
What happened
On 8 August 2015 at about 0930 Western Standard Time (WST), a Cessna 208B, registered VHLNH, departed Kununurra, Western Australia, on a scenic flight to the Bungle Bungle Range. On board were the pilot and 12 passengers. The weather was fine and clear, with an easterly wind blowing at about 13 knots. The pilot conducted all normal pre-flight procedures, including an engine runup to confirm that the engine and other systems were functioning normally.
The flight departed from runway 12 and made a right turn to the south to follow the standard Kununurra to Bungles departure route. After levelling at about 700 ft above mean sea level (about 550 ft above ground level), the pilot reduced engine power and propeller RPM for a level segment of the departure. The pilot then commenced a commentary for the benefit of the passengers.
Soon after the pilot commenced the commentary, when the aircraft was about 1.5 NM south of the airport, engine oil appeared on the windscreen. The pilot turned back towards the airport but oil on the windscreen soon turned into an opaque film, substantially limiting forward visibility. Additionally, a number of engine instrument indications were abnormal and white smoke began to enter the cabin through cockpit vents. Although the smoke dissipated quickly, the pilot continued to monitor for any signs of a fire in the engine compartment.
The pilot made a MAYDAY[1] call on the Kununurra CTAF,[2] broadcasting that the engine had failed and that the aircraft was returning to land on runway 12. The pilot of another aircraft operating in the area at the time heard the MAYDAY call and relayed relevant information to Air Traffic Control (ATC) (located in Brisbane), who initiated an emergency response.
At around the same time that the pilot made the MAYDAY call, they also attempted to ascertain the extent of the engine malfunction. Advancing the power lever produced a change in engine sound and an increase in engine torque. Although the propeller was turning, there was no audible response and no apparent change in propeller RPM when the pilot advanced the propeller lever. The pilot also noted that the engine low oil pressure light was illuminated, and deduced that the propeller had probably feathered as a consequence of engine oil loss.
The pilot found that the engine/propeller were capable of providing a small amount of positive thrust (but not sufficient to maintain level flight), so established the aircraft in descent, holding a speed of about 85 to 95 knots. The pilot elected to leave the flaps set at 10 degrees, which was the same position that was set at the time the engine problem first became apparent. The pilot assessed that the aircraft could reach runway 12, but with little margin.
Another aircraft operated by the same company as the aircraft involved in the incident was about to depart Kununurra, and had lined up on runway 12. Upon hearing the MAYDAY call, the pilot of that aircraft vacated the runway. The incident pilot advised the pilot in the other aircraft (vacating the runway) of the nature of their predicament, particularly the extent to which forward visibility was affected, and sought their assistance. The incident pilot also advised the Airport Safety Officer on the CTAF that assistance may be required after landing,[3] and advised the passengers that an emergency landing at Kununurra was required.
With forward visibility substantially limited, the pilot maintained orientation using ground based navigation aids, GPS information and the view of landmarks from the side windows. The dark shape of a nearby waterway to the south of the airport was evident, but forward visibility was so poor that the pilot was unable to effectively identify roadways or cleared areas through the windscreen.
With some directional guidance from the pilot of the aircraft that had vacated the runway, and by reference to navigational instruments, the incident pilot was able to position the aircraft on final approach to runway 12. The turn onto final approach was made through about 100 degrees, at around 150 ft above ground level, and required about 50 degrees angle of bank. The pilot elected to leave the flap setting at 10 degrees throughout the approach and for the landing. The aircraft landed firmly, with the pilot unable to effectively judge flare height due to the restricted visibility.
After landing, the pilot found that forward visibility was obscured to the extent that they were unable to taxi safely. The Airport Safety Officer moved alongside the aircraft in a vehicle to guide the pilot to the next taxiway exit. When safely clear of the runway, the pilot contacted ATC and cancelled the MAYDAY.
The time from take-off to landing was about 2 minutes and 15 seconds. From the time the pilot broadcast a MAYDAY call to the time of landing was about 1 minute and 20 seconds. At its furthest point, the aircraft was about 2.3 NM south of the airport.
After exiting the runway and coming to a stop, the pilot completed the engine shut-down checks. No reaction was felt or heard when the pilot selected the propeller lever to the feather position as part of the shutdown procedure (normally, there was an audible change as the pitch of the propeller changed). After exiting the aircraft, the pilot found that the propeller was in the feather position, and had seized. The extent of oil loss was also apparent, with oil smeared over much of the forward fuselage, particularly the engine cowls and windscreen (Figure 1).
Figure 1: Photographs of VH-LNH after the aircraft had landed, with oil visible on the engine cowl and forward fuselage

Source: Aircraft operator
Aside from the apparent engine and propeller system problem, there was no damage to the aircraft and the pilot and passengers were uninjured.
Subsequent on-site inspection of the engine by engineering staff revealed that an oil leak had developed at a join between the oil transfer elbow and oil transfer tube at the forward end of the engine. This assembly was part of a larger assembly that transferred oil under pressure to the reduction gearbox at the front of the engine. One of the oil transfer elbow mounting lugs (that secured the elbow to engine assembly) was found to be fractured, allowing the oil transfer elbow to move and unseat the O-ring between the elbow and the tube (Figures 2 and 3).
Figure 2: Photograph (in situ) showing fractured oil transfer elbow mounting lug and the unseated O-ring seal
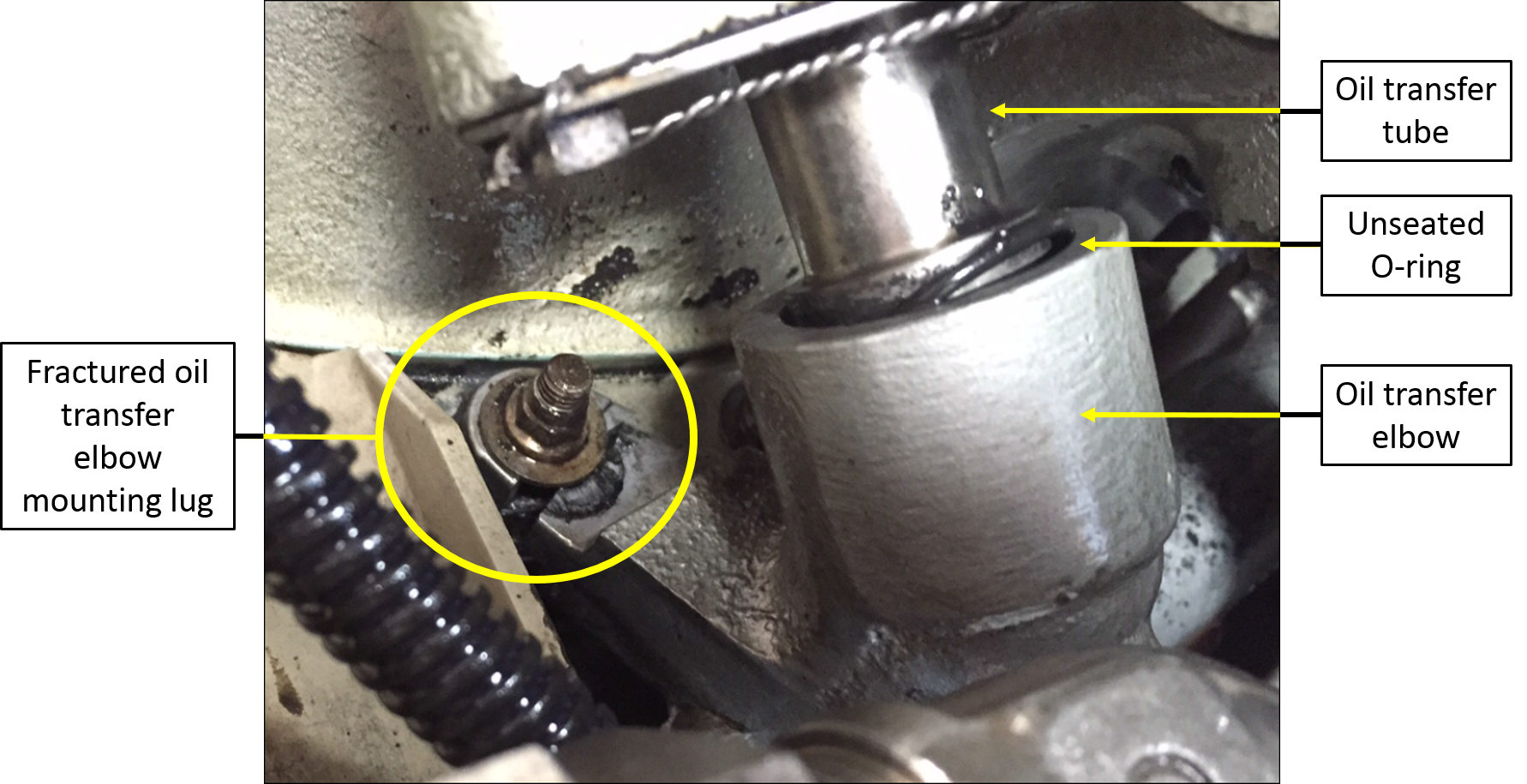
Source: Aircraft operator (annotations by the ATSB)
Figure 3: Oil transfer elbow assembly
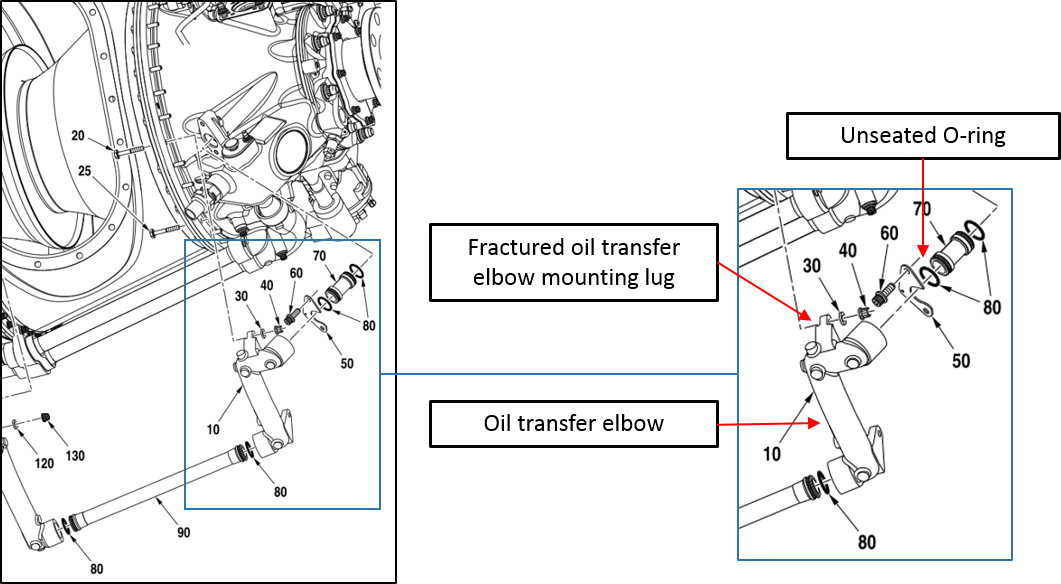
Source: Engine manufacturer (annotations by the ATSB)
Technical follow-up
Following the incident, the operator submitted a Service Difficulty Report (SDR) to CASA. The engine was removed from the aircraft by the operator and dispatched to a repair and overhaul facility for further examination. The oil transfer elbow (with cracked mounting lug) was removed and sent to the engine manufacturer for detailed analysis. The results of those examinations are summarised in the following paragraphs.
Engine teardown
The engine teardown did not reveal any unrelated engine abnormalities that might have contributed to the oil transfer elbow mounting lug fracture. Among other things, the report noted that there was little or no engine oil remaining in the engine and that the reduction gearbox could only be turned with considerable force (more than the amount of force that would normally be required). The report also noted that the propeller shaft would not rotate.
Inspection of the engine confirmed that an oil transfer elbow mounting lug had fractured and the report noted that the ‘hardware holding it in place was loose’. The lug was found to have completely broken through, and it was noted that a segment of the lug was missing (Figure 4). The report also noted that the O-ring (see Figures 2 and 3) had moved.
Figure 4: Fractured lug (the figure on the right shows that a segment of the lug was missing)

Source: Pacific Turbine (left) and CASA (right)
Mounting lug fracture analysis
The manufacturer’s examination of the fractured oil transfer elbow mounting lug and associated securing assembly allowed them to draw a number of conclusions, including:
- The fracture of the lug occurred due to fatigue originating from multiple locations on the side of the mounting lug that meets with the face of the mounting flange. The fatigue mode was found to be high-cycle, under unidirectional bending.
- Wear and imprint marks on the securing assembly (bolt, nut and washer) and the fractured lug suggested that the bolt was sitting askew in the bore of the flange to which the elbow mounting lug was secured. The report commented that this wear pattern was consistent with a lack of pre-load on the bolt.
- The lack of pre-load on the bolt that secured the mounting lug to the flange was considered to be the initiating factor that led to fracture of the mounting lug. The reason for the lack of preload on the bolt could not be ascertained.
- Impact marks were identified on the oil transfer elbow, which may have been caused by interference from tooling used to conduct unrelated maintenance in the vicinity of the oil transfer elbow. This damage was found to be superficial which suggested that it played no part in fracture of the mounting lug.
CASA comments
At the time that this report was prepared, CASA was continuing to consider relevant information, including the manufacturer’s fracture analysis report. Notwithstanding their ongoing consideration of relevant information, CASA did not believe that there was any conclusive evidence of a lack of pre-load on the bolt. CASA commented to the effect that the typical signs of an incorrectly torqued fastener were not evident, and noted that the separated portion of the lug remained in place after the lug had fractured – that was unlikely if there was a lack of pre-load on the bolt. CASA also commented to the effect that incorrect installation of the oil transfer elbow (mounting lug), rather than incorrect installation of the mounting lug bolt, may have been the origin of the problem. CASA reported that this is a scenario that is known to have occurred in practise.
Engine teardown facility comments
Staff from the engine teardown facility suggested that the following may assist in preventing similar occurrences:
- Paint-free lug and flange mating surfaces: Paint on the elbow mounting lug and/or the mating face of the flange to which the lug is secured may wear with working and vibration. This wear has the potential to loosen the fastener and amplify the effects of vibration on lug security.
- Lug strengthening: The construction of the elbow transfer tube is such that the mounting lug itself is substantially narrower than the stem leading to the lug (see Figure 4). Added thickness/material depth would strengthen the lug.
- Expanded and mandated inspection: Mandating inspection of the elbow mounting lug (see CASA Airworthiness Bulletin 72-004 below), and including oil transfer elbow mounting lug inspection as a specific task during relevant engine servicings.
Related background information
Similar occurrences
ATSB investigations AO-2010-005, AO-2008-005 and AO-2010-003 identified the failure of the same oil transfer elbow fitting that fractured in the case of this occurrence. In two cases (AO2008005 and AO-2010-005), the investigations found that oil transfer elbow mounting lug failures were a consequence of other unrelated engine problems (compressor turbine blade failures). In one case (AO-2010-003), both oil transfer elbow mounting lugs were fractured, but the cause of those fractures could not be conclusively determined.
Advice from the engine manufacturer suggested that there have been a number of oil transfer elbow mounting lug failures reported over the past 15 years, including those investigated by the ATSB. In most cases, either a vibration source or mechanically induced damage was found to be a contributor. The manufacturer identified the possibility that tooling could interfere with the elbow fitting during removal and installation of nearby engine components.
Possible sources of oil transfer elbow damage – manufacturer comments
During the course of the investigation (but aside from the specific nature of the mounting lug fracture in this case), the engine manufacturer highlighted possible sources of oil transfer elbow damage that could ultimately lead to mounting lug fracture. While these comments may not be specifically relevant in this case, they are noteworthy and warrant the attention of organisations involved in the logistics of transporting and/or maintenance of PT6A114A and similar engines:[4]
- Pratt and Whitney Canada Service Information Letter. In 2008, the manufacturer issued a Service Information Letter (SIL Gen PT6A026 applicable to all PT6A engines) to remind operators of the precautions to be taken when installing, removing and performing maintenance on external engine tubes, lines and fittings. The letter pointed out that:
Investigations of incidents in service (including in-flight shut downs) have determined that mishandling tubes and fittings during normal maintenance activities can subject these components to distortion or stresses beyond normal utilisation, leading to fracture during subsequent operation.
- Reduction gearbox chip detector removal/installation. The engine manufacturer commented that the proximity of the oil cooler and reduction gearbox magnetic chip detector may be a factor if tooling used to install or remove those components is allowed to interfere with the oil transfer elbow, and induce mechanical stress on the mounting lug. To that end, the reduction gearbox maintenance manual (in the areas dealing with removal and installation of the magnetic chip detector) included the following caution:
AVOID FORCING OR CONTACT WITH THE OIL PRESSURE TRANSFER ELBOW WHEN YOU REMOVE THE CHIP DETECTOR. DAMAGE TO THE ELBOW MOUNTING LUGS CAN OCCUR RESULTING IN LOSS OF ELBOW RETENTION AND OIL LEAKAGE.
CASA Airworthiness Bulletin 72-004
In 2010, CASA released an Airworthiness Bulletin (AWB) AWB 72004 which identified a possible link between the incorrect installation of an engine mount bracket assembly (vibration isolator), and fatigue cracking in the oil transfer elbow fitting. The AWB identified the possibility that fatigue failure of the oil transfer elbow fitting may be linked to unusual vibration caused by incorrect installation of the engine upper vibration isolator. The AWB went on to recommend that operators inspect the relevant vibration isolators for correct installation, and inspect oil transfer elbow fittings for any signs of cracking.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce safety risk. The ATSB understands that the following safety actions are being considered in response to this occurrence.
Engine manufacturer
After reviewing the circumstances surrounding this incident (and noting concerns that the oil transfer elbow may be interfered with or damaged during unrelated engine maintenance in the area of the elbow), the engine manufacturer is considering adding information in relevant publications and issuing a Service Information Letter. Publication amendments are likely to draw attention to the need to refer to relevant instructions if the oil transfer elbow is removed/replaced during fuel nozzle replacement. The Service Information Letter is likely to provide information and warnings with respect to the possibility of damage to the oil transfer elbow during engine maintenance. The Service Information Letter is also likely to include information and warnings related to removal and installation (or other disturbance) of the oil transfer elbow.
Civil Aviation Safety Authority
At the time this report was written, CASA was continuing to consider relevant information, which may lead to a re-issue of AWB-72004.
Operator
Prior to this incident, the operator was already in the practice of periodically inspecting the area of the fractured lug (although those inspections did not alert the operator to the problem in this case), In response to this incident, the operator intends to expand the periodic inspection to include removal of the bolt and an inspection of the internal radius of the mounting lug for signs of crack development.
Safety message
The manner in which the pilot handled a very difficult set of circumstances provides some positive examples for other pilots to consider.
- The pilot maintained positive control of the aircraft, despite the challenging circumstances. The adage ‘aviate-navigate-communicate’ continues to prove a fundamentally effective prioritisation guide for pilots.
- The pilot used available resources including other pilots, ATC, and the Airport Safety Officer, to assist in dealing with the circumstances. The combined efforts of those involved clearly contributed to a favourable outcome. The principles of effective crew resource management extend to all operations, including single pilot operations.
- The pilot conducted a pre-flight emergency self-briefing. Even though it may be impractical to consider all possible emergency scenarios during a pre-flight emergency self-briefing, having a general plan in mind may be important, particularly when confronted with a time-critical and stressful situation.
The incident highlights also the importance of care and attention to detail when conducting maintenance on aircraft engines and accessories. This is particularly important where critical components are known to be susceptible to damage through interference from tooling or mishandling. Manufacturers, regulatory authorities, operators and aircraft maintenance organisations all have fundamentally important roles to play in maintenance of the highest practicable standards of airworthiness.
Aviation Short Investigations Bulletin - Issue 48
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2016
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
__________
- MAYDAY is an internationally recognised call for urgent assistance.
- CTAF means Common Traffic Advisory Frequency. It is the frequency on which pilots operating at a non-towered aerodrome should make positional radio broadcasts.
- The pilot intended to highlight that fire services may be required after landing, but it is not clear whether the intended message was fully understood by the Airport Safety Officer. Fire services were not ordered, but the Airport Safety Officer was standing-by to render assistance as required.
- With respect to the incident that precipitated this ATSB investigation, CASA commented that there was no information in the aircraft records that documented when the oil transfer elbow was last removed. Additionally, there was no evidence available from log book records of other maintenance events that may have had an effect on the integrity of the oil transfer elbow.