Safety summary
What happened
On 29 May 2017 at about 2225, a passenger train struck a protection officer at Petrie Station, Queensland, while walking on the track after placing permanent way protection equipment for a track closure on the Kippa-Ring line. As a result of the collision, the protection officer sustained fatal injuries.
What the ATSB found
The ATSB found that the protection officer did not apply personal continual vigilance (PCV) techniques while walking within 3 m of a track (the Danger Zone). PCV required the track worker to have clear and adequate sighting of tracks approaching their location, and frequently look (approximately every 5 seconds) in both directions for approaching rail traffic.
Although the reasons why the protection officer did not apply continual vigilance techniques could not be determined, it was possible that he had no expectation of rail traffic, and a number of factors that increased risk were identified. The ATSB found that the protection officers were not advised of the protection task and its earlier start time requirement, and felt pressure to continue with the task. Relating to the task, a Train Notice Diagram was provided to the protection officers which was incorrectly marked with the open and closed roads, which was likely linked to the Train Notice Diagram layout being conducive to misinterpretation.
It was also found that the protection officers working on the closure were unfamiliar with the new rail environment at Petrie, which had an uncommon grade separation of lines and there was no process for familiarisation. There was also no requirement to obtain train running information, meaning the protection officers were unaware of the location and direction of trains approaching their location. The process for selecting protection measures also did not drive selection to reasonable and practicable higher levels of protection.
What's been done as a result
Immediately following the accident, Queensland Rail (QR) proactively suspended all work within the danger zone of its running lines, later reinstating work in the Danger Zone with the prohibition of PCV.
Since the accident, QR reported that it has undertaken independent reviews on its safe work on track systems including PCV, use of mobile devices in the rail corridor, and its worksite protection compliance inspection systems. QR have since re-introduced PCV with some additional controls identified and validated from their independent reviewer.
QR have also re-enforced the message of ‘the right to stop work and getting safety right before commencing’ as part of its ongoing network pre-start brief project. They have also organised the development of a consistent process for marking up Train Notice Diagrams, including the provision of retraining protection officers in relation to PCV, mobile phones, pre-start briefs, and safeworking documentation.
Safety message
‘Safe work on track’ continues to be one of ATSB’s SafetyWatch priorities. To minimise risk, rail organisations should ensure processes relating to track work include provisions for protection officers to have sufficient resources, including time for task, information about the work environment, including train movements, and adequate protection available for the work.
On 29 May 2017 at about 2225 Eastern Standard Time,[1] passenger train T570 struck and fatally injured a protection officer (PO1) adjacent to Petrie Station, Queensland. PO1 was walking back to his work team vehicle after placing permanent way protection equipment for a track closure on the Kippa-Ring rail line in preparation for maintenance activities.
Possession planning for closure
Around 26 April 2017, a possession planning coordinator[2] commenced planning for a scheduled closure of the Kippa-Ring rail corridor on 29 May 2017 from Petrie Station to the end of the line at Kippa-Ring Station (Figure 1). The closure was required to facilitate planned maintenance works on both overhead wiring and track infrastructure.
Figure 1: South-Eastern Queensland rail lines north of Brisbane

Image shows the rail lines from Brisbane through Petrie, the Caboolture line continuing after Dakabin towards Narangba, and the newer Moreton Bay line also known as the Kippa-Ring rail line from Petrie to Kippa-Ring (depicted in red). Source: Australian Government National Map, annotated by ATSB
Also on 26 April 2017, the team seeking access for the Kippa-Ring line closure submitted a protection officer resource request to the night shift protection officer supervisor.[3] The supervisor later recorded the protection task and resource allocation for the Kippa-Ring line closure in his handwritten diary.
On 18 May 2017, the possession planning coordinator emailed the night shift protection officer supervisor (supervisor) requesting the name of the protection officer who would be in charge of the Kippa-Ring rail line closure. This information was required to finalise the Train Notice[4] associated with the closure. As the supervisor was preparing to commence leave (between 19 May 2017 and 28 May 2017), he forwarded the possession planning coordinator’s emailed request to the acting night shift protection officer supervisor (acting supervisor 1).[5] The acting supervisor 1 replied to the possession planning coordinator providing the name of the protection officer (PO3) who would be in charge of the Kippa-Ring rail line closure. The acting supervisor 1 also recorded the names of the four assigned protection officers (PO1, PO2, PO3 and PO4) into the handwritten diary.
Planning the week prior to closure
On 22 May 2017, one week prior to the day of the closure, the possession planning was complete and a Train Notice associated with the Kippa-Ring rail line closure was published.[6] The Train Notice detailed the purpose of the closure, the proposed work, the type of protection required and the extent of the closure including the signal numbers protecting the closure and the name and contact details of the protection officer in charge (PO3).
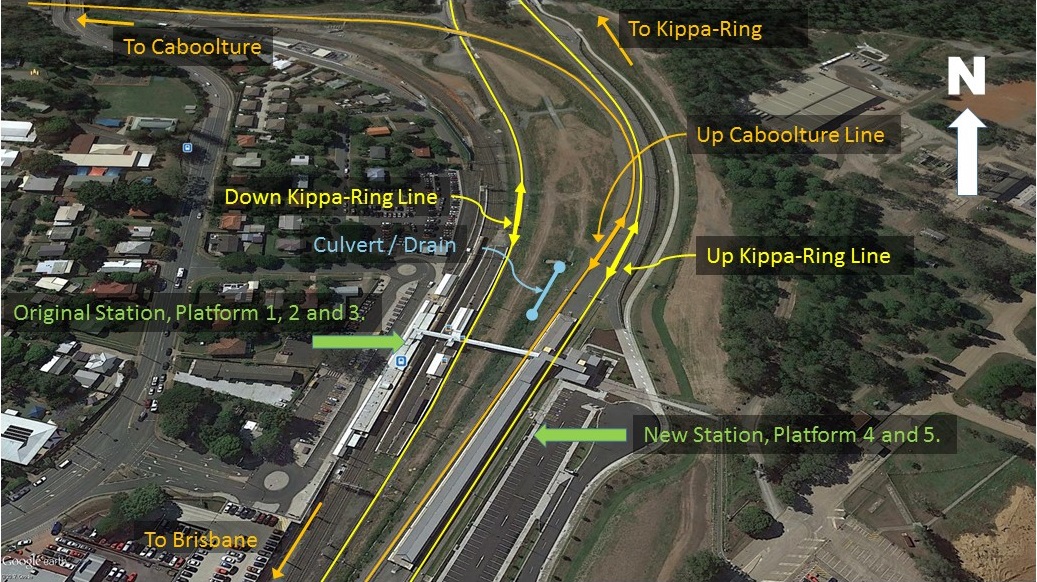
The team of four protection officers were required to establish the Kippa-Ring rail line closure using a Track Occupancy Authority (TOA).[7] Three of the four protection officers (PO1, PO2, and PO3) were assigned to Petrie Station, while PO4 was to be assigned to Kippa-Ring Station at the other end of the closure. The protection measures at Petrie involved the placement of permanent way stop signs[8] and three railway track signals[9] at signals PE67 and PE73 (Figure 2), closing the routes from Petrie towards the Kippa-Ring line.
Figure 2: Signal layout information for Petrie Station, with location of permanent way protection equipment placed by protection officers 
Image shows location of signals, station platform numbering, and location where protection officers placed permanent way protection equipment and parked their vehicle. Lines closed as part of the Kippa-Ring line closure shown in red. Source: Queensland Rail, annotated by ATSB
The Train Notice for the Kippa-Ring line closure nominated a track closure commencement time of 2200. On 26 May 2017, one of the access seekers assigned to work within the Kippa-Ring rail line closure emailed the two acting supervisors requesting his work group briefing be held at Albion Depot at 2045 on 29 May 2017.
On 28 May 2017, acting supervisor 1 communicated via email an acceptance of the briefing location request, and agreed to the start time. The acting supervisor 2 and the normal supervisor were included in this communication. An earlier shift start time than the normal 2100 shift start would be required for this. However, the protection officers were not advised of their work task or briefing details, nor were they advised that an earlier shift start was required to accommodate the planned work.
On the night prior to the accident, the normal supervisor returned from leave. At this time, neither of the acting supervisors nor the normal supervisor detected that the protection officers had not been advised of the protection task and earlier shift start time requirement for the Kippa-Ring rail line closure.
Work on night of closure
The base depot and shift start location for the protection officers and supervisor on the night of the accident was the Mayne Depot. At about 2040 on the night of the accident (29 May), the supervisor, telephoned PO3 to enquire why he had not arrived at Mayne Depot for the early shift start time. PO3, who was travelling to work in the presence of PO1 and PO2, indicated that he and the others were unaware of the early shift start requirement and their involvement with the Kippa-Ring line closure.
In an attempt to avoid delaying the required closure, the supervisor marked up the Train Notice Diagram,[10] a task normally undertaken by a protection officer in charge. The diagram showed the worksite safety information, such as safe places, intended permanent way protection equipment location, open and closed track information, and other relevant information. However, the supervisor’s ‘mark ups’ on the Train Notice Diagram contained errors which did not accurately display which tracks were open or closed at Petrie Station.
Upon arrival at Mayne Depot, the supervisor presented PO3 with the Train Notice and the marked up Train Notice Diagram. Two of the protection officers (PO2 and PO3) recalled, that following their arrival at the Mayne Depot they advised the supervisor of their concerns regarding their lack of familiarity with the Petrie area, and the short time frame. The supervisor recalled reassuring the protection officers that it was a simple and straightforward task.
The briefing with the maintenance crew was at Albion Depot, so a short time later, PO1, PO2, and PO3 departed their base depot for Albion Depot (Figure 1). The fourth protection officer (PO4) departed the Mayne Depot for the end of the Kippa-Ring rail line. At about 2120, PO1, PO2 and PO3 arrived at Albion Depot. Members of the maintenance crew observed that PO3 looked ‘flustered’, and recalled that he apologised for being late. PO2 and PO3 later recalled feeling rushed to implement the closure.
At about 2120, PO3 participated in a briefing of the maintenance crew at the Albion Depot. After the briefing had concluded, PO1, PO2, and PO3 travelled to Petrie Station (Figure 1). Prior to commencing protection work, PO2 and PO3 reported undertaking a pre-start brief for the implementation of protection. Video footage showed PO1, PO2, and PO3 were in discussions together at the bonnet of their vehicle for approximately 90 seconds. However, the recorded pre-start briefing form contained errors and inconsistent sign-off entries.
A short time after the pre-start brief was reported as completed, PO3 contacted the network control officer (NCO)[11] to confirm[12] their location at Petrie. This was done by PO3 confirming the displayed aspect of a signal on the Down[13] Kippa-Ring line. As none of the protection officers at Petrie had worked at that location since major changes to the rail infrastructure had been completed,[14] there was some initial confusion in locating the correct signal to confirm their location.
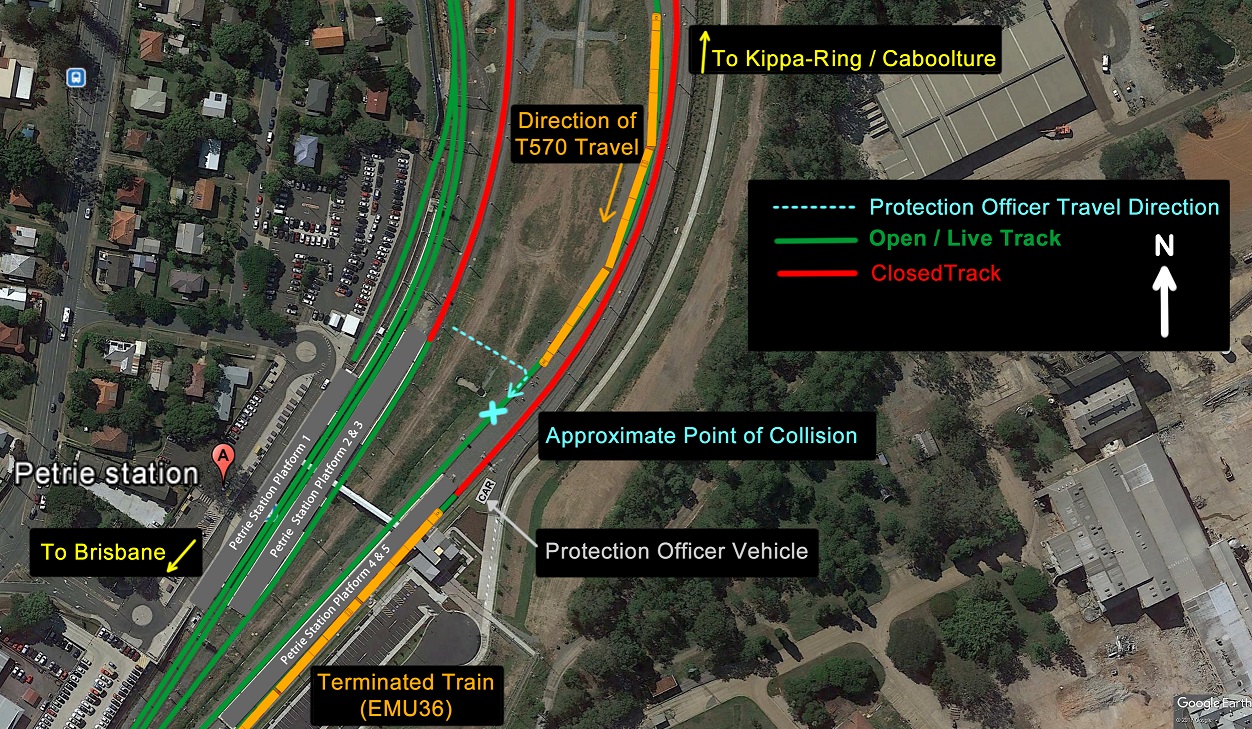
At about 2215, after confirming their location at Petrie, PO3 commenced establishing the TOA for the Kippa-Ring rail line closure. Once blocking facilities had been applied for the closure, PO1 and PO2 entered the rail corridor. PO1 and PO2 placed permanent way stop signs and railway track signals adjacent to signal PE67 to block the Down Kippa-Ring line, and signal PE73 to block the Up Kippa-Ring line, respectively (Figure 2). As a culvert and small drain blocked a direct route from the protection officers’ vehicle to signal PE67, PO1 chose to walk 20 m along the middle of the Up Caboolture line (which was open for rail traffic) until there was clear access to walk across to signal PE67 (Figure 3). Video footage showed PO1 was likely not surveying for rail traffic behind him during this walk.
Figure 3: Petrie stormwater culvert/drain layout

The images shows the stormwater drain/culvert (blue dashed line) and the direction of the protection officer’s travel to and on return from PE67 near platform 3 (yellow dashed line). Source: Google Earth, Annotated by the ATSB.
At about 2222, after PO1 and PO2 had placed the permanent way stop signs and railway track signals, PO1 walked to the northern end of Platform 3 where he met with a station officer. They were engaged in conversation for a short time before the protection officer turned and walked in the direction of the protection officers’ vehicle.
PO1 again walked in the middle of the Up Caboolture line, the reverse path he had previously used to avoid the culvert and drain (yellow line in Figure 3). Video footage showed that PO1 was looking in his direction of travel, and was not looking behind him. At about this time, a passenger train, designation T570, approached Petrie Station on the Up Caboolture main line from the north. The distance separating train T570 and the protection officer when PO1 reached the Up Caboolture line was about 400 m.
The train’s headlights and ditch lights were on and functioning correctly as the train travelled a 50 km/h sweeping right hand curve (Figure 4). However, the lights only illuminated a short length of track ahead due to the curvature of the track. With his back to the train, PO1 was not aware of the approaching train and the driver of the train was unaware PO1 was positioned in the middle of the rail lines.
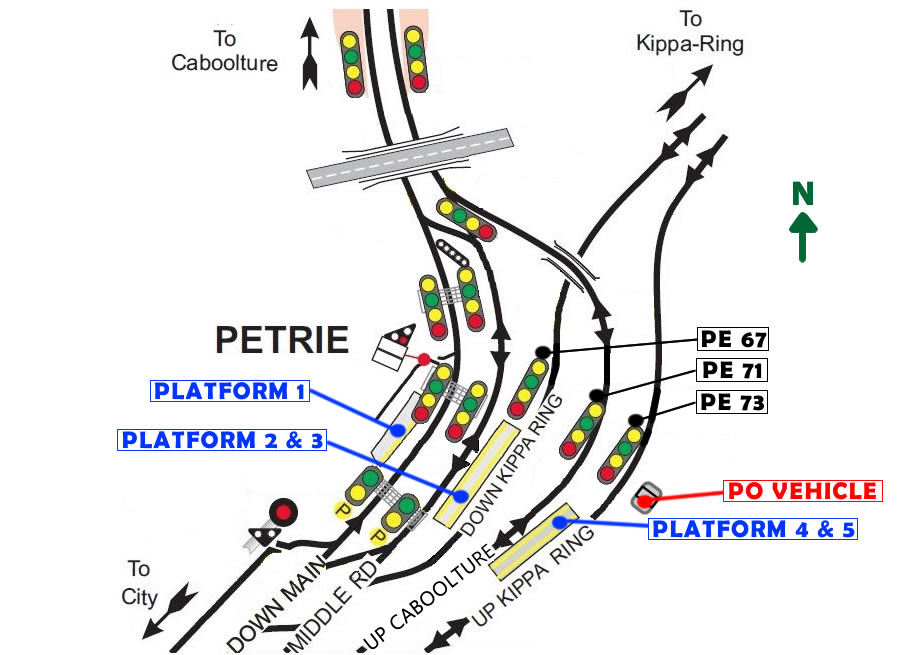
Figure 4: Layout of the Petrie Station

This image shows the location of platform 3, in relation to the stormwater culvert/drain (depicted in blue). As well as Caboolture lines (Up depicted in solid orange, and Down in dashed orange line) and the Kippa-Ring lines (Up depicted in solid yellow, and Down in dashed yellow line). The direction of travel of train T570 on the Up Caboolture line and the collision location is also shown. Source: Google Earth, annotated by ATSB
At about 2225, video footage showed PO1 had stopped walking in the middle of the rail lines at the same time as his mobile phone clipped to the front of his shirt illuminated. He remained in a stationary position, for about 6 seconds, with the phone illuminated and his back to the approaching train. As the train exited the sweeping curve, the headlights shone directly on PO1. Upon sighting PO1, the train driver applied the emergency brake and sounded the train horn. The protection officer attempted to vacate the track, however, there was insufficient time and the train collided with the PO1 (Figure 4). As a result of the collision, PO1 sustained fatal injuries.
__________
- Eastern Standard Time (EST): Coordinated Universal Time (UTC) + 10 hours.
- A position within the Queensland Rail Planning Centre responsible for possession planning. Source: Queensland Rail (QR) Queensland Rail Possession Planning Protocols MD-12-938.
- A supervisor who is responsible for the management of protection officer resources, and communication of protection tasks to protection officers.
- A notice issued by an access provider which contains safe-working information for workers. Source Queensland Rail (QR) Queensland Network Rules and Procedures Glossary MD-12-189.
- As part of a previous organisational structure change, an acting night shift protection officer supervisor (acting supervisor1) had been added to the night shift protection officer team. In addition, due to the normal supervisor’s leave, a second acting night shift protection officer supervisor (acting supervisor2) was assisting with the supervisor responsibilities.
- The publishing of a Train Notice is when the notice comes into effect and is distributed to operational rail safety workers advising them of the planned changes.
- Track Occupancy Authority is ‘An authority for Competent Workers and their equipment to occupy a defined portion of track for a specified period’. Source: Queensland Network Rules and Procedures Glossary MD-12-189.
- A red double sided reflectorised sign that is secured to the left rail as seen by the crew of approaching rail traffic, warns rail traffic to stop and marks the outer limits of protection for a worksite or obstruction. Source: Queensland Network Rules and Procedures, QR6007: Signs – General, MD-12-189 Version 1.1.
- A device attached to the rail that explodes on impact, and is used to attract attention of rail traffic crews. Source: Queensland Network Rules and Procedures Glossary, MD-12-189 Version 1.2.
- Train Notice Diagram is a map which shows rail infrastructure layout and operational information for a defined area.
- A competent worker who authorises, and may issue, occupancy authorities, and who manages rail traffic paths to ensure safe and efficient transit of rail traffic in the network. Source QR Queensland Network Rules and Procedures Glossary.
- ‘Confirm’ in this context, refers to the process whereby the NCO confirms the location of the protection officer by manipulating a signal aspect at the worksite and verifying what aspect the protection officer observes.
- ‘Down’ rail lines indicate that the normal direction of travel on these lines is away from a state capital city, Brisbane in this case. ‘Up’ rail lines indicate travel towards a capital city.
- The Petrie station and rail infrastructure experienced an upgrade and redesign when connecting to the new Kippa-Ring rail corridor in October 2016. The Station gained two new platforms to facilitate train and passenger activity. The new platforms 4 and 5 are an island configuration between the Up Caboolture and Up Kippa-Ring main lines.
Protection officers
A protection officer was defined within the Queensland Rail Network Rules and Procedures (QNRP) as a competent worker responsible for managing the rail safety component of worksite protection.
Protection officer PO1
PO1 was the protection officer struck by train T570.
Queensland Rail (QR) had employed PO1 for 36 years, with the last 17 years in a protection officer role. PO1 held current competencies for his role as a protection officer, with his last reaccreditation assessment satisfactorily completed on 12 May 2016. A periodic health assessment of PO1 was undertaken on 10 February 2017, with PO1 being recorded as fit for duty.
A toxicology examination for alcohol and prescribed drugs recorded a negative test result.
PO1 had taken leave in the days prior to the accident, with the accident occurring early in his first night back at work. It was unlikely that PO1 was experiencing a level of fatigue known to have a demonstrated effect on performance.
Protection officer PO2
PO2 was the protection officer placing permanent way protection equipment adjacent to signal PE73 at Petrie.
QR had employed PO2 for 22 years, with the last 10 years being in a protection officer role. PO2 held current competencies for his role as a protection officer, with his last reaccreditation assessment satisfactorily completed on 24 April 2015.
The ATSB reviewed the drug and alcohol test results, and rosters (with respect to fatigue). In conjunction with the PO2 comments and his leave in the days prior to the accident, these human performance factors were not considered a factor in this accident.
Protection officer PO3
PO3 was the protection officer in charge of implementing the protection and managing the rail safety component and implementation documentation associated with the closure.
PO3 was employed at QR for 21 years, with the last 11 years being in a protection officer role. PO3 held current competencies for his role as a protection officer, with his last reaccreditation assessment satisfactorily completed on 9 April 2015.
The ATSB reviewed the drug and alcohol test results, and rosters (with respect to fatigue). In conjunction with the PO3 comments and his leave in the days prior to the accident, these human performance factors were not considered a factor in this accident.
Protection officer PO4
PO4 was the protection officer tasked with clipping points at the Kippa-Ring Station end of the closure. Whilst PO4 was part of the protection officer team, he was not directly involved in the accident at Petrie.
Location
Petrie Station is located 28.5 km north of the Roma Street Station, Brisbane on the North Coast Line in Queensland. It services the suburb of Petrie in the Moreton Bay region, and is the junction for the main lines between Brisbane, Caboolture, and the recently commissioned Kippa-Ring rail line (Figure 5).
The Kippa-Ring rail line, also known as the Moreton Bay rail line and Redcliffe Peninsula line, was a 12.6 km dual-track passenger rail line between Petrie and Kippa-Ring. The Kippa-Ring rail line construction was completed in October 2016, with significant changes to rail infrastructure in the Petrie Station area.
Figure 5: Portion of Queensland Rail South-Eastern Queensland network

Image shows rail lines from Brisbane through Petrie, the Caboolture line continuing after Petrie towards Caboolture, and the Redcliffe Peninsula line also known as the Kippa-Ring line continuing from Petrie to Kippa-Ring. Source: Queensland Rail, annotated by ATSB
The new Kippa-Ring rail line connected to the existing QR network at Petrie Station. In respect to Petrie (Figure 6), this connection led to the construction of:
- additional platforms (island platform 4 and 5)
- track duplication south of Petrie to Lawnton
- connection to new Kippa-Ring line
- grade separation[15] of the Up Caboolture and Down Kippa-Ring lines at Petrie.
Figure 6: Rail infrastructure changes in vicinity of Petrie Station

Image shows new and changed rail infrastructure configurations in red within the Petrie Station precinct. Source: Queensland Rail, annotated by ATSB.
Petrie Station consisted of five passenger platforms, with Platform 1 serviced by a down direction rail line and Platforms 2 to 5 serviced with bi-directional[16] lines. The line allocations for each of the platforms were as follows (Figure 7):
- Platform 1 – Down Caboolture Line
- Platform 2 – Middle Road (predominantly down line, but could be bi-directional)
- Platform 3 – Down Kippa-Ring Line (predominantly down line, but could be bi-directional)
- Platform 4 – Up Caboolture Line (predominantly up line, but could be bi-directional)
- Platform 5 – Up Kippa-Ring Line (predominantly up line, but could be bi-directional).
Figure 7: Petrie Station layout

Image shows platform and line allocation. Up and Down Caboolture lines depicted in orange, and Up and Down Kippa-Ring lines depicted in yellow. Source: Google Earth, annotated by ATSB
Platforms 1, 2, and 3, were separated by about 40 m from Platforms 4 and 5 due to a stormwater culvert/drain (Figure 7). Platforms 4 and 5 were configured in an island platform arrangement in a separate structure, and were connected to the other Petrie platforms by an overhead pedestrian walkway (Figure 7).
The Up Caboolture line and the Down Kippa-Ring line were grade separated about 400 m north-west of the Petrie Station (Figure 7). The grade separation created a relatively uncommon configuration in the QR Network, whereby two adjacent platforms (4 and 5) both serviced tracks that carried mainly Up direction traffic.
Organisation
QR provided suburban commuter rail services on the City network, covering Brisbane, Ipswich, Sunshine Coast and Gold Coast in South-Eastern Queensland. Queensland Rail was both a rail infrastructure manager and rolling stock operator.
Management of change
To manage rail safety legislative obligations, rail operators were required to establish and implement a safety management system (SMS).[17] One element of an SMS was a subsystem that provides for the management of changes. This subsystem is aimed to ensure that changes that may affect the safety of rail operations were identified and managed, so far as is reasonably practicable.
Kippa-Ring rail line changes
The Queensland Department of Transport and Main Roads was the agency responsible for the Kippa-Ring rail line project, who had engaged a third party design and construction contractor. On completion of the project, QR accepted management and control responsibility for the new infrastructure.
QR determined this was a complex change within the guidelines of its management of change processes. From this, a Rail Safety Management Plan was developed for the new Kippa-Ring rail line. This plan focussed on the changes resulting from QR’s acceptance of the new infrastructure, and the planned commencement of operations on the new infrastructure. The plan did not identify protection officers and other track workers as stakeholders, nor include the need for familiarisation for protection officers and track workers as a risk.
Protection officer familiarisation
The protection officers involved in this accident had not worked at Petrie since the completion of the rail infrastructure changes associated with the new Kippa-Ring line.
At the time of the accident, QR relied on protection officers becoming familiar with a new location by reviewing Train Notice Diagrams or route maps. These Train Notice Diagrams and route maps provided information about the configuration of rail infrastructure as well as some operational information (Figure 8). The diagrams and maps were limited in the topological information they contained, such as physical barriers that might create additional safety hazards to the work at the intended location.
Figure 8: Queensland Rail Train Notice Diagram and Route Map sample

Image shows samples of the information available from a Queensland Rail train notice diagram and route map for Petrie. Noting that there is limited information about physical site topology. Source: Queensland Rail, annotated by ATSB
The protection officers advised that when they had advanced warning of a protection task at a new or unfamiliar location, whilst not a QR requirement, they would consider a visit to the worksite in the days preceding the intended work. This opportunity was not available in this case.
Safeworking systems
Safeworking systems are an integrated system of procedures and technology aimed at ensuring the safe operation of trains including the protection of people and property on or about a railway.[18]
In June 2012, QR implemented the Queensland Network Rules and Procedures (QNRP) Standard as the safeworking system for their network. The QNRP Standard was aligned, with some exceptions, to the suite of Australian Network Rules and Procedures (ANRP). The ANRP was maintained and updated as required by the Rail Industry Safety Standards Board (RISSB) in collaboration with industry representatives. Since QR implemented the QNRP Standard in 2012, sections of the RISSB ANRP relevant to this investigation have been amended (2013 and 2014).
The QNRP Standard, among other safety measures, put in place specific safety measures for the risk of collision between rail traffic and workers. The QNRP specified the minimum requirements for trackside protection for anyone who entered the rail corridor, and for those who performed activities in the Danger Zone.[19]
The safety controls or protection levels relevant to track workers accessing rail corridors ranged from the higher safety level work on track authorities to means of protection followed by the lower level safety measures (Figure 9).
Figure 9: Image depicting protection levels of safety controls for accessing rail corridors

The image shows the lower protection level safety measures, through the means of protection to the higher protection level work on track authorities. Source: ATSB
The relevant protection officer undertook a safety assessment when choosing the appropriate track access method or the level of protection. The QNRP referred to two safety assessment documents for recording the safety assessment: Corridor Access Safety Assessment (SW61), and Trackside Safety Protection Planner (SW01).[20] These documents provided guidance on the selection of protection level, and recorded details of the intended track access safety assessment (Figure 10).
Figure 10: Image depicting protection level selection guidance within track access safety assessment QNRP forms SW01 and SW61

This image shows the portions of the track access safety assessment documents (SW01 and SW61) which were designed to assist the decision making process for protection level selection. Source: Queensland Rail, annotated by the ATSB
As included in the design of the safety assessment forms SW61 and SW01, there were two main safety hazards that protection officers needed to consider when determining what level of protection to select. These were:
- the safety hazards to rail traffic from the intended work
- safety hazards to track workers and protection officers from rail traffic while within the proposed worksite.
The decisions related to the rail traffic risk assessment required the protection officer to consider what work was to be undertaken and whether that work would make the track unsafe for rail traffic by breaking or obstructing the track (Figure 11). This was followed by a consideration of the rail infrastructure/operational configuration and site topology effects on the protection officer, and ultimately track workers ability, to sight an approaching train and move to a safe place before the train arrived (Figure 11).
Figure 11: Flowchart showing protection level selection decision-making process (starting in the top left), informed by Queensland Rail SW61 and SW01 forms.

This image shows a protection level selection flowchart created by the ATSB to explain the protection level selection decision making process and decision assistance guidance contained in Queensland Rail Corridor Access Safety Assessment (SW61) and Trackside Safety Protection Planner (SW01) forms. Source: ATSB
There were some common baseline safety requirements between work on track authorities, means of protection, and safety measures for workers accessing the Danger Zone. These were:
- Track workers must wear high-visibility clothing.
- Electronic communications devices were not to be used in the Danger Zone.
- Track workers must not step on points, interlocking equipment, or rails.
- Track workers must not wear or use anything that prevents them from seeing or hearing rail traffic.
The differences between the work on track authorities, means of protection, and safety measures that are relevant to this investigation are explained below in the context of the Kippa-Ring line closure at Petrie.
Track Occupancy Authority (Authority)
Track Occupancy Authority (TOA) is an authority for competent workers and their worksite equipment to occupy a defined portion of track for an agreed period. A TOA essentially is issued to the access seeker and provides sole occupancy except where joint occupancy is negotiated. A TOA is intended for work that breaks or obstructs the track, or where a safety assessment has determined a lower protection level is not appropriate. The implementation of a TOA in an application similar to the Kippa-Ring line closure at Petrie required the following safety controls:
- The protection officer must contact the Network Control Officer (NCO) and request the TOA. The protection officer must clearly describe the location, work site limits, work to be undertaken, and proposed start finish times.
- The NCO must test and confirm the location of the worksite with the protection officer and ensure that the track within the proposed worksite limits is unoccupied.
- The NCO must apply blocking facilities[21] and secure points to prevent unauthorised rail traffic into the portion of track within the TOA limits.
- The protection officer must confirm that the NCO has applied blocking facilities, and ask for the train running information for rail traffic planned to pass through the work location.
- NCO must authorise TOA.
- The protection officer must place in-field protection consisting of railway track signals[22] and stop signs at the limits of the TOA or 500 m on either side of the worksite.
- Depending on operational and network configurations, the protection officer may clamp points in a position to direct rail traffic away from the TOA limits.
Absolute Signal Blocking (Means of protection)
Absolute Signal Blocking (ASB) is a means of protection used by competent workers to carry out work on track. ASB is only available in remote controlled signalling territory and uses controlled absolute signals set at STOP with blocking facilities applied. ASB is not permitted to be used for work that breaks or obstructs the track, and does not provide exclusive occupancy to the access seeker. The implementation of an ASB in an application similar to the Kippa-Ring line closure at Petrie required the following safety controls:
- The protection officer must contact the NCO and request the ASB. The protection officer must clearly describe the location, the absolute signals to be used to protect the work site limits, work to be undertaken, and proposed start finish times.
- The NCO must test and confirm the location of the worksite and the controlled absolute signals with the protection officer, and ensure that the track within the proposed worksite limits is un-occupied.
- The NCO must set the controlled absolute signals to stop and apply blocking facilities and secure points to prevent unauthorised rail traffic into the portion of track within the ASB limits.
- The protection officer must confirm that the NCO has set the controlled absolute signals for the work site to stop and applied blocking facilities.
Look Out Working (Safety measure)
Look Out Working (LOW) is a safety measure used by competent workers to carry out work on track without a formally issued work on track authority, or means of protection. While the QNRP permits the use of LOW at night for protection officers placing permanent way protection equipment, a local understanding/practice within the protection officer business unit precluded the use of LOW at night. LOW was restricted to applications where workers, tools and equipment could be cleared from the track to a safe place 10 seconds before the arrival of rail traffic. LOW required competent workers to be assigned as lookouts,[23] where their sole role was to keep watch for approaching rail traffic and warn workers to move to the designated safe place. The implementation of LOW in an application similar to the Kippa-Ring line closure at Petrie required the following safety controls:
- The protection officer must contact the NCO and notify them of their intent to use LOW. The protection officer must clearly communicate their name, contact details, location of work site, type of work to be done, and proposed start and finish times.
- The protection officer must determine how many lookouts are required and their placement to ensure the minimum sighting distance is achieved to provide adequate warning to the people within the work site.
- The protection officer must determine communication arrangements for lookouts to warn workers (this excludes radios or telephones).
- Lookouts must keep watch for rail traffic approaching the worksite and warn workers immediately if rail traffic approaches the worksite.
- Lookouts must remain in their designated position and not do any other work while performing lookout duties.
On 7 March 2014, QR published a Critical Safety Alert advising that the use of LOW at night was prohibited except for the placing or removal of permanent way protection equipment. However, a local rule or understanding corroborated by several QR representatives, confirmed that it was accepted policy that LOW was not to be used at night even for placement or removal of permanent way protection equipment.
Personal Continual Vigilance (Safety measure)
Personal Continual Vigilance (PCV) is a safety measure used by competent workers to walk from place to place in the Danger Zone and do no work other than place/remove permanent way protection equipment. The ANRP equivalent process had been amended in June 2014. This amendment brought in an option for rail operators like QR to consider adopting a requirement that, before walking in the Danger Zone, workers must contact network control and get information about rail traffic for that location. Although QR had considered this optional requirement from the ANRP amendment, it had elected not to adopt it. As such, the QNRP version of PCV at the time of the accident did not require any communications or operational train running advice from the network controller before accessing the Danger Zone using PCV. In addition to this, the QNRP specified that competent workers must not rely on train running information. This requirement was consistent with the understanding of protection officers, who advised that NCOs do not like to provide train running information. Therefore, the implementation of PCV in an application similar to the Kippa-Ring line closure at Petrie required the following safety controls:
- The track worker must make sure that they can see that tracks are clear of approaching rail traffic.
- The track worker must look frequently (approximately every 5 seconds) in both directions for approaching rail traffic.
- The track workers must not rely on another person to give warnings of approaching rail traffic.
Protection officers reported that the common operational practice was to select PCV as the preferred choice for initial access to the Danger Zone when placing permanent way protection equipment, or when crossing from place to place.
Safeworking comparison
The comparison of each of the safety controls for the work on track authority, means of protection, and safety measures relevant to the investigation is summarised and displayed in Table 1:
Table 1: Comparison of summarised safeworking tasks between protection levels relevant to this investigation
|
Safety control |
TOA |
ASB |
LOW |
PCV |
|
Requires notification to NCO of intent to access Danger Zone |
|
|
|
|
|
Requires NCO authority / permission to proceed |
|
|
|
|
|
Requires NCO confirmation of location |
|
|
|
|
|
Requires NCO to block signals / points |
|
|
|
|
|
Requires protection officer to confirm application of NCO blocks |
|
|
|
|
|
Requires protection officer to request train running information |
|
|
|
|
|
Requires protection officer to place in-field protection/point clamps |
|
|
|
|
|
Requires adequate sighting distance of approaching rail traffic |
|
|
|
|
|
Requires lookout to solely look out for trains and warn workers |
|
|
|
|
|
Requires track worker to look frequently in both directions |
|
|
|
|


Possession task
On the night of the accident, maintenance access seekers planned to close and take possession of the Kippa-Ring rail line using a TOA to facilitate maintenance inspections of the overhead traction wiring equipment and the distribution of track ballast to rail turnouts. The closure was scheduled to commence at 2200 on 28 May 2017 until 0320 on 29 May 2017, and was to be repeated on the following night.
Possession planning
The QR track possession planning processes encompass the planning for business and customer continuity, accomplishment of works, safety within the worksite, and safety of normal operations. Possession planning in QR began with a possession bid raised by an access seeker. Possession bids were lodged within a database, which tracks the planning activities in relation to a possession.
As per planning protocols, a possession planning coordinator was assigned planning responsibility for the Kippa-Ring line closure prior to the scheduled closure. The possession planning coordinator initially undertakes a review of the possession bid to determine the complexity of the planning work required. This review considers the proposed possession dates/times, proposed worksite limits, adjacent signals, rail infrastructure geography, overhead isolation points, and what are the most appropriate bus transfer points for passengers. This review leads to the determination of the most appropriate level of protection for the worksite and the development of a traffic plan for the rail service changes to facilitate the possession.
The possession planning coordinator determined that a TOA would be the most appropriate protection level, with signal PE67 and PE73 at Petrie Station and the end of the Kippa-Ring rail line being the worksite protection limits for the possession. The traffic plan which was developed required the termination of all Kippa-Ring line rail services at Petrie Station. Alternate bus services were provided for QR customers between 2200 and 0320 on the night of the accident (29 May 2017) and the following night (30 May 2017). The traffic plan was completed on 27 April 2017, and the possession bid was approved on 3 May 2017.
The possession planning coordinator then commenced drafting a Train Notice for the altered safeworking arrangements. The possession planning coordinator, upon completing their draft of the Train Notice, organised for an independent review of the Train Notice, as per planning protocols. The review was completed on 22 May 2017, with the Train Notice published later that same day.
The publishing of the Train Notice concluded the possession planning coordinator’s involvement unless a further change to the Train Notice or the possession plan was required. At this stage, the planning and risk management associated with the placement of the protection within the Danger Zone for the track possession became the responsibility of the protection officer. The ATSB found that the possession planning for the proposed Kippa-Ring line closure was adequate.
Possession implementation
The published Train Notice for the Kippa-Ring rail line closure prescribed the protection level of TOA with the following limits:
- The Up Kippa-Ring line from the end of the Kippa-Ring line to signal PE73 at Petrie.
- The Down Kippa-Ring line from signal PE67 Petrie to the end of the Kippa-Ring line.
To facilitate the implementation of the TOA for the Kippa-Ring rail line closure, protection officers PO1, PO2, and PO3 were required to access the Danger Zone at Petrie to place stop signs and railway track signals at signals PE73 and PE67 at Petrie (Figure 12).
The protection officers at Petrie were to be protected on the Up and Down Kippa-Ring lines by the signal blocking applied by the NCO as part of the TOA requirements. Personal Continual Vigilance (PCV) was the protection level selected for all other rail lines at Petrie, including the Up Caboolture line where the collision occurred.
The fourth protection officer, PO4 was assigned to the end of the Kippa-Ring rail line and was to access the Danger Zone at Kippa-Ring to secure and lock points at the entrance to a stabling yard to prevent rollingstock accessing the Kippa-Ring rail line.
Figure 12: Petrie Station, showing placement of permanent way protection equipment for Kippa-Ring line closure.

Image indicates the location, and permanent way protection equipment type and placement for the Kippa-Ring line closure on the night of the accident. Source: Google Earth, annotated by ATSB
To access the rail corridor and Danger Zone to place the permanent way protection equipment for assigned protection tasks, protection officers also need to consider their own protection in line with the Queensland Rail Network Rules and Procedures. Queensland Rail have documented their processes for implementing track protection within a safe work method statement (SWMS). The SWMS assigns responsibility to the protection officer for implementing the pre-planning, and site arrival tasks for implementation of protection.
Pre-planning
The pre-planning work sequence required the protection officer in charge to use route maps, train notice diagrams, and train notices to plan and undertake the safety assessment. The safety assessment was recorded on QR forms SW01 and SW61. The SW01 form required a worksite sketch, which provided details of the closed tracks, worksite limits, safe areas, and other safety information. QR representatives reported that these sketches were generally undertaken using a Train Notice Diagram as a base, with the protection officer marking up the required safety information to assist in communicating this information at the pre-start brief.
In regards to the Kippa-Ring closure, a Train Notice Diagram for the Petrie Station area was used to sketch or mark-up the closure information. The base (unmarked) Train Notice Diagram displayed the rail infrastructure layout of the Petrie Station, and about 3 km of the Up and Down Northern Lines towards Caboolture. The layout of the Train Notice Diagram was arranged with the Petrie Station layout at the top of the page, with the Caboolture line extension displayed at the bottom of the page (Figure 13).
Figure 13: Train Notice Diagram 126, for Petrie Station

Image showing Train Notice Diagram TN 126. Train Notice Diagram TN 126 describes the rail infrastructure layout and some operational information for Petrie Station. Noting the connection points on the map between the two portions of the Caboolture line. This Train Notice Diagram was used as the base or starting point for recording the worksite sketch information required by the safety assessment and Queensland Rail SW01 Form. Source: Queensland Rail, annotated by ATSB
The mark-up of the safety information on the Train Notice Diagram involved highlighting the closed tracks, and recording where the permanent way protection equipment was to be placed (Figure 14). QR representatives advised that this mark-up would normally be undertaken by the protection officer in charge. However, in this case the supervisor marked up the Train Notice Diagram. The supervisor’s mark-up contained errors that did not accurately depict the open and closed tracks (Figure 14).
Although not a formal process, an independent check of this mark-up would normally be undertaken by either the supervisor or one of the other senior leaders before the protection officers departed for the worksite. On the night of the accident, no independent check of the Train Notice Diagram mark-up was conducted.
Figure 14: Train Notice Diagram pre-planning mark-up

Image showing the Petrie Train Notice Diagram marked up with closure safety information. Noting that highlighted portions of track are intended to depict closed tracks and other markings relate to the location of permanent way protection equipment placement. Image also shows marking error where the Caboolture line was marked as closed. Source: Queensland Rail, annotated by ATSB
The pre-planning work sequence included checks of required equipment and worksite transport, plus the drafting of the pre-start safety briefing in preparation for delivery at the worksite.
Site arrival
Upon arrival at the planned worksite, the protection officer in charge was required to work through the SWMS onsite task sequence to ensure the following tasks were undertaken:
- Confirm correct network location with the NCO, plus complete and read back applicable safeworking forms (SW08 for TOA).
- Communicate pre-start brief to worksite participants.
- Place track protection for possession.
- Complete checklist for protection of track closures, so that all permanent way protection equipment used was recorded and accounted for.
- Contact the NCO and advise what permanent way protection equipment had been placed, and the time that it was undertaken.
Mobile communication devices
A key component of a protection officer’s role is to communicate safeworking information to NCO’s, other protection officers and personnel within their assigned worksite. To facilitate communication, QR issued protection officers with mobile phones.
To manage the risk of distraction in the Danger Zone, the QR safety rules and procedures stated that personnel were not to use mobile communication devices within the Danger Zone.
In addition to this, and specific to protection officers, observational and verbal reaccreditation assessments were undertaken periodically. These reaccreditation assessments included verbal questioning of protection officers on QR’s policies with respect to mobile communication equipment use in the Danger Zone.
An Apple branded mobile phone had been issued to PO1 by QR. Phone records were obtained from the QR mobile phone service provider. The records indicated that no incoming or outgoing phone calls or text messages had been transmitted at the time of the collision. Additionally, email accounts linked to the mobile phone had not been accessed since 13 March 2017. A post-accident examination of the mobile phone settings revealed that a number of mobile phone applications had been permitted to trigger notifications.[24]
Previous occurrences
A review of previous ATSB investigation reports found several investigations relating to track work, which are listed below by common safety factors. The ATSB also periodically conducts research on safe work on track, specifically focusing on track workers involved in conflicts or potential conflict with trains.
Worksite briefing – train running information
RO-2011-006: Collision between freight train 7SP3 and a track mounted excavator near Jaurdi, Western Australia, on 28 March 2011.
On 28 March 2011, at about 1308, a freight train 7SP3 collided with a track mounted excavator between Jaurdi and Darrine, Western Australia. The train driver sustained a minor injury. There was significant damage to the lead locomotive and the excavator, and minor damage to the track as a result of the accident.
The ATSB found that two track mounted excavators had been placed back on the track without permission of the Authorised Employee responsible for the coordination of track side safeworking activities between Jaurdi and Darrine. Another finding was that although separate pre-work briefings were conducted, there was no discussion about train running information and site protection between the Supervisor (Excavators) and the Supervisor (Track Machines).
RO-2015-019: Track worker struck by a passenger train, near Laverton Station, Victoria, on 2 October 2015.
On 2 October 2015, at about 0916, a train departing Laverton Station approached a worksite where a supervisor was marking a track to identify dog spikes to be removed, with a lookout for his protection. The lookout observed the train, warned workers of its approach and signalled to the driver that the track was clear. However, as the train took the crossover, the supervisor was foul of the track, and was struck by the train that was travelling at about 59 km/h. The supervisor suffered serious injuries.
The ATSB found that the pre-work briefing was not conducted. This meant that not everyone in the work group had a clear understanding of train movements that morning. The supervisor may also have thought that the train would proceed on its track and not take the crossover track to his location. It was also concluded that on the train’s approach, the train was given the all clear to proceed prior to the supervisor moving to a position of safety, clear of all tracks.
Protection selection
RO-2015-002: Collision between track worker and passenger train at Guildford, Western Australia on 10 February 2015.
On 10 February 2015, a Public Transport Authority (PTA) maintenance crew commenced work at Meadow Street, Guildford, Western Australia. The crew’s assigned tasks included maintaining the pedestrian gates adjacent to the level crossing. At about 1035, one of the track workers was struck by a Perth-bound suburban passenger train. The track worker sustained fatal injuries.
The ATSB investigation found that the PTA maintenance workers had not implemented any form of track worker protection at the work site. This was partially due to the PTA not having documented instructions specifying the level of protection required, preferring that track workers make their own assessment based on their knowledge of the Network Rules. The ATSB found that, under these arrangements, track workers could make an incorrect assessment, placing themselves at a greater risk of being struck by a train.
__________
- The crossing of a track by another track, roadway or pedestrian pathway by an underbridge or an overbridge, rather than crossing at the same elevation. Source: RISSB Glossary of Railway Terminology, Version 1 3 December 2010.
- A line on which the signalling permits trains to be signalled normally in either direction. Source: RISSB Glossary of Railway Terminology, Version 1 3 December 2010.
- A safety management system (SMS) is a rail transport operator’s primary means for identifying hazards, recording the risks to safety it has identified within its operations, and detailing how those risks are managed and monitored. Source: Office of the National Rail Safety Regulator Website.
- Rail Industry and Safety Standards Board, 2010, National Guideline Glossary of Railway Terminology, Version 1.3.
- Danger Zone is all space within 3 m horizontally from the nearest rail and any distance above or below this 3 m, unless a safe place exists or can be created. Source QR Queensland Network Rules and Procedures Glossary.
- At the time of the accident, QR forms SW01 – Trackside Safety Planner and SW61 – Corridor Access Safety Assessment had recently been combined to reduce duplication (SW01 – Corridor Safety Planner and Assessment - MD-11-279 V7.1). As the information content had not changed, Queensland Rail permitted the superseded SW01 and SW61 use until printed stocks of these forms were depleted. The protection officer in charge was using the superseded forms.
- A facility or device used by a competent worker to prevent either unintended issue of an Occupancy Authority, or operation of points or signalling equipment. Source Queensland Rail (QR) Queensland Network Rules and Procedures Glossary MD-12-189.
- A device attached to a rail that explodes on impact; used to attract attention of rail traffic crews. Source Queensland Rail (QR) Queensland Network Rules and Procedures Glossary MD-12-189.
- A competent worker responsible for keeping watch for approaching rail traffic and for warning other workers to stand clear of the line before the rail traffic arrives. Source Queensland Rail (QR) Queensland Network Rules and Procedures Glossary MD-12-189.
- A notification in the Apple branded mobile phone context is an attention seeking signal that could be badges, sounds, banners, and/or alerts that a mobile phone application can generate to get the attention of the mobile phone user.
On 29 May 2017 at about 2225, a passenger train T570 struck a protection officer at Petrie Station while he was returning to the work team vehicle after placing permanent way protection equipment for a track closure on the Kippa-Ring rail line. As a result of the collision, PO1 sustained fatal injuries.
The ATSB found no technical faults with the train or the driver’s actions on approach to Petrie Station. Speed and braking were consistent with sound driving practice. Consequently, the analysis will focus on the following topics:
- the events leading up to the Kippa-Ring line closure
- Queensland Rail (QR) safeworking procedures.
Personal Continual Vigilance
Personal Continual Vigilance (PCV) was a safety measure available for accessing the Danger Zone to place/remove permanent way protection equipment. PCV required the track worker to see that tracks are clear, frequently look (approximately every 5 seconds) in both directions for approaching rail traffic and not rely on another person to give warning. Consequently, PCV is largely reliant on the track worker having some awareness of their surrounds and an understanding of where the most likely hazards may appear.
A method used in some rail networks, which is consistent with the optional Australian Network Rules and Procedures (ANRP) 2001 requirements, is for track workers to seek some operational awareness of their location by requesting and receiving train running information from the network control officer (NCO). Train running information is defined within the Queensland Rail Network Rules and Procedures (QNRP) as information about rail traffic movement and frequency provided for a particular location. However, the QNRP prohibits the use of train running information being used by protection officers and track workers to provide information about the running of rail traffic.
Further to this, the QNRP is unclear regarding the format of train running information. For example, it is not clear whether it is information about predicted rail traffic timetabled arrival times/frequency through a location, or simply the provision of the current location of the rail traffic approaching the protection officer/track worker’s location. While some logic can be seen in the prohibition of the former, it is possible that train running information describing the current location of the approaching rail traffic could provide protection officers/track workers a benefit from the knowledge of what direction the next rail traffic could approach their location.
On the night of the accident, the protection officers did not seek train running information from the NCO. The protection officers were reliant on their own personal vigilance when within the Danger Zone of the live tracks, in this instance the Up Caboolture line at Petrie.
It is known that providing location information increases the likelihood of detecting targets during visual search tasks.[25] As applicable to rail, having additional information of the environment, in this case the location of any approaching trains, should increase the opportunity for protection officers to detect them while in the Danger Zone.
From this, the ATSB found that there is no requirement in the QNRP for protection officers (when using PCV) to notify the NCO of an intention to access the railway Danger Zone or obtain approaching train running information. Consequently, the protection officers had no knowledge of the direction and location of approaching train movements when accessing the Danger Zone. While the application of PCV may provide a risk control for identifying an approaching train, it only does so if applied effectively. Knowledge of approaching trains in the vicinity through provision of train running information may encourage the more diligent application of PCV.
Personal Continual Vigilance implementation
Protection Officer (PO1) actions
After the placement of permanent way protection equipment and while returning to the work vehicle, PO1 walked along the middle of the track on the Up Caboolture line (Road 4) in a south-westerly direction. This track was live and not part of the Kippa-Ring line closure. The two adjacent tracks, which comprise the Up and Down Kippa-Ring lines (Road 3 and 5) were protected by the closure. The direction PO1 was walking meant that his back was facing the train involved in the collision, which was approaching from the north. Video footage from Petrie Station showed PO1 walking along the track, and was not turning his head every 5 seconds to check for approaching traffic.
It was evident that protection officer PO1 did not apply continuous vigilance techniques when accessing the Danger Zone in accordance with PCV rules. Consequently, he did not see the approaching train in time to avoid being struck by the train.
The ATSB explored the underlying reasons why PCV had not been implemented. While there was some factors that potentially explain PO1’s actions, its effect on the accident could not be determined. The subsequent analysis discusses this evidence and provides possible reasons why PCV was not implemented.
Worksite and Task familiarity
After arrival at Petrie, PO2 and PO3 reported undertaking a pre-start brief. The opportunity for pre-start discussions for all three protection officers together at the bonnet of their vehicle was limited to about 90 seconds. In addition to this, the recorded pre-start brief forms contained errors and inconsistent sign-off entries; it is possible that the recording of the pre-start brief had been rushed.
Further to this, PO1 was not involved, nor required to be, at the briefing of the maintenance workers at Albion Depot, and was not present when PO2 and PO3 discussed details of the closure with the supervisor upon arriving at Mayne Depot. Therefore, PO1’s opportunity for familiarisation of task and safety requirements was possibly limited to the content of the pre-start brief conducted at Petrie.
In October 2016, Petrie Station was opened with its new layout. The new layout included a grade separation of the Up Caboolture Main and the Down Kippa-Ring lines which is an uncommon infrastructure configuration within the QR network. This grade separation creates the situation where the Up Caboolture Main and the Up Kippa-Ring lines are adjacent to each other as they feed into the island configuration platform (Figure 7 above).
The Kippa-Ring line construction was managed and conducted by an independent third party. There were limited opportunities for QR protection officers to become familiar with the new rail infrastructure configuration and layout during construction.
Following the completion of construction, QR took on the management and operation of the new Kippa-Ring line. The implementation of the QR management of change processes for the new Kippa-Ring rail line did not specifically include familiarisation as a risk to protection officers and other track workers. Nor did it specifically identify them as stakeholders to the changes. Therefore, it is likely that the protection officers’ opportunity for familiarisation of the new infrastructure was limited to general staff communications, media coverage, and when tasked with work in the new areas.
The protection officers who worked on the Kippa-Ring Line closure had not been to Petrie since the new layout was completed. Whilst it cannot be confirmed, it is possible that PO1 may have been confused about which tracks were open and closed at Petrie. Particularly as he was unfamiliar with the new layout and which direction the approaching trains were likely to appear from.
The ATSB found that the protection officers were not familiar with the new rail infrastructure and uncommon site layout at Petrie Station. This was influenced, in part, by the late communication of the task assignment.
QR relied on protection officers obtaining familiarity with a new or unfamiliar location by reviewing Train Notice Diagrams or route maps. While these Train Notice Diagrams and route maps provide some information, there were limitations in the topographical information available. The limitations included information about site entry and exit points, rail infrastructure configuration with respect to local physical environment, such as any physical obstructions or barriers to access/escape or sighting of approaching trains.
Protection officers advised that when they had advanced warning of a protection task at a new or unfamiliar location, whilst not a QR requirement, they would consider a visit to the worksite in the days preceding the intended work. While this may assist with familiarisation, there was no formal requirement within the QR safety management system for ensuring the provision of adequate time for the protection officers to familiarise themselves with new or changed work sites.
Train Notice Diagram
The layout and clarity of information is a factor of how people process the information. A principle for information processing is proximity, where display elements that are located close together will tend to be grouped together.[26] Another principle is one of legibility of information,[27] with one example being size. The size of a character for instance, must be large enough so the human eye can resolve the details.
The Train Notice Diagram for Petrie Station (TN 126) was characterised with the extension of the Up and Down Caboolture main lines printed below the Up and Down Kippa-Ring lines (Figure 15).
Figure 15: Train Notice Diagram TN 126, for Petrie Station

Image showing Train Notice Diagram TN 126, which describes the rail infrastructure layout and some operational information for Petrie Station. This diagram has been annotated to show the connection points between the two portions of the Caboolture line, and the conspicuity of the connection point character. Source: Queensland Rail, annotated by ATSB
This layout is potentially conducive to misinterpretation as the Up and Down Caboolture rail lines can be associated as being linked to the Up and Down Kippa-Ring lines due to their close proximity. This is further influenced by the small size and conspicuity of the ‘connection point A’ character used to link or connect the two Caboolture line sections. The potential for error can increase, particularly under conditions of low lighting, or as relevant to this accident, under time pressure.
On the night of the accident, the normal night shift supervisor departed from the normal process, and marked up the Train Notice Diagram himself for the protection officers tasked with the Kippa-Ring line closure. The supervisor incorrectly interpreted the lower line section on Train Notice Diagram (TN 126) as the Kippa-Ring line, and incorrectly marked the open Up and Down Caboolture lines as closed (Figure 16).
The red highlighter marking on the Train Notice Diagram (Figure 16) indicating the Up and Down Kippa-Ring lines and Up and Down Caboolture lines could have been interpreted that these lines were closed. The majority of interviewed protection officers and protection officer supervision staff had difficulties detecting the error, and after the error had been pointed out believed the error had the potential to be confusing.
Figure 16: Train Notice Diagram TN 126, of Petrie Station, as marked up for the Kippa-Ring line closure.

Image showing Train Notice Diagram TN 126 as marked up in error for the Kippa-Ring line closure. Noting that the highlighted portions of the track are intended to show closed track sections within the planned closure, and red arrow indicates connection points of track sections. Source: Queensland Rail, annotated by ATSB
Likely, due to time pressures, the supervisor departed from the normal process and did not seek an independent check of the marked-up Train Notice Diagram from one of the other senior leaders.
It can be observed that there was a potential for confusion in interpreting the Train Notice Diagram with the mark-up errors. However, it cannot be determined what effect the Train Notice Diagram mark-up errors had, if any, on PO1’s understanding of which tracks were open and closed.
Time and work pressure
The protection officers involved in this accident were inadvertently not notified of this task until the night of the accident. This notification was prompted following the supervisor’s phone call enquiry as to the protection officer’s whereabouts when they did not arrive early for their work shift to accommodate the earlier task start time. This then influenced a perception of limited time available to become familiar with the task requirements and perform relevant duties.
Work pressure is defined as degree to which employees feel under pressure to complete work, amount of time to plan and carry out work, and balance of workload.[28] One source of work pressure can be supervisors[29] whereby a supervisor’s influence shapes employee’s habits.
Employees who perceive that they are under pressure to increase production may deviate from safety rules that impede their progress, or perform tasks with less care, increasing the likelihood of errors. There is evidence for a link between work demands and accident involvement, where the higher the perception of work demands, the more accidents that occur.[30] Time pressure has also been found to degrade performance, such as task or load shedding, and a trading of accuracy for speed.[31]
As part of the investigation, the following perceptions were noted as indicators of work pressure. The protection officer in charge (PO3) said he did not feel confident in completing the closure because he was not route competent with the area. He mentioned this concern to the supervisor who said he should be fine to complete the closure because it was a simple closure. He also felt pressured to complete the closure.
PO3 recalled they were ‘rushing’ and felt they had limited opportunity to organise the task properly. He was also observed to appear ‘flustered’ when he arrived at Albion Depot.
PO2 also recalled that he was rushing to complete the pre-start briefing book so the workers from Albion could continue with their tasks. In summary, as the protection officers were inadvertently not advised of their task until the night of the accident, they had insufficient time to prepare for the task and experienced pressure to complete the task within the scheduled time. Given they were also unfamiliar with the area and were working with a marked-up train diagram that contained errors, this time pressure to start and complete their tasks had the potential to lead to the protection officers making mistakes.
Complacency
Complacency is ‘the failure to recognise the gravity of a situation or to follow procedures or standards of good practice’.[32] The rail environment can be repetitive and workers can often operate within the same territory over many years.[33] This means that they are likely to repeatedly encounter the same conditions, which can increase the likelihood of complacency. It is possible that PO1 realised he was walking on an open line but chose not to practice PCV due to complacency. However, there was limited evidence to support complacency in this case.
Distraction from mobile communication devices
Immediately prior to the collision with passenger train T570, PO1 was walking within the Danger Zone of the Up Caboolture line with his back towards the approaching train. Co-workers recalled, and video footage confirmed, that the mobile phone was normally clipped to the front of PO1’s shirt. About 6 seconds prior to the collision, video footage shows PO1’s phone illuminating. At the same time, PO1 stops walking and tilted his head towards his mobile phone.
There was no evidence to support that the mobile phone illuminated at the time of the accident due to the receipt or transmission of any phone calls, text messages or emails. A post-accident examination of the mobile phone settings revealed that a number of mobile phone applications had been permitted to trigger notifications. However, it could not be determined which or even whether a notification led to the phone’s illumination. Overall, the reason why the phone illuminated is unknown.
QR policies prohibit the use of mobile communication devices while in the Danger Zone, requiring personnel to move to a safe place if required to use a mobile communication device in a rail corridor. Protection officer reaccreditation assessments successfully completed by PO1 included verification of an understanding of QR’s polices with respect to mobile communication devices in the Danger Zone.
The effects of mobile phone distraction on performance is well documented in literature in different contexts. Research in pedestrian usage of mobile phones has found that people using their phone (phone call, texting, or listening to music) are less likely to look around their surroundings, recall features of their surroundings, are more likely to engage in unsafe behaviours, and have an increased risk of being struck by a vehicle.[34],[35]
It is important to note the dangers of using mobile phones while undertaking another task. In this case, it was evident that immediately prior to the collision, the protection officer’s attention was diverted to his mobile phone. However, the protection officer was already in a position of danger with a collision imminent at the time when the protection officer’s attention was diverted to his mobile phone.
Safeworking systems - Protection selection
Petrie Station provided reasonable opportunity to sight rail traffic approaching from the Caboolture direction. PO3 had recorded conflicting sighting information in the safety assessment documentation. However, his selection of PCV to protect the protection officers for the open Up Caboolture line (Road 4) at Petrie was compatible with the guidance contained within the QNRP and safety assessment guidance documents SW01 and SW61.
While this decision was compatible, the QNRP provided alternate levels of protection that provided higher levels of protection than PCV. For example, Absolute Signal Blocking (ASB), or Look Out Working (LOW). Noting that the additional protection officer actions required for LOW or ASB compared to PCV are not substantial, and provide a higher level of protection.
The QNRP provided some encouragement to drive selection of higher levels of protection, although it was not consistent for all protection levels or methods. For example, the LOW rule and procedure QR3013 states ‘If the Absolute Signal Blocking or Electronic Authority System Blocking methods are practical, these are the preferred methods over the Lookout Working method’. Whereas there is no such preference suggestion included for PCV.
In consideration of this, the ATSB examined the protection selection decision-making guidance contained within the Queensland Rail Corridor Access Safety Assessment (SW61), and Trackside Safety Protection Planner (SW01). This examination focussed on the effectiveness of the safety assessment documentation in meeting QR’s intent to drive selection of a protection type that provides the highest level of protection.
LOW was prohibited at night, and accepted practice extended this to include the placing or removal of permanent way protection equipment. In respect to hazards associated with protection officers entering rail corridors to place or remove permanent way protection, the local preclusion of LOW as a protection option had an effect on the safety assessment and ultimately protection selection decisions. In explanation, when a safe place is accessible and adequate sighting distance to approaching rail traffic can be maintained, the guidance contained within SW01 and SW61 with the preclusion of LOW leads the user to selecting PCV. Noting that ASB and work on track authorities are not considered for selection unless sighting distance cannot be maintained (Figure 17).
Figure 17: Flowchart showing effect of local preclusion of LOW on protection selection decision-making process, informed by Queensland Rail SW61 and SW01 forms.

This image shows protection level selection flowchart created by the ATSB to explain the effect of the local preclusion of LOW on the protection level selection decision-making process and decision assistance guidance contained in Queensland Rail Corridor Access Safety Assessment (SW61) and Trackside Safety Protection Planner (SW01) forms. Note that the labels, A, B, C within this image depict the procedural flow, which starts at A and proceeds through B to C. Source: Queensland Rail, Annotated by the ATSB.
Protection officers reported that the common operational practice was to select PCV as the preferred choice for initial access to the Danger Zone when placing permanent way protection equipment, or when crossing from place to place.
It is noted that the safety assessment decision-making systems did not require the user to justify or record reasons for rejecting higher levels of protection that might be available (i.e. ASB, or Work on Track Authorities) before selecting the lowest in PCV. There is a risk that this may allow the selection of PCV to be seen as an easier option requiring less additional paperwork.
In summary, the ATSB found that the systems and practices for the selection of protection measures for the placement of permanent way protection equipment did not drive selection to, or seek a justification for the rejection of available, reasonable and practicable higher-level protection measures.
The ATSB has previously undertaken analysis of notifiable occurrence data in regards to safe work on track. This analysis was published in 2017 (RI-2014-011) and found that among the most common events that expose track workers to the highest risk of a collision with rail traffic was the type of protection being insufficient or incorrect.
__________
- Posner, MI, Snyder, CRR, and Davidson, BJ 1980, Attention and the detection of signals, Journal of Experimental Psychology: General, 109(2), 160-174.
- Proctor, RW and Proctor, JD, 2012 Sensation and perception. In Salvendy, G (ed), Handbook of Human Factors and Ergonomics (3rd ed), New Jersey: John Wylie & Sons.
- Salvendy, G 2012, Handbook of Human Factors and Ergonomics, New Jersey: John Wylie & Sons.
- Glendon AI and Stanton, NA 2000, Perspectives on safety culture, Safety Science, 34(1-3), 193-214.
- Kath, LM, Marks, KM, and Ranney, J 2010, Safety climate dimensions, leader-member exchange, and organizational support as predictors of upward safety communication in a sample of rail industry workers. Safety Science, 48, 643-650.
- Clarke, S 2006, Safety climate in an automobile manufacturing plant: The effects of work environment, job communication and safety attitudes on accidents and unsafe behaviour, Personnel Review, 35, 413-430.
- Staal, MA 2004, Stress, cognition, and human performance: a literature review and conceptual framework. Moffett Field: NASA.
- Dekker, S 2000, The field guide to human error. Bedford: Cranfield University Press.
- Sussman, D and Coplen, M 2001, Fatigue and alertness in the United States railroad industry part 1. Transportation Research Part F; traffic psychology and behaviour, 3(4), 211-220. (Although the referenced paper is related to train drivers, the concept is also applicable to track workers.)
- Schwebel, D, Stavrinos, D, Byington, KW, Davis, T, O’Neal, EE, and de Jong, D 2012, Distraction and pedestrian safety: how talking on the phone, texting, and listening to music impact crossing the street. Accident Analysis & Prevention, 45, 266-271.
- Nasar, J, Hecht, P, and Wener, R 2008, Mobile phones, distracted attention, and pedestrian safety. Accident Analysis & Prevention, 40(1), 69-75.
From the evidence available, the following findings are made with respect to the collision between a passenger train and track worker at Petrie Station, Brisbane, Queensland on 29 May 2017. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
- The protection officer PO1 did not apply continuous vigilance techniques when accessing the Danger Zone in accordance with personal continual vigilance (PCV) rules. Consequently, he did not see the approaching train in time to avoid being struck.
Other factors that increased risk
- There was no requirement in the Queensland Rail Network Rules and Procedures for protection officers (when using PCV) to notify the network control officer of an intention to access the railway Danger Zone or obtain approaching train running information. Consequently, the protection officers had no knowledge of the direction and location of approaching train movements when accessing the Danger Zone.
- The protection officers were not familiar with the new rail infrastructure and uncommon site layout at Petrie Station.
- Queensland Rail had no process for ensuring the provision of adequate time for the protection officers to familiarise themselves with new or changed work sites.
- The Train Notice Diagram representation of connecting lines for Petrie Station was conducive to misinterpretation.
- The night shift protection officer supervisor inadvertently marked some open lines as closed on the Train Notice Diagram for Petrie Station used by the protection officers. Independent verification was not undertaken, so the error was not identified.
- The protection officers were inadvertently not advised of the early work shift start requirement. This resulted in the protection officers having insufficient time to prepare for the task and they experienced pressure to complete the task within the scheduled time.
- Immediately prior to the collision, the protection officer’s attention was diverted to his mobile phone.
- The systems and practices for the selection of protection measures for the placement of permanent way protection equipment did not drive selection to, or seek a justification for the rejection of available, reasonable and practicable higher-level protection measures.
Additional safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
As a result of this occurrence, Queensland Rail (QR) has advised the ATSB they have or are taking the following safety actions:
- Immediately following the accident, QR issued a critical safety alert prohibiting all non-safety critical work in the Danger Zone or running lines managed by its Rail Management Centre.
- QR later issued another critical safety alert reinstating work in the Danger Zone with the exception of personal continual vigilance (PCV) on running lines managed by its Rail Management Centre.
- Prior to reinstating the wider use of PCV, a review of PCV was conducted and risk assessed. A number of amendments to the practices and processes in force on the 29 May 2017 have been made. These amendments have been subject to external independent validation and include:
- not using PCV unless specific training has been attained
- reinforcing the requirement to consider a higher level of protection before using PCV
- performing a safety assessment and documenting it on a corridor safety planner and assessment form (SW01) before using PCV for any reason
- only using PCV in groups of two or more, where one of the group is to act as a spotter
- clarifying that PCV can only be used for walking directly across the track from safe place to safe place, or for placement of permanent way protection equipment.
- QR implemented the recommendations and improvements from its ongoing Network Pre-Start Brief Project, including training of employees and enhancing the delivery of the brief.
- QR provided retraining to PO2 and PO3 with respect to the use of PCV, completion of pre-start briefs, safeworking paperwork and use of mobile phones.
- QR engaged an independent rail safety management expert to lead a task force charged with conducting a comprehensive review of hazards, environmental factors, current safety controls and opportunities for safety improvement relating to the safeworking aspect of work on track within the QR network. This review included an examination of:
- the protection planning process
- human factors review of task distribution for protection officers
- task design with respect to safety prioritisation and communication
- team structure in relation to risk and safety culture, including an examination of management supervision and risk complacency.
- Completed an internal review of the Worksite Protection Compliance Inspections Review process and the protection officer 12 month monitoring process. This review raised three secondary recommendations, which are currently ongoing.
- Engaged a consultancy firm to undertake a review of the safety considerations for workers using mobile devices (phones, radios, tablets, mp3 players, etc.) in the rail corridor, in particular risks associated with:
- a worker being struck by a train
- distraction while performing safety critical tasks.
- This review examined the adequacy of current safety controls, opportunities to further reduce risk including benchmarking against other railways and comparable industries.
- Published and issued critical safety alerts relating to the risk of mobile phones in the Danger Zone across the QR network.
- QR reinforced its message about the right to stop work and getting safety right before commencing as part of the Network pre-start brief.
- QR developed a procedure to ensure a uniform and consistent process for marking up Train Notice diagrams, MD-18 352 Detailed Work Plan for Worksite Protection; full implementation of this process is currently ongoing.
Sources of information
The sources of information during the investigation included:
- Queensland Rail
- Queensland Police Service
- Rail Safety Workers involved in accident
- Recorded Data
- Rail Industry Safety and Standards Board (RISSB).
References
Rail Industry and Safety Standards Board, 2010, National Guideline Glossary of Railway Terminology
Clarke, S 1999, Perceptions of organizational safety: implications of the development of safety culture, Journal of Organizational Behaviour, 20, 185-198.
Clarke, S 2006, Safety climate in an automobile manufacturing plant: The effects of work environment, job communication and safety attitudes on accidents and unsafe behaviour, Personnel Review, 35, 413-430.
Dekker, S 2000. The Field Guide to Human Error. Bedford: Cranfield University Press.
Glendon, AI and Stanton, NA 2000, Perspectives on safety culture, Safety Science, 34, 193-214.
Human Engineering 2005 A review of safety culture and safety climate literature for the development of the safety culture inspection toolkit, Research report 367, Bristol: Human Engineering.
Kath, LM, Marks KM, and Ranney, J 2010, Safety climate dimensions, leader–member exchange, and organizational support as predictors of upward safety communication in a sample of rail industry workers, Safety Science, 48, 643-650.
Nasar, J, Hecht, P, and Wener, R, 2008, Mobile telephones, distracted attention, and pedestrian safety. Accident analysis & prevention, 40(1), 69-75.
Posner, MI, and Snyder, CRR, and Davidson, BJ 1980, Attention and the detection of signals, Journal of Experimental Psychology: General, 9, 160-174.
Proctor, RW and Proctor, JD, 2012 Sensation and perception. In Salvendy, G (ed), Handbook of Human Factors and Ergonomics (3rd ed), New Jersey: John Wylie & Sons.
Queensland Rail, Version 1.2 2013, Queensland Network Rules and Procedures, QR2001 – Walking in the Danger Zone.
Rail Industry and Safety Standards Board, Version 1.2 2014, Australian National Rules and Procedures, ANRP2001 – Walking in the Danger Zone.
Salvendy, G 2012, Handbook of Human Factors and Ergonomics (4th edition), New Jersey: John Wiley & Sons.
Schwebel, DC, Stavrinos, D, Byington, KW, Davis, T, O’Neal, EE, and De Jong, D 2012, Distraction and pedestrian safety: how talking on the phone, texting, and listening to music impact crossing the street. Accident Analysis & Prevention, 45, 266-271.
Staal, MA 2004, Stress, cognition, and human performance: a literature review and conceptual framework. Moffett Field: NASA.
Sussman, D and Coplen, M 2001, Fatigue and alertness in the United States railroad industry part I: The nature of the problem. Transportation Research Part F: Traffic Psychology and Behaviour, 3, 211-220.
Young, MS and Stanton, NA 2002, Malleable attentional resources theory: a new explanation for the effects of mental underload on performance. Human Factors, 44, 365-375.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to Queensland Rail, the Office of the National Rail Safety Regulator, and individuals directly involved in the occurrence.
Submissions were received from Queensland Rail and the Office of the National Rail Safety Regulator. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2020
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |