
What happened
On the 18 July 2017, Pilatus PC‑12, registered VH-FDJ departed Alice Springs, Northern Territory for Adelaide, South Australia, on a routine single-pilot aeromedical patient transfer flight. During the approach into Adelaide, the pilot noted that the aircraft’s autopilot system failed to intercept the localiser for the Adelaide runway 23 instrument landing system (ILS) approach.
Unaware of why the autopilot did not intercept the localiser, the pilot then became focussed on determining the cause of the autopilot tracking issue while attempting to re-establish the aircraft back on the ILS to continue the approach. The pilot reported this resulted in high workload that was further increased by the tracking information displayed on the aircraft’s course deviation indicator not reflecting the position information being communicated by ATC.
The pilot continued the approach and commenced further descent after observing that the aircraft was close to becoming established on the localiser and that the glideslope was becoming active. Soon after, ATC notified the pilot that the aircraft was below the minimum permitted altitude for the aircraft’s position and instructed the pilot to climb the aircraft to a safe altitude. The pilot then conducted another ILS approach and landed.
What the ATSB found
The unexpected failure of the autoflight system to intercept and track the localiser resulted in the aircraft deviating from the surveyed instrument approach path and significantly increased the pilot’s workload.
The pilot’s focus on resolving the aircraft's lateral tracking and perceived autoflight issues during the localiser intercept decreased his attention on managing the aircraft’s approach profile. That led to the aircraft descending off-track below the minimum safe altitude.
Detection of the off‑track descent and subsequent intervention by the air traffic controller restored safe operation.
What's been done as a result
Following this incident, the operator amended their descent, arrival, and approach procedures, and training and checking procedures to be more prescriptive. In addition, the operator introduced dual global positioning systems, with moving map and chart overlay displays into their legacy aircraft, to improve pilot situation awareness.
Safety message
Adequate approach preparation, and management of aircraft flight profile and automation is vital to ensure pilots maintain manageable workloads and positional awareness during an approach. Additionally, pilots should not hesitate to conduct a go-around or a missed approach should the functionality of the aircraft’s automation, or the validity of positional information, be in doubt.
On the 18 July 2017 a Pilatus PC12, registered VH-FDJ, departed Alice Springs, Northern Territory, for a routine single-pilot aeromedical patient transfer flight to Adelaide, South Australia. The departure from Alice Springs and subsequent en-route phase of the flight was reported by the pilot to have proceeded normally.
Recorded data indicated that the aircraft reached the pilot’s calculated descent point from a cruise altitude of FL 250,[1] at about 42 NM (78 km) to the north-west of Adelaide Airport.
Before descending, the pilot reported that he obtained the available weather for Adelaide Airport and prepared the aircraft’s autoflight system for the arrival. This included programming the standard arrival route (STAR)[2] and instrument landing system (ILS)[3] approach frequency. The pilot also reported reviewing the respective arrival and approach charts displayed on the electronic flight bag screen.
At about 1240 Central Standard Time,[4] the aircraft left FL 250 to commence the Salty 1 STAR (Figure 1) and subsequently the runway 23[5] ILS. The pilot reported that as he was unfamiliar with the Salty 1 STAR, he elected to utilise the aircraft’s autoflight system and the Garmin 430 avionics system for navigation and descent.
Figure 1: Extract from the Adelaide Standard Instrument Arrival
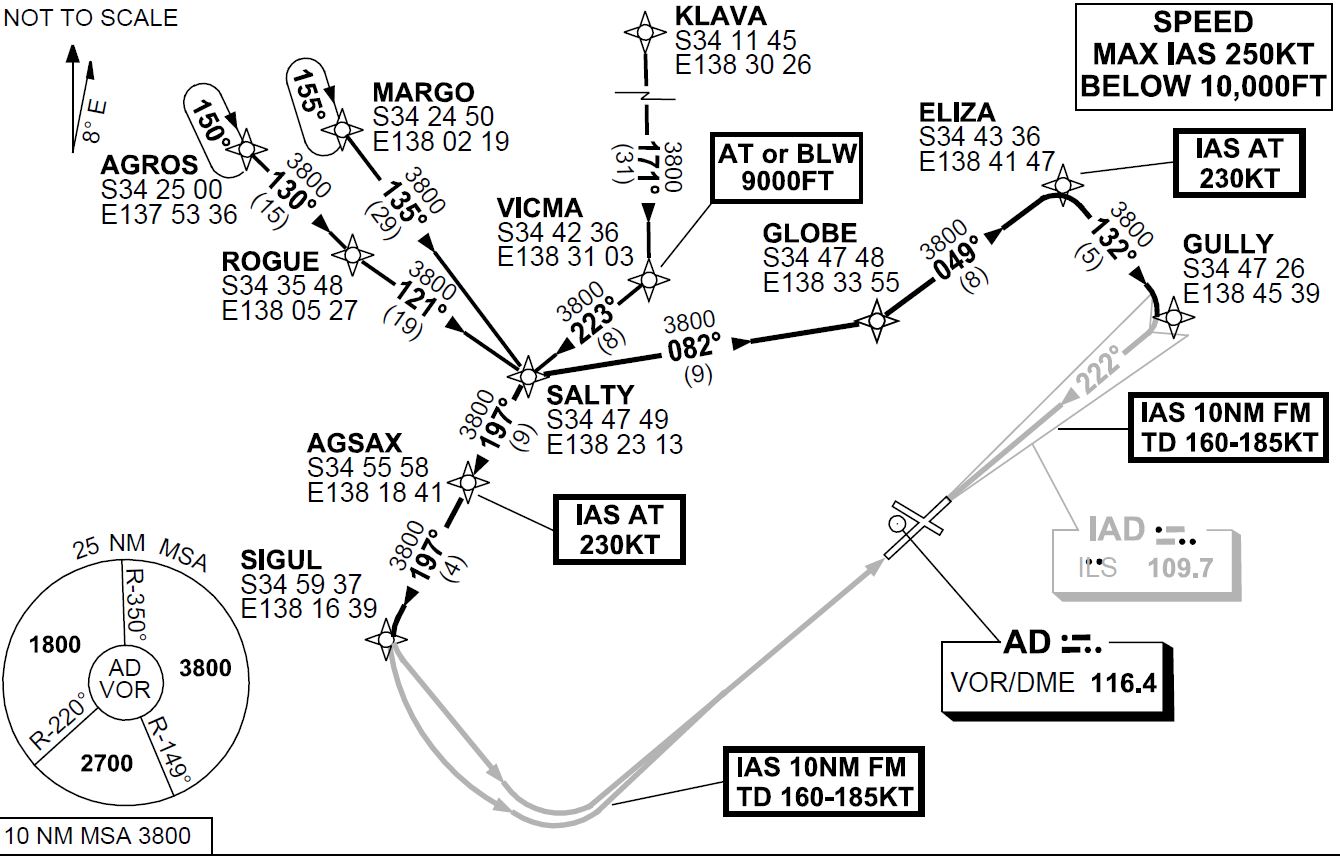
Source: Airservices Australia modified by the Australian Transport Safety Bureau
The pilot reported that, during the descent, he noted a higher-than-normal groundspeed due to the strong westerly tailwind, however this decreased as the approach progressed to lower altitudes. As the aircraft approached the GLOBE waypoint, the pilot crosschecked the aircraft’s profile using the global positioning system (GPS) unit’s calculated profile. Noting that the aircraft was slightly high at that position, the pilot increased the selected descent rate on the autoflight system.
Just after passing the ELIZA waypoint and prior to turning inbound to intercept the localiser at GULLY, the pilot changed the primary navigation source from GPS navigation mode to a heading mode. This autoflight mode change was required to enable the pilot to set the inbound course for the ILS, to facilitate an intercept of the localiser for the runway 23 ILS approach. The pilot then recalled changing the autoflight system back to navigation mode to continue navigation to the waypoint GULLY and armed the approach mode for the ILS intercept. The estimated time available to complete these tasks was less than two minutes.
The pilot reported that the aircraft overshot the required intercept at GULLY. In response, he manipulated the autoflight system by turning the aircraft in the control wheel steering mode in an attempt to re-capture the localiser. At about that time, air traffic control (ATC) advised the pilot that the aircraft had flown through the localiser, ATC issued altitude and heading instructions to assist with a re-intercept. The pilot reported that this required him to cancel the current autoflight selections, including approach mode, to enable a heading to be selected and flown. The workload at this time was reported by the pilot to have been high as he attempted to determine the functionality of the aircraft’s autoflight and navigation systems.
Soon after, ATC gave the pilot radar information that positioned the aircraft left of the localiser. A clearance to conduct the ILS approach was then communicated, with a further request for the pilot to confirm when he was established on the approach. The pilot recalled that at that time he was still trying to determine the issues with the autoflight system and why the course deviation indicator (CDI) was giving conflicting information, indicating the aircraft was slightly right of the localiser. There was no recorded communication from the pilot reporting that the aircraft was established on the approach.
While trying to re-establish the aircraft on the localiser, the pilot observed the glideslope becoming active. As he believed that the aircraft was close to intercepting the inbound track, the descent was continued.
Recorded information confirmed that a short time later, ATC issued an altitude alert to the pilot to check his altitude. This was followed with instructions to climb to a new cleared altitude, to maintain the required terrain clearance, and to fly a different heading in anticipation of conducting another ILS approach.
The pilot reported that he followed the ATC issued radar vectors back to the commencement of the runway 23 ILS approach, where an intercept of the localiser using the autoflight system was made. The second approach was flown without issue.
Pilot information
The pilot was appropriately qualified for the flight, holding a Commercial Pilot Licence (Aeroplane). He also held an instrument rating for both multi-engine and single-engine aeroplanes. The pilot’s logbook recorded a total aeronautical experience of about 6,250 hours.
The logbook indicated that the pilot had about 5,800 hours in command of single-engine aircraft, which included about 640 hours flying Pilatus PC12 (PC12) aircraft.
The pilot had reportedly used the Garmin 430 avionics system before and had previous experience flying the PC12 legacy aircraft (see the section titled Operations). The pilots training file noted the pilot appeared to have no difficulty using the Garmin 430.
The appropriate flight reviews and proficiency checks had been conducted and the pilot was deemed competent to conduct line flying operations by the operator on the 5 July 2017.
The pilot held a valid class 1 aviation medical certificate and reported that he was well-rested prior to the flight and was in good health.
Weather
The pilot reported experiencing a strong westerly tailwind of about 57 kt during the descent and that the approach was conducted in instrument meteorological conditions. However, he noted that as the aircraft descended, the wind decreased and cloud layers were observed.
During the time of the aircraft’s arrival, the trend forecast for Adelaide Airport indicated a cloud base of 1,800 ft with broken cloud at 6,200 ft and wind from 280° M at 19 kt. There were also expected periods of up to 30 minutes duration where the weather would deteriorate, with the wind at 270° M at 22 kt gusting to 38 kt and the visibility reducing to 3,000 m in showers of rain.
Operations
The operator conducted aeromedical services throughout most regions of South Australia and the Northern Territory. The Pilatus PC12 aircraft was the only aircraft type used by the operator. The operator had three variants of the PC12, namely the PC12/45, PC12/47 and PC12/47E. The older PC12/45 and PC12/47 (sometimes referred to as the ‘legacy’) had different avionics and operating characteristics to the newer PC12/47E (referred to as the ‘NG’).
The operator had a valid Air Operator’s Certificate that enabled the use of PC12 aircraft in the charter and aerial work categories, which included the conduct of ambulance functions. The operator also had approval to conduct training and proficiency checks in accordance with the Civil Aviation Safety Regulations 1998.
The operator’s PC12 flight training manual provided basic reference material that related to initial pilot training. The flight training manual included an outline of the training syllabus, checklists and some lesson plans to assist the instructor with training preparation. The flight training manual did not provide any guidance to pilots as to the procedures and operational considerations while flying the PC12.
The flying operations manual outlined the standard operating procedures (SOPs) for a descent and approach. It included that:
At an appropriate time, the pilot is to review the intended approach procedure, including where applicable:
a. instrument or visual approach,
b. airfield information from ERSA, Jeppesen or OPS28 Airfield Register,
c. If an instrument approach procedure is required:
- correct chart, aids and frequencies,
- airfield elevation and MSA [minimum sector altitude],
- initial approach altitude and entry procedure,
- approach procedure,
- visual procedure - restrictions, runway, aircraft configuration, and
- missed approach procedure.
Checklists used by pilots during flight listed that an ‘approach review’ was to be completed before transition. It was reported by the operator that in the case of longer flights, such as Alice Springs to Adelaide, an approach review and flight instrument setup actions should be completed before commencing the descent.
There was no guidance for pilots as to the operator’s expected flight instrument settings for the arrival. However, the operations manual highlighted the importance of pre-arrival planning and flight instrument set-up during the approach/landing phase. It included procedures for the conduct of a non-precision approach (other than area navigation[6]), area navigation approach and precision approach. There was no guidance to pilots as to when an approach review/brief and flight instrument setup should occur.
The operators expected instrument setup for VH-FDJ (FDJ) differed from other PC12 aircraft in the operator’s fleet due to variation in FDJ’s avionics. The operations manual required that specific familiarisation training was required for pilots flying VH-FDJ due to the differences with all other aircraft in the fleet. The pilot had conducted in-flight training in FDJ prior to the incident.
It was reported by the operator that a pilot flying FDJ should ensure that the inbound course was set on the CDI prior to commencing the STAR. This would alleviate the requirement to change between navigation modes once the STAR had commenced. It would also reduce pilot workload during the descent and arrival.
Training
The operator conducted ground theory training, endorsements, and line training for pilots flying the PC12 variants. The PC12 fleet comprised nine of the newer (NG) type aircraft fitted with ‘glass cockpit’ avionics, and eight older (legacy) type aircraft, with different avionics and operating characteristics. Training provided pilots with familiarity of both types. The occurrence pilot had significant previous experience on the legacy PC12 so the major component of his in command under supervision (ICUS) training concentrated on the NG variant.
The operator’s flight training records identified that the pilot had successfully completed all components of the operators training syllabus. However, notes made during the training identified that the pilot had difficulty at times with profile management, and approach preparation. These issues were not apparent during the pilot’s final flight check for commencement of line operations.
The pilot completed about 96 hours of in-flight training before being approved to conduct line flying operations on the 5 July 2017. The training consisted of 28 training flights, which included 24 flights with the newer PC12 NG variant and four flights with the PC12 legacy aircraft.
Following this occurrence, the pilot completed six remedial flights, two of which were in legacy aircraft. Those flights identified that the pilot required additional training with approach preparation. This included conducting more thorough approach briefings and ensuring that the approach checks and setup were not left too late in order to avoid high workload situations. The pilot’s training notes also emphasised the importance of conducting a go-around if the approach became unstable. At the end of this training the pilot was re‑checked and resumed line flying operations.
Related occurrences
A database search identified a number of occurrences with aircraft descending below the minimum safe altitude. The occurrences have primarily involved aircraft on approach to land. They include situations where pilot(s) attention has been on other tasks during higher workload phases of flight, such as during the later stages of an instrument approach. The ATSB has published the following related safety investigation reports.
AO-2015-018: Flight path management and descent toward the lower limit of controlled airspace involving Airbus A320, VH-VND, on approach to Melbourne Airport, Victoria, on 11 February 2015
On 11 February 2015, an Airbus A320 aircraft, registered VH‑VND and operated by Tiger Airways, was conducting a scheduled passenger service from Hobart Airport, Tasmania to Melbourne Airport, Victoria.
At about 1750 Eastern Daylight-saving Time, about 9 NM (17 km) north of Melbourne Airport, and after the flight crew had been cleared by air traffic control to conduct a visual approach, the aircraft descended below the minimum safe altitude, though the aircraft remained in controlled airspace.
During the descent, both flight crew became preoccupied with other tasks inside the flight deck, which had the effect of increasing their workload and distracting them from monitoring the aircraft’s flight path and altitude. About two minutes after commencing descent on the visual approach, the flight crew levelled the aircraft after realising that it appeared to be low on profile. A safety alert issued by air traffic control soon followed and in response, the aircraft was climbed to intercept the recommended visual approach descent profile. The remainder of the flight was uneventful and the aircraft landed on runway 16 at Melbourne Airport.
AO-2016-012: Descent below segment minimum safe altitude during a non-precision instrument approach involving Airbus A320, PK-AXY, 17 km WSW Perth Airport, Western Australia on 19 February 2016
On the evening of 19 February 2016, an Airbus A320 aircraft, registered PK-AXY and operated by PT Indonesia AirAsia was on a scheduled passenger service from Denpasar, Indonesia to Perth, Australia. During cruise, the captain’s flight management and guidance computer (FMGC1) failed. Due to the failure, the flight crew elected to use the first officer’s duplicate systems. For the aircraft’s arrival in Perth there was moderate to severe turbulence forecast below 3,000 ft with reports of windshear. The crew commenced an ILS approach to runway 21.
During the approach, the flight crew made a number of flight mode changes and autopilot selections, normal for an ILS approach with all aircraft operating systems available. However, some of those flight modes and autopilot selections relied on data from the failed FMGC1 and the auto-thrust system commanded increased engine thrust. The crew did not expect this engine response and elected to conduct a go-around. With an increasing crosswind on runway 21, the crew accepted a change of runway, to conduct a non-precision instrument approach to runway 06.
With the time available, the first officer programmed the new approach into his FMGC and conducted the approach briefing. During this period, the captain hand flew the aircraft and manually controlled the thrust. During the approach to runway 06, the crew descended the aircraft earlier than normal, but believed that they were on the correct flight path profile.
While descending, both flight crew became concerned that they could not visually identify the runway, and focused their attention outside the aircraft. At about that time, the approach controller received a ‘below minimum safe altitude’ warning for the aircraft. The controller alerted the crew of their low altitude and instructed them to conduct a go-around. The crew then conducted another approach to runway 06 and landed.
__________
- Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 370 equates to 37,000 ft.
- Standard Instrument Arrival (STAR): A designated IFR arrival route linking a significant point, normally on an air traffic services route, with a point from which a published instrument approach procedure can be commenced.
- Instrument Landing System (ILS): A precision instrument approach system which normally consists of the following electronic components: VHF Localiser, UHF Glideslope and VHF Marker Beacons.
- Central Standard Time (CST): Coordinated Universal Time (UTC) + 9.5 hours.
- Runway number: the number represents the magnetic heading of the runway.
- Area navigation (RNAV): A method of navigation which permits aircraft operation on any desired flight path within the coverage of ground or spacebased navigation aids, or within the limits of the capability of selfcontained aids, or a combination of these.
Approach preparation and management
A number of factors lead to the pilot not being fully prepared for the arrival and subsequent instrument landing system (ILS) approach to Adelaide Airport. Although the importance of early preparation and maintenance of an appropriate flight path profile was reinforced during the pilot’s line training, the impact of not fully configuring the aircraft’s instrumentation earlier in the approach was likely not recognised by the pilot. This, combined with the effect of a tailwind during the approach, reduced the available time for the pilot prepare for the localiser intercept.
While it could not be determined why the aircraft’s autoflight system did not capture and track the localiser, it was possible that a late setup of the inbound course and arming of the approach provided insufficient time for the autopilot to turn the aircraft. From the available evidence it was likely that the pilot had less than two minutes to setup the instrumentation, arm the approach and prepare for the intercept.
It is possible that during preparation for the approach, the pilot incorrectly set the reciprocal of the inbound course on the aircraft’s course deviation indicator (CDI), resulting in displayed tracking indications that were not in the command sense. That would account for the difference between the aircraft’s position, relative to the localiser, displayed to the pilot compared to that advised by air traffic control. That discrepancy created confusion over the aircraft’s actual position and, in combination with the unexpected overshoot of the localiser, significantly increased the pilot’s workload in managing the ILS approach.
The pilot became focussed on resolving the aircraft's lateral tracking and perceived autoflight issues during the localiser intercept. His recollection of being aware that the aircraft was descending but unaware of its specific altitude was consistent with decreased attention on managing the aircraft’s approach profile. That led to the aircraft descending off-track below the minimum safe altitude until identified and remedied by the positive actions of the controller.
Pilot workload
When the aircraft did not automatically intercept the localiser as expected the pilot’s workload started to increase.
Workload has been defined by Orlady & Orlady (1999) as ’reflecting the interaction between a specific individual and the demands imposed by a particular task. Workload represents the cost incurred by the human operator in achieving a particular level of performance’.
Each individual has a finite set of mental resources which allow them to process information and identify appropriate tasks. The set is a variable trait, and will vary with many factors including the experience, training, recency and familiarity with a situation, stress and fatigue. Harris (2011) stated ’High workload is associated with increased error rates (and hence an associated decrease in safety margins) as well as having the effect of reducing overall productivity and increasing occupational stress’.
When the workload gets too high for the available set of resources, an individual will start to task shed, initially systematically and eventually indiscriminately as the workload continues to increase. Green et al. (1996) identified, ‘as the demands of the task, or the workload, are increased, the standard of our performance is achieved. Any increase in workload after this point leads to an overall degradation in performance. At extremely high levels of workload (overload), important information may be missed due to the narrowing or focussing of attention onto only one aspect of the task.’
The United Kingdom Civil Aviation Authority publication CAP 737 (2016) states workload ‘is linked to almost all other areas within cognition and performance, particularly attention, vigilance, fatigue, skills, and multi-tasking.’
Approach and landing is a well-known period of high workload for pilots. In this occurrence, the following factors had the potential to increase the pilot’s workload:
- an increased ground speed
- limited recent experience with the autoflight system fitted to this aircraft type
- the high intrinsic workload of single-pilot IFR flight
- restrictions of the single-channel autoflight system in setting up the ILS instrumentation.
While the pilot had the correct intentions for the approach, once the error arose with the aircraft tracking, the pilot became unable to effectively monitor the approach while troubleshooting the situation. Following the intervention of air traffic control, the situation was resolved and the second approach was flown without issue.
Training
The pilot’s initial training with the operator appeared to address identified approach management issues by the time he was cleared to conduct line flying operations. Recognising that subsequent remedial training identified the need for closer study and briefing of instrument approaches, it is difficult to ascertain if more approach consolidation conducted prior to the incident would have prevented it.
Despite profile management and approach preparation being reinforced during the pilot’s training, the standard operating procedures outlined in the company operations manual did not give guidance to pilots as to when and how the aircraft was expected to be configured for the approach. Although an approach review was required, information pertaining to the expected cockpit and approach setup may have benefited the occurrence pilot. More generally, the absence of such guidance increases the likelihood of greater variation in how approaches are conducted.
From the evidence available, the following findings are made with respect to flight below the minimum permitted altitude involving Pilatus PC-12, registered VH-FDJ, that occurred about 19 km north‑east of Adelaide Airport, South Australia on 18 July 2017. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
- The unexpected failure of the autoflight system to intercept and track the localiser resulted in the aircraft deviating from the surveyed instrument approach path and significantly increased the pilot’s workload.
- The pilot’s focus on resolving the aircraft's lateral tracking and perceived autoflight issues during the localiser intercept decreased his attention on managing the aircraft’s approach profile. That led to the aircraft descending off-track below the minimum safe altitude.
Other factors that increased risk
- The pilot did not initiate a missed approach despite being uncertain of the displayed navigation system information and aircraft position. This limited the opportunity for the pilot to resolve any perceived navigation issues at a safe altitude and in a more controlled environment.
- Approach guidance in the operations manual did not include detail of the expected cockpit and approach setup preparation. That increased the risk that variation in the conduct of approaches may be introduced into operations.
Other findings
- Detection and intervention by the air traffic controller following the off‑track descent below the minimum permitted altitude restored safe operation.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Royal Flying Doctor Service Central Operations
Since this occurrence, the operator has implemented the following improvements:
- amended the descent, arrival and approach procedures to include more prescriptive requirements
- upgraded the legacy fleet to include dual global positioning system equipment with moving map and chart overlay displays to improve pilot situation awareness
- rewritten the Training and Checking manual to include more prescriptive training
- strengthened the Safety Management System, including the introduction of a phased implementation of a change management program
- changed the initial pilot training, which is now conducted by their recently approved Part 141 organisation.
Sources of information
The sources of information during the investigation included:
- Airservices Australia
- Civil Aviation Safety Authority
- FlightAware
- the flight crew and operator.
References
Civil Aviation Authority, 2016, CAP737 – Flight-crew human factors handbook, Civil Aviation Authority, United Kingdom.
Green RG, Muir H, James M, Gradwell, D, Green RL (1996) Human Factors For Pilots, Second Edition, Ashgate, England.
Harris, D (2011) Human Performance on the Flight Deck, Ashgate, England.
Orlady H & Orlady LM (1999) Human Factors in Multi-Crew Flight Operations, Ashgate, England.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to Airservices Australia, the flight crew, the operator and the Civil Aviation Safety Authority.
A submission was received from the operator. The submission was reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2018
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |