Safety summary
What happened
At 2026[1] on 8 November 2014, train 735, a TasRail intermodal freight service, departed Burnie bound for Brighton in Tasmania. The train travelled to Conara Junction and stopped to complete a scheduled change of driver. At 0303 on 9 November 2014, train 735 resumed its journey to Brighton.
After passing through the Rhyndaston tunnel, the train commenced its descent into Colebrook. During the descent, the driver noted that the train was travelling at below the track speed limit at 20 km/h and took actions to speed the descent. Subsequently, the train rapidly accelerated to above the track speed limit, and at 0521 it derailed at the 64.7 km mark near Colebrook after failing to negotiate a left curve in the track.
The derailment caused extensive damage to both locomotives, the nine wagons and the track.
What the ATSB found
The ATSB found that the driver’s delayed reaction to the acceleration of train 735 allowed it to travel at an excessive speed of 65 km/h in a section of track with a 35 km/h speed limit around a track curve located at the 64.7 km mark. The train’s excessive speed as it traversed the curve, created forces that caused the locomotives and wagons to roll over and derail. It was apparent that the driver of train 735 made inappropriate decisions regarding managing the momentum of descent.
Examination of TasRail’s driver training, competency assurance and fatigue management processes found no inadequacies that could be held as contributory to the driver’s handling of the train during the descent. Accordingly, and based on the available evidence, it appeared that the erroneous train handling techniques applied in this case were atypical and not reflective of training delivered by TasRail or the broader capabilities of its drivers.
What's been done as a result
TasRail has developed further strategies to ensure train drivers have, and are able to maintain, adequate route knowledge, situational awareness and train management skills. TasRail also implemented an advanced train control system, which provides for improved monitoring of rail vehicles, including train handling (over-speed) alarms/alerts to both the driver and train controller.
Safety message
Safely negotiating a train’s passage over undulating terrain relies heavily on the train driver closely and continually monitoring the train’s performance; proactively applying the appropriate handling techniques and driving strategy to ensure train speeds remain within prescribed limits at all times.
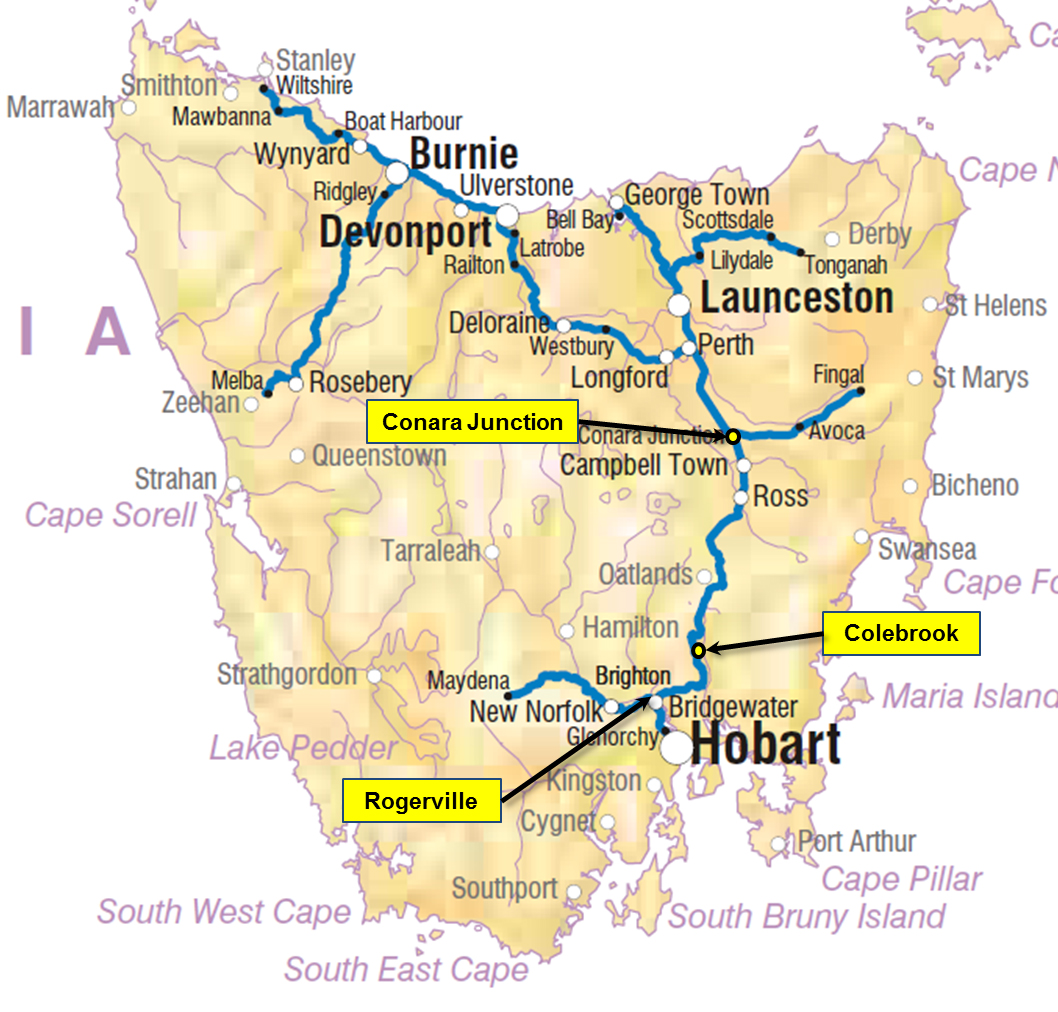
Location map – Tasmania
Source: NatMap Railways of AustraliaTasRail Network
__________
At 2026[2] on 8 November 2014, train 735, a scheduled intermodal freight service operated by TasRail as a driver-only operation[3], departed Burnie, bound for Brighton (south of Brighton) in Tasmania. At 0300 on 9 November, there was a scheduled change of drivers at Conara Junction, with the new driver to take the train through to Brighton.
Conara Junction is approximately 140 km from Brighton by rail and most of the journey is over rolling tablelands with gentle grades. The last 40 km of the journey includes a 13 km descent into the Coal River Valley, most of which has a posted track speed of 35 km/h due to the steep grades and tight radius curves.
The passage of train 735 from Conara Junction to Rhyndaston Tunnel (the top of the descent) was uneventful. At 0512, the driver called Train Control, reported the train clear of the tunnel, and then commenced descending the grade using the locomotive dynamic brake[4].
At 0516, the train crossed the level crossing at Mud Walls Rd, at a speed of 30 km/h. The train’s data logger showed that shortly thereafter, the speed had dropped to 20 km/h and the driver disengaged the dynamic brake and increased the throttle.
Once in power, it took 34 seconds for the train to accelerate to 39 km/h, and in an attempt to slow the acceleration, the driver reduced the throttle. This action did not slow the train and it continued accelerating.
At a speed of 54 km/h, the driver attempted to regain control of the train by moving the throttle from power into dynamic brake. During the transition from power to dynamic brake, the train continued to accelerate and reached a speed of 58 km/h before the recorded data showed a partial service brake application.
At around 0521, train 735 entered a series of adjoining curves with both the service and dynamic brakes applied. The train continued to accelerate and gain momentum; reaching a peak speed of 65 km/h as it crossed a short bridge near the exit of a curve at the 64.7 km mark near Colebrook.
As train 735 traversed the curve at speed, it was unable to maintain normal contact with the rail. Consequently, both locomotives and the following four wagons rolled onto their sides and came to a rest in the cess drain on the right hand side of the track. The force generated during the derailment sheared the draft gear of locomotive TR07, which detached it from TR10. That same force also caused locomotive TR07 to uncouple from the rest of the train. At some stage, during the derailment, the train brake pipe was severed which initiated an emergency brake application.
A further five wagons also derailed, but remained within the ballast area of the track formation. Many of the containers from the derailed wagons sustained damage and some were cast down the railway embankment. The remaining seven wagons at the end of the train did not derail and were undamaged.
Figure 1: Locomotives TR10 and TR07 with wagons of train 735 at the derailment site

Image shows the lead locomotive (TR10) and trailing wagons having tipped onto their side after attempting to traverse a left-hand curve. The driver (who sustained minor injuries) was able to exit the locomotive via the front windscreen, which is designed as an emergency exit. Source: ATSB
Events post-derailment
The TR class locomotives include a feature that automatically notifies train control of an emergency brake application. Having received that alert from locomotive TR10 resulting from the derailment, the train controller[5] attempted to call the driver of train 735. The driver reported hearing the call, but was unable to find the radio microphone within the overturned locomotive cab and was unable to respond. However, the driver did subsequently locate a mobile phone and used it to contact the train controller and report the emergency. During the conversation, the driver advised having sustained minor injuries.
The driver reported being able to escape the locomotive cabin through an emergency exit[6], with the train’s dangerous goods cargo manifest in hand. The train controller commenced notifying emergency services and TasRail first responders, while the driver checked the train to ascertain the extent of damage and the state of the dangerous goods freight. Subsequently, the driver notified train control that a quantity of leaded petrol had been spilled, however there had not been a fire. Train control informed the Tasmania Fire Service, which dispatched a team to manage the spill.
__________
- The 24-hour clock used in this report is Australian Eastern Daylight Time (EDT).
- Driver-only operation means there is only one person in the cab of the locomotive who is responsible for the operation of the train.
- Dynamic brake is the use of the locomotive’s traction motors to effect braking. The traction motors become generators and the power generated is converted to heat that is dissipated through fan-cooled resistor grids in the locomotive.
- The train controller was located at the TasRail Train Control Centre in Launceston, Tas.
- TR class locomotive windscreens are designed for removal as an emergency exit. In this case, the driver had some trouble removing one window due to a dash-mounted camera, but managed to push out the other window, against the dirt piled up on the outside.
Incident location
The derailment occurred at the 64.7 km mark on the Tasmanian South Line, approximately 2 km north of Colebrook and approximately halfway down the 13 km descent that starts at the Rhyndaston Tunnel.
The posted track speed alternates between 35 and 40 km/h over the course of the descent. The approach to the derailment site had a listed track speed of 35 km/h, increasing to 40 km/h soon after exiting the curve.
Environmental conditions
Recorded weather observations for the morning of 8 November 2014 from the Bureau of Meteorology weather station located at Tunnack, Tasmania showed a maximum temperature of 18.1°C at 0900 with strong Northerly winds gusting to 72 km/h.
The ATSB discussed these conditions with the driver of train 735 and determined that it was unlikely that they had contributed to the derailment.
Train information
Train 735 was a regular freight service operated by TasRail between Burnie and Brighton. The TR class locomotives generally hauled these trains.
On 8 November 2014, train 735 departed Burnie with two locomotives (TR10 leading, TR07 trailing) and 30 wagons. The majority of the wagons were new TQAY two-unit[7] vehicles, with the remainder a mixture of older container wagons, including QLE and QL types. At Western Junction, en route to Brighton, the train crew decoupled 14 wagons and then continued the journey with the remaining 16 wagons. Four of the 16 wagons remaining in the consist were the older QLE or QL types. These wagons have a different brake application and release rate to the new TQAY wagons and thus the Train Manifest Report included the following train operational advice:
DANGER – INCREASED RISK OF DERAILMENT
Due to differing brake application and release rates your train may be subject to high in train forces.
DO NOT release brake applications of less than 100kPa at less than 20 km/h – Wait for the train to stop.
The train has a high power/weight ratio. You must consider shutting down or turning off excess power.
The train has a high-proportion of dual-stage brake wagons, brake applications greater than minimum will be required to control the train.
All wagons were loaded and conventionally arranged such that the heavier wagons were to the front of the consist and the lighter wagons to the rear. Two of the heavier wagons were carrying containers filled with leaded petrol (classed as a dangerous good); one of these wagons derailed and leaked after the derailment. None of the wagons on train 735 had any defects identified for repair.
Driver information
At the time of the derailment, the driver of train 735 had been working with TasRail for 13 months; having previously trained as a driver and driven trains in Queensland. At the time of the derailment, the driver held all necessary competencies and authorisations.
After the derailment, the driver underwent drug and alcohol testing, the results of which were negative.
Track information
The Tasmanian South Line opened in November 1876 and consists of narrow gauge track that has sections of steep gradients and sharp curves.
The descent from the Rhyndaston Tunnel into Colebrook and the Coal River Valley has many tight radius curves and drops 200 m over its 13 km length, with grades ranging from 1:125 to 1:31[8].
The 1500 m of track leading into the derailment site flattens in grade from 1:41 to 1:100. The derailment occurred at the end of the 1:41 grade where it flattens out to 1:125.
The derailment occurred on a compound curve[9] of 190 m radius, tightening to 110 m radius in the direction train 735 was travelling.
The mandated track speed though the compound curve was 35 km/h.
Track design
The track on which a train travels is an alignment and is described in two dimensions. First, the horizontal alignment defines where the track goes. The second component is vertical alignment, which defines the track’s elevation (rise and fall).
A railway is a guided transportation system. That is, a train driver only has direct control over the speed and forward/reverse directional aspects of train movement over an alignment defined by the track.
As any rail vehicle in motion traverses a curve, the vehicle transmits a centrifugal force to the rail at the point of wheel contact. This force is a function of the curve radius and superelevation[10], speed and mass (weight) of the vehicle, and acts at the centre of gravity of the rail vehicle.
To determine track speed limits, operators and infrastructure managers consider both the type of rail traffic and the track alignment. To ensure the safe passage of rolling stock, operators/drivers formulate driving strategies and apply the necessary train handling skills to ensure the train speed remains within the track limits.
The importance of remaining within track speed limits is particularly relevant when traversing a track curve. By travelling at, or below the maximum allowable track speed, the vehicle stays within the tolerances allowed for centrifugal force. The faster a vehicle travels the more likely it is to derail, either through flange-climb or through overturning.
The point of derailment for train 735 was at the 64.7 km mark, on the exit of a 110 m radius track curve with a maximum allowable speed of 35 km/h.
In 2013 and 2014, a capital works project upgraded the track in the area leading up to the point of derailment. During those works, TasRail installed concrete sleepers and replaced the existing rail with continuously welded 41 kg/m rail. Taking into account the maximum allowable speed of 35 km/h, the ATSB considered that the specifications for the track infrastructure and curve were adequate to facilitate normal operations. There was no evidence to indicate that the track had any existing defects or anomalies that could have contributed to the derailment.
The derailment of train 735
Figure 2: Sequence of events for the derailment of train 735
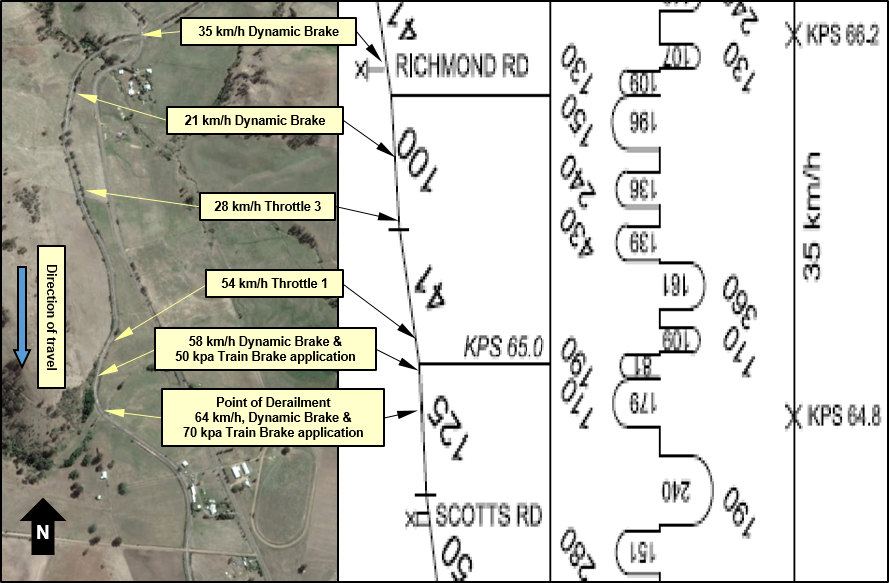
The image shows an aerial view of the track from Richmond Road (top) and a track geometry graph showing gradient, curvature and posted track speeds. The annotations show driver actions and track speed (obtained from locomotive data loggers) at the key points during the train’s descent and subsequent derailment (bottom). Source: Google Earth and TasRail
At 0519 on 9 November 2014, train 735 traversed the track section between the Rhyndaston Rd and Richmond Rd level crossings – a fall in elevation of about 90 m over a distance of approximately 4 km. It crossed Richmond Rd at a speed of 35 km/h with its speed slowed by the locomotives’ dynamic brake. At this time, the train was travelling within the maximum speed limit of 35km/h and was under the driver’s control.
About 500 m later in its descent, the train travelled through a short section of flat terrain and slowed to 21 km/h. The driver chose to move out of dynamic braking and into throttle position 3 and, in doing so, caused the train to accelerate (Figure 2).
Train 735 accelerated from 21 km/h to 54 km/h over a distance of about 700m, before the driver moved the throttle from position 3 to 1. At 54 km/h, train 735 was travelling at 19 km/h over the maximum allowed track speed and in the midst of a track curve with a 179 m radius. The high train speed combined with the track curve radius significantly increased the risk of derailment.
By the time the driver actively attempted to slow the train, it had reached 58 km/h. At this time, the driver moved the throttle from position 1 into full dynamic brake and made a ‘service’ application of the train brakes.
The movement of the throttle from position 1 to full dynamic brake at a speed of 58 km/h did not allow sufficient time for the locomotive to go through the required transitional set-up phase. During this transition phase, the dynamic brake does not take effect, as the locomotive needs to reverse the polarity of its traction motors and effectively turn them into generators before being able to retard the momentum of the train.
Further, the service application of the train brake requires time for the air pressure to reduce in the train brake pipe and allow the wagon brakes to take effect.
By the time the driver attempted to slow the train, it was out of control and rapidly descending the grade towards Scotts Rd.
The train reached a maximum speed of 65 km/h as it exited the compound track curve located at the 64.7 km mark. It was at this location that the wagon immediately behind the locomotives derailed by rolling off the track. The rolling of this wagon transferred forces through the couplers to the locomotives ahead and the wagons immediately following it. This rolling force, in conjunction with the outward centrifugal forces acting on the vehicles themselves allowed both the locomotives and the three wagons following to roll onto their sides and derail to the right hand side of the track on the outside of the curve.
Driver performance
The sequence of events in the moments leading up to the derailment suggested the driver had a delayed response to visual indications of the train’s performance and speed. Further, the driver’s decision-making in relation to train handling appeared to lack an appropriate consideration or understanding of the train’s braking characteristics. The ATSB explored possible reasons for this and reviewed the driver’s operational knowledge, work schedule and the effects of fatigue on human performance.
Fatigue
In the context of human performance, fatigue is a physical and psychological condition primarily caused by prolonged wakefulness and/or insufficient or disturbed sleep.[11] Fatigue can have a range of influences on performance, such as decreased short-term memory, slowed reaction time, decreased work efficiency, reduced motivational drive, increased variability in work performance, increased errors of omission and an increase in the level of acceptable risk that is tolerated.[12] Fatigue impairment has been identified as a causal factor in many rail accidents and incidents.
It is generally agreed that most people need at least 7 to 8 hours of sleep each day to achieve and maintain maximum levels of alertness and performance. In this case, the derailment occurred on what was the driver’s third successive night shift. The driver had finished work at 0815 on 8 November and started the next shift (in which the derailment occurred) at 2359. The driver reported that during the intervening rest break on 8 November, they had obtained approximately 9.5 hours of good quality sleep, in two blocks from 1030 to 1400 and from 1930 to 2200. They reported obtaining approximately 6.5 hours of sleep during the rest break on 7 November, totalling 16 hours of sleep for the 48 hours before the occurrence. The driver reported feeling alert at the start of the shift.
Based solely on sleep obtained, the driver would not appear to have been at an increased risk of fatigue-impaired performance. However, while hours of sleep is a primary determinant of fatigue impairment, there are other factors which can influence fatigue, including time of day of both sleep and work. To assist with assessing fatigue likelihood based on these factors, the driver’s work schedule and reported sleep were modelled using biomathematical fatigue prediction modelling software[13]. The analysis suggested that a person exposed to this work and sleep schedule would, during the entire occurrence shift, be at least mildly affected by fatigue and be deteriorating as the shift progressed. The modelling suggested that a reaction time in the range of 1.4-times that of a well-rested person could be expected at the time of the derailment.
Considering these factors, it appears possible that the driver’s performance was mildly affected by fatigue – attributable to time of day effects after driving continuously for 5.5 hours through the night. This to some extent might explain the driver’s slowed response to the visual cues presented during the critical moments of the train’s descent. However, it is important to note that the actions required for managing a train’s descent through this area is largely not time-critical whereby reaction time has a significant influence, and considering the driver’s reported alertness, the ATSB considered that driver fatigue impairment was not a factor in the development of this occurrence.
Operational knowledge
While the driver had a good general operational understanding, they did lack some technical knowledge of the train’s specific characteristics which may have contributed to the decision-making process during the descent and immediately prior to the derailment. This was especially evident in the driver’s management of the locomotive throttle and dynamic brake.
The driver’s decision to move from dynamic brake application to throttle position 3 took place at a critical point in the descent. The driver, upon reflection on the incident, believed that had they not moved into throttle, the train would have slowed to a stop. Records of other train descents of the same grade suggest otherwise.
Records of descents made by other trains show that those drivers controlled their train’s descent, by modulating the dynamic brake or using a combination of service brake and dynamic brake. In doing so, the train maintained a reduced speed for a short period before accelerating down the falling grade with the driver countering the acceleration by increasing the level of dynamic braking.
In summary, it was apparent that the driver of train 735 made inappropriate decisions regarding managing the momentum of descent, especially with respect to the train braking techniques required when descending the grades from the Rhyndaston Tunnel into Colebrook. This ultimately led to the train’s derailment at the 64.7 km mark near Colebrook, Tasmania.
__________
- A wagon consisting of two permanently coupled platforms, each platform independently supported on a pair of bogies.
- The grade of the railway is expressed as the vertical rise (or fall) per unit of distance.
- A compound curve comprises of two or more differing radii but in the same direction.
- The height difference, at a common location, between the running surfaces of two rails. Similar to the camber of a roadway.
- National Transport Commission, 2008. National Rail Safety Guideline. Management of Fatigue in Rail Safety Workers.
- Battelle Memorial Institute 1998, An Overview of the scientific literature concerning fatigue, sleep, and the circadian cycle, Report prepared for the Office of the Chief Scientific and Technical Advisor for Human Factors, US Federal Aviation Administration.
- The Fatigue Avoidance Scheduling Tool (FAST), and the Fatigue Risk Index (FRI).
Train handling
The management of a train’s movement along a track alignment is the core skill set of train drivers and commonly referred to as ‘train handling’.
In essence, good train handling is the accurate use of locomotive controls to limit the amount of in-train forces while moving the train in a specific direction at a designated speed. Accurate use of the locomotive controls requires the driver to have sound technical and practical knowledge of a locomotive’s capabilities. A driver’s knowledge base is formed at the beginning of their career. It is then developed over time by working with different types of locomotives over varying networks.
Train 735’s driver had worked for another operator and driven trains for 5 years prior to arriving at TasRail. Those trains were consistent in length and weight and operated over the same track sections for every journey. The typical type of learning undertaken by the driver prior to arriving at TasRail relied on the acquisition of knowledge by rote learning[14]. This is in contrast to learning with comprehension and understanding, where a driver is equipped to apply knowledge to tasks requiring a particular or unique solution, rather than one that has been learned only by repetition.
This form of learning from their previous role may have influenced the driver’s actions during the descent toward Colebrook. However, when transferring to a different rail operator, drivers are normally required to undertake further training to ensure competency against operator specific safety management systems, including the operational environment. The ATSB examined TasRail’s training systems in relation to route knowledge and train handling through the area of the derailment.
TasRail training
To supplement the driver’s knowledge of the locomotive controls and improve train-handling ability, drivers routinely complete route knowledge training.
Route knowledge training involves the driver trainee travelling (as an observer) over designated routes with a more experienced and competent driver. During each journey, an instructor[15] will provide train handling advice and other general information relating to the section traversed. At the commencement of the training program, the instructor or training coordinator provides the driver with documentation containing route maps and other necessary information relevant to the sections over which the driver will be operating. During the training, the driver can make notes that are relevant to the driving strategy they have developed by combining their train handling ability with the learned route knowledge.
At the completion of the training program, the driver will demonstrate train handling ability and route knowledge during a practical assessment. At the completion of the assessment, the driver is debriefed and, in consultation with the instructor, decides whether they are confident and competent to commence full mainline operations. To ensure skill maintenance and development, a driver will complete ongoing annual assessments of route knowledge competency and driving strategy.
The ATSB’s review of TasRail’s training documentation for train 735’s driver indicated that the training methodology described had been followed and the driver recorded as achieving satisfactory competencies.
During initial enquiries, the driver of train 735 informed the ATSB of signing the route knowledge and competency documentation. Further, the driver stated that they were confident in their ability to safely manage the journey of a train over the TasRail network.
However, at interview, and after having time to reflect on the incident, the driver advised the ATSB that they probably should not have signed the competency. The driver attributed this to the:
- undulating terrain,
- age of the infrastructure,
- constant change in instructor during the training period
- questions about the time taken, and
- lack of opportunity to drive during the training period.
At the commencement of the training period, the driver recalled being supplied with route maps and gradient diagrams by an instructor. However, the single page (A3) document provided limited detail. Over the subsequent 21 trips during this training period, the driver considered the document to be hard to read especially while driving, so chose not to use it.
The ATSB made further enquiries to verify TasRail’s practical application of its training methodology and driver accreditation practice. The ATSB found TasRail’s training documentation and training delivery to be generally consistent with industry practice and sufficient for training drivers operating over their network.
In the months leading up to the derailment, after signing off as having learned the route, the driver made multiple trips in varying train types and lengths along the network section where the derailment occurred. The driver made these journeys without incident and did not report any difficulties in negotiating the section. Further, TasRail did not have, nor did the driver produce, any evidence to suggest the driver had trouble driving trains along any part of the TasRail rail network.
The ATSB compared records of descents by other trains, down the same grade by other drivers, in the days prior to the derailment. Records indicate that all other drivers routinely applied a similar driving strategy and were able to control train speeds predominantly by use of the locomotives’ dynamic brake.
The locomotive operational data (from multiple descents) suggested that TasRail drivers generally apply consistent and appropriate train handling techniques when traversing that track section.
However, the strategy applied to the train 735’s descent on 9 November 2014 was different. The driver placed the locomotive throttle into position 3 at a critical time in the descent and allowed the train’s speed to increase to 54 km/h before taking any corrective action. Further, the action taken was not sufficient to arrest the train’s acceleration and it reached a maximum speed of 65 km/h before derailing as it traversed the curve.
Consideration was given to the fact that the derailment occurred over a section of track where the driver of train 735 had safely negotiated the descent of multiple trains in the six months prior to the derailment. It was only in this specific instance that evidence suggested the driving strategy was different and that proved to be critical to the derailment of train735.
Despite the ATSB’s inquiries, it was unclear why the driver had handled the train in this manner during the descent on 9 November 2014.
__________
From the evidence available, the following findings are made with respect to the derailment of train 735 near Colebrook, Tasmania on 9 November 2014. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
- Train 735 derailed due to excessive speed through a track curve at the 64.7 km mark.
- The driver of train 735 did not demonstrate effective train handling techniques at critical moments when descending the grades from the Rhyndaston Tunnel into Colebrook. This was especially evident in the application of locomotive throttle at a critical point in the descent.
Other findings
- The ATSB found no evidence to suggest that the driver of train 735 had received insufficient training or had previously experienced any difficulty in driving trains along any part of the TasRail network.
- There was no evidence of any defects or anomalies in the track at the 64.7 km mark that could have contributed to the derailment.
- There was no evidence of any fatigue-related issues that may have contributed to the inappropriate train handling techniques applied by the driver in this case.
- The locomotive data logs from a number of previous descents, by other trains and drivers, demonstrated consistent and appropriate train handling techniques.
Sources of information
The sources of information during the investigation included:
- Bureau of Meteorology
- TasRail
- National Guideline Glossary of Railway Terminology Version 1.0, 3 December 2010 Railway Industry Safety and Standards Board of Australia (RISSB)
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the driver of train 735, TasRail, and the Office of the National Rail Safety Regulator (ONRSR).
Submissions were received from TasRail, and the Office of the National Rail Safety Regulator. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2016
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence
Proactive safety action taken by TasRail
- In response to the derailment near Colebrook, TasRail has taken the following action:
- Following the derailment, TasRail developed strategies to ensure train drivers have, and are able to maintain, adequate route knowledge, situational awareness and train management skills. TasRail also implemented a regular audit of data from locomotive data loggers and developed a policy with respect to the use of electronic mobile devices.
- TasRail has since invested in an Advanced Network Train Control System (ANCS). The benefits include:
- Fully automated system, reducing input/output errors and substantially reducing safe working breaches
- Provides full visibility of all vehicles on the network in real time
- Enables early intervention to prevent incidents from occurring or to reduce the severity of incidents
- Reduces the risk of an on-track collision and/or derailment
- Improves train speed compliance through recording of speed and location data. Will send train handling alarms/alerts to the Locomotive Driver (and the Train Controller) – for example if a train is travelling over speed limits
- Improved capacity to manage and monitor track work and train working by streamlining the transmission and authorisation of network access authorities
- Increases productive track access time, significantly improving the efficiency of infrastructure maintenance and upgrade activities
- Fuel savings from reduced track access downtime
- GPS positioning increases the accuracy of information
- Operational efficiencies from improved freight movements and reliability of train operations
- Capability to introduce a ‘track and trace’ data facility for customers
- Provides Train Controllers with an improved working environment (previous system required an excessively high reliance on procedural compliance)