
Safety summary
What happened
On 11 July 2015, the Melbourne to Albury service 8625 was approaching Wallan crossing loop when the train traversed the points into the loop road at excessive speed. As a result, the passengers and crew experienced a rough ride resulting in some passengers requiring medical attention from the on board service crew. The service crew reported the incident to V/Line operations and the train continued on to Seymour.
On arrival at Seymour, the train was met by a Regional Driver Supervisor (RDS). The RDS questioned the driver about the rough ride at Wallan and after a short discussion, the train departed making scheduled stops along the way.
Shortly after a stop at Euroa station, some of the passengers approached the conductor about persons in their care showing signs of discomfort and stress as a result of the earlier rough ride. The conductor decided to arrange for an ambulance to meet the train at Benalla station. Meanwhile, V/Line operations were arranging to have the driver of 8625 relieved of duty at Benalla.
On arrival at Benalla station, the conductor told the driver of 8625 that he was to be relieved of duty. Ambulance officers treated some of the injured passengers for minor injuries with one passenger and their carer taken to a nearby hospital. The service continued onto Albury with the new driver.
What the ATSB found
The ATSB found that the driver of train 8625 did not demonstrate effective train handling techniques when approaching a signal displaying a low speed aspect. As a result, 8625 traversed the points at a speed significantly greater than the allowable engineering speed.
In addition, the driver did not immediately report the severity of the incident to the ARTC train control or V/Line. As a result, the possibility of infrastructure damage exposed trains travelling on the Standard Gauge at Wallan to a potentially elevated safety risk.
The ATSB also found that V/Line did not have a procedure in place that specifically required other V/Line employees to report incidents in the event that a driver did not. Furthermore, the ATSB found that V/Line’s processes did not consider the potential for rolling stock or infrastructure damage in the event that a train had traversed a turnout at significantly greater speed than designed.
What's been done as a result
V/Line have developed and implemented a procedure, which acknowledges and addresses the risk associated with gross over-speed. They have also updated their Just Culture policy in relation to reporting and have incorporated redundant pathways to ensure reporting should a driver fail to do so.
Safety message
All incidents that could compromise the safety integrity of the network must be reported immediately to Train Control. Operators need to ensure robust reporting procedures are implemented.
For incidents that involved gross over-speed, train operators should implement procedures that identify and manage the risk appropriately.
At 1802[1], on 11 July 2015, V/Line passenger train 8625, departed Southern Cross Station (Melbourne, Victoria) for a scheduled service to Albury (New South Wales).
Shortly after departing Southern Cross Station, train 8625 stopped on the passing loop at Tottenham and waited for a freight service to pass on the main line. Train 8625 then continued onto Broadmeadows for its first scheduled stop. At about 1840, train 8625 departed Broadmeadows, bound for its next scheduled stop at Seymour (Figure 1).
Figure 1: Location map – Wallan, Seymour, Benalla Victoria
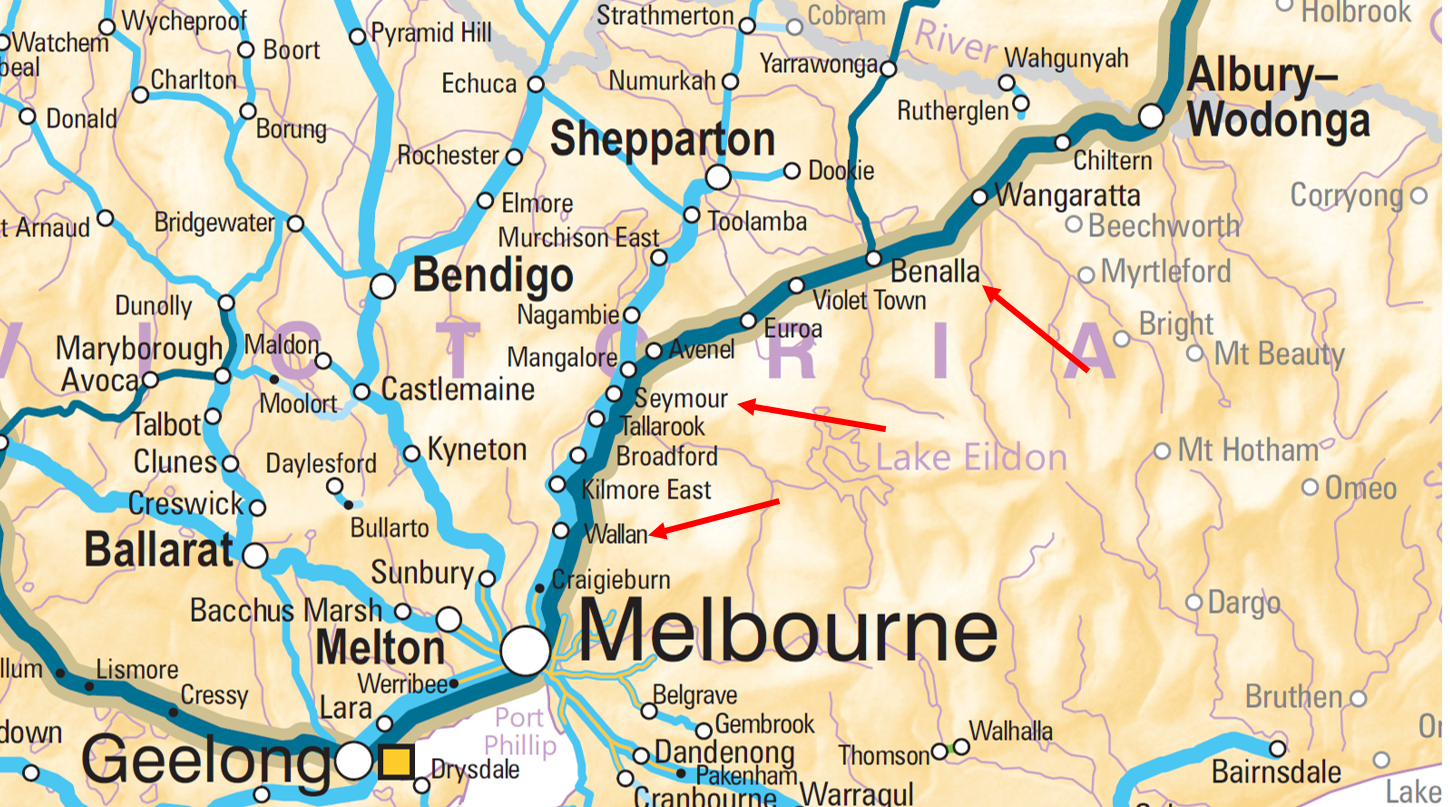
Source: NatMap Railways of Australia
At about 1845, the Australian Rail Track Corporation (ARTC) Network Control Officer (NCO) had set the signals at Wallan (Figure 1) for train 8625 to take the passing loop, allowing an oncoming Melbourne bound train to pass on the main line. This action set number 3 points for the passing loop and then the signal interlocking cleared signal WLN/2 for a low speed entry into the loop track. Signal WLN/2 is located about 50 m from the turnout (number 3 points) and signal ES1475 about 3.5 km from the turnout (Figure 2).
Figure 2: Signalling approaching Wallan

The above schematic shows the position of the signals, level crossings, and points. The signals show the aspects at the time of the train approaching ES1475 and WLN/2. Not to scale. Source: ATSB
At about 1858, train 8625 approached signal ES1475 displaying a yellow aspect and passed it travelling at about 104 km/h. It was just after sunset and it had been raining intermittently. The driver continued on to Wallan, managing the train’s throttle to maintain a speed of about 100 km/h.
About 2 minutes later, train 8625 approached and passed signal WLN/2 signal displaying a low speed aspect (Figure 4). At about this point, the driver placed the train’s throttle into the idle position. At the time, the train was travelling at a speed of about 98 km/h.
Shortly after, train 8625 crossed over number 3 points and onto the loop track, travelling at about 97 km/h. The train swayed violently, severe enough that some of the passengers were thrown out of their seats. About 5 seconds after passing over the points (a distance of about 185 m), the driver made a service brake application. The train stopped about 1.5 km later, at WLN/U6 signal (Figure 3) in readiness for its departure.
Figure 3: Layout of signalling at Wallan loop Standard Gauge.

Figure 3 shows the location of the signalling. Train 8625 arrived at Wallan from Melbourne (from left of figure 3) Once 8625 traversed the number 3 points the train came to a stand at WLN/U6 signal on the loop track (No.2 road) waiting for train 6WP2 to approach from the Seymour (right side of Figure 3) on the main line (No.1 road). Source ARTC
Figure 4: Approaching WLN 2 signal and 3 points into Wallan Loop road.
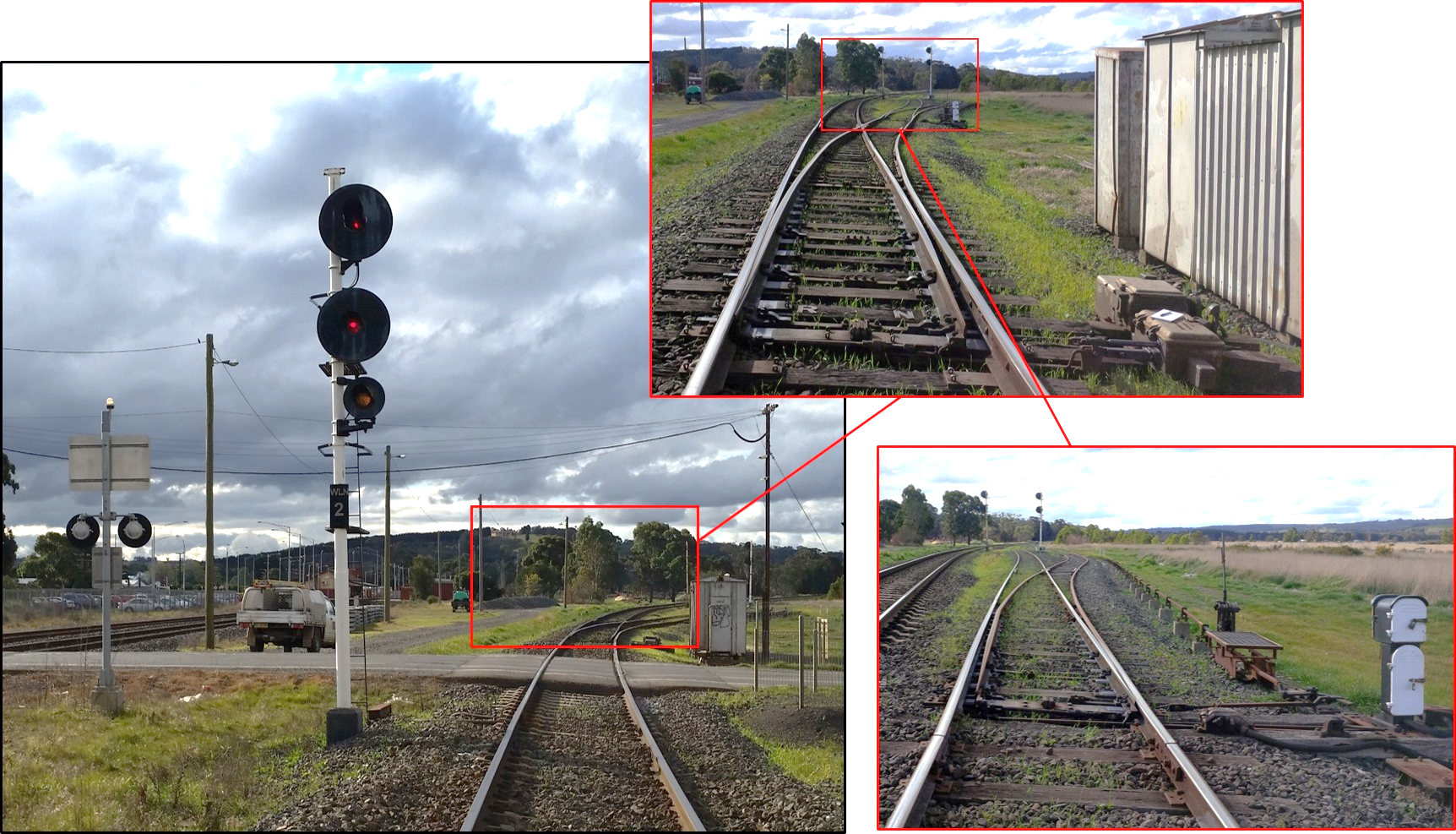
Figure 4 shows the location at and beyond WLN/2 signal over Wallan Whittlesea Rd and approaching 3 points with the signal and points set for the loop road. Note the low speed aspect (yellow) on the ‘C’ arm. At the time, 8625 was travelling over 90 km/h. The top right call out box shows number 3 points in the reverse position and the loop road diverging to the right hand side. The lower right hand call out box show the track layout beyond 3 points through the cripple road points (right hand side). Train 8625 was traversing the middle road (Figure 3 No.2 road) after traversing 3 points in reverse. Source: ATSB
After stopping at signal WLN/U6, the driver contacted the conductor to apologize for the rough ride into the loop road. The conductor responded on the radio that they were attending to some of the passengers who had been thrown out of their seats. At that time the driver of train 8625 did not contact ARTC NCO to advise of the occurrence.
Post incident
At about 1905, freight service 6WP2 passed through Wallan on the main line and continued over number 3 points towards Melbourne. There was no report from the crew to the ARTC Network Controller regarding any rough ride over number 3 points at Wallan.
Shortly after the passage of 6WP2, signal WLN/U6 (Figure 3) cleared to proceed and train 8625 continued on towards Seymour.
As the train continued towards Seymour, the buffet car attendant contacted the V/Line Network Customer Centre[2] (NCC) to report the rough ride incident on the 8625 Albury service and that passengers had been shaken up. The buffet car attendant then contacted the driver via the radio and asked him to also talk to the NCC regarding the incident.
The driver contacted the NCC and advised that he went a bit quick over the points at Wallan, but that everything was OK. The operations officer enquired about the passenger injuries and informed the driver that the Regional Driver Supervisor (RDS) would be notified. The driver asked that the incident not be reported to the RDS, but the NCC explained that it was protocol to report incidents causing injuries, via text message, to the RDS as well as other appropriate staff within operations.
Meanwhile, a relief service crew (excluding driver) were waiting to join train 8625 at Seymour station. The buffet car attendant on train 8625 contacted Seymour station to advise the relief service crew that there had been a rough ride event and to keep an eye on the passengers when they took over the service. At about the same time, the NCC contacted the on-duty RDS, who was also located at Seymour, and requested the RDS meet the train to enquire further with the driver regarding the incident.
At about 1940, train 8625 arrived at Seymour and the relief service crew boarded the train. The conductor joining the service noticed that some of the passengers disembarking from the train were in some discomfort. He talked to the outgoing conductor who informed about the condition of the remaining injured passengers, including a passenger in a wheel chair that had also sustained an injury. Passengers also remarked to the conductor about the violent nature of the event.
The RDS also met the driver at Seymour and discussed the reported rough ride at Wallan. The driver informed that the train was going a bit quick over the points at Wallan. The RDS was not aware that the train was in fact traversing the points into the loop road at the time of rough ride. The RDS advised the driver to be careful of his speed and to slow down. As the RDS walked away, an off-duty driver travelling on the train approached the RDS and explained that the service was signalled into the loop road at Wallan. The RDS re-engaged with the driver and verified that the train was signalled into the loop road at Wallan. Upon ascertaining that the train was going into the loop road, the RDS acknowledged that the move into the loop road was a low speed and that driver was going too fast for the move over the points. The RDS then reiterated to the driver to slow down and take more care on the rest of his journey.
At about 1944, train 8625 departed Seymour to continue its journey, with scheduled stops at Avenel, Euroa, and Violet Town.
Meanwhile, the (V/Line) General Manager Train Services contacted the RDS to discuss the situation. A decision was made for the RDS to relieve the driver of train 8625.
The RDS departed Seymour by taxi and travelled towards Violet Town to meet and take over control of the service.
Shortly after at about 1955, Melbourne bound freight service 7MP7 was travelling through Wallan on the mainline. There was no report of 7MP7 experiencing any rough ride as it passed through Wallan and over number 3 points.
While on route to Violet Town, the RDS contacted the ARTC NCO to request that train 8625 be held at Violet Town to relieve the driver. At that time, the NCO had not been advised of the incident that had occurred at Wallan.
After some further consideration, V/Line operations decided to hold the train at Benalla (about 25 km past Violet Town) to avoid disrupting passengers transferring to a bus service and to avoid blocking the town’s main road over the railway tracks. The RDS contacted the ARTC Train Control and advised that the train would be held at Benalla instead of Violet Town. Again, the NCO was not told of the incident at Wallan.
Shortly after, the RDS contacted ARTC again to inform the NCO of the incident at Wallan regarding the over-speed (rough ride) over the points. In response, the NCO advised that they would slow further trains through Wallan until the points (track) at Wallan could be inspected for damage.
As train 8625 continued towards Benalla making its scheduled stops, the service crew attended to the remaining passengers who were in various levels of discomfort. At about 2046, when between Violet Town and Benalla, the conductor was made aware of a high dependency passenger that was in some discomfort caused by a knock to the head during the incident. The passenger’s carer requested that an ambulance attend to the person. The conductor placed a call to the Emergency Services Telecommunications Authority (ESTA commonly known as ‘000’) and requested that an ambulance meet the train at Benalla station to attend to the injured passengers.
Soon after, another passenger approached the conductor concerning a possible injury to their child. The conductor informed the passenger that an ambulance was meeting the train at Benalla where passengers would be assessed.
Not long after placing the call to ‘000’, the conductor then returned a missed call to his manager. The manager informed the conductor that they could not contact the driver via radio or phone, and asked about the driver’s general demeanour. The conductor advised that the driver’s behaviour had appeared normal. The manager asked the conductor to approach the driver at Benalla to advise that the RDS was on the way to take charge of the train.
Train 8625 arrived at Benalla at about 2053, about the same time as the ambulance. Some of the injured passengers left Benalla on a connecting bus service without seeking treatment, noting also that some had left the service prior to Benalla. The remaining injured passengers were treated at the station and it was decided to convey one person to hospital for further observation.
Meanwhile, the conductor radioed the driver and asked to speak to him at the front of the train on the platform. The conductor informed the driver that he was not to continue and that the RDS was coming to relieve him.
Shortly after the RDS arrived at Benalla and performed an alcohol breath test on the driver. The driver then returned to Melbourne by taxi.
At about 2135, train 8625 continued to Albury under the control of the RDS.
At about 2200, ARTC track and signal maintenance staff arrived at Wallan to inspect and test the signalling. About an hour later, maintenance staff reported to ARTC train control that the equipment and track had been tested ok and was clear for normal traffic to resume. The temporary speed restricted on that section of track was removed and services through the area returned to normal.
The rolling stock was not examined for any damage until the train had returned to Melbourne the following day. The inspection did not find any damage as a result of the over-speed entry at Wallan.
__________
Location and track information
Wallan is located on the Melbourne to Sydney mainline about 47.5 km[3] from Southern Cross Station Melbourne.
The track is a bidirectional standard gauge[4] track consisting of continuously welded rail on concrete sleepers, fastened by resilient clips. Crossing loops[5] are provided at various locations, including Wallan, to facilitate the passing or crossing of trains. The loop track is often referred to as the loop road or Number 2 road.
A railway station is located at Wallan. However, the station only services an adjacent broad-gauge[6] track. There are no passenger facilities for standard gauge trains travelling through Wallan.
The Australian Rail Transport Corporation (ARTC) lease and manage the standard gauge track, with signal control from the ARTC Network Control Centre South at Junee (NSW).
The line speed through Wallan is 130 km/h. However, the signalled speed for the diverging route over the turnout into the loop road is 15 km/h (low speed signal).
Track inspection
Post incident track inspection at Wallan loop was undertaken by the ARTC later that evening. The track was undamaged and there was no pre-existing track condition evident that may have contributed to the rough ride.
Signalling
The signalling at Wallan loop on the standard gauge is a CTC[7] relay based type interlocking.
The three-position signal heads used on signals ES1475 and WLN/2 were Westinghouse K3 searchlights (Figure 5). The K3 searchlight signals are a long-range signal head and have a viewing range of up to 2500 m in clean air.
Figure 5: Signal WLN2 and ES 1475

Signals WLN/2 and ES1475 taken on the 7 July after the incident during testing of the signals. Signal WLN/2 is displaying a red over red over yellow aspect (Low speed). Signal ES1475 is displaying a yellow over red aspect (Normal speed warning). Both signals are displaying the aspects that the driver would have seen approaching Wallan. The ‘A’ arms on both signals are K3 (long-range) Searchlight signals. Source: ARTC.
Signal testing
The ARTC examined the operation of signal ES1475 and WLN/2 and number 3 points at Wallan Standard Gauge Loop. The tests concluded that the signalling and points equipment were working as per design at the time of the incident.
Signal sighting and operation
The ARTC conducted an inspection on the sighting distance of the signals. Both ES1475 and WLN/2 was found to be in good working order with no issue of sighting over the designed viewing distance.
The ATSB site inspection also noted that the sighting distance from ground level for both signals was clear and unobstructed for the respective distances.
Number 3 Points and turnout
Number three points at Wallan are McKenzie and Holland M23A dual operation points.[8] The points are on a 1 in 10[9] turnout. The designed speed of the turnout when track conditions are optimum is 40 km/h. At Wallan however, the signalling aspect for the movement over the points is 15 km/h.
At the time train 8625 was traversing the turnout, the train was travelling at approximately 97 km/h. This was about 80 km/h greater than the signalled speed and about 55 km/h greater than the turnout design speed. As a result, there would have been significant lateral forces on the rolling stock and infrastructure as the train traversed the turnout into the loop road.
The over-speed entry into the loop road contributed to the excessive lateral forces (rough ride) experienced by the passengers and crew on-board train 8625.
Train information
The Melbourne to Albury V/Line service is a driver-only[10] locomotive hauled passenger service consisting of an N class locomotive (N464) and an N class carriage set (SN16). Carriage set SN16 consisted of three economy wagons, a buffet car, and a first class car. There was also a parcel van/cargo carriage at the rear of the train.
In addition to the driver, train 8625 was also serviced by a crew consisting of a conductor and a service attendant for the buffet car. The conductor provided customer service and was responsible for all passenger operations and their welfare.
Rolling stock inspection and maintenance
In April 2015, Locomotive N464 underwent schedule maintenance and was returned to service in May 2015.
In June 2015, carriage set SN16 underwent scheduled maintenance and was returned to service in the same month.
On 12 July (the day following the incident), inspection of carriage set SN16 was undertake by Bombardier to determine if there was any damage as a result of the over-speed. No subsequent damage was found.
During interview, the driver stated that the train felt ok to continue and there were no issues with it as a result of the over-speed.
V/Line’s internal report concluded that there was no pre-existing condition of N464 or SN16 that may have contributed to the occurrence.
The ATSB noted that following the incident at Wallan, the passenger service ran to Albury and back to Southern Cross station the following day before being inspected for damage. While no problems may have arisen, the condition of the rolling stock was not considered until after it having returned to Melbourne.
Train Driver
The Melbourne to Albury service was operated with a driver as the sole person in the locomotive cab (driver-only operation). The driver was qualified in October 2014, to operate the driver-only service but was undergoing Train Driver Safety Audits as a result of a performance management issue.
Training
The driver of 8625 was certified competent to operate diesel hauled trains on the Southern Cross to Albury line. He had completed a written exam on 28 October 2014 and completed a route knowledge assessment on 30-31 October 2014. The assessment included completing four return trips while being supervised and assessed by a trainer driver. However, neither the written nor the practical assessments included a movement into the loop road at Wallan.
Drugs and Alcohol medical
The driver underwent testing for drugs and alcohol at Benalla Station and returned zero readings.
At the time of the incident, the driver was deemed to be medically fit for driver-only train operations.
Fatigue
The driver’s roster, sleep patterns, and general health were analysed. The investigation concluded that fatigue impairment was unlikely to be a contributing factor to this incident.
Train handling
Track speed permitted on the main line through Wallan is 130 km/h. However, V/Line mandates that V/Line trains are limited to 100 km/h.
At the time of the incident signal ES1475 was indicating a yellow aspect informing the driver that the next signal (WLN/2) was at stop. After passing ES1475 a driver should be managing the train to stop at signal WLN/2 (Figure 6).
On approach to signal WLN/2 (about 200 m prior the signal), a low speed aspect would have been visible, indicating that a route had been set for the loop road (Figure 6). The driver must be prepared to stop clear of any obstruction and not exceed a speed of 15km/h.
Figure 6: Typical speed profile versus actual speed
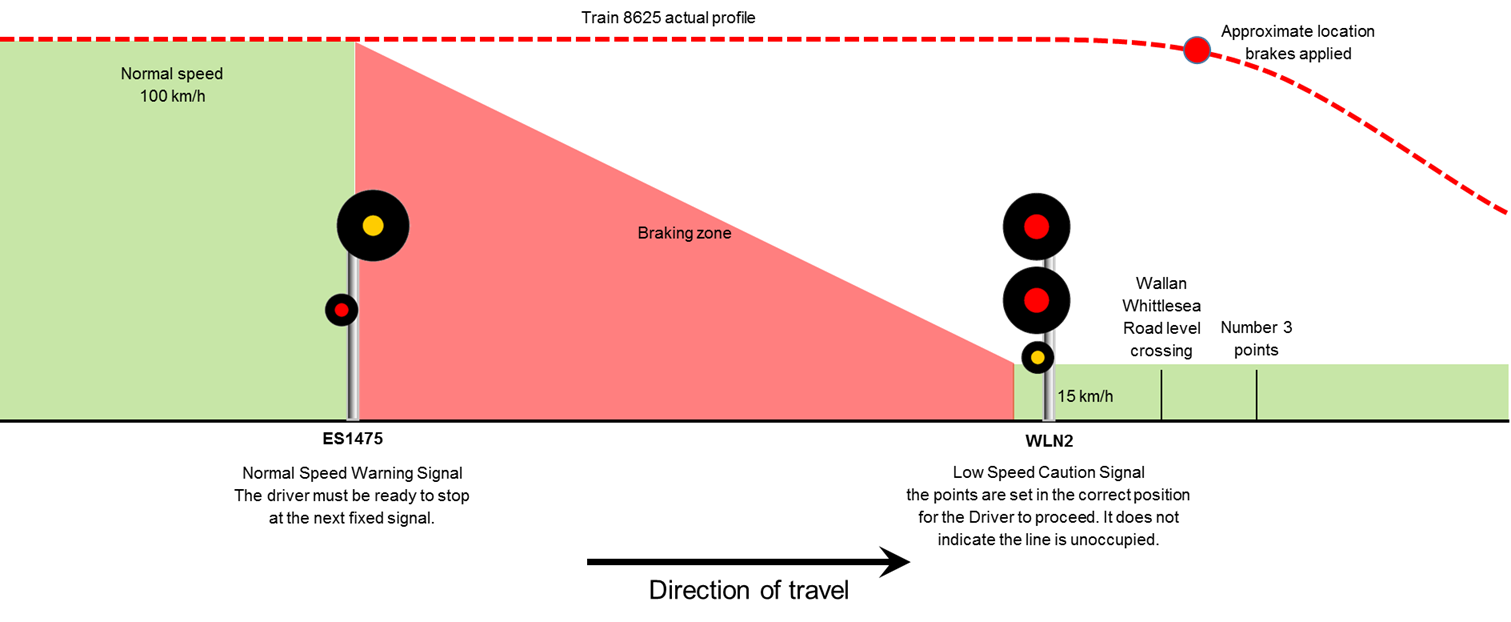
Figure 5 illustrates the typical speed profile for a train being signalled into the loop compared to the speed data taken from the locomotive data logger. Not to scale. Source: ATSB.
Train data logger
Locomotive N464 was fitted with a Fischer data logger device, which captured various parameters, including:
- Time, speed, distance
- Throttle position
- Brake pipe pressures
- Horn (Country and Town)
- Vigilance
- Dynamic brake
The data logger showed that on the approach to both signals the driver was making slight changes to the throttle to maintain speed of about 100 km/h (track speed). The driver also sounded the horn for the approach to Beveridge Rd and Wallan Whittlesea Rd level crossing. However, the data showed no reduction of the throttle nor brake application, at the point where a response to signals ES1475 & WLN/2 would be expected (Figure 6).
Analysis showed that the driver was managing the train in a manner consistent with being signalled straight through Wallan on the mainline. However, with the route set for the loop road, the train traversed the points at more than 90 km/h, significantly greater than the designed (signalled) speed.
The driver of train 8625 did not demonstrate effective awareness and train handling techniques consistent with approaching a signal displaying a low speed aspect.
Drivers awareness of the signalling system at Wallan
The driver had been trained on the Southern Cross to Albury section (otherwise known as route knowledge). The driver was supervised during his training and made four returned trips before being assessed as competent to drive a train on this network.
During interview, the driver was asked questions regarding the signalling at Wallan. In particular, the driver was asked about signals ES1475 and WLN/2.
The driver explained the type of aspects ES1475 would show in relation to the signal ahead (in this case WLN/2). The driver explained that if ES1475 were showing a yellow aspect, then the signal ahead (WLN/2) would be at stop[11] (red over red).
When discussing WLN/2 signal, the driver commented that he had never been signalled into the loop track at Wallan before and that his expectation was a yellow on the “B” arm. However, at Wallan the aspect for trains to enter the loop track is in fact a “C” commonly referred to as a low speed. The driver was not aware the WLN/2 signal would show a low speed aspect for the move into the loop road and that the “B” is a fixed red[12] aspect.
Although there may have been some confusion on what aspect the driver was expecting, when viewing WLN/2 displaying a low speed at distance, the driver would have seen a red signal (stop aspect). As such, the driver should have been preparing the train to stop at the signal. At a distance of around 200 m, the driver should have seen the ‘C’ arm low speed illuminated. Having slowed the train in preparation to stop, a driver would then proceed into the loop road at a speed no greater than 15 km/h.
Although the driver was not aware of the signal indications for the Loop Road at Wallan, the driver should have been handling the train in preparation for stopping at the signal.
Driver history
The driver of 8625 started his career in 1984 as a fireman[13] with V/Line in Bendigo Victoria. In 1988, the driver transferred to Metro Trains in Melbourne to drive on the electrified network. In 2007, the driver returned to V/Line under the “Right of Return” agreement.
Right of return agreement
Under an agreement between V/Line and the Victorian government, a policy for ‘right of return’ was an historical arrangement dating back to the separation of electric trains and diesel services in Victoria. When the split happened drivers were told in order to complete their training they would have to transfer over to the electric trains. At the time, they were given a commitment from the Government that they could return at any time provided that V/Line was recruiting for drivers.
Under the agreement, drivers accepted back did not have to go through a recruitment process. The right of return was premised on the proviso that the driver had continuous service with electric trains and the driver had not refused re-employment with V/Line if an offer was made.
Drivers accepted under the right of return agreement were treated as a transfer. Medical records would be transferable, but the driver’s performance history was not disclosed.
Training and performance
In this case, the driver of 8625 was accepted back under the right of return agreement to V/Line in July 2007 as a Conversion Driver. V/Line acquired the driver’s medical history. V/Line also attempt to ascertain if there was any disciplinary action with Metro Trains. Due to privacy constraints, it was up to the discretion of Metro Trains or the employee to provide the information. At the time, no information was given to V/Line regarding any driver performance issues.
The driver underwent a conversion driver program, which recognised prior knowledge and experience. The driver then underwent network specific training eventually progressing to the North East network.
During the driver’s progression to operate through various networks, the driver was also undergoing performance management for various indiscretions, which included issues with inattentiveness.
Over the next six years, the driver had a number of incidents recorded against his driving record. Formal performance interviews and V/Line’s demerit point system were used to manage these incidents. Some of the incidents included SPAD’s[14] and failure to stop at platforms. These types of incidents could be attributed to lack of concentration (inattentiveness).
The most recent incident was a SPAD in February 2014. Following this incident, the driver received a final written warning and was placed on a schedule of Train Driver Safety Audits (TDSA) and check rides.
Driver performance management
As a result of the SPAD in February 2014, (when considering the drivers prior history) V/Line issued the driver a final written notice as per V/Line’s Employee Misconduct and Discipline Procedure HRPR-33.
The driver was also required to undergo the following auditing process:
- Check rides
- 1 TDSA per month for the first six months then,
- 1 TDSA per three months for the following 12 months
Train Driver Safety Audits
V/Line Train Driver Safety Audits Policy states that:
Train Driver Safety Audits (TDSA) are aimed at ensuring that the functions associated with train driving are performed in accordance with the Book of Rules and Operating Procedures 1994, specified standards, Polices and all relevant Work Instructions and Procedures.
The policy also describes the following categories of Safety Audits as:
- Train Driver Safety Audit
- Train Drivers Safety Re-accreditation Audit
- Train Driver Promotion Assessment
- Trainee Train Driver Safety Validation
- Practical Driver Trainer Safety Audit
When considering the above categories of safety audits, the driver underwent a series Train Driver Safety Audits. The procedure explains it as:
Train Driver Safety Audit – Safety Audit conducted on all drivers that assumed the full responsibility of the position.
TDSA’s are used to monitor a drivers performance with regard to the functions associated with driving trains within the relevant rules and operation procedures on an annual basis (Train Driver Safety Audits).
Check ride
The driver underwent two separate check rides in March and April 2015 before undergoing the TDSA’s.
During the drivers first check ride over a return journey to Southern Cross Station, the auditor commented on the report that the driver;
An observation was if the driver is distracted in any way in the sense of talking on a phone or radio or having someone in the cab making conversation etc. It is my opinion that he may struggle to determine the sense of what situation he is in. i.e. speed restrictions, signals ahead at Stop, approaching platforms and how to prioritise tasks to keep the situation safe not only for himself but for others.
The second check ride was conducted over the period of two weeks. The auditor surmised in the report that;
The driver showed good concentration for all trips but I must comment that he did miss two warning boards without good reason and not centring reverser at signals after his previous misdemeanours with SPAD’s.
Train Driver Safety Audits regime
In the first 6 months all but one TSDA’s was supplied to the ATSB (June 2014 is missing).
For the following 3 months, TDSA between the month of October 2014 and June 2015 there was only one TDSA documented (June 2015). In that time, there should have been another TDSA’s sometime around February/March 2015.
The driver was currently undergoing the second phase of the TDSA regime in undertaking an audit every 3 months for the next 12 months (audits scheduled to finish around October 2015) at the time of the occurrence.
After reviewing the TDSA’s that were supplied to the ATSB none of the RDS’s undertaking the audits commented on any issues of performance such as losing concentration. In general, the driver performed without incident during the audits with the exception of a small non-conformance.
At the time of the occurrence at Wallan, the driver was still undergoing the TDSA/check ride process.
Reporting an incident
The driver of 8625 did not report the incident to (V/Line) Centrol[15] or the ARTC Network Control. The initial report to V/Line operations was made by the buffet attendant as a result of the minor injuries suffered to passengers.
Once V/Line operations became aware of the injuries, an internal notification was sent out via text to the General Manager for Train Services and relevant staff. However, even once the extent of the over speed was known, no one within V/Line Operations immediately contacted the ARTC Network Control to notify them of the over-speed at Wallan number three Points.
V/Line reporting procedure
V/Line procedure SAPR-33 Incident and Hazard Reporting defines a Rail Safety Incident as;
A circumstance, act or omission relating to rail infrastructure or operations that had the potential to result in the death or serious injury to any person, or significant damage to property. Includes:
- Any defect in, or failure of, any part of the rail infrastructure or rolling stock and/or
- Any failure or breach of any rail operations practice, procedure, or rule.
The over-speed at Wallan constituted a Rail Safety Incident as it breached the rule of entering into the loop on a low speed at 15 km/h.
For reporting Rail Safety Incidents SAPR-33 requires that;
To report a Rail Safety Incident on V/Line or Metro Infrastructure, contact Centrol immediately (at first safe opportunity) using train to base radio or telephone:
(Note: If an incident occurs in a network not controlled by V/Line. The incident should be reported to the infrastructure managers train control via train-to-base radio. The incident must also be reported to V/Line – either via Centrol or the Report a HSE incident online form).
ARTC TA20 Section 1 General Rules state;
Rule 6b; Conditions that can or do affect the safety of rail operations in the Network must be reported promptly to the Network Controller responsible for the affected portions of the track.
Train operators are to immediately notify infrastructure owners of any incident that can compromise the safety integrity of the network to the infrastructure owner. ARTC Emergency Management procedure, TA44 requires that once an operator becomes aware of an actual incident, they are to take all necessary steps to ensure that the incident site is protected and immediately contact ARTC Network Control to ensure the protection of the network.
Incident management
At the time of the occurrence the driver attempted to ‘down play’ the incident with the V/Line NCC for fear of reprisals and asked that the RDS not be notified. However, due to the excessive speed, the occurrence increased the safety risk in relation to the network (damaged track), potential damage to rolling stock, as well as possible passenger injuries. At the time, the driver was more focussed on trying to avoid any escalation of the incident and was less focussed on the issues such as damaged track rolling stock and passenger injuries.
The driver was spoken to on the platform at Seymour by the RDS to establish the cause of the rough ride. At the time during the conversations the RDS was determining the drivers demeanour and if the driver was affected by drugs and alcohol.
The RDS understood the complexities of removing the driver from service, locating a relief driver at short notice and the possibility of cancelling the service. The RDS also understood the track speed at Wallan Loop over the points.
The RDS, while anecdotally knowing the drivers past history, did not have access to the driver’s performance history with V/Line. While this RDS does not manage this driver, to be able to make an informed decision on the driver’s capacity to continue, it would have been advantageous to have had access to, or been provided with information about the driver’s history and ongoing performance issues at that time.
In hindsight, due to the severity (speed) of the incident, the effort in trying to conceal and ‘down play’ the incident, and the driver’s prior history, the RDS should have relieved the driver at Seymour regardless of the operational issue surrounding the cancellation of the service. However, the RDS was not comfortable in respect to the organisational pressures in making such a decision without a clear policy on relieving a driver for a gross over speed.
Driver fit to continue
There is no V/Line policy for RDS’s when dealing with performance issues such as a significant over-speed to relieve the driver. The Locomotive Driver Demerit OPPR-33 policy deals with the duty of an RDS to stand drivers down on the advice of an irregularity. However, in regards to standing down a driver as a result of an over-speed, it is not specific about how to deal with an over-speed greater than 21 km/h in relation to relieving a driver.
Passenger welfare
At the time of the occurrence, passengers were thrown around the carriage with some sustaining some bumps and scalding from hot drinks. Also traveling on the service was two high dependency passengers one of which was ejected from their wheelchair. The service crew administered first aid to those passengers that requested some assistance.
When the train was at Seymour, there was no communication between conductors (those joining and leaving the service), the RDS and V/Line NCC regarding passenger welfare or any further medical assessment or assistance.
Once the service had departed Seymour, the new conductor (now on the service) was approached by concerned passengers that were caring for high dependency person(s) with concerns.
Rolling stock fit to continue
The over-speed at Wallan over the points would have placed excessive lateral loads on the track and rolling stock. The excessive lateral load could have damaged the rolling stock or track (points).
At the time, the driver considered the train safe to continue because in the driver’s opinion the train felt normal after the event. Similarly, once the RDS and V/Line operations became aware of the excessive speed that the train traversed the points there was no consideration given to the state of the rolling stock to continue. It was not until the next day that the rolling stock was examined.
__________
- Distance in kilometres from a track reference point at Southern Cross Station.
- The name given to the gauge of track 1435mm wide between running rails.
- A length of track connected to the main line by switches at both ends to provide a facility that permits trains to both cross and pass each other.
- The name given to the gauge of track of 1600mm wide between running rails
- CTC – Centralised Traffic Control. A system of remotely controlling the points and signals at a number of interlocked stations, junctions and crossing loops in automatic signalling areas, from a centralised control or signal box.
- Dual control points - A power operated point machine also equipped for hand operations.
- 1 in 10 refers to the crossing rate of the turnout. The crossing rate is a measure of the angle made by the rail gauge faces at the theoretical point. The larger the crossing rate, the smaller the angle the faster the speed through the crossing.
- Driver-only operations do not have a second person in the cab.
- WLN/2 signal was showing a Red over Red over Yellow indication. The yellow is a low speed signal. At approach distance, the driver would only see the Red over Red signal as the yellow (low speed) is focused for a short range viewing of around 200 meters.
- Fixed red is a signal that can only show a red aspect (single position)
- Fireman is a term used for the second person/observer.
- Signals Passed At Danger
- Centrol is the V/Line train control centre.
The driver of 8625 tried to under report the severity of the occurrence. V/Line operations then contributed to the delay in notification as a result of operational impact to services. This also contributed to the delayed reporting to the network owner.
In the first instance, a timely notification to the network owner was delayed by the driver’s attempts to cover up and under report the occurrence. Once V/Line understood the extent (speed) of the over speed, there was still a delay in notifying ARTC train control as V/Line operations was more concerned with managing the relief of the driver, ensuring minimal impact to passengers travel, and containing the train at Benalla.
At the time, there was no consideration of the fit state of the rolling stock at the time. It was not until the return of 8625 the following day to Southern Cross Station was there an inspection of the rolling stock.
Reporting a Rail Safety Incident
ARTC Emergency Management procedure, TA44 requires that any responsible rail employee must immediately report any Rail Safety Incidents that can compromise the safety integrity of the network to the network owner.
V/Line policy SAPR-33 Incident and Hazard Reporting procedure requires that the driver communicate all safety matters that can compromise the safety of the network immediately to the effected network owner or V/Line operations. However, on this occasion the driver did not report it and instead tried to downplay the incident.
The driver not immediately report the severity of the over-speed to ARTC Train Control as required under procedure SAPR-33. As a result of not immediately reporting the incident, other services running on that section of track were expose to a potentially elevated risk.
V/Line reporting procedure
During the process of information coming from the field, the RDS, conductor, and train driver were reporting back to different people within V/Line operations. However, there was no coordinated communications to a central point within V/Line operations.
When a Rail Safety Incident occurs in V/Line territory, it is reported to V/Line train control (Centrol). V/Line train control assumes not only the train control function but also (in this case) coordinates any notifications process such as emergency services.
When a Rail Safety Incident occurs in non-V/Line territory, the assumption is that the driver has made the report to the affect network owner. Once the information has been passed on to Centrol, they then notify internal stakeholders, rail regulator, and the Australian Transport Safety Bureau.
Throughout the process of a notification of a Rail Safety Incident being reporting on a network other than V/Line’s, there is no step to ensure that the affected network owner has been notified.
V/Line does not have a procedure that ensures that the affected network owner is immediately notified of an incident (Rail Safety Incident) if the driver has not reported it.
Reporting by employee
V/Line SAPR-33 HSE Incident and Hazard Reporting Procedure states that any employee or sub-contractor must immediately report any Rail Safety Incident. The policy dictates that any Rail Safety Incident must be communicated through the train driver.
Conductor Emergency Procedures also states that any communications should go through the driver. Any delays or disruptions to services can be reported directly Network Customer Centre.
There is reference to an incapacitated driver whereby the conductor would contact NCC directly. However, there is no provision to make any contact with NCC if there is an immediately notifiable rail safety incident that the driver has not reported.
V/Line had no provision in place whereby service crew may take action in the event that a driver does not (or cannot) respond appropriately to a rail safety incident.
Reporting by Network Customer Centre (NCC)
V/Line have an NCC Incident Escalation Procedure OPPR-57 on the reporting and escalation of a safety incident. The procedure defines a serious incident and the communication protocol.
There is no specific requirement to ensure that the relevant network owner (ARTC) has been notified of a serious incident. By definition of the procedure OPPR-57, a safety issue that can affect the network is required by SAPR-33 and ARTC’s TA 44 to be immediately reported.
V/Line’s policy SAPR-33 requires that the driver is to inform the infrastructure owner regarding any incident as well as V/Line NCC. As a result of the non-reporting of the occurrence by the driver, ARTC Network Control was not immediately notified.
The ARTC Network Control was contacted on two separate occasions by V/Line operations and on the third occasion (75 minutes after the incident) was formally notified of the over speed event at Wallan.
Any incident the compromises the safety integrity of the network must be report directly to the infrastructure owners Train Control. As a result of the delay, a freight and inter-rail service had passed over the section of track (points) of the over-speed exposing the services to a potentially elevated risk.
Even after NCC was aware of the incident, there were no steps in place to ensure that ARTC was aware of the incident.
V/Line’s procedure OPPR-57 Cars (NCC) Office Escalation Procedure did not include a requirement to contact the infrastructure manager in the event that the assessed severity of an incident had escalated.
Rolling stock fit to continue
V/Line consideration of a gross over speed is in relation to the driver demerit points system (driver performance). As a result, V/Line did not understand the risk associated with a gross over-speed (greater than 21 km/h) when considering the rolling stock.
V/Line did not have an effective procedure in place to reduce the risk when dealing with the management of a gross over-speed incident. With no procedure in place the train was allow to continue on as the operational staff directly involved with the service could make a determination on how to best manage the incident.
As a direct result of having no procedure (guidance) and not considering the risk, V/Line allowed the train to continue. The result of allowing the train to continue exposed passengers and other network users to risk as the rolling stock had not been considered for its fitness to continue.
V/Line’s processes did not consider the potential for rolling stock damage in the event that a train had traversed a turnout at significantly greater speed than designed.
From the evidence available, the following findings are made with respect to the over-speed that occurred at Wallan Crossing Loop on the standard gauge 47 km north of Southern Cross Station by rail in Victoria, on 11 July 2015. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
- The driver of train 8625 did not demonstrate effective awareness and train handling techniques consistent with approaching a signal displaying a low speed aspect.
- Train 8625 traversed the points at a speed significantly greater than the engineering speed, contributing to the excessive lateral forces (rough ride) experienced by the passengers and crew.
Other factors that increased risk
- The driver did not immediately report the severity of the over-speed to ARTC Train Control as required under procedure SAPR-33. As a result of not immediately reporting the incident, other services running on that section of track were expose to a potentially elevated risk.
- V/Line does not have a procedure that ensures that the affected network owner is immediately notified of an incident (Rail Safety Incident) if the driver has not reported it.
- V/Line had no systems in place whereby service crew may take action in the event that a driver does not (or cannot) respond appropriately to a rail safety incident.
- V/Line’s OPPR-57 Cars (NCC) Office Escalation Procedure did not include a requirement to contact the infrastructure manager in the event that the assessed severity of an incident had escalated.
- V/Line’s processes did not consider the potential for rolling stock damage in the event that a train had traversed a turnout at significantly greater speed than designed.
Other findings
- All signalling associated with incident at Wallan Loop was tested after the incident and found to be working as per design with no signal sighting issues.
- The V/Line internal report determined that there was no pre-existing defect with the rolling stock that may have contributed to the rough ride.
- There was no pre-existing track condition evident that may have contributed to the rough ride.
Sources of information
The sources of information during the investigation included the:
- V/Line
- ARTC
- Emergency Service Telecommunications Authority (ESTA (000))
References
RISSB Glossary of Railway Terminology – Guidelines Vol 1 2010
Westinghouse Brake and Signal product information for Searchlight Signals Style K2 & K3
V/Line Just Culture Policy SAPO-10 14/1/2013
V/Line Locomotive Driver Demerit System Procedure OPPR-33
V/Line Train Driver Safety Audits procedure OPPR-15
V/Line Train Driver Safety Audits checklist OPFO-13 Rev10
V/Line Position Description for Conductors
V/Line internal report into the over-speed at Wallan 11 July 2015
V/Line Conductor Emergency Procedures Conductor Training May 2015
V/Line Employee Misconduct and Discipline Procedure HRPR-33 Rev 8
V/Line HSE Incident and Hazard Reporting SAPR-33
V/Line NCC Incident Escalation Procedure OPPR-57 Rev 2
V/Line memo; VPO386-Speed Restrictions on North East Standard Gauge
Turnout design and components. Robin Stevens Queensland Rail
TA20 Section 2 Fixed Signals 4 October 2015 Rev 2
TA20 Section 1 General Rules 4 October 2015 Rev 2
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Australian Rail Track Corporation, V/Line, the driver of 8625, and the Office of the National Rail Safety Regulator.
Submissions were received from Australian Rail Track Corporation, V/Line, the driver of 8625, and the Office of the National Rail Safety Regulator. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2017
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence
V/Line
V/Line have investigated and implemented the following short-term actions:
- The HSE Incident and Hazard Reporting Procedure (SAPR-33) has been revised and updated, and the online form for reporting incidents has also been revised to facilitate easy reporting. The Just Culture Policy (SAPO-10), which emphasises reporting responsibilities, was updated in July 2015 and Just Culture awareness and training will be conducted as part of the upcoming People Manager Induction and other Awareness training.
- An Incident Response Procedure providing a clear, documented process to assist in decisions about driver relief has been revised and is in place and an interim briefing process for interim response has been delivered and implemented into daily operations.
- HSE discussed this potential issue with People & Capability staff on 10th December 2015 to ensure that the principles of Just Culture are understood and that final warning communications are delivered clearly in accordance with these principles.
V/Line have investigated and are implementing the following longer term actions:
- The operational history of existing right of return drivers will be reviewed to identify any potential 'at risk' drivers (who will be subject to safety profiling and retraining as needed). NB. Review of drivers will be prioritised according to known incident history.
- Consideration of audible warnings for approaching signals and passing lanes in the business case for the Driver Advisory System. The V/Line Rollingstock department, has taken responsibility for this Project and a Project Nomination is being developed and funding is yet to be confirmed.
- V/Line and ARTC have held discussions regarding TPWS fitment and have agreed to work together on a train enforcement solution including TPWS. The Installation of TPWS on the North Eastern Line has been included in the Network Safety funding submissions that PTV has made to government.
- A review is currently underway to consider redundant reporting pathway(s) in the event that a driver fails to report an incident.
- V/Line’s Just Culture Implementation Procedure has been updated to reflect the criticality of appropriate incident reporting.
- A Rail Resource Management training program (named ‘Operational Awareness Training’) has been developed and is currently being rolled out to all staff in operational safety roles at V/Line to promote non-technical skills development.
- A formal on call process has been introduced to ensure the correct driver relief processes are followed after confirmed or alleged incidents and relevant staff have been briefed on their requirements when responding to such incidents.
- An internal review of potentially ‘at risk’ drivers has been undertaken and these are being monitored on a case by case basis as relevant.
- In relation to tracking driver development plans, a lead has been implemented for monitoring the current database to improve date tracking.
- A new Competence Management System for V/Line drivers is under development to support appropriate management of driver competence, including the management of non-technical skill deficiencies.