
Executive summary
What happened
On the morning of 5 January 2023, a British Aerospace BAE 146-200, registered VH-SFV and operated by Pionair Australia, operated a freight transport flight in darkness from Brisbane to Rockhampton, Queensland. After discontinuing a required navigation performance approach to runway 33 at Rockhampton because of low cloud, the crew conducted a missed approach and commenced a second approach at 0358 local time.
When commencing the second approach, the captain began descending the aircraft from 3,500 feet above mean sea level at the initial approach fix waypoint SARUS. Prior to crossing the intermediate fix at the waypoint BRKSI, the aircraft descended below the 3,000 ft segment minimum safe altitude (SMSA). The aircraft then continued descending on about a 3° profile and crossed BRKSI at 1,705 ft (1,295 ft below the SMSA) before then also descending below the next SMSA of 1,500 ft a few seconds later.
As the aircraft continued descending toward the minimum descent altitude, the flight crew recognised that the aircraft had descended below the SMSA and immediately commenced a missed approach. At about the same time, the ground proximity warning system activated.
What the ATSB found
The ATSB found that the captain commenced the second approach descent early based upon the incorrect application of their preferred regular descent technique but from a lower altitude. Additionally, the first officer did not identify the early descent due to an incorrect mental model of the aircraft's position in relation to the required flightpath. This led to the aircraft twice descending below segment minimum safe altitudes.
The ATSB also found that due to the time of the approaches and inadequate sleep, both flight crewmembers were likely experiencing a level of fatigue known to adversely affect performance. This, in combination with a period of high workload associated with the missed approach and second approach, led to the early descent and monitoring errors.
Finally, while the operator's flight crew rosters were compliant with applicable regulations and adequate sleep opportunities were available, the rosters were irregular and disruptive to the flight crew's sleep patterns which adversely impacted their ability to obtain adequate sleep prior to the incident flight.
What has been done as a result
Following the occurrence, the operator implemented several organisational, operational, and training changes including:
- the establishment of a fatigue safety action group
- a temporary reduction in total operational workload to reduce roster pressures and increase roster stability while training of additional flight crew was completed
- revisions to standard operating procedures to clarify actions and reduce workload during approaches
- revision of the training programs for flight management computer use during approaches.
Safety message
This incident illustrates the human factors implications associated with the combination of increased workload and the effects of fatigue.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported by industry. One of the priorities is improving the management of fatigue, which is the physical and psychological state typically caused by prolonged wakefulness and/or inadequate sleep.
Managing fatigue is a shared responsibility. This incident emphasises the importance of operators providing predictable and stable rosters to support pilots in achieving adequate sleep. Also highlighted, is the importance of pilots monitoring their own health and wellbeing to ensure that they are well-rested, especially when conducting overnight operations.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
At 0238 local time on 5 January 2023, a British Aerospace BAE 146-200, registered VH-SFV and operated by Pionair Australia, departed Brisbane, Queensland (QLD) for a freight transport flight to Rockhampton, QLD with 2 crewmembers on board.[1] The captain was acting as pilot flying, and the first officer was acting as pilot monitoring.[2]
At 0300, as the aircraft climbed through flight level 220,[3] air traffic control cleared the flight to track to the waypoint SARUS. This waypoint was the initial approach fix for the required navigation performance (RNP) approach for runway 33 at Rockhampton and the tracking allowed the crew to proceed directly from the cruise and descent to a straight-in RNP approach (Figure 1).
Figure 1: First approach

Source: Operator and Google Earth, annotated by the ATSB
At 0330, the aircraft crossed SARUS to commence the RNP approach for runway 33. As was the captain’s normal practice (see the section titled Crew approach techniques), the aircraft crossed SARUS at 4,980 ft above mean sea level while descending. The aircraft continued descending along the approach until reaching the 710 ft minimum descent altitude (MDA) for the approach. Upon reaching the MDA, the crew could not see the runway lights due to cloud and commenced a missed approach.
The crew carried out the missed approach, climbed to 4,500 ft and returned to the waypoint SARUS to prepare for a second approach (Figure 2). At SARUS, the crew conducted a holding pattern and descended to the minimum holding altitude of 3,500 ft. While conducting the holding pattern, the crew obtained updated weather information from ATC, reactivated the pilot-activated runway lights, completed an approach briefing and readied the aircraft for the second approach.
Figure 2: Flight path of first missed approach, holding and second approach
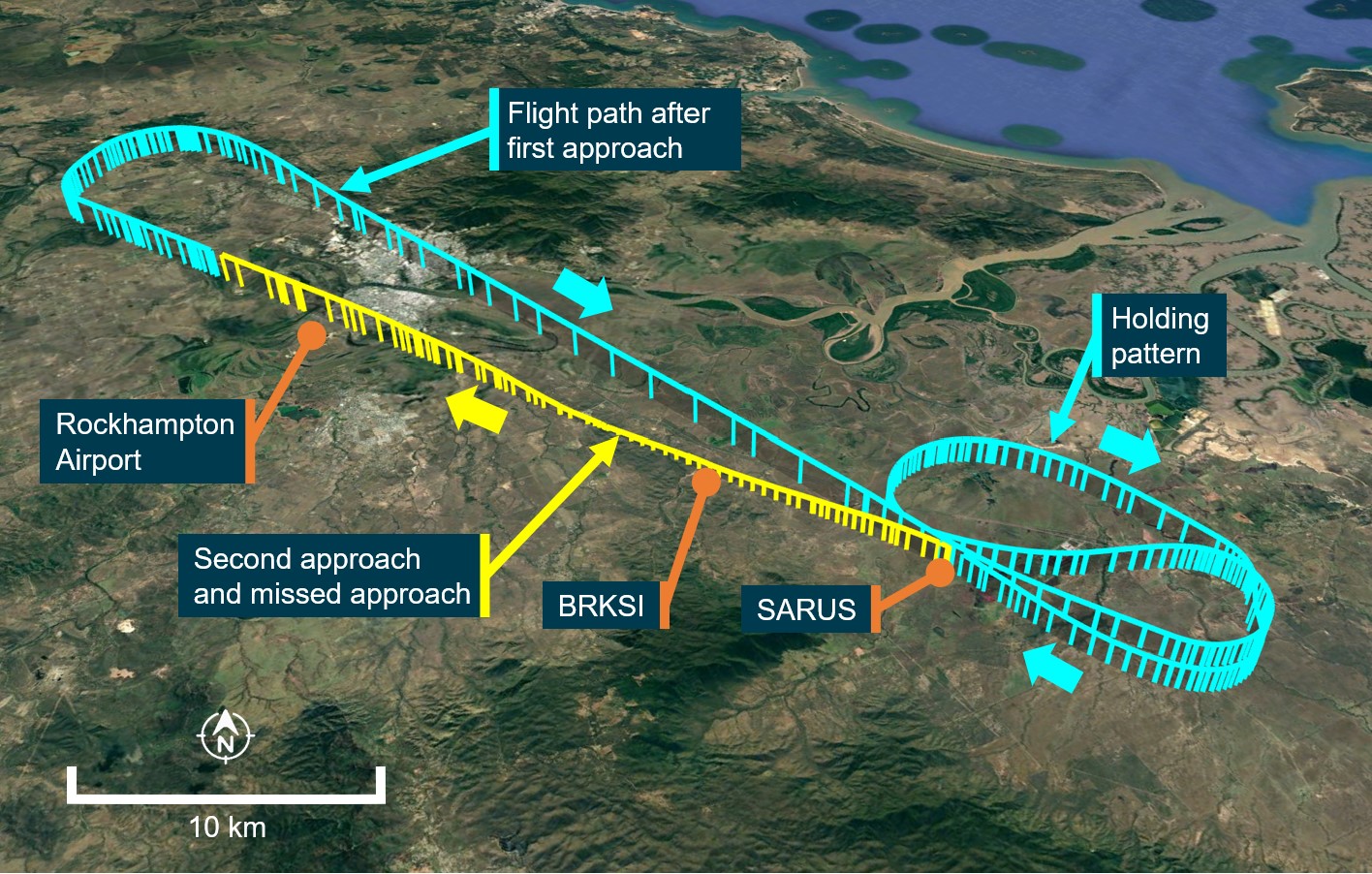
Source: Operator and Google Earth, annotated by ATSB
At 0358, the aircraft crossed SARUS at 3,500 ft to begin the second approach and, the captain applied their usual descent technique and commenced descending. At the same time, the first officer made a radio broadcast on the Rockhampton common traffic advisory frequency (CTAF). As the first officer was busy with the broadcast, the captain took on the pilot monitoring task of calling out the aircraft’s altitude and distance to run to the next waypoint (BRKSI).
After completing the radio calls, the first officer took over the pilot monitoring tasks and started to call out the altitude and distance to run, continuing from the captain’s previous callout but incorrectly believing that the aircraft had already passed BRKSI.
At 0358:55, prior to crossing BRKSI, the aircraft descended below the 3,000 ft segment minimum safe altitude (SMSA) (Figure 3). The aircraft continued descending on about a 3° approach profile and crossed BRKSI at 1,705 ft (1,295 ft below the SMSA) before then descending below the next SMSA of 1,500 ft, 24 seconds later at 04:00:56.
Figure 3: Rockhampton RNP runway 33 approach chart

Source: Airservices
As the aircraft continued descending toward the MDA, along a descent profile consistent with it being one approach segment further along than it actually was, the flight crew recognised that the ground lighting appeared different to the first approach and that distance measuring equipment indications were not as expected. In response, the first officer looked at the flight management computer and identified that the next waypoint was BRKSF, not the expected missed approach point, and immediately called for the captain to conduct a missed approach.
At about the same time, 0401:54, the ground proximity warning system generated a ‘terrain’ alert (see the section titled Ground proximity warning system). The crew then conducted a second missed approach. The minimum height recorded during the approach was 602 ft above ground level.
Following the missed approach, the crew diverted to Mackay, QLD and landed without further incident. The crew then completed a return trip to Rockhampton and Brisbane before completing their duty.
Context
Crew details
The captain held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. The captain had over 16,400 hours of flying experience, of which about 2,000 were on the BAE 146.
The first officer held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. The first officer had over 2,400 hours of flying experience, of which about 280 were on the BAE 146.
The first missed approach at Rockhampton was the first officer’s first missed approach in a BAE 146 aircraft (other than in a simulator).
Crew approach techniques
The crewmembers regularly operated from Brisbane to Rockhampton. When conditions favoured a runway 33 approach at Rockhampton, both crewmembers preferred to conduct an RNP approach by tracking straight in from the inbound track via SARUS.
When operating as pilot flying, the captain preferred to conduct a constant descent from the cruise segment to cross SARUS at about 5,000 ft above mean sea level while continuing the descent into the approach.
The first officer usually descended and levelled at 3,500 ft prior to crossing SARUS as this allowed additional time to configure the aircraft for the approach before continuing the approach descent from the waypoint BRKSI.
Both descent methods were consistent with the operator’s procedures.
Flight crew fatigue and workload
Crewmember sleep details
On the morning of 4 January, the captain and first officer completed a 9-hour duty together at 0445. Following this, the captain had about 2 hours of sleep and the first officer about 3 hours. In the evening, the captain had a further period of about 3 hours of sleep, waking at 2100 and the first officer about 2.5 hours before waking at 2130. On the previous day (3 January), the captain had about 4 hours of sleep while the first officer had about 7 hours. Therefore, at the commencement of duty at 0140 on 5 January, the captain had achieved about 9 hours of sleep in the preceding 48 hours, while the first officer had achieved about 12.5 hours.
Prior to 3 January, the captain had 2 days free of duties and the first officer had 11 days free.
Causes and effects
Civil Aviation Safety Authority (CASA) advisory publication CAAP 48-01 v3.2 Fatigue management for flight crew members provides a substantial amount of information on flight crew fatigue, sleep, workload, and the effects of sleep loss on performance.
The publication stated that the average adult needs between 7 to 9 hours of quality sleep per day to sustain normal performance and that obtaining sufficient, quality sleep during the optimum window for rest was essential. In the absence of sufficient sleep, the brain does not operate effectively and both concentration and decision making are negatively impacted. In addition, the effects of restricting sleep accumulate with pilots becoming progressively less alert and functional with each further day of sleep restriction. This is described as accumulating a ‘sleep debt’.
Insufficient sleep can lead to a deterioration in an individual’s processing speed and ability to maintain attention. More complex mental tasks, such as anticipating events, planning, and reacting to novel situations are also negatively impacted. These capabilities are critical to aviation safety, particularly during critical and high workload phases such as an instrument approach. Furthermore, once people are sufficiently fatigued, they are no longer able to reliably assess their own levels of fatigue, and consequently relying solely on self-assessment of fatigue can be flawed.
Additionally, the time of day can also have an impact on sleep and performance. Humans exhibit various predictable physiological and behavioural rhythms within a period of about a day known as circadian rhythms. These rhythms include periods of reduced alertness corresponding with the body temperature decreasing to its lowest level from 0300 to 0600 and, to a lesser extent, from 1600 to 1800. These circadian rhythms are synchronised to the solar day by external factors, the most important of which is the external light-dark cycle. Therefore, night work is particularly challenging, as it requires an individual to override the circadian rhythm to maintain adequate alertness.
The CASA advisory publication also emphasised the following with regard to flight crew duty rosters:
Operator guidance
Pionair’s operations manual included a Fatigue Management Policy which provided crewmembers with fatigue guidance and, in part, aimed to:
- ensure that crewmembers were aware of the accrual, and identification of (and need to address) fatigue that can arise from work and personal factors
- embrace a fair and just reporting culture to facilitate improvement of fatigue management understanding and procedures
- facilitate fatigue management rostering and practices that avoid disruptive roster patterns and minimise the risks associated with fatigued crewmembers, with the goal of having no flight operations on which crewmembers are fatigue impaired to the extent that safety is impacted.
This policy also stated the following with regard to determining personal fatigue level:
The policy also required a crewmember to notify the operator should the crewmember believe that because of fatigue they were not fit for duty. Fatigue management is also emphasised in CAAP 48‑01 as a shared responsibility between the operator and crewmembers.
Roster stability
Both crew members reported that inconsistent and varying rosters reduced their ability to achieve sufficient and good quality sleep. Prior to departure, the captain and first officer discussed the difficulty in obtaining sleep the previous day. The captain recalled feeling moderately tired, although neither crewmember reported feeling unfit for duty or felt the need to make a fatigue report prior to commencing duty.
The ATSB undertook an analysis of the operator’s rostering practices. This analysis included examinations of the rosters of the operating crew and a further 4 flight crew (2 captains and 2 first officers) and found the following:
- regarding maximum flight and duty hours, number of consecutive duties during window of circadian low, and minimum hours off-duty; all rosters assessed were compliant with Civil Aviation Order 48.1 as applicable at the time of the occurrence
- there was no pattern to the rosters and there was variability in terms of duty start times which was also evident during consecutive days of duty
- some duty start times were in forward rotation and some in backwards rotation[4]
- crew were not completing more duties than originally rostered, nor completing duties during standby periods
- almost all the recorded duty times varied from the published roster but in most cases did not affect maximum duty period or minimum off-duty periods.
Aircraft details
General
The BAE 146 is a 4-engine, high-wing, regional jet aircraft. VH-SFV was manufactured in 1987 and was configured for air freight operations (Figure 4).
Figure 4: VH-SFV

Source: ATSB
Instrumentation
The BAE-146 entered service in 1983 and was fitted with an analogue cockpit based upon technologies and ergonomic considerations of the time (Figure 5). When manufactured, VH‑SFV was not equipped with an integrated flight management computer (FMC) although one was later fitted to allow for operational practices introduced since the aircraft’s manufacture. The FMC fitted to VH-SFV included a lateral navigation function but did not include a vertical navigation function or vertical path protection. Management of the vertical profile of the approach using the autopilot was achieved using the vertical speed mode. In this mode, the PF used the control column to descend the aircraft and, once the desired descent rate was achieved, pressed a ‘sync’ button to enter the targeted vertical speed into the autopilot.
Figure 5: VH-SFV instrumentation
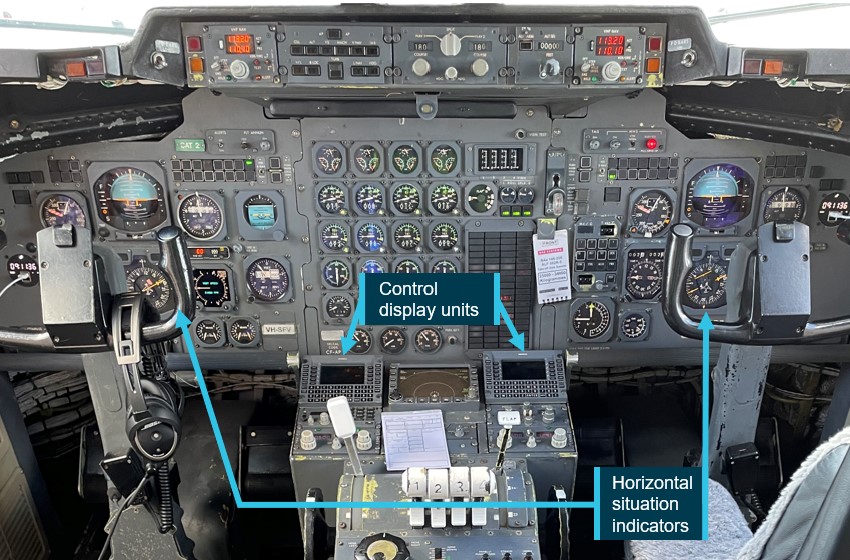
Source: ATSB
The control display units (CDU) of the FMC were positioned on the centre pedestal of the cockpit and allowed for the entry of navigation data. During an RNP approach, the FMC provided a waypoint distance to run indication on the horizontal situation indicator, but did not identify the waypoint name (Figure 6). Waypoint information, including the waypoint where the aircraft was tracking from and to, and the subsequent approach waypoint was displayed on the CDU screen (Figure 7).
Figure 6: Horizontal situation indicator display
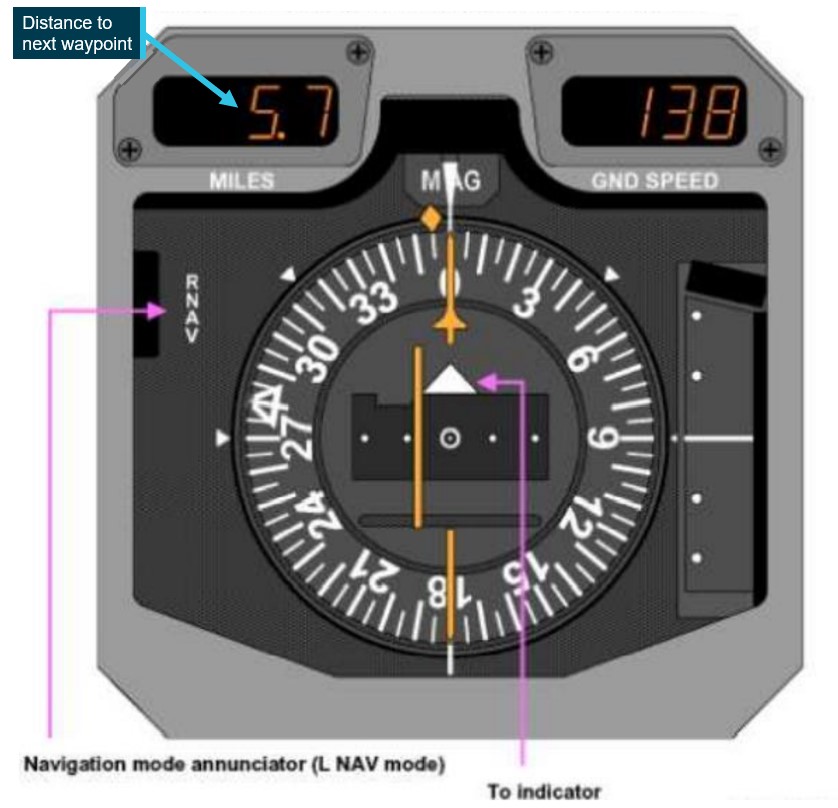
Source: Pionair Australia, modified and annotated by ATSB
Figure 7: Control display unit

Source: Pionair Australia
Ground proximity warning system
The aircraft was equipped with an enhanced ground proximity warning system (EGPWS). This system used aircraft inputs, including geographic position, attitude, altitude, and speed combined with internal terrain, obstacles, and airport runway databases to predict potential conflicts between the aircraft flight path and terrain or an obstacle. When a terrain or obstacle conflict was detected, the system provided a visual and audio warning alert.
Meteorology
Both approaches at Rockhampton were conducted in dark night conditions.
At 0336, the time of the commencement of the first missed approach, the Bureau of Meteorology (BoM) automatic weather station at Rockhampton Airport recorded the wind as 3 kt from 273° magnetic. Cloud cover was recorded: few[5] at 526 ft above mean sea level (AMSL) and scattered at 5,746 ft. Visibility was recorded as 23 km.
About 22 minutes later, at 0358, as the crew commenced the second approach, the station recorded the wind as 5 kt from 225° magnetic. Cloud cover was recorded as: few at 922 ft and scattered at 1,936 ft AMSL. Light rain had been recorded at the station in the preceding minute and visibility was recorded as 6,700 m.
Aerodrome weather information service
Rockhampton Airport was equipped with an aerodrome weather information service (AWIS), providing observations of meteorological conditions observed at the airport. These observations were available via telephone or air traffic control briefing. The Rockhampton AWIS was not available on a discrete radio frequency.
Rockhampton RNP runway 33 approach
Minimum descent altitude and missed approach requirements
For a 2-dimensional approach, to allow for the transition from descent to a level segment or missed approach without descending below the minimum descent altitude (MDA), the operator’s procedures required the addition of 50 ft to the 660 ft MDA. This provided a 710 ft MDA for the RNP approach in Rockhampton.
When the aircraft reached the missed approach point, if visual reference with the runway was not established (as occurred during the first approach), a missed approach was required.
Approach procedure chart
Airservices Australia and Jeppesen (an approved data service provider) published charts for the RNP runway 33 procedure. The charts produced by both organisations were designed and published in accordance with International Civil Aviation Organisation (ICAO) guidance.[6] The crew of VH-SFV used an electronic approach chart provided by Jeppesen, which was presented in dark mode for the night approach.
The Airservices Australia chart vertical profile presentation included the full approach, including the waypoint SARUS. This chart also included the minimum altitude of 3,500 ft at SARUS, the distance to the missed approach point of 15.3 nm (Figure 8) and the segment minimum safe altitude (SMSA) of 3,000 ft between SARUS and BRKSI. The Jeppesen chart (Figure 9) vertical profile commenced at waypoint BRKSI and did not include the waypoint SARUS, nor the SMSA between SARUS and BRKSI.
Figure 8: Airservices Australia RNP runway 33 approach chart
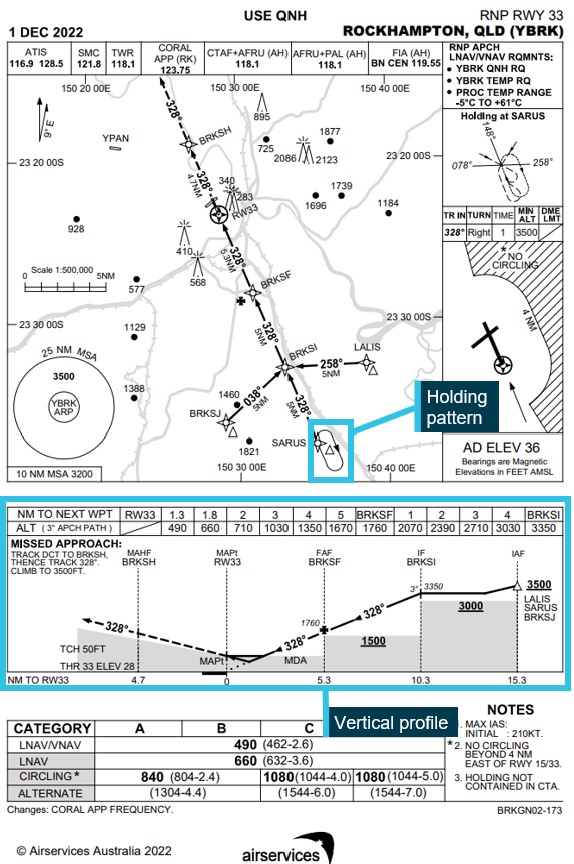
Source: Airservices, annotated by ATSB
Figure 9: Jeppesen RNP runway 33 approach chart (dark)
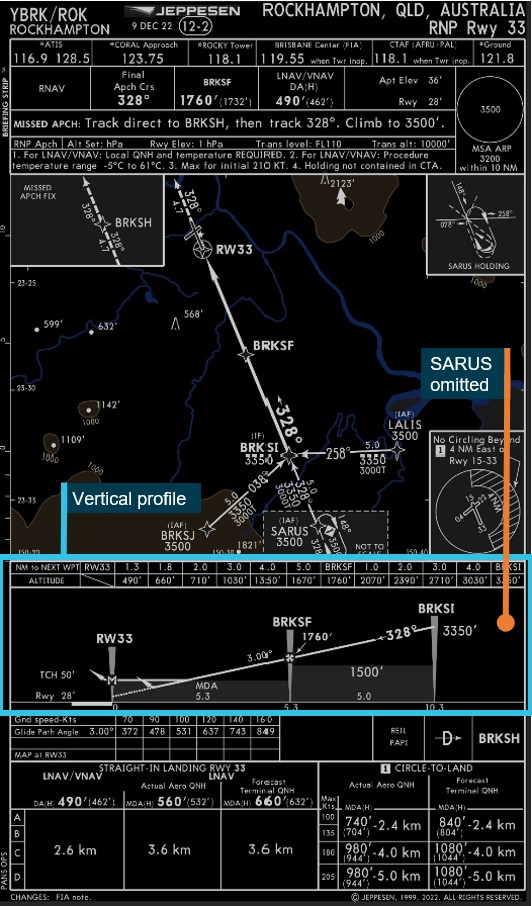
Source: Pionair Australia, annotated by ATSB
To provide a standardised presentation of aeronautical data for Jeppesen charts worldwide, Jeppesen chart design specifications directed that the vertical profile commence at the intermediate fix (IF) when an approach has multiple transitions. Jeppesen noted that this was the most common worldwide depiction of profile information. As the Rockhampton RNP approach had multiple transitions leading to the BRKSI IF, the vertical profile commenced at that waypoint.
Recorded data
Analysis of flight data from VH-SFV’s flight data recorder showed the descent profiles of the 2 approaches (Figure 10). The profiles show a similar descent angle, but with the second approach displaced by about 5 nm (1 approach segment).
Figure 10: RNP approach procedure showing the descent profiles of the 2 approaches
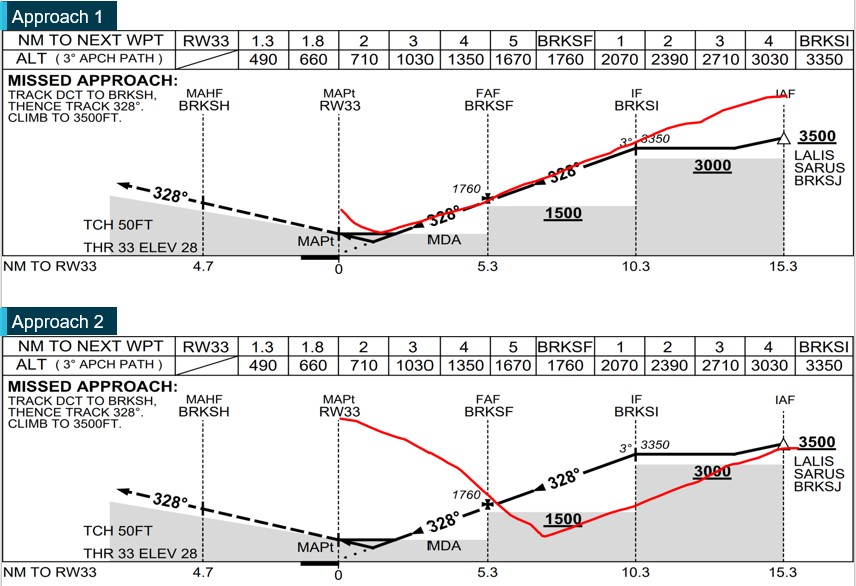
Source: Airservices and ATSB
Safety analysis
Early descent and error identification
After completing the first approach and missed approach, the crew completed a holding pattern to prepare for a second approach. The holding pattern provided a straight track to the initial approach fix SARUS, similar to the normal sequence for the crew when conducting a Brisbane to Rockhampton flight. The captain’s normal practice for this straight-in approach was to have the aircraft descending to cross SARUS at about 5,000 ft above mean sea level and to continue descending towards the next waypoint, BRKSI, while remaining above the 3,000 ft segment minimum safe altitude (SMSA).
On this occasion, following the missed approach and holding pattern, the aircraft crossed SARUS, and the captain immediately commenced descending as per their normal practice, but from the minimum holding altitude of 3,500 ft rather than their accustomed crossing altitude of 5,000 ft during a straight-in approach. This resulted in the aircraft incorrectly descending along a profile consistent with being one approach segment further along than its actual position.
As the aircraft descended along a normal descent angle, but one segment early, it twice descended below SMSAs. In dark night and cloudy conditions, this removed terrain and obstacle separation protections.
As the aircraft approached the minimum descent altitude, the different external sight picture and distance measuring equipment indications led the first officer to check the control display unit indications and identify that the aircraft was one approach segment behind their mental model of the approach and immediately call for a missed approach. At about the same time, the aircraft penetrated the ground proximity warning system warning envelope and a ‘terrain’ alert sounded.
The first officer’s normal practice when acting as pilot flying was to commence the approach from 3,500 ft at the waypoint after SARUS ‑ BRKSI. At the time of the descent of the second approach, the first officer’s focus was on completing radio broadcasts. While the first officer completed these broadcasts, the captain took over the callout and monitoring of descent distance and altitudes, temporarily removing the first officer from the approach monitoring task. When the first officer took over the task, they commenced monitoring the approach in the belief that the aircraft had already passed their preferred approach descent commencement point, BRKSI. Additionally, the next waypoint information was not immediately visible on the horizontal situation indicator and further contributed to the early descent error not being immediately recognised.
In addition, the Jeppesen approach chart used by both crews, while designed and published in accordance with ICAO guidance, did not include the waypoint SARUS or the SMSA for the SARUS-BRKSI segment on the vertical profile depiction. Although not considered contributory, this potentially limited the usefulness of the chart as an aid in enabling the crew to identify the early descent error.
Fatigue and workload
The approaches took place during the crew’s window of circadian low, a time of increased fatigue risk. Additionally, the crew were likely subject to an accumulated sleep debt resulting from the inability to get adequate sleep on the day prior to the incident as well as on the previous day. Both crew had also achieved less sleep than was considered adequate in Pionair’s fatigue management policy, particularly the captain. This sleep debt resulted in both flight crewmembers likely experiencing a level of fatigue known to adversely affect performance at the time of the approaches.
In addition, the second approach commenced during a period of high workload. The crew had completed one approach and a missed approach, the first in a BAE 146 aircraft (other than in a simulator) for the first officer. The crew then positioned the aircraft in the holding pattern and prepared for the second approach in dark and turbulent conditions. During the holding pattern, with Rockhampton Airport meteorological information not available via radio, the first officer obtained this information through air traffic control while also making the standard broadcasts to both air traffic control and on the common traffic advisory frequency. The aircraft’s analogue instrumentation and rudimentary autopilot systems also required significant input from the crew, further increasing the workload. The high workload, combined with the likely effects of fatigue, contributed to the early descent error made by the captain (as pilot flying) and to the first officer not immediately identifying the error (as pilot monitoring).
Stable rostering
The crews were operating night duties, which required sleeping during normal wakeful periods. This required the crew to adapt their sleeping patterns to match the available sleep opportunities. On the day prior to the occurrence duty, despite an adequate opportunity being available, both crewmembers were unable to obtain adequate sleep. The ATSB’s analysis of the operator’s rosters found that the rosters were irregular, unpredictable and that the duty hours operated were often inconsistent and varied from those rostered. This was disruptive to the crew’s sleep patterns and reduced their ability to effectively adapt to the available sleep opportunities, which in turn adversely impacted their ability to obtain adequate sleep prior to the incident flight.
Managing fatigue is a shared responsibility of the operator and crew. Part of this responsibility is the requirement of crew to self-report if they believe that they are unfit for duty due to fatigue. However, a known effect of fatigue is a reduction in an individual’s ability to accurately self-assess their fatigue level. This can reduce the effectiveness of crew self-reporting as a means of preventing crew from operating when fatigued, further reinforcing the need for stable and predictable rosters.
While the rostering practices increased the risk of the crew being unable to obtain adequate sleep, they were not considered contributory to the incident. Both the rosters and duties operated by the crews were found to be compliant with regulatory requirements. Furthermore, the time of the incident was generally associated with a reduction in human alertness and high fatigue risk, while also coinciding with a period of high workload following a missed approach and preparation for a second approach. Finally, the existence of other protections such as the ground proximity warning system alert were assessed as being effective in alerting the crew to the situation in sufficient time to take action.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the descent below minimum altitude involving British Aerospace BAE 146, VH-SFV, 15 km south of Rockhampton Airport on 5 January 2023.
Contributing factors
- Following a missed approach, a second approach descent was commenced early when the captain applied their regular descent technique, but from a lower altitude, while the first officer did not identify the early descent due to an incorrect mental model of the aircraft's position along the approach. This resulted in the aircraft twice descending below segment minimum safe altitudes.
- Due to the time of the approaches and inadequate sleep, both flight crewmembers were likely experiencing a level of fatigue known to adversely affect performance. This, in combination with a period of high workload associated with the second approach, led to the early descent and monitoring errors.
Other factors that increased risk
- While the operator's flight crew rosters were compliant with applicable regulations and adequate sleep opportunities were available, the rosters were irregular and disruptive to the flight crew's sleep patterns. This adversely impacted their ability to obtain adequate sleep prior to the incident flight.
Other finding
- As the aircraft descended toward the approach minimum descent altitude one approach segment early (prior to the final approach fix), the flight crew identified the error and commenced a missed approach. At about the same time, the ground proximity alert activated.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Safety action not associated with an identified safety issue
Proactive safety action by Pionair Australia
| Action number: | AO-2023-004-PSA-01 |
| Action organisation: | Pionair Australia |
Following the occurrence, the operator implemented the following organisational, operational, and training changes:
- a fatigue safety action group was established
- From 8 May to 17 July 2023, the operator temporarily reduced total operational workload to reduce roster pressures, increase roster stability and complete training of additional flight crew
- to reduce workload during required navigation performance (RNP) approaches, standard operating procedures were revised to require crew to configure the aircraft for landing, including completion of the landing checklist, prior to crossing the initial approach fix
- the BAE146 standard operating procedures manual section 'Decision at the Minima' was amended to include instructions for crew to state the following (as applicable): ‘When approaching the initial approach fix, cleared for the approach, and compliance with any altitude restriction is assured, set the altitude selector to the minimum descent altitude or decision altitude.’
- the operations manual instructions limiting multiple approaches to 2 was revised to include all operations (passenger and freight) and the guidance wording changed from ‘should’ to ‘shall’
- the operations manual was revised to clarify the guidance for temporary removal of flight crew from duty following an incident
- the simulator training program was revised to include use of the flight management computer during RNP approaches
- the flight training department revised the BAE 146 RNP approach ground theory training guidance for flying RNP approaches using the Universal UNS-1 Lw flight management system (as fitted to VH-SFV)
- guidance was distributed to all flight crew highlighting the absent initial approach fixes and total distance to the missed approach point information of Jeppesen RNP charts
The operator also advised that details of the incident will be disseminated to all flight crew and incorporated into training courses.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Pionair Australia
- the flight crew
- Civil Aviation Safety Authority
- Airservices Australia
- recorded flight data from VH-SFV
- Bureau of Meteorology
Reference
Civil Aviation Safety Authority 2020, Civil Aviation Advisory Publication 48-01 v3.2 Fatigue management for flight crew members.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Pionair Australia
- the flight crew
- Civil Aviation Safety Authority.
Submissions were received from:
- Pionair Australia
- Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The flight was operated under Civil Aviation Safety Regulations Part 121 (Air transport operations - larger aeroplanes).
[2] Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[3] Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 220 equates to 22,000 ft.
[4] A forward rotating roster is one in which shifts commence later on successive days. A backwards rotating roster is one in which shifts commence earlier.
[5] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky.
[6] International Civil Aviation Organization 2016, Aeronautical Chart Manual third edition, document 8697.