
History of the flight
The pilot hired a Beechcraft D55 Baron aircraft for travel associated with business commitments and submitted an instrument flight rules (IFR) flight plan from Bankstown to Warren and return. The flight to Warren proceeded normally. The pilot obtained an amended forecast before the return flight. The forecast indicated instrument meteorological conditions (IMC) for his arrival. Accordingly, he replanned via Bathurst in anticipation of an instrument arrival procedure to Bankstown.
The pilot departed Warren at 1628 ESuT and at 1705 reported 20 NM north west of Bathurst at 9,000 ft. That placed the aircraft inside controlled airspace without a clearance. The pilot was subsequently issued a clearance along the planned track. Approaching Bankstown the pilot encountered IMC and requested a Bankstown Radar Two arrival, anticipating a cloud break procedure from a radar vector. However, due to the missed approach flight path of that procedure conflicting with Sydney airspace requirements, the Sydney departures (west) controller, after determining that the pilot did not want the GPS approach, advised the pilot to expect a clearance for the Runway 11C Radar/Bankstown NDB/Sydney DME instrument approach. The pilot acknowledged the instruction. The approach controller subsequently observed the aircraft on radar to the right of the assigned approach track. He advised the pilot that he was right of track and cleared him to leave controlled airspace tracking to Bankstown along that procedure.
The pilot contacted Bankstown tower and advised that he was flying the Bankstown Runway 11C Global Positioning System (GPS) approach. The tower controller, who had been expecting the aircraft to be on a Runway 11C Radar/Bankstown NDB/Sydney DME approach, queried the pilot as to which approach he was using. The pilot confirmed that he was flying the GPS approach.
Recorded radar data showed that the aircraft had closely tracked the Runway 11C GPS approach path to a point 17 NM from Sydney, heading about 120 degrees at 2,500 ft. The aircraft then turned left to a heading of about 065 degrees and descended to 600 ft. The descent rate during that period was between 2,200 and 3,400 ft per minute. The aircraft then turned right to about 240 degrees and climbed to 1,100 ft. The minimum altitude for that segment of the approach profile was 1,400 ft. The Sydney departures (west) controller observed the aircraft on radar and advised the Bankstown tower controller. A short time later, the tower controller heard the transmission 'India Lima Mike emergency emergency'. Subsequent transmissions from the tower controller to the pilot went unanswered.
A witness, located approximately 2.5 km east of the accident site, reported seeing an aircraft pass overhead on a westerly heading with its engines surging before stopping. Other witnesses saw an aircraft apparently attempting to land in a nearby field. They described its approach as steep and slow. The aircraft descended into a grass-covered gully and impacted the ground. The impact collapsed the extended landing gear and the aircraft, although otherwise intact, was substantially damaged. The pilot, who was the sole occupant, received severe head and facial injuries.
Witnesses described weather conditions at the time of the accident as overcast with light rain falling and visibility estimated to have been between 3 and 5 km.
The pilot later stated that he had not previously flown a Runway 11C Radar/Bankstown NDB/Sydney DME instrument approach. Although he had acknowledged the controller's instructions for the approach to Bankstown, his intention had been to descend to the lowest safe altitude (LSALT) on that track and, if not in visual contact with the ground, to climb and divert to Bathurst. He reported that when he was not visual at 600 ft he commenced a climbing right turn onto a reciprocal track with the intention of diverting.
The pilot reported that after initiating the climbing turn onto a westerly heading, the left engine failed. He carried out the initial actions for engine failure but did not check the fuel selection at that time. He reported that checking the fuel selection was an item of his memorised trouble checks that in a multi-engine aircraft are performed after the initial actions and prior to feathering and securing the failed engine. However, before commencing the trouble checks the right engine failed and the pilot discontinued any further checks. He broadcast an emergency radio transmission and concentrated on controlling the aircraft. When clear of cloud, he manoeuvred the aircraft to avoid some towers and positioned the aircraft for a landing ahead, clear of houses and power lines.
The pilot later stated that he had intended to change from the auxiliary fuel tanks to the main tanks before commencing the approach. However, anxiety at having to fly an unfamiliar approach in IMC had distracted him and he had forgotten to change tanks. The pilot had not referred to either the approach or landing checklists that each included a check of the fuel tank selection.
Pilot experience, qualifications and recency
The pilot held a Commercial Pilot Licence and a valid Class 2 Medical Certificate. His Command Instrument Rating was endorsed for ILS, LLZ, VOR and NDB approaches. A log book entry on 24 May 1996 certified him as competent to use the GPS for en route navigation only. His total instrument flight time was 129 hours. No instrument flight time was recorded in the 90 days prior to the accident. His instrument rating renewal on 13 April 1999 had included an NDB approach. He had subsequently recorded an NDB approach, in flight, on 13 August 1999 and had made two practice NDB approaches in a ground procedure trainer on 20 September 1999. Recent experience requirements in Civil Aviation Orders Part 40.2.1 specified that the holder of a command instrument rating must not carry out an NDB approach in IMC unless in the preceding 90 days the holder has flown that type of approach either in flight or in a synthetic flight trainer.
At the time of the occurrence the pilot was operating under the privileges of a Command Instrument Rating (Multi-engine). On 10 March 2000 the Civil Aviation Safety Authority promulgated Civil Aviation Order 40.2.3 "Private IFR Rating" that allowed private pilots who had received appropriate training to fly in IMC under conditions less strict than those required for an instrument rating. The Private IFR Rating specified a flight review at intervals of two years. Civil Aviation Advisory Publication 5.13-1(0) Private IFR Rating recommended that recent experience requirements of the command instrument rating be used for guidance as to instrument flight time and instrument approaches.
The pilot had recorded 45.7 hours on the Beechcraft Baron type. His initial Baron endorsement training was undertaken in the B58 model but all his recent time on type was in the D55 model.
Fuel system and management
The D55 Baron fuel system consisted of a separate main and auxiliary tank in each wing. A selector for each fuel system was located on the floor between the front seats. The selector had four positions marked OFF, AUX, MAIN and CROSSFEED. A placard on the fuel selector directed pilots to use the auxiliary tanks in level flight only. The Pilot's Operating Handbook advised pilots to preplan fuel and fuel tank management before the actual flight and to utilize the auxiliary tanks only in level cruise flight. The last item of the descent checklist was "Fuel Selector Valves - MAIN".
Single fuel quantity indicators for both the left and right fuel systems were mounted on the pilot's lower panel. A toggle switch on the electrical sub-panel enabled selection of the quantity indication for either the main or auxiliary tanks.
The later model Beechcraft B58 Baron has a single tank in each wing, simplifying fuel selection and fuel quantity indication.
Wreckage examination
Examination of the wreckage did not reveal any pre existing defect that may have contributed to the accident sequence. There was no fuel in the auxiliary tanks. Approximately 170 litres of Avgas was recovered from the main tanks. The fuel selectors and the fuel quantity gauge switch were selected to the auxiliary tank positions. The wing flaps were not extended.
The aircraft was certified for IFR flight and was equipped with a GPS receiver that met the requirements for conducting GPS non-precision approaches. Documentation found in the wreckage included a set of current approach charts but the investigation was unable to determine which approach chart the pilot had used for the approach.
Shoulder harness attachment
The upper attachment of the pilot's shoulder harness failed during the accident sequence. The harness had no inertia reel and required manual adjustment. The pilot reported that he had been unable to adjust the shoulder harness as firmly as he desired. Examination of the upper attachment found that the installation was not in accordance with the approved modification and the bolt had pulled through the window pillar (see photos Fig. 1 and 2 below). The attachment for the right seat shoulder harness conformed to the approved modification.
Figure 1: Photograph of the failed shoulder harness attachment showing (above) where the bolt had pulled through the pillar.

Figure 2: Photograph of the bolt and harness end fitting.

Attachments for the shoulder harnesses had been installed in January 1973. This was carried out to comply with Airworthiness Directive AD /GENERAL/28 "Safety Belt and Harness Installations" that was issued in May 1972. The AD required an additional, single, shoulder strap to be fitted to the front cockpit seats of all Australian registered aircraft. The aircraft's logbook indicated compliance with the AD in accordance with an approved design drawing.
Figure 3: Cross-section through pilot's window pillar as appeared on the approved modification drawing.
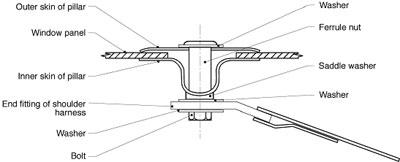
Figure 4: Cross-section through pilot's window depicting the installation as found on VH-ILM.
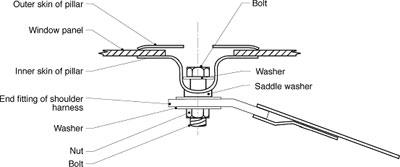
The investigation was unable to determine how and when this attachment was altered. Maintenance records showed that since modification the aircraft had been resprayed and the pilot's side window panel had been replaced. Either procedure may have required removal and reinstallation of the attachment. The attachment in the aircraft, as depicted in the diagram at Fig. 4, was significantly weaker than the approved method of attachment shown in the diagram at Fig. 3, thereby reducing the protection provided by the design. The fact that it was an incorrect installation may not have been apparent to maintenance personnel. The approved installation drawings were held by the organisation that originally performed the modification and were not readily available for reference by subsequent maintenance personnel.
Maintenance personnel normally referred to the illustrated parts catalogue for identifying correct components and assemblies. That catalogue, produced by the aircraft manufacturer, did not incorporate modifications by other than the aircraft manufacturer. As such, the modification of the shoulder harness installation did not appear in the catalogue. Approved maintenance data, as required under Civil Aviation Regulation CAR 2A, provided guidance as to the information and documentation required to assist licenced aircraft maintenance engineers (LAMEs) to carry out aircraft maintenance, including modifications.
Civil Aviation Regulation 50A entitled "Aircraft Log Book" stated in part;
"…the holder of the Certificate of Registration for an Australian aircraft must:
(a) keep a log book for the aircraft, and
(b) make the log book available, and other documents referred to in the log book, available to CASA and to persons engaged in maintenance on the aircraft…."
Investigation into a fatal floatplane accident at Calabash Bay, NSW on 26 July 1998 (Occurrence 199802830) also found incorrectly fitted seat belt attachments. The report noted that failure of these attachments might have contributed to the severity of injury to the occupants. In both the Calabash Bay accident and this occurrence, aircraft had been found to have been operated with incorrectly attached restraint systems.