
Executive summary
What happened
On 16 May 2022, a Robinson Helicopter Company (RHC) R44, registered VH-KOV and operated by Wellspring Rural Services Pty Ltd, was being used to conduct a series of sightseeing flights over the Limmen National Park, Northern Territory, with a pilot and 3 passengers on board.
During cruise flight, vibrations were detected through the helicopter, subsequently the pilot observed the engine RPM rise and then drop to zero. Having assessed that the engine had failed, the pilot initiated an autorotation and the helicopter subsequently collided with terrain. Two passengers sustained serious injuries, with the pilot and remaining passenger sustaining minor injuries. The helicopter was substantially damaged.
What the ATSB found
The ATSB found that during cruise, the clutch actuator lower bearing seized resulting in a total loss of drive from the engine to the rotor system. This bearing had not been maintained in accordance with the maintenance procedures, which likely resulted in its failure.
It was also identified that the passengers did not receive a pre-flight safety brief resulting in them being unaware of the emergency procedures and the safety equipment on the helicopter.
In December 2021, the Civil Aviation Safety Authority (CASA) released Civil Aviation Safety Regulation (CASR) Part 133, which changed the regulations related to air transport passenger carrying operations in helicopters. The ATSB found that there were several changes to the requirements which were not promulgated to operators in the documentation released to explain the regulatory changes, including the mapping of Civil Aviation Regulations to CASR Parts 91, 119 and 133–Australian air transport operations–rotorcraft and CASA Part 133 Key operational changes with suggested text.
CASR Part 133 required changes to the pre-flight passenger safety briefing for aircraft with a seating capacity of less than 6 people, including that passengers were briefed on the emergency brace position with information specific to their aircraft type and model. However, while CASA provided guidance on how to brace in some configurations, they did not provide specific information on how to brace in a helicopter, such as the R44, which has 3-point harnesses installed.
It was also identified that the emergency locator transmitter (ELT), which activated 10 hours after the accident, was not being maintained and the operator had not been advised of this.
Finally, the ATSB also found that the Robinson Helicopter maintenance procedures and CASA guidance did not provide clear guidance on how ELTs in helicopters should be maintained.
What has been done as a result
As a result of this investigation the maintainer contacted each of the operators of the helicopters they maintain to ensure they were aware that the emergency locator transmitter (ELT) was not being maintained and to ensure they were carrying a personal locator beacon in the helicopter.
The Civil Aviation Safety Authority (CASA) also updated the airworthiness bulleting (AWB) 02-002 to include information on ELT maintenance and guidance if the information contained within the aircraft’s maintenance schedule is not sufficient.
The ELT manufacturer has also advised the discrepancy between the service letter and the installation manual will be corrected to reflect that the self-test should be a recommended practice as the current regulations do not require a self-test.
CASA also released a revised multi-part advisory circular (AC) 91-19, AC 121-04, AC 133-10, AC 135-12 and 138-10 version 1.1 Passenger safety information to include information on how to brace in a helicopter with a 3-point harness. This now contains a specific section for rotorcraft with a lap strap and single diagonal shoulder harness.
Safety message
This investigation highlights the importance of following the manufacturer’s maintenance procedures. If a maintainer considers that additional maintenance should be conducted on any component in an aircraft, they should contact the manufacturer for engineering advice before varying from the procedure.
Emergency locator transmitters (ELTs) are now mandatory equipment in an air transport helicopter with more than 3 seats, however, they are only effective if they are operational. To ensure this is the case, there should be clear procedures on how they should be maintained. Operators are also reminded that they should be ensuring a self-test of the unit is conducted monthly to verify the ELT is operational.
The occurrence
On 16 May 2022, a Robinson Helicopter Company (RHC) R44, registered VH-KOV and operated by Wellspring Rural Services Pty Ltd, was being used to conduct a series of sightseeing flights over the Limmen National Park including Lorella Springs Wilderness Park, Northern Territory, with a pilot and 3 passengers on board.
During the initial flight, the helicopter flew from the main house at Lorella Springs to the coast (Figure 1 inset), landing at 2 different locations where the passengers disembarked to fish. They then flew to a third location, where the passengers disembarked to swim at a waterhole. While the passengers swam, the pilot lit a fire to boil water for some refreshments. The fire was extinguished prior to departure.
The helicopter departed at approximately 1533 local time and flew to a valley which had sandstone rock formations along both sides of the valley, known as the Lost City, rising approximately 150 ft above the valley floor. They initially flew along the eastern side and then returned on the western side of the valley, at approximately 500 ft above the valley floor (Figure 1).
Figure 1: VH-KOV flight track overflying the Lost City
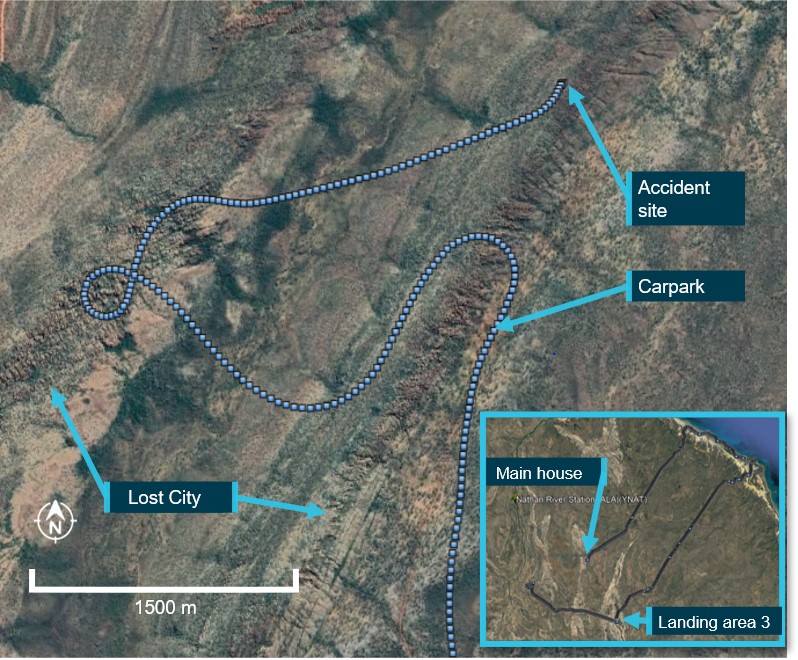
The dotted line is the final track of VH‑KOV, the inset details the track the helicopter took for the sight-seeing tour.
Source: Google Earth and OzRunways data, annotated by ATSB
The pilot later recalled that, as the helicopter re-crossed the valley to return to the main house, they detected a burning smell and recalled that within a couple of seconds the engine began to run slightly rough.
In response to the malfunction, the pilot advised their initial concern was getting over the sandstone formations on the eastern side of the valley and then landing at a nearby carpark ‑ the only clear space to land in the area. As the pilot lowered the collective to reduce power, in case the engine failed, they checked the engine oil temperature, pressure and cylinder head temperature gauges, which were all in the normal range.
Within about 3 seconds, the vibrations through the helicopter increased. A passenger in the right rear seat later reported detecting a light in the top left of the console along with a warning buzzer at this time, however this was not recalled by anyone else in the helicopter. The pilot observed the engine RPM suddenly rise, then drop to zero and assessed that the engine had failed. Still on the valley side of the sandstone formations, the pilot initiated an autorotation into an area of less dense trees. Prior to the flare just above the treetops, the pilot instructed the passengers to ’brace’.
The pilot advised that the helicopter fell through the trees, contacting the ground initially on the right front side, nose low, and then the helicopter spun and rolled on to the left side facing the opposite way to the direction of travel (Figure 2).
Figure 2: VH-KOV

Source: Operator
The pilot advised that they undid their seatbelt and collected the emergency kit from under their seat. This contained a first aid kit, emergency rations and a satellite sleeve.[1] They then moved to the side of the helicopter and tried unsuccessfully to connect their mobile phone to the satellite sleeve (see the section titled Satellite sleeve) to raise an alert.
As a result of the impact, fuel was leaking from between the back seats onto the passenger in the rear left seat. The passenger located in the rear right seat, released themself from their seatbelt and assisted the other rear seat passenger out of the helicopter. The passengers asked the pilot for a fire extinguisher and were advised there was none onboard. They also requested a first aid kit, however this was not provided and the passengers later advised there was no first aid kit on the aircraft. Together, the passengers then assisted the front seat passenger to exit the helicopter.
The passengers then asked the pilot to ensure the emergency locator transmitter (ELT) (see the section titled Emergency locator transmitter) was working. The pilot re-entered the wreckage and selected the ELT remote switch in the cockpit to ON and reselected the main battery to ON, however the ELT unit failed to activate. As they were concerned about a fire starting due to the leaking fuel, the pilot and passengers began to walk to the carpark, about 1.5 km from their location.
When the helicopter did not arrive back at the main house at the pre-arranged SARTIME,[2] the operator took a second company R44 to search for VH-KOV. They flew directly to the landing area near the waterhole where the operator identified that the remains of the fire were still warm. Consequently, they flew towards the Lost City searching for VH-KOV as this was the next destination on the standard route flown during the scenic flight.
The operator detected the accident pilot and passengers near the carpark and landed the helicopter close to them. They then transported them, in 2 groups, back to the main house.
Two passengers sustained serious injuries, with the pilot and remaining passenger having minor injuries. The helicopter was substantially damaged.
Context
Helicopter
The Robinson Helicopter Company (RHC) R44 Raven I is a four-seat helicopter, with hydraulically boosted flight controls. It is powered by a Lycoming O-540-F1B5 series, six-cylinder carburetted piston engine. VH-KOV, serial number 1762, was manufactured in 2007 and placed on the Australian register in the same year. The front passenger and pilot doors had been removed, leaving the rear passenger doors installed. Quick disconnect pilot controls for the front left seat had also been removed. In July 2015, the helicopter had undergone an overhaul at 2,200 hours with a second overhaul due in 116.4 hours.
The helicopter was maintained in accordance with the manufacturer’s maintenance schedule, which required a periodic inspection every 100 hours or 12 months, whichever came first. A periodic inspection was completed on 30 July 2021 at 4,183.7 hours in-service. The accident occurred at 4,283.6 hours.
The RHC maintenance manual stated that the ‘inspection interval may be extended up to 10 hours, without accumulation’. There were a number of occasions where the operator had overflown the 100 hourly inspection requirements, however the following inspection interval had not been reduced by the overflown hours. The operator had recorded the overflown hours and had purchased a second R44 to reduce the likelihood of this occurring in the future.
Table 1 details maintenance actions conducted between the last periodic inspection and the accident.
Table 1: Overview of recent maintenance
| Date | Hours | Description of maintenance conducted |
| 16 May 2022 | 4,283.6 | Accident |
| 6 May 2022 | 4,261.1 | Crank seal renewed, clutch actuator tension microswitch renewed, cooling fan balanced. |
| 24 March 2022 | 4,235.4 | New starter fitted |
| 18 October 2021 | 4,234.6 | 50 hr - #2 cylinder replaced. |
| 30 July 2021 |
4,183.7
|
Periodic – plus clutch actuator down and maximum limit microswitches renewed, crank seal renewed, upper and lower bearings serviced, #3 and 5 cylinders replaced, right magneto replaced. |
Accident site
The ATSB did not attend the accident site. The helicopter was partly disassembled on site, including engine removal, and transported to Queensland for examination. Engine and airframe examinations were conducted between 19–21 September 2022.
Engine inspection
The engine teardown inspection was conducted at a CASA-authorised engine overhaul facility and observed by the ATSB. On removal of the cooling fan shroud, the engine cooling fan was found to have separated due to a fracture of the shaft at the clutch actuator lower bearing (Figure 3). The fracture location showed evidence of significant overheating. All associated components were retained for further detailed examination.
Some of the engine components displayed damage consistent with an overspeed event, however examination of the engine did not identify any condition or failure that would have resulted in sudden power loss or stoppage.
Helicopter examination
The ATSB examined the airframe at a storage facility. The tail cone and main rotor transmission assembly had been removed to assist transport. Similarly, the main rotor blades, sectioned near the hub, and some sections of the landing gear had also been removed and were not available for examination. The tail rotor gearbox and stabiliser assemblies separated from the helicopter during the impact sequence. All damage was consistent with overstress from impact forces. In addition, the examination identified:
- flight control continuity
- some impact damage to the fuel tanks however, the bladders were intact
- the fuel tank interconnect line had fractured in overstress and was the reason for the post‑impact fuel leak
- the main and tail rotor transmission assemblies exhibited no evidence of failure and could be rotated without restriction.
In summary, no failure or other condition, beyond the fan shaft failure, was identified that would have affected normal operation of the helicopter.
Lower sheave and fan shaft
Examination of the aft face of the lower sheave revealed accumulated grease consistent with it extruding past the lower bearing seal over a period of time. The maintainer reported wiping the sheave clean each time they worked on the helicopter however, the accumulated grease was not consistent with this having occurred at the last reported maintenance action requiring the bearings to be lubricated, 10 days prior to the accident or 22 hours of operation.
The fan shaft failed at the location of the lower bearing. The shaft exhibited deformation, necking, and gouging consistent with localised frictional heating. Circumferential scoring on the fracture surface was a result of the powered shaft contacting the bearing housing.
Figure 3: Lower sheave showing accumulated grease and failure of the shaft to the cooling fan

Source: ATSB
Lower bearing
The ATSB examined the clutch actuator lower bearing at its Canberra technical facility. The forward face of the bearing housing exhibited matching gouging from contact with the rotating fractured engine output shaft (Figure 4). The cover plate was removed, and the bearing was found to have seized. The damage observed was consistent with intense heat and subsequent seizing of some of the rollers. The cage and intermediate spacer were also found to be heat-damaged.
Figure 4: Damage to lower actuator bearing
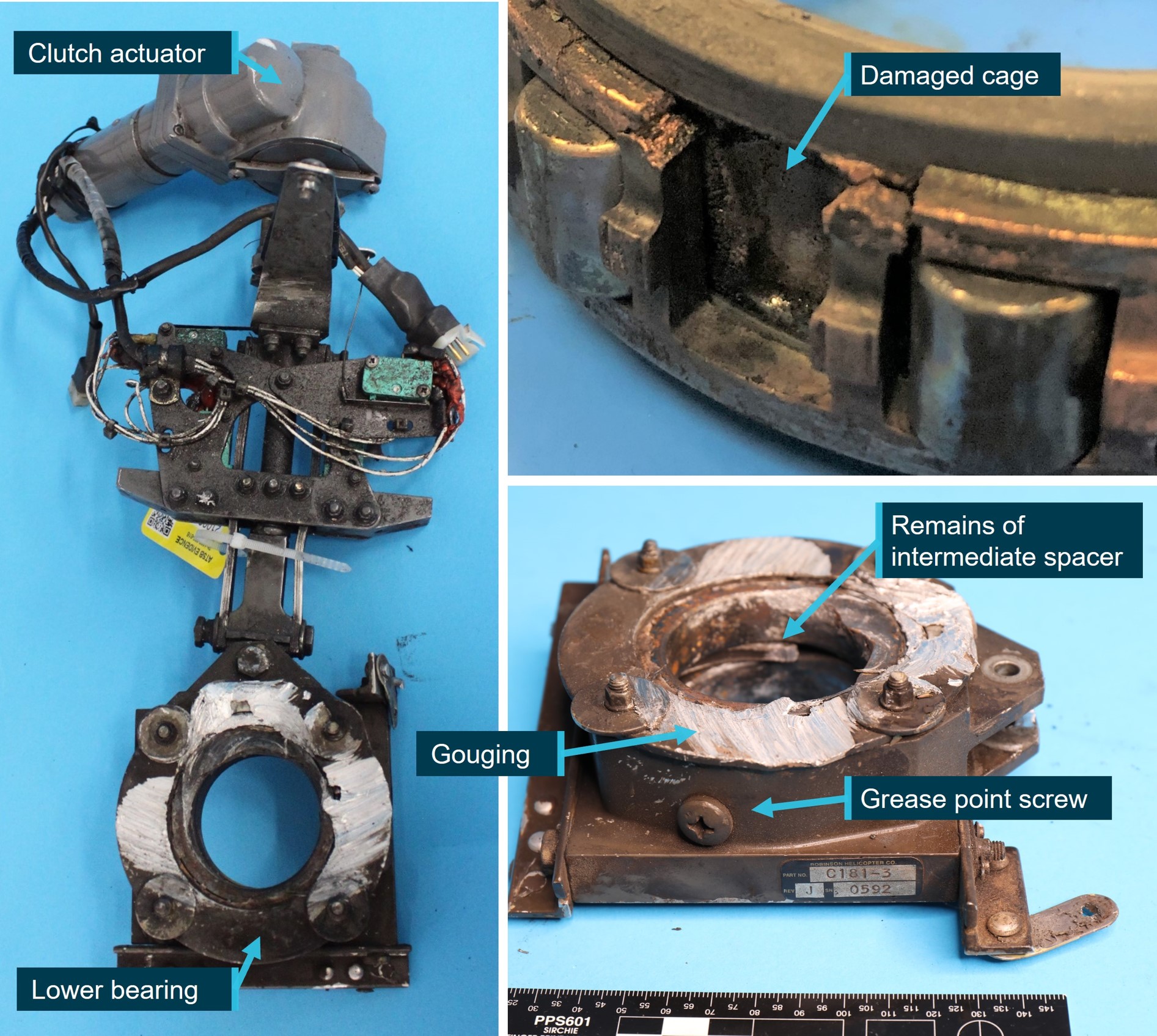
Source: ATSB
Grease residue was visible in the bearing housing (Figure 5) however, the intense heat associated with the bearing and fan shaft failure precluded the ability to determine the quality and quantity of grease and the condition of the seals prior to the occurrence.
Figure 5: Lower actuator bearing housing, showing minimal dried grease

Source: ATSB
R44 drivetrain
A V-belt sheave is bolted directly to the engine output shaft (Figure 6). Rubber V-belts transmit power to the upper sheave, which contains an overrunning clutch. The upper sheave transmits engine power via a shaft both forward to the main rotor and aft to the tail rotor.
A bearing, connected to an electric clutch actuator, is mounted between a direct-drive fan wheel and the engine on the engine output shaft. The fan supplies cooling air to the cylinders and oil cooler via a fibreglass and aluminium shroud.
Figure 6: R44 drive system
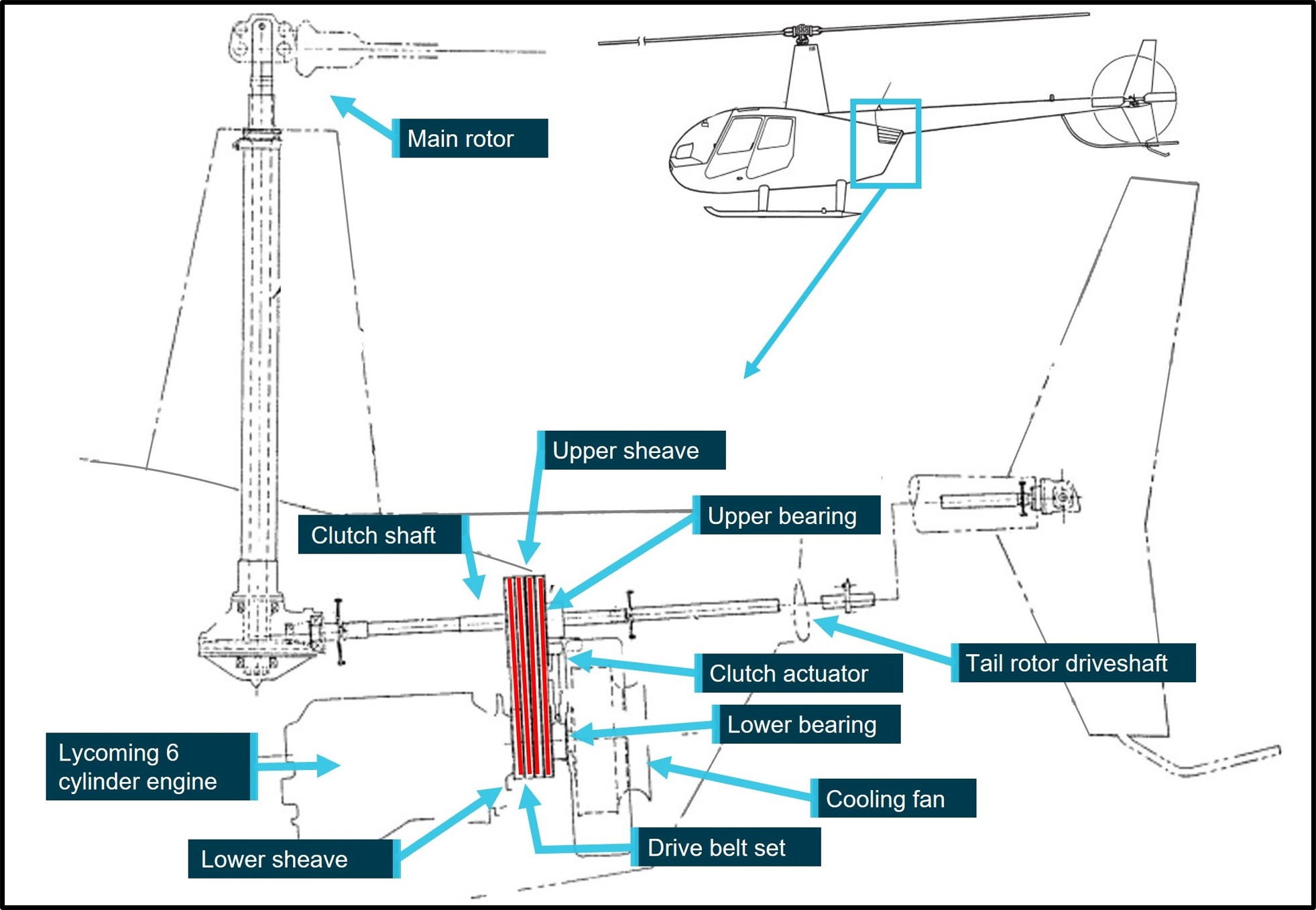
Source: Robinson Helicopter Company, annotate by ATSB
The electric clutch actuator (Figure 4) raises the upper sheave and tensions the V-belts. The actuator senses compressive load and switches off when the belts are properly tensioned. The ‘clutch’ caution light, located in the top left of the console, illuminates when the actuator is engaging, disengaging, or retentioning the V-belts. Regarding activation of the light, the pilot operating handbook (POH) stated:
If … the [clutch] light flickers or comes on in flight and does not go out within 10 seconds, pull CLUTCH circuit breaker and land as soon as practical. Reduce power and land immediately if there are other indications of drive system failure (be prepared to enter autorotation).
RHC Safety Tip 7 included:
A change in sound or vibration of the helicopter may indicate an impending failure of a critical component. If unusual sound or vibration begins in flight, make a safe landing and have aircraft thoroughly inspected before flight is resumed.
RHC Safety Notice SN-28
Listen for impending bearing failure included:
An impending ball or roller bearing failure is usually preceded by a noticeable increase in noise. The noise will typically start several hours before the bearing actually fails or before there is any increase in bearing temperature. To detect pending failure of a drive system bearing, the pilot should uncover one ear and listen to the sound of the drive system during start-up and shutdown. After the pilot becomes familiar with the normal sound of the drive system, he should be able to detect the noise of a failing bearing. The failing bearing will produce a loud whine, rumble, growl or siren sound…Failure of a bearing in flight could result in a serious accident.
Do not rely on telatemps to indicate impending bearing failure. A failing bearing may not run hot enough to black out the telatemps until it actually starts to disintegrate. This may occur only seconds before complete failure.
Clutch light warning
It is normal for the clutch light to come on occasionally in flight for a short time (approximately 3 to 6 seconds) to re-tension the drive belts. If the clutch light flickers or does not go out within 10 seconds, it can indicate a belt or bearing failure….
If additional symptoms of drive system failure (smell of hot rubber, noise or vibration) are present, land immediately. If tachometer needle split occurs, enter autorotation.
The operator advised they listened for sounds of bearing noises during the start-up and shutdown of the helicopter and had not detected any unusual noises or vibration. The accident pilot advised this was their first flight in VH-KOV this season and they had not noticed anything unusual during the flight.
Robinson Helicopter Company maintenance requirements
Periodic inspection
As part of a periodic inspection, a helicopter was subject to a ground inspection, engine run up and flight check. This included checking for ‘no unusual bearing noise when varying RPM through operating range (mechanic to listen near V-belt drive)’. These inspections were not included in the worksheet records however, the maintainer reported they were completed each time.
Lower bearing
The fan shaft assembly, including lower bearing had been replaced at the 2,200-hour overhaul. The periodic inspection checklist required:
Inspect as much of bearing as can be seen. Inspect fibreglass scroll area at bearing attachment brackets for signs of cracking. Check bearing seals for evidence of deterioration…Inspect bearing per Section 2.502 if discrepancies are found.
RHC required the bearing to be inspected as per section 2.502 whenever there was a bearing discrepancy, or the fan wheel was removed. Section 2.502 required removal of the fan wheel and disconnection of the clutch actuator from the lower bearing. The bearing was to be rotated by hand to ‘verify no roughness, scraping or excessive looseness’. In addition, there was a requirement to ‘verify no seal damage, no heat damage and lubricate as per Section 1.140’.
The lower bearing was to be lubricated as per Section 1.140 every 300 hours or 3 years, whichever came first, or as directed by 2.502. The procedure required 4–5 g of the specified grease to be injected, by syringe, into the bearing via a screw hole (Figure 4). A ground run was to be conducted at 102% RPM for 2 minutes. Following shutdown, the bearing was to be inspected and cleaned of escaped grease.
Upper bearing
There was no maintenance requirement to lubricate the upper bearing on the R44. In contrast, the upper bearing on the R22 was to be lubricated every 300 hours or 12 months. The R22 upper bearing lubrication procedure required a syringe be filled with 2–3 g of grease. The syringe tip was to be inserted against the ‘cleaned’ inner lip of the rubber seal and grease injected into the bearing. Once the syringe was removed, the deflected seal could be gently manoeuvred back into place.
VH-KOV bearing lubrication
A review of the maintenance records identified documented lubrication of both the upper and lower bearings (Table 2).
Table 2: Recorded lubrication of the upper and lower bearings
| Date | Hours since previous service | Description of maintenance conducted |
| 17 July 2015 | New bearings installed | |
| 11 October 2016 | 367.8 | Upper and lower bearing serviced |
| 25 April 2018 | 515.6 | Upper and lower bearing serviced |
| 16 May 2019 | 401.7 | Upper and lower bearing lube |
| 26 August 20 | 374.1 | The bearings were not specifically mentioned however, the 300-hour inspection included lubrication of the lower bearing |
| 12 May 2021 | 221 | Upper and lower bearing serviced |
| 30 July 2021 | 103.5 | Upper and lower bearing serviced |
The maintainer advised they greased the bearings more often that the 300-hour requirement as the grease used, Grease 28, is very thin and as the helicopters were operating in a hot environment ‘we like to over maintain our bearings because if we didn’t, they would run dry’. Further, the maintainer advised they did not always certify the additional greasing in the maintenance records and therefore the frequency could not be verified.
Considering the recorded lubrication intervals of the lower bearing, Robinson Helicopters stated:
We do not see damaged lower bearings in any significant numbers. The ones that do get reported, typically have a poor service history. Every instance of bearing damage is going to be different so it would be impossible to apply a timeline to complete bearing failure after an unknown amount of damage. These particular bearings appear to have gone over 1000 hours since the most likely time of damage (after the 515-hour interval) and it is highly likely that signs of damaged bearings existed (noise, actuator issues, grease outside the seals, rough running bearings, etc.). There are two occasions…where the scroll had been removed for actuator repair when the mechanic should have put his/her hand on the bearing and rotated it to feel for roughness and any grease on the lower sheave would have been right there in plain view.
When questioned on the method for lubricating the upper bearing, the maintainer stated that they used the same method as for the lower bearing, via the screw hole. However, the ATSB inspected the upper bearing and noted the telatemp was covering the screw, with no evidence of it having been accessed. Additionally, the seal on the upper bearing, which was a type of rigid polymer, showed distortion consistent with the R22 syringe lubrication method (Figure 7). The grease was found to be solid and dark in colour (Figure 8). RHC advised that typically after 2,200 hours of operating, the grease will be dark brown but not grainy or gritty.
Figure 7: Distortion to the upper bearing seal
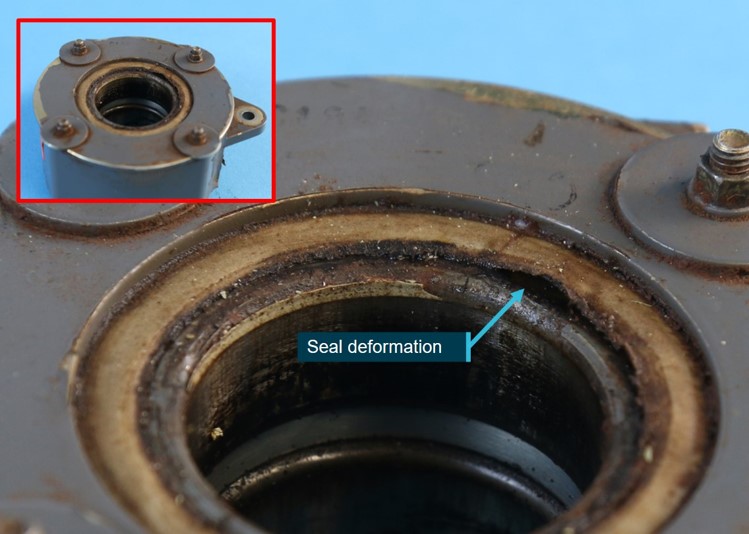
Source: ATSB
Figure 8: Grease found within the upper bearing

Source: ATSB
General provisions for lubricating bearings
Under-lubrication of a bearing can lead to over-heating due to the friction between the moving parts. However, lubricating more often than the procedures require can also result in over‑heating. When too much grease is added to the bearing cavity, it will result in the rotating bearing elements beginning to churn the grease and pushing it aside. This results in energy loss and rising temperatures. Over a long period of time, the grease will thicken into a hard, crusty build-up which can then impair lubrication and block new grease getting to the core. Excessive grease can also prevent heat from being dissipated, as the grease does not transfer heat from the load zone.
RHC advised the consequences of greasing more or less often than required was not specifically mentioned in the maintenance manual as it was considered to be a basic maintenance practice, which should be covered during initial training. RHC also advised that, lower bearing maintenance and troubleshooting was covered in their Robinson Helicopter factory maintenance course.
Troubleshooting
The maintainer had replaced 3 of the 4 microswitches for the clutch actuator at the last periodic inspection and 22 hours prior to the bearing failure (refer Table 1). Replacing the microswitches required that the fan wheel be removed and hence, as per the procedure, the bearing was required to be lubricated.
There was no information in the trouble shooting section of the RHC maintenance manual to advise that if the microswitches were being replaced, then the maintainer should inspect the bearing. However, RHC advised this information was covered in their Robinson Helicopter factory maintenance course.
The troubleshooting section for ‘clutch light flickers in flight’ included to check the upper and lower bearing for rough running however, the operator had not noted a flickering clutch light prior to the accident flight.
Emergency locator transmitter
The KANNAD 40 AF-Compact emergency locator transmitter (ELT) fitted to the helicopter consisted of a remote switch/annunciator, located in the cabin left of the cyclic, and a transmitter, located in the main transmission bay, and normally selected to ‘ARM’.[3] With the transmitter selected to ARM, the 3‑position remote switch/annunciator, with indicator light, operated as follows:
- ON – ELT activated
- ARM – permitted ELT activation when subjected to high ‘G’ load
- Test/RESET – allowed brief functional testing of the ELT or reset in case of inadvertent activation
- Light – red light illuminated when the ELT was transmitting.
The remote switch in the cabin was normally selected to ARM during flight.
During the helicopter inspection, the remote switch in the cockpit was found in the ON position. It was reported that the ELT unit was also found in the ARMED position after the helicopter was transported. There were no indications of damage to the battery. The ELT mount was found secured to the correct frame with the required Velcro mounting strap and additional secondary black cloth strap. The antenna was securely mounted under the cowl. Due to the discontinuity of the wiring after the helicopter was moved, the wiring was not examined.
The ELT did not activate when the accident occurred however, the signal was received by the Australian Maritime Safety Authority (AMSA) about 10 hours later. The ELT was not examined and therefore the reason for the delay in transmission could not be determined. AMSA was contacted and confirmed there were no areas in Australia where an ELT signal could not be detected by satellite. The accident was in a remote location and so interference by a person was considered unlikely. Despite this, interference by an animal or a change in the conditions were possible. There was no forecast rain in the area.
Robinson Helicopter Company ELT maintenance procedures
While optional on the R44, many were fitted with the Kannad automatic fixed 406AF ELTs. Due to the high frequency of fitment, the ELT was recorded as a periodic inspection item in Chapter 1 of the maintenance manual where it stated that United States (US)‑registered helicopters were required to be inspected every 12 months, in accordance with the Code of federal regulations (CFR) 91.207 Emergency locator transmitters. This regulation does not apply to helicopters, however RHC advised it was guidance for the inspection of an ELT for US‑registered helicopters.
The ELT was not recorded as an inspection item on the periodic inspection worksheets in Chapter 2 of the maintenance manual for the R44 helicopter. In contrast, the R22 and R66 helicopter periodic inspections did list the ELT in their periodic inspection worksheets however, the inspection was limited to ensuring the ELT was secure in its mount and would not foul the drivetrain.
Chapter 37 Electrical systems of the maintenance manual stated that the component manufacturer’s instructions should be followed to conduct maintenance.
ELT manufacturer maintenance procedures
The ELT manufacturer’s installation and operation procedures recommended that a self-test be conducted once a month and that it was mandatory that the batteries be changed:
- on or before the battery expiration date
- following 1 hour of real use
- use in an emergency, or
- inadvertent activation of unknown duration.
In addition, the manufacturer acknowledged that some national aviation authorities may require a periodic inspection. They provided service letter SL S18XX502-25-12 with guidance on periodic inspection procedures to satisfy requirements as directed by the US, Canada and Europe. The service letter also stated that all other countries should refer to the local regulations and it was ‘the responsibility of the customer (aircraft owner) to determine which tests are applicable to its ELT’.[4]
Australian maintenance requirements for ELT
Airworthiness Bulletin 02-002 Emergency Locator Transmitter (ELT) installation and maintenance stated that:
A periodic inspection of the ELT system should be carried out in accordance with approved data, which can include FAA AC 43 13-1B Chapter 12-22, if AC 43.13-1B is identified in the aircraft logbook statement as part of the aircraft maintenance data, or is otherwise identified or incorporated in an approved System of Maintenance.
The aircraft’s maintenance documentation stated that minor repair work should be conducted in line with AC 43.13-1B Acceptable methods, techniques, and practices – aircraft inspection and repair, however CASA confirmed that this does not include maintenance actions. CASA also advised Federal Aviation Regulations do not apply in Australia and therefore operators cannot maintain the ELT in accordance with FAR 91.207.
VH-KOV ELT maintenance history
The operator advised that they occasionally conducted a self-test on the ELT, which it always passed. They presumed the ELT was being maintained during the 100-hourly inspection conducted by the maintenance organisation.
The maintainer advised that they did not maintain ELTs as the helicopters they maintained either had the units removed or switched to OFF, as they would ‘randomly transmit’. They further advised that they would have informed the operator of VH-KOV that the ELT would not be maintained when they initially began to maintain the helicopter in 2016. The maintainer also stated that they endorsed the maintenance release to state that pilots are required to carry a personal emergency position-indicating radio beacon (EPIRB)[5] or satellite phone. The ATSB could find no record of this endorsement on the current or previous maintenance releases for VH-KOV.
The ATSB assessed the maintenance records and confirmed the ELT was serviced at the 2,200 hour major inspection on 17 July 2015. The only record of the ELT being inspected since then was on 2 occasions in 2018, when a different maintenance organisation conducted the periodic inspections. In addition, there was no note for the battery life in the maintenance records. An inspection of the ELT identified the battery had expired in March 2022.
At the time of the occurrence there was no regulatory requirement for VH-KOV to be fitted with an ELT (see the section titled Regulatory requirements around carriage of ELT). While optional, where it was fitted, it is important that a pilot is made aware of its operational status. Civil Aviation Advisory Publication (CAAP) 37-01 v5.1 Minimum equipment lists[6] included:
The operator or maintenance personnel must place the placard on or near inoperative equipment or instruments so that it is visible to the flight crew and alerts them to the inoperative equipment.
While the CAAP is only advisory, it represents best practice and an opportunity to ensure any pilot or maintainer is readily aware of the operational status of a component. There was no placard, or other notification, near the remote switch in VH-KOV to advise the ELT was not being maintained.
Inadvertent activation
AMSA was contacted to confirm if they had records of ELTs in Robinson Helicopters activating without cause. They advised that they were aware of the issue and considered it was due to:
- the position of the ELT switch between the front passenger seat and the pilot seat allowing accidental activation of the ELT switch when entering or exiting the aircraft.
- water ingress in the ELT assembly (the ELT is mounted inside the main transmission bay, which is not weatherproof). This was a regular and repeated event for Robinson helicopters.
RHC was contacted to see if they knew of any issues within the world fleet – they advised that one of their Australian repair stations confirmed they were aware of this issue. However, they advised there were no reports of issues in South Africa, Alaska or Canada other than ‘moving things in the cabin’ and hitting the switch.
The South African, US, and Canadian regulations require regular maintenance of the ELT unit.
The ELT manufacturer has advised that most inadvertent activations are due to water ingress in the wiring between the remote control panel and the ELT unit, however, this could not be verified.
Regulatory requirements around carriage of ELT
MOS Part 133 section 11.41 Carriage of ELTs required that a helicopter with more than 3 seats must be fitted with an automatic ELT. However, the transitional requirements allow operators to continue to operate under the previous legislation until 2 December 2023. The previous legislation, Civil Aviation Regulation 252A, permitted a helicopter on a flight within 50 NM from the departure aerodrome to operate without an ELT. As such, at the time, VH‑KOV did not require an ELT to be fitted.
The Mapping of Civil Aviation Regulations to CASR Part 91, 119 and 133-Australian air transport operations-rotorcraft identified this change to the legislation, however there is no mention of the change in the key operational changes document.
ELT effectiveness
Research conducted by the ATSB in 2013, A review of the effectiveness of emergency locator transmitters in aviation accidents identified that, while ELTs only activated in 40-60% of accidents in which their activation was expected, they were directly responsible for saving an average of 4 lives per year.
Operational considerations
Flight in a designated remote area
The flight was conducted in a designated remote area and as such was required to carry ‘survival equipment for sustaining life appropriate for the area being overflown’. The pilot reported that the helicopter had a survival bag which contained a first aid kit, extra food, water, satellite sleeve, mosquito dome, thermal blanket, and a signal mirror. However, passengers disputed that a first aid kit was available.
Legislation
On 2 December 2021, new legislation came into force that required charter operations to comply with Civil Aviation Safety Regulations (CASR) Part 91, 119 and 133 and the corresponding manuals of standards. This introduced a number of changes to the requirements for this operation type, some of which were notified by the Civil Aviation Safety Authority (CASA) to operators in a document highlighting the key operational changes. During the introduction period, there were some transitional exemptions in place to give operators time to comply. Some of the changes, discussed below, were relevant to this occurrence.
At the time of the accident, the operator’s procedures had not been changed to reflect the new regulations however, they had submitted an exposition, written by a third-party contractor, to CASA for approval. They also advised that they had an expectation that the new requirements did not come into effect until March 2023.
Safety briefing
In accordance with the Manual of Standards (MOS) Part 133 Chapter 7 Safety briefings, instructions and demonstrations, the pilot of a helicopter must provide passengers with a verbal safety briefing. With the introduction of the new legislation, the information required to be briefed had been updated and now included, among other new requirements, information on when and how to assume the brace for impact (brace) position. The changes to the briefing requirements were not included in the key operational changes document promulgated by CASA. The legislation was in transition and after 1 December 2022, required an operator to supply a safety briefing card to all passengers specific to the helicopter type and model, which included detail on how to assume the emergency brace position.
The inclusion of having to show passengers how to brace during the oral safety briefing, in a helicopter with more than 3 passengers and less than 6 seats, was a new requirement and CASR 133.240(3)(b) required that this be specific to the aircraft type and model.
CASA released a multi-part advisory circular (AC) 91-19, AC 121-04, AC 133-10, AC 135-12 and 138-10 version 1.0 Passenger safety information, coincident with the requirement to brief passengers on the brace position coming into effect. This AC was to give operators ‘guidance regarding the requirements for safety briefing cards and passenger safety briefings, instructions and demonstrations’. It stated that when passengers are informed about the correct use of equipment and the actions to take in the event of an emergency, including how to brace, the survival rate was improved. It also stated that bracing before impact reduces:
- flailing by having the forward-facing occupant flex, bend, or lean forward over their legs in some manner
- secondary-impact injuries by pre-positioning the body, predominantly the head, against the surface that it would otherwise strike during that secondary impact, thus reducing the momentum of the head and other parts of the body.
The AC included an appendix that provided information on the recommended brace positions for specific seat positions and restraint types. However, it did not indicate how to brace in a helicopter with a 3‑point harness (lap strap and shoulder harness with a single diagonal strap), as was the harness available in the R44. General guidance, applicable to all brace positions, in section A.2.1 of the appendix advised that:
- The lower torso should be firmly against the back of the seat.
- The lap strap portion of the seatbelt should be worn as tight and as low across the hips as possible. The more tightly the lap strap is adjusted, the better restraint it will provide.
- If the seatbelt includes a shoulder harness, the harness should be adjusted so that it is tight but does not pull the lap portion of the seatbelt upward.
- The webbing of a lap strap and shoulder harness should lie flat against the body and should not be twisted.
- Knees should be pressed together, and feet should be flat on the floor.
The US Code of federal Regulations Part 29 – Airworthiness standards: Transport category rotorcraft Subpart A 29.2 (a) required that a Category B rotorcraft[7] manufactured after 16 September 1992, was required to have a combined safety belt and shoulder harness with a single-point release. This requirement was also stated in section 27.785 (b) of the European Aviation Safety Agency CS-27 Certification specifications for small rotorcraft, which was released in 2003.
Advice was sought from CASA on how to brace in a helicopter with a 3-point harness, with the following response provided:
As detailed in A.3 of Appendix A to AC 133-10, there are a great number of variables affecting the brace position to be adopted. The AC aims to identify some general principles that will allow an operator to select an appropriate brace position in the context of their operation.
The information relating to brace positions contained in Appendix A of Multi-Part AC 133-10 is based on ICAO document 10086 Manual on Information and Instructions for Passenger Safety and Transport Canada Civil Aviation (TCCA) Advisory Circular TCCA AC 700-036 – Brace for Impact Positions for all Aircraft Occupants, which is also referenced in ICAO document 10086.
…Neither document (i.e., ICAO 10086 or TCCA AC 700-036) provide guidance on passenger brace positions for helicopters fitted with a 3-point harness.
RHC was contacted to seek advice on how best to brace using the harness in the R44. They advised that they do not have specific information on the brace position and recommended to use either the brace position in section A.2.1 of the AC or the brace position A.5 Forward-facing passenger seats fitted with a lap strap and single diagonal shoulder harness, which stated:
A.5.1 In a forward-facing passenger seat fitted with a lap strap and single diagonal shoulder harness, passengers should brace according to Figure 2 [Figure 9] below and comply with the accompanying instructions:
a. Adjust shoulder harness to remove slack.
b. Rest chin on sternum, head should be tucked down as far as possible to try to eliminate secondary impact of the chin with the sternum.
c. Hands can be positioned on the lap, front edge of the seat can be held (do not lock elbows or wrists), or occupant can sit on palms of their hands (palms must be ‘up’ to avoid breaking wrists). Do not hold on to restraint system with hands; this can introduce slack into the restraint system.
Figure 9: Diagram of how to brace in a forward-facing passenger seat with 3-point harness
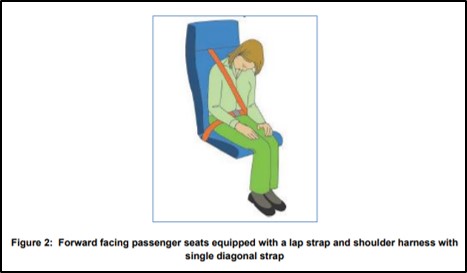
Source: CASA Multi-part advisory circular AC 133-10 Version 1.0
Transport Canada was also contacted in relation to the content contained within Canadian AC 700-036 and provided the following response:
Prior to the publication of AC 700-036, Transport Canada guidance had simply stated that ‘Helicopter occupant brace positions are the same as those for aeroplane occupants’, which was aligned with the guidance from the U.S. FAA at the time (i.e., AC 121-24C). During the development of the revised Canadian guidance in response to the recommendations contained in report DOT/FAA/AM-15/17, 2015-11-19 — Effect of Passenger Position on Crash Injury Risk in Transport-Category Aircraft, there was an identified need to provide guidance for helicopter occupants, specifically for those involved in offshore operations.
The focus was on offering guidance with respect to two specific configurations of passenger restraint systems: lap strap only and dual upper torso straps. As no new or unique recommendations were available or suggested for a helicopter passenger using a lap strap and diagonal shoulder strap (e.g., 3-point harness), the general guidance applicable to all aircraft passengers continues to be used for such a restraint system configuration (e.g., Sections 4.3 Forward-facing Seats Equipped with a Lap Strap and Shoulder Harness and 4.9 Aft-facing Seats Equipped with a Lap Strap and Shoulder Harness).
In the context of US operations, the Federal Aviation Administration (FAA) AC 121-24D Appendix 4 Brace-for-impact positions stated that:
Helicopter passengers … should adopt the same positions as recommended for aircraft seats of similar orientations and restraint system configuration; however, if possible, the occupants of all seat types should grip the edge of the seat pan, to help maintain orientation in the event of a rollover.
Both the pilot and the operator advised that they briefed passengers on how to brace in the event of an emergency. The operator advised they would advise passengers ‘not to lean forward’ and ‘always to sit up with a straight back’.
Safety brief prior to accident flight
On the morning of the accident flight, VH-KOV had been flown for 3–4 hours prior to arriving at Lorella Springs, as the operator’s second R44 had a minor fault. This resulted in the passengers waiting for the helicopter to arrive.
The passengers all reported they did not receive a safety briefing prior to the flight. However, they advised that they understood how to fasten the 3-point harness, their hand luggage was stored securely, and the operation of the headset was discussed with the pilot. When questioned sometime after the accident, the pilot advised they did not remember completing the briefing but would find it odd if they had not done so. They advised that normally their pre-flight briefing included:
- avoiding the tail rotor
- trip hazards such as skids
- how to get in and out of the helicopter
- door operation
- seatbelt operation
- no smoking
- not to interfere with controls
- brace position.
However, they also advised feeling slightly rushed due to the late arrival of the helicopter and that they were concentrating on checking the helicopter, refuelling, completing a fuel drain and checking the oil levels.
The passengers all commented that when the pilot called ‘brace’ prior to the accident, they did not know how to do so.
Pilot leaving controls
Prior to take-off, the passenger in the rear left seat could not close their door securely. In response, the pilot exited the helicopter, leaving the engine running and walked around to the left side to secure the door. The operator’s operations manual stated that:
the pilot-in-command must remain at the controls … from the time at which the engine is started prior to a flight, until the engine is stopped at the termination of a flight unless … the helicopter is fitted with a serviceable means of locking the cyclic and collective controls and … the pilot considers that their absence from the cockpit is essential to the safety of the helicopter...
The operator confirmed the helicopter had no modifications for locking the cyclic or collective.
The R44 is equipped with adjustable friction on the cyclic and collective, to allow a pilot to elect their desired level of force required to manipulate controls. This may be adjusted to suit conditions such as long flights, turbulence etc. These friction devices do not lock the controls and as such, RHC safety notice 17 stated:
NEVER EXIT THE HELICOPTER WITH THE ENGINE RUNNING
CASA had also advised in a previous ATSB investigation that a friction lock was not a substitute for a locking device.
CASR Part 91.550 (b) Seating for flight crew members required that at all times during the flight, ‘a pilot must occupy a pilot seat with the seatbelt securely fastened’. Where previously there was an exemption that a pilot of a helicopter could exit the cockpit if the helicopter had a means of locking the cyclic and collective, this exemption has been repealed.[8]
Operations manual
The operator’s operations manual, written by a third party, required that prior to boarding the helicopter the passengers be shown a helicopter safety card which provided information on how to enter and exit the helicopter when the rotors were turning. The passengers advised they did not receive a briefing on how to do this. One of the passengers reported that when they landed at the various stops, they were advised to leave the helicopter ‘going forward’. They exited the helicopter after landing while the rotors were turning at 2 landing sites carrying their fishing rods, and a third site, while the pilot allowed the helicopter engine to cool down.
Weight and balance
The operator’s operations manual stated that load calculations were to be made with actual weights for all passengers and baggage, using the loading form from the flight manual, however it then stated that a pre-calculated load and trim sheet could be used but may only be prepared by the chief pilot. The pilot advised they regularly use the pre-calculated weight form and an application on their electronic flight bag to calculate the weight and balance for the helicopter. The passengers advised they submitted their actual weights to the operator before the flight.
The ATSB assessed that the helicopter was operated within the weight and balance requirements for the flight.
Emergency equipment
Fire extinguisher
There was no fire extinguisher on the helicopter and the operator advised they did not carry one as they considered that if a fire started in flight, they would land immediately and exit the helicopter. However, their operations manual required that a portable fire extinguisher be carried on all flights.
Prior to December 2021, an airworthiness directive (AD/general/65 amendment 4) required that all aircraft with a maximum take-off weight of greater than 2,750 kg carry a fire extinguisher. The R44 does not fit into this category. CASA did recommend in AWB 26-002 Issue 3 Selection and Installation of Handheld Portable Fire Extinguishers, that all aircraft have at least one fire extinguisher accessible to a pilot.
Manual of standards Part 133 section 11.46 Hand-held fire extinguishers required that a rotorcraft must carry at least 1 hand-held fire extinguisher. However, the removal of the weight limit was not identified in the CASR Part 133 Key operational changes document. CASA advised this change was stated in the information they released to assist operators to write an exposition and had been discussed in early consultation with operators.
First aid kit
Satellite sleeve
The operator advised that they used a satellite sleeve rather than a satellite phone in their operations. A satellite sleeve connected the user’s mobile phone to the satellite system and allowed them to make phone calls and send text messages. The operator advised that on the 20 April 2022, the unit was tested and found to be fully charged and operational. It was then switched to OFF and stored in a pouch on the helicopter.
The pilot had received training on how to use the unit and had the required application on their phone. Additionally, when the application is opened on a mobile phone, it provided simple instructions on how to use the device. The unit was tested after the accident and, while fully charged, it was not operational for unknown reasons.
Related occurrences
The ATSB identified two previous occurrences where the clutch actuator lower bearing had failed.
ATSB investigation 19905646
On the 25 November 1998, about 20 minutes after take-off, the pilot noticed a burning smell, and felt a slight shudder closely followed by the helicopter’s clutch light flickering. The pilot landed the float‑equipped helicopter on water with minimal impact forces.
The subsequent investigation revealed the fan shaft bearing located on the fan shaft between the engine and the cooling fan had overheated, melted and seized resulting in the shaft fracture. The examination by RHC revealed the lower actuator bearing lost lubrication after 926.4 hours of service, however they were unable to establish why this occurred with a distorted seal, loss of grease and water ingress considered the most likely sequence of events.
Aviation accident summaries ERA16LA216
The second failure occurred in the US in 2016, where 2 people were seriously injured. The helicopter was over a saltwater pond, about 300 ft above ground level. At that time, the pilot felt a lateral shudder followed by the clutch light illuminating. The helicopter then began a violent yaw and the low oil pressure light illuminated. The pilot performed an autorotation to shallow water near the shoreline.
Examination of the airframe revealed that the engine cooling fan had separated with the lower sheave being caked in grease, consistent with grease leaking from the clutch actuator lower bearing for a significant time. The roller bearings were found seized with no grease recovered. The investigation found that the times in the aircraft maintenance documentation had been incorrectly recorded. Consequently, the helicopter had not been maintained in accordance with procedures and the airframe major overhaul was due 59.5 hours prior to the accident. The lower bearing would have been replaced during this overhaul. Also, the lower bearing had not been serviced in accordance with procedures. While the bearing had been lubricated annually in the 2 years preceding the accident, there was no recorded servicing during a period of 4 years 11 months and 685.1 hours prior to this.
Safety analysis
Introduction
While flying at about 500 ft above a valley floor, the helicopter started to vibrate and within seconds, the clutch actuator lower bearing failed. This resulted in a loss of drive to the main and tail rotors and it is possible the engine stalled as it was unloaded. As the helicopter was flying over rising terrain, the pilot had very few recovery options, and they conducted an autorotation into trees resulting in serious injuries to 2 passengers and minor injuries to the remaining passenger and the pilot. The helicopter sustained substantial damage.
This analysis will consider the factors around the seizure of the lower bearing, passenger briefing, the introduction of new legislation by the Civil Aviation Safety Authority, and the issues around the maintenance of emergency locator transmitters (ELTs) in Australia.
Lower bearing seizure
The investigation identified that the lower bearing seized, resulting in the failure of the fan shaft. The maintainer advised that they had checked the bearing for roughness during maintenance about 20 flight hours prior to the accident and did not detect any issues. Additionally, the operator advised they regularly listened for unusual noises in the drive train as they shut down the engine, and none had been detected. On the day of the occurrence, the helicopter had been operated for approximately 5.1 hours, including several engine shut-downs, with neither pilot identifying anything unusual prior to the sudden failure of the bearing.
After the occurrence lower bearing was installed at the major inspection, the time between lubrication was initially greater than the required 300 hours. However, in more recent times, the maintainer advised they were lubricating the bearing more frequently than required as they felt this was warranted in the hot operating environment. In addition, the lower bearing was to be lubricated every time the fan wheel was removed, which had the potential to result in more frequent lubrication. However, the fan removal also afforded the opportunity for thorough inspection of the lower sheave.
Robinson Helicopter’s assessment was that bearing damage that ultimately led to failure most likely occurred during the period of initial under‑lubrication following fitment. They further advised that signs of bearing damage, including:
- noise
- rough running bearings
- actuator issues
- grease outside the seals
should have been evident. As detailed above, no noise or roughness was identified, but the accumulation of dried grease on the lower sheave indicated that grease had been leaking past the seal and/or over greased for an extended period. The bearing was also reaching the end of its service life.
Distortion to the upper bearing seal was consistent with that bearing being lubricated despite there being no procedural requirement to do so. Further, inspection identified that the grease was solid and therefore not likely to have been effectively lubricating and cooling the bearing.
Due to the extent of the damage to the lower bearing, the specific reason for its failure could not be identified. However, the available evidence indicates it was probably due to the inconsistent lubrication of the bearing. Both lubricating the bearing more and less often than required by the procedures can result in damage. Not following the maintenance procedures increases the likelihood of the bearings failing prior to their service life. Further, such failures can occur at a critical phase of flight, where the opportunity for a successful forced landing may be reduced.
The RHC maintenance procedures did not specify that the lower bearing should not be over lubricated and included a requirement to lubricate the bearing every time the cooling fan was removed, which was required when the clutch micro switches were replaced. The procedures also did not identify, in the trouble shooting section, that frequent changing of the micro switches could be an indication that the lower bearing was failing.
Passenger briefing
The passengers did not receive a safety briefing prior to the flight, which resulted in them being unaware of the safety equipment in the helicopter. Having knowledge of what is available, and how it is used, is important in the event of an emergency, especially if the pilot is incapacitated and/or the flight is in a designated remote area. Fortunately, this did not affect the outcome on this occasion as the operator responded quickly when the helicopter did not return after the SARTIME had elapsed.
Although not related to the accident, the passengers also did not receive a specific briefing on how to leave the helicopter with the rotors turning. Landing in a remote area, with no ground staff and unknown/undulating terrain levels, increases the risk of passengers inadvertently walking into the rotor arcs. They were also carrying fishing rods, which added to the risk level. According to the United States (US) Federal Aviation Authority (FAA) Helicopter flying handbook, ‘People have been injured, some fatally, in helicopter accidents that would not have occurred had they been informed of the proper method of boarding or deplaning’.
Another result of not receiving a safety brief was that the passengers were not given any information on how to brace during the accident. While all 3 passengers advised they did not know how to brace, it is difficult to assess if their injuries were increased as a result of not being briefed. An accident of this nature, where the helicopter falls through trees and spins, introduces many forces which cannot be foreseen when designing a general brace position. It is also very difficult to assess which people will adopt the demonstrated brace position when faced with an emergency.
Regulatory change management
Despite the variables outlined above, research has shown that knowledge of the appropriate brace position offers the best chance to reduce injury. As such, it is now a requirement that during the passenger safety briefing prior to a flight, passengers are informed of the brace position specific to the aircraft type. Despite that, this requirement, along with other new requirements for the passenger safety brief, for operators of smaller helicopters, were not identified in the document released by CASA to advise operators what had changed with the introduction of new regulations.
Also, the multi-part Advisory Circular (AC), released by CASA to give operators guidance for safety briefing cards and passenger briefings, did not give specific advice on how to brace in a helicopter with a 3-point harness. This harness type is used extensively in helicopters flying in Australia, including the R44.
The helicopter did not have a fire extinguisher on board, contrary to the operator’s operations manual. If, as on this occasion, operators are using a third party to write their exposition, it is vital that they have a full understanding of what is written to ensure they are complying with their own company procedures.
A fire extinguisher is now mandatory in all helicopters operating under the Civil Aviation Safety Regulation (CASR) Part 133. The change to this requirement for helicopters weighing less than 2,750 kg was also not stated in the document released to advise operators around the changes to the regulations.
As these were relatively small wording changes as part of the introduction of extensively revised regulations, they could be overlooked by an operator.
ELT maintenance procedures
The ELT fitted to VH‑KOV did not activate until many hours after the ground impact. The maintainer had not maintained the unit since taking over the aircraft maintenance and had not advised the operator of this. However, as the unit eventually operated, it was likely serviceable.
The Robinson Helicopter Company (RHC) maintenance manual Chapter 1-General stated that US registered helicopters should be maintained in accordance with FAR 91.207. This regulation, however, applied to airplanes only. The statement was also unclear as to how helicopters based outside the US were to be maintained. In addition, Chapter 2 - Inspections did not list a procedure for an inspection of the ELT, although inspections were listed for both the R22 and R66 helicopters. These inspections listed requirements to ensure the ELT unit was secure in the helicopter rather than ensuring it was operational.
The maintenance requirements from the ELT manufacturer required that the battery be changed when required and recommended that a self-test be conducted monthly. If the ELT had been placarded as not being maintained, this may have prompted the operator to have performed a self-test of the unit on a regular basis. As the self-test was a recommended procedure, it is not required to be written in any maintenance documentation. As such, it is likely an operator/pilot could be unaware of the procedure. An investigation conducted by the ATSB –AO-2021-020 Wirestrike and collision with terrain involving Robinson R22, VH-KLY 75 km west-north-west of Hay, New South Wales on 26 May 2021– is an example of where the pilot had selected the ELT remote switch in the cockpit to ARM, however, the ELT was selected OFF at the unit. If the pilot of VH‑KLY had conducted a self-test of the unit, they would have realised that the unit was not operational.
The CASA Airworthiness Bulletin (AWB) 02-002, released on 15 November 2013, recommended that maintainers conduct maintenance on the ELT in accordance with approved data. However, as is the case for this helicopter, the approved data only required the operation of the unit to be checked when the batteries were replaced. This could result in the unit’s operational status only being ascertained every 6-7 years.
As shown in the ATSB research report, A review of the effectiveness of emergency locator transmitters in aviation accidents, ELTs in Australia only activate in 40-60% of accidents, but are effective in saving lives. Additionally, and as confirmed by AMSA, ELT units in Robinson Helicopters also activate erroneously. The lack of a formalised maintenance requirement may contribute to this.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the to the clutch actuator lower bearing seizure and collision with terrain involving Robinson Helicopter R44, VH-KOV on 16 May 2022.
Contributing factors[9]
- During cruise flight, the clutch actuator lower bearing seized resulting in a total loss of drive from the engine to the rotor system. The subsequent autorotation and collision with terrain over an inhospitable area, resulted in serious injuries to 2 passengers and minor injuries to the pilot and remaining passenger.
- The clutch actuator lower bearing was not being maintained in accordance with the manufacturer’s maintenance procedures, which likely resulted in the bearing failure.
Other factors that increased risk
- The passengers did not receive a pre-flight safety brief resulting in them being unaware of the emergency procedures, safety equipment and brace position. They also exited the helicopter prior to the accident while the rotors were turning, without a specific briefing.
- There was no fire extinguisher on board the helicopter. While this did not influence the outcome in this case due to the absence of post‑impact fire, it reduced the overall safety of the flight.
- As part of the regulatory changes to Civil Aviation Safety Regulation Part 133, the Civil Aviation Safety Authority changed the regulations relating to the carriage of fire extinguishers and passenger briefing. These safety‑related changes were not promulgated to operators in documentation related to the regulatory changes.
- Civil Aviation Safety Regulation Part 133 required that pilots brief passengers on the emergency brace position with information specific to their aircraft type and model. However, while the Civil Aviation Safety Authority provided guidance on how to brace in some configurations, they did not provide specific information on how to brace in a helicopter, like the R44, which had a 3-point harness.
- The emergency locator transmitter did not activate until 10 hours after the accident, reducing the likelihood that the helicopter’s occupants would be found in a timely manner.
- The emergency locator transmitter was not being maintained and the maintainer had not advised the operator.
- The Robinson R44 maintenance manual did not give clear guidance on how an emergency locator transmitter (ELT) should be maintained in aircraft outside the United States (US) and there was no procedure for inspecting its security. The US regulations referred to aeroplanes only and so there is no regulatory requirements to maintain an ELT in the US.
- The Civil Aviation Safety Authority did not provide clear guidance on how emergency locator transmitter units should be maintained.
- The emergency locator transmitter (ELT) manufacturer Kannad’s maintenance procedures stated that the monthly self-test of the ELT unit was recommended rather than required, which could result in the unit’s operation only being ascertained every 6-7 years. Current regulations do not mandate such a test.
Safety actions
|
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out. |
Safety action by the involved maintainer
The maintainer of the helicopter involved contacted each of the operators of the helicopters they maintained to ensure they were aware that the emergency locator transmitter (ELT) was not being maintained and to ensure they were carrying a personal locator beacon in the helicopter.
Safety action by the Civil Aviation Safety Authority addressing the guidance on how to brace in a helicopter with a 3-point harness
The Civil Aviation Safety Authority has released multi-part advisory circular (AC) 91-19, AC 121-04, AC 133-10, AC 135-12 and 138-10 version 1.1 Passenger safety information to include information on how to brace in a helicopter with a 3-point harness.
Safety action by the Civil Aviation Safety Authority addressing the guidance on emergency locator transmitter (ELT) installation and maintenance
The Civil Aviation Safety Authority has updated airworthiness bulletin (AWB) 02-002 to include information on ELT maintenance and guidance if the information contained within the aircraft’s maintenance schedule is not sufficient.
Safety action taken by Orolia the manufacturer of the emergency locator transmitter (ELT)
The manufacturer of the ELT has advised that the discrepancy between the service letter and the installation manual will be corrected to reflect that the self-test should be a recommended practice as the current regulations do not require a self-test.
AMSA Australian Maritime Safety Authority
AWB Airworthiness bulletin
AC Advisory Circular
AD Airworthiness Directive
CAAP Civil Aviation Advisory Publication
CASA Civil Aviation Safety Authority
CASR Civil Aviation Safety Regulations
CAR Civil Aviation Regulations
ELT Emergency locator transmitter
FAA Federal Aviation Authority
MOS Manual of Standards
POH Pilot operating handbook
RHC Robinson Helicopter Company
SL Service letter
US United States
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- pilot of the accident flight
- passengers
- operator
- maintainer
- Australian Maritime Safety Authority
- Civil Aviation Safety Authority
- Robinson Helicopter Company
- photographs taken on the day of the accident
- Transport Canada.
References
ATSB research report, A review of the effectiveness of emergency locator transmitters in aviation accidents, May 2013, Australia
Airworthiness Bulletin 02-002 Emergency Locator Transmitter (ELT) installation and maintenance, November 2013, Australia
CASA (Civil Aviation Safety Authority) multi-part Advisory Circular (AC) 91-19, AC 121-04, AC 133-10, AC 135- 12 and 138-10 version 1.0 Passenger safety information, August 2021, Australia
Transport Canada Advisory Circular (AC) 700-036 Brace for impact positions for all aircraft occupants, Issue 1, September 2016 Canada
FAA (Federal Aviation Authority) Advisory Circular 121-24D Appendix 4 Brace-for-impact positions, May 2019 United States
FAA (Federal Aviation Authority) Helicopter flying handbook, United States
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- pilot of the accident flight
- operator
- maintainer
- Australian Maritime Safety Authority
- Civil Aviation Safety Authority
- United States National Transportation Safety Board
- Robinson Helicopter Company
- Transport Canada.
- Bureau d'Enquêtes et d'Analyses (France)
- Orolia SAS
Submissions were received from:
- pilot of the accident flight
- operator
- maintainer
- Civil Aviation Safety Authority
- Robinson Helicopter Company
- Bureau d'Enquêtes et d'Analyses (France)
- Orolia SAS
- Transport Canada
- passengers
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Draft investigation report submission from the helicopter maintainer
The helicopter maintainer’s representative requested that their submission be attached to the report. As such, the following document is appended:
Introduction
We note that the ASTB has prepared a draft report in relation to a clutch actuator lower bearing seizure and collision with terrain involving Robinson Helicopter Company, R44, VH-KOV near Nathan River Station, Northern Territory on 16 May 2022. The following is a submission pursuant to section 26 of the Transport Safety Investigation Act 2003 on behalf of the “maintainer” referred to in that report.
We note that s.25(3) of the Act includes that, “A published report may include submissions that were made by persons to the ATSB in response to a draft report... “. We further note that s.12AA(1)(c)(i) of the Act provides that the ATSB's function is to improve transport safety by means that include identifying factors that contribute, or have contributed, to transport safety matters. This submission is intended to assist the ATSB in identifying factors that may have contributed to this incident.
The draft report
The Executive Summary for the draft report includes that, “The ATSB found that during cruise, the clutch actuator lower bearing seized resulting in a total loss of drive from the engine to the rotor system. This bearing had not been maintained in accordance with the maintenance procedures, which likely resulted in its failure.” We submit that theory is drawn from certain assumptions, which assumptions may need revision in light of certain objective facts. We further submit that the objective facts suggest another factor may have contributed to the incident.
Page 5 of the draft report states that, “Examination of the aft face of the lower sheave revealed accumulated grease consistent with it extruding past the lower bearing seal over a period of time. The maintainer reported wiping the sheave clean each time they worked on the helicopter however, the accumulated grease was not consistent with this having occurred in the last 10 days or 22 hours of operation. The fan shaft failed at the location of the lower bearing. The shaft exhibited deformation, necking, and gouging consistent with localised frictional heating. Circumferential scoring on the fracture surface was a result of the powered shaft contacting the bearing housing.”
At page 22 of the draft report it is then stated that, “The accumulation of dried grease on the lower sheave indicated that grease had been leaking past the seal and/or over greased for an extended period.” The opinion that the dried grease was an accumulation of residue from a prolonged period of over-lubrication is, with respect, incorrect.
Firstly, to the use of the term “over-lubrication” is a mischaracterisation of the increased maintenance conducted by the maintainer. While additional events of lubrication occurred, they did not involve an application of excess lubricant so as to cause extrusion of that excess such as would cause a residue to accumulate. The process by which the maintenance is conducted and the components themselves limit the volume of lubricant that may be applied and do not result in residual lubricant remaining present.
Secondly, the as noted at page 4 of the draft report indicates, the components examined by the ATSB were apparently inspected approximately 126 days after the incident: “The ATSB did not attend the accident site. The helicopter was partly disassembled on site, including engine removal, and transported to Queensland for examination. Engine and airframe examinations were conducted between 19–21 September 2022.” That period between the incident and examination, during which the components in question were left undisturbed, does not appear to be accounted for in the draft report observations about the extent to which a “minimal dried grease” was observed on the lower actuator bearing housing (page 8, Figure 5).
Thirdly, the draft report does not account for the possibility that a “minimal” amount of lubricant may have escaped into the housing after the failure, at which point the components would have been super-heated due to the friction generated in the incident, which heat may have then caused the lubricant to dry out between the incident and the inspection 126 days later.
Fourthly, while the Executive Summary of the draft report states that, “During cruise flight, vibrations were detected through the helicopter, subsequently the pilot observed the engine RPM rise and then drop to zero”, the body of the report provides relevant additional details:
i. At page 1, the draft report notes that, “The pilot reported that, as the helicopter re-crossed the valley to return to the main house, they detected a burning smell and recalled that within a couple of seconds the engine began to run roughly.”
ii. At page 2, the draft report then notes that, “As the pilot lowered the collective to reduce power, in case the engine failed, they checked the engine oil temperature, pressure and cylinder head temperature gauges, which were all in the normal range. Within about 3 seconds, the vibrations through the helicopter increased. The pilot observed the engine RPM suddenly rise, then drop to zero and assessed that the engine had failed.”
iii. At page 9 the draft report notes that, “The operator advised they listened for sounds of bearing noises during the start-up and shutdown of the helicopter and had not detected any unusual noises or vibration.”
The theory that dried grease accumulated over time from over-lubrication and caused the bearing to fail appears to be borne out of the opinion that what is depicted in Figure 5 is an accumulation of dried grease from over-lubrication. Without that opinion, another source for failure must be considered.
The observations of those onboard do not require a conclusion that the causative event initiated from over-lubrication. Another possibility is that the lower fan shaft failed first, leading to a disruption of the bearing, ultimately leading to seizure, which seizure then expelled a quantity of lubricant which was super-heated and subsequently dried before being examined. This possibility is consistent with the observations of those onboard.
The clutch actuator lower bearing engages the main rotor. Seizure means an automatic loss of drive. Another possibility is that the bearing, which was nearing the end of its serviceable term, spontaneously failed and caused the seizure. Seizure as a result of spontaneous failure could, given the damage observed, have resulted in the expulsion of the lubricant that was subsequently observed in Figure 5 as “minimal dried grease”.
At page 5 of the draft report it is said that, “The maintainer reported wiping the sheave clean each time they worked on the helicopter however, the accumulated grease was not consistent with this having occurred in the last 10 days or 22 hours of operation.” Thus the observation of “minimal dried grease” is offered as a reason for rejecting the maintainer’s evidence. However, since the maintainer’s evidence is otherwise uncontradicted and unchallenged, the “minimal dried grease” may be seen as consistent with having in fact resulted from the seizure, rather than being the cause of it.
Further evidence that the incident may have originated with the lower fan shaft (and note due a residue of dried grease which the maintainer says was not present prior to the incident) comes from the condition of the clutch actuator observed in Figure 4 on page 7 of the draft report. Close examination of Figure 4 reveals that the clutch actuator is in an over-travel state with the tension spring damaged. It is also apparent that the fan shaft has failed from the lower bearing inner race spinning and creating excess heat, which heat would then have transferred to the lower bearing, which by failure would have super-heated the lubricant upon seizure would have expelled it to where it was then observed 126 days later.
We submit that what can also been seen in the photo of the lower bearing inner race is abrasions that may have been caused from excessive clearance between the fan shaft and lower bearing inner race. If the failure originated in connection with the fan shaft, what appears as scoring on the fan shaft may be linked to weakening and shearing. We note that the lower bearing, fan shaft and fan dropping down into the fan scroll would have released drive belt tension, causing an engine over speed and loss of drive to the main rotor transmission. This is consistent with the observations of those onboard, reported at pages 1 and 2 of the draft report:
“The pilot reported that, as the helicopter re-crossed the valley to return to the main house, they detected a burning smell and recalled that within a couple of seconds the engine began to run roughly”; and
“As the pilot lowered the collective to reduce power, in case the engine failed, they checked the engine oil temperature, pressure and cylinder head temperature gauges, which were all in the normal range. Within about 3 seconds, the vibrations through the helicopter increased. The pilot observed the engine RPM suddenly rise, then drop to zero and assessed that the engine had failed.”
We submit that these alternatives – the incident arising from a failure of either the fan shaft or the bearing should be included in the final report. We further submit that the characterisation of the maintainer’s increased frequency of lubrication as “over-lubrication” is not correct.
The specifications for a 12-month, 100 hourly check in section 2.140 of the manual, under item 7, states that if any discrepancies exist the maintainer is to inspect the bearing in accordance with section 2.502. That section then directs to section 1.140, which instructs the maintainer to lubricate the bearing with 4-5 grams of grease. Similarly, in section 2.501, it states that if any discrepancy is suspected, or the fan is removed, to proceed in accordance with section 2.502 and section 1.140, which is to lubricate the bearing with 4-5 grams of grease. In addition, in table 1 scheduled maintenance inspections it is stated that the maintainer is to grease the bearings in accordance with section 1.140, i.e. with 4-5 grams of grease every 300 hours or 3 years. Each of these grease applications is for the same amount – 4-5 grams. That is the prescribed volume on each occasion. The application of that amount, in accordance with the manual is, by definition, not over-lubrication.
In addition, because the bearing is a greaseable bearing and not a non-greaseable sealed bearing, Section 1.140 bearing lubrication instructs the maintainer to ground run the machine at 102% for 2 minutes after lubrication, and to then shut down and wipe any escaped excess grease. By following this procedure on each occasion the maintainer has not over-lubricated and has prevented any accumulation of residue.
Conclusion
Maintenance in accordance with the manual includes re-lubrication of the bearing every time the fan comes off. Given the various occasions for removal of the fan, the manual indicates re-lubrication of bearing could be, for example, as frequent as every 100 hours or whenever additional work is carried out that requires removal of the fan. The procedure for re-lubrication ensures that “over-lubrication” does not result. The hypothesis that the bearing seized due to “over-lubrication” by the maintainer therefore is, with respect, not correct.
We submit that the ATSB should consider instead the two alternative hypotheses: that the bearing near the end of its serviceable life spontaneously failed, or the incident independently arose due to some unspecified failure in the fan shaft. We also request that this submission should be included with the final report in accordance with s.25(3) of the Act.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] A device used to connect mobile phones to the satellite system.
[2] A SARTIME is the time nominated by a pilot for the initiation of Search and Rescue (SAR) action.
[3] Selecting the ELT transmitter to OFF is only recommended for maintenance, storage and shipment. The ELT can also be activated by selecting the transmitter to ON
[4] The service letter, in contradiction to the installation procedures, stated that the monthly self-test was a requirement, however the manufacturer advised this is not the case.
[5] Emergency position-indicating radio beacon: A type of emergency locator beacon used to locate people in need of immediate assistance.
[6] The minimum equipment list (MEL) is a list which provides for the operation of aircraft, subject to specified conditions, with particular equipment inoperative. It is prepared by an operator in conformity with, or more restrictive than, the manufacturer’s MEL established for the aircraft type.
[7] Rotorcraft with 1) a maximum weight of 20,000 pounds or less and 2) 9 or less passenger seats may be type certificated as Category B rotorcraft.
[8] CAO 95.7 – exemption from the provisions of the Civil Aviation Regulations 1998 – Helicopters (12/12/2004) was repealed on 2 December 2021.
[9] The helicopter maintainer disagreed with the contributing safety factors identified by the ATSB and requested that their submission be included in the final investigation report in accordance with s.25(3) of the Transport Safety Investigation Act 2003 (Appendix A).