
Executive summary
What happened
On the morning of 23 February 2022, a Piper Aircraft Corporation PA-25-235/A9, registered VH‑SEH, was conducting agricultural spreading operations from a private landing area located near Seaview, Victoria. At 0711, the pilot commenced take-off for the first load of the day. The aircraft accelerated along the prepared strip and briefly became airborne. The outboard section of the aircraft’s left wing impacted trees and detached from the aircraft. The aircraft rolled to the left, pitched down, and collided with terrain. The pilot, who was the sole occupant, was fatally injured and the aircraft was destroyed.
What the ATSB found
The ATSB found that the take-off was attempted at an aircraft weight that likely did not permit sufficient performance to clear the trees at the end of the strip. Although the pilot had conducted take-offs using the Seaview runway strip in previous years, the increased height of trees at the northern end of the strip were found to have reduced safety margins to some extent.
It was also identified that engine power during take-off may have been slightly lower than normal. This may have been due to the water content of the air, carburettor ice, or the carburettor heat selector may have been inadvertently left on during the take-off. However, a conclusion regarding the existence of these scenarios could not be drawn with any certainty.
The ATSB also found that the pilot likely initiated a jettison of the hopper contents shortly after becoming airborne, but any effect this had on the aircraft’s performance was probably negligible.
Safety message
Aircraft operators and pilots are reminded of the hazards associated with operations from small landing areas that are not prepared as permanent runways. In any case, pilots should ensure aircraft loads are within specified limits, appropriate for the environmental conditions, and will result in the required performance to maintain safety margins.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On 23 February 2022 at about 0650 local time, the pilot of a Piper Aircraft Corporation PA-25-235/A9, registered VH-SEH, departed Leongatha Aerodrome, Victoria, for a positioning flight to a private landing area[1] situated 25 km to the north in the locality of Seaview. The aircraft was reportedly carrying full fuel (170 L) prior to take-off.
The aircraft landed at about 0700 in preparation for the aerial spreading of superphosphate pellets. The pilot had been tasked to spread 41,000 kg of superphosphate fertiliser at 6 nearby properties. It was anticipated this would take about 80 loads and 8 hours to complete.
The loader driver[2] for the day’s activities arrived at the Seaview landing area at about 0705. On arrival, the loader driver found VH‑SEH parked with the engine stopped and the pilot out of the aircraft. The pilot had filled the loader’s bucket with superphosphate prior to the arrival of the loader driver.
The loader driver and the pilot had a short conversation and the pilot returned to the aircraft. The loader driver transferred the superphosphate to the aircraft’s hopper with the pilot on board the aircraft. The loader driver could not see how much superphosphate had been loaded into the bucket, and the weighing system in the loader only indicated weight at the time of filling the bucket.
The loader driver then parked the loader at the southern end of the landing area and prepared for the next load. A short time later, the pilot started the aircraft’s engine and remained at the southernmost point of the landing area for about 5 minutes.
Based on local weather observations and a witness’s video recording of the take-off, the weather at the time of the accident was fine with the wind likely calm. The loader driver described the weather conditions at the time as good.
According to witness reports, the pilot was wearing a 4-point harness and a helmet. Data from an onboard GPS device showed that the pilot commenced the take-off on the prepared runway strip at about 0711 (Figure 1).
The runway strip went downhill, and then uphill, where it branched into 2 sections. According to the 2 witnesses and the recorded video, the aircraft accelerated along the strip and traversed the right section where the strip divided.
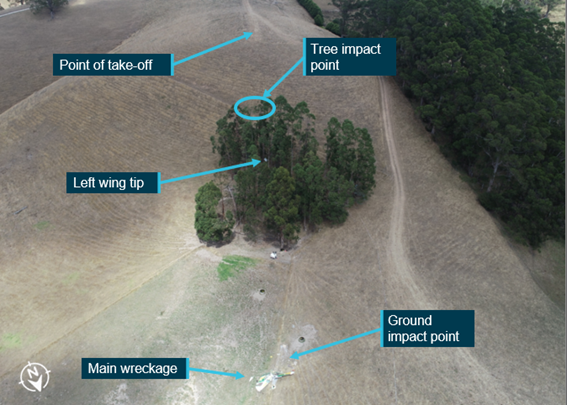
The aircraft briefly became airborne at a point at the end of the strip where the terrain dropped away. The outboard section of the aircraft’s left wing then impacted trees and separated the left outboard section of wing. The aircraft rolled to the left, pitched down, and collided with terrain about 30 m beyond the trees (Figure 2). The pilot was fatally injured and the aircraft was destroyed.
Figure 1: Runway strip overview

Source: ATSB
Figure 2: End of runway strip and impact points
Context
Pilot information
The pilot held a valid class 1 aviation medical certificate and a commercial pilot licence (aeroplane), having completed a flight review and an aerial application proficiency check on 11 November 2021. At the time of the accident, the pilot had about 12,350 hours total aeronautical experience. The pilot was the owner and chief pilot of the aerial work operator, which conducted mostly aerial application activities.
The pilot was reported to be fit and healthy and there was no indication they were experiencing a level of fatigue known to affect performance. The post-mortem and toxicology examinations did not identify any indicators of incapacitation or substances that could have affected the pilot’s capacity to perform the flight.
Aircraft information
General information
The aircraft was a 2-seat Piper Pawnee PA-25-235/A9 with a 6-cylinder, normally aspirated Textron Lycoming O-540-H2A5 engine driving a 2-blade McCauley Propellers 1A200/FA8452 fixed-pitch propeller (Figure 3). This propeller was designed for increased efficiency during cruise compared with other propeller options, but also resulted in decreased climb performance and increased the take-off distance required. The propeller was first installed on the aircraft in March 2019.
Figure 3: A similar Piper PA-25-235/A9 configured for agricultural spreading

Source: ATSB
The aircraft was originally manufactured as a single-seat PA-25-235 in 1974. In 1988, the aircraft was involved in an accident while conducting herbicide spraying near Deddick Park, Victoria. The outboard section of the right wing collided with a tree. The aircraft climbed steeply then descended in a nose-down attitude and impacted terrain.[3]
In 1989, the aircraft was rebuilt and converted to an ‘A9’ variant. This conversion included the installation of a second seat (in a side-by-side configuration), replacement of the fabric-covered wings with metal wings, the installation of a larger chemical hopper, and the fitment of a larger Lycoming O-540-H2A5 engine. Flying controls were on the left side.
The engine was last overhauled in March 2021, and the last periodic inspection was carried out in July 2021 with no defects recorded. At the time of the accident, the aircraft had accumulated 9,543.5 hours total time in service, and the engine had accumulated 159 hours since overhaul.
Aircraft hopper
The hopper was located between the instrument panel and the engine firewall. It was constructed from fiberglass and had a 544 kg maximum permissible load. Its volume (200 gallons, or 757 L) was sufficient to hold up to about 800 kg of superphosphate pellets. There was a clear section in the cockpit, with graduations in gallons, to enable the pilot to see how much volume of product was in the hopper.
The quantity of superphosphate on board the aircraft during the take-off could not be determined. Those familiar with the recent operating practices of the pilot of the accident flight reported that, if weather and strip surface conditions were favourable, it was normal for the pilot to take a full load of superphosphate on the first flight from a landing area. Otherwise, the pilot would normally opt to take a reduced load on a first flight. A typical reduced load for this pilot was reported as being about 400 kg.
The aircraft was fitted with an emergency hopper dump mechanism. The mechanism allowed a pilot to dump all or part of the hopper contents if the aircraft did not achieve the required performance. To do so, the pilot would push a button on the spread/dump lever (to enable the lever to move past a gate) and move the lever past the spread selection to the full forward position. This would fully open the hopper door located on the underside of the aircraft fuselage. A full load of superphosphate was expected to completely jettison in about 4 seconds. Dumping the hopper load would significantly, and almost immediately, reduce the aircraft’s weight and increase performance.
The total elapsed time from the aircraft becoming airborne to impacting the trees was 2 seconds.
Performance
The approved flight manual for VH‑SEH contained take-off performance charts that could be applied to calculate a performance-limited maximum take-off weight using aircraft and environmental parameters for a given flight. These charts included a wet or dry surface and long or short grass. Such charts had reduced applicability for landing areas with significant changes in slope, and rough surface conditions were not captured by the charts. The aircraft operator’s operations manual (OM) contained the responsibilities for company pilots. The OM stated:
In determining that an operation can be conducted safely, the pilot will consider:
a) carriage of heavier than manufacturers’ recommended weights
b) strip length and conditions, particularly in relationship to the performance parameters of the particular aircraft used by the Company
c) strip altitude and density altitude
d) wind speed and direction, especially any downwind component
e) obstacles
The OM also stated:
Pilots are responsible for the safety of the aircraft. Many accidents have loading as a causal factor. That is, the aircraft may have flown off the same landing area with the same load but slightly different environmental conditions. The decision to dump a load may be relatively cheap when compared to repairing an aircraft. The ability to dump the load is the last line of defence in the accident chain but it remains a very good defence and should be used as required. Pilots should make a conscious decision on each take off about how much load they will take and at what stage they will either abort take-off or dump the load in the event that the aircraft fails to become airborne at the expected time. To make this decision, pilots should have firmly in their mind where the aircraft should get airborne.
The ATSB undertook performance calculations using known and estimated aircraft and environmental information, including fuel and hopper loads. It was estimated that the aircraft was probably near the performance-limited maximum take-off weight for a level (no slope) strip the same length as the actual strip, without any load in the hopper. Using an estimated weight range for the hopper load of 400–544 kg, the aircraft would have been over the performance-limited maximum take-off weight for an equivalent-length level strip. This range of hopper loads would have resulted in a take-off weight of about 1,400–1,544 kg. The aircraft’s maximum take-off weight was 1,315 kg.
Carburettor heat
Carburettor icing occurs when water vapour freezes within an engine’s carburettor due to a decrease in temperature and pressure within the carburettor. The likelihood of carburettor icing increases with humidity and at partial power settings (for example, when idling). If ice accumulates within a carburettor, the flow of air to the engine (and, ultimately, available power) reduces.
A carburettor heat control was available in VH‑SEH. When selected, warm air was directed from a heat exchanger on the exhaust system to the carburettor inlet, melting any ice in the carburettor. The operator’s other pilots reported that it was standard practice to apply carburettor heat during ground operations, selecting it off just prior to commencing the take-off. The purpose of this practice was to prevent carburettor ice build-up during engine idling.
It was reported that the application of carburettor heat in VH‑SEH would result in a propeller speed reduction of about 100 RPM and, if inadvertently left on during take-off, would significantly increase the take-off distance required. Due to the level of damage, the ATSB could not determine the position of the carburettor heat control at the time of the accident or whether carburettor icing occurred during the take-off.
Water vapour and engine performance
High concentrations of water vapour within the air (a high relative humidity) can impact engine performance. The water vapour alters the fuel to air ratio, causing enrichment, as well as reducing the burning and cooling efficacy of the engine. This reduces the power output of engine and may increase the take-off distance required. The ATSB could not determine the relative humidity at the landing area at the time of the accident (see also Weather information).
Runway strip
The runway strip at Seaview was prepared annually for aerial agricultural operations by the operator of VH‑SEH. The prepared strip had been mowed into a ‘Y’ configuration by the pilot of the accident flight in the days before the accident. It consisted of mowed grass and the surface was hard and rough from previous cattle movements. The strip was at an elevation of about 1,100 ft above mean sea level (AMSL) and each branch provided about 360 m take-off and landing distance on the ground.
Take-offs were always conducted in the same direction due to the more downwards slope. In this direction, the strip followed the natural terrain, with a downwards then upwards slope before dropping steeply towards the stand of trees. The left branch was oriented to the left of the trees and the right branch was oriented directly towards the trees (Figure 4).
Figure 4: Runway strip ‘Y’ intersection showing the left and right branches with the trees at the runway’s end

Source: ATSB
The pilot had not operated from this strip for at least 2 years prior to the accident. It was reported that the trees at the end of the strip had grown about 3–10 ft during that time. The pilot was reportedly aware of the hazard presented by the trees, having commented on their growth over the years. In the days prior to the accident, the pilot had communicated their intent to use the right side of the prepared strip for the day’s operations. Another of the operator’s pilots reported preferring the left branch of the strip in order to avoid the trees. The reasons for the accident pilot’s preferred use of the right branch could not be determined.
Site and wreckage
The wreckage was located about 30 m north of the stand of trees at the northernmost end of the strip. The trees were about 90 ft in height above ground level (AGL). Damage to the trees indicated the left wing impacted the trees at a height of about 74 ft AGL. Examination of the accident site indicated the aircraft impacted the ground inverted with an angle of entry of about 50° with the left wing low, and came to rest about 8 m from the initial impact point. The cabin sustained significant damage (Figure 5). Significant curved compression damage was evident on the leading edge of the left wing consistent with tree impact damage (Figure 6).
Figure 5: Aircraft wreckage

Source: ATSB
Figure 6: Outboard section of left wing with tree impact damage

Source: ATSB
The hopper door was open, and superphosphate had spilled from the hopper with most in the vicinity of the fuselage. Superphosphate was also found in smaller quantities near the initial impact point with the trees and scattered from halfway between the aircraft’s point of take-off to the wreckage site. The scattered pellets were consistent with a pilot-initiated release (and not post-impact scatter); however, it could not be determined if the mechanism had been activated in the spread or emergency dump position. The position of the spread/dump lever at the time of impact could not be determined.
Examination of the propeller, along with ground marks, indicated the propeller was rotating under power at the time of impact.
External examination of the engine did not identify any obvious defects. The engine tachometer displayed a needle ‘slap mark’[4] indicating about 2,240 RPM.[5] The throttle position at the time of impact could not be determined due to disruption of the controls.
There were no evident pre-impact defects with the aircraft structure and flight control continuity was confirmed as far as possible. The flap handle was in the top notch, indicating full flap. The operator’s other pilots reported that it was normal practice to apply full flap at the lift-off point, followed by a gradual reduction of flap setting as the aircraft climbed away.
ATSB analysis (based on estimates of the aircraft’s speed, impact angle and damage to the aircraft) indicated the impact forces for this type of accident would normally be expected to result in fatal injuries irrespective of any safety equipment worn.
Weather information
Recorded meteorological data for the landing area was not available. The weather conditions captured on the video recording made by a nearby witness included no cloud, visibility greater than 10 km and wind calm.
At the time of take-off, there was no fog at the landing area, there was a layer of fog in a nearby valley below the landing area. Given the proximity of the fog (saturated airmass), it indicates that conditions conducive with reduced engine performance and/or carburettor icing may have been present at the landing area. Recorded information
Accident video
The video recording captured by the witness was 30 seconds in length and commenced 6 seconds prior to the initiation of the take-off roll, ceasing 1 second after the aircraft impacted trees. No anomalies were evident in engine sound recorded on the video, such as rough running or power reduction during the take-off roll.
Audio spectrogram analysis of the video recording indicated that the aircraft’s propeller speed was likely about 2,357–2,587 RPM during the take-off roll, and this was maintained until the collision with the trees. The operator’s other pilots indicated that a typical propeller speed for VH‑SEH during take-off was about 2,500 RPM.
Global positioning system
A Tracmap Aviation TMA384 GPS device was recovered from the accident site and the stored data was downloaded. The data captured the aircraft’s arrival at the Seaview landing area, and the moments prior to take-off, but the device did not capture the subsequent take-off or the accident sequence. This was probably due to power supply disconnection during impact, preventing data being written to the memory card.
Safety analysis
The accident flight was the first load of the day and the aircraft had almost full fuel on board. Although the amount of superphosphate loaded onto the aircraft could not be determined, it was likely that the aircraft’s weight exceeded the performance-limited maximum take-off weight for the strip as well as the aircraft’s documented maximum take-off weight. This likely degraded the aircraft’s take-off performance significantly and contributed to the aircraft being unable to clear the stand of trees downslope of the lift-off point.
Additionally, the tachometer slap mark and the audio spectrogram analysis of the video recording indicated the power generated by the engine during the take-off may have been slightly lower than normal. No obvious defects were identified with the engine and the propeller was rotating under power at the time of impact. The relative humidity at the time of take-off could not be established. However, it is possible the aircraft’s engine performance was negatively impacted by the volume of water present within the air, affected by carburettor ice, or the carburettor heat selector may have been inadvertently left on during the take-off. Although these scenarios could explain a reduced propeller speed, there was insufficient evidence available to determine whether these events took place.
Although the pilot had conducted take-offs using the Seaview runway strip in previous years, the increased height of trees at the northern end of the strip had reduced safety margins to some extent. The aircraft struck the trees about 16 ft from the top, which meant that even without their estimated 3–10 ft extra height, there would not have been sufficient clearance for a safe take-off.
The investigation was unable to determine why the pilot elected to prepare, and use, a strip orientated directly towards the trees when an alternate take-off option was available.
A limited number of superphosphate pellets were found scattered between the aircraft’s point of take-off and the location where the aircraft impacted the ground. This indicated the pilot likely attempted to jettison the hopper contents around the time of becoming airborne. However, the effect this jettison would have had on the aircraft’s performance was probably insufficient for it to clear the trees, given that it would have had to gain about 16 ft in 2 seconds with some of the load still on board.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision with terrain involving Piper PA-25, VH-SEH, near Seaview, Victoria, on 23 February 2022.
Contributing factors
- The take-off was attempted at an aircraft weight that did not permit sufficient performance to clear a stand of trees downslope of the lift-off point. As a result, the aircraft impacted the trees and collided with terrain.
Other factor that increased risk
- Although successful take-offs had been made using the prepared strip in previous years, the increased height of trees at the end of the strip reduced the safety margins over time.
Other findings
- The pilot likely attempted to jettison the hopper contents shortly after becoming airborne. However, the jettison would have only been partially completed by the time the aircraft collided with the trees, and there had probably been insufficient time for the aircraft to gain enough height to clear them in the intervening period.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- Bureau of Meteorology
- operator, 2 of the operator’s other pilots and loader driver
- Civil Aviation Safety Authority
- Victoria Police
- maintenance organisation
- witness and witness video.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the Civil Aviation Safety Authority
- the operator.
A submission was received from a party familiar with the operator’s activities. The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Landing area: a place, whether or not an aerodrome, where an aeroplane is able to take off and land.
[2] Loader driver: an operator of loading equipment to support aerial application operations.
[3] ATSB investigation 198801404, Piper PA25-235 (Pawnee), VH-SEH, "Deddick River" (24 km NE of Gelantipy) Victoria, 9 November 1988.
[4] Needle slap mark: an imprint made on the gauge face by the instrument’s needle at time of impact.
[5] The propeller speed prior to the aircraft impacting the terrain would have been higher than indicated by the slap mark due to the slowing of the engine during the impact sequence, as well as the angle of impact tending to push the needle left just before making the mark.





