
Executive summary
What happened
On 6 June 2023, the cabin crew of a QantasLink Boeing 717-200 aircraft, registered VH-NXM and operated by National Jet Systems, noticed a transient chlorine odour during the climb out of Sydney Airport, New South Wales. The cabin crew reported dizziness, mild discomfort described as pressure increasing in their head, and a metallic taste. The flight crew were advised, and the operator’s cabin air quality event procedure was completed.
About 76 minutes later, when the aircraft was on approach to Hobart Airport, Tasmania, the flight crew noticed a chlorine odour coming from the flight deck air-conditioning vents, lasting about 10 seconds. Shortly after, the captain noticed the onset of hypoxia-like symptoms and assessed themselves as unfit to continue as pilot flying.
The captain handed over pilot flying duties to the first officer and continued in the role of pilot monitoring for the remainder of the flight. The first officer, who was not experiencing any symptoms at that stage, continued the approach.
Shortly before landing, the first officer noticed that their reaction to an aircraft deviation was slowed and they started to experience cognitive difficulties. The landing was completed without further incident. After shutdown, both pilots reported a persistent headache, the captain also experienced ongoing symptoms of confusion and lethargy and attended a local hospital for medical tests.
What the ATSB found
The ATSB found that while the National Jet Systems’ cabin air quality events procedure captured the recording/reporting of odours, post-flight care of crew and maintenance actions, it did not consider the possible application of the smoke/fumes procedure or incapacitation procedure. As a result, there was an increased risk of flight crew being adversely affected by such an event during a critical stage of flight.
It was also identified that although National Jet Systems had procedures for recognition and management of pilot incapacitation, the associated training did not include the identification and response to subtle physical or cognitive incapacitation.
What has been done as a result
On 16 June 2023, National Jet Systems issued a Safety Action Notice (NJS-SAN-2023-018) reminding flight crews to consider supplemental oxygen use and the declaration of a PAN in response to a cabin air quality event.
On 2 March 2024, National Jet Systems advised the ATSB of the following safety actions taken as a result of this occurrence:
- The flight crew recurrent simulator training syllabus had been updated to include in‑seat instruction specific to pilot incapacitation, followed by a practical exercise donning oxygen masks and conducting an approach, landing, and taxiing to the gate while using oxygen.
- A review of smoke/fumes checklist and simulator training was undertaken.
- Learnings from this occurrence have been incorporated into the newly‑introduced company A220 aircraft smoke/fumes, hypoxia, and incapacitation procedures.
- A review of hypoxia training material to include specific reference to histotoxic hypoxia was undertaken, with draft content awaiting input from the Qantas chief medical officer.
- Aircrew emergency procedures documentation and training pertaining to the recognition and management of crew incapacitation have been updated to include subtle and cognitive incapacitation.
Safety message
Airborne contaminants may result in the rapid onset of incapacitation, which although possibly subtle, can significantly affect the safety of flight. Physical or cognitive incapacitation can occur for many reasons and may be difficult for others, or even the sufferer of, to detect and respond to.
Flight crews should therefore be alert to the potential hazards posed by odours and fumes and not hesitate to use supplemental oxygen. The use of oxygen is a proven mitigating action in the case of environmental hazards and its rapid use ensures flight crews’ physical and mental capacity is maintained.
The occurrence
On 6 June 2023, a QantasLink Boeing 717-200 aircraft operated by National Jet Systems as QF1541 and registered VH-NXM, was conducting a scheduled passenger flight from Sydney, New South Wales to Hobart, Tasmania. On board were the captain as pilot flying (PF), first officer as pilot monitoring (PM),[1] 3 cabin crew and 54 passengers.
The aircraft departed Sydney at about 1943 local time and during the climb, the 2 cabin crew members at the front of the cabin detected a strong chlorine odour in the area of the forward galley, which was unnoticed by the flight crew. The cabin crew advised the flight crew of the odour, and once established in the cruise, the captain sought further information in accordance with company cabin air quality event procedure. The forward cabin crew reported dizziness, a feeling of pressure in the head, and a metallic taste, but that the odour had gone, and the symptoms were not increasing. The cabin crew member at the rear of the aircraft reported no odours or symptoms and stated that none of the passengers had complained of odours or appeared to be experiencing discomfort. The 2 affected cabin crew assessed themselves as fit to continue the flight. As a result, the captain elected to continue the flight to Hobart.
At about 2108, about 10 NM from Hobart Airport (Figure 1) and at an altitude of about 4,000 ft, the captain noticed a chlorine odour, which they assessed as coming from the flight deck air‑conditioning gasper vents. The first officer noticed the odour shortly after the captain but neither the captain nor first officer experienced any effects at this time. The captain and first officer reported that the odour was transient and disappeared after about 10 seconds.
About 30 seconds later, while the flight crew were configuring the aircraft for landing[2] on runway 30, the captain noticed quickly developing adverse effects on vision, mental capacity, and movement, and self-assessed as unable to safely fly the aircraft. The captain later described the symptoms as fogginess of thought, confusion, deteriorating situational awareness, weakness and tingling in the arms and legs, and narrowing of vision. The captain indicated their intention to transfer control of the aircraft to the first officer by stating ’your controls’. At that time the first officer noticed that the captain looked pale but did not appear incapacitated.
Figure 1: VH-NXM track showing approach to Hobart Airport and key events
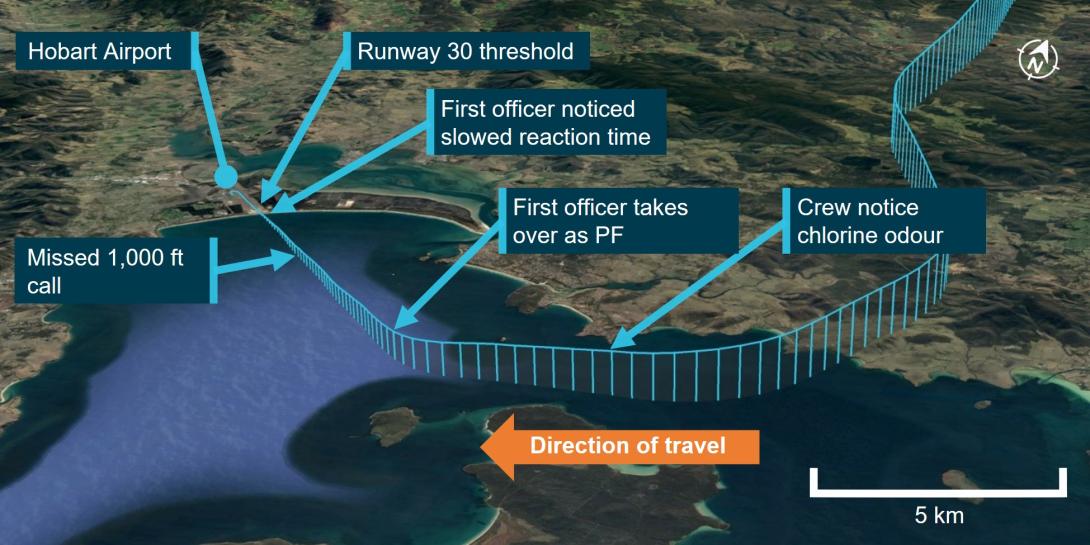
Source: Google earth and Flight radar. Annotated by the ATSB
When about 8.5 NM from the runway at an altitude of about 3,250 ft, the first officer took over the role of PF. At the same time, the captain communicated that they were able to continue as PM with the assistance of the first officer. The first officer noted that the captain correctly actioned the commands to lower the flaps and landing gear to configure the aircraft for landing. The first officer was not experiencing negative symptoms at that stage and, as the odour was not detectable, assessed that emergency oxygen was not required.
Shortly after, the first officer noticed that the captain was struggling to read the checklist and was tripping over words, but managed to self-correct and read back air traffic control calls correctly. The first officer visually monitored the captain’s condition and ensured that no inadvertent contact was made with the flight controls.
At about 3 NM from the runway and an altitude of 1,000 ft, the first officer noted that the captain, as PM, had not made the required ‘stable’ call to confirm the aircraft was stabilised on the approach. The first officer prompted the captain with a call of ‘1,000 feet’, and the captain responded with ‘stable’. The first officer confirmed that the aircraft was stable and continued the approach. The first officer considered making a PAN[3] call, but assessed it was unnecessary due to the immediacy of landing.
At about 100 ft above the runway elevation, the first officer experienced difficulties keeping the aircraft lined up with the runway centreline. The first officer reported that the aircraft was drifting to the right of the centreline, and that their reactions to correct the drift were slower than normal. The first officer also reported feeling ‘hazy’, however these difficulties were not communicated to the captain at that time.
At about 2113, the aircraft landed at Hobart Airport and was taxied to a parking bay. The flight crew was assessed by a company medical doctor via teleconference, during which the doctor observed that the captain’s speech was noticeably affected, consistent with impairment. This resulted in the captain attending hospital for further testing.
The 2 forward cabin crew later reported the same smell on landing and again both felt similar mild symptoms. The first officer also reported a dull headache post‑flight, which lasted about 2 days.
Context
Personnel information
Flight crew information
The captain and first officer each held an air transport pilot (aeroplane) licence with a multi-engine command instrument rating and a class 1 aviation medical certificate.
At the time of the occurrence, the captain had accrued 10,670 flying hours with 5,780 of those on the Boeing 717-aircraft type. The first officer had accrued 6,984 flying hours, of which 1,614 were on the Boeing 717-aircraft type.
Post-flight medical tests
Several samples of the captain’s blood were analysed after the event to identify exposure to any toxins. The initial blood sample taken several hours after the aircraft landed found the carbon dioxide (CO2) level was slightly elevated and carbon monoxide (CO) was within the normal range. A second sample taken about an hour later showed that the levels of CO and CO2 had reduced.
Due to the time between the event and the first blood sample, and the low levels of CO and CO2 measured, the blood test results were considered to be inconclusive. The presence of an elevated CO2 level indicated the possibility of exposure to that gas, but the time, magnitude and source of the exposure could not be determined.
The first officer attended hospital the next morning for precautionary blood tests, the results showed no elevated levels of CO or CO2.
Aircraft information
Aircraft air-conditioning and pressurisation system
On Boeing 717 aircraft, pressurisation and temperature control is achieved by using bleed air from both engines. The hot, pressurised air is cooled by 2 independent pressurised air-conditioning kits (PACKs) and distributed to the flight deck and cabin. Cabin pressure is controlled by a single out‑flow valve, which is automatically modulated to open to decrease cabin air pressure and closed to increase cabin air pressure as required throughout the phases of a flight (Figure 2).
Figure 2: Simplified Boeing 717 normal air distribution
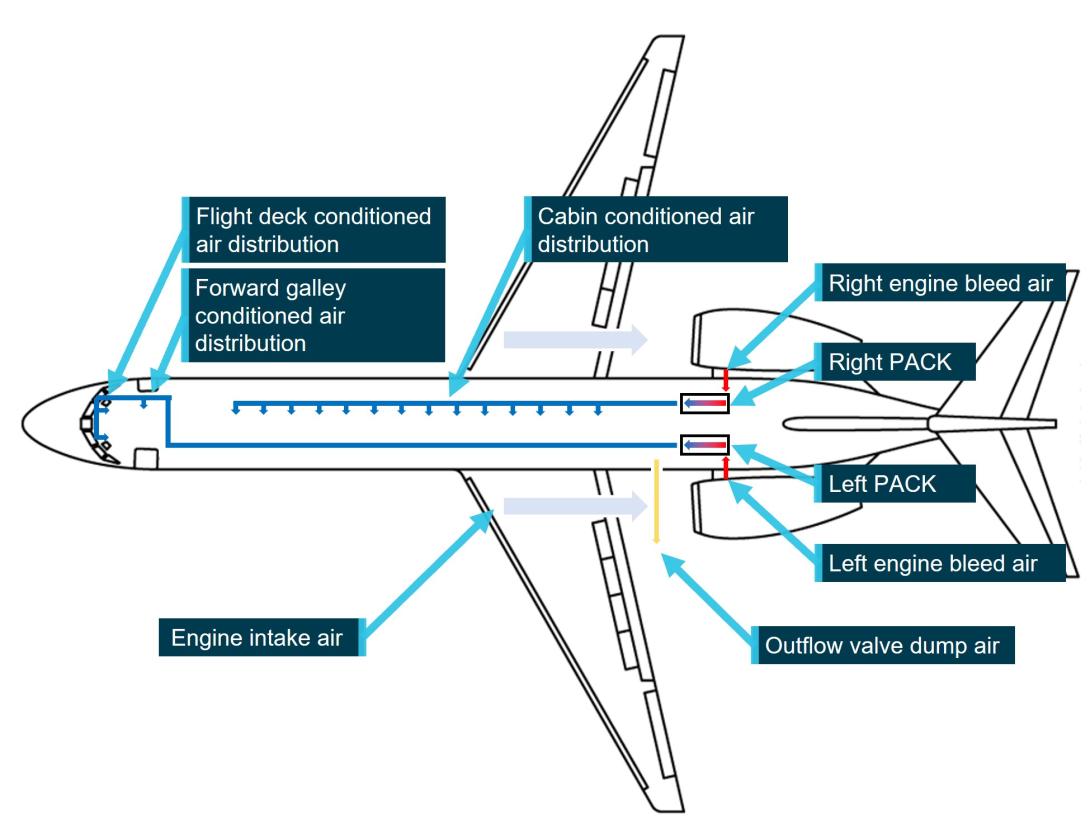
Source: Boeing. Modified and annotated by the ATSB
Typically, the left engine and left PACK are used to supply air to the flight deck and forward galley area, and the right engine and right PACK are used to supply the passenger cabin. Although, if required, either the left or right system can supply the air pressure and temperature control requirements of the entire aircraft.
The aircraft does not use recirculated cabin air, therefore air within the aircraft is completely replaced by the incoming air before being dumped overboard via the outflow valve. By controlling the flow of air through the outflow valve, the system regulates cabin air pressure throughout all phases of flight. In normal operation, pressurised air is sourced from the engine bleed air ducts, however for emergency operation, outside ram air can be selected to supply the PACKs which bypasses the engines and relies on aircraft forward movement to provide pressure.
Condensation is removed from the conditioned air by 2 independent water separators located at each PACK output manifold. Air entering the water separator is made to rotate by vanes in the inlet ducting. Centrifugal force causes the heavy water droplets to move to the outside of the separator and is collected by a coalescer bag and collector assembly, the water is then directed overboard, and the dry air continues through the system (Figure 3). The coalescer bags can be cleaned or replaced as required to prevent the build-up of contaminants and odours in the system.
Figure 3: Water separators
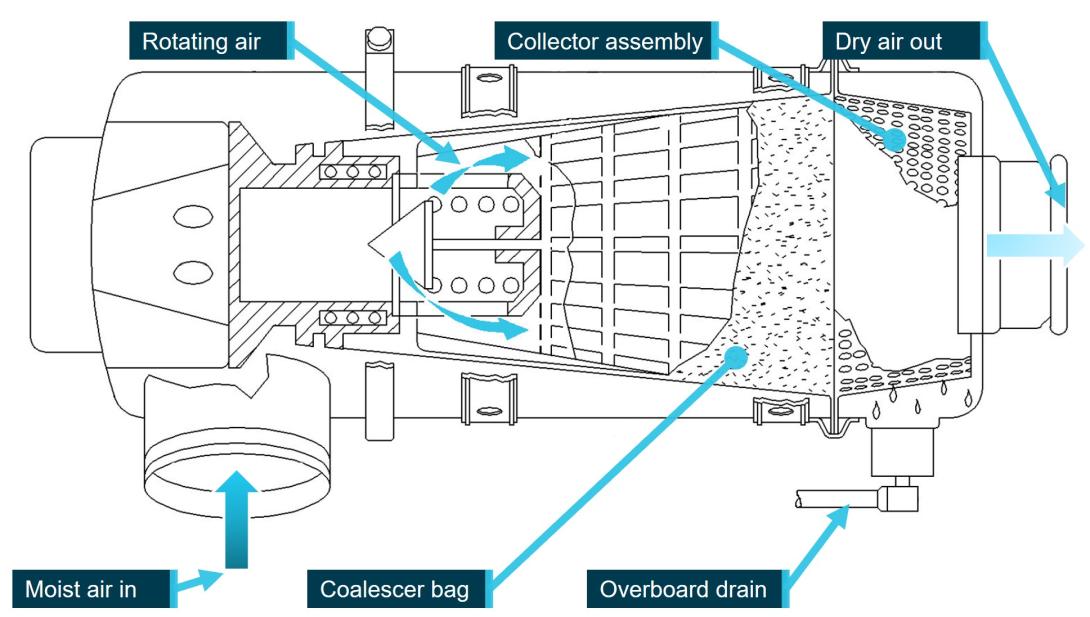
Source: Boeing. Modified and annotated by the ATSB
During normal operation, the system automatically controls aircraft air temperature and pressure to maintain the optimum environment inside the aircraft for comfort and safety. If required, the flight crew can manually control system temperature, airflow, and PACK bleed air source, as well as manually control aircraft pressurisation. In both manual and automatic modes, the system is protected from overheat or freezing by a series of temperature control switches and sensors.
On the incident flight, the air-conditioning and pressurisation system was operating in automatic mode, with the left PACK supplying the flight deck and forward galley area, and the right PACK supplying the passenger cabin and rear galley.
Aircraft supplementary oxygen systems
Crew emergency oxygen system
Supplemental oxygen systems are provided to supply breathable oxygen in the case that the aircraft air is not capable of supporting respiration, either due to loss of air (oxygen) pressure or environmental contaminants. They can also be used as first aid to maintain blood oxygen levels in the case of medical emergency.
The flight deck oxygen system supplies oxygen to the flight crew in the case of an emergency. The system consists of a pressurised oxygen cylinder, 3 full face masks – one located at each of the captain, first officer, and observer seated positions – and a distribution system. A single, high‑pressure gaseous oxygen supply cylinder supplies oxygen to all 3 flight deck masks.
The masks are located in stowage containers at each flight crew location. Removal of the mask from the container aligns supply valves and supplies oxygen to the mask. An inflatable harness ensures that quick donning is possible by a range of users. Integrated goggles afford protection to the eyes from smoke or other airborne irritants, and a regulator allows manual selection of oxygen supply modes for various requirements (Figure 4).
Figure 4: Flight crew oxygen masks
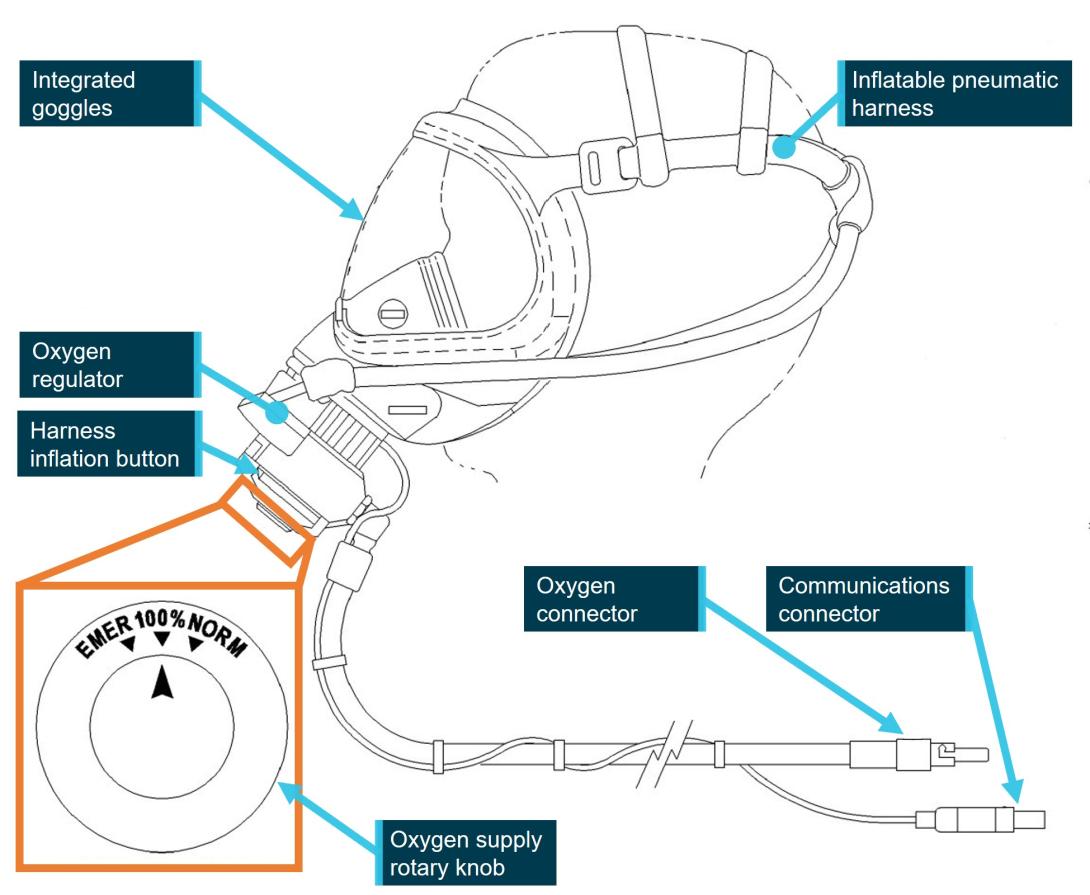
Source: Boeing. Modified and annotated by the ATSB
In an emergency, the pilot removes the mask from the container by grasping and pulling on the protruding regulator. The harness is inflated by squeezing 2 buttons on either side of the regulator, allowing the user to don the mask in a downward sweeping motion. Releasing the buttons deflates the harness and pulls the mask onto the pilot’s face resulting in an airtight seal between the mask and face. Oxygen supply mode is selected by way of a rotary knob on the front of the regulator to suit the emergency, and communication is enabled by an integrated dynamic microphone. The donning of the mask is designed to be completed quickly with one hand and without the need for further adjustment.
Additional portable oxygen systems, including breathing equipment, are located throughout the cabin and flight compartment, and are intended for use in medical emergencies or unexpected cabin depressurisation.
Flight crew procedures for oxygen system
Specific National Jet Systems policy and procedures for the use of supplementary or emergency oxygen by crews were dependent on the emergency.
Following a loss of cabin pressure at altitude, emergency oxygen was expected to be used promptly without the need to reference written procedures. The automatic, immediate response was required to ensure that the risk of hypoxia[4] was not realised, which might affect the flight crew’s cognitive ability and safety of flight.
Smoke, fire, or fumes on the flight deck also required an automatic response with regards to oxygen use, however the definition of smoke and fumes requiring a response rested with the flight crew’s judgement of the hazard. The procedure detailed in the Quick Reference Handbook involved the use of supplemental oxygen by the flight crew, descent to 9,000 ft, and the removal of the smoke or fumes by ventilation. National Jet Systems advised that that procedure was considered inappropriate for cabin air quality (CAQ) events (see the section titled Cabin air quality events) and it had never been used by their crews in response to a CAQ event.
The National Jet Systems Emergency Procedures Manual stipulated the administration of oxygen by a cabin crew member responding to a pilot incapacitation event, inferring that total incapacitation had occurred and the pilot was unable to apply oxygen themselves.
Lastly, the National Jet Systems B717 Pilot Handbook – Checklist procedures stated:
Crew oxygen masks must be donned and communications established when their use is required. This includes but is not limited to:
- Loss of cabin pressure.
- Prior to the discharge of any fire extinguisher in or near the flightdeck.
- Contamination, (smoke).
- The concentration of fumes or odours, either present or anticipated on the flight deck.
National Jet Systems' annual recurrent training in the use of oxygen in flight included both theory and practical assessments in the flight simulator. The training was designed to validate flight crews’ response to a loss of cabin pressure and smoke/fumes on the flight deck.
Crew use of oxygen
In this event, oxygen was not used by the cabin or flight crew. The cabin crew did not consider themselves incapacitated, and their symptoms were mild and short-lasting. During the in-flight discussion between the flight and cabin crew regarding the departure CAQ event, the captain reminded the cabin crew to use oxygen if their symptoms persisted.
The captain reported at the time they first experienced symptoms, they did not assess themselves as incapacitated and therefore there was no requirement for a go-around or declaration of a PAN, and that a go-around would have exacerbated the situation as it would have significantly extended the airborne exposure time. The captain reported that this was a CAQ event and although oxygen was available, they did not correlate flight crew use of supplemental oxygen with a CAQ event response.
At the time the captain handed over control of the aircraft, the first officer’s focus was on configuring the aircraft for landing, and the welfare of the captain. The first officer reported that they did not think oxygen was required considering the smell had ceased and symptoms were not being experienced. Further, the first officer did not consider that the captain was incapacitated as they were performing the pilot monitoring role, albeit with some prompting.
The crew reported that they had infrequently practised donning the mask during practical training. The captain further reported that in their last simulation, the mask tended to fog up, and that communicating was more difficult with it on.
The Qantas chief medical officer reported that the use of supplemental oxygen would have prevented further ingestion of any airborne contaminants present. Furthermore, had the contaminant been CO or CO2, use of oxygen was the only method able to provide rapid improvement in the crew’s condition.
Cabin air quality events
Sources of cabin air quality events
Modern aircraft air-conditioning and pressurisation systems are complex and involve significant variables in pressures, temperatures, and operating environments. Several major studies have been completed by authorities worldwide to assess the quality of cabin air and determine the source of contaminants. To date, the consensus is that aircraft cabin air quality is typical of indoor environments and considered safe. However, concerns have been raised about the possibility of contaminants which may contribute to long and/or short-term health effects. Cabin air contaminants are more likely to be detected during take-off or landing (EASA 2017).
In the 12 months preceding the incident flight, the operator recorded 28 CAQ events on Boeing 717 aircraft, 19 of which resulted in mild symptoms such as nausea, headaches, or irritated eyes or throat in the crew. Eleven of the 28 events involved reported odours during take‑off/climb and again during descent/landing. None of the recorded events affected safety of flight and were therefore categorised as innocuous by the operator.
Generally, and not specific to the Boeing 717 aircraft, known possible causes of CAQ issues include:
- engine oil introduced into the airpath by leaking internal engine or auxiliary power unit compressor seals
- hydraulic oil or exhaust gases introduced into the airpath from external aircraft sources
- dirty or defective water separator bags or components
- build-up of contaminants within the air-conditioning packs or ducting
- the use of aircraft cleaning or de-icing chemicals, inadvertently introduced into the airpath
- introduction of bio-effluents into the airpath in flight
- external environment airborne fumes, gases or pollution
- fumes from internal cabin or cargo compartment sources.
Routine inspections and maintenance of known sources of odours and fumes were conducted to reduce CAQ events. Additionally, these sources often guided the immediate action of maintenance crews in response to a CAQ event. However, the source of reported odours or fumes were often not determined.
Recent VH-NXM cabin air quality reports and maintenance
In the 6 days prior to the incident flight on 6 June 2023, maintenance records for VH-NXM documented other reports of cabin air quality issues (Table 1).
Table 1: VH-NXM CAQ events and maintenance
| Date | Flights | Defect | Maintenance Action |
| 1 June 2023 | 1 Flight | Forward and aft cabin crew report rotten garbage smell following application of take-off thrust, lasting 5 minutes. | Both coalescer bags replaced and cleanout of the high‑pressure ducting with auxiliary power unit bleed air carried out. |
| 1 Flight | No CAQ Issues | ||
| 2 June 2023 | 4 Flights | No CAQ Issues | |
| 4 June 2023 | 1 Flight | Chlorine smell was reported at the forward and aft galleys and the flight deck during take-off for between 3-5 minutes. Cabin crew reported mild symptoms (dizziness and shaking). The flight was diverted to Sydney. | System inspected for signs of oil leaks. Ground functional check carried out; no odours detected on ground. |
| 1 Flight | No CAQ Issues | ||
| 5 June 2023 | 2 Flights | No CAQ Issues | |
| 6 June 2023 | 1 Flight | No CAQ Issues | |
| Incident Flight |
In response to the incident flight, the following maintenance actions were completed:
- inspection of air conditioning/pressurisation system ducting and associated hardware for evidence of oil or other contaminants, or unserviceability
- inspection of both PACKs and water separator drain lines
- inspection and replacement of both PACK coalescer bags
- cleanout/burnout of pneumatic high-pressure ducting
- standard troubleshooting post cabin air quality event to locate sources of oil or hydraulic fluid that may have inadvertently entered the airpath
- ground testing and flight testing with particulate and air quality analysers onboard
- inspection of oil replenishment records to identify notable consumption or loss
- inspection of both aft toilet chemical injection systems.
The reported CAQ event could not be replicated on the ground or air by maintenance crews, therefore a definitive source of the chlorine odour was not determined.
National Jet Systems Cabin Air Quality events procedure
The National Jet Systems in-flight procedure in response to CAQ events was divided into 2 sections.
Section 1 was designed to record details of the event such as odour strength and description, time and duration of the event, and aircraft configuration at the time of the event. This was primarily intended to assist ground maintenance crews in the identification and rectification of faults during post-flight maintenance.
Section 2 was used in the case of reported crew or passenger physical symptoms resulting from the fumes event. This was to ensure post-flight medical care of crew and passengers if required, and to enable consistent recording of events and their impact on crew or passengers.
On the incident flight, both sections of the procedure were completed, and the operator was notified of the occurrence prior to arrival into Hobart.
Flight crew incapacitation
Symptoms and causes of incapacitation
Pilot incapacitation may be obvious or subtle, with symptoms ranging from total loss of function or consciousness to minor impacts on perception or executive function. Management of obvious incapacitation involves crew reacting to overt observable action or inaction. However, subtle incapacitation requires recognition of sometimes fleeting outward symptoms and reacting in a way that does not further degrade safety of flight (ICAO 2012).
The majority of reported pilot incapacitation events are caused by gastrointestinal upset, most commonly attributed to food poisoning (ATSB 2007). This type of incapacitation is characterised by clear outward symptoms and well-established responses by the crew.
Another source of pilot incapacitation is hypoxia. Hypoxia is caused by the interference in delivery of oxygen to the body. This can be the result of low oxygen pressure due to altitude, displacement of oxygen in the air by airborne contaminants, interference of oxygen in the blood due to toxins such as carbon monoxide, or restriction of blood flow due to rapid decompression, cold environment, or medical events (FAA 1991). The symptoms of hypoxia range, depending on the magnitude and speed of the source, from mild discomfort and subtle incapacitation to unconsciousness. In all cases the immediate application of supplemental oxygen will reverse the symptoms of hypoxia.
The symptoms of subtle incapacitation include degraded decision making, perception, awareness of surroundings, vision, motor control and coordination, concentration, behaviour, or memory. Symptoms can be fleeting or long lasting and difficult for others to detect; moreover, it is possible for the person experiencing the symptoms to be unaware of their presence.
This difficulty in detection is what constitutes the primary risk of this type of incapacitation, and as one of the first symptoms experienced affects cognition, it can be difficult or impossible for the person experiencing the incapacitation to recognise or respond to appropriately. Minor levels of incapacitation may be rationalised by the person suffering symptoms or by those observing; for example, difficulty maintaining altitude might be attributed to a lack of recent exposure to aircraft manual control (ICAO 2012).
Another consideration when discussing pilot incapacitation is the effect of stress on flight crews during a non-normal event, which is amplified if the event takes place during a critical stage of flight (NASA 2015):
Situational stress can adversely affect the cognition and skilled performance of pilots, as well as experts in other domains. Emergencies and other threatening situations require pilots to execute infrequently practiced procedures correctly and to use their skills and judgment to select an appropriate course of action, often under high workload, time pressure, and ambiguous indications, all of which can be stressful.
The Qantas chief medical officer asserted that the effect of stress can cause a physiological response (including hyperventilation) which is difficult to differentiate from symptoms caused by any external physical sources. In fact, the stress response itself can increase anxiety resulting in a feedback loop and severe distress for the sufferer, manifesting as physical incapacitation.
Flight crew procedures and training for crew incapacitation events
The National Jet Systems pilot incapacitation procedure involved the unaffected pilot using a cabin crew member to assist the flight crew by securing the incapacitated pilot in their seat and away from flight controls, and the application of first aid if required. The primary purpose of the procedure was to prevent inadvertent interference with the safe flight of the aircraft and to provide medical aid if necessary. The use of oxygen was stipulated in the context of first aid, if required.
Flight and cabin crews underwent recurrent practical training and assessment in the conduct of incapacitation procedures. Specific pilot incapacitation training at National Jet Systems was conducted at:
- Boeing 717 Command Upgrade Training (one segment dedicated to pilot incapacitation during a simulator session)
- annual practical emergency procedures training (one practical segment dedicated to pilot incapacitation, conducted with flight crew and cabin crew as a combined group, in an aircraft or synthetic trainer)
- initial and 4-yearly Boeing 717 Pilot Low Visibility Procedures Take-Off Training (one exercise dedicated to a pilot incapacitation event during take-off).
The National Jet Systems Aircraft General Operating Policy & Procedure, section 5.4.8 Flight crew/cabin crew incapacitation, stated:
When a Flight Crew member becomes incapacitated in flight, as a minimum, a PAN should be declared and the aircraft should be landed at the nearest suitable airport … Any apparent incapacitation of flight crew or cabin crew should not go unnoticed.
Flight crew members should be alert to the possibility of sudden or subtle incapacitation of an operating Flight Crew member, particularly during take-off and landing manoeuvres. To protect against subtle incapacitation, Flight Crew members are required to acknowledge supporting calls. Acknowledgement is normally the word “Checked”.
National Jet Systems’ training syllabus also included relevant recurrent human factors and threat and error management training.
Two communication rule
Modern passenger aircraft use 2-pilot crews to share workload and provide redundancy in an emergency. Duties are clearly defined and split between pilot flying (PF) and pilot monitoring (PM). While the PF and PM duties can be performed by the captain or first officer, the captain retains authority on the aircraft. However, safe operation relies on the first officer monitoring the captain’s actions and challenging or intervening if necessary.
Roles are clearly defined between the PF and PM, in part to ensure that a breakdown in the system can be quickly recognised. While the PM generally handles radio calls, checklists, and monitors the status of the aircraft and PF, the PF ensures that the PM completes the appropriate checklist, checklist items and radio calls, and the PF responds with an appropriate call, usually ‘checked’. This is known as the ‘two communication rule’ and is widely used because an error or absence of a call will quickly indicate a system problem, or issue with a flight crew member (ICAO 2012).
The two communication rule is reliant on a culture on the flight deck typified by a low flight deck authority gradient[5] and a high level of situation awareness. Understanding of what should be happening at any given phase of flight is critical to the effectiveness of the rule, the adherence to standard operating procedures is therefore a key component to enable crews to quickly identify subtle incapacitation in others (ICAO 2012).
The National Jet Systems B717 Pilot Handbook, Section 11.1.1 Standard Phraseology, stated:
… The absence of a standard callout at the appropriate time may indicate a malfunction of an aircraft system or indication, or indicate the possibility of incapacitation of the other pilot.
Similar occurrences
Between 2013 and 2023, the ATSB recorded 205 flight crew incapacitation occurrences, 7 were related to cabin air quality, of which 2 took place on commercial passenger jet aircraft.
The following are summaries of notable CAQ incident investigations.
United Kingdom Air Accident Investigations Branch Airbus A320-232 G‑EUYB 09-20
On 23 September 2019, the flight crew of an Airbus A320-232 detected an odour described as a sweaty sock smell while climbing through about 10,000 ft after departing Zurich Airport. The co‑pilot stated that they had experienced similar odours on the aircraft type before but described this instance as much stronger than previously experienced. The odour lasted about 30 seconds. The crew discussed options and elected to continue the flight; the flight crew's previous experience suggested that if the smell was going to reoccur it was most likely to occur when thrust was reduced for descent so, during the cruise, they discussed their actions if the smell returned and reviewed the SMOKE/FUMES/AVNCS SMOKE checklist.
The crew detected strong acrid fumes on the flight deck while on approach to London Heathrow Airport, United Kingdom. They enacted their plan and donned oxygen masks, declared a PAN, and completed the landing.
After landing, the copilot removed their mask to check for the continued presence of the odour. It was still present, so the flight crew shut down both engines, opened the flight deck windows, and started the auxiliary power unit. Shortly after, the copilot became nauseous and vomited out the flight deck window. A cabin crew member came onto the flight deck to assist and noted a chemical smell on the flight deck. They also confirmed that there were no smells or reports of illness in the cabin.
Both flight crew attended hospital, but results were not published.
The Air Accident Investigations Branch conducted a test of the aircraft air conditioner systems on the ground with engines, auxiliary power unit, and ground power. No odours or defects were identified. A comprehensive inspection and associated aircraft systems was carried out, and no sources of the fumes was identified.
The report concluded:
While it has not been possible to positively identify the compound that was responsible for the fumes and odours experienced in G-EUYB, or any of the other recent events, a number of common factors have been identified. The majority of events occurred after the aircraft had been parked or operated in precipitation. The fumes become apparent during the later stages of the descent, sometimes preceded by a minor event during the climb phase. The generation of fumes appears to be transient; they dissipate rapidly and leave no detectable trace. No link between changes to engine power or changes in other system settings and the generation of fumes was identified.
In some cases, the presence of fumes has resulted in physiological reactions which have interfered with a flight crew member’s ability to carry out their normal duties. However, by following the smoke and fume checklist, and donning oxygen masks the flight crew were able to ensure the continued safety of the aircraft.
French Bureau d’Enquêtes et d’Analyses (BEA) 2017-0658 Airbus A320 EC‑HQJ
On 17 November 2017, the pilots of an Airbus A320 complained of an unpleasant smell and irritations while taxiing behind a Cessna Citation prior to departure from Geneva-Cointrin Airport, Sweden. During the initial climb the crew experienced nausea and dizziness, which became progressively worse as the flight continued.
During the cruise, the captain donned their supplemental oxygen mask and reported an improvement of symptoms. A short time later, the first officer donned their supplemental oxygen mask due to worsening symptoms, a PAN was declared, and the aircraft diverted to Marseilles‑Provence Airport, France. The flight crew remained on oxygen for the remainder of the flight and landed without further incident.
Blood samples were taken, and tests showed no signs of carbon monoxide poisoning, but no other toxicological tests were carried out on the blood samples. Nausea and dizziness were reported for several days following. Hair samples were taken from the flight crew and analysed, but the analysis did not find substances in quantities corresponding to a one-off significant exposure in relation with the event.
Inspection of both aircraft involved identified no relevant defects or causes of contaminated air.
The reported concluded:
Despite the wide range of actions undertaken, the investigation was not able to factually identify what caused the flight crew’s symptoms and physical discomfort. The hypothesis of them having inhaled an excessive quantity of carbon monoxide, contained in exhaust gases emanating from the Cessna Citation which had been in front of the A320, is consistent with the information collected and can explain the symptoms observed (dizziness and nausea). Nitrogen oxide and sulphur oxide compounds present in exhaust gases may also have contributed to the acrid and irritating odours smelt while taxiing. However, it cannot be excluded that the crew were intoxicated by another substance which either quickly disappeared or which was not specifically searched for in the samples taken from the aeroplane as to date, not identified, even in the most recent studies.
Toxic substances were searched for in the hair samples using the most effective, innovative techniques to date. The BEA believes that the use of these techniques on matrices such as saliva, blood or urine, sampled as quickly as possible after the symptoms, and in particular as soon as possible after landing, would increase the chances of detecting a wider range of potentially toxic substances.
Swedish Accident Investigation Board RL 2001:41e BAE 146-200 SE-DRE
On 12 November 1999, the crew of a British Aerospace BAe 146-200 were scheduled to carry out 3 return flights between Stockholm and Malmö, Sweden.
During the first flight, a cabin crew member experienced a faint feeling. On the second flight cabin crew members experienced an odd pressure in the head, nasal itching, ear pain, and the feeling of ‘moon walking’. The issue was discussed with the pilots on both occasions, and on both occasions the pilots reported feeling no symptoms.
On the third flight, the cabin crew again reported discomfort similar to the preceding flights, but more pronounced. On descent to Malmö Airport, the copilot suddenly became nauseous and donned their oxygen mask. After about 10 seconds, the captain also became nauseous and donned their oxygen mask. After a few seconds on oxygen, the copilot started to feel better, however the captain’s condition continued to deteriorate. The captain reported feeling dizzy, and having difficulty with physiological motor response, simultaneity, and in focusing. The captain started to feel better after breathing oxygen for several minutes, and the landing was completed without further incident.
No medical examinations were performed after the incident.
A comprehensive technical investigation was conducted to attempt to determine a source of foul air. This included cabin air quality tests during test flights, bleed air analysis during a test run of an engine with an identified oil leak in an engine test cell, and dismantling and inspection of the engine. Despite these efforts, a definitive explanation for the incident was not identified.
The report concluded:
- Air samples taken during engine testing and aircraft test flights provided no indication of what/which chemical substances caused the symptoms.
- No technical fault that can explain the incident has been found.
- The location of the customer bleed port for the air-conditioning system is not optimal on the engine type.
- Knowledge is lacking concerning modern lubrication oils’ characteristics at very high pressure and temperatures and their effect on human health.
- Instructions are lacking concerning how crews shall act during flight when suspicion arises about contaminated cabin air.
Safety analysis
Introduction
During climb, the 2 cabin crew members in the forward galley smelt a chlorine odour and experienced associated mild symptoms, which abated after a short time, before returning again on landing. The air-conditioning system was in the normal configuration so that bleed air from the left engine and pressurised air-conditioning kit was distributed to the flight deck and forward galley, while the right side supplied the passenger cabin. Although left-side air was also being distributed to the flight deck, the flight crew did not detect odour during the climb. The crew treated the odour as a cabin air quality (CAQ) event and conducted the associated reporting actions.
Later in the flight, on approach to Hobart Airport, the flight crew noticed a chlorine odour and the captain experienced the rapid onset of symptoms of incapacitation, including cognitive impairment. The captain handed over pilot flying duties to the first officer and assumed the responsibilities of pilot monitoring.
Just before landing, the first officer reported feeling some symptoms of incapacitation but due to the proximity to landing and perceived difficulties of donning the oxygen mask, the first officer assessed that supplemental oxygen was likely to increase the risk to safety of flight. A go-around was considered, but the first officer assessed that continuing the landing was the safest overall course of action. Both flight crew members were partially incapacitated during the landing and subsequent taxi to the parking bay.
The odour and symptoms were consistent with that experienced earlier by the cabin crew, albeit with the flight crew experiencing more serious effects. The reason for the captain experiencing more debilitating effects slightly earlier than the first officer and for the cabin crew’s symptoms being subjectively milder, could not be determined. Whether a stress response to a non-normal situation in a high workload phase of flight exacerbated or contributed to the symptoms experienced by the flight crew on the incident flight was also not determined. The same aircraft had a reported CAQ event 2 days prior to the incident, in which cabin and flight crew smelt chlorine and only the cabin crew reported any symptoms, which were mild. Following the 6 June 2023 occurrence, maintenance engineers conducted an inspection of the aircraft to identify a source of the odours, none were found, and the event was not able to be reproduced on the ground or during a subsequent test flight.
Cabin air quality events procedure
Based on occurrences recorded by the ATSB and the aircraft operator, most CAQ events are short-lived and benign, with exposed crew experiencing no or mild symptoms. However, in rare cases the effects can be more serious and affect the safety of flight. Crew incapacitation may be partial or complete, and symptoms can range from the obvious, such as vomiting or loss of consciousness, to the subtle, such as mild cognitive impairment, or difficulty executing a task. In accordance with the operator’s procedures, the appropriate response depended on the extent of the effects experienced by the crew.
The history of reported CAQ events not impacting safety of flight likely influenced the intent of the operator’s CAQ event procedure, which detailed steps to report an event to assist in post-flight maintenance activities, and to assess an affected individual’s fitness to continue or return to duty. In response to the transient odour and symptoms reported during climb by the cabin crew, the flight crew completed the CAQ event procedure. Although the CAQ event procedure did not require consideration of supplemental oxygen, the captain reminded the affected cabin crew members to use supplemental oxygen if required. The CAQ event procedure did not require crews to consider actions in the event flight crews were affected by airborne contaminants.
The operator’s emergency procedure for smoke/fumes and the pilot handbook included that crew oxygen masks must be donned when concentration of fumes or odours were detected or anticipated on the flight deck. However, when the flight crew experienced the chlorine odour and more serious symptoms, they assessed it was a transient CAQ event rather than a fumes event and therefore were not required to use supplemental oxygen. Additionally, the captain’s first symptoms were likely cognitive impairment, which may have affected their judgement regarding the need for supplemental oxygen. If cognitive incapacitation is due to hypoxia or environmental contaminants, the window of opportunity to recognise and react to it can be very small before more significant cognitive effects impair decision making.
According to the operator’s medical officer, use of supplemental oxygen can have operational challenges but will not cause harm. Its use prevents further inhalation of contaminated air, preventing symptoms from worsening. In particular, it reverses the effects of hypoxia, including exposure to carbon monoxide and dioxide, and is also useful in the case of many medical emergencies.
National Jet Systems’ record of CAQ events showed 28 reported events in the 12 months prior to the incident flight, often during descent/landing preceded by events during take-off and climb. Eleven of the 28 events reported symptoms such as nausea/vomiting, headache, dizziness, or discomfort of the eyes and throat, but none of these effects impacted the safety of flight. The potential for a recurrence in the same flight was not considered in the CAQ event procedure. Additionally, the procedure did not include consideration of a CAQ issue leading to a fumes or incapacitation event.
As a result, the crew were unprepared for the subsequent fumes and incapacitation event, which occurred at a critical phase of flight, and did not use oxygen to significantly reduce the risk of both flight crew becoming partially incapacitated. The effectiveness of such preparation was demonstrated in a 2019 incident investigated by the United Kingdom Air Accident Investigations Branch. In that incident, following a mild transient CAQ event during the climb, the flight crew reviewed their smoke/fumes procedure, and discussed and planned to use oxygen if an event recurred. As a result, the flight crew quickly donned oxygen and declared a PAN when they detected fumes on approach.
Pilot incapacitation training
Multiple studies have identified gastrointestinal illness caused by food poisoning as the most common cause of pilot incapacitation. This finding has shaped pilot incapacitation training and procedures to ensure that the most prominent threat is adequately covered. The most salient features of food poisoning are obvious symptoms, the ability for the sufferer to communicate their distress, and ability to retain cognitive capacity. Training in recognition and response of pilot incapacitation has also been focused on the immediately hazardous effects of sudden and total incapacitation. The operator’s training in the use of supplemental oxygen for incapacitation focused on response to these events and did not encompass precautionary use of supplemental oxygen, or oxygen use during critical stages of flight.
The captain self-assessed as being unable to continue as pilot flying and handed over the duty to the first officer in accordance with the operator’s procedures, but did not communicate the severity of the difficulties experienced to the first officer. Although the captain knew and understood the symptoms and response to hypoxia, at the time, likely due to cognitive impairment, the captain did not recognise the hypoxia-like symptoms or identify supplemental oxygen as an appropriate response.
The National Jet Systems pilot incapacitation training focused on responding to overt or obvious incapacitation rather than the response to subtle incapacitation. The operator’s policy manual specified the flight crew’s absence of a standard call, or an acknowledgement of a standard call, as an indicator of pilot subtle incapacitation. In this case the first officer recognised that the captain had missed the stable approach call required at 1,000 ft altitude, and prompted the captain who then made the correct call.
Without the benefit of formalised training in the response to partial or cognitive incapacitation, and due to the absence of symptoms experienced by the first officer at that time, the first officer continued the landing without the use of supplemental oxygen. Additionally, the first officer assessed that the operator’s pilot incapacitation procedure and requirement to broadcast a PAN call were inappropriate in this event, as the captain was not completely incapacitated, and the aircraft was close to landing. While the proximity to landing limited the opportunity for the first officer to take any further action, the absence of training in management of subtle physical or cognitive incapacitation increased the risk of both flight crew members becoming impaired and unable to safely continue the flight.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the flight crew incapacitation involving Boeing 717-200, VH-NXM on approach to Hobart Airport, Tasmania on 6 June 2023.
Contributing factors
- The flight crew noticed a chlorine odour during the approach to Hobart Airport. Shortly after, the captain experienced the rapid onset of symptoms of incapacitation, resulting in them handing over pilot flying duties to the first officer.
- Just before landing, the first officer experienced symptoms of incapacitation, specifically slowed reaction time. Due to the impending landing, and perceived difficulties of donning the mask, supplemental oxygen was considered but not used. A go‑around was also considered but rejected following an assessment that continuing the landing was the safest course of action.
- National Jet Systems’ cabin air quality events procedure focused on the recording/reporting of odours, post-flight care of crew and maintenance actions. However, it did not consider the possible application of the smoke/fumes procedure, or incapacitation procedure. As a result, there was an increased risk of flight crew being adversely affected by such an event during a critical stage of flight. (Safety issue)
Other factors that increased risk
- Although National Jet Systems had procedures for recognition and management of pilot incapacitation, the associated training did not include the identification and response to subtle physical or cognitive incapacitation. (Safety issue)
Safety issues and actions
|
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
National Jet Systems cabin air quality event procedures
Safety issue number: AO-2023-026-SI-01
Safety issue description: National Jet Systems’ cabin air quality events procedure focused on the recording/reporting of odours, post-flight care of crew and maintenance actions. However, it did not consider the possible application of the smoke/fumes procedure, or incapacitation procedure. As a result, there was an increased risk of flight crew being adversely affected by such an event during a critical stage of flight.
National Jet Systems pilot incapacitation training
Safety issue number: AO-2023-026-SI-02
Safety issue description: Although National Jet Systems contained procedures for recognition and management of pilot incapacitation, the associated training did not include the identification and response to subtle physical or cognitive incapacitation.
Glossary
CAQ Cabin air quality
CO Carbon monoxide
CO2 Carbon dioxide
PACK Pressurised air-conditioning kit
PF Pilot flying
PM Pilot monitoring
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the flight crew
- National Jet Systems
- Qantas chief medical officer
- aircraft QAR data
- Boeing Aircraft Company
- Airservices Australia
- Bureau of Meteorology.
References
Australian Transport Safety Bureau. (2007) Pilot Incapacitation: Analysis of Medical Conditions Affecting Pilots Involved in Accident and Incidents. 1 January 1975 to 31 March 2006. B2006/0170
Dismukes, K., Goldsmith, T. & Kochan, J. (2015). Effects of acute stress on aircrew performance: Literature review and analysis of operational aspects. National Aeronautics and Space Administration. (NASA) Report: NASA/TM-2015–218930.
European Aviation Safety Agency. (2017) CAQ Preliminary cabin air quality measurement campaign. EASA_REP_RESEA_2014_4
Federal Aviation Administration. (1991) Civilian training in high altitude flight physiology (FAA) Report: DOT/FAA/AM-91/13
International Civil Aviation Organisation. (2012). Manual of Civil Aviation Medicine (3rd ed.) ICAO Doc 8984, Montréal.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the flight crew
- National Jet Systems
- Civil Aviation Safety Authority
- Boeing Aircraft Company
- Qantas chief medical officer
- United States National Transportation Safety Board
Submissions were received from:
- the incident flight captain
- National Jet Systems
- Boeing Aircraft Company
- Qantas chief medical officer
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. Terminology An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] Configuring for landing includes lowering wing flaps and slats, lowering landing gear and arming the speed brake.
[3] PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[4] Hypoxia: is a physical state where sufficient oxygen is not available for the body to sustain life either due to low blood oxygen levels, or inadequate blood supply to the body.
[5] Authority gradient: the authority relationship between the captain and first officer. For example, in the case of a domineering captain and an unassertive first officer, the gradient is considered high.