomalies. Therefore, it could not be established if this was also related to power turbine vibrations. Regardless, the repetitive replacement of a component should be cause for further investigation as trend monitoring has been shown to enable early detection of developing issues.
In addition to the above, the ATSB’s review of the 2018 maintenance records for HUE found inconsistencies in the documentation with regard to certification requirements. Likewise, following an audit in late 2018, the Civil Aviation Safety Authority also identified discrepancies regarding incomplete documentation and tasks being certified as completed although some had not been completely performed, covering the period 2016 to 2018. They subsequently issued three findings to the maintenance organisation.
While the ATSB was unable to review Encore Aviation’s operating procedures, the above demonstrates short comings in their maintenance practices and processes relating to inspections, record keeping and trend monitoring. Therefore, as was the case for HUE, it was unlikely that they were sufficient to detect the potential impending failure of safety critical components.
Forced landing
The lifting operation was being conducted over remote and mountainous terrain, with the drill site, that included a helipad, as the only clear area for a landing. On the day of the accident, ground personnel were observed moving in and around the drill site, including when HUE was on approach for the twelfth load. Therefore, when the engine failed, the pilot was not assured that the drill site was clear of personnel underneath. Consequently, out of concern for these people, the pilot moved HUE away from the drill site towards a river, which required the helicopter to clear a line of trees.
To clear the drill site and trees, the pilot had to reduce the rate of the autorotative descent, which resulted in sacrificing main rotor speed for range. Any loss of rotor speed will reduce the energy available for the rotor blades to cut through trees and arrest the rate of descent before contact with the ground. The helicopter subsequently impacted trees, leading to a complete loss of control before impacting the riverbed about 250 m away from the drill site. The combination of these factors likely contributed to the severity of the impact.
Alternatively, if the pilot was assured that ground personnel were clear of, or able to clear the drill site following the engine failure, the drill site and associated cleared area may have provided a suitable area for a forced landing. The option of a suitable forced landing site within the normal autorotation range profile would have allowed the pilot to use the stored rotor energy to conduct a normal autorotative landing and significantly reduce the risk of serious injuries.
Risk assessment for lifting operations
While the GHD risk management plan considered ground personnel during load lifting and take-off or landing, it did not capture hazards associated with the approach to, and during load hook-up. Consequently, the hazard of personnel being struck by the helicopter was not identified in this plan for the accident phase of flight. Similarly, risk controls in the event of an emergency did not specifically address the risk to personnel working near or underneath the helicopter. This indicated that, following an engine power loss, the documented plan would require the pilot in command to conduct the emergency landing, while also communicating with ground personnel to ensure they were clear of the drill site, which included the load pick-up area.
In this case, the pilot and witness statements, and time-lapse imagery, showed that the situation developed rapidly, with little time for decision-making and coordination. Although, it was reported that ‘sterile zone’ protocols were discussed, these were not documented in the risk management plan, despite other hazards and controls being identified. Therefore, a pre‑established plan detailing the actions and expectations of the pilot and ground personnel in the event of an emergency during this phase of flight would have been more ideal. This could have been achieved during a hazard identification workshop and documented in the risk management plan. This would have provided a prompt for the briefing on the day during the ‘toolbox talk’ and acted as an additional reference to those involved in the lifting operation.
Snowy Hydro contracted several organisations in support of the Snowy 2.0 project for the ground-based survey works and helicopter support. While the roles of each organisation were clear, there appeared to be a misunderstanding as to who was responsible for safely integrating the ground and air operations. This likely resulted in less oversight of the overall operation than was intended. This may have influenced the risk management plan not being sent to the accident pilot prior to the ‘toolbox talk’, which may have provided further opportunity to explicitly capture certain aspects of the load‑lifting operation.
Preplanning for an emergency situation is a critical component of risk management. For HUE, none of the controls in the risk management plan addressed the hazard of an emergency landing when on approach for load pick-up. As a result, this plan did not provide assurance to the pilot that ground personnel would be clear of the area if a forced landing at the drill site was required. This likely resulted in the pilot’s decision to attempt the forced landing away from the drill site to a less suitable location.
Upper torso restraint
The pilot was not wearing a UTR at the time of the accident as it interfered with the vertical reference flying that was being conducted. Consequently, the collision resulted in the pilot flailing forward at the waist and the pilot’s face impacting the instrument panel. The impact with the panel resulted in the pilot sustaining serious facial injuries. Although wearing a helmet probably reduced the potential for non‑facial head injuries, the helmet did not provide facial protection for the impact with the panel.
If the UTR fitted to the helicopter had been worn by the pilot, this would have significantly reduced the forward flailing motion of the pilot’s torso. Flail analysis of the potential torso movement with a UTR revealed it was virtually certain that the pilot’s face would not have struck the panel and therefore, would not have sustained the associated facial injuries. However, the ATSB noted that there appeared to be very limited after-market solutions currently available to the problem of vertical reference flying with a correctly worn UTR.
Upper torso restraints in vertical reference flying
In the last 21 years, from the ATSB investigations in which the use of a UTR was known, it was found that 83 per cent of pilots involved in vertical reference flying accidents were not effectively wearing the UTR, including the accident pilot. This was consistent with investigations from Canada and the experience of local industry members, who reported that it was a common practice for the UTR to be either partially worn or not at all.
In a short study of accidents where the helicopter was substantially damaged or destroyed, it was found to be significantly more likely for injuries to occur during vertical reference flying compared with the mean for other helicopter aerial work. This included two accidents where the head injuries were likely incurred from improper or lack of UTR use. This was consistent with the available literature, where it was found that wearing a lap-belt and UTR considerably reduced the likelihood of a fatal or serious injury to pilots in the event of an accident. In contrast, wearing a lap‑belt only significantly increased the chances of pilots sustaining upper body injuries. Therefore, the lack of use of the UTR was considered to be a large reduction in safety margins. Since most vertical reference flying in Australia is conducted for firefighting activities, this is currently the sector with the greatest exposure.
Therefore, based on investigation findings and reported industry experience, it was likely that UTRs were not routinely worn by a notable proportion of pilots during vertical reference flying. They were considered unlikely fit-for-purpose due to of the pilot’s inability to effectively view the long-line underneath the helicopter. This problem likely extended across the Australian helicopter industry and was not specific to the accident pilot or helicopter type.
Sacksafoam hose attachment
In response to the engine failure, the pilot attempted to jettison the long-line and strops from the helicopter. This opened the airframe mounted belly hook, which released the long-line, and the remote hook at the end of the long-line (via the electrical cable), which jettisoned the lifting strops. However, the wreckage examination established that the long‑line, which remained tethered by the Sacksafoam hose, did not fully detach from the helicopter. The fitment of a screw-clamp, installed by the pilot for firefighting operations in addition to the barbed connector, likely prevented the separation of the operator hose from the Sacksafoam hose. In turn, this prevented the long‑line from completely detaching. Although the retained lifting equipment did not contribute to the collision with terrain in this instance, it presented a snagging hazard, which increased the risk of a higher severity occurrence.
Emergency response
Prior to the sound of the helicopter impact, members of the ground personnel departed the drill site, with fire extinguishers and a first aid kit, and headed in the direction of the accident site. They assisted the pilot out of, and away from the helicopter, where medical aid could be administered. In addition, they extinguished a small fire in the engine bay, mitigating the risk of this, combined with leaking fuel, developing into a fuel-fed fire. These actions likely reduced the risk of more severe injuries to the pilot.
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision with terrain involving a Garlick Helicopters UH-1H, VH-HUE, 24 km south-east of Talbingo, New South Wales, on 17 April 2018.
Contributing factors
- On approach for a long-line lifting operation, the inner struts of the engine exhaust diffuser fractured as a result of fatigue cracking, which led to a complete loss of engine power.
- The fatigue cracks in the exhaust diffuser were likely present, but not detected in at least 34 daily and 2 phased maintenance inspections.
- Encore Aviation's maintenance practices and processes related to inspections, record keeping and trend monitoring, were likely inadequate to detect the potential impending failure of safety critical components. (Safety issue)
- The pilot did not have assurance that ground support personnel could vacate the drill site in an emergency. As a result, although the engine failed close to the cleared area, the pilot conducted the forced landing to a less suitable location, increasing the severity of impact forces during the subsequent collision with terrain.
- GHD's documented risk assessment for helicopter operations did not consider the hazard of an emergency landing at the drill site. This increased the risk that ground personnel were not clear of the load pick-up area in the event an emergency landing was required. (Safety issue)
- The upper torso restraint fitted to the pilot's seat was not worn during the long-line operations, which virtually certainly resulted in the pilot sustaining serious head injuries from the collision with terrain.
- Upper torso restraints were likely not routinely worn by a notable proportion of pilots conducting vertical reference flying operations in Australia, as they were likely not fit-for-purpose, increasing the risk of serious injury in the event of an accident.
Other factors that increased risk
- A screw-clamp was retrofitted to the firefighting retardant delivery hose, which prevented the long-line from being released from the helicopter during the emergency.
Other findings
- The immediate response of the ground personnel to extinguish a small fire and assist the pilot to exit the helicopter, likely reduced the risk of more severe injuries to the pilot.
|
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Maintenance practices and processes
Safety issue number: AO-2021-031-SI-01
Safety issue description: Encore Aviation's maintenance practices and processes related to inspections, record keeping and trend monitoring, were likely inadequate to detect the potential impending failure of safety critical components.
Risk assessment for lifting operations
Safety issue number: AO-2021-031-SI-02
Safety issue description: GHD's documented risk assessment for helicopter operations did not consider the hazard of an emergency landing at the drill site. This increased the risk that ground personnel were not clear of the load pick-up area in the event an emergency landing was required.
| AC | Advisory circular |
| AHIA | Australian Helicopter Industry Association |
| BITRE | Bureau of Infrastructure, Transport and Regional Economics |
| CAAP | Civil Aviation Advisory Publication |
| CASA | Civil Aviation Safety Authority |
| EST | Australian eastern standard time |
| FAA | United States Federal Aviation Administration |
| GPS | Global positioning system |
| ICA | Instructions for Continued Airworthiness |
| KNOTS | Nautical miles per hour |
| LAME | Licenced aircraft maintenance engineer |
| N2 | Rotational speed of the power turbine |
| NSW RFS | New South Wales Rural Fire Service |
| NTSB | United States National Transportation Safety Board |
| PT | Power turbine |
| QCPM | Quality Control and Procedures Manual |
| RPM | Revolutions per minute |
| SIDS | Supplemental Inspection Documents |
| SMS | Safety management system. A systematic approach to organisational safety encompassing safety policy and objectives, risk management, safety assurance, safety promotion, third party interfaces, internal investigation and SMS implementation. |
| SWMS | Safe Work Method Statement |
| TSB | Transportation Safety Board of Canada |
| US | United States |
| UTC | Coordinated Universal Time |
| UTR | Upper torso restraint |
Sources of information
The sources of information during the investigation included:
- accident witnesses
- Airservices Australia
- the Bureau of Meteorology
- the Bureau of Infrastructure, Transport and Regional Economics
- the Civil Aviation Safety Authority
- Encore Aviation
- GHD Limited
- Honeywell Aerospace
- the pilot of the accident flight and another pilot who conducted flights for the operator
- recorded data from the GPS unit on the aircraft
- Snowy Hydro Limited.
References
Civil Aviation Safety Authority (2007). Safety Management Systems: An Aviation Business Guide, Canberra, Australia.
Coltman, J.W. Bolukbasi, A.O. Laananen, D.H. (1985). Analysis of Rotorcraft Crash Dynamics for Development of Improved Crashworthiness Design Criteria, DOT/FAA/CT-85/11, US Department of Transportation, Federal Aviation Administration.
National Transportation Safety Board (2011). Airbag Performance in General Aviation Restraint Systems, Safety Study, NTSB/SS-11/01, Washington, D.C.
Young J.W. (1967). Functional Comparison of Basic Restraint Systems. Federal Aviation Administration, Office of Aviation Medicine Report No. AM 67-13.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Australian Helicopter Industry Association
- Bureau of Infrastructure, Transport and Regional Economics
- Bureau of Meteorology
- chief engineer
- Civil Aviation Safety Authority
- Encore Aviation
- field-based LAME
- Garlick Helicopters
- GHD Limited
- Heli Surveys Pty Limited
- Honeywell Aerospace
- Mulligan Geotechnical Pty Ltd
- pilot
- Snowy Hydro Limited
- United States National Transportation Safety Board.
Submissions were received from:
- Australian Helicopter Industry Association
- Bureau of Infrastructure, Transport and Regional Economics
- Bureau of Meteorology
- Civil Aviation Safety Authority
- Encore Aviation
- Garlick Helicopters
- GHD Limited
- Heli Surveys Pty Limited
- Honeywell Aerospace
- pilot
- Snowy Hydro Limited.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendix A – Injuries associated with vertical reference flying compared to other aerial work operations
This Appendix documents a short study conducted by the ATSB to provide further context of the relative exposure to injury during vertical reference flying operations to complement the analysis related to occupant protection systems. The objective of this study was to identify the chances of receiving an injury during an accident when conducting vertical reference flying compared to the mean of all other aerial work operations. To achieve this, statistical assessments comparing proportions of injuries to damage between groups were performed. The characteristics of injuries sustained are also discussed.
Methodology
Records from the ATSB’s occurrence database were extracted for review. Two groups of interest were identified in the study: vertical reference flying operations; and all remaining helicopter aerial work operations. To identify vertical reference flying operations, records were extracted when terms indicating fire control or other sling-load operations were identified. Preliminary results were then manually verified to include only those operations likely to involve long-line operations. The following fire control helicopter operations were excluded from these results: helicopters using integrated tanks drawing water through a snorkel (not using a fire bucket); winching or transporting fire control crews; and reconnaissance and fire spotting.
Only occurrences where the helicopters were substantially damaged or destroyed (accidents) were selected for analysis. These were selected as an indicator of significant whole of airframe accelerations. Consequently, it was expected that people on board were more likely to have experienced significant accelerating forces during impact that may lead to injuries. Accidents where the pilot experienced larger forces were also more likely to require the fitted restraint systems to mitigate injury risk. These accidents typically involved collisions with terrain or hard landings into clear and unsuitable areas.
A small number of vertical reference flying accidents were identified where substantial damage occurred, such as a tail rotor collision with a water bucket on the ground, where minimal accelerations were anticipated. However, these were included in this analysis to allow a fairer comparison with other aerial work operations where the damage was not characterised.
Results
Comparisons of injury proportions with other aerial work
Between 2000 and 2019, 15 accidents[17] were identified involving vertical reference flying where the helicopter was substantially damaged (13 accidents) or destroyed (2 accidents). Over the same period, 329 damaging accidents were identified for remaining aerial work operations.
The relative likelihood of accidents with injuries is shown in Figure A1 in comparison to the mean of all remaining aerial work operations (percentage of accidents where injuries occurred when the helicopter was substantially damaged or destroyed). Values were calculated based on the highest injury sustained to a flight crew member[18], meaning that each accident was only counted once.
Figure A1: Percentage of accidents with substantial damage or helicopter destruction by highest crew injury for vertical reference flying and other helicopter aerial work, 2000 to 2019

One fatal, three serious and five minor highest injury accidents with substantial damage or airframe destruction occurred for vertical reference flying, equating to 60 per cent (9/15) for this operation. In contrast, about 35 per cent (114/329) of all other helicopter aerial work accidents with the same damage categories resulted in injuries. The mean for all other helicopter aerial work produced a significantly lower percentage of accidents with injuries in comparison to vertical reference flying.[19] Considering only serious and minor injury accidents as an indication of known survivable impacts, the difference was also significant between vertical reference operations and all other helicopter aerial work.[20] This indicated that it was very likely that the chances of an injury were higher during vertical reference flying, than the mean of all other aerial work, in survivable impacts.
Injury characteristics
To identify the possible injury mechanisms, the characteristics of injuries sustained by specific body area were examined for each of the nine injury-related vertical reference flying accidents. This was also compared to known usage of upper torso restraints (UTRs). A limiting factor was that injuries were not known for the remaining all other aerial work operations. As a result, it was not possible to establish if differences existed between injury severity mechanisms, such as lack of UTR use, between the two groups.
Head injuries were identified in four accidents involving vertical reference flying. Upper torso restraints were not worn by two of these pilots: this accident (AO-2018-031) and a non‑survivable accident (AO-2018-057). Another head injury occurred when the UTR was worn loosely (AO-2009-076). In the two survivable accidents, the lack of use, or incorrect use of the UTR probably increased the severity of the injuries leading to facial fractures and hospitalisation.
It was uncertain how the fourth head injury occurred, with investigation (200300011) concluding that this probably resulted from striking the helicopter door frame or being struck in the helmet by the main rotor blade. However, it was unable to be determined if the pilot was wearing a UTR.
The serious injury accident involving spinal fractures (AO-2009-081) likely resulted from vertical acceleration forces through the seat during impact, following descent into trees. In this accident, the utilisation of the UTR was not examined, and it was not recorded if these restraints were worn. However, it was not expected that these would have prevented the serious back injuries sustained by the pilot in this case. Smalls cuts and scratches were reported in two minor injury accidents with one including seatbelt bruising and ligament or tendon damage on the pilot’s left shoulder from the UTR. The nature of the two other minor injuries were not recorded.
In summary, two of the three survivable accidents (including this accident) with head injuries likely resulted from the pilot’s head striking the airframe structure. In these two cases, investigations found that this was related to the lack of use, or incorrect use of UTRs.
Conclusion
In conclusion, it was found to be significantly more likely to receive an injury during vertical reference flying compared to the mean of all other helicopter aerial work activities. Two of the three survivable impacts with head injuries during vertical reference flying accidents were likely made more severe due to limited or no UTR use. Although it was possible that these injuries contributed to the difference between the proportion of injuries between the two groups, this was unable to be determined as the nature of injuries or UTR usage in other aerial work was not known. This supports the need for further research in this area.
__________
- These numbers differ from the analysis conducted for investigated upper torso restraint usage in the section titled ‘Utilisation of upper torso restraints’ due to the analysis of this Appendix including investigated and non investigated occurrences.
- A small proportion of accidents with crew injuries (9%) had multiple crew onboard. These included aeromedical flights, fire spotting and operations with a second pilot. These are not expected to impact on results. The remaining accidents with crew injuries involved single pilots.
- Fisher’s Exact Test (one-tailed): Number of substantially damaging impacts with injuries and without injuries for vertical reference flying vs other helicopter aerial work, p = 0.044, odds ratio 2.8.
- Fisher’s Exact Test (one-tailed): Number of substantially damaging impacts with minor and serious injuries, and without injuries for vertical reference flying vs other helicopter aerial work, p = 0.023, odds ratio 3.5.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2021
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |