
Safety summary
What happened
At 0400 on 28 February 2015, a harbour pilot boarded the container ship Maersk Garonne for its passage into Fremantle’s Inner Harbour. The pilotage generally progressed as intended by the pilot until the ship approached the entrance channel 40 minutes later. At this stage, he became concerned that the assisting harbour tugs would not be at the channel’s entrance before the ship.
At 0442¾, the pilot decided to delay entering the channel by taking Maersk Garonne outside (south of) the channel and entering it later. At 0448, the ship grounded in charted shallow water. The ship did not suffer any damage and was re-floated on the rising tide about 3½ hours later.
What the ATSB found
The ATSB investigation found that bridge resource management was not effectively implemented on board Maersk Garonne. As a result, the ship’s bridge team was not fully engaged in the pilotage and did not effectively monitor the ship’s passage. While the master retained responsibility for safe navigation of the ship, the harbour pilot was the only person actively focused on the pilotage. Consequently, single-person errors that occurred went undetected or inadequately challenged and uncorrected.
The investigation identified that Fremantle Pilots’ publicly available passage planning guidance for the pilotage was inadequate and was not effectively implemented. Further, Fremantle Pilots’ pilotage procedures did not include abort points or contingency plans for identified risks.
The investigation also found that procedures for tugs to be on station at the entrance to the port, or for their co-ordinated movement, were not clearly defined.
What has been done
Fremantle Pilots, the port’s pilotage provider, has reviewed and updated its website, procedures and training with respect to pilotage, passage planning and communications. This includes simulator training for emergencies.
Svitzer Australia, the towage provider, has updated its procedures to include defined on-station times for tugs.
Fremantle Ports, the port authority, has advised that it has clarified the role of the vessel traffic service in assisting ship arrivals and berthing.
The safety actions noted above, together with joint simulator exercises, clarify the roles and responsibilities of all parties with respect to monitoring and management of pilotages. This increases safety margins and reduces the likelihood of a similar incident in the future.
Maersk Garonne’s managers have issued fleet circulars to emphasise and clarify the roles and responsibilities of the master and ship’s crew during navigation with a pilot on board. The managers have also implemented a fleet-wide program that includes education and auditing to ensure compliance with bridge procedures.
Safety message
Comprehensive passage planning that includes risk-assessed contingency planning is vital to safe pilotage and underpins effective bridge resource management. The potentially severe consequences of a pilotage accident means that a low accident rate in the past is not a reliable indicator of safety risk.
During the early hours of 28 February 2015, the 292 m, 4,318 TEU,[1] fully cellular container ship Maersk Garonne (Figure 1) arrived off the Port of Fremantle, Western Australia, after a voyage from Singapore. At 0200,[2] the master arrived on the ship’s navigation bridge (bridge) and at 0300, he took over the conduct (con) of the ship as it approached the Fremantle outer pilot boarding ground. The second mate, who was the officer of the watch (OOW), remained on the bridge to assist the master when required.
Figure 1: Maersk Garonne aground and being assisted by tugs

Source: Tristan Yuswak
Just before 0400, the 4-8 third mate[3] came to the bridge and took over the watch from the second mate. The master directed him to go on deck to escort the pilot to the bridge. By 0403, the harbour pilot and an observer[4] had boarded Maersk Garonne.
At 0400, the weather was fine and clear with the wind from the south-southeast at 9 knots.[5] The forecast was for winds of 15-20 knots from the southeast. Low water was at 0352 (0.51 m) with high water expected at 1849 (0.97 m).
At 0406, the pilot and observer arrived on the bridge. The master and pilot exchanged information and discussed the pilotage at the chart table, over the navigational chart. The pilot was informed that the main engine was at half ahead, the engine had been tested astern, the ship was on hand steering and that all equipment was working as expected. The thrusters were being tested at that time. Maersk Garonne’s draught was 12.2 m forward and 12.4 m aft.
The pilot ordered full ahead and altered the ship’s heading[6] towards the Approach Channel. The master positioned himself behind the engine telegraph in preparation for engine orders and the OOW, the third mate, was at the chart table plotting positions as the transit progressed.
At 0407, the pilot made VHF radio contact with the Port of Fremantle[7] and advised the duty vessel traffic service officer (VTSO) that Maersk Garonne was approaching the Fairway Landfall buoy. The route for the ship into the port via the Deepwater Channel (DWC) was confirmed, and that there was no outbound traffic. The pilot and master then continued discussing the pilotage, including the information provided on Fremantle Pilots’ ‘master/pilot exchange of information’ (MPX) form and the ship’s pilot card. This included the pilot’s intended track from the pilot boarding ground to the berth, where to expect the tugs, tide and weather conditions and berthing arrangements.
By 0410, conversations on the bridge included some social topics. The pilot and observer were engaged in varied discussions when the pilot was not giving helm orders.
Figure 2: Section of navigational chart Aus 112 showing Maersk Garonne’s track

Source: Australian Hydrographic Service (annotated by ATSB)
At 0413, the ship passed the Fairway Landfall buoy (Figure 2) and continued in a south-easterly direction at 14 knots,[8] toward the DWC, about 3 miles[9] off. At 0422, the pilot ordered 10° of starboard rudder and at 0426, a heading of 178°.
At 0430, Maersk Garonne exited the DWC, at a speed of about 16 knots. The pilot then ordered a heading of 170° towards the port entrance channel, about 3½ miles further south. Between helm orders, the bridge conversations continued on marine and social topics, mostly between the pilot and the observer.
At about this time, the chief mate arrived on the bridge to relieve the third mate as OOW for the arrival. They discussed the situation and exchanged watch information.
At 0435, the pilot contacted VTS and reported that the ship was passing Hall Bank (Figure 2). He also confirmed the ship’s berthing arrangements (port side alongside at berth 8). The VTSO replied that Maersk Garonne was all clear to enter the Inner Harbour and that the tugs were ‘getting underway’. Both tugs had been berthed close to each other at the C Shed wharf, about 1½ miles from the entrance channel entrance (one of them, Svitzer Falcon, had departed the wharf by 0433).
At 0435½, the pilot ordered a heading of 165° and 2 minutes later, the main engine was reduced to half ahead.
At 0436, after the third mate had plotted the position on the chart, the chief mate took over the watch. The third mate then left the bridge to stand by at the forward mooring station.
Table 1: Selected ship data leading up to the grounding
| Local time | Heading (True) | Speed (Knots) | Main engine status | Rudder (degrees) | Turn rate (⁰/min to Port) |
| 04:35:00 | 170 | 16.7 | Full ahead | - | - |
| 04:37:32 | 166 | 16.3 | Half ahead | - | - |
| 04:41:07 | 166 | 14.5 | Slow ahead | Port 20 | 0 |
| 04:41:36 | 159 | 14.2 | Slow ahead | Hard to Port | 20 |
| 04:42:58 | 123 | 10.9 | Slow ahead | Midships | 25 |
| 04:44:29 | 102 | 9.2 | Slow ahead | Stbd 10 | 14 |
| 04:44:59 | 099 | 8.9 | Slow ahead | Midships | 9 |
| 04:45:23 | 098 | 8.8 | Slow ahead | Port 20 | 7 |
| 04:45:35 | 098 | 8.7 | Slow ahead | Hard to Port | 11 |
| 04:46:48 | 082 | 7.9 | Half ahead | Hard to Port | 18 |
| 04:47:07 | 079 | 7.4 | Half ahead | Hard to Port | 16 |
| 04:48:00 | 071 | 2.1 | Half ahead | Hard to Port | 12 |
| 04:48:27 | 070 | 0.2 | Stop | Hard to Port | 0 |
Source: Maersk Garonne’s voyage data recorder
At 0437, the pilot attempted to establish contact with the two tugs assigned to the ship. A response was received immediately from Svitzer Falcon. The pilot advised its master of the intended berthing arrangements and to make fast on the starboard shoulder.[10]
At 0440, the Svitzer Falcon’s master advised the pilot that the other tug, Svitzer Eagle, was letting go his lines. The pilot said he would keep going and then advised Svitzer Falcon to make fast off the starboard quarter. Shortly after, Svitzer Eagle’s master called and the pilot advised him to make fast on the starboard shoulder. The pilot did not know that Svitzer Eagle had not left the wharf.
At 0441, the pilot ordered 20° of port rudder and slow ahead on the main engine to commence the turn to the entrance channel (Figure 3). Thirty seconds later, he ordered hard to port to slow the ship for entry into the channel.
At 0442¾, the pilot advised Svitzer Falcon’s master of his intentions and said that he was '…just going to go south of that first green buoy there…just want to wash a bit more speed off, so I'm just going to keep that one to port, then I'll come in between the two greens’. The ‘first green buoy’ was the starboard hand buoy No. 1 and the other ‘green’ was beacon No. 2 (Figure 3 insert). After communicating this intention of taking the ship south of the entrance channel and entering it later, the pilot advised Svitzer Falcon's master to pass down the ship’s port side.
At 0443, with Maersk Garonne’s speed at 10.9 knots and the ship turning at 25° per minute to port, the pilot ordered midships rudder. The master immediately queried the pilot. The pilot responded that he was ‘…just going to go south of this first green buoy captain, just come in…from that direction’ as he had ‘to kill a little bit of time for the second tug’ because ‘the second tug is running a little bit late.’ The master acknowledged his understanding, and that there was ‘no problem.’ At this time, Svitzer Falcon was to the south of the starboard hand buoy No. 1. Meanwhile, Svitzer Eagle was just leaving the wharf.
At 0444½, as the ship bore down on buoy No. 1, the pilot ordered 10° of starboard rudder. The ship’s speed was now 9.2 knots and its turn rate had reduced to 14° per minute. The ship was on a heading of 102° and its bridge was positioned approximately in the middle of the entrance channel (Figure 3). Svitzer Eagle was now off the wharf and visible to the pilot about 1½ miles distant.
Soon after, the chief mate queried the pilot as the starboard hand buoy No. 1 was on the port bow. The pilot advised him that the ship would pass to starboard of the buoy. The chief mate then alerted him to the shallow water ahead.
At 0445, the pilot, also aware of the shoal ahead, ordered midships rudder and, in quick succession, port 20° and hard to port.
Figure 3: Section of navigational chart Aus 113 showing Maersk Garonne’s track from 0440 at one-minute intervals (inset shows the grounded ship and the tugs at 0448½)
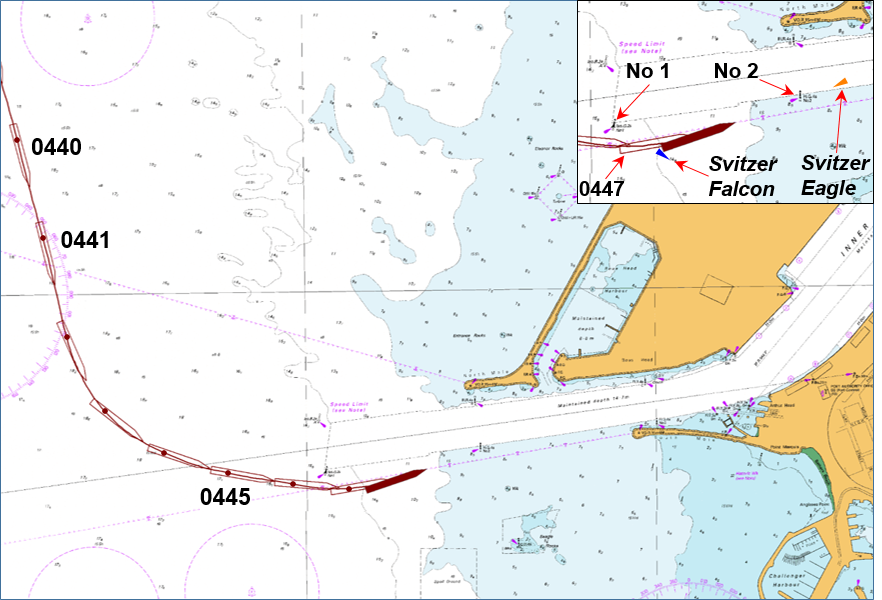
Source: Australian Hydrographic Service (annotated by ATSB)
At 0446¾, as the ship passed buoy No. 1 (abeam of the ship’s bridge), the pilot ordered half ahead on the main engine in an attempt to turn more quickly to port and enter the channel. He also said aloud that the ship ‘could be in a spot of bother here’. The ship was approximately parallel to the entrance channel, still turning to port and its speed was 7.9 knots.
At 0447¼, the master informed the pilot that the echo sounder was showing a depth of 1 m under the keel. The pilot noted the depth and ordered the bow thruster full power to port. Maersk Garonne’s speed was 7.4 knots and over the following 70 seconds the ship slowed and came to a gentle stop as its hull rode up onto the sand and mud bottom to the south of the entrance channel. At 0448¼, the chief mate stated that the ship had no speed, and shortly thereafter, the pilot ordered the main engine to stop. Svitzer Eagle was then about 2 cables[11] from the ship’s bow.
Subsequently, the pilot made a number of unsuccessful attempts to re-float the ship using its main engine, bow and stern thrusters and the tugs. At 0502, he informed the VTSO that the ship had grounded. He requested an additional tug and a relief pilot.
At 0542, the relief pilot boarded the ship. The original pilot remained on board to assist. By this time, the ship’s crew had inspected the cargo holds and sounded the tanks and depths surrounding the ship. The damage assessments did not indicate a breach in the ship’s hull.
Over the following hours, 900 m³ of water ballast was discharged from the forward tanks to reduce the forward draught to assist re-floating. Two additional tugs also arrived to assist.
By 0824, Maersk Garonne was re-floated using its main engine and thrusters with the four tugs assisting. The VTSO then directed that the ship be moved to and anchored in Gage Roads to await hull inspections and investigations.
On the following morning, 1 March, divers conducted an underwater hull inspection. No breaches were found and damage was limited to minor paint scraping.
Main engine trials were completed satisfactorily in the afternoon and the ship was safely berthed in Fremantle that evening.
At 1100 on 3 March, after completing its cargo operations, Maersk Garonne departed Fremantle.
__________
- Twenty-foot Equivalent Unit, a standard shipping container. The nominal size of a ship in TEU refers to the number of standard containers that it can carry.
- All times referred to in this report are local time, Coordinated Universal Time (UTC) + 8 hours.
- Maersk Garonne carried two third mates, one keeping the 4-8 watch and the other the 8-12 watch.
- A navigational student accompanied the harbour pilot on an observation trip.
- One knot, or one nautical mile per hour, equals 1.852 kilometres per hour.
- All ship’s headings in this report are in degrees by gyro compass with negligible error.
- Fremantle Port Authority operates a 24 hour Vessel Traffic Service (VTS), the call sign for which is ‘Port of Fremantle’.
- All ship speeds referred to in this report are ‘made good/over the ground’.
- A nautical mile of 1,852 metres.
- A shoulder is the area where a ship’s hull form changes from the bow shape to the parallel mid body.
- One cable equals one tenth of a nautical mile or 185.2 m.
Maersk Garonne
At the time of the incident Maersk Garonne was registered in Denmark and classed with Bureau Veritas. The ship was owned and managed by Maersk.[12] It was on a regular service between ports in Asia and Australia and frequently called at Fremantle.
Maersk Garonne was fitted with navigational equipment required for a ship of its size under SOLAS.[13] The navigation equipment included an electronic chart display and information system (ECDIS) and two radars, which both had automatic radar plotting aid (ARPA) and other target tracking functions. Both radars had data inputs from the ship’s automatic identification system (AIS) transceiver and global positioning system (GPS) receiver unit.
The ship had a multi-national, mostly Filipino, crew of 18. This included four mates with an additional third mate on board to assist in maintaining the rest hour requirements of the STCW Code.[14]
The master had 39 years at sea and held a Romanian master mariner’s certificate of competency. He had sailed as master for 14 years and been with Maersk for the last 7 years. It was his first assignment on Maersk Garonne and he had joined about 2 months before the incident.
The chief mate held a Philippines master mariner’s certificate of competency, first obtained in 2007. He had been at sea for 16 years, all on container ships. He had sailed as chief mate for 7 years and been with Maersk for the previous 5 years. It was his first time on Maersk Garonne and he had joined about 7 weeks before the incident. The chief mate did not keep watches at sea.
The helmsman at the time of the incident was an able seaman with 28 years of seagoing experience, 22 of which had been on container ships. He had been with Maersk for 15 years. His routine duties on many ships had included those as a helmsman. He had joined Maersk Garonne 2 weeks before the grounding.
Port of Fremantle
The Port of Fremantle is Western Australia’s principal national and international sea gateway for container and general cargo trades.[15] Fremantle is a sheltered, all-weather port situated on the west coast about 20 km from the State capital, Perth.
The port operates from two locations: the Inner Harbour is located at the entrance to the Swan River and the Outer Harbour is about 20 km to the south at Kwinana-Cockburn Sound. The port had 2,277 ship visits in the 2013-14 financial year and handled more than 700,000 TEU.[16]
The Fremantle Port Authority operating under the name Fremantle Ports is the port’s strategic manager. Fremantle Ports publishes, and makes available online,[17] a Port Information Guide, which provides relevant port and related information for port users. The information includes details for communications, pilotage, arrival and departure requirements, port navigation, security and safety.
Pilotage in the Port of Fremantle is compulsory for ships over 150 GT,[18] unless the master holds a pilotage exemption certificate, and any ship so directed by the harbour master. Pilotage services are provided by Fremantle Pilots.
Fremantle Pilots
Fremantle Pilots (FP) is a privately owned company[19] that provides contracted pilotage services within the Port of Fremantle and to the ports of Albany and Bunbury as required. Fremantle Pilots provides service to more than 5,100 vessel movements annually. Pilot bookings are managed through the Port of Fremantle via the vessel’s contracted shipping agent.
All pilots undertake continuous professional development including bridge resource management (BRM) and related training, manned model and ship simulator ship-handling training, including contingency planning for emergencies.
The pilot assigned to Maersk Garonne on 28 February held an unrestricted licence as a port pilot issued by Fremantle Ports and a master mariner’s certificate of competency issued by the Australian Maritime Safety Authority (AMSA). He had 15 years of pilotage experience in various Australian ports and had worked for FP since 2004.
Passage plan
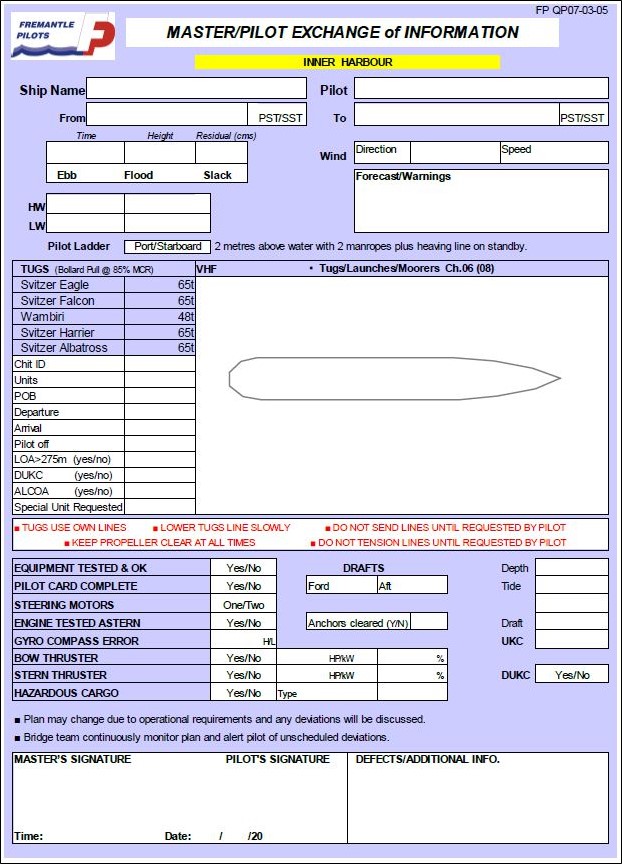
Fremantle Pilots provides information on its website[20] for ships’ masters relevant to arrival in Fremantle. This includes a master - pilot exchange of information (MPX) form (Appendix A) and waypoint lists to ‘assist vessel masters with preparing their passage plan’. The company also stated that ‘a detailed plan for the proposed passage is a requirement’ and that passage planning was through the master - pilot exchange. The MPX form was based upon IMO principles to assist:
- gathering all information relevant to the contemplated voyage or passage
- detailed planning of the whole voyage or passage from berth to berth…
- execution of the plan; and monitoring the progress of the vessel in the implementation of the plan.
The information stated that the ‘role of our Pilot is to create a shared mental model of the plan and establish themselves within the bridge team utilising proper bridge resource management (BRM) practices.’ The information also cautioned that ‘waypoints lists are typical arrivals and departures (courses) and any variations will (be) discussed by the Pilot with the Master and bridge team accordingly.’
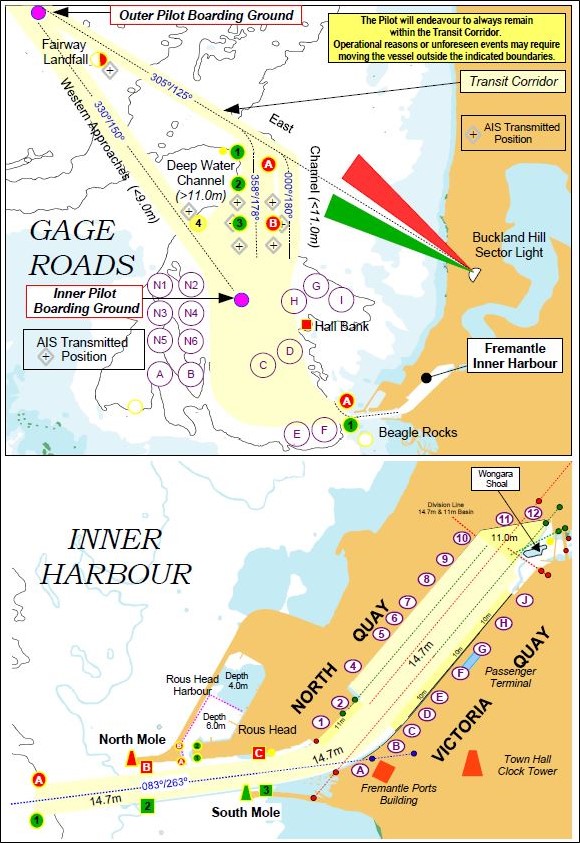
The inbound track, described by the arrival waypoint list, from the outer boarding ground to the Inner Harbour, is shown in green in Figures 5 and 6.
Portable pilotage unit
Fremantle Pilots issues its pilots with portable pilotage units (PPU). A PPU is an aid to pilotage operations with the intent to improve safety and efficiency of the operation. Its primary use is to provide independent, accurate GPS position, course and speed information. A PPU also provides other information such as charts, passage plan and AIS information. All pilots are trained in the use of the equipment and FP requires a PPU to be used for all pilotages from the outer boarding ground to Gage Roads.
Fremantle Pilots’ Procedures and Guidelines[21] stated that the PPU is to ‘provide additional information to assist the pilot’s assessment and decision making processes, and should be used in conjunction with all means available to the pilot.’ It is, however, ‘…not to be used as the sole means of assessing situational awareness’ and was not ‘to interfere with the comprehensive process required of the Master/Pilot exchange of information.’
Towage
The towage requirements for a ship entering the Port of Fremantle are set by the harbour master and outlined in the Port Information Guide. Towage requirements for ships over 275 m in length are assessed on a case by case basis. The ship’s agent orders the tugs through Fremantle Ports with a minimum of 2 hours’ notice required for the tugs to be on station.
For entry into the Inner Harbour, FP’s procedures require assisting tugs to be on station near the entrance buoys ‘A’ and ‘1’ before the ship’s arrival.
The pilot may make contact with the tugs to confirm they are in position, before arrival at the entrance buoys. The procedures stated that no ship is to enter the Inner Harbour without the assigned tug/s in attendance. The accepted practice was that the tugs be in position and/or made fast before the ship entered the entrance channel. Any tug delays were to be relayed to the pilot, who would determine if an adjustment in speed or course is necessary and/or to abort the approach.
Safe navigation
The Bridge Procedures Guide[22] states that safe navigation of a ship requires that it not be exposed to unnecessary danger and that at all times it can be controlled within acceptable margins. This requires effective command, control, communication and management of the ship.
A key accepted and practised principle of safely navigating a ship is bridge resource management (BRM). Passage planning is central to BRM. Regulation, training, guidelines, and multiple procedures apply to these concepts and enshrine them and their usage in the maritime industry.
Bridge resource management
Bridge resource management (BRM) is defined as the use and coordination of all the skills and resources (people, procedures and equipment) available to the entire bridge team to achieve the established goal of optimum safety and efficiency.[23] All individuals make errors, and BRM aims to minimise the occurrence and outcome of errors through the best possible use of resources.
All ship’s navigators must have training, and demonstrate competence, in BRM techniques.[24]
In areas of increased risk to safe navigation, a pilot is often added to the ship’s navigation team. The pilot’s local knowledge and practised piloting techniques are intended to, and should, reduce risks to an acceptable level.
The ship’s master and the pilot are responsible for taking steps to actively engage and include other members of the ship’s bridge team in the pilotage. Through effective BRM, all personnel involved in the navigation of the ship should have a clear understanding of, and expectations for, the pilotage. However, where marine casualties have occurred with a pilot on board, many have been attributed to flawed master - pilot relationships. In many cases, when the pilot boarded the ship, the master and deck officers ceased to monitor navigation and the position of the ship.
Bridge resource management is a broad topic which covers many inter-related subjects, including but not limited to:
- shared mental model
- situational awareness
- error management
- contingency planning
- challenge and response
- distractions and interruptions.
Safety management systems
The organisations responsible for ensuring Maersk Garonne was safely navigated into the Port of Fremantle included Maersk (the ship’s managers), Fremantle Pilots and Fremantle Ports. Each organisation had a safety management system (SMS), training and processes aimed at achieving that objective.
Each SMS included sections relating to BRM and passage planning and the master - pilot exchange of information (MPX).
Passage planning
Passage planning is necessary to allow the entire bridge team to arrive at a shared understanding of what ‘should’ happen during the passage and thus ensure the ship can be safely navigated between ports from berth to berth. The margins of safety in restricted coastal waters can be critical, limiting the time available to take corrective action when required. Careful passage planning is used to make a pilotage passage safer, for example, by setting limits that make unsafe deviations from the plan readily apparent.
The ship’s master is required to develop a plan for its safe and efficient passage between ports.[25] Detailed plans are needed to ensure appropriate margins of safety are maintained at all times.
The International Maritime Organization (IMO) provides guidelines[26] for voyage planning, which comprises four distinct stages:
- appraisal during which all information relevant to the passage is considered
- planning when a detailed plan for the voyage is prepared
- execution of the plan, including suitable alterations to the passage plan as required by circumstances
- monitoring the execution of the plan including ensuring all navigators know and understand it.
Section 2.6 of the Bridge Procedures Guide, states:
Of particular importance is the need to monitor the position of the ship approaching the wheel over position at the end of the track, and checking that the ship is safely on the new track after alteration of course.
Pilotage
A ship is exposed to higher risks in pilotage areas because of the reduced margins of safety due to factors which often include reduced depth and width of fairways, increased traffic, tidal variations and stronger currents. The pilot, as the port’s primary risk mitigation tool for the pilotage area, provides skills and local area knowledge - valuable additions to the bridge team’s resources.
However, a pilot is not a replacement for any of the ship’s bridge team members. The master and the ship’s bridge team are always responsible for its safe navigation, even when navigating with a pilot.[27] It is necessary, therefore, that the ship’s crew works with the pilot by observing good BRM practice in executing the agreed passage plan. This approach helps all to work together to ensure that errors are detected early and corrected before the ship is put into any danger.
Master - pilot exchange
The master - pilot information exchange (MPX) is the first opportunity for the pilot and master to exchange critical information to facilitate a safe and effective pilotage. In effect, it is the meeting in which the pilot and the master agree on a common passage plan. Alterations are made as required to decide how the pilotage will be done jointly. The MPX aims to ensure that the ship’s bridge team and the pilot share the same understanding of, and expectations for, the pilotage. It also helps to establish appropriate working relationships with defined roles and responsibilities.
__________
- A. P. Moller-Maersk, Denmark. The ship was managed by Maersk Line Ship Management, Singapore.
- International Maritime Organisation (IMO), 1974, The International Convention for the Safety of Life at Sea, 1974, as amended (SOLAS), IMO, London.
- International Maritime Organisation (IMO) 1978, International Convention on Standards of Training Certification and Watchkeeping for Seafarers, 1978, as amended (STCW Code), IMO, London.
- Fremantle Ports, n.d., Western Gateway to World Trade, viewed 16 April 2015, <http://www.fremantleports.com.au>
- Fremantle Ports Annual Report 2014.
- www.fremantleports.com.au
- Gross tonnage is a measurement of the enclosed internal volume of a ship and its superstructure with certain spaces exempted
- Fremantle Pilots is the registered name and call sign for the Fremantle, Kwinana and Cockburn Sound Pilots.
- www.fremantlepilots.com.au
- Fremantle Pilots has a documented system for pilotage activities associated with the safe navigation and effective transit and berthing of vessels within the Port of Fremantle. Part of this suite is its safety management system incorporating Pilotage Operations – Procedures and Guidelines.
- International Chamber of Shipping (ICS) 2007, Bridge Procedures Guide, 4th edn, Marisec Publications, London.
- Nijjer, R 2000 Bridge Resource Management: The Missing Link, Sea Australia 2000, Sydney.
- International Maritime Organisation (IMO) 1978, International Convention on Standards of Training Certification and Watchkeeping for Seafarers, 1978, as amended (STCW Code), Section A-II/1, Standards regarding the master and deck department, IMO, London.
- International Maritime Organisation (IMO), 1974, The International Convention for the Safety of Life at Sea, 1974, as amended (SOLAS 1974), Chapter V, regulation 34 Safe navigation and avoidance of dangerous situations, IMO, London.
- International Maritime Organisation (IMO) 2004, Resolution A.893(21) Guidelines for voyage planning, IMO, London.
- Australian Maritime Safety Authority 2014, Marine Notice 17/2014 Sound navigational practices, AMSA, Canberra.
The grounding
At 0400 on 28 February 2015, a harbour pilot boarded Maersk Garonne for its passage into Fremantle. The master informed him that the ship’s equipment and machinery were in working order. In turn, the pilot briefed the master and marked his intended course on the diagram in the master - pilot exchange (MPX) form. The ship’s officer of the watch (OOW) and helmsman were also on the bridge.
Over the next 35 minutes, the pilotage generally progressed as intended by the pilot. However, as the ship exited the Deepwater Channel (DWC), the pilot conducted the ship to the east of both the planned track on the ship’s chart and his own intended track on the MPX form. At no stage did the ship’s bridge team members challenge the pilot regarding this deviation from the plan.
Figure 4: Sections of navigational chart Aus 113 showing the progress of Maersk Garonne and the tugs from 0441
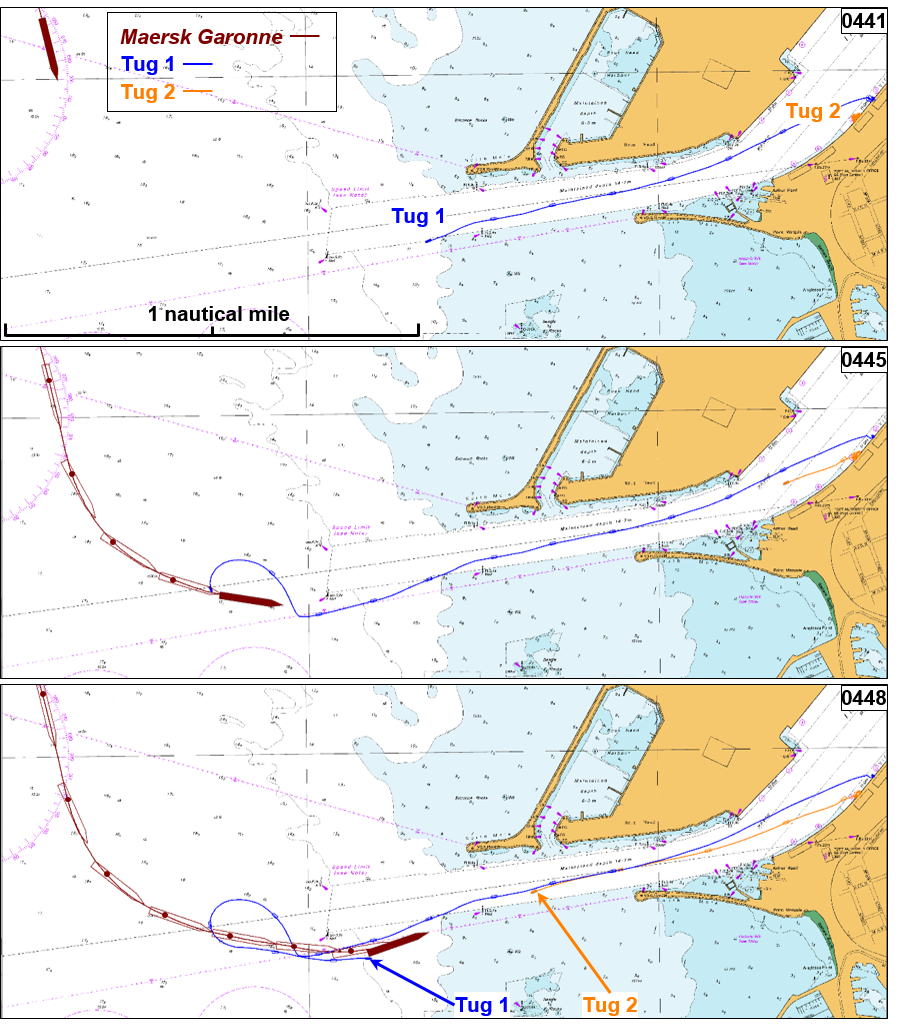
Source: Australian Hydrographic Service (annotated by ATSB)
Then, as the ship approached the entrance channel, the pilot became concerned that it would arrive there before the two harbour tugs were in position. After some radio communications with one of the tug masters, the pilot decided to delay the ship’s entry into the channel.
At 0443, the pilot began manoeuvring Maersk Garonne to delay entering the channel (Figure 4). He intended to do so by taking the ship outside, and south of, the channel and then enter between the starboard hand buoy No. 1 and beacon No. 2. However, at 0448, while it was still outside the channel, the ship grounded in an area of charted shallow water.
Execution of the pilotage
Master - pilot exchange
The Fremantle Pilots’ (FP) passage planning for inbound ships, utilised a MPX form based on the IMO’s recommended operational procedures[28] for maritime pilots. This form contained harbour and towage information, transit corridor and channel chartlets and checklist prompts for items of discussion (see Appendix A).
Further, FP’s procedures and guidelines stated:
It should be further noted that the Master/Pilot Information Exchange form does not fulfil the purpose of a passage plan and is used only as a means of effectively exchanging information between the Pilot and the Master to facilitate a safe and effective pilotage operation.
For the arrival of Maersk Garonne, the MPX took place immediately after the pilot arrived on the bridge. This was normal practice, and bridge audio recordings show that the principal information exchange took place before the ship passed the Fairway Landfall buoy. During this discussion, brief mention was made of intended tracks by indicating that the transit would be via the DWC, and that tugs were expected just outside the entrance channel.
However, several items were not discussed, at any stage during this time, or the remainder of the pilotage, including:
- ship’s speeds
- planned track details, such as true courses, course alterations, wheel over positions, cross-track error limits and main engine/speed requirements/changes
- contingency plans and/or abort points
- communication with VTS and tugs.
After the MPX was completed, the master did not update the OOW with the information exchanged, including the pilot’s intended track, which was different to that marked on the ship’s chart. Further, no designated roles and responsibilities in support of the pilot were assigned to the ship’s bridge team members. Such duties may have encouraged them to become more actively engaged in the pilotage. Consequently, members of the ship’s bridge team remained unaware of important details of the pilotage passage that were essential to safe navigation.
Passage planning
The passage plan for a pilotage forms the basis on which all bridge team members involved build their understanding of what the pilotage will involve. This model should then be shared between all personnel involved in the navigation of the ship into port.
Fremantle Pilots required a passage plan to be prepared for any, and all, pilotages. Its procedures and guidelines stated:
An essential part of the Pilot's passage plan is the laying down of courses between the point of origin and proposed destination.
Once on board the vessel, the Pilot, in consultation with the Master and his bridge team, will complete the plan making alterations as required.
Maersk Garonne’s master’s passage plan included the pilotage into Fremantle’s Inner Harbour. The ship’s SMS procedures required specific items to be marked on the chart, including:
- parallel indexing
- methods and frequency of position fixing
- clearing lines and bearings
- safe speed and necessary speed alterations
- changes in machinery status
- contingency plans
- abort positions.
However, only the safe speed and speed alterations were included in the passage plan, and only the planned track was marked on the chart. This suggests that the ship’s bridge team members expected the pilot to provide much of the missing information.
Planned courses
There were three possible intended tracks for Maersk Garonne's pilotage into the Port of Fremantle on 28 February (shown in different colours in Figure 5):
- derived from FP’s published waypoint list (green)
- Maersk Garonne’s passage plan marked on the ship’s chart (blue)
- pilot’s intended track marked on the MPX form (black).
None of these tracks was followed - the ship actually followed the track shown in red. Further, the three different, possible intended tracks meant that the ship’s bridge team members did not have the same understanding as the pilot of the track he intended to follow.
Awareness and understanding of the plan
At no stage was either OOW briefed on the key details discussed during the MPX. Therefore, the OOWs were unaware that the courses marked on the ship’s chart were not to be followed. Further, the pilot did not inform the ship’s master or bridge team members that he intended to conduct the ship to the east of the marked courses and the hand drawn track on the MPX form.
As a result, the ship’s bridge team members were unable to develop and maintain a shared understanding and mental model of the plan and expectations for the pilotage as it progressed. Their ability to maintain situational awareness was compromised by not knowing what the plan was. Hence, they were not actively engaged in the pilotage and were therefore unable to assist in the detection and management of errors or deviations from the plan.
Further, no opportunities to clarify the plan and then jointly execute and monitor it were taken. For example, the significant deviation from the charted course on departure from the DWC was not communicated or challenged.
Previous tracks
The ATSB investigation analysed recent inbound pilotage tracks of ships similar in size to Maersk Garonne during the 2 months preceding its grounding. The tracks of more than 40 ships greater than 250 m in length are shown below (Figure 6).
All tracks were within the approved Fremantle Ports transit corridor, however, the analysis showed that none of the tracks was consistent with FP’s published waypoint list (green line in Figure 6). The analysis also showed that Maersk Garonne’s track on 28 February was at the eastern extremity of the others. Had the ship followed the published track it would have been 6 cables further to the west. This would then have provided more time and distance for the second tug to be on station, or its position to be verified, and for the pilot to consider aborting the approach.
Figure 5: Comparison of Maersk Garonne's intended and actual tracks on 28 February
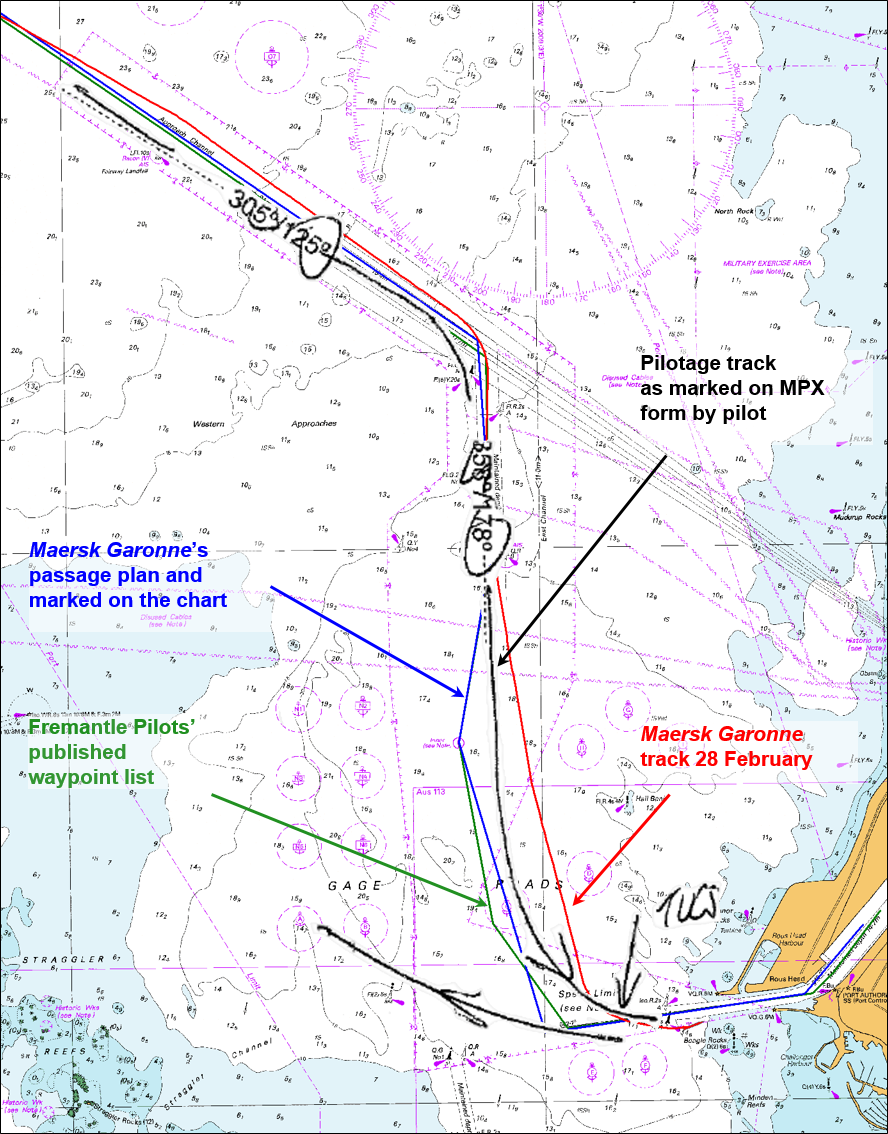
Source: Australian Hydrographic service (annotated by ATSB)
Transit speed
Fremantle Ports’ Port Information Guide states that ships transiting channels shall maintain a speed consistent with safe navigation. In addition, the port’s operational parameters stated that ships with draughts greater than 12 m should not exceed 13 knots in the DWC. However, the pilot’s MPX form did not refer to recommended speeds or speed restrictions for the transit.
Maersk Garonne’s master’s passage plan for the pilotage included maximum and minimum speeds. The maximum speed south of the DWC was 12 knots, reducing to less than 8 knots for the entrance channel.
However, Maersk Garonne transited the DWC at about 16 knots. The pilot maintained this speed until south of Hall Bank, when the main engine speed was reduced to half ahead. The ship’s speed reduced slowly until the pilot started the turn towards the entrance channel, at which time it was 14.5 knots. The pilot intended to maintain a higher speed to improve the ship’s manoeuvrability as in his experience the ship did not turn well at slow speed.
Figure 6: Inbound pilotage tracks of ships greater than 250 m in length in the 2 months preceding the grounding
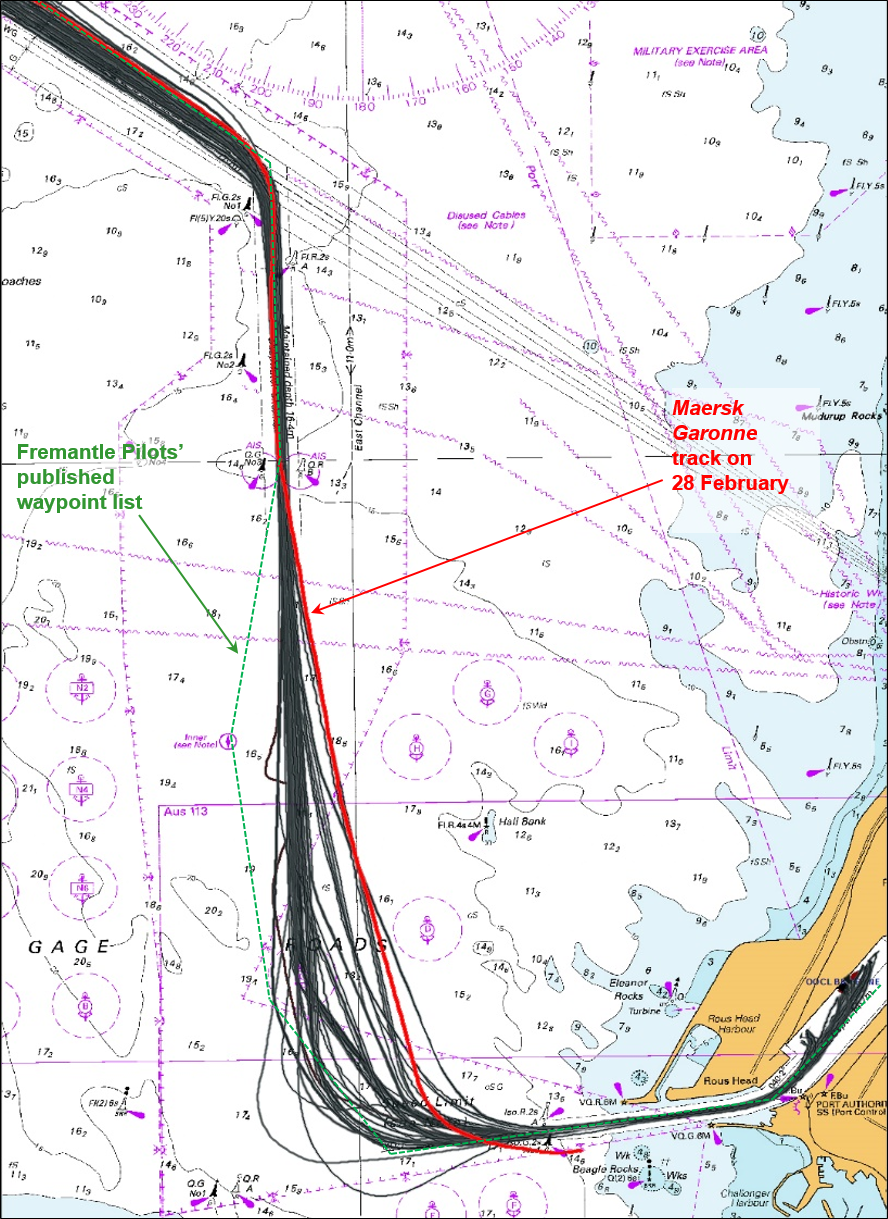
Source: Australian Hydrographic Service (annotated by ATSB)
Neither the pilot nor any of the ship’s bridge team members discussed the ship’s speed at any time. The speed was consistently above the maximums mentioned in the port’s operating parameters and Maersk Garonne’s passage plan. Had the speed been maintained within the port parameters and/or the ship’s passage plan, the ship would have arrived at the pilot’s intended position to turn towards the entrance at least 3 minutes later than it did (0441). While 3 minutes would not have ensured either of the tugs was on station on time, it would have provided more time on board the ship to detect, manage and potentially recover from the errors that occurred.
Contingency planning
Contingency planning is a risk management tool, which adds significant control to better manage emergencies. Anticipation of, and preparation for, an adverse event makes the reaction to it more effective. The reaction may then be one from a known and practised range of options, rather than an unknown, instantaneous reaction in an unexpected and stressful situation. Learning only from real emergencies is not practical and therefore should be enhanced through training, ideally simulation, in a controlled environment, especially for foreseeable risks.
The harbour pilot is the local knowledge expert and is employed to conduct the ship because of this specific knowledge. Maersk Garonne’s pilot had many years of pilotage experience, including more than 10 years in Fremantle, and was also an experienced ship’s master. He was familiar with the ship’s manoeuvring characteristics, having conducted it numerous times in or out of the port.
Maersk Garonne’s maximum draught of 12.2 m and length overall of 292 m were at the upper end of ship size/dimensions permitted in Fremantle. The ship’s manoeuvring information poster was also displayed on the bridge. At interview, the pilot stated that the size and manoeuvrability of the ship at various speeds influenced the decisions he made regarding the ship’s track and turns.
The pilot knew the information about the ship and had a comprehensive knowledge of the pilotage area. He should, therefore, have been keenly aware that the ‘no-go area’ outside the marked channel was unsuitable for a deep draught vessel. Therefore, entering the channel between starboard hand buoy No. 1 and beacon No. 2 should never have been considered a safe option.
At interview, the pilot acknowledged that he was aware that going south of the channel was not an option for the large ship. He also indicated that his plan (that is, going south of the channel) was an ‘ambitious manoeuvre’ to overcome earlier errors but he thought he would still ‘make it’. These statements support the fact that experts also make poor decisions in unexpected situations, particularly when pressed for time. They also highlight the importance of contingency planning.
Fremantle Pilots’ (FP) procedures included guidelines on the identification, assessment and management of hazards and risks. These were recorded using job hazard analysis (JHA) documents. The JHA for Inner Harbour arrival identified risks such as the tugs not standing by and ship’s system faults, and provided risk controls for such events. However, neither the JHA, nor other FP’s procedures, included any formalised contingency plans for the risks identified.
Similarly, ‘no-go areas’ and abort points should have been marked on the ship’s chart. Hence, the ship’s bridge team, especially the master, should have known that navigating outside the channel was not a safe option. However, when the pilot informed him of his intentions, the master did not have an appropriate level of situational awareness and agreed with the pilot without a challenge.
At 0441, the pilot commenced the turn toward the entrance. At 0442¾, he informed the tug master of his intention to go south of the first green buoy (the starboard hand buoy No. 1). Figure 7 shows the final stages of the grounding with an indicative turning circle, based on the ship’s manoeuvring information,[29] shown. This simple analysis shows that options, though limited, remained available to safely manoeuvre or stop the ship before it passed south of the entrance channel.
No contingency plans were recorded or discussed. Therefore, when the tugs were not on station as the pilot expected, he did not have any preplanned or practised manoeuvres to fall back on. He then had to make decisions quickly and under increasing levels of stress. This resulted in manoeuvring the deep draught ship into charted shallow waters outside the marked channel.
Figure 7: Maersk Garonne’s track with the ship’s turning circle overlaid
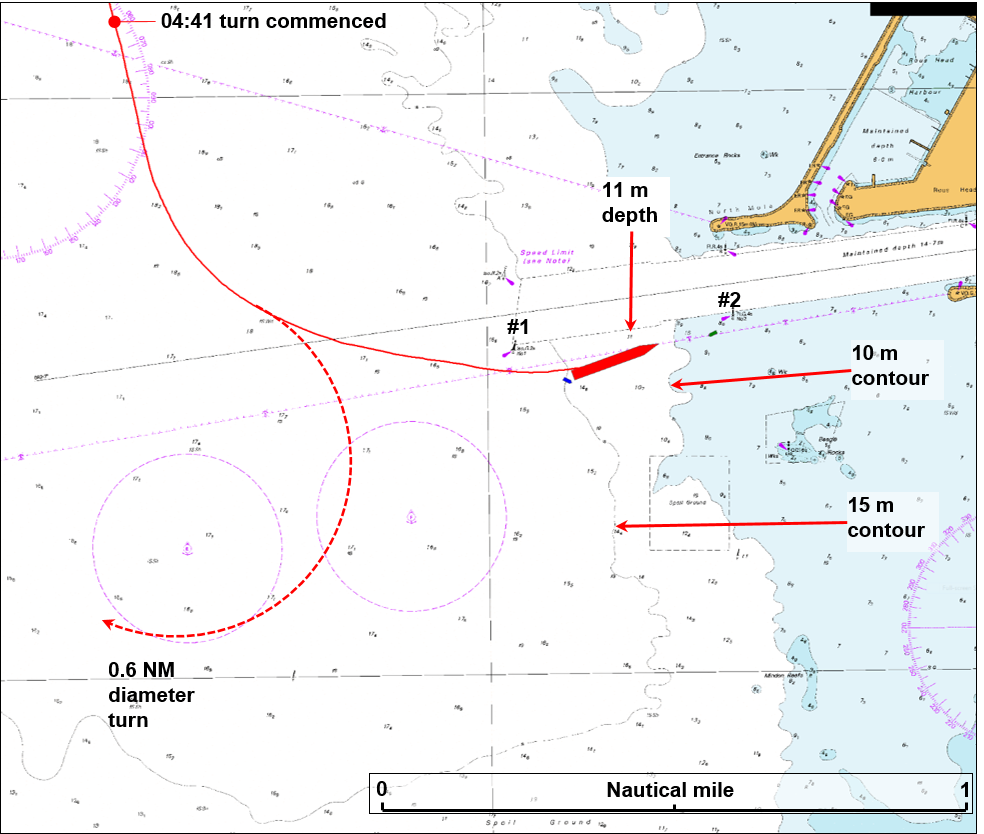
Source: Australian Hydrographic Service (annotated by ATSB)
Bridge resource management
Maersk Garonne’s safety management system contained a procedure for navigation with a pilot on board. This procedure outlined the strategies and requirements for the master and bridge team members to follow. The subjects mentioned included crewmember responsibilities, communications, master - pilot exchange, manoeuvring, the route to be followed and the passage plan. However, many of these were not followed and BRM was ineffective.
Roles and responsibilities
Safe navigation requires that all bridge team members involved are aware of their roles and responsibilities. Analysis of marine incidents by AMSA has identified that many incidents are attributed to single-person errors.[30] During pilotage, many of the navigational decisions are made by the pilot alone. Therefore, to make it more likely that single-person errors (made by the pilot) are detected early, all bridge team members must have an understanding of individual roles and responsibilities in executing the agreed plan.
The master and the ship’s bridge team are always responsible for its safe navigation, and are therefore expected to participate fully in navigation during pilotage. They must continue to monitor the safe passage of the ship and critically appraise the pilot’s advice. In order to do this, and to ensure safe and efficient navigation, they should fully support the pilot as a valuable resource and addition to the team.
On 28 February, when the pilot took the conduct of Maersk Garonne, in effect, he became the only one actively focused on the pilotage. After the initial exchange of information between the master and pilot, no tasks were assigned to, or updates provided to the bridge team. There was, then, an absence of clearly defined roles and responsibilities for team members.
Shared mental model
Each individual member of a team will develop a mental model of what they think will occur during the task being completed. Each person’s mental model is based upon the information available to them at the time. Ensuring that each member of a bridge team shares the same mental model of the passage plan is central to effective BRM.
Shared mental models serve three critical purposes: they help people to describe, explain and predict events in a common environment. Any team that must adapt quickly to changing tasks might draw on shared or common mental models for those tasks. In order to adapt effectively, team members must be able to predict what their teammates are going to do, and what they are going to need to be able to do it.[31]
At the start of the pilotage, as Maersk Garonne approached the Fairway Landfall buoy, the ship’s bridge team members shared a common mental model of the progress of the pilotage. The intended track through the DWC, marked by the pilot on the MPX form, was consistent with that on the ship’s chart as per its passage plan (Figure 5).
However, as the ship left the DWC, the pilot ordered a heading of 170°. From this point, the pilot’s intended track diverged from the ones marked on the ship’s chart and the MPX form. The ship’s bridge team members did not challenge this deviation and subsequently, no longer had a shared mental model for the pilotage.
Situational awareness
A team’s situational awareness is closely associated with the concept of shared mental model. Situational awareness has been variously defined, including simply as knowing what is going on around you. In relation to a ship’s passage, it includes knowing what has recently happened, what is happening and, based on where the ship is, what is about to happen.
Careful observation and understanding of the situation around you should achieve one of two things: it should reinforce your understanding and confidence in the mental model of the passage, or it should highlight a misunderstanding or an error and trigger actions to clarify or correct the situation.
Situational awareness is dependent on working memory and is, therefore, affected by distraction, interruption and stimulus overload. Collective (team) situational awareness can be enhanced by:
- monitoring the progress of the agreed plan
- communicating with each other about the situation to share individual awareness and discuss differences
- anticipating next conditions
- checking one another.
There were many resources available on board Maersk Garonne to assist in establishing and maintaining situational awareness. These included ship’s equipment such as the radars and the AIS receiver, as well as human resources which could be assigned to gather or verify information.
As the ship left the DWC, and navigated to the east of the ship’s passage plan track, the master and OOW progressively lost situational awareness. Their mental models of the pilotage changed and they were unable to anticipate or monitor the ship’s progress against an agreed plan. Despite this, they did not communicate with the pilot or each other to attempt to clarify the plan or the deviation from it.
There was no agreed plan, and, as a consequence, there was no shared mental model of the pilotage. The pilot was the only one who knew what his plan was. Therefore, he was the only one that was in a position to be able to maintain situational awareness.
However, the pilot did not have his personal pilotage unit (PPU), as required by FP procedures, to assist him. Before boarding the ship, he found the PPU was not charged. As there was no spare battery, he left the PPU charging. He did not consider using the ship’s power supply to charge/use the PPU.
In addition to this, while Maersk Garonne was not required to have an electronic chart display and information system (ECDIS), it was fitted with one.[32] However, the ECDIS was not operational. The master had identified this in the pre-arrival notification but Fremantle Ports did not pass this information to the pilot. Nor did the master inform the pilot of this during the MPX.
Consequently, as other position monitoring resources on board were not effectively used, and without the PPU or ECDIS to monitor the passage, the pilot believed that the ship was further to the west than it was. However, this was not the case and his decision-making was hampered. The situation was compounded when the pilot became occupied with contacting the tugs.
Error management
The detection and management of errors is a key safety aspect in the process of avoiding serious incidents. Having accepted the premise that all individuals make errors, error management then seeks to detect and control the mistakes to minimise any negative outcomes.
There are two components to error management:
- error reduction – measures designed to limit the occurrence of errors
- error containment – measures designed to limit the adverse consequences of those errors that still occur.
The capacity of a system to minimise the outcome of an error, or series of errors, is determined by the system’s margin for error. The bigger the margin for error, the greater the capacity to overcome errors. Time is a key common element in error management. The more time available to detect, assess and respond to an error, the more appropriate the response is likely to be.
On board Maersk Garonne, none of the bridge team members adequately monitored the actions of other members of the team or the ship’s progress. As a consequence, there was no effective detection and management of, or recovery from, errors which occurred, as the bridge team members did not:
- clarify and agree upon the planned or intended track
- engage all team members in the pilotage
- delegate tasks, such as ensuring the locations and movement of tugs
- ensure everyone had a common mental model of the intended passage
- challenge the deviation from the planned track
- have in place or discuss contingency plans
- use all bridge equipment to monitor the ship’s progress
- critically appraise and verify communications regarding movement of the tugs.
Hence, the margins for error eroded and this led to the ship being navigated outside the channel.
Challenge and response
Effective communication is central to bridge resource management (BRM). It is essential to prevent errors leading to undesirable outcomes. Challenge and response is a BRM technique in which a person’s perception of an error, in the execution of the plan, is confirmed or denied by asking and/or responding to questions. That is, if unsure of exactly what is occurring, a person should ask others to clarify the situation, and a response is required.
While the pilot’s plan was not communicated to the rest of the bridge team, it should have been evident to the OOW that the track marked on the ship’s chart was not being followed (when the ship exited the DWC). That neither OOW raised this important matter with the master or the pilot is indicative of the level of BRM. The OOW only challenged the pilot when the ship was outside the entrance channel and with the starboard hand buoy to port. The ship was now in a ‘no-go area’ with shallow water ahead. However, the challenge was ineffective, as it was too late.
Distractions
Interruptions or distractions during the completion of a task increase the likelihood of error. Distractions can be related to the task or from some external, unrelated source or event. An individual, or team, can also become completely occupied (fixated) with one event or task and therefore distracted from the overall objective.
Minimising possible distractions is important for effective BRM. For example, many ships, and passenger ships in particular, have a ‘red zone’ system during periods of increased risk to navigation, such as pilotages. This method restricts access and internal communication to the bridge to only those involved in navigational tasks. This reduces unnecessary and undesirable sources of distraction.
During this pilotage there were a number of distractions with attempting to establish contact with both tugs, by radio and then visually. The pilot was trying to establish whether or not the second tug would be on station before the ship arrived at the entrance channel. These distractions occupied the pilot’s attention just as the ship was approaching a period of heightened activity and manoeuvring. Throughout this period, he did not check the ship’s position by any means available and relied upon the leading lights as a transit for the wheel over point. However, the ship was much further to the east than he believed.
As the turn commenced, the pilot used the rudder hard to port to slow the ship in preparation for entering the entrance channel. He then became concerned that the tugs would not be on station as he expected so he altered his plan and decided to go south of the channel. He ordered the rudder midships to slow the rate of turn. However, he became concerned that the ship would collide with No. 1 buoy. His attention now turned to avoiding the buoy and he ordered starboard rudder to ensure the ship would pass south of it. This manoeuvre became his focus to the exclusion of other critical navigational risks.
Had the pilot had an accurate understanding and appraisal of the ship’s position and its progress during the turn, he could have manoeuvred to avoid the shallow water before becoming fixated with clearing the buoy.
Change of OOW
The need to change the OOW during a pilotage is a foreseeable risk. The change involves possible disruption to the bridge team and distraction of personnel, including the pilot. There is also the risk of loss of information during the handover, a loss of the shared mental model and loss of situational awareness.
The pilotage from the Fremantle outer pilot boarding ground to the Inner Harbour should have taken about 90 minutes. The ship’s third mate took over the 4-8 watch at 0400, and was to be at the forward mooring station for berthing shortly after 0430. Consequently, two changes of watch occurred in 30 minutes. The chief mate took over at about 0430, when the ship was passing Hall Bank. This was also at about the time the pilot became occupied with contacting the tugs and then turning the ship towards the entrance channel.
The risks associated with handing over the watch during the pilotage had not been considered and the change of OOW added unnecessary distractions.
Observers
There is the potential for additional personnel on the bridge of a ship during pilotage operations to be a distraction.[33] While the presence of observers on the bridge at such times may sometimes be acceptable, it needs to be carefully managed. For example, there is a need for observers for training purposes, of pilots and ship’s crew, and for checking or auditing purposes.
During the pilotage of Maersk Garonne, a navigational student observer was occupying some of the pilot’s time and attention. In such situations, the interaction of observers with the bridge team, and especially the pilot, needs to be controlled to prevent distraction. Bridge recordings show that the pilot and observer were engaged in conversation, interspersed with communications with the ship’s personnel, as late as 0444¾. This was during a period of heightened activity as it was when the chief mate commented that the starboard hand buoy No. 1 was off the port bow and just after the pilot had ordered 10° of starboard rudder to avoid the buoy.
The dynamic between pilot and ship’s bridge team members altered due to the presence of the observer and his interaction with the pilot.[34] Further, while this was not identified as having directly contributed to the incident, the conversation between the observer and the pilot reduced the opportunity for the ship’s crew to interact with the pilot. This factor may have affected the building of a shared mental model and maintaining situational awareness.
External resources in pilotage
Vessel traffic service
Fremantle Ports maintains a 24-hour vessel traffic service (VTS)[35] in accordance with international guidelines. As part of its function, the VTS organises and manages traffic within its VTS area, and provides essential information related to ship movements.
The duty VTS officer (VTSO) is required to maintain a continuous watch, monitoring shipping traffic and provide information to ships, pilots, tugs and other users. The VTSO also provides information about ship movements, berth allocations and other matters related to the safety of navigation and weather within port waters.
At 0435 on 28 February, the VTSO provided tug information, which was taken by the pilot as confirmation that his plan (mental model) was progressing as expected. Therefore, the pilot continued with his plan and started the turn toward the entrance channel. Had the communication between the VTSO and pilot clearly identified that both tugs had not yet departed the wharf, the pilot may have decided to alter his plan or abort the approach to the entrance channel.
Tugs and towage
Tugs are essential resources for safely berthing a ship. Therefore, clear and unambiguous plans, information and communications are required to ensure the most effective use of tugs. In this way, the tugs, their roles and expectations can be integrated into the shared mental model for the pilotage.
At 0435, the VTSO advised the pilot that the tugs were getting underway. However, only one tug had departed the wharf. About 3 minutes later, the pilot contacted the tugs. The master of the tug that was underway answered promptly and informed the pilot that the other tug was on the way. Consequently, he believed that both tugs were en route to the entrance channel buoys. Therefore, he decided to continue the pilotage but altered the positions (forward or aft) for making fast the tugs based upon their expected order of arrival.
At 0440½, the master of the tug that was still alongside the wharf contacted the pilot, just as he was starting the ship’s turn toward the entrance channel. The pilot informed him to make fast on the starboard shoulder. However, neither the fact that the tug was still alongside the wharf nor its expected time at the entrance channel buoys were discussed. It was not until 0444 that the tug departed the wharf. In the meantime, the pilot had started the turn to port and had to alter his plan after not being able to sight the tug.
Entry into the Inner Harbour required tugs to be in attendance. Fremantle Pilots’ (FP) accepted practice was for the tugs to be in position and/or made fast before the ship entered the entrance channel. As tugs being delayed was a foreseeable risk, FP should have had measures in place to ensure clear and unambiguous communications between pilots and tugs. Such measures should necessarily include contingency plans to mitigate risk in the event that tugs are delayed.
Further, Fremantle Ports and its contracted towage provider had not adequately ensured that such risks to the port were mitigated. Procedures for tugs to be on station at the entrance to the port, or for their co-ordinated movement, were not clearly defined.
__________
- International Maritime Organisation, 2003, Resolution A.960(23) Recommendations on training and certification and on operational procedures for maritime pilots other than deep-sea pilots, IMO London.
- Maersk Garonne’s manoeuvring information diagram indicated a stopping distance of about 1.5 miles and a turning circle of about 0.6 miles in diameter when partially loaded, at half speed (about 13 knots), in shallow water.
- Australian Maritime Safety Authority 2009, Marine Notice 07/2009 Bridge Resource Management (BRM) and Torres Strait Pilotage, AMSA, Canberra. Note that this marine notice is no longer current and may contain information which is no longer applicable.
- Cannon-Bowers, J A, Salas, E, & Converse, SA 1993, ‘Shared mental models in expert team decision making’, in Mathieu, J, Heffner, T, Goodwin, G, Salas, E, and Cannon-Bowers, J 2000, ‘The influence of Shared Mental Models on Team Process and Performance’ Journal of Applied Psychology 2000, Vol 85, No. 2 (pp. 273-283), American Psychological Association Inc, 2000.
- SOLAS 1974 (as amended) Chapter V regulation 19.2 Shipborne navigational equipment and systems, requires existing cargo ships of Maersk Garonne’s size (≥50,000 GT) to have ECDIS fitted by July 2016.
- Schager, B 2008, Human error in the maritime industry, Marine Profile Sweden.
- Greche, RG, Horbery, TJ & Koester, T 2008, Human factors in the maritime domain, CRC Press, London.
- A service implemented by a Competent Authority, designed to improve the safety and efficiency of vessel traffic and to protect the environment. The service should have the capability to interact with the traffic and to respond to traffic situations developing in the VTS area.
From the evidence available, the following findings are made with respect to the grounding of the container ship Maersk Garonne at the entrance to the Port of Fremantle, Western Australia, on 28 February 2015. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
- At 0448 on 28 February 2015, Maersk Garonne grounded in charted shallow water while it was being manoeuvred outside the shipping channel at the harbour entrance.
- The harbour pilot conducting Maersk Garonne had decided to delay the ship’s entry into the entrance channel because it was arriving there earlier than the two harbour tugs assigned to assist it.
- Maersk Garonne’s speed until approaching the entrance channel had exceeded both the ship’s passage plan speed and the port’s recommended speed resulting in it arriving there at least 3 minutes earlier than it would have at those slower speeds.
- The manoeuvre to delay the ship’s entry into the channel had become the pilot’s primary focus in the period leading up to the grounding.
- The pilot was not carrying a portable pilotage unit as required by Fremantle Pilots’ procedures and this affected his ability to accurately monitor the ship’s position and progress.
- The ship’s bridge team members did not effectively challenge the pilot’s plan to take the ship outside the channel or take any action to prevent the grounding.
- Bridge resource management (BRM) was not effectively implemented on board Maersk Garonne. The ship’s passage plan for the pilotage was inadequate, its bridge team members were not actively engaged in the pilotage and they did not effectively monitorthe ship’s passage. [Safety Issue]
- Fremantle Pilots’publicly available information to assist ships' masters with preparing a berth to berth passage plan was inadequate and ineffectively implemented. The information provided consisted essentially of a list of waypoints, which wasroutinely not followed.[Safety issue]
- Fremantle Pilots’procedures did not include any contingency plans, including abort points, for risks identifiedfor the pilotage. [Safety issue]
- Procedures for harbour tugsto meet inbound ships andfor their co-ordinated movement in the Fremantle pilotage area were not clearly defined. On 28 February,inadequate co-ordination of the tugs and ineffective communication between Maersk Garonne’s pilot and the tug masters resulted in both tugs, the second one in particular,being significantly delayed from when they could reasonably have been expected to be on station.[Safety issue]
The safety issues identified during this investigation are listed in the Findings and Safety issues and actions sections of this report. The Australian Transport Safety Bureau (ATSB) expects that all safety issues identified by the investigation should be addressed by the relevant organisation(s). In addressing those issues, the ATSB prefers to encourage relevant organisation(s) to proactively initiate safety action, rather than to issue formal safety recommendations or safety advisory notices.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are repeated separately on the ATSB website to facilitate monitoring by interested parties. Where relevant the safety issues and actions will be updated on the ATSB website as information comes to hand.
Bridge resource management
Bridge resource management (BRM) was not effectively implemented on board Maersk Garonne. The ship’s passage plan for the pilotage was inadequate, its bridge team members were not actively engaged in the pilotage and they did not effectively monitor the ship’s passage.
Marine Safety Issue: MO-2015-002-SI-01
Passage plan
Fremantle Pilots’ publicly available information to assist ships' masters with preparing a berth to berth passage plan was inadequate and ineffectively implemented. The information provided consisted essentially of a list of waypoints, which was routinely not followed.
Marine Safety Issue: MO-2015-002-SI-02
Contingency planning
Fremantle Pilots’ procedures did not include any contingency plans, including abort points, for risks identified for the pilotage.
Marine Safety Issue: MO-2015-002-SI-03
Towage procedures
Procedures for harbour tugs to meet inbound ships and for their co-ordinated movement in the Fremantle pilotage area were not clearly defined. On 28 February, inadequate co-ordination of the tugs and ineffective communication between Maersk Garonne’s pilot and the tug masters resulted in both tugs, the second one in particular, being significantly delayed from when they could reasonably have been expected to be on station.
Marine Safety Issue: MO-2015-002-SI-04
Sources of information
The sources of information during the investigation included:
- the master and crewmembers of Maersk Garonne
- the marine pilot on board the ship at the time of the grounding
- Maersk Line Ship Management
- Fremantle Pilots
- Fremantle Ports
- the Australian Maritime Safety Authority (AMSA).
References
Australian Maritime Safety Authority 2009, Marine Notice 07/2009 Bridge Resource Management (BRM) and Torres Strait Pilotage, AMSA, Canberra. Note that this marine notice has been cancelled and may contain information which is no longer applicable.
Australian Maritime Safety Authority 2012, Marine Order 21 (Safety of navigation and emergency procedures) 2012, AMSA, Canberra.
Australian Maritime Safety Authority 2013, Marine Notice 15/2013 Vessel Traffic Services – Responsibilities of Authorities, AMSA, Canberra.
Australian Maritime Safety Authority 2014, Marine Notice 17/2014 Sound navigational practices, AMSA, Canberra.
Di Lieto, A 2015, Bridge Resource Management, Hydeas, Brisbane, Australia.
Greche, RG, Horbery, TJ & Koester, T 2008, Human factors in the maritime domain, CRC Press, London.
International Chamber of Shipping (ICS) 2007, Bridge Procedures Guide, 4th Ed, ICS, London.
International Maritime Organisation (IMO), 1974, The International Convention for the Safety of Life at Sea, 1974, as amended (SOLAS 1974), IMO, London.
International Maritime Organisation (IMO) 1978, International Convention on Standards of Training Certification and Watchkeeping for Seafarers, 1978, as amended (STCW Code), IMO, London.
International Maritime Organisation (IMO) 2004, Resolution A.960(23) Recommendations on training and certification and operational procedures for maritime pilots other than deep-sea pilots, IMO, London.
International Maritime Organisation (IMO) 2004, Resolution A.893(21) Guidelines for voyage planning, IMO, London.
Jonker, C.M., van Riemsdijk, M.B. and Vermuelen, B 2011, ‘Shared Mental Models’, Coordination, Organizations, Institutions, and Norms in Agent Systems VI, Springer, Canada, pp. 132-51.
Reason, J 2008, The Human Contribution, Ashgate, Farnham, England.
Schager, B 2008, Human error in the maritime industry, Marine Profile Sweden.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Australian Maritime Safety Authority (AMSA), the Danish Maritime Accident Investigation Board, Maersk Line Ship Management, Fremantle Ports, Svitzer Australia, Fremantle Pilots, the pilot on board at the time, and Maersk Garonne’s master, chief mate and third mate.
Submissions were received from AMSA, Maersk Line Ship Management, Fremantle Ports, Svitzer Australia, Fremantle Pilots and the pilot on board at the time. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Appendix A – Fremantle Pilots’ Master/Pilot exchange form
Fremantle Pilots’ Master/Pilot exchange of information form, reproduced below, comprises two A4 sized pages and is available from www.fremantlepilots.com.au
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2016
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |