
Executive summary
The ATSB conducts 'no-blame' investigations for the purpose of improving transport safety. ATSB investigations are independent of other investigations, including those conducted by the Civil Aviation Safety Authority and the Northern Territory Police Force.
What happened
On 28 February 2022, at about 0900 local time, a pilot and an egg collector were preparing to commence crocodile egg collection activities near King River, Northern Territory, using a Robinson R44 Raven II helicopter, registered VH-IDW and operated by Helibrook. The activity was conducted under a Civil Aviation Safety Authority (CASA) instrument authorising the pilot to carry a sling person (egg collector) on a 100 ft line attached to the helicopter.
At 1024, the crews of 2 other R44 helicopters collecting crocodile eggs nearby became concerned that they had not heard any communications from the crew of VH-IDW, which they reported was unusual. One of those helicopters returned to the area where VH-IDW was last seen and, at 1036, the search pilot found the fatally injured egg collector on the ground, wearing their harness and attached to the sling line, which was disconnected from the helicopter. The helicopter had collided with terrain 44 m beyond the sling person, and the pilot lay beside the helicopter having sustained serious injuries.
The ATSB referred matters concerning possible offences under the Transport Safety Investigation Act 2003 relating to the status of evidence available to the ATSB for the purposes of its 'no-blame' safety investigation to the Australian Federal Police for investigation. The referral did not concern the circumstances of the accident itself. The Australian Federal Police referred the matters to the Northern Territory Police as part of its broader investigations.
What the ATSB found
The ATSB found that the helicopter was likely not refuelled at the en route fuel depot, which was about three quarters of the way between the departure location on the outskirts of Darwin and a clearing near King River where the helicopter and crew were to commence crocodile egg collecting. The pilot did not identify the reducing fuel state before the helicopter’s engine stopped in flight due to fuel exhaustion. During the subsequent autorotation, the pilot released the egg collector above a likely‑survivable height, fatally injuring them. The pilot then completed the autorotation to the ground, but there was insufficient main rotor energy to cushion the landing. This resulted in serious injuries to the pilot and substantial damage to the helicopter.
The ATSB found that Helibrook’s CASA-approved safety management system was not being used to systematically identify and manage operational hazards. As a result, the risks inherent in conducting human sling operations, such as carriage of the egg collector above a survivable fall height, were not adequately addressed.
The ATSB also found that CASA did not have an effective process for assuring an authorisation would be unlikely to adversely affect safety. As a result, CASA delegates did not use the available structured risk management process to:
- identify and assess risks
- ensure suitable mitigations were included as conditions of the instrument
- assess the effects of changes on the overall risk.
This resulted in removal of instrument conditions limiting the height, speed and exposure for the sling person, which permitted carriage of the egg collector at a non‑survivable fall height.
In addition to the above contributing factors to the accident, the ATSB identified the following factors that increased risk but there was insufficient evidence to show they contributed to the accident or severity of the consequences, or to another contributing safety factor. The ATSB identified that CASA's lack of effective process resulted in the continued operation of piston engine helicopters for human sling operations without adequate mitigations. This included the issue of a 3-year instrument to Helibrook shortly prior to the commencement of improved regulations that would require a turbine engine helicopter for human slinging operations. Although conducting the operation with a piston helicopter increased the overall risk of the activity compared with use of a turbine helicopter, previous accident data showed fuel exhaustion was as likely to occur in a piston as it was in a turbine engine helicopter.
Although not likely to result in sudden power loss, engine defects present at the time of the accident likely affected the engine’s maximum power output and fuel consumption. Additionally, Helibrook had likely overrun the helicopter's maintenance, inspection and overhaul periods, which increased the likelihood of the helicopter experiencing a technical failure or malfunction.
The ATSB also found that the pilot’s exposure to cocaine within the previous few days increased the likelihood of fatigue, depression and inattention, however there was insufficient evidence to determine whether these effects occurred.
Finally, the ATSB found that the helicopter's emergency locator transmitter had been removed from its mount prior to the accident. Therefore, it could not activate automatically, which likely delayed the emergency response.
What has been done as a result
CASA implemented significant changes to its internal processes to ensure that the assessment and management of safety risks of new aviation activities (and associated approvals) were standardised in accordance with the CASA Risk Management Manual and that decision-making was appropriately documented. Additionally, CASA developed an ‘exemption protocol suite’ of documents, which detailed the principles, protocols and work instructions for CASA’s regulatory exemption process. CASA also completed and provided exemplar bowtie and aviation safety risk assessments using the structured process.
Following this accident, Helibrook advised that it had ceased operation and the helicopter fleet was being sold. In addition, the chief executive officer/chief pilot was no longer involved with the operation. CASA confirmed that as Helibrook no longer had the required key personnel, it was considered to be suspended from operation. Under those circumstances, the operator’s safety management system was no longer in use.
Safety message
The contributing factors to this fatal accident highlight the significant influence that the actions and decisions of pilots, operators and the regulator can all have on aviation safety.
Fundamentally, this occurrence illustrates the importance of effective fuel management. It is vital to use all available means, including accurate fuel records and quantity cross‑checks, to ensure that pilots accurately know their aircraft’s fuel state. This is especially critical when operating a helicopter where a fuel‑related power loss offers few safe options, such as inside the height-velocity avoid area with a vulnerable human external load. Pilots also should understand the functionality and limitations of any installed low fuel warning systems.
At the operator and regulatory level, effective safety management processes that identify and safely manage hazards are vital to preventing future accidents.
The occurrence
On 28 February 2022, the crews of 3 Robinson R44 helicopters were preparing to conduct crocodile egg collection in Arnhem Land, Northern Territory. Each helicopter was operated by a different aircraft operator, contracted to Wild Harvest Northern Territory, and crewed by a pilot and an egg collector.
One of the helicopters was an R44 Raven II, registered VH-IDW, operated by Helibrook. The method of egg collection included slinging the collector underneath the helicopter, in a harness attached to a 100 ft ‘long line’ (see the section titled R44 human external cargo operations).[1]
The pilot of VH-IDW reported that they arrived at Helibrook’s hangar at Noonamah, on the outskirts of Darwin, Northern Territory at about 0530 local time, conducted the daily inspection of the helicopter and found no defects.
The other 2 R44 helicopters involved in the egg collection on the accident day arrived at Noonamah at about 0645. Their crews reported briefing together with the VH-IDW crew. The briefing involved discussing the day’s plan, including who was collecting from which nests, and where they would meet to refuel. The plan was to refuel at Mount Borradaile en route to King River, then collect eggs from about 15 nests located between King River and Maningrida, which was 90 km beyond King River (Figure 1). The crews then planned to refuel at Maningrida, before continuing south-east to collect additional eggs.
At about 0703, the 3 helicopters departed Noonamah for Mount Borradaile, 205 km east-north-east, where fuel drums had been pre-positioned. At 0743, having travelled 111 km from Noonamah, a photo was taken in the cockpit of VH-IDW. The image showed the accident pilot as the passenger, seated in the left front seat, and the egg collector piloting the helicopter from the right seat. Based on the time taken to reach that point, the helicopter probably arrived at Mount Borradaile at about 0816.
Figure 1: Map showing key locations and times

Source: Google Earth with OzRunways data, annotated by the ATSB
The 3 R44 helicopters landed at Mount Borradaile for the planned refuelling, where the crews intended to ‘hot refuel’[2] each helicopter from fuel drums. A witness reported that the 3 R44 helicopters departed Mount Borradaile at about 0830 to track towards King River. One helicopter continued past King River to the north-east and commenced collecting eggs. OzRunways[3] data for the other 2 helicopters, including VH-IDW, recorded their arrival near King River at 0850.
At a clearing near King River, 60 km beyond Mount Borradaile, the second helicopter’s crew retrieved a harness from VH-IDW. Two witnesses reported that the accident pilot was in the left passenger seat and the egg collector was in the pilot seat and flew VH-IDW to King River, where the dual controls were removed. However, the accident pilot and one other egg collector reported that the dual controls had been removed at Mount Borradaile and the pilot had swapped to the pilot seat and flown VH-IDW from Mount Borradaile to King River. While VH-IDW was still on the ground, the second helicopter departed to commence collecting eggs about 12 km to the north-east. Data recorded from an egg collection application showed that the crew of the 2 helicopters, other than VH‑IDW, conducted operations from 9 nests (Figure 2) between 0911 and 1014.
Figure 2: Accident area including King River, accident site and nests

Source: Google earth overlaid with nest collection data, annotated by the ATSB
At 1036, they located the accident site closest to the first planned nest and landed nearby. They found the sling person (egg collector) fatally injured. VH-IDW was located 44 m beyond the sling person, substantially damaged having collided with trees and terrain (Figure 3). The accident pilot had sustained serious injuries and was found lying beside the helicopter. After providing reassurance to the pilot of VH-IDW, the other pilot returned to their helicopter and briefly became airborne to get mobile reception and call for assistance. The first call to emergency services was received at 1046.
Figure 3: VH-IDW accident site

Source: CareFlight
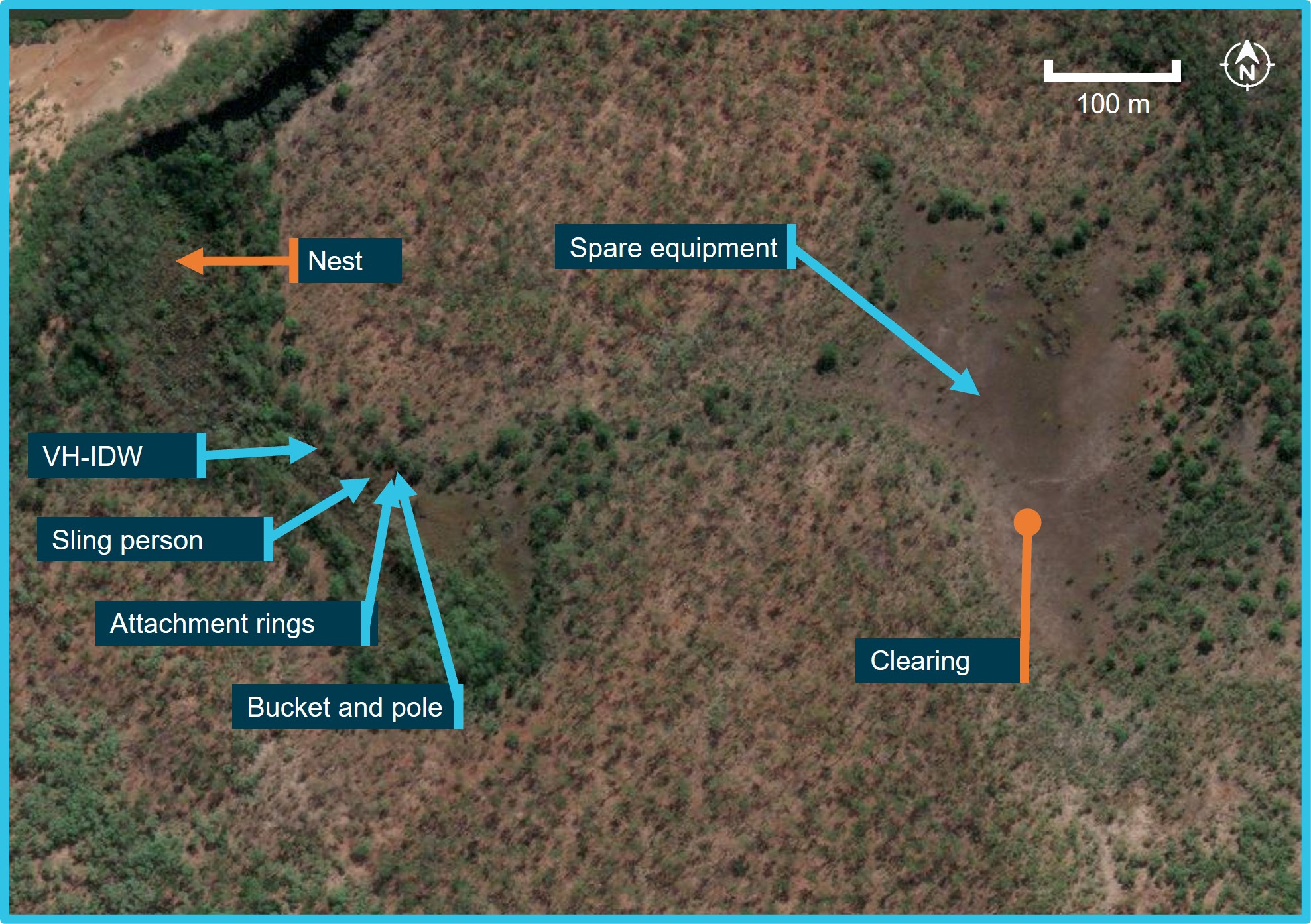
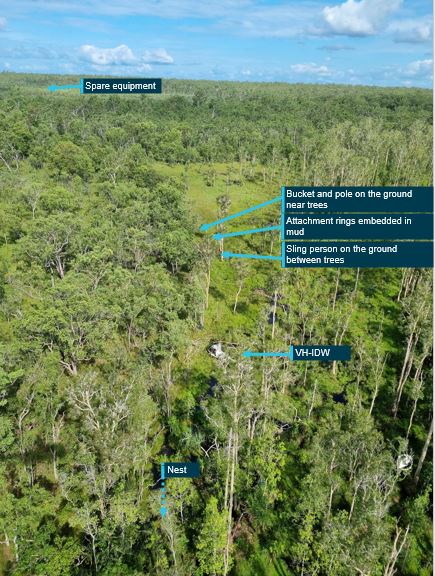
The second helicopter and remaining crew arrived at the site about 1 hour later. They found spare egg collection equipment from VH-IDW in the clearing where VH-IDW was last seen before the accident. The accident site was between the clearing and the closest of 3 nests that were to be collected by VH-IDW’s crew. No eggs had been collected.
Based on photos and reports from those who attended the site on the accident day, the egg collector’s bucket and pole were the first items in the accident trail (Figure 4). The pole was vertical with one end embedded in the ground. About 4 m beyond the pole, the long line attachment rings were found, also embedded in wet ground, with the long line loosely coiled over about 8 m. The egg collector was found wearing a harness, which was intact, firmly secured and attached to the long line, and their helmet was on the ground nearby. The long line was not connected to the helicopter.
Figure 4: Accident trail
Source: Apple Maps annotated by the ATSB
Following notification of the accident, a CareFlight rescue helicopter departed Darwin at 1122, arrived at the accident site at 1232, and departed with the injured pilot at 1310. As they departed the site, another Helibrook R44 helicopter arrived with Helibrook’s chief pilot, a Wild Harvest Northern Territory representative and an off-duty Northern Territory Police Force officer.
A CareFlight nurse remained at the site until the rescue helicopter returned at 1532 to retrieve the deceased egg collector, departing about 20 minutes later. The crews of the other 3 helicopters reported departing about 20 minutes after the rescue helicopter.
Context
Personnel information
Pilot information
Qualifications and experience
The pilot held a commercial pilot licence (helicopter) with low-level and sling ratings. At the time of the accident, the pilot had recorded about 2,500 hours total aeronautical experience. The pilot’s most recent flight review was on 21 May 2021. The pilot had recorded 340.1 hours of sling experience, the most recent of which was gained in May 2021. The pilot had been contracting to Helibrook for 8–9 years, including for crocodile egg collection. In addition, the pilot operated their own R44 helicopters and contracted to other operators. According to the pilot’s logbook, they had first conducted slinging of human external cargo (HEC) for crocodile egg collection on 13 December 2017. Their last recorded HEC sling time was in March 2020, but the pilot reported having also conducted human slinging for egg collection in the wet season from December to May of 2020–2021 and 2021–2022.
Documents provided by the operator indicated that the pilot had completed a proficiency check flight with the Helibrook chief pilot on 3 August 2021 in the pilot’s R44 II helicopter, which was not fitted with dual hooks. The pilot had recorded a flight time of 0.8 hours in their logbook with no reference to conducting sling operations, whereas the Helibrook Rotary Pilot Competency Check form stated the flight time as 1.1 hours. According to the form, the pilot had demonstrated competency in pre-flight tasks, normal and emergency procedures and the following specialised tasks:
- search and rescue
- charter
- sling operations
- croc egg harvesting
- aerial advertising – banner towing
- supply dropping
- surveillance
- hover exit entry.
The pilot was also a licenced aircraft maintenance engineer and the head of aircraft airworthiness and maintenance control (HAAMC) for Helibrook.
Medical and toxicology
The pilot held a class 1 aviation medical certificate with no restrictions, valid to 27 May 2022.
A blood sample was taken from the pilot at 1638 on the accident day, 11 minutes after the pilot’s arrival at Royal Darwin Hospital. Toxicology results from the sample identified several substances administered by CareFlight and Royal Darwin Hospital medical staff. Additionally, the results detected 2 metabolites of cocaine – ecgonine methyl ester and benzoylecgonine – at low levels (less than 0.01 mg/L). These results were identified using mass spectrometry and considered to be reliable indications of previous cocaine exposure. These metabolites can be detected in the blood up to 3–4 days after exposure (see the section titled Cocaine metabolites).
Cocaine itself is generally detectable in blood tests for up to 1–2 days after exposure and was not detected in the pilot’s blood.
The pilot had no reported medical conditions and in the self-disclosure section of their aviation medical application, they had advised not using any drugs or recreational substances within the last 5 years. The pilot also advised the ATSB that they did not use cocaine.
Anticonvulsant medication levetiracetam was also identified in the pilot’s toxicology results. There was no evidence of this having been administered by CareFlight or Royal Darwin Hospital medical personnel, although it was consistent with emergency treatment for the pilot's injuries. There was also no evidence obtained to indicate that the pilot had recently visited a doctor, had a condition requiring the medication, or obtained a prescription for it. A pharmacological expert advised the ATSB that even if it had been present before the accident, it was one of the least likely anticonvulsant drugs to interfere with cognitive process as there was evidence of its widespread positive effects on cognition. It was also less likely to produce ataxia[4] and dizziness than other antiepileptic drugs.
Recent history
The pilot reported having limited recollection of events leading up to, and including, the accident sequence. Despite that, the ATSB was able to identify the following activity in the days leading up to the accident.
On 24 February 2022, the pilot was operating a Robinson R22 helicopter (not associated with Helibrook) to locate crocodile nests, when an engine valve failed, requiring the pilot to conduct a forced landing. The pilot reported feeling ‘pretty rattled’ by it.
The next day, after repairs were conducted on the R22, its engine again lost power during take-off. Additionally, the day’s egg collection activities were suspended due to rain and the pilot’s partner reported that they spent a quiet evening at home together.
On 26 February, the pilot was involved in crocodile egg collection activities, which were again suspended due to rain. The pilot consumed alcohol that evening and reportedly attended a party, returning home between 0100 and 0200 the following morning. The pilot left again before their partner awoke between 1000 and 1100 on 27 February. Rideshare records from the pilot’s phone indicated that a car was used between 0243 and 0306, and again at 1040, with no end time recorded.
Information obtained from the pilot’s phone showed that later that day, the pilot started operating VH-IDW at 1545 and conducted crocodile egg collection about 60 km south‑west of Darwin, until 1810. This was consistent with information subsequently provided by the helicopter operator. The pilot’s partner reported that the pilot went to bed at about 2130 that evening and left for work at about 0445 on the accident morning.
The ATSB considered whether the pilot’s activity in the preceding days may have led to them being fatigued at the time of the accident. Specific factors that potentially increased fatigue risk included:
- the pilot likely experienced a high level of stress following 2 engine power losses, leading to an unscheduled overnight stay at accommodation away from the pilot’s home
- the pilot’s usual sleep pattern was significantly disrupted on one night, getting to sleep around 6 hours after the usual reported sleep time
- over the previous 4 nights, the pilot slept in 3 different locations, which had the potential to affect sleep quality
- the pilot only had 6–7 hours sleep opportunity on each of the 2 nights before the accident, meaning that the pilot was probably carrying some level of sleep debt at the time of the accident
- on the day of the accident the pilot awoke during the window of circadian low, which also has the potential to affect the pilot’s sleep debt
- consumption of alcohol or exposure to recreational drugs is known to reduce sleep quality
- hot, humid weather conditions, such as those in the Northern Territory in February, are associated with reduced sleep quality and quantity.
While a number of these factors could combine to increase likelihood, there was insufficient evidence to establish if the pilot was likely experiencing a level of fatigue known to affect performance at the time of the accident. In a statement provided to the ATSB in response to the draft report, the pilot reported that they were not tired or affected by alcohol or drugs on commencing the operation of the helicopter.
Egg collector information
At the time of the accident, the egg collector had passed their private pilot licence (helicopter) flight test but not yet been issued that licence.
Wild Harvest Northern Territory annual requirements
Wild Harvest Northern Territory (WHNT) held a suite of documents for crocodile egg collection, which included safe work method statements[5] and procedures. WHNT engaged multiple helicopter operators each season to undertake crocodile egg collection. At the start of each egg collection season, those intending to conduct egg collection, including pilots and collectors, attended a WHNT ground-based training and administration day. Both the accident pilot and the egg collector attended this training on 1 December 2021, and had signed safe work method statement sign-on sheets for:
- ground operations for croc egg collecting, including:
- equipment checks
- personal protective equipment
- safety around helicopters
- firearm safety
- selecting and collecting nests
- human sling operations (see the section titled Operator risk assessment)
- safe handling of fuel.
Aircraft information
General history
VH-IDW was a 4-seat Robinson Helicopter Company (Robinson) R44 Raven II (R44 II) helicopter, certified in accordance with United States (US) Federal Aviation Regulations (FAR) Part 27 and manufactured in the US in 2008. The helicopter was first registered in Australia in July 2008 and had a standard certificate of airworthiness and was to be operated in the normal category.[6] The helicopter was powered by a 6-cylinder Textron Lycoming IO-540-AE1A5 engine derated to 205 brake horsepower (BHP) with a maximum 5-minute take-off power of 245 BHP.
In December 2009, at 62.2 total hours in service, the helicopter was involved in a dynamic rollover that resulted in sudden stoppage/damage to the main/tail rotor and the engine. The aircraft was returned to Robinson for overhaul, including the engine. The hour meter was reset to zero, and the helicopter was returned to service in May 2012.
Helibrook commenced operating VH-IDW on 15 October 2020 and, as the registered operator, was responsible for the continuing airworthiness of the helicopter. VH-IDW was to be maintained in accordance with the airframe and engine manufacturers’ maintenance schedule, which required a periodic inspection every 100 hours or 12 months, whichever occurred sooner. The engine and airframe were subject to overhaul at 2,200 hours or 12 years, whichever occurred first. Additionally, any instructions for continued airworthiness on approved modifications, such as cargo hooks, were to be complied with. The helicopter was fitted with an hour meter activated by a combination of oil pressure and an electrical switch on the collective.[7] The hour meter was an acceptable means of recording time in service, however it could be disconnected, which would prevent flight hours being recorded.
On 22 October 2020, shortly after the helicopter was purchased by Helibrook, a 100‑hourly inspection was carried out on VH-IDW, at which time the helicopter’s total time in service, recorded in the maintenance records was 1,577.9 hours and the hour meter read 1515.75. The maintainer reported that in November 2021, the hour meter was rolled forward 62.2 hours to match the helicopter’s total time in service for ease of record-keeping. At the accident site, the helicopter hour meter read 2,070.05 hours, which equated to 2,007.85 hours since overhaul.
Maintenance release
A maintenance release is required to be carried on an aircraft as an ongoing record of the aircraft’s time-in-service and airworthiness status. Subject to conditions, a maintenance release is valid for a set period, nominally 100 hours in service or 12 months from issue.
A daily inspection was required to be carried out and the maintenance release signed to show the inspection had been completed, prior to the first flight of the day. The inspection and certification could be made by any pilot licenced to fly the aircraft, or an appropriately licenced aircraft maintenance engineer. After the last flight of the day and before the aircraft was next flown, the total daily flight time was required to be entered and the progressive total time in service recorded.
VH-IDW’s maintenance release, current at the time of the accident, was provided to the ATSB on 3 March 2022. It had been issued on 7 February 2022, with 2,036.3 hours total time in service recorded. The accident pilot’s signature was on the maintenance release for 8, 9 and 10 February, with 7.6, 4.3 and 1.5 hours recorded respectively.
The accident pilot’s signature was on the maintenance release for the accident day. The pilot initially reported having conducted the daily inspection of VH-IDW on the morning of the accident, found no defects and signed the maintenance release. However, the pilot subsequently reported being unsure when they had signed the maintenance release for the accident day’s flight.
No defects had been recorded on part 2 of the maintenance release. Additionally, there were no entries on part 2 of the maintenance releases from when the fuel calibration was certified on 1 May 2020 to the accident day to indicate any issue with the fuel calibration, calibration card or fuel quantity indication.
Recent maintenance
On 15 January 2022, due to a pilot reporting that the engine was ‘low on power’, the maintainer adjusted the magneto engine timing and renewed the spark plugs.
On 7 February 2022, the maintenance organisation completed a periodic inspection of VH-IDW. During that inspection, the No. 6 cylinder was replaced due to failed compression, however, there was no documentation supporting that a post-replacement compression check had been conducted. Other maintenance items completed at that time included replacement of the engine-driven fuel pump and the tail rotor assembly.
On 11 February 2022, with 2,050.09 hours recorded in the engine logbook, a Helibrook pilot had reported an ‘intermittent miss in flight’ to the maintainer. The maintainer identified that the left magneto had a failed drive bearing and replaced it with an overhauled magneto. The right magneto timing was also adjusted. The worksheet stated ‘compression test ok’ but no figures were recorded. The maintainer reported checking compression during troubleshooting for the intermittent miss but did not record the figures as they were satisfactory. The maintainer then recorded conducting a post-maintenance flight of 0.8 hours with no issues identified.
Recorded hours and other observations
The pilot’s logbook did not contain any entries relating to the operation of VH-IDW, and the pilot’s last logbook entry was in their own helicopter on 12 February 2022. Additionally, and despite the pilot reporting conducting egg collecting using VH‑IDW in previous seasons, the earlier VH-IDW maintenance releases covering the previous egg collection season did not contain any entries by the accident pilot. However, this did not preclude the pilot having flown VH-IDW after another person conducted the daily inspection and signed the maintenance release.
The pilot reported that VH-IDW had flown significantly more hours than were recorded and that the hour meter was never operating when they flew it, although they could not recall whether the hour meter was operating on the accident morning. The pilot estimated that they had flown VH‑IDW for about 70 hours in the 2021–22 crocodile egg collection season and had also flown it during 2020–21. The ATSB obtained invoices that indicated the pilot had conducted over 36 full days of egg collection in 2020–21 and 2021–22 seasons, all of which were reported to have been in VH‑IDW. Due to the apparent discrepancy in operating hours, the ATSB compared the hours recorded on VH-IDW’s maintenance releases from November 2020 to the accident day with:
- the pilot’s time (in units of days/half days) invoiced for crocodile egg collection
- spreadsheets recording hours for helicopters (by operator and helicopter type) and day/half‑day rates for personnel involved in crocodile egg collection
- the pilot’s phone records of start and stop times for VH-IDW
- recorded egg collection data (see the section titled Crocodile nest data)
- fuel uplift records
- evidence of VH-IDW being operated for a purpose other than egg collecting.
There were 21 days identified when VH-IDW was operating and there was no entry on the maintenance release, some of which were recorded as 10 to 11 hours of helicopter operation. For all other entries for crocodile egg collection, only a portion of the spreadsheet time was recorded – including as little as 10% of the hours recorded on the spreadsheet on single days. On those days, collected nests were recorded on the crocodile egg collection application and for many of them, the pilot had retained a record of VH-IDW start and stop times consistent with the spreadsheet’s recorded hours. The review of the spreadsheets and comparison with VH-IDW’s maintenance release hours included consideration of whether multiple Helibrook R44s were operating on a given day.
The accident pilot reported that the helicopter had not ‘missed a beat this season’, then subsequently described VH-IDW’s performance as good and that it flew well, but that it was nearing the end of its overhaul life and had problems in the weeks prior to the accident. These included a damaged inlet valve, a loose induction tube and fuel injector. The latter 2 items were recorded as rectified on the maintenance release on 14 December 2021. There was no documented recent inlet valve replacement identified but the No. 2 cylinder exhaust valve was replaced on 22 April 2021. When questioned whether there was any indication that the helicopter was overrunning the 100-hour inspection intervals, the maintainer reported that it was difficult to determine whether a helicopter had done 100 or more hours when it arrived for maintenance.
A maintainer who previously maintained Helibrook helicopters from June 2016 to January 2020, reported that they had previously found a Helibrook R44’s hour meter disconnected. In addition, the operator had leased a helicopter from the maintainer and a comparison of recorded GPS flight data with documented flight times showed that the hour meter had been disconnected and about 4 hours of the 14 hours flown during the cross-hire period were not recorded on the maintenance release.
A Civil Aviation Safety Authority (CASA) airworthiness inspector produced a report as part of CASA’s review of this accident. The report identified that VH-IDW’s engine-driven fuel pump had been replaced at reducing hours since new: 733.4 in 2017, 651.9 in January 2020, then, after purchase by Helibrook, at 387.8 hours in April 2021 and 263.2 hours in February 2022. The report stated this was indicative of flight hours not being accurately recorded.
Fuel capacity, calibration and indications
The R44 II POH stated that for tanks fitted with bladders (including VH‑IDW), the main fuel tank capacity was 115 L, of which 112 L was usable, and the auxiliary tank capacity was 65 L, of which 64 L was usable. Of the combined 180 L capacity, the total usable fuel was 176 L. The POH defined usable fuel as the fuel available for flight planning.
Unusable fuel is the amount of fuel in the tank/s below which continued running of the engine while performing the most adverse manoeuvre cannot be assured. Below this level, there is the potential to un-port[8] the fuel tank outlet due to fuel movement. In straight and level flight, some of the unusable fuel is likely to reach the engine. In the R44 II, the main tank to engine fuel union is located on the inboard side of the tank, forward and near its base.
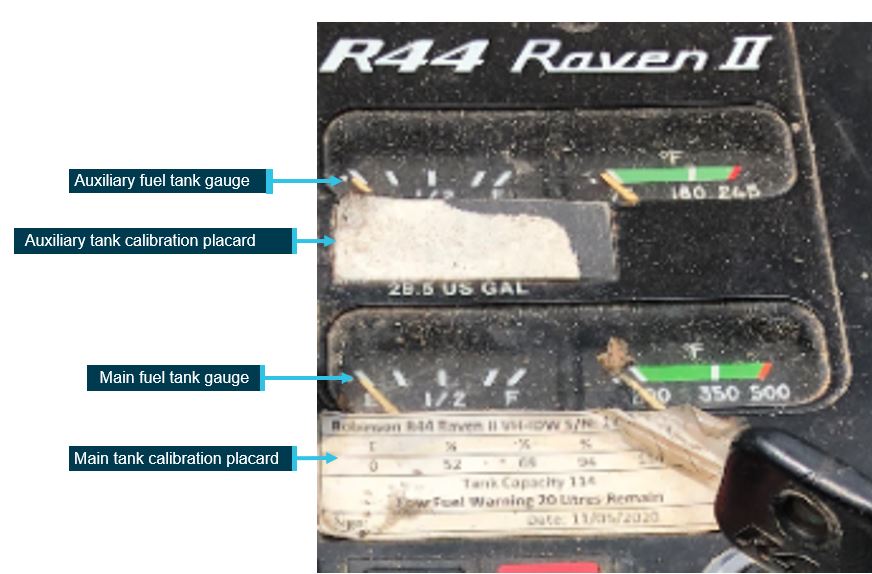
Calibration of the main and auxiliary tank fuel gauges was required every 48 months. The last calibration was conducted by a CASA‑authorised maintainer in May 2020. The calibration is shown in Figure 5. The associated placards for the main and auxiliary tank gauge calibration were affixed in the cockpit, but the auxiliary tank placard was damaged and illegible (Figure 6).
Figure 5: Fuel tank gauge calibration as recorded in May 2020
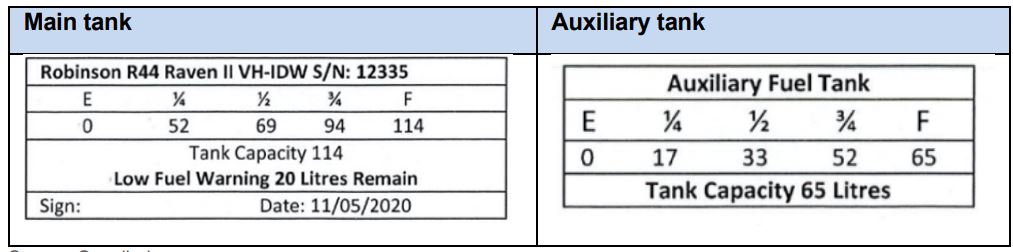
Source: Supplied
Figure 6: VH-IDW cockpit photo showing fuel gauges and placards
Source: ATSB
The main tank placard stated that the low fuel warning light would illuminate when 20 L total fuel (usable and unusable) remained (Figure 6). According to the maintenance manual, the low fuel warning switch was not subject to calibration. The organisation that conducted the fuel calibration reported that, to establish the 20 L figure, they drained the tank, checked the low fuel light was illuminated, then added fuel until the low fuel light went out. The pilot reported that the light would illuminate with 18 L total fuel remaining. Both those figures differed from the POH, which stated that the low fuel warning light would illuminate with approximately 3 US gallons (11 L) of usable fuel remaining (14 L total fuel in the main tank) (Figure 7).
Figure 7: Low fuel warning
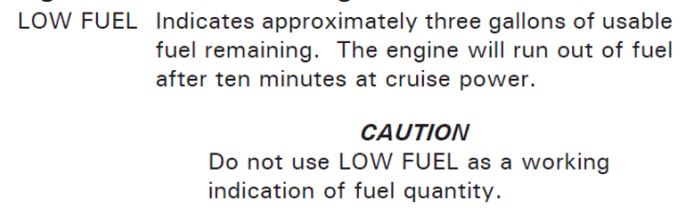
Source: Robinson R44 II Pilot’s Operating Handbook
The Robinson R44 II POH included Safety Notice SN-15 – Fuel exhaustion can be fatal, which advised pilots never to rely solely on the fuel gauge or low fuel warning light but to always record the hour meter reading each time the fuel tanks were filled. This enabled pilots to monitor fuel consumption and endurance. In addition, the POH required the pilot to visually check fuel quantity at each tank during the pre-flight. VH‑IDW was also fitted with a fuel flow transducer and an associated Fuel Scan (totaliser) instrument in the cockpit. The instrument could display fuel flow and other parameters including fuel used and fuel or time remaining. However, the display of accurate fuel quantity relied on the correct amount of fuel to be entered following engine start and the in-flight photograph taken en route from Noonamah for Mount Borradaile identified that the Fuel Scan instrument display was not visible.
Manifold pressure limits
Maximum continuous power manifold pressure limits were prescribed in the POH (Figure 8).
Figure 8: R44 II Maximum continuous power, manifold pressure limits
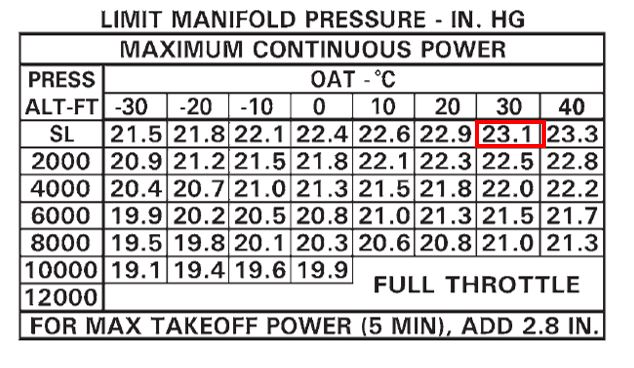
The red square depicts the limit for the conditions at the time the in-flight photo was taken.
Source: Robinson Helicopter Company, annotated by the ATSB
Flying with a higher manifold pressure than the prescribed limit may exceed the approved torque for the rotor drive system. Robinson advised that if excessive power was held continuously, the helicopter would exceed the normal flight envelope, likely causing stress to drive system components that were not designed for such loads.
Robinson safety notice SN-37 – Exceeding approved limitations can be fatal, stated:
Robinson also advised that higher‑than‑normal manifold pressure for a given airspeed could also indicate an engine issue. If one or more cylinders were not operating correctly, higher manifold pressure would be required to produce the same power. In this case, the higher manifold pressure may not exceed the approved torque for the rotor drive system.
Hydraulic flight control assistance
The main rotor flight controls are hydraulically boosted to eliminate cyclic[9] and collective feedback forces. The hydraulic system operates at a pressure between 450–500 psi and consists of a pump, 3 servos, a reservoir, and interconnecting lines. The pump is mounted on, and driven by, the main rotor gearbox. A servo is connected to each of the 3 push-pull tubes that activate the main rotor swashplate. The reservoir is mounted on the steel tube frame behind the main rotor gearbox and includes a filter, pressure relief valve, and pilot-controlled pump bypass valve. A sight gauge for pre-flight fluid level checks is incorporated in the reservoir, which has a vented filler cap.
The pump bypass valve is solenoid-actuated and controlled by the hydraulic switch on the cyclic. When selected to HYD (on), the solenoid is deactivated. This fail-safe ensures hydraulic assist is retained in the event of a loss of electric system power. The switch should be on from start-up to shutdown, except during the hydraulic system check or simulated hydraulic failure training. When selected to off, power is applied to the solenoid and high-pressure hydraulic fluid is returned to the reservoir, removing hydraulic assist from the controls.
Robinson reported being unaware of any instances of the solenoid actuating in flight and causing a loss of hydraulic assist in the controls. The ATSB occurrence database contained 3 hydraulic related occurrences in R44 helicopters since 1997, none of which resulted in a loss of control or an accident. The first was the result of the pilot inadvertently switching off the hydraulic master switch in flight, the second was a failure of the hydraulic pump, and the third was a hydraulic leak.
Inadvertent engine stoppage
Robinson advised that there had been several accidents in which a pilot had inadvertently induced an engine stoppage by rolling off the throttle too fast. This had occurred in flight training when simulating an engine failure and in response to abnormal situations such as rapid engine RPM changes or discrepancy between engine and rotor RPM.
Skids
The helicopter had previously been fitted with floats, which had been removed, but the skid extenders necessary for float fitment remained fitted to the helicopter.
Emergency locator transmitter
The helicopter had a factory mount for an emergency locator transmitter (ELT) and associated wiring in the main rotor gearbox bay however no ELT was fitted to VH‑IDW, nor was one required to be. When fitted, the ELT is connected to an external antenna. The ELT had an arm/on/off switch, and a remote switch was located next to the cyclic, with a default position of ‘armed’.
Pannier
A pannier for the carriage of egg collection equipment was fitted on the left side of VH-IDW. This had been approved by a CASA-authorised aeronautical engineer under an engineering order, although the associated rotorcraft flight manual supplement (RFMS) was not inserted in the POH.
Dual hook system
VH-IDW was originally fitted with dual hooks for HEC under an engineering order. The engineering order required that the hook system be maintained in accordance with the instructions for continued airworthiness and operated in accordance with the associated flight manual supplement. The engineering order was replaced by a CASA-approved supplemental type certificate (STC)[10] in 2021. The system and hook part numbers and the maintenance requirements were unchanged, and the only change was a reduction in the maximum allowable hook weight from 150 to 129 kg (and the associated placard). This was to provide a greater safety margin for HEC operations for the same hook and its strength rating.
The STC approved nominated R44 and R44 II helicopters to be:
- modified with a dual Onboard Systems International cargo hook kit for HEC operations in accordance with Master Document List R5106-07-R5 (28 July 2021)
- maintained in accordance with Instructions for Continued Airworthiness (ICA) R5106-09-R11 (21 July 2021)
- operated in accordance with RFMS R5106-25-R13 (11 June 2021), which was required to be inserted in the POH. The associated RFMS was not contained within VH-IDW’s POH.
The dual hooks could attach to rings on a 100 ft long line, enabling the carriage of a person below the helicopter. The 2 hooks could be released by the pilot by pressing 2 independent buttons of the primary quick release system (PQRS) or pulling 2 manual handles of the back-up quick release system (BQRS). In addition to 2 independent actions, the PQRS buttons were recessed into a housing to further reduce the likelihood of inadvertent pilot activation. The dual hook and release systems were designed to provide redundancy in case of failure.
Following electrical or manual activation, the hook arm would remain open, until it was manually relatched by pushing the hook up by hand to the closed/locked position (Figure 9). (Note: the red component in Figure 9 is the manual release lever).
Figure 9: Onboard Systems hook open and closed/locked (same part number as those installed on VH-IDW)

Source: Onboard Systems
Serviceability
The Onboard Systems HEC dual hook system was installed on VH-IDW on 23 October 2020. The ICA required the external load operation hours to be recorded when the primary hook, or both hooks, were used for external load operations in flight.[11] There was no evidence that external load operation hours were recorded on either hook. There was also no record in the aircraft maintenance documentation of the required 100-hourly/annual checks having been conducted. Finally, one of the hooks had been removed from another helicopter prior to being installed on VH‑IDW and had exceeded its 3 years in‑service limit.
The RFMS included the requirement for the pilot to conduct a functional check of the quick release systems prior to commencing the day’s HEC operations. The pilot reported that their normal procedure was to test that the primary and back-up quick releases were functional before the sling person hooked up but could not recall whether they had done so on the accident day.
Meteorological information
The helicopter departed Noonamah on the accident morning at about 0703. The weather conditions at the time included a light northerly wind and scattered low cloud. At 0743, the helicopter was en route, 60 NM beyond Noonamah and 50 NM from Mount Borradaile. The nearest Bureau of Meteorology weather station was at Point Stuart (Figure 1), where, at 0800, the wind was a north-north-westerly at 10–14 kt, the temperature was 27.5 °C and the QNH[12] 1008 hPa.
The Bureau of Meteorology weather station nearest the accident site was South Goulburn Island Airport (Warruwi), 29 km north-north-west. At 0930, the recorded meteorological conditions were westerly wind at 6 kt, temperature 29 ⁰C, dewpoint 24 ⁰C, QNH 1010 hPa and no cloud. Similar conditions were recorded at Oenpelli, 63 km south-west, and Maningrida, 90 km east-south-east of the accident site.
Recognising that the winds at these recording stations were light and the actual accident time unknown, the accident trail was consistent with it being approximately into wind. At the sea level elevation of the accident site, with QNH 1010 hPa and temperature 29 ⁰C, the calculated pressure altitude was 90 ft and density altitude[13] was 1,770 ft.
Recorded data
Mobile devices
There was a mobile telephone and an iPad on board the helicopter at the time of the accident with the potential to contain data relevant to the accident sequence. The ATSB was able to recover information from the pilot’s phone pertaining to their activities in the days prior to the accident, records of hours the pilot operated VH-IDW and previous maintenance release practices. However, no data directly relevant to the accident flight was able to be recovered.
The egg collector’s phone had been operating in the vicinity of the accident site, but was missing and could not be obtained by the ATSB for analysis and the iPad was severely damaged in the accident impact, rendering any stored data unrecoverable.
Phone records show the last mobile data session before the accident, commenced on the pilot’s phone at 0847:37 and the egg collector’s phone at 0858:16. The egg collector was sent a text message at 0923:44 but the message was not received. This indicated that the phone was either out of mobile range, which occurred below about 300 ft in the vicinity of the accident site, or was off/not powered.
In-flight photo
A georeferenced in-flight photo was taken at 0743 on the accident morning, 111 km beyond Noonamah and 94 km prior to the Mount Borradaile refuelling stop, on a direct track between the 2 locations (Figure 10). The photo showed:
- the fuel gauges reading just below three quarters full
- the Fuel Scan instrument was not operating
- the manifold pressure about 24 inches of mercury (inHg)
- an indicated airspeed 90 kt
- the engine and rotor RPM about 103%
- a chronometer indicating 00:45.
The photo also showed the accident pilot seated in the left seat as a passenger and the egg collector piloting the helicopter from the right seat.
Figure 10: Cut-out of in-flight photo taken at 0743 showing cockpit indications

Source: Northern Territory Police, annotated by the ATSB
As detailed in VH-IDW’s POH, for the pressure altitude at sea level and temperature 30 °C, the maximum continuous power was 23.1 inHg manifold pressure (red box in Figure 8). Based on the aircraft’s height, temperature and QNH at Point Stuart and interpolating the POH table, the maximum continuous power was about 23 inHg. Robinson advised that exceeding the manifold pressure limits with an engine functioning normally would be expected to result in a higher airspeed or rate of climb than depicted in the photo.
Assuming VH-IDW departed Noonamah at 0703, which was the time one of the other R44s departed, it averaged 90 kt ground speed to the in-flight photo location.
Crocodile nest data
A custom-built iPad application named ‘Crocpad’ was used to record the collection of eggs and nest locations. In the week prior to the accident, pilots (including the accident pilot) had conducted flights to locate the nests and entered each nest’s location into Crocpad.
The Crocpad data included fields for the device name, status, created date and modified date. The device name was that used by the person who located the nest (for example, ‘my iPad’). The created date contained the date and time the nest was located, at which time the nest’s status was set to LOCATED. When a nest was subsequently either COLLECTED or DELETED, the modified date was amended with the date and time this occurred. This did not need to be the same person or Crocpad that located the nest. The device name was not updated when a nest was collected or deleted, and remained as the device name that had been used to locate the nest. The Crocpad data would update to the server when in mobile range, which the accident site was not. The iPad that was running Crocpad in VH-IDW had not updated the server with any information before it was severely damaged in the accident impact. The 9 nests amended on 28 February are shown in Table 1 and Figure 11.
Table 1: Crocpad data for 28 February 2022
| Nest number | Local time | Status |
| 1 | 0911 | COLLECTED |
| 2 | 0912 | DELETED |
| 3 | 0915 | COLLECTED |
| 4 | 0935 | COLLECTED |
| 5 | 0955 | COLLECTED |
| 6 | 0955 | COLLECTED |
| 7 | 1009 | COLLECTED |
| 8 | 1011 | COLLECTED |
| 9 | 1014 | COLLECTED |
Figure 11: Crocpad data showing nests recorded as collected or deleted on 28 February 2022

Source: Crocpad data overlaid on Google Earth, annotated by ATSB
On the accident morning, after departing the King River set-down area, the pilots and egg collectors of the 2 helicopters other than VH-IDW, reported meeting at a patch of 3 nests (No.1 to No. 3), then one helicopter went to a single nest (No. 4), before re-joining the crew of the other helicopter at another patch of nests (No. 5 to No. 9).
Figure 12: Inset from Figure 11 showing nests in the vicinity of the accident site with the status of ‘located’ on the Crocpad data

Source: Crocpad data overlaid on Google Earth, annotated by ATSB
OzRunways data
OzRunways flight path data was obtained for 2 of the R44 helicopters, including VH-IDW. The data contained tracks commencing about halfway between Mount Borradaile and the King River, and ceasing near the clearing where VH-IDW and its crew were last seen prior to the accident (Figure 13). The data for VH-IDW was recorded on the egg collector’s iPhone from 0841:28 to 0850:13 local time and uploaded to the OzRunways server. The data covered about 15 NM, equating to a ground speed of about 100 kt. The other track was from 0840:22 to 0850:15, indicating the 2 helicopters were operating in company.
Figure 13: Recorded OzRunways tracks of VH-IDW and another R44 helicopter

Source: OzRunways data overlaid on Google Earth, annotated by ATSB
No OzRunways data was retrieved from the accident pilot’s phone and no data had uploaded to the server from the pilot’s phone or iPad. The pilot reported that they generally used landmarks to navigate for the ferry flight, and would only use OzRunways, in combination with Crocpad, for the egg collection.
Communications
The egg collector carried a UHF radio to enable communication with the pilot. It was reported that as the egg collector usually held a bucket in one hand and a pole in the other, it was difficult for them to press the transmit button to talk to the pilot, so they would usually use hand signals to communicate. The accident pilot subsequently reported that egg collectors could easily hold the crate and pole in one hand, making the radio accessible. Additionally, the accident pilot reported that as the helicopter radio was selected to VHF at the time of the accident, they could not have quickly communicated with the egg collector as it would have required switching the radio selector to UHF.
The pilot who was first on the accident site estimated that the accident occurred at about 0922 while they were on the ground and out of radio range. This estimation was based on the pilot not hearing an unintelligible radio transmission, later attributed to IDW, that was reported to have been heard by the crew of the other R44 which was airborne at the time.
Accident site assessment
The ATSB attended the accident site on 2 March 2022. The site was in a paperbark swamp approximately 440 m east of the clearing where spare equipment was found and where VH-IDW was last seen. From the egg collector to the helicopter, the accident trail lay in an approximately north‑westerly direction towards, and about 150 m before, a nest that was assigned to the crew of VH-IDW.
Assuming a direct transit from the clearing towards the first nest, the trees between where the helicopter probably took off, and where the egg collector was released, were 12–15 m tall. The trees in the vicinity of the target crocodile nest were at least 18 m tall. The bucket and pole were reported to have been found on the ground between trees about 4 m prior to the long line attachment rings. The egg collector was located about 8 m beyond the attachment rings and between 2 trees (Figure 14). On the first tree in the direction of flight, a section of bark had peeled away, about 4–5 m above the ground. While this may have been evidence of possible recent impact, no associated bark was found on the equipment or egg collector.
Figure 14: Accident trail
Source: Northern Territory Police annotated by ATSB
The helicopter impacted the ground upright 44 m beyond the sling person, with the fuselage oriented on a heading of about 060° (Figure 15). The main rotor blades had struck one tall slender tree 3 times, indicating a vertical descent through the tree. The tree was about 9 m tall, with 2 distinctive upper branches that forked from the main trunk about 5 m above the ground. One rotor blade severed one upper branch 8 m above the ground, where the branch diameter was 35–40 mm). A blade then severed the trunk at the fork, 5 m above the ground, where the branch diameter was 50–55 mm. The final cut of the main trunk occurred 1.1 m above the ground, which was below the normal main rotor blade height above the ground in a level attitude.
The severed main tree stump (diameter 150 mm) was 2.4 m in front of the helicopter’s nose, leaning about 55° in the direction of main rotor rotation. The helicopter was facing over 90° right of the apparent direction of travel, consistent with rotation of the fuselage due to the main rotor blade’s impact with the tree trunk or pilot pedal input. During the accident sequence, one main rotor blade fractured about 1 m inboard from the blade tip, with the fragment located 45–50 m north‑west of the wreckage. It was noted that the main rotor pitch control link associated with this blade had fractured in overstress, with no damage to the other pitch link.
Figure 15: Site overview, with the orange arrow showing approximate direction of the accident trail

Source: Northern Territory Police, annotated by the ATSB
In addition to multiple rotor strikes to a single tree, indications of a mostly vertical descent, slightly right and nose-down attitude and a heavy impact included:
- the landing gear had splayed almost to horizontal, and fractured
- the forward cross tube was pushed up into the cabin, significantly reducing the available space in the rear cabin, resulting in empty egg crates in the middle of the back seats being distorted and wedged up against the internal cabin roof
- both skids had fractured forward of the front struts
- deformation to the nose was more pronounced to the right of the landing lights
- the pilot’s seat was collapsed towards the front right corner.
The base of the pilot’s seat had crushed, as designed, to absorb impact forces. The pilot’s restraint had reportedly been cut by those first on site and used in providing first aid to stabilise their injuries.
All the helicopter components were located in the vicinity of the accident site, indicating that there was no in-flight breakup. The forward doors were not installed, and the rear doors had been ejected on impact but were reportedly moved and placed under the pilot for support.
The helicopter was in a black dirt swamp and surrounded by water, up to about 0.5 m deep. The swamp had a gentle flow away from the helicopter, in a northerly direction, toward a nearby creek that was part of the King River system. When the ATSB attended the site 2 days after the accident, both fuel tank caps were correctly fitted, there was no fuel smell, no fuel in the auxiliary tank and a very small quantity of fuel at the bottom of the main tank.
The impact forced the right side of the transmission deck up to contact the underside of the auxiliary tank, such that the fuel drain could not be accessed. There was no evidence of fuel leaks on the transmission deck, from either tank or associated fuel lines. The right-side low orientation of the helicopter would have directed any fuel in the main tank to the engine fuel hose union near the base of the inboard side of the tank. Any fluid that leaked from the helicopter would have flowed downstream and away from the site.
The first person to arrive at the site could not recall checking the fuel tanks, but 2 others who arrived in the second Helibrook helicopter reported having observed the first person to arrive look in one tank and advise that there was fuel visible. In addition, the Helibrook chief pilot who was on board the second Helibrook helicopter reported looking in one tank and seeing a shimmer of fluid however, they did not dip the tanks to check the quantity. The first person to arrive at the accident site reported that there had been a fuel smell, but subsequently reported that the fuel smell may have been from a damaged jerry can that had been behind the pilot’s seat at the time of the accident.
A CareFlight first responder who arrived at 1232 reported that there was no smell or indication of fuel, only hydraulic fluid, which created a sheen on the water. A photo taken at 1555 on the accident day showed a slick on the water near the accident site. It was unknown whether that was from hydraulic fluid, fuel or another source. The ATSB obtained images of the site taken in June 2022, 4 months after the accident, in which there was no evidence of vegetation dieback that can indicate fuel contamination. However, 206.2 mm of rainfall had been recorded at the nearest Bureau of Meteorology weather station (Warruwi Airport) since the accident, reducing the likelihood that vegetation dieback would be evident.
The first person to arrive at the accident site also reported that there was no power to the aircraft when they arrived, but they switched off the electrical system master and alternator switches as a precaution, and rotated the main rotor blades to provide shade for the pilot. They further reported the fuel mixture control was in the full rich position and the magnetos were selected to ‘Both’, consistent with positions identified by the ATSB on site. The engine RPM governor switch, located at the forward end of the collective, was found in the OFF position. The hour meter read 2070.05. The stowage space under both forward seats was inspected, with nothing being located under the left seat and several small items, including a damaged headset, under the pilot’s seat. The POH and maintenance release were not in the helicopter.
No oil was found in the hydraulic system, however, hydraulic fluid was observed on the main transmission deck. The hydraulic switch was selected ON at the cyclic. Flight control continuity from the tail rotor to the main rotor head, above the transmission deck, was established. The fuses for the belt tensioning actuator, in-use and spare, were noted to be the correct amperage and undamaged. All 4 drive belts were present. The distorted pannier prevented easy access to the left side of the engine and the underside of the helicopter was not accessible due to the collapsed landing gear and distortion to the engine cowls. On-site images indicated that the engine was probably above the water level, however, water may have entered the cowls on impact.
The tail cone remained connected to the fuselage. There was no damage to the upper vertical fin and horizontal stabiliser. The tail cone and the lower vertical fin displayed compression damage consistent with terrain impact.
The tail rotor assembly was secure and rotated freely. Oil was evident in the tail rotor gearbox sight glass and the chip detector was clear of metal contamination. The tail rotor blades were in new condition and undamaged, with some light wood debris at the tip on the leading edge of one tail rotor blade. There was some corresponding minor scuffing to a partially submerged, sodden tree branch immediately under the tail rotor, consistent with contact following a vertical descent.
The ELT’s mount was located in the main rotor gearbox bay however, the ELT was not installed. The ELT harness, which included a quick disconnect socket, and antenna cable, were secured with cable-ties. The ELT end of the antenna cable was secured to the helicopter frame with tape. The remote switch, located next to the cyclic, was in the default ‘armed’ position.
Following on-site examination, VH-IDW was slung from the site by another helicopter. People on the ground when VH-IDW was lifted from the accident site did not report observing any fuel leaking from the helicopter. During the retrieval, VH-IDW was lifted multiple times, and also put down heavily en route to Jabiru, Northern Territory due to a technical issue with the slinging helicopter. At Jabiru, VH-IDW was loaded upright onto a truck and transported 252 km by road to a secure facility in Darwin for detailed examination. The switch positions identified on site were not altered during the retrieval and arrived in the same positions.
Helicopter examination
Hook system
The hook electric and manual release systems could not be functionally tested due to impact damage. However, both manual release T handles were found in the down position (not activated) and visual inspection did not identify any faults with the dual hook system. The hooks were found in the ‘up and locked’ position when the wreckage was lifted during retrieval from the accident site. Following activation, the hook arm would normally remain open, until manually relatched by pushing the hook up to the closed/locked position. In this instance, having had to open to release the egg collector, they were likely closed by the subsequent helicopter ground impact.
Drivetrain
Continuity of the drivetrain was established from the main rotor gearbox to the tail rotor gearbox, including all flex couplings. There was some distortion to the main rotor gearbox input driveshaft yoke and flex coupling, along with minor scraping on the transmission deck under the intermediate flex plate which was consistent with an unpowered rotor system (see the section titled Autorotation) during a heavy impact.
The main rotor gearbox could be rotated without restriction and the oil level was in the middle of the sight glass. Several main rotor gearbox mounts were fractured and the chip detector was damaged from perforating the transmission deck but was clear of debris. There was no indication of overheating of the main gearbox or clutch assemblies.
The clutch assembly was disassembled with no obvious damage to the sprags or race surface, consistent with the helicopter being in autorotation during multiple tree strikes before impacting the ground.
The belt tensioning actuator assembly had fractured in overstress at the connection to the upper bearing assembly and at the actuating rod. The actuator rod extension was consistent with properly engaged belts, which included assessment of expected stretch typical of their time in service. The drive belts were intact and appeared in reasonable condition although they were displaced from their respective sheave grooves, which was typical of heavy impact and actuating rod failure.
Main rotor
The main rotor head droop stops were undamaged with no evidence of excessive teeter or mast bumping. Both blades exhibited rearward distortion about mid-span, with some mild upward coning, indicative of low energy during the descent and tree strikes (Figure 16). The fractured pitch link failed in overstress at the upper rod end thread. The corresponding rod end was secured to the pitch horn, with a slight inboard deflection consistent with the rotor strike and blade fracture. The associated fractured blade had more pronounced coning near the hub, and impact marks and deformation on the lower surface, consistent with the blade being able to rotate about the pitch axis (up) following the pitch link failure. The blade tip was likely liberated at the stump strike.
Figure 16: VH-IDW’s main rotor blades showing rearward bending and fracture
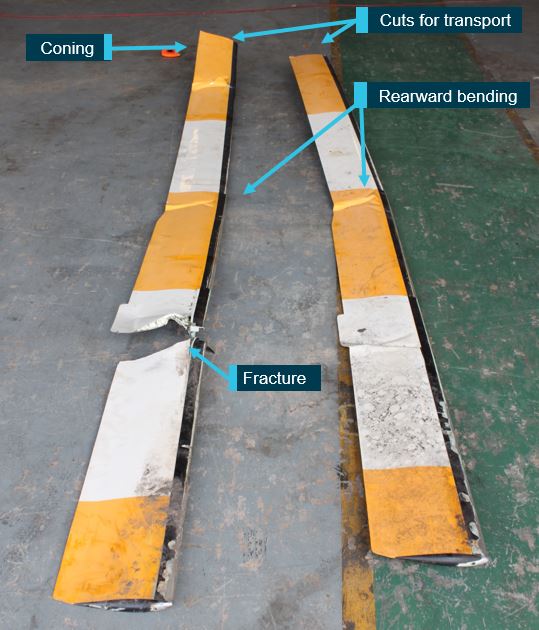
Both main rotor blades were cut at the accident site to facilitate transport to Darwin
Source: ATSB
Control continuity
Flight control continuity was established throughout. Many control tubes had fractured due to overstress associated with impact, but the corresponding rod ends were secured to bell cranks. The left seat quick-disconnect (dual) controls were not installed and the cyclic boot was in place. The collective friction device had fractured due to impact forces. There was some movement in the collective, but it was restricted due to damaged control tubes. The overtravel spring was bent in a manner consistent with impact damage.
Engine RPM governor
A power source was applied to the governor motor. The motor operated in both directions with no evidence of interference. The governor wiring loom connector was secure and there was no evidence of loose or deformed pins. The governor switch was functional, with the governor itself sent to Robinson for testing under supervision of the US National Transportation Safety Board and found serviceable.
Hydraulics
The aft servo return line tee union was found to have fractured in overstress. The filter was clear with no sediment and the pump was secure. The solenoid that actuated the pressure shut-off valve was also tested and found functional.
Emergency locator transmitter
As detailed above, on-site examination identified that no ELT was fitted to the helicopter. The ATSB was subsequently provided with an ELT by the helicopter operator, who reported that they had removed it from the site after the accident. They advised that it was typically carried under one of the seats, otherwise it would get wet and erroneously activate. The produced ELT was registered to a former Helibrook chief pilot and not associated with any aircraft registration. It appeared intact, in reasonable condition, was switched off and its battery was due to expire in August 2022.
The Australian Maritime Safety Authority confirmed that previous unintended ELT activations had occurred due to water ingress and identified one record of activation of the ELT associated with VH-IDW, which occurred on 28 December 2021. A company representative for VH-IDW had advised the authority that the ELT had self-activated, likely due to water making contact with the ELT while collecting crocodile eggs. That ELT was not the one provided to the ATSB.
Warning and caution lights
All warning and caution lights were inspected, and electrical continuity confirmed. The filaments of the low rotor, low fuel, alternator and governor warning lamps were subsequently inspected under a microscope with none found stretched or broken as sometimes occurs if illuminated at impact. However, due to variables that affect the rate of acceleration applied to the filament, the absence of filament stretch does not enable a conclusion regarding whether or not the light was illuminated.
Electrical system
The helicopter battery was found out of the battery box but still connected to the helicopter by the battery leads. The alternator control unit was secure and connected.
Hour meter
One of the 2 electrical connections at the back of the hour (Hobbs) meter was found finger tight. Despite that, the connector would not move freely and had a lock washer under the nut to prevent it from coming loose during operation. However, only a small amount of hand pressure was needed to move the connection, consistent with it having been tightened by hand rather than with a spanner or socket.
Indications of engine rotation at impact
There were no indications of engine rotation at impact, evidenced by:
- no rotational damage to the engine cooling fan or housing
- no slippage to the cooling fan retention nut alignment mark
- no evidence of rotational scoring to the alternator housing or cooling fan and backing plate.
Significantly, impact damage and bending to the upper sheave forward end, lower surface was consistent with impact with the starter ring gear, and showed defined teeth impact marks, with no smearing (Figure 17).
This strongly supported the ring gear being stationary (engine stopped) when the helicopter collided with terrain.
Figure 17: Upper sheave damage from impact with non-rotating starter ring gear
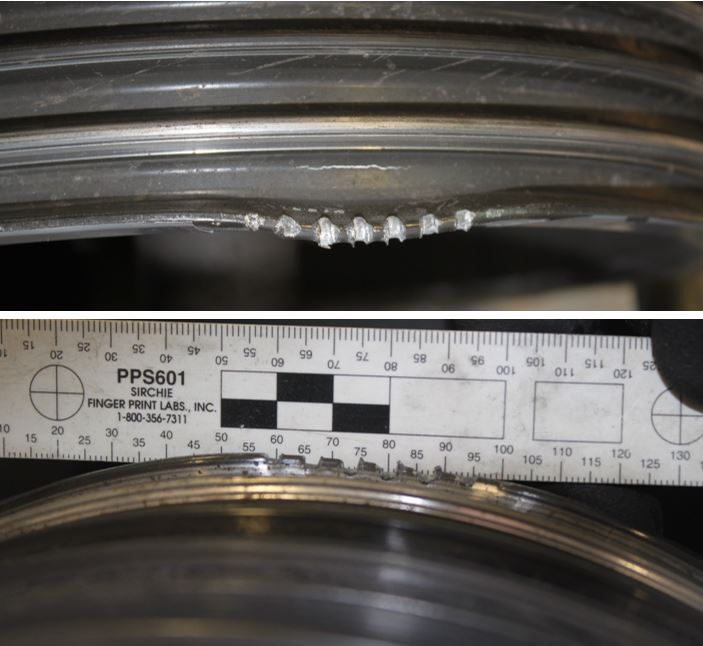
Source: ATSB
Powerplant
External engine examination
External examination found no evidence of a catastrophic engine failure. The throttle butterfly was fully open at the fuel control unit, however as the impact forces would have tended to pull it open, the throttle position prior to impact could not be determined.
Oil
The engine oil cap and dipstick were secure, and the sump plug was relatively clean. The ATSB drained 8.6 L of oil from the engine with no significant debris found in the oil. The recommended maximum engine oil quantity was 9 quarts (8.5 L). Although the oil level slightly exceeded the maximum recommended capacity, it would not have affected the engine’s performance. The oil filter was opened and inspected with nil contamination identified on the filter element.
Air
Induction air enters through an opening on the right side of the fuselage and passes through the air filter within the air box. Air then passes along a flexible sceet duct, through the fuel control unit and into the engine. The air intake was damaged consistent with accident impact, but there was no evidence of blockage or ingestion of foreign material. The air box casing was distorted, also consistent with accident damage, though the filter was clean and there was no sign of blockage. The induction sceet hose had been crushed consistent with impact forces. The induction hose was also checked for delamination, due to a previously-identified issue with some induction hoses, and none was evident.
Engine examination
The engine was shipped to a CASA-authorised maintenance facility for examination under ATSB’s supervision. Differential compression checks were carried out on the assembled engine. Cylinders No. 3 and No. 6 were below the limit of 60/80, which the engine manufacturer advised was the point that removal and overhaul should be considered (Table 2). However, cylinder compression is normally checked on a warm engine, as a cold engine may not provide reliable results.
Table 2: Compression checks of assembled engine – red denotes below limit
| Cylinder No.: | 1 | 2 | 3 | 4 | 5 | 6 |
| Compression | 78/80 | 70/80 | 45/80 | 60/80 | 78/80 | 0/80 |
The cylinders were then removed from the engine and subjected to a second, differential compression check on a test bench. During testing, the valves were tapped to ensure any debris was not preventing a good seal. All cylinders then reached or exceeded 70/80 except cylinder No. 6, which only attained 5/80. The leak from cylinder No. 6 was visually identified as coming from both valve seats.
The valves from cylinder No. 6 were removed and the seating surface contact was examined. The seating faces were uneven (nonconcentric), particularly on the intake, and the exhaust seat had a low spot consistent with the valve not sealing properly (Figure 18). The poorly seated valves would have accounted for the low compression although the valves appeared in good condition with no evidence of carbon build-up. The No. 6 cylinder had been overhauled in 2016 and a vacuum pressure test was reportedly conducted at the time to check for leaking, however the results weren’t recorded. After overhaul, the cylinder was stored until installation in VH-IDW in 2022.
Figure 18: No. 6 cylinder intake and exhaust seats showing nonconcentric valve seating and low spot

Source: ATSB
The engine examination also found corrosion in all intake tubes, consistent with post-accident moisture from the impact in the swamp.
Prior to removing the cylinders, the valve trains were removed, and the hydraulic plungers were returned to a dry/deflated condition. After reassembly, the rocker arm to valve clearances were checked and only 5 of the 12 clearances were found to be within the engine manufacturer’s service limits. Table 3 shows the resulting clearances, with those out of service limits highlighted in red. Valve clearances were set on installation of the cylinder and can vary with wear. Insufficient clearance may prevent the valve from closing properly and excessive clearance can reduce valve lift and duration.
Table 3: Rocker arm to valve clearance – red denotes outside limits (0.28–0.80”)
| Cylinder No. | Intake valve | Exhaust valve |
|---|---|---|
| 1 | 0.110 | 0.047 |
| 2 | 0.022 | 0.024 |
| 3 | 0.032 | 0.036 |
| 4 | 0.016 | 0.095 |
| 5 | 0.000 | 0.052 |
| 6 | 0.000 | 0.047 |
The low compression in cylinder No. 6 would reduce the maximum power output and at any achievable power output, the fuel consumption would be higher than an engine with compressions within service limits. No defects were identified that should have resulted in sudden power loss or engine stoppage.
The ATSB also obtained an expert opinion from the engine manufacturer, regarding the engine and specifically the low compression result. They advised that low compression in the cold test scenario was not necessarily representative of results obtained from a warm engine. They also stated that the low compression would not result in a significant power reduction or sudden engine stoppage.
Loose B nut
At the engine examination, it was identified that the ‘B’ nut[14] on the fuel control unit (FCU) was loose – about 1.5 turns from tight. This was not indicative of its security at the time of the accident as it was loosened by an ATSB investigator during engine removal prior to shipping for examination.
Ignition system
The engine data plate recorded the engine-to-magneto timing as 20° before top dead centre. The left magneto[15] timing to the engine was found at about 35° and the right magneto timing at 23°. The incorrect timing of the left magneto was assessed as having resulted from impact forces, which resulted in mount fracture and anticlockwise rotation of the magneto that advanced the timing. The external oil filter impacted the right magneto.
Testing of spark plugs and visual inspection of the ignition leads found no defects of the ignition system.
The magnetos were functionally tested and internally inspected at a CASA-authorised electrical and instrument maintenance facility, under the supervision of the ATSB. The magnetos were run on a test bench and both functioned throughout the normal operating range, with nil faults. The magnetos were then partially disassembled for internal examination and testing including points gap and continuity, internal timing, coil and capacitor serviceability. Both magnetos were found to be in normal operating condition.
Fuel system examination
Fuel tanks
The fuel system includes one main and one auxiliary tank, a gascolator, and a shut-off valve, with the associated pilot control knob located between the front seats. The fuel shut-off selector knob was found separated from the control tube and free to rotate however, the valve position was consistent with the fuel selected to the on position. The auxiliary tank was correctly interconnected with the main tank and, due to it being mounted higher than the main tank, would empty first while fuel remained in the main tank. The inter-tank flexible hose assembly was found clear of obstructions.
The fuel tank bladders remained intact despite splitting along riveted joins and punctures to the outer aluminium tanks. The aluminium tanks showed impact damage and subtle deformation (Figure 19 and Figure 20). Robinson assessed that the deformation of the fuel tanks was consistent with ‘lower fuel quantity’ but could not determine whether the deformation was due to impact damage, bulging of internal contents, or a combination of both. Robinson provided an image of an auxiliary tank that was known to have been nearly full at impact for comparison, which presented severe bulging over the entire tank (Figure 20). When compared with the exemplar image, the damage to VH-IDW’s fuel tanks was assessed as representative of the high vertical impact resulting in severe distortion to the airframe around the tanks, with little or no fuel within. This was also consistent with an ATSB investigation into a previous Robinson R22 accident, in which the tank was half-full on impact and displayed distinctive bulging from the internal contents that was not evident in the deformation of VH-IDW’s tanks.
Figure 19: VH-IDW’s auxiliary and main tanks showing subtle deformation and compression damage

Source: ATSB
Figure 20: An exemplar auxiliary tank known to be nearly full at impact and VH-IDW’s

Source: RHC, annotated by the ATSB
All remnant fuel was drained from the main tank on arrival at Darwin. It comprised about 250 ml of blue fuel (Figure 25), contained minimal debris/sediment and was tested clear of water. No fuel was found in the auxiliary tank. Noting as detailed previously (see the section titled Fuel capacity, calibration and indications) that the helicopter’s fuel system had 4 L of unusable fuel, the relatively small recovered quantity indicated that fuel had either been removed from the tanks after the accident or, considered more likely, had leaked out following the accident and/or during the transport from the accident site to Darwin.
Pressurised fuel system
The pressurised fuel system includes an engine-driven fuel pump, an electric (auxiliary) fuel pump and a fuel return line, which allows pump supply in excess of engine demand to return to the fuel tanks. If pressure from the electric pump is low in flight, a pressure switch illuminates the auxiliary fuel pump caution light. Return fuel passed through the fuel pressure relief valve (FPRV) and then flowed to a tee junction connected to the auxiliary tank. The return fuel jet and tee assembly were found to be installed correctly.
The FPRV was tested on a rig, to simulate both fuel return and static leak from the tank back into the engine fuel system. The FPRV fully opened at about the expected parameter however, a small bypass at lower pressures was noted. Robinson reported that the flow curve was similar to other FPRVs they have seen with significant time in service, and advised that:
The electric fuel pump was connected to a power source and operated. The pump was then disassembled, and the pump vane could be rotated manually. The electric motor was worn, with brushes almost down to the leads and the commutator grooved (Figure 21).
Figure 21: Electric fuel pump showing worn brush and commutator
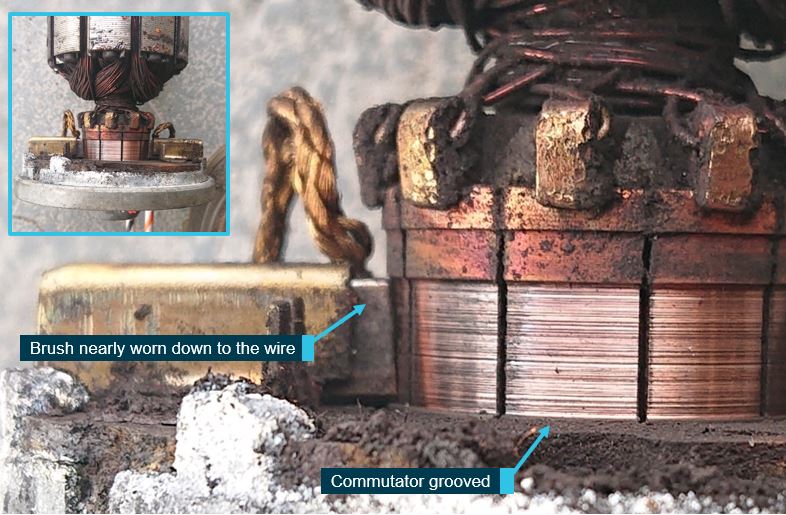
Source: ATSB
There was no sign of particulate contamination or water in the fuel system.
The mechanical (engine-driven) fuel pump serial number matched that recorded as being installed on 7 February 2022. The pump was not blocked, and no defects were found. In addition, function of the driving plunger was observed with engine rotation.
Fuel control unit examination
The FCU was examined by a specialist at a CASA-authorised maintenance facility, overseen by the ATSB. There was no fuel found in the FCU, and the finger filter was clear. The throttle arm was distorted and there was damage to the FCU body, near the mixture control lever, consistent with impact forces. The nozzles were all visually clear and were bench tested. The fuel flow was within the service limits for overhauled nozzles (31.4–32.6 lb/h) except No. 6, which was slightly low (31.0 lb/h). The fuel system specialist advised the slightly reduced flow would not stop the engine from operating.
On the test bench, the FCU tested slightly high (running slightly rich) at the lower power setting, and within limits at all other settings including maximum power. The specialist advised that it was not uncommon for the low-test point to become overly rich. During the testing, flushed fuel was passed through a filter membrane with no contaminants collected. The FCU diaphragm was in good condition and there was no evidence of water contamination in the FCU. Throughout the examination and disassembly no seals or O-rings were found to be failed or damaged. The throttle mechanism was functional.
Fuel system disruption
The fuel lines, flow divider and gascolator were all clean, and empty of fuel. The gascolator drain valve was found depressed against the firewall when examined at the Darwin hangar but reset when manipulated. Upward forces during impact distorted the aircraft structure around the drain assembly resulting in the drain extender tube, used to compress the drain valve, bending and splitting (Figure 22).
Following removal from the accident site, yellow sand was observed in the end of the tube, which was consistent with the site where the helicopter was set down during the wreckage retrieval. The sand likely entered the tube as the skids were removed prior to extrication of the wreckage from the swamp, leaving the tube as the lowest point below the fuselage. The gascolator bowl was dry and the filter screen was clear. Examination of the cowls did not identify any discolouration or staining that would be associated with leaking fuel, either prior to, or after the accident.
Figure 22: Gascolator, drain valve and tube, and R44 II Illustrated Parts Catalog extract

Source: Robinson Helicopter Company and ATSB
The fuel flow transducer, positioned between the fuel control unit and flow divider, had a fractured outlet fitting. The fracture surface was consistent with impact damage, with no evidence of pre‑existing fatigue. On behalf of the ATSB, Robinson conducted a test by removing the fuel line (and transducer) from the FCU outlet with the fuel valve open, mixture full rich and throttle full open. Robinson found that due to gravity, the fuel flowed out at a significant rate and would eventually empty the tanks. Loose black organic soil consistent with the accident site filled the transducer end of the fractured fitting (Figure 23), which likely would have been dislodged at the fuel flow rate demonstrated by Robinson.
The flow divider was opened and noted to be dry and clean, and there were no contaminants or restrictions that would have prevented fuel flowing through each of the nozzles and into the cylinders.
Figure 23: Fractured fitting between transducer and flow divider
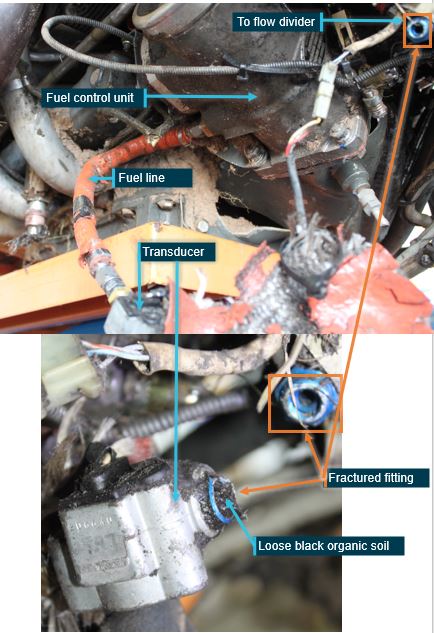
Source: ATSB
The fuel gauges and low fuel switch were independent systems, in that the low fuel switch would illuminate the low fuel warning lamp, independently of the fuel sender position. The float-operated low fuel switch assembly, located in the main tank, was electrically tested, while manipulating the float up and down, and found to be functional. Additionally, the low fuel switch and lamp were signed off as having been tested by the maintainer on 7 February 2022, as part of the periodic inspection.
The ATSB removed the fuel quantity senders from both tanks and tested the sender calibration in Darwin in June 2022. Further testing of the main tank senders and gauge was conducted by Northern Territory Police on behalf of ATSB in August 2023.
Both senders moved smoothly throughout the operating range. The R44 Maintenance Manual fuel quantity sender check specified positioning the float arm at 4 noted heights and measuring the resistance at each point to verify it was within the specified tolerance. The main tank sender could not be positioned to the up stop height and at the down stop was slightly below the down stop height for the testing, and measured slightly above the resistance range at the intermediate heights. When the fuel gauge was connected to the sender and a power source, the fuel quantity indicator needle moved smoothly from empty to full. The 4 sender test heights corresponded to the gauge indications at Empty, 1/4,1/2 and Full. As a result of the sender float arm position, the gauge very slightly overread (within a needle-width) at the lower 3 indications.
The results were sent to Robinson for expert assessment. Robinson advised that the testing indicated the main tank gauge would have been reading slightly higher than what was actually in the main tank, but ‘nowhere near’ the calibration sticker figures, which indicated the main tank gauge was underreading.
Examination of the auxiliary tank sender base plate identified a slight bend to the sender pole and that the strainer and siphon assemblies were distorted. It could not be determined if the distortion was associated with the fuselage impact forces, or pre-existing. Regardless, the strainer distortion would not have affected fuel flow to the tank interconnect hose. In addition, the siphon, part of the fuel tank drain system would have no effect on fuel supply to the engine. The ATSB determined that the auxiliary tank sender was within the required resistance range at the up and down stops.
Partial power loss
Robinson advised that main rotor blade strike, or strikes, to a tree could stall an engine at low power or idle, prior to impact with the terrain. The ATSB assessed all available evidence against the engine manufacturer’s troubleshooting tables for Low power and uneven running and Failure of engine to develop full power. In addition, the 29 items on Robinson’s troubleshooting checklist for low power were reviewed. All applicable items were tested where possible, within the constraints of damage. Nothing was identified that would likely result in a sudden onset of low power.
Fuel considerations
Fuel uplift
Procedure for filling tanks
The placard adjacent to the auxiliary fuel tank stated that the procedure to fill the tanks to full fuel entailed filling the main tank, then the auxiliary tank, then topping up the main tank. This procedure was required due to the self-levelling of the interconnected tanks.
The Helibrook operations manual included a procedure for hot refuelling (with the engine running). The manual stated that Robinson helicopters were not to be refuelled with the engine running,
The Helibrook safety manager advised that they did not have a completed form for the pilot or the egg collector of VH-IDW, and there was no other evidence to indicate whether they had undertaken the training. The egg collector in the second helicopter to land at Mount Borradaile previously flew and collected eggs for Helibrook and was the only person present who had completed the required training to hot refuel a Helibrook R44 helicopter.
Noonamah
Based on interviews with the helicopter operator, pilot and fuel supplier, and the 2 most recently delivered fuel batch receipts, the Noonamah fuel storage tank contained blue 100 low lead (LL) Avgas. A total fuel quantity of 440 L was recorded as being taken from the Noonamah tank on 28 February, but there were no records of the quantity uplifted to individual helicopters. As well as VH-IDW, at least one of the other 2 R44 helicopters was reportedly refuelled when they arrived at Noonamah at about 0645 and several jerry cans were also filled from the Noonamah storage tank. The Helibrook R44 helicopter that flew to the site after the accident may also have used fuel included in that total.
The quantity and source of fuel remaining in VH-IDW prior to refuelling on the accident morning could not be determined. The accident pilot reported that they would have filled the helicopter to full at Noonamah, in accordance with normal procedures. They also stated that their usual practice was to set the chronometer to zero after fuelling the helicopter. Other pilots reported that normal practice was to ensure sufficient fuel to get to Mount Borradaile, but not necessarily to fill both tanks.
In a submission provided to the ATSB following review of the draft report, one of the egg collectors operating on the accident day reported that VH-IDW was filled with 100 LL fuel at a Helibrook base near Sweets Lagoon, 33 NM from Noonamah at the end of the previous day’s activities. They further reported that they were present at the hangar on the accident morning and had not observed VH-IDW being fuelled. Based on that account, if the helicopter was not refuelled at the hangar on the accident morning it would have departed Noonamah with 23-25 L less than the full fuel tank capacity.
As detailed previously, based on the georeferenced in-flight photograph, VH-IDW probably arrived at Mount Borradaile at about 0816. This time was consistent with the departure and arrival time recorded on a GPS device on the third R44 helicopter to arrive at Mount Borradaile that morning.
There were no records of the fuel uplifted at Mount Borradaile. Those present at Mount Borradaile reported that the R44 helicopters were hot refuelled. The accident pilot reported that their normal action was to always fill the helicopter to full at Mount Borradaile.
An Airbus/Eurocopter AS350 helicopter, with a pilot and crewman onboard, had landed at Mount Borradaile before the three R44 helicopters arrived. The helicopter was associated with the crocodile egg collection and its pilot was waiting for the pilot of the third R44 helicopter, who was the operator of the AS350, to assist with a maintenance issue with the AS350.
In preparation for the R44 refuelling, the AS350 crewman rolled 2 200 L drums out, checked they were marked WHNT, and verified they were labelled 100/130 green Avgas. They further recalled that the first drum had been partly used, and its lid was on tightly and difficult to open.
The helicopter crews reported that VH-IDW arrived first of the 3 R44s at Mount Borradaile. There were consistent recollections that the egg collector was in the pilot seat of VH‑IDW, and the accident pilot was in the passenger seat of VH-IDW, when it arrived. Pilot 2 (P2) and egg collector 2 (E2) were in the second helicopter and pilot 3 (P3) and egg collector 3 (E3) in the third.
When P3 arrived, they reportedly went immediately to the AS350 and did not witness the refuelling. The accident pilot could not confidently recall the refuelling events at Mount Borradaile, other than that they got into the third R44 and moved it up to the fuel drum. P2 reported that there was no drum pump carried in VH-IDW that day, and the pump used for refuelling was from the second helicopter. P2 and E2 reported that the pump from their helicopter was used by the accident pilot to put fuel into the main tank of VH-IDW, before the second helicopter moved to the drum. A submission to the ATSB following review of the draft report included a statement made in April 2023 by E2. In their statement, E2 reported that they had not seen VH-IDW being refuelled at Mount Borradaile.
In a statement to the ATSB in March 2022, E3 reported that when they arrived in the third helicopter at Mount Borradaile, they went to hold the hose for the accident pilot, who was getting ready to fuel VH‑IDW. They recalled that the third helicopter was refuelled next, and the second helicopter was still refuelling when the other 2 helicopters departed Mount Borradaile. However, in a subsequent statement in September 2022, E3 stated that they observed the egg collector partially fuelling VH-IDW before they took over and personally filled VH-IDW to full after first helping to refuel the third helicopter.
The AS350 crew reported that the 3 R44 helicopters left Mount Borradaile at 0830, which was consistent with the OzRunways recorded data for 2 of the 3 helicopters.
Based on the planned fuel figures, each R44 would have consumed about 80–90 L of fuel to reach Mount Borradaile. They therefore needed at least 80–90 L to fully fill at Mount Borradaile (noting that would have resulted in a minimum of 50% of the fuel in the tanks being 100/130 Avgas). The pump transferred about 1 L per revolution from the drum to the tank. After refuelling, the standard operating procedure required pilots to conduct fuel drains from 3 points on each helicopter to check for water and other contaminants. It was possible to fill each helicopter within a few minutes, particularly as several people capable of pumping fuel and conducting fuel drains were at Mount Borradaile.
The WHNT fuel drums at Mount Borradaile contained green-coloured 100/130 ‘leaded’ fuel.[16] The same person who rolled out the 2 fuel drums for the R44 pilots to refuel on the accident day, subsequently identified those drums and provided samples to the ATSB for testing. The person identified that as the drums had been reused, they had old 100 LL labels on the side, and the current 100/130 fuel labels on the top (Figure 24). WHNT was also clearly painted on the drums. The person checked the labels and seals, and recalled that the fuel in the drums was green.
Figure 24: WHNT fuel drum at Mount Borradaile showing distinct paint and labels. Inset: Fuel sample

Source: Supplied, annotated by the ATSB
The first drum rolled out was emptied on the accident morning then placed upside down by the AS350 crewman. As a result, when that crew person subsequently obtained fuel samples on behalf of the ATSB, the drum was distinctive as it had mud on the lid from having stood inverted. It was identified as the drum most likely to have been used first on the accident morning and VH‑IDW was reportedly the first helicopter to land at Mount Borradaile that morning. Samples from all 4 WHNT 100/130 drums at Mount Borradaile were taken to Darwin by WHNT and the ATSB arranged for the fuel to be tested.
The ATSB was subsequently advised that there were many empty fuel drums at Mount Borradaile, including some containing 100 LL located near the 100/130 drums. This raised the possibility that the drums used on the day of the accident may have been misidentified when samples were subsequently collected on behalf of the ATSB. However, a photo of one of those drums showed it was not painted with WHNT but was labelled with a different crocodile farm name and had a fuel expiry date of 13 October 2021. Additionally, the owner of the fuel supply reported that due to the remoteness and the criticality of having fuel available, they would not expect pilots to use fuel purchased for other operators and had not been advised of any fuel being wrongly taken.
Fuel testing and analysis
Testing of the fuel drained from VH-IDW found it was consistent with 100 LL fuel, partially evaporated due to handling post-accident (see Appendix A – Fuel analysis). Gas chromatography with mass spectrometry testing of the VH-IDW sample found that it comprised less than approximately 1% 100/130 Avgas (1% was the testing limit of distinguishing between 100 LL and 100/130). There was also no evidence of contamination with Jet A-1, diesel, premium 98 petrol (car fuel) or Opal (low-aromatic car fuel used in the Northern Territory).
Samples from the 4 drums at Mount Borradaile containing green 100/130 fuel supplied by WHNT were obtained. The fuel from the 2 drums identified as having been used on the accident morning, were tested and found to meet the specifications of 100/130 fuel in accordance with the supplied batch test results. Figure 25 shows the colour of the Mount Borradaile sample compared with the remaining fuel recovered from VH‑IDW.
Figure 25: Comparison of Mount Borradaile sample and VH-IDW fuel

Source: ATSB
Fuel jerry cans
Images provided to the ATSB from first responders at the accident site showed 2 jerry cans in VH‑IDW, one behind each of the front seats. The jerry cans were subsequently removed from the helicopter and were not at the site when the ATSB arrived, nor subsequently provided to verify their contents. Those first on site and the accident pilot reported that both were full at the time of the accident and had probably been filled at Noonamah that morning. The jerry can behind the pilot seat was reportedly damaged on impact and may have leaked fuel, although no one reported detecting fuel leaking at the time.
The ATSB considered the potential effect of interference with the site in relation to the laboratory fuel testing results. The only plausible scenario that permitted both the described full refuelling at Mount Borradaile with 100/130 fuel and the residual 100 LL identified in testing was if 40 L of 100 LL fuel was poured from the jerry cans into VH-IDW after the accident and then most of it subsequently leaked away before the ATSB assessed the tank fuel quantity on arrival at the accident site. To dilute the 100/130 fuel component to less than the tested 1%, there would have to have been less than approximately 800 ml of fuel remaining in tank at the time prior to the addition of 100 LL from the jerry cans, comprised of approximately 50% 100/130 and 50% 100 LL fuel.
No one at the site, including the first to arrive, who was there until 1555, reported seeing anyone pour fuel into, or drain fuel from, VH-IDW. It was also reported that fuel from the 2 jerry cans was emptied into other helicopters that attended the site prior to their return to Darwin. Further, the empty jerry cans were then reportedly used to transfer fuel from a fuel drum to a helicopter at Mount Borradaile on the return to Darwin.
Fuel flow
The Helibrook operations manual required pilots to use a fuel flow rate of 60 L/h for flight planning purposes for R44 II helicopters for ‘normal, specialised and holding’, and a fixed reserve of 20 minutes (20 L). In a submission to the ATSB draft report, the pilot stated that VH‑IDW’s normal fuel burn was 60 L/h. The operator reported that VH-IDW normally consumed about 65–70 L/h.
Robinson does not publish fuel flow rates for their helicopters. They provide a planning fuel flow of 60 L/h and guidance including to record the hour meter reading each time fuel tanks are filled, check the fuel level in the tanks visually, continually check hour meter and fuel gauges, and to refuel before the main tank fuel gauge reads less than 1/4 full.
With 176 L of usable fuel (full fuel) with no reserves, VH-IDW would have the following endurance:
- 2 hours 56 minutes at 60 L/h
- 2 hours 42 minutes at 65 L/h
- 2 hours 31 minutes at 70 L/h.
Required engine power, and therefore fuel flow, is highest during take-off, landing and while hovering. As such, when conducting low‑speed flight while carrying an external load, the engine would be operating at high power and fuel flow rate.
Low compression in one cylinder results in less power produced compared to the other cylinders. Therefore, a higher power setting and increased overall fuel usage would be required to achieve the same airspeed as a fully serviceable engine. The actual increase in fuel consumption on the accident day due to low compression in the number 6 cylinder could not be quantified as the specific compression was unknown.
Regarding in-flight fuel re-planning and quantity measurement, the Helibrook operations manual stated:
Single-pilot low-level aerial work activities undertaken by this company are such that the priority of maintaining control of the aircraft and awareness of their surroundings prevents more than a visual scan of the fuel quantity gauges. For these operations where the recording of fuel figures may be detrimental to safe flight, fuel state will be managed using visual gauge checks, watches and reference to elapsed flight time.
The pilot reported never using the fitted fuel flow meter and the display was not visible in the in‑flight photo.
Operational information
Loading and performance
The RFMS required that the weight and centre of gravity be checked to verify the helicopter remained within the approved limits throughout each flight. Although not required to be documented, there was no evidence that a weight and balance assessment had been conducted on the accident day.
Based on photos, interviews, and evidence from the accident site, when the helicopter departed Noonamah on the accident morning with the pilot and egg collector on board, its contents included:
- slinging equipment
- 6 to 10 egg collecting buckets and poles
- 2 x 20 L jerry cans filled with 100 LL Avgas fuel
- 8 x 1 quart (0.95 L) engine oil cartons
- fishing rod/s, firearms, drink bottles, ammunition and personal effects.
The ATSB did not have access to many of these items and it is unknown if other items may have been on board but removed from the site. Therefore, the helicopter’s exact total weight at the time of the accident could not be calculated. However, based on the available information, the helicopter was likely operating below the maximum allowable weight of 1,134 kg at the time of the accident.
In addition to the gross weight limit, it was also a requirement of the RFMS for HEC operations that the aircraft was operated at a weight at which the helicopter could hover out of ground (OGE) effect[17] at least 3,000 ft above the ground. Due to the above uncertainty associated with the helicopter’s actual weight (including its fuel quantity), and the identified low engine cylinder compression, it was not possible to determine whether OGE performance existed at the time of the accident. However, in the ambient conditions at the time of the accident, the helicopter would not have met the 3,000 ft out of ground effect hover capability requirement at its maximum gross weight (1,134 kg).
The RFMS also stated that the maximum weight permitted on the dual hooks was 129 kg including the sling person, line, harness, equipment, bucket and crocodile eggs. At the time of the accident, the egg collector with equipment weighed 118 kg and the line weighed 26 kg. The total weight on the hooks was therefore 144 kg plus the bucket, pole and small items that were not weighed. Although this exceeded the permitted weight, there was no evidence the hooks or associated equipment had failed.
Autorotation
In the event of an engine power loss, drive is no longer supplied to the rotor system and the pilot must lower the collective and sometimes conduct an initial flare to maintain sufficient rotor RPM while establishing autorotation. In an autorotation, the rotor blades are driven solely by the upward flow of air through the main rotor. The total energy available for an autorotation in the event of a power loss comes from the kinetic energy of the rotor blades and airspeed, and potential energy, which is directly proportional to the height.
Several factors affect the rate of descent in autorotation: bank angle, density altitude, gross weight, rotor RPM, trim condition, and airspeed. Two aspects pilots commonly use for managing distance travelled and rate of descent, are airspeed and rotor RPM.
In an autorotation in an R44 II, the rate of descent is high at zero airspeed, lowest at 55 kt, and increases again at higher airspeeds. The only energy available to arrest the descent rate for landing is the forward speed of the helicopter and the rotational kinetic energy stored in the rotor blades. Maintaining adequate rotor RPM is essential to ensure sufficient energy to flare the helicopter for landing. The flare is a critical manoeuvre that ensures safe completion of a power-off landing. The flare simultaneously decreases forward speed and rate of descent while increasing rotor RPM. Flaring too far away from the ground will leave the helicopter without sufficient energy to cushion the landing.
The R44 II POH stipulated that in the event of complete power loss, the pilot was to immediately lower the collective to enter autorotation. The specific procedure for power failure between 8 and 500 ft above ground level was:
- Lower collective immediately to maintain rotor RPM.
- Adjust collective to keep RPM between 97 and 108% or apply full down collective if light weight prevents attaining above 97%.
- Maintain airspeed until ground is approached, then begin cyclic flare to reduce rate of descent and forward speed.
- At about 8 feet AGL, apply forward cyclic to level ship and raise collective just before touchdown to cushion landing. Touch down in level attitude and nose straight ahead.
The minimum rate of descent during an autorotation was about 1,350 ft per minute at an airspeed of 55 kt and rotor RPM 97% when below 500 ft.
Height-velocity diagram
A height-velocity (H/V) diagram is required for single-engine helicopters certified under FAR Part 27. The diagram:
defines an envelope of airspeed and height above the ground from which a safe power-off or one engine inoperative (OEI) landing cannot be made (FAA, 2014).
The Robinson R44 II Pilot’s Operating Handbook (POH)[18] included the H/V diagram for R44 II helicopters, including VH-IDW (Figure 26).
Figure 26: Robinson R44 II height-velocity diagram
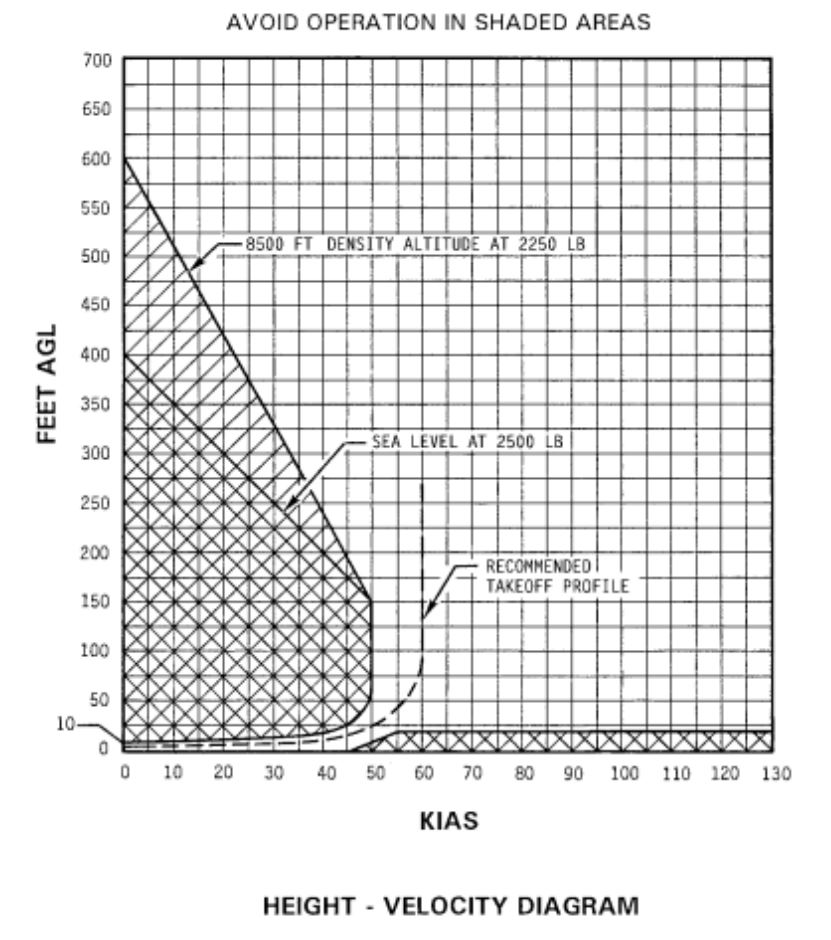
Source: Robinson Helicopter Company R44 II POH
When operating at low speed in the shaded (or ‘avoid’) area on the left side of the diagram, in the event of a power loss, a pilot may have insufficient height to accelerate to the speed required to autorotate successfully (autorotation speed).[19] Above a certain height above the ground, at least 400 ft for the R44 II depending on the density altitude, it is possible for a pilot to achieve autorotation speed even from a high hover (FAA, 2019). In the shaded area on the lower right side of the diagram, the combination of faster airspeed and proximity to the ground provides limited reaction time for the pilot in the event of in-flight emergencies. The FAA Helicopter Flying Handbook (FAA, 2019), stated:
The unshaded region of the diagram shows the combinations of airspeed and height above the ground that allows a pilot to successfully complete a landing in a full autorotation without requiring exceptional skill. At low heights (below about 10 ft) with low airspeed, such as a hover taxi, the helicopter is in a safe part of the H/V diagram. There, a pilot can use the kinetic energy from the rotor disc to cushion the landing with collective, converting rotational inertia to lift. An increase in height without a corresponding increase in airspeed puts the helicopter above a survivable un‑cushioned impact height, until a height is reached from which rotor inertia and gravitational potential energy can be converted to sufficient lift to reduce the vertical velocity at impact to a survivable value (FAA, 2019).
Rotorcraft flight manual supplement
Limitations and procedures for HEC operations
A requirement of certification of the dual hooks for HEC was to have the appropriate limitations and procedures for conducting human external cargo operations incorporated in the rotorcraft flight manual supplement (RFMS). The first draft of the RFMS associated with the STC for the hooks system was developed in 2013, and revision 13 of the R44 RFMS for HEC Dual Hook was approved by CASA, along with the STC, in July 2021.
The CASA-approved rotorcraft flight manual supplement
The CASA-approved RFMS and associated STC were specifically for the activity of collecting crocodile eggs, and some operational procedures were included in the RFMS. The RFMS Introduction stated that it was only valid if the operator also had ‘CASA approved operational procedures for use of the HEC Dual Hook system’.
The RFMS Section 1 General, contained a warning of elevated risk to aircrew ‘and particularly the Human External Cargo (HEC)’ involved in helicopter crocodile egg collection operations. The elevated risks included:
It then detailed additional risks including the:
- ‘use of a low powered single piston engine helicopter’
- lack of a ‘spotter’ in the aircraft due to R44 weight restrictions
- isolated nature of crocodile egg collection
- potential for crocodile attack.
Section 2 Limitations included:
- a maximum airspeed of 60 kt during HEC operations
- maximum 15 kt wind
- no operations within 5 NM of lightning
- a weight limit such that the helicopter has out-of-ground-effect hover capability at least 3,000 ft above ground level
- maximum 129 kg down weight: combined weight carried on the hooks including the HEC person, line, harness, equipment, crocodile eggs and their container
- HEC line length between 48 and 105 ft (15–32 m).
The RFMS Section 3 Emergency procedures stated:
In establishing the emergency procedures, the design engineer advised that considerations of the line disconnecting (uncommanded) resulting in release of the HEC, were addressed by the hooks’ compliance with FAR certification standards for hooks for HEC. They reported that it was recognised that engine failure was the biggest risk. In managing this risk, the expectation was that an engine would rarely stop suddenly – usually running rough and degrading over a period of 30–60 seconds before stopping. It was considered that expected behaviour should give a pilot time to manoeuvre the helicopter away from the HEC, preferably downwind.
Furthermore, the design engineer advised that the emergency procedures were based on minimising risk to the HEC because the sling person was unprotected, whereas the pilot had a seat, restraint, and airframe as protection. Jettisoning the HEC from higher than 10 to 15 ft above ground would likely result in fatality, therefore keeping the HEC on the line while the helicopter autorotated, was assessed as offering a better overall outcome. The design engineer reported that at the time of the STC approval, the FAA advised that they could see ‘almost no circumstances in which the pilot would release the HEC’, but that more recently FAA’s emphasis had changed to requiring a very high degree of engine and systems reliability.
Comparison emergency procedures
US Department of the Interior
The US Department of the Interior (DOI) defined the transport of one or more people suspended beneath a helicopter as ‘short-haul’. The DOI Helicopter Short-Haul Handbook outlined minimum policies, procedures, qualifications, training requirements and equipment for helicopter short-haul programs, and was accepted as ‘best-practice’ guidance material.
Chapter 6: Emergency procedures (US DOI, 2010) stated:
The only difference between this text and the CASA-approved RFMS Emergency procedures, was that the DOI Handbook stated that ‘Release of the short-haul line is a possible consideration’, whereas the RFMS stated ‘Apart from in exceptional circumstances, release of the HEC line is not an operational consideration’, while HEC is attached beneath the aircraft. Both documents stated that the HEC survival was best assured by the sling person remaining attached to the line in the event of an emergency landing.
Other dual hooks for HEC RFMS
There were no STCs for dual hooks for HEC for R44 helicopters in Canada or the US. The ATSB reviewed the RFMS and STCs for dual hooks for HEC (using single turbine engine helicopters) that were approved in Canada and the US. Those STCs were used for multiple activities, unlike the R44 dual hooks with HEC for crocodile egg collection, which were only approved for that activity.
In Canada, single turbine engine HEC was only approved for rescue and similar activities considered to be in the public interest, that is, where there is a value of life consideration. The RFMS approved by Transport Canada incorporated only emergency procedures as they related to failure of the hook system. For example, a Transport Canada-approved RFMS for Bell 206L‑series helicopters HEC dual hook system Emergency/malfunction procedures section consisted of:
- the need to release both hooks to jettison HEC
- actions in the event of (hydraulic) failure of the PQRS to open the HEC hook
- uncommanded release of either hook system.
An FAA-approved RFMS for Bell 206L/407 had emergency procedures for the event of electrical failure of the hooks, plus the following statement:
An FAA-approved RFMS for MD Helicopters MD 369 Emergency procedures stated:
In summary, a Transport Canada-approved test pilot advised that an RFMS associated with an STC for dual hooks for HEC would document how to release a load, and procedures in the event of failure of the hooks or quick release system (QRS), but would not address particular operational scenarios. The expectation was that these would generally be contained in an operator’s standard operating procedures approved by the Operational Authority.
Operator information
Helibrook
Helibrook held an air operator’s certificate issued 2 April 2020, with an expiry date of 31 July 2022. Under the certificate, Helibrook was permitted to conduct charter and aerial work operations, including sling load operations. At the time of the accident, Helibrook had one Bell 206L and 3 Robinson R44 II helicopters.
The 3 key positions at Helibrook were the head of aircraft airworthiness and maintenance control (HAAMC), who was the accident pilot of VH-IDW, the chief executive officer (CEO), who was also the chief pilot, and the safety manager.
Head of aircraft airworthiness and maintenance control
The accident pilot was a licenced aircraft maintenance engineer and had held the role of Helibrook’s HAAMC since 12 July 2019. The Helibrook operations manual defined the HAAMC role as follows.
Chief pilot
The chief pilot was responsible to CASA for all operational matters affecting the safety of flying operations. The chief pilot’s responsibilities listed in Helibrook’s operations manual included:
- safe and efficient operation of the aircraft
- monitoring operational standards
- maintaining training records and supervising the training and checking of pilots and crew including of equipment used
- ensuring pilot flight and duty times were accurately recorded
- ensuring the aircraft were appropriately maintained.
Prior to holding the chief pilot role, the Helibrook CEO had been subject to CASA enforcement action. As a result, CASA imposed a variation on the pilot’s helicopter licence. The variation required the CEO to attend aviation theory remedial training and testing, and complete four 6‑monthly flight reviews with a CASA-approved examiner. These were aimed at ensuring ongoing proficiency in making appropriate safety judgements.
The CEO reported completing the first of those flight reviews and aviation theory training on 6 July 2019. On the same day, the CEO submitted an application to CASA for approval to become Helibrook’s chief pilot. The applicant’s previous breaches meant they did not meet one of the criteria for the chief pilot appointment, which required the person to have ‘maintained a satisfactory record in the conduct or management of flying operations’. CASA offered the applicant the opportunity to demonstrate an acceptable means of compliance with that requirement and submit a safety case stating how they would manage the risks.
Having provided a response to CASA, the chief pilot applicant was required to conduct 2 flights with a CASA flight operations inspector and complete associated ground activities. The CEO conducted the first CASA assessment flight on 6 August 2019 and was assessed satisfactory. The activities assessed were a charter flight and simulated crocodile egg collection. The examiner identified some gaps in knowledge of recent legislation, which the applicant was reported to be working to address. The examiner’s notes described an experienced pilot with a good safety focus.
The CEO’s second chief pilot assessment flight and ground activity was conducted on 25 November 2019. The examiner commented that the CEO demonstrated the ability to supervise and mentor other pilots and was assessed as suitable for consideration for appointment as chief pilot of Helibrook.
CASA subsequently approved the CEO as Helibrook’s chief pilot on 20 January 2020. Additionally, the CEO was provided with an exemption removing the requirement for the previously imposed 6-monthly flight review checks. As part of the process for the CEO to conduct the chief pilot role, Helibrook introduced a safety management system (SMS) and appointed a safety manager.
Safety manager
The safety manager was recruited by the Helibrook CEO in August 2019. The safety manager was also assigned the roles of operations manager and drug and alcohol management plan (DAMP) officer for Helibrook. Apart from a short period in 2020, when the safety manager worked for Helibrook in the Northern Territory, including as a helicopter charter pilot, the safety manager lived interstate and conducted the safety manager, operations manager, and DAMP officer roles remotely.
Documented key responsibilities of the safety manager included:
- maintaining the safety management system and ensuring it was relevant to the operations
- conducting hazard and risk identification
- conducting incident and accident investigations.
Safety management system
Overview
Attributes of a safe organisation include a healthy safety culture with appropriate risk management processes, which achieves safety objectives through internal responsibility rather than relying on regulatory compliance (CASA, 2019). The International Civil Aviation Organization (ICAO, 2018) defined an SMS as:
It is designed to continuously improve safety performance through the identification of hazards, collection and analysis of safety data and safety information, and continuous assessment of safety risks. An SMS seeks to proactively mitigate safety risks before they result in aviation accidents and incidents.
The Helibrook SMS manual version 1.0 was issued on 1 August 2019 and accepted by CASA on 22 November 2019. Although not generally required by CASA regulations at the time, it was introduced to demonstrate a commitment to safety and thereby aid in obtaining CASA’s approval of the chief pilot. The SMS manual outlined the company’s safety policy, objectives, and responsibilities for supporting the SMS and reporting of incidents, risks and hazards. It stated:
Helibrook’s SMS manual stated that it was to be updated annually, by the CEO in collaboration with the safety manager, and that safety meetings were to occur monthly and involve the safety manager, CEO/chief pilot and HAAMC.
Safety risk management
Safety risk management includes hazard identification, and safety risk assessment, mitigation and risk acceptance (ICAO, 2018). The safety risk management process is continuous and risk mitigation strategies must be monitored to determine whether they are effective. Helibrook’s SMS manual stated the aim of risk management was ‘to treat or control risks to as low as reasonably practicable’. Their stated risk management tools included a documented risk assessment, evaluation and treatment process, a master risk register, and a regular hazard and risk review process.
Hazard identification
According to ICAO (2018), a hazard can be considered as a dormant potential for harm, which is present in one form or another within the system or its environment. Therefore, hazard identification is the first step in the safety risk management process. The intention is to proactively identify hazards before they lead to accidents, incidents, or other safety‑related occurrences. Hazard identification may also consider hazards that are generated outside of the organisation and outside their direct control, such as weather (ICAO, 2018).
The Helibrook SMS manual listed several means of identifying hazards including reporting systems, audits, staff input, and experience.
Helibrook hazards
The Helibrook hazard register, titled Hazards and Risks, listed items under 7 headings: organisation, operational, helicopter, pilot and flight crew, operating environment, weather and egg collecting. The following 2 lists are relevant to this investigation:
On 30 September 2019, in response to a request from CASA, the safety manager identified 13 hazards ‘that have the potential to cause harm to pilots and passengers’ and proposed actions to mitigate associated risks. None were associated with crocodile egg collection operations.
Risk assessment
A risk assessment is a process where hazards and the chances of an adverse event happening due to the hazard were identified, analysed, and evaluated (CASA, 2021). This evaluation was expressed in terms of likelihood and consequence and should highlight the risks to be considered before and while carrying out an operation.
Organisations should have multiple layers of controls or defences in place to manage their identified hazards (CASA, 2014). Risk assessments should be carried out across all levels of an organisation and at different stages in the operation. These could consist of a formal, documented process or a continuous ongoing mental assessment carried out by a pilot, or a combination of both. An example of a formal risk assessment would be an operational risk assessment conducted by the operator to consider and evaluate the risks associated with the type of work being undertaken.
The Helibrook operations manual stated that the ability to identify hazards and assess risks was an important component of their continuous safety improvement process. It stated that if a risk assessment was required, the chief pilot would conduct and document the process, which included assessing the risk, developing risk control strategies and implementing them, then assessing those controls. The Helibrook operations manual standard operating procedure for crocodile egg harvesting included that in the event of an aircraft failure:
- the sling person must have a clear understanding of the risk and implications of such an emergency
- the risk of injury will be reduced providing all height and speed limitations are adhered to
- prior to slinging, the pilot must advise the sling person of the high risk nature of the operation and what steps shall be taken to reduce the risk.
Risk register
Safety risk management activities should be documented, including any assumptions underlying the probability and severity assessment, decisions made, and risk controls implemented (ICAO, 2018). A tool such as a risk register could be used to ensure identified hazards were tracked and mitigated as part of a formal risk management process of prioritisation, documentation, and assessment. The register could include the hazard, potential consequences, assessment of the associated risks, and any controls put in place to manage the risk (ICAO, 2018).
Safety reporting system
The effectiveness of a safety reporting system partly relies on the promotion of a positive reporting culture and proactive identification of safety deficiencies. One way of achieving this is by clearly stating that reported information will be used solely to support the enhancement of safety (International Civil Aviation Organization, 2018). This also included a culture where people can report without fear of punishment (Reason, 1998). The Helibrook SMS described a formal reporting system as a key element of the SMS.
Safety culture
CASA SMS booklet 2 – Safety policy and objectives stated that good safety management ‘is not about having an SMS manual on the shelf…it needs context to be effective’. Further, that the ‘ultimate responsibility for safety rests on the shoulders of senior managers’, who should demonstrate a commitment to safety. This included maintaining a positive safety culture.
Safety culture has been defined as 'the set of enduring values, behaviors and attitudes regarding safety, shared by every member at every level of an organization' (SM ICG, 2019). More simply, it is ‘what goes on when no-one is watching’ (EASA, n.d.). Additionally, the effectiveness of a safety management system has been shown to be dependent on the safety culture (SM ICG, 2019).
The Hudson Ladder defined 5 steps, or maturity levels, in the evolution of safety culture (Figure 27). The first step – pathological (‘who cares as long as we’re not caught’) – was not really a culture of safety (Hudson, n.d.). The second step, a reactive safety culture, was one in which safety was a burden imposed by the regulator. In a reactive culture, action was only taken in response to an incident, and often involved blame or punishment. In a poor safety culture, ‘not everyone takes safety seriously, are not watchful, are complacent and compromise too readily’ (ARPANSA, n.d.). In contrast, a positive safety culture ensures operations are conducted as safely as practicable, which reduces the risk of accidents occurring.
CASA described safety culture elements, in which an example ‘enabler’ of a positive safety culture was that an ‘effective method of hazard identification has been established’. The converse example ‘disabler’ of a positive safety culture was ‘no effort is spent on hazard identification’ (CASA, 2021).
Figure 27: Hudson Ladder
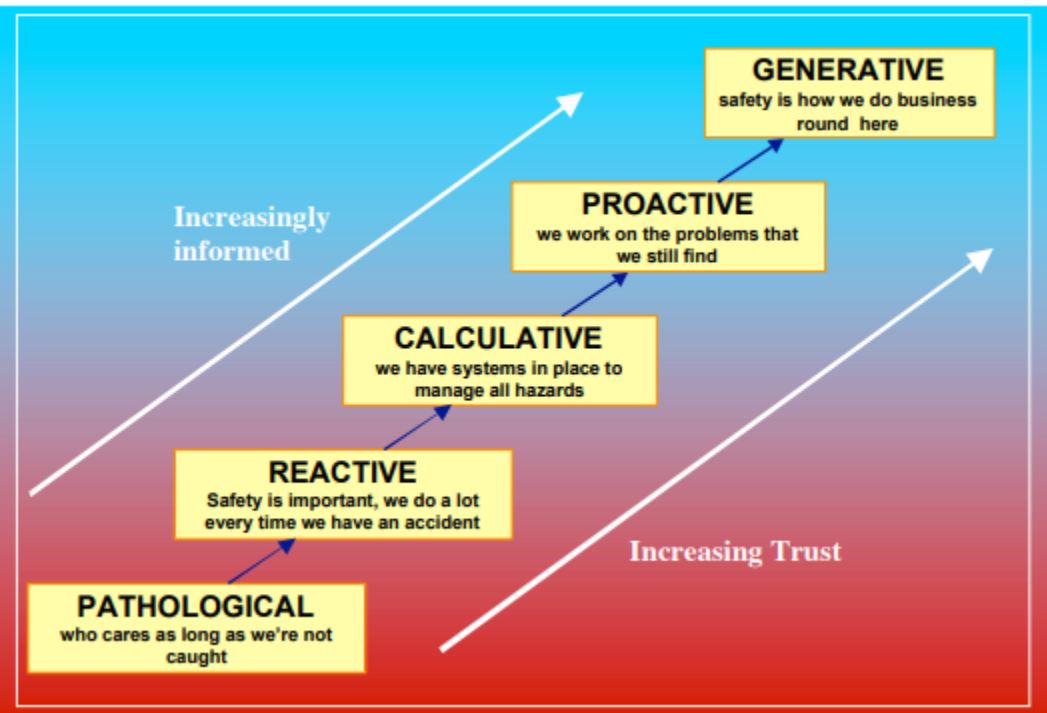
Source: Hudson n.d.
Helibrook’s safety management
Helibrook’s SMS manual had not been amended since initial issue and no meetings had been conducted since the introduction of the SMS. The safety manager described their role as ‘lacking’ and reported that most of their time was devoted to managing day-to-day operations (in their other role as Helibrook’s operations manager).
The safety manager also described the Helibrook hazard register as ‘a bit lacking’, with many of the listed items not actually hazards. Additionally, there was no assessment of risks, controls or mitigation strategies. Helibrook did not have or maintain a formal risk register, or any alternate means to track and identify hazards and associated controls for their operation. The safety manager also reported that no risk assessment had been conducted of any of Helibrook’s approved activities, including crocodile egg collection (an activity which the safety manager had not actually observed). The CASA instrument that approved human external cargo operations stipulated that human slinging could only be conducted if it was assessed as reducing the risk of heat exhaustion and/or crocodile attack. Despite that, there was no documented means of assessing the relative risks.
Safety equipment, maintenance and time to rebuild/overhaul were listed on the hazard register relating to ‘Helicopter’, however no risks had been identified with VH-IDW. The safety manager also reported being unaware that VH-IDW’s ELT was not installed.
The safety manager described Helibrook’s reporting culture as ‘not great’, with only one incident in Helibrook’s safety reporting system – a hard landing involving VH-XHB, which occurred on 30 August 2020, while the safety manager was at the site. In relation to that occurrence, the safety manager submitted an incident report to ATSB on 1 September 2020.
The report stated the pilot was the only person on board at the time of the accident. However, the ATSB obtained footage taken by one of 3 passengers on board at the time. The safety manager was nearby at the time of the accident and, despite the detail on the incident report, reported being unaware how many people were on board. The safety manager was also the Helibrook DAMP officer and had not requested drug and alcohol testing of the pilot following that incident, as they did not think the incident was sufficiently serious to warrant it. In response to that incident, the safety manager reported proposing a windsock be put in the area to assist pilots identifying the wind direction, as misidentification of the wind direction was assessed as a factor contributing to the incident.
The safety manager did not conduct an internal investigation into the accident involving VH‑IDW and several months after the accident reported that they did not know what happened, had not seen the aircraft or been able to obtain any information about it. As the DAMP officer, the safety manager had also not requested testing of the accident pilot.
Helibrook operations manual
CASA first assessed and accepted the Helibrook operations manual in December 2016. The Helibrook operations manual version 7.3 was accepted by CASA on 28 February 2020. The manual included a standard operating procedure (SOP) for crocodile egg harvesting. That SOP was approved by CASA on 11 June 2020. CASA’s approval of the slinging operation was based on reducing the overall risk of crocodile attack and heat exhaustion. The SOP stated that the primary reason for slinging personnel was to:
It further stated:
The intent of the latter statement appeared to be to avoid operating in and around a helicopter if personnel were affected by fatigue.
One requirement of the procedure was for the chief pilot to have briefed the pilot before the pilot was permitted to conduct HEC sling loads. The briefing was to include a minimum 30-minute oral brief, a minimum 30-minute equipment demonstration/inspection and a minimum of 1 hour flying time. This was to be documented on a pilot competency check form. There was no record this had been conducted for the accident pilot.
Additionally, Helibrook did not have documented training for the pilot to conduct HEC slinging operations, or evidence that the pilot had trained in Helibrook’s emergency procedures for HEC slinging. The pilot reported having demonstrated some criteria and conducted ergonomic testing of the switches with CASA, but could not recall specific training by the operator. At the start of each season, the pilot completed annual administration and recurrency with WHNT but no helicopter-based training specifically for the activity.
The pilot reported that they did not generally practise emergency procedures for slinging. In their most recent operator proficiency check, the pilot recalled conducting autorotations and other emergencies. They did not practise releasing the sling load, as the pilot reported doing it ‘every day’ and it was ‘just two pushes of the buttons’. The chief pilot reported that it was ‘too dangerous to put yourself in an autorotation in that scenario to practise’, but they did general emergencies/autorotations as part of the training.
The SOP included ‘Safety aspects to consider before approaching a nest’. It required pilots and sling persons to assess slinging access to the nest including consideration of timber, trees and obstacles. It stated: ‘Should there be obstacles that will affect the safe operation then the sling option will be abandoned’.
Pilots were also required to be ‘fully conversant’ with the CASA instrument (approving use of HEC for crocodile egg collection) including the conditions and limitations. The requirement for the pilot to brief the crew/sling person on the emergency procedures was included.
Emergency procedures for crocodile egg harvesting
Helibrook’s standard operating procedure
The SOP included the following section titled Emergency procedures:
The following emergency procedures were then specified:
| Partial engine failure malfunction |
The pilot in command shall attempt to place the Sling Person on the nearest safe area and release the strops from the aircraft The aircraft shall proceed to land at the nearest suitable area |
| Complete engine failure |
The pilot in command shall release the Sling Person as close to the ground as practicable and attempt the cushioning of the aircraft onto the ground, forward of the Sling Person and clear Note: At any time that a Sling Person is on the strop (long-line) he / she shall not be any more than five (5) m above the immediate ground and or vegetation Should an engine failure occur the aircraft will already be in the high hovering state which is outside a safe auto-rotational envelope therefore the pilot will only be able to cushion the aircraft the best he / she can The Sling Person shall do his / her best to move away from the aircraft or where the aircraft is coming to rest |
Training in emergency procedures
Planning for emergency procedures is a critical component of risk management in HEC operations (DOI, 2010). A study into the human factors aspects of human external loads recommended that all HEC crewmembers be initially and continually trained and practised in emergency procedures (Shehab, Schlegel & Palmerton, 1998). For any in-flight emergency, training is essential to ensure a pilot responds quickly and appropriately. The FAA General Aviation Joint Steering Committee’s Safety Enhancement Topic – Emergency Procedures Training (FAA, 2013), stated:
In the event of an engine power loss while operating in the H/V avoid area, a safe outcome is not always possible, and a pilot has very limited time to respond to achieve the most effective autorotation possible. In the event of a power loss with an external load, the decision to release a load is dependent on the load characteristics. For non-HEC, the load would be jettisoned to reduce aircraft weight, prevent the load from interfering with controllability and increase survivability of the helicopter’s landing.
For HEC, the pilot must decide whether to put the sling person on the ground or to release them. If the sling person is placed on the ground at a speed that minimises their risk of injury, the helicopter will descend rapidly from the height of the length of the sling line, increasing the pilot’s injury risk. The pilot’s injury risk is reduced as the impact velocity decreases. The minimum rate of descent of an R44 II helicopter in an autorotation is achieved at 55 kt airspeed. A sling person would be unlikely to survive an autorotation to the ground with that combination of vertical and horizontal velocity.
Although the Helibrook SOP permitted a sling person to be carried up to 5 m above vegetation (including trees), releasing the sling person more than 5 m above the ground is likely to result in fatal injuries. Additionally, release of the sling person with any horizontal velocity may make it difficult for them to remain erect, increasing the risk of landing other than feet first and increased injury severity.
Release of the sling person
The CASA-approved RFMS stated that survivability of HEC personnel during an in-flight emergency was best accomplished by having the sling person remain attached to the helicopter, unless they were snagged on terrain or likely to become so. However, the Helibrook emergency procedure in the event of engine failure stated that the pilot ‘shall release the sling person as close to the ground as practicable’.
CASA’s instrument approving HEC for crocodile egg collection required pilots to comply with both the RFMS and the company operations manual, and the onus was on the helicopter operator to ensure there was no discrepancy between the 2 documents. When asked about the discrepancy between the RFMS emergency procedure to keep the HEC attached to the line and Helibrook’s emergency procedure to release the HEC, the accident pilot reported that the RFMS stated it was the pilot’s discretion whether to jettison the HEC in the event of an engine failure.
The pilot commented that they ‘did not agree with’ the RFMS procedure to leave the sling person connected in the event of emergency, as that was ‘not a good method at all’. The pilot further commented that with a complete engine failure when operating above trees, if they left the HEC attached to the helicopter, the helicopter would either descend 100 ft vertically on top of the sling person, or the sling person would be dragged through the trees.
The chief pilot advised that in the event of an issue with the helicopter with HEC the pilot would flare the helicopter to try to ‘get the sling person off safely’, and in doing so, sacrifice themselves (and the helicopter) because they would lose rotor RPM. They further stated that in the event of engine failure while slinging, they would likely have their head out the door (watching the sling person) and would look in at the cockpit instruments and identify what had happened. The pilot reported that if they had forward speed, they would flare to release the sling person as safely as possible, then nose forward to try to regain airspeed before flaring the helicopter onto the ground.
Operating height
The Helibrook emergency procedure stated that the HEC ‘shall not be more than 5 m above the ground and or vegetation’. The accident pilot reported that when slinging with HEC, they tried to minimise the height and distance, and the sling person would usually be just above the treetops. The chief pilot also reported that they would go over trees and another pilot who had previously conducted crocodile egg collection reported that the SOP requirement to be not more than 5 m above the ground or vegetation was interpreted to include not more than 5 m above 30.5 m (100 ft) trees. One of the other operators conducting crocodile egg collection reported that they had normalised operating above treetop height, and had removed the height reference from their operations manual. The amendment to that operations manual had been accepted by CASA.
Operating above trees increased both the height of the fall if the sling person was released and the likelihood of having to release the sling person to prevent entanglement with vegetation rather than place them on the ground.
R44 human external cargo operations
Requirements for human external cargo operations
A CASA-authorised aeronautical (design) engineer first issued an engineering order approval for installation of a hook system on an R44 helicopter in December 2007, to enable slinging of an egg collector onto a crocodile nest to facilitate egg collection. However, the approval for fitment of the hook system did not in itself provide approval to conduct external load operations. To make it clear that operational approval was also required, the RFMS associated with the engineering order for the hooks system stipulated that use of the hooks was limited to the commercial collection of crocodile eggs in accordance with CASA-approved operational procedures.
CASA authorisation
Civil Aviation Regulations 151 and 250, which were in force throughout the 2007–2021 period of instrument approvals, did not permit a person to be picked up or carried outside a helicopter without CASA’s authorisation and permission. For crocodile egg collection, CASA issued instruments to helicopter operators that authorised the pilot in command to pick up a person under Civil Aviation Regulation 151(3) and permitted the pilot to carry that person in a harness system attached to the R44 helicopter under Civil Aviation Regulation 250(2). Civil Aviation Safety Regulations Part 11 applied to this authorisation. Specifically, CASR 11.055 (1)(d)[20] stated that CASA may grant the authorisation only if ‘granting the authorisation would not be likely to have an adverse effect on the safety of air navigation’ (CASR, 2010).
Key safety considerations
For the helicopter and pilot (and any other occupants), the key risk that results from carrying (slinging) a person under the helicopter is an event in which the HEC becomes entangled or a similar scenario that may cause a loss of control to the helicopter. Additionally, slinging involves operation in the H/V avoid area, and carries similar hazards to the helicopter and occupants as any other operation in that flight regime.
As the sling person is outside the protection of the helicopter, consideration is required of the likelihood of any scenario where they may collide with an obstacle or the ground, such as a fall resulting from deliberate or inadvertent release of the hooks.
Certification of dual hooks for HEC
Certification requirements
In 2013, CASA identified that the hooks that were being used for crocodile egg collection operations were not certified for HEC. The premise for the certification of any jettisonable external load was that it could be released, without exceptional pilot skill, to prevent hazard to the aircraft, such as causing a loss of control. For HEC, in addition to the need to be able to rapidly release the load to avoid a hazard to the aircraft, it was also necessary to minimise the probability of inadvertent release.
The design engineer then commenced a process to enable the hooks to be approved for HEC by meeting the certification requirements of US FAR 27.865. Compliance was demonstrated except for the requirement that the hooks would not open uncommanded and release the HEC or fail to release, due to electromagnetic interference (EMI). Given limited time until the crocodile egg collection season started that year (December 2013), CASA approved the design engineer to continue to authorise installation of the dual hooks under the engineering order with an interim approval exempting compliance with the FAR EMI requirement until March 2014. The operation continued to be conducted in accordance with a separate CASA operational approval (instrument).
Equivalent level of safety
About 12 months later (after the March 2014 deadline had passed), the design engineer advised CASA that the EMI testing had not been carried out and sought an equivalent safety determination[21] for the requirement. The basis for the proposed equivalent level of safety was that the operational limitations for HEC specific to the egg collection role ‘reduce the risk to equivalent or less than that of a system showing compliance’. That is, there would not be an unacceptable level of risk to the sling person if the hooks released due to EMI while the sling person was on the line, or to the pilot and helicopter if the hooks failed to release due to EMI.
A suite of supporting documents was supplied to CASA, including one that documented operational conditions to reduce exposure to EMI. Another key document proposed limitations to the height the HEC could be carried, to reduce the consequences in the event of release of the sling person due to EMI.
HEC height limitations
In approving crocodile egg collection operations with HEC, CASA had imposed speed and height limitations – that the HEC was to be carried at walking pace and not more than 5 m above the ground or obstacles. The HEC height limitations document relating to EMI risk proposed that those conditions already in place would provide an equivalent level of safety to compliance with the requirement that EMI must not result in release of the hooks. The report concluded that the proposed limitations provided ‘a strictly controlled level of risk for the HEC person in crocodile egg collection operations’. The proposed limitations included ‘a speed not exceeding walking pace’ and that:
The report referenced scientific studies into injuries and mortality due to falls from heights. These studies identified a significant increase in the likelihood of mortality associated with:
- falls from heights above 5 m
- increased age
- landing other than feet first
- head injury.
Based on these factors, the report noted 4 conditions associated with crocodile egg collection that mitigated against the risk of injury in falls from heights. These were that:
- only fit, young persons were employed
- any release would have the person in the best orientation, normally erect, and a maximum of three body lengths above the ground, minimising the time for the orientation to be upset
- use of parachute fall landing technique[22]
- use of helmets to prevent head injuries.
Design compliance
In October 2015, a new hook wiring design was bench tested and the 28 Volt electrical system was found compliant with the EMI requirement. At that time, CASA requested the design engineer lodge an application for the hooks to be fitted under an STC.
In the same month, the design engineer provided CASA with a compliance report detailing assessment of the R44 dual hook for HEC installation with FAR 27.865 – External loads. Demonstration of the reliability of the system included completion of a Failure Modes and Effects Analysis,[23] showing that all potential failure modes of the QRS that may result in catastrophic failures, serious injuries or fatalities were extremely improbable (in the order of 10-9 or less), and any less significant failures were improbable (in the order of between 10-7 and 10-9). The FAA Advisory Circular (AC) 27-1B regarding Reliability of the external load system, including QRS, stated:
In meeting all requirements of FAR 27.865, failure of the hooks resulting in the release of the HEC or failing to release were assessed as extremely improbable. These therefore met the defined acceptable (tolerable) level of safety. Having conducted the analysis for failure modes of the hooks, the design engineer described helicopter engine or control loss as ‘the most significant risk for this operation and can only partly be ameliorated’. Further, that the ‘only amelioration which can be applied is’:
Instrument conditions
Purpose of the conditions
In granting an authorisation to conduct HEC, CASA could specify conditions that were required to be complied with when operating under the authorisation. These were stipulated in an authorisation instrument. CASA delegates stated that the instrument conditions were designed to mitigate the risks of the activity.
Previous CASA instrument conditions
The first CASA authorisation instrument for R44 HEC for crocodile egg collection, was reported to have been issued in 2007 associated with the first fitment of a hook system to an R44 helicopter for HEC. CASA was unable to find any record of instruments issued prior to 2010 or any documented safety case or risk assessment associated with the first instruments that were issued for the activity.
The ATSB obtained instruments issued to several operators from 2010 to 2021 and interviewed several CASA delegates who had approved instruments for the activity, or were involved in the approval process from 2013 onwards.
The 2010 instrument was issued for both R44 and Bell 206 helicopters. All subsequent instruments were for R44 (and R44 II) helicopters only. The 2010 instrument listed 20 conditions, most of which appeared in all subsequent instruments. Included in the conditions were limitations to the height, speed and distance the sling person could be carried. Appendix C – HEC height, speed and distance/time conditions 2010–2021 includes a table of the HEC limitation conditions in the instruments issued from 2010 to 2021.
For the instruments issued from 2010 to 2013 (inclusive), these conditions were:
- The person is not lifted to a height of greater than 5 metres above the ground or obstacles.
- The aircraft is not flown at a ground speed greater than walking pace when the person is carried under the helicopter.
- The maximum distance the person is carried under the helicopter is 500 metres for each pick up.
Request for changes to conditions
In 2013, one operator requested an amendment to the conditions, including replacing HEC height, speed and distance limits with pilot-assessed safe height, speed, and distance. In response, CASA asked the operator to conduct a risk assessment.
That operator provided CASA with an assessment of risks identified for human sling operations for crocodile egg collection. The assessment was derived from a WHNT safe work method statement provided to all operators involved in the crocodile egg collection. The assessment detailed 7 steps in the job sequence. For each of those, it identified ‘What can go wrong’, assessed the initial risk, proposed control measures and assessed the resulting risk.
The job sequence ‘Lift collector and transit to crocodile nest’ obtained an initial risk rating of ‘catastrophic’. The likelihood was assessed as ‘very possible – will probably occur in most circumstances’; the consequences were assessed as ‘extreme – fatality or multiple fatalities’.
The list of hazards for that risk included equipment failure, falling from height and external load limitations (along with crocodile attack, adverse weather, fatigue/heat exposure/exhaustion, flora and fauna). The risk was reduced to ‘high’: unlikely – could happen sometime, with extreme consequences of one or multiple fatalities, with the following proposed mitigations:
Engine mechanical failure and fuel exhaustion/starvation were not included in the hazards for the slinging component therefore no relevant mitigations were included. Engine mechanical failure was however identified as a hazard in the non-slinging job sequences ‘Start aircraft and take-off’, Fly/Ferry to collection areas’ and ‘Return to base/ferry to next job’. Mitigations for engine mechanical failure included the daily inspection, emergency training and rescue plans, adherence to helicopter limitations, and pilot training/experience.
The CASA delegate who assessed the provided risk assessment described it as basic and the requested condition changes were not granted. However, there was no documentation provided that correlated the risk assessment with CASA’s retention of the conditions in the instrument.
2014 and 2015
The 2014 and 2015 instruments were valid from December to the following May, consistent with the crocodile egg collection season. In 2014, the 2013 condition that limited the HEC height to 5 m above the ground or obstacles was amended to:
No documented reason for amendment to the operating height conditions was provided. The delegate who made that amendment reported that the purpose was to make it clearer and avoid ambiguity. The delegate also amended the speed condition to be less prescriptive and provide ‘flexibility to operate more safely’. The HEC speed limitation was changed from ‘walking pace’ to:
A new condition was also added in the 2014 instrument, which stated that the sling person must be provided with a copy of the instrument and ‘made aware, in writing, that the hook system is not certified for human use’. That condition was retained in all subsequent instruments.
2016
In 2016, the CASA delegate was invited to a demonstration of human slinging for simulated crocodile egg collection. Following the demonstration, the height condition was amended to provide the operators ‘some relief to be able to go over obstacles that might be in their flight path to go from one point to another’ as follows:
When asked how lifting the HEC above the nominal survivable height of 5 m affected the activity risk, the delegate commented that it was not un-survivable because ‘the operator had an obligation to conduct the operation in a safe manner’. Additionally, in 2016, the 500 m distance limit the HEC could be carried was amended to:
In 2016, Helibrook received their first instrument for R44 HEC for crocodile egg collection. The chief pilot had previously been involved in conducting the same operation for different AOC holders.
2017 and 2018
The ATSB obtained instruments issued to 3 operators in 2017, including Helibrook. As Helibrook was oversighted by a different CASA regional office to the other operators, multiple delegates were involved in the instrument approvals.
Late in 2016, the EMI test report demonstrating compliance of the hook system was completed. As a result, the HEC height limit was removed from the RFMS for the hooks, which was only required to consider failure of the hook system, not failure of the helicopter and associated operational safety limitations. A 60 kt speed restriction was included in the RFMS, based on reported feedback from an egg collector stating that was a suitable operating speed. It was noted at the time the amendments were made to the RFMS, that operational limitations specified in CASA’s operational instrument would be ‘overarching and could contain more conservative limitations’. However, when CASA asked for advice regarding limitations, the design engineer advised that additional limitations were unnecessary as the system was now HEC compliant.
The 2017 delegates and their CASA subject matter experts – airworthiness/engineering and the previous delegate – agreed that as the height limitation had been removed from the RFMS, it could also be removed from the CASA instrument, because inadvertent release was now extremely unlikely as the hook system was compliant. It was also assessed that there was no longer any purpose in stipulating a speed limit because ‘at 500 ft above ground level…forward speed will have no bearing on the HEC’s chances of survivability’. Therefore, the height limitation condition and the clause in the speed condition regarding minimisation of injury to the HEC were removed from the 2017 instrument conditions. However, the pilot-assessed safe speed and minimum distance conditions were retained.
The delegates reported that they relied on information provided by the subject matter experts and assessed that there were reasonable mitigations in place with the conditions. One delegate reported that they had accessed relevant files and had conversations with other delegates. They therefore assessed that the activity presented an acceptable risk, particularly as the instrument was a renewal for an activity that had been conducted without accident or serious incident for at least 5 years.
Although the height and speed limit conditions were removed once the hooks were HEC compliant, the instrument condition advising that the hooks were not certified for human use was retained. The delegate reported that their understanding was that the hooks were satisfactory and fit for purpose but not certified or approved by CASA.
The instrument delegate responsible for the instrument issued to Helibrook assessed that the activity was high risk, but accepted by CASA. Further, they considered that the removal of the height limitation was ‘a small change’ and nothing significant that would affect the operation.
From 2018, the instruments were issued for a 12-month period from December.
2019 and 2020
The CASA flight operations inspector responsible for oversighting Helibrook was assigned as the delegate for Helibrook’s instrument renewal in 2019 and 2020. The delegate assessed that the Helibrook operations manual had reasonable procedures for the activity, the sling equipment was approved, and the chief pilot and/or pilots involved had sling approval and relevant experience.
The delegate assessed that as it was a renewal, the procedures were in place and if they continued doing what they were doing previously, there was probably no reason not to allow them to continue what was an established activity. They also assessed that minimisation of exposure was included in the operator’s procedures. The delegate did not identify any discrepancies between the operations manual, RFMS and the instrument conditions.
Delegate guidance material
In an email to the ATSB, CASA reported that there was no ‘granular documented process’ for approving instruments like the R44 Dual Hooks for HEC for Crocodile Egg Collection authorisation. The CASA Air Operator’s Certificate (AOC) Process Manual included a section on CASA approvals and exemptions, with a process map and the administrative steps required. Additionally, CASA’s Air Operator’s Certificate Handbook provided detailed information for assessing and issuing an AOC, including:
- process overview
- assessment criteria, methodology and link to checklists for AOC approvals
- operational personnel
- inspection of specialised equipment fitted to aircraft
- assessing an operations manual
- volume 2 provided guidance for assessing an application to include an aerial work purpose on an AOC, which included appropriate operations manual content, inspection of specialised equipment and review of the chief pilot's experience and qualifications
- volume 4 included assessing safety management systems with a sub-section on safety risk management, which included guidance to assure an acceptable level of safety existed.
The CASA delegates approached by the ATSB reported that the AOC‑related documents provided broad or generic guidance, and while similar principles could be used for assessing a request for an authorisation and permission instrument, they did not contain specific relevant guidance.
Safety assessment
To determine how CASA delegates assessed that safety was preserved when issuing authorisations, the ATSB requested detail of any risk assessments associated with the instruments. In response, CASA advised that they could not locate any risk assessments and that they had not conducted any specific testing or assessment of the risk profile for the activity of R44 HEC for crocodile egg collection. Specifically, CASA also advised that they had no evidence of any risk assessments associated with the instruments issued to Helibrook between 2016 and 2021.
CASA required a request for an authorisation to be made in writing and when assessing a request, delegates relied on the advice of other CASA personnel with subject matter expertise and experience. This advice was generally communicated by emails, some of which were filed in the records management system, or by telephone. The assessment was then made based on judgement of the activity’s reasonableness, but there was no documented acceptable risk level.
Although they reported not having seen a CASA risk assessment for the activity, the involved delegates assumed that a safety case would have been provided with the first operator’s request for approval for the activity (sometime prior to 2013) and that had been assessed and accepted by CASA. The activity was understood to be high risk, but delegates believed that CASA accepted that risk level. In particular, as the 2013 instruments were signed by a senior CASA manager, this was interpreted as an endorsement that it was appropriate to continue issuing the approvals.
Additionally, the annual approvals for operators were considered to be reissues of instruments for a previously accepted activity, albeit to varying helicopter operators. All the operators conducting crocodile egg collection each season received essentially the same instrument, although some conditions varied from one year to another. Prior to issuing Helibrook’s first instrument in 2016, a CASA inspector verified that the operator had:
- a procedure for conducting the activity
- appropriately experienced personnel
- relevant documentation and sling equipment.
For an annual issue of an instrument to an operator who had previously held the authorisation, the delegate’s primary check was whether there had been changes to procedures or personnel since the previous issue. The delegates reported that if there had been no changes to procedures, and no enforcement action taken against an operator, they had no reason not to reissue the instrument. Additionally, as mentioned above, they assessed that the activity was being done safely as there had been no reported accidents or serious incidents.
The delegates all reported that the instrument conditions were intended to mitigate the risks associated with the activity, and that they assessed there were sufficient conditions and procedures in place to mitigate the risk to a reasonable level. Additionally, they considered that there was an onus on the operators to act safely and to advise CASA, via their operating procedures, how they were going to reduce the associated risks.
Human external cargo rotorcraft load combination decision
In August 2013, a CASA project was initiated to consider existing HEC regulations and propose amendments to Civil Aviation Order (CAO) 29.6, which only applied to non-human sling operations. The project identified that permissions being issued by CASA regional offices were not issued on the basis of a risk assessment or reflective of international standards. Specifically, in the US, United Kingdom and Canada, HEC was not permitted with piston engine rotorcraft and, CASA had assessed that the use of piston engine helicopters increased the risks to HEC compared with turbine engine rotorcraft. Additionally, in 2013, helicopter operators involved in the powerline industry had approached CASA for HEC approval using turbine engine rotorcraft, consistent with international requirements.
As a result of the project, in October 2013, the then CASA Director of Aviation Safety (DAS) signed an internal minute that recommended CASA restrict HEC operations to the following requirements:
- single engine turbine powered rotorcraft with a usage monitoring system
- out of ground effect hover performance with a performance buffer
- restrictions on who could be carried
- an attachment means certified for the carriage of humans.
The minute also recommended that the proposed standard be communicated to CASA field officers for consideration in all authorisation/permission approvals, while the proposed amendment to CAO 29.6 to reflect the policy was being drafted.
As a component of the project, a CASA risk workshop on crocodile egg collection using HEC was held on 20 November 2013. While no minutes were recorded from the meeting, a draft risk management plan (RMP) provided to the ATSB formed the basis of the discussions.
Risk management plan
The stated purpose of the RMP was:
The RMP was drafted by a senior standards officer with significant helicopter and HEC expertise using a CASA general aviation operations template. The scope included that the assessment:
The assumptions listed in the RMP were:
The overall operational risk of the activity was assessed with an initial risk rating of high (7), which ‘needs senior management attention’, and the residual risk (with controls in place) of medium (5), requiring ‘management responsibility’.
CASA’s General aviation operations group risk matrix utilised to assess the operational risk is depicted in Appendix B – CASA operational group risk matrix (2013). Extreme and high risks were required to be reported to senior management and have detailed treatment plans, ‘which reduce the risk in accordance with the ALARP [as low as reasonably practicable] principle’. CASA AC 138-05 – Aerial work risk management defined ALARP as ‘the point where the costs of introducing further safety measures to lower a risk outweigh the safety benefit. However, a risk should be tolerated only if there is a clear benefit such as a compelling operational need’ (CASA, 2022).
The broad risk categories considered in assessing the risk associated with HEC operation were:
- engine failure/malfunction inside the H/V envelope with HEC attached
- insufficient excess power available for role and environment
- equipment/hardware failure of rotorcraft system or subsystem
- human error while undertaking HEC operation.
Potential risk controls were:
- preference of multi engine turbine rotorcraft with [one engine inoperative] OEI accountability
- preference to single engine turbine rotorcraft
- usage monitoring systems of pertinent parameters
- equipment standards to HEC design criteria
- limitation of exposure measured in time, distance, speed and height [above ground level] AGL
- CASA increased surveillance of operations whilst under limited conditions
- CASA mandated minimum experience level and qualification to conduct HEC
- increased engine and critical component inspection criteria
- mandated excess power margin requirements for [hover out of ground effect] HOGE conditions
- limitations in environmental conditions including wind azimuth, velocity, humidity.
The RMP identified 26 individual hazards, all of which were assessed as initially not ALARP. Some of the documented hazards were linked to the R44 POH and Robinson Safety Notices. Proposed operational mitigations included additional regulatory oversight to ensure procedures were followed and maintenance/overhaul requirements were adhered to.
For the hazard of single engine piston rotorcraft engine failure while operating in the H/V envelope, the likelihood was assessed as rare – 1 in 10,000 to 1 in 100,000, with severe consequences – multiple life-threatening injuries/less than 10 fatalities, and an overall medium risk. Suggested mitigations to reduce the residual risk, still rated as medium, included:
- minimise exposure time for HEC and enforce conservative limits of distance, height and time
- require engine usage monitoring system
- use fuel injected models only
- require single engine turbine to reduce failure rate, or multi-engine rotorcraft with one engine inoperative accountability; or in consultation with the manufacturer increase inspection requirements including engine compression checks, and reduce overhaul period.
There was no assessment of the hazard of fuel exhaustion, but fuel starvation or contamination was assessed. For these, the initial risk was assessed as unlikely, and the consequences were severe with an overall high risk rating. With mitigations including fuel checks, minimum fuel requirements, fuel usage policy and turbine engine, the residual risk was medium, requiring CASA management responsibility.
The author of the RMP subsequently advised the ATSB that the omission of fuel exhaustion as a hazard was unintended, and that the proposed mitigations were also applicable to fuel exhaustion.
CASA’s Flight Standards Branch advised the ATSB that the RMP was never finalised, and the risk controls proposed to mitigate the risks of continuing R44 HEC for a further 6-month period were not implemented. The draft RMP was however used by CASA Flight Standards Branch to propose HEC standards, first for an amendment to Civil Aviation Order 29.6, which was subsequently discontinued (in 2016), and then for the development of CASR Part 138.
CASA also advised that the RMP was used to consider the potential viability of allowing single engine piston helicopter HEC operations based on an equivalent level of safety. This would have required demonstration that the piston engine helicopter had a similar in-flight failure rate as a turbine engine helicopter with a usage monitoring system. Members of CASA’s Flight Standards Branch presented this option to operators in 2014, however, no operator attempted to demonstrate this equivalence.
Intent to amend approval conditions from 2014
On 6 December 2013, CASA’s operations division sent a letter to an operator that had previously been authorised to conduct R44 HEC operations. The letter included the proposed future position requiring single engine turbine power rotorcraft with a usage monitoring system and other requirements as per the revised policy position approved by the then DAS. The letter stated that CASA had:
The letter then detailed the relative risks of single engine piston rotorcraft compared with single engine turbine rotorcraft. This included detail that in the US from 2004–2008, the accident rate of single engine piston rotorcraft on average exceeded 1 per 10,000 flight hours and was more than 3 times that of single engine turbine rotorcraft. Engine failure inside the H/V envelope was identified as one of the main risks related to single engine rotorcraft. It also listed other known failure modes of R44 rotorcraft that had been identified in the RMP.
In summary, the letter advised the operator that CASA intended to renew the authorisation with some changes to the conditions for one more season before turbine engine rotorcraft would be required. At the time, the cargo hooks were not certified for HEC and a proposed condition was that the authorisation did not override engineering or airworthiness limitations.
Response to the proposed changes
The design engineer responsible for the hooks system responded to CASA’s letter on behalf of operators that conducted crocodile egg collection. The response disputed the safety data referenced in CASA’s letter, requested coordination between CASA’s certification/airworthiness and operations personnel and continued R44 operation for one more season to allow operators time to address the proposed requirements.
In response, a CASA regional manager made a documented recommendation to a senior manager within CASA that R44 HEC operations continue. The recommendation outlined CASA’s authorisations of R44 HEC operations for crocodile egg collection, the 2013 DAS decision to establish formal policy (including the use of turbine powered rotorcraft for human sling load operations) and that since that decision, CASA had undertaken work regarding the appropriateness of piston engine rotorcraft to carry human external cargo.
The recommendation also advised that that operator had requested reissue of the authorisation to continue to operate until CAO 29.6 changes were finalised. In support of the request for continued R44 HEC operations, the design engineer provided their comparative analysis of Bell 206 (turbine helicopter) and R44 engine failure data. Additionally, the regional manager proposed that extra conditions be included in the instrument to ‘mitigate those risks further’. Key additional conditions from the precedent instrument (which was valid from 2 December 2011 to 31 December 2013) were:
- the hooks are to be certified for use in human sling load operation
- engineering orders must confirm that all things attached to the hook systems are fit for purpose
- the aircraft is to be operated in accordance with the approved FMS
- daily inspection includes sling system/equipment
- the pilot is required to verify the engine is capable of normal rated power with no defects evident and to certify this on the maintenance release
- only persons employed or contracted for egg collection can be carried.
The reasons given for the recommendation were that:
- the overall risk to safety of the egg collector could be reduced by the use of the R44 aircraft type
- other operational activities permitted by CASA possessed ‘equal hazards and risks, such as mustering operations, night agricultural operations, and parachuting activities’.
The senior manager agreed with the recommendation and signed instruments authorising continued R44 HEC operations for crocodile egg collection to the end of April 2014 for 2 operators.
The CASA delegate who approved the following year’s instrument assumed that one reason the 2013 instruments were signed by a senior manager was to demonstrate that CASA senior management was aware of the operational approvals process and was satisfied it was appropriate to issue the instruments.
Proposal to discontinue CAO amendments
In 2016, the then DAS agreed with a proposal from CASA Flight Standards Division to close the existing project to amend CAO 29.6, as it had been ‘superseded by Part 138’. The finalisation of Part 138 was reported to be ‘imminent’, with a proposed effective date of September 2018. The proposal included that crocodile egg collection would ‘continue as per current exemptions until such time as Part 138 is made and the regulation commences’.
Transitional regulations
At the time of the accident, Helibrook and other operators were conducting crocodile egg collection under their AOC as an aerial work operation. From 2 December 2021, crocodile egg collection required a CASR Part 138 Certificate (instead of an AOC) to authorise the operation. The crocodile egg collection operation (carriage of a person outside a rotorcraft) was categorised as an aerial work class D external load operation under CASR Part 138.[24] Chapter 15 of the Part 138 manual of standards (MOS) – Rules for external load operations, applied to the activity.
Section 15.06(3)(e) applied to rotorcraft that cannot hover out of ground effect with one engine inoperative, requiring section 9.05(b), (c), (d) and (e) of the MOS to be complied with. This required the rotorcraft to have:
- a turbine engine
- a usage monitoring system
- control to be maintained in all phases of flight in the event of a hydraulics failure or alternatively dual hydraulics
- redundant means of controlling fuel flow to the engine.
CAR 151 and 250 were repealed on 2 December 2021. An authority under CAR 151(3) and a permission under CAR 250(2) applied to CASR Part 138. The Part 138 requirements were more onerous than the existing instrument issued to Helibrook for crocodile egg collection, which permitted use of a piston-engine helicopter without a usage monitoring system. In order to permit continued egg collection using the R44 an exemption was granted under Division 11.F.1, including CASR 11.170(3), which stated:
Despite the intended safety improvement associated with the introduction of Part 138 requirements, Helibrook’s instrument was issued on 9 September 2021, with a 3‑year validity period. Under the transitional legislation, it would cease at the earliest of the:
- expiry of the instrument (31 December 2024)
- second anniversary of the instrument commencement (7 September 2023)
- day the operator’s AOC expired (31 July 2022, extended to July 2023 after the accident).
Considering these criteria, Helibrook would be required to comply with CASR Part 138 and Part 138 MOS when its AOC expired.
Briefing note July 2021
In July 2021, an internal briefing note to a senior CASA manager stated that:
The briefing note outlined the risk assessment and subsequent work, which had concluded that HEC operations were very high risk for the sling person. It stated that the risk could be substantially mitigated through the use of a turbine engine helicopter with a usage monitoring system. Additionally, the hook system needed to provide redundancy in the case of failure of the hooks/system.
The Background section of the briefing note included that CASA’s previous permission instruments had not been issued on the basis of a risk assessment, and that the risk had been assessed in 2013 as unacceptable without mitigation. Further, that CASA’s authorisation of R44 HEC operations was not reflective of international standards and significantly differed from the FAA, Transport Canada and EASA. At that time these organisations generally required multi turbine engine helicopters with one engine inoperative accountability for commercial operations, with the use of high-reliability single turbine engine helicopters permitted for limited specified operations.
The Way Forward section of the document noted that some helicopter operators were already conducting powerline maintenance work using a single engine turbine helicopter for HEC, based on the CASR Part 138 standards.
Helibrook’s 2021 instrument
The 2020 instruments were valid until 31 December 2021. On 2 September 2021, the Helibrook safety manager emailed CASA’s Regulatory Services requesting a renewal of the instrument with the 2020 instrument attached to the email. After payment, the task was assigned to the delegate on 9 September 2021, who recalled that it was relatively urgent. The delegate reported being unaware of the history of the authorisation, but was aware of the general risk of the operation and that it had been assessed by multiple sections within CASA.
The delegate reviewed the file relating to the most recent instruments and emailed the previous approver asking whether there were any concerns regarding reissue of the instrument to Helibrook. The previous approver advised that:
- the STC for the hooks had been issued on 30 July 2021
- there had been no changes to Helibrook’s equipment or procedures that they were aware of
- CASR Part 138 was not yet in force
- considering the above, they saw no reason why a new instrument should not be issued.
They also commented that they did not believe there was a compelling statistical argument to justify the higher cost of a turbine engine helicopter that would be required under Part 138.
The delegate then signed the instrument on 9 September 2021 with an expiry date of 31 December 2024. There was no change to the conditions from the previous year’s instrument. The references to the now redundant EO were not removed. Condition 23 stated that when the STC is approved, ‘all aircraft previously certified to the [engineering order] EO will be shown to be compliant with and certified to the STC within 14 days of the STC being approved, after which time aircraft certified only to the EO may no longer undertake this work’. Helibrook did not update the hook installation on VH-IDW to the STC. The delegate reported that they were unsure about whether the hooks had been certified. The delegate also reported being unaware of the implications of the impending Part 138 requirements when they issued the instrument for a 3-year period.
At the time of the accident, VH-IDW was operating under CASA Instrument CASA.CARRY.0163 Revision 1, issued to Helibrook and dated 7 September 2021 (2 days prior to it being assigned to the delegate).
There were 34 listed conditions that Helibrook and the pilot in command were required to comply with (Appendix D – Instrument conditions). There was no limitation specified for the HEC carriage height. Key conditions discussed previously included:
- The pilot in command and sling person were required to have completed a course of training for the activity promulgated in the helicopter operator’s operations manual. The operator’s training course was to include not less than 1 hour of flight time and 1 hour of ground instructional time.
- A thorough pre-flight briefing was to include actions to be taken by crew members during possible emergencies – the briefing was to be conducted in accordance with the briefing procedures in the operations manual.
- The helicopter was required to be compliant with the STC SVR 541 and to be operated in accordance with the FMS, which details normal and emergency procedures associated with the activity.
- The pilot and operator were required to comply with the relevant procedures in the company operations manual.
- The pilot was required to have continuous and clear radio communications with the sling person throughout.
- The pilot was required to fly the helicopter at a ‘safe speed’ and to carry the sling person ‘for the minimum distance and time required in order to safely conduct the activity’.
- The sling person was required to wear an Australian Standard helmet (‘appropriate to the risks encountered during the activity’).
- Prior to commencement of the activity each day, the pilot was required to verify that the engine was producing normal rated power output, and that no defects were evident which could lead to power reduction during those operations.
- The sling person must be made aware, in writing, that the hook system is not certified for human use.
Engine failure probability analysis
US data
Data based on the Lycoming Service Reporting Database, National Transportation Safety Board Aviation Accident Database, FAA Service Difficulty Reports, and FAA Accident and Incident Database System from 31 December 2016 to 31 December 2021, found power loss rate (incidents per 100,000 flight hours) were 0.54 for the R44 and 0.11 for the R44 II. These helicopter types therefore met the EASA requirements[25] for ‘Helicopter operations without an assured safe forced landing capability’ engine in-service sudden power loss rate requirement of not more than 1 per 100,000 (1 x 10-5) engine hours in a 5-year moving window. For that data, where the cause of the engine failure was unknown, or where maintenance was identified as the reason for the failure, they were counted as 0.5 and 0 events respectively.
Australian data
A review of R44 and R44 II engine failure occurrences reported to the ATSB,[26] compared with flight hours for the period 2011 and 2020 showed the average engine failure rate was 4.4 per 100,000 flight hours. Unlike the power loss rate data above, these did not consider whether the failure resulted from maintenance or an unknown reason, which may account for the higher engine failure rate in Australia. Fuel exhaustion and fuel starvation were not coded as engine failures.
In addition to engine failures, the ATSB identified R44/R44 II accidents and serious incidents that occurred during the same period, which would likely result in injury to the sling person if they occurred during slinging operations. These were primarily losses of control and occurred at a rate of 2.8 per 100,000 flight hours. The combined rate of engine failure and other occurrence types likely to result in injury to the sling person was 7.2 per 100,000 flight hours.
At risk time
To quantify the risk of the activity, it was necessary to approximate the amount of time HEC was being conducted each year in Australia under a CASA authorisation. In the 2020–21 and 2021–22 seasons, 3 helicopter operators had CASA authorisation for R44 HEC operations to conduct crocodile egg collection. Of those, 2 contracted to WHNT and one operator supplied a different crocodile farm. WHNT provided total invoiced hours for 3 R44 helicopter operators for those seasons, one of which did not have a CASA instrument for HEC, but the ATSB obtained evidence from February 2021 showing dual hooks installed on their helicopter. In the 2020–21 season, 566.1 hours were invoiced and 507.3 in the following season, in which activities were suspended following the accident. This included the accident pilot, operating VH-IDW as one of the 2 HEC helicopters for WHNT, who had invoiced 21.5 full days of conducting crocodile egg collection for the 2021–22 season to 22 February 2022 (approximately 200 hours).
WHNT initially estimated that they were generally slinging about half the total engine-running time, and later revised this to about 20% of the total time for the 3 helicopters operating for WHNT. The other (non-WHNT) operator estimated they did about 15 hours of HEC each season.
Based on the information and approximations provided, the ATSB assessed the effect of slinging a person under an R44 helicopter for 200 hours per year. On average, an engine failure or in-flight emergency likely to result in an accident, would occur once every 69 years while slinging a person.
Exceeded maintenance intervals
Exceeding maintenance, inspection and overhaul limits, increases the probability of an in-flight engine failure. The Robinson R44 Maintenance Manual stated that it ‘is the operator’s responsibility to maintain a record of time in service for the airframe, engine and life-limited components…[an] hour meter is an acceptable means of recording time in service’. The manual included the warning that:
Lycoming Service Instruction 1009BE – Time between overhaul (TBO) schedules included the warning that ‘Operation of an engine in a non-airworthy condition could result in loss of life, serious injury, and damage to property’. Additionally, the Lycoming operator’s manual included:
Previous occurrences
HEC accident
On 11 May 2022, a Bell Helicopter Textron Canada 407 helicopter was conducting HEC training in Livermore, California, US. The helicopter was about 175 ft above ground level with a sling person on a 60-ft long line when the engine lost power. The pilot manoeuvred the helicopter and partially raised the collective when the sling person was about 15 ft above the ground (AGL) and cushioned them onto the ground. The sling person was uninjured.
The pilot then manoeuvred the helicopter away from the sling person and when about 10 ft AGL, raised collective and released the sling line. The helicopter landed hard resulting in substantial damage to the helicopter and serious injury to the pilot, who had to be extricated from the wreckage. At the time of publication of this report, the US NTSB investigation was ongoing however, the occurrence showed that in a helicopter with more main rotor inertia than an R44, it is possible to cushion the HEC onto the ground, but the ensuing autorotative landing can result in serious injuries to the pilot.
Fuel exhaustion occurrences
Safety publication
The ATSB Avoidable Accidents publication Starved and exhausted: Fuel management aviation accidents (ATSB, 2013) defined 2 main reasons why fuel stops getting to an engine during flight:
- Fuel exhaustion happens when there is no usable fuel remaining to supply the engine/s.
- Fuel starvation happens when the fuel supply to the engine/s is interrupted although there is adequate fuel on board.
The report stated that the ATSB received an average of 21 reports of fuel exhaustion or starvation occurrences each year. Fuel exhaustion occurrences were normally either the result of an error in pre-flight fuelling, or a number of seemingly minor aspects of fuel planning and management during the flight. Consideration of different fuel consumption rates depending on the activity being conducted and flight conditions is a key component of fuel planning.
The chance of fuel exhaustion is reduced if a pilot accurately determines the amount of fuel on board prior to starting, by cross-checking from multiple sources. These include fuel quantity gauges, dipsticks, totalisers/flow meters and calculations from previous refuels and fuel usage regularly checked for accuracy.
ATSB fuel exhaustion occurrences 2011–2020
The ATSB occurrence database held 54 fuel exhaustion occurrences for the 10-year period 2011‑2020. Considering the involved engine types, 49 were piston, 4 were turbine and 1 engine type was unknown. However, of the total aircraft, only 5 were helicopters, 3 of which had turbine engines and 2 were piston engine helicopters. Neither of the piston helicopters were an R44, but one of the occurrences involved a piston engine R22 Beta helicopter conducting mustering operations. Given the small data set, there was no significant difference in engine type for helicopter fuel exhaustion occurrences.
For 14 of the 54 occurrences, the total flight time of at least one pilot was recorded. Table 4 details the number of occurrences, the number of those where the total flight time of one pilot was known, and the median total flight time. The median total flight time of a pilot involved in a fuel exhaustion occurrence was 1,227 hours with a range of 20 to 14,500 hours. This suggests that experience is not a mitigation against fuel exhaustion occurrences.
Table 4: Fuel exhaustion occurrences 2011–2020, engine type (1 unknown), median and range of pilot total flight time (TT)
| Occurrence category | Number of occurrences | Piston engine | Turbine engine | Number with known pilot TT | Median of known TT (range) |
| Exhaustion | 54 | 49 | 4 | 14 |
1,227 (20–14,500) |
Source: ATSB occurrence data
ATSB investigation AO-2010-073
On 4 October 2010, a Robinson R22 Beta helicopter collided with the ground while conducting cattle mustering operations. The pilot was fatally injured, and the helicopter sustained substantial damage. The investigation found that the collision with terrain was probably a result of engine stoppage due to fuel exhaustion, while operating at low altitude. The investigation also found that:
Long line fuel exhaustion accident
In 2012, the US National Transportation Safety Board investigated an MD Helicopters 500D helicopter accident, in which the engine lost power while a utility worker was suspended on a long line attached to the helicopter. The investigation analysis included the following:
The National Transportation Safety Board determined the accident to be a result of improper maintenance resulting in erroneous fuel gauge indications, combined with the pilot’s inadequate fuel management. The investigation also found there were no written company procedures or fuelling records to track fuel loading and time-based fuel consumption.
Survivability
Post-mortem report
The post-mortem examination of the egg collector found multiple blunt force injuries resulting from a fall from a height. The examination identified that there were numerous head, neck, and torso (or trunk) injuries. There was also external evidence of blunt force trauma to the upper and lower limbs, but there were no underlying skeletal injuries. No obvious evidence of fuel was found on the egg collector’s clothing to indicate a fuel leak prior to the accident, but the clothing was not specifically tested for the presence of fuel. Additionally, no bark residue, indicative of tree contact, was identified.
Height of fall
Three studies conducted on patients presenting to an emergency or trauma centre following a fall from height analysed injuries sustained and the height of the fall (Icer and others, 2013, Liu and others, 2008, Nau and others, 2021). The studies found that the overall injury severity was higher with increasing fall height. With increased height of the fall, there was a significantly higher severity of thoracic and pelvic injuries, whereas the severity of head injuries and spinal fractures did not increase with fall height. Life-threatening injuries were more likely the higher the fall height, and falls greater than 18 m were usually fatal (Nau and others, 2021).
In one study, the mean fatal fall height was 6.61 m, noting that the study excluded people who had died before arriving at the hospital. About 30% of people who fell from 10 m or higher died, which was twice the percentage of those who fell from 6–9.9 m and nearly 3 times that of those who fell from 3.1–6 m. Of those fatally injured, 91% sustained head injuries. The study found haemopneumothorax[27] and subarachnoid haemorrhage[28] were the most important factors affecting mortality (Icer and others, 2013). Another study also found severe head injury was a significant prognostic factor for mortality in people who fell from heights of at least 6 m (Liu and others, 2009).
These research findings were consistent with a retrospective study of autopsy reports (Abder-Rhman, Jaber, & Al-Sabaileh, 2018), which found that internal injuries were directly proportional to the height of the fall. Head injury was the most common fatal injury in all heights, chest injuries and skull base fractures were more prevalent in falls from above 3 m, and abdominal injuries were mainly prominent in heights above 9 m.
The Civil Aeromedical Research Institute of the US FAA report Human survivability of extreme impacts in free-fall, analysed factors affecting survivability in individuals who survived falls from heights of up to 84 m (275 ft) (Snyder, 1963). Among other factors, the study found that orientation of the body was important. The initial impacts were feet-first in 10 of the 12 cases of survived falls from over 33 m (100 ft). The impact force was found to be greatly attenuated by bending and flexion of the leg muscles.
Freefall orientation
The sling person’s harness is designed to keep them in an upright position. Keeping the sling person attached during an emergency landing would allow them to remain upright and impact the ground feet first, decreasing the mortality risk. When the sling person is released, they have no means of orientating themselves and are more likely to tumble, increasing the likelihood of landing other than feet first, thereby potentially increasing risk of fatal injury.
Injury assessment
A forensic pathologist assessed the egg collector’s injuries and found that there was evidence of significant head injury due to ground impact. In assessing the height from which the sling person was likely released, the pathologist referenced research showing that higher mortality is found in falls from greater heights and that the threshold for suffering major trauma from a fall from a height is at least 6.1 m (20 ft). Further, that pelvic fractures occur significantly more often if the fall height is at least 6 m, and chest trauma is more common the higher the height of the fall.
Based on the research and the egg collector’s extensive pelvic, spinal, and chest fractures, the forensic pathologist assessed that they likely fell from a height above 5 m.
Egg collector helmet
The egg collector’s helmet was found nearby, and the helmet’s clasp receptacle had fractured.
The instrument issued to Helibrook for picking up and carrying a sling person under an R44 helicopter for crocodile egg collection stipulated that the sling person was to wear a helmet that ‘meets the Australian standard appropriate to the risks encountered during the activity’. The sling person’s helmet had a sticker showing compliance with American National Standard for Industrial Head Protection ANSI/ISEA Z89.12009 Type I Class C. This standard was amended (in 2014) to Z89.1-2014.
The standard stated that Type I helmets were ‘intended to reduce the force of impact resulting from a blow only to the top of the head’. (The Class C (‘conductive’) helmets also provided no electrical protection). In contrast, Type II helmets met additional requirements for lateral impact protection (front, back and sides) and chin strap retention. In this accident, a Type II helmet would not have reduced the severity of the egg collector’s injuries to a survivable level.
Pilot restraint and helmet
The pilot sustained swelling and bleeding on the brain indicative of rapid deceleration and acceleration. Although the pilot was not wearing a helmet, it would likely not have reduced the severity of head injury in this accident as no head impact occurred. The pilot reported always wearing the 4-point restraint and could not recall how they exited the helicopter.
Pilot seat
R44 helicopter seats are designed to crush and absorb impact forces. Under the seat is a stowage area marked with a weight limit and a limitation for storage of soft articles only. The pilot reported that they normally had the following under their seat: lunch, water bottle, satellite phone, first aid kit and a raincoat. A broken headset and other small items were found under the pilot seat and photos from the site showed other items that were removed before ATSB arrived that may also have been stored under the seat.
Impact forces crushed the seat into the storage area, with the seat box and support structure collapsing. Additionally, the fuselage belly pushed upwards after the undercarriage skids exceeded their capability. The floor also pushed up to the level of the collapsed seat pan.
This indicated that the energy absorption capability of the airframe with respect to the seat installation had been exceeded. The seat probably collapsed onto the contents of the stowage compartment and may have contributed to the pilot’s injuries.
Cocaine metabolites
In Australia, cocaine is classed as a ‘Schedule 8 – controlled drug’. Cocaine is a central nervous system stimulant and an illicit drug, unless there is evidence it is used for medical purposes. In a dilute solution, it is used as a topical anaesthetic for limited purposes and is listed as an unrestricted Schedule 8 substance in Northern Territory hospitals. A deputy director at Royal Darwin Hospital advised that cocaine was not stocked in the Emergency Department and was not administered to the pilot at Royal Darwin Hospital. CareFlight NT’s Medical Director advised that their aircraft did not carry topical cocaine.
In the context of aviation safety, detrimental effects of cocaine can occur in the hours immediately after use, and depending on the regularity and dose used, there may also be longer-term effects. Immediate effects of a moderate dose of cocaine on skills performance can include risk-taking, inattentiveness and poor impulse control. During the ‘crash phase’, which lasts 9 hours to 4 days following cocaine use, the user can feel depressed, agitated, irritable, and there can be significant fatigue and lack of energy (Isenschmid, 2002). As the effects of cocaine wear off, the user can suffer fatigue, depression, sleepiness, and inattention (Couper and Logan, 2014).
Cocaine is metabolised in the body to benzoylecgonine and ecgonine methyl ester. Blood concentration of cocaine decreases rapidly and is typically detectable in blood 1–2 days after use. Cocaine metabolites benzoylecgonine and ecgonine methyl ester may be detectable for at least 3–4 days after cocaine use. The presence of benzoylecgonine and other cocaine metabolites in blood in the absence of cocaine usually indicates the cocaine exposure did not occur immediately prior to the blood sampling (Isenschmid, 2002). A toxicological pharmacologist advised the ATSB that it was extremely difficult to correlate blood cocaine concentration with the timing and quantity of exposure to the drug. They also assessed that the pilot’s toxicological results were indicative of exposure to cocaine possibly up to about 4 days prior, but not in the previous 24 hours.
CASR 91.520 detailed that a crew member is unfit for duty if their ability to perform the duty is likely to be impaired because they have used a psychoactive substance such as cocaine. Pilots are required to declare recreational drug use to a designated aviation medical examiner.
Safety analysis
Introduction
From about 0850 on 28 February 2022, the crew of Robinson R44 II helicopter, VH-IDW, were preparing to conduct crocodile egg collection, near King River, Northern Territory. The helicopter was operating under a Civil Aviation Safety Authority (CASA) instrument that authorised the pilot to operate with a person in a harness system (‘sling person’) outside and attached to the helicopter, for the purpose of collecting crocodile eggs. The authorisation was subject to conditions that were intended to mitigate the risks of the operation.
After hearing no communications from the pilot of VH-IDW for more than one hour, another pilot conducting egg collection nearby commenced a search. They found the accident site about 150 m from the first nest they expected VH-IDW’s crew to collect eggs from. The egg collector lay fatally injured on the ground, wearing their harness and attached to one end of the sling. The attachment rings at the other end of the sling were not connected to the helicopter, which had collided with the ground upright, 44 m from the egg collector, and was substantially damaged. The pilot sustained serious injuries.
There were no witnesses to the accident and the accident pilot had no recollection of the accident and limited recollection of the hours leading up to it. No recorded data to accurately determine the accident sequence, including the time of the accident, was recoverable.
There was no fuel present in the helicopter’s auxiliary tank and a very small quantity in the main tank. Assessment of the helicopter indicated that the engine was stopped before the helicopter impacted the ground. Additionally, there was no evidence of failure of the harness, sling, attachments or the hooks system. There was also no evidence of failure or defects to the airframe or the helicopter’s systems likely to have contributed to the accident.
This analysis will discuss:
- fuel uplift
- the pilot’s awareness of the helicopter’s fuel state
- potential reasons for the in-flight engine stoppage
- the circumstances relating to the release of the sling person and the helicopter’s collision with terrain.
The influence of the helicopter operator’s safety management system and the Civil Aviation Safety Authority’s (CASA’s) process for issuing authorisation instruments will also be analysed. Finally, the potential contribution of the helicopter’s state of airworthiness, presence of cocaine metabolites in the pilot’s toxicology results and lack of emergency location transmitter fitted to the helicopter will also be considered.
Fuel uplift
After reportedly being filled with fuel, the helicopter departed from the operator’s hangar at Noonamah on the outskirts of Darwin at about 0703 in company with 2 other R44 helicopters. Fuel receipts showed that the Noonamah fuel tank contained only blue‑coloured 100 low lead (LL) Avgas fuel and there was no record of the quantity of fuel uplifted to VH-IDW at Noonamah on the accident morning. An in-flight photo taken en route to Mount Borradaile showed the chronometer reading 45 minutes, which the pilot reported usually setting to zero after refuelling.
A subsequent report that VH-IDW was filled the evening prior to the accident and not on the accident morning, suggested that VH-IDW departed with less than full fuel (151–153 L usable). However, the in-flight photo showed the gauges reading slightly below 3/4, consistent with the helicopter having departed Noonamah at or near full, based on the reported fuel flow rate of about 65 L/h.
Based on flight data, witness accounts and evidence from the in-flight photo, the 3 helicopters probably arrived at the en-route fuel depot at Mount Borradaile at around 0816. The accident pilot reported that they always left Mount Borradaile with full fuel tanks and their intention had been to refuel there. However, they were unable to confidently recall the specific fuelling activities at Mount Borradaile or events thereafter.
There were consistent recollections from others present at Mount Borradaile that VH-IDW was the first helicopter to arrive and that it did not have a fuel drum pump on board to transfer fuel from the drum stock. However, there were also differing recollections of the order in which the R44s were refuelled, with each helicopter being repositioned in turn close to the drums and the entire activity being undertaken without shutting any of the aircraft down. Two people reported seeing the accident pilot pumping fuel, including into VH-IDW. However, in a submission following review of the draft report, one of those reported not having seen anyone fuel VH-IDW. One other person reported assisting the pilot to pump fuel. However, that person’s recollection subsequently changed to having observed the egg collector partially fuelling VH-IDW before taking over to finish the fuelling themselves.
In the approximately 14 minutes the helicopters were at Mount Borradaile, there was probably sufficient time to refuel 3 helicopters given the number of people available to assist. Two witnesses reported that the egg collector was flying VH-IDW, from the right seat, when it departed Mount Borradaile, and that the accident pilot removed the dual controls after arriving at King River. However, the accident pilot and another egg collector reported that the accident pilot had flown VH-IDW from Mount Borradaile, having removed the dual controls there.
The ATSB’s assessment, based on the consistent accounts of the first 2 witnesses and recorded GPS data transmitted to a server from the egg collector’s phone indicating they were using an electronic flight bag application to navigate between Mount Borradaile and King River, was that it was more likely that the egg collector flew VH-IDW from Mount Borradaile to King River.
The person who prepared the 2 fuel drums for the R44 crews on the accident morning at Mount Borradaile had a detailed recollection of which drums were used and subsequently obtained fuel samples from those drums for ATSB testing. The samples were confirmed as green‑coloured 100/130 fuel in accordance with the relevant specifications and the delivered batch test data.
The first person to arrive at the accident site, reported that there was a fuel smell but later assessed that may have been from a leaking jerry can stored behind the pilot’s seat. The first emergency responder on site reported the absence of a fuel smell, but noted leaking hydraulic fluid that created a sheen on the water. The Helibrook chief pilot also reported that there was no fuel smell when they arrived. As the helicopter wreckage was in a swamp, with water slowly running downstream, it was possible for fuel to also drain away, although no one observed that occurring. There were also varying reports that people who attended the site after the accident looked in one or both fuel tanks and detected fuel, but no one attempted to measure the quantity.
When ATSB investigators arrived at the accident site 2 days after the accident, there was no fuel present in the auxiliary tank and only a small quantity of fuel in the main fuel tank. Although it was not possible to accurately measure the quantity in the main fuel tank on‑site, it was assessed by the ATSB investigators to be significantly less than the documented unusable quantity of 4 L. Recognising that the worst‑case helicopter orientation is used to arrive at that unusable fuel quantity, it is possible to consume some of the published 4 L in‑flight. However, it was considered unlikely that the small remaining quantity observed by the ATSB on‑site would have sustained the engine. As such, following the ground collision some fuel was either removed from the helicopter or was able to drain away.
Examination of the helicopter identified that it was possible for fuel to drain under gravity from the tanks through the fuel system and out via either a fractured fitting between the fuel flow transducer and flow divider, or through the drain at the gascolator. However, the loose organic black soil from the accident site that filled the fractured transducer fitting would likely have been flushed out if fuel had drained through that route. There was also no fuel staining on the cowls, but this may have been due to water ingress into the cowls at the accident site. Images taken of the site 4 months after the accident showed no evidence of vegetation dieback that would be indicative of significant fuel leakage, however over 200 mm of rain had fallen in the intervening period.
The helicopter manufacturer assessed that the deformation of the fuel tanks was consistent with a lower fuel quantity, but was unable to distinguish between some or no usable fuel remaining, or between impact damage and possible bulging due to internal contents. However, the degree of tank deformation indicated that the helicopter was not filled with any significant amount of fuel at Mount Borradaile unless the accident occurred at about the time the helicopter was located. This was considered unlikely because the accident occurred between the clearing and the first target nest in the direction of travel that morning. Other than the egg collector’s phone briefly contacting a cell tower at 0858, there was no evidence the crew planned to go anywhere other than the 3 nests they had been allocated to collect, and no eggs had been collected. There was no communication between the cell tower and the pilot’s phone at that time.
Scientific testing of the fuel drained from VH-IDW after the accident found that it was 100 LL Avgas and likely contained no more than 1% 100/130 fuel, consistent with residue from previous fuelling. This physical evidence opposed any significant quantity of 100/130 fuel being added to the tank at Mount Borradaile. Although it was later reported that it was possible for other drums at Mount Borradaile containing 100 LL to have been used, the distinct drum markings and reported general usage of the fuel location made that unlikely.
The potential effect of interference with the site was considered in relation to the removal of the jerry cans and the fuel testing results. The only plausible scenario that permitted both refuelling at Mount Borradaile to occur and the sole presence of 100 LL when chemically tested was if 40 L of 100 LL fuel was poured from the jerry cans into VH-IDW after the accident and then subsequently largely leaked away.
While it was possible that the addition of 40 L of 100 LL from the jerry cans could produce the attained test results, there was no evidence that occurred. Conversely, those on‑site reported that one of the jerry cans was damaged on impact and fuel from the jerry cans out of VH-IDW was used to fuel one of the other helicopters before departing the accident site. This was consistent with reports of empty jerry cans being used at Mount Borradaile to transfer fuel from a drum to a helicopter on the return trip. Additionally, the lack of fuel smell, cowl staining and soil lodged in the fractured transducer fitting also indicated that 40 L of fuel was not poured through the system.
Considering the relatively greater strength of the technical evidence, the ATSB concluded that the helicopter was probably not refuelled at Mount Borradaile prior to the commencement of the egg collecting activity.
Detection of low fuel state
The sources of information for the pilot regarding the helicopter’s fuel state were the chronometer, fuel totaliser, fuel log, fuel gauges and low fuel warning system.
The pilot’s normal practice, consistent with the in-flight photo was to reset the chronometer to zero following refuelling. The chronometer did not store data and therefore its reading at the time of accident could not be determined. The pilot reported that they did not use the totaliser, which was not visible in the in-flight photo. Further, there were no records of fuel uplifted to VH-IDW for the accident day.
When tested, the main tank indication overread within a needle-width at empty, a quarter and half full. The auxiliary tank gauge indicated very close to the actual fuel level. The placard below the main fuel tank gauge, from the last fuel calibration, indicated the main tank gauge would significantly underread. Therefore, had the pilot been relying on the calibration placard’s quantity to interpret the gauges, there would have been less fuel in the main tank than expected, other than when full or empty. However, based on the in-flight photo showing the fuel gauges, and testing of the gauge senders and gauges, the gauges would likely have been reasonably accurate.
The calibration placard also stated the low fuel warning light would illuminate with 20 L fuel total remaining and the pilot recalled that it would illuminate with 18 L remaining. However, according to VH-IDW’s Pilot’s Operating Handbook, the low fuel warning light would illuminate with 11 L of usable fuel remaining, which would be 14 L total. It is therefore likely that, if the light illuminated in flight, the pilot would think there was more fuel remaining than the POH indicated. The accident pilot also reported that their normal practice was to depart Mount Borradaile with full fuel. This expectation may have influenced the degree to which the pilot focused on the fuel quantity.
The low fuel warning system was found to be functional. However, it is possible that, if the low fuel light and/or fuel gauges were indicating low fuel, the accident pilot may have dismissed these cues as they would not have been consistent with their expectation. Additionally, had the low fuel light illuminated, the pilot may have thought there was more fuel remaining than actual.
A previous ATSB investigation into a Robinson R22 accident that occurred during mustering operations, found that the nature of the operation potentially diverted the pilot’s attention away from monitoring the helicopter’s fuel state. This resulted in probable fuel exhaustion and stoppage of the engine in flight. This potential also existed in conducting slinging operations, as the pilot would have had their head out the door, looking down at the sling person, and not at the instrument panel or gauges. This limitation of monitoring gauges was included in the Helibrook operations manual and suggested pilots conducting low-level aerial work operations also monitor elapsed flight time. However, had the chronometer been reset to zero at Mount Borradaile but the helicopter not refuelled, this would have provided an erroneous indication of time since refuelling.
Had the pilot detected a low fuel situation, there were 2 jerry cans of 100 LL fuel in VH-IDW that could be used for refuelling and multiple landing sites were available. Ultimately, while indications of the in-flight fuel state should have been available to the pilot, the pilot may have not observed them, dismissed them as erroneous or misinterpreted them. In any case, it is likely that the pilot did not recognise the helicopter’s fuel state.
In assessing whether the pilot’s experience as a helicopter pilot and in slinging operations would mitigate the risk of fuel exhaustion, the ATSB reviewed fuel exhaustion occurrences in the 10-year period 2011–2020. The median total experience of pilots involved in fuel exhaustion occurrences reported to the ATSB in that period was 1,227 hours. This illustrates that experience alone does not mitigate fuel exhaustion.
In-flight event assessment
The ATSB analysed what in-flight event occurred that led to the egg collector dropping their equipment, the pilot releasing them, and the subsequent helicopter collision with terrain. The orientation of the accident trail was consistent with the route between the clearing and the nest most likely to be collected first. There was no evidence of snagging of the sling line or egg collector that led the pilot to release them. There was also no evidence of in-flight breakup or damage to the helicopter airframe due to failure, bird strike, or consistent with a manoeuvring error or mishandling.
Significantly, there was physical evidence that the engine was stationary when the helicopter impacted the ground, and no evidence that supported engine rotation was identified. Based on advice from the helicopter manufacturer, the ATSB assessed whether the engine had stopped in flight or because of the main rotor blade striking the tree while the engine was producing low power. The damage to the main rotor blade, including one broken pitch link, was consistent with a tree strike in a low rotor energy state. The diameter of the branches struck on the first 2 strikes was assessed as too small to stop the engine. The last tree strike was more substantial but occurred below the main rotor blade height, indicating the helicopter impacted the ground prior to that strike. On balance it was therefore considered likely that the engine stopped in flight.
Reason for engine stoppage
Pilot action
The ATSB assessed the possibility of inadvertent pilot-induced engine stoppage in the context of the pilot’s logged total helicopter flight experience of about 2,500 hours and more than 300 hours of sling time. Robinson advised that there had been several accidents in which a pilot had inadvertently induced an engine stoppage by rolling off the throttle too fast. This had occurred in flight training when simulating an engine failure and as an incorrect response to abnormal situations such as a sudden change in engine RPM or discrepancy between engine and rotor RPM.
It was considered very unlikely that the pilot would have simulated an engine failure at any stage during the accident flight. Although it could not be determined whether there was another situation that led to the pilot quickly rolling off the throttle, this would be a highly unlikely response of an experienced pilot, while conducting human external cargo (HEC) operations.
Aircraft, engine and fuel system examinations
The ATSB conducted extensive airframe and component examinations. Independent experts were engaged to conduct engine and fuel system examinations, overseen by the ATSB and other involved parties. The results were also analysed by manufacturers of the helicopter and engine, and other specialists. There was no evidence of a defect that could have led to sudden stoppage of the engine, of any critical component of the engine, fuel, or other helicopter system. Examination of the engine and fuel system found:
- no evidence of any issue with air intake to the engine or the exhaust system
- low static compression in one cylinder, but the actual compression was probably higher when the engine was running and warm, which was unlikely to have resulted in sudden in-flight complete or substantial power loss
- several valve clearances were out of service limits
- no evidence of any issue with the spark plugs, ignition leads or magnetos
- no fuel remaining in the system other than the main fuel tank, no evidence of fuel contamination with debris, water, or wrong fuel, no defects in the fuel system and no condition likely to prevent usable fuel reaching the engine.
The out‑of‑limit valve clearances and low cylinder compression probably reduced the power that the engine was able to produce. However, the accident was not consistent with insufficient power available to lift the sling person, as the maximum power required would have occurred during the lift and before forward speed (consistent with the accident trail) was achieved. The ATSB assessed VH-IDW for all the possible reasons for an engine problem listed by the engine and helicopter manufacturer. The aircraft, engine and fuel system examinations did not identify any failure or condition, other than an absence of fuel throughout the system, that would likely result in sudden complete or substantial engine power loss.
Fuel exhaustion
The helicopter had not been shut down between when it was started before 0700 and last seen at a clearing near King River at about 0855. No recorded data was available to indicate the helicopter’s movements after 0900, including at the time of accident. However, the egg collector’s phone was momentarily in range of the nearest phone tower at 0858 and the accident pilot’s phone was not. As mobile phone reception was only in range when about 300 ft above the accident site, this may indicate that the egg collector was briefly airborne in the helicopter at that time.
As described above, the accident occurred between the clearing and VH-IDW’s first target nest, and no eggs had been collected. Additionally, no communication had been made with VH-IDW since about 0900, and it was considered unusual for the crew not to communicate for over an hour.
The operator reported VH-IDW’s normal fuel flow was 65–70 L/h, equating to a fuel endurance between 2 hours 31 minutes and 2 hours 42 minutes. Had the helicopter not been refuelled since 0658 at Noonamah, the helicopter would have exhausted usable fuel between 0929 and 0940. Furthermore, if the helicopter had been refuelled the previous evening and then travelled for about 23 minutes to Noonamah, and was not fuelled prior to the start of the accident day, fuel exhaustion was possible from 0904. Low cylinder compression evident in the No. 6 cylinder at engine examination, and high power settings, as evident in the in-flight photo, increase fuel consumption. Fuel exhaustion was therefore possible earlier than 0929. This was consistent with the search pilot’s estimation that the accident occurred at about 0922, when they were on the ground and out of communication range, and other crew heard a static radio transmission that may have been from VH-IDW.
The helicopter’s hour meter read 2070.05 at the accident site and the maintenance release recorded 2067.6 at the end of the previous day. This indicated the helicopter had a flight time of 2.45 hours (not including time on the ground), which would also support fuel exhaustion. However, this was considered unreliable evidence as the pilot reported that the hour meter was never running when they operated VH-IDW, in which case the maintenance release did not reflect actual hours flown.
In summary, considering the:
- likely lack of fuel on site, including in the helicopter tanks
- elapsed time since last probable refuelling
- timeframe in which the accident likely occurred
- the absence of any fault with the helicopter likely to result in sudden or substantial power loss
fuel exhaustion was assessed as the probable reason for engine stoppage.
Release of sling person and helicopter terrain impact
There was no evidence of a failure of the hooks system or sling equipment. The pilot reported that they always checked both quick release systems were functional before slinging. Had the experienced egg collector not attached themselves correctly, it was unlikely the pilot would have been able to lift them into the air attached to the helicopter and traverse above trees before they were released. By design and certification, inadvertent release of the hooks by the pilot was extremely improbable. Furthermore, inadvertent release of the egg collector would not have resulted in the subsequent helicopter ground collision without an additional failure/malfunction or mishandling. Therefore, the pilot almost certainly released the sling person, consistent with their stated procedure in the event of an engine failure or malfunction in the vicinity of trees.
Due to a lack of recorded data or recollection from the pilot, an assessment could not be made of the height and speed of the helicopter when the engine stopped or the egg collector was released. The trees between where the helicopter probably took off and the vicinity of the accident site were between 12–15 m tall, with taller trees up to 18 m tall closer to the crocodile nest site. The pilot’s reported procedure was to remain within about 5 m above the vegetation and therefore, if following their stated practice, the egg collector was likely about 20 m above the ground when the power loss occurred. Considering the length of the sling line, that would have positioned the helicopter about 50 m (164 ft) above the ground.
To estimate the height from which the egg collector was released, their injuries were assessed by a forensic pathologist using survivability research into falls from heights. Based on the injuries sustained, the pathologist assessed that the egg collector likely fell from at least 5 m above the ground. Additional research reviewed by the ATSB that considered how specific injuries varied with height indicated a likelihood that the egg collector was released from above 9 m, from which most falls are fatal.
Based on the pilot’s reported normal practice to minimise height and speed while slinging, the helicopter was likely operating within the ‘avoid’ area of the helicopter’s height-velocity graph. In that area, the combination of height and airspeed was such that a pilot may have been unable to complete an autorotation landing without damage. This was consistent with the low rotor energy and crushing of the fuselage evident in the damage sustained by VH-IDW.
The helicopter’s vertical descent through at least the last 8 m (24 ft), which was the height of the tree that the main rotor blade struck 3 times, was consistent with an attempt to avoid the obstacles ahead (due to densely growing tall trees) relative to the direction of travel.
Helibrook safety management
Helibrook had introduced a CASA-accepted safety management system (SMS) in conjunction with CASA’s approval of the Helibrook chief pilot. This included purchase of a third‑party produced SMS manual and assigning the operations manager to also perform the safety manager role. The SMS manual stated that through the SMS, Helibrook would identify hazards and risks, with the goals of minimising risk, maintaining the health of stakeholders, and continually improving safety.
An assessment of the operator’s SMS following the accident quickly identified that in the 2 years since its approval, Helibrook had not implemented the system described in the SMS manual. Time or resources had not been allocated to safety management tasks, and the safety manager’s priority had been to fulfill their other role as operations manager. There was no evidence of a maturing safety culture, in which effective hazard identification enabled actions to proactively manage risks and prevent accidents. No formal, documented risk assessment had been conducted for any of Helibrook’s approved activities, including human external cargo (HEC) operations. As an operator conducting a specialised high-risk activity, application of the SMS would have assisted the identification of hazards and risk controls to reduce the risk of harm to operating crew.
CASA’s approval to conduct HEC operations required the pilot and egg collector to assess that the risk of heat illness and crocodile attack outweighed the risks of slinging. A structured risk process would have provided a means for this assessment to be made as well as identifying occasions when slinging was unacceptably risky. The same process should also have identified mitigations to reduce the:
- likelihood of an emergency event occurring, such as:
- good maintenance practices and adherence to operating limitations to ensure ongoing helicopter airworthiness
- ensuring that required pilot briefing and training in HEC operations were conducted, including fuel management
- consequences of an in-flight emergency, such as height and speed limits for carrying the sling person, and fitting the helicopter with an emergency locator transmitter.
In not using their SMS, Helibrook did not identify the risks associated with conducting human external cargo operations, particularly the carriage of the egg collectors at non‑survivable fall heights, and ensure they were adequately managed.
The Civil Aviation Safety Authority’s approval process
Approval process
Picking up and carrying a person outside a helicopter was not permitted without specific authorisation. CASA could only grant such an authorisation, if doing so would be unlikely to have an adverse effect on safety. To ensure safety was preserved, CASA could impose conditions set out in an authorisation instrument.
Guidance was available for the administrative side of processing a request for an authorisation. However, there were no guidance or tools for conducting the safety assessment to determine whether an authorisation and its conditions assured the preservation of safety. Flight operations considerations for approving an aerial work activity were detailed in the Air Operator’s Certificate (AOC) Handbook, but this did not include the management of risk. The AOC handbook also contained safety management and risk assessment guidance for assessing an AOC holder's SMS, but the CASA delegates contacted by the ATSB as part of this investigation did not consider this relevant to the instrument approval process.
The first approval instrument to conduct HEC operations for the purpose of crocodile egg collection was reported to have been issued in 2007, and subsequently reissued generally on an annual basis. CASA was unable to locate records of instruments issued before 2010, any assessment as to whether the authorisation was likely to adversely affect safety, or how the imposed conditions mitigated the risks. The first instrument obtained by the ATSB was for 2010 and listed 20 conditions. These included a requirement that hooks were fitted to the helicopter under an appropriate design approval and limitations to the height, speed and distance the sling person could be carried.
The CASA delegates who issued authorisation instruments for R44 HEC for crocodile egg collection from 2013–2021 incorrectly assumed a risk assessment had been performed when the first instrument was issued. The delegates also assumed previous approvals meant that the risks of HEC operations had been assessed as acceptable by CASA, and that the conditions included in the instrument mitigated the risks. However, none of the delegates had sighted a risk assessment for the activity, nor did they conduct one, including when changing or removing instrument conditions. Additionally, although the instrument only permitted operators to conduct HEC if there was an overall safety advantage in reducing the risk of crocodile attack and heat illness, CASA did not ensure that the operators had a process for assessing the relative risks.
In the absence of a formal risk assessment process, delegates based their approval of the activity and the imposed conditions on the advice of CASA flight operations and airworthiness inspectors, and a reasonableness test. Additionally, delegates considered the instruments were reissues of an existing approval even when removing or amending conditions. Therefore, if there were no changes to procedures and no accidents, they assessed that there was no reason not to issue an authorisation, as the level of safety was considered not to have changed.
A draft HEC in piston engine rotorcraft risk management plan (RMP) using a CASA general aviation template was prepared by CASA Flight Standards Branch personnel and presented to CASA executive in 2013. The RMP and associated template was a formal risk assessment tool. The RMP assessed that HEC operations in single engine piston (R44) and turbine helicopters was an unacceptable risk without mitigations to improve helicopter reliability, and speed, height and duration limitations for carrying the HEC.
The RMP formed the basis of CASA’s proposed standard to cease issuing approvals for HEC with the R44 and to require a single engine turbine helicopter with a usage monitoring system. This was due to the associated higher risk of in-flight power loss and additional failure modes of an R44. The turbine engine requirement aligned with US and European regulations and was to be included as an amendment to Civil Aviation Order 29.6. That amendment was abandoned in 2016, due to planned implementation in 2018 of the same ruleset incorporated in Civil Aviation Safety Regulations Part 138. However, regulatory change took longer than anticipated, and Part 138 was implemented in December 2021. None of the delegates involved in approving instruments after 2013 reported having seen the RMP.
As the instrument conditions were described as risk mitigations, a formal risk assessment would have enabled delegates to quantify the change in overall risk associated with changes to, or removal of, conditions. Without a formal risk management process, CASA delegates were unable to show in a structured way that an authorisation did not adversely affect safety or that the conditions included in an authorisation were sufficient to achieve the required level of safety.
Influence on human external cargo risks
Once the hooks met the required certification standard, failure of the hooks was extremely improbable. As a result, CASA approved amendments to the rotorcraft flight manual supplement associated with the dual hooks. These included the removal of limits for the height and distance a sling person could be carried and an increase of the maximum slinging speed to 60 kt. However, this did not consider circumstances that could result in release of the sling person, other than failure of the hooks.
CASA delegates then removed the HEC limitations from CASA’s instrument conditions. It is unclear why these conditions were removed. However, as a formal risk assessment was not performed it was not identified that there were other failure conditions likely to result in release of the sling person and that the removal of height and speed limits for carrying the sling person significantly increased the overall risk.
Falls from greater than 5 m above the ground are more likely to result in a fatality. CASA’s removal of those limitations meant that an operator could both operate within an authorisation instrument’s conditions and permit an avoidable fatal outcome for a sling person in the event of an emergency release, such as occurred during this accident.
Continued unmitigated operational risk
As CASA delegates had not formally assessed the operational risk of using an R44 helicopter they continued to approve R44 HEC for crocodile egg collection without assurance that aviation safety was preserved. Although CASA’s RMP assessed that a single turbine engine helicopter with a usage monitoring system had a higher reliability and less likelihood of engine failure than an R44 helicopter, it did not consider or compare the hazard of fuel exhaustion.
Having formally assessed the risks for the RMP in 2013, the following year, CASA Flight Standards Branch personnel engaged with operators who conducted HEC for crocodile egg collection and advised of CASA’s intent to require a turbine helicopter with a usage monitoring system for improved helicopter reliability. CASA personnel then drafted the relevant legislation and engaged with the industry before it was finalised. Although operators had been notified and engaged during the rulemaking process, shortly prior to commencement of the regulations in 2021, a CASA delegate issued Helibrook with a 3-year instrument approving continued use of an R44 helicopter for human slinging operations. This resulted in continuation of what CASA had assessed as an unacceptable ongoing risk.
There was insufficient data available of helicopter fuel exhaustion accidents to indicate an increased risk in piston engine helicopters compared with turbine engine helicopters. There was also insufficient evidence from which to assess the difference in outcome between an autorotation in a single engine turbine helicopter and in an R44. Single engine turbine helicopters, with a higher inertia rotor than the R44, may provide more opportunity to place the sling person on the ground, as occurred in a Bell 407 accident in the US in 2022, and reduce the consequences for the pilot in an autorotative landing. However, operating in any helicopter's height-velocity avoid area does not ensure a safe landing can be made.
Without adequate height and speed limitations to protect the sling person, there is no evidence that the use of a single turbine engine helicopter would have altered the outcome in this accident.
Engine defects
The low compression in one cylinder and valve clearances out of service limits increased the likelihood that the engine's maximum power output was reduced. Although the engine was derated, to counter the reduction in performance at higher density altitudes, the defects increased the risk of having insufficient performance for the helicopter to hover out of ground effect, essential to conduct slinging operations.
The higher-than normal fuel flow for slinging operations was unlikely to have affected the pilot’s assessment of fuel endurance. This was because the pilot had conducted slinging in VH-IDW the day prior to the accident and the fuel flow would unlikely have changed since then. The in-flight photo taken on the accident morning showed the helicopter operating above the manifold pressure limit at the time, which may have been symptomatic of reduced engine performance.
The approval to conduct HEC operations required that the engine was capable of making maximum rated power and able to hover out of ground effect 3,000 ft above the ground. Poor engine condition increased the likelihood of insufficient power available to conduct safe slinging operations and of an in-flight failure. However, there was no evidence of any failure or condition that would have suddenly stopped or significantly reduced engine power.
Helicopter hours overrun
Accurate recording of time in service is required to ensure helicopter components are inspected, overhauled or replaced within life limits. Exceeding the life limits increases the probability of component failure and renders the helicopter unairworthy.
VH-IDW was to be maintained in accordance with the airframe and engine manufacturers’ maintenance schedule, which required a periodic inspection every 100 hours or 12 months, whichever occurred sooner, and was subject to overhaul at 2,200 hours or 12 years, whichever occurred first. Based on a review of VH-IDW’s maintenance releases, at the periodic inspections, the helicopter’s hour meter matched the time in service recorded on the maintenance release.
Based on the hour meter reading at the accident site, VH-IDW had about 192 hours until overhaul. The ATSB found the hour meter connected, but one of the 2 connections was only finger tight, consistent with having been connected by hand. Additionally, the hour meter had almost certainly been disconnected for periods, resulting in under-recording of the hours in operation. Based on a comparison of the hours recorded on VH-IDW’s maintenance releases with hours recorded in spreadsheets and on the pilot’s phone, it was likely the helicopter had been overrunning the 100-hour maintenance intervals and had exceeded its overhaul life. This was also supported by a CASA airworthiness inspector’s review of maintenance records, which identified the engine-driven fuel pump being replaced at decreasing recorded hourly intervals, as VH-IDW approached its end of overhaul life and while being operated by Helibrook.
In-use hours for the hooks were independent from total helicopter hours but were also not being recorded. Additionally, one hook was overdue for overhaul based on calendar time and the hooks had not been maintained as required, but there was no evidence these had failed.
Although overrunning maintenance, inspection and overhaul periods increased the likelihood of component failure, there was no evidence of an engine, airframe or hook component failure that resulted in the engine stoppage, helicopter accident or increased severity of injuries or damage. Despite that, while operating in the height-velocity avoid area, a successful autorotation was not guaranteed. Therefore, high reliability of the helicopter and systems was necessary to mitigate the risks to the pilot and the sling person. In stopping the hour meter and exceeding maintenance, inspection and overhaul limits, the operator increased the likelihood of a catastrophic component failure of the helicopter. This posed an unnecessary increase in risk for the pilot and particularly sling crew conducting HEC operations.
Cocaine metabolites
Cocaine is an illicit drug and can have deleterious effects on pilot performance. Possible effects include risk-taking, inattentiveness and poor impulse control. Although the pilot reported that they did not use cocaine, very low levels of cocaine metabolites were found in the pilot’s toxicology results.
On the basis that the metabolites indicate exposure to cocaine, the detected levels indicated the pilot had not been exposed to cocaine within the previous 24 hours and may not have been affected by cocaine on the accident day. There was insufficient evidence to enable an assessment of whether the drug contributed to the development of the accident. However, the indication of exposure to cocaine is highlighted, as the effects of cocaine and post-cocaine exposure clearly increase risk to aviation activities. The post-cocaine exposure effects can include fatigue, depression and inattention.
Emergency locator transmitter
The helicopter's emergency locator transmitter was not mounted and did not activate in the accident impact. Although the actual time of the accident could not be established, there is a high likelihood that it was a significant time before the helicopter was located. Therefore, had the emergency locator transmitter been fitted and activated on impact, emergency medical care may have arrived sooner.
Immediate notification to rescue medical services can have a significant effect on the outcome for occupants of a serious aircraft accident. Although prompt medical attention would not have altered the outcome for the egg collector, the pilot’s condition likely worsened over time since the accident. The actions of the individual to search for VH‑IDW and alert emergency services contributed to the pilot’s survival, but more timely initiation of medical assistance would have reduced the risks of exacerbating the pilot’s injuries and deterioration of their condition.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’. In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
At the time this report was published there were ongoing police investigations concerning the status of evidence at the accident site. Acknowledging this, the following findings are made with respect to the collision with terrain involving Robinson R44 II, VH-IDW, at King River, Northern Territory, on 28 February 2022 on the evidence obtained by the ATSB.
Contributing factors
- Following likely not refuelling at Mount Borradaile, the pilot did not identify the reducing fuel state before the helicopter engine stopped, probably due to fuel exhaustion.
- During the autorotation, the pilot released the egg collector above a likely survivable height, resulting in their fatal injuries.
- The pilot continued the autorotation to the ground but there was insufficient main rotor energy to cushion the landing, resulting in serious injuries to the pilot and substantial damage to the helicopter.
- Helibrook’s approved safety management system was not being used to systematically identify and manage operational hazards. As a result, risks associated with conducting human external cargo operations such as carriage of the egg collector above a survivable fall height were not adequately addressed. (Safety issue)
- The Civil Aviation Safety Authority (CASA) did not have an effective process for assuring an authorisation would be unlikely to have an adverse effect on safety. As a result, CASA delegates did not use the available structured risk management process to identify and assess the risks, ensure appropriate and adequate mitigations were included as conditions of the approval, or assess the effects of changes on the overall risk. (Safety issue)
- CASA's lack of effective process for assuring an authorisation would be unlikely to have an adverse effect on safety resulted in the removal of height, speed, and exposure limits, which permitted carriage of the egg collector above a survivable fall height.
Other factors that increased risk
- CASA's lack of effective process for assuring an authorisation would not have an adverse effect on safety resulted in the continued operation of piston engine helicopters for human sling operations without adequate mitigations and the issue of a 3-year instrument to Helibrook shortly prior to the commencement of improved regulations, which would require a turbine engine helicopter for human slinging operations.
- Several engine defects were present at the time of the accident. Although there was no defect likely to result in sudden power loss, these factors likely affected the engine maximum power output and fuel consumption.
- Helibrook had likely overrun the helicopter's maintenance, inspection and overhaul periods, which increased the likelihood of the helicopter experiencing a technical failure or malfunction.
- The presence of cocaine metabolites in the pilot’s blood sample indicated the pilot had been exposed to cocaine within the previous few days, increasing the likelihood of fatigue, depression and inattention.
- The helicopter's emergency locator transmitter had been removed from its mount prior to the accident. Therefore, it could not activate automatically, which likely delayed the emergency response.
Safety issues and actions
|
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
CASA lack of effective process
Safety issue number: AO-2022-009-SI-01
Safety issue description: The Civil Aviation Safety Authority (CASA) did not have an effective process for assuring an authorisation would be unlikely to have an adverse effect on safety. As a result, CASA delegates did not use the available structured risk management process to identify and assess the risks, ensure appropriate and adequate mitigations were included as conditions of the approval, or assess the effects of changes on the overall risk.
Helibrook inadequate safety management
Safety issue number: AO-2022-009-SI-02
Safety issue description: Helibrook’s approved safety management system was not being used to systematically identify and manage operational hazards. As a result, risks associated with conducting human external cargo operations such as carriage of the egg collector above a survivable fall height were not adequately addressed.
Glossary
| AC | Advisory circular |
| AEB | Airworthiness and Engineering Branch |
| AMSA | Australian Maritime Safety Authority |
| AOC | Air Operator’s Certificate |
| AWB | Airworthiness bulletin |
| BHP | Brake horsepower |
| BQRS | Back-up quick release system |
| CAO | Civil Aviation Order |
| CAR | Civil Aviation Regulations |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| CST | Central Standard Time |
| DAMP | Drug and alcohol management plan |
| DAS | Director of Aviation Safety |
| DOI | (US) Department of the Interior |
| EASA | European Union Aviation Safety Agency |
| ELT | Emergency locator transmitter |
| EMI | Electromagnetic interference |
| EO | Engineering order |
| EPIRB | Emergency position indicating radio beacon |
| FAA | (US) Federal Aviation Administration |
| FAR | (US) Federal Aviation Regulations |
| FCU | Fuel control unit |
| FMEA | Failure modes and effects analysis |
| FPRV | Fuel pressure relief valve |
| HAAMC | Head of aircraft airworthiness and maintenance control |
| HEC | Human external cargo |
| HF | High frequency |
| H/V | Height-velocity |
| IAS | Indicated airspeed |
| ICAO | International Civil Aviation Organization |
| KIAS | Knots indicated airspeed |
| LL | Low lead |
| MOS | Manual of standards |
| MR | Maintenance release |
| NT | Northern Territory |
| NTSB | (US) National Transportation Safety Board |
| POH | Pilot’s operating handbook |
| PQRS | Primary quick release system |
| RFMS | Rotorcraft flight manual supplement |
| RHC | Robinson Helicopter Company |
| RMP | Risk management plan |
| RPM | Revolutions per minute |
| SMS | Safety management system |
| SN | Safety Notice |
| SOP | Standard operating procedure |
| SPO | Specialised operation |
| STC | Supplemental type certificate |
| SWMS | Safe work method statement |
| TBO | Time between overhaul |
| UHF | Ultra high frequency |
| US | United States |
| USG | US gallons |
| VHF | Very high frequency |
| WHNT | Wild Harvest Northern Territory |
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- pilot of the accident flight
- other pilots who conducted flights for the operator
- other crews conducting egg collecting
- helicopter maintainer
- helicopter operator and chief pilot
- Northern Territory Police Fire and Emergency Service
- Wild Harvest Northern Territory
- Civil Aviation Safety Authority
- CareFlight
- helicopter manufacturer
- engine manufacturer
- Defence Science and Technology Group
- recorded data from OzRunways.
References
ATSB (2013), Starved and exhausted: Fuel management aviation accidents. Avoidable Accidents No. 5.
Abder-Rhman, H., Jaber, M.S., & Al-Sabaileh, S.S. (2018). Injuries sustained in falling fatalities in relation to different distances of falls. Journal of Forensic and Legal Medicine 54:69-73.
Australian Radiation Protection and Nuclear Safety Agency (n.d.) Safety culture, https://www.arpansa.gov.au/regulation-and-licensing/safety-security-transport/holistic-safety/safety-culture, ARPANSA, accessed 3 January 2023.
Civil Aviation Safety Authority (2021). Aerial work risk management (advisory circular AC138-05 v1.1), https://www.casa.gov.au/aerial-work-risk-management, CASA, accessed 22 December 2022.
Civil Aviation Safety Authority (2014). SMS for aviation – a practical guide, Safety Risk Management, https://www.casa.gov.au/search-centre/safety-kits/resource-kit-develop-your-safety-management-system, CASA, accessed 22 December 2022.
Civil Aviation Safety Authority (2019) Resource booklet 2: Safety culture, Safety behaviours: human factors for pilots, 2nd edition, https://www.casa.gov.au/search-centre/safety-kits/safety-behaviours-human-factors-pilots, CASA, accessed 22 December 2022.
Canada Environmental Technology Centre (CETC) Oil Properties database, https://www.etc-cte.ec.gc.ca/databases/OilProperties/Default.aspx, accessed 21/08/2022.
Civil Air Navigation Services Organisation (2008) Safety culture definition and enhancement process, https://www.icao.int/NACC/Documents/Meetings/2018/ASBU18/OD-10-Safety Culture Definition and Enhancement Process.pdf, CANSO, accessed 22 December 2022.
Couper, F.J. and Logan, B.K. (2014 revision). Drugs and Human Performance Facts Sheets. Technical Report DOT HS 809 725, National Highway Traffic Safety Administration (NHTSA), Washington DC.
Department of Defence, Defence Science and Technology Group (2022). Fuel analysis for ATSB Investigation AO-2022-009 involving Robinson R44, VH-IDW. DSTG-CR-2022-0060.
Department of the Interior (2010). Helicopter short-haul handbook. US DOI 351 DM 1
European Union Aviation Safety Agency (n.d) Safety culture, EU-South East Asia Aviation Partnership Project (EU-SEA APP), EASA.
Federal Aviation Administration (2014). Advisory Circular 27-1B, https://www.faa.gov.documentLibrary/media/Advisory_Circular/AC_27-1B___.pdf, accessed 4 June 2023.
Federal Aviation Administration (2013). Emergency procedures training, www.FAAsafety.gov, accessed 21 December 2022.
Federal Aviation Administration (2019). Helicopter Flying Handbook. FAA-H-8083-21B
Federal Aviation Administration (2020). Safety management system, 8000.369C, FAA: Washington, DC.
Hudson P (n.d.) Safety management and safety culture – the long, hard and winding road, https://skybrary.aero/sites/default/files/bookshelf/2417.pdf, Leiden University, The Netherlands, accessed 22 December 2022.
International Civil Aviation Organization (2018). Safety Management Manual, 4th edition. ICAO Doc 9859, Montreal.
Icer, M., Guloglu, C., Orak, M., Ustundag, M. (2013). Factors affecting mortality caused by falls from height. Ulus Travma Acil Cerr Derg, November 2103, 19(6):529-535 doi:10.5505/tjtes.2013.77535
Isenschmid, D.S. (2002), Cocaine – Effects on human performance and behavior. Forensic Science Review, 14:61; 2002.
Liu, C.-C., Wang, C.-Y., Shih, H.-C., Wen, Y.-S., Wu, J.-K., Huang, C.-I., . . . Huang, M.-S. (2009). Prognostic factors for mortality following falls from height. Injury – International Journal of the Care of the Injured, 40, 595-597.
Nau, C., Leiblein, M., Verboket, R.D., Hörauf, J.A., Sturm, R., & Marzi, I. (2021). Falls from Great Heights: Risk to Sustain Severe Thoracic and Pelvic Injuries Increases with Height of the Fall. Journal of Clinical Medicine, 10(2307):1-9. doi:https://doi.org/10.3390/jcm10112307
Papdimitriou-Olivgeris, M., Panteli, E., Koutsileou, K., Boulovana, M., Zotou, A., Marangos, M., Fligou, F. (2021). Predictors of mortality of trauma patients admitted to the ICU: a retrospective observational study. Brazilian Journal of Anesthesiology. 71:23-30.
Reason, J., 1998. Achieving a safe culture: theory and practice. Work & Stress, 12(3), pp. 293-306.
Safety Management International Collaboration Group (2019) Industry safety culture evaluation tool and guidance, https://www.skybrary.aero/enhancing-safety/sm-icg-safety-management-products, SM ICG, accessed 22 December 2022.
Shehab, R.L., Schlegel, R.E., and Palmerton, D.A., (1998). A human factors perspective on human external loads, The university of Oklahoma and FAA Civil Aeromedical Institute. Federal Aviation Administration. DOT/FAA/AM-98/13
Snyder, R.G. (1963). Human survivability of extreme impacts in free-fall. Civil Aeromedical Research Institute, Aeromedical Research Division. Oklahoma City: Federal Aviation Administration.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- pilot of VH-IDW
- helicopter operator
- helicopter maintainer
- helicopter manufacturer
- helicopter engine manufacturer
- Civil Aviation Safety Authority
- United States National Transportation Safety Board
- Wild Harvest Northern Territory
- emergency responders
- other people involved in the egg collection operation
- various subject matter experts.
Submissions were received from:
- pilot of VH-IDW
- helicopter operator
- helicopter maintainer
- helicopter manufacturer
- Civil Aviation Safety Authority
- Wild Harvest Northern Territory
- emergency responders
- other people involved in the egg collection operation
- various subject matter experts.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Fuel analysis
Initial fuel analysis
The ATSB drained the remaining fuel from VH-IDW after it was relocated to a hangar in Darwin. The observed blue colour of the fuel was consistent with 100 low-lead (LL) fuel. The fuel was stored in an unsealed container overnight resulting in some evaporation. The remaining 235 mL of fuel was sent to Intertek for testing to determine the fuel type. The initial tests requested were for fuel density and aromatics as these are key distinguishing properties between fuel types.
The density of the VH-IDW sample was 729.1 kg/m3 and contained 11.8 % v/v aromatics, see column 4 in Table 5.
The ATSB then obtained the invoices, fuel release notes and certificates of quality for the 100/130 Avgas fuel drums delivered to Mount Borradaile and the 2 most recent (prior to the accident day) batches of 100 LL Avgas delivered to the storage tank at Helibrook’s Noonamah base. In a submission provided following review of the ATSB draft report, Helibrook advised that VH‑IDW had been filled the night before the accident from its base at Sweets Lagoon, which also had 100 LL fuel. Fuel receipts showed 100 LL Avgas with batch density 718.3 kg/m3.
The fuel batch delivered in the drums to Mount Borradaile was green, had a density of 693.7 kg/m3 and 0.7% v/v aromatics, see column 3 in Table 5. The 100 LL fuel delivered to the Noonamah tank was blue, had a density of 715.4 and aromatics of about 15%, based on certificates of quality of recent fuel batches delivered to Darwin Port, see column 2 in Table 5.
The ATSB arranged for samples to be taken from 4 WHNT drums at Mount Borradaile, including the 2 identified as the drums used to refuel the R44 helicopters on the accident day. The first drum rolled out on the day was reportedly not full and its density was slightly higher than the batch testing as shown in column 5 of Table 5. The second drum closely matched the delivered batch results.
The initial comparison between the VH-IDW sample and 100 LL fuel indicated that the sample was consistent with partially evaporated 100 LL fuel. However, it was postulated that the reduction in aromatics could also result from a mixing of 100 LL and 100/130 fuel.
To determine whether the VH-IDW sample contained a proportion of 100/130 fuel, or any other fuel type, the ATSB liaised with 2 fuel experts – one from Viva energy, involved in the supply of the 100 LL Avgas, and the other in distribution of the 100/130 Avgas. The Viva expert suggested the ATSB request a distillation of the VH-IDW sample. The distillation process separates the sample into its component hydrocarbons. The sample would be heated then put into a distillation column where different products boil off at different temperatures. However, insufficient fuel remained from the VH-IDW sample to conduct that test. As an alternative, the Viva expert recommended conducting a simulated distillation, which only uses a very small quantity of fuel.
Intertek conducted the simulated distillation, which involved using a method for crude oil, with the results shown in column 4 of Table 5. The final boiling point obtained for the VH-IDW sample was significantly higher than the values stated in the certificates of quality for the batches of 100 LL and 100/130 fuels, and that obtained by using the normal fuel distillation method on the Mount Borradaile sample, all shown in row 9 of Table 5.
Table 5: Initial fuel test results
| Tested property | 100 LL delivered batch | 100/130 delivered batch | VH-IDW sample | Mount Borradaile sample 4 |
|---|---|---|---|---|
| Density @15 °C kg/m3 | 715.4 | 693.7 | 729.1 | 704.5 |
| Aromatics %v/v | Est. 15% | 0.7 | 11.8 | N/A |
| Colour | blue | green | blue | green |
| Distillation Initial boiling point °C | 38 | 36 | 58* | 43 |
| Distillation 10% °C | 72 | 54 | 99* | 85 |
| Distillation 50% °C | 102 | 102 | 112* | 105 |
| Distillation 90% °C | 112 | 112 | 124* | 113 |
| Distillation final boiling point °C | 139 | 131 | 188 | 130 |
| Tetraethyl lead g-Pb/L | 0.39 | 0.732 | Inconsistent** | N/A |
* Distillation for VH-IDW was done with incorrect method (used for crude oils not Avgas)
** Different TEL g-Pb/L values were obtained with 3 separate tests
The ATSB again consulted the Viva expert to understand the implications of the high final boiling point. They advised that, among other fuels, Jet A1 (kerosene) and unleaded car petrol have higher final boiling points than Avgas. This prompted further testing to determine whether the VH‑IDW sample was contaminated with another fuel type.
The Viva expert then liaised with Intertek on the ATSB’s behalf to conduct a gas chromatography test to analyse the hydrocarbons and compare the VH-IDW sample with Jet A1, unleaded petrol and 100 LL Avgas. They advised that the chromatogram of VH-IDW showed no traces of Jet A1, or unleaded petrol, but was consistent with partial evaporation of 100 LL Avgas. While this ruled out contamination with an unsuitable fuel type, it did not enable a determination of whether the VH‑IDW sample contained a significant proportion of 100/130 fuel.
As the lead content of 100/130 fuel is nearly twice that of the 100 LL, the Viva expert recommended that ATSB request Intertek conduct testing of the tetraethyl lead (TEL) content of the VH-IDW sample. The first test of the VH-IDW sample resulted in a value (1.370 g-Pb/L) which exceeded the test method upper limit of detection of > 1.3 g-Pb/L. Consequently, the ATSB requested Intertek retest the sample. Intertek conducted 2 subsequent tests of the VH-IDW sample and obtained values of 0.969 and 0.558 g-Pb/L.
Intertek was unsure why the results were inconsistent, and their final report stated they were unable to report a value due to the lack of a consistent result. Additionally, Intertek advised the ATSB that following the third TEL test, the colour of the VH-IDW fuel sample unexpectedly turned from blue to yellow-green. The ATSB then engaged the Defence Science and Technology Group (DSTG) for independent expert advice and provided all remaining fuel samples to DSTG.
The Viva expert’s assessment of the test results was that the VH-IDW sample was consistent with 100 LL Avgas that had undergone significant evaporation of the lighter boiling components. They assessed that there was no kerosene or road grade petrol in the sample. Based on the colour, prior to the sample turning yellow-green, they assessed that there was no more than 5% v/v of 100/130 fuel in the VH-IDW sample.
Defence Science and Technology Group analysis
Gas chromatography with mass spectrometry
DSTG conducted gas chromatography with mass spectrometry (GC-MS) analysis of the VH-IDW fuel and samples of blue 100 LL and green 100/130 Avgas fuel. The 3 resulting GC-MS traces were overlaid on each other for comparison. This showed that the VH‑IDW sample was missing, or had a very low concentration of, low boiling point compounds, consistent with evaporation. The DSTG report referenced a study performed by Canada’s Environmental agency, which found that a 33% evaporation of Avgas 100 LL resulted in a density change from 714.3 to 725.8 kg/m3 (CETC, 2022). Additionally, evaporation skews results such as distillation profile, TEL and total aromatics content. The evaporation skewed the trace for VH‑IDW towards the heavier side, exaggerating those peaks, including the peak for TEL. Tetraethyl lead was readily identified by DSTG using GC-MS, which showed a high concentration that could be attributed to evaporation and/or residual elements in the fuel tank.
The VH-IDW trace was more consistent with 100 LL than 100/130 fuel, although some extremely low concentrations overlapped with 100/130. This suggested that remnant fuel from previous days may have been detected in the GC-MS analysis. A comparison of the VH-IDW sample with the Mount Borradaile drum sample showed distinct differences in the GC-MC traces, and the VH-IDW sample had a significant number of peaks found only in 100 LL Avgas.
Ultraviolet-visible spectroscopy
The VH-IDW sample was blue when drained from the fuel bladder by the ATSB and when it arrived at Intertek. Following testing for TEL at Intertek, it turned a yellow-green colour. On arrival at DSTG, they described the VH-IDW sample as visually a deeper yellow-green than the 100/130 Avgas sample from Mount Borradaile and lacked the blue that was observed by ATSB investigators. DSTG therefore conducted ultraviolet-visible (UV-Vis) spectroscopy to compare VH‑IDW sample with 100 LL and 100/130 Avgas and, if possible, determine the source of the colour change.
Dyes were isolated using solid phase extraction and evaporated then dissolved in heptane prior to analysis. The UV-Vis spectra of the VH-IDW sample found blue dyes common to the Avgas 100 LL and 100/130 (batch and Mount Borradaile) samples. However, the VH-IDW sample did not contain a yellow dye found in the 100/130 samples. The absence of the yellow dye indicated 100/130 Avgas was not present in the VH-IDW sample at any significant concentration. DSTG subsequently assessed that there was likely less than 1% of 100/130 fuel in the VH-IDW sample.
The compounds contributing to the yellow-green colour were not in 100 LL or 100/130 Avgas and were not attributed to an approved yellow Avgas fuel dye. Further analysis to determine the likely source of the colour was ongoing at the time of the publication of this report.
Findings
The DSTG report found that the VH-IDW sample was consistent with Avgas 100 LL that had partially evaporated. The GC-MS trace of the VH-IDW sample significantly overlapped with the 100 LL sample. The UV-Vis spectra absorptions of the VH-IDW sample closely matched the dye for 100 LL Avgas. The 100/130 levels in the VH-IDW sample were assessed as trace volumes, subsequently approximated at less than 1% of otherwise 100 LL fuel. This was evidence that there was no refuelling of VH-IDW with 100/130 prior to the accident.
There was no evidence of Opal, premium 98 petrol, diesel or Jet A-1 fuel in the VH-IDW sample. The distillation method used by Intertek, although undertaken due to the small available volume of fuel, was for crude oil and not valid for other fuels. Consequently, the resultant high final boiling point was consistent with an incorrect test method rather than an accurate representation of the distillation profile.
At the time of writing, the nature of the colour contamination that occurred at Intertek was still under investigation.

Appendix C – HEC height, speed and distance/time conditions 2010–2021
| Year | Height | Speed | Distance/time |
|---|---|---|---|
| 2010-2013 | The person is not lifted to a height of greater than 5 metres above the ground or obstacles | The aircraft is not flown at a ground speed greater than walking pace when the person is carried under the helicopter | The maximum distance the person is carried under the helicopter is 500 metres for each pick up |
| 2014-2015 | The person is not lifted to a height of greater than 5 metres above the ground or water. To remove doubt, this instrument does not permit lifting of a person to a height greater than 5 metres above an obstacle. The height restriction is in reference to the ground or water in all instances | The aircraft is to be flown at speed that is consider by the pilot in command to be a safe speed, taking into consideration the prevailing wind direction, wind speed, and aircraft performance when the person is carried under the helicopter. Minimisation of injury to the person in the event of hook release (whether planned or inadvertent release) must be considered in the context of the total forward speed of the person over the ground | The maximum distance the person is carried under the helicopter is 500 metres for each pick up |
| 2016 | The person is only to be lifted to a height above the ground or water that enables the person and aircraft to safely traverse over natural obstacles. In all other instances, the person is not to be lifted more than 5 metres above the ground or water. Minimisation of injury to the person in the event of hook release (whether planned or inadvertent release) must be considered in the context of the height the aircraft is operated above the ground or water at any particular time | The aircraft is to be flown at speed that is consider by the pilot in command to be a safe speed, taking into consideration the prevailing wind direction, wind speed, and aircraft performance when the person is carried under the helicopter. Minimisation of injury to the person in the event of hook release (whether planned or inadvertent release) must be considered in the context of the total forward speed of the person over the ground | The person is only to be carried for the minimum distance and time required in order to safely conduct the activity, taking the possible effects of suspension trauma on the person into consideration. To avoid any ambiguity, the intent of this condition is that the person is not to be carried for the purpose of positioning flights over landing sites where it would be possible to conduct the safe donning or removal of the person from the strop used to carry the person |
| 2017-2021 | N/A | The aircraft is to be flown at a speed that is considered by the pilot in command to be a safe speed, taking into consideration the prevailing wind direction, wind speed, and aircraft performance when the person is carried under the helicopter | The person is only to be carried for the minimum distance and time required in order to safely conduct the activity, taking the possible effects of suspension trauma on the person into consideration. To avoid any ambiguity, the intent of this condition is that the person is not to be carried for the purpose of positioning flights over landing sites where it would be possible to conduct the safe donning or removal of the person from the strop used to carry the person |
Appendix D – Instrument conditions
Instrument conditions – CASA.CARRY.0163 Revision No: 1 (Helibrook)
This instrument is subject to the condition that the pilot in command and the operator must each ensure that:
1. The flying operations for the purpose of the activity are only done so utilising the Robinson Helicopter Company R44 helicopter type and only where the person and pilot in command both determine there is an overall safety advantage to the operation by reducing the risk of crocodile attack and heat exhaustion to the person; and
2. Persons other than crew members essential to the activity are not carried; and
3. Life jackets are worn by all crew members for all flights where the takeoff, positioning flights or approach path is so disposed that, in the event of a mishap occurring during operations, it is reasonably possible that the aircraft would be forced to land onto water; and
4. The pilot in command and the person have successfully completed a course of training for the activity promulgated in the operator’s operations manual which includes not less than 1 hour of actual flight time and 1 hour of ground instructional time; and
5. All crew, including the person being slung, have been inducted into the operator’s organisation, and have been included in the operator’s Drug and Alcohol Management Plan requirements; and
6. No pilot shall undertake the activity unless he or she has a minimum of 100 hours experience in helicopter external sling load operations; and
7. Only one person is carried below the aircraft at any one time; and
8. The chief pilot has personally authorised the flight program for the day associated with operations under this instrument; and
9. A thorough preflight briefing specifically related to each flight is conducted by the pilot in command to all personnel associated with the particular flight and is to include actions to be taken by crew members during possible emergencies encountered during the activity. The briefing is to be in accordance with, but not limited to, the activity briefing procedures promulgated in the operator’s operations manual; and
10. The pilot in command has continuous and clear radio communications with the person throughout the activity; and
11. The aircraft is to be flown at a speed that is considered by the pilot in command to be a safe speed, taking into consideration the prevailing wind direction, wind speed, and aircraft performance when the person is carried under the helicopter; and
12. Wind conditions, including wind gusts, for the area of proposed operation, must not exceed 15 knots; and
13. Operations not to be conducted within 5 kilometres of thunderstorm activity or observed lightning strikes. Should thunderstorm activity or lightning strikes be observed, activities under this instrument are to be terminated as soon as safely possible; and
14. The person is only to be carried for the minimum distance and time required in order to safely conduct the activity, taking the possible effects of suspension trauma on the person into consideration. To avoid any ambiguity, the intent of this condition is that the person is not to be carried for the purpose of positioning flights over landing sites where it would be possible to conduct the safe donning or removal of the person from the strop used to carry the person; and
15. The person wears a helmet that meets the Australian standard appropriate to the risks encountered during the activity; and
16. The person must wear an Australian Standard harness (designed for lifting a person) connecting them to the strop at all times during flight to and from the crocodile egg collection site. The person may be released from the strop during the actual process of crocodile egg collection; and
17. The person carries a readily accessible harness knife capable of cutting the lifting strop or harness in an emergency; and
18. All legislative requirements pertaining to the conduct of sling load operations are complied with; and
19. All normal and emergency equipment utilised for the conduct of the activity are serviceable; and
20. The helicopter carries a portable satellite phone with all crew members trained in its use; and
21. The person carries, and is trained to activate, a portable emergency location transmitter; and
22. Prior to the approval of CASA STC SVR 541, the aircraft must have been modified in accordance with, and remain compliant with, Engineering Order (EO) TDE5106-04-R2, dated 12/12/17 or later approved revision.
23. When CASA STC SVR 541 is approved, all aircraft previously certified to the EO will be shown to be compliant with and certified to the STC within fourteen (14) days of the STC being approved, after which time aircraft certified only to the EO may no longer undertake this work. Further aircraft to be used after the STC approval date will only be certified in accordance with the STC; and
24. Aircraft approved under EO TDE5106-04-R2 or later approved revision are to have the HEC Lines and harnesses installed and maintained in accordance with the EO approved data; and
25. Aircraft approved under STC SVR 541 are to have the HEC Lines and harnesses installed and maintained in accordance with the STC approved data; and
26. Other hook down equipment, such as collection basket/cages, helmets and other things will be determined by the Operator as being fit for purpose and meeting any required workplace or industrial standard; and
27. Aircraft operated under the EO TDE5106-04-R2 or later approved revision, are to be operated in accordance with an approved aircraft flight manual supplement R5106-101-R2 or later approved revision which details normal and emergency procedures associated with the activity; and
28. Aircraft operated under STC SVR 541 are to be operated in accordance with an approved aircraft flight manual supplement R5106-25-R9 or later approved revision which details normal and emergency procedures associated with the activity; and
29. The daily inspection schedule for each aircraft utilised for the activity incorporates detailed requirements for the inspection of any component, part or system utilised as part of human sling load operations; and
30. Prior to the commencement of the activity each day, the pilot in command has verified the aircraft engine is producing normal rated power output, and that no defects are evident which could lead to power reduction during those operations; and
31. Only persons employed or contracted for the purposes of the activity are carried. To avoid any ambiguity, this instrument does not permit persons who have provided consideration of any nature to any party to conduct egg collection activities or to be slung from the aircraft involved in such activities; and
32. The person must be provided with a copy of this instrument and must be made aware, in writing, that the hook system is not certified for human use; and
33. The operator and the pilot in command must comply with all applicable instructions relating to the activity contained within the operator’s operations manual. The operator must not, without the prior written consent of CASA, revise any part of its operations manual relating to the authorisation and permission given under this instrument.
Any breach of the conditions of this instrument will result in the instrument being immediately cancelled by CASA.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Long lines are lightweight, high‑strength, low‑stretch ropes used for carrying loads underneath a helicopter.
[2] Refuelling conducted while the engine(s) are operating and the rotors are turning.
[3] OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[4] Loss of coordination of the muscles, especially of the extremities (Macquarie Dictionary).
[5] Safe work method statement (SWMS): a document that sets out high risk activities, the hazards associated with the activities and measures required to be in place to control the risks to an acceptable level.
[6] Normal category rotorcraft have a maximum take-off weight (MTOW) up to 3,175 kg and up to 9 passenger seats.
[7] Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[8] Manoeuvring with low fuel levels can result in fuel flowing away from the fuel tank outlet, or port, to the engine. This disrupts the engine fuel supply, resulting in power fluctuations and/or engine stoppage.
[9] Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[10] A supplemental type certificate (STC) is a type certificate (TC) issued when an applicant has received regulatory approval to modify an aeronautical product from its original design. The STC, which incorporates by reference the related TC, approves not only the modification but also how that modification affects the original design.
[11] The primary hook could be used for non-human cargo lifting operations and, as such, could accrue more operational hours than the secondary hook (required for HEC operations).
[12] QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
[13] The altitude in the International Standard Atmosphere at which a given air density is found.
[14] B nut - threaded sleeve nut that provides clamping force to ensure an effective/good seal to fuel, air and oil lines.
[15] Due to engine installation orientation, the engine right magneto is located on the left side of the helicopter. Further, the engine right magneto contains a second set of points that provided a signal to the governor and engine tachometer.
[16] The lead content of 100/130 is about 0.732 g Pb/L and the lead content of 100 LL fuel is approximately 0.38 g Pb/L.
[17] Out of ground effect: helicopters require less power to hover when in ‘ground effect’ than when out of ‘ground effect’ due to the cushioning effect created by the main rotor downwash striking the ground. The height of ‘ground effect’ is usually defined as more than one main rotor diameter above the surface.
[18] The Pilot’s Operating Handbook (POH) incorporates the US Federal Aviation Administration-approved Rotorcraft Flight Manual.
[19] Autorotation is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
[20] This was CASR 11.055 (1)(d) in 2010 and CASR 11.055 (1A)(e) in 2013, but the wording is the same in both.
[21] Equivalent level of safety means an alternative action taken provides a level of safety equal to that provided by the requirements for which equivalency is being sought.
[22] The parachute landing fall is used to spread the forces of impact across various parts of the body to reduce the risk of injury. The landing position is with the knees slightly bent and feet together. The feet and toes contact the ground first, followed by a sideways roll onto the legs and torso then the back. (ParachutingInjuries_FS_12-006-1115.pdf (army.mil))
[23] A Failure Modes and Effects Analysis is a systematic method of identifying the failure modes and the failure outcome. The assessment may be quantitative or qualitative.
[24] Part 138 MOS definition: Class D external load means a load that is a person, carried external to the rotorcraft, by a rotorcraft in an external load operation.
[25] EASA-OPS Part CAT AMC1 CAT.POL.H.305(b)
[26] Transport Safety Investigation Regulation 2.4 (2)(e) and (2)(f)(i) specified that these occurrences were required to be reported if they occurred when the aircraft was boarded for flight and it involved the use of any procedure for overcoming an emergency or resulted in difficulty controlling the aircraft.
[27] Haemopneumothorax is the condition of having air and blood in the chest cavity.
[28] Subarachnoid haemorrhage is bleeding in the space that surrounds the brain.

