
Safety summary
What happened
On 13 September 2017, the crew of a Boeing 737, registered VH-VUE and operated by Virgin Australia, were flying a scheduled passenger flight from Melbourne, Victoria to Adelaide, South Australia. Shortly before top of descent, air traffic control instructed the crew to perform a high-speed descent. The crew commenced descent with the first officer as pilot flying and the autopilot engaged, and intended to target a descent speed of 320 kt, which was higher than the normal descent speed of 280 kt.
During the descent, the first officer attempted to manage airspeed fluctuations by using changes in the autopilot modes and reductions in the target airspeed. As the aircraft descended through around 17,000 ft, the tailwind affecting VUE decreased suddenly and significantly. The reduction in tailwind caused the indicated airspeed to increase and approach the maximum operating speed limit of 340 kt.
The captain responded to the sudden increase in airspeed by abruptly pulling back on the control column, causing the autopilot to disconnect. The resulting control forces caused sudden changes to the aircraft’s pitch attitude and vertical acceleration. Two cabin crew who had been standing in the rear galley were injured, with one sustaining serious injuries.
What the ATSB found
The ATSB found that a sudden reduction in tailwind caused the airspeed to increase towards the maximum operating speed. The safety implications associated with this event related to the captain’s sudden control inputs to prevent an overspeed, and the consequent effects of vertical acceleration on the aircraft and its occupants. Although there was a resulting one knot overspeed from the sudden speed increase, it was not by an amount that required any structural inspections to ensure the ongoing airworthiness of the aircraft, according to the guidance provided by the aircraft manufacturer.
Even though the autopilot was operating correctly, when the aircraft was approaching and exceeding the maximum operating speed, the captain’s perception was that the autopilot was not controlling the aircraft and that urgent intervention was necessary. However, the captain did not follow the normal procedure for taking over control of pilot flying duties. The large pitch control inputs made by the captain were probably influenced by the captain’s perception of urgency.
The ATSB also found that the captain was highly concerned about avoiding an overspeed. This was partly because of a perception that Virgin Australia were also concerned about overspeed and wanted to avoid overspeed events, and partly because of a perception that minor overspeeds had significant implications for the safety of the aircraft. These factors contributed to how the captain responded to the sudden increase in airspeed towards the maximum operating speed.
The crew identified the risk of overspeed earlier in the descent, but did not discuss how they would manage that risk. This reduced the pilots’ ability to effectively respond to the overspeed situation, and probably contributed to the rapid, reflexive nature of the captain’s control inputs.
What's been done as a result
Virgin Australia have updated the training and information provided to pilots about overspeed and overspeed recovery. The intent of these actions was to reinforce the correct overspeed recovery technique, and to provide a greater opportunity for pilots to understand the negative safety implications of manual inputs to correct a minor overspeed. These actions have included an animation showing pilots mishandled and correct overspeed recoveries, and an update to manuals which explains that the 737 has been flight tested at speeds above VMO.
Virgin Australia have also changed procedures for ground handling staff when responding to requests from emergency services.
Safety message
During this accident, the pilots accepted and targeted an air traffic control instruction to conduct a high-speed descent. Due to increased kinetic energy and reduced margins to placard speed limits, high-speed descents involve a higher level of risk, including increased risk of harm due to abrupt control input. Pilots are entitled to decline air traffic control instructions where they do not perceive they can safely comply.
This accident highlights the challenges pilots face when responding to sudden or unexpected situations. There will often be a reduction in safety when pilots perceive a situation is urgent and when they make decisions rapidly and reflexively. In these situations, pilots may not be able to effectively process information or make good decisions.
Wherever possible, pilots should take the opportunity provided in an earlier stage in flight to identify risks and take steps to reduce the likelihood of a critical situation developing. Potential threat identification and planning for their management should also involve considering, as a multi-person crew, what the implications of a perceived risk might be, and how to respond if the threat does develop. By taking steps in an earlier stage in flight, pilots can improve their ability to respond effectively to threats. The Federal Aviation Administration Aeronautical Decision Making material provides pilots with accessible guidance on these concepts.
On the afternoon of 13 September 2017, the crew of a Boeing 737-800 aircraft, registration VH‑VUE (VUE) and operated by Virgin Australia (VA), were operating a scheduled passenger service from Melbourne, Victoria to Adelaide, South Australia. The scheduled departure time for this flight was 1605 CST.[1]
The flight crew comprised the captain and the first officer (FO), and these pilots had flown VUE together on the preceding flight. The cabin crew comprised the cabin supervisor (CS) and three other cabin crew. There were 151 passengers on-board.
In preparation for the flight to Adelaide, the flight crew reviewed various information relating to the en route and destination weather conditions. The captain briefed the CS, advising the expected flight time was 65 minutes and that the forecast weather was the same as local conditions in Melbourne, which the CS perceived as cloudy.
For the flight to Adelaide, the FO was pilot flying (PF) and the captain was pilot monitoring (PM).[2] At 1610, VUE departed from Melbourne and climbed to flight level (FL) 360.[3] The departure, climb and cruise were uneventful.
Crew instructed to perform high-speed descent
At about 1642, the aircraft was south-east of Adelaide, maintaining FL 360 and approaching top of descent. Air traffic control (ATC) issued the crew clearance to conduct a DRINA NINE ALPHA standard instrument arrival route[4] (STAR) for an approach to runway 23, and when ready descend to FL 250. This STAR provided tracking information including a series of waypoints, altitude and speed restrictions, positioning the aircraft to the north-east of Adelaide to commence an approach to runway 23.
Figure 1 shows the flight path of VUE, with the DRINA NINE ALPHA STAR waypoints overlaid. The original STAR procedure is provided in Appendix A – DRINA NINE ALPHA STAR. This procedure required inbound aircraft track to the DRINA waypoint, then to pass overhead COMLY at or below 13,000 ft.
A few minutes after issuing the STAR, when VUE was 136 NM (252 km) south-east from Adelaide and 93 NM (172 km) from the DRINA waypoint, ATC cancelled all speed restrictions and instructed the crew to maintain maximum speed on descent, which the pilots understood as an instruction to make a high-speed descent. The FO said to the captain that they would ‘see how (the aircraft would) go’ with an airspeed of 320 kt, but that this might be too fast. The captain responded by saying ‘she’ll be right, don’t overspeed’.
Figure 1: Flight path of VH-VUE with DRINA NINE ALPHA STAR waypoints overlaid

Source: Google Earth, with aircraft track and Airservices Australia waypoint information overlaid by ATSB
Descent into Adelaide
Prior to commencing the descent, the crew set up the aircraft’s flight management system (FMS) based on the ATC clearance, and then commenced the approach briefing. The crew programmed a selected airspeed of 310 kt into the FMS.
At about 1652 the captain briefed the CS for the descent, advising that the aircraft would commence its descent to Adelaide in around 30 seconds, and that the expected arrival time was 15 minutes earlier than planned.
Soon after VUE began descending, airspeed started to increase. The FO made a number of changes to the autopilot mode and settings in order to prevent airspeed from increasing too much (see Recorded information). However, airspeed continued to increase. The crew remarked that the changes to the autopilot mode and settings did not help much, with the FO saying that the autopilot ‘doesn’t (manage airspeed) very well…it just doesn’t like to hold her steady’. The captain reminded the FO ‘don’t overspeed’.
Recorded data indicates the crew began increasing the selected airspeed on the mode control panel (MCP) incrementally during the early stages of the descent when approaching the start of the STAR. (Figure 11 in Appendix B – Flight data recorder data shows changes to the selected airspeed, actual airspeed, autopilot modes and other recorded parameters during the descent.)
At about 1654, when VUE was descending through FL 335, the flight crew made the ‘cabin crew prepare for landing’ announcement. Shortly after, the flight crew continued the approach briefing, including briefly reviewing threats (see Other flight crew procedures), then performed the descent checklist.
The crew selected the briefed descent airspeed of 320 kt at about 1656, when the aircraft was descending through FL 250, and the aircraft reached that speed soon after. VUE remained at 320 kt for the following few minutes.
About two minutes later, the aircraft was approaching waypoint DRINA descending through FL 220, when the FO saw the tops of stratocumulus cloud, which the FO thought were about at FL 150.
The FO suggested that it may be appropriate to activate the fasten seat belt sign. The captain responded that the conditions at the time were good, and the FO agreed with that assessment. The captain asked the FO if there were any reports or concerns of turbulence. The FO responded that there had been no reports and was not worried. The fasten seat belt sign remained off.
According to information provided in ATSB interviews after the accident, the captain also wanted to leave enough time for the cabin crew to complete their duties. The FO thought the clouds beneath VUE might be associated with turbulence later in the descent, but at that time the FO was comfortable with the seatbelts sign remaining off for ‘a bit longer’.
At around this time, the FO reduced the selected airspeed to 310 kt. Soon after, VUE commenced the turn towards COMLY.
Captain intervention
At about 1659, VUE was 15 NM (28 km) from COMLY and descending through FL 170. Airspeed reduced by around 10 kt to the selected 310 kt.
Airspeed then started to increase, first gradually, then more rapidly. The flight crew observed the indicated airspeed approaching VMO (maximum operating speed), and the FO observed the airspeed trend indicator[5] move past the lower band of the red bars on the primary flight display airspeed indicator. Both pilots expressed statements of concern and alarm.
The captain called ‘pull-up’ while also making two abrupt nose-up inputs on the left (captain-side) control column. The first was 49 lb (about 22 kg), which caused the autopilot to disconnect. The captain abruptly released the controls and then made a second control input of 28 lb (about 13 kg) about 4 seconds later.
The FO heard the autopilot disconnect audible alert and saw the captain pulling on the control column and acknowledged that the captain had control of the aircraft.
About 8 seconds after the captain’s initial nose-up input and autopilot disconnect, the captain prompted the FO to resume duties as pilot flying, and a normal transfer of control was performed. The flight crew perceived they had encountered severe atmospheric turbulence. Shortly after the FO resumed pilot flying duties, the captain said ‘better put the belts on’, to which the FO responded ‘check’.
The FO continued to fly the aircraft for around 30 seconds before re-engaging the autopilot. During this period, the FO made several nose-down inputs, peaking at 32 lb (about 15 kg) 10 seconds after the initial nose-up input. Shortly after the autopilot was re-engaged, cabin crew contacted the flight crew and reported that the cabin was not secure, and that one of the cabin crew members at the rear of the aircraft had broken their leg.
With the captain communicating with the cabin crew, the FO (who was pilot flying) notified ATC that VUE would not meet the height requirement for COMLY due to encountering turbulence. ATC advised the crew that they could cancel all height requirements and reduce their speed.
Around 90 seconds later, ATC contacted the crew of VUE to confirm their report of severe turbulence. The captain responded in the affirmative and added that the turbulence was associated with some cloud.
Events in the cabin
The cabin crew recalled that the flight had been smooth during the cruise and initial descent, with no turbulence experienced. At the time the flight crew made the ‘cabin crew prepare for landing’ announcement, the in-flight food and drink service had been completed and rubbish collected. Following this announcement, the cabin crew completed duties including securing the cabin for landing. The cabin crew then returned to the forward and rear of the aircraft, with the two cabin crew members in the rear of the aircraft standing in the galley eating a meal.
Cabin crew members recalled an abrupt upset in the cabin, which they perceived as sudden and without warning. One of the cabin crew members in the rear galley was thrown up towards the ceiling, then fell to the floor. The cabin crew member felt their leg snap on landing and was unable to move from the floor.
The sudden changes in pitch attitude also injured the other crew member in the rear of the aircraft. This crew member struck their jaw on the galley bench and had other minor injuries to their body and face.
The CS reported to the ATSB that they experienced muscular skeletal injuries from the accident and had sought out chiropractic care.
After the aircraft had stabilised, the cabin crew member who suffered a leg injury was given oxygen using a portable on-board cylinder.
At about 1704, the CS confirmed with the flight crew the requirement for an ambulance and that the injured cabin crew member was unable to move to a seat for landing and would stay on the galley floor.
The CS then made positional changes among the cabin crew, moving the uninjured cabin crew member from the forward cabin to the rear, and the cabin crew member who sustained minor head injuries to the front. The CS also briefed able-bodied passengers in the last seating row about what the cabin crew might request, to assist with disembarkation if the situation escalated or in case of another emergency. The cabin crew members took their assigned seats for landing.
Coordination and response at Adelaide Airport
At about 1702, the captain contacted VA ground personnel in Adelaide and notified them that a cabin crew member had been injured during turbulence and requested an ambulance on arrival.
The flight crew then notified ATC about the injured cabin crew member and requested Aviation Rescue Firefighting (ARFF) personnel to meet VUE at the arrival gate to provide first aid until the ambulance arrived.
Around the same time, VA personnel notified the SA Ambulance Service (SAAS) of the injury on-board VUE, and that an ambulance was required at the emergency gate at Adelaide Airport, to go airside.[6]
At about 1709, ATC notified ARFF about the accident, and a crew were dispatched around two minutes later. An ARFF officer also contacted SAAS, to confirm an ambulance was en route. During this phone call, the ARFF officer directed the ambulance to the arrival gate via the upstairs sections of the main terminal.
VUE arrived at its bay at around 1719. ARFF personnel had pre-positioned at the bay and entered the cabin via the rear stairs soon after the aircraft arrived. A VA ground supervisor also came into the cabin to assist with the situation. The SAAS patient treatment record indicated the ambulance crew arrived at the Adelaide Airport terminal entrance at 1719, and proceeded to the arrival gate, commencing treatment at 1725.
There was extensive discussion between the ARFF, the SAAS and the VA ground supervisor about how to remove the injured cabin crew member from the aircraft. With a badly broken leg, the injured cabin crew member was not able to walk or to sit in a wheelchair, and the ambulance stretcher did not fit down the aircraft aisle. The emergency services personnel suggested using a scissor lift or catering truck appliance and asked the ground supervisor to assist with this. The ground supervisor advised that no scissor lift was available and declined the use of the catering truck.
After considerably more deliberation, the injured cabin crew member suggested that the ambulance officers conduct the extraction from the aircraft using a slide sheet. Emergency services personnel used the slide sheet to drag the injured cabin crew member along the aisle to the front of the aircraft, then placed the injured cabin crew member on a stretcher. SAAS records showed the ambulance departed the airport at 1845.
__________
- All times in this report are expressed in terms of Central Standard Time (CST, UTC+9:30)
- Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
- At altitudes above 10,000 ft in Australia, an aircraft’s height is measured in hundreds of feet above the standard atmospheric pressure datum of 1013.25 hPa. A height 35,000 ft above that standard pressure datum would be expressed FL 350.
- A standard instrument arrival routes (STAR) is a designated arrival route linking a significant point, normally on an air traffic services route, with a point from which a published instrument approach procedure can be commenced.
- The airspeed trend indicator is on the primary flight display, and shows the predicted airspeed in 10 seconds time. The context section of the report provides more detail about airspeed indicators in the 737
- The term ‘airside’ means the restricted part of an aerodrome where aircraft movements occur, and where unauthorised personnel are excluded for security and safety reasons. This includes the aircraft parking apron and the runways.
Flight crew information
The captain joined Virgin Australia (VA) as a Boeing 737 (737) first officer in 2003 and received command upgrade in 2012. The captain had a total flying experience of around 18,000 hours, including over 4,000 hours as captain and almost 6,000 hours as a first officer in the 737.
The captain reported being rested before starting work on the day of the accident. The captain woke at around 0530 for a 0930 sign on, had completed two short sectors prior to the accident flight and had one short sector scheduled afterwards. On the second sector, the captain had flown into Melbourne with the accident flight first officer (FO).[7]
The FO joined VA as a Boeing 777 second officer in 2010, and qualified as a 737 FO in 2012. The FO had a total experience of around 8,500 hours, including around 3,500 hours in the 737.
The FO reported having a normal sleep on the night before the accident and was feeling alert at the top of descent into Adelaide. The FO recalled waking at 0500 on the day of the accident and leaving for work at 0645 for a 0830 sign on. The accident flight was the FO’s third of four scheduled short sectors that day.
Cabin crew information
The cabin supervisor (CS) joined VA in 2003 and became cabin supervisor in 2004. The CS was also involved in training other cabin crew, including instructing cabin crew non-technical skills.
The cabin crew member who sustained serious leg injuries had worked as a cabin crew member since 2002 and joined VA in 2005. The cabin crew member also had qualifications as an enrolled nurse, and was a first aid instructor at VA.
The cabin crew member who sustained minor head and facial injuries had only recently joined VA, and the accident occurred on this cabin crew member’s first day after paired ‘buddy’ training.
Aircraft information
VH-VUE was a Boeing 737-800. There were no indications that any mechanical issues with the aircraft were contributory to the accident. After the accident, maintenance personnel conducted a severe turbulence inspection which did not identify any damage or faults.
Airspeed indications
Figure 2 illustrates how airspeed indications are displayed to the crew on the 737 primary flight display.
Figure 2: Airspeed indications on the 737 primary flight display

Source: Boeing 737 Flight Crew Operating Manual (FCOM). Copyright Boeing.
- Item 1 and Item 5: Selected airspeed. The magenta numbers (Item 1) and speed bug (Item 5) display the targeted airspeed, set by the pilots. In the example shown, this is 250 kt.
- Item 2: Speed trend vector. The green arrow displays the predicted airspeed in 10 seconds time. This prediction is derived from the air data inertial reference system and is based on the current airspeed and acceleration. In the example shown, the green arrow predicts the airspeed increasing to about 258 kt.
- Item 3: Current airspeed. The white value displays the current calibrated airspeed. The value shown is between 242 and 243 kt.
- Item 4: Maximum operating speed. The lower of the red bars indicates the maximum speed as limited by lowest of the landing gear placard speed, flap placard speed, or VMO/MMO.
Prior to the autopilot disconnect, the flight crew observed the current indicated airspeed increase to near VMO. The FO also observed the speed trend vector increase to within the lower band of the red bars, indicating that if not slowed the airspeed would exceed VMO within the next 10 seconds. According to the captain’s interview with the ATSB, the captain did not specifically look at the speed trend vector prior to pulling back on the control column in response to the sudden speed increase.
Autopilot modes and airspeed management
Airspeed is the result of the balance between thrust and drag, both of which can be controlled by the automatic flight system (AFS) or the flight crew. The 737 AFS consists of the automatic flight director system (AFDS) and the autothrottle and can operate in multiple vertical and lateral navigation modes. When engaged, the vertical navigation modes control the vertical path and speed by adjusting engine thrust (through the autothrottle) and pitch attitude (through the AFDS). The vertical navigation modes seek to maintain waypoint altitude and speed crossing restrictions programmed into the flight management system in the vertical navigation path mode, or values input to the vertical speed and altitude controls on the mode control panel (MCP).
When the autothrottle is engaged in a mode to control airspeed, the airspeed is adjusted by increasing or decreasing the engine thrust. Alternatively, when the AFDS is in a mode that controls airspeed, airspeed is adjusted by changing the pitch attitude to increase or decrease the drag. To increase the airspeed, the pitch is reduced (nose down), and to decrease the airspeed the pitch is increased (nose up). Depending on the mode engaged, the AFS alters the pitch or thrust commands to attain and/or maintain either the airspeed selected in the flight management system or on the MCP.
Sudden changes in the magnitude of head/tailwind can have the effect of changing the airspeed. For example, a decrease in a tailwind can result in an effective increase in airspeed, all other factors being equal. In order to maintain the target airspeed, the AFS will either pitch the nose of the aircraft up or down, or increase/decrease thrust (depending on the selected mode).
Figure 3 shows the 737 MCP. Located on the glareshield panel, pilots use the MCP to select autopilot modes, and change autopilot target values such as airspeed and vertical speed. For example, pilots can use the IAS/MACH selector to change the MCP selected airspeed or use the vertical speed thumbwheel to change the target vertical speed.
Figure 3: 737 mode control panel

Source: Boeing 737 FCOM. Annotated and cropped by ATSB. Copyright Boeing.
For most of the descent into Adelaide, the pilots engaged the AFS in level change mode. In this mode, the autothrottle engages in the RETARD then ARM modes, meaning the autothrottle reduces the thrust setting to idle, and the pilots have manual thrust control using the thrust levers. The AFDS engages the speed mode, which means the AFDS commands adjustments to pitch attitude to maintain the speed set in the MCP IAS/MACH selector. The AFS system will not accept a selected airspeed greater than VMO.
The FO, who was pilot flying (PF), also intermittently selected the vertical speed mode. In this mode, the AFDS commands pitch attitude adjustments to hold the target vertical speed entered using the MCP vertical speed thumbwheel. The autothrottle is engaged in speed mode to hold the selected airspeed. In descent, engine thrust will be at idle, meaning the autothrottle cannot reduce thrust to target a reduced airspeed.
The AFS mode reversion provides automatic controls which provide additional protections when the AFDS or autothrottle alone are insufficient to prevent exceeding a placard limit speed. In the case of VMO, if the autothrottle is engaged in speed mode and the thrust levers are at idle, the engine thrust cannot be reduced further to prevent a speed increase. If the AFDS is in vertical speed mode, the AFS mode will automatically change to level change mode to provide speed control using pitch attitude changes.
Although different AFS modes automatically maintain the selected airspeed and prevent VMO overspeed, the AFS is not capable of preventing temporary exceedances in certain circumstances. Where the aircraft encounters sudden environmental changes, such as severe windshear, this may exceed the performance capability of the AFS. This may result in temporary overspeed, particularly when the aircraft is operating close to VMO or other limit speeds.
Control options for disconnecting the autopilot
Figure 4 shows the 737 autopilot disengage controls. The autopilot is typically disengaged by pressing the autopilot disengage button on either control wheel. A ‘disengage’ bar is also available on the MCP, which can be pulled down to disengage the autopilot. The position and design of these controls is such that they are accessible from the position of either pilot, and are simple to operate.
Figure 4: 737 Autopilot disengage controls

Source: Boeing 737 FCOM, Cropped and annotated by ATSB. Copyright Boeing.
The autopilot will also disengage if the pilot applies sufficient force to ‘breakout’ or ‘pull through’ the flight controls. After the autopilot has been disconnected, the pilot has full manual control of the aircraft’s pitch and roll attitude. An audible autopilot disconnect alert tone is produced whenever the autopilot is disconnected.
For this event, the captain pulled back on the flight controls, and did not report using either the disengage bar or switch. This action resulted in the autopilot disconnecting due to the breakout function.
Speed brakes
Pilots can extend the 737 speed brakes to increase drag, using the speed brake lever. The Boeing 737 Flight Crew Training Manual (FCTM) provided procedures for using the speed brakes in-flight. These procedures said that ‘the speedbrake may be used to correct the descent profile if arriving too high or too fast’. These procedures also noted that using speed brakes enabled the aircraft to decelerate up to 50 per cent more quickly.
For this event, the pilots did not use speed brakes to reduce airspeed prior to the overspeed or during the recovery.
Atmospheric conditions
Crew perceptions of weather conditions
In preparation for the flight, the pilots reviewed information about the forecast meteorological conditions. The information provided to the pilots included the significant weather charts for Australia for Flight Level (FL) 100-250 and FL 250-650, as well as the trend forecast, meteorological aerodrome report and aerodrome forecast for Adelaide. Other documents included the VA operational flight plan for the flight to Adelaide.
The significant weather charts (shown in Appendix C – Significant weather chart) forecast an area of moderate clear air turbulence from FL 100 to FL 250, which covered the planned route from around 95 NM (175 km) east of Adelaide. The aerodrome forecast for Adelaide was for westerly winds of 20 kt with gusts up to 30 kt, together with intermittent periods of reduced visibility in rain showers and small hail, and broken cloud at 2,500 ft.
The operational flight plan included a dispatcher note to the crew stating that the flight had been planned at FL 360 as this level had been reported ‘smooth’ by previous crews.
The captain reported considering that the overall weather conditions were mostly fine, although noting there was a chance of clear air turbulence en route. The FO identified that conditions may include gusty winds, and noted the forecast included small hail.
The crew reported that the actual conditions for the majority of the descent were smooth. At interview, the FO said that VUE was not in cloud at any time. At the time of the overspeed and sudden changes in pitch attitude, the FO recalled that that VUE was passing through thin wispy cloud.
The captain reported being surprised by the overspeed and perceived turbulence, because there had not been any returns on the weather radar, and that VUE was flying in light cirriform type cloud. The captain recalled the crew had not received any reports of turbulence from ATC or other aircraft. The captain’s initial notification of the accident to the ATSB stated that the overspeed and perceived turbulence occurred when VUE was in cirrus type cloud tops.
At 1645, a pilot of an aircraft departing Adelaide reported to the Adelaide approach controller that they had encountered light and occasionally moderate turbulence between FL 140 to 170. The crew on board VUE were not aware of this report.
Atmospheric data recorded by aircraft
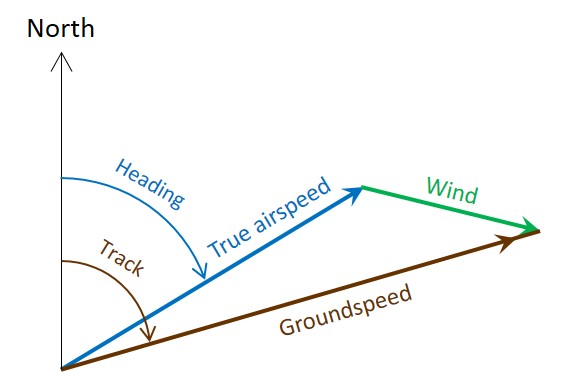
The ATSB derived estimates of the instantaneous local wind speeds during the descent using the airspeed, groundspeed, track and heading information recorded by the flight data recorder (FDR).
The path that the aircraft travels over the ground is a combination its speed and direction through the air and the movement of the air through which it is travelling. As such, the local wind vector (speed and direction) is derived as the difference between the true airspeed and the groundspeed vectors, as shown in Figure 5.
Figure 5: Calculation of local wind vector (green) using the true airspeed (blue) and groundspeed (brown) vectors.
Source: ATSB
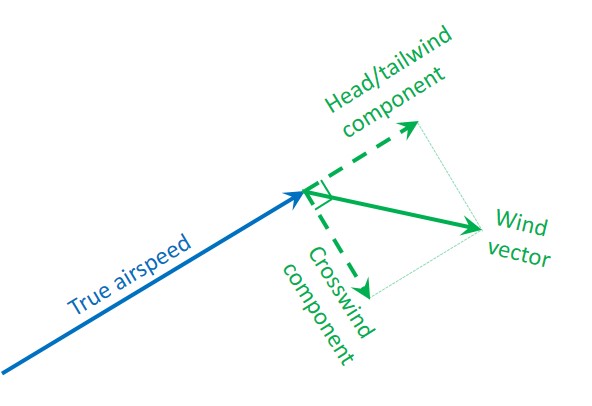
The wind vector may be illustrated as two components when referenced to the true airspeed. The component of the wind vector parallel to the true airspeed is the head/tailwind component, and the perpendicular component is the crosswind (Figure 6). The wind vector represents the direction that the wind is coming from, so with reference to the aircraft, a positive parallel component is a tailwind.
Figure 6: Wind components. The component of the wind that is parallel to the true airspeed is the head/tailwind and the perpendicular component is the crosswind.
Source: ATSB
Figure 7 shows the variation in the calculated wind vector and headwind components around the time of the autopilot disconnect. During that period, the wind component changed from almost no headwind component to a tailwind of about 25 kt, where it stabilised for about 10 seconds. Immediately before the overspeed, tailwind dropped by about 13 kt in around 2 seconds. This appears to have been due to a combination of a decrease in the wind strength and a change in the direction of the wind.
Figure 7: Plot of the calculated wind (light green), wind direction (yellow), headwind component (dark green), and aircraft heading (blue) during a two minute period around the autopilot disconnect.

Source: ATSB
Estimating wind information from FDR data is complex, and the reliability and validity of information recorded by aircraft sensors may be influenced by factors such as the sensor location and the sampling rate. Aircraft are also operating in a complex three-dimensional environment, where the aircraft body angles may not be aligned with the aerodynamic flight path vectors (for example, the vector directions may be effected by angle of attack and sideslip angles).[8] The ATSB analysis was based on a simplified two-dimensional model of the aircraft environment.
While the ATSB’s analysis is appropriate for the purpose of estimating relative changes in the wind, analysis conducted by the manufacturer provided further certainty on the estimated wind changes. The manufacturer conducted a kinematic consistency analysis, which they describe as being ‘used to correct inherent inconsistencies often present in recorded data from different sensors because of the presence of instrumentation biases due to misalignment in inertial measurements, contamination of pressure and altitude measurements due to flow separation, and sample rate differences.’
The manufacturer’s kinematic consistency analysis also found that there was a sudden decrease in the tailwind component shortly before the airspeed rapidly increased towards VMO. This change in tailwind component was of a similar magnitude to that calculated in the ATSB’s analysis.
Recorded information
Personnel from VA secured a copy of the quick access recorder (QAR) data for analysis and provided a copy of that data to the ATSB. The FDR and cockpit voice recorder (CVR) were also removed and sent to the ATSB laboratory in Canberra for analysis. The following describes the recorded sequence, changes to the aircraft autopilot modes and key flight data parameters during the descent into Adelaide:
- The flight crew commenced the descent with the autopilot engaged. Shortly after commencing the descent, the FO selected the level change AFS mode. There was a gradual increase in airspeed from around 1653:30, when VUE was descending through FL 340.
- At 1654:10, the FO briefly changed the AFDS command mode to vertical speed, with a setting of -650 ft/min, winding back to -450 ft/min. This was consistent with the pilots controlling the aircraft speed by reducing the descent rate. A few seconds later, the level change mode was re-engaged.
- The computed airspeed reached the selected target airspeed (320 kt) about 1656:30, as VUE was passing through FL250. For the next few minutes, airspeed was stable at around 320 kt.
- Figure 8 shows the changes to the autopilot modes and airspeed from 1658:00, when VUE was descending through around FL 200. Figure 9 shows changes to the flight controls and the aircraft vertical acceleration during that period.
- At 1658:18 the FO reduced the target airspeed to 310 kt. While the AFDS responded accordingly by adjusting the pitch angle, airspeed remained at about 320 kt.
- The FO selected the vertical speed mode again at 1658:38, with a vertical speed of -2,600 ft/min. The AFDS responded by adjusting the pitch angle to meet the new selected vertical speed. The FO then gradually wound back the selected vertical speed to -1,200 ft/min. The aircraft achieved the selected vertical speed, but airspeed remained at around 320 kt. At 1658:52, the FO re-engaged the level change mode.
- At about the same time, the autopilot commanded a turn towards the COMLY waypoint, as part of the STAR. The tailwind started to increase from around 20 kt to 38 kt, which contributed to the computed airspeed decreasing towards the target airspeed (310 kt). As the computed airspeed approached the selected airspeed, the autopilot decreased the pitch attitude.
- At 1659:05, the FO then selected the target airspeed to 300 kt. However, airspeed began to increase, from about 310 kt to 320 kt.
- The AFS and both pilots responded to the increase in airspeed. At 1659:10, the AFDS reduced the nose-down pitch angle. At about the same time, the FO engaged the vertical speed mode, quickly winding the selected vertical speed back from -1,200 ft/min to -400ft/min.
- At 1659:14, as the aircraft was descending through around 17,000 ft, the tailwind component quickly reduced from 23 to 12 kt and the wind direction changed (as described in Atmospheric data recorded by aircraft above). The airspeed quickly increased towards VMO (340 kt).
- At 1659:16 (vertical purple dotted line in Figure 8 and Figure 9), the captain suddenly pulled back on the control column, with a maximum 49 lb backwards control force. This caused the autopilot to disconnect and resulted in a large increase in the aircraft pitch attitude.
- The captain suddenly released the controls after the autopilot disconnect, then pulled back on the controls again a few seconds later. The vertical acceleration rapidly increased to 2.3 g, before rapidly decreasing to 0.9 g. This was immediately followed by another rapid increase to 1.95 g, consistent with the second nose-up control input made by the captain.
- At 1659:19, the airspeed peaked at 341 kt, before declining quickly to around 280 kt.
Figure 8: Recorded data parameters including autopilot modes, pitch angle and vertical acceleration

Source: ATSB
Figure 9: Recorded data parameters including control column force

Source: ATSB
Windshear and autopilot performance
The ATSB considered the influence of wind changes on the changes to VUE’s airspeed during the descent. Figure 10 shows the changes in computed airspeed and headwind immediately before and after the overspeed and autopilot disconnect. This analysis indicates that there was a 10 kt speed increase between 1659:06 and 1659:13 that did not appear to be due to change in the headwind component. However, between 1659:14 and 1659:16 (when the autopilot disconnected), the rapid increase in the computed airspeed was consistent with a 12-14 knot change in the headwind component. The second rise in computed airspeed about 2 seconds later was also consistent with another change in the headwind component. This is consistent with a windshear encounter during the descent into Adelaide.
Figure 10: Comparison of the calculated headwind changes (green) and the computed airspeed (blue) in the two minute period around the autopilot disconnect.

Note on graph vertical axes: the left (wind component) and right (airspeed) are on the same relative scale (that is, a 10 knot change in the wind is the same as a 10 knot change in the airspeed). The computed airspeed scale is shifted to provide comparison.
Source: ATSB
When the FO engaged the vertical speed mode to respond to the speed increase, this automatically changed the autothrottle mode from ARM to MCP SPD. Because the thrust was already at idle, there was no capability for the autothrottle system to reduce the airspeed by reducing the thrust. Thus, when the AFS mode was changed, the AFS did not have an effective control over the airspeed, aside from mode reversion to level change mode.
The FCOM states that mode reversion occurs slightly before the aircraft reaches VMO, but does not define the exact point of reversion. In this case, because the pull-through of the control column disengaged the autopilot, this prevented the mode reversion system from engaging. It is unknown to what extent the aircraft would have exceeded VMO had AFDS continued to manage airspeed and the captain not intervened in this way.
The vertical speed selected by the FO was less than the current vertical speed, which would normally be expected to reduce the airspeed. However, the change in the headwind component was probably too rapid for this to be effective. In this instance, it may have been more effective to have left the AFS in level change mode, where the AFDS could provide management of the airspeed.
Handover and takeover procedures
Duties within the cockpit are normally allocated such that only one pilot, the pilot flying (PF), is responsible for manipulating the flight controls and providing input to the AFS. This delineation of responsibilities is important, for maintaining certainty of who is controlling an aircraft.
VA manuals described the procedures for handover and takeover of flying duties. The procedures stated that handover must always be done in a ‘positive manner’ using standard phraseology.[9]
The captain noted that the intervention procedures normally included notifying the PF, and waiting for the PF to relinquish control. The captain identified not saying anything prior to pulling back on the control column, and described this as a reflex action. The captain implied that the decision to take control was rapid, and that a quick action was required given what they perceived to be the state of the aircraft.
The FO reported noticing that the captain had control when the autopilot disconnect audible alert was heard and the captain was observed making control inputs. The FO reported relinquishing control and immediately assumed the role of pilot monitoring (PM). The CVR recorded the autopilot disconnect tone, followed shortly by the FO saying ‘you got it’ then ‘you have control’. Shortly after, the captain said to the FO ‘you go, no you’re right’, and the FO responded ‘I have control’.
Safety systems for overspeeds
Safety implications of VMO overspeed
The United States’ Federal Aviation Regulations (FAR) 25.1505 - Maximum operating limit speed defined VMO as ‘a speed that may not be deliberately exceeded in any regime of flight (climb, cruise, or descent’. These regulations state that VMO/MMO must be sufficiently below the design dive speed of the aircraft, to make it highly improbable that the latter speeds will be inadvertently exceeded in operations.[10] Other regulations provide further guidance on the calculation of the margins between VMO/MMO and these other limit speeds.
The FCTM described the concept of VMO and the causes of VMO overspeed:
VMO/MMO is the airplane maximum certified operating speed and should not be exceeded intentionally. However, crews can occasionally experience an inadvertent overspeed. Airplanes have been flight tested beyond VMO/MMO to ensure smooth pilot inputs will return the airplane safely to the normal flight envelope…Although autothrottle logic provides for more aggressive control of speed as the airplane approaches VMO or MMO, there are some conditions that are beyond the capability of the autothrottle system to prevent short term overspeeds
In a section related to procedures for rapid descent, the FCTM stated:
When descending at speeds near VMO / MMO with the autopilot engaged, short-term airspeed increases above VMO / MMO may occur. These are most often due to wind and temperature changes. These short-term increases are acceptable for this manoeuvre and the autopilot should adjust the pitch to correct the airspeed to below VMO / MMO.
The FCTM said that any time VMO is exceeded, the maximum airspeed should be noted in the flight log. A VA Flight Crew Information Bulletin (FCIB) issued on 4 October 2016 similarly noted that pilots should make maintenance log entries and safety reports for any overspeeds.
The 737 maintenance manual required a structural examination of the aircraft if a VMO exceedance was greater than 20 kt (that is, where airspeed exceeded 359 kt). There were no maintenance actions required for VMO overspeeds less than 20 kt.
VA management of overspeed and flight crew understanding of overspeed implications
VA utilise a flight data analysis program (FDAP) to systematically analyse the flight data generated in each flight, in order to make comparisons between actual operations and company procedures, and to identify non-normal occurrences. VA’s internal investigation into the accident involving VUE noted that during the period 2014 to 2016 there was a tendency for pilots who exceeded VMO to be made subject to operational clearance (SOC). The VA investigation report identified that these overspeed events were often unavoidable. Pilots declared SOC must cease flying duties until given formal notification that the SOC restriction was been removed. Pilots declared SOC typically underwent remedial training and re-assessment prior to resuming flying duties.
The VA internal investigation noted that in early 2017 (before the accident), VA management of minor exceedances shifted, which VA described as a shift in risk tolerance. After this change, the usual response involved reviewing recorded data from the flight, and no further action would typically be pursued if that review identified the crew action had been in line with procedures. After the accident involving VUE, VA provided education to pilots about the FDAP and the management of safety events during 2018 and 2019 (see Safety issues and actions).
The FO stated that it was ‘not a nice feeling’ when an aircraft exceeded VMO. However, the FO also reported intending to let the aircraft overspeed prior to the captain’s intervention. The FO believed that if they had exceeded VMO, the aircraft would be recovered to normal flight, and would require an engineering inspection and safety report.
During company interviews following the accident, the captain reported being mindful that a VMO exceedance would flag in the FDAP. During interview with the ATSB, the captain reported perceiving it was very important to prevent the aircraft from exceeding VMO, and that there was a recent significant focus within VA relating to avoiding overspeeds, which included extensive simulator and classroom training over a period of around 12 months, focussing on the correct use of the overspeed procedures described in the FCTM. The captain described being wary of avoiding overspeed if possible, because it was not good for the aircraft, and because the company did not want any overspeeds.
The captain also stated that VA pilots were generally wary about overspeeds. Although both pilots perceived that 320 kt was the standard or usual target speed for high-speed descent, the captain related that some company pilots would only target 300 kt during descent to avoid exceeding VMO. The captain reported hearing informal rumours prior to the accident that having an overspeed would result in ‘the company wanting to have words with you’. The captain said that their preference for avoiding overspeed was probably influenced by the company’s preference to have less overspeed events.
Information the captain provided at interview indicated a limited awareness of the relationship between VMO and the other aircraft limit speeds. The captain indicated not being aware that overspeeds less than 359 kt did not require maintenance inspection, and did not cause any other delay or significant consequence. When the captain saw the airspeed increasing towards VMO, the captain thought this meant the autopilot was not controlling the aircraft.
Speed management and overspeed recovery
There were no specific procedures for the management of high-speed descents. As such, there were no procedures that described the target speeds pilots should adopt during high-speed descents, or how pilots should use autopilot modes or speed brakes to manage speed in these situations.
Other VA and Boeing procedures described the methods pilots should use to manage speed around VMO, including recovering from overspeed. The 737 FCTM provided procedures for avoiding and recovering from overspeed, including in the descent stage of flight. In the section titled ‘Overspeed’ the FCTM stated that:
If autothrottle corrections are not satisfactory, deploy partial speed brakes slowly until a noticeable reduction in airspeed is achieved…
When encountering an inadvertent overspeed condition, crews should leave the autopilot engaged unless it is apparent that the autopilot is not correcting the overspeed. However, if manual inputs are required, disengage the autopilot. Be aware that disengaging the autopilot to avoid or reduce the severity of an inadvertent overspeed may result in an abrupt pitch change.
During climb or descent, if VNAV or LVL CHG pitch control is not correcting the overspeed satisfactorily, switching to the V/S mode temporarily may be helpful in controlling speed. In the V/S mode, the selected vertical speed can be adjusted slightly to increase the pitch attitude to help correct the overspeed. As soon as the speed is below VMO/MMO, VNAV or LVL CHG may be re-selected.
VA sent company pilots a Flight Safety Notice in 2014, titled Exceedance of VMO/MMO and Assigned Altitude. Although this notice primarily related to overspeed associated with entry to Jetstreams on climb on in cruise, it highlighted that
VMO/MMO is the maximum operating speed and should not be exceeded intentionally, however small excursions of a short-term or transient in nature are within the design envelope of a jet transport aircraft. That is, there is minimal operational impact. Notwithstanding this, anytime VMO/MMO is exceeded the maximum speed and time above
VMO/MMO should be noted. VMO/MMO exceedance poses less risk generally than an excursion beyond a cleared altitude or Flight Level. A VMO/MMO exceedance is preferable to an altitude bust, or large abrupt control inputs.
Any VMO/MMO exceedance must be entered in the Maintenance log and a safety report must be submitted.
The Flight Safety Notice also highlighted relevant sections of the FCOM and FCTM.
In 2016, VA sent company pilots two FCIBs titled ‘Managing VMO Exceedances and Wind Gradients near Jet Streams’ and ‘Assigned Altitude Overshoot and Overspeed Exceedances’. These bulletins provided further information about the risk of overspeed and how they should be avoided and managed, including:
- A number of VA crew had pulled back on the control column in an attempt to avoid overspeed. This had led to autopilot disconnection, large abrupt control inputs and significant g forces.
- The focus ‘needs to be on a preventative strategy and recovery technique’.
- High-speed descents need to be managed carefully, and this may include early descent at reduced speed to avoid potential overspeed.
- Level change or vertical navigation speed are the recommended modes for high-speed descents in conditions with steep wind gradients or turbulence.
- ‘It is preferable to accept a temporary overspeed (provided it is not excessive or sustained) rather than…large abrupt control inputs at high altitude’.
- The recovery technique for overspeeds is to ‘leave the autopilot engaged unless it is apparent that the autopilot is not correcting the overspeed. Be aware that disengaging the autopilot to avoid or reduce the severity of inadvertent overspeed may result in an abrupt pitch change and high ‘g’.’
- On descent, crews should command reduced airspeed and use temporary vertical speed mode selections to recover from overspeed.
Both the captain and the FO had passed simulator training sessions focusing on overspeeds, with the most recent session for each pilot occurring in 2014. The simulator scenario involved an overspeed during the cruise stage of flight, and pilots were evaluated based on their application of the procedures described in the FCTM.
The pilots recalled VA training and procedures for managing and recovering from overspeed. The captain recalled that VA training on overspeed recovery included using the vertical speed autopilot mode, and the speed brake. The captain also recalled that one VA training document stated that a small overspeed was better than an abrupt recovery. However, the captain noted that there was ambiguity in what was a small overspeed that could be allowed, as opposed to a larger overspeed, which was problematic. That is, the captain identified that the procedures did not define what a ‘small’ overspeed was.
The FO recalled pilots were taught to use the level change and vertical speed AFS modes and speed brake to recover from overspeed, and that if the aircraft was going to overspeed, to let it overspeed. The FO reported believing they would have applied the speed brake to recover from the overspeed situation, had the captain not intervened.
Control sensitivity at high-speeds
As a general principal, aircraft control systems are more sensitive in high energy states such as high-speed, high-altitude flight. This means that control inputs have larger effect when the aircraft is at higher speed. The FCTM noted the potential for over-control due to increased control sensitivity at high-speed, stating:
There have been reports of passenger injuries due to over-controlling the airplane during high altitude, high airspeed flight when overriding the control column with the autopilot engaged or after disengaging the autopilot with the disconnect switch.
Pilots should understand that, in general, the airplane is significantly more sensitive in pitch response (load factor) to column movement at cruise than it is at lower speeds associated with take-off and landing.
The captain reported not expecting to pull back very forcefully when taking manual control of the aircraft. However, reflecting on the development of the accident, the captain considered that their control inputs may have exacerbated what they perceived as the turbulence experienced by the aircraft.
Summary of overspeed safety systems
The ATSB considered the safety systems used by VA to reduce the risk of overspeed and unsafe interventions during overspeed events. Although no procedures specifically related to managing airspeed during high-speed descents, other procedures described the methods for managing airspeed around VMO. Both pilots understood the procedures for managing airspeed on descent, and the FO reported planning to apply the speed brake prior to the captain’s intervention.
Within the safety system, there were controls that sought to reduce the likelihood of pilots unnecessarily taking manual control to prevent overspeed. The documentation suite instructed pilots that the autopilot should be left engaged. During post-accident interviews with the ATSB, both pilots exhibited a good understanding of those procedures.
The defences associated with preventing unsafe pilot interventions during overspeed were thus mainly procedural controls. This is understandable, as pilots should have the ability to take manual control of the aircraft if they perceive the need to do so. The defences within the safety system were associated with supporting effective decisions about intervening.
Pilots’ understanding of aircraft capabilities and limitations is informed by documentation and training. In this case, the documentation provided by VA and Boeing did provide a reasonable indication that minor overspeeds were not problematic. The FCTM advised that pilots sometimes inadvertently encounter overspeed during operations near VMO, and this message was reinforced in the FCIB. The FCTM also contained emergency rapid descent procedures in which VMO was intentionally targeted, and therefore it would be a reasonable inference that minor exceedance of VMO would not risk the safety of the aircraft.
However, the documentation provided by VA and Boeing did not clearly express the tolerances of the 737 to minor overspeeds. VA documentation said that flight crews should document their airspeed any time airspeed exceeded VMO, even though a maintenance inspection was required only for exceedances above 359 kt. In this regard, the documentation provided to pilots could be interpreted as any exceedance of the VMO limit of 340 kt had safety implications.
Although the captain had concerns about an overspeed, this was probably not due to any systemic deficiencies in the documentation, or the training provided to flight crews. It is likely that all pilots, to some extent, have an aversion to exceeding defined limitations. The captain’s concerns about exceeding VMO were probably a reflection of this. Additional context about tolerances beyond VMO in documentation and training may reduce pilots’ concerns about minor overspeeds.
ATC speed control procedures
Air traffic control (ATC) instructions to arriving aircraft can include speed control. Speed control instructions may be based on considerations such as aircraft operational requirements and requirements for managing inbound aircraft traffic. The Airservices Australia Manual of Air Traffic Services (MATS) stated that when applying speed control, ATC should (among other responsibilities):
advise the pilot of future intentions; advise the pilot to resume normal speed as soon as the application of speed control is no longer necessary; and make speed adjustments judiciously in advance of the point at which the new speed is required, depending on the aircraft type and amount of adjustment involved.
MATS identified a speed guidance for Virgin 737 aircraft of 280 kt at 30 NM from an aerodrome. This documentation also identified that the maximum descent speed for these aircraft was 340 kt.
In November 2017 (after the accident), Airservices Australia published a revised MATS, which specifically advised controllers to ‘avoid cancelling published speed restrictions for arriving aircraft, except when necessary for traffic management or aircraft operational requirements’. Changes also included that controllers should not use the phrases ‘NO ATC SPEED RESTRICTIONS’ or ‘NO SPEED RESTRICTIONS’ when issuing speed control instructions to aircraft on a standard instrument arrival route. MATS was later revised to show a maximum descent speed of 320 kt for Virgin 737s.
VA advised that they had asked Airservices to review and change the MATS speed table to align the maximum descent speeds for the B737 for all operators. VA also advised the ATSB that they had asked Airservices to review the terminology ATC were using for issuing speeds on descent, to ensure that standard phraseology was being used.
Airservices advised the ATSB that there had been no internal reviews or investigations associated with this accident.
Acceptance of high-speed descent clearance
As a general principle, the captain of an aircraft has responsibility for ensuring the operational control of an aircraft, which includes accepting air traffic control requests for high-speed descent. The captain reported having no hesitation to deny an ATC request to conduct a high-speed descent, if the captain felt that was necessary.
The captain also reported not being able to recall if ATC instructed the aircraft to ‘make maximum speed’, or if the clearance was to target 320 kt. The FO recalled that ATC had issued the crew with a clearance for a high-speed descent but did not recall any details of the wording of that clearance. The implication, therefore, is that the pilots perceived the instruction issued by ATC as a clearance to conduct a high-speed descent; both pilots recalled that 320 kt was selected as a target speed in response to this clearance.
The ATSB did not find that the wording of the high-speed descent instruction by ATC had any influence on the target speed set by the pilots, or how the pilots managed their speed during the descent.
Other flight crew procedures
The descent procedures applicable to the crew of VUE were described in the 737 Flight Crew Operations Manual (FCOM). These procedures specified the requirement for crews to conduct an ‘approach briefing’ prior to the top of descent. The VA Operating Policies and Procedures Manual stated that flight crews should conduct a review of threats as part of the arrival briefing, which is equivalent to the approach briefing.
The procedures for the threat and error management review stated that the purpose was to review potential threats and determine the best management strategy. The procedure identified possible threats, including significant weather, and noted that the identified list of threats was not exhaustive. The procedures did not identify overspeed as a possible threat.
During the descent into Adelaide, the flight crew briefly conducted a review of threats. The FO noted the potential threats of turbulence and exceedances. The crew did not observe any indications suggesting turbulence. However, when the FO mentioned the threat of exceedances, the captain made a strong informal interjection saying ‘Don’t exceed anything…’ The crew did not discuss these threats any further, nor did they discuss a management strategy.
Cabin crew briefings
VA procedures required the flight crew to brief the cabin crew at different stages of the flight, including pre-flight and at the top of descent. The procedures stated that the pre-flight briefing should include information about the en route weather, any special considerations, and any deviation from normal conditions. Similarly, the top of descent briefing was required to include information about the possibility of turbulence, adverse weather, likelihood of the seatbelt sign being activated early, and ‘other anticipated special considerations for descent, approach and arrival’.
The captain briefed the CS pre-flight, and before top of descent into Adelaide. Neither briefing mentioned the forecast clear air turbulence, nor was the possibility of turbulence otherwise indicated. The top of descent briefing did not mention the planned high-speed descent.
The cabin supervisor (CS) reported that their prior experience was that captains usually advised the cabin crew about planned high-speed descents. The CS perceived this was best practice as it allowed the cabin crew to have awareness of the changed descent conditions.
The ATSB also spoke to a senior pilot from VA about cabin crew briefings for high-speed descents. That pilot reported that it was not typical for captains to brief cabin crew about a planned high-speed descent, and explained that in many cases, ATC issue clearance for high-speed descent after the top of descent. The procedures did not include a requirement to include planned high-speed descent in cabin crew briefings.
The ATSB does not draw an inference from the absence of information about the high-speed descent from the top of descent briefing. However, as expanded on in Unsecured cabin crew, cabin crew are reliant on the pilots for information about the descent conditions, and in this instance the cabin crew had no opportunity to modify their procedures during the descent.
Cabin crew procedures
Normal cabin preparation for landing
VA cabin crew procedures stated that the flight crew would make the ‘cabin crew prepare for landing’ announcement 10 minutes before the crew were required to be seated for landing, and that this would be at about 20,000 ft or higher for 737 aircraft. Cabin crew were then required to:
- cease all service involving carts
- secure their area of responsibility, including cabin and galley areas.
Toilets could still be used at this time.
The procedures required the PM to activate the fasten seat belt sign at transition level[11] or 10,000 ft, whichever occurred first. After the PM had switched on the fasten seat belt sign, the procedures were for the cabin crew leader to then make the ‘seat belt sign for landing’ announcement. Cabin crew were then required to:
- check their area of responsibility and ensure passenger seat belts are fastened, toilets are locked, and personal electronic devices are away.
- return to their seat within one minute and be secured for landing including using a shoulder harness.
Prior to the sudden changes in pitch attitude, the ‘cabin crew prepare for landing’ announcement had been made, and the cabin crew had performed the duties required following that. The flight crew had not turned on the fasten seat belt sign, and there was no requirement for the cabin crew to be seated. The sudden pitch changes occurred about 7 minutes after the flight crew made the ‘cabin crew prepare for landing’ announcement.
The ATSB also sought to identify when the seatbelt sign was activated after the overspeed and sudden pitch changes. At interview, the captain reported believing the seatbelt sign was activated immediately after the sudden pitch changes. However, both the CS and the injured cabin crew member said that they observed the seatbelt sign remain off throughout the descent. The FO reported not being able to recall whether the seatbelt light was turned on immediately after the sudden pitch changes or later in the descent.
The illumination of seatbelt sign was not a parameter recorded on either the FDR or the QAR. However, when the seatbelt sign is turned on or off, a distinct audible tone is produced. The prescribed standards for Airborne Passenger Address Amplifiers are for the activation of the seatbelt sign to be associated with a single 494 Hz low tone (equivalent to musical note B). Other signals are associated with a high tone (587 Hz), and combinations of high and low tones.
The ATSB review of the CVR identified a single low tone, consistent with the activation of the seatbelt sign, at 1659:30. This was after the sudden pitch changes, and consistent with the pilots expressing the intent to turn the seatbelt sign on.
Cabin preparation in turbulent conditions
The VA Aircrew Emergency Procedures Manual described procedures for situations when pilots expected turbulence based on information from sources such as the Bureau of Meteorology, weather radar, ATC and reports from other aircraft. If the flight crew judged that turbulence was likely, they were required to inform the cabin crew during the briefings or another suitable time. The pilots were required to activate the fasten seat belt signs no later than one minute prior to the anticipated turbulence.
When turbulence was expected, the procedures instructed cabin crew to prioritise personal safety, and to not risk personal injury by continuing service. During actual turbulence, the procedures said cabin crew should secure themselves by sitting down or holding on to seat backs, evacuation handles or grab handles, where possible.
Because the descent conditions were smooth, and the captain did not perceive there was a risk of turbulence, the pilots did not turn on the fasten seat belt signs.
Stowage of oxygen bottles
The VA Aircrew Emergency Procedures Manual stated that on-board oxygen bottles could be used for a first aid situation. During landing, the procedures said that the oxygen bottles should be secured under a seat. These procedures also specified ‘precautions’ about the use of oxygen bottles, including ‘do not drop or bump oxygen bottle’.
The cabin crew related that their training had emphasised the importance of properly stowing portable oxygen bottles during approach and landing. However, they were unable to comply with the procedures on this occasion, because the injured cabin crew member was not able to move into a seated position. The injured cabin crew member reported maintaining a firm grip on the oxygen bottle during the approach and landing.
The ATSB sought information from the aircraft manufacturer in relation to securing oxygen bottles during landing. The manufacturer subsequently provided the following guidance:
- If the condition does not allow proper stowage, the oxygen bottles have shoulder straps that can provide some level of containment.
- For a condition where a cabin crew member could not be seated for landing, the crew member should position themselves against structure forward of their position for support in any deceleration condition associated with landing.
- The operator can evaluate their own configuration and determine the best course of action for the situation encountered in the occurrence.
Cabin crew incapacitation
The VA Cabin Crew Policy and Procedures Manual described procedures for managing cabin crew member incapacitation. Cabin crew were required to administer first aid, advise the CS and flight crew as soon as possible and place the crew member in a non-exit row passenger seat. The procedure was to then liaise with the captain on positional changes and alternate procedures for landing and reassign cabin duties based on the captain’s instructions. The procedures also included instructions for a single cabin crew member to operate two exit doors in these situations. The CS recalled VA cabin crew emergency procedures training was based on a single incapacitation. The CS said that scenario-based training for multiple incapacitation would have assisted the CS’ response to the accident.
Following the overspeed and cabin injuries, the CS advised the flight crew that the injured crew member was unable to move into an aircraft seat, and that the remaining crew would be repositioned to monitor the rear doors and the injured cabin crew member. The flight crew considered this information during the approach and landing, with the captain saying to the FO ‘Try to make it as smooth as possible. Try not to hit on the brakes too hard. I think (the injured cabin crew member) may still be on the floor’.
Management of injured persons at Adelaide Airport
Adelaide Airport Aerodrome Emergency Plan
The Adelaide Airport Aerodrome Emergency Plan (AEP) provided guidelines to co-ordinate response to and recovery from emergencies at the airport. The medical emergency procedures included that the SA Ambulance Service (SAAS) was the control agency. This means that SAAS were responsible for the overall direction of the activities associated with the response, including tasking and co-ordinating other agencies.
For medical emergencies, the AEP included procedures for notifying airport management, SAAS and Aviation Rescue Firefighting (ARFF). The AEP stated that ‘the plan is based on the assumption that each agency with a statutory responsibility has in place appropriate supporting procedures which deals with that agency’s response in accordance with this plan’.
Adelaide Airport also had procedures and plans related to co-ordinating ambulance access airside. In these procedures, airlines and the SAAS were to notify Adelaide Airport. An airport operations officer could then arrange for an escort from the airport emergency gate to the airside location.
Adelaide Airport advised that there were no entries made in their operations logs in relation to the accident, with the implication being that Adelaide Airport emergency operations personnel had not been alerted to the situation. Adelaide Airport personnel were not requested to arrange for airside ambulance access to VUE.
Relevant VA procedures and context
The VA Guest Services Procedures Manual contained procedures for medical emergencies ‘In Flight or Aircraft Not Parked at Terminal’. These included procedures for the flight crew to contact the medical information provider Medlink, so that Medlink could support the assessment and treatment of the affected persons. During this occurrence, the flight crew determined that it was appropriate to prioritise the descent and landing, so Medlink was not contacted at any stage.
The manual also included procedures for co-ordinating disembarkation, which were that:
The AMCO (Airport movement coordinator)/Airport Manager/attending medical personnel, in consultation with the pilot-in-command, will decide the method of disembarkation and which door the guests are to disembark from that will allow the medical team to, where required, gain immediate access to the person requiring medical assistance.
For this occurrence, the flight crew were not involved in consultation with the medical personnel about the extraction of the injured cabin crew. The captain perceived that with emergency services personnel, cabin crew and the ground operations supervisor in the rear cabin, there was not enough room for him, and also that the attending personnel were managing the situation.
VA advised the ATSB that in the event of a medical emergency response, once the ARFF personnel arrived on scene, VA personnel were no longer involved in the decision making around extraction of injured persons.
The ARFF officers asked the VA ground operations supervisor about access to a scissor lift or a catering truck. The ground operation supervisor identified that there was no scissor lift available and told the ARFF approval was not given for the use of the catering truck. In interview, the ground operations supervisor related that their concerns about using the catering truck included:
- The catering truck was not VA equipment and was operated by a contractor.
- The use of the catering truck was not part of VA ground handling procedures.
- The ground operations supervisor had never heard of the catering truck being used for the purpose of removing an injured person from an aircraft.
- The ground operations supervisor perceived that there was a significant fall from height risk. The normal operation of the catering truck involved the use of harnesses. The ground handling supervisor also said that from its ‘lowered’ position, there is around 1.5 m from the catering truck platform to the ground.
The ground operations supervisor perceived that working from heights risks were a main safety focus for VA ground operations. The ground operations supervisor had concerns about what would happen if the injured cabin crew member fell during a lift onto a catering truck, from the perspective of the injured cabin crew being seriously injured and also in terms of repercussions for the ground operations supervisor. The ground operations supervisor recalled a previous incident where someone was injured falling from an aircraft, which added to the concern about the fall from heights risk.
The ground operations supervisor also related that, at around the time the request to use the catering truck was made, the ambulance officers were on-board the aircraft. The ground operations supervisor perceived that the ambulance officers had control of the situation and the injured cabin crew member was in a stable condition. Also perceiving that the emergency services personnel were working towards a plan for the extraction from the aircraft, the ground operations supervisor did not consider it was necessary to explore further the option of arranging the catering truck.
Airport Rescue and Fire Fighting procedures
During an emergency response, ARFF provided first aid to injured persons until ambulance personnel arrive. Once the ambulance personnel are on-site, ARFF procedures were to hand over treatment and management of any casualties.
The ARFF personnel reported they had previously used scissor lift and catering truck appliances in similar situations, and perceived that this would be appropriate for removing the injured cabin crew member. However, this option was not given further consideration after the VA ground services manager denied the request.
ARFF reported that their officers did not assist with the removal of the injured cabin crew member. The ARFF officers handed over treatment and management of the injured cabin crew member to the SAAS and followed the direction of SAAS thereafter.
Previous occurrences
The ATSB reviewed recent accidents involving cabin crew injuries resulting from manual flight control inputs to prevent overspeed during descent. The following four examples were identified which show themes in the development and consequences in these accidents. This is not an exhaustive set of all similar accidents in the time period.
- AO-2014-032 In-flight upset, inadvertent pitch disconnect, and continued operation with serious damage involving ATR 72 aircraft, VH-FVR, 47 km WSW of Sydney Airport, NSW, on 20 February 2014. In this occurrence, a rapidly decreasing tailwind lead to an increase in airspeed towards VMO. In response to the unexpectedly high airspeed trend indication and proximity to VMO, the captain made nose-up pitch commands without following the take-over procedure. The aircraft pitched up and down suddenly, and a cabin crew member in the rear of the cabin suffered a broken leg.
- AO-2015-041 Flight path management occurrence involving Boeing 737, VH-YID, 55 km from Adelaide Airport, South Australia, on 9 May 2015. During a high-speed descent, the airspeed increased towards VMO. The first officer responded to the unintended speed increase by pulling back on the control column until the autopilot entered a secondary mode. There was a sudden release of the control column, and one cabin crew member in the rear of the aircraft fell, sustaining a knee injury.
- AAIB investigation into Boeing 737-8AS, Serious injury to cabin crew, during descent to Manchester Airport, United Kingdom, on 14 January 2017. During a high-speed descent, a decrease in tailwind contributed to a VMO overspeed. Because the captain perceived that the autopilot was not correcting the situation, the captain disengaged the autopilot using the autopilot disengage button, and pulled back on the control column. During the accident investigation, the captain reported pulling back with more force than intended. The aircraft experienced abrupt pitch changes and one cabin crew member in the rear of the aircraft suffered a fractured ankle.
- AO-2017-030 Flight path management occurrence involving Boeing 737, VH-VZZ, near Canberra Airport, ACT, on 13 March 2017. During a high-speed descent, a sudden decrease in tailwind contributed to an increase in airspeed towards VMO. The pilot flying pulled back on the control column, causing the autopilot to disconnect. The aircraft experienced sudden pitch changes, and a cabin crew member in the rear of the aircraft suffered a fractured leg.
As this summary indicates, overspeed is a risk during high-speed descent, particularly if the aircraft encounters a sudden change in wind. Pilots have responded to overspeeds by making large pull-back control forces. As highlighted in this accident and the summarised previous occurrences, the application of large control forces to correct or prevent overspeed can cause significant injuries in the cabin.
Previous VA overspeeds and autopilot disconnects
The ATSB reviewed data from other overspeed events involving VA 737s in the years prior to the occurrence. VA provided summary details of flight data from all VA 737 flights from 2014-2017, where airspeed exceeded VMO. This showed numerous overspeed exceedances, none of which involved a maximum airspeed above 359 kt, so none required a maintenance inspection.
VA also extracted data to describe 737 flights from the same period where the airspeed from top of descent to FL 50 was between 319 kt and 339 kt, to understand the actions of pilots attempting to control speed close to VMO In its internal investigation report, VA observed that ‘the data demonstrates in the last three years B737 pilots have entered CWS Pitch or manual control in an attempt to avoid a VMO/MMO exceedance or to rapidly decelerate below it.’ The data did not indicate the portion of these events where the autopilot was disengaged using the dedicated controls compared to flight control pull-through.
__________
- Both pilots were based in Melbourne. Expressed as local times for the pilots’ home base (UTC +10:00), the captain woke at 0600 for a 1000 sign on. The FO woke at 0530, left home at 0715 for a 0900 sign on.
- See ‘The Answer is Blowin’ in the Wind - The Use of Recorded/Derived Wind Data in Investigations’ by Neil Campbell (2012), for an overview of the complexities in estimating wind information from FDR data.
- The standard phraseology for transferring control is ‘I have control’ for the pilot taking PF duties, and ’you have control’ for the pilot relinquishing PF duties
- The design dive speed of an aircraft is a more restrictive limit, designed to provide a margin between maximum cruise and operating speeds and the capabilities of the aircraft. For more information about design dive speeds and the calculations of airspeed margins see FAR 25.335 Design airspeeds and FAR 25.253 - High-speed characteristics.
- The transition level represents the upper band of the transition layer, below which pilots much reference the local area QNH for altimetry. The transition level will be between 11,000ft and 12,500 ft, depending on QNH. For more information about these concepts, see the Aeronautical Information Package, published by Airservices Australia.
Introduction
During a high-speed descent, the airspeed of VH-VUE increased unexpectedly and briefly exceeded the VMO limit of 340 kt. This was contrary to the operating procedures provided by the manufacturer and the operator, and contrary to the intentions of the flight crew. The captain responded to the sudden increase in airspeed by pulling back on the control column causing the autopilot to disconnect. This caused pitch changes that resulted in large changes to vertical acceleration and injuries to cabin crew at the rear of the aircraft.
The recorded data showed the development of the pitch changes was sudden, and that the onset coincided with the autopilot disconnect. The pitch changes dissipated after the large control inputs had ceased. From this, the ATSB determined that it was highly unlikely that atmospheric turbulence caused the pitch changes.
Although VMO was exceeded, it was not by an amount that required any structural inspections to ensure the ongoing airworthiness of the aircraft, according to 737 maintenance manual. The captain’s intervention probably reduced the magnitude of the eventual overspeed, and it is unknown to what extent the aircraft would have exceeded VMO had the captain not intervened. However, the recorded data indicated that the autopilot was responding to the speed increase by raising the pitch of the aircraft. Furthermore, the pilots could have used the autopilot disengage controls rather than applying breakout force and could have reduced the aircraft speed using the speed brakes.
Therefore, the safety hazards involved in this accident were primarily associated with how the captain acted to prevent overspeed, and the consequent effects of vertical acceleration on the aircraft and its occupants.
Development of the overspeed
The flight crew accepted an instruction from air traffic control to perform a high-speed descent. Accepting a high-speed descent instruction was not unusual, and the ATSB did not find that the issuance or acceptance of a high-speed descent were factors that increased risk. However, targeting a higher descent speed reduces the margin between the target airspeed and airspeed limitations, and the risk of injury due to sudden control inputs will increase due to higher speed and increased kinetic energy.
The flight crew managed the descent using level change autopilot mode, with intermittent use of the vertical speed command mode. This was generally consistent with procedures and airspeed was generally stable at 320 kt during the early descent.
However, about 30 seconds after the turn towards COMLY, when VUE was descending through around 17,000 ft, a sudden decrease in tailwind associated with a windshear encounter led to a rapid increase in airspeed.
After observing the speed increase and trend towards the maximum operating speed (VMO), the first officer (FO) changed the autopilot mode from level change to vertical speed. This is commonly used by flight crew to reduce the airspeed because, in a descent, reducing the vertical speed raises the nose of the aircraft, which consequently also reduces the aircraft’s airspeed. This was also consistent with the procedures in the Flight Crew Training Manual, and bulletins produced by the operator.
However, vertical speed mode does not directly control the aircraft’s speed, and if a windshear results in a large and rapid airspeed change, it may not provide sufficient speed control. Use of control modes that directly control the airspeed, such as the level change mode, allow the aircraft to respond directly to the airspeed changes. This is why the automatic speed protection will change from vertical speed to level change mode. Noting, however, that for very rapid wind changes, as was seen on this occasion, even the automatic flight director system (AFDS) may not be able to prevent an overspeed.
A few seconds later, the captain, who was pilot monitoring (PM) responded to the increasing airspeed by pulling back on the control column, which resulted in the autopilot disconnecting. Two seconds after the autopilot disconnect, the VMO was exceeded by one knot.
Neither crew member applied the speed brakes to prevent the speed increase, nor during recovery from the overspeed. Although they need to be applied with care at high speed, the use of speed brakes would have reduced the likelihood of an overspeed without generating large flight loads and pitching motions.
Intervention to correct speed increase
The captain responded to the unexpected speed increase by pulling back firmly and abruptly on the control column to raise the pitch attitude of the aircraft’s nose. The captain took manual control of the aircraft without notifying the FO (who was pilot flying). This was not consistent with the normal process for handover and takeover. In situations where the pilot monitoring (not flying) perceives immediate action is required to avoid a hazardous situation, there will be a tendency for the transfer of control to happen more rapidly. However, it is still important for flight crew to formally identify who has control, to maintain clarity of the pilots’ roles.
Perceived urgency and lack of autopilot control
The large pull-back control input caused an autopilot disconnect and sudden changes in pitch attitude, resulting in injuries to the cabin crew.
The initial forceful pull back on the control column was in response to what the captain perceived to be a situation involving a nose-down attitude and an unexpectedly high airspeed indication. The sudden pull-back movement was a reflexive application of well-rehearsed basic flying principles, being consistent with an attempt to raise the nose of the aircraft, rather than an explicit attempt to disconnect the autopilot.
The captain indicated at interview that their pull on the control column was more forceful than planned. Consistent with this, the 49 lb backwards force applied by the captain is a large amount of force for a pitch up manoeuvre during high-speed flight and was not consistent with procedures that cautioned against making large control inputs during high-speed, high-altitude flight.
The ATSB considered the reasons for the captain’s large control input and the absent transfer of control. When the captain saw the airspeed increasing unexpectedly and approaching VMO, the captain perceived that the autopilot was not controlling the aircraft, and that an urgent intervention was necessary. The captain related this response to a reflex, impulsive response, with the implication being the action was rapid and without conscious deliberation.
It is likely that the captain’s perception of urgency affected how the captain responded to the sudden speed increase, and contributed to the captain responding rapidly, with a low level of conscious analysis. Research shows that when individuals perceive they need to respond rapidly to a situation, they tend to consider fewer options and less information (Dismukes, Goldsmith, & Kochan, 2015) and typically use rapid, associative and unconscious information processing, which is primarily influenced by pre-existing knowledge and beliefs (Klein, 2008). Research summarised by Means, Salas, Crandall and Jacobs (1993) suggests that in real-world settings, there is a speed/accuracy trade-off between rapid intuitive decisions and more time-consuming analytical decision making.
Other research describes how individuals interact with control systems changes depending on the perceived time available. According to Hollnagel (1998), where the individual perceives there is a large amount of time, he or she is able to look ahead and think about higher level goals. The individual can sample a large amount of information, and feed-forward to test the effect of actions. However, when the individual perceives he or she has little or no time, the most obvious feature of the environment and the immediate needs of the situation will dominate the choice of action. There is no planning or analysis; the individual is essentially seeing and responding.
It was evident that the captain of VUE perceived there was no time to evaluate the sudden airspeed increase and needed to respond urgently because of a perception that the autopilot was not controlling the aircraft. While an overspeed event may not be desirable, this perception to respond urgently was inconsistent with the documentation provided by the manufacturer and the operator about the aircraft safety around VMO. Overall, the documentation implied that minor exceedances of VMO were not hazardous to the safety of the aircraft.
Concerns and beliefs about overspeed
The captain was highly concerned about overspeed, and this probably contributed to the captain’s assessment that the increase in airspeed towards VMO meant the aircraft was not in a controlled state, and that urgent action was necessary. The captain was mindful of avoiding overspeed during the descent and made several comments to the FO along the lines of ‘don’t overspeed’.
The captain’s concerns about avoiding overspeed were influenced by a perception that Virgin Australia (VA) were also concerned about overspeed and wanted to reduce overspeed events. The captain reported hearing rumours that other VA crews had been subject to some form of management review after experiencing overspeeds. Although VA had changed their management of overspeed events prior to the occurrence, it is unknown how flight crew understood these changes. In this event, it is possible that the captain’s concerns about overspeed were a carry-over from the operator’s previous management of overspeed events.
The captain’s concern about the increase in airspeed towards VMO was also influenced by perceptions and beliefs about the airspeed limits of the aircraft. The captain indicated not being aware that there was a margin between VMO and the requirement for a maintenance inspection at 359 kt, or that there was a margin between VMO and the structural limitations of the aircraft.
Influence of the speed trend vector
The speed trend vector is located on the same instrument display as the airspeed indicator. In this case, the FO reported observing the trend indicator moving towards the maximum operating speed (VMO). However, the trend indicator is not a recorded parameter in the flight data recorder, so the ATSB was unable to determine what the speed trend vector showed during the development of the overspeed. The captain reported not specifically looking at the speed trend vector prior to making the abrupt control input. While it is possible the captain’s perception of urgency was influenced by a high airspeed trend projection while observing the airspeed indicator, there was no direct evidence of this effect.
A previous ATSB investigation (AO-2014-032) found that in that instance, the speed trend vector probably indicated a projected speed well above VMO. The investigation found that the captain responded to the high trend airspeed indication by perceiving a need to intervene immediately and made pitch control inputs without following the normal take-over procedure.
Flight crew risk planning and descent preparation
As highlighted in this occurrence, pilots’ management of unexpected events or hazards during descent can be fraught with risk. The descent phase of flight is complex, and there are multiple considerations for the flight crew to manage. Pilots’ ability to manage threats is complicated by perceptions of urgency or threat to the aircraft. In these circumstances, pilots are more likely to use rapid, associative modes of response, rather than planned and analytical behaviours.
Explicit consideration and management of threats is likely to mitigate the known limitations of decision making in real-world settings. The value of formal threat review procedures, in which threats and their responses are deliberately considered ahead of encountering them, is that this removes the requirement to think and act in a time-pressured, tightly coupled setting. By considering potential threats at an earlier stage in flight, threat reviews also allow flight crews to make tactical adjustments, and to observe the effects. When pilots identify potential actions prior to being in a perceived emergency, they can also think through the implications of those actions as a crew. The FAA Aeronautical Decision Making (ADM) educational material provides further support for how threat identification and planning can help address some of these biases and tendencies in decision making.
In this occurrence, the flight crew did not effectively prepare for the risk of overspeed in the arrival briefing. Although the pilots identified overspeed was a potential risk during the high-speed descent, they did not discuss what the implications of an overspeed would be, or what actions they would take if speed started to increase unexpectedly. The crew did not elaborate about the risk of overspeed, apart from the captain saying ‘don’t exceed anything’. This was contrary to the intentions of the procedures, which indicated flight crews were to discuss threats and their management at the top of descent.
Other than the formal procedural control of the threat and error management review, there were other opportunities for the crew to think about the management of a potential overspeed at an earlier stage of the flight. The crew were evidently aware of the risk of overspeed throughout the descent, with the captain saying to the FO ‘don’t overspeed’ on several occasions, and the FO remarking that the autopilot was not very effective at holding the speed steady. Although the FO expressed a plan to reduce the target speed during the descent, there was no discussion of what the crew would do if that did not have the desired effect, or if the airspeed exceeded VMO.
Overall, this was a lost opportunity for the flight crew to effectively manage the risk of overspeed. The pilots were in a position where they had time and space to think about a potential overspeed as a crew. At the top of descent, the pilots could consider the tolerances of the aircraft to airspeed exceedances, and how they could respond safely given the high-energy state of the aircraft.
However, as the aircraft continued the descent and operated close to VMO, the time available to the flight crew reduced. When the captain saw the airspeed suddenly increase, the captain perceived the crew were in a position where there was no time to discuss the situation with the FO, to think about the implications of the overspeed, or to consider the consequences of the pull-back control action. In this way, the absence of planning at an earlier stage in the descent affected how the captain managed the risk of overspeed during the occurrence and increased the risk of unsafe intervention.
Unsecured cabin crew
Seatbelts are a very effective defence against injuries during events where cabin occupants are affected by upset forces. Analysis by the FAA shows that from 1980-2003, there were only four cases of serious injuries on United States carriers during turbulence accidents where the injured person was seated with seatbelts fastened.[12] Conversely, the FAA says that around 58 people are injured each year by turbulence while not wearing seatbelts. Consequently, procedures that require the use of seatbelts, and other methods to secure cabin occupants, are the primary means of preventing injuries during these types of events. The cabin crew were not secured prior to the sudden change in pitch attitude, which increased the likelihood of injuries.
There is a regulatory requirement for cabin crew and passengers to be seated with seatbelts fastened in turbulent conditions,[13] and procedures required the pilots to brief the cabin crew about expected turbulence during both the pre-flight and top of descent briefings. However, neither of the briefings included the forecast clear air turbulence.
Cabin crew briefings are important defences for the safe preparation of the cabin, to mitigate the risk of injury. The cabin crew do not have access to meteorological information or other indications about what is likely to happen in the descent, and therefore their ability to adequately prepare for turbulence is dependent on the information provided by the pilots. When cabin crew are adequately briefed, they can modify their duties and take other steps, such as ensuring they are seated as early as possible. Because the cabin crew were not aware of the forecast clear air turbulence, they had no ability to modify their procedures.
The ATSB considered the influence of the briefings on the injuries sustained by the cabin crew. Although the flight crew reported that they were aware of forecast moderate clear air turbulence during the descent, they perceived the conditions as smooth, and noted that there had been no returns on the aircraft weather radar. Based on the information available to him, the captain did not perceive that a turbulence encounter was likely. The injury to the cabin crew was not caused by a clear air turbulence encounter. Therefore, although the absence of briefing information about the forecast clear air turbulence was not helpful for the ability of the cabin crew to prepare for descent, this did not contribute to the injuries sustained in the accident.
During this occurrence, the ‘cabin crew prepare for landing’ announcement was made about 7 minutes before the sudden changes in pitch attitude, and the fasten seat belt signs had not been turned on. This meant that, based on normal procedures, there was no requirement or expectation from the cabin crew that they should be seated.
Delayed removal of injured cabin crew from aircraft
Defences that assist in the recovery from incidents and accidents form part of the overall safety systems for planned operations into aerodromes. For accidents involving injuries to aircraft occupants, an effective safety system should include the ability to extract casualties from aircraft. Although the use of the slide sheet was not typical, there was no evidence of any safety issues posed by this method. However, the ATSB did consider that the time taken to extract the cabin crew as indicative of a delayed response to the accident. After the arrival of VUE at Adelaide, it took over 90 minutes for the injured cabin crew to be removed from the aircraft and taken to hospital.
The communication between the crew, VA, Airport Rescue and Firefighting (ARFF) and SA Ambulance Service (SAAS) was generally effective and emergency services were notified promptly after the accident. The SAAS crew did not utilise the emergency gate to access the aircraft, because they were directed to the main terminal by ARFF. While the ARFF were at the gate when VUE arrived, the SAAS arrived shortly after. However, there was no evidence that the non-use of the emergency gate affected the timing of the response. As such, the delays associated with removing the injured cabin crew member from the aircraft were related to the on-board co-ordination of the extraction.
The main factor that complicated the extraction of the injured cabin crew was the decision by the VA ground operations supervisor to deny the request to use the catering truck. The ARFF utilise the available resources dependent on the needs of a situation, and the attending firefighters had experience using catering truck vehicles in situations like the occurrence. The ARFF had a reasonable expectation that a catering truck would be made available to them upon request.
The ground operations supervisor performs a defined role within the overall context of the normal airline operations, and the ground operations supervisor’s decision making authority is typically constrained to this role. It is not typical for the ground operations supervisor to make decisions or accept perceived risks relating to departures from procedures. In this context, it is understandable that the ground operations supervisor would be hesitant to grant permission to use equipment owned and operated by another company, which they had no experience using, and which they perceived involved a risk of injury.
On this occasion, the decision making about utilising the catering truck could have been supported by guidance from more senior personnel within VA operations, such as the flight crew. However, the flight crew did not enter the cabin after the aircraft landed, and the ground operations supervisor did not perceive there to be a need to seek their advice, as the ground operations supervisor considered the cabin crew’s condition was being managed by the ambulance officers.
Additionally, within the context of an emergency response, control agencies have a responsibility to exercise authority to task and direct individuals. There must be absolute clarity over who has control of an incident response, and the requirement of other personnel to follow directions. The Adelaide Airport Aerodrome Emergency Plan identified the SAAS as the control authority for a medical emergency. However, ambulance personnel are not likely to have extensive experience in working in and around aircraft, or to be familiar with the aerodrome emergency plans. Ambulance personnel will probably rely on the advice of ARFF and other aviation personnel to identify suitable and available equipment.
The ATSB considers that the overall response by attending personnel, including the response to the request for use of the catering truck, was indicative of a lack of clarity of control responsibility. Agencies involved in the aerodrome safety system at Adelaide Airport may consider additional methods to ensure a shared understanding of the structure of control and authority in medical emergencies.
With the ARFF and ambulance personnel on site, it is likely that the extraction of the injured cabin crew could have been escalated if there was a critical need. While the delayed extraction did not increase safety risk in this instance, the ATSB considers there are opportunities to improve how airside personnel work with emergency services.
__________
From the evidence available, the following findings are made with respect to the overspeed and cabin crew injury involving Boeing 737, VH-VUE, 42 NM east-south-east of Adelaide Airport, South Australia, on 13 September 2017. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
- During a high-speed descent, a sudden decrease in tailwind associated with windshear caused airspeed to approach and exceed the aircraft maximum operating speed (VMO). The flight crew did not apply speed brakes to arrest the speed increase.
- In response to the airspeed rapidly increasing towards VMO, the captain (pilot monitoring) perceived a need to immediately intervene and made pitch control inputs without following the normal take-over procedure and alerting the first officer (pilot flying).
- The magnitude of the captain's control input was probably greater than intended. This was influenced by a perception that the autopilot was not controlling the aircraft, so an urgent intervention was required. The magnitude of the control input caused sudden pitch changes, resulting in the injuries to the cabin crew.
- Although the flight crew identified the risk of overspeed during the high-speed descent into Adelaide, they did not consider steps for mitigating that risk, or how they would manage an overspeed during the descent. This reduced the likelihood of the crew effectively responding to the unexpected increase in airspeed.
Other findings
- Although the weather forecast included moderate clear air turbulence and the aircraft was making a high-speed descent, the pilots perceived that flying conditions were smooth and elected not to activate the fasten seat belt sign. The cabin crew briefings did not mention the forecast clear air turbulence. The cabin crew were not secured prior to the sudden pitch changes, which increased the likelihood of injuries.
- The ground handling supervisor assessed there was a significant fall from height risk associated with the unsecured use of the catering truck. For that reason, the ground handling supervisor did not agree to the emergency services request to use that equipment to remove the injured cabin crew.
Additional safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
The captain and the first officer (FO) of VH-VUE both underwent training and assessment after the accident. This included a review of the flight data from the accident flight, the autopilot management and other recovery techniques during that flight, as well as the correct recovery actions from an overspeed. Both pilots were assessed as having demonstrated a competent standard during these reviews.
Virgin Australia (VA) have provided pilots with additional training and information about overspeed, overspeed prevention and overspeed recovery:
- In 2018, VA pilots were shown animations demonstrating mishandled and correct overspeed recoveries. VA will also include the accident occurrence as part of future non-technical skills training for pilots and cabin crew.
- The Flight Crew Information Manual was updated to include a section on ‘Managing VMO/MMO Exceedances’. This section stated that aircraft have been tested beyond VMO/MMO, and that these speeds include a margin below the speeds that require maintenance action or threaten the structure of the aircraft. The manual also stated that it is acceptable to refuse an ATC instruction to perform a high-speed descent. The manual identified that disengaging the autopilot to respond to an overspeed may result in abrupt pitch change.
- A Flight Crew Information Bulleting (FCIB) was sent to VA 737 pilots identifying that there had been many instances where pilots had manually intervened to respond to an overspeed or possible overspeed, and that several of these events had resulted in serious injuries. The FCIB provided information to pilots including that VMO/MMO are not never exceed speeds, and that it is acceptable to refuse an instruction to conduct a high-speed descent. The FCIB emphasised that it is preferable to accept a temporary overspeed than to make large abrupt control inputs.
- An email was sent to all VA 737 flight crew, reiterating much of the information covered in the other material. This email also identified the actions pilots should apply if they allowed the autopilot to recover the overspeed, but perceived speed continue to increase or that the autopilot was not handing the situation. These procedures were to hold the control wheel and ensure there is no back pressure being applied to the controls, disengage the autopilot, then slowly raise the nose of the aircraft.
Virgin Australia have updated materials provided to ground handling staff and other personnel working airside. The updated procedures say that in situations where emergency services are in attendance, VA team members should follow reasonable directions from those agencies. Where VA team members are in doubt, the updated procedures say they should liaise with the captain, on-board cabin crew leader or airport manager, as applicable.
To respond to the perceptions within the pilot group and to further educate flight crew about management of flight safety events and the how the flight data analysis program (FDAP) worked, VA pilots undertook non-technical skills training on the FDAP during 2018/19, and senior members of the VA flight operations and safety team conducted roadshows on the management of safety events during the same period.
Sources of information
The sources of information during the investigation included:
- Interviews with personnel including the flight crew and members of the cabin crew
- Recorded information from on-board recorders
- Meteorological information from the day of the accident
- Records from emergency services operators
- Manuals and other documentation related to flight crew, cabin crew and ground crew procedures
- Expert analysis provided by the aircraft manufacturer.
References
Campbell, N. (2012), The answer is blowin’ in the wind” The use of recorded FDR wind data in investigations. International Society of Air Safety Investigators conference 2012. Retrieved from www.asasi.org
www.asasi.org/papers/2012/The Use of Recorded FDR Wind Data in Investigations - Neil Campbell.pdf
Dismukes, R. K., Goldsmith, T. E., & Kochan, J. A. (2015). Effects of Acute Stress on Aircrew Performance: Literature Review and Analysis of Operational Aspects. Moffett Field, CA: National Aeronautics and Space Administration.
Hollnagel, E. (1998). Context, cognition, and control. In Y. Waern, Co-operation in process management - Cognition and information technology. London: Taylor and Francis.
Klein, G. (2008). Naturalistic decision making. Human Factors, 50(3), 456-460.
Means, B., Salas, E., Crandall, B., & Jacobs, T. O. (1993). Training decision makers for the real world. In G. Klein, J. Orasanu, R. Calderwood, & C. E. Zsambok, Decision making in action: Models and methods (pp. 305-326). Norwood, NJ: Ablex.
Reason, J. (1990). Human Error. Cambridge: Cambridge University Press.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to Virgin Australia, Boeing, Airservices Australia, Adelaide Airport, SA Ambulance Service, the Civil Aviation Safety Authority, the captain, the first officer, the cabin crew on board VH-VUE, and the Virgin Australia ground supervisor.
Submissions were received from Virgin Australia, Boeing, the cabin supervisor and the cabin crewmember who sustained the broken leg. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendix A – DRINA NINE ALPHA STAR
Figure A: DRINA NINE ALPHA STAR

Source: Airservices Australia
Appendix B – Flight data recorder data
Figure 11: Selected parameters during descent

Source: ATSB
Appendix C – Significant weather chart
Figure C: Significant weather chart for Australia, FL 100-250. This chart was valid 0600 UTC and used for operations three hours either side of that time. The red line shows the flight planned route of VH-VUE. A body of clear air turbulence is indicated by the long-dash line, and affects the planned route, to the west of the 140° meridian of longitude.

Source: Virgin Australia, originally produced by Bureau of Meteorology
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2020
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |