
What happened
On the morning of 21 February 2017, the pilot of a Beechcraft B200 King Air aircraft, registered VH-ZCR was conducting a charter passenger flight from Essendon Airport, Victoria to King Island, Tasmania with four passengers on board.
The aircraft’s take-off roll was longer than expected and a yaw to the left was observed after rotation. The aircraft’s track began diverging to the left of the runway centreline before rotation and the divergence increased as the flight progressed. The aircraft entered a shallow climb followed by a substantial left sideslip with minimal roll. The aircraft then began to descend and the pilot transmitted a Mayday call. The aircraft subsequently collided with a building in the Bulla Road Precinct Retail Outlet Centre of Essendon Airport.
The aircraft was destroyed by the impact and post-impact fire, and all on board were fatally injured. The building was severely damaged and two people on the ground received minor injuries.
What the ATSB found
The ATSB found that the pilot did not detect that the aircraft’s rudder trim was in the full nose-left position prior to take-off. The position of the rudder trim resulted in a loss of directional control and had a significant impact on the aircraft’s climb performance in the latter part of the flight.
At the time of the accident, the operator did not have an appropriate flight check system in place for VH-ZCR. Although this did not contribute to this accident, it increased the risk of incorrect checklists being used, incorrect application of the aircraft's checklists, and checks related to supplemental equipment not being performed.
The aircraft’s cockpit voice recorder did not record the accident flight due to a tripped ‘impact switch’, which was not reset prior to the accident flight. This deprived the investigation of potentially valuable recorded information.
The ATSB determined that the aircraft was operated above its maximum take-off weight on the accident flight. This was not considered to have influenced the accident.
The ATSB also found that the presence of the building struck by the aircraft did not increase the severity of the consequences of this accident. In the absence of that building, the aircraft’s flight path would probably have resulted in an uncontrolled collision with a busy freeway, with the potential for increased ground casualties.
Although not contributing to this accident, the ATSB identified that two other buildings within the retail precinct exceeded the airport’s obstacle limitation surfaces. While those exceedances had been approved by the Civil Aviation Safety Authority, the ATSB identified several issues relating to the building approval process for the precinct.
What's been done as a result
It is beyond the scope of this investigation to consider in detail the issues identified with the Bulla Road Precinct building approval processes. These issues will be addressed in the current ATSB Safety Issues investigation The approval process for the Bulla Road Precinct Retail Outlet Centre AI-2018-010.
Safety message
Cockpit checklists are an essential tool for overcoming limitations with pilot memory, and ensuring that action items are completed in sequence and without omission. The improper or non-use of checklists has been cited as a factor in some aircraft accidents. Research has shown that this may occur for varying reasons and that experienced pilots are not immune to checklist errors. This accident highlights the critical importance of appropriately actioning and completing checklists.
This accident also emphasises the importance of having flight check systems in place that are applicable to specific aircraft in their current modification status. In addition, it emphasises:
- the value of cockpit voice recorders
- the significance of ensuring aircraft weight and balance limitations are not exceeded
- the challenges associated with decision-making in critical stages of a flight such as the take-off ground roll.
Beechcraft B200 King Air aircraft, registered VH-ZCR immediately prior to collision with a building in the Bulla Road Precinct

Source: Supplied
On 21 February 2017, the pilot of a Beechcraft B200 King Air aircraft, registered VH-ZCR (ZCR), and operated by Corporate & Leisure Aviation, was conducting a charter passenger flight from Essendon Airport,[1] Victoria to King Island, Tasmania. There were four passengers on board.
ZCR had been removed from a hangar and parked on the apron the previous afternoon in preparation for the flight (Figure 1). The pilot was first seen on the apron at about 0706 Eastern Daylight-saving Time.[2] Closed-circuit television (CCTV)[3] recorded the pilot walking around the aircraft and entering the cabin, consistent with conducting a pre-flight inspection of the aircraft.
Figure 1: Aircraft taxi and flight track from Airservices Australia ADS-B data

Source: Google, annotated by the ATSB
At about 0712, the pilot entered ZCR’s maintenance provider’s hangar. A member of staff working in the hangar reported that the pilot had a conversation with him that was unrelated to the accident flight. The pilot exited the hangar about 0715 and had a conversation with another member of staff who reported that their conversation was also unrelated to the accident flight.
The pilot then returned to ZCR, and over the next 4 minutes he was observed walking around the aircraft. The pilot went into the cabin and re-appeared with an undistinguishable item. The pilot then walked around the aircraft one more time before re-entering the cabin and closing the air stair cabin door. At about 0729, the right engine was started and, shortly after, the left engine was started.
Airservices Australia (Airservices) audio recordings indicated that, at 0736, the pilot requested a clearance from Essendon air traffic control (ATC) to reposition ZCR to the southern end of the passenger terminal. ATC provided the clearance and the pilot commenced taxiing to the terminal.
At the terminal, ZCR was refueled and the pilot was observed on CCTV to walk around the aircraft, stopping at the left and right engines[4] before entering the cabin. The pilot was then observed to leave the aircraft and wait for the passengers at the terminal. The passengers arrived at the terminal at 0841 and were escorted by the pilot directly to the aircraft. At 0849, the left engine was started and, shortly after, the right engine was started.
At 0853, the pilot requested a taxi clearance for King Island, with five persons onboard, under the instrument flight rules.[5] ATC instructed the pilot to taxi to holding point 'TANGO' for runway 17,[6] and provided an airways clearance for the aircraft to King Island with a visual departure. The pilot read back the clearance.
Airservices Automatic Dependent Surveillance Broadcast (ADS-B)[7] data[8] (refer to section titled Air traffic services information - Automatic Dependent Surveillance Broadcast data) indicated that, at 0854, ZCR was taxied from the terminal directly to the holding point. The aircraft did not enter the designated engine run-up bay positioned near holding point TANGO. At 0855, while holding at TANGO, the pilot requested a transponder code. The controller replied that he did not have one to issue yet. Two minutes later the pilot contacted ATC and stated that he was ready and waiting for a transponder code. The controller responded with the transponder code and a clearance to line-up on runway 17. At 0858, ATC cleared ZCR for take-off on runway 17 with departure instructions to turn right onto a heading of 200°. The pilot read back the instruction and commenced the take-off roll.
The aircraft’s take-off roll along runway 17 was longer than expected. Witnesses familiar with the aircraft type observed a noticeable yaw[9] to the left after the aircraft became airborne. The aircraft entered a relatively shallow climb and the landing gear remained down. The shallow climb was followed by a substantial left sideslip[10], while maintaining a roll[11] attitude of less than 10° to the left. Airservices ADS-B data indicated the aircraft reached a maximum height of approximately 160 ft above ground level while tracking in an arc to the left of the runway centreline (Figure 1). The aircraft’s track began diverging to the left of the runway centreline before rotation and the divergence increased as the flight progressed.
Following the sustained left sideslip, the aircraft began to descend and at 0858:48 the pilot transmitted on the Essendon Tower frequency repeating the word ‘MAYDAY’[12] seven times in rapid succession. Approximately 10 seconds after the aircraft became airborne, and 2 seconds after the transmission was completed, the aircraft collided with the roof of a building in the Essendon Airport Bulla Road Precinct - Retail Outlet Centre (outlet centre), coming to rest in a loading area at the rear of the building.
CCTV footage from a camera positioned at the rear of the building showed the final part of the accident sequence with post-impact fire evident; about 2 minutes later, first responders arrived on-site. At about 0905 and 0908 respectively, Victoria Police and the Metropolitan Fire Brigade arrived.
The pilot and passengers were fatally injured, and the aircraft was destroyed. There was significant structural, fire and water damage to the building. Additionally, two people on the ground received minor injuries and a number of parked vehicles were damaged.
__________
- On 15 November 2017, Essendon Airport was re-named Essendon Fields Airport.
- Eastern Daylight-saving Time (EDT): Coordinated Universal Time (UTC) + 11 hours.
- Due to the position of ZCR in relation to the CCTV camera, the ATSB was unable to distinguish specific details of the pilot’s actions.
- CCTV footage showed the pilot moving to the right side of the aircraft, but he went out of view. The pilot’s shadow could be seen in a position likely consistent with the right engine; he was not, however, visible in the footage.
- Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex, as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
- Runway number: the number represents the magnetic heading of the runway.
- ADS-B is an air traffic surveillance technology that enables aircraft to be accurately tracked by air traffic controllers and other pilots without the need for conventional radar.
- ADS-B data is transmitted from the aircraft multiple times a second and includes Global Positioning System latitude, longitude, groundspeed, track angle, vertical speed and pressure altitude. Estimated heights have been derived from the pressure altitude data, after barometric correction, and terrain elevation data. The resolution of pressure altitude data was 25 ft.
- The motion of an aircraft about its vertical or normal axis.
- Sideslip is an uncoordinated flight condition which can be expressed as the angular difference between the aircraft’s heading and the relative airflow. In a left sideslip, the aircraft’s nose is pointing to the left of the relative airflow.
- The movement of an aircraft about its longitudinal axis.
- MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
Pilot information
The pilot held a Commercial Pilot (Aeroplane) Licence, issued in September 1994, and attained his rating to operate the B200 aircraft in September 2004. He held a valid Class 1 Aviation Medical Certificate issued by the Civil Aviation Safety Authority (CASA) with a requirement to wear distance vision correction.
The pilot’s logbook showed a total flying experience of 7,681 hours to the last recorded flight on 18 February 2017. In the previous 90 days, the pilot had flown 66 hours and in the previous 30 days, he had flown 16 hours. He had a total of 73 hours in VH-ZCR (ZCR) and last flew the aircraft on 3 January 2017. Other records supplied by the operator indicated the pilot had accrued more than 2,400 hours in B200 aircraft.
Proficiency checks and flight reviews
The pilot had last completed a multi-engine flight review on 7 October 2016, valid to 31 October 2017 in ZCR. Records supplied by the operator also showed that the pilot had satisfactorily completed a Civil Aviation Order 20.11 emergency procedures proficiency check on 10 March 2016, valid until 9 March 2017.
The Civil Aviation Regulations 1988 regulation 224(A)(3)(d) stated that a pilot in command who was 65 years of age or older must successfully complete an instrument proficiency check (IPC) or flight review in an aircraft of the same category or an approved flight simulator for the category of aircraft, within 6 months before the date of a flight. The pilot, who was 67 years old at the time of the accident, last completed an IPC on 7 October 2016, about 4 months prior to the accident.
Following an incident[13] involving the pilot at Mount Hotham, Victoria on 3 September 2015, the pilot accepted CASA’s suggestion to undergo an IPC with a CASA flight operations inspector. That check flight was conducted on 19 October 2015. The pilot did not pass this IPC and it was recommended that the pilot conduct simulator training. There was no record in the pilot’s logbook to indicate that simulator training had been conducted, however, the pilot subsequently passed the IPC with the same CASA flight operations inspector on 3 November 2015.
CASA records stated that, other than the two IPC’s conducted with the CASA flight operations inspectors, the majority of the pilot’s flight tests and proficiency checks, including both instrument rating and Civil Aviation order 20.11 checks, were conducted by the same CASA Approved Testing Officer.
In response to the Mount Hotham incident, CASA compiled an audit report in January 2016. In that report, it was also commented that the pilot would benefit from ongoing training opportunities in a B200 simulator. The report indicated the simulator would have provided:
…an opportunity for non-jeopardy training in a variety of areas not possible in the aircraft. The use of a simulator assists in the development and maintenance of decision-making, situational awareness and practical skills, as well as exposing the pilot to real time scenarios and associated flight management practices.
The ATSB was unable to find any evidence to indicate that the pilot attended a B200 simulator after January 2016, however, CASA did not mandate that the pilot conduct the simulator training.
72-hour history
The pilot’s logbook showed the pilot conducted a flight from King Island to Essendon on 18 February 2017. He was reported to have then had two days away from flying duties. The pilot was also an air operator’s certificate (AOC) holder and, as such, was required to manage a business, including ensuring regulatory compliance. It is not known how much time the pilot spent managing his aircraft charter business during his two days away from flying duties.
The pilot was reported to normally go to bed between 2030 and 2100, or earlier if an early flight was scheduled for the next day. Evidence from Airservices indicated that the pilot’s National Aeronautical Information Processing System (NAIPS) user account was accessed at 2356 on the evening of 20 February 2017, to obtain aerodrome forecasts and Notice(s) to Airmen (NOTAM)[14] for Essendon, Victoria and King Island, Tasmania.
The same NAIPS account was accessed again on the morning of the accident, between 0456 and 0458, to obtain aerodrome forecasts and NOTAM for Essendon, King Island, Launceston, and Devonport, Tasmania. The pilot reportedly woke around this time, had breakfast and a beverage before leaving home for the drive to Essendon Airport. Traffic dependent, this drive was estimated to be between 1 hour 15 minutes and 2 hours.
On the above information, it was considered that the pilot had a sleep window of approximately 8 hours, but had a period of wakefulness during the night, when he briefly checked NAIPS. It is not known how long the period of wakefulness was and therefore not possible to assess the potential for it to have resulted in acute fatigue. Fatigue is a function of both sleep obtained and time awake however, and the pilot had been awake for about 4 hours at the time of the accident. That period of wakefulness is unlikely to have aggravated any feelings of fatigue associated with the previous night’s rest period.
The ATSB was also provided with varying accounts of factors that may have increased the pilot’s level of longer‑term fatigue, however, there was insufficient evidence to determine whether fatigue was a contributing factor to this accident.
Aircraft information
ZCR was a twin-engine turboprop aircraft with retractable landing gear, a pressurised cabin and a T-tail horizontal stabiliser (Figure 2). The aircraft was manufactured in the United States by the Raytheon Aircraft Company in 1996 and was issued with serial number BB-1544. At the time of the accident, Textron Aviation Inc. was the Type Certificate holder[15] for the aircraft. Textron Aviation Inc. branded the aircraft as a Beechcraft B200. The aircraft was imported into Australia and registered as ZCR on 9 October 2014.
After arriving in Australia, ZCR was reconfigured with a corporate-style interior and a passenger cabin seating capacity of seven. The aircraft was operated in the charter category. It had accumulated 6,997 flight hours prior to the accident flight.
Figure 2: Beechcraft B200 King Air, VH-ZCR

Source: Courtesy of FlightAware (flightaware.com)
Aircraft records
ZCR had a current Certificate of Registration and Airworthiness. The aircraft’s current maintenance release was destroyed in the accident. A copy of that maintenance release, at issue, was provided to the ATSB by ZCR’s maintainer. The maintenance release was due to expire on 16 December 2017 or upon 7,188 hours total time-in-service, whichever came first. The maintenance release also indicated that ZCR was equipped to be operated under the IFR and in the charter operational category.
Part 1 of the aircraft’s Logbook Statement specified the aircraft was to be maintained in accordance with aircraft manufacturer’s maintenance schedule and applicable Airworthiness Directives. A review of the maintenance documentation did not reveal any anomalies that may have contributed to the accident.
The following summarises the maintenance and activities conducted in ZCR leading up the accident:
- 16 December 2016 - major maintenance and rectifications were completed. A subsequent post-maintenance check flight was conducted with the accident pilot and a licenced aircraft maintenance engineer.
- 28 December 2016 - all the main landing gear tyres were replaced.
- 3 January 2017 - a flight was conducted by the accident pilot and a co-pilot. This was the last flight captured on the aircraft’s cockpit voice recorder.
- 12-13 January 2017 - the pilot who flew the aircraft reported experiencing a landing gear malfunction.
- 31 January 2017 - the landing gear power pack and the emergency locator transmitter battery were replaced. This was the last maintenance recorded in the aircraft’s records.
- 5 February 2017 - the aircraft operated for 6 hours without any reported defects and did not fly again until the accident flight on 21 February 2017.
- 20 February 2017 - the aircraft was towed out of a hangar adjacent to the maintenance provider and parked on the tarmac.
The ATSB did not identify any maintenance having been performed between 5 February and the accident flight on 21 February.
Operating speeds
The following information details the operating speeds and limitations applicable to ZCR (Table 1).
Table 1: Summary of operating speeds

Aircraft systems information
Flight control overview
The B200 aircraft is fitted with conventional flight controls connected to the aircraft’s primary flight control surfaces. The primary flight controls consist of the rudder, elevators and ailerons, which control the aircraft about the yaw, pitch and roll axes respectively (Figure 3).
The pilot controls an aircraft by manipulating the control wheel and rudder pedals, which deflect the ailerons, elevators and rudder. Deflection of an aircraft’s primary flight control surfaces changes the aerodynamic shape and therefore the amount of lift generated by the associated part of each wing, vertical stabiliser or horizontal stabiliser. These local variations in lift result in changes to the aircraft attitude and consequently flight path.
Any deflection of the primary flight control surfaces into the adjacent airflow produces aerodynamic forces on the surface and corresponding loads on the control wheel or rudder pedals. The magnitude of the aerodynamic force is principally related to the amount of flight control surface deflection, airspeed, and trim tab deflection.
On the B200 aircraft, adjustable trim tabs are attached to the trailing edge of the primary flight controls. These tabs are used to ‘trim’ or counteract the aerodynamic forces felt by the pilot on the control wheel or rudder pedals. During flight, deflection of an aircraft’s trim tab produces an aerodynamic force on the aft part of the associated primary surface. The tabs have the capacity, when adjusted in the opposite direction to the deflection of the primary surface, to modify the aerodynamic force on the surface and correspondingly, reduce the load felt by the pilot on the control wheel or rudder pedals. The effectiveness of a trim tab is principally related to the amount of deflection and the aircraft’s airspeed.
Figure 3: Position of the elevator, aileron and rudder trims on a B200 aircraft and the pitch, roll and yaw axes

Source: ATSB
Trim tab positions were adjusted on ZCR by rotating trim wheels, located on the centre pedestal (Figure 4). Moving the trim wheels transmitted rotary motion to screw jack actuators that positioned each tab. A position indicator for each trim tab was integrated with the respective trim control wheel.
Figure 4: Position of the elevator trim wheel, aileron trim wheel and rudder trim wheel on the centre pedestal of a B200 aircraft

Source: Australasian Jet Pty Ltd, annotated by the ATSB
Rudder trim
The rudder trim was manually controlled using a trim wheel located on the right side of the centre pedestal (Figure 5). Cables extend rearward from the wheel, through the airframe, to the rudder trim tab actuator. Rotating the wheel to the left moved the trim tab to the right, which in turn moved the rudder to the left, resulting in nose-left movement about the aircraft’s yaw axis. Rotating the wheel to the right results in yaw to the right. Operation of the rudder trim control showed that three turns through about 180 degrees were required in order to achieve full deflection either side of neutral.
Figure 5: Rudder trim indicator in the full nose-left, neutral and nose-right positions

Source: ATSB
Rudder boost system
The aircraft was fitted with a rudder boost system that aided the pilot in maintaining directional control in the event of an engine failure. Two pneumatic-boost servos were incorporated into the rudder system, which actuated the rudder control cables. This assisted the pilot by reducing the required rudder pedal force. The rudder boost system is controlled by a toggle switch on the centre pedestal, below the rudder trim wheel labelled RUDDER BOOST – OFF. The switch is to be turned on before flight.
Autopilot control
The aircraft was fitted with a three-axis autopilot and flight director system. The autopilot used a combination of sensors, electrical servos, guidance displays, mode selectors and flight control computers. These systems provide either full autopilot control of the aircraft, with simultaneous flight director monitoring or manual control in response to flight director steering commands.
The autopilot uses electric servos which are connected directly to the primary aileron, elevator and rudder control cables and to the elevator trim system. The autopilot is not connected to the aileron or rudder trim systems. The elevator trim system had an additional electric servo to control pitch trim independently of the autopilot utilising trim switches on the control wheel.
A component of the autopilot which affects aircraft yaw though the rudder system is called the yaw damper. The yaw damper can be operated independently to the rest of the autopilot system. Its function is to assist the pilot in maintaining directional control, and to increase passenger ride comfort. While the system could be used at any altitude and was required above flight level[16] 170, it should be deactivated for take-off and landing. The yaw damper is actuated through the rudder autopilot servo, which is connected directly to the rudder cables and has no connection to the rudder trim cables.
Flap system description
The aircraft had four flaps, one inboard, and one outboard per wing. The flaps are normally in the fully retracted position. They are extended to slow the aircraft and allow it to land at a lower airspeed. They can also be used to aid short field take-off performance in the APPROACH position. The flaps were operated using a sliding selector positioned on the centre pedestal. Flap travel was registered on an indicator above the pedestal, the indicator represents flap position in a percentage. There were three detents in the selector assembly that correspond with:
- UP or 0%, representing fully retracted, 0⁰ of travel
- APPROACH or 40%, representing 14⁰ of flap down travel
- DOWN or 100%, representing full extension, 35⁰ of flap down travel.
The flaps cannot be stopped in-between any of the three positions. If an asymmetric flap condition is detected, power to the electric flap motor is disconnected.
Flight control locks
While parked, the flight and engine controls were mechanically locked by a U-shaped clamp and two pins (Figure 6). The pins lock the control wheel and rudder pedals and the U-shaped collar fits around the engine control levers to prevent movement when the lock is installed. The rudder pin locked the nose wheel steering in the neutral position, making normal ground manoeuvring impossible. The control wheel lock prevents movement of the elevators and ailerons making it unlikely the aircraft could be rotated on take-off. The control lock components were connected together by chain and were to be removed prior to towing the aircraft. The control lock mechanism shown below was consistent with the description of the lock used in ZCR.
Figure 6: Example of the control lock, fitted to a B200 aircraft

Source: Textron Aviation Inc., annotated by the ATSB
Engine controls
The B200 propulsion system is operated using three sets of controls located in the engine controls section of the centre pedestal (Figure 7):
- Power levers control engine power from the idle position through to take-off power. When the power levers are lifted and pulled aft over a gate, they control propeller reverse thrust for slowing the aircraft after landing and for taxi operations.
- Propeller levers control propeller revolutions per minute (RPM). The propellers can be feathered by moving the levers past detents and back to the full aft position.
- Condition levers are used to select high or low idle and to shut the engines down.
Friction locks
Four friction locks were located on the engine control quadrant. One each for the left and right power levers, one for the propeller levers and one for the condition levers (Figure 7). When rotated in an anti-clockwise direction, the propulsion systems controls moved freely. When rotated in a clockwise direction, the levers progressively become resistant to movement, preventing the levers from moving out of position.
Figure 7: Engine control pedestal showing power levers, propeller levers, condition levers and friction locks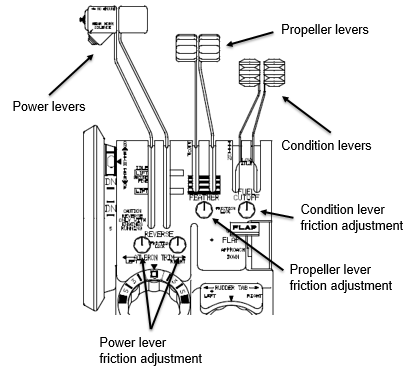
Source: Textron Aviation Inc., annotated by the ATSB
Power lever roll back (creep)
Throughout the investigation, the ATSB spoke with numerous B200 pilots who highlighted the importance of ensuring power lever frictions were adequately tightened prior to take-off. In their experience, if inadequate power lever friction was set, the power levers could ‘creep’ back from the full-power position when the pilot removed their hand from the levers after take-off.
If power lever movement is not noticed, the aircraft may not climb and accelerate normally, and rudder force may be required to keep the aircraft straight. In addition, the auto-feather system will be disarmed if either power lever moves back past the ‘90% engine’ speed position (refer to section titled Autofeather system below).
Autofeather system
ZCR was equipped with an auto feathering system, which provided a means for automatically feathering the propellers in the event of an engine failure. Feathering reduces drag by increasing the angle of the propeller blades until they are parallel with the aircraft’s line of flight.
Airport information
Essendon Airport is located about 8 km to the south-east of Melbourne Airport. It provided facilities and services for international and domestic corporate aircraft, aircraft maintenance, airfreight, and aircraft charter. It was also the base for emergency services fixed-wing aircraft and helicopters for police, air ambulance and firefighting aircraft operations.
It has two runways aligned 17/35 and 08/26 (Figure 8). Runway 17/35 was the runway-in-use at the time of the accident and was 1,504 m in length, with a 0.9 per cent slope down to the south. Runway 08/26 was 1,921 m in length. Three windsocks were positioned around the airport, one of which was located adjacent to the northern end of runway 17/35.
Airservices provided air traffic services to the flight crew of aircraft operating at Essendon and in the surrounding airspace. At the time of the accident, the pilot of ZCR was communicating with Essendon Tower.
The Airservices publication En Route Supplement Australia (the ERSA) indicated that a bird hazard existed at the airport. A helicopter pilot who had landed shortly before the accident could not recall observing any bird activity in the area. Similarly, a pilot positioned on the eastern side of runway 17/35, who observed ZCR take off, reported that he did not observe birds in the vicinity off the aircraft during take-off and climb.
Figure 8: Essendon Airport and the location of the ATC tower, windsocks, and proximity of the Bulla Road Precinct

Source: Google, annotated by the ATSB
Bulla Road Precinct obstacle limitation surface exceedances
ZCR collided with a building constructed on the south-eastern corner of Essendon Airport (Figure 8). This building was one of four, collectively known as the Bulla Road Precinct – Retail Outlet Centre (outlet centre), proposed by the airport lessee in 2003, approved by the Federal Government in 2004, and completed in 2005.
The ERSA, a component of the Aeronautical Information Publication, publishes information about an airport’s infrastructure and, in particular, runway data and airspace obstructions that may affect operations at the airport. The airport data for Essendon included seven obstacles that breached the airport’s obstacle limitation surfaces (OLS). Four of those obstacles infringed the runway 26 transitional surface component of the OLS and were associated with two buildings within the outlet centre that were not struck by the aircraft. CASA accepted the breaches in 2015 after the airport operator applied lighting and colour to the obstacles to mitigate their risk to aircraft operations.
The OLS are a series of surfaces that set the height limits of objects around an airport. The transitional surface is a component of the OLS that is immediately adjacent to the runway area. The runway area includes the runway itself and an adjacent area that is required to be graded and clear of all obstacles. The intent of the OLS is to provide airspace around an airport that is kept as free as possible from obstacles so as to permit the intended aircraft operations at the airport to be conducted safely, as well as to prevent the airport from becoming unusable as a result of growth of obstacles around it. The airport operator is responsible for establishing an applicable OLS. The surfaces of the OLS are based on a complex set of criteria that include whether the runway is used for departures and/or landings, and the types of approaches attached to that runway.
At the request of the investigation, the airport operator produced an OLS based on runway 17/35 only, and mapped the outlet centre obstacles in relation to this particular OLS. That data identified that the listed obstacles did not penetrate the OLS for runway 17/35. The airport operator also identified a further three obstacles that were not listed in the ERSA as breaching the OLS. They were not listed as they were considered minor breaches of the OLS. These obstacles related to light poles in the area of the outlet centre. The aircraft did not collide with any of the obstacles that breached the OLS.
Meteorological information
The automatic terminal information service (ATIS) information current at the time of the aircraft’s departure indicated that runway 17 was being used for departures and runway 26 for arrivals. The wind was reported as 340° at 5 kt, all tailwind on runway 17, the conditions were CAVOK,[17] and the temperature was 12 °C. Subsequent ATIS information issued after the accident indicated the airport was closed, due to the accident, and the wind was variable[18] at 5 kt.
The Bureau of Meteorology provided the ATSB with one-minute interval data recorded by the Essendon automatic weather station. At 0859, the wind was 322° at 4 kt gusting to 5 kt, which would have resulted in about a 4 kt tailwind on runway 17. The temperature was 14 °C.
The Essendon air traffic controllers indicated that, on the morning of the accident, the windsocks were showing nil wind but the anemometer[19] was indicating winds up to 5 kt. Consequently, using the least favourable scenario, the controllers stipulated on the ATIS that the wind speed was 5 kt, which was the maximum allowable tailwind on the nominated runway-in-use. The controllers also reported that, when the anemometer reading was less than about 7-8 kt, the readings became unreliable due to the siting of the anemometer. The automatic weather station was positioned on the eastern side of runway 17/35. The wind anemometer was located about 10 m south-east of the station.
On 14 September 2017, the Bureau of Meteorology advised the ATSB that the anemometer had been in the same position since 2003. Since the accident, however, a potential issue with the anemometer siting had been raised, which they were investigating.
Two witnesses, both of whom were pilots familiar with the B200 aircraft type, were positioned on the eastern side of runway 17/35 at the time of ZCR’s departure. They recalled that the wind was ‘fairly calm’ and there was no adverse weather present at the time. Images of the smoke plume and video footage of the windsock adjacent to the northern end of runway 17/35 taken shortly after the accident also showed that the wind at ground level was negligible (Figure 9 and Figure 10).
Overall, the wind conditions around the time of the accident were likely to have been calm. However, it could not be ruled out that the wind conditions ranged to a maximum of 5 kt tailwind on runway 17, which was within the aircraft’s limitations.
Figure 9: Photographs of the smoke plume that provided an indication of the wind conditions

Source: Alex Poole (left) and David Bell (right)
Figure 10: Indications of wind from the windsock located adjacent to the northern end of runway 17/35

Source: Victoria Police
Air traffic services information
Flight plan
The pilot’s flight plan submitted to Airservices specified a scheduled departure time of 0830 from Essendon and a total estimated elapsed time of 36 minutes to King Island. The plan also indicated that the flight was a ‘non-scheduled air service’ to be conducted under the instrument flight rules, and there was to be five persons on board.
MAYDAY call
The MAYDAY call broadcast by the pilot of ZCR shortly after take-off was reviewed by the ATSB. No additional information regarding the nature of the emergency was identified. In addition, the ATSB’s assessment of the pilot’s speech characteristics was unable to provide any further information.
Automatic Dependent Surveillance Broadcast data
Automatic Dependent Surveillance Broadcast (ADS-B) data was obtained from Airservices. The ADS-B data was transmitted from the aircraft multiple times per second using the aircraft’s mode‑S transponder.[20] ADS-B parameters include latitude, longitude, groundspeed, track angle, vertical speed and pressure altitude. With the exception of pressure altitude, these parameters were sourced from the aircraft’s GPS. Pressure altitude information was sourced from ZCR’s static system.[21]
The ADS-B pressure altitude data was considered more accurate than the GPS vertical rate data. Following the observed sideslip in the latter part of the flight, however, the pressure data was no longer considered reliable. This was due to the local airflow effects near the static ports induced by the substantial sideslip (refer to section titled Aircraft flight path profile).
The following information was derived from the ADS-B data:
- ZCR performed a rolling take-off after turning onto runway 17 from holding point TANGO.
- ZCR reached the rotation speed of 94 kt at about 730 m from the threshold of runway 17. The aircraft’s derived acceleration was refined using CCTV footage.
- ZCR became airborne about 1,015 m from the threshold of runway 17. The aircraft’s rotation point was confirmed using CCTV footage.
- The aircraft began to deviate to the left of the runway centre-line between ADS-B data points A and B (Figure 11). The rate of deviation was initially constant but then increased as the flight progressed (Figure 12).
- ZCR became airborne at a groundspeed of about 111 kt.
- Using the rate of change in ADS-B pressure altitude data, ZCR’s initial rate of climb was about 1,100 ± 200 feet per minute.
- ZCR stopped accelerating about 5 seconds after becoming airborne.
- The maximum groundspeed recorded for the flight was 116 kt.
- ZCR reached a height, above ground level (AGL), of no more than 160 feet.
- The MAYDAY call was initiated about 7 seconds after ZCR became airborne. At this time, ZCR’s airspeed was decreasing, the vertical speed was changing from a climb to a descent and the track was deviating to the left at an increasing rate.
- The final ADS-B data point was recorded at 0858:52, about 10 seconds after the aircraft became airborne and about half a second before the collision with the outlet centre building.
Figure 11: ADS-B data showing initiation of ZCR’s divergence from the runway centreline between points A and B

Source: Google, annotated by the ATSB
Figure 12: ADS-B data points showing ZCR’s increasing divergence from the runway centreline as the flight progresses

Source: Google, annotated by the ATSB
Witness observations
A number of witnesses were interviewed by the ATSB and Victoria Police. The following provides a description of the observations by the key witnesses and a combined summary of the other witnesses interviewed.
Key witnesses
Pilots on the eastern side of runway 17
Two B200 pilots were positioned on the eastern side of runway 17, in line with the air traffic control tower (Figure 13). Both witnesses observed the aircraft taxiing past the control tower toward the runway 17 threshold. The witnesses were unable to observe the beginning of the take-off roll; they could, however, hear the aircraft’s engines, which they reported as sounding normal. Shortly after commencing the take-off roll, the aircraft came into view. The witnesses were expecting the aircraft to become airborne around their position, however ZCR continued along the runway. They commented that it appeared that the aircraft became airborne near the runway intersection or about two‑thirds along the runway, which was considered an unusually long take-off roll.
Figure 13: Image showing the key witness positions relative to ZCR’s track

Source: Google, annotated by the ATSB
One of the witnesses reported observing the aircraft in a shallow climb after it became airborne. Immediately after, or possibly several aircraft lengths after, a left turn was observed. The turn was described as a ‘flat’, yawing or skidding turn rather than a rolling turn, with possibly 5-10° angle of bank, at a ‘very slow’ speed. The aircraft then appeared to be at right angles to the runway, heading in an easterly direction. The aircraft was observed climbing no higher than about 100 ft AGL, before descending. The witness stated that he then lost sight of the aircraft behind the buildings. Overall, the witness believed there was something wrong when the aircraft was on the ground as well as when it was airborne.
The other witness reported that, after it became airborne, the aircraft immediately yawed left, similar to that experienced with a strong crosswind. He further reported the aircraft did not climb and the aircraft’s attitude was about 5° nose-up, which was less than half of what he would normally expect. He reported the aircraft’s wings were level and it continued yawing left and climbed to no more than 100-150 ft AGL. The witness then observed the aircraft stop climbing and adopt an almost level attitude, which coincided with the left yaw increasing. The witness stated the aircraft was going ‘extremely slow’ and was almost ‘floating’. The aircraft descended and then disappeared behind the buildings.
Both witnesses reported that the landing gear had remained extended. They further stated that there were no unusual sounds heard during the take-off, such as the propellers trying to stay ‘on speed’, sounds associated with the propellers feathering or changing pitch, and no compressor stall sounds. The aircraft sounded normal.
Refuelling operator
A local refuelling operator had stopped his truck adjacent to runway 17, facing south, to take a phone call. While on the phone, the operator observed ZCR shortly after becoming airborne. The aircraft was at about 30-40 ft AGL and climbing in what he believed to be a normal take-off configuration.
When the aircraft was about over the runway intersection, he saw the aircraft yaw ‘savagely’ left, but stay relatively ‘flat’; the aircraft did not bank. He did not observe any corrections to the yaw. The aircraft climbed to no more than 100-200 ft before it began to descend rapidly. He lost sight of the aircraft as it descended behind the outlet centre buildings.
As the operator remained in his truck with the engine running, he was unable to hear any sounds associated with ZCR. The landing gear was reported to have remained extended.
Air traffic controllers
One of the Essendon Tower air traffic controllers observed ZCR’s take-off roll and reported that the aircraft accelerated as expected and appeared normal. The aircraft appeared to rotate at the correct position. He did not hear any unusual noises from the aircraft as it went past the tower.
After this, the air traffic controller moved his attention to other work-related activities. Shortly after, the controller heard a MAYDAY call, which he recognised as being from ZCR. He was expecting the pilot to continue the MAYDAY call and provide further details. At the same time, he looked at the aircraft and noted that the aircraft was facing east instead of south. The aircraft was in a ‘flat’ orientation and appeared to be travelling ‘very slowly’ compared with what he would expect. The nose then dipped and the aircraft disappeared behind the outlet centre buildings. The controller advised the Melbourne departures controller of the accident, instructed an airport safety vehicle to attend the accident site, and dealt with other aircraft traffic.
Another air traffic controller in the Essendon Tower first sighted ZCR when it was airborne and near the runway intersection, at about 50-100 ft AGL. That controller reported that the aircraft was low, but there was nothing untoward at that time. After hearing the MAYDAY call, the controller observed the aircraft facing east in a nearly level attitude and moving slowly. The aircraft climbed to an estimated 200 ft before descending and disappearing behind the outlet centre buildings.
Helicopter pilot
At the time of the accident, a helicopter pilot had just landed and was positioned on the southern apron, facing in an easterly direction, and preparing to shut down. The pilot saw ZCR shortly after it became airborne and reported that it appeared normal. At that time, he could see the right side of the aircraft. However, when ZCR was around the runway intersection, the aircraft started to yaw left, which the pilot stated was unusual. He was now looking more directly behind the aircraft. He reported the aircraft was possibly rolling left, but only by about 5-10°. The aircraft climbed to about 100-200 ft AGL, before it started to descend. It disappeared behind the outlet centre buildings and seconds later, the pilot saw smoke rising from where the aircraft had disappeared from view. As the helicopter was still running, the pilot was unable to identify any sounds associated with ZCR.
Crane operator
A crane operator was working directly opposite the accident site, on the other side of the Tullamarine Freeway (Figure 14). The crane was facing in a north-westerly direction and the operator had an unobstructed view of Essendon Airport out his right window. The distance between the ground and the operator’s eye level in the cabin was about 24 m.
Figure 14: Position of the crane relative to the accident site, with the crane inset

Source: Victoria Police, annotated by the ATSB
The operator reported hearing the sound of an aircraft’s engines, which sounded loud and in close proximity. The engines appeared to be operating normally and there were no indications of ‘misfiring or distress’. Having been alerted by the sound, the operator looked out the right window and saw the aircraft at about 25-35 m above the ground. Referring to (Figure 15), the aircraft’s initial position was close to being in-line with the hook of the crane at the accident site and the airport building in the background. The operator identified the aircraft as a twin-engine, low‑winged, turboprop aircraft.
The aircraft was described as moving or sliding towards him, but not facing him. The aircraft’s nose was about 10-15° to the left of his position and about 10° or ‘slightly down’. The operator had a view of the right side of the aircraft and believed that the right engine was operating. He was unable to comment if the left engine was also operating or recall if the landing gear was extended.
After this, the aircraft descended to the right over the billboard second from the right. The aircraft yawed further left, possibly an angle of 30-40°, before momentarily disappearing behind the billboard on the far right. The aircraft impacted the roof and parapet wall, and flames ensued immediately after. The aircraft continued moving forward and came to rest in the loading area at the rear of the building.
Figure 15: View of the accident site from the crane operator’s right cabin window

Source: ATSB
General witness observations
Multiple witnesses were interviewed by the ATSB and Victoria Police. These witness observations may have been influenced by the varied physical locations, environmental conditions, and the short time frame within which the accident occurred.
Although there were several inconsistencies, the majority of the witnesses reported that the aircraft was relatively flat with wings level or in a slight bank. They described the aircraft as moving sideways, ‘drifting’ or ‘crabbing’ like in a crosswind or yawing, and that it was low. One witness, who was a pilot, saw the aircraft shortly after becoming airborne. He observed it conduct a 5-10° left bank and veer left, as if ‘full rudder was being applied’. He described the aircraft as initially heading about 150°, but finished facing to the east, with wings level and the landing gear remaining extended.
With regard to the engine sounds, there was some variation in observations between the witnesses. The majority, however, including one familiar with the B200 aircraft, reported that the engine sound was loud and constant.
Aircraft flight path profile
Following witness observations of a significant left yaw, the ATSB attempted to define the aircraft’s sideslip and roll angles at different points along the flight path using video footage from CCTV and a vehicle dashboard camera. Still images were extracted from the CCTV and dashboard camera footage, and the location of the aircraft was determined using ADS-B data at points A through G (Figure 16). ZCR’s track was determined at each point using ADS-B data.
Figure 16: ZCR’s track, location of the cameras and location of ZCR in each analysed image
 Source: Google, annotated by the ATSB
Source: Google, annotated by the ATSB
The aircraft’s heading was determined at each point by relating the distance between the landing gear wheels to an angular displacement. The height of the aircraft’s tail was measured in pixels to provide a datum for pixel size (Figure 17).
Figure 17: Example of method for estimating sideslip angle, image is from level 1 main apron camera

Left image (a) shows the use of objects in the image to determine the location of the aircraft.
Right image (b) demonstrates measurement of the height of the tail and distance between the left wheel (LW), right wheel (RW) and the nose wheel (NW).
Note: in Figure (a) the smoke has been overlayed on the image to give an approximate location of the accident site in relation to the aircraft.
Source: Essendon Airport, annotated by the ATSB
At points E and F, the aircraft was too far away from the camera to use this method. For these two points, an estimated heading was determined graphically by aligning a scaled diagram of the aircraft with the CCTV image (Figure 18).
Figure 18: Example of graphical method for estimating sideslip angle

Source: Essendon Airport, annotated by the ATSB
The angular difference between the aircraft heading and the aircraft track gives the sideslip angle. The methods used to determine the aircraft’s sideslip angle at each point and the probable accuracy are summarised in (Table 2).
Roll was calculated using the following two methods:
- The relative height of each wheel was measured and then related to an angular displacement on the aircraft’s roll axis. This method was used for the Bulla Road dashboard camera.
- Drawing lines on the still image that were representative of the wing angle and the height difference in the wheels, then determining the aircraft’s rotation by measuring the angular difference between the representative line and a known level surface in the image.
The methods used to estimate ZCR’s sideslip and roll contained the following assumptions and potential errors:
- It was assumed that the aircraft was far enough away from the camera that perspective did not introduce significant error.
- The tail was assumed to be in a perpendicular plane to the camera and therefore the viewed height of the tail was its actual height.
- There were potential errors in measuring distances and heights in pixels, these errors were cumulative.
- The error in the calculations varied depending on ZCR’s distance from the camera, picture quality and viewing angle of the aircraft. The more accurate sideslip angles were about ± 5o, with the least accurate calculation about ± 20o.
- The images were examined to determine the amount of distortion from the lens, in particular fisheye distortion. The outlet centre camera had substantial fisheye distortion and therefore some analysis, roll angle in particular, was limited (Figure 19). The ‘Level 1 main apron’ camera appeared to have minimal distortion, despite having a wide-angle lens (Figure 20).
Figure 19: Outlet centre camera 83 still used for analysis, showing significant fisheye distortion in the image

Horizontal green line in inset image represents the distance between the main landing gear and the vertical green line represents the height of the tail as a reference. Source: Essendon Direct Factory Outlet, annotated by the ATSB
Figure 20: Time-lapse image of the aircraft flight path taken from the Essendon Airport Level 1 main apron camera
 CCTV frame rate 30 images/minute, screenshots were taken every 2 seconds. Source: Essendon Airport, annotated by the ATSB
CCTV frame rate 30 images/minute, screenshots were taken every 2 seconds. Source: Essendon Airport, annotated by the ATSB
Figure 21: Bulla Road dashboard camera footage with zoomed inset depicting measurements used for sideslip and roll calculations

Source: Supplied
In summary, the results below demonstrate a substantial left sideslip between points D and G with minimal left roll. These results were consistent with witness observations and analysis of the accident site roof impact marks.
Table 2: Results of sideslip study
| Identifier | Camera location | Aircraft Track (T) | Left sideslip angle and tolerance |
Aircraft roll to the left | Comments/limitations |
| A | Lvl1 main apron (Figure 20) |
176° | 2° ± 5° | N/A | Aircraft probably still on runway so unlikely to have any sideslip. |
| B | Outlet centre camera 83 (Figure 19) |
170° | 5° ± 10° | N/A | Image contained significant fisheye. |
| C | Lvl1 main apron | 160 - 165° | 0 ± 10° | 4-6° | The estimated location of the aircraft meant the aircraft track could vary by 5°. |
| D | Lvl1 main apron | 155 - 160° | 35° ± 15° | 6-9° |
A graphical method was used to determine the sideslip angle. A sideslip of 35° is very high so is more likely to be at the lower end of the error band rather than the upper. |
| E | Lvl1 main apron | 142° | 50° ± 20° | Too far away to determine |
A graphical method was used to determine the sideslip angle. The distance and the viewing angle reduced accuracy. A sideslip of 50° is extremely high so is more likely to be at the lower end of the error band. |
| F | Lvl1 main apron | 130° | 25o ± 10° | Too far away to determine | A graphical method was used to determine the sideslip angle. The distance and the viewing angle reduced accuracy. |
| G | Bulla Rd (Figure 21) |
115° | 25° ± 5° | 6° |
Correlation of ADS-B data and sideslip information
Sideslip information was correlated with Airservices ADS-B data to determine the relationship between the aircraft’s sideslip and performance. This comparison found that the reduction in ZCR’s airspeed, identified by the ADS-B data, correlated with the onset of the sideslip. This was most likely due to the increase in drag from the sideslip (Figure 22).
Similarly, the aircraft’s climb performance also reduced at the same time as the onset of the sideslip. As the ADS-B barometric data was considered unreliable while the aircraft was in a substantial sideslip, a time-lapse image was produced to provide an indicative depiction of the aircraft’s vertical flight path (Figure 23). The substantial sideslip was first observed at point 6 in Figure 23, at this point the image shows the aircraft transitioning from a climb to a descent.
Figure 22: Comparison of groundspeed and sideslip angle against time measured from the beginning of the take-off roll

Source: ATSB
Figure 23: Time-lapse CCTV image of the ZCR’s flight path, with images taken every second
Source: Linfox, annotated by the ATSB
Recorded information
Cockpit voice recorder
ZCR was fitted with a cockpit voice recorder (CVR) as required by Civil Aviation Order 20.18. The aircraft was not fitted with a flight data recorder, nor was it required to be by Australian regulations.
CVR systems provide a record of flight crew conversations. In addition, the CVR can provide a record of the cockpit audio environment, including sounds relating to engine/propeller operation, aural alerts, operation of switches and levers, activation of the landing gear, and the weather such as rain or hail.
The CVR control unit, located in the cockpit, allows a pilot to test the serviceability of the CVR system. The power supply for the CVR unit was fitted with an ‘impact switch’ designed to stop the recorder and prevent any erasure feature from functioning when deceleration forces similar to those expected in an accident are sensed.
ZCR was fitted with a Fairchild model A100S CVR in June 1996, at about the time the aircraft entered service. The fire-damaged CVR was removed from the wreckage and transported to the ATSB’s technical facilities in Canberra for examination. The CVR was successfully downloaded, however, no audio from the accident flight was recorded. The recovered audio related to a previous flight on 3 January 2017. This recording began at the expected time prior to engine start. The recording stopped, however, at about the time the aircraft landed at the arrival aerodrome. The post-landing taxi and engine shutdowns were not recorded. It was likely that the ‘impact switch’ was activated during the landing and power was removed from the CVR.
CVR serviceability checks and maintenance
An applicable CASA airworthiness directive relating to the CVR, AD/REC/1, (www.casa.gov.au) was carried out by ZCR’s maintenance provider in December 2016. The maintenance action included replacing the ‘impact switch’. No defects were logged following the conduct of the inspection.
CVR system operating instructions
Following a CVR installation in an aircraft, supplemental material related to the operation of the CVR must be attached to the Pilots Operating Handbook (POH) or approved Airplane Flight Manual (AFM). A copy of the Raytheon Aircraft Company Beechcraft Super King Air B200/B200C AFM supplement was provided by the aircraft manufacturer. That supplement indicated that a self‑test must be successfully accomplished prior to flight. This was to be achieved following the procedure below (Figure 24). Due to fire damage to the aircraft, the ATSB could not determine if the AFM contained this supplement. (For further information on checklists refer to section titled Organisational information – Flight Check System).
Figure 24: Supplemental procedure for testing CVR serviceability

Source: Aircraft manufacturer
A pilot who regularly flew ZCR was aware that it was fitted with a CVR and he would test the system as described above. He could not recall, however, if there was a specific checklist item for this. He also commented that other B200 aircraft he had operated were not fitted with CVRs. Similarly, another pilot who was aware of the CVR was using another company’s checklist and could not recall if there was a checklist item regarding the CVR. That pilot also stated that he did not operate the CVR in ZCR. A CASA-authorised testing officer who had flown ZCR stated that he had used the checklist in the aircraft, but was not aware that it was fitted with a CVR, suggesting the CVR checklist items were not included in ZCR’s checklist.
It is unknown if the accident pilot was aware that ZCR was fitted with a CVR and the requirement to conduct the self-test prior to flight. Of note, the pilot previously flew another B200 aircraft, which was not fitted with a CVR.
Dashboard camera audio frequency analysis
A witness driving on the Tullamarine Freeway provided dashboard camera footage of the accident to the ATSB. The footage featured a sound consistent with an aircraft passing nearby immediately prior to the collision with the outlet centre.
Frequency analysis determined that the aircraft’s engine power was at a high level, loud enough to drown out background noises such as car, road and airflow noise. Only one propeller frequency was present, meaning that either both propellers were at similar RPM or only one propeller was operating at the identified frequency and the other propeller was not detected in the frequency analysis. While the ATSB could not establish if one or both engines were operating at a high level, the analysis determined that the propeller RPM(s) were at the nominal take-off setting of 2,000 RPM.
Wreckage and impact information
Accident site
The aircraft intially contacted the roof of a building in the outlet centre adjacent to the southern end of runway 17 (Figure 25). A search of the runway and surrounding area did not identify any items related to ZCR. In addition, there was no evidence of a bird strike under the aircraft’s flight path or at the accident site.
After colliding with the building’s roof and parapet wall, the aircraft came to rest in a loading zone at the rear of the building. A post-impact fuel-fed fire severely damaged the wreckage and initiated a fire in the building.
Figure 25: Accident site overview

Source: Metropolitan Fire Brigade (Melbourne), annotated by the ATSB
Impact mark analysis
Marks from the landing gear and slash marks from the left propeller’s blades were identified on the building’s roof. These marks were used to determine the aircraft’s initial impact attitude by aligning a scaled diagram of a B200 aircraft with an image of the marks (Figure 26).
Figure 26: Outlet centre roof impact damage with scaled aircraft aligned with impact marks
 Note: Landing gear wheels are offset to the right and apparent wingspan is reduced to allow for a slight left bank. Source: Metropolitan Fire Brigade (Melbourne), annotated by the ATSB
Note: Landing gear wheels are offset to the right and apparent wingspan is reduced to allow for a slight left bank. Source: Metropolitan Fire Brigade (Melbourne), annotated by the ATSB
Analysis of the roof impact marks indicated that:
- the aircraft had a heading angle of about 86 ⁰ (T)
- the ground track was about 114 ⁰ (T)
- the aircraft was at a sideslip angle of about 28⁰ left of track
- the aircraft was slightly left-wing and nose-low with a shallow angle of descent at the initial roof impact
- after the initial impact, the aircraft rotated left on its vertical axis until the fuselage was about parallel with the rear parapet wall of the building.
Propeller slash marks
Nine propeller slash marks were located in the building’s roof (Figure 27). Analysis of those slash marks indicated that they had been created by the left propeller blades cutting through roofing material while rotating.
Figure 27: Left propeller slash marks in roofing material with tape measure showing distance between cuts

Source: ATSB
The last 2 seconds of ADS-B data indicated ZCR’s ground speed was about 108 kt. Allowing for potential aircraft deceleration due to the nose landing gear colliding with the roof, prior to the left propeller blades making contact, the left propeller RPM was calculated as being consistent with ZCR’s nominal take-off setting of 2,000 RPM. This was consistent with the estimated propeller RPM established from the dashboard camera audio frequency analysis (refer to section titled Recorded information - Dashboard camera audio frequency analysis).
An estimate of ZCR’s sideslip angle was also obtained by measuring the angle between the flight path and the slash marks, corrected for aircraft speed and propeller RPM. Using this method, the angle of sideslip at impact was calculated as being about 29° to the left. The results of this method to calculate sideslip at impact was consistent with the impact mark analysis above.
Other damage
After the initial impact, the aircraft collided with a concrete parapet wall before coming to rest in the building’s rear loading area. There was significant structural damage to the building, and the retail business operating in that section of the building incurred significant fire and water damage. Several vehicles parked at the rear of the building were also damaged or destroyed.
Aircraft wreckage
The majority of the aircraft was damaged or destroyed as a result of the collision with the building and subsequent fire. The damage precluded a complete examination of many components and systems (Figure 28). All major parts of the aircraft were accounted for at the accident site. On-site examination of the wreckage did not identify any pre-impact faults with the aircraft that could have contributed to the accident.
Figure 28: Main wreckage

Source: ATSB
The outboard right-wing sections, main landing gear lower sections, both engines, and both propellers separated from the aircraft during the accident sequence and were located at the accident site. The nose gear oleo and wheel assembly came to rest on the Tullamarine Freeway, about 65 m from the main wreckage, in the direction of the flight.
Tyre marks on the building’s roof and damage to the main and nose landing gear assemblies indicated that the landing gear was down during the accident sequence. Dashboard camera footage of the aircraft just prior to impact, along with witness observations, further supported the landing gear being in the down position.
Rudder
The majority of the vertical stabiliser was destroyed by fire (Figure 29). The rudder flight control surface was still attached to what remained of the vertical stabiliser. The rudder control cables, bell cranks, and push-pull tubes were inspected from the cockpit through to the tail with no pre‑impact faults identified.
Figure 29: Remains of the vertical stabilizer on its left side showing position of rudder and trim actuator

Source: ATSB
Rudder trim
The left rudder trim cable had failed at a position towards the rear of the fuselage. Inspection of the cable fracture revealed necking-type failure of individual strands within the cable. That, and the way the cable was splayed, were indicative of an overstress fracture, likely as a result of the collision (Figure 30).
Figure 30: Schematic of rudder trim system showing the approximate cable fracture point (left) and a picture of the left rudder trim cable fracture (right)

Source: Textron Aviation Inc. and ATSB
The rudder trim actuator screw jack was extended 43 mm when measured from the actuator body to the center of the rod end, which equated to the rudder trim being in the full nose-left position. Due to the significant yaw observed by witnesses, the rudder actuator was removed from the wreckage for further detailed examination. This examination determined that the rudder trim tab actuator was likely in the full nose-left position at impact (refer to section titled Appendix B – Rudder trim tab actuator examination).
Abrasion marks and compression damage were present on the right side of the empennage, rudder, and rudder trim tab, indicating that the area had come in contact with a hard flat abrasive surface (Figure 31). Abrasion on the rudder trim tab trailing edge was significantly greater than the corresponding abrasion on the rudder trailing edge, shown in Detail A (Figure 32 and Figure 33). The abrasion damage indicated that the rudder trim tab was positioned to the right of the rudder surface during the impact sequence. The angular displacement of the rudder trim tab could not be determined from the abrasion marks, however the displacement indicated that the rudder trim was in a nose-left position at impact.
Figure 31: Empennage and rudder viewed from the right showing abrasion damage

Source: ATSB
Figure 32: Rudder and rudder trim showing abrasion damage

Source: ATSB
Figure 33: Detail A. Close-up of abrasion damage to rudder and upper surface of rudder trim trailing edge

Source: ATSB
Analysis of the roof impact marks and CCTV footage showed that the aircraft had contacted the concrete parapet wall on the right side of the empennage before exiting the roof of the building. It was likely that the impact with the wall caused the abrasion damage to the empennage and rudder.
Rudder boost system
The rudder boost control system was destroyed by fire, however, sections of the rudder boost actuators were located within ZCR’s empennage. No anomalies were identified in the remaining sections of the actuators.
Elevator trim
Both the left and right elevator trim actuators were found in a position that equated to a full nose‑up trim position. Witnesses, CCTV and ADS-B evidence either opposed or did not support ZCR having full nose-up trim at take-off. It is possible that the elevator trim was moved to this position by the pilot in an attempt to control the aircraft’s flight path or the trim may have moved as a result of impact forces. The ATSB determined however, that it was unlikely that the elevator trim was in the full nose-up position at take-off and did not examine the trim tab actuators any further in order to confirm their position at impact.
Flap system
The left inboard and outboard flap control surfaces were destroyed by fire. The right inboard and outboard flaps had separated from the aircraft and broken into numerous sections during the impact sequence.
All four flap actuators were identified in the wreckage. The left inboard and outboard actuator outer bodies had been fire-damaged, however, their internal shafts and attachment points were present.
Initial on-site examination of the aircraft wreckage indicated the flaps were extended approximately 10°. More detailed analysis of the left inboard and outboard actuators, however, found they were likely in the fully retracted, UP position, when the aircraft collided with the building. An accurate assessment of the right-wing flap positions was not possible due to impact and fire damage.
Flight control locks
Remnants of the flight control locks including the locking pin for the control column, some chain and the ‘remove before flight’ warning sign were located to the rear of the co-pilot seat in the cockpit. In addition, the area surrounding the rudder locking pin receptacle was searched and the pin was not located.
Cockpit instruments and switches
Due to significant fire damage, the cockpit switch positions, instrument settings and cockpit trim indicator positions could not be determined. The available cockpit instruments were inspected and none retained any useful information.
Engine controls
An inspection of the remaining sections of the engine control pedestal and engine control linkages was performed from the cockpit through to the engines. There was significant disruption to the engine controls due to fire and impact damage. For that reason, continuity of the engine controls could not be fully established. No pre-impact defects, however, were identified in the remaining control sections.
The position of the power levers, condition levers, propeller levers and corresponding friction control knobs could not be accurately determined due to the extent of the damage.
The propeller control system was inspected in detail. The control system had fractured in overload in several locations due to propeller and engine separation during the accident sequence. There were no pre-impact defects identified within the propeller control system.
Engines
The left engine had separated from the aircraft and broken into three sections: the accessory drive with the compressor inlet, the compressor and turbine modules, and a forward section of the reduction gearbox which remained attached to the propeller (Figure 34). The engine had sustained significant impact and fire damage. An external inspection did not identify any pre‑impact defects.
Figure 34: Right engine assembly, shown upside down and viewed from its left side

Left propeller with attached forward section of reduction gearbox not shown. Source: ATSB
The right engine had detached from the aircraft and separated into two sections at the reduction gearbox. It sustained significant impact and fire damage (Figure 35). An external inspection of the engine was conducted with no pre-impact defects identified.
The engines were removed from the accident site and taken to a secure facility for further examination.
Figure 35: Right engine assembly, shown upside down and viewed from its left side

Right propeller with attached forward section of reduction gearbox not shown. Source: ATSB
Engine examinations
Both engines were retained by the ATSB for further examination in order to determine:
- if there were any defects present which could have contributed to the accident
- the engine power outputs at impact.
The PT6A-42 engine utilises a two-stage power turbine to drive the propeller shaft via a reduction gearbox (RGB) that is located at the front of the engine. The propeller shaft transmits torque from the engine’s reduction gearbox to the propeller.
The detailed engine examinations found
- no defects that were likely to have prevented normal operation of the engines
- there was similar evidence of rotation in both engines
- both propeller shafts had fractured at a similar position and the fracture surfaces appeared similar
- the left engine’s reduction gearbox planetary gears had indentations and tooth bending.
An accident investigator from the engine manufacturer, Pratt & Whitney Canada, travelled to Australia to assist with the examinations. The engine manufacturer’s report concluded that both engines were producing similar power at impact.
The reduction gearboxes were retained for further examination at the ATSB laboratories in Canberra (refer to section titled Appendix A - Reduction gearbox and propeller shaft assembly examinations).
Both engines’ fuel control units, fuel pumps, propeller governors, overspeed governors and torque limiter units were sent to the engine manufacturer for testing, where possible, followed by disassembly and inspection under the supervision of the Transportation Safety Board of Canada. The examinations did not identify any pre-impact faults that would have prevented normal engine operation.
Propellers
The left propeller was connected to a section of the reduction gearbox that had separated from the engine. The connected section housed the overspeed governor and propeller governor with its reversing lever and control linkage still attached. Inspection of those components and remaining controls did not identify any pre-impact issues.
All four blades remained attached to the propeller assembly (Figure 36). The propeller assembly was heavily sooted and charred, with heat damage to the de-ice boots and wiring. Three of the blades had portions of the tips fractured. All blades exhibited varying amounts of chordwise rotational scoring and leading edge gouging.
The propeller cut through roofing material and the supporting structure during the impact sequence, demonstrating significant rotational energy (Figure 37).
Figure 36: Left propeller viewed from the rear, showing blade-tip fractures, blade gouges and blade bending

Source: ATSB
Figure 37: Left propeller cuts through roof structure

Source: ATSB
The right propeller remained connected to a section of the reduction gearbox section that had separated from the engine. The propeller was located on the roof of the building.
The damage to the right propeller was similar to the left propeller but with less apparent heat damage (Figure 38). All four blades remained attached to the propeller assembly. All blades exhibited varying amounts of chord-wise rotational scoring and leading edge gouging.
Both propellers were retained for further examination by the ATSB.
Figure 38: Front view of the right propeller showing bending, chordwise twisting, and leading edge gouging of the propeller blades

Source: ATSB
Propeller examinations
Both propellers were examined in order to determine the level of power being produced by each engine at impact. An accident investigator from Hartzell Propeller travelled to Australia to assist with the subsequent propeller examination at an approved facility.
The propellers were four-blade Hartzell constant speed propellers Model HC-D4N-3A with D9383K blades installed on the aircraft under Raisbeck Engineering Supplemental Type Certificate SA2698NM. They had a feathering and reverse pitch capability.
Oil pressure from the propeller governor is used to reduce the blades’ pitch angles. A feathering spring and blade counterweight forces are used to move the blades to the high pitch/feather direction in the absence of governor oil pressure. The propeller utilises an aluminium hub with aluminium blades. Rotation is clockwise as viewed from the rear.
Both the left and right propellers exhibited similar damage consistent with high power output at impact. There were no discrepancies noted on either propeller that would have prevented or degraded normal operation prior to the impact. Blade and internal impact damage indicated both propellers impacted at positive blade angles of attack. At an estimated impact speed of 108 kt with the propellers at 2,000 RPM, preload plate impact marks suggest a geometric blade angle that was approximately equal to the engines take-off power of 850 horsepower.
Medical and pathological information
The pilot held a Class 1 Aviation Medical Certificate that was valid until 20 May 2017. The pilot was required to wear distance vision correction and have available reading correction while exercising the privileges of his licence.
The pilot’s CASA medical records indicated that he was diagnosed with Type 2 diabetes in 2007. At the time of the accident, the pilot was reportedly on multiple oral medications to manage his diabetes and was considered to have met the CASA requirements for maintaining his medical certificate. The records also showed that, as part of the pilot’s annual medical requirements, an echocardiogram was performed in 2016, which revealed an abnormal mitral valve. This was repaired in July of that year, with a post-operative follow-up identifying nil issues. CASA subsequently reviewed the pilot’s medical history and he was advised on 4 February 2017 that he could continue exercising the privileges of his licence, but should cease flying if there was a change in his treatment or condition.
The pilot’s post-mortem examination established that the pilot succumbed to injuries sustained during the impact sequence. Mild to moderate coronary artery atherosclerosis[22] was noted, along with signs of mitral valve annuloplasty.[23] There was no evidence, however, of any significant natural disease which may have caused or contributed to the accident. Further, the toxicology results did not identify any substance that could have impaired the pilot’s performance or that were not noted in the pilot’s CASA medical records. While post-mortem results for the passengers were not provided to the ATSB at the time of writing, given the injuries sustained by the pilot and the results of his post-mortem, the accident was not survivable.
The pilot’s family described him as being fit for his age and indicated that he regularly exercised.
Organisational information
Corporate & Leisure Aviation
Corporate & Leisure Aviation was solely operated by the accident pilot. The pilot generally flew the B200 aircraft and Piper Chieftains on charter flights, golf and fishing trips, and some corporate flights. A pilot who had previously worked with the accident pilot reported that he was a ‘one-man show’ and that he did not have many ‘outside influences’ or much checking. The accident flight was booked by a specialty golf tour company who had used Corporate & Leisure Aviation on several previous occasions.
Air operator’s certificate
A CASA AOC was re-issued to the accident pilot (certificate holder) on 17 July 2014, valid until 31 July 2017.[24] The AOC schedule stipulated that the certificate holder was approved to conduct charter operations within Australian territory and was authorised to operate several Australian-registered aircraft types and models, including the B200 aircraft.
The accident pilot was approved as the AOC holder’s Chief Pilot on 17 February 1999. A CASA review following the accident found that the AOC holder had no outstanding non-compliance notices (NCNs) or safety alerts.
CASA surveillance and non-compliance notices
A review of CASA records found they had conducted surveillance on the pilot’s AOC on 43 occasions since initial issue. On 5 November 2015, CASA conducted an audit of the AOC, and identified 11 findings, of which nine were NCNs. Of significance to this investigation was:
- NCN 713808: The operator did not have a flight check system approval, which was required for the B200 aircraft.
Flight Check System
A flight check system (FCS) is the combination of a specified operator’s activities, processes and documentation that together provide a system for the safe conduct of flight operations in a specified aircraft. Civil Aviation Regulations 1998 (CAR), regulation 232 Flight check system stated that:
- The operator of an aircraft shall establish a flight check system for each type of aircraft, setting out the procedure to be followed by the pilot in command and other flight crew members prior to and on take-off, in flight, on landing and in emergency situations.
- A flight check system shall be subject to the prior approval of CASA, and CASA may at any time require the system to be revised in such manner as CASA specifies.
- The pilot in command must ensure that the check lists of the procedures are carried in the aircraft and are located where they will be available instantly to the crew member concerned.
CASA further define an aircraft checklist and checklist procedure as:
Aircraft checklist is: The physical presentation of an efficient sequence of checks used to verify that the correct aircraft configuration has been established in specified phases of flight.
Checklist procedure for an aircraft is: The process by which the checks and the checklist are implemented efficiently and effectively.
CASA exempts some operators of the requirement to have a CASA-approved FCS, but they are not exempt from the requirement to establish and use a FCS (EX38/2004). With regard to the accident pilot’s AOC, the only aircraft required to have a CASA-approved FCS was ZCR.
In the case of commercial operations, the operator must ensure that the FCS is outlined in their operations manual. Also, if the information, procedures or instructions are contained in the AFM, then the operator must ensure that the operations manual refers to that AFM.
Non-Compliance Notice 713808
CASA records showed that NCN 713808 was issued to Corporate & Leisure Aviation (the operator) on 3 February 2016 and required an acceptable response to CASA within 30 days. CASA worked with the operator to achieve compliance and in December 2016, they received an updated operations manual with a section addressing checklist requirements for the B200 aircraft. Appendix B0-1 to the operations manual stated that, for ZCR:
The currently approved CASA check lists for both Normal and Emergency Procedures will be used at all times. Copies of checklists are readily accessible to pilots in the cockpit of all company Aircraft, and a copy is also available in the company reference library. Checklists are in a tabbed booklet format suitable for use on the pilot’s knee, and include tabbed emergency procedures at the back for easy access. The currently approved CASA checklist is the manufacturer’s checklist P/N 101‐590010‐157E issued July 1996.
CASA indicated this was an acceptable means of compliance and closed NCN 713808 on 20 December 2016 in their internal tracking system. The operator was not formally advised that the NCN had been closed, and a CAR 232 approval was not issued at this time. CASA correspondence with the operator indicated that they intended to inspect the checklist in the aircraft prior to the approval being issued, however, this did not occur before the accident flight.
The ATSB sought further clarification from CASA regarding the acquittal of NCN 713808 and were advised that a CAR 232 approval had been issued to the operator in 2006, however, the FOI who issued NCN 713808 was not aware of this approval. This approval referenced checklist part number 101-590010-157E.
ZCR checklists
The aircraft manufacturer advised the ATSB that the checklist, referenced by part number 101‑590010-157E, in the CASA CAR 232 approval and the operators manual was the incorrect checklist for ZCR. The manufacturer further advised that that they had no record of a quick reference checklist being purchased for ZCR; it was possible, however, that the operator obtained a checklist from another source.
Due to fire damage to ZCR, the ATSB could not determine which checklist was in the aircraft. The aircraft manufacturer provided a copy of the checklist referenced in the operations manual, a copy of the correct checklist by serial number for ZCR, 101-590010-309F, and a copy of a POH applicable to ZCR. The manufacturer advised that the checklists were unlikely to contain checks related to modifications to the aircraft such as the CVR. The three checklist sources were compared and it was found that, in regard to the rudder trim and weight and balance items, the checklists were identical. None of the checklists contained CVR checks.
A summary of checklist items required to be performed before take-off, related to the rudder trim and the aircraft’s weight and balance is below (Table 3). When followed, the checklists required the position of the rudder trim be checked five times and the weight and balance of the aircraft be checked once before take-off.
Table 3: Checklist item summary
| Checklist | Rudder trim | Weight and Balance |
| PREFLIGHT INSPECTION | Trim Tabs - SET TO “0” UNITS & Rudder, Rudder Tab… - CHECK |
- |
| BEFORE ENGINE STARTING | …Rudder trim controls - SET | Weight and C.G. - CHECKED |
| ENGINE STARTING | - | - |
| BEFORE TAXI | - | - |
| BEFORE TAKEOFF (RUNUP) | Trim Tabs - CONFIRM SET | - |
| BEFORE TAKEOFF (FINAL ITEMS) | Trim - CONFIRM SET | - |
Operational information
Yaw damper and rudder boost operation
The ATSB was unable to determine whether the yaw damper was engaged on the accident flight or when the pilot normally engaged the yaw damper (refer to section titled Aircraft wreckage – Cockpit instruments and switches). There was no evidence found to support a rudder boost malfunction (refer to section titled Aircraft wreckage – Rudder boost system inspection).
Both systems could be disconnected by the pilot and the aircraft manufacturer advised that the pilot should have easily been able to overcome forces generated by the rudder boost and yaw damper systems.
B250 flight simulator
In order to determine the effects of full left rudder trim on take-off and climb performance, a flight was performed in a King Air 250 Level D flight training simulator[25]. The simulator performance was similar, though not identical to ZCR. The accident weather, airport location and maximum take-off weight were used to make the flight conditions as similar as possible to the accident flight. The pilot who performed the flight commented that:
The yaw on take-off was manageable but at the limit of any normal control input. Should have rejected the take-off. After take-off the aircraft was manageable but challenging up to about 140 knots at which time because of aerodynamic flow around the rudder it became uncontrollable. Your leg will give out and then you will lose control. It would take an exceptional human to fly the aircraft for any length of time in this condition. The exercise was repeated 3 times with the same result each time. Bear in mind I had knowledge of the event before performing the take-offs.
The pilot also stated that it could be possible for a pilot to misinterpret the yaw as being caused by an engine power loss rather than from a mis-set rudder trim.
Sideslip effects on performance
An increase in an aircraft’s sideslip angle will decrease aerodynamic efficiency and aircraft performance. It was not possible to quantify the effects on ZCR without flight testing or complex engineering modelling. Both these options were outside the scope of the investigation and this information was not held by the aircraft manufacturer.
A sideslip will affect aircraft performance in a number of ways, including by:
- reducing thrust, due to the change in propeller inflow angles
- increasing form drag[26] as a greater surface area of the aircraft is facing the relative airflow (Figure 39 and Figure 40)
- reducing the amount of wing available to produce lift, due to the fuselage and engine cowls blanking airflow to portions of the wing (Figure 41)
- creating a rolling moment (in the case of a nose-left yaw it will create a left wing-down rolling moment).
Opposite aileron input would have been required to keep the wings level during the observed sideslip in this event. This aileron input will have the effect of further increasing drag on the aircraft.
Figure 39: Image of exemplar aircraft taken directly front on showing the profile facing into the relative airflow

Source: ATSB
Figure 40: Image of exemplar aircraft taken at an angle of 30o showing the increase in engine cowl fuselage and vertical tail surface that would be exposed to the relative airflow with a sideslip of 30o

Source: ATSB
Figure 41: Diagram showing sections of the wing that will be blanked by a 30o yaw angle excluding the effect of the propeller wash

Note: As a result of the propeller wash straightening out the airflow over sections of the wings, they will not receive as much blanking as is depicted in the diagram. Source: ATSB
Take-off weight estimations
A copy of the passenger/cargo manifest and load sheet for the accident flight, that was required to be left at the aircraft’s departure airport, was not located. Consequently, the ATSB estimated ZCR’s weight and balance based on a combination of known and estimated weights of the pilot, passengers, baggage, and fuel on board. From this, it was estimated that ZCR’s weight at the beginning of the flight was about 240 kg above the aircraft’s maximum take-off weight of 5,670 kg.
The occupant seating positions were established from information provided by Victoria Police. This information indicated the front right or co-pilot seating position was unoccupied. ZCR’s balance charts did not allow a centre of gravity[27] position to be determined for an aircraft above its maximum take-off weight. The charts were extrapolated, however, and assuming the forward and aft centre of gravity limits remained linear at higher weights, ZCR was determined to probably be within the forward and aft centre of gravity limits.
While the golf tour organiser provided their clients with limitations on baggage weights, they reported that the pilot had previously used scales to weigh bags. The organiser indicated, however, that they were not aware of any further checks conducted by the pilot. CCTV footage of the passengers arriving at the airport did not show their bags being weighed. The ATSB was unable to confirm if the pilot had verified the aircraft’s weight and balance prior to departing.
Take-off performance estimations
The ATSB estimated the ground roll distance and climb performance expected for ZCR on the day of the accident. The following conditions were used to establish these estimates:[28]
- The pilot was reported to use ‘APPROACH flap’ for take-off. However, as the flaps were found in the UP position and this setting was recommended by the aircraft manufacturer for this take‑off, ‘flaps UP’ was used for the estimates.
- The ATSB’s take-off weight estimate (refer to section titled Operational information - Take-off weight estimations).
- While a review of the meteorological information identified that the wind conditions could have ranged from 0 kt to no more than a 5 kt tailwind. The worst-case scenario of a 5 kt tail wind was used.
The figures were manually extracted from the performance charts contained in Section V – Performance of the Raisbeck Engineering B200 POH and AFM supplement (85‑116). As the charts did not account for take-off weights greater than the maximum take-off weight, these figures were extrapolated. The resultant figures should not be considered as absolute, but rather as an estimate due to charting errors and extrapolation.
Based on the worst-case scenario of the higher take-off weight and a 5 kt tailwind, the ground roll should have been about 594 m.[29] This was only 5 per cent more than the distance calculated for ZCR at its maximum take-off weight, however the actual ground roll estimated by the ATSB from ADS-B data and CCTV footage was 71 per cent longer (refer to section titled Air traffic services information – Automatic Dependent Surveillance Broadcast data). These calculations demonstrate that the higher take-off weight alone did not result in the delayed take-off.
With regard to ZCR’s climb performance, the expected best rate of climb performance with both engines operating and the landing gear retracted was estimated as 2,360 feet per minute. Textron Aviation Inc. advised the ATSB that the climb penalty for having the landing gear extended was 630 feet per minute. Consequently, ZCR’s expected climb performance should have been about 1,730 feet per minute. These figures assume that maximum continuous power was set on both engines and the two-engine best rate of climb speed of 121 kt was maintained.
The aircraft manufacturer also provided the ATSB with the aircraft’s expected take-off performance. While some of the variables used to establish these figures differed from that used by the ATSB, most likely as the most up-to-date information was not available at that time, a broad comparison of the results showed that they were reasonably consistent.
Fuel-related information
At 0743 on the morning of the accident, a refuelling agent received a telephone request from the pilot for fuel to be uplifted into ZCR. Between 0750 and 0806, a total of 705 L of JetA1 was uplifted to the main tanks and a total of 401 L was uplifted to the auxiliary tanks. The ATSB determined that after refuelling the main tanks were likely full and the auxiliary tanks contained 401 L.
A complete daily check of the fuel quality was conducted at 0550 and 1210. That check established that the fuel from the fuel truck was ‘clear bright’ in appearance, and there was nil water or sediment present. An additional check was conducted soon after the accident, at 1000, which did not identify any contamination.
There were no reports of aircraft having refuelled at Essendon experiencing fuel-related issues around the time of the accident flight.
Pre-flight inspections and before take-off checks
Cockpit checklists are an essential tool for overcoming limitations of pilot memory, and ensuring that action items are completed in sequence and without omission. According to Degani & Wiener (1990):
The major function of the flight deck checklist is to ensure that the crew will properly configure the airplane for any given segment of flight. It forms the basis of procedural standardization in the cockpit.
Nagano (1975), cited in Degani & Wiener (1990), also stated that another objective of an effective checklist was to promote a positive attitude to the use of checklists. This relied on the checklist not only being ‘well grounded’ in the current operating environment, but also the checklist user understanding the importance of the checklist rather than regarding it as a nuisance task.
Checklist devices have evolved over the years and range from paper to electronic formats. The paper checklist is commonly used and consists of a list of items written on paper card. One of the key disadvantages of the paper checklist is that there is no mechanism for pilots to distinguish between checklist items that have been completed and those that have not. Further, pilots, in particular experienced pilots, may be tempted to memorise the checklist to avoid the burden of reading it from the card (Degani & Wiener, 1990). Irrespective of the device employed, generally, there are two distinct checklist methods:
- Challenge-response: Flight-phase related actions are performed by the pilot from memory and the checklist is then used to verify that critical items have been correctly performed. For multi‑crew operations, this may involve the pilot monitoring reading the item to be checked and the pilot flying confirming the status or configuration of that item (Hawkins, 1993).
- Read-and-do: A method for leading and directing the pilot in configuring the aircraft using as a ‘step-by-step, cookbook approach’. For multi-crew, this may involve one pilot calling for an item, and the other pilot setting that item and verbalising its status (Degani & Wiener, 1990).
With regard to the use of checklists in this accident, the pilot’s operations manual stated that:
The Pilot in Command shall ensure that the aircraft checklist is carried out in detail for every flight – this includes private, aerial work and charter operations. The method of carrying out the checklist shall be “Read and Do” or “Do and Check” for all flights.
PREFLIGHT INSPECTION checklist
As the accident flight was the first flight of the day, all items on the PREFLIGHT INSPECTION checklist [30] had to be completed. CCTV footage captured ZCR parked outside near the maintenance provider’s hangar on the morning of the accident. The pilot was observed arriving at ZCR and walking around the aircraft and entering the cabin. This suggested that the pilot was conducting a pre-flight inspection. The specific details of that inspection could not be determined, however, due to the aircraft’s distance from the camera.
The PREFLIGHT INSPECTION checklist included setting the trim tabs in the cockpit to ‘0’ units then visually checking the rudder and rudder tab when conducting the external walk-around (Figure 42). An example of a B200 checklist used by an Australian operator called for a ‘function check’ of the manual trim system to be performed, which included the rudder trim. A previous employee of this operator indicated that the function check for the rudder trim involved moving the trim wheel from full left to full right deflection and then back to the centre position. Any subsequent checks of the trim were to confirm that they were correctly set. Another pilot who had operated ZCR also indicated that he would exercise the limits of the trim systems during the pre-flight inspection. The ATSB was unable to determine the accident pilot’s practices with regard to checking the trim positions during the pre-flight inspection.
Figure 42: B200 rudder with rudder trim tab set to the full nose-left position

Images taken while standing at the rear of the aircraft. Source: ATSB
BEFORE ENGINE STARTING and BEFORE TAXI checklists
The BEFORE ENGINE STARTING checklist included;
- confirming the rudder trim controls were set
- checking the aircraft’s weight and centre of gravity
- checking that the flight control locks were removed
- checking the rudder boost and elevator trim switches were ON.
The BEFORE TAXI checklist included checking and setting the flaps, and checking the flight controls for freedom of movement and proper direction of travel.
BEFORE TAKEOFF (RUNUP) checklist
Similar to the PREFLIGHT INSPECTION checklist, all items on the BEFORE TAKEOFF (RUNUP) checklist were to be completed for the accident flight. Items on this checklist included;
- checking the autopilot and yaw damper
- checking the electric elevator trim
- confirming the trims tabs were set
- checking and testing the functionality of the primary governors, overspeed governors and rudder boost system
- checking and arming the autofeather system.
Some of these checks required the aircraft’s engines to be increased to a relatively high power setting to test a number of systems. Consequently, the checks would typically be performed away from any persons and other aircraft.
A number of experienced B200 pilots were consulted regarding the conduct of these checks. Some of these pilots reported that the checks should be performed when the aircraft was stationary, such as in the designated run-up bay. While others indicated that the checks could be done while taxiing or at the holding point. Similarly, the Essendon Tower controllers also stated that they have observed pilots of turboprop aircraft utilise both options. They further commented that it was not unusual for pilots to taxi directly to the holding point and report ready for take-off, without entering the run-up bay.
The CCTV footage of ZCR parked outside showed the left engine being started, followed by the right engine 1 minute later. About 2 minutes after this, the taxi toward the passenger terminal was commenced. A person positioned in an adjacent hangar provided no indications that the BEFORE TAKEOFF (RUNUP) checks were conducted at this time. Similarly, there was no indication from the ATC audio recordings that the pilot had requested a clearance to conduct run-ups either on the apron or in the designated run-up bay. Further, the ADS-B data did not show the aircraft stopping at any stage while taxiing to the terminal or, later, the holding point, which would have been consistent with conducting stationary engine run-ups. A pilot who also observed ZCR taxiing to the holding point, stated that he did not hear any run-ups, but had also considered that they may have been completed prior to that time.
BEFORE TAKEOFF (FINAL ITEMS) checklist
The BEFORE TAKEOFF (FINAL ITEMS) checklist included confirming the autofeather was armed, and the trims and flaps were set as required.
TAKEOFF checklist
After take-off, the TAKEOFF checklist called for the landing gear to be retracted when a positive rate of climb was established and then for the flaps to be raised when at a minimum speed of 121 kt (indicated airspeed). The accident pilot had previously advised the ATSB that it was his standard practice for take‑off to use ‘one stage of flap because it gets me off the ground quicker’. The last recorded flight on the cockpit voice recorder and the pilot’s CASA-Approved Testing Officer also confirmed that he used flap for take-off.
Checklist discipline
When discussing the importance of checklists, Hawkins (1993) stated that:
It is widely accepted that the proper, disciplined use of cockpit checklists is an essential element in flight safety. This reflects the view of the aircraft manufacturer, regulatory agencies, pilot bodies and airlines. It is a concept long accepted in civil aviation…In spite of this general agreement on the significance of the checklist to flight safety, lack of proper checklist discipline remains a major issue.
In previous correspondence between the accident pilot and the ATSB when discussing checklists, the pilot stated that:
…You don’t get complacent as a pilot but you get into a routine. The same as your pre-take-off checks, you get a routine and you don’t need to use a checklist because you are doing it every day, you are flying it every day… I take-off with one stage of flap because it gets me of the ground quicker. And I never change my routine...
Given the above comments previously made by the pilot, the ATSB received information from numerous persons who flew with the pilot in order to establish his use of checklists. A summary of their comments is below:
- An engineer who flew with the accident pilot on a post maintenance check flight reported that the pilot elected not to conduct the BEFORE TAKEOFF (RUNUP) checks as they had already been done earlier in the day. The engineer also commented that they took off with the pressurisation system incorrectly set and during the flight he noticed that the right wing locker was open. Reportedly, the pilot did not refer to a checklist throughout the flight.
- A previous passenger reported that the pilot did not close the main cabin door until he was prompted by that passenger just prior to take-off. The cabin door is required to be checked in the BEFORE ENGINE STARTING checklist. Further, when the door is open, a red DOOR UNLOCKED warning light will illuminate on the annunciator panel in the cockpit to alert the pilot.
- Another pilot reported having a conversation with the accident pilot about the use of checklists when hiring a B200 aircraft. When confirming if there was a checklist in the aircraft, the accident pilot indicated that he did not believe in checklists. He further commented that he felt comfortable with flying the aircraft and did not believe the checklist was necessary. However, the ATSB was unable to establish if the accident pilot was indicating that he would use his own checklist or would rely on memory to perform the checklist items.
- The accident pilot’s CASA-approved testing officer advised that the pilot would use a checklist the majority of the time, though he could not recall if the pilot used the aircraft’s checklist or his own.
- Another pilot who flew with the accident pilot on occasion indicated that he had observed the pilot using the checklist that was approved in his operations manual at that time.
- A pilot (co-pilot) who flew with the accident pilot (captain) on the last flight recorded on ZCR’s cockpit voice recorder also stated that they had used a checklist. A review of that recording also showed the captain and co-pilot appeared to be using the ‘challenge and response’ checklist methodology. The co-pilot read the item to be checked and the captain confirmed the status of the item.
- During the conduct of the pilot’s instrument proficiency checks in October and November 2015, the CASA flight operations inspector noted that the pilot was using a laminated checklist with what appeared to contain the abbreviated normal procedures.
While there was variable evidence showing the pilot’s checklist discipline, the ATSB was unable to establish if he was using a checklist on the accident flight or if he relied on memory to action checklist items.
Why checklists are not completed
Checklists are an essential defence against pilot errors, however, this can sometimes fail. Various research studies have provided insights as to why checklist procedures may not always be completed, including:
- Attitude: Hawkins (1993) highlighted that, ‘probably the greatest enemy of error-free, disciplined checklist use is attitude – a lack of motivation…to use the checklist in the way it should be used’.
- Distractions and interruptions: Distractions and interruptions can result in a disruption to the sequential flow of the checklist. This not only means that the pilot will have to memorise the location of that disruption, but it may also lead to a checklist error or omission (Degani & Wiener, 1990).
- Expectation and perception: Degani & Wiener (1990) found that, when the same task is performed repetitively, such as a checklist, the process becomes automatic. The user will create a mental model of that task, and with experience, this model will become more rigid, leading to faster information processing and the ability to divide one’s attention. While this will ultimately reduce the user’s workload, this model may adjust or even override ‘seeing what one is used to seeing’. In the study conducted by Degani & Wiener (1990), many of the pilots interviewed commented that they had seen a checklist item in the improper status, but perceived it to be in the correct status. For example, the flaps were set at zero, but the pilot perceived them to be at the 5° position as this was what they were expecting to see.
- Time pressures: The speed of performing the checklist may affect the accuracy of the check. For example, if a pilot scans the item to be checked quickly due to time pressures, the accuracy of the pilot’s perception will degrade and the possibility of error will increase (Degani & Wiener, 1990).
A study was conducted by Dismukes & Berman (2010) to explore why checklists (and monitoring) sometimes fail to catch errors and equipment malfunctions. One of the study’s authors conducted 60 observation flights from the cockpit jumpseat of three airlines. These observations identified 899 deviations, of which 22 per cent were related to checklist use. Checklist deviations were mainly associated with the pre-taxi, taxi-out, descent and approach phases of flight. The identified deviations were categorised into six types and the results are presented below and in Figure 43:
- Flow-check performed as read-do: Normal checklist procedures generally require pilots to check and/or set the items in a sequence or flow. After completing this flow, the checklist is performed to confirm that the critical items have been correctly actioned. However, if the flow is not performed and only the checklist is completed, items not on the checklist will be omitted.
- Responding without looking: The authors described two situations when this may occur. The first is when a pilot responds from memory of having recently set or checked that item as part of the flow. Basically, the current situation may be confused with the previous situation. Secondly, a pilot may look directly at the item to be checked, but perceive it to be in the correct position when it is not. A pilot may respond without looking due to habit or when under time pressures.
- Checklist item omitted, performed incorrectly, or performed incompletely: The pilot’s response is incorrectly worded, one or more elements of a multi-item response are omitted or combined into a single response, or the checklist is not verbalised completely. The research found that, while in some cases the checklist item was deferred and later forgotten, in other instances the checklist was interrupted by external influences and an item was disregarded. In contrast, on many occasions an item was omitted when no external disruption occurred.
- Poor timing of checklist: The checklist is conducted at the wrong time or at a time that interfered with higher priority tasks, or it was self-initiated at the incorrect time.
- Checklist performed from memory: Similar to that identified by Degani & Wiener (1990), when a pilot has completed a checklist many times, performance becomes mainly automatic, fast and fluid, and requires minimal cognitive effort. Forcing oneself to read each checklist item may be awkward, effortful and time-consuming. Therefore, pilots may be inclined to perform the checklist from memory rather than from the physical checklist.
- Failure to initiate checklists: Failing to initiate a checklist may be the result of distractions, other competing demands on the pilot’s attention, or due to circumstances forcing procedures to be performed out of sequence.
Figure 43: Dismukes & Berman (2010) checklist deviations

Source: Dismukes & Berman (2010), modified by the ATSB
The authors also evaluated the consequence of just more than half of the flights observed. Of these, 89 per cent had no discernible outcome other than a minor reduction in the effectiveness of defences. However, 9 per cent resulted in an undesired aircraft state. These included mis‑configuration of an aircraft system from failing to set a switch correctly during a flow. Some of these items were on checklists and were missed in both the flow and checklist. This shows that experienced pilots are not immune to checklist deviations.
Related occurrences
A review of the ATSB’s occurrence database and the United States’ National Transportation Safety Board’s (NTSB) online database identified three potentially similar accidents that involved an aircraft taking off with the rudder trim not correctly set.
Australian occurrence
Loss of control, 7km west-south-west of Tamworth Airport, New South Wales, on 7 March 2005, VH-FIN (ATSB investigation 200501000)
At about 1326 Eastern Daylight-saving Time on 7 March 2005, the pilot of a Cessna Aircraft Company 310R, registered VH-FIN, took off from runway 30 Right at Tamworth Airport, for Scone, New South Wales. Approximately 1 minute after becoming airborne, the pilot reported flight control difficulties. At about 1329, the aircraft impacted the ground in a cleared paddock about 7 km west-south-west of the airport. The pilot was fatally injured and the aircraft was destroyed by the impact forces and post-impact fire.
Examination of the aircraft's mechanical flight control systems, autopilot and electric trim system did not reveal any evidence of pre-impact malfunction. Those results, however, were inconclusive due to the extensive impact and fire damage.
A periodic maintenance inspection carried out in the days before the flight resulted in the rudder trim tab being set at the full right position and possibly aileron and elevator trim tabs being set at non-neutral positions prior to the flight. There were indications that the pilot was rushed and probably overlooked the rudder and aileron trim tab settings prior to takeoff. The aircraft flight path reported by witnesses was found to be consistent with the effect of abnormal rudder and/or aileron trim tab settings.
United States occurrences
Loss of control in-flight, Hayward, California, 16 September 2009, B200 N726CB, (NTSB accident number WPR09LA451)
The aircraft had just undergone routine maintenance and this was planned to be the first flight after the inspection. During the initial climb, the pilot observed that the aircraft was drifting to the left. The pilot attempted to counteract the drift by application of right aileron and right rudder, but the aircraft continued to the left. The pilot reported that, despite having both hands on the control yoke, he could not maintain directional control and the aircraft collided into a building. The aircraft subsequently came to rest on railroad tracks adjacent to the airport perimeter.
A post-accident examination revealed that the elevator trim wheel was located in the 9-degree NOSE-UP position; normal take-off range setting is between 2 and 3 degrees NOSE-UP. The rudder trim control knob was found in the full left position and the right propeller lever was found about one-half inch forward of the FEATHER position; these control inputs both resulted in the airplane yawing to the left.
The pilot did not adequately follow the aircraft manufacturer's checklist during the pre-flight, taxi, and before take-off, which resulted in the aircraft not being configured correctly for take-off. This incorrect configuration led to the loss of directional control immediately after rotation. A post‑accident examination of the airframe, engines, and propellers revealed no anomalies that would have precluded normal operation. The pilot was the only person on-board and he was uninjured.
Runway excursion, Oneida, Tennessee, 25 September 2014, Beech C90, N211PC (NTSB accident number ERA14CA458)
According to the pilot's written statement, he departed runway 05 and the airplane veered ‘sharply’ to the right. The pilot assumed a failure of the right engine and turned to initiate a landing on runway 23. Seconds after the aircraft touched down it began to veer to the left. The pilot applied power to the left engine and right rudder, but the aircraft departed the left side of the runway, the right main and nose landing gear collapsed and the aircraft came to rest resulting in substantial damage to the right wing. The pilot reported that he had failed to configure the rudder trim prior to take-off and that there were no pre-impact mechanical malfunctions or anomalies that would have precluded normal operation. The pilot was the only person on-board and he was uninjured.
__________
- ATSB Transport Safety Report Near-collision and Operational Event involving Beech Aircraft Corp. B200, VH-OWN and Beech Aircraft Corp. B200, VH-LQR, Mount Hotham Victoria on 3 September 2015 AO-2015-108.
- Notice(s) to Airmen (NOTAM): A notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personal concerned with flight operations.
- The Type Certificate holder is responsible for the design and continued airworthiness support of the aircraft.
- Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 170 equates to17,000 ft.
- Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
- The Airservices Manual of Air Traffic Services, Section 3.1.1.6, stated that the term ‘variable’ was used when it was not possible to report a mean wind direction such as, in light wind conditions (3 kt or less) or if the wind was veering or backing by 180° or more (e.g. passage of thunderstorm or localised wind effect).
- An instrument used for measuring the velocity of moving air. This particular installation was owned and operated by the Bureau of Meterology.
- Transponder: A receiver/transmitter, which generates a reply signal upon proper interrogation; the interrogation and reply being on different frequencies. Mode S has altitude capability and also permits data exchange.
- An aircraft static system comprises sensors which detect the ambient air pressure unaffected by the forward motion of the aircraft.
- www.healthdirect.gov.au/coronary-heart-disease-and-atherosclerosis
- Mitral valve annuloplasty is a surgical technique used to repair leaking mitral valves.
- The pilot was first issued with an AOC on 8 June 1995.
- There are four levels of full flight simulator, levels A - D, level D being the highest standard
- Form drag or pressure drag is the drag caused by the separation of the boundary layer from the surface of an object and the wake created by that separation. Form drag is reduced by the use of streamlined shapes, so that the boundary layer remains attached to the object for as long as possible, in addition to creating the smallest profile facing into the relative airflow.
- The centre of gravity (CG) of an aircraft is the point over which the aircraft would balance if it was possible to suspend it at that point.
- The ATSB established a number of estimates based on a variation of the conditions detailed herein. However, for the purposes of the report, the most reasonable estimate is only presented.
- Take-off performance figures assume that take-off power was set prior to brake release, the landing gear was not retracted, and the runway surface was paved, level and dry.
- The checklists mentioned herein does not include all checklists required to be actioned by pilot. It only includes those specifically related to certain aspects of the occurrence.
Introduction
After a delayed lift-off from runway 17, VH-ZCR (ZCR), was observed in a substantial sideslip to the left. Control of the aircraft could not be maintained, and shortly after, it collided with the roof of a building in the Essendon Airport, Bulla Road Precinct - Retail Outlet Centre (outlet centre).
The ATSB established that the pilot was appropriately qualified to perform the flight. The ATSB did not find any evidence of pilot incapacitation or a mechanical fault with the aircraft that contributed to the accident. Further, it was unlikely that the weather conditions influenced the development of the accident.
This analysis will examine the possible reasons for the left sideslip and its consequence on aircraft control and performance. It will also discuss the serviceability of the cockpit voice recorder (CVR), the aircraft’s take-off weight, and the operator’s flight check system. The proximity of the outlet centre to Essendon Airport will also be analysed.
The occurrence
Ground roll, flight path and aircraft attitude
Automatic Dependent Surveillance Broadcast (ADS-B) data and closed-circuit television (CCTV) footage revealed ZCR reached the required rotation speed of 94 kt when about 730 meters from the threshold of runway 17. The aircraft then remained on the ground for an additional 285 meters and rotated at 111 kt. The data also showed that, at some point between 470 m and 920 m from the threshold, ZCR’s ground track began to veer left from the runway centreline.
At rotation, a witness familiar with the aircraft type observed a yaw to the left followed by a relatively shallow climb. The ATSB’s analysis of ZCR’s flight path profile and the impact sequence found that, the aircraft had minimal sideslip for the initial climb followed by substantial sideslip for the later part of the flight and at impact. The analysis also found there was minimal left roll, not exceeding 10° for the duration of the flight.
Aircraft performance
ZCR’s actual take-off roll, to the required rotation speed of 94 kt, was about 136 m longer than the ATSB’s estimated distance of 594 m. However, the estimated distance did not account for the rolling take-off conducted by the pilot or possible drag penalties resulting from the mis-set rudder trim. Considering these factors, it was likely that ZCR accelerated as expected, with both engines producing take-off power, to 94 kt.
The ADS-B data indicated that ZCR reached a maximum height of no more than 160 ft. The ADS‑B barometric altitude data became unreliable following the onset of the sideslip at 125 ft, however, CCTV footage and Global Positioning System rate data indicated ZCR maintained a brief and shallow climb after this point. The initial climb rate was broadly consistent with the expected performance of the aircraft with the landing gear down, allowing for a minor out of balance condition, not maintaining the best rate of climb airspeed and tolerances in the data. Following the onset of the sideslip, ZCR began a descent followed by the collision with the outlet centre building.
The data also showed an increased divergence from the runway centreline when airborne and a reduction in aircraft acceleration, rate of climb, and airspeed following the commencement of the sideslip. This was consistent with the theoretical effects of a substantial left sideslip on ZCR’s performance.
Engine power
Asymmetric engine power can result in a yawing moment in a twin-engine aircraft. As a substantial sideslip was observed by witnesses and later confirmed through CCTV footage analysis, the possibility of a left engine power reduction was considered.
A reduction in left engine power would have exacerbated the left yaw, however, this was discounted as the key witnesses reported that the engine/s sounded normal and the ATSB’s dashboard camera audio frequency analysis detected no change in engine sound. In addition, engine and propeller impact evidence support the left engine producing take-off power at impact.
There was no evidence to indicate that the left yaw was the result of an asymmetric engine power condition.
Rudder
Given the substantial left sideslip and no evidence of an asymmetric engine power condition, the ATSB considered various inputs to the rudder system that could induce the sideslip. These included:
- the yaw damper system
- the rudder boost system
- manipulation of the rudder pedals by the pilot
- rudder trim position.
There was no evidence to support a yaw damper or rudder boost malfunction. In addition, the aircraft manufacturer advised that these systems could be physically overpowered by the pilot or the respective systems turned off. Application of left rudder by the pilot was also considered unlikely as there was no evidence to support, or plausible reason identified to account for the pilot applying left rudder and maintaining this input until impact.
The on-site and post on-site examinations of the aircraft found that the rudder trim was in the full nose-left position at the time of impact. This was consistent with the substantial sideslip at impact, derived from the roof collision marks. As the ATSB established that ZCR’s engines were capable of normal operation and were operating at similar settings, there was no apparent reason identified, such as an asymmetric power condition that would have required the use of full rudder trim by the pilot.
A malfunction of the rudder trim system resulting in a full nose-left setting was also considered unlikely, as the rudder trim control system is manually operated by the pilot. The system has no connection to the autopilot/yaw damper or electric trim systems.
As it was unlikely that the pilot had set full nose-left trim during or after take-off, the rudder trim was probably mis-set in the full nose-left position prior to take-off.
Mis-set rudder trim
Some previous occurrences have shown that a mis-set trim situation has occurred as a result of maintenance performed on the aircraft immediately prior to the flight. It was considered unlikely in this occurrence, however, as maintenance had not been performed on ZCR since 5 February 2017 and the aircraft had flown in the intervening time.
While the ATSB could not exclude the possibility that the rudder trim had been manipulated by unknown persons prior to the accident flight, the aircraft had been stored in a secure hangar until the previous afternoon. After this, ZCR was parked outside the hangar within the confines of the airport. Consequently, the ATSB considered actions performed by the pilot prior to take-off.
Prior to take-off, there were several opportunities in the pre-flight inspection and before take-off checklists for the pilot to set and confirm the position of the rudder trim. A review of the CCTV footage showed the pilot moving in and around ZCR when parked outside the hangar, consistent with performing a pre-flight inspection. The pre-flight inspection required the rudder trim to be set in the cockpit and the external trim tab to be visually inspected. The ATSB was unable to determine if the rudder trim was in full nose-left prior to the pilot arriving at the aircraft or if the pilot inadvertently left the trim in that position. In any case, the visual inspection of the rudder trim tab was an opportunity to identify the mis-set trim. From the footage, it could not be established if the PRE-FLIGHT INSPECTION checklist was followed completely.
Further, a review of the witness observations, ADS-B data and air traffic control audio recordings found no evidence to suggest that the BEFORE TAKEOFF (RUNUP) checks had been completed by the pilot. However, the ATSB could not discount that they were done while parked at the passenger terminal or during taxi.
The pilot’s practices with regard to setting and confirming the position of the rudder trim, such as performing a function check, could not be established. Further, while there was some evidence to indicate that the pilot may have relied on memory to perform checks rather than reference physical checklists or that he did not always complete checklists, it was unknown if this practice was applied on the accident flight.
Previous findings by Dismukes et al (2007) cited in Dismukes & Berman (2010) have found that accidents very rarely occur due to one single error but rather, from the convergence of task demands, coincidental events, organisational factors and human factors. As research has shown, a diverse range of factors can lead to checklist deviations such as distractions, interruptions, time pressures, expectations, and relying on memory. While the ATSB was unable to establish why the rudder trim on ZCR was in the full nose-left position, a distraction or interruption may have influenced the pilot’s check actions. Despite this, however, there were several opportunities in the pre-flight and before take-off checklists to check and correct the trim position.
Of note, the on-site examination of ZCR also found the flaps in the UP position, though it was the pilot’s normal practice to use APPROACH flaps for take-off. It could not be discounted that the flaps were retracted after take-off, but unlikely given the short time frame from take-off to the accident, and the pilot’s likely focus of attention on attempting to control the aircraft with the mis‑set trim condition. However, the ATSB was unable to establish if the pilot had purposely elected not to use flaps for take-off in this case or if this item was possibly missed or forgotten when performing his checks.
Loss of control
As the aircraft’s airspeed increased during the take-off roll, and airflow over the control surfaces increased, the rudder trim would have become more effective. It is likely this would have resulted in an increasing tendency for the aircraft to veer or yaw to the left. This would have required the pilot to apply right rudder pedal input to maintain the runway centreline using the nose wheel steering. The divergence left of centreline observed on the ADS-B data could support the rudder trim having an influence on ZCR’s heading during the take-off roll.
As previously established, ZCR accelerated as expected to the rotation speed of 94 kt. The aircraft was not rotated at this point, however, but rather at 111 kt and 1,015 m along the runway. For the B200 aircraft, the rotation speed is also the take-off decision speed, by which time any decision to reject a take-off must be made. For example, if an engine failure occurs at or below this speed, the take-off should be rejected. Above this speed, however, the take-off must be continued unless the pilot believes the aircraft will not fly.
It was possible that the pilot expected, either through training or previous experience, that the most likely reason for a yaw on the take-off roll was due to asymmetric engine power rather than a mis-set trim. This would not have been reflected on the cockpit instruments, however, as the engines were likely to have been operating normally. This conflicting information could have confused or distracted the pilot resulting in a delay in rotating while troubleshooting. Diagnosing an unknown issue during a critical phase of flight would have been challenging. As the aircraft approached 111 kt, the pilot may have considered that there was insufficient runway remaining to safely reject the take-off without the risk of a runway overrun. There was insufficient evidence to determine why the pilot delayed rotation from 94 kt to 111 kt or why the take-off was not rejected. This accident highlights the decision-making challenges during critical stages of flight, especially when faced with a novel or unusual problem.
After take-off, it was likely that the pilot was applying right rudder pedal in an attempt to compensate for the yaw induced by the mis-set rudder trim. The mis-set trim would have had a stronger influence on the aircraft’s heading once airborne due to the loss of directional control provided by ZCR’s nose wheel steering. While the ATSB was unable to quantify the rudder pedal forces required to overcome the mis-set rudder trim, when tested in a B250 class-D simulator, the forces could only be countered by the pilot for a short period of time. The pilot who flew the simulator commented that he was able to offset the rudder force ‘until his leg gave out’. This happened on three consecutive attempts.
Given the simulator results, once the pilot of ZCR was no longer able to counteract the rudder forces, the yaw resulting from the mis-set trim likely had a significant effect on the aircraft’s climb performance and controllability. The ATSB’s analysis of the ADS-B data and CCTV footage found a clear correlation between ZCR yawing and a reduction in performance. ZCR’s performance degraded to the point at which control could not be maintained and the aircraft subsequently collided with the outlet centre.
The adverse effect on performance and control of a mis-set rudder trim during take-off has also been shown in previous similar occurrences. While these occurrences varied, they all resulted in significant control difficulties and a loss of performance. This was consistent with the results of the B250 simulator flights, where each flight resulted in a loss of control.
Cockpit voice recorder
The ATSB publication Black box flight recorders highlights the benefits of aircraft flight recorders such as the CVR as an invaluable tool in identifying the factors behind an accident. The CVR not only records the pilot’s voice, it creates a record of the total audio environment in the cockpit area.
Checking the serviceability of the CVR is required before the first flight of the day. ZCR’s CVR did not record the accident flight as a result of the impact switch tripping on a previous flight in January 2017. Consequently, ZCR was operated on multiple flights by several pilots in the intervening period with the CVR unserviceable. The ATSB could not determine why the impact switch was not reset, however, it was likely that the checklist being used in ZCR did not alert the pilots to the requirement to check the CVR. While this had no influence on the accident, ZCR’s CVR being inoperable resulted in a potentially valuable source of information not being available to the investigation.
Aircraft take-off weight
The ATSB estimated ZCR’s maximum take-off weight was exceeded by 240 kilograms. The corresponding ground roll distance for this weight was only 5 per cent more than that calculated for the maximum take-off weight. Similarly, ZCR’s climb performance would have reduced only slightly with the additional weight. Further, while ZCR was estimated to be within the forward and aft centre of gravity limits, the ATSB was unable to determine if the overweight condition affected the pilot’s ability to control the left yaw.
ZCR’s actual take-off roll was significantly more, and its climb performance was significantly less, than performance calculations estimated. Therefore, the overweight condition alone did not result in the longer take-off roll and reduced climb performance.
The ATSB was unable to establish if the pilot had verified the aircraft’s weight and balance prior to departing. However, ZCR’s overweight condition was unlikely to have contributed to the likelihood of the accident occurring or to the severity of the outcome of the accident.
Flight Check System
In late 2015, the Civil Aviation Safety Authority (CASA) had identified that the operator did not have an approved flight check system for ZCR. CASA subsequently issued the operator with a non-compliance notice. In late 2016, CASA closed the notice on the basis that the checklist requirements stipulated in the operator’s amended operations manual met the requirements of a flight check system. However, the checklists to be used in ZCR had not been sighted by CASA at that time and the aircraft manufacturer advised the ATSB that the checklist nominated in the operations manual was not applicable to ZCR. In addition, the nominated checklist did not contain checks for supplemental equipment such as the CVR. Incorporating checks for supplemental equipment in a consolidated and easy‑to‑access cockpit checklist is a key requirement for a flight check system.
Consequently, at the time of the accident, the operator did not have an appropriate flight check system in place for ZCR. The ATSB sought further information from CASA regarding the acquittal of NCN 713808 and was advised that a Civil Aviation Regulation 232 approval was issued to the operator in 2006, however, the checklist part number nominated in the approval was not applicable to ZCR and did not contain required checks for supplemental equipment.
B200 checklists reviewed by the ASTB all included identical checks for setting and confirming trim positions. While the ATSB was unable to establish what checklist was being used by the pilot, an appropriate flight check system was unlikely to have varied the checks related to ZCR’s rudder trim. Therefore, it is unlikely that the inappropriate flight check system influenced the accident. It may, however, have been a missed opportunity to ensure the CVR was operational and would have ensured any other checks required as a result of any modifications to ZCR were included in the checklists used by the pilot.
Bulla Road Precinct – Retail Outlet Centre approval process
Although there were exceedances identified with the Essendon Airport overall obstacle limitation surfaces (OLS), ZCR did not collide with the sections of the outlet centre which breached the OLS. In addition, the outlet centre did not impinge on the required obstacle clearance zones for a departure from runway 17.
It was unlikely that the outlet centre had an influence on the severity of the accident. In the absence of the Retail Outlet Centre buildings, the aircraft’s trajectory would likely have resulted in the aircraft colliding with the Tullamarine freeway, east of the Bulla Road overpass. Dashboard camera footage provided to the ATSB indicated that there was a significant amount of traffic on the Tullamarine Freeway at the time, with potential for casualties on the ground.
The reasons for the OLS breaches were complex and related to the airport operator’s obligation to establish an OLS in accordance with applicable standards and CASA advice to, and oversight of, the airport operator. It is beyond the scope of this investigation to adequately examine the issues found with the outlet centre building approval processes. Consequently, the ATSB has initiated a separate investigation, AI-2018-010. That investigation will examine the building approval process from an aviation safety perspective, including any airspace issues associated with the development, to determine the transport safety impact of the development on aviation operations at Essendon Airport.
From the evidence available, the following findings are made with respect to the collision with terrain involving Beechcraft B200 King Air, registered VH-ZCR that occurred at Essendon Airport, Victoria on 21 February 2017. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
- The aircraft's rudder trim was likely in the full nose-left position at the commencement of the take-off.
- The aircraft's full nose-left rudder trim setting was not detected by the pilot prior to take-off.
- Following a longer than expected ground roll, the pilot took-off with full left rudder trim selected. This configuration adversely affected the aircraft's climb performance and controllability, resulting in a collision with terrain.
Other factors that increased risk
- The flight check system approval process did not identify that the incorrect checklist was nominated in the operator’s procedures manual and it did not ensure the required checks, related to the use of the cockpit voice recorder, were incorporated.
- The aircraft's cockpit voice recorder did not record the accident flight, resulting in a valuable source of safety related information not being available.
- The aircraft's maximum take-off weight was likely exceeded by about 240 kilograms.
- Two of the four buildings within the Bulla Road Precinct Retail Outlet Centre exceeded the obstacle limitation surface (OLS) for Essendon Airport, however, the OLS for the departure runway was not infringed and VH-ZCR did not collide with those buildings.
Other findings
- The presence of the building struck by the aircraft was unlikely to have increased the severity of the outcome of this accident.
- Both of the aircraft’s engines were likely to have been producing high power at impact.
Pilot details
| Licence details: | Commercial Pilot (Aeroplane) licence |
| Ratings: | Multi-engine aeroplane class and instrument ratings |
| Endorsements: | Manual propeller pitch control, pressurisation system, retractable undercarriage and gas turbine engine; B200 endorsement issued on 8 September 2004 |
| Medical certificate: | Valid and current Class 1 |
| Aeronautical experience: | 7,681.8 hours flying experience |
| Last flight review: | 7 October 2016 |
Aircraft details
| Manufacturer and model: | Beechcraft King Air B200 | |
| Year of manufacture: | 1996 | |
| Registration: | VH-ZCR | |
| Serial number: | BB-1544 | |
| Total Time In Service | 6,996.7 flight hours as of 5 February 2017 | |
| Type of operation: | Charter (passenger) | |
| Certificate of registration: | 16 Dec 2013 issue date | |
| Certificate of airworthiness: | 9 Oct 2014 issue date | |
| Maintenance release: | A 133390 | |
| Time since last maintenance: | 6 flight hours | |
| Persons on board: | Crew – 1 | Passengers – 4 |
| Injuries: | Crew – 1 (fatal) | Passengers – 4 (fatal) |
| Damage: | Destroyed | |
Left engine information
| Manufacturer: | Pratt & Whitney Canada |
| Model: | PT6A-42 |
| Type: | Turboprop |
| Serial number: | PCE- 93132 |
| Time since overhaul: | 497.7 flight hours, fitted on 11 Dec 2012 |
| Total time in service: | 13,175.3 flight hours |
Right engine information
| Manufacturer: | Pratt & Whitney Canada |
| Model: | PT6A-42 |
| Type: | Turboprop |
| Serial number: | PCE-93904 |
| Time since overhaul: | 499.8 flight hours, fitted on 10 Oct 2012 |
| Total time in service: | 8,829.8 flight hours |
Left propeller information
| Manufacturer: | Hartzell |
| Model: | HC-D4N-3A |
| Type: | Constant speed, full feathering & reversing |
| Serial number: | FY-3552 |
| Total time in service: | 509.3 flight hours |
Right propeller information
| Manufacturer: | Hartzell |
| Model: | HC-D4N-3A |
| Type: | Constant speed, full feathering and reversing |
| Serial number: | FY-3554 |
| Total time in service: | 501.5 flight hours |
Sources of information
The sources of information during the investigation included:
- Textron Aviation Inc.
- Pratt & Whitney Canada
- Hartzell Propeller
- the Bureau of Meteorology
- the Civil Aviation Safety Authority
- Airservices Australia
- Victoria Police
- the Victorian Institute of Forensic Medicine
- the Metropolitan Fire Brigade
- a number of witnesses
- Corporate & Leisure Aviation records
- numerous B200 pilots
- Essendon Fields Airport
- Bulla Road Precinct Retail Outlet Centre
References
CASA (2015), A review of the case for change: Scientific support for CAO 48.1 Instrument 2013. CASA SMS & HF Section – Fatigue Management Standard Division.
Degani, A. & Wiener, E.L. (1990). Human Factors of Flight-Deck Checklists: The Normal Checklist (NASA Contractor Report 177549). Washington, DC: National Aeronautics and Space Administration.
CASA Air Operator’s Certificate Handbook Volume 2 – Flying Operations (February 2018 Version 2.1).
Civil Aviation Regulations 1998 (Cth), Volume 3, regulation 232 - Flight check system (Austl.).Dismukes, K.R. & Berman, B. (2010). Checklists and Monitoring in the Cockpit: Why Crucial Defenses Sometimes Fail (NASA TM 2010-216396). Washington, DC: National Aeronautics and Space Administration.
Hawkins, F.H. (1993). Human factors in flight (2nd Ed.) Aldershot, England: Ashgate Publishing.
House of Representatives Standing Committee on Communication, Transport and the Arts, (1999), Beyond the Midnight Oil: Managing Fatigue in Transport.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the aircraft owner and maintainer, Textron Aviation Inc., Pratt & Whitney Canada, Hartzell Propeller, the Bureau of Meteorology, the Civil Aviation Safety Authority, the Department of Infrastructure, Regional Development and Cities, Essendon Fields Airport, Bulla Road Precinct Retail Outlet Centre, the Victorian Institute of Forensic Medicine, the Transport Safety Board of Canada, the US National Transportation Safety Board and the US Federal Aviation Authority.
Submissions were received from the aircraft owner and maintainer, Textron Aviation Inc., Pratt & Whitney Canada, Hartzell Propeller, the Civil Aviation Safety Authority and Essendon Fields Airport. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Appendix A – Reduction gearbox and propeller shaft assembly examinations
On-site examination determined that both engines were rotating at impact and there were no signs of pre-impact failure. During that examination, the propeller shaft fracture surfaces and reduction gear boxes (RGB)s were examined and it was determined that further detailed inspection at the ATSB laboratories might be able to assist in determining the relative power output of each engine at impact.
Propeller shafts
Visual examination of the propeller shafts from the left and right engines revealed that they had fractured at almost identical locations (Figure 44, Figure 45 and Figure 46). The fracture features from both shafts were also near-identical in appearance. Both were inclined at 900 to the shaft axis with a smooth and regular surface texture. A high-magnification examination of the fracture surfaces was completed using a scanning electron microscope (SEM), which confirmed the presence of ductile tearing from overstress associated with the accident sequence. No evidence of pre-existing defects that might have contributed to the propeller shaft fractures were identified. The fracture surfaces were consistent with torsional loads being the dominant load case that led to the failure of the shafts, rather than bending loads from ground impact.
Figure 44: Pratt & Whitney Canada PT6A-42 engine showing the general layout of the RGB in relation to the location of the propeller shaft fracture

Source: Pratt & Whitney Canada, annotated by the ATSB
Figure 45: Left and right propeller shaft fractures

Source: ATSB
Figure 46: Fractured portion of the propeller shaft from the left and right engines

Note the almost identical planar fracture surfaces. Source: ATSB
The ATSB determined that with little difference between the shaft fractures, and torsion being the dominant load case for both shafts, it was unlikely that there was a significant power difference between the two engines at impact. Further, features identified on the fracture surfaces were characteristic of significant torsional loading at the time of impact.
Reduction gearbox examination
A two-stage sun and planetary gear assembly is contained within the reduction assembly to reduce the engine rpm at maximum continuous power from 38,100 rpm at the gas-generator down to 2,000 rpm at the propeller shaft.
Tooth damage was observed on the stage-2 planetary gears from the left RGB. Three of the five gears from the stage-2 carrier displayed similar levels of tooth damage (Figure 47). Indentations and tooth bending along the planet gear tooth profile suggests significant torsional loads were transmitted into the gearbox at the time of the accident.
Scoring was present on the stage-2 carrier housing end surfaces for both the left and right engines. The scoring was the result of rotational contact between the housing and the respective carrier bearing and its bolts. Such damage is indicative of significant RPM at the time of impact.
Figure 47: Left engine RGB stage-2 planetary tooth deformation

Source: ATSB
Appendix B – Rudder trim tab actuator examination
On-site examination of the aircraft wreckage found the rudder trim tab actuator was in the full nose-left position. The actuator was examined at the ATSB laboratories in order to determine its position at impact.
Rudder trim tab actuator operation
The range of movement of the rudder trim tab is 15 degrees either side of neutral. Adjusting the trim wheel position moves the left and right cables, which in turn either extends or retracts the actuator through its range of movement (Figure 48). Tension on the right cable translates the cable forward along the actuator barrel and retracts the actuator. Conversely, tension on the left cable translates the cable rearward along the barrel and extends the actuator (Figure 49).
When the actuator is fully retracted, the rudder trim tab is at 15 degrees to the right, corresponding to an aircraft nose-left yaw. When the actuator is fully extended, the trim tab is at 15 degrees to the left, corresponding to a nose-right yaw. (Refer to the ‘Aircraft systems information’ section of this report for more details on aircraft flight controls).
Figure 48: Schematic of the B200 rudder trim actuator
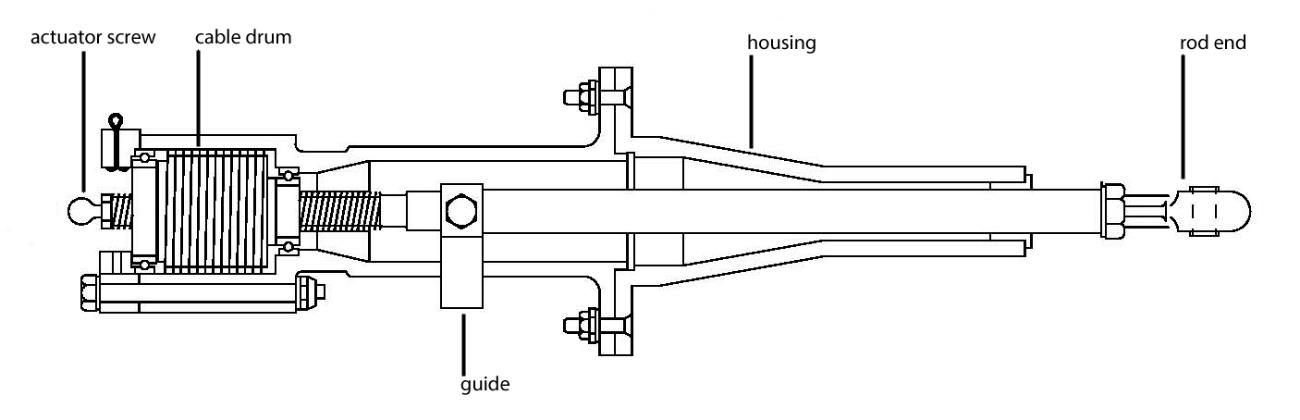
Source: Beechcraft, annotated by ATSB
Figure 49: Rudder trim actuator showing the cable position along the barrel

Left image shows the actuator fully retracted and set to full nose-left position, right image shows the actuator fully extended and set to full nose-right. Source: ATSB
Initial observations
The actuator had sustained significant heat damage from the post-accident fire (Figure 50). The rod end was retracted and the guide was noted to be in the full nose-left position, and the cable was in the forward position on the drum. Measurements established that the rod end extended 43mm from the end of the housing, which correlated to a rudder trim tab deflection of approximately 15-degrees to the right. The left cable had fractured forward of the actuator. Right cable damage included kinking and wire strand fracture where it entered the actuator housings.
Figure 50: General view of the rudder trim actuator, as received from the accident site

Source: ATSB
Disassembly
Prior to disassembly, a radiographic examination of the actuator was conducted under the supervision of the ATSB. The examination enabled further understanding of the internal structure of the actuator assembly. No internal anomalies were identified.
In order to examine the internal components of the actuator with minimal disturbance to any potential witness marks that had been created during the accident sequence, the housing was sectioned between the guide and the cable drum. Once sectioned, the drum and cable were removed from the housing (Figure 51).
Figure 51: Disassembled and sectioned rudder trim actuator

Source: ATSB
Examination
Following disassembly, the components were examined using a binocular microscope. Abrasion damage was identified within the housing at the location where the right cable exited the housing, as found at the accident site. The cable was kinked and several individual wires had been overstressed, likely from contact with the housing. The location of the abrasion damage was consistent with the final wrap of cable about the drum (Figure 52 and Figure 53).
Figure 52: Actuator housing showing the location of the abrasion damage

Sliding contact from the right cable (left image) produced abrasion damage within the housing (right image). Source: ATSB
Figure 53: Abrasion damage to the housing attributed to sliding contact from the right cable

Source: ATSB
In order to further characterise the damage, the actuator housing was examined at high magnification using a SEM. The examination confirmed that the damage was consistent with abrasion from sliding contact with the cable (Figure 54 and Figure 55). No additional damage or features were observed on the actuator drum housing to indicate the actuator was in any position, other than fully retracted at the time of the accident.
Cable damage supports both the left and right cables being under high tension as a result of impact forces. In addition, the lack of any additional abrasion damage to the housing from cable contact indicates that the cable had not spooled through the actuator drum during the accident sequence.
Figure 54: High magnification SEM image of the abrasion damage

Source: ATSB
Figure 55: Higher magnification SEM image of the abrasion damage

The red lines highlight the abrasion and scoring resulting from sliding contact between the trim cable and the actuator housing. Source: ATSB
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2018
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |




